Mancuso, Gregory G. Dolnikowski, Ernst J. Schaefer and Daniel J. Rader K. Welty, Aisha Faruqi, Megan L. Wolfe, Chorthip Nartsupha, Andres G. Digenio, James P. John S. Millar, Margaret E. Brousseau, Margaret R. Diffenderfer, P. Hugh, R. Barrett, Francine B100 Metabolism in Humans Effects of the Cholesteryl Ester Transfer Protein Inhibitor Torcetrapib on Apolipoprotein Print ISSN: 1079-5642. Online ISSN: 1524-4636 Copyright © 2006 American Heart Association, Inc. All rights reserved. Greenville Avenue, Dallas, TX 75231 is published by the American Heart Association, 7272 Arteriosclerosis, Thrombosis, and Vascular Biology doi: 10.1161/01.ATV.0000219695.84644.56 2006; 2006;26:1350-1356; originally published online March 30, Arterioscler Thromb Vasc Biol. http://atvb.ahajournals.org/content/26/6/1350 World Wide Web at: The online version of this article, along with updated information and services, is located on the http://atvb.ahajournals.org/content/suppl/2006/04/02/01.ATV.0000219695.84644.56.DC1.html Data Supplement (unedited) at: http://atvb.ahajournals.org//subscriptions/ at: is online Arteriosclerosis, Thrombosis, and Vascular Biology Information about subscribing to Subscriptions: http://www.lww.com/reprints Information about reprints can be found online at: Reprints: document. Question and Answer Permissions and Rights page under Services. Further information about this process is available in the which permission is being requested is located, click Request Permissions in the middle column of the Web Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for can be obtained via RightsLink, a service of the Arteriosclerosis, Thrombosis, and Vascular Biology in Requests for permissions to reproduce figures, tables, or portions of articles originally published Permissions: by guest on February 18, 2014 http://atvb.ahajournals.org/ Downloaded from by guest on February 18, 2014 http://atvb.ahajournals.org/ Downloaded from by guest on February 18, 2014 http://atvb.ahajournals.org/ Downloaded from by guest on February 18, 2014 http://atvb.ahajournals.org/ Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Mancuso, Gregory G. Dolnikowski, Ernst J. Schaefer and Daniel J. RaderK. Welty, Aisha Faruqi, Megan L. Wolfe, Chorthip Nartsupha, Andres G. Digenio, James P.
John S. Millar, Margaret E. Brousseau, Margaret R. Diffenderfer, P. Hugh, R. Barrett, FrancineB100 Metabolism in Humans
Effects of the Cholesteryl Ester Transfer Protein Inhibitor Torcetrapib on Apolipoprotein
Print ISSN: 1079-5642. Online ISSN: 1524-4636 Copyright © 2006 American Heart Association, Inc. All rights reserved.
Greenville Avenue, Dallas, TX 75231is published by the American Heart Association, 7272Arteriosclerosis, Thrombosis, and Vascular Biology
doi: 10.1161/01.ATV.0000219695.84644.562006;
2006;26:1350-1356; originally published online March 30,Arterioscler Thromb Vasc Biol.
http://atvb.ahajournals.org/content/26/6/1350World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://atvb.ahajournals.org/content/suppl/2006/04/02/01.ATV.0000219695.84644.56.DC1.htmlData Supplement (unedited) at:
http://atvb.ahajournals.org//subscriptions/
at: is onlineArteriosclerosis, Thrombosis, and Vascular Biology Information about subscribing to Subscriptions:
http://www.lww.com/reprints
Information about reprints can be found online at: Reprints:
document. Question and AnswerPermissions and Rightspage under Services. Further information about this process is available in the
which permission is being requested is located, click Request Permissions in the middle column of the WebCopyright Clearance Center, not the Editorial Office. Once the online version of the published article for
can be obtained via RightsLink, a service of theArteriosclerosis, Thrombosis, and Vascular Biologyin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on February 18, 2014http://atvb.ahajournals.org/Downloaded from by guest on February 18, 2014http://atvb.ahajournals.org/Downloaded from by guest on February 18, 2014http://atvb.ahajournals.org/Downloaded from by guest on February 18, 2014http://atvb.ahajournals.org/Downloaded from
Effects of the Cholesteryl Ester Transfer Protein InhibitorTorcetrapib on Apolipoprotein B100 Metabolism in Humans
John S. Millar, Margaret E. Brousseau, Margaret R. Diffenderfer, P. Hugh R. Barrett,Francine K. Welty, Aisha Faruqi, Megan L. Wolfe, Chorthip Nartsupha, Andres G. Digenio,
James P. Mancuso, Gregory G. Dolnikowski, Ernst J. Schaefer, Daniel J. Rader
Objective—Cholesteryl ester transfer protein (CETP) inhibition with torcetrapib not only increases high-density lipoproteincholesterol levels but also significantly reduces plasma triglyceride, low-density lipoprotein (LDL) cholesterol, andapolipoprotein B (apoB) levels. The goal of the present study was to define the kinetic mechanism(s) by which CETPinhibition reduces levels of apoB-containing lipoproteins.
Methods and Results—Nineteen subjects, 9 of whom were pretreated with 20 mg atorvastatin, received placebo for 4weeks, followed by 120 mg torcetrapib once daily for 4 weeks. Six subjects in the nonatorvastatin group received 120mg torcetrapib twice daily for an additional 4 weeks. After each phase, subjects underwent a primed-constant infusionof deuterated leucine to endogenously label newly synthesized apoB to determine very low-density lipoprotein (VLDL),intermediate-density lipoprotein (IDL) and LDL apoB100 production, and fractional catabolic rates (FCRs). Once-daily120 mg torcetrapib significantly reduced VLDL, IDL, and LDL apoB100 pool sizes by enhancing the FCR of apoB100within each fraction. On a background of atorvastatin, 120 mg torcetrapib significantly reduced VLDL, IDL, and LDLapoB100 pool sizes. The reduction in VLDL apoB100 was associated with an enhanced apoB100 FCR, whereas thedecreases in IDL and LDL apoB100 were associated with reduced apoB100 production.
Conclusions—These data indicate that when used alone, torcetrapib reduces VLDL, IDL, and LDL apoB100 levelsprimarily by increasing the rate of apoB100 clearance. In contrast, when added to atorvastatin treatment, torcetrapibreduces apoB100 levels mainly by enhancing VLDL apoB100 clearance and reducing production of IDL and LDLapoB100. (Arterioscler Thromb Vasc Biol. 2006;26:1350-1356.)
Key Words: very low-density lipoproteins � triglyceride � low-density lipoproteins� cholesteryl ester transfer protein � CETP inhibition � lipoprotein kinetics
An elevated level of plasma cholesterol is a major riskfactor for the development of cardiovascular disease.1
Current treatments to reduce plasma cholesterol levels in-clude diet, exercise, and treatment with cholesterol-loweringmedications.1 Recently, a new class of drug designed toincrease high-density lipoprotein (HDL) cholesterol levelsthrough the inhibition of cholesteryl ester transfer protein(CETP) has been developed.2 CETP mediates the bidirec-tional exchange of cholesteryl ester and triglyceride betweenHDL and the apolipoprotein B (apoB)–containing lipopro-teins, as well as among the different classes of apoB-containing lipoproteins. The main result of CETP activity isnet transfer of cholesteryl ester from HDL to very low-density lipoproteins (VLDLs) and net transfer of triglyceridefrom VLDL to HDL. Thus, CETP provides a link between themetabolism of apoB-containing lipoproteins and HDL. Ex-
pression of CETP in mice,3 which normally lack CETP, ormanipulation of CETP activity in other animals that expressCETP4,5 changes the plasma concentration of apoB-containing lipoproteins in addition to expected changes inHDL cholesterol (HDL-C). In humans, CETP inhibitors notonly raise HDL-C but also result in a significant reduction intriglyceride and low-density lipoprotein (LDL) cholesterollevels.6,7
We reported previously the effects of a CETP inhibitor,torcetrapib, on plasma lipoproteins in subjects selected forlow HDL-C (�40 mg � dL�1).8 In these subjects, torcetrapibtreatment resulted in a dose-dependent increase in HDL-Cand reduction in triglyceride and LDL cholesterol (LDL-C)levels. We conducted kinetic studies to define the mecha-nism(s) by which torcetrapib, alone or on a background withthe 3-hydroxy-3-methylglutaryl–coenzyme A reductase in-
Original received August 17, 2005; final version accepted March 16, 2006.From the Institute for Translational Medicine and Therapeutics (J.S.M., A.F., M.L.W., D.J.R.), University of Pennsylvania School of Medicine,
Philadelphia; Lipid Metabolism Laboratory (M.E.B., M.R.D., F.K.W., C.N., E.J.S.), JM-USDA-HNRCA at Tufts University, and Tufts-New EnglandMedical Center, Boston, Mass; Schools of Medicine and Pharmacology (P.H.R.B.), University of Western Australia, Perth, Australia; Division ofCardiology (F.K.W.), Beth Israel Deaconess Medical Center, Boston, Mass; Clinical Research and Development (A.G.D., J.P.M.), Pfizer, Inc., Groton,Conn; and Mass Spectrometry Laboratory (G.G.D.), JM-USDA-HNRCA at Tufts University, Boston, Mass.
Correspondence to John S. Millar, PhD, 644 BRB II/III, 421 Curie Blvd, Philadelphia, PA 19104. E-mail [email protected]© 2006 American Heart Association, Inc.
Arterioscler Thromb Vasc Biol. is available at http://www.atvbaha.org DOI: 10.1161/01.ATV.0000219695.84644.56
1350 by guest on February 18, 2014http://atvb.ahajournals.org/Downloaded from

hibitor atorvastatin, influences lipoprotein and apolipoproteinmetabolism. We reported previously that torcetrapib slowedthe rate of clearance of apoA-I in plasma.9 Here, we report theeffects of torcetrapib on the metabolism of VLDL,intermediate-density lipoprotein (IDL), and LDL apoB100 inhumans.
MethodsSubjectsSubjects were recruited at the University of Pennsylvania, Philadel-phia, and Tufts-New England Medical Center, Boston, Mass. Sub-jects met the following eligibility criteria: age between 18 to 70years, HDL-C of �40 mg � dL�1, triglycerides �400 mg � dL�1,LDL-C �160 mg � dL�1, and a body mass index between 18 and 35kg � m�2. Subjects having an LDL-C of �160 mg � dL�1 whilestabilized on 20 mg atorvastatin for a minimum of 4 weeks wereeligible to participate in the atorvastatin arm of this study. The studyprotocol was approved by the human investigation review commit-tees of each institution, and informed, written consent was obtainedfrom each participant.
Experimental DesignThe study was a placebo-controlled, fixed-sequence crossover designstudy. A total of 19 subjects were enrolled, with 10 subjects in thenonatorvastatin group and 9 subjects in the atorvastatin group. Adetailed description of the study design, depicted in Figure 1, hasbeen reported previously.8,9 All subjects received placebo for 4weeks, followed by 120 mg torcetrapib once daily for an additional4 weeks. Six subjects from the nonatorvastatin group also partici-pated in a third phase, in which they received 120 mg torcetrapibtwice daily for 4 weeks.
At the end of each 4-week phase, subjects underwent a primed-constant infusion of deuterated leucine under constantly fed condi-tions to determine the kinetics of apoB100.10 At 11 AM, [5,5,5-2H3]-L-leucine (10 �mol � kg body wt�1) was injected intravenously as abolus followed by a continuous infusion (10 �mol � kg bodyweight�1 � hr�1), over a 15-hour period. Blood was collected atselected time points over the 15-hour infusion period as described.9
Plasma Lipid and Lipoprotein DeterminationsAll laboratory personnel were blinded to the treatment phase. Bloodsamples for lipid and lipoprotein analyses were collected fromsubjects after a 12- to 14-hour fast into tubes containing EDTA.Plasma LDL-C levels were measured directly with the use of areagent kit (Genzyme Diagnostics). Plasma HDL-C levels weredetermined after dextran sulfate-magnesium precipitation of apoB-containing lipoproteins.11 Total cholesterol, LDL-C, HDL-C, andplasma triglyceride levels were determined using enzymatic meth-ods12 standardized through the Centers for Disease Control (Atlanta,Ga). Lipid composition on lipoprotein fractions isolated by sequen-tial ultracentrifugation was measured using enzymatic reagents for
total and free cholesterol, triglyceride, and phospholipids (WakoChemicals USA).
Lipoprotein subclass concentrations were determined by protonnuclear magnetic resonance spectroscopy conducted on plasmasamples (LipoScience). For the present study, LDL subclasses weredefined as follows: large (21.3 to 23.0 nm), medium (19.8 to 21.2nm), and small (18.3 to 19.7 nm).
Quantitation and Isolation of ApolipoproteinsVLDL, IDL, and LDL were isolated by sequential ultracentrifuga-tion. Fasting plasma apoB levels were measured on a Cobas Fara II(Roche, Inc.) with an immunoturbidimetric assay using reagents andcalibrators from Wako Diagnostics (Wako Chemicals USA). Non-fasting apoB levels were measured using an apoB ELISA.13 LDLapoB was calculated as the difference between plasma and VLDLplus IDL apoB. ApoB100 was isolated from VLDL, IDL, and LDLby SDS-PAGE using a Tris-glycine buffer system as describedpreviously.14 The proportion of apoB within the triglyceride-richlipoprotein fraction that was B100 and B48 was determined bydensitometric scanning of Coomassie-stained gels.
Determinations of Isotopic EnrichmentApoB100 bands were excised from polyacrylamide gels, hydrolyzedin 12N HCl at 110°C for 24 hours, and amino acids converted toN-heptafluorobutyramide derivatives and analyzed as describedpreviously.9,15
Kinetic AnalysisThe kinetics of VLDL, IDL, and LDL apoB100 were assessed usinga previously described multicompartmental model.16 The SAAM IIprogram was used to fit the model to the observed tracer data andVLDL and IDL apoB100 concentration data using a weightedleast-squares approach to determine the best fit. ApoB100 pool size(PS) in each fraction was computed as: PS (mg)�apoB100 concen-tration (mg � dL�1) � plasma volume (0.45 dL � kg�1 bodyweight) � body weight (kg).
ApoB100 production rate (PR) in each fraction was calculatedusing the formula: PR (mg � kg�1 � day�1)�[fractional catabolic rate(FCR; pools � day�1) � PS (mg � pool�1)] � body weight (kg�1).
One subject in the nonatorvastatin group that also participated inthe 120 mg twice daily phase of the study had unsatisfactory tracerenrichment data. The tracer data for this subject were not modeled,and all data for this subject were excluded from the kinetic dataanalysis.
Statistical AnalysesBecause of the relatively small sample sizes used in the study, anonparametric approach to data analysis was chosen. The Wilcoxonmatched-pair signed-rank test (single paired comparisons), con-ducted with the Intercooled Stata 8.2 for Windows program (Stata-Corp), was used to assess differences between the placebo and 120mg once daily drug phase within a given group. The Friedman test(multiple paired comparisons), conducted with GraphPad Prismversion 3.00 for Windows (GraphPad Software), was used to assessdifferences among drug phases in subjects enrolled in both the 120mg once daily group and 120 mg twice daily group followed byDunn’s test to detect individual differences post hoc. A 2-sided Pvalue of �0.05 was considered statistically significant. The percent-age change between torcetrapib and placebo phases was computedfor individual subjects. Multiple regression was conducted withIntercooled Stata 8.2 for Windows using a backward stepwiseapproach. All data in the text and tables are presented as median(25th percentile to 75th percentile). Analyses were conducted on thefull set of subjects in each group unless otherwise indicated.
ResultsPlasma LipidsChanges in plasma lipids in these subjects treated with 120mg torcetrapib once daily have been reported previously8 and
Figure 1. Flow chart depicting the design of the study.
Millar et al Effects of CETP Inhibition on ApoB100 Metabolism 1351
by guest on February 18, 2014http://atvb.ahajournals.org/Downloaded from
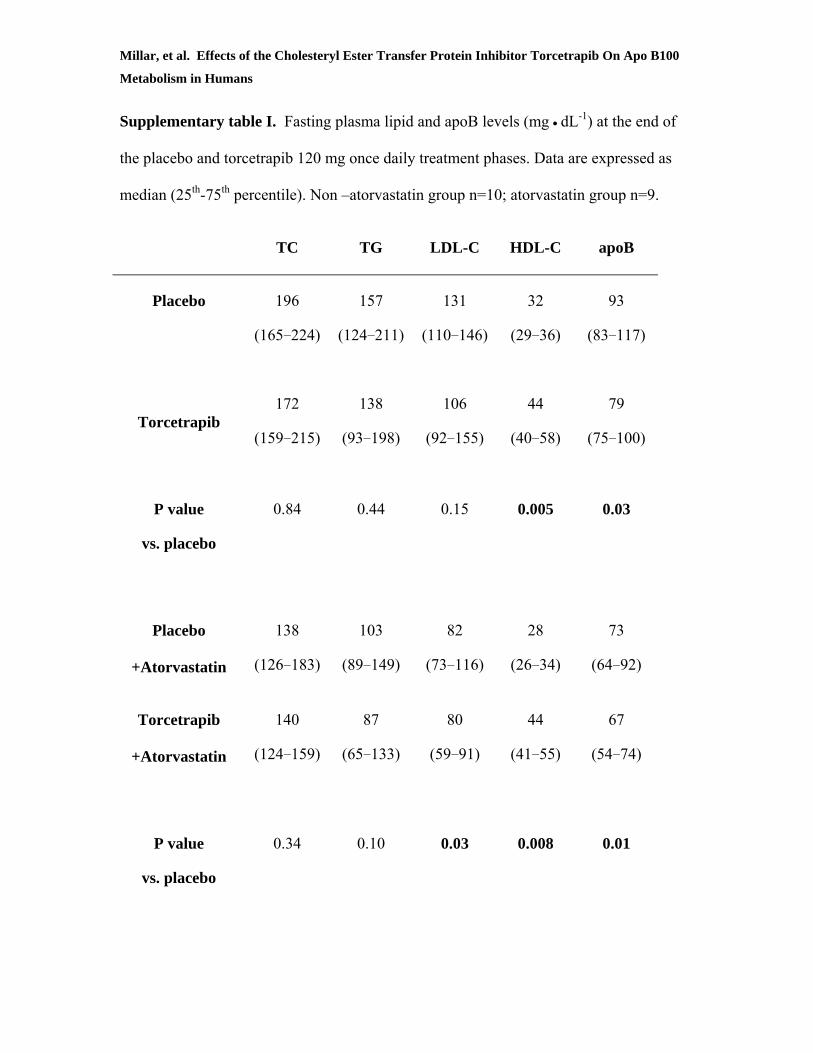
are shown in the supplemental Table (available online athttp://atvb.ahajournals.org). After the placebo phase, the nona-torvastatin group had median total cholesterol and LDL-C levelsof 196 and 131 mg � dL�1, respectively, and median triglycerideand total plasma apoB levels of 157 and 93 mg � dL�1, respec-tively. After treatment with 120 mg torcetrapib once daily, thesevalues decreased to 172 and 106 mg � dL�1 for total cholesteroland LDL-C, respectively, and to 138 and 79 mg � dL�1 fortriglyceride and apoB, respectively. The decrease in total apoB(P�0.02) in response to torcetrapib was statistically significant.
Changes in plasma lipids in response to treatment with 120mg torcetrapib once daily on a background of atorvastatinhave been reported previously8 and are shown in the supple-mental Table. Under treatment with 20 mg atorvastatin plusplacebo, these subjects had median total cholesterol andLDL-C levels of 138 and 82 mg � dL�1, respectively, and totaltriglyceride and plasma apoB levels of 103 and 73 mg � dL�1.Adding 120 mg torcetrapib to the existing atorvastatin treat-ment resulted in changes in the median total cholesterol andLDL-C levels to 140 and 80 mg � dL�1 and total triglycerideand apoB levels changed to 87 and 67 mg � dL�1, respectively.The decreases in LDL-C (P�0.03) and total apoB (P�0.01)were statistically significant.
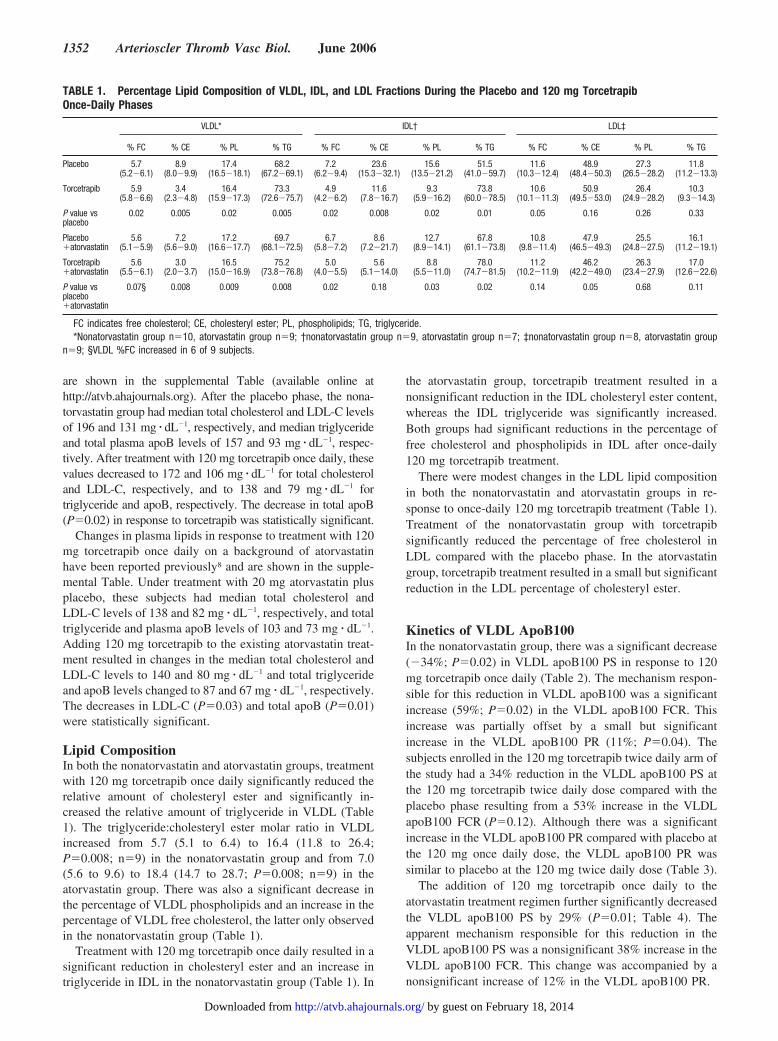
Lipid CompositionIn both the nonatorvastatin and atorvastatin groups, treatmentwith 120 mg torcetrapib once daily significantly reduced therelative amount of cholesteryl ester and significantly in-creased the relative amount of triglyceride in VLDL (Table1). The triglyceride:cholesteryl ester molar ratio in VLDLincreased from 5.7 (5.1 to 6.4) to 16.4 (11.8 to 26.4;P�0.008; n�9) in the nonatorvastatin group and from 7.0(5.6 to 9.6) to 18.4 (14.7 to 28.7; P�0.008; n�9) in theatorvastatin group. There was also a significant decrease inthe percentage of VLDL phospholipids and an increase in thepercentage of VLDL free cholesterol, the latter only observedin the nonatorvastatin group (Table 1).
Treatment with 120 mg torcetrapib once daily resulted in asignificant reduction in cholesteryl ester and an increase intriglyceride in IDL in the nonatorvastatin group (Table 1). In
the atorvastatin group, torcetrapib treatment resulted in anonsignificant reduction in the IDL cholesteryl ester content,whereas the IDL triglyceride was significantly increased.Both groups had significant reductions in the percentage offree cholesterol and phospholipids in IDL after once-daily120 mg torcetrapib treatment.
There were modest changes in the LDL lipid compositionin both the nonatorvastatin and atorvastatin groups in re-sponse to once-daily 120 mg torcetrapib treatment (Table 1).Treatment of the nonatorvastatin group with torcetrapibsignificantly reduced the percentage of free cholesterol inLDL compared with the placebo phase. In the atorvastatingroup, torcetrapib treatment resulted in a small but significantreduction in the LDL percentage of cholesteryl ester.
Kinetics of VLDL ApoB100In the nonatorvastatin group, there was a significant decrease(�34%; P�0.02) in VLDL apoB100 PS in response to 120mg torcetrapib once daily (Table 2). The mechanism respon-sible for this reduction in VLDL apoB100 was a significantincrease (59%; P�0.02) in the VLDL apoB100 FCR. Thisincrease was partially offset by a small but significantincrease in the VLDL apoB100 PR (11%; P�0.04). Thesubjects enrolled in the 120 mg torcetrapib twice daily arm ofthe study had a 34% reduction in the VLDL apoB100 PS atthe 120 mg torcetrapib twice daily dose compared with theplacebo phase resulting from a 53% increase in the VLDLapoB100 FCR (P�0.12). Although there was a significantincrease in the VLDL apoB100 PR compared with placebo atthe 120 mg once daily dose, the VLDL apoB100 PR wassimilar to placebo at the 120 mg twice daily dose (Table 3).
The addition of 120 mg torcetrapib once daily to theatorvastatin treatment regimen further significantly decreasedthe VLDL apoB100 PS by 29% (P�0.01; Table 4). Theapparent mechanism responsible for this reduction in theVLDL apoB100 PS was a nonsignificant 38% increase in theVLDL apoB100 FCR. This change was accompanied by anonsignificant increase of 12% in the VLDL apoB100 PR.
TABLE 1. Percentage Lipid Composition of VLDL, IDL, and LDL Fractions During the Placebo and 120 mg TorcetrapibOnce-Daily Phases
VLDL* IDL† LDL‡
% FC % CE % PL % TG % FC % CE % PL % TG % FC % CE % PL % TG
Placebo 5.7(5.2�6.1)
8.9(8.0�9.9)
17.4(16.5�18.1)
68.2(67.2�69.1)
7.2(6.2�9.4)
23.6(15.3�32.1)
15.6(13.5�21.2)
51.5(41.0�59.7)
11.6(10.3�12.4)
48.9(48.4�50.3)
27.3(26.5�28.2)
11.8(11.2�13.3)
Torcetrapib 5.9(5.8�6.6)
3.4(2.3�4.8)
16.4(15.9�17.3)
73.3(72.6�75.7)
4.9(4.2�6.2)
11.6(7.8�16.7)
9.3(5.9�16.2)
73.8(60.0�78.5)
10.6(10.1�11.3)
50.9(49.5�53.0)
26.4(24.9�28.2)
10.3(9.3�14.3)
P value vsplacebo
0.02 0.005 0.02 0.005 0.02 0.008 0.02 0.01 0.05 0.16 0.26 0.33
Placebo�atorvastatin
5.6(5.1�5.9)
7.2(5.6�9.0)
17.2(16.6�17.7)
69.7(68.1�72.5)
6.7(5.8�7.2)
8.6(7.2�21.7)
12.7(8.9�14.1)
67.8(61.1�73.8)
10.8(9.8�11.4)
47.9(46.5�49.3)
25.5(24.8�27.5)
16.1(11.2�19.1)
Torcetrapib�atorvastatin
5.6(5.5�6.1)
3.0(2.0�3.7)
16.5(15.0�16.9)
75.2(73.8�76.8)
5.0(4.0�5.5)
5.6(5.1�14.0)
8.8(5.5�11.0)
78.0(74.7�81.5)
11.2(10.2�11.9)
46.2(42.2�49.0)
26.3(23.4�27.9)
17.0(12.6�22.6)
P value vsplacebo�atorvastatin
0.07§ 0.008 0.009 0.008 0.02 0.18 0.03 0.02 0.14 0.05 0.68 0.11
FC indicates free cholesterol; CE, cholesteryl ester; PL, phospholipids; TG, triglyceride.*Nonatorvastatin group n�10, atorvastatin group n�9; †nonatorvastatin group n�9, atorvastatin group n�7; ‡nonatorvastatin group n�8, atorvastatin group
n�9; §VLDL %FC increased in 6 of 9 subjects.
1352 Arterioscler Thromb Vasc Biol. June 2006
by guest on February 18, 2014http://atvb.ahajournals.org/Downloaded from
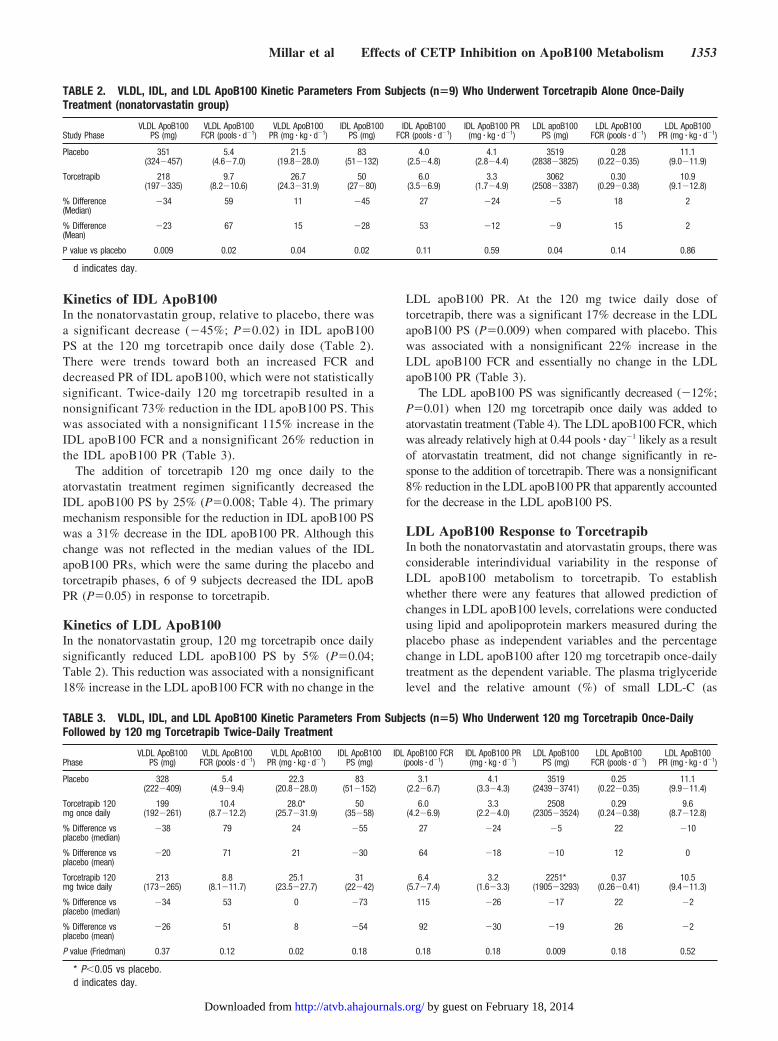
Kinetics of IDL ApoB100In the nonatorvastatin group, relative to placebo, there wasa significant decrease (�45%; P�0.02) in IDL apoB100PS at the 120 mg torcetrapib once daily dose (Table 2).There were trends toward both an increased FCR anddecreased PR of IDL apoB100, which were not statisticallysignificant. Twice-daily 120 mg torcetrapib resulted in anonsignificant 73% reduction in the IDL apoB100 PS. Thiswas associated with a nonsignificant 115% increase in theIDL apoB100 FCR and a nonsignificant 26% reduction inthe IDL apoB100 PR (Table 3).
The addition of torcetrapib 120 mg once daily to theatorvastatin treatment regimen significantly decreased theIDL apoB100 PS by 25% (P�0.008; Table 4). The primarymechanism responsible for the reduction in IDL apoB100 PSwas a 31% decrease in the IDL apoB100 PR. Although thischange was not reflected in the median values of the IDLapoB100 PRs, which were the same during the placebo andtorcetrapib phases, 6 of 9 subjects decreased the IDL apoBPR (P�0.05) in response to torcetrapib.
Kinetics of LDL ApoB100In the nonatorvastatin group, 120 mg torcetrapib once dailysignificantly reduced LDL apoB100 PS by 5% (P�0.04;Table 2). This reduction was associated with a nonsignificant18% increase in the LDL apoB100 FCR with no change in the
LDL apoB100 PR. At the 120 mg twice daily dose oftorcetrapib, there was a significant 17% decrease in the LDLapoB100 PS (P�0.009) when compared with placebo. Thiswas associated with a nonsignificant 22% increase in theLDL apoB100 FCR and essentially no change in the LDLapoB100 PR (Table 3).
The LDL apoB100 PS was significantly decreased (�12%;P�0.01) when 120 mg torcetrapib once daily was added toatorvastatin treatment (Table 4). The LDL apoB100 FCR, whichwas already relatively high at 0.44 pools � day�1 likely as a resultof atorvastatin treatment, did not change significantly in re-sponse to the addition of torcetrapib. There was a nonsignificant8% reduction in the LDL apoB100 PR that apparently accountedfor the decrease in the LDL apoB100 PS.
LDL ApoB100 Response to TorcetrapibIn both the nonatorvastatin and atorvastatin groups, there wasconsiderable interindividual variability in the response ofLDL apoB100 metabolism to torcetrapib. To establishwhether there were any features that allowed prediction ofchanges in LDL apoB100 levels, correlations were conductedusing lipid and apolipoprotein markers measured during theplacebo phase as independent variables and the percentagechange in LDL apoB100 after 120 mg torcetrapib once-dailytreatment as the dependent variable. The plasma triglyceridelevel and the relative amount (%) of small LDL-C (as
TABLE 2. VLDL, IDL, and LDL ApoB100 Kinetic Parameters From Subjects (n�9) Who Underwent Torcetrapib Alone Once-DailyTreatment (nonatorvastatin group)
Study PhaseVLDL ApoB100
PS (mg)VLDL ApoB100
FCR (pools � d�1)VLDL ApoB100
PR (mg � kg � d�1)IDL ApoB100
PS (mg)IDL ApoB100
FCR (pools � d�1)IDL ApoB100 PR(mg � kg � d�1)
LDL apoB100PS (mg)
LDL ApoB100FCR (pools � d�1)
LDL ApoB100PR (mg � kg � d�1)
Placebo 351(324�457)
5.4(4.6�7.0)
21.5(19.8�28.0)
83(51�132)
4.0(2.5�4.8)
4.1(2.8�4.4)
3519(2838�3825)
0.28(0.22�0.35)
11.1(9.0�11.9)
Torcetrapib 218(197�335)
9.7(8.2�10.6)
26.7(24.3�31.9)
50(27�80)
6.0(3.5�6.9)
3.3(1.7�4.9)
3062(2508�3387)
0.30(0.29�0.38)
10.9(9.1�12.8)
% Difference(Median)
�34 59 11 �45 27 �24 �5 18 2
% Difference(Mean)
�23 67 15 �28 53 �12 �9 15 2
P value vs placebo 0.009 0.02 0.04 0.02 0.11 0.59 0.04 0.14 0.86
d indicates day.
TABLE 3. VLDL, IDL, and LDL ApoB100 Kinetic Parameters From Subjects (n�5) Who Underwent 120 mg Torcetrapib Once-DailyFollowed by 120 mg Torcetrapib Twice-Daily Treatment
PhaseVLDL ApoB100
PS (mg)VLDL ApoB100
FCR (pools � d�1)VLDL ApoB100
PR (mg � kg � d�1)IDL ApoB100
PS (mg)IDL ApoB100 FCR
(pools � d�1)IDL ApoB100 PR(mg � kg � d�1)
LDL ApoB100PS (mg)
LDL ApoB100FCR (pools � d�1)
LDL ApoB100PR (mg � kg � d�1)
Placebo 328(222�409)
5.4(4.9�9.4)
22.3(20.8�28.0)
83(51�152)
3.1(2.2�6.7)
4.1(3.3�4.3)
3519(2439�3741)
0.25(0.22�0.35)
11.1(9.9�11.4)
Torcetrapib 120mg once daily
199(192�261)
10.4(8.7�12.2)
28.0*(25.7�31.9)
50(35�58)
6.0(4.2�6.9)
3.3(2.2�4.0)
2508(2305�3524)
0.29(0.24�0.38)
9.6(8.7�12.8)
% Difference vsplacebo (median)
�38 79 24 �55 27 �24 �5 22 �10
% Difference vsplacebo (mean)
�20 71 21 �30 64 �18 �10 12 0
Torcetrapib 120mg twice daily
213(173�265)
8.8(8.1�11.7)
25.1(23.5�27.7)
31(22�42)
6.4(5.7�7.4)
3.2(1.6�3.3)
2251*(1905�3293)
0.37(0.26�0.41)
10.5(9.4�11.3)
% Difference vsplacebo (median)
�34 53 0 �73 115 �26 �17 22 �2
% Difference vsplacebo (mean)
�26 51 8 �54 92 �30 �19 26 �2
P value (Friedman) 0.37 0.12 0.02 0.18 0.18 0.18 0.009 0.18 0.52
* P�0.05 vs placebo.d indicates day.
Millar et al Effects of CETP Inhibition on ApoB100 Metabolism 1353
by guest on February 18, 2014http://atvb.ahajournals.org/Downloaded from
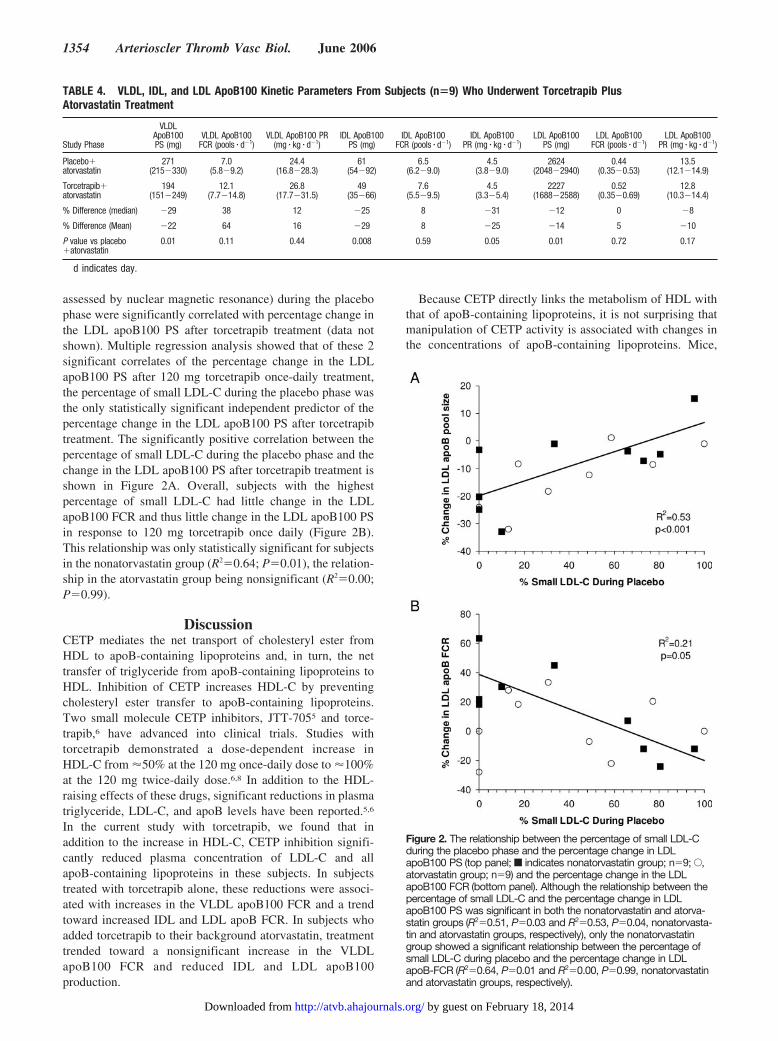
assessed by nuclear magnetic resonance) during the placebophase were significantly correlated with percentage change inthe LDL apoB100 PS after torcetrapib treatment (data notshown). Multiple regression analysis showed that of these 2significant correlates of the percentage change in the LDLapoB100 PS after 120 mg torcetrapib once-daily treatment,the percentage of small LDL-C during the placebo phase wasthe only statistically significant independent predictor of thepercentage change in the LDL apoB100 PS after torcetrapibtreatment. The significantly positive correlation between thepercentage of small LDL-C during the placebo phase and thechange in the LDL apoB100 PS after torcetrapib treatment isshown in Figure 2A. Overall, subjects with the highestpercentage of small LDL-C had little change in the LDLapoB100 FCR and thus little change in the LDL apoB100 PSin response to 120 mg torcetrapib once daily (Figure 2B).This relationship was only statistically significant for subjectsin the nonatorvastatin group (R2�0.64; P�0.01), the relation-ship in the atorvastatin group being nonsignificant (R2�0.00;P�0.99).
DiscussionCETP mediates the net transport of cholesteryl ester fromHDL to apoB-containing lipoproteins and, in turn, the nettransfer of triglyceride from apoB-containing lipoproteins toHDL. Inhibition of CETP increases HDL-C by preventingcholesteryl ester transfer to apoB-containing lipoproteins.Two small molecule CETP inhibitors, JTT-7055 and torce-trapib,6 have advanced into clinical trials. Studies withtorcetrapib demonstrated a dose-dependent increase inHDL-C from �50% at the 120 mg once-daily dose to �100%at the 120 mg twice-daily dose.6,8 In addition to the HDL-raising effects of these drugs, significant reductions in plasmatriglyceride, LDL-C, and apoB levels have been reported.5,6
In the current study with torcetrapib, we found that inaddition to the increase in HDL-C, CETP inhibition signifi-cantly reduced plasma concentration of LDL-C and allapoB-containing lipoproteins in these subjects. In subjectstreated with torcetrapib alone, these reductions were associ-ated with increases in the VLDL apoB100 FCR and a trendtoward increased IDL and LDL apoB FCR. In subjects whoadded torcetrapib to their background atorvastatin, treatmenttrended toward a nonsignificant increase in the VLDLapoB100 FCR and reduced IDL and LDL apoB100production.
Because CETP directly links the metabolism of HDL withthat of apoB-containing lipoproteins, it is not surprising thatmanipulation of CETP activity is associated with changes inthe concentrations of apoB-containing lipoproteins. Mice,
TABLE 4. VLDL, IDL, and LDL ApoB100 Kinetic Parameters From Subjects (n�9) Who Underwent Torcetrapib PlusAtorvastatin Treatment
Study Phase
VLDLApoB100PS (mg)
VLDL ApoB100FCR (pools � d�1)
VLDL ApoB100 PR(mg � kg � d�1)
IDL ApoB100PS (mg)
IDL ApoB100FCR (pools � d�1)
IDL ApoB100PR (mg � kg � d�1)
LDL ApoB100PS (mg)
LDL ApoB100FCR (pools � d�1)
LDL ApoB100PR (mg � kg � d�1)
Placebo�atorvastatin
271(215�330)
7.0(5.8�9.2)
24.4(16.8�28.3)
61(54�92)
6.5(6.2�9.0)
4.5(3.8�9.0)
2624(2048�2940)
0.44(0.35�0.53)
13.5(12.1�14.9)
Torcetrapib�atorvastatin
194(151�249)
12.1(7.7�14.8)
26.8(17.7�31.5)
49(35�66)
7.6(5.5�9.5)
4.5(3.3�5.4)
2227(1688�2588)
0.52(0.35�0.69)
12.8(10.3�14.4)
% Difference (median) �29 38 12 �25 8 �31 �12 0 �8
% Difference (Mean) �22 64 16 �29 8 �25 �14 5 �10
P value vs placebo�atorvastatin
0.01 0.11 0.44 0.008 0.59 0.05 0.01 0.72 0.17
d indicates day.
Figure 2. The relationship between the percentage of small LDL-Cduring the placebo phase and the percentage change in LDLapoB100 PS (top panel; f indicates nonatorvastatin group; n�9; E,atorvastatin group; n�9) and the percentage change in the LDLapoB100 FCR (bottom panel). Although the relationship between thepercentage of small LDL-C and the percentage change in LDLapoB100 PS was significant in both the nonatorvastatin and atorva-statin groups (R2�0.51, P�0.03 and R2�0.53, P�0.04, nonatorvasta-tin and atorvastatin groups, respectively), only the nonatorvastatingroup showed a significant relationship between the percentage ofsmall LDL-C during placebo and the percentage change in LDLapoB-FCR (R2�0.64, P�0.01 and R2�0.00, P�0.99, nonatorvastatinand atorvastatin groups, respectively).
1354 Arterioscler Thromb Vasc Biol. June 2006
by guest on February 18, 2014http://atvb.ahajournals.org/Downloaded from

which do not normally express CETP, increase their LDL-Clevels in response to CETP expression.3 The increase inLDL-C resulting from CETP expression in mice is associatedwith an increased cholesteryl ester content in VLDL andLDL17 and downregulation of hepatic LDL receptor,18 pre-sumably as a result of increased cholesteryl ester delivery tothe liver.
Studies in CETP-deficient subjects have shed some lighton possible mechanisms responsible for the reduced levels ofapoB100-containing lipoproteins in CETP deficiency. CETP-deficient subjects have IDL and LDL apoB100 levels that are�50% of normal.19 Kinetic studies revealed that these re-duced levels were the result of increased fractional catabo-lism of IDL and LDL apoB100, probably because of hepaticLDL receptor upregulation.19 We observed a nonsignificanttrend toward an increase in VLDL, IDL, and LDL apoB100fractional catabolism with CETP inhibition in subjects in thenonatorvastatin group. Although it is likely that the trendtoward an increase in the IDL and LDL apoB100 FCR wasthe result of LDL receptor upregulation, the LDL receptor hasbeen shown to have minimal impact on the clearance ofVLDL apoB100 in humans.20 Instead, we suggest that theenhanced VLDL apoB100 fractional catabolism may be theresult of compositional changes in VLDL lipids in responseto CETP inhibition. The relative enrichment with triglyceride,as indicated by the increased molar ratio of triglyceride tocholesteryl ester in the core of the VLDL, may make VLDLa better substrate for lipoprotein lipase in vivo. Alternatively,the change in VLDL composition may have increased li-poprotein lipase activity by altering the exchangeable apoli-poprotein content of VLDL. Such a change could alsoincrease receptor-mediated clearance of VLDL remnantsfrom plasma and conversion of VLDL to LDL.21
The decrease in VLDL and LDL apoB100 levels inresponse to atorvastatin treatment has been reported to beattributable to increased fractional catabolism,22 althoughreduced VLDL production has also been reported in somesubjects in response to statin treatment.23,24 Reduced CETPexpression has been reported in subjects treated with atorva-statin25 and may have contributed to the significantly in-creased IDL FCR in these subjects. The addition of torce-trapib to atorvastatin treatment resulted in further apoB100decrease in all lipoprotein fractions. The magnitude of thedecrease was similar to what was observed with torcetrapibalone, indicating that there was an additive effect of combin-ing torcetrapib with atorvastatin treatment on apoB100 kinet-ics. The VLDL apoB100 PS was reduced as a result of a trendtoward increased VLDL apoB100 clearance, similar to whatwas seen with torcetrapib alone. However, the changes inIDL and LDL apoB100 PS resulted from a different mecha-nism than what was found during treatment with torcetrapibalone. The subjects in the atorvastatin group had a relativelyhigh IDL and LDL apoB100 FCR during treatment withatorvastatin alone when compared with the nonatorvastatingroup likely attributable to upregulation of LDL receptorswith statin therapy. The addition of torcetrapib provided nofurther increase in the IDL and LDL apoB100 FCRs, perhapsindicating maximal upregulation of apoB100 clearance bythis pathway had already been achieved before the addition of
torcetrapib. Instead, there was reduced IDL apoB100 produc-tion and a trend toward reduced LDL apoB100 production.The mechanism responsible for this decrease in IDL and LDLapoB100 production is not clear but may relate to changes inlipoprotein lipid and apolipoprotein composition21 in re-sponse to torcetrapib in these subjects.
The individual response of LDL apoB100 PS to 120 mgtorcetrapib once daily in subjects in both the atorvastatin andnonatorvastatin groups was variable, ranging from a 33%decrease in the LDL apoB100 PS to a 15% increase (data notshown). We found that the best predictor of the percentagechange in the LDL apoB100 PS response to torcetrapibtreatment was the relative amount (%) of small LDL-C duringthe placebo phase. Small LDL has been shown to bind poorlyto the LDL receptor and is associated with elevated triglyc-eride levels.26 Interestingly, the percentage of small LDL-Cduring the placebo phase was a significant predictor of thechange in the LDL apoB100 FCR in response to torcetrapibin subjects in the nonatorvastatin group. However, thisinverse relationship between the percentage of small LDL-Cand the change in the LDL apoB100 FCR in response totorcetrapib was not observed in subjects in the atorvastatingroup. This is consistent with the finding that a change in theLDL apoB100 PR appeared to be primarily responsible forlowering the LDL apoB100 PS in these subjects. Regardlessof the mechanism for the decrease in LDL apoB100 PS,subjects with a relatively high percentage of small LDL-Cmight have less of an LDL apoB100 PS change in response totorcetrapib treatment, something that should be examined infuture studies.
In conclusion, these data suggest that treatment withtorcetrapib alone lowers VLDL, IDL, and LDL apoB100 PSby increasing VLDL, IDL, and LDL apoB100 clearance. Ona background of atorvastatin, where LDL apoB100 FCR isincreased, the addition of torcetrapib to treatment does notfurther increase LDL apoB100 clearance but appears to lowerthe LDL apoB100 PS by enhancing VLDL apoB100 clear-ance and reducing LDL apoB100 production. In both cases,the overall effect of torcetrapib on lowering apoB100 PSscould contribute to a beneficial effect on atherosclerosisdespite different kinetic mechanisms.
AcknowledgmentsThis work was supported in part by the Department of ClinicalResearch, Medicinal Products Research and Development, Pfizer,Inc., Groton, Conn. Support was also provided by the GeneralClinical Research Center of the University of Pennsylvania (M01-RR00040) and the General Clinical Research Center of Tufts-NewEngland Medical Center (M01-RR00054). M.E.B. and E.J.S. weresupported in part by National Institutes of Health (NIH) grantR01-HL60935 from the National Heart, Lung and Blood Institute.P.H.R.B. is a fellow of the National Health and Medical ResearchCouncil of Australia and is partially supported by NIH/NationalInstitute of Biomedical Imaging and Bioengineering grant P41EB-001975. The authors thank the nursing and dietary staff of eachclinical research center, as well as Anna DiFlorio, Linda Morrell,Rodrigo Ferreira, and Judith R. McNamara for excellenttechnical assistance.
References1. Expert Panel on Detection, Evaluation, and Treatment of High Blood
Cholesterol in Adults. Executive summary of the third report of the
Millar et al Effects of CETP Inhibition on ApoB100 Metabolism 1355
by guest on February 18, 2014http://atvb.ahajournals.org/Downloaded from

National Cholesterol Education Program (NCEP) Expert Panel onDetection, Evaluation, and Treatment of High Blood Cholesterol inAdults (Adult Treatment Panel III). J Am Med Assoc. 2001;285:2486–2497.
2. Barter PJ, Brewer HB Jr, Chapman MJ, Hennekens CH, Rader DJ, TallAR. Cholesteryl ester transfer protein: a novel target for raising HDL andinhibiting atherosclerosis. Arterioscler Thromb Vasc Biol. 2003;23:160–167.
3. Agellon LB, Walsh A, Hayek T, Moulin P, Jiang XC, Shelanski SA,Breslow JL, Tall AR. Reduced high density lipoprotein cholesterol inhuman cholesteryl ester transfer protein transgenic mice. J Biol Chem.1991;266:10796–10801.
4. Gaynor BJ, Sand T, Clark RW, Aiello RJ, Bamberger MJ, Moberly JB.Inhibition of cholesteryl ester transfer protein activity in hamsters altersHDL lipid composition. Atherosclerosis. 1994;110:101–109.
5. Okamoto H, Yonemori F, Wakitani K, Minowa T, Maeda K, Shinkai H.A cholesteryl ester transfer protein inhibitor attenuates atherosclerosis inrabbits. Nature. 2000;406:203–207.
6. de Grooth GJ, Kuivenhoven JA, Stalenhoef AFH, de Graaf J,Zwinderman AH, Posma JL, van Tol A, Kastelein JJP. Efficacy andsafety of a novel cholesteryl ester transfer protein inhibitor, JTT-705, inhumans: a randomized phase II dose-response study. Circulation. 2002;105:2159–2165.
7. Clark RW, Sutfin TA, Ruggeri RB, Willauer AT, Sugarman ED, Magnus-Aryitey G, Cosgrove PG, Sand TM, Wester RT, Williams JA, PerlmanME, Bamberger MJ. Raising high-density lipoprotein in humans throughinhibition of cholesteryl ester transfer protein: an initial multidose studyof torcetrapib. Arterioscler Thromb Vasc Biol. 2004;24:490–497.
8. Brousseau ME, Schaefer EJ, Wolfe ML, Bloedon LT, Digenio AG, ClarkRW, Mancuso JP, Rader DJ. Effects of a potent inhibitor of cholesterylester transfer protein on plasma lipoproteins in subjects with low HDLcholesterol. N Engl J Med. 2004;350:1505–1515.
9. Brousseau ME, Diffenderfer MR, Millar JS, Nartsupha C, Asztalos BF,Welty FK, Wolfe ML, Rudling M, Bjorkhem I, Angelin B, Mancuso JP,Digenio AG, Rader DJ, Schaefer EJ. Effects of cholesteryl ester transferprotein inhibition on high-density lipoprotein subspecies, apolipoproteinA-I metabolism, and fecal sterol excretion. Arterioscler Thromb VascBiol. 2005;25:1057–1064.
10. Cohn JS, Wagner DA, Cohn SD, Millar JS, Schaefer EJ. Measurement ofvery low density and low density lipoprotein apolipoprotein (Apo) B-100and high density lipoprotein Apo A-I production in human subjects usingdeuterated leucine. Effect of fasting and feeding. J Clin Invest. 1990;85:804–811.
11. Warnick GR, Benderson J, Albers JJ. Dextran sulfate-Mg2� precipitationprocedure for quantitation of high-density lipoprotein cholesterol. ClinChem. 1982;28:1379–1388.
12. McNamara JR, Schaefer EJ. Automated enzymatic standardized lipidanalyses for plasma and lipoprotein fractions. Clin Chim Acta. 1987;166:1–8.
13. Ordovas JM, Peterson JP, Santaniello P, Cohn JS, Wilson PW, SchaeferEJ. Enzyme-linked immunosorbent assay for human plasma apoli-poprotein B. J Lipid Res. 1987;28:1216–1224.
14. Cohn JS, McNamara JR, Cohn SD, Ordovas JM, Schaefer EJ. Plasmaapolipoprotein changes in the triglyceride-rich lipoprotein fraction ofhuman subjects fed a fat-rich meal. J Lipid Res. 1988;29:925–936.
15. Millar JS, Lichtenstein AH, Cuchel M, Dolnikowski GG, Hachey DL,Cohn JS, Schaefer EJ. Impact of age on the metabolism of VLDL, IDL,and LDL apolipoprotein B-100 in men. J Lipid Res. 1995;36:1155–1167.
16. Parhofer KG, Barrett PHR, Bier D, Schonfeld G. Determination of kineticparameters of apolipoprotein B metabolism using amino acids labeledwith stable isotopes. J Lipid Res. 1991;8:1311–1323.
17. Jiang XC, Masucci-Magoulas L, Mar J, Lin M, Walsh A, Breslow JL,Tall A. Down-regulation of mRNA for the low density lipoproteinreceptor in transgenic mice containing the gene for human cholesterylester transfer protein. Mechanism to explain accumulation of lipoproteinB particles. J Biol Chem. 1993;268:27406–27412.
18. Liu J, Zhang YL, Spence MJ, Vestal RE, Wallace PM, Grass DS. LiverLDL receptor mRNA expression is decreased in human ApoB/CETPdouble transgenic mice and is regulated by diet as well as the cytokineoncostatin M. Arterioscler Thromb Vasc Biol. 1997;17:2948–2954.
19. Ikewaki K, Nishiwaki M, Sakamoto T, Ishikawa T, Fairwell T, Zech LA,Nagano M, Nakamura H, Brewer HB Jr, Rader DJ. Increased catabolicrate of low density lipoproteins in humans with cholesteryl ester transferprotein deficiency. J Clin Invest. 1995;96:1573–1581.
20. Millar JS, Maugeais C, Ikewaki K, Kolansky DM, Barrett PH, BudreckEC, Boston RC, Tada N, Mochizuki S, Defesche JC, Wilson JM, RaderDJ. Complete deficiency of the low-density lipoprotein receptor is asso-ciated with increased apolipoprotein B-100 production. ArteriosclerThromb Vasc Biol. 2005;25:560–565.
21. Millar JS, Lichtenstein AH, Ordovas JM, Dolnikowski GG, Schaefer EJ.Human triglyceride-rich lipoprotein apo E kinetics and its relationship toLDL apo B-100 metabolism. Atherosclerosis. 2001;155:477–485.
22. Forster LF, Stewart G, Bedford D, Stewart JP, Rogers E, Shepherd J,Packard CJ, Caslake MJ. Influence of atorvastatin and simvastatin onapolipoprotein B metabolism in moderate combined hyperlipidemicsubjects with low VLDL and LDL fractional clearance rates. Atheroscle-rosis. 2002;164:129–145.
23. Cuchel M, Schaefer EJ, Millar JS, Jones PJ, Dolnikowski GG, Vergani C,Lichtenstein AH. Lovastatin decreases de novo cholesterol synthesis andLDL Apo B-100 production rates in combined-hyperlipidemic males.Arterioscler Thromb Vasc Biol. 1997;17:1910–1917.
24. Berglund L, Witztum JL, Galeano NF, Khouw AS, Ginsberg HN,Ramakrishnan R. Three-fold effect of lovastatin treatment on low densitylipoprotein metabolism in subjects with hyperlipidemia: increase inreceptor activity, decrease in apoB production, and decrease in particleaffinity for the receptor. Results from a novel triple-tracer approach. JLipid Res. 1998;39:913–924.
25. Guerin M, Egger P, Soudant C, Le Goff W, van Tol A, Dupuis R,Chapman MJ. Dose-dependent action of atorvastatin in type IIB hyper-lipidemia: preferential and progressive reduction of atherogenic apoBcontaining lipoprotein subclasses (VLDL-2, IDL, small dense LDL) andstimulation of cellular cholesterol efflux. Atherosclerosis. 2002;163:287–296.
26. Berneis KK, Krauss RM. Metabolic origins and clinical significance ofLDL heterogeneity. J Lipid Res. 2002;43:1363–1379.
1356 Arterioscler Thromb Vasc Biol. June 2006
by guest on February 18, 2014http://atvb.ahajournals.org/Downloaded from
Millar, et al. Effects of the Cholesteryl Ester Transfer Protein Inhibitor Torcetrapib On Apo B100
Metabolism in Humans
Supplementary table I. Fasting plasma lipid and apoB levels (mg • dL-1) at the end of
the placebo and torcetrapib 120 mg once daily treatment phases. Data are expressed as
median (25th-75th percentile). Non –atorvastatin group n=10; atorvastatin group n=9.
TC TG LDL-C HDL-C apoB
Placebo 196
(165−224)
157
(124−211)
131
(110−146)
32
(29−36)
93
(83−117)
Torcetrapib
172
(159−215)
138
(93−198)
106
(92−155)
44
(40−58)
79
(75−100)
P value
vs. placebo
0.84
0.44
0.15
0.005
0.03
Placebo
+Atorvastatin
138
(126−183)
103
(89−149)
82
(73−116)
28
(26−34)
73
(64−92)
Torcetrapib
+Atorvastatin
140
(124−159)
87
(65−133)
80
(59−91)
44
(41−55)
67
(54−74)
P value
vs. placebo
0.34
0.10
0.03
0.008
0.01
Millar, et al. Effects of the Cholesteryl Ester Transfer Protein Inhibitor Torcetrapib On Apo B100
Metabolism in Humans
Supplementary table II. Fasting plasma lipid and apoB levels (mg • dL-1) at the end of
the placebo, torcetrapib 120 mg once daily and torcetrapib 120 mg twice daily treatment
phases. Data are expressed as median (25th-75th percentile); n=6.
TC TG LDL-C HDL-C apoB
Placebo
204
(171−225)
152
(115−211)
137
(113−155)
33
(30−37)
113
(85−117)
Torcetrapib
120 mg once
daily
211
(159−237)
112
(88−181)
137
(100−165)
51
(42−66)
89
(76−106)
Torcetrapib
120 mg twice
daily
200
(165−236)
96
(72−152)
121
(70−152)
74*
(53−81)
83*
(62−102)
P value
(Friedman)
0.96 0.25 0.18 <0.001 0.002
*p<0.05 vs. placebo
Related Documents











