Effects of Family History of Alcohol Use Disorders on Spatial Working Memory BOLD Response in Adolescents Andrea D. Spadoni, Andria L. Norman, Alecia D. Schweinsburg, and Susan F. Tapert From the Joint Doctoral Program at University of California and San Diego State University (ADSp); VA San Diego Healthcare System (ALN, ADSp, SFT); Department of Psychiatry (ADSc, SFT), University of California, San Diego, California. Abstract Background—A positive family history (FH) of alcohol use disorders (AUD) has been linked to increased risk for the development of AUD, and neurocognitive factors have been postulated as important underlying mechanisms of familial alcoholism transmission. Methods—We used functional magnetic resonance imaging (fMRI) during a spatial working memory (SWM) and vigilance paradigm to investigate potential neurodevelopmental differences linked to familial density of AUD in 72 adolescents aged 12 to 14 years. Results—Youth with denser family histories of AUD showed less activation during a simple vigilance condition relative to SWM in cingulate and medial frontal gyri (β = 0.28, p = 0.03), and a trend for more relative activity during rest (β = −0.25, p = 0.07) in this cluster. Conclusions—Youth with greater familial densities of AUD may be less successful at modulating activity of the default network, potentially indicating a greater propensity for task- independent thought or reduced inhibition of task-irrelevant processing. Failure to moderate activation of the default network may have implications for cognitive efficiency and goal directed behavior in youth with dense FH. Further, aberrant activation in cingulate regions may be linked to genetic variation in GABA receptor units, suggesting a useful endophenotype for risk associated with alcohol dependence. Keywords Adolescence; fMRI; Spatial Working Memory; Family History of Alcoholism; Default Network; Cingulate Youth with a positive family history (FHP) of alcohol use disorders (AUD) are 2 to 5 more times likely to develop drinking problems than those negative for this trait (FHN) (Cloninger et al., 1986; Schuckit, 1985). Underlying neurobiological mechanisms have been proposed as moderating this increased risk, as FHP youth often perform differently than FHN controls on tests of neurocognitive function. For example, nonabusing FHP adolescent males performed worse than FHN boys on tests of language functioning and academic achievement (Giancola et al., 1993; Hegedus et al., 1984; Najam et al., 1997; Poon et al., 2000; Sher et al., 2000; Tarter et al., 1984; Viken et al., 1999), organization of new information (Peterson et al., 1992), executive cognitive functioning (Giancola et al., 1996; Harden and Pihl, 1995), perseveration (Giancola et al., 1993), working memory (Corral et al., 1999; Harden and Pihl, 1995; Ozkaragoz et al., 1997), nonverbal memory (Sher et al., 1991), visuospatial skills (Berman and Noble, 1995; Corral et al., 1999; Garland et al., 1993; Reprint requests: Susan F. Tapert, PhD, University of California, San Diego, 3350 La Jolla Village Drive (116B), San Diego, CA 92161; Fax: 858-642-6340; E-mail: [email protected]. NIH Public Access Author Manuscript Alcohol Clin Exp Res. Author manuscript; available in PMC 2009 July 1. Published in final edited form as: Alcohol Clin Exp Res. 2008 July ; 32(7): 1135–1145. doi:10.1111/j.1530-0277.2008.00694.x. NIH-PA Author Manuscript NIH-PA Author Manuscript NIH-PA Author Manuscript

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Effects of Family History of Alcohol Use Disorders on SpatialWorking Memory BOLD Response in Adolescents
Andrea D. Spadoni, Andria L. Norman, Alecia D. Schweinsburg, and Susan F. TapertFrom the Joint Doctoral Program at University of California and San Diego State University(ADSp); VA San Diego Healthcare System (ALN, ADSp, SFT); Department of Psychiatry (ADSc,SFT), University of California, San Diego, California.
AbstractBackground—A positive family history (FH) of alcohol use disorders (AUD) has been linked toincreased risk for the development of AUD, and neurocognitive factors have been postulated asimportant underlying mechanisms of familial alcoholism transmission.
Methods—We used functional magnetic resonance imaging (fMRI) during a spatial workingmemory (SWM) and vigilance paradigm to investigate potential neurodevelopmental differenceslinked to familial density of AUD in 72 adolescents aged 12 to 14 years.
Results—Youth with denser family histories of AUD showed less activation during a simplevigilance condition relative to SWM in cingulate and medial frontal gyri (β = 0.28, p = 0.03), anda trend for more relative activity during rest (β = −0.25, p = 0.07) in this cluster.
Conclusions—Youth with greater familial densities of AUD may be less successful atmodulating activity of the default network, potentially indicating a greater propensity for task-independent thought or reduced inhibition of task-irrelevant processing. Failure to moderateactivation of the default network may have implications for cognitive efficiency and goal directedbehavior in youth with dense FH. Further, aberrant activation in cingulate regions may be linkedto genetic variation in GABA receptor units, suggesting a useful endophenotype for riskassociated with alcohol dependence.
KeywordsAdolescence; fMRI; Spatial Working Memory; Family History of Alcoholism; Default Network;Cingulate
Youth with a positive family history (FHP) of alcohol use disorders (AUD) are 2 to 5 moretimes likely to develop drinking problems than those negative for this trait (FHN) (Cloningeret al., 1986; Schuckit, 1985). Underlying neurobiological mechanisms have been proposedas moderating this increased risk, as FHP youth often perform differently than FHN controlson tests of neurocognitive function. For example, nonabusing FHP adolescent malesperformed worse than FHN boys on tests of language functioning and academicachievement (Giancola et al., 1993; Hegedus et al., 1984; Najam et al., 1997; Poon et al.,2000; Sher et al., 2000; Tarter et al., 1984; Viken et al., 1999), organization of newinformation (Peterson et al., 1992), executive cognitive functioning (Giancola et al., 1996;Harden and Pihl, 1995), perseveration (Giancola et al., 1993), working memory (Corral etal., 1999; Harden and Pihl, 1995; Ozkaragoz et al., 1997), nonverbal memory (Sher et al.,1991), visuospatial skills (Berman and Noble, 1995; Corral et al., 1999; Garland et al., 1993;
Reprint requests: Susan F. Tapert, PhD, University of California, San Diego, 3350 La Jolla Village Drive (116B), San Diego, CA92161; Fax: 858-642-6340; E-mail: [email protected].
NIH Public AccessAuthor ManuscriptAlcohol Clin Exp Res. Author manuscript; available in PMC 2009 July 1.
Published in final edited form as:Alcohol Clin Exp Res. 2008 July ; 32(7): 1135–1145. doi:10.1111/j.1530-0277.2008.00694.x.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Ozkaragoz and Noble, 1995; Ozkaragoz et al., 1997; Sher et al., 1991) and attention (Tarteret al., 1989). Multigen-erational transmission (Conrod et al., 1995; LeMarquand et al., 1999;Peterson et al., 1996; Pihl and Bruce, 1995), high familial density (Hill et al., 2000a), earlyAUD onset in father (Tarter et al., 1989), active paternal alcoholism (Ozkaragoz et al.,1997), and genotypic features (Berman and Noble, 1995) increase the link between FHP andcognitive functioning. However, other studies have not observed relationships between FHPstatus and neurocognition (Finn and Justus, 1999; Schuckit et al., 1987), and the neuralmechanisms predicting FHP individuals’ risk for AUD remains unclear.
In an attempt to link neurobehavioral differences in FHP individuals to their increased riskfor AUD, it has been proposed that a positive FH may involve familial transmission of asubtle neurodevelopmental delay. FHP youth have demonstrated smaller volumes of theright amygdala (Hill et al., 2001), which tends to increase in volume over childhood andadolescence. Slowed rate of change in P300 amplitude (Almasy et al., 1999; Begleiter et al.,1984; Polich et al., 1994; Porjesz et al., 1998) and delayed maturation of postural sway (Hillet al., 2000a,b) have also been found among FHP youth. Children of alcoholics demonstratesmaller intracranial volume, which may indicate reduced brain growth (Gilman et al., 2007).Differences in P300 amplitude and postural stability disappear over time, suggesting thatthese abnormalities may correspond to an inherited developmental lag (Bauer andHesselbrock, 1999; Hill et al., 1999; Polich et al., 1994). During this period of prolongedneurodevelopment, FHP youth who initiate drinking could be at increased risk for problembehaviors (Hill et al., 2000a; Hingson et al., 2006; King and Chassin, 2007). Therefore,understanding the neural characteristics of FHP youth may help determine potentialpremorbid abnormalities in the brain functioning of individuals who develop AUD and howthese factors contribute to increased risk.
The neural substrate of spatial working memory (SWM) may be especially relevant inidentifying mechanisms of increased risk in FHP individuals. The neural mechanisms ofspatial working memory (SWM) processing involve a front-oparietal network including thedorsolateral prefrontal cortex, posterior parietal cortices, cingulate regions, and medialfrontal cortex (Casey et al., 1997; Courtney et al., 1998; Goldman-Rakic, 1987; McCarthy etal., 1996). While frontal regions are linked to executive control and parietal cortices toaccurate and effortful performance (Nelson et al., 2000), the cingulate regions and medialfrontal gyrus contribute to tasks effecting conflict and discrimination between responses(Casey et al., 1997), and are part of a “default network” activating in response to simple orrest conditions (Greicius et al., 2003), particularly after cognitively challenging tasks, asprocessing resources reallocate from areas engaged in task requirements (McKiernan et al.,2003). Studies of nondrinking FHP individuals have identified disorganization of P300source density maps in the frontoparietal network (Hada et al., 2001), potentially indicatingaberrant frontoparietal circuitry (Rangaswamy et al., 2004a) involved in SWM processing,and raising the possibility that reorganization of alcoholics’ frontoparietal pathways used tocomplete SWM tasks (Pfefferbaum et al., 2001; Tapert et al., 2001, 2004) may be moderatedby premorbid FH effects. Therefore, differences in the neural substrate of SWM may belinked to FH status, and aid identification of factors promoting alcohol drinking or relatedbehaviors.
Because SWM substrates reorganize during adolescence (Nelson et al., 2000; Schweinsburget al., 2005a; Thomas et al., 1999), its examination during this period may capture a subtleneurodevelopmental lag in FHP youth. For example, compared to adults, children showmore widespread (Thomas et al., 1999) and bilateral (Courtney et al., 1997; Jonides et al.,1993; Smith et al., 1996) dorsolateral prefrontal cortex activation, while adults show moreparietal activity (Thomas et al., 1999). Across adolescence (i.e. ages 12 to 18), increasingpre-frontal and inferior parietal activation and decreasing superior parietal response as well
Spadoni et al. Page 2
Alcohol Clin Exp Res. Author manuscript; available in PMC 2009 July 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

as medial deactivation (i.e., activating more during baseline) is seen in response to SWM(Schweinsburg et al., 2005a). Thus, the underlying neural mechanisms of SWM developover adolescence, shifting more inferior and posterior, and lateralizing to the righthemisphere, possibly reflecting shifts in strategic and cortical organization (Scherf et al.,2006; Schweinsburg et al., 2005a; Thomas et al., 1999). Considering these and otheradolescent neurodevelopments (Giedd et al., 1999; Gogtay et al., 2004; Sowell et al., 2001),lags in neuromaturation may be detected, highlighting potential endophenotypes for thedevelopment of AUD.
Subtle delays in neurodevelopment might place FHP adolescents at increased risk forsubsequent AUD due to lagged acquisition of cognitive and behavioral correlates. Typicalneurodevelopments such as cortical thinning (Sowell et al., 2001), prefrontal myelination(Giedd et al., 1996; Gogtay et al., 2004), regional specialization (Durston et al., 2006)accompany improved performances on cognitive abilities throughout adolescence.Progressed spatial working memory, verbal working memory, and executive functioningoften parallel specific neurodevelopmental processes (Conklin et al., 2007; Durston et al.,2006; Eigsti et al., 2006; Shaw et al., 2006). Changes in reward neurocircuitry are alsotheorized to develop across adolescence (Galvan et al., 2007). In sum, delayedneurodevelopment during adolescence may lead to increased vulnerability for problembehaviors. The aim of this study is to contrast blood oxygen level dependent (BOLD)response patterns to SWM and simple vigilance in youth with varied familial densities ofAUD, utilizing a neurocognitive substrate that (1) changes in a predictable manner overadolescent development and (2) engages brain regions that appear sensitive to FH-relatedabnormalities. We hypothesize that youths with dense familial AUD will demonstrateBOLD activation patterns indicative of protracted neurodevelopment. Specifically, wepredict that with increasing FH density, there will be greater BOLD activation to SWM inmore superior and bilateral regions than among FH negative counterparts.
METHODSParticipants
Youth were selected from an ongoing longitudinal study that follows youth with and withoutrisk factors for AUD (i.e., conduct disorder and positive family histories) from ages 12 to 14through young-adulthood to identify neurocognitive risk factors for substance problems(Anderson et al., 2005; Nagel et al., 2005, 2006; Schweinsburg et al., 2005b). The focus ofthis analysis was to identify neural features of FHP youth vis-à-vis fMRI response to aSWM task. Recruitment fliers were mailed to households of San Diego area middle schoolstudents. Youth eligibility was preliminarily ascertained through a brief telephone interview.After a description of the study, written informed consent and assent, approved by theUniversity of California San Diego Human Research Protections Program, were obtainedfrom parents and adolescents, respectively. Eligible youth were administered a 90-minutedetailed screening interview covering personal substance use histories using the CustomaryDrinking and Drug Use Record (Brown et al., 1998), psychiatric diagnoses using theComputerized Diagnostic Interview Schedule for Children (C-DISC-4.0; Shaffer et al.,2000), and FH using the Family History Assessment Module (FHAM; Rice et al., 1995).The FHAM and C-DISC were also administered to parents by different interviewers tocorroborate adolescent reports. Diagnoses were considered present if either respondents’report or the combined report indicated the disorder. In cases of discrepancies, additionaldata were obtained, or data were coded to represent the lower level of functioning.Exclusionary criteria were: premature birth; reports of maternal drinking or drug use duringpregnancy; parental history of psychosis, bipolar I, or antisocial personality disorder; historyof neurological problems, head trauma, learning disabilities, Axis I psychiatric disorderother than conduct disorder or oppositional defiant disorder, or psychiatric medication use;
Spadoni et al. Page 3
Alcohol Clin Exp Res. Author manuscript; available in PMC 2009 July 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

MRI contraindications (e.g., braces); noncorrectable sensory impairments; nonfluency inEnglish; and left-handedness.
After excluding for excessive movement (n = 5), abnormal brain anatomy (n = 4), signaldrop-out (n = 4), neuropsychological scores below the normal range (n = 1), or ≤50%accuracy on the fMRI task (n = 2), remaining participants (n = 72, 43% female, 78%Caucasian) were ages 12 to 14, typically from upper middle to upper class families, andaverage to high average intellectually. History of alcohol and other drug use was minimal(see Table 1). Adolescents who met for conduct disorder (n = 7 “mild” and n = 5 “moderate”in severity) were included, as this was evenly distributed across FH density values.
MeasuresFamily History of Substance Use Disorders—Biological parents’ and grandparents’lifetime history of AUD was obtained from both parents and participant using the FHAM.Most participants had 2 biological parents as informants, and all participants had at leastone. For each participant, an index of FH density was computed: each parent with a historyof AUD contributed 0.5 and each grandparent with AUD history added 0.25 to the score(range 0 to 2) (Zucker et al., 1994). Stoltenberg et al. (1998) found this density measureprovided a valid characterization of familial AUD and may provide greater sensitivity thancategorical approaches.
Family Background—Socioeconomic status scores for each participant were derivedusing the Hollingshead scale, which combines educational attainment and occupation ofeach parent (Hollingshead, 1965).
Psychiatric Functioning—Diagnoses were derived for participants using youth andparent reports from the C-DISC-4.0 (Shaffer et al., 1996). The Child Behavior Checklist(CBCL; Achenbach and Rescorla, 2001) provided levels of psychopathological syndromesbased on parent report.
State Measures—Mood was assessed at the time of scanning with the Beck DepressionInventory (Beck, 1978) and state scale of the Spielberger State Trait Anxiety Inventory(Spielberger et al., 1970).
Self-Rating Scale for Pubertal Development—Physical development was assessedwith a sex-specific 5-item self-report measure (Petersen et al., 1988). Youth selected 1 of 5sex-specific statements ranging from “has not begun yet” to “seems complete” indicatingcurrent level of pubertal development. Multiple domains of secondary sex characteristicdevelopment (e.g., menstruation, facial hair growth, etc.) were sampled to most closelyascertain Tanner staging, characterized as pre-, early, mid-, late, or postpubertal. Pubertalstaging is relevant here, as any FH-related differences could account for developmentaldiscrepancies in brain activation.
Youth Substance Use—The Customary Drinking and Drug Use Record (Brown et al.,1998) provides a detailed assessment of past 3-month and lifetime use of alcohol, nicotine,and other drugs.
Neuropsychological Testing—The Vocabulary, Similarities, Block Design, andMatrices subtests of the Wechsler Abbreviated Scale of Intelligence (WASI) were used toensure participants’ scores fell within the normal range (Wechsler, 1999). Right-handednesswas confirmed with the Edinburgh Handedness Inventory (Oldfield, 1971).
Spadoni et al. Page 4
Alcohol Clin Exp Res. Author manuscript; available in PMC 2009 July 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

ProceduresParticipants completed the protocol across 2 appointments, which included a 1-hour scansession. Images were acquired on a 1.5 Tesla General Electric Signa LX scanner. A high-resolution structural image was collected in the sagittal plane using an inversion recoveryprepared T1-weighted 3-dimensional spiral fast-spin echo sequence (repetition time = 2,000ms; echo time = 16 ms; field of view = 240 mm; resolution = 0.9375 mm × 0.9375 mm ×1.328 mm) (Wong et al., 2000). Functional imaging was collected in the axial plane usingT2-weighted spiral gradient recall echo imaging (repetition time = 3,000 ms; echo time = 40ms; flip angle = 90°; field of view = 240 mm; 20 continuous slices; slice thickness = 7 mm;in-plane resolution = 1.875 mm × 1.875 nm; 156 repetitions).
Task stimuli were presented from a laptop computer through a data projector to a screen inthe MRI room near the foot of the scanner bed. The participant viewed stimuli through amirror mounted on the head coil. The fMRI task (Kindermann et al., 2004; Tapert et al.,2001), adapted from McCarthy and colleagues (McCarthy et al., 1994), was chosen toexplore the neural substrates of SWM functioning and probe the integrity of these brainregions in adolescents at risk for AUD. The task consists of 18 20-second blocks alternatingbetween experimental (SWM) and baseline (vigilance) condition, with blocks of rest(fixation cross in the center of the screen) in the beginning, middle, and end. In the SWMcondition, abstract line drawings appear 1 at a time in 1 of 8 locations. Participants are topress a button when a design appears in a location already occupied in that block. Onaverage, 3 of the 10 trials in each block are repeat locations, and repeats are 2-back. In thevigilance condition, the same stimuli are presented in the same locations, but a dot appearsabove figures on 30% of trials, and participants are to press a button when a dot appears.The purpose of the vigilance condition is to control for simple motor and attention processesinvolved in the SWM condition. In both conditions, stimuli are presented for 1,000 ms, andeach interstimulus interval is 1,000 ms (total time: 7 minutes, 48 seconds). Uponcompletion, participants and parents are financially compensated for their time.
Data AnalysisData were processed and analyzed using Analysis of Functional NeuroImages (AFNI;afni.nimh.nih.gov; Cox, 1996). Motion in the time series data was corrected by registeringeach acquisition to a minimally deviant repetition with an iterated least squares algorithm(Cox and Jesmanowicz, 1999); 3 rotational and 3 displacement parameters were output foreach repetition of each participant. Trained raters examined the corrected time series dataand removed repetitions containing residual visually discernible head motions. If >22% ofrepetitions were removed, the participant was not included (n = 5 not described in thispaper). On average, 6% of repetitions were removed due to movement. Time series datawere deconvolved with a reference vector coding the alternating task conditions whilecovarying for linear trends and the motion correction applied to control for spin historyeffects (Bandettini et al., 1993), and modeling typical delays in the hemodynamic response(Bandettini et al., 1993; Boynton et al., 1996). Functional data were transformed intostandardized space (Lancaster et al., 2000; Talairach and Tournoux, 1988) and resampledinto 3.5 mm3 voxels, and a spatial smoothing Gaussian filter (full-width half maximum =3.5 mm) was applied. These steps resulted in a fit coefficient for each voxel representingBOLD response to SWM relative to the vigilance task condition; separate coefficientsmodeled SWM relative to fixation, and vigilance relative to rest.
To determine whether bulk motion during the task differed as a function of FH, eachparticipant’s absolute mean for each of the 6 motion parameters across the time series datawas evaluated with Spearman rank-order correlations. For estimating task-correlated motion,
Spadoni et al. Page 5
Alcohol Clin Exp Res. Author manuscript; available in PMC 2009 July 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

the 6 parameters were correlated with the task reference vector for each participant. Thesevalues were also correlated with FH density scores with Spearman rank-order correlations.
A single sample t-test was conducted to indicate voxels responding to SWM relative tovigilance across all participants (n = 72). To control for Type I error, a combination of t-statistic magnitude and cluster volume thresholding was applied (Forman et al., 1995; Ward,1997) by only interpreting clusters comprised of at least 22 contiguously activated voxels ata < 0.025 (≥943 μl in volume). Eleven clusters surpassed this threshold. The largest cluster(342,486 μl) was reduced into 9 smaller regions of interest defined using regional proximity,established correlates of brain structure to function (Heilman and Valenstein, 1972, 2003),and the direction of BOLD activation (i.e., areas activating preferentially to SWM weregrouped separately from those activating to vigilance; see Fig. 1). For each of the resulting19 clusters (see Table 3), average activation for each participant was converted into z-scores.
Z-scores representing SWM response relative to vigilance for each of the 19 clusters werescreened for outliers using 3 regression-based diagnostic approaches: Studentized deletedresiduals > ±3, leverage values >0.17, and Mahalanobis distance > critical value > 16.27 (p= 0.001, dfbetas > ±1 or dffits > ±1). One case was determined as unduly influential in theright cerebellar tonsil.
To determine whether FH density predicted BOLD response in regions that reliablyactivated to SWM relative to vigilance, the average activations for 15 of these 19 clusterswere entered as dependent variables for hierarchical regressions performed in SPSS 14.0(Chicago, IL). The right cerebellar tonsil cluster was excluded as a statistical outlier (seeabove). Three other clusters (left cerebellar tonsil, and left and right precentral motorcortices) were not entered into the equation because FH effects were not expected in theseregions. Bulk motion in the roll and pitch directions were included as covariates, and FHdensity was entered on the second step. The presence of conduct disorder was not related toindependent or dependent variables, and mothers’ education was related to FH but notactivation, and therefore not included. Bonferroni correction was applied, and regressionswere considered significant at α ≤ 0.003.
RESULTSParticipant Characteristics
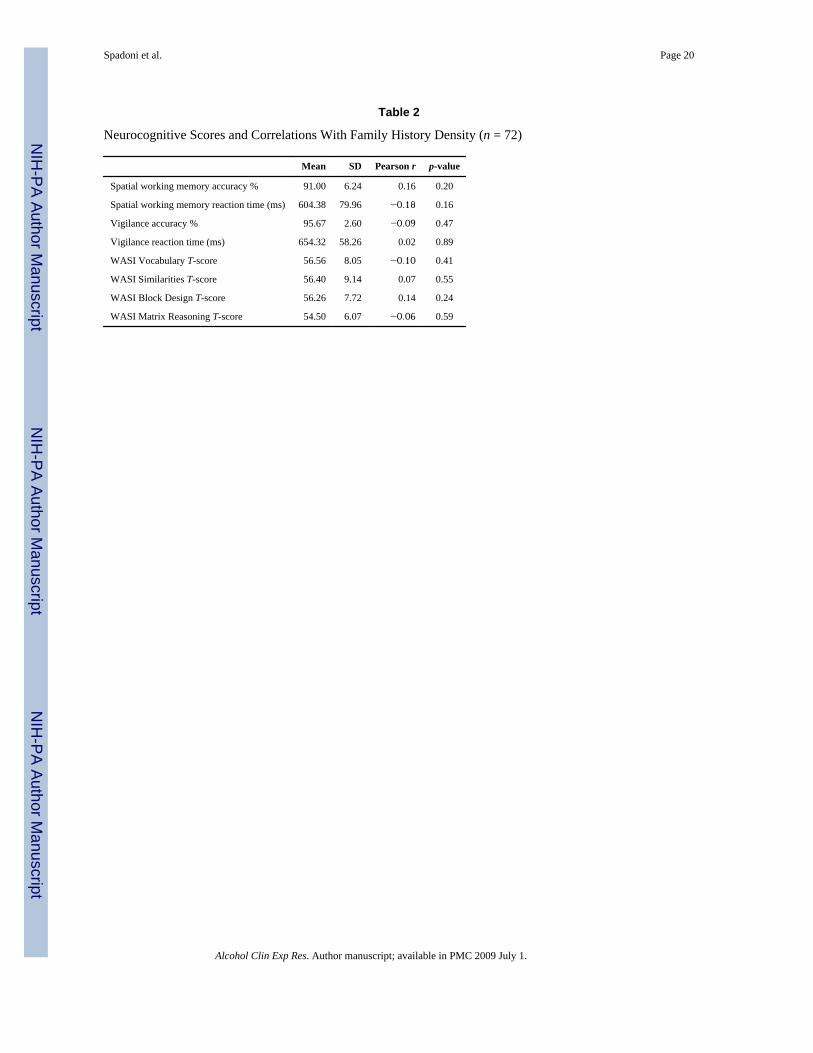
FH density was not significantly related to gender, conduct disorder diagnosis, CBCLscores, or other indicators of mood or demography. FH density negatively correlated withmaternal years of education (r = −0.25, p = 0.03, see Table 1). Performance onneuropsychological tests and the SWM task did not differ as a function of FH density (seeTable 2). Increased age was related to faster reaction time in the vigilance condition (r =−0.31, p = 0.01) and to better accuracy in SWM (r = 0.28, p = 0.02) and vigilanceconditions (r = 0.28, p = 0.02). Pubertal development scores indicated that, on average,males were nearly at mid-puberty, while females were between mid- to late puberty.Pubertal development was not related to SWM task performance or neuropsychological testscores (ps > 0.05).
MotionThe maximum values of rotation and displacement were modest (roll = 0.18°, pitch = 1.28°,yaw = 0.35°, superior = 0.80 mm, left = 0.24 mm, posterior = 0.39 mm). Spearman rank-order correlations demonstrated that FH density was not related to bulk motion in anydirection (ps > 0.20), but FH density was related to task-correlated motion in the roll (i.e.,ear-to-shoulder) and yaw (i.e., nodding) rotations (β = 0.27, p = 0.03; β = 0.28, p = 0.02,respectively).
Spadoni et al. Page 6
Alcohol Clin Exp Res. Author manuscript; available in PMC 2009 July 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

SWM Activation and Family HistoryAcross participants, the pattern of SWM relative to vigilance was consistent with existingliterature (Barch et al., 1997; Courtney et al., 1998; D’Esposito et al., 1998; Jonides et al.,1993; Smith and Jonides, 1998), involving bilateral dorsolateral prefrontal and parietalcortices activating to SWM blocks, and medial frontal and cingulate regions activating tovigilance blocks (see Table 3). A hierarchical regression determined whether FH densitywould predict SWM relative to vigilance response in the 15 areas of interest that reliablyactivated to the task. Task-correlated motion (roll and yaw) parameters were entered on step1, and centered FH density was entered on step 2. Considering a Bonferroni correction forthe number of regressions evaluated (α = 0.05/15 = 0.003), greater FH density was related todecreased SWM response relative to vigilance in a region encompassing bilateral cingulate,posterior cingulate, and extending into the medial frontal gyri at a trend level, above andbeyond effects of motion [F (3,66) = 4.26, p = 0.008; R2Δ = 7%, β = 0.28, p = 0.03] (seeFig. 2).
Follow-Up AnalysesTo clarify this pattern of activation, 2 single-sample t-tests in AFNI compared SWM relativeto fixation, and vigilance relative to fixation activations (a < 0.025, ≥943 μl, n = 70). In theSWM relative to fixation contrast, many regions activated preferentially to SWM, and thecingulate/medial frontal gyral region activated more during fixation blocks than duringSWM blocks. In the vigilance relative to fixation contrast, the cingulate/medial frontal gyruscluster, superior cingulate, medial frontal gyrus, and paracentral lobule showed significantlygreater BOLD response during fixation blocks, while more inferior areas of the cingulateactivated preferentially to the vigilance condition (see Fig. 3). Two separate regressionsexamined the relationship between BOLD response and FH density for each subregion ofactivation within the larger cluster, for the vigilance relative to fixation contrast. Thesuperior portion of the cluster, which activated preferentially to the fixation condition,showed a trend-level negative relationship between BOLD response to vigilance relative tofixation and increasing FH density [F(3,62) = 2.49, p = 0.07, β = −0.25, p = 0.07]. Theinferior area, which activated preferentially to the demands of vigilance, did not relate to FHdensity. Taken together, these results suggest less BOLD response during vigilance andmore activity during fixation (or rest-related response) with increasing FH density.
DISCUSSIONThe goal of this study was to explore the relationship between FH of AUD and brainresponse to SWM and simple vigilance in adolescents ages 12 to 14 with very limitedhistories of alcohol or drug use. We predicted there would be greater BOLD activation toSWM in more superior and bilateral brain regions with increasing FH density, suggesting aneurodevelopmental lag in brain regions sensitive to FH-related abnormalities. Contrary toour hypothesis, FH status did not predict activation to the SWM task. Therefore, findings donot necessarily support a neurodevelopmental delay as a mechanism through which youthwith familial AUD are at risk for AUD. However, adolescents with greater familial densitiesof AUD demonstrated less response than FHN youth during a simple vigilance baselinecondition in medial brain regions including the posterior cingulate, cingulate gyrus, andmedial frontal gyrus. In addition, participants with greater FH densities demonstrated moreBOLD response than FHN youth during rest periods in the more superior aspects of thismedial region. While unrelated to the a priori hypothesis, these findings may provideinteresting insights to the cognitive style of youth with familial AUD.
Midline structures such as the posterior cingulate cortex, medial frontal gyri, and anteriorcingulate have been consistently found to “deactivate,” or respond preferentially to the
Spadoni et al. Page 7
Alcohol Clin Exp Res. Author manuscript; available in PMC 2009 July 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

baseline condition as compared to the more demanding condition of many fMRI paradigms(Binder et al., 1999; Greicius et al., 2003; Hampson et al., 2006; McKiernan et al., 2003).This increased midline activity during a passive state (e.g., fixation) or conditions requiringlittle cognitive processing (e.g., vigilance), relative to regions needed for cognitivelydemanding conditions, has been linked to a propensity for stimulus independent thought, ormind wandering (Gusnard et al., 2001; Mason et al., 2007; McGuire et al., 1996; McKiernanet al., 2006). This could in turn relate to compromised appraisal of emergent risk situationsand reduced tendencies to carefully consider outcomes of behavioral selections. Weobserved that increased FH density was linked to more fixation-related BOLD response andless vigilance response in the cingulate. Potentially, this may indicate that adolescents withdenser FH engage in less stimulus independent thought during easy task conditions (i.e., inresponse to a vigilance task), but more such thought when task demands cease (i.e., duringfixation). A task with varied rest durations and task demands could help ascertain if thisactivation pattern is beneficial to performance by maintaining cognitive arousal (Mason etal., 2007), or counter-productive, by allocating resources away from the target task.
Previous work investigating the utility of the default network suggests that activation inmidline structures decreases in response to greater task difficulty (Greicius and Menon,2004; Greicius et al., 2003; McKiernan et al., 2003). McKiernan et al. (2003) contrastedBOLD activation during a parametrically-manipulated short-term memory condition toresponse obtained during a target discrimination condition. As task demands increased,processing reserves were reallocated from default areas to regions necessary for the activecondition. The authors concluded that the magnitude by which midline activation changedrepresented the degree to which resting state activity was inhibited to maintain successfultask-relevant processing. Functional connectivity studies also support the notion thatopposing activation patterns between default and higher-order cortical regions may serve toenhance performance (Greicius et al., 2003). Hampson et al. (2006) reported that increasingworking memory performance positively correlated with the strength of connectivity in thedefault network, and proposed that lateral prefrontal regions may actively suppressactivation of midline structures to augment performance. Similarly, a greater inversecorrelation between activity in the default network and task-related activation was positivelyassociated with intra-individual consistency in behavioral performance (Clare Kelly et al.,2008). In other words, the strength of the correlation may represent an index of neuralregulation between default and task-active “modes” (Clare Kelly et al., 2008). Together,current findings suggest that adolescents with dense FH may be less successful inmoderating the default network in response to cognitive load. This difference could havepotential consequences for downstream cognitive functioning, or serve as an additionalendophenotype to help identify youth at greater risk of developing CNS disinhibitory relatedbehaviors.
In FH dense adolescents, compromised neural regulation of midline regions may have directbehavioral sequelae. The functional consequences of these findings may be evident in thepoorer neurocognitive and academic performance of some individuals (Corral et al., 1999;Giancola et al., 1996; Hegedus et al., 1984; Najam et al., 1997; Poon et al., 2000), or markbehavioral disinhibition. However, in this sample, youth with greater familial AUD did notscore differently from FHN youth on neuropsychological tests, and measures of behavioralinhibition were not linked to this pattern of activation. Thus, an alternative explanation forsmaller magnitudes of vigilance-related activation with increasing FH density is that FH-dense adolescents were less challenged by the SWM condition than FHN youth, thusrequiring fewer cognitive resources to complete the task. Future studies that parametricallymanipulate task difficulty will help characterize how the default network develops acrossadolescence, and elucidate whether this finding supports an FH-related developmental lag.
Spadoni et al. Page 8
Alcohol Clin Exp Res. Author manuscript; available in PMC 2009 July 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Additionally, studies that include participants with more behavioral problems might uncovera relationship.
Our findings have potentially interesting implications for the interpretation of anomalouselectrophysiological characteristics theorized to be biological vulnerabilities for AUD andbehavioral disinhibition, such as reduced P300 amplitude and increased resting betafrequency (Bauer and Hesselbrock, 1993; Hesselbrock et al., 2001; Polich et al., 1994;Porjesz et al., 2005; Rangaswamy et al., 2004a). The relationship between genetic featuresthat determine characteristics of brain oscillations could participate in the mechanism forsuch predispositions. Specifically, EEG beta frequency has been linked to receptor genes forgamma-aminobutyric acid (GABA) that are involved in inhibitory neural networks(Rangaswamy et al., 2004b). The balance of inhibitory inter-neurons and excitatorypyramidal cells depends on the action of GABA subunits (Whittington et al., 2000). Becausealcoholics and their children demonstrate increased beta activity, this may indicate animbalance between excitation and inhibition (Porjesz and Rangaswamy, 2007). Variations inGABA receptor genes affect neural inhibition and thus the level of neural excitability,thereby influencing the predisposition to develop alcohol dependence and relateddisinhibitory disorders (Begleiter and Porjesz, 1999). Interestingly, GABA appears tospecifically influence activity in the default network regions (Northoff et al., 2007) that heredemonstrated decreased vigilance and increased fixation response in FHP youth. Northoff etal. (2007) reported that GABA concentration predicted the magnitude of negative BOLDresponse (relative to a resting state) in the anterior cingulate. Additionally, the anterior andposterior cingulate gyri and medial frontal gyri have been indicated as potential sources ofthe P300. For instance, Ardekani et al. (2002) found a correlation between event-relatedpotentials and BOLD activation to a visual odd-ball task. However, studies mappinganatomical origins of electrophysiological data have yet to reach consensus. Nonetheless, anintriguing body of emerging evidence suggests that suboptimal modulation of defaultnetworks in response to cognitive demands may relate to atypical electrophysiologicalactivity and behavioral disinhibition in nondrinking FHP individuals.
Additional data support the link between substance use risk and activation of structuresinvolved in the default network. Paulus et al. (2005) reported that decreased BOLDactivation in response to a decision making task in the posterior cingulate and medial frontalgyrus predicted relapse in stimulant dependent adults. They proposed that relapsingindividuals may be impaired in gathering adequate controlled processing resources duringdecision making, resulting in poor assessment abilities (Paulus et al., 2005). Taken togetherwith our results, difficulty engaging this region even for simple tasks may be connected toCNS disinhibition and risk for impulsive behaviors. While the neural underpinnings ofrelapse and risk for AUD are likely distinct, we suggest that subtle neural responsedifferences may influence the risk FHP adolescents have for developing patterns of problemdrinking.
This study has several limitations. First, participant motion, although relatively modest, wasrelated to FH density, and thus needed to be controlled statistically. Second, characterizingthe relationship between brain regions supporting higher-order cognitive demands and thedefault network will require functional connectivity analyses, which are beyond the scope ofthis report. Third, most participants had highly educated, affluent parents, and all were freefrom medical and psychiatric problems; while this minimizes a variety of potentialconfounds, results may not generalize to the broad population of youths at risk for AUD.Fourth, activation in the default network has not been characterized across adolescence, sowe cannot yet determine if the response pattern observed here represents a developmentallag. Finally, FH results were relatively modest and did not survive strict Bonferronicorrection.
Spadoni et al. Page 9
Alcohol Clin Exp Res. Author manuscript; available in PMC 2009 July 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

The current investigation suggests that functional neuroimaging may be useful foridentifying neurocognitive risk factors associated with familial density of AUD. Althoughwe did not find evidence that BOLD response specifically during spatial working memorydemands was related to FH, we observed that greater neural activity during rest and reducedactivity during an active baseline condition were linked to denser FH. We theorize that thismay indicate an imbalance between excitatory and inhibitory action during neuraltransmission determined by genetic variation in GABAergic mechanisms. Behaviorally,CNS disinhibition might translate into reduced ability to inhibit task irrelevant stimuli or anincreased risk for impulsive behavior. Further understanding of the default network inrelation to CNS disinhibition and behavioral inhibition may help inform preventionprogramming and identify youth at risk for substance problems. Longitudinal studies mayestablish a causal link between neurocognitive characteristics and the risk for developingAUD.
AcknowledgmentsResearch supported by NIAAA grants R01 AA13419, T32 AA013525, and F31 AA016727. The authors thankValerie Barlett, Lisa Caldwell, and Sonja Eberson for assistance with subject recruitment and data management,and Sandra A. Brown, Ph.D. and Edward P. Riley, Ph.D. for their continued support.
ReferencesAchenbach, TM.; Rescorla, LA. Manual for the ASEBA School-Age Forms & Profiles. University of
Vermont, Research Center for Children, Youth, & Families; Burlington, VT: 2001.Almasy L, Porjesz B, Blangero J, Chorlian DB, O’Connor SJ, Kuperman S, Rohrbaugh J, Bauer LO,
Reich T, Polich J, Begleiter H. Heritability of event-related brain potentials in families with ahistory of alcoholism. Am J Med Genet. 1999; 88:383–390. [PubMed: 10402506]
Anderson KG, Schweinsburg AD, Paulus MP, Brown SA, Tapert SF. Examining personality andalcohol expectancies using fMRI with adolescents. J Stud Alcohol. 2005; 66:323–331. [PubMed:16047521]
Ardekani BA, Choi SJ, Hossein-Zadeh GA, Porjesz B, Tanabe JL, Lim KO, Bilder R, Helpern JA,Begleiter H. Functional magnetic resonance imaging of brain activity in the visual oddball task.Brain Res Cogn Brain Res. 2002; 14:347–356. [PubMed: 12421658]
Bandettini PA, Jesmanowicz A, Wong EC, Hyde JS. Processing strategies for time-course data sets infunctional MRI of the human brain. Magn Reson Med. 1993; 30:161–173. [PubMed: 8366797]
Barch DM, Braver TS, Nystrom LE, Forman SD, Noll DC, Cohen JD. Dissociating working memoryfrom task difficulty in human prefrontal cortex. Neuropsychologia. 1997; 35:1373–1380. [PubMed:9347483]
Bauer LO, Hesselbrock VM. EEG, autonomic and subjective correlates of the risk for alcoholism. JStud Alcohol. 1993; 54:577–589. [PubMed: 8412148]
Bauer LO, Hesselbrock VM. P300 decrements in teenagers with conduct problems: implications forsubstance abuse risk and brain development. Biol Psychiatry. 1999; 46:263–272. [PubMed:10418702]
Beck, AT. Beck Depression Inventory (BDI). Psychological Corp; San Antonio, TX: 1978.Begleiter H, Porjesz B. What is inherited in the predisposition toward alcoholism? Alcohol Clin Exp
Res. 1999; 23:1125–1135. [PubMed: 10443977]Begleiter H, Porjesz B, Bihari B, Kissin B. Event-related brain potentials in boys at risk for
alcoholism. Science. 1984; 225:1493–1496. [PubMed: 6474187]Berman SM, Noble EP. Reduced visuospatial performance in children with the D2 dopamine receptor
A1 allele. Behav Genet. 1995; 25:45–58. [PubMed: 7755518]Binder JR, Frost JA, Hammeke TA, Bellgowan PS, Rao SM, Cox RW. Conceptual processing during
the conscious resting state. A functional MRI study. J Cogn Neurosci. 1999; 11:80–95. [PubMed:9950716]
Spadoni et al. Page 10
Alcohol Clin Exp Res. Author manuscript; available in PMC 2009 July 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Boynton GM, Engel SA, Glover GH, Heeger DJ. Linear systems analysis of functional magneticresonance imaging in human V1. J Neurosci. 1996; 16:4207–4221. [PubMed: 8753882]
Brown SA, Myers MG, Lippke L, Tapert SF, Stewart DG, Vik PW. Psychometric evaluation of theCustomary Drinking and Drug Use Record (CDDR): a measure of adolescent alcohol and druginvolvement. J Stud Alcohol. 1998; 59:427–438. [PubMed: 9647425]
Casey BJ, Castellanos FX, Giedd JN, Marsh WL, Hamburger SD, Schubert AB, Vauss YC, VaituzisAC, Dickstein DP, Sarfatti SE, Rapoport JL. Implication of right frontostriatal circuitry inresponse inhibition and attention-deficit/hyperactivity disorder. J Am Acad Child AdolescPsychiatry. 1997; 36:374–383. [PubMed: 9055518]
Clare Kelly AM, Uddin LQ, Biswal BB, Castellanos FX, Milham MP. Competition between functionalbrain networks mediates behavioral variability. Neuroimage. 2008; 39:527–537. [PubMed:17919929]
Cloninger CR, Sigvardsson S, Reich T, Bohman M. Inheritance of risk to develop alcoholism. NIDARes Monogr. 1986; 66:86–96. [PubMed: 3106820]
Conklin HM, Luciana M, Hooper CJ, Yarger RS. Working memory performance in typicallydeveloping children and adolescents: behavioral evidence of protracted frontal lobe development.Dev Neuropsychol. 2007; 31:103–128. [PubMed: 17305440]
Conrod PJ, Pihl RO, Ditto B. Autonomic reactivity and alcohol-induced dampening in men at risk foralcoholism and men at risk for hypertension. Alcohol Clin Exp Res. 1995; 19:482–489. [PubMed:7625586]
Corral MM, Holguin SR, Cadaveira F. Neuropsychological characteristics in children of alcoholics:familial density. J Stud Alcohol. 1999; 60:509–513. [PubMed: 10463807]
Courtney SM, Petit L, Maisog JM, Ungerleider LG, Haxby JV. An area specialized for spatial workingmemory in human frontal cortex. Science. 1998; 279:1347–1351. [PubMed: 9478894]
Courtney SM, Ungerleider LG, Keil K, Haxby JV. Transient and sustained activity in a distributedneural system for human working memory. Nature. 1997; 386:608–611. [PubMed: 9121584]
Cox RW. AFNI: software for analysis and visualization of functional magnetic resonanceneuroimages. Comput Biomed Res. 1996; 29:162–173. [PubMed: 8812068]
Cox RW, Jesmanowicz A. Real-time 3D image registration for functional MRI. Magn Reson Med.1999; 42:1014–1018. [PubMed: 10571921]
D’Esposito M, Aguirre GK, Zarahn E, Ballard D, Shin RK, Lease J. Functional MRI studies of spatialand nonspatial working memory. Brain Res Cogn Brain Res. 1998; 7:1–13. [PubMed: 9714705]
Durston S, Davidson MC, Tottenham N, Galvan A, Spicer J, Fossella JA, Casey BJ. A shift fromdiffuse to focal cortical activity with development. Dev Sci. 2006; 9:1–8. [PubMed: 16445387]
Eigsti IM, Zayas V, Mischel W, Shoda Y, Ayduk O, Dadlani MB, Davidson MC, Lawrence Aber J,Casey BJ. Predicting cognitive control from preschool to late adolescence and young adulthood.Psychol Sci. 2006; 17:478–484. [PubMed: 16771797]
Finn PR, Justus A. Reduced EEG alpha power in the male and female offspring of alcoholics. AlcoholClin Exp Res. 1999; 23:256–262. [PubMed: 10069554]
Forman SD, Cohen JD, Fitzgerald M, Eddy WF, Mintun MA, Noll DC. Improved assessment ofsignificant activation in functional magnetic resonance imaging (fMRI): use of a cluster-sizethreshold. Magn Reson Med. 1995; 33:636–647. [PubMed: 7596267]
Galvan A, Hare T, Voss H, Glover G, Casey BJ. Risk-taking and the adolescent brain: who is at risk?Dev Sci. 2007; 10:F8–F14. [PubMed: 17286837]
Garland MA, Parsons OA, Nixon SJ. Visual spatial learning in nonalcoholic young adults with andthose without a family history of alcoholism. J Stud Alcohol. 1993; 54:219–224. [PubMed:8459716]
Giancola PR, Martin CS, Tarter RE, Pelham WE, Moss HB. Executive cognitive functioning andaggressive behavior in preadolescent boys at high risk for substance abuse/dependence. J StudAlcohol. 1996; 57:352–359. [PubMed: 8776676]
Giancola PR, Peterson JB, Pihl RO. Risk for alcoholism, antisocial behavior, and responseperseveration. J Clin Psychol. 1993; 49:423–428. [PubMed: 8315046]
Spadoni et al. Page 11
Alcohol Clin Exp Res. Author manuscript; available in PMC 2009 July 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Giedd JN, Blumenthal J, Jeffries NO, Castellanos FX, Liu H, Zijdenbos A, Paus T, Evans AC,Rapoport JL. Brain development during childhood and adolescence: a longitudinal MRI study. NatNeurosci. 1999; 2:861–863. [PubMed: 10491603]
Giedd JN, Snell JW, Lange N, Rajapakse JC, Casey BJ, Kozuch PL, Vaituzis AC, Vauss YC,Hamburger SD, Kaysen D, Rapoport JL. Quantitative magnetic resonance imaging of human braindevelopment: ages 4–18. Cereb Cortex. 1996; 6:551–560. [PubMed: 8670681]
Gilman JM, Bjork JM, Hommer DW. Parental alcohol use and brain volumes in early- and late-onsetalcoholics. Biol Psychiatry. 2007; 15:15.
Gogtay N, Giedd JN, Lusk L, Hayashi KM, Greenstein D, Vaituzis AC, Nugent TF III, Herman DH,Clasen LS, Toga AW, Rapoport JL, Thompson PM. Dynamic mapping of human corticaldevelopment during childhood through early adulthood. Proc Natl Acad Sci U S A. 2004;101:8174–8179. [PubMed: 15148381]
Goldman-Rakic PS. Circuitry of primate prefrontal cortex and regulation of behavior byrepresentational memory. Handbook of physiology, the nervous system, higher functions of thebrain. 1987; 5:373–417.
Greicius MD, Krasnow B, Reiss AL, Menon V. Functional connectivity in the resting brain: a networkanalysis of the default mode hypothesis. Proc Natl Acad Sci U S A. 2003; 100:253–258. [PubMed:12506194]
Greicius MD, Menon V. Default-mode activity during a passive sensory task: uncoupled fromdeactivation but impacting activation. J Cogn Neurosci. 2004; 16:1484–1492. [PubMed:15601513]
Gusnard DA, Akbudak E, Shulman GL, Raichle ME. Medial prefrontal cortex and self-referentialmental activity: relation to a default mode of brain function. Proc Natl Acad Sci U S A. 2001;98:4259–4264. [PubMed: 11259662]
Hada M, Porjesz B, Chorlian DB, Begleiter H, Polich J. Auditory P3a deficits in male subjects at highrisk for alcoholism. Biol Psychiatry. 2001; 49:726–738. [PubMed: 11313040]
Hampson M, Driesen NR, Skudlarski P, Gore JC, Constable RT. Brain connectivity related to workingmemory performance. J Neurosci. 2006; 26:13338–13343. [PubMed: 17182784]
Harden PW, Pihl RO. Cognitive function, cardiovascular reactivity, and behavior in boys at high riskfor alcoholism. J Abnorm Psychol. 1995; 104:94–103. [PubMed: 7897058]
Hegedus AM, Alterman AI, Tarter RE. Learning achievement in sons of alcoholics. Alcohol Clin ExpRes. 1984; 8:330–333. [PubMed: 6377954]
Heilman KM, Valenstein E. Frontal lobe neglect in man. Neurology. 1972; 22:660–664. [PubMed:4673341]
Heilman, KM.; Valenstein, E. Clinical Neuropsychology. 4. Oxford University Press; New York:2003.
Hesselbrock V, Begleiter H, Porjesz B, O’Connor S, Bauer L. P300 event-related potential amplitudeas an endophenotype of alcoholism–evidence from the collaborative study on the genetics ofalcoholism. J Biomed Sci. 2001; 8:77–82. [PubMed: 11173979]
Hill SY, De Bellis MD, Keshavan MS, Lowers L, Shen S, Hall J, Pitts T. Right amygdala volume inadolescent and young adult offspring from families at high risk for developing alcoholism. BiolPsychiatry. 2001; 49:894–905. [PubMed: 11377407]
Hill SY, Shen S, Lowers L, Locke J. Factors predicting the onset of adolescent drinking in families athigh risk for developing alcoholism. Biol Psychiatry. 2000b; 48:265–275. [PubMed: 10960157]
Hill EM, Stoltenberg SF, Burmeister M, Closser M, Zucker RA. Potential associations among geneticmarkers in the serotonergic system and the antisocial alcoholism subtype. Exp ClinPsychopharmacol. 1999; 7:103–121. [PubMed: 10340151]
Hill SY, Shen S, Locke J, Lowers L, Steinhauer S, Konicky C. Developmental changes in posturalsway in children at high and low risk for developing alcohol-related disorders. Biol Psychiatry.2000a; 47:501–511. [PubMed: 10715356]
Hingson RW, Heeren T, Winter MR. Age at drinking onset and alcohol dependence: age at onset,duration, and severity. Arch Pediatr Adolesc Med. 2006; 160:739–746. [PubMed: 16818840]
Hollingshead, AB. Two-Factor Index of Social Position. Yale University Press; New Haven, CT:1965.
Spadoni et al. Page 12
Alcohol Clin Exp Res. Author manuscript; available in PMC 2009 July 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Jonides J, Smith EE, Koeppe RA, Awh E, Minoshima S, Mintun MA. Spatial working memory inhumans as revealed by PET. Nature. 1993; 363:623–625. [PubMed: 8510752]
Kindermann SS, Brown GG, Zorrilla LE, Olsen RK, Jeste DV. Spatial working memory amongmiddle-aged and older patients with schizophrenia and volunteers using fMRI. Schizophr Res.2004; 68:203–216. [PubMed: 15099603]
King KM, Chassin L. A prospective study of the effects of age of initiation of alcohol and drug use onyoung adult substance dependence. J Stud Alcohol Drugs. 2007; 68:256–265. [PubMed:17286344]
Lancaster JL, Woldorff MG, Parsons LM, Liotti M, Freitas CS, Rainey L, Kochunov PV, NickersonD, Mikiten SA, Fox PT. Automated Talairach atlas labels for functional brain mapping. HumBrain Mapp. 2000; 10:120–131. [PubMed: 10912591]
LeMarquand DG, Benkelfat C, Pihl RO, Palmour RM, Young SN. Behavioral disinhibition induced bytryptophan depletion in nonalcoholic young men with multigenerational family histories ofpaternal alcoholism. Am J Psychiatry. 1999; 156:1771–1779. [PubMed: 10553742]
Mason MF, Norton MI, Van Horn JD, Wegner DM, Grafton ST, Macrae CN. Wandering minds: thedefault network and stimulus-independent thought. Science. 2007; 315:393–395. [PubMed:17234951]
McCarthy G, Blamire AM, Puce A, Nobre AC, Bloch G, Hyder F, Goldman-Rakic P, Shulman RG.Functional magnetic resonance imaging of human prefrontal cortex activation during a spatialworking memory task. Proc Natl Acad Sci U S A. 1994; 91:8690–8694. [PubMed: 8078943]
McCarthy G, Puce A, Constable RT, Krystal JH, Gore JC, Goldman-Rakic P. Activation of humanprefrontal cortex during spatial and nonspatial working memory tasks measured by functionalMRI. Cereb Cortex. 1996; 6:600–611. [PubMed: 8670685]
McGuire PK, Paulesu E, Frackowiak RS, Frith CD. Brain activity during stimulus independentthought. Neuroreport. 1996; 7:2095–2099. [PubMed: 8930966]
McKiernan KA, D’Angelo BR, Kaufman JN, Binder JR. Interrupting the “stream of consciousness”:an fMRI investigation. Neuroimage. 2006; 29:1185–1191. [PubMed: 16269249]
McKiernan KA, Kaufman JN, Kucera-Thompson J, Binder JR. A parametric manipulation of factorsaffecting task-induced deactivation in functional neuroimaging. J Cogn Neurosci. 2003; 15:394–408. [PubMed: 12729491]
Nagel BJ, Barlett VC, Schweinsburg AD, Tapert SF. Neuropsychological predictors of BOLDresponse during a spatial working memory task in adolescents: what can performance tell us aboutfMRI response patterns? J Clin Exp Neuropsychol. 2005; 11:631–644.
Nagel BJ, Medina KL, Yoshii J, Schweinsburg AD, Moadab I, Tapert SF. Age-related changes inprefrontal white matter volume across adolescence. Neuroreport. 2006; 17:1427–1431. [PubMed:16932152]
Najam N, Tarter RE, Kirisci L. Language deficits in children at high risk for drug abuse. J ChildAdolesc Subst Abuse. 1997; 6:69–80.
Nelson CA, Monk CS, Lin J, Carver LJ, Thomas KM, Truwit CL. Functional neuroanatomy of spatialworking memory in children. Dev Psychol. 2000; 36:109–116. [PubMed: 10645748]
Northoff G, Walter M, Schulte RF, Beck J, Dydak U, Henning A, Boeker H, Grimm S, Boesiger P.GABA concentrations in the human anterior cingulate cortex predict negative BOLD responses infMRI. Nat Neurosci. 2007; 10:1515–1517. [PubMed: 17982452]
Oldfield RC. The assessment and analysis of handedness: the Edinburgh inventory. Neuropsychologia.1971; 9:97–113. [PubMed: 5146491]
Ozkaragoz TZ, Noble EP. Neuropsychological differences between sons of active alcoholic and non-alcoholic fathers. Alcohol Alcohol. 1995; 30:115–123. [PubMed: 7748268]
Ozkaragoz T, Satz P, Noble EP. Neuropsychological functioning in sons of active alcoholic,recovering alcoholic, and social drinking fathers. Alcohol. 1997; 14:31–37. [PubMed: 9014021]
Paulus MP, Tapert SF, Schuckit MA. Neural activation patterns of methamphetamine-dependentsubjects during decision making predict relapse. Arch Gen Psychiatry. 2005; 62:761–768.[PubMed: 15997017]
Petersen AC, Crockett LJ, Richards MH, Boxer AM. A self report measure of pubertal status:reliability, validity, and initial norms. J Youth Adolesc. 1988; 17:117–133.
Spadoni et al. Page 13
Alcohol Clin Exp Res. Author manuscript; available in PMC 2009 July 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Peterson JB, Finn PR, Pihl RO. Cognitive dysfunction and the inherited predisposition to alcoholism. JStud Alcohol. 1992; 53:154–160. [PubMed: 1560666]
Peterson JB, Pihl RO, Gianoulakis C, Conrod P, Finn PR, Stewart SH, LeMarquand DG, Bruce KR.Ethanol-induced change in cardiac and endogenous opiate function and risk for alcoholism.Alcohol Clin Exp Res. 1996; 20:1542–1552. [PubMed: 8986201]
Pfefferbaum A, Desmond JE, Galloway C, Menon V, Glover GH, Sullivan EV. Reorganization offrontal systems used by alcoholics for spatial working memory: an fMRI study. Neuroimage.2001; 14:7–20. [PubMed: 11525339]
Pihl R, Bruce K. Cognitive impairment in children of alcoholics. Alcohol Health Res World. 1995;19:142–147.
Polich J, Pollock VE, Bloom FE. Meta-analysis of P300 amplitude from males at risk for alcoholism.Psychol Bull. 1994; 115:55–73. [PubMed: 8310100]
Poon E, Ellis DA, Fitzgerald HE, Zucker RA. Intellectual, cognitive, and academic performanceamong sons of alcoholics, during the early school years: differences related to subtypes of familialalcoholism. Alcohol Clin Exp Res. 2000; 24:1020–1027. [PubMed: 10924005]
Porjesz B, Begleiter H, Reich T, Van Eerdewegh P, Edenberg HJ, Foroud T, Goate A, Litke A,Chorlian DB, Stimus A, Rice J, Blangero J, Almasy L, Sorbell J, Bauer LO, Kuperman S,O’Connor SJ, Rohrbaugh J. Amplitude of visual P3 event-related potential as a phenotypic markerfor a predisposition to alcoholism: preliminary results from the COGA Project. CollaborativeStudy on the Genetics of Alcoholism. Alcohol Clin Exp Res. 1998; 22:1317–1323. [PubMed:9756048]
Porjesz B, Rangaswamy M. Neurophysiological endophenotypes, CNS disinhibition, and risk foralcohol dependence and related disorders. Scientific World Journal. 2007; 7:131–141. [PubMed:17982586]
Porjesz B, Rangaswamy M, Kamarajan C, Jones KA, Padmanabhapillai A, Begleiter H. The utility ofneurophysiological markers in the study of alcoholism. Clin Neurophysiol. 2005; 116:993–1018.[PubMed: 15826840]
Rangaswamy M, Porjesz B, Ardekani BA, Choi SJ, Tanabe JL, Lim KO, Begleiter H. A functionalMRI study of visual oddball: evidence for frontoparietal dysfunction in subjects at risk foralcoholism. Neuroimage. 2004a; 21:329–339. [PubMed: 14741671]
Rangaswamy M, Porjesz B, Chorlian DB, Wang K, Jones KA, Kuperman S, Rohrbaugh J, O’ConnorSJ, Bauer LO, Reich T, Begleiter H. Resting EEG in offspring of male alcoholics: betafrequencies. Int J Psychophysiol. 2004b; 51:239–251. [PubMed: 14962576]
Rice JP, Reich T, Bucholz KK, Neuman RJ, Fishman R, Rochberg N, Hesselbrock VM, Nurnberger JIJr, Schuckit MA, Begleiter H. Comparison of direct interview and family history diagnoses ofalcohol dependence. Alcohol Clin Exp Res. 1995; 19:1018–1023. [PubMed: 7485811]
Scherf KS, Sweeney JA, Luna B. Brain basis of developmental change in visuospatial workingmemory. J Cogn Neurosci. 2006; 18:1045–1058. [PubMed: 16839280]
Schuckit MA. Genetics and the risk for alcoholism. Jama. 1985; 254:2614–2617. [PubMed: 4057470]Schuckit MA, Butters N, Lyn L, Irwin M. Neuropsychologic deficits and the risk for alcoholism.
Neuropsychopharmacology. 1987; 1:45–53. [PubMed: 3509067]Schweinsburg AD, Nagel BJ, Tapert SF. fMRI reveals alteration of spatial working memory networks
across adolescence. J Int Neuropsychol Soc. 2005a; 11:631–644. [PubMed: 16212691]Schweinsburg AD, Nagel BJ, Tapert SF. fMRI reveals alteration of spatial working memory networks
across adolescent development. J Int Neuropsychol Soc. 2005b; 11:631–644. [PubMed: 16212691]Shaffer D, Fisher P, Lucas CP, Dulcan MK, Schwab-Stone ME. NIMH Diagnostic Interview Schedule
for Children Version IV (NIMH DISC-IV): description, differences from previous versions, andreliability of some common diagnoses. J Am Acad Child Adolesc Psychiatry. 2000; 39:28–38.[PubMed: 10638065]
Shaffer D, Gould MS, Fisher P, Trautman P, Moreau D, Kleinman M, Flory M. Psychiatric diagnosisin child and adolescent suicide. Arch Gen Psychiatry. 1996; 53:339–348. [PubMed: 8634012]
Shaw P, Greenstein D, Lerch J, Clasen L, Lenroot R, Gogtay N, Evans A, Rapoport J, Giedd J.Intellectual ability and cortical development in children and adolescents. Nature. 2006; 440:676–679. [PubMed: 16572172]
Spadoni et al. Page 14
Alcohol Clin Exp Res. Author manuscript; available in PMC 2009 July 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Sher KJ, Bartholow BD, Wood MD. Personality and substance use disorders: a prospective study. JConsult Clin Psychol. 2000; 68:818–829. [PubMed: 11068968]
Sher KJ, Walitzer KS, Wood PK, Brent EE. Characteristics of children of alcoholics: putative riskfactors, substance use and abuse, and psychopathology. J Abnorm Psychol. 1991; 100:427–448.[PubMed: 1757657]
Smith EE, Jonides J. Neuroimaging analyses of human working memory. Proc Natl Acad Sci U S A.1998; 95:12061–12068. [PubMed: 9751790]
Smith EE, Jonides J, Koeppe RA. Dissociating verbal and spatial working memory using PET. CerebCortex. 1996; 6:11–20. [PubMed: 8670634]
Sowell ER, Thompson PM, Tessner KD, Toga AW. Mapping continued brain growth and gray matterdensity reduction in dorsal frontal cortex: inverse relationships during postadolescent brainmaturation. J Neurosci. 2001; 21:8819–8829. [PubMed: 11698594]
Spielberger, CD.; Gorsuch, RL.; Lushene, RE. Manual for the State-Trait Anxiety Inventory.Consulting Psychologists Press; Palo Alto, CA: 1970.
Stoltenberg SF, Mudd SA, Blow FC, Hill EM. Evaluating measures of family history of alcoholism:density versus dichotomy. Addiction. 1998; 93:1511–1520. [PubMed: 9926555]
Talairach, J.; Tournoux, P. Three-Dimensional Proportional System: An Approach to CerebralImaging. Thieme; New York: 1988. Coplanar Stereotaxic Atlas of the Human Brain.
Tapert SF, Brown GG, Baratta MV, Brown SA. fMRI BOLD response to alcohol stimuli in alcoholdependent young women. Addict Behav. 2004; 29:33–50. [PubMed: 14667419]
Tapert SF, Brown GG, Kindermann SS, Cheung EH, Frank LR, Brown SA. fMRI measurement ofbrain dysfunction in alcohol-dependent young women. Alcohol Clin Exp Res. 2001; 25:236–245.[PubMed: 11236838]
Tarter RE, Hegedus AM, Winsten NE, Alterman AI. Neuropsychological, personality, and familialcharacteristics of physically abused delinquents. J Am Acad Child Psychiatry. 1984; 23:668–674.[PubMed: 6512118]
Tarter RE, Jacob T, Bremer DL. Specific cognitive impairment in sons of early onset alcoholics.Alcohol Clin Exp Res. 1989; 13:786–789. [PubMed: 2690663]
Thomas KM, King SW, Franzen PL, Welsh TF, Berkowitz AL, Noll DC, Birmaher V, Casey BJ. Adevelopmental functional MRI study of spatial working memory. Neuroimage. 1999; 10:327–338. [PubMed: 10458945]
Viken RJ, Kaprio J, Koskenvuo M, Rose RJ. Longitudinal analyses of the determinants of drinkingand of drinking to intoxication in adolescent twins. Behav Genet. 1999; 29:455–461. [PubMed:10857250]
Ward, BD. Simultaneous Inference for FMRI Data. Biophysics Research Institute, Medical College ofWisconsin; Milwaukee, WI: 1997.
Wechsler, D. Manual for the Wechsler Abbreviated Scale of Intelligence. Psychological Corporation;San Antonio, TX: 1999.
Whittington MA, Traub RD, Kopell N, Ermentrout B, Buhl EH. Inhibition-based rhythms:experimental and mathematical observations on network dynamics. Int J Psychophysiol. 2000;38:315–336. [PubMed: 11102670]
Wong EC, Luh WM, Buxton RB, Frank LR. Single slab high resolution 3D whole brain imaging usingspiral FSE. Proc Int Soc Magn Reson Med. 2000; 8:683.
Zucker, RA.; Ellis, DA.; Fitzgerald, HE. Developmental evidence for at least two alcoholisms: I. In:Babor, TF.; Hesselbrock, V.; Meyer, RE.; Shoemaker, W., editors. Biopyschosocial variationamong pathways into symptomatic difficulty, in Types of Alcoholics: Evidence from Clinical,Experimental and Genetic Research. The New York Academy of Sciences; New York: 1994. p.134-146.
Spadoni et al. Page 15
Alcohol Clin Exp Res. Author manuscript; available in PMC 2009 July 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Fig. 1.(A) Results of the single sample t-test, showing regions with significant activation amongadolescent participants (n = 72) during the SWM task; red indicates increased BOLDresponse contrast to the SWM blocks, and blue indicates increased BOLD response contrastto the vigilance blocks (p < 0.025, clusters > 943 μl). (B) Delineation of regions resultingfrom reduction of the largest cluster that significantly activated to the SWM task.
Spadoni et al. Page 16
Alcohol Clin Exp Res. Author manuscript; available in PMC 2009 July 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
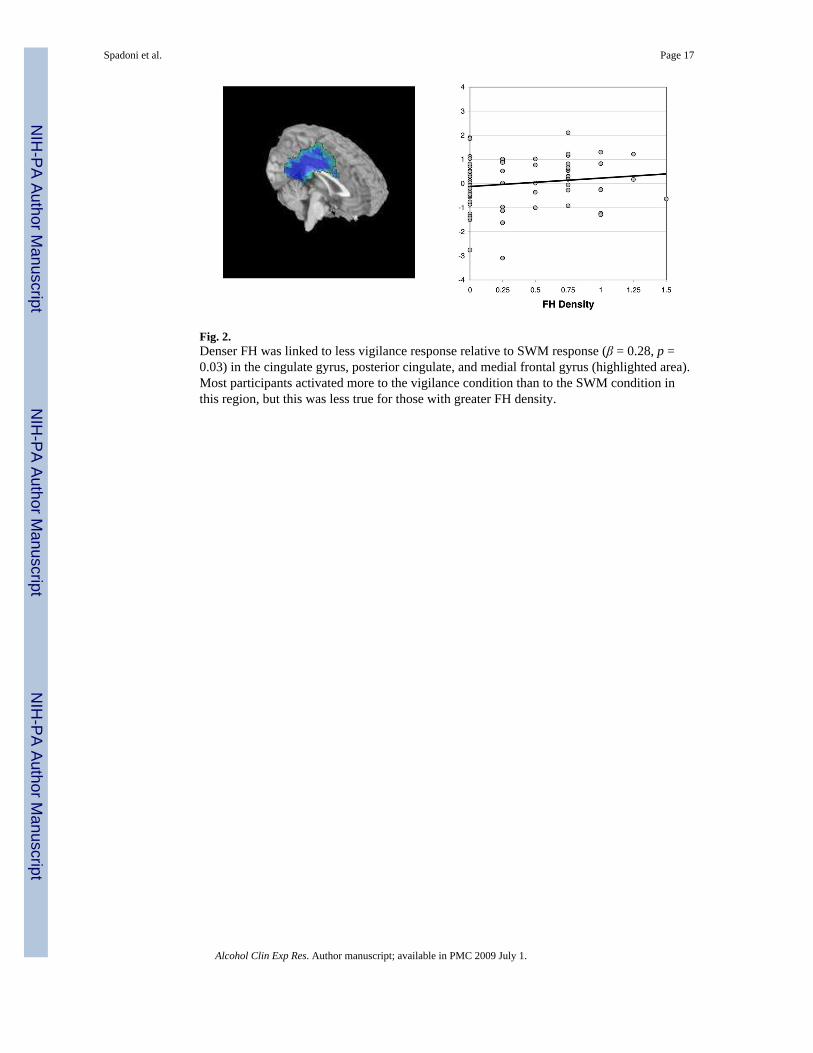
Fig. 2.Denser FH was linked to less vigilance response relative to SWM response (β = 0.28, p =0.03) in the cingulate gyrus, posterior cingulate, and medial frontal gyrus (highlighted area).Most participants activated more to the vigilance condition than to the SWM condition inthis region, but this was less true for those with greater FH density.
Spadoni et al. Page 17
Alcohol Clin Exp Res. Author manuscript; available in PMC 2009 July 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Fig. 3.Activation during vigilance relative to fixation was examined in the region in which SWMrelative to vigilance related to FH density. The area in white (superior cingulate; denotedwith crosshairs) preferentially activated to fixation, and was related to FH density at a trendlevel (see graph; β = −0.25, p = 0.07). The regions in black (posterior cingulate)preferentially activated to vigilance condition, but were not related to FH density scores.
Spadoni et al. Page 18
Alcohol Clin Exp Res. Author manuscript; available in PMC 2009 July 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Spadoni et al. Page 19
Table 1
Participant Characteristics and Correlations With Family History Density (n = 72)
M (SD) Pearson r p-value
Age in years (range 12–14) 13.25 (0.81) −0.11 0.34
Pubertal development
Girls 3.65 (0.71) −0.21 0.26
Boys 2.89 (0.70) −0.03 0.88
Father education 16.35 (2.20) −0.20 0.11
Mother education* 15.49 (2.32) −0.25 0.03
Father annual salary ($K) 87.88 (68.04) 0.34 0.77
Mother annual salary ($K) 35.59 (42.49) −0.12 0.31
CBCL Internalizing T-score 46.55 (6.41) 0.15 0.22
CBCL Externalizing T-score 45.85 (6.41) 0.08 0.55
Beck Depression Inventory total 2.60 (3.12) 0.05 0.71
Spielberger State Anxiety T-score 28.68 (7.03) 0.16 0.19
Lifetime uses of alcohol 0.85 (2.68) −0.10 0.40
Alcoholic drinks per occasion 0.17 (0.53) −0.08 0.50
Lifetime uses of cigarettes 0.10 (0.42) −0.14 0.25
Lifetime uses of marijuana 0.23 (0.74) −0.07 0.54
ANOVAs comparing FH density across categories:
% F-value
Sex (% female) 43 1.65 0.15
Ethnicity (% Caucasian) 78 1.12 0.36
Conduct disorder diagnosis 16 1.92 0.09
Parental marital status 1.34 0.25
Single 4
Married to each other 81
Divorced 14
Other 1
Living arrangement* 2.67 0.02
Both biological parents 81
Single parent 10
Parent and step-parent 8
*p < 0.05.
Alcohol Clin Exp Res. Author manuscript; available in PMC 2009 July 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Spadoni et al. Page 20
Table 2
Neurocognitive Scores and Correlations With Family History Density (n = 72)
Mean SD Pearson r p-value
Spatial working memory accuracy % 91.00 6.24 0.16 0.20
Spatial working memory reaction time (ms) 604.38 79.96 −0.18 0.16
Vigilance accuracy % 95.67 2.60 −0.09 0.47
Vigilance reaction time (ms) 654.32 58.26 0.02 0.89
WASI Vocabulary T-score 56.56 8.05 −0.10 0.41
WASI Similarities T-score 56.40 9.14 0.07 0.55
WASI Block Design T-score 56.26 7.72 0.14 0.24
WASI Matrix Reasoning T-score 54.50 6.07 −0.06 0.59
Alcohol Clin Exp Res. Author manuscript; available in PMC 2009 July 1.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Spadoni et al. Page 21
Tabl
e 3
Reg
ions
Act
ivat
ed to
SW
M R
elat
ive
to V
igila
nce
Con
ditio
ns (C
lust
ers >
943
μl,
p <
0.02
5, n
= 7
2)
RL
AP
ISB
A+ /−
SWM
Bra
in r
egio
ns
−13
−18
376,
8, 4
7+
Med
ial m
iddl
e, su
perio
r & in
ferio
r fro
ntal
gyr
i; an
terio
r to
post
erio
r cin
gula
tea
−7
5651
19, 7
, 40,
39,
5+
Prec
uneu
i, su
perio
r & in
ferio
r par
ieta
l lob
ules
174
5−
Occ
ipita
l, lin
gual
& fu
sifo
rm g
yria
6−46
119,
10−
Med
ial &
mid
dle
fron
tal g
yri
034
2918
, 30
−C
ingu
late
regi
ons a
nd m
iddl
e fr
onta
l gyr
us, p
oste
rior c
ingu
late
, med
ial f
ront
al g
yria
−42
106
13, 4
, 41,
42,
22,
21,
40
−In
sula
, stri
atum
; inf
erio
r fro
ntal
gyr
us; t
rans
vers
e, su
perio
r & m
iddl
e te
mpo
ral g
yri;
para
/hip
poca
mpa
l gyr
i, am
ygda
la; i
nfer
ior p
arie
tal
lobu
le
5132
842
, 21,
34
−Te
mpo
ral g
yri,
infe
rior p
arie
tal l
obul
e, su
pram
argi
nal,
mid
dle
& su
perio
r tem
pora
l gyr
ia
2521
335
, 28
−Pa
rahi
ppoc
ampa
l gyr
i, hi
ppoc
ampu
s, in
sula
, tha
lam
usa
26−12
844
, 47
+C
auda
te, i
nsul
a, c
ingu
late
, mid
dle
fron
tal g
yrus
; tha
lam
us, p
utam
en; i
nfer
ior f
ront
al g
yrus
−23
−11
10+
Insu
la, c
auda
te, s
triat
uma
31−47
910
+M
iddl
e &
supe
rior f
ront
al g
yri
225
47−
Para
cent
ral l
obul
esa
−32
−7
−34
38, 3
6, 2
1−
Supe
rior &
mid
dle
tem
pora
l gyr
i, un
cus
54−21
1045
−In
ferio
r fro
ntal
gyr
us, p
rece
ntra
l gyr
us
−56
29−15
20+
Mid
dle
tem
pora
l gyr
us in
to in
ferio
r tem
pora
l gyr
us
+, c
lust
ers a
ctiv
ated
pre
fere
ntia
lly to
the
SWM
con
ditio
n;
− , clu
ster
s act
ivat
ed p
refe
rent
ially
to th
e vi
gila
nce
cond
ition
.
a Div
ided
from
the
larg
est c
lust
er.
Alcohol Clin Exp Res. Author manuscript; available in PMC 2009 July 1.
Related Documents











