275 Effects of Hormone Replacement Therapy on Lipoprotein(a) and Lipids in Postmenopausal Women Chee Jeong Kim, Hak Chul Jang, Dong Hee Cho, Yong Ki Min Abstract High concentrations of lipoprotein(a) [Lp(a)], an independent risk factor for atherosclerosis, cannot be managed by the usual lipid-lowering agents. It has been suggested that Lp(a) levels are related to female sex hormones. Estrogen replacement therapy makes the lipid profiles favorable for delaying atherosclerosis in postmenopausal women. The effects of the combination therapy of estrogen and progesterone on lipids are controversial. This study was designed to evaluate the effect of female sex hormones on the concentration of Lp(a) and to clarify the influence of progesterone on the effect of estrogen in postmenopausal women. Postmenopausal women (n=184) were divided into four groups: control; 0.625 mg conjugated equine estrogen (CEE) plus 10 mg medroxy- progesterone acetate (MPA); 0.625 mg CEE plus 5 mg MPA; and 0.625 mg CEE only. Medication for 2 months lowered the concentrations of Lp(a) by 20% in all treated groups. The decrease was more pronounced in subjects with a relatively higher basal Lp(a) concentration. Estrogen replacement ther- apy raised the concentration of high-density lipoprotein choles- terol and decreased low-density lipoprotein cholesterol without changing total cholesterol. The combination therapy of estrogen and progesterone abolished the effect of estrogen on high- density lipoprotein cholesterol. Hormone replacement therapy lowered Lp(a) levels in postmenopausal women. The effect was prominent in subjects with high basal Lp(a) levels. This de- crease may be one of the mechanisms of the cardioprotective effects of estrogen. The cardioprotective effect of estrogen cannot be applied to the combination therapy due to the adverse effect of progesterone on high-density lipoprotein cho- lesterol. (Arterioscler Thromb. 1994;14:275-281.) Key Words • lipoprotein(a) • lipids • estrogen • progesterone • menopause L ipoprotein(a) [Lp(a)] consists of low-density li- poprotein (LDL)-like particles and a specific glycoprotein, apolipoprotein(a) [Apo(a)]. 1 A high concentration of Lp(a) is thought to be an inde- pendent risk factor for cardiovascular 27 and cerebrovas- cular 7 - 8 diseases. It cannot be lowered by the usual treatments for hyperlipidemia, 912 and only a few drugs reduce Lp(a) concentrations. 1318 Recently, epidemiological investigations have re- ported that concentrations of Lp(a) are higher in post- menopausal women than in premenopausal women 19 and that postmenopausal women taking female sex hormones have lower Lp(a) levels than those not taking such medication. 20 Small-sized studies 21 - 22 also show that hormone replacement therapy (HRT) in post- menopausal women lowers the concentration of Lp(a) markedly. Premenopausal women have lower cardiovascular morbidity and mortality than men of a similar age. After menopause, the incidence of cardiovascular diseases increases and no difference is noticed during the eighth decade between men and women. 23 Female sex hor- mones have been used for the alleviation of postmeno- pausal symptoms and the treatment of osteoporosis. Most but not all reports have shown that estrogen replacement therapy in postmenopausal women re- Received July 19, 1993; revision accepted November 15, 1993. From the Departments of Internal Medicine (C.J.K., H.C.J., Y.K.M.) and Clinical Pathology (D.H.C.), Cheil General Hospital, Seoul, Korea. Correspondence to Chee Jeong Kim, MD, Internal Medicine, Cheil General Hospital, 1-23 Mookchung-Dong, Chung-Ku, Seoul, Korea 100-380. duces cardiovascular mortality. 24 2<s The changes in lipid profiles 27 - 2 * and the modulation of vasomotor tone 29 have been proposed as the mechanisms of the cardio- protective effect of estrogen. The effect of estrogen on various kinds of cholesterol has been well described in many studies 27 - 28 ; it delays atherosclerosis by increasing the concentration of high- density lipoprotein cholesterol (HDL-C) and by de- creasing the concentration of low-density lipoprotein cholesterol (LDL-C). Because estrogen replacement therapy increases the risk of endometrial cancer, pro- gesterone has been added, and the risk has become negligible. 30 - 31 However, progesterone has an adverse effect on lipids. 27 - 32 The effect of the combination ther- apy of estrogen and progesterone on lipids has been evaluated by many authors, but most studies had rela- tively small numbers of cases and yielded inconsistent results. 33 - 34 Thus, the purposes of this study were to evaluate the effect of estrogen and progesterone on the concentration of Lp(a) and to clarify the influence of progesterone on lipid levels when administered with estrogen to postmenopausal women. Methods Subjects This study was a prospective, controlled trial to evaluate HRT on Lp(a) and lipid levels in postmenopausal women. Between April 1991 and March 1992, 184 women who had been amenorrheic for over 1 year without hysterectomy or had serum follicle-stimulating hormone concentrations over 20 mlU/L were enrolled. Their ages ranged from 33 through 68 years with a mean of 51.1 ±4.9 years. Patients who had diseases that influence lipid levels, such as diabetes mellitus, chronic by guest on June 26, 2018 http://atvb.ahajournals.org/ Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
275
Effects of Hormone Replacement Therapyon Lipoprotein(a) and Lipidsin Postmenopausal Women
Chee Jeong Kim, Hak Chul Jang, Dong Hee Cho, Yong Ki Min
Abstract High concentrations of lipoprotein(a) [Lp(a)], anindependent risk factor for atherosclerosis, cannot be managedby the usual lipid-lowering agents. It has been suggested thatLp(a) levels are related to female sex hormones. Estrogenreplacement therapy makes the lipid profiles favorable fordelaying atherosclerosis in postmenopausal women. The effectsof the combination therapy of estrogen and progesterone onlipids are controversial. This study was designed to evaluate theeffect of female sex hormones on the concentration of Lp(a)and to clarify the influence of progesterone on the effect ofestrogen in postmenopausal women. Postmenopausal women(n=184) were divided into four groups: control; 0.625 mgconjugated equine estrogen (CEE) plus 10 mg medroxy-progesterone acetate (MPA); 0.625 mg CEE plus 5 mg MPA;and 0.625 mg CEE only. Medication for 2 months lowered theconcentrations of Lp(a) by 20% in all treated groups. The
decrease was more pronounced in subjects with a relativelyhigher basal Lp(a) concentration. Estrogen replacement ther-apy raised the concentration of high-density lipoprotein choles-terol and decreased low-density lipoprotein cholesterol withoutchanging total cholesterol. The combination therapy of estrogenand progesterone abolished the effect of estrogen on high-density lipoprotein cholesterol. Hormone replacement therapylowered Lp(a) levels in postmenopausal women. The effect wasprominent in subjects with high basal Lp(a) levels. This de-crease may be one of the mechanisms of the cardioprotectiveeffects of estrogen. The cardioprotective effect of estrogencannot be applied to the combination therapy due to theadverse effect of progesterone on high-density lipoprotein cho-lesterol. (Arterioscler Thromb. 1994;14:275-281.)
Key Words • lipoprotein(a) • lipids • estrogen •progesterone • menopause
Lipoprotein(a) [Lp(a)] consists of low-density li-poprotein (LDL)-like particles and a specificglycoprotein, apolipoprotein(a) [Apo(a)].1 A
high concentration of Lp(a) is thought to be an inde-pendent risk factor for cardiovascular27 and cerebrovas-cular7-8 diseases. It cannot be lowered by the usualtreatments for hyperlipidemia,912 and only a few drugsreduce Lp(a) concentrations.1318
Recently, epidemiological investigations have re-ported that concentrations of Lp(a) are higher in post-menopausal women than in premenopausal women19
and that postmenopausal women taking female sexhormones have lower Lp(a) levels than those not takingsuch medication.20 Small-sized studies21-22 also showthat hormone replacement therapy (HRT) in post-menopausal women lowers the concentration of Lp(a)markedly.
Premenopausal women have lower cardiovascularmorbidity and mortality than men of a similar age. Aftermenopause, the incidence of cardiovascular diseasesincreases and no difference is noticed during the eighthdecade between men and women.23 Female sex hor-mones have been used for the alleviation of postmeno-pausal symptoms and the treatment of osteoporosis.Most but not all reports have shown that estrogenreplacement therapy in postmenopausal women re-
Received July 19, 1993; revision accepted November 15, 1993.From the Departments of Internal Medicine (C.J.K., H.C.J.,
Y.K.M.) and Clinical Pathology (D.H.C.), Cheil General Hospital,Seoul, Korea.
Correspondence to Chee Jeong Kim, MD, Internal Medicine,Cheil General Hospital, 1-23 Mookchung-Dong, Chung-Ku, Seoul,Korea 100-380.
duces cardiovascular mortality.24 2<s The changes in lipidprofiles27-2* and the modulation of vasomotor tone29
have been proposed as the mechanisms of the cardio-protective effect of estrogen.
The effect of estrogen on various kinds of cholesterolhas been well described in many studies27-28; it delaysatherosclerosis by increasing the concentration of high-density lipoprotein cholesterol (HDL-C) and by de-creasing the concentration of low-density lipoproteincholesterol (LDL-C). Because estrogen replacementtherapy increases the risk of endometrial cancer, pro-gesterone has been added, and the risk has becomenegligible.30-31 However, progesterone has an adverseeffect on lipids.27-32 The effect of the combination ther-apy of estrogen and progesterone on lipids has beenevaluated by many authors, but most studies had rela-tively small numbers of cases and yielded inconsistentresults.33-34 Thus, the purposes of this study were toevaluate the effect of estrogen and progesterone on theconcentration of Lp(a) and to clarify the influence ofprogesterone on lipid levels when administered withestrogen to postmenopausal women.
MethodsSubjects
This study was a prospective, controlled trial to evaluateHRT on Lp(a) and lipid levels in postmenopausal women.Between April 1991 and March 1992, 184 women who hadbeen amenorrheic for over 1 year without hysterectomy or hadserum follicle-stimulating hormone concentrations over 20mlU/L were enrolled. Their ages ranged from 33 through 68years with a mean of 51.1 ±4.9 years. Patients who had diseasesthat influence lipid levels, such as diabetes mellitus, chronic
by guest on June 26, 2018http://atvb.ahajournals.org/
Dow
nloaded from
276 Arteriosclerosis and Thrombosis Vol 14, No 2 February 1994
liver disease, infectious diseases, or other endocrinologic dis-eases, were excluded. None had received hormonal prepara-tions before the study. The subjects were divided into fourgroups: group A (n=29), a control group without medication;group B (n=67), treated with 0.625 mg conjugated equineestrogen (CEE) and 10 mg medroxyprogesterone acetate(MPA); group C (n=65), treated with 0.625 mg CEE and 5mg MPA; and group D (n=23), treated with 0.625 mg CEEalone in subjects with a prior hysterectomy. The medicationwas prescribed cyclically every 30 days for 2 months. CEE wasadministered from the 1st through the 25th day, and MPA wasadded from the 16th through the 25th day. No medication wasprescribed from the 26th through the 30th day.
Determination of Lp(a) and Lipid ConcentrationsAfter overnight fasting, blood samples were placed in diso-
dium-EDTA tubes and plain tubes before and after thecompletion of medication for 2 months. Serum was isolatedand stored at -70°C for later Lp(a) measurement. Theconcentration of Apo(a) was determined by two-site immuno-radiometric assay using a commercial radioimmunoassay kit(Pharmacia) as described.6 In brief, the assay is based on thedirect sandwich technique, in which two monoclonal antibod-ies are directed against separate antigenic determinants on theApo(a) molecule. The concentration of Lp(a) protein wascalculated approximately by using a conversion factor of 1 asproposed by Pharmacia Co. Interassay coefficients of variationwere 5.8% and 7.2% for high (mean, 45.7 mg/dL) and low(mean, 12.3 mg/dL) control levels, respectively. Intra-assaycoefficient of variation was 2.6%. The concentrations of totalcholesterol and triglyceride were determined by an enzymaticmethod using an automatic analyzer (Hitachi 7150). Theconcentrations of total protein, albumin, fasting blood sugar,aspartate aminotransferase, alanine aminotransferase, bloodurea nitrogen, and creatinine were also measured. The con-centrations of HDL-C, LDL-C, and very-low-density lipopro-tein cholesterol (VLDL-C) were determined by electropho-retic methods using an HDL-C supply kit (HelenaLaboratory). The lipoproteins were separated according totheir electrophoretic mobility on cellulose acetate in a Tris(2-amino-3-[hydroxymethyl]-l,3-propanediol)-barbital buffer,pH 8.8. Fractions were visualized with the production ofquinoneimine by an enzymatic method using cholesterol es-terase, cholesterol oxidase, 4-aminoantipyrine, phenol, andperoxidase. The relative percent of each fraction was obtainedby scanning in a densitometer equipped with a 500- or 505-nmfilter (Helena Laboratory). The concentrations of HDL-C,VLDL-C, and LDL-C were calculated by multiplying eachratio with total cholesterol. Follicle-stimulating hormone wasmeasured by immunoradiometric assay using a radioimmuno-assay kit (Serono Diagnostic).
Statistical AnalysisData were expressed as mean±SD; Lp(a) data were also
expressed as median. The data were stored on an IBMcomputer using DBASE III+ (Ashton-Tate). Statistical analysiswas performed with the STATISTICAL PACKAGE FOR THE SOCIALSCIENCES (SPSS Inc). The concentrations of Lp(a), VLDL-C,
Lipoprotein(a)
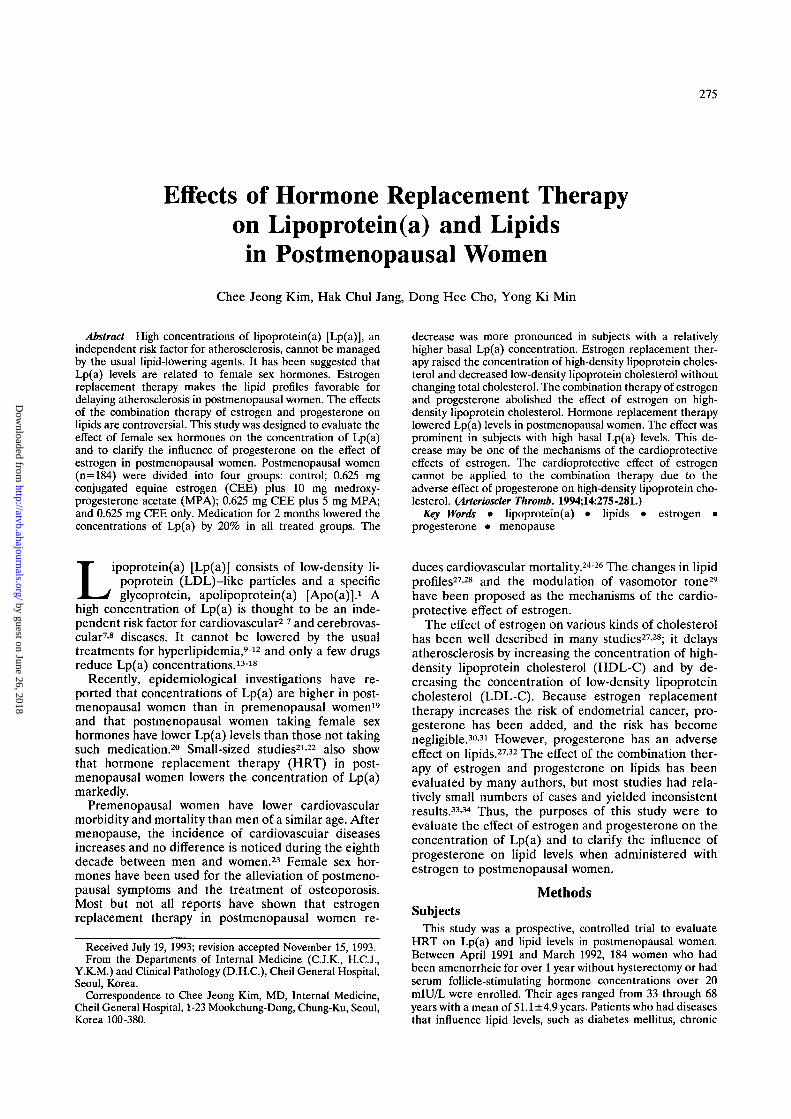
FIG 1. Bar graph showing the distribution of lipoprotein(a)levels for all subjects.
and triglyceride were transformed logarithmically if necessary.A Wilcoxon signed-rank test was used to compare the concen-trations of Lp(a), VLDL-C, and triglyceride before and aftermedication. Differences in the other parameters were ana-lyzed by paired t test. ANOVA or a Kruskal-Wallis test wasused to evaluate the differences among groups. A Mann-Whitney U test, Student's unpaired t test, logistic regressionanalysis, and multiple stepwise regression analysis were usedto observe the parameters influencing the effect of medication.The relations between Lp(a) and other parameters wereanalyzed by simple linear regression and multiple stepwiseregression. Significance was inferred when /><.05.
ResultsBaseline Data
The distribution of Lp(a) levels was skewed (Fig 1);concentrations between 10 and 20 mg/dL were the mostfrequent. The mean and median values of total caseswere 35.9±34.7 and 23.9 mg/dL, respectively. Basalclinical characteristics were similar in all groups (Table1). Age, body mass index, total cholesterol, and LDL-Cwere higher in groups A and D than in groups B and C.The concentration of Lp(a) was lower in group D than inother groups. None of these differences were significant.
Changes of Lp(a) With HRT
After 2 months of medication, the concentrations ofLp(a) were reduced from 36.7±30.9 mg/dL, 36.5±35.2mg/dL, and 31.2±33.8 mg/dL to 28.5±24.4 mg/dL,28.1±30.7 mg/dL, and 24.6±30.4 mg/dL in group B(P<.0001), group C (i><.0001), and group D (P<.001),respectively (Table 2). Lp(a) concentrations did not alterin the control group. The decreases of Lp(a) concentra-tions expressed as percentages were 14.7±44.4%,22.2±34.8%, and 25.7±33.4% in groups B, C, and D,
TABLE 1. Comparison of Baseline Clinical and Biochemical Parameters AmongFour Groups
Group
A
B
C
D
Age, y
51.7±7.3
50.7±4.0
50.8±4.7
52.3±3.8
BMI, kg/m2
24.7±3.0
24.2±3.1
24.2±2.5
24.7±2.3
TC, mg/dL
223.8±25.8
215.1 ±35.9
218.4±41.2
224.7±31.2
Lp(a), mg/dL
36.4±43.3(18.7)
36.7±30.9 (27.9)
36.5±35.2 (23.9)
31.2±33.8 (19.3)
BMI indicates body mass index; TC, total cholesterol; and Lp(a), lipoprotein(a). Values aremean±SD (median). There were no statistically significant comparisons.
by guest on June 26, 2018http://atvb.ahajournals.org/
Dow
nloaded from
Kim et al Lipoprotein(a) and Hormone Replacement Therapy 277
TABLE 2. Changes in Lipoprotein(a) Concentrations 2 Months After HRT
Basal
2 Months
Change
Change, %
P
Group A
36.4±43.34(18.7)
36.4±37.93(23.1)
NS
Group B
36.7±30.9(27.9)
28.5±24.4(20.0)
-8.2±12.2
-14.7±44.4
<.0001
Group C
36.5±35.2(23.9)
28.1+30.7(17.2)
-8.4±12.5
-22.2±34.8
<.0001
Group D
31.2+33.8(19.3)
24.6±30.4(10.5)
-6.7+9.1
-25.7±33.4
<.001
HRT indicates hormone replacement therapy; NS, not significant. Values are mean±SD (median)and are expressed in milligrams per deciliter.
respectively. The differences among groups wereinsignificant.
Parameters Influencing the Effect of HRT on Lp(a)When treated subjects were divided into a response
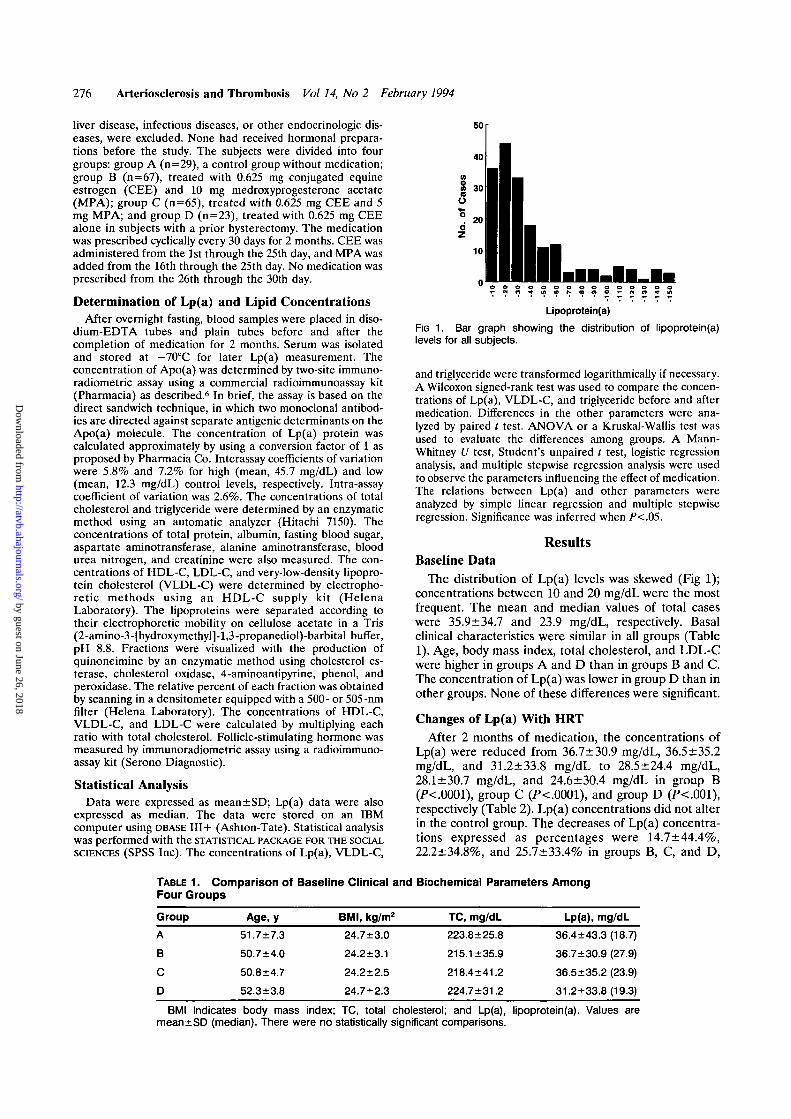
group (n= 126), in which the concentration of Lp(a) wasdecreased with medication, and a nonresponse group(n=29), in which the concentration of Lp(a) was in-creased or not changed, predictive variables for re-sponse were high concentrations of Lp(a), globulin, andtotal protein (Table 3). Among these, logistic regressionanalysis showed that high concentrations of Lp(a) andglobulin were independent variables. The differences inthe concentrations of Lp(a) before and after medicationwere related to basal concentrations of Lp(a) {r=.55,P<.0001; Fig 2) and total cholesterol (r=.18, P<.05)positively, and albumin (r=-.17, P<.05) negatively.Among them, only Lp(a) concentration was an indepen-dent variable. Percent changes of the concentration ofLp(a) were positively related to the concentrations ofglobulin (r=.26, i><.005), Lp(a) (r=.22, P<.005), andtotal protein (r=.21, P<.05). Among them, the concen-trations of globulin and Lp(a) were independent vari-ables by multiple stepwise regression analysis.
TABLE 3. Parameters Influencing the Effect of HRT onLipoprotein(a) Concentrations
ParameterNo Response
(n=29)Response(n=126)
Cholesterol, mg/dL
HDL-C, mg/dL
LDL-C, mg/dL
Lp(a), mg/dL
Triglyceride, mg/dL
Protein, g/dL
Albumin, g/dL
Globulin, g/dL
AST, IU/L
ALT, IU/L
SAP, IU/L
FSH, mlU/L
212.1+39.8
68.8±16.8
127.6±28.7
20.8±21.7
129.6±81.6
7.4±0.3
4.7±0.2
2.7±0.4
18.7±3.6
13.9±6.1
77.2±20.7
64.3±34.3
219.3+37.0
67.8±15.3
133.8±28.2
39.3±34.3
130.2±68.2
7.6+0.4
4.7±0.2
2.9±0.4
20.0±5.6
16.8±8.2
83.2+20.8
70.4±29.7
NS
NS
NS
<.001
NS
<.005
NS
<.005
NS
NS
NS
NS
HDL-C indicates high-density lipoprotein cholesterol; LDL-C,low-density lipoprotein cholesterol; Lp(a), lipoprotein(a); AST,aspartate aminotransferase; ALT, alanine aminotransferase;SAP, serum alkaline phosphatase; and FSH, follicle-stimulatinghormone. Values are mean±SD.
Changes in Other LipidsThe concentrations of total cholesterol were de-
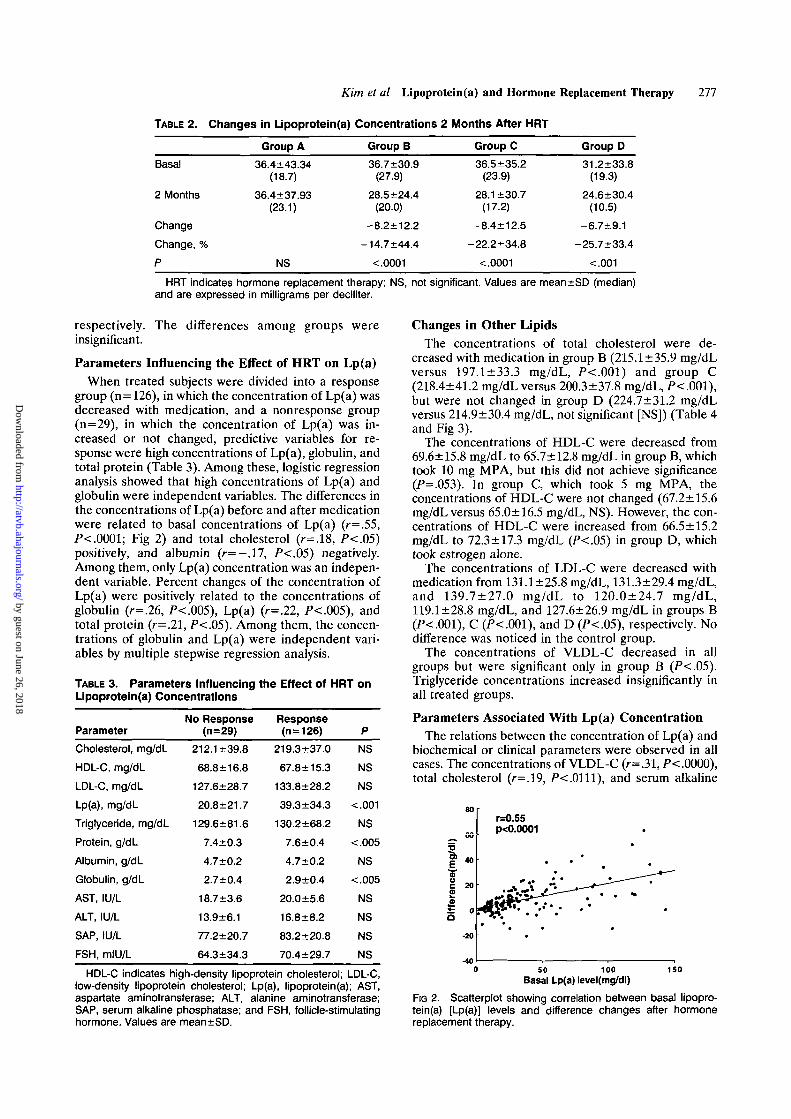
creased with medication in group B (215.1 ±35.9 mg/dLversus 197.1 + 33.3 mg/dL, /><.001) and group C(218.4±41.2 mg/dL versus 200.3±37.8 mg/dL, /><.001),but were not changed in group D (224.7±31.2 mg/dLversus 214.9±30.4 mg/dL, not significant [NS]) (Table 4and Fig 3).
The concentrations of HDL-C were decreased from69.6±15.8 mg/dL to 65.7±12.8 mg/dL in group B, whichtook 10 mg MPA, but this did not achieve significance(P=.O53). In group C, which took 5 mg MPA, theconcentrations of HDL-C were not changed (67.2+15.6mg/dL versus 65.0±16.5 mg/dL, NS). However, the con-centrations of HDL-C were increased from 66.5±15.2mg/dL to 72.3 ±17.3 mg/dL (P<.05) in group D, whichtook estrogen alone.
The concentrations of LDL-C were decreased withmedication from 131.1±25.8 mg/dL, 131.3±29.4 mg/dL,and 139.7±27.0 mg/dL to 120.0±24.7 mg/dL,119.1±28.8 mg/dL, and 127.6±26.9 mg/dL in groups B(P<.001), C (i><.001), and D (P<.05), respectively. Nodifference was noticed in the control group.
The concentrations of VLDL-C decreased in allgroups but were significant only in group B (P<.05).Triglyceride concentrations increased insignificantly inall treated groups.
Parameters Associated With Lp(a) ConcentrationThe relations between the concentration of Lp(a) and
biochemical or clinical parameters were observed in allcases. The concentrations of VLDL-C (r=.31, /><.0000),total cholesterol (r=.19, P-c.Olll), and serum alkaline
I
£a
40
-40
r=0.55p<0.0001
50 100Basal Lp(a) level(mg/dl)
150
FIG 2. Scatterplot showing correlation between basal lipopro-tein(a) [Lp(a)] levels and difference changes after hormonereplacement therapy.
by guest on June 26, 2018http://atvb.ahajournals.org/
Dow
nloaded from
278 Arteriosclerosis and Thrombosis Vol 14, No 2 February 1994
TABLE 4. Changes in Lipid Profiles 2 Months After HRT
TC
HDL-C
LDL-C
VLDL-C
TG
Basal
2 Month
P
Basal
2 Month
P
Basal
2 Month
P
Basal
2 Month
P
Basal
2 Month
P
Group A
223.8±25.8
212.9±34.8
NS
72.0±17.2
67.8+19.6
NS
134.4±20.9
131.5±27.3
NS
16.4±9.8
15.1+9.8
NS
137.8±71.4
133.2±53.5
NS
Group B
215.1 ±35.9
197.1 ±33.3
<.001
69.6±15.8
65.7±12.8
.053
131.1+25.8
120.0±24.7
<.01
17.0±15.9
12.6±7.6
<.O5
120.5±65.2
132.4±95.8
NS
Group C
218.4±41.2
200.3±37.8
<.001
67.2±15.6
65.0±16.5
NS
131.3±29.4
119.1 ±28.8
<.01
18.7±14.8
15.4±12.3
NS
136.0±76.7
140.0+86.1
NS
Group D
224.7±31.2
214.9±30.4
NS
66.5±15.2
72.3±17.3
<.O5
139.7±27.0
127.6±26.9
<.O5
18.4+11.7
15.0±12.3
NS
140.1 ±70.5
150.9±100
NS
HRT indicates hormone replacement therapy; TC, total cholesterol; HDL-C, high-density lipoprotein cholesterol;LDL-C, low-density lipoprotein cholesterol; VLDL-C, very-low-density lipoprotein cholesterol; and TG, triglyceride.Values are mean±SD and are expressed in milligrams per deciliter.
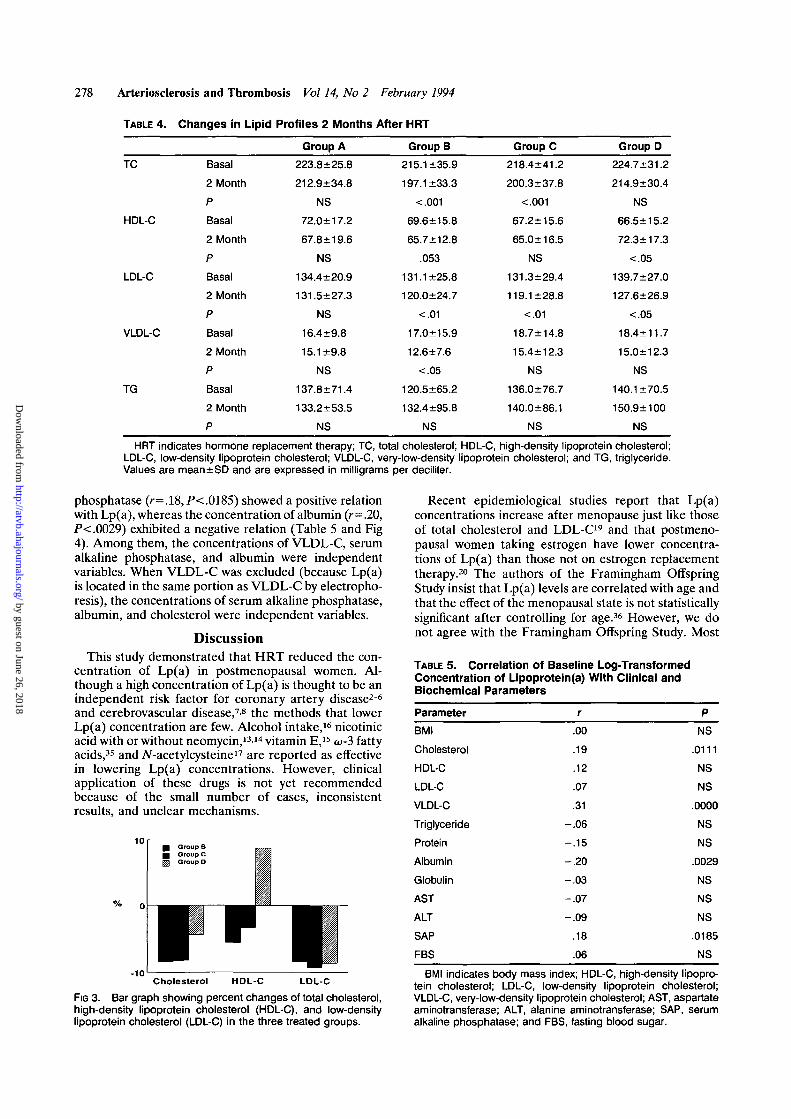
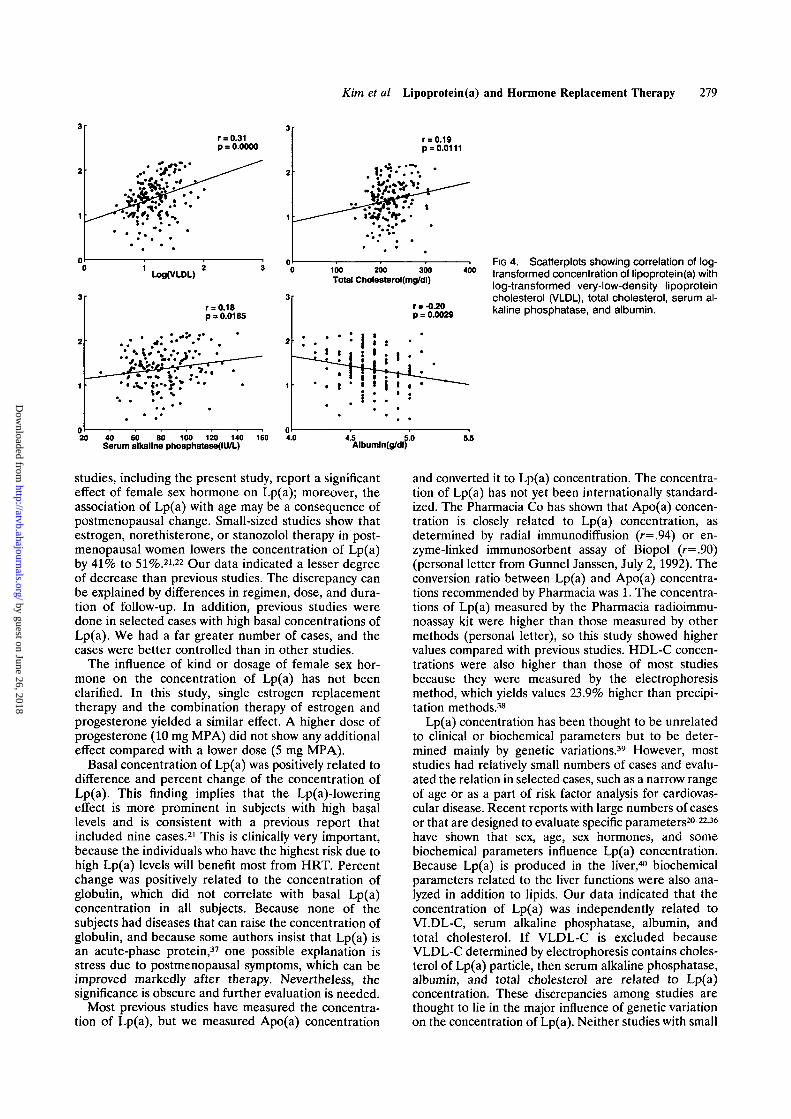
phosphatase (r=.18,P<.0!85) showed a positive relationwith Lp(a), whereas the concentration of albumin (r = .20,P<.0029) exhibited a negative relation (Table 5 and Fig4). Among them, the concentrations of VLDL-C, serumalkaline phosphatase, and albumin were independentvariables. When VLDL-C was excluded (because Lp(a)is located in the same portion as VLDL-C by electropho-resis), the concentrations of serum alkaline phosphatase,albumin, and cholesterol were independent variables.
DiscussionThis study demonstrated that HRT reduced the con-
centration of Lp(a) in postmenopausal women. Al-though a high concentration of Lp(a) is thought to be anindependent risk factor for coronary artery disease26
and cerebrovascular disease,7'8 the methods that lowerLp(a) concentration are few. Alcohol intake,16 nicotinicacid with or without neomycin,1314 vitamin E,15 w-3 fattyacids,35 and A^-acetylcysteine17 are reported as effectivein lowering Lp(a) concentrations. However, clinicalapplication of these drugs is not yet recommendedbecause of the small number of cases, inconsistentresults, and unclear mechanisms.
10
-10Cholesterol HDL-C LDL-C
FIG 3. Bar graph showing percent changes of total cholesterol,high-density lipoprotein cholesterol (HDL-C), and low-densitylipoprotein cholesterol (LDL-C) in the three treated groups.
Recent epidemiological studies report that Lp(a)concentrations increase after menopause just like thoseof total cholesterol and LDL-C19 and that postmeno-pausal women taking estrogen have lower concentra-tions of Lp(a) than those not on estrogen replacementtherapy.20 The authors of the Framingham OffspringStudy insist that Lp(a) levels are correlated with age andthat the effect of the menopausal state is not statisticallysignificant after controlling for age.36 However, we donot agree with the Framingham Offspring Study. Most
TABLE 5. Correlation of Baseline Log-TransformedConcentration of Lipoprotein(a) With Clinical andBiochemical Parameters
Parameter r P
BMI .00 NS
Cholesterol .19 .0111
HDL-C .12 NS
LDL-C .07 NS
VLDL-C .31 .0000
Triglyceride -.06 NS
Protein -.15 NS
Albumin -.20 .0029
Globulin -.03 NS
AST -.07 NS
ALT -.09 NS
SAP .18 .0185
FBS .06 NS
BMI indicates body mass index; HDL-C, high-density lipopro-tein cholesterol; LDL-C, low-density lipoprotein cholesterol;VLDL-C, very-low-density lipoprotein cholesterol; AST, aspartateaminotransferase; ALT, alanine aminotransferase; SAP, serumalkaline phosphatase; and FBS, fasting blood sugar.
by guest on June 26, 2018http://atvb.ahajournals.org/
Dow
nloaded from
Kim et al Lipoprotein(a) and Hormone Replacement Therapy 279
r = 0.31p = 0.0000
r = 0.19p = 0.0111
U>g(VLDL) 100 200 300Total Cholosterol(mg/dl)
400
r = 0.18p = 0.0185
•/ ' A : •**••**••I
r = -O.20p = 0.0029
FIG 4. Scatterplots showing correlation of log-transformed concentration of lipoprotein(a) withlog-transformed very-low-density lipoproteincholesterol (VLDL), total cholesterol, serum al-kaline phosphatase, and albumin.
. • : i •• | • :
I I 1 : I
20 40 60 80 100 120 140 160Serum alkaline phosphatase(IU/L) Album! n(g/dl)'
studies, including the present study, report a significanteffect of female sex hormone on Lp(a); moreover, theassociation of Lp(a) with age may be a consequence ofpostmenopausal change. Small-sized studies show thatestrogen, norethisterone, or stanozolol therapy in post-menopausal women lowers the concentration of Lp(a)by 41% to 51%.21-22 Our data indicated a lesser degreeof decrease than previous studies. The discrepancy canbe explained by differences in regimen, dose, and dura-tion of follow-up. In addition, previous studies weredone in selected cases with high basal concentrations ofLp(a). We had a far greater number of cases, and thecases were better controlled than in other studies.
The influence of kind or dosage of female sex hor-mone on the concentration of Lp(a) has not beenclarified. In this study, single estrogen replacementtherapy and the combination therapy of estrogen andprogesterone yielded a similar effect. A higher dose ofprogesterone (10 mg MPA) did not show any additionaleffect compared with a lower dose (5 mg MPA).
Basal concentration of Lp(a) was positively related todifference and percent change of the concentration ofLp(a). This finding implies that the Lp(a)-loweringeffect is more prominent in subjects with high basallevels and is consistent with a previous report thatincluded nine cases.21 This is clinically very important,because the individuals who have the highest risk due tohigh Lp(a) levels will benefit most from HRT. Percentchange was positively related to the concentration ofglobulin, which did not correlate with basal Lp(a)concentration in all subjects. Because none of thesubjects had diseases that can raise the concentration ofglobulin, and because some authors insist that Lp(a) isan acute-phase protein,37 one possible explanation isstress due to postmenopausal symptoms, which can beimproved markedly after therapy. Nevertheless, thesignificance is obscure and further evaluation is needed.
Most previous studies have measured the concentra-tion of Lp(a), but we measured Apo(a) concentration
and converted it to Lp(a) concentration. The concentra-tion of Lp(a) has not yet been internationally standard-ized. The Pharmacia Co has shown that Apo(a) concen-tration is closely related to Lp(a) concentration, asdetermined by radial immunodiffusion (r=.94) or en-zyme-linked immunosorbent assay of Biopol (r=.9O)(personal letter from Gunnel Janssen, July 2, 1992). Theconversion ratio between Lp(a) and Apo(a) concentra-tions recommended by Pharmacia was 1. The concentra-tions of Lp(a) measured by the Pharmacia radioimmu-noassay kit were higher than those measured by othermethods (personal letter), so this study showed highervalues compared with previous studies. HDL-C concen-trations were also higher than those of most studiesbecause they were measured by the electrophoresismethod, which yields values 23.9% higher than precipi-tation methods.38
Lp(a) concentration has been thought to be unrelatedto clinical or biochemical parameters but to be deter-mined mainly by genetic variations.39 However, moststudies had relatively small numbers of cases and evalu-ated the relation in selected cases, such as a narrow rangeof age or as a part of risk factor analysis for cardiovas-cular disease. Recent reports with large numbers of casesor that are designed to evaluate specific parameters20-2236
have shown that sex, age, sex hormones, and somebiochemical parameters influence Lp(a) concentration.Because Lp(a) is produced in the liver,40 biochemicalparameters related to the liver functions were also ana-lyzed in addition to lipids. Our data indicated that theconcentration of Lp(a) was independently related toVLDL-C, serum alkaline phosphatase, albumin, andtotal cholesterol. If VLDL-C is excluded becauseVLDL-C determined by electrophoresis contains choles-terol of Lp(a) particle, then serum alkaline phosphatase,albumin, and total cholesterol are related to Lp(a)concentration. These discrepancies among studies arethought to lie in the major influence of genetic variationon the concentration of Lp(a). Neither studies with small
by guest on June 26, 2018http://atvb.ahajournals.org/
Dow
nloaded from
280 Arteriosclerosis and Thrombosis Vol 14, No 2 February 1994
numbers of cases nor uncontrolled studies can overcomea high p error by genetic determination, and the influ-ence of parameters can be masked. Thus, investigationsthat compare the concentration of Lp(a) between inde-pendent groups must have large numbers of cases orlarge differences that overwhelm the genetic control.
In the 1970s, cohort studies for the effect of estrogenon cardiovascular disease showed different results, withrelative risks of 0.3 through I.6.24-25 But most cohortstudies in the 1980s reported that estrogen replacementtherapy in postmenopausal women reduces cardiovas-cular morbidity or mortality with relative risks of 0.3through 0.75.24-25 Several mechanisms have been pro-posed for the cardioprotective effect of estrogen.Among them, change of lipid profiles was the mostattractive.27-28 Estrogen replacement therapy in post-menopausal women reduced LDL-C and increasedHDL-C. Total cholesterol was either decreased or notchanged. In the present study, LDL-C and HDL-Cchanged as in previous studies, and in group D, to whomonly estrogen was administered, total cholesterol didnot change. These findings might be favorable for thecardiovascular system and are consistent with recentcohort studies. But the lipid change is not a return to thepremenopausal state, but rather the therapeutic effectof estrogen, because the concentrations of total choles-terol and LDL-C are increased and HDL-C is notchanged after menopause.36'4142
Endometrial cancer is one of the serious complica-tions of estrogen replacement therapy. When progester-one is added to prevent endometrial hyperplasia, therisk of endometrial cancer becomes negligible.30-31 It isgenerally accepted that progesterone decreases HDL-Cconcentration and increases the risk of cardiovasculardisease.27-32 Many studies have evaluated the influenceof progesterone on lipid profiles when it is sequentiallycombined with estrogen in postmenopausal women.However, the results of these small-sized studies are notconclusive.33-34 Recently some authors have insisted onthe innocuous nature of progesterone.20'41 The Athero-sclerosis Risk in Communities Study Investigators20
report the possibility that combination therapy is betterthan estrogen alone for the prevention of atherosclero-sis because it results in a decrease in triglyceride, factorVII, and protein C levels and that there is no differencein HDL-C levels between these two groups. In ourstudy, estrogen alone increased HDL-C, but the com-bination of 5 mg MPA with estrogen offset the effect ofestrogen on HDL-C, and the HDL-C concentration wasnot changed. The combination of 10 mg MPA withestrogen decreased HDL-C with borderline significance(i'=.053). These findings are consistent with old reportsbut are at odds with the new argument about theinnocuous nature of progesterone. Different resultsmight be explained by sampling time in the medicationcycle. In this study, blood was obtained after 25 days ofmedication. If sampling were done during the estrogenadministration period, the effect of progesterone mightbe masked. We believe that a long-term, large-scalefollow-up study is needed before definite conclusionscan be reached.
The combination therapy of estrogen and progester-one decreased LDL-C, and ultimately total cholesteroldecreased markedly because of the decrease of LDL-Cwithout a change in HDL-C. Because some authors
insist that a decreased HDL-C concentration is a moreimportant risk factor than high LDL-C in cardiovascu-lar disease in women,43 the cardioprotective effect ofestrogen cannot be applied to the combination therapyof estrogen and progesterone. In contrast to estrogenreplacement therapy, the lipid change that results fromcombination therapy is consistent with the premeno-pausal state.3641-42
In summary, estrogen replacement therapy in post-menopausal women lowers the concentration of Lp(a),especially in subjects with high basal concentrations. Itmight be one of the mechanisms for the cardioprotec-tive effect of estrogen replacement therapy. The com-bination of estrogen and progesterone did not result inany additional reduction of Lp(a) concentration, nor didthe dose of progesterone influence the results. Thus,HRT can be used for lowering the concentration ofLp(a) in selected patients. But because the combinationtherapy of estrogen and progesterone negated the effectof estrogen on HDL-C, the cardioprotective effect ofestrogen replacement therapy cannot be extended tocombination therapy.
AcknowledgmentsThis study was supported by a grant from the Cheil Re-
search Institute. We thank Mrs Mi Hyun Park and Mr DongRyong Yang for their expert laboratory assistance.
References1. Utermann G. The mysteries of lipoprotein(a). Science. 1989;246:
904-910.2. Berg K, Dahlen G, Frick MH. Lp(a) lipoprotein and pre-beta,-
lipoprotein in patients with coronary heart disease. Chn Genet.1974;6:230-235.
3. Dahlen GH, Guyton JR, Attar M, Farmer JA, Kautz JA, GottoAM. Association of levels of lipoprotein Lp(a), plasma lipids, andother lipoproteins with coronary artery disease documented byangiography. Circulation. 1986;74:758-765.
4. Genest J Jr, McNamara JR, Ordovas JM, Jenner JL, SilbermanSR, Anderson KM, Wilson PWF, Salem DN, Schaefer EJ. Lipo-protein cholesterol, apolipoprotein A-l and B and lipoprotein(a)abnormalities in men with premature coronary artery disease.JAm Coll Cardiol. 1992;19:792-802.
5. Hoefler G, Harnoncourt F, Paschke E, Mitrl W, Pfeiffer KH,Kostner GM. Lipoprotein(a): a risk factor for myocardial infarction.Arteriosclerosis. 1988;8:398-401.
6. Rosengren A, Wilhelmsen L, Erikssen E, Risberg B, Wedel H.Lipoprotein(a) and coronary heart disease: a prospective study ina general population sample of middle aged men. BMJ. 1990;301:1248-1251.
7. Murai A, Miyahara T, Fujimoto N, Matzuda M, Kameyama M.Lp(a) lipoprotein as a risk factor for coronary heart disease andcerebral infarction. Atherosclerosis. 1986;59:199-204.
8. Zenker G, Koeltringer P, Bone G, Niederkorn G, Pfeiffer K,Juergens G. Lipoprotein(a) as a strong indicator for cere-brovascular disease. Stroke. 1986;17:942-945.
9. Berg K, Leren TP. Unchanged serum lipoprotein(a) concen-trations with lovastatin. Lancet. 1989;2:812. Letter.
10. Vessby B, Kostner G, Lithell H, Thomis J. Diverging effects ofcholestyramine on apolipoprotein B and lipoprotein(a). Athero-sclerosis. 1982;44:61-71.
11. Alber JJ, Canaba VG, Warnick GR, Hazzard WR. Lp(a) lipo-protein: relation to sinking pre-/3 lipoprotein, hyperlipopro-teinemia and apolipoprotein B. Metabolism. 1975;24:1047-1054.
12. Maeda S, Okuno M, Abe A, Noma A. Lack of effect of probucol onserum lipoprotein(a) levels. Atherosclerosis. 1989;79:267-269.Letter.
13. Gurakar A, Hoeg JM, Kostner G, Papadopoulos NM, Brewer HBJr. Levels of lipoprotein Lp(a) decline with neomycin and niacintreatment. Atherosclerosis. 1985;57:293-301.
14. Lepre F, Campbell B, Crane S, Hickman P. Low-dose sustainedrelease nicotinic acid (Tri-B3) and lipoprotein(a). Am J Cardiol.1992;70:133.
by guest on June 26, 2018http://atvb.ahajournals.org/
Dow
nloaded from

Kim et al Lipoprotein(a) and Hormone Replacement Therapy 281
15. Noma A, Maeda S, Okuno M, Abe A, Muto Y. Reduction of serumlipoprotein(a) levels in hyperlipidemic patients with a-tocopherylnicotinate. Atherosclerosis. 1990;84:213-217.
16. Vaelimaeki M, Laitinen K, Ylikahrit R, Ehnholm C, Jauhiainen M,Bard JM, Fruchart JC, Taskinen MR. The effect of moderatealcohol intake on apolipoprotein A-I-containing lipoproteins andlipoprotein(a). Metabolism. 1991;40:1168-1172.
17. Gavish D, Brewer JL. Lipoprotein reduction by N-acetylcysteine.Lancet. 1991 ;337:203-204.
18. Alber JJ, Taggart HM, Applebaum-Bowden D, Haffner S, ChestnutCH, Hazzard WR. Reduction of lecithin-cholesterol acyltransferase,apolipoprotein D and the Lp(a) lipoprotein with anabolic steroidstanozolon. Biochim Biophys Acta. 1984;795:293-303.
19. Meilahn EN, Kuller LH, Matthews KA, Stein EA. Lp(a) concen-trations among pre- and postmenopausal women over time: theHealthy Women Study. Circulation. 1991;84(suppl II):II-546.Abstract.
20. Nabulsi AA, Folsom AR, White A, Patsch W, Heiss G, Wu KK,Szklo M. Association of hormone-replacement therapy withvarious cardiovascular risk factors in postmenopausal women.N EnglJMed. 1993;15:1069-1075.
21. Soma M, Fumagalli R, Paoletti R, Meschia M, Carena Miani M,Crosignani P, Ghanem K, Gaubatz J, Morrisett JD. Plasma Lp(a)concentration after oestrogen and progestagen in postmenopausalwomen. Lancet. 1991;1:612. Letter.
22. Farish E, Rolton HA, Barnes JF, Hart DM. Lipoprotein(a) con-centrations in postmenopausal women taking norethisterone. BMJ.1991;303:694.
23. Kannel WB, Hjortland MC, McNamara PM, Gordon T. Menopauseand risk of cardiovascular disease.,4/in Intern Med. 1976;85:447-452.
24. Knopp RH. The effect of postmenopausal estrogen therapy on theincidence of arteriosclerotic vascular disease. Obstet Gynecol. 1988;72:23S-30S.
25. Bush TL, Barrett-Conner E. Noncontraceptive estrogen use andcardiovascular disease. Epidemiol Rev. 1985;7:80-104.
26. Wilson PWF, Garrison RJ, Castelli WP. Postmenopausal estrogenuse, cigarette smoking and cardiovascular morbidity in women over60: the Framingham Study. N Engl J Med. 1985;313:1038-1043.
27. Lobo RA. Effects of hormone replacement on lipids and lipo-proteins in postmenopausal women. / Clin Endocrinol Metab. 1991;73:925-930.
28. Walsh BW, Schiff I, Rosner B, Greenberg L, Ravnikar V, SacksFM. Effects of postmenopausal estrogen replacement therapy onthe concentrations and metabolism of plasma lipoproteins. N EnglJMed. 1991;325:1196-1204.
29. Kloudy Williams K, Adams MR, Sidney Klophenstein H. Estrogenmodulates responses of atherosclerotic coronary arteries. Circu-lation. 1990;81:1680-1687.
30. Gambrell RD Jr. The menopause: benefits and risks of estrogen-progestogen replacement therapy. Fertil Steril. 1982;37:457-474.
31. Smith DC, Prentice R, Thompson DJ, Herrman WL. Associationof exogenous estrogen and endometrial carcinoma. N Engl J Med.1975;293:1164-1167.
32. Farish E, Fletcher CD, Hart DM, Dagen MM, Parkin DE. Lipo-protein and apoprotein levels in postmenopausal women duringtreatment with norethisterone. Clin Chim Acta. 1986;159:147-151.
33. Wahl P, Walden CW, Knopp R, Hoover J, Wallace R, Heiss G,Rifkind B. Effect of estrogen/progestin potency on lipid/lipoproteincholesterol. NEngl] Med. 1983;308:862-867.
34. Hirvonen E, Maelkoenen M, Manninen V. Effect of differentprogestogen on lipoproteins during postmenopausal replacementtherapy. N Engl J Med. 1981;304:560-563.
35. Schimidt EB, Klausen IC, Kristensen SD, Lervang HH, FaergemanO, Dyerberg J. The effect of n-3 polyunsaturated fatty acids onLp(a). Clin Chim Acta. 1991;198:271-278.
36. Jenner JL, Ordovas JM, Lamon-Fava S, Schaefer MM, WilsonPWF, Castelli WP, Schaefer EJ. Effect of age, sex, and menopausalstatus on plasma lipoprotein(a) levels: the Framingham OffspringStudy. Circulation. 1993;87:1135-1141.
37. Maeda S, Abe A, Seishima M, Makino K, Noma A, Kawade M.Transient changes of serum lipoprotein(a) as an acute phaseprotein. Atherosclerosis. 1989;78:145-150.
38. Naito HK. Reliability of lipid, lipoprotein, and apolipoproteinmeasurements. Clin Chem. 1988;34:B84-B94.
39. Boerwinkle E, Leffert CC, Lin J, Lackner C, Chiesa G, Hobbs HH.Apolipoprotein(a) gene accounts for greater than 90% of thevariation in plasma lipoprotein(a) concentrations. / Clin Invest.1992;90:52-60.
40. Tomlinson JE, McLean JW, Lawn RM. Rhesus monkey apoli-poprotein^): sequence, evolution, and site of synthesis. I BiolChem. 1989;264:5957-5965.
41. Gambrell RD Jr, Teran A. Changes in lipids and lipoproteins withlong-term estrogen deficiency and hormone replacement therapy.Am J Obstet Gynecol. 1991;165:307-317.
42. Heiss G, Tamir I, Davis CE, Tyroler HA, Rifkind BM, SchonfeldG, Jacobs D, Frantz ID Jr. Lipoprotein-cholesterol distributions ina selected North American population: the Lipid Research ClinicsProgram Prevalence Study. Circulation. 1980;61:302-315.
43. Bush TL, Fried LP, Barrett-Conner E. Cholesterol, lipoproteins,and coronary heart disease in women. Clin Chem. 1988;34:B60-B70.
by guest on June 26, 2018http://atvb.ahajournals.org/
Dow
nloaded from

C J Kim, H C Jang, D H Cho and Y K Minwomen.
Effects of hormone replacement therapy on lipoprotein(a) and lipids in postmenopausal
Print ISSN: 1079-5642. Online ISSN: 1524-4636 Copyright © 1994 American Heart Association, Inc. All rights reserved.
Avenue, Dallas, TX 75231is published by the American Heart Association, 7272 GreenvilleArteriosclerosis, Thrombosis, and Vascular Biology
doi: 10.1161/01.ATV.14.2.2751994;14:275-281Arterioscler Thromb Vasc Biol.
http://atvb.ahajournals.org/content/14/2/275World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://atvb.ahajournals.org//subscriptions/
at: is onlineArteriosclerosis, Thrombosis, and Vascular Biology Information about subscribing to Subscriptions:
http://www.lww.com/reprints
Information about reprints can be found online at: Reprints:
document.Permissions and Rights Question and AnswerFurther information about this process is available in theis being requested is located, click Request Permissions in the middle column of the Web page under Services.Clearance Center, not the Editorial Office. Once the online version of the published article for which permission
can be obtained via RightsLink, a service of the CopyrightArteriosclerosis, Thrombosis, and Vascular Biology Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on June 26, 2018http://atvb.ahajournals.org/
Dow
nloaded from
Related Documents











