i “EFFECTIVENESS OF PLANNED TEACHING PROGRAMME ON KNOWLEDGE REGARDING POST OPERATIVE MANAGEMENT OF PATIENTS WITH CABG AMONG STAFF NURSES WORKING IN POST OPERATIVE CARDIAC UNITS OF SELECTED HOSPITALS AT MANGALORE”. By JOSEPHINA THOMAS Dissertation submitted to the Rajiv Gandhi University of Health Sciences Bangalore, Karnataka In partial fulfilment of the requirements for the degree of MASTER OF SCIENCE IN MEDICAL SURGICAL NURSING Under the guidance of Mrs. J. SATHYA SHENBEGA PRIYA, M.Sc (N) HOD Department of Medical Surgical Nursing Karavali College Of Nursing Science Mangalore, Karnataka.575013 2013

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
i
“EFFECTIVENESS OF PLANNED TEACHING PROGRAMME ON
KNOWLEDGE REGARDING POST OPERATIVE MANAGEMENT
OF PATIENTS WITH CABG AMONG STAFF NURSES WORKING
IN POST OPERATIVE CARDIAC UNITS OF SELECTED
HOSPITALS AT MANGALORE”.
By
JOSEPHINA THOMAS
Dissertation submitted to the
Rajiv Gandhi University of Health Sciences
Bangalore, Karnataka
In partial fulfilment of the requirements for the degree of
MASTER OF SCIENCEIN
MEDICAL SURGICAL NURSING
Under the guidance of
Mrs. J. SATHYA SHENBEGA PRIYA, M.Sc (N)HOD
Department of Medical Surgical Nursing
Karavali College Of Nursing Science
Mangalore, Karnataka.575013
2013
ii
© Rajiv Gandhi University of Health Sciences, Karnataka
DECLARATION BY THE CANDIDATE
I hereby declare that this dissertation/thesis titled “EFFECTIVENESS OF PLANNED
TEACHING PROGRAMME ON KNOWLEDGE REGARDING POST
OPERATIVE MANAGEMENT OF PATIENTS WITH CABG AMONG STAFF
NURSES WORKING IN POST OPERATIVE CARDIAC UNITS OF SELECTED
HOSPITALS AT MANGALORE” is a bonafide and genuine research work carried out
by me under the guidance of Mrs. J. SATHYA SHENBEGA PRIYA, M.Sc(N), Head of
the Department, Medical Surgical Nursing, Karavali College Of Nursing Science ,
Mangalore.
Date: Signature of the candidate
Place: MangaloreMs. JOSEPHINATHOMAS
iii
CERTIFICATE BY THE GUIDE
This is to certify that the dissertation entitled “EFFECTIVENESS OF PLANNED
TEACHING PROGRAMME ON KNOWLEDGE REGARDING POST
OPERATIVE MANAGEMENT OF PATIENTS WITH CABG AMONG STAFF
NURSES WORKING IN POST OPERATIVE CARDIAC UNITS OF SELECTED
HOSPITALS AT MANGALORE” is a bonafide research work done by Ms.
JOSEPHINA THOMAS in partial fulfillment of the requirement for the degree of
Master of Science in Nursing.
Date: Signature of the Guide
Place: Mangalore Mrs. J. Sathya Shenbega Priya
Asso. Professor & Hod
Medical Surgical Nursing Department,
Karavali College Of Nursing Science,
Mangalore, Karnataka.575013
iv
ENDORSEMENT BY THE HOD, PRINCIPAL/
HEAD OF THE INSTITUTION
This is to certify that the dissertation entitled “EFFECTIVENESS OF
PLANNED TEACHING PROGRAMME ON KNOWLEDGE REGARDING POST
OPERATIVE MANAGEMENT OF PATIENTS WITH CABG AMONG STAFF
NURSES WORKING IN POST OPERATIVE CARDIAC UNITS OF SELECTED
HOSPITALS AT MANGALORE” is a bonafide research work by Ms. JOSEPHINA
THOMAS under the guidance of Mrs. J. SATHYA SHENBEGA PRIYA, M.Sc(N),
Head of the Department, Medical Surgical Nursing, Karavali College Of Nursing
Science , Mangalore.
Seal and Signature of HOD Seal and Signature of Principal
Mrs. J. Sathya Shenbega Priya Prof. Stella Sagaya Mary J, MSc(N)
Asso. Professor & HOD Principal
Medical Surgical Nursing Department, Karavali College Of Nursing Science,
Karavali College Of Nursing Science, Mangalore, Karnataka.575013
Mangalore, Karnataka.575013
Date: Date:
Place: Mangalore Place: Mangalore
v
COPYRIGHT
Declaration by the candidate
I hereby declare that the Rajiv Gandhi University of Health Sciences, Karnataka
shall have all the rights to preserve, use and disseminate this dissertation/thesis in print or
electronic format for academic/research purpose.
Date:
Place: MangaloreJOSEPHINA THOMAS
© Rajiv Gandhi University of Health Sciences, Karnataka

vi
ACKNOWLEDGEMENT.
"Gratitude is the memory of heart"
With great pleasure and deep satisfaction I offer a bouquet of gratitude to everyone
around me who contributed towards the successful completion of my dissertation.
Above all I am grateful to the God almighty for His grace and blessings throughout
my study without which nothing would have been possible.
First and foremost is my sincere gratitude to Sri. S Ganesh Rao, chairman of
Karavali Group of Colleges and Mrs. Latha G Rao, director of Karavali Group of
Colleges for providing me an opportunity to study in their prestigious institute.
I express my sincere and whole hearted gratitude to Prof. Stella Sagaya Mary J,
Principal, Karavali College of Nursing Science, Mangalore for her constant support and
valuable guidance throughout the study.
I would like to express my deep sense of thanks to Mrs. J. Sathya Shenbega Priya
Associate Professor and Head of the Department of Medical Surgical Nursing Science
Mangalore, for her kind co-operation and suggestions for the improvent of this study,
under whose guidance this dissertation work had been carried out.
I extent my sincere thanks and appreciation to the management of District
Wenlock Hospital, KMC Hospital, Omega Hospital Mangalore, for giving me an
opportunity to conduct the study in their prestigious institution.
I extent my gratitude to all members of the research committee and all the teaching
faculty of Karavali College Of Nursing Science Mangalore, for their help rendered
throughout the study.
vii
I extent owe a debt of thanks to the entire Medical , Nursing, and Statistics experts
foe validating the contents of the tool and protocol and for their valuable suggestions,
inspiring discussions for their improvement of my study.
I am grateful to librarian of Karavali College of Nursing Science Mangalore, for his
help rendered.
I will be failing in my duty if do not recall the sample who willingly participated in
this study would not have been possible.
My expression of heartfelt gratitude and thanks in ample measure to my father and
mother-in-law, parents, sisters, brothers for their constant encouragement and support
offered throughout my study.
My expression of heartfelt gratitude and thanks is not sufficient for my loving
husband Mr. Josemon Thomas T who motivated me to do my higher studies and whose
constant encouragement and support helped me to do the study successfully.
I remain ever grateful to my child Selina Marium Jose for her motivation offered
throughout my study.
Thanks are also to my well wishers and friends who have helped me directly and
indirectly in the process of this study
Ms. Josephina Thomas
.
viii
LIST OF ABBREVIATIONS USED
PTCA : Percutaneous transluminal coronary angioplasty
ACB : Aorto coronary bypass
CABG : Coronary Artery Bypass Grafting
EHIRC : Escorts Heart Institute and Research Centre.
UK : United Kingdom
USA : United States of America.
SD : Standard deviation
PTP : Planned Teaching Programme
CHD : Coronary heart disease
CAG : Coronary Angiogram
SSI : Surgical Site Infection
HPA : Health Protection Agency
CAD : Coronary Artery Disease
CVD : Cardiovascular disease
ICU : Intensive Care Unit
PPC : Postoperative Pulmonary Complications
ICCU : Intensive Coronary Care Unit
US : United States
CR : Cardiac rehabilitation
DREAM : Diet, Relaxation, Exercise, Attitude, Motivation
CTICU : Cardio Thoracic Intensive Care Unit
PCI : Percutaneous coronary intervention
KMC : Kasturba Medical College
ix
ABSTRACT
Cardiovascular disease is the world's leading killer, accounting for 16.7 million or
29.2 per cent of total global deaths. Coronary Artery Bypass Graft (CABG) surgery is the
surgical procedure performed to relieve angina and reduce the risk of death from coronary
artery disease. It has been used to improve patient outcomes related to cardiac symptoms,
prolonged life and health related quality of life.
The care of the CABG patient is intense, complex and rewarding. A competent
nurse in the post-operative ICCU can facilitate patient adjustment, pain control, donor site
care, early mobilization, initiate exercise regimen, ensure adequate nutritional status,
coping of family, and also able to identify and report complication effectively, which can
save the life of the patient and pace up rehabilitation. Hence the researcher decided to
improve their knowledge by using PTP regarding post operative management of CABG
patients.
The objectives of the study are
1. To determine the level of knowledge among staff nurses regarding post operative
management of patients with CABG
2. To evaluate the effectiveness of planned teaching programme on level of knowledge
regarding post operative management of patients with CABG among staff nurses in Post
Operative Cardiac Units.
3. To find out the association between levels of knowledge regarding post operative
management of patients with CABG among staff nurses in Post Operative Cardiac Units.
with their selected demographic variables such as age, sex, educational qualification,
experience in Post Operative Cardiac Units, participation in any special training
programme on post operative management of CABG and availability of any additional
x
information on post operative management of patient with CABG within last one month of
research study.
Hypotheses
The following hypotheses will be tested at 0.05 level of significance.
H1: Mean post test knowledge score of postoperative management of patients with CABG
among staff nurses in Post Operative Cardiac Units will be significantly higher than mean
pre test knowledge score.
H2: There will be significant association between pre test level of knowledge score of
staff nurses regarding post operative management of patients with CABG and with their
demographic variables such as age, sex, educational qualification, experience in Post
Operative Cardiac Units, participation in any special training programme on post operative
management of CABG and availability of any additional information on post operative
management of patient with CABG within last one month of research study.
Method
An evaluatory approach with pre-experimental one group pre-test post-test design
was used for this study. The study was carried out in KMC, Mangalore and Omega
Hospital, Mangalore. The sample comprised of 50 staff nurses who met the inclusion
criteria and were chosen by purposive sampling technique. Formal written permission was
obtained from the authorities to conduct the study .Data was collected by administering a
structured knowledge questionnaire before and after the administration of planned
teaching programme. A post-test was conducted on the 7th day using the same tool. The
data was analyzed using descriptive and inferential statistics. Paired t’ test was used to find
xi
the effectiveness of planned teaching programme and chi-square was used to find the
association of pre-test knowledge score with selected demographic variables.
Results
The mean post-test knowledge score (X2 = 23.58) was higher than the mean pre-
test knowledge score (X1 = 13.28). The mean percentage knowledge score of pre-test was
maximum in the area of Unit II- Coronary artery bypass grafting (37%) and minimum in
the area of Unit I -Anatomy and Physiology of Heart (32%) whereas the mean percentage
knowledge score of post-test was maximum in the area of Unit I-Anatomy and Physiology
of Heart (82%) and less in the area of Unit III- Post- Operative Management Of CABG
Patient (78%).
The mean difference between post-test and pre-test knowledge score was highly
significant. There was no significant association of pre-test knowledge score with selected
demographic variables at 0 .05 level of significance.
Interpretation and conclusion
The study had shown that majority of the staff nurses had inadequate knowledge
on post operative management of CABG patient. However the knowledge has
significantly improved after the administration of PTP; hence it is concluded that Planned
Teaching Programme is an effective teaching strategy in improving the knowledge of staff
nurses regarding post operative management of CABG patient.
Keywords
Effectiveness; Planned Teaching Programme (PTP); Staff nurses; Post operative
management of patients with CABG; Post Operative Cardiac Unit.
xii
TABLE OF CONTENTS
CHAPTER
NOTITLE Pg. No
1. Introduction 1-8
2. Objectives 9-17
3. Review of literature 18-30
4. Research methodology 31-44
5. Results 45-66
6. Discussion 67-71
7. Conclusion 72-76
8. Summary 77-80
9. Bibliography 81-86
10. Annexure 87-136
xiii
LIST OF TABLES
Sl .No. TABLES Page No
1.
2.
Schematic representation of experimental design
Frequency and percentage distribution of demographic variablesof staff nurses.
33
47
3. Assessment of Pre-test and Post-test knowledge on postoperative management of patients with CABG among staffnurses working in Post Operative Cardiac Units.
54
4. Pre-test and post-test knowledge scores on post operativemanagement of patients with CABG among staff nursesworking in Post Operative Cardiac Units.
56
5. Area wise mean, SD and mean percentage of pre-test and post-test knowledge scores of staff nurses regarding the postoperative management of patients with CABG.
57
6. Effectiveness of PTP on item wise correct response of staffnurses in pre test and post test with regard to knowledgeregarding the anatomy and physiology of heart.
58
7. Effectiveness of PTP on item wise correct response of staffnurses in pre test and post test with regard to knowledgeregarding the Coronary artery bypass grafting.
59
7.1 Effectiveness of PTP on item wise correct response of staffnurses in pre test and post test with regard to knowledgeregarding the post- operative management of CABG patient.
60
7.2 Effectiveness of PTP on item wise correct response of staffnurses in pre test and post test with regard to knowledgeregarding the post- operative management of CABG patient.
61
7.3 Effectiveness of PTP on item wise correct response of staffnurses in pre test and post test with regard to knowledgeregarding the post- operative management of CABG patient.
62
8 Paired‘t’ test showing the significance of mean differencebetween pre-test and post-test knowledge scores of staff nursesafter the administration of PTP.
63
9 Association of the pre-test knowledge scores with selecteddemographic variables.
65
xiv
LIST OF FIGURES
Fig. No. TITLE Page No.
1 Theoretical frame work based on Ludwig von Bertalanffy
Theory(1968)
16
2 Schematic representation of the research design. 34
3 Pie diagram showing the percentage distribution of staff
nurses according to their age in years.
48
4 Exploded pie diagram showing the distribution of staff nurses
according to their gender.
49
5 Bar diagram showing the percentage distribution of staff
nurses according to their educational qualification.
50
6 Pie diagram showing the percentage distribution of staff
nurses according to their years of experience in Post
Operative Cardiac units.
51
7 Pyramid diagram showing percentage distribution of staff
nurses based on previous exposure to in-service educational
programs on care of CABG patients.
52
8 Bar diagram showing the percentage distribution of staff
nurses according to the availability of any additional
information on post operative management of patient with
CABG within last one month.
53
9 Ogive representing pre-test and post-test knowledge scores of
staff nurses regarding the post operative management of
patients with CABG.
55
xv
LIST OF ANNEXURES
Sl. No ANNEXURE Page No.
1.
2.
3.
Letter requesting permission for modification of title of the
study
Letter requesting permission for conducting pilot study,
reliability and pretesting of the tool.
Letter requesting permission to conduct main study
87
88
89-90
4. Letter requesting for expert opinion to establish content
validity of the research tool
91
92
5.
6.
Letter of acceptance form for tool validation
Content Validity Certificate 93
7. Criteria check list for validation of the tool 94-95
8. Letter seeking consent of subjects for participation in the
study.
96
9. Blue print for structured knowledge questionnaire regarding
post operative management of patients with CABG
97
10. Structured knowledge questionnaire to assess the
knowledge of staff nurses regarding pre and post operative
management of CABG
98-105
11. Answer key 106
12. Evaluation criteria for content validity of PTP on post
operative management of patients with CABG
107-108
13. Planned Teaching Programme 109-124
14. AV aids 125-128
15. List of experts who validated the tool and Structured
Teaching Programme
129
16. Statistical formulae used in the study 130
17. Master sheet data 131-136

1
1. INTRODUCTION
“Where your heart is there is your treasure also”
--Jesus Christ
Cardiovascular disease is the world's leading killer, accounting for 16.7 million or
29.2 per cent of total global deaths. Heart-attack victims are just the first wave of a
swelling population of Asians with heart problems; global cardiovascular disease related
deaths now occur in nations which cover most countries in Asia. The genetic
predisposition and acquisition of traditional risk factors at a rapid rate as a result of
urbanization seems to be the major cause. While efforts are being made to contain this
epidemic by educating public and applying preventive measures, the ever increasing
burden of patients with symptomatic and life threatening manifestations of the disease is
posing a major challenge. This requires a concerted effort to develop modern facilities to
treat these patients. The healthcare facilities to manage these high risk patients by
contemporary methods like percutaneous coronary revascularization and surgical
methods have shown a very promising trend during the last decade1.
Coronary artery bypass grafting is a surgical procedure performed to relieve
angina and reduce the risk of death from coronary artery disease. In angina or after a
heart attack (myocardial infarction) certain areas of the heart do not receive adequate
blood supply and these areas are starved of oxygen and nutrients and this result in areas
of the heart that are ischemic. In CABG these areas are re-perfused using 'free vein or
arterial bypass' that connect the normal areas of the arteries to less perfused areas and
2
'bypass' the blocked arteries. The bypass sections of the arteries or veins are harvested
from elsewhere from the body like the leg or the arm or from within the chest itself2.
According to the World Health Report, circulatory diseases such as heart attacks
kill more people than any other disease, accounting for at least 15 million deaths every
year. In developing countries these diseases also account for about 25% of all deaths.
Coronary heart disease accounted for more than 7 million deaths worldwide and was
responsible for about one-third of all deaths in industrialized countries. Cardiovascular
disease (CVD) was certified to be the primary cause of death in 43.33% of all deaths in
Australia and 41.97% in Victoria. The majority of these deaths were from coronary heart
disease (CHD). The Victorian Inpatient Minimum Database for the 12 month periods
highlights the rapid increase in the number of patients admitted to hospital with CHD and
a rapid increase in the number of major interventions in its treatment. The mortality
attributable to CVD in India is expected to rise by 103 per cent in men and 90 per cent in
women from 1985 to 20153.
CABG produces the most dramatic and rewarding relief of severe disability in a
high proportion of patients. The development of CABG provides an example of the
interdependence and interaction of many different fields of technology and science
leading to surgical advance. CABG is very effective at prolonging life and relieving
angina in appropriately selected patients. However, these patients are at high risk for
disease progression and recurrence of cardiac events such as angina, myocardial
infarction, repeat revascularization and death; hence CABG surgery is a stressor not only
to the patient but also to those caring after them4.
3
Today’s cardiovascular nursing care takes account of not only the individual but
also the family, work and leisure, from both health and medical care perspective along
the complete care chain; so training of nurses according to patients’ and their needs is
extremely important for improving the quality of life of the patient having undergone
cardiac surgery5.
NEED FOR THE STUDY
Coronary Artery Bypass Graft (CABG) surgery, recently called aortocoronary
bypass (ACB) is the surgical procedure performed to relieve angina and reduce the risk of
death from coronary artery disease. Arteries or veins from elsewhere in the patient’s body
are grafted to the coronary arteries to bypass atherosclerotic narrowing and improve the
blood supply to the coronary circulation supplying the myocardium. Commonly used
conduits in CABG are the internal mammary arteries, radial arteries and the greater
saphenous vein6.
During this century, the number of CABG surgeries done per day is increasing in
a tremendous manner. According to American Heart Association statistics, in 2009,
5, 48,000 bypass surgeries were done in United States. Of these 3, 23, 000 were men and
2, 25,000 were women7. Each year nearly 3, 00,000 bypass surgeries are performed in US
which means 61 in every 1, 00,000 people have a coronary bypass operation. In Britain,
only 6 in every 1, 00,000 have the same operation. In Japan, 1 in 1, 00,000 patients will
have a coronary bypass operation8.
A comparative study was conducted to study of the use of cardiac procedures
between the United States and Ontario, Canada. 224,258 Medicare patients were
compared to 9,444 patients of a similar age. In the U.S. patients 34.9% underwent
4
coronary angiograms versus 6.7% of the Canadian patients. For coronary artery bypass
surgery, 10.6% U. S. patients underwent this treatment, versus only 1.4% of the Canadian
patients. The 30 day mortality for the U.S. patients was 21.4% versus 22.3% for the
Canadian patients. At one year the mortality was 34.3% in the United States and 34.4% in
Canada. The study shows a strikingly higher use of cardiac procedures and the high
mortality rates related to CABG9.
Even as CVD rates skyrocket, the availability of better cardiology facilities and
dedicated cardiac centres have come as a welcome relief and India has seen a big leap in
the fields of interventional cardiology and cardiac surgery in recent times. Coronary
artery bypass graft surgery (CABG) was first performed in India in 1975 about 13 years
after its advent in 1962. In the mid 1990 some 10,000 CABG surgeries were being
performed annually in India. Presently the annual number is about 60000 according to
industry sources1.
A retrospective survey was conducted by Escorts Heart Institute and Research
Centre (EHIRC), New Delhi to explore the cardiovascular disease trends in India
between 1988 and 2005. According to EHIRC data 33,686 CABG surgeries were
performed in their hospitals during this period. Of these, majority (26,238) belonged to
the age group 51-65 years. In 2005 alone 3500 cases were performed and the highest
mortality rate (23%) was seen in patients >70 years10.
CABG patients require prompt support to go through the most crisis situation of
their life. The association of the heart with life and death intensifies their emotional and
psychological needs. It is the responsibility of the nurse to prioritize the needs carefully,
educate the client and family and enable the client to go through the crucial post
5
operative period safely. The immediate postoperative period for the patient who has
undergone cardiac surgery presents many challenges to the health care team. The goal of
postoperative care is to ensure that patients have good outcomes after surgical
procedures. A good outcome includes recovery without complications and adequate pain
management11.
A descriptive study was conducted in Brazil among 574 patients referred to
CABG surgery to analyze the incidence and temporal distribution of cardiac
complications during waiting for elective coronary artery bypass grafting and to identify
predictive factors of such complications. Median time to surgery was 126 days (5–1022).
Results revealed that sudden or cardiac death occurred in 2.5% and myocardial infarction
or unstable angina occurred in 22.9%. Most complications (72.1%) were observed within
120 days. The main factors predictive of sudden or cardiac death were severe left
ventricular dysfunction and heart failure. The researcher concluded that during long delay
for coronary artery bypass surgery, cardiac events are frequent and tend to occur early12.
Comprehensive ongoing assessment and report of any deviation from normal
status is crucial from the part of the nurse to ensure safe recovery from post-operative
period. Postoperative care involves assessment, diagnosis, planning, intervention, and
outcome evaluation. Nurse’s responsibility include monitoring neurological status,
respiratory status, cardiac status, peripheral vascular status, renal function, fluid and
electrolyte status and pain. As the patient regains consciousness and progresses through
the post operative period, the nurse expands the assessment to include parameters
indicative of psychological and emotional status. The family’s needs also should be
assessed. The nurse ascertains how they are coping with the situation; determines their
6
psychological, emotional, and spiritual needs and finds out whether they are receiving
adequate information about the patient condition13.
Good post operative care is easiest when the operation has been correctly
performed. The major areas of post operative care includes maintenance of patent airway,
infection prevention, wound care, hemodynamic monitoring, post operative exercises,
diet, prevention of post operative complications, medications, management of stress and
anxiety and follow up care. All this will reduce the incidence of complications after
cardiac surgeries and these patients will have a better quality of life. The major
complications following CABG include myocardial infarction, arrhythmias,
haemorrhage, cardiac tamponade, wound infection, deep vein thrombosis, pulmonary
embolism and respiratory problems requiring prolonged ventilation. The need for long
term follow up and aftercare of coronary artery surgical patients is stressed, so that the
true benefit to the patient in terms of improved quality and quantity of life may be
established14.
CABG wound site infections remain a challenge for health care institutions that
provide this surgical service. The multi-centre US National Health care Safety Network
(NHSN) reported in 2008 their 2 year data (2006-’07) for CABG SSI rates of 3.29%
(2,259/68,647). UK’s Health Protection Agency (HPA) reported a similar rate, 3.2% in
2008 from about 4,200 CABG procedures15.
A study was conducted in Mumbai to report post operative wound infection
among patients underwent CABG surgery. 615 patients were studied. Suspected sites of
infection were cultured and antibiotic susceptibility of cultured organisms was tested.
7
Postoperative follow up was for two months. The results showed that 116 (18.86%)
developed SSI, involving sternum 75%, leg 21.3%, and forearm sites 3.44%. Sternal site,
obesity, diabetes mellitus and female sex were associated with significantly higher
infection rates. It is concluded that the post CABG surgery SSI rate is high and sternum
and leg are the common infection sites. This suggests limited concern to the care of
surgical wound sites by nurses16.
An exploratory descriptive study based on naturalistic decision-making was
conducted in 2006 to describe critical care nurses' perceptions of assuming responsibility
for the nursing management of cardiac patients in the initial two-hour postoperative
period. Thirty-eight nurses were interviewed immediately following a two-hour
observation of their clinical practice. Nurses described their perceptions of managing
patients in terms of how they felt about making decisions for complex cardiac surgical
patients and in terms of how clinical processes unique to the admission phase impacted
their decision-making. Feelings expressed by nurses in this study highlight the need for
clinical supervision and appropriate allocation of resources during the immediate
recovery period after cardiac surgery. Nurses identified ways to improve clinical
processes that impacted their decision-making during the immediate recovery of cardiac
surgical patients17.
Nurse is the immediate caregiver for the patient, a competent nurse in the post-
operative cardiac units can facilitate patient adjustment, pain control, donor site care,
early mobilization, initiate exercise regimen, ensure adequate nutritional status, coping of
family, and also able to identify and report complication effectively, which can save the
life of the patient and pace up rehabilitation. From the clinical experience the researcher

8
felt that staff nurses in post operative cardiac units lack skill in handling CABG patients
effectively due to lack of knowledge regarding care. Based on the above information the
researcher felt the need to assess the knowledge of staff nurses in postoperative cardiac
units regarding post-operative management of CABG patients and planned to conduct a
teaching programme among staff nurses to enhance their knowledge.
9
2. OBJECTIVES
The development of a research problem is a creative process that depends on
imagination and ingenuity. Research questions are the specific queries researchers want
to answer in addressing the research problem. Research questions guide the types of data
collected in a study. Researcher who makes specific predictions about answers to
research questions pose hypotheses that are tested empirically53.
A research objective is a clear, concise, declarative statement, which provides
direction to investigate the variables53.
This chapter deals with main objectives of the study, the concepts involved and
the conceptual framework on which the study is based.
Statement of the problem:
“Effectiveness of planned teaching programme on knowledge regarding post operative
management of patients with CABG among staff nurses working in Post Operative
Cardiac Units of selected hospitals at Mangalore”.
Objectives of the study
The objectives of the study are
1. To determine the level of knowledge among staff nurses regarding post operative
management of patients with CABG
2. To evaluate the effectiveness of planned teaching programme on level of knowledge
regarding post operative management of patients with CABG among staff nurses in Post
Operative Cardiac Units.
10
3. To find out the association between levels of knowledge regarding post operative
management of patients with CABG among staff nurses in Post Operative Cardiac Units
with their selected demographic variables such as age, sex, educational qualification,
experience in Post Operative Cardiac Units, participation in any special training
programme on post operative management of CABG and availability of any additional
information on post operative management of patient with CABG within last one month
of research study.
Operational definitions
Effectiveness: Refers to the extent to which the teaching program will achieve the
desired result among staff nurses in enhancing knowledge regarding post operative
management of patients with CABG.
Planned teaching programme: In this study, planned teaching program refers to
systematically developed instructional and teaching aid designed for educating the
Post Operative Cardiac Units staff nurses regarding post-operative management of
patients with CABG.
Knowledge: In this study, knowledge refers to the responses given by the staff nurses
in the Post Operative Cardiac Units regarding post-operative management of patients
with CABG.
Post Operative Cardiac Units Staff Nurses: in this study staff nurses are,
professionally qualified nurses working in Post Operative Cardiac Units of the
selected hospital with the age group of 20-60 years.
Coronary Artery Bypass Grafting (CABG): CABG is a surgical procedure
performed to relieve angina and reduce the risk of death from coronary artery disease.
11
Arteries or veins from elsewhere in the patient’s body are grafted to the coronary
arteries to bypass atherosclerotic narrowing and improve the blood supply to the
coronary circulation supplying the myocardium (heart muscle).
Post-operative care: Care given after surgery until the patient is discharged from the
hospital or surgicenter and, in some cases, continuing on an ambulatory basis.
Postoperative care is aimed at meeting the patient's physical and psychological needs
directly after surgery.
Assumption
The study assumes that:
1. Staff nurses working in Post Operative Cardiac Units have inane knowledge
regarding post operative management of CABG patients.
2. Planned teaching programme may be effective in enhancing knowledge regarding
post operative management of CABG patients among staff nurses in Post Operative
Cardiac Units.
3. Planned teaching programme may result in enhancing competency of staff nurses and
may encourage use of evidence based practices.
4. Planned teaching programme may result in better nurse-patient relationship and
increase patient satisfaction.
Delimitation
The study is delimited to staff nurses
1. Between the age group of 20-60 years.
2. Working in Post Operative Cardiac Units of selected hospitals at Mangalore.
12
Hypotheses
The following hypotheses will be tested at 0.05 level of significance.
H1: Mean post test knowledge score of postoperative management of patients with
CABG among staff nurses in Post Operative Cardiac Units will be significantly higher
than mean pre test knowledge score.
H2: There will be significant association between pre test level of knowledge score of
staff nurses regarding post operative management of patients with CABG and with their
demographic variables such as age, sex, educational qualification, experience in Post
Operative Cardiac Units, participation in any special training programme on post
operative management of CABG and availability of any additional information on post
operative management of patient with CABG within last one month of research study.
Variables
Variables are an attribute of a person or objects that varies or takes different values.
Independent variable: Planned teaching programme on knowledge regarding
postoperative management of CABG patients.
Dependent variable: Level of knowledge among staff nurses regarding post-
operative management of CABG.
Conceptual framework
A conceptual framework broadly presents an understanding of the phenomenon of
interest and reflects the assumptions and philosophic views of the model designer.
13
A conceptual frame work is a theoretical approach to the study of problems that
are scientifically based and emphasis the selection arrangement and classification of its
concepts18.
The purposes of the conceptual framework are to organize concepts that
represent essential knowledge that might be used by many disciplines and to construct
theories from the framework and test them from the perspective of nursing as a
discipline. The conceptual framework includes goal, structure, function, resources and
decision making; these are known as essential elements.
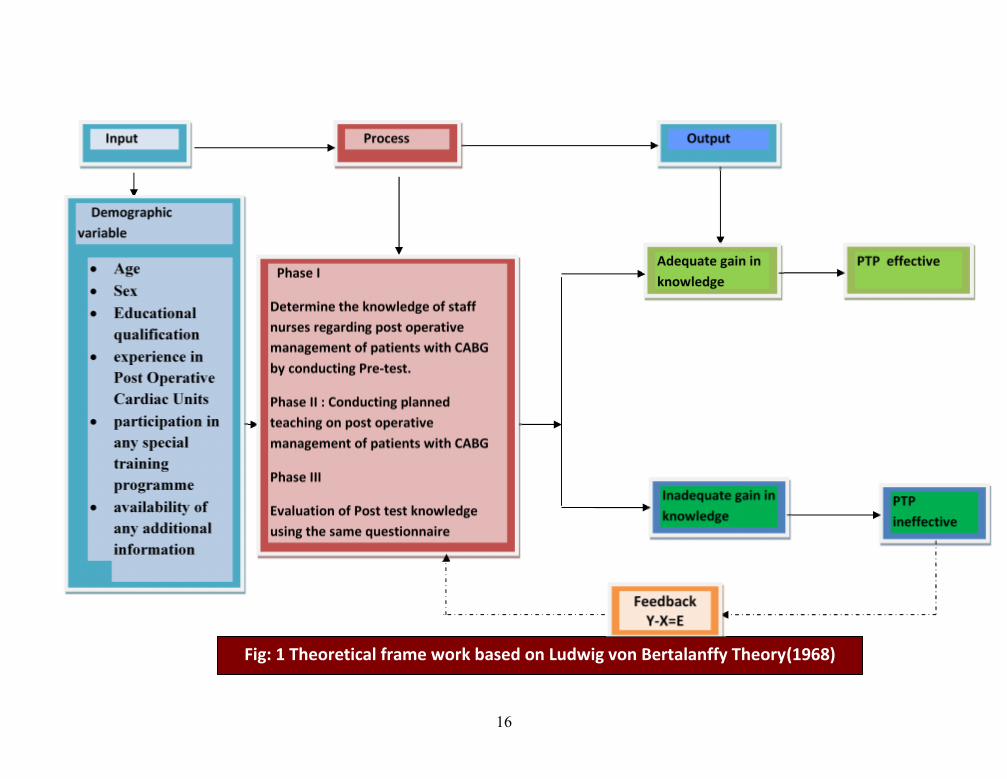
The present study aims to evaluate the effectiveness of planned teaching
program on knowledge regarding post operative management of patients with CABG
among staff nurses working in Post Operative Cardiac Units. The conceptual framework
of this study was based on the general system theory proposed by a biologist, Ludwig
Von Bertalanffy in 1968. According to him a system is a whole, which functions as a
whole by virtue of its independent parts. The definition implies that whole of the system
is distinguishable from its environment and it has parts, which have their independent
functions. It also states that functioning of independent part is responsible for the
functioning of the whole18.
Elements of system
The system is composed of both structural and functional components that
interact with in a boundary that filters the type and rate of exchange with the
environment. Living systems are open because there is an ongoing exchange of matter,
14
energy and information. The following elements are common to systems, i.e., input,
throughput, output and feedback.
Input
Input consists of matter, energy and information received from the environment and
man. It may be money, resources or time.
In the present study input refers to the demographic variables of the staff nurses,
which include age, sex, educational qualification, experience in Post Operative Cardiac
Units, participation in any special training programme on post operative management of
CABG and availability of any additional information on post operative management of
patient with CABG within last one month of research study.
Throughput
Throughput consists of matter, energy and information that is modified or
transformed within the system. It is a series of actions by which the system converts its
energy, input from the environment into products and services that are usable by the
system. The process can be modified in response to the feedback.
In this study the throughput or process includes three phases, the first phase was
determining the knowledge of staff nurses about post operative management of patients
with CABG by administering structured knowledge questionnaire. The second phase
consists of conducting planned teaching on post operative management of patients with
CABG. The third phase consists of evaluation of target group for change in knowledge
15
regarding post operative management of patients with CABG after administering planned
teaching (post-test).
Output
Output consists of matter, energy and information that is released from the system
in to the environment.
In the present study, evaluation of effectiveness of planned teaching programme on
post operative management of patients with CABG is the output that may also be
regarded as the product of the process. This is achieved through the comparison between
pre-test and post-test knowledge scores of the subjects. The output decides the
modification to be done at the input and process level. The increase in post-test score is
an indication of the effectiveness of planned teaching programme. Output becomes
feedback to the person and to the environment.
Feedback
Feedback consists of information regarding environmental responses used by the
system (may be positive, negative or neutral).
In the present study, it is the process within which the matter, energy and
information as systems output provides feedback for corrective action to change, enhance
or stabilize the system. Accordingly, the higher score obtained by staff nurses in the post-
test indicates that the planned teaching programme is effective in increasing the
knowledge of staff nurses. A low score in post-test indicates the need for repeating or
modifying the planned teaching programme. (Figure: 1).
16
OutputProcessInput
Demographicvariable
Age Sex Educational
qualification experience in
Post OperativeCardiac Units
participation inany specialtrainingprogramme
availability ofany additionalinformation
PTP effectiveAdequate gain inknowledge
Phase I
Determine the knowledge of staffnurses regarding post operativemanagement of patients with CABGby conducting Pre-test.
Phase II : Conducting plannedteaching on post operativemanagement of patients with CABG
Phase III
Evaluation of Post test knowledgeusing the same questionnaire
PTPineffective
Inadequate gain inknowledge
FeedbackY-X=E
X-
Fig: 1 Theoretical frame work based on Ludwig von Bertalanffy Theory(1968)

17
Summary:
This chapter has dealt with the problem statement, objectives, operational
definition, variables, assumptions, delimitations, hypothesis and conceptual framework
used for the study.

18
3. REVIEW OF LITERATURE
Review of literature is a critical summary of research on a topic of interest,
often prepared to put a research problem in context. A literature review helps to lay
the foundation for a study and can also inspire new research ideas.
Review of literature is defined as a broad, comprehensive, in depth, systematic
and critical review of scholarly publications, audiovisual materials and personal
communications19
Review of literature is based on an extensive survey of books, journals and
international nursing indices. It provides basis for selection and formulation of the
problem, justifies the need for the study, develops the proper conceptual model for the
study, throws light on the feasibility of the study, provides methodology for
comparison and replication and helps to avoid obstacles and making generalizations.19
The literature was reviewed by using MEDLINE, CINHAL, YAHOO search
engine, GOOGLE search engine and PUBMED search apart from research and non
research literature from journals and books, to have a better understanding and to gain
insight in to the selected problem under study.
The review of current study is organized under the following headings:
Literature related to:
1. Incidence and prevalence of CABG.
2. Post operative management of CABG patient.
3. Complications in CABG patients.
4. Knowledge of staff nurses regarding management of CABG patient.
5. PTP as an effective teaching aid.
19
1. Literature related to incidence and prevalence of CABG
A randomized controlled trial was conducted in South Africa among 2290
patients to analyze the demographic data and outcome of acute coronary syndrome in
South African Asian Indian population. The participants were divided into three age
subgroups, ≤ 45 yrs (young), >45 yrs (middle), >65 yrs (old). All three age groups
were predominantly males, but this was more evident in the younger and middle age
groups and became less striking as the proportion of females increased with age. 48%
were subjected to angiographic studies and among them 14% underwent CABG. This
shows the increasing prevalence of coronary disease and cardiac surgery20.
A cross-sectional study was conducted to examine the differences in the rates
of coronary artery bypass grafting (CABG) between white and black Medicare
patients in United States. The data were from 2006 Health Care Financing
Administration hospital claims records on all Medicare patients, the 2008 update of
the Bureau of Health Professions area resource file, and the 2005 Census Bureau's
county population estimates file. Sex and age adjusted CABG rates for whites and
blacks over the age of 65 years were computed for each of 50 states and 305 Standard
Metropolitan Statistical Areas. The CABG rate was 27.1 per 10000 for whites (40.4
for white men and 16.2 for white women), but only 7.6 for blacks (9.3 for black men
and 6.4 for black women). The study concluded that race is strongly associated with
CABG rates, and this association is greater for men than for women and greater in the
Southeast than in other parts of the country21.
A comparative study was conducted in Urban Kerala to assess the rates of
various strategies used to treat coronary blockages. The coronary angiographic
profiles of 131 consecutive female patients subjected to coronary angiography were
20
analyzed. Of these, 53% patients had abnormal coronaries. PCI was done in 40%,
CABG surgery in 37% and medical management advised for only 23% patients.
Results reveal that the coronary revascularization procedures like CABGs are
booming even in a developing country like India22.
A descriptive study was done in Coimbatore, Tamil Nadu to analyze the
revascularization pattern in female cases of coronary artery disease. Out of 400
patients who underwent CAG between May 2003 and Dec 2004, CABG was advised
for 129 patients and among these, 49 (38%) underwent the procedure and this was
done more in older age group. The study concluded that there seemed to be a trend
toward more females with coronary artery disease going for surgical
revascularization23.
2. Literature related to post operative management of CABG patient
A randomized controlled trial study was conducted to examine the effects of a
short intervention on behavioral risk factor modification in patients with coronary
artery disease (CAD) on Type A behavior. Samples were the acute myocardial
infarction patients or patients who underwent coronary artery bypass grafting
(CABG). They were randomly assigned to an 8-week multiple risk modification
group program (n = 94) or to a control group (n = 90) that received usual care with
standard physical exercise training. The result had shown that the intervention was
effective in reducing hostility and total Type A behavior at post intervention (P = .01)
and at 9-month follow-up (P = .03). The study concludes that a short behavioral
intervention for coronary patients can result in relatively large and persistent
reductions in cognitive aspects of Type A behavior and hostility, in particular24.
21
A two-phase naturalistic inquiry and a thematic analysis was done in Australia
to examine the range of post discharge issues, concerns and needs of patients and their
family carers after discharge after CABG surgery, and to explore their perceptions of
unmet needs one year later. Interviews were conducted with 30 patients and their
carers 4-5 weeks after coronary artery bypass grafting (phase 1) and 1 year after the
initial interview (phase 2). Thematic analysis was used to identify the major concerns
of participants. All participants recommended strengthening discharge planning with
more accurate information about what to expect during recovery, to help them
anticipate fluctuations in health and wellbeing. The findings suggest a need to
improve discharge preparation and provide enhanced home support services25.
A descriptive study was conducted in Jordan to describe the perceived learning
needs of patients who undergo CABG surgery before discharge, and describe the
perceived learning needs of CABG patients as perceived by nurses, in order to
establish a meaningful educational program. A convenient sample of 104 subjects
divided to 52 patient and 52 nurses were selected. Patient learning needs scale (PLNS)
was used for eliciting data about learning needs of Jordanian CABG patients. The
study identified the following dimensions of learning needs which includes wound
care, symptoms and complications, risk factors, diet, medications, surgery related
concerns and activity and return to work. There was significant difference between the
dimensions of learning needs of patients and nurses26.
A focus group technique was used to explore patient expectations of open-
heart surgery and recovery in Pennsylvania. The sample included eighteen
participants who underwent CABG or valve replacement surgery for the first time.
Five common themes described the patient’s surgical event which includes

22
acknowledging the disease, preoperative perceptions that patients formed while
waiting for surgery, identifying expectations of surgery and recovery, health and
illness transitions and acceptance of recovery. The findings support the need for
improved teaching methods that focus on realistic outcomes and follow-up services
that continue after discharge27.
A randomized study was conducted in Netherlands to compare the
effectiveness of a low frequency exercise program with a high frequency one after
uncomplicated coronary artery bypass graft (CABG) surgery. The data collected from
246 patients. The result had shown patients with the high frequency exercise program
achieved functional milestones faster than patients with the low frequency exercise
program (p = 0.007). The satisfaction degree was greater in the high frequency group
(p = 0.032). The study had concluded a high frequency exercise program leads to
earlier performance of functional milestones and yields more satisfaction after
uncomplicated CABG surgery and this should lead to an earlier discharge28.
A prospective study was conducted in Belgium to assess whether CR is
equally effective for suppressing the two-year cardiovascular event incidence after
CABG or PCI. 194 PCI and 149 CABG patients participated in a three-month CR
program, while 245 PCI and 89 CABG patients received standard care. Both CABG
and PCI patients included into CR showed a significantly lower mortality, as
compared to control patients (0.6% vs. 4.2%, P< 0.05). The study suggests that total
cardiovascular disease incidence was significantly lower as a result of CR in CABG
patients, but not in PCI patients29.
A ten year follow-up study was conducted in Kolkata to evaluate whether
smoking cessation reduces restenosis after CABG among 1141 patients who
23
underwent CABG. Smoking status post-CABG revealed that 45% quitted smoking
whereas 55% continued it. 29% of patients had symptomatic restenosis requiring
repeat PTCA/ CABG within ten years. In the restenosis group, 48% were smokers,
31% were ex-smokers and 21% were non smokers. Repeat intervention was required
in 19.2% for those who quitted smoking compared to 79.8% who continued to smoke.
The study concludes that smoking cessation after CABG was an important
independent predictor of restenosis and patients who continued to smoke after CABG
had a greater risk of restenosis requiring repeat CABG or PTCA than patients who
stopped smoking30.
An experimental study was conducted in Chennai to evaluate the effectiveness
of structured cardiac rehabilitation program in Indian setup among seventy-four
patients who underwent CABG. The patients were evaluated prior to surgery and were
initiated into lifestyle changes based on Diet, Relaxation, Exercise, Attitude and
Motivation (DREAM) concept on discharge post operatively. The patients were
advised unsupervised walking exercise based on target heart rate of 60 – 75% based
on age. The follow up was made every fifteen days. There was a favorable change in
functional capacity (11.4 + 1.59 METS), resting rate pressure double product, fasting
blood sugar, total cholesterol, triglycerides and anthropometric indices. The results
suggest an encouraging pattern for effective cardiac rehabilitation program that can
also be used for secondary prevention of Coronary Artery Disease in India31.
A descriptive study was conducted in Mumbai to study the effectiveness of a
cardiac rehabilitation program among cardiac patients. Forty seven patients were
enrolled for the study. Of these thirty had undergone CABG, nine underwent
angioplasty and six were on medical management for stable Congestive Heart
Disease. They were enrolled in the cardiac rehabilitation department for an endurance
24
training program. All of them reported a boost in their self confidence levels and
reported a high level of motivation to continue with their previous levels of physical
activity32.
3. Literature related to post CABG complications
An evaluative study was conducted in selected hospitals Italy, among 74,577
patients of different age groups and gender to examine the rates of complications
following coronary artery bypass surgery. A significant effect modification by gender
was found in 39 hospitals; the adjusted odds ratios showed significant increased risk
for females. In three of these hospitals a significant increased risk was found for older
age. Two hospitals showed a significant excess risk for patients’ ≥75 years. The result
shows that women and elderly are more prone for post operative complications after a
CABG33.
A retrospective study was done in Canada to analyze the risk factors acting on
the gastro intestinal (GI) complications seen after cardiac operations performed under
cardio pulmonary bypass. The overall mortality was 346 (2.55%) of 13,544 patients
who participated in the study. GI complications developed in 128 patients (0.94%).
Among those, 18(14.1%) died because of complications, the most common of which
was bleeding. The study concluded that GI complications remain a significant concern
after CABG. Higher-risk patients can be identified and treated prophylactically and in
the post-operative period34.
A retrospective and prospective literature review was carried out in Boston,
USA using Medline for articles published in the past 30 years to assess whether
gastrointestinal (GI) complications following CABG surgery are associated with a
high morbidity and mortality, prolonged hospital stay and increased cost of
hospitalization. They reviewed 151,652 patients reported over the past 30 years; GI
25
complications occurred on average after 1.21% of cardiac operations and had an
associated mortality of 34.1%. The most common risk factors identified include age
greater than 70 years, low cardiac output, peripheral vascular disease, reoperative
surgery, chronic renal insufficiency, increased number of blood transfusions,
prolonged cardiopulmonary bypass time, arrhythmias, and use of an intra aortic
balloon pump. Delayed diagnosis was associated with poor outcomes. The study
concluded that GI complications are rare events, but early diagnosis is essential35.
A retrospective cohort study was conducted in Canada to determine current
risk factors for postoperative pulmonary complications (PPCs) in CABG surgery
patients. Health records were reviewed for patients (n=315) who had CABG surgery
at a large quaternary healthcare centre over a 4 month period. Results show that PPCs
occurred in 99.4% of this CABG surgical cohort. Atelectasis, pleural effusion,
atelectasis with pleural effusion, and pneumonia were the most frequent PPCs post
CABG surgery. The study concluded that early identification of patients at risk for
developing PPCs and timely management can reduce the PPC rates in post-CABG
patients36.
A descriptive study was conducted in Mumbai among 2175 patients between
2003 and 2005 to assess the complications associated with off-pump CABG. Post-
operatively the thirty day mortality rate was 0.64%, neurological complication 0.73%,
peri-operative myocardial infarction 1.7%, reoperation for bleeding 0.55%, post-
operative AF rate 5.65%, deep wound infection rate 0.22% and superficial wound
infection rate 0.55%. The study concluded that off-pump CABG provides excellent
results with very low morbidity and mortality37.
26
4. Literature related to knowledge of staff nurses regarding management of
CABG patient
A focus group study was conducted in Canada to identify nurses' learning
needs to prepare patients for managing pain before and after discharge home from
cardiac surgery and to develop a pain education intervention for nurses. Participants
(N = 22) were asked about their perceptions of patients' education needs for pain
management after cardiac surgery and approaches to help nurses meet these needs.
Participants identified the most common pain knowledge gaps for patients before and
after discharge after cardiac surgery and they also identified their most helpful
educational approaches being brief in-services, hands-on learning, lunch-and-learn
sessions, and designated education days38.
An experimental study was conducted in Bosnia and Herzegovina, Norway
among 1276 patients to assess the outcome of a training given to surgeons and critical
care nurses on coronary artery bypass surgery. Operations were performed before
training in 540 and after in 736 patients. Overall mortality for coronary bypass
grafting surgery was 1.6%, and the major complication rate was 4.5%. Patients
operated after training developed fewer complications and had a shorter length of stay.
Unfavourable outcome was more common in patients who were operated before. The
result shows that proper training of cardiac surgeons and critical care nurses in the
management of CABG patient are found to be effective39.
A descriptive study was conducted in Australia to evaluate patients undergoing
coronary artery bypass surgery (CABG) and to assess their understanding of the risks
of interventions and baseline level of understanding of medical concepts and to
evaluate the medical staff's understanding of medical negligence and informed
consent. Fifty CABG patients and forty medical staff were interviewed over a six-
27
month period. Patients were interviewed with questionnaires focusing on the consent
process, the patient's understanding of CABG and associated risks and understanding
of medical concepts. Medical staffs were questioned on the process of obtaining
consent and understanding of medico legal concepts. The results showed that patients
undergoing CABG have a poor understanding of their disease, their intervention, and
its complications. Medical staff showed a poor knowledge of the concepts of material
risk and medical negligence requiring much improved education of both junior
doctors, specialists and nursing personnel40.
A descriptive study was conducted in Finland to describe coronary artery
bypass grafting (CABG) and percutaneous Trans luminal coronary angioplasty
(PTCA) patients’ need for nursing informational support in health-related (HRQoL)
items before and after coronary artery procedures. The study sample (N=625)
consisted of consecutive male (N=439) and female (N=176) patients with CAD who
were treated with elective CABG or PTCA. Patients in both groups reported needing
the most information about recovery and psychosocial functioning before and after
the treatments. The results suggest the need for educating nurses regarding care of
patients who underwent cardiac procedures41.
An experimental study was conducted in Canada to assess the relationship
between nurses' pain knowledge and pain management outcomes for their
postoperative cardiac patients. Nurses (n=94) from four cardiovascular units in three
university-affiliated hospitals were interviewed along with 225 of their assigned
patients following initial, uncomplicated coronary artery bypass graft (CABG)
surgery. Patients reported moderate to severe pain but received only 47% of their
prescribed analgesia. Patients' perceptions of their nurses as resources with their pain
were not positive. The results showed that nurses' knowledge scores were not
28
significantly related to their patients' pain ratings or analgesia administered. Critical
deficits in knowledge and misbelieves about pain management were evident for all
nurses42.
A descriptive study was conducted to describe the social support for CABG
surgery patients and their significant others from nurses during hospitalization. Fifty
three patients and forty seven significant others participated in the study. Significant
others felt that they had received more information and guidance on the patient’s
hospitalization than on home care, as about half of the significant others had not
received guidance on wound care or written instructions for home. This reveals that a
major group of nurses are still unaware about the need of social support for CABG
patients and their relatives5.
A descriptive survey was conducted in Sweden to describe the use of
pedagogically related keywords and the content of notes connected to these keywords,
as they appear in nursing records in a coronary artery bypass graft (CABG) surgery
rehabilitation unit. The records of 265 patients admitted to a rehabilitation unit
following CABG surgery were analyzed and the pedagogically related keywords:
communication, cognition/development and information/education were selected. The
study concluded that the documentation of pedagogical activities in nursing records
was infrequent and inadequate and recommended to document the patients' need for
knowledge and the nurses' teaching in the patient records. This reveals the limited
knowledge of nurses regarding proper maintenance of nursing records of a CABG
surgery patient43.
A descriptive study was conducted in United States to assess the competency
in cardiac examination skills of medical staffs including cardiology fellows, medical
students, nursing personals and others. A validated 50-question, computer-based test
29
was done for the 860 study participants. Except cardiology fellows, all participants
demonstrated low specificity for systolic murmurs and low sensitivity for diastolic
murmurs. The study concluded that improvement in cardiac examination competency
require training in simultaneous audio and visual examination. This shows limited
knowledge of nurses regarding cardiac examination of a patient44.
A descriptive study was carried out in 1998 to assess the knowledge and
practices of nursing personal regarding immediate post operative care of cardiac
surgery client on ventilator in Cardio Thoracic Intensive Care Unit in selected
Hospitals of Hyderabad. 30 nurses working in CTICU with at least 6 months
experience were selected by purposive sampling. Data was collected by observational
checklist and questionnaire. The study revealed that majority of nurses had below
average knowledge and practices and more than one third of nurses had above
average knowledge and practices45.
5. Literature related to PTP as an effective teaching aid
Health education plays an important role in helping the people to
achieve optimum health. A properly performed study should include
dissemination of information to create a psychologically positive atmosphere for
the work. Most of the planned teaching programme showed that they are very
effective.
A study was conducted to assess the effectiveness of PTP on knowledge
and practice of endotracheal suctioning among staff nurses in different
intensive care units of selected hospital in Mangalore. An evaluative research
approach was done. Sample size was 50 and purposive sampling was used. The
overall mean post-test knowledge score (27.5) was significantly higher than the
30
overall means pre-test score (17.0), the paired ‘t’ test value is 24.42 (t49 – 3.4
P 96 < 0.01)46.
An evaluatory study was conducted in the effectiveness of PTP to the
32 caregivers of bedridden neurological hospitalized patients on bedsore at
KMC Hospital Manipal. A pre-experimental approach was used with one group
pre-test-post-test design and data collected was from 32 care givers of patients
with Barden score ≤16. A convenient sampling technique was used to select the
sample. The instruments used for the study were Braden scale, structured
questionnaire and observation checklist. The finding of the study revealed that
caregivers significantly gained knowledge and ability regarding prevention of
bed sores and the PTP was effective in terms of preventing bedsore in their
patients.47
An evaluatory approach one group pre-test post-test study was conducted to
assess the effectiveness of planned teaching programme on biomedical waste
management among forty staff nurses working in a selected hospital at Mangalore.
The study findings revealed that knowledge scores of staff nurses were inadequate
before the administration of planned teaching program. The planned teaching program
facilitated them to update their knowledge related to biomedical waste management.
Post-test knowledge scores of the staff nurses significantly increased after the planned
teaching program48.
Summary
This chapter dealt with literature review under several headings. This review
has helped the researcher to gain confidence for conducting the study and for better
understanding of various research techniques that could be used.

31
4. METHODOLOGY
Research methodology is a way to systematically solve the research problem.
It describes various steps that are generally adopted by the researcher in studying the
research problem, along the logic behind them and explain why the researcher uses a
particular method or technique so that the research results are capable of being
evaluated by the researcher or by others.49
Research methodology chapter of the research study indicates the researcher’s
over all plans for obtaining answer to research questions and it spells out the strategies
that the researcher adopts to develop the information that is accurate objective and
interpretable.
Research methodology describes research design, setting, population,
sampling technique, development of tool, pilot study, procedure for data collection
and plan for data analysis.50
Research approach:
Research approach is a systematic, controlled, empirical and critical
evaluation of natural phenomena guided by theory and hypothesis about the presumed
relations among the phenomena. 49
Evaluative research is an applied form of research that involve finding out
how well a programme, procedure or policy is working. Its goal is to assess and
evaluate success of a programme.
In view of the nature of the problem under study and to accomplish the
objectives of the study evaluative approach was found to be appropriate to describe

32
the effectiveness of planned teaching programme on post operative management of
patients with CABG.
Research design:
The research design is the overall plan for obtaining answer to the question
being studied and for handling some of the difficulties encountered during the
research process.49
Pre experimental one group pre-test post-test design is the most appropriate
design for measuring the impact or effectiveness of a programme. No comparison
with the control group is provided. The advantage is that the design can measure the
situation, phenomenon, issue, problem or attitude. The design is described as two sets
of cross-sectional observations on the same population to find out the change in the
phenomenon or variable in two points of time.
In view of the nature of the problem under study and to accomplish the
objectives of the study, pre-test post-test design with evaluative approach was found
to be appropriate to evaluate the effectiveness of planned teaching programme on post
operative management of patients with CABG among staff nurses. No comparison
with the control group is provided.
33
Table 1: Schematic representation of pre experimental design
Pre Test Treatment Post Test
O1 X O2
E = O2- O1
O1 – Pre-test knowledge score of staff nurse on day 1.
X – Implementation of Planned teaching programme regarding post
operative management of patients with CABG among staff nurses on
day 1.
O2 – Post test knowledge score of staff nurses on day 7.
E - Effectiveness of Planned teaching programme regarding post
operative management of patients with CABG among staff nurses.

34
Day 1
Administration ofplannedteachingprogrammeon postoperativemanagement of patientswith CABG
FIGURE 2: SCHEMATIC REPRESENTATION OF STUDY DESIGN
Descriptive andinferentialstatistics
Mean Median SD Paired
‘t’test
Day 7
Assessment ofpost testknowledgewith samestructureknowledgequestionnaire
Day I
Assessment ofPretestknowledge withstructuredknowledgequestionnaire
KasturbaMedicalCollege,Mangaloreand OmegaHospital,Mangalore
50 staffnurses.
Purposivesamplingtechnique
Staffnursesworking inPostoperativecardiacUnits
AnalysisPost test
(Y)
TreatmentPre-test
(X)
Researchsetting
Sampleandsamplingtechnique
PopulationResearchDesign
Pretest posttest designwithoutcontrolgroup.
35
Setting:
Setting is the physical location and conditions in which data collection takes place
The study was conducted in Postoperative cardiac Units of Kasturba Medical College, and
Omega Hospital, Mangalore.
The hospitals were selected for the study on the basis of:
Geographical proximity
Feasibility of conducting the study
Availability of sample
Variables under investigation:
Variable is a quality of an organism, group or situation that takes on different
values.49 Research variables are concepts at various levels of abstraction that are
measured, manipulated and controlled in a study.
Independent variable: The variables which can be purposely manipulated and controlled
in a study. In the present study the independent variable is the planned teaching
programme on post operative management of patients with CABG.
Dependent variable: Change occurring as a result of manipulation of Independent
variable. In the present study it refers to the knowledge of staff nurses about post operative
management of patients with CABG.
Extraneous variable (Demographic variable).Independent variable that are not related
to the purpose of the study, but may affect the dependent variable are termed as extraneous
variable50. In the present study the demographic variables are age, sex, educational
qualification, experience in Postoperative cardiac Units, participation in any special
36
training programme on post operative management of CABG and availability of any
additional information on post operative management of patient with CABG within last
one month of research study.
Population:
Population is the entire group of members, objects or events which have at least one
characteristic in common and must be defined specifically and unambiguously.49
In the present study the population consists of staff nurses working in
Postoperative cardiac Units of selected hospitals at Mangalore.
Sampling procedure:
Sampling technique:
Sampling is a process of selecting a group of people, events or portion of the
population to represent the entire population49
Purposive sampling is adopted for the study. Here the samples are chosen by
choice not by chance, through a judgment made by the researcher based on his or her
knowledge about the population. The researcher believes that some subjects are fit for
research compared to other individuals53. In the present study, the samples are staff nurses
working in Postoperative cardiac Units of selected hospital, Mangalore. Therefore this
sampling technique is best suited for the study.
Sample and sample size:
Sample refers to the subset of a population selected to participate in a research
study50.
37
The sample for the present study consisted of 50 staff nurses who met the inclusion
criteria.
Inclusion criteria for sampling
Staff nurses in Postoperative cardiac Units
Who are in the age group of 20-60 years.
Who are willing to participate in the study.
Who are available at the time of data collection period.
both sexes will be selected
Exclusion criteria for sampling
Staff nurses in Postoperative cardiac Units,
Who do not have any experience in Postoperative cardiac Units
Who are not able to watch and hear due to physical challenges.
Who are on leave vacancy or absence of duty.
Development of the tool:
A tool or instrument is the written device that a researcher uses to collect data.
The instrument selected in a research should be the vehicle that would best obtain
data for drawing conclusions which were pertinent to the study. To fulfil the objectives of
the study a closed-ended structured knowledge questionnaire was prepared to measure the
dependent variable before and after the administration of PTP
38
An intense search of related literature and experts in the field of Medical and
Surgical nursing were consulted for developing an appropriate tool. Items of the tool were
collected, scrutinized, selected and checked for overlapping.
The tool was prepared on the basis of the objectives of the study. The following steps were
adopted prior to the development of the tool
1. Review of literature
2. Preparation of blue print
3. Consulting with guide and subject experts.
Preparation of the blue print:
A blue print of structured knowledge questionnaire on post-operative management
of patients with CABG was prepared. It consisted of three sub areas. It depicted the
distribution of items according to the content areas based on three domains, namely,
knowledge, comprehension and application. Knowledge domain had 14 items (46.66%),
comprehension had 11 items (36.66%), and application had 05 items (16.66%) covering
all aspects of CABG.
Description of the tool:
The tool was constructed in two parts. Part I consists of demographic variables. Part
II consists of 30 items on CABG under Unit I, II and III.
Part I: Includes 6 items of demographic variables such as age, sex, educational
qualification, experience in Postoperative cardiac Units, participation in any special
training programme on post operative management of CABG and availability of any
additional information on post operative management of patient with CABG within last
one month of research study.

39
Part II: It consists of total 30 items related to knowledge regarding CABG. There were
three units. Unit I consists of four items assessing the knowledge related to anatomy and
physiology of heart. Unit II consists of five items assessing the knowledge related to
Coronary Artery Bypass Grafting. Unit III consists of twenty one items assessing the
knowledge related to post operative management of CABG patient.
Development of criteria checklist for validating the tool:
Criteria checklist was developed to validate the tool regarding accuracy, relevance
and appropriateness of the tool. Criteria checklist consists of three columns namely agree,
disagree and remarks column. Experts were requested to give their valuable opinion and
suggestions.
Development of planned teaching programme
Teaching plan is a guide for the teacher because it helps to cover the topics
comprehensively with proper sequence of points and without missing anything.
The steps to prepare teaching plan are:
Review of literature
Framing the outline of the teaching plan
Preparation and organization of content.
Deciding the method of instruction and AV aids.
Development of criteria checklist.
Content validation of the PTP.
Pretesting of the planned teaching programme.
Preparation of the final draft.
Editing the teaching plan.
Evaluating the teaching plan.
40
Review of literature
An extensive literature review was undertaken regarding post operative
management of CABG patient from the conceptual and data base material, internet
sources, journals etc to prepare the planned teaching programme.
Framing the outline of the teaching plan:
The outline of the teaching plan was framed which included setting up of the general
and specific objectives, specifying the date, time, place, and size of the group, number of
sessions and duration of sessions
Preparation and organization of content:
Content of the planned teaching programme was prepared and organized under
various headings according to the specific objectives.
Deciding the method of instruction and AV aids:
The method of instruction adopted was lecture cum discussion. Visual aids used is
power point
Development of criteria checklist:
The criteria checklist was developed to evaluate the teaching plan based on criteria
stated. It consisted of four items under the headings objective, content, organization and
practicability. It was sent to experts to get their opinions and suggestions regarding the
relevance, appropriateness, accuracy and degree of agreement in each item of the planned
teaching programme.
41
Content validation of the PTP and tool:
The prepared instrument, along with validity seeking letter, acceptance form,
problem statement, objectives, hypothesis, operational definitions, blue print, checklist,
planned teaching programme, and answer key was submitted to experts in the field of
Medicine, Surgery and Nursing.
Based on the expert suggestions given by the nine subject experts, modification
and rearrangement of items were made. Thus the final draft of 30 items was made.
Pretesting of the PTP and tool:
Pre testing of the tool was done among five staff nurses working in Wenlock
Hospital, Mangalore along with PTP to determine the feasibility, understandability and
ambiguity of the tool and also to check the time required to complete the tool.
The tool was found to be clear and feasible and was understood well by the
samples. Time taken to complete the tool was 35 minutes.
Preparation of the final draft of planned teaching programme:
Final draft of planned teaching programme was organized under various headings
such as anatomy and physiology of heart, Coronary Artery Bypass Grafting and post
operative management of CABG patient.
Editing the teaching plan:
The prepared teaching programme was edited by professional editors.
42
Reliability:
The reliability of a research instrument is defined as the extent to which the
instrument yields the same result on repeated measures.49
The reliability of a measuring tool can be assessed in the aspect of stability,
internal consistency and equivalence depending on the nature of the instrument.
The internal consistency (homogenity) approach to estimate an instrument’s
reliability is probably the most widely used method. Indices of homogeneity estimates the
extent to which different subparts of an instrument are equivalent in terms of measuring
the critical attribute
In the present study reliability of the tool was tested by administering it on five
staff nurses working in Wenlock Hospital, Mangalore. In order to ascertain reliability of
structured knowledge questionnaire split half method was used. The test was divided into
two equivalent halves and correlation for the half test was calculated, using Karl Pearson
Correlation Coefficient formula, and significance of correlation was tested using
Spearman Brown prophesy formula. The ‘r’ value was 0.89 and the tool was found
reliable.
Pilot study:
Pilot study is a smaller version of the proposed study conducted to refine the
methodology. It is developed similar to the proposed study, using similar objectives,
similar setting, similar treatment and similar data collection procedure and analysis
techniques.50
43
Pilot study was conducted among five staff nurses working in Postoperative
cardiac Units, Wenlock Hospital, Mangalore in September 2012 to find the feasibility of
the study. Samples were selected by using purposive sampling technique. The subjects for
pilot study possessed the same characters as that of the same samples for final study.
The collected data was analyzed by using descriptive and inferential statistics.
Assessment of level of knowledge of the staff nurses regarding post operative management
of CABG revealed that 33.3% respondent had poor knowledge, 66.6% had average
knowledge, and none had good or very good knowledge. The mean±SD of pre-test was
10.8±2.29 with a mean percentage of 42% where as post test was 21.1±1.56 mean
percentage of 81%. The difference was 39%, which shown an increase in knowledge after
administration of PTP.
It was found that the study was feasible, the questionnaire and PTP were relevant
and the time and cost of the study was within the limit.
Data collection procedure:
Prior permission was obtained from the concerned authority of the selected
hospitals at Mangalore. Keeping in mind the ethical aspect of research data was collected
after informed consent of the sample. The respondents were assured of the anonymity and
confidentiality of the information provided by them. The researcher has collected data
from 50 samples in Kasthurba Medical College, Mangalore and Omega Hospital,
Mangalore. Data collection period was from 2nd October to 15th November 2012.
Pre test was conducted on first day followed by the teaching programme. Lecture
cum discussion was the method of instruction. Visual aid like power point is used. The
44
duration of the session was 60 minutes. After seven days a post test was conducted, using
the same questionnaire to evaluate the effectiveness of planned teaching programme.
Plan for data analysis:
Descriptive statistics are useful for summarizing empirical information. Inferential
statistics, which is based on laws of probability, provides a means of drawing conclusion
about the population from which data is obtained for sample. Data will be analyzed using
descriptive and empirical statistics.
Data analyzed by the following steps:
Data arranged in a master sheet.
Descriptions of the subjects with respect to demographic variables were presented
using frequencies, and percentage.
Mean, standard deviation, mean percentage were used to evaluate the effectiveness of
the PTP.
Statistical significance of the effectiveness of the PTP was analysed using a paired ‘t’
test.
Data were represented in tables, graphs and diagrams.
SUMMARY:
This chapter has dealt with the research methodology adopted for the study. It
included research approach, research design, population, sample, sampling technique,
research setting, and study instruments, development of PTP, pilot study, and procedure
for data collection and plan for data analysis.
45
5. RESULTS
The description of result is the heart of a research project. It is the communication
of facts, measurements, and observation gathered by the research worker. For achieving
the results the collected data must be processed and analyzed in an orderly coherent
fashion. The term analysis means the computation of certain measures that exist among
data groups.
This chapter deals with the analysis and interpretation of the results of the data
collected from the sample of 50 staff nurses regarding knowledge on post operative
management of patients with CABG. Keeping in view the objectives of the study pre
experimental one group pre-test post-test design with an evaluative approach was adopted to
evaluate the effectiveness of planned teaching programme. The gathered data was then
organized, tabulated, analyzed and interpreted using descriptive and inferential statistics.
The data has been analyzed and interpreted in the light of the objectives and
hypothesis of the study.
Objectives of the study
1. To determine the level of knowledge among staff nurses regarding post operative
management of patients with CABG
2. To evaluate the effectiveness of planned teaching programme on level of knowledge
regarding post operative management of patients with CABG among staff nurses in
Post Operative Cardiac Units.
3. To find out the association between levels of knowledge regarding post operative
management of patients with CABG among staff nurses in Post Operative Cardiac
Units with their selected demographic variables.
46
Organization of findings
The collected information was organized and presented in four parts:
Part I: Description of the demographic variables of staff nurses.
Part II:Analysis of knowledge scores of staff nurses regarding post operative management
of patients with CABG.
Assessment of pre-test and post-test knowledge level on post operative management of
patients with CABG among staff nurses in Post Operative Cardiac Units.
Part III: Evaluation of effectiveness of the planned teaching programme on post operative
management of patients with CABG among staff nurses in Post Operative Cardiac Units.
Section A:
Quartile distribution of the pre-test and the post-test knowledge scores of staff nurses
regarding post operative management of patients with CABG
Section B:
a) Comparison of pre-test and post-test knowledge scores of staff nurses regarding post
operative management of patients with CABG.
b) Area wise effectiveness of PTP on post operative management of patients with CABG
among staff nurses in Post Operative Cardiac Units.
c) Item wise effectiveness of PTP on post operative management of patients with CABG
among staff nurses in Post Operative Cardiac Units.
Part IV: Testing of hypotheses
• Testing of hypothesis, H1
• Testing of hypothesis, H2
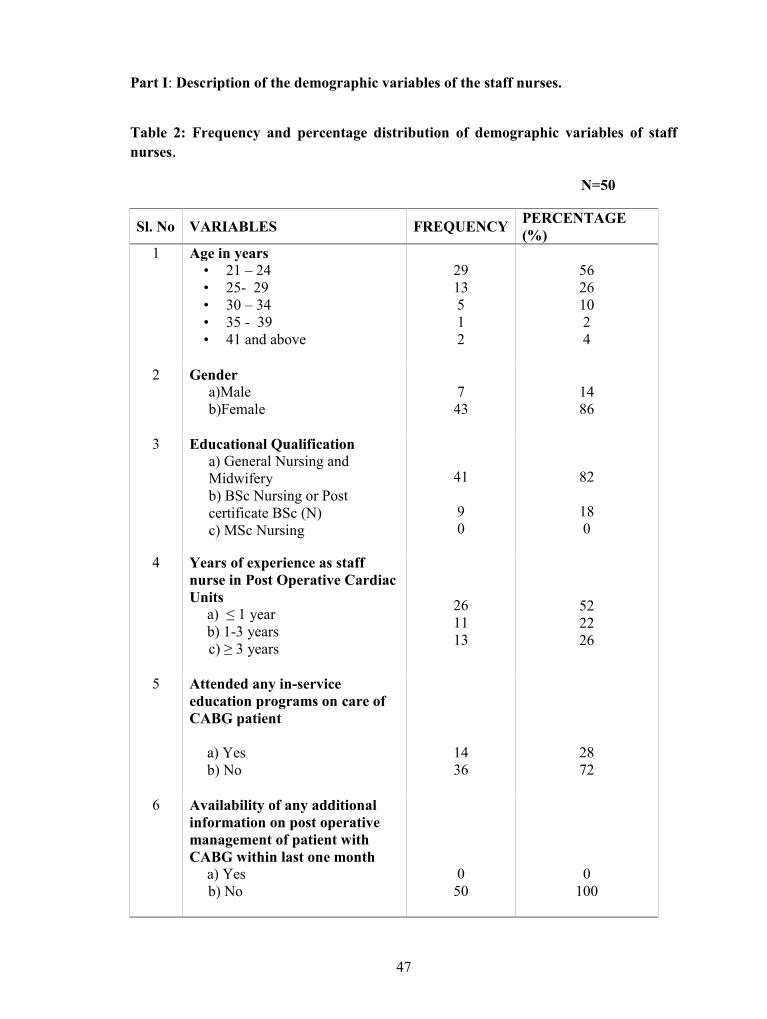
47
Part I: Description of the demographic variables of the staff nurses.
Table 2: Frequency and percentage distribution of demographic variables of staffnurses.
N=50
Sl. No VARIABLES FREQUENCY PERCENTAGE(%)
1 Age in years• 21 – 24• 25- 29• 30 – 34• 35 - 39• 41 and above
2913512
56261024
2 Gendera)Maleb)Female
743
1486
3 Educational Qualificationa) General Nursing andMidwiferyb) BSc Nursing or Postcertificate BSc (N)c) MSc Nursing
41
90
82
180
4 Years of experience as staffnurse in Post Operative CardiacUnits
a) ≤ 1 yearb) 1-3 yearsc) ≥ 3 years
261113
522226
5 Attended any in-serviceeducation programs on care ofCABG patient
a) Yesb) No
1436
2872
6 Availability of any additionalinformation on post operativemanagement of patient withCABG within last one month
a) Yesb) No
050
0100
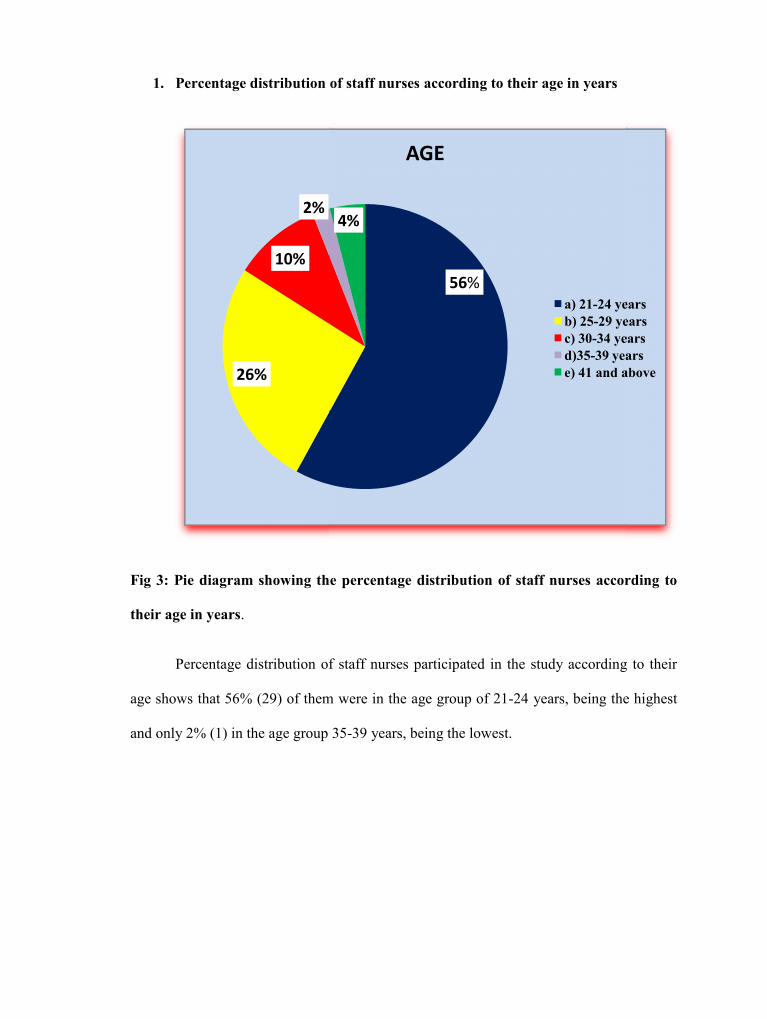
48
1. Percentage distribution of staff nurses according to their age in years
Fig 3: Pie diagram showing the percentage distribution of staff nurses according to
their age in years.
Percentage distribution of staff nurses participated in the study according to their
age shows that 56% (29) of them were in the age group of 21-24 years, being the highest
and only 2% (1) in the age group 35-39 years, being the lowest.
26%
10%
2%4%
48
1. Percentage distribution of staff nurses according to their age in years
Fig 3: Pie diagram showing the percentage distribution of staff nurses according to
their age in years.
Percentage distribution of staff nurses participated in the study according to their
age shows that 56% (29) of them were in the age group of 21-24 years, being the highest
and only 2% (1) in the age group 35-39 years, being the lowest.
56%
2%4%
AGE
a) 21-24 yearsb) 25-29 yearsc) 30-34 yearsd)35-39 yearse) 41 and above
48
1. Percentage distribution of staff nurses according to their age in years
Fig 3: Pie diagram showing the percentage distribution of staff nurses according to
their age in years.
Percentage distribution of staff nurses participated in the study according to their
age shows that 56% (29) of them were in the age group of 21-24 years, being the highest
and only 2% (1) in the age group 35-39 years, being the lowest.
a) 21-24 yearsb) 25-29 yearsc) 30-34 yearsd)35-39 yearse) 41 and above
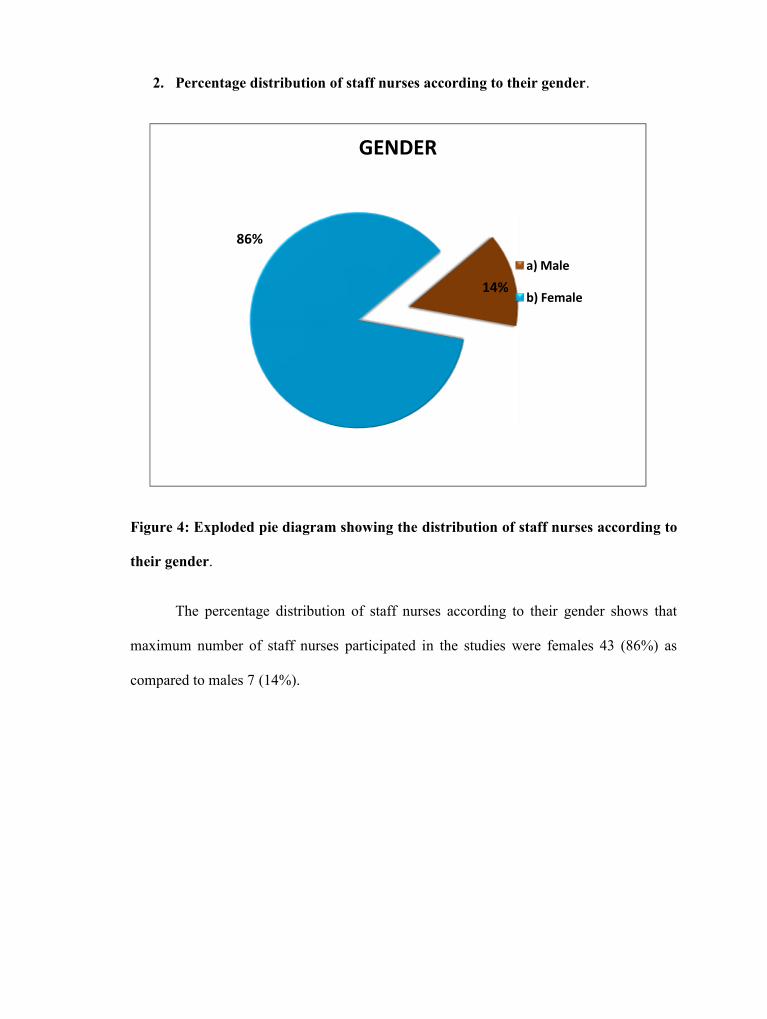
49
2. Percentage distribution of staff nurses according to their gender.
Figure 4: Exploded pie diagram showing the distribution of staff nurses according to
their gender.
The percentage distribution of staff nurses according to their gender shows that
maximum number of staff nurses participated in the studies were females 43 (86%) as
compared to males 7 (14%).
86%
49
2. Percentage distribution of staff nurses according to their gender.
Figure 4: Exploded pie diagram showing the distribution of staff nurses according to
their gender.
The percentage distribution of staff nurses according to their gender shows that
maximum number of staff nurses participated in the studies were females 43 (86%) as
compared to males 7 (14%).
14%
GENDER
a) Male
b) Female
49
2. Percentage distribution of staff nurses according to their gender.
Figure 4: Exploded pie diagram showing the distribution of staff nurses according to
their gender.
The percentage distribution of staff nurses according to their gender shows that
maximum number of staff nurses participated in the studies were females 43 (86%) as
compared to males 7 (14%).
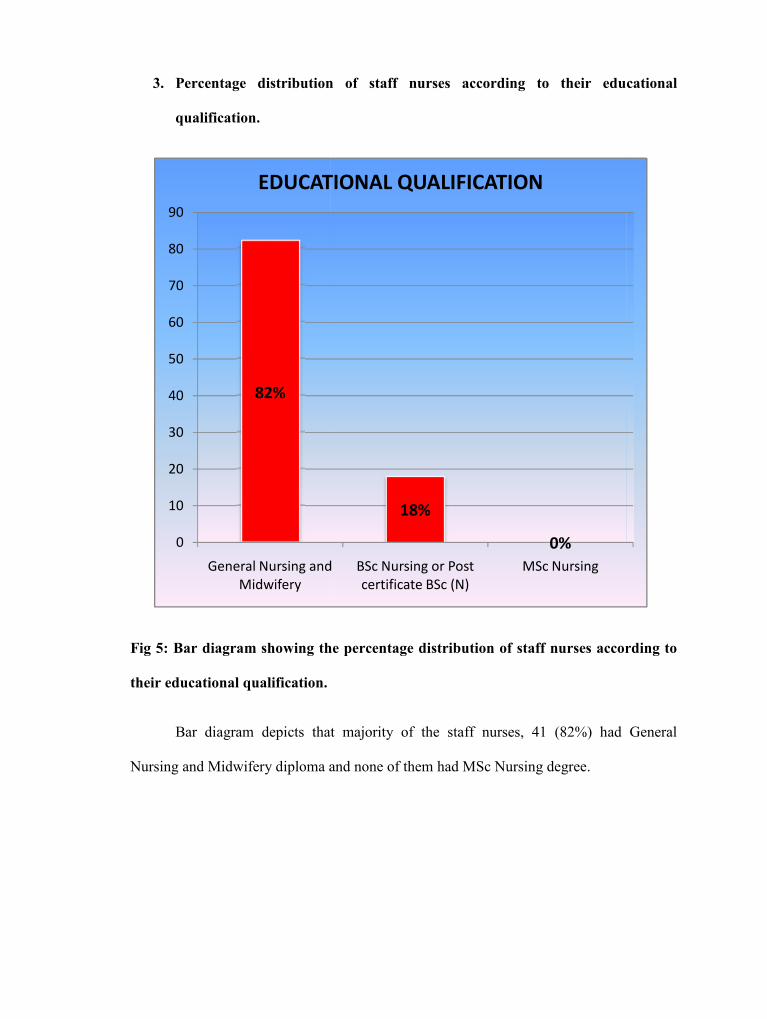
50
3. Percentage distribution of staff nurses according to their educational
qualification.
Fig 5: Bar diagram showing the percentage distribution of staff nurses according to
their educational qualification.
Bar diagram depicts that majority of the staff nurses, 41 (82%) had General
Nursing and Midwifery diploma and none of them had MSc Nursing degree.
82%
0
10
20
30
40
50
60
70
80
90
General Nursing andMidwifery
EDUCATIONAL QUALIFICATION
50
3. Percentage distribution of staff nurses according to their educational
qualification.
Fig 5: Bar diagram showing the percentage distribution of staff nurses according to
their educational qualification.
Bar diagram depicts that majority of the staff nurses, 41 (82%) had General
Nursing and Midwifery diploma and none of them had MSc Nursing degree.
18%
0%General Nursing and
MidwiferyBSc Nursing or Postcertificate BSc (N)
MSc Nursing
EDUCATIONAL QUALIFICATION
50
3. Percentage distribution of staff nurses according to their educational
qualification.
Fig 5: Bar diagram showing the percentage distribution of staff nurses according to
their educational qualification.
Bar diagram depicts that majority of the staff nurses, 41 (82%) had General
Nursing and Midwifery diploma and none of them had MSc Nursing degree.
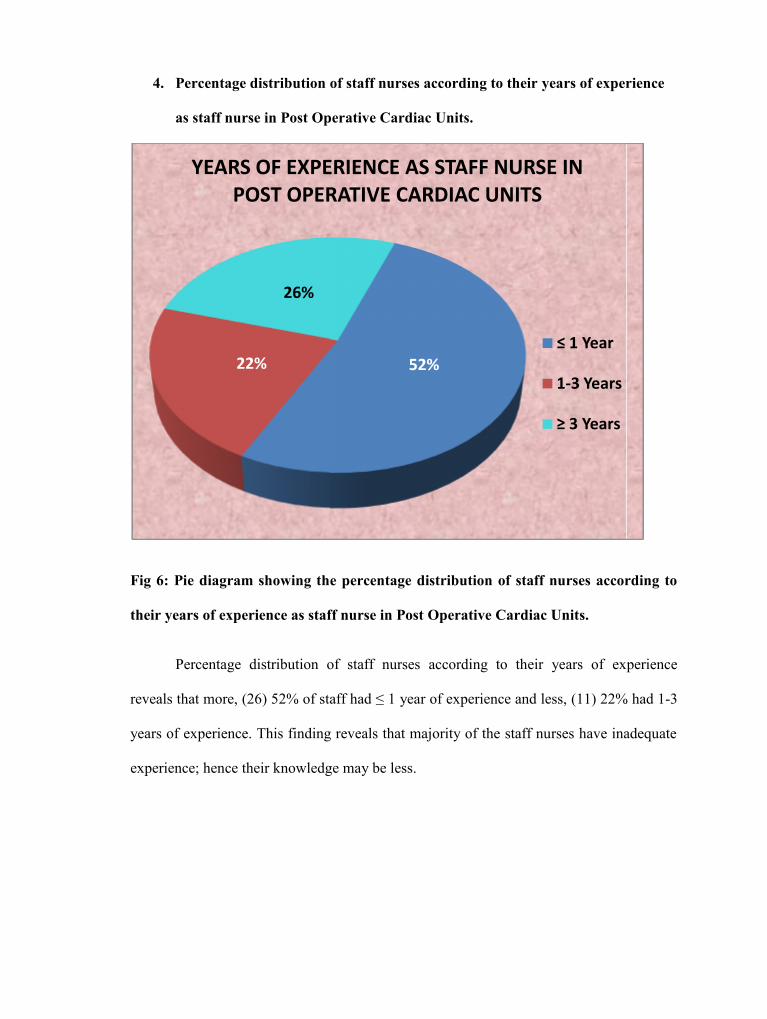
51
4. Percentage distribution of staff nurses according to their years of experience
as staff nurse in Post Operative Cardiac Units.
Fig 6: Pie diagram showing the percentage distribution of staff nurses according to
their years of experience as staff nurse in Post Operative Cardiac Units.
Percentage distribution of staff nurses according to their years of experience
reveals that more, (26) 52% of staff had ≤ 1 year of experience and less, (11) 22% had 1-3
years of experience. This finding reveals that majority of the staff nurses have inadequate
experience; hence their knowledge may be less.
22%
26%
YEARS OF EXPERIENCE AS STAFF NURSE INPOST OPERATIVE CARDIAC UNITS
51
4. Percentage distribution of staff nurses according to their years of experience
as staff nurse in Post Operative Cardiac Units.
Fig 6: Pie diagram showing the percentage distribution of staff nurses according to
their years of experience as staff nurse in Post Operative Cardiac Units.
Percentage distribution of staff nurses according to their years of experience
reveals that more, (26) 52% of staff had ≤ 1 year of experience and less, (11) 22% had 1-3
years of experience. This finding reveals that majority of the staff nurses have inadequate
experience; hence their knowledge may be less.
52%
YEARS OF EXPERIENCE AS STAFF NURSE INPOST OPERATIVE CARDIAC UNITS
≤ 1 Year
1-3 Years
≥ 3 Years
51
4. Percentage distribution of staff nurses according to their years of experience
as staff nurse in Post Operative Cardiac Units.
Fig 6: Pie diagram showing the percentage distribution of staff nurses according to
their years of experience as staff nurse in Post Operative Cardiac Units.
Percentage distribution of staff nurses according to their years of experience
reveals that more, (26) 52% of staff had ≤ 1 year of experience and less, (11) 22% had 1-3
years of experience. This finding reveals that majority of the staff nurses have inadequate
experience; hence their knowledge may be less.
1-3 Years
≥ 3 Years
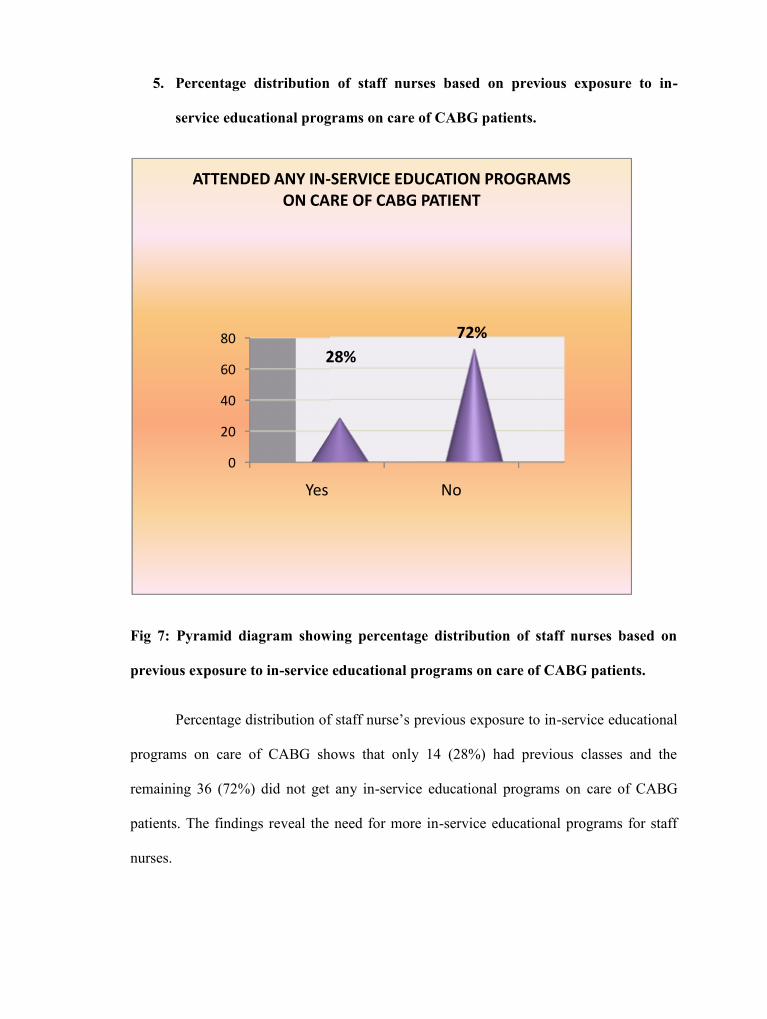
52
5. Percentage distribution of staff nurses based on previous exposure to in-
service educational programs on care of CABG patients.
Fig 7: Pyramid diagram showing percentage distribution of staff nurses based on
previous exposure to in-service educational programs on care of CABG patients.
Percentage distribution of staff nurse’s previous exposure to in-service educational
programs on care of CABG shows that only 14 (28%) had previous classes and the
remaining 36 (72%) did not get any in-service educational programs on care of CABG
patients. The findings reveal the need for more in-service educational programs for staff
nurses.
0
20
40
60
80
Yes
28%
ATTENDED ANY IN-SERVICE EDUCATION PROGRAMSON CARE OF CABG PATIENT
52
5. Percentage distribution of staff nurses based on previous exposure to in-
service educational programs on care of CABG patients.
Fig 7: Pyramid diagram showing percentage distribution of staff nurses based on
previous exposure to in-service educational programs on care of CABG patients.
Percentage distribution of staff nurse’s previous exposure to in-service educational
programs on care of CABG shows that only 14 (28%) had previous classes and the
remaining 36 (72%) did not get any in-service educational programs on care of CABG
patients. The findings reveal the need for more in-service educational programs for staff
nurses.
Yes No
28%72%
ATTENDED ANY IN-SERVICE EDUCATION PROGRAMSON CARE OF CABG PATIENT
52
5. Percentage distribution of staff nurses based on previous exposure to in-
service educational programs on care of CABG patients.
Fig 7: Pyramid diagram showing percentage distribution of staff nurses based on
previous exposure to in-service educational programs on care of CABG patients.
Percentage distribution of staff nurse’s previous exposure to in-service educational
programs on care of CABG shows that only 14 (28%) had previous classes and the
remaining 36 (72%) did not get any in-service educational programs on care of CABG
patients. The findings reveal the need for more in-service educational programs for staff
nurses.
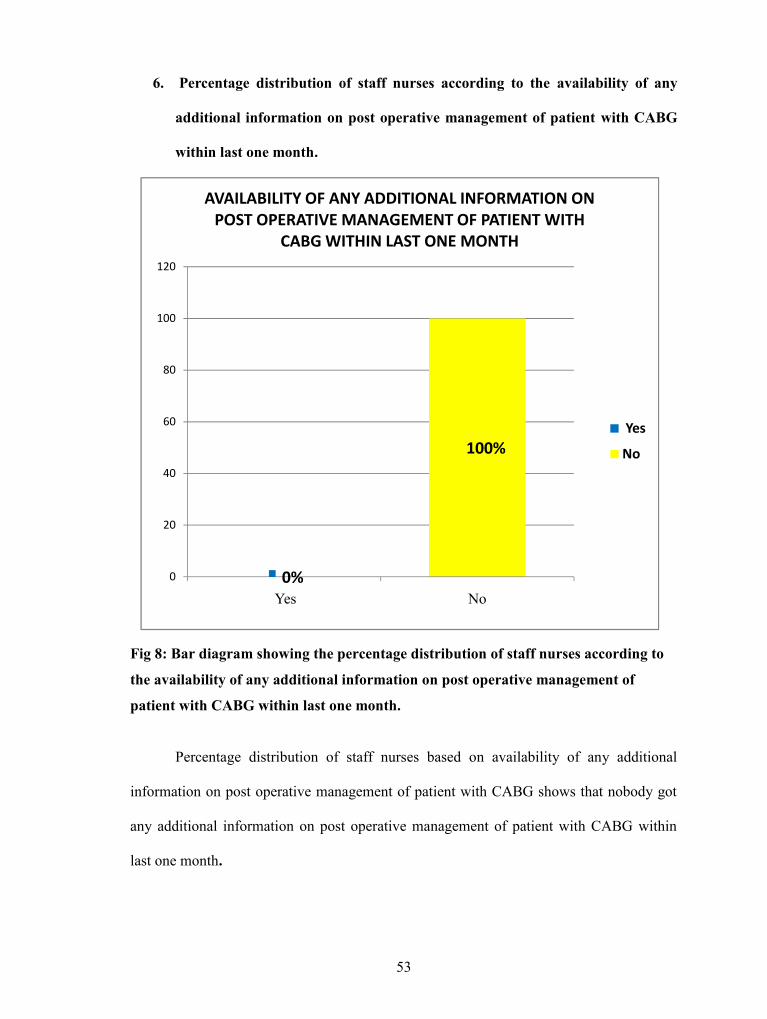
53
6. Percentage distribution of staff nurses according to the availability of any
additional information on post operative management of patient with CABG
within last one month.
Fig 8: Bar diagram showing the percentage distribution of staff nurses according to
the availability of any additional information on post operative management of
patient with CABG within last one month.
Percentage distribution of staff nurses based on availability of any additional
information on post operative management of patient with CABG shows that nobody got
any additional information on post operative management of patient with CABG within
last one month.
0%
100%
Yes No0
20
40
60
80
100
120
AVAILABILITY OF ANY ADDITIONAL INFORMATION ONPOST OPERATIVE MANAGEMENT OF PATIENT WITH
CABG WITHIN LAST ONE MONTH
Yes
No
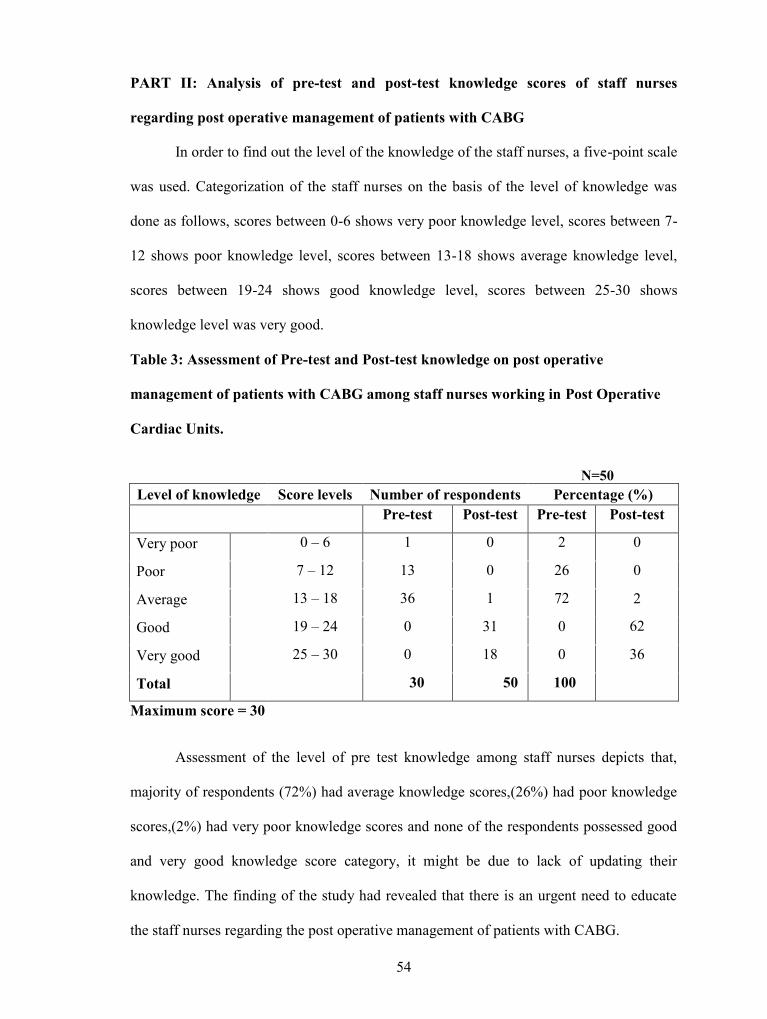
54
PART II: Analysis of pre-test and post-test knowledge scores of staff nurses
regarding post operative management of patients with CABG
In order to find out the level of the knowledge of the staff nurses, a five-point scale
was used. Categorization of the staff nurses on the basis of the level of knowledge was
done as follows, scores between 0-6 shows very poor knowledge level, scores between 7-
12 shows poor knowledge level, scores between 13-18 shows average knowledge level,
scores between 19-24 shows good knowledge level, scores between 25-30 shows
knowledge level was very good.
Table 3: Assessment of Pre-test and Post-test knowledge on post operative
management of patients with CABG among staff nurses working in Post Operative
Cardiac Units.
N=50Level of knowledge Score levels Number of respondents Percentage (%)
Pre-test Post-test Pre-test Post-test
Very poor 0 – 6 1 0 2 0
Poor 7 – 12 13 0 26 0
Average 13 – 18 36 1 72 2
62Good 19 – 24 0 31 0
Very good 25 – 30 0 18 0 36
Total 30 50 100
Maximum score = 30
Assessment of the level of pre test knowledge among staff nurses depicts that,
majority of respondents (72%) had average knowledge scores,(26%) had poor knowledge
scores,(2%) had very poor knowledge scores and none of the respondents possessed good
and very good knowledge score category, it might be due to lack of updating their
knowledge. The finding of the study had revealed that there is an urgent need to educate
the staff nurses regarding the post operative management of patients with CABG.
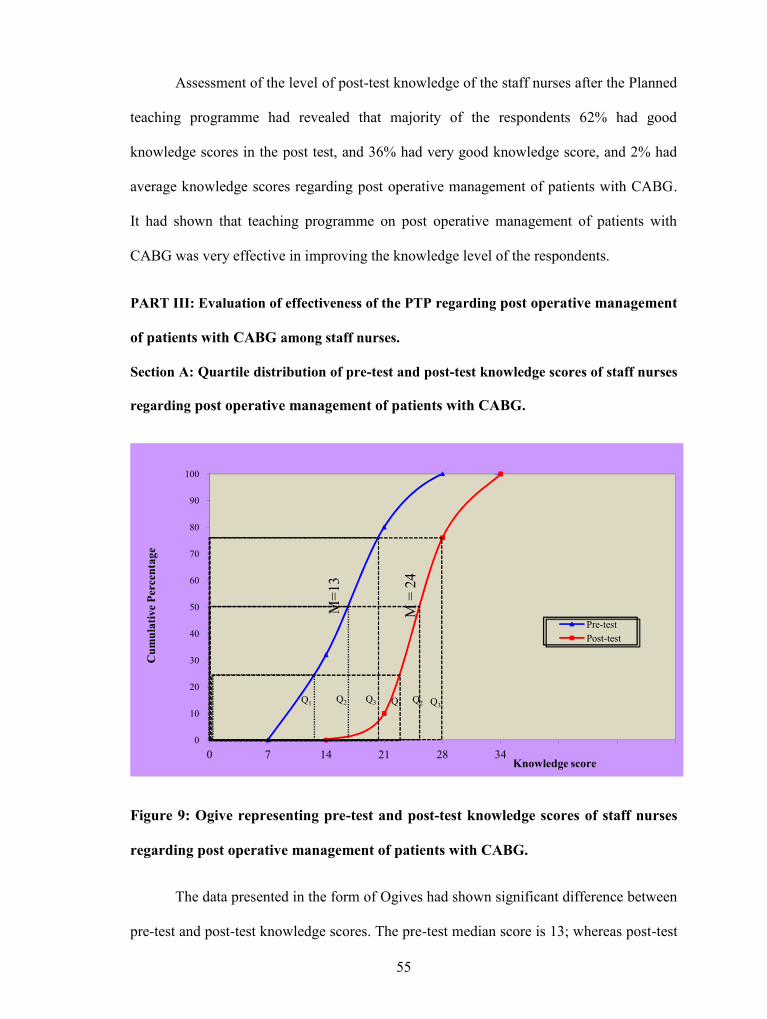
55
Assessment of the level of post-test knowledge of the staff nurses after the Planned
teaching programme had revealed that majority of the respondents 62% had good
knowledge scores in the post test, and 36% had very good knowledge score, and 2% had
average knowledge scores regarding post operative management of patients with CABG.
It had shown that teaching programme on post operative management of patients with
CABG was very effective in improving the knowledge level of the respondents.
PART III: Evaluation of effectiveness of the PTP regarding post operative management
of patients with CABG among staff nurses.
Section A: Quartile distribution of pre-test and post-test knowledge scores of staff nurses
regarding post operative management of patients with CABG.
Figure 9: Ogive representing pre-test and post-test knowledge scores of staff nurses
regarding post operative management of patients with CABG.
The data presented in the form of Ogives had shown significant difference between
pre-test and post-test knowledge scores. The pre-test median score is 13; whereas post-test
0
10
20
30
40
50
60
70
80
90
100
0 7 14 21 28 34
Cum
ulat
ive
Perc
enta
ge
Knowledge score
Pre-testPost-test
M=1
3
M =
24
Q1 Q1Q2 Q2Q3 Q3
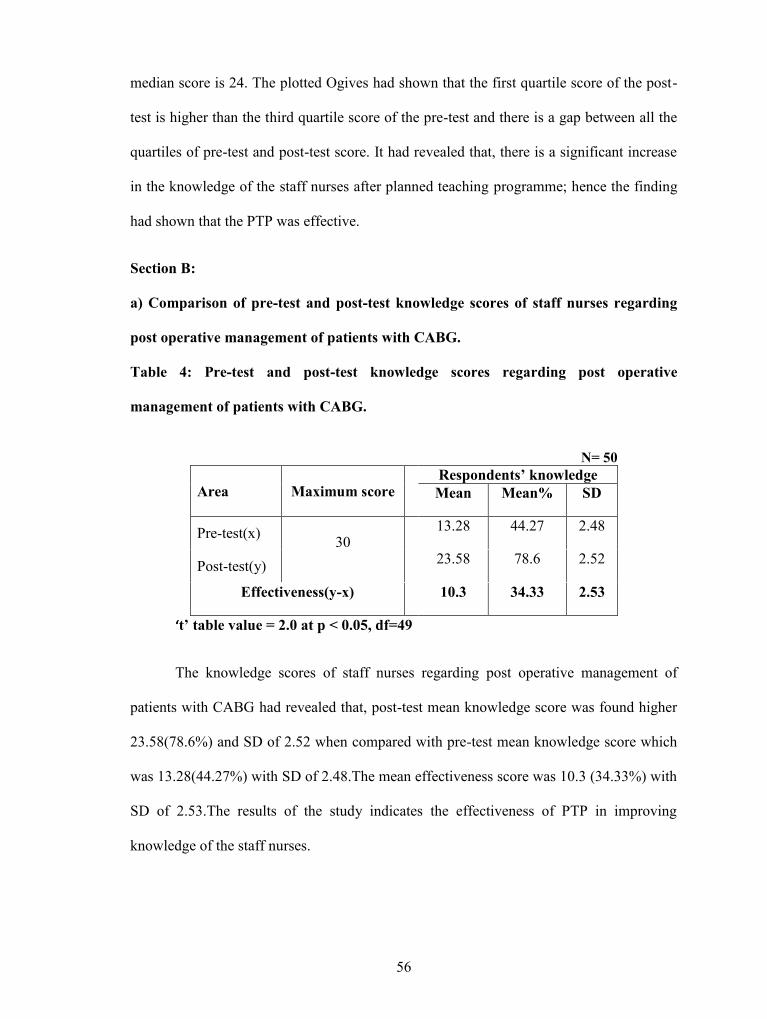
56
median score is 24. The plotted Ogives had shown that the first quartile score of the post-
test is higher than the third quartile score of the pre-test and there is a gap between all the
quartiles of pre-test and post-test score. It had revealed that, there is a significant increase
in the knowledge of the staff nurses after planned teaching programme; hence the finding
had shown that the PTP was effective.
Section B:
a) Comparison of pre-test and post-test knowledge scores of staff nurses regarding
post operative management of patients with CABG.
Table 4: Pre-test and post-test knowledge scores regarding post operative
management of patients with CABG.
N= 50
Area Maximum scoreRespondents’ knowledgeMean Mean% SD
Pre-test(x) 3013.28 44.27 2.48
Post-test(y) 23.58 78.6 2.52
Effectiveness(y-x) 10.3 34.33 2.53
‘t’ table value = 2.0 at p < 0.05, df=49
The knowledge scores of staff nurses regarding post operative management of
patients with CABG had revealed that, post-test mean knowledge score was found higher
23.58(78.6%) and SD of 2.52 when compared with pre-test mean knowledge score which
was 13.28(44.27%) with SD of 2.48.The mean effectiveness score was 10.3 (34.33%) with
SD of 2.53.The results of the study indicates the effectiveness of PTP in improving
knowledge of the staff nurses.
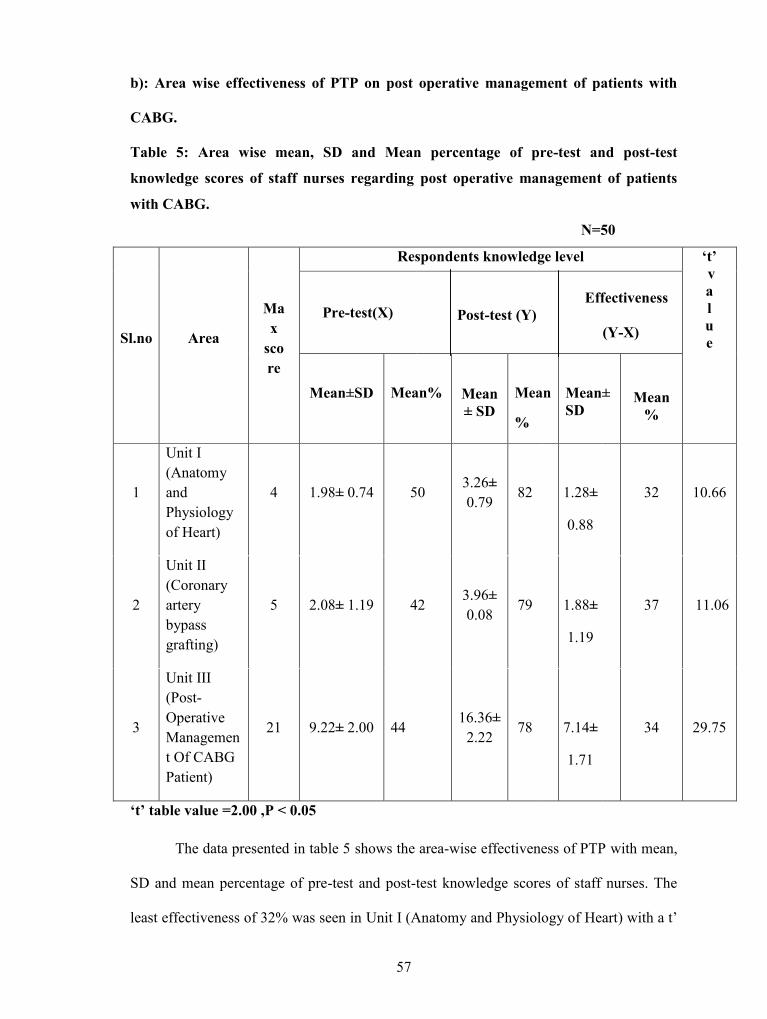
57
b): Area wise effectiveness of PTP on post operative management of patients with
CABG.
Table 5: Area wise mean, SD and Mean percentage of pre-test and post-test
knowledge scores of staff nurses regarding post operative management of patients
with CABG.
N=50
Sl.no Area
Max
score
Respondents knowledge level ‘t’value
Pre-test(X)Effectiveness
Post-test (Y)(Y-X)
Mean±SD Mean% Mean± SD
Mean
%
Mean±SD
Mean%
1
Unit I(AnatomyandPhysiologyof Heart)
4 1.98± 0.74 503.26±0.79
82 1.28±
0.88
32 10.66
2
Unit II(Coronaryarterybypassgrafting)
5 2.08± 1.19 423.96±0.08
79 1.88±
1.19
37 11.06
3
Unit III(Post-OperativeManagement Of CABGPatient)
21 9.22± 2.00 4416.36±
2.2278 7.14±
1.71
34 29.75
‘t’ table value =2.00 ,P < 0.05
The data presented in table 5 shows the area-wise effectiveness of PTP with mean,
SD and mean percentage of pre-test and post-test knowledge scores of staff nurses. The
least effectiveness of 32% was seen in Unit I (Anatomy and Physiology of Heart) with a t’
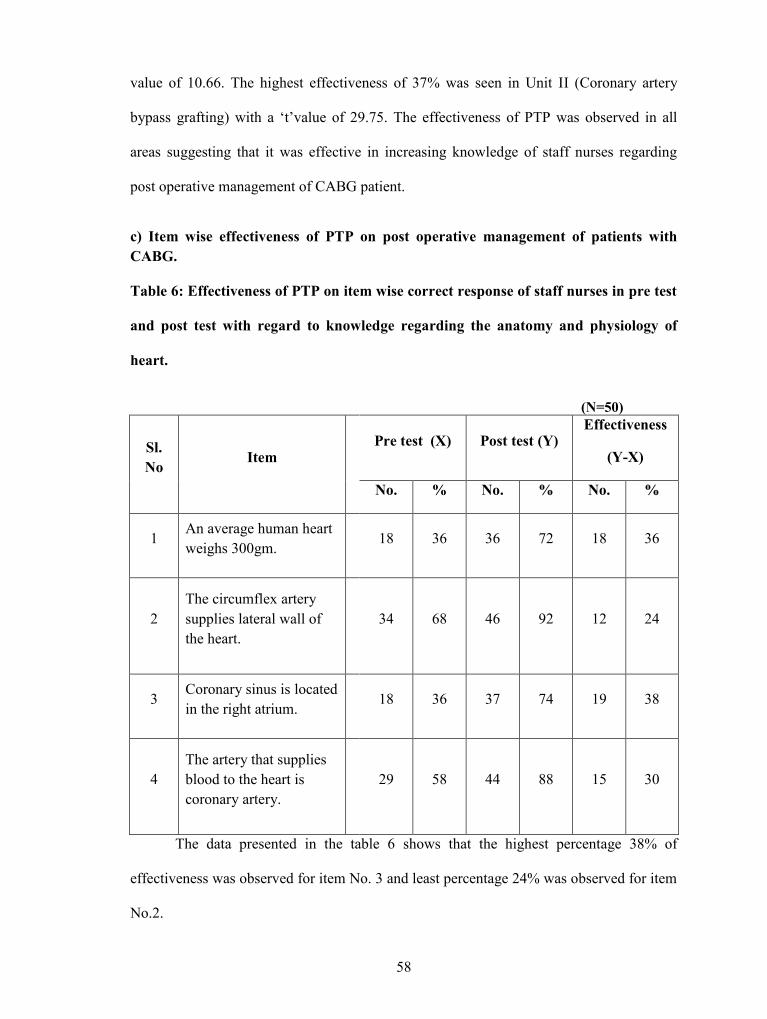
58
value of 10.66. The highest effectiveness of 37% was seen in Unit II (Coronary artery
bypass grafting) with a ‘t’value of 29.75. The effectiveness of PTP was observed in all
areas suggesting that it was effective in increasing knowledge of staff nurses regarding
post operative management of CABG patient.
c) Item wise effectiveness of PTP on post operative management of patients withCABG.
Table 6: Effectiveness of PTP on item wise correct response of staff nurses in pre test
and post test with regard to knowledge regarding the anatomy and physiology of
heart.
(N=50)
Sl.No Item
Pre test (X) Post test (Y)Effectiveness
(Y-X)
No. % No. % No. %
1An average human heartweighs 300gm.
18 36 36 72 18 36
2The circumflex arterysupplies lateral wall ofthe heart.
34 68 46 92 12 24
3Coronary sinus is locatedin the right atrium.
18 36 37 74 19 38
4The artery that suppliesblood to the heart iscoronary artery.
29 58 44 88 15 30
The data presented in the table 6 shows that the highest percentage 38% of
effectiveness was observed for item No. 3 and least percentage 24% was observed for item
No.2.
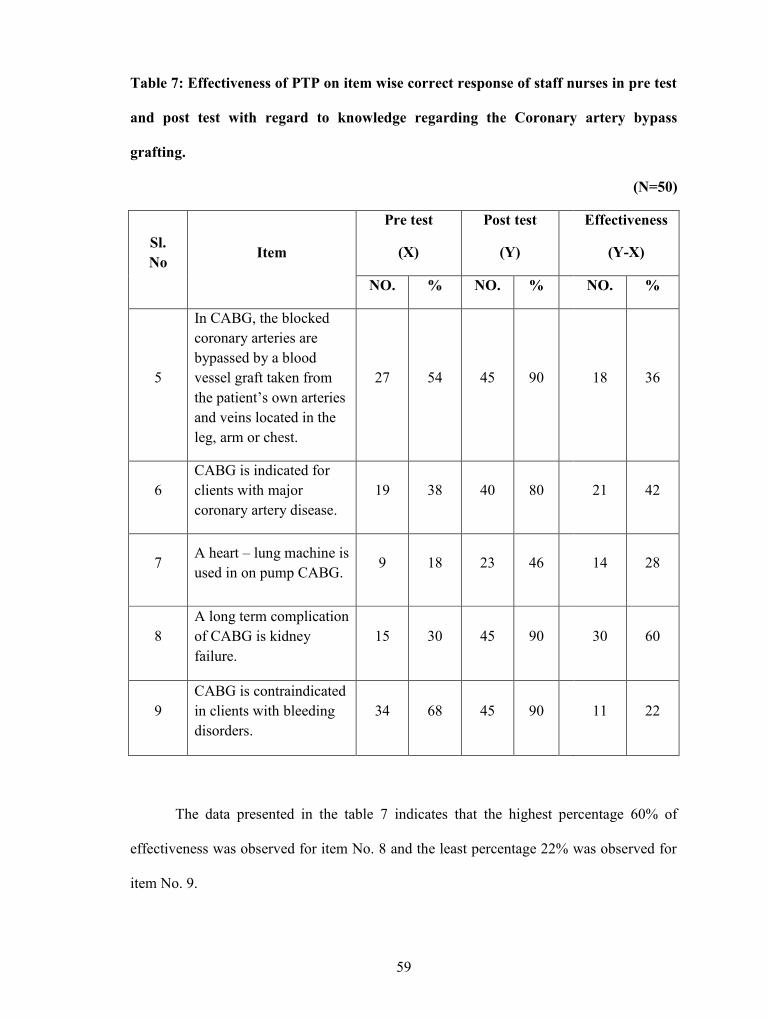
59
Table 7: Effectiveness of PTP on item wise correct response of staff nurses in pre test
and post test with regard to knowledge regarding the Coronary artery bypass
grafting.
(N=50)
Sl.No Item
Pre test
(X)
Post test
(Y)
Effectiveness
(Y-X)
NO. % NO. % NO. %
5
In CABG, the blockedcoronary arteries arebypassed by a bloodvessel graft taken fromthe patient’s own arteriesand veins located in theleg, arm or chest.
27 54 45 90 18 36
6CABG is indicated forclients with majorcoronary artery disease.
19 38 40 80 21 42
7A heart – lung machine isused in on pump CABG.
9 18 23 46 14 28
8A long term complicationof CABG is kidneyfailure.
15 30 45 90 30 60
9CABG is contraindicatedin clients with bleedingdisorders.
34 68 45 90 11 22
The data presented in the table 7 indicates that the highest percentage 60% of
effectiveness was observed for item No. 8 and the least percentage 22% was observed for
item No. 9.
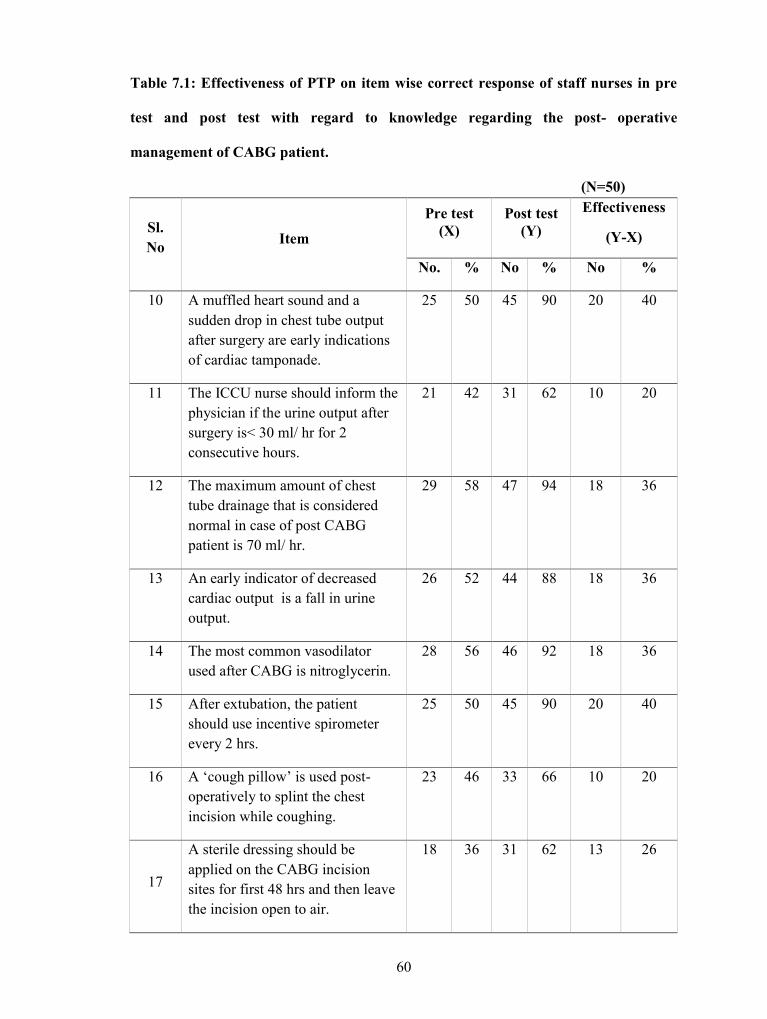
60
Table 7.1: Effectiveness of PTP on item wise correct response of staff nurses in pre
test and post test with regard to knowledge regarding the post- operative
management of CABG patient.
(N=50)
Sl.No Item
Pre test(X)
Post test(Y)
Effectiveness
(Y-X)
No. % No % No %
10 A muffled heart sound and asudden drop in chest tube outputafter surgery are early indicationsof cardiac tamponade.
25 50 45 90 20 40
11 The ICCU nurse should inform thephysician if the urine output aftersurgery is< 30 ml/ hr for 2consecutive hours.
21 42 31 62 10 20
12 The maximum amount of chesttube drainage that is considerednormal in case of post CABGpatient is 70 ml/ hr.
29 58 47 94 18 36
13 An early indicator of decreasedcardiac output is a fall in urineoutput.
26 52 44 88 18 36
14 The most common vasodilatorused after CABG is nitroglycerin.
28 56 46 92 18 36
15 After extubation, the patientshould use incentive spirometerevery 2 hrs.
25 50 45 90 20 40
16 A ‘cough pillow’ is used post-operatively to splint the chestincision while coughing.
23 46 33 66 10 20
17
A sterile dressing should beapplied on the CABG incisionsites for first 48 hrs and then leavethe incision open to air.
18 36 31 62 13 26
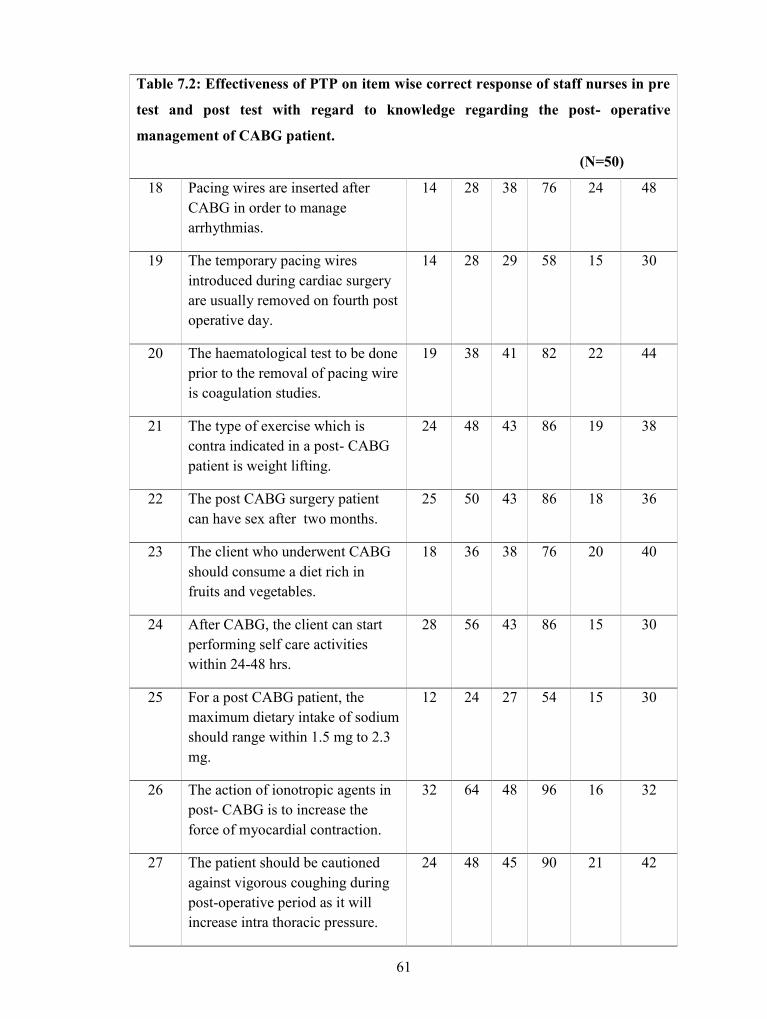
61
Table 7.2: Effectiveness of PTP on item wise correct response of staff nurses in pre
test and post test with regard to knowledge regarding the post- operative
management of CABG patient.
(N=50)
18 Pacing wires are inserted afterCABG in order to managearrhythmias.
14 28 38 76 24 48
19 The temporary pacing wiresintroduced during cardiac surgeryare usually removed on fourth postoperative day.
14 28 29 58 15 30
20 The haematological test to be doneprior to the removal of pacing wireis coagulation studies.
19 38 41 82 22 44
21 The type of exercise which iscontra indicated in a post- CABGpatient is weight lifting.
24 48 43 86 19 38
22 The post CABG surgery patientcan have sex after two months.
25 50 43 86 18 36
23 The client who underwent CABGshould consume a diet rich infruits and vegetables.
18 36 38 76 20 40
24 After CABG, the client can startperforming self care activitieswithin 24-48 hrs.
28 56 43 86 15 30
25 For a post CABG patient, themaximum dietary intake of sodiumshould range within 1.5 mg to 2.3mg.
12 24 27 54 15 30
26 The action of ionotropic agents inpost- CABG is to increase theforce of myocardial contraction.
32 64 48 96 16 32
27 The patient should be cautionedagainst vigorous coughing duringpost-operative period as it willincrease intra thoracic pressure.
24 48 45 90 21 42
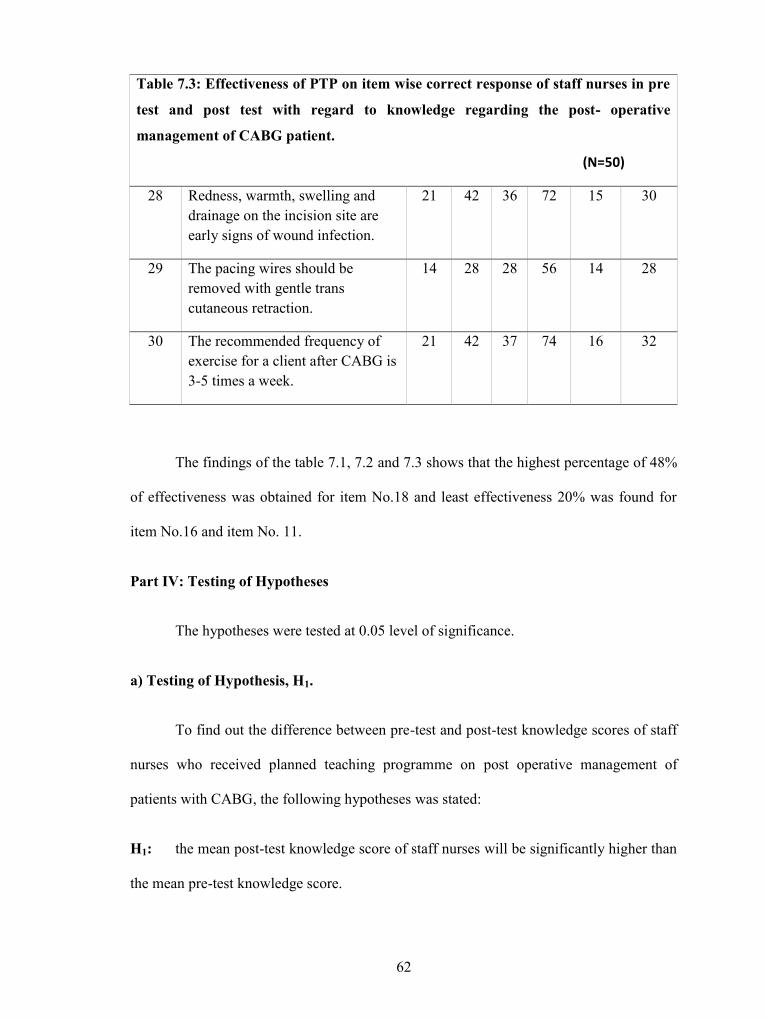
62
Table 7.3: Effectiveness of PTP on item wise correct response of staff nurses in pre
test and post test with regard to knowledge regarding the post- operative
management of CABG patient.
(N=50)
28 Redness, warmth, swelling anddrainage on the incision site areearly signs of wound infection.
21 42 36 72 15 30
29 The pacing wires should beremoved with gentle transcutaneous retraction.
14 28 28 56 14 28
30 The recommended frequency ofexercise for a client after CABG is3-5 times a week.
21 42 37 74 16 32
The findings of the table 7.1, 7.2 and 7.3 shows that the highest percentage of 48%
of effectiveness was obtained for item No.18 and least effectiveness 20% was found for
item No.16 and item No. 11.
Part IV: Testing of Hypotheses
The hypotheses were tested at 0.05 level of significance.
a) Testing of Hypothesis, H1.
To find out the difference between pre-test and post-test knowledge scores of staff
nurses who received planned teaching programme on post operative management of
patients with CABG, the following hypotheses was stated:
H1: the mean post-test knowledge score of staff nurses will be significantly higher than
the mean pre-test knowledge score.
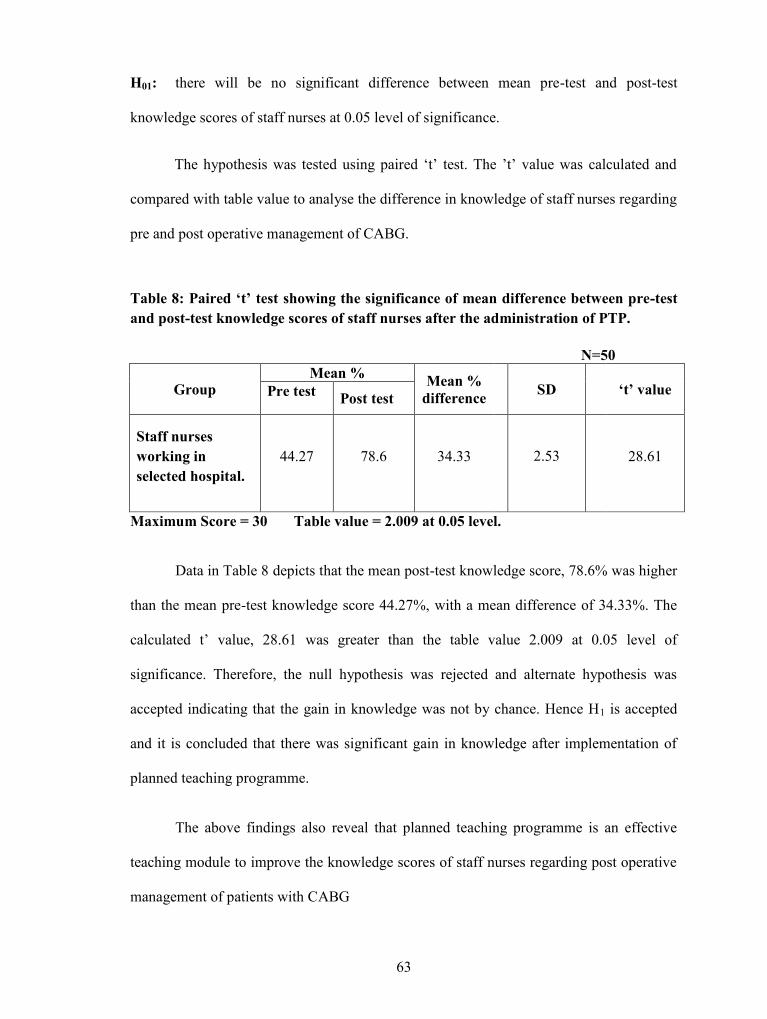
63
H01: there will be no significant difference between mean pre-test and post-test
knowledge scores of staff nurses at 0.05 level of significance.
The hypothesis was tested using paired ‘t’ test. The ’t’ value was calculated and
compared with table value to analyse the difference in knowledge of staff nurses regarding
pre and post operative management of CABG.
Table 8: Paired ‘t’ test showing the significance of mean difference between pre-testand post-test knowledge scores of staff nurses after the administration of PTP.
N=50
GroupMean % Mean %
difference SD ‘t’ valuePre test Post test
Staff nursesworking inselected hospital.
44.27 78.6 34.33 2.53 28.61
Maximum Score = 30 Table value = 2.009 at 0.05 level.
Data in Table 8 depicts that the mean post-test knowledge score, 78.6% was higher
than the mean pre-test knowledge score 44.27%, with a mean difference of 34.33%. The
calculated t’ value, 28.61 was greater than the table value 2.009 at 0.05 level of
significance. Therefore, the null hypothesis was rejected and alternate hypothesis was
accepted indicating that the gain in knowledge was not by chance. Hence H1 is accepted
and it is concluded that there was significant gain in knowledge after implementation of
planned teaching programme.
The above findings also reveal that planned teaching programme is an effective
teaching module to improve the knowledge scores of staff nurses regarding post operative
management of patients with CABG
64
b) Testing of Hypothesis, H2.
To evaluate the association of knowledge score with selected demographic
variables, the following hypotheses was stated:
H2: There will be significant association between pre-test knowledge score of the staff
nurses on post operative management of patients with CABG with selected demographic
variables.
H02: There will be no significant association between pre test knowledge score of the
staff nurses on post operative management of patients with CABG with selected
demographic variables at 0.05 level of significance.
Chi- Square test’ was done to analyse the significant association of pre test
knowledge scores with selected demographic variables such as age, sex, educational
qualification, experience in Post Operative Cardiac Units, participation in any special
training programme on post operative management of CABG and availability of any
additional information on post operative management of patient with CABG within last
one month of research study.
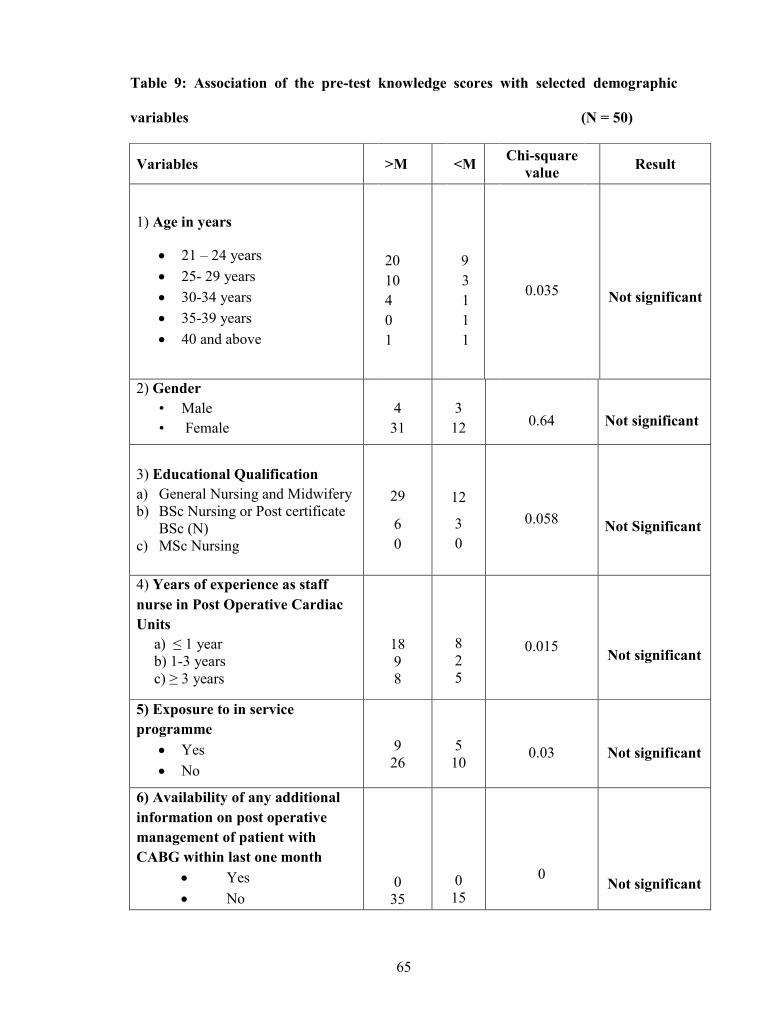
65
Table 9: Association of the pre-test knowledge scores with selected demographic
variables (N = 50)
Variables >M <M Chi-squarevalue Result
1) Age in years
21 – 24 years 25- 29 years 30-34 years 35-39 years 40 and above
2010401
93111
0.035 Not significant
2) Gender• Male• Female
431
312 0.64 Not significant
3) Educational Qualificationa) General Nursing and Midwiferyb) BSc Nursing or Post certificate
BSc (N)c) MSc Nursing
29
60
12
30
0.058 Not Significant
4) Years of experience as staffnurse in Post Operative CardiacUnits
a) ≤ 1 yearb) 1-3 yearsc) ≥ 3 years
1898
825
0.015 Not significant
5) Exposure to in serviceprogramme
Yes No
926
510
0.03 Not significant
6) Availability of any additionalinformation on post operativemanagement of patient withCABG within last one month
Yes No
035
015
0 Not significant
66
Data presented in table 9 shows that the chi square values of all demographic
variables, ie age, sex, educational qualification, experience in Post Operative Cardiac
Units, participation in any special training programme on post operative management of
CABG and availability of any additional information on post operative management of
patient with CABG within last one month of research study are not significant at 0.05
level of significance. Hence the null hypothesis H02 is accepted and research hypothesis is
rejected for all the demographic variables. Thus it is concluded that there was significant
association of pre-test knowledge score of staff nurses regarding pre and post operative
management of CABG and their educational qualification and area of experience.
Summary
This chapter has dealt with the analysis and interpretation of the study. The data
gathered was summarized in the master sheet and both descriptive and inferential statistics
were used for analysis. Sample characteristics were analysed using percentage. Paired t
test was used to analyse the effectiveness of planned teaching programme on post
operative management of CABG patient. The study findings had shown that there was a
significant increase in post test knowledge scores compared to pre test knowledge scores.
Then chi- square test was used to analyse the association of pre-test knowledge scores
with selected demographic variables and it was found to be not significant for all
demographic variables.
67
6. DISCUSSION
The purpose of this study was to evaluate the effectiveness of planned teaching
programme on knowledge regarding post operative management of patients with CABG
among staff nurses working in Post Operative Cardiac Units and to find out the association
of pre test knowledge scores of staff nurses with selected demographic variables. Fifty
staff nurses meeting the inclusion criteria were selected using purposive sampling
technique and data were collected before administering planned teaching programme
using structured knowledge questionnaire. Then these nurses were asked to complete same
questionnaire one week after the educational intervention. This chapter presents a discussion
of the study findings with reference to the objectives and hypotheses stated and the
comparison of these to the literature.
The findings of the study are as follows
Part I: Description of the demographic variables of staff nurses.
Part II: Analysis of knowledge scores of staff nurses regarding post operative
management of patients with CABG among staff nurses working in Post Operative
Cardiac Units.
Part III: Evaluation of effectiveness of the planned teaching programme on post operative
management of patients with CABG among staff nurses working in Post Operative
Cardiac Units.
Part IV: Testing of hypotheses.
68
Part I: Description of the demographic variables of staff nurses.
Distribution of the staff nurses with respect to their demographic variables shows
that highest percentage (56%) was in the age group of 21-24 years, maximum number
(86%) participated in the study were females, highest percentage (82%) has General
Nursing and Midwifery diploma, most (52%) of staff has ≤ 1 year of experience in Post
Operative Cardiac Units, many (72%) did not get any in-service classes on care of CABG
patients and nobody got any additional information on post operative management of
patient with CABG within last one month.
The above study findings is supported by another study conducted in USA to
explore and describe the experiences of registered nurses regarding in-service training
programs in their institutions and, to make recommendations to Nursing Service Managers
relating to the development of effective in-service training programs in their institutions. A
qualitative, exploratory, descriptive design was implemented. Data was analysed using
Tesch's descriptive approach. The study results showed that majority of registered nurses
experienced in-service training programs in their institution as inadequate. This highlights
the need for conducting more in-service education programmes to improve the knowledge
and skills of the staff nurses51.
Part II: Analysis of knowledge scores of staff nurses regarding post operative
management of patients with CABG among staff nurses working in Post Operative
Cardiac Units.
The findings of this study had shown that during pre-test, 72% of the sample
obtained scores ranging between 13 and 18 and none of them scored above 20 against the
maximum score of 30. The mean pre-test score was 13.28. Assessment of the level of
knowledge of the staff nurses after the administration of planned teaching programme
69
shows that majority of the respondents (62%) had good knowledge score, and 36% had
very good knowledge score on post operative management of patients with CABG. It
shows that planned teaching programme on post operative management of patients with
CABG was very effective in improving the knowledge level of the respondents.
An evaluatory approach one group pre-test post-test study was conducted to assess
the effectiveness of planned teaching programme on biomedical waste management
among forty staff nurses working in a selected hospital at Mangalore. The study findings
revealed that knowledge scores of staff nurses were inadequate before the administration
of planned teaching program. The planned teaching program facilitated them to update
their knowledge related to biomedical waste management. Post-test knowledge scores of
the staff nurses significantly increased after the planned teaching program which indicates
that the PTP regarding biomedical waste management was highly effective in enhancing
the knowledge levels of the nurses48.
Part III: Evaluation of effectiveness of the planned teaching programme on post
operative management of patients with CABG among staff nurses working in Post
Operative Cardiac Units.
The knowledge score of staff nurses on post operative management of patients
with CABG reveals that, post-test mean knowledge score was higher 23.58(78.6%) with
SD of 2.52 when compared with pre-test mean knowledge which was 13.28(44.27%) with
SD of 2.48. The mean effectiveness score was 10.3 (34.33) with SD of 2.53. Area wise
comparison of effectiveness of PTP also shows significant difference between pre test and
post test. Maximum effectiveness (37%) was observed in Unit II. Item wise analysis of
effectiveness of PTP shows that the highest percentage (60%) of effectiveness was
observed for item no. 8 and least (20%) was observed for item no. 11 and item no. 16. All
70
these findings indicate that there is significant gain in knowledge on post operative
management of patients with CABG among staff nurses after PTP.
A study was conducted to assess the effectiveness of PTP on knowledge
and practice of endotracheal suctioning among staff nurses in different intensive
care units of selected hospital in Mangalore. An evaluative research approach was
done. Sample size was 50 and purposive sampling was used. The overall mean post-test
knowledge score (27.5) was significantly higher than the overall means pre-test
score (17.0), the paired ‘t’ test value is 24.42 (t49 – 3.4 P 96 < 0.01). This shows that
PTP is an effective teaching aid for improving knowledge of staff nurses.46
Part IV: Testing of Hypotheses
Chi-square test was done to analyze the association between the pre-test
knowledge scores and the selected demographic variables. The study findings show that
shows that the chi square values of all demographic variables, i.e. age, sex, educational
qualification, experience in Post Operative Cardiac Units, participation in any special
training programme on post operative management of CABG and availability of any
additional information on post operative management of patient with CABG within last
one month of research study are not significant at 0.05 level of significance. Hence the
null hypothesis H02 is accepted and research hypothesis is rejected for all the demographic
variables.
The study is supported by study conducted in Mangalore about the knowledge of
nursing students on complementary therapies. The chi square values of demographic
variables like age, educational qualification, type of family, interest to work as nurse
midwife, and health information were (0.424, 0.349, 0.424, 0.471, 0.913) not significant at
0.05 level of significance. Results indicated that there is no significant association between

71
any of the demographic variables such as age, religion, education other than nursing and
their interest to work as nurse midwives and their knowledge.52
Summary
This chapter had discussed the significant findings of the study in relation to other
studies. Other studies have shown that the planned teaching programme is effective in
increasing the knowledge of staff nurses. Therefore, it was concluded that the gain in
knowledge of staff nurses through PTP on post operative management of patients with
CABG was significant.
72
7. CONCLUSION
The main aim of the study was to assess the knowledge of staff nurses regarding
post operative management of patients with CABG and teach them about it. Teaching was
given through PTP which helped the staff nurses to gain knowledge and skills on post
operative management of patients with CABG. The following conclusions were drawn on
the basis of findings of the study:
In the pre test, the distribution of staff nurses according to their level of knowledge
showed that majority of respondents, 72% had average knowledge scores and 26% had
poor knowledge scores.
Mean percentage of the knowledge score in the pre test was 44.27% with mean±
SD of 13.28±2.48, which had increased after administration of PTP with mean percentage
of 78.6% and mean± SD of 23.58±2.52. The planned teaching programme tested in the
study was found to be effective (t= 28.61, p< 0.05) in improving the knowledge on post
operative management of patients with CABG among staff nurses. This shows that PTP is
an effective teaching method for providing information.
Association of demographic variables with pre test scores was computed using chi-
square test. Analysis showed that, there is no significant association of selected
demographic variables with pre test knowledge scores.
Thus the findings indicate that there is lack of knowledge among staff nurses
regarding post operative management of patients with CABG and information through
various means like planned teaching programme is an important source of improving the
knowledge.
73
Nursing implications
Nursing is built on a body of knowledge discreetly synthesized from physical,
biological, and social science and uniquely applied as a humanistic discipline of caring for
people wherever they are recognizing the health care needs of patients. Nurses must
incorporate scientific knowledge and technical advances into their practice to assist the
patients in remaining well and functioning at the maximum level. The findings of the
study have several implications in the field of nursing practices, nursing education,
nursing administration and research.
Nursing Practice
All nurses have the responsibility to provide adequate care for the patients
undergoing CABG. These responsibilities are outlined in standards of practice, best
practice guidelines, and institutional policies and procedures. The implications for nursing
from this study include an emphasis of the need for nurses to gain knowledge regarding
post operative management of CABG patients and utilise this in their daily clinical
practice. This can be accomplished through preventing complications, reducing pain,
providing psychological support and providing discharge advices for the patients along
with appropriate interventions and documentation of findings, in accordance with the
standards of practice and institutional policies. Nurses must continue to expand their
knowledge and provide their patients with state of the art pre and post operative pain
management. The planned teaching programme used in the present study is one of the
means to improve nurses’ skills to reach positive outcome through appropriate knowledge.
74
Nursing Education
Education on post operative management of CABG patient should be an essential
part of nursing curricula at both graduate and undergraduate levels. Nursing curricula
should incorporate the entire major strategies essential in caring for patients admitted for
CABG. This will provide all nurses with a basic foundation on which they can grow in
their knowledge of caring Post Operative Cardiac Units patients, as it relates to caring
patients with differing cardiac surgeries. Their role is pivotal in raising awareness and
increasing the knowledge base of nurses, regarding the impact on patient outcomes that is
caused by unskilled and careless management. Special classes and in-service education
programmes should be conducted. The teaching programme can act as a good teaching
and learning material.
Nursing Administration
Nurse administrators in the inpatient setting are ultimately responsible for ensuring
positive patient outcomes. Administrators of clinical organizations must ensure proper
nursing management to their patients and to the community. The primary focus of today’s
healthcare administrators is to deliver cost-effective care and ensure patient satisfaction.
They also have the duty and responsibility to empower and align with the staff nurses to
implement a strategic plan designed to improve nursing management practices within their
organizations. By supporting staff nurses in continuing educational activities,
administrators will ensure adequate post operative management activities, improve patient
outcomes, and increase nursing and patient satisfaction.
Nursing Research
The present study has identified the gaps in knowledge of nurses regarding care of
CABG patients. This study guides future research related to testing the effects of
educational interventions in improving knowledge of nurses in other areas of cardiology
75
nursing. In addition, the replication of the study should be carried out with a larger sample
and multiple locations.
Limitations
The limitations of the present study are:
1. The study was confined to a small sample selected by purposive sampling techniques
which restricts the generalizability.
2. The study lacked control group to allow testing for an increase in knowledge without
planned teaching programme.
3. No attempt was made to do the follow-up to measure the retention of knowledge of the
staff nurses.
4. The utilisation of PTP by staff nurses could not be assessed in the live situation,
individually due to lack of time.
Suggestions
This study suggests that nurses need more information about management of
CABG patients so that these cases are recommended as applied results of this research:
- Holding classes and educational courses for staff nurses.
- Paying more attention to selection of Post Operative Cardiac Units staff.
- Designing policies for increasing the motivation for care giving among nurses.
- Taking measures for improving the quality of nursing courses.
- Determination of a clear administrator for training the nursing staff in each hospital.
76
Recommendations
Keeping in view the findings of the present study, the following recommendations are
made for further study:
1. A similar study can be conducted on a larger sample which may help to draw more
definite conclusions and make generalizations.
3. An experimental study could be undertaken with a control group.
4. A follow-up study of the PTP could be carried out to find the effectiveness in terms of
retention of knowledge.
Summary
This chapter has dealt with the conclusion drawn based on the findings of the study
and implication for nursing practice, nursing education, nursing administration and
nursing research, limitations, suggestions and recommendations of the study.
.
77
8. SUMMARY
This chapter presents a brief summary of research study. This chapter also includes
recommendations for future research and limitations of the study.
The main aim of the study was to evaluate the effectiveness of planned teaching
program on knowledge regarding post operative management of patients with CABG
among staff nurses working in Post Operative Cardiac Units of selected hospitals at
Mangalore
Objectives of the study
The objectives of the study are
1. To determine the level of knowledge among staff nurses regarding post operative
management of patients with CABG
2. To evaluate the effectiveness of planned teaching programme on level of
knowledge regarding post operative management of patients with CABG among
staff nurses in Post Operative Cardiac Units.
3. To find out the association between levels of knowledge regarding post operative
management of patients with CABG among staff nurses in Post Operative Cardiac
Units with their selected demographic variables i.e. age, sex, educational
qualification, experience in Post Operative Cardiac Units, participation in any
special training programme on post operative management of CABG and
availability of any additional information on post operative management of patient
with CABG within last one month of research study
78
Hypotheses
In order to assess the effectiveness of the PTP in terms of gain in knowledge on
post operative management of patients with CABG, the following hypotheses were
formulated and tested at 0.05 level of significance.
H1: Mean post test knowledge score of postoperative management of patients with CABG
among staff nurses in Post Operative Cardiac Units will be significantly higher than mean
pre test knowledge score.
H2: There will be significant association between pre test level of knowledge score of
staff nurses regarding post operative management of patients with CABG and with their
demographic variables such as age, sex, educational qualification, experience in Post
Operative Cardiac Units, participation in any special training programme on post operative
management of CABG and availability of any additional information on post operative
management of patient with CABG within last one month of research study.
Assumption
The study assumes that:
1. Staff nurses working in Post Operative Cardiac Units have inane knowledge regarding
post operative management of CABG patients.
2. Planned teaching programme may be effective in enhancing knowledge regarding post
operative management of CABG patients among staff nurses in Post Operative Cardiac
Units.
3. Planned teaching programme may result in enhancing competency of staff nurses and
may encourage use of evidence based practices.
4. Planned teaching programme may result in better nurse-patient relationship and increase
patient satisfaction.
79
Variables
• Independent variable: Planned teaching programme on knowledge regarding
postoperative management of CABG patients.
• Dependent variable: Level of knowledge among staff nurses regarding post-
operative management of CABG.
Conceptual framework adopted for the study
The conceptual framework for the present study was developed based on the
general system theory proposed by Ludwig Von Bertalanffy. This model had comprised
of concepts such as input which refers to demographic variables of the staff nurses, which
include age, sex, educational qualification, experience in Post Operative Cardiac Units,
participation in any special training programme on post operative management of CABG
and availability of any additional information on post operative management of patient
with CABG within last one month of research study; process which refers to the
administration of Structured Teaching Programme and output which is the knowledge
gained by the staff nurses and feedback.
Research methodology of the study
Pre experimental one group pre and post test design (O1 X O2) was adopted for the
study. The sample comprised of 50 staff nurses who fulfilled the inclusion criteria,
selected by purposive sampling technique.
The investigator prepared a structured knowledge questionnaire with 30 questions
and a planned teaching programme was developed based on review of literature and
discussion with the guide and other experts. The validity of the tool was carried out by
using Spearman Rank Correlation Coefficient and the tool was found reliable (r1 = 0.89).
80
A pilot study was conducted on five staff nurses in Wenlock Hospital, Mangalore in
September 2012. The main study was conducted from 2nd October to15th November 2012
at KMC, Mangalore and Omega Hospital, Mangalore among 50 staff nurses.
The data were analyzed with descriptive and inferential statistics (paired‘t‘ test and
chi squire test). The significance of PTP was proved with enhancement in the post-test
score and a mean of 23.58 in comparison to the mean of 13.28 in pre-test. It was also
evident from the paired t‘test (t=28.61; P < 0.05). This suggested that the PTP was
effective in improving the knowledge of staff nurses on post operative management of
CABG patient. No significant association was found between pre-test knowledge score
with selected demographic variables.
The findings of the present study will have great implications for nursing
education, nursing practice, nursing administration, and nursing research. Further research
studies are recommended to produce more reliable result.
The overall experience of conducting the study was a satisfying one. The constant
encouragement and guidance of the guide, cooperation and interest of the hospital
authorities and the respondents to participate in the study contributed to the successful
completion of the study. The respondents were satisfied and happy with the information
they received. The study was a new learning experience for the investigator. The present
study identified a great need for the staff nurses to update their knowledge regarding post
operative management of CABG patient. The study revealed that planned teaching
programme can be used as an effective teaching strategy.
81
9. BIBLIOGRAPHY
1. Kaul U, Bhatia V. Perspective on coronary interventions & cardiac surgeries in India.
Indian J Med Res 132 2010 Nov; 543-48.
2. Medindia. Coronary Artery Bypass Grafting (CABG). [Cited 2010]. Available from
www.medindia.net/Consumer Health/Health Information
3. Dr Alan G, Dr Marian W. Best Practice Guidelines for Cardiac Rehabilitation and
Secondary Prevention [Online]. 1999 Apr 8 [cited 1999 Jun 10]; Available from:
http://rubens.its.unimelb.edu.au/~heart/
4. Baskett RJF, Buth KJ, Collicott C, Ross DB. Preoperative cardiovascular risk factor
control in elective coronary artery bypass graft patients: A failure of present
management. Can J Cardiol 2002;18(4): 397-402.
5. Ozer N. The problems and needs of caregivers after coronary artery bypass graft
surgery: A literature review. 4th International Congress of Surgical and Operating
Room Nursing; 2003 Oct 22-26; School of Nursing, Atatürk University, Erzurum,
Turkey.
6. Wikimedia foundation. Coronary artery bypass surgery. [cited 2010 Jun 26].
Available from http://en.wikipedia.org/wiki/Coronary_artery_bypass_surgery
7. American Heart Association. American heart association’s heart disease and stroke
statistics 2009 update [cited Nov 18 2010]. Available from
www.americanheart.org/presenter.jhtml
8. Heart disease quotes. Heart bypass(allopathy). [cited Aug 2010]. Available from
www.whale.to/m/quotes20.html
82
9. Mortality Statistics On Bypass Surgery And Angioplasty [Cited Nov 2009]. Available
from www.heartprotect.com/mortality-stats.htm
10. Trehan N. Cardiovascular disease trends in India. Escorts Heart Institute and
Research Centre; 2006 Nov 16; New Delhi, India.
11. Suzanne C, Brenda GB, Janice LH , Kerry HC. Brunner and Suddarth's Textbook of
Medical Surgical Nursing. 12th edn. Lippincott Williams & Wilkins
12. Cesena FH, Favarato D, César DF, Oliveira SA, Luz PL. Cardiac complications
during waiting for elective coronary artery bypass graft surgery: incidence, temporal
distribution and predictive factors. Eur J Cardiothorac Surg 2004; 25:196-202.
Available from indmed.nic.in/imcwebij.html.
13. .Lewis SM, Heitkemper MM, Dirksen SR. Medical Surgical Nursing. 6th edition.
America: Mosby Publishers; 2000.
14. Philip K, Caves. Preoperative and postoperative management of patients undergoing
coronary artery bypass grafts. World J Surg 1978; 2: 829-842. Available from
www.springerlink.com/content/h60715241n57t514
15. Coronary artery bypass graft infection. [cited Nov 2009]. Available from
www.nuh.com.sg/infection/coronary-artery-bypass-graft-cabg-infections.html
16. Bhatia JY, Pandey K, Rodrigues C, Mehta A, Joshi VR. Postoperative wound
infection in patients undergoing coronary artery bypass graft surgery: a prospective
study with evaluation of risk factors. Indian J Med Microbiol 2003 Oct-Dec;
21(4)246-51.
17. Currey J, Browne J, Botti M. Haemodynamic instability after cardiac surgery: nurses'
perceptions of clinical decision-making. J Clin Nurs. 2006 Sep; 15(9):1081-90.
83
18. George B Julia. Nursing theories-the base for professional practice. 5th edition.New
Jersey: Prentice hall; 2002
19. Singh K.S. Methodology of research in education. 3rd edition. Patna: Sterling
publications pvt. Ltd; 2001.
20. Renjith R, Pegoraro RJ. Demographic data and outcome of acute coronary syndrome
in South African Asian Indian population. Indian Heart Journal 2005 Sept-Oct;
57(5):547.
21. Goldberg K C, Hartz A J, Jacobsen S J, Krakauer H, Rimm A A. Racial and
community factors influencing Coronary Artery Bypass Graft surgery rates for all
1986 Medicare patients. JAMA 1992; 267(11):1473-1477.
22. Daniel R, Padmaja N P. Angiographic profile of CAD in women in Urban Kerala.
Indian Heart Journal 2005 Sept-Oct; 57(5):548.
23. Sambasivam K A, Natarajan S. Revascularization pattern in female CAD. Indian
Heart Journal 2005 Sept-Oct; 57(5):558
24. Sebregts EH, Falger PR, Appels A, Kester AD, Bär FW. Psychological effects of a
short behavior modification program in patients with acute myocardial infarction or
coronary artery bypass grafting. A randomized controlled trial. J Psychosom Res
2005 May;58(5):417-24.
25. Theobald, Karen, McMurray, Anne. Coronary artery bypass graft surgery: discharge
planning for successful recovery. Journal of Advanced Nursing 47(5):483-491.
26. Omar A O, Saber A, Awad A, Atawi S. Perceived learning need for Jordanian nurses
and patient who undergo CABG surgery. [Online]. 2003 [cited 2004 Feb]; Available
from:URL:http://faculty.ksu.edu.sa/omar%20omari/.../Patient%20learning%20needs.
84
27. Chunta KS. Using Focus Groups to Explore Expectations of Open-Heart Patients.
SOJNR 9(1).
28. Van der Peijl ID, Vliet Vlieland TP, Versteegh MI, Lok JJ, Munneke M, Dion RA.
Exercise therapy after coronary artery bypass graft surgery: a randomized comparison
of a high and low frequency exercise therapy program. Ann Thorac Surg 2004
May;77(5):1535-41.
29. Hansen D, Dendale P, Leenders M, Berger J, Raskin A, Vaes J, et al. Reduction of
cardiovascular event rate: different effects of cardiac rehabilitation in CABG and PCI
patients. Acta Cardiol. 2009 Oct;64(5):639-44.
30. Binayak D, Michael W, Crean P.Smoking cessation reduces restenosis after CABG-
A ten year follow up study. Indian Heart Journal 2005 Sept-Oct; 57(5): 558.
31. Manoj S, Karthikeyan D, Davis S. Cardiac Rehabilitation For CABG Patients in
South Indian Setup : A Prospective Study. IJPMR 15, April 2004; 23-33.
32. Ashish C, Salgaonkar P. Marathan participation in heart disease patients. Indian Heart
Journal 2005 Sept-Oct; 57(5): 558.
33. Maraschinia A, Seccarecciaa F, D'Errigoa P, Rosatoa S. Role of gender and age on
early mortality after coronary artery bypass graft in different hospitals: data from a
national administrative database. Interact CardioVasc Thorac Surg 2010; 11:537-542.
34. Bolcal C, Iyem H, Sargin M. Gastrointestinal complications after cardio pulmonary
bypass: 16 year experience. Can J Gastroenterol 2005 Oct;19(10): 613-17.
35. Rodriguez R, Robich MP, Plate JF, Trooskin SZ, Sellke FW. Gastrointestinal
complications following cardiac surgery: a comprehensive review. Epub 2010 Mar;
25(2): 188-97
85
36. Jensen L, Yang L. Risk factors for postoperative pulmonary complications in
coronary artery bypass graft surgery patients. Eur J Cardiovasc Nurs. 2007
Sep;6(3):241-6.
37. Rath PK, Saha KK. Off pump CABG. Heart Journal 2005 Sept-Oct; 57(5): 556.
38. Leegaard M, Watt-Watson J, McGillion M, Costello J, Elgie-Watson J, Partridge K.
Nurses' educational needs for pain management of post-cardiac surgery patients: A
qualitative study. J Cardiovasc Nurs 2011 July-Aug; 26(4): 312-320.
39. Bergsland J, Kabil E, Mujanovic E, Terzic I. Training of cardiac surgeons and nurses
for Bosnia and Herzegovina: Outcomes in coronary bypass grafting surgery. Ann
Thorac Surg 2007; 83:462-467.
40. Larobina ME, Merry CJ, Negri JC, Pick AW. Is informed consent in cardiac surgery
and percutaneous coronary intervention achievable? ANZ J Surg. 2007 Jul;77(7):530-
34.
41. Kattainen E, Meriläinen P, Jokela V. CABG and PTCA patients’ expectations of
informational support in health- related quality of life themes and adequacy of
information in 1-year follow-up. Euro J Cardiovas Nurs 2004 July; 3(2): 149-163.
42. Watt-Watson J, Stevens B, Garfinkel P, Streiner D, Gallop R. Relationship between
nurses' pain knowledge and pain management outcomes for their postoperative
cardiac patients. J Adv Nurs. 2001 Nov;36(4):535-45.
43. Bergh AL, Bergh CH, Friberg F. How do nurses record pedagogical activities?
Nurses' documentation in patient records in a cardiac rehabilitation unit for patients
who have undergone coronary artery bypass surgery. J Clin Nurs. 2007
Oct;16(10):1898-907.
86
44. Vukanovic-Criley JM, Criley S, Warde CM, Boker JR, Guevara-Matheus L,
Churchill WH, et al. Competency in cardiac examination skills in medical students,
trainees, physicians, and faculty: A multicenter study. Arch Intern Med. 2006 Mar
27;166(6):610-16.
45. Sumitra.P.S 1998: Study to assess the knowledge and proclices of nursing personel on
immediate post operative care of cardiac surgery patient on ventilator page no 1- 2
46. Mathew 2001. Effectiveness of planned teaching programme on knowledge and
practice of endotracheal suctioning among staff nurses in the different ICU’s of
selected hospitals in Mangalore. (Unpublished thesis RGUHS Bangalore).
47. Nair. Effectiveness of a PTP to the 32 categories of bedridden neurological patients
on prevention of bedsore at ICMC, Manipal.
48. Rani, Ruby 2006.A study on effectiveness of planned teaching programme on
biomedical waste management among staff nurses working in a selected hospital at
Mangalore. (Unpublished thesis Manipal).
49. Polit DF, Hungler BP. Essentials of nursing research methods. Appraisal and
utilization. 5th ed. Philadelphia: JB Lippincott Company;2001.
50. Basavanthappa BT. Nursing research. 2nded, New Delhi: Jaypee Brothers
Medical Publishers; 2000
51. Norushe TF, Van Rooyen D, Strumpher J. In-service education and training as
experienced by registered nurses. Curationis. 2004 Nov;27(4):63-72.
52. Bincy B Samuel, 2010, effectiveness po PTP on complimentary therapies on labour
among nursing students in Mangalore unpublished MSc thesis, RGUHS, Bangalore.
53. Suresh K S. Nursing research & statistics. 1sted, New Delhi: Mosby Saunders
Publishers; 2011

87
ANNEXURE 1
88
ANNEXURE 2
Letter requesting permission to conduct pilot study, reliability and pretesting of thetool
Ref. No. KCNS/M.Sc(N) Dissert/867/2012-13
Date: 15-09-2012
To,The Superintendent,Gov. Wenlock Dist, HospitalMangalore
Respected Sir/Madam,
Sub: Letter seeking permission to conduct study.
With reference to above subject, Ms. Josephina Thomas, Student of IInd year M.Scnursing in Medical & Surgical Nursing department at our college of Nursing Science. She hasselected the following topic as her dissertation to be submitted Rajiv Gandhi University of healthScience, Bangalore in partial fulfilment of her course. Hence, I request you to give permission tocarry out her dissertation work in your esteemed institution. The data collection period isSeptember-October 2012.
Kindly permit her do the dissertation. I assure you that her study will not affect thesample/participants. The anonymity of the information will be kept confidential.
Topic “A study on the effectiveness of planned teaching programme on knowledge regardingPost operative Management of Patient with CABG among staff nurses working in Postoperative cardiac Units of selected hospitals of Mangalore.
Thanking you,
89
ANNEXURE 3
Letter seeking permission to conduct the main study

90
91
ANNEXURE 4
Letter requesting for expert opinion to establish content validity of the research tool
From,Ms. Josephina ThomasII year M.Sc. Nursing studentKaravali College of NursingMangalore.
To,
Subject: Request for expert opinion and suggestions to establish content validity of
the research tool.
Respected Sir/Madam,
I Ms. Josephina Thomas, II year M.Sc. Nursing student of KaravaliCollege of Nursing have selected the following topic for my dissertation to be submitted toRajiv Gandhi University of Health Sciences in partial fulfillment for the requirement foraward of Master of Sciences in Nursing.
Topic: “EFFECTIVENESS OF PLANNED TEACHING PROGRAMME ONKNOWLEDGE REGARDING POST OPERATIVE MANAGEMENT OFPATIENTS WITH CABG AMONG STAFF NURSES WORKING IN POSTOPERATIVE CARDIAC UNITS OF SELECTED HOSPITALS ATMANGALORE.”
Here with I have enclosed
• Objectives of the study, operational definitions and hypotheses.
• Demographic Performa
• Blueprint, tool and planned teaching.
• Criteria checklist.
I humbly request you to go through the items and give your valuablesuggestions and opinions to develop the content validity of the tool. Kindly suggestmodifications, additions and deletions, if any, in the remark column.
Thanking you in anticipation,
Date: Yours faithfully
Place: Mangalore Ms. Josephina Thomas
92
ANNEXURE 5Acceptance form for tool validation
NAME: -------------------------------
DESIGNATION: -------------------------------
NAME OF THE COLLEGE/HOSPITAL: -------------------------------
Statement of acceptance / non acceptance
I give my acceptance / non-acceptance to validate the tool.
Topic: “ EFFECTIVENESS OF PLANNED TEACHING PROGRAMME ON
KNOWLEDGE REGARDING POST OPERATIVE MANAGEMENT OF
PATIENTS WITH CABG AMONG STAFF NURSES WORKING IN POST
OPERATIVE CARDIAC UNITS OF SELECTED HOSPITALS AT
MANGALORE “
Date:
Place: Signature of the expert
93
ANNEXURE 6CONTENT VALIDITY CRETIFICATE
94
ANNEXURE 7Criteria checklist for validation of the tool
Instruction: Please review the items in the tool and give your valuable suggestions
regarding accuracy, relevance and appropriateness of the content. Kindly put a tick mark ()
in the appropriate column. If there are any suggestions or comments please mention in the
remarks column.
DEMOGRAPHIC VARIABLES
Q.No Agree Disagree Remarks
1.
2.
3.
4.
5.
6.
STRUCTURED KNOWLEDGE QUESTIONNAIRE
Q.No Agree Disagree Remarks
1.
2.
3.
4.
5.
6.
7.
8.
9.
95
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
96
ANNEXURE 8
Letter requesting Consent of the subjects for the participation in the study
Dear respondent,
I am a second year M. Sc. Nursing student of Karavali College of
Nursing, Mangalore. As a partial fulfilment of Master of Nursing Degree, I am conducting
a research study on the following topic:
“EFFECTIVENESS OF PLANNED TEACHING PROGRAMME ON
KNOWLEDGE REGARDING POST OPERATIVE MANAGEMENT OF
PATIENTS WITH CABG AMONG STAFF NURSES WORKING IN POST
OPERATIVE CARDIAC UNITS OF SELECTED HOSPITALS AT
MANGALORE.”
In this regard I would like to administer a questionnaire. I assure you that
the information obtained from you will be kept strictly confidential and used for the study
purpose only.
I expect your whole-hearted cooperation and will be grateful to you for the same.
Yours’ sincerely,
Signature of the participant Ms. Josephina Thomas
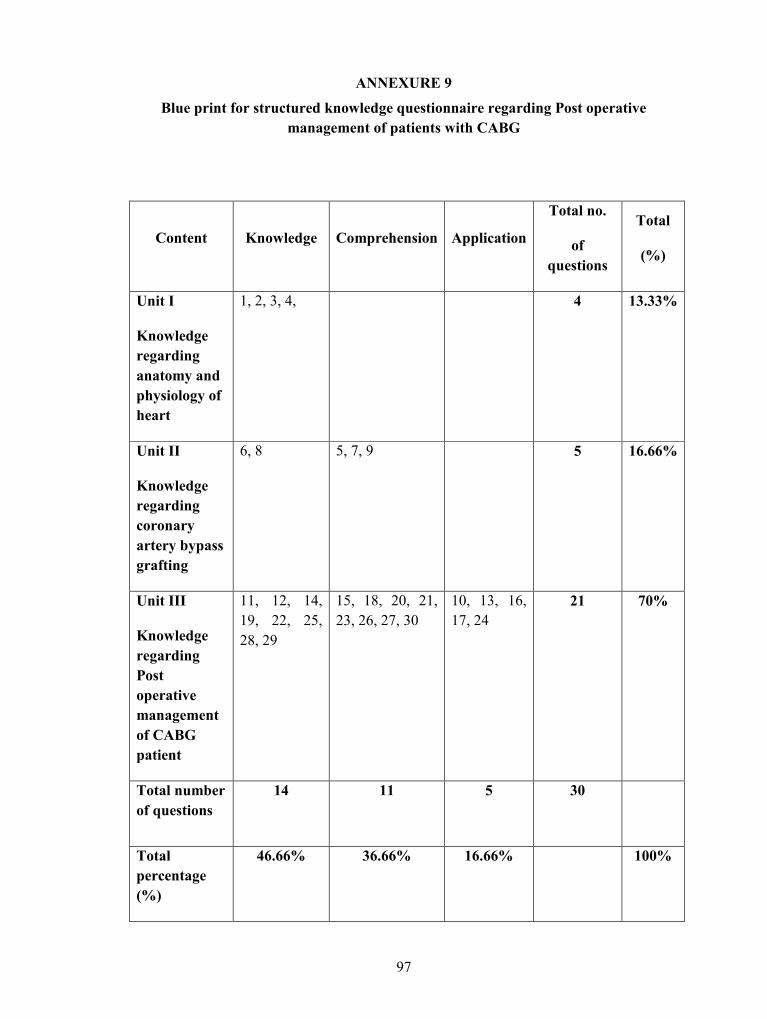
97
ANNEXURE 9Blue print for structured knowledge questionnaire regarding Post operative
management of patients with CABG
Content Knowledge Comprehension Application
Total no.
ofquestions
Total
(%)
Unit I
Knowledgeregardinganatomy andphysiology ofheart
1, 2, 3, 4, 4 13.33%
Unit II
Knowledgeregardingcoronaryartery bypassgrafting
6, 8 5, 7, 9 5 16.66%
Unit III
KnowledgeregardingPostoperativemanagementof CABGpatient
11, 12, 14,19, 22, 25,28, 29
15, 18, 20, 21,23, 26, 27, 30
10, 13, 16,17, 24
21 70%
Total numberof questions
14 11 5 30
Totalpercentage(%)
46.66% 36.66% 16.66% 100%
98
ANNEXURE 10
TOOL
Structured Knowledge Questionnaire To Assess The Knowledge Of Staff NursesRegarding Post Operative Management Of Patients With CABG
PART: 1 Demographic Profile
Instructions:
Please read the following questions carefully and choose the correct answer from the
choices given and indicate by placing a tick ( ) mark in the brackets provided. Please
answer for all the items.
1. Age in years.
a) 20-24 ( )
b) 25-29 ( )
c) 30 -34 ( )
d) 35 - 39 ( )
e) 40 and above ( )
2. Gender
a) Male ( )
b) Female ( )
3. Educational qualification
b) General Nursing and Midwifery ( )
c) BSc Nursing or Post certificate BSc (N) ( )
d) MSc Nursing ( )
4. Total years of experience in ICCU
a) ≤ 1 year ( )
b) 1-3 years ( )
c) ≥3 years ( )

99
5. Did you participate in any special training programme on post operative management of
CABG?
a) No ( )
b)Yes ( )
If Yes Specify -------------
6. Did you get any additional information on post operative management of patient with
CABG within last one month?
a) No ( )
b) Yes ( )
If Yes, Source of additional information:
b.1 Special training programme ( )
b.2 Journals ( )
b.3 News Papers ( )
b.4 Any Other, Specify ----------------
100
PART- 2 Structured Knowledge Questionnaire
Instructions:
Please read the following questions carefully and choose the correct answer from the
choices given and indicate by placing a tick ( ) mark in the brackets provided. Please
answer for all the items.
UNIT I: ANATOMY AND PHYSIOLOGY OF HEART
1) The average weight of an adult human heart is :
a) 3gm
b) 30gm ( )
c) 300gm ( )
d) 3000gm ( )
2) The circumflex artery supplies :
a) anterior wall of the heart ( )
b) posterior wall of the heart ( )
c) lateral wall of the heart ( )
d) inner wall of the heart ( )
3) Coronary sinus is located in the :
a) right atrium ( )
b) left atrium ( )
c) aorta ( )
d) pulmonary vein ( )
4) The artery that supplies blood to the heart is :
a) aorta ( )
b) coronary artery ( )
c) coronary sinus ( )
d) pulmonary artery ( )
101
UNIT II: CORONARY ARTERY BYPASS GRAFTING
5) In CABG, the blocked coronary arteries are bypassed by a blood vessel graft taken
from the patient’s own arteries and veins located in :
a) the leg, arm or chest ( )
b) the heart only ( )
c) the heart or lungs ( )
d) any part of the body ( )
6) CABG is indicated for clients with :
a) major coronary artery disease ( )
b) congenital heart disease ( )
c) severe hypotension ( )
d) cardiomyopathy ( )
7) A heart – lung machine is used in :
a) off pump CABG ( )
b) on pump CABG ( )
c) closed CABG ( )
d) open CABG ( )
8) A long term complication of CABG is :
a) portal hypertension ( )
b) infertility ( )
c) reynaud’s disease ( )
d) kidney failure ( )
9) CABG is contraindicated in clients with
a) more than three blockages ( )
b) age less than 50 years ( )
c) angina ( )
d) bleeding disorders ( )
102
UNIT III: POST OPERATIVE MANAGEMENT OF CABG PATIENT
10) A muffled heart sound and a sudden drop in chest tube output after surgery are
early indications of :
a) heart failure ( )
b) respiratory failure ( )
c) cardiac arrest ( )
d) cardiac tamponade ( )
11) The ICCU nurse should inform the physician if the urine output after surgery is :
a) > 30 ml/ hr for 2 consecutive hours ( )
b) < 30 ml/ hr for 2 consecutive hours ( )
c) < 60 ml/ hr for 2 consecutive hours ( )
d) > 60 ml/hr for 2 consecutive hours ( )
12) The maximum amount of chest tube drainage that is considered normal in case of a
post CABG patient is :
a) 7 ml/ hr ( )
b) 70 ml/ hr ( )
c) 170ml/hr ( )
d) 700 ml/ hr ( )
13) An early indicator of decreased cardiac output :
a) a sudden drop in chest tube drainage ( )
b) a fall in urine output ( )
c) severe nausea and vomiting ( )
d) strong and bounding peripheral pulses ( )
14) The most common vasodilator used after CABG is :
a) nitro-glycerine ( )b) digoxin ( )c) salbutamol ( )d) lasix ( )

103
15) After extubation, the patient should use incentive spirometer :
a) every 30 min ( )
b) every 2 hrs ( )
c) every 6 hrs ( )
d) 3 times a day ( )
16) A ‘cough pillow’ is used post-operatively to :
a) prevent coughing and related pain ( )
b) wean the patient from ventilator ( )
c) splint the chest incision while coughing ( )
d) elevate the chest region of the patient ( )
17) A sterile dressing should be applied on the CABG incision sites :
a) for first 48 hrs and then leave the incision open to air ( )
b) until the sutures are removed ( )
c) until the pacing wires are removed ( )
d) until the wound heals completely ( )
18) Pacing wires are inserted after CABG in order to :
a) manage arrhythmias ( )
b) increase blood supply to heart ( )
c) inject medications ( )
d) reduce risk for infection ( )
19) The temporary pacing wires introduced during cardiac surgery are usually removed
on :
a) first post operative day ( )
b) second post operative day ( )
c) third post operative day ( )
d) fourth post operative day ( )
20) The haematological test to be done prior to the removal of pacing wire is :
a) S. Cholesterol level ( )
b) ESR level ( )
c) coagulation studies ( )
d) blood culture ( )
21) The type of exercise which is contra indicated in a post- CABG patient is :
a) jogging ( )
b) cycling ( )
104
c) rowing ( )
d) weight lifting ( )
22) The post CABG surgery patient can have sex after :
a) two weeks ( )
b) one month ( )
c) two months ( )
d) three months ( )
23) The client who underwent CABG should consume a diet rich in :
a) salt and oil ( )
b) egg and meat ( )
c) dairy products ( )
d) fruits and vegetables ( )
24) After CABG, the client can start performing self care activities :
a) within 24-48 hrs ( )
b) only after four days ( )
c) only after one week ( )
d) after discharge from hospital ( )
25) For a post CABG patient, the maximum dietary intake of sodium should range
within:
a) 1.5 µg to 2.3 µg ( )
b) 1.5 mg to 2.3 mg ( )
c) 1.5 gm to 2.3 gm ( )
d) No restriction for Na ( )
26) The action of ionotropic agents in post- CABG is to :
a) increase the force of myocardial contraction ( )
b) decrease the force of myocardial contraction ( )
c) increase vascular resistance ( )
d) decrease vascular resistance ( )
27) The patient should be cautioned against vigorous coughing during post-operative
period as it will increase :
a) risk for infection ( )
b) risk for graft rejection ( )
c) blood pressure ( )
d) intra thoracic pressure ( )
105
28) Redness, warmth, swelling and drainage on the incision site are early signs of
wound :
a) approximation ( )
b) infection ( )
c) healing ( )
d) dehiscence ( )
29) The pacing wires should be removed :
a) with gentle trans cutaneous retraction ( )
b) by re exploring the chest wall ( )
c) by inserting a central venous catheter ( )
d) through coronary angiogram ( )
30) The recommended frequency of exercise for a client after CABG is :
a) 2-3 times daily ( )
b) 3-5 times a week ( )
c) once in a week ( )
d) as the client wish ( )
106
ANNEXURE 11
Answer key
Q.No. Answer Q.No. Answer
1 c 16 C
2 C 17 A
3 a 18 A
4 b 19 D
5 A 20 C
6 A 21 D
7 B 22 C
8 D 23 d
9 D 24 a
10 d 25 B
11 B 26 A
12 B 27 D
13 B 28 B
14 A 29 A
15 B 30 B
107
ANNEXURE-12
Evaluation criteria for content validity of PTP on post operative management ofpatients with CABG among staff nurses
NO CRITERIA
I
(Stronglyagree)
II
(Agree)
III
(Disagree) REMARKS
I Formulation of objectives
1 Comprehensiveenough
2 Realistic to achieve
3 Objectives are in termsof staff nurse’sbehavioral outcome.
II Selection of content
1 Content providesaccurate information asper the objectives
2 Content is according tothe level ofunderstanding of staffnurses.
III Organization of content
1 Logical sequence
2. Continuity ofpresentation
3. Integration of thecontent
IV Feasibility\practicability

108
1. The PTP content isacceptable to the staffnurses
2. The content is to thelevel of staff nurses’understanding.
3. The content isconventional to handleand conduct.
4. The content isinteresting to the staffnurses
5. The content iseconomical in terms ofcost, effort and time.
Any other suggestions
Signature of the Valuator

109
ANNEXURE 13
A PLANNED TEACHING PROGRAMME
ON
POST OPERATIVE MANAGEMENT OF PATIENTS WITH CABG
110
TOPIC : Post operative management of patients with CABG
GROUP : Staff nurses working in Post Operative Cardiac Units
NUMBER OF PARTICIPANTS : 50
PLACE : Conference hall
DURATION : 1 hour
METHOD OF TEACHING : Lecture cum discussion
A V AIDS : L C D
GENERAL OBJECTIVES
On completion of teaching session the staff nurses gain in depth knowledge regarding coronary artery bypass graft surgery, its
indications, contraindications, complications and post operative management and able to apply the gained knowledge in their daily life.
SPECIFIC OBJECTIVES
After completion of the class, staff nurses will be able to,
1. Explain anatomy and physiology of heart
2. Discuss the blood supply to the heart.
3. Define CABG.
4. List down the purposes of CABG
5. Enumerate the indications and contraindications of CABG.
6. Describe the types of CABG.
7. List down the complications of CABG.
8. Explain the post operative management of CABG
111
SPECIFICOBJECTIVE
Introduce thetopic
Explainanatomy andphysiology ofheart
CONTENT
INTRODUCTIONCoronary artery bypass grafting is a surgical procedure
performed to relieve angina and reduce the risk of death fromcoronary artery disease. The care of post CABG patient is intense,complex and rewarding. These patients require prompt support togo through this most crisis situation of their life. It is theresponsibility of the nurse to prioritize the needs carefully, educatethe client and family and enable the client to go through the crucialpost operative period safely.
ANATOMY AND PHYSIOLOGY OF HEART
• Heart is a hollow muscular organ for circulation of blood.
• Heart is situated under the ribcage in the centre of the chestbetween right and left lungs.
• Heart is encased in a serous membrane, the Pericardium.
• Its muscular walls beat, or contract, pumping bloodcontinuously to all parts of your body.
• The size of the heart can vary depending on the age, size, andthe condition of heart. A normal, healthy, adult heart mostoften is the size of an average clenched adult fist.
TEACHERS’LEARNERS’ACTIVITY
Teacher:Introducesthe topicLearner:Listens
Teacher:explainsLearner: listens
A.V AIDS
LCD
Heart
EVALUATION
What is theaverageweight of ahumanheart?
112
• The heart weighs approximately one pound or 300gm.
• The four chambers of the heart constitute the right- and leftsided pumping systems.
• The right side of the heart, made up of the right atrium and rightventricle, distributes venous blood (deoxygenated blood) to thelungs via the pulmonary artery (pulmonary circulation) foroxygenation. The right atrium receives blood returning from thesuperior vena cava (head, neck, and upper extremities),inferior vena cava (trunk and lower extremities), and coronarysinus (coronary circulation).
• The left side of the heart, composed of the left atrium and leftventricle, distributes oxygenated blood to the remainder of thebody via the aorta (systemic circulation). The left atriumreceives oxygenated blood from the pulmonary circulation viathe pulmonary veins.
Function of the heart• The heart works as a pump moving blood around in our
bodies to nourish every cell. Used blood is drawn from thebody by the right half of the heart, and then sent to the lungsto be reoxygenated. Blood that has been reoxygenated by thelungs is drawn into the left side of the heart and then pumpedinto the blood stream.
Which bloodvessel carriesdeoxygenated blood fromheart tolungs?
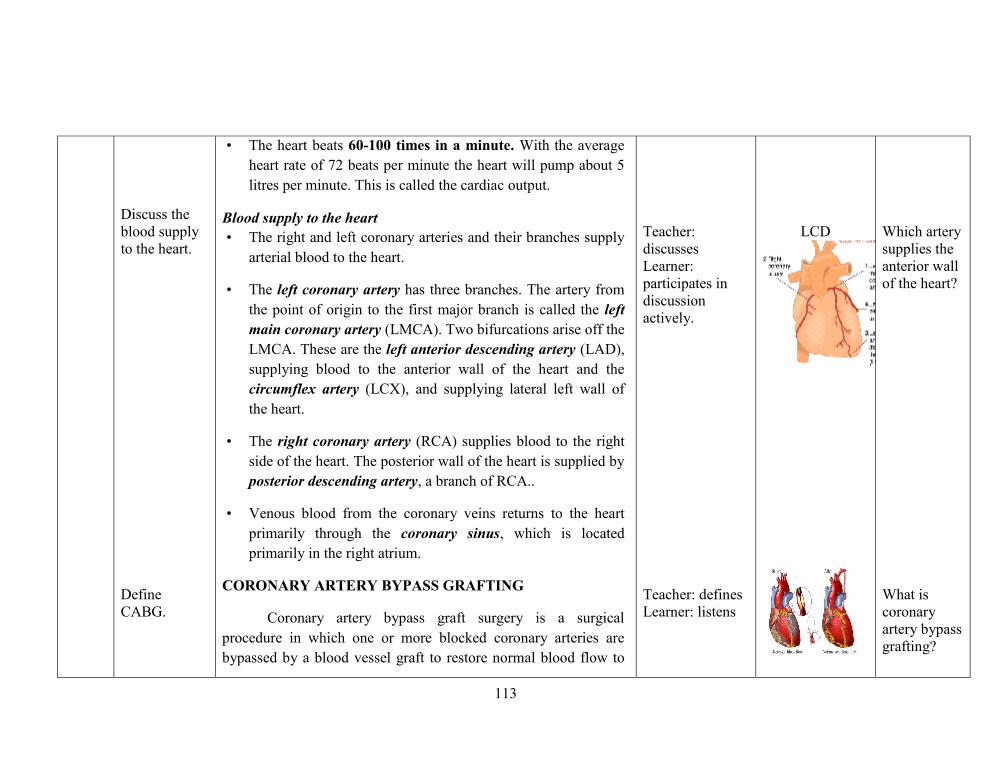
113
Discuss theblood supplyto the heart.
DefineCABG.
• The heart beats 60-100 times in a minute. With the averageheart rate of 72 beats per minute the heart will pump about 5litres per minute. This is called the cardiac output.
Blood supply to the heart• The right and left coronary arteries and their branches supply
arterial blood to the heart.
• The left coronary artery has three branches. The artery fromthe point of origin to the first major branch is called the leftmain coronary artery (LMCA). Two bifurcations arise off theLMCA. These are the left anterior descending artery (LAD),supplying blood to the anterior wall of the heart and thecircumflex artery (LCX), and supplying lateral left wall ofthe heart.
• The right coronary artery (RCA) supplies blood to the rightside of the heart. The posterior wall of the heart is supplied byposterior descending artery, a branch of RCA..
• Venous blood from the coronary veins returns to the heartprimarily through the coronary sinus, which is locatedprimarily in the right atrium.
CORONARY ARTERY BYPASS GRAFTING
Coronary artery bypass graft surgery is a surgicalprocedure in which one or more blocked coronary arteries arebypassed by a blood vessel graft to restore normal blood flow to
Teacher:discussesLearner:participates indiscussionactively.
Teacher: definesLearner: listens
LCD Which arterysupplies theanterior wallof the heart?
What iscoronaryartery bypassgrafting?
114
List down thepurposes ofCABG
Enumerate theindicationsandcontraindications of CABG.
Describe thetypes ofCABG.
the heart. These grafts usually come from the patient's ownarteries and veins located in the leg, arm, or chest.
Purposes
• Restore blood flow to the heart.
• Enable the patient to resume a normal lifestyle
• Relieves chest pain and ischemia,
• Improves the patient's quality of life
• To lower the risk of a heart attack
Indications
• Patients who cannot tolerate PTCA
• Patients with blockages in at least three major coronaryarteries
• Patients with angina
• Do not respond well to drug therapy.
Contraindications
• Bleeding disorders.
• Acute Cerebral vascular Accident
Types• On-pumpCABG: requires surgeon to open the chest bone
(sternum), stop the patient's heart, and place the patient
Teacher:Lists downLearner:Listens
Teacher:enumeratesLearner:Listens
Teacher:describesLearner:Listens
LCD
LCD
LCD
What are thepurposes ofCABG?
What are thecontraindications ofCABG?
115
List down thecomplicationsof CABG.
on a heart lung machine which takes over the function ofthe patient's heart while the bypass is performed.
• Off pumpCABG: The surgeon operates directly on thebeating heart, reducing the risk for peri-operativebleeding and stroke associated with the on-pumpprocedure.
Complications
• Immediate Complications• Bleeding
• Infection
• Heart attack
• Damage to the aorta
• Abnormal heart rhythms
• High or low blood pressure
• Long Term Complications• Kidney Failure
• Stroke
• Atherosclerotic disease of saphenous vein grafts
• Depression or severe mood swings
Teacher:listsLearner:listens
LCD
What is on-pumpCABG?
What are thelong termcomplications of CABG?

116
Explain thepost operativemanagementof CABG.
• Possible short-term memory loss, difficulty thinkingclearly, and problems concentrating for long periods
POST OPERATIVE MANAGEMENT OF CABG PATIENT
• ASSESSMENT
• Monitor vital signs, oxygen saturation, andhemodynamic parameters every 15 minutes.
• Initial hypothermia and bradycardia are expected; theheart rate should return to the normal range withrewarming.
• The blood pressure may fall during rewarming asvasodilation occurs. Hypotension and tachycardia,however, may indicate low cardiac output.
• Pulmonary artery pressure (PAP), pulmonary arterywedge pressure (PAWP), cardiac output, and oxygensaturation are monitored to evaluate fluid volume, cardiacfunction, and gas exchange.
• Auscultate heart and breath sounds on admission and atleast every 4 hours.
• A ventricular gallop, or S3, is an early sign of heartfailure; an S4 may indicate decreased ventricularcompliance. Muffled heart sounds may be an earlyindication of cardiac tamponade.
• Adventitious breath sounds (wheezes, crackles, or rales)may be a manifestation of heart failure or respiratory
Teacher:explainsLearners:Listens
Teacher:explainsLearners:Listens
LCD
LCD What is theearlyindication ofcardiactamponade?
117
compromise.• Assess skin colour and temperature, peripheral pulses,
and level of consciousness with vital signs.• Pale, mottled, or cyanotic colouring, cool and clammy
skin, and diminished pulse amplitude are indicators ofdecreased cardiac output.
• Continuously monitor and document cardiac rhythm.• Dysrhythmias are common, and may interfere with
cardiac filling and contractility, decreasing the cardiacoutput.
• Measure intake and output hourly. Report urine outputless than 30 ml/h for 2 consecutive hours.
• A fall in urine output may be an early indicator ofdecreased cardiac output.
• Record chest tube output hourly.• Chest tube drainage greater than 70 ml/hr or that is warm,
red, and free flowing indicates haemorrhage and maynecessitate a return to surgery.
• A sudden drop in chest tube output may indicateimpending cardiac tamponade.
• Monitor haemoglobin, hematocrit, and serumelectrolytes.
• A drop in haemoglobin and hematocrit may indicatehaemorrhage that is not otherwise obvious.
• Electrolyte imbalances, potassium, calcium, andmagnesium in particular, affect cardiac rhythm andcontractility.
Teacher:explainsLearners:Listens
LCD Which is theneed formonitoringcardiacrhythmcontinuouslyin a postCABGpatient?
118
INCREASING CARDIAC OUTPUT• Administer intravenous fluids, fluid boluses, and blood
transfusions as ordered.• Fluid and blood replacement helps ensure adequate
blood volume and oxygen-carrying capacity.• Administer medications as ordered. Medications ordered in
the early postoperative period to maintain the cardiac outputinclude
• Inotropic drugs (e.g., dopamine, dobutamine) to increasethe force of myocardial contractions.
• Vasodilators (e.g., nitroprusside or nitroglycerin) todecrease vascular resistance and after load
• Antidysrhythmics to correct dysrhythmias that affectcardiac output.
• Keep a temporary pacemaker at the bedside; initiatepacing as indicated.
MAINTAINANCE OF AIRWAY
• Note endotracheal tube (ETT) placement on chest X-ray.Mark tube position and secure in place. Insert an oral airwayif an oral ETT is used.
• Maintain ventilator settings as ordered. Monitor arterialblood gases (ABGs) as ordered.
• Suction as needed to clear airway secretions.• Prepare for ventilator weaning and extubation, as
appropriate. The client is removed from the ventilator and
Teacher:explainsLearners:Listens
Teacher:explainsLearners:Listens
LCD
LCD
Which arethe majordrugs givenin the earlypostoperativeperiod ofCABGsurgery?
Whyvigorouscoughing iscontraindicated afterCABGsurgery?
119
extubated as soon as possible to reduce complications.• After extubation, teach use of the incentive spirometer, and
encourage use every 2 hours. Frequently turn and encouragemovement.
• Encourage deep breathing; advise against vigorouscoughing. Vigorous coughing may excessively increaseintrathoracic pressure and cause sternal instability.REDUCING PAIN
• Frequently assess for pain, including its location andcharacter .Document its intensity using a standard painscale. Assess for verbal and nonverbal indicators of pain.
• Administer analgesics on a scheduled basis, by PCA, or bycontinuous infusion for the first 24 to 48 hours.
• Premedicate 30 minutes before activities or plannedprocedures.
• Teach use of a “cough pillow” to splint chest incision anddecrease pain.
PREVENTING INFECTION• Assess sternal wound every shift. Document redness,
warmth, swelling, and/or drainage from the site. Note woundapproximation.
• Maintain a sterile dressing for the first 48 hours, and thenleave the incision open to air. The sterile dressing preventsearly contamination of the wound, whereas leaving exposingthe incision after 48 hours promotes healing.
• Report signs of wound infection: a swollen, reddened area
Teacher:explainsLearners:Listens
LCD
120
that is hot and painful to the touch; drainage from thewound; impaired healing, or healed areas that reopen.
• Culture wound drainage as indicated. Identifying theinfective organism facilitates appropriate antibiotic therapy.
• Collaborate with the dietician to promote nutrition and fluidintake. Good nutritional status is vital to healing andimmune function.
REMOVING TEMPORARY PACING WIRESAtrial and/or ventricular pacing wires are frequently
inserted at the end of a cardiac surgical procedure. Their mainuse is to improve hemodynamic function in the presence ofarrhythmias as well as to suppress atrial and ventriculartachyarrhythmia.
• Pacing wires are usually removed on the fourthpostoperative day.
• Prior to removal, a coagulation screen should be checked.• Wires are removed with gentle transcutaneous retraction.• The patient's vital signs should be monitored following wire
removal to allow early identification of the rare but well-documented potential complications.
ASSISTING IN LIFESTYLE CHANGES/ CARDIACREHABILITATION
The discharge nurse should assist the patient to makeseveral lifestyle changes after surgery, including:
Teacher:explainsLearners:Listens
Teacher:explainsLearners:Listens
LCD
LCD What is theneed to quitsmokingafter CABGsurgery?
121
• Quitting smoking. Smoking cause damage to the bypassgrafts and other blood vessels, increases the patient's bloodpressure and heart rate, and decreases the amount of oxygenavailable in the blood.
• Managing weight. Maintaining a healthy weight, bywatching portion sizes and exercising, is important. Beingoverweight increases the work of the heart.
• Making dietary changes. The American HeartAssociation's dietary guidelines, are as follows:
• Less than 7% of calories coming from saturated fat.
• Less than 1% of calories from trans fat
• Less than 300 mg of dietary cholesterol per day.
• Consume fish, especially oily fish, twice a week.
• Choose whole-grain, high fibre foods.
• Consume a diet rich in fruits and vegetables.
• Select all fat free, 1 percent, or low fat dairy products.
• Cut back on foods and beverages with added sugar.
• Choose and prepare foods with little or no added salt.Aim to eat 1,500 mg – no greater than 2,300 mg ofsodium per day.
• If you consume alcohol do so in moderation.
• Balance calorie intake and physical activity to maintain ahealthy body weight.
Teacher:explainsLearners:Listens
LCD What is theneed formanagingweight in apost CABGperson?
122
• Taking medications as prescribed. Aspirin and other heartmedications may be prescribed, and the patient may need totake these medications for life.
• Safe sex. After two months of post CABG surgery thepatient can have sex. If recurrent chest pain, abnormal heartrhythms or heart failure at intermediate or high risk ofheart-related problems occur during sex, consult the doctorand then resume sex.
• Following up with health care providers: The patientmust schedule follow-up visits to determine how effectivethe surgery was, to confirm that progressive exercise is safe,and to monitor his or her recovery and control risk factors.
• POST- CABG EXERCISE REGIMEN
In-hospital phase• In the coronary care unit, assisted range of motion
exercises can be initiated within the first 24-48 hours.
• Low-risk patients should be encouraged to sit in a bedsidechair and begin to perform self-care activities (e.g.,shaving, oral hygiene, sponge bathing).
Post discharge phase• This phase of recovery includes low-level exercise and
physical activity and lasts for about 2-6 weeks of recovery.
Teacher:explainsLearners:Listens
Teacher:concludes thetopicLearner: listens
LCD
LCD
What is theneed forfollow upvisits afterCABGsurgery?
How long isthe usualwarm upperiod ofexerciseregimen?
123
Conclude thetopic
Supervised exercise• Exercise sessions are usually scheduled 3 times a week at the
rehabilitation facility, may last for 3-6 months.
• Type of exercise: aerobic exercises like walking, jogging,cycling, rowing, and stair climbing.
• Frequency — the recommended frequency of exercise isthree to five times a week.
• Content and duration — it is important that each sessionconsist of a 5- to 10-minute warm-up phase, a conditioningphase of at least 20 minutes, and a 5- to 10-minute cool-downphase.
• Intensity: This is based upon the patient's heart rate or thelevel of exertion.
Maintenance phase• The exercise sessions are usually scheduled 3 times a week
and are designed to continue for the patient's lifetime.
• Activities consist of the type of exercises the patient enjoys,
such as walking, bicycling, or jogging.
CONCLUSION
The immediate postoperative period for the patient who has
undergone cardiac surgery presents many challenges to the health
124
care team. The goal of postoperative care is to ensure that patients
have good outcomes after surgical procedures. A good outcome
includes recovery without complications and adequate pain
management. Periodic assessment and reporting of any deviation
or complication of the client’s health status become the sole
responsibility of critical care nurse.
BIBLIOGRAPHY
• Suzanne C, Brenda GB, Janice LH , Kerry HC. Brunner and
Suddarth's Textbook of Medical Surgical Nursing. 12th edn.
Lippincott Williams & Wilkins.
• The human heart; Available from http://www.
worldinvisible.com/apologet/humbody/ heart.htm.
• What is Coronary artery bypass graft surgery [cited Oct 2010].
Available from
http://faculty.ksu.edu.sa/albloushi/Critical%20Care%20Nursin
g%202007/CABG.pdf
• Nursing care of the client having a coronary artery bypass
graft [cited Nov 2009]. Available from
artery_bypass_graft.pdf
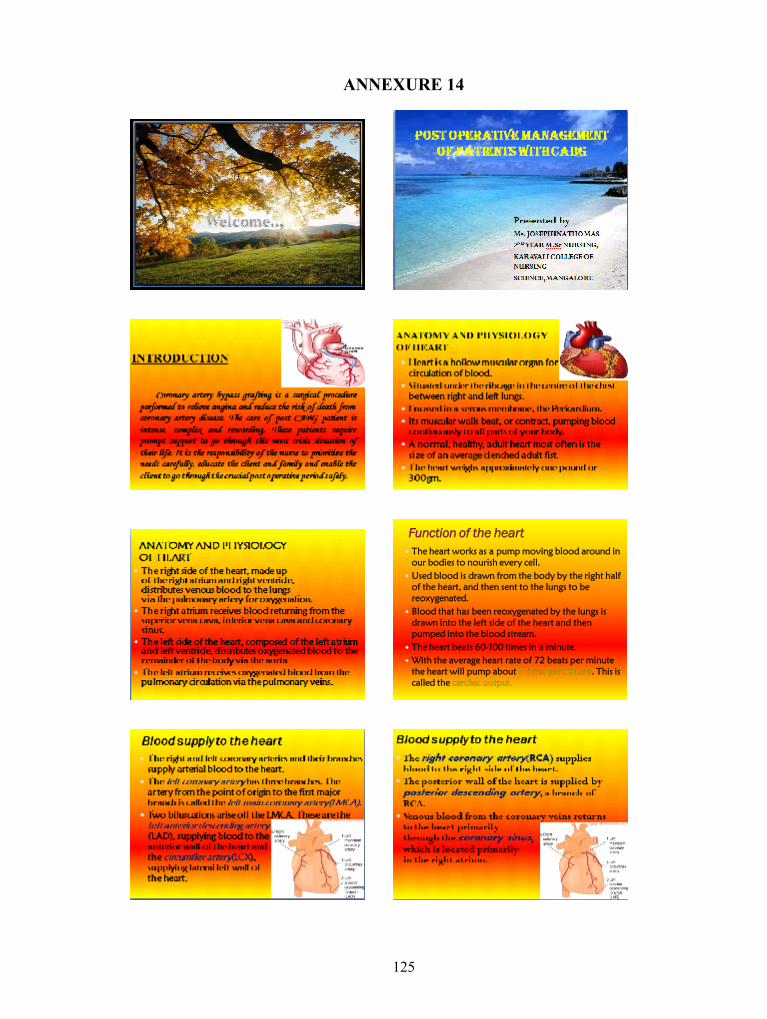
125
ANNEXURE 14
Function of the heart The heart works as a pump moving blood around in
our bodies to nourish every cell. Used blood is drawn from the body by the right half
of the heart, and then sent to the lungs to bereoxygenated.
Blood that has been reoxygenated by the lungs isdrawn into the left side of the heart and thenpumped into the blood stream.
The heart beats 60-100 times in a minute. With the average heart rate of 72 beats per minute
the heart will pump about 5 litres per minute. This iscalled the cardiac output.
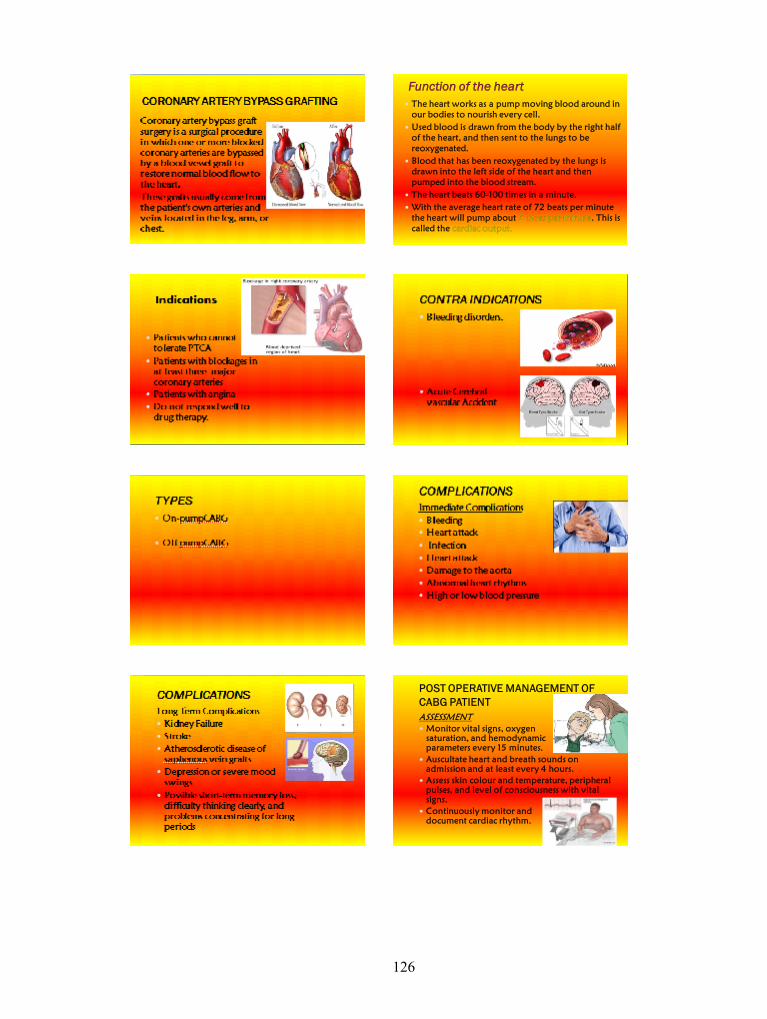
126
Function of the heart The heart works as a pump moving blood around in
our bodies to nourish every cell. Used blood is drawn from the body by the right half
of the heart, and then sent to the lungs to bereoxygenated.
Blood that has been reoxygenated by the lungs isdrawn into the left side of the heart and thenpumped into the blood stream.
The heart beats 60-100 times in a minute. With the average heart rate of 72 beats per minute
the heart will pump about 5 litres per minute. This iscalled the cardiac output.
POST OPERATIVE MANAGEMENT OFCABG PATIENTASSESSMENT Monitor vital signs, oxygen
saturation, and hemodynamicparameters every 15 minutes.
Auscultate heart and breath sounds onadmission and at least every 4 hours.
Assess skin colour and temperature, peripheralpulses, and level of consciousness with vitalsigns.
Continuously monitor anddocument cardiac rhythm.
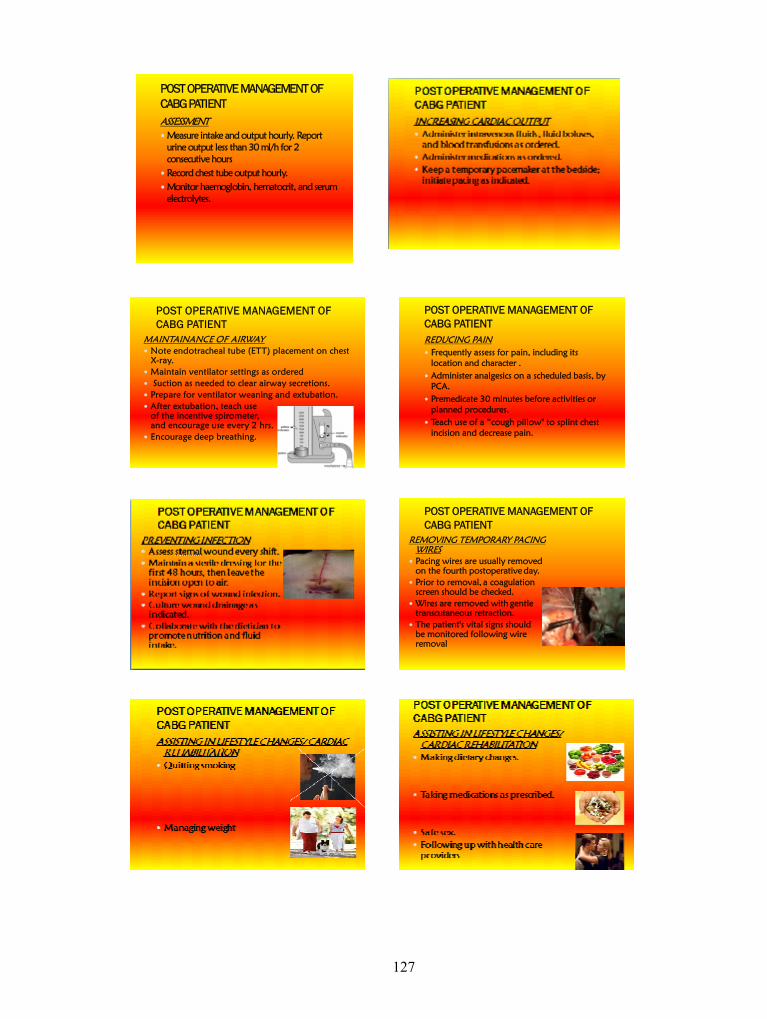
127
POST OPERATIVE MANAGEMENT OFCABG PATIENTASSESSMENT Measure intake and output hourly. Report
urine output less than 30 ml/h for 2consecutive hours
Record chest tube output hourly. Monitor haemoglobin, hematocrit, and serum
electrolytes.
POST OPERATIVE MANAGEMENT OFCABG PATIENT
MAINTAINANCE OF AIRWAY Note endotracheal tube (ETT) placement on chest
X-ray. Maintain ventilator settings as ordered Suction as needed to clear airway secretions. Prepare for ventilator weaning and extubation. After extubation, teach use
of the incentive spirometer,and encourage use every 2 hrs.
Encourage deep breathing.
POST OPERATIVE MANAGEMENT OFCABG PATIENTREDUCING PAIN Frequently assess for pain, including its
location and character . Administer analgesics on a scheduled basis, by
PCA. Premedicate 30 minutes before activities or
planned procedures. Teach use of a “cough pillow" to splint chest
incision and decrease pain.
POST OPERATIVE MANAGEMENT OFCABG PATIENT
REMOVING TEMPORARY PACINGWIRES
Pacing wires are usually removedon the fourth postoperative day.
Prior to removal, a coagulationscreen should be checked.
Wires are removed with gentletranscutaneous retraction.
The patient's vital signs shouldbe monitored following wireremoval
128
POST OPERATIVE MANAGEMENT OFCABG PATIENTPOST- CABG EXERCISE REGIMEN In-hospital phase Post discharge phase Supervised exercise Maintenance phase
129
ANNEXURE 15
List of experts who validated the tool and Structured Teaching Programme
1. Mrs. Swapna Dennis, M Sc (N)HOD- Medical Surgical NursingYenepoya College Of NursingYenepoya UniversityMangalore
2. Mrs. Latha. S.Asst. Professor and HODNitte Usha Institute of Nursing ScienceMangalore
3. Mrs. Sonia D’SouzaAsst. ProfessorFr. Muller College Of NursingMangalore
4. Mr. Gireesh. G.R.Associate ProfessorShree Devi College of NursingMangalore
5. Mrs. Vasantha GLecturerFr. Muller College Of NursingMangalore.
6. Mrs. SushmaLecturerNitte Usha Institute of Nursing ScienceMangalore
7. Mrs. Sunitha. RLecturerYenepoya Nursing CollegeMangalore.
8. Dr. Tanmay R BhutAssistant ProfessorDepartment Of MedicineK.S. Hegde HospitalMangalore
9. Dr. A.G. JayakrishnanChief cardio thoracic surgeonOmega HospitalMangalore.
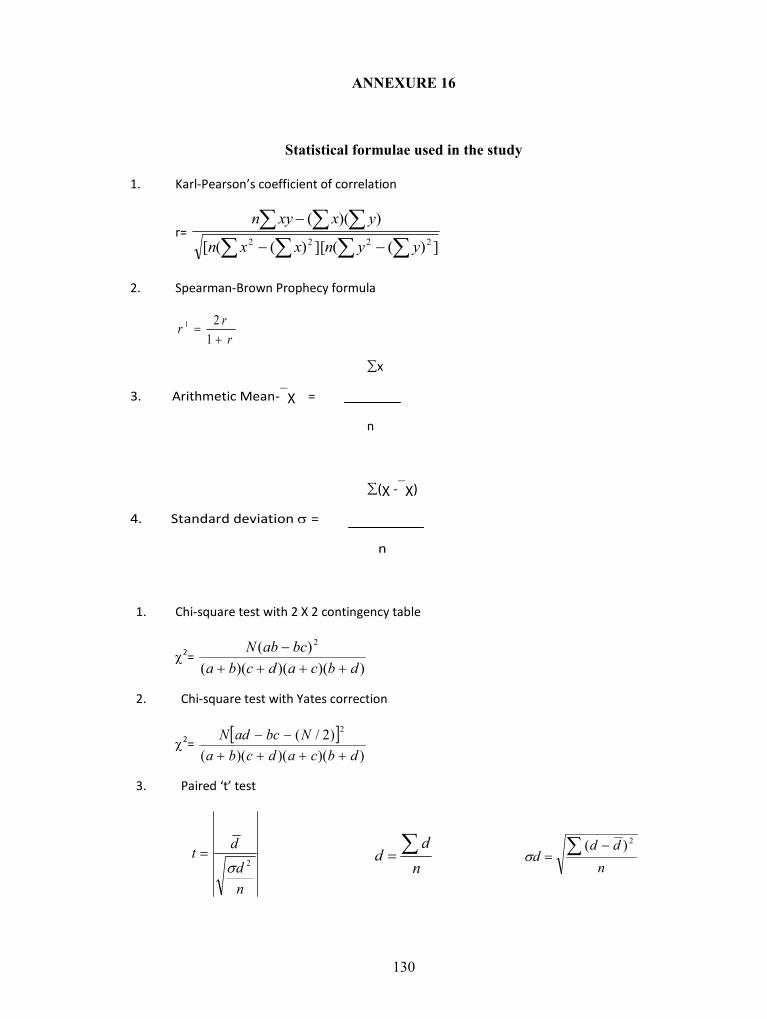
130
ANNEXURE 16
Statistical formulae used in the study
1. Karl-Pearson’s coefficient of correlation
r=
])((][)(([
))((2222 yynxxn
yxxyn
2. Spearman-Brown Prophecy formula
rrr
1
21
∑x
3. Arithmetic Mean-χ =
n
∑(χ -χ)
4. Standard deviation =
n
1. Chi-square test with 2 X 2 contingency table
2=))()()((
)( 2
dbcadcbabcabN
2. Chi-square test with Yates correction
2=
))()()(()2/( 2
dbcadcbaNbcadN
3. Paired ‘t’ test
nd
dt2
n
dd
ndd
d
2)(
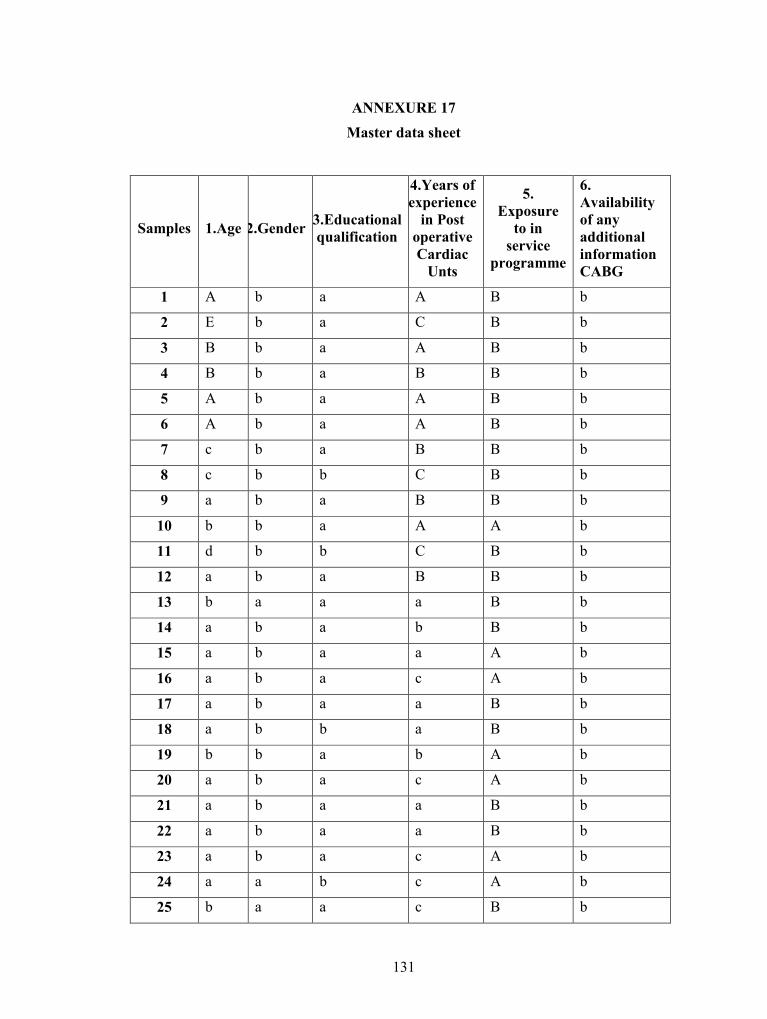
131
ANNEXURE 17Master data sheet
Samples 1.Age 2.Gender 3.Educationalqualification
4.Years ofexperience
in PostoperativeCardiac
Unts
5.Exposure
to inservice
programme
6.Availabilityof anyadditionalinformationCABG
1 A b a A B b
2 E b a C B b
3 B b a A B b
4 B b a B B b
5 A b a A B b
6 A b a A B b
7 c b a B B b
8 c b b C B b
9 a b a B B b
10 b b a A A b
11 d b b C B b
12 a b a B B b
13 b a a a B b
14 a b a b B b
15 a b a a A b
16 a b a c A b
17 a b a a B b
18 a b b a B b
19 b b a b A b
20 a b a c A b
21 a b a a B b
22 a b a a B b
23 a b a c A b
24 a a b c A b
25 b a a c B b
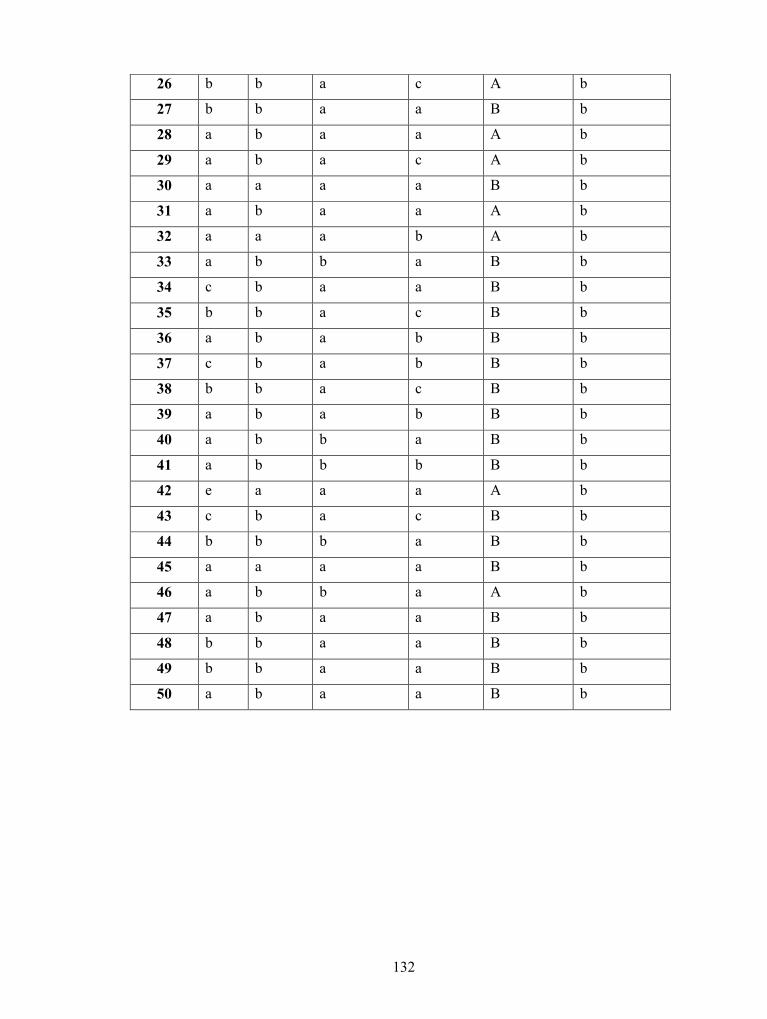
132
26 b b a c A b
27 b b a a B b
28 a b a a A b
29 a b a c A b
30 a a a a B b
31 a b a a A b
32 a a a b A b
33 a b b a B b
34 c b a a B b
35 b b a c B b
36 a b a b B b
37 c b a b B b
38 b b a c B b
39 a b a b B b
40 a b b a B b
41 a b b b B b
42 e a a a A b
43 c b a c B b
44 b b b a B b
45 a a a a B b
46 a b b a A b
47 a b a a B b
48 b b a a B b
49 b b a a B b
50 a b a a B b
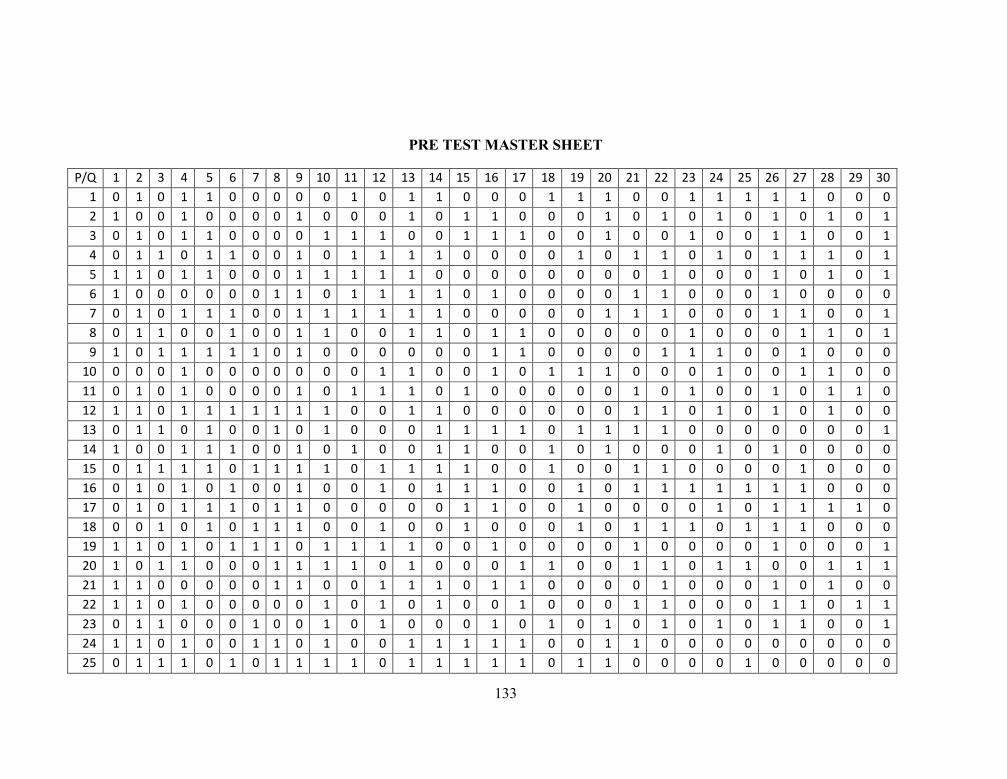
133
PRE TEST MASTER SHEET
P/Q 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 301 0 1 0 1 1 0 0 0 0 0 1 0 1 1 0 0 0 1 1 1 0 0 1 1 1 1 1 0 0 02 1 0 0 1 0 0 0 0 1 0 0 0 1 0 1 1 0 0 0 1 0 1 0 1 0 1 0 1 0 13 0 1 0 1 1 0 0 0 0 1 1 1 0 0 1 1 1 0 0 1 0 0 1 0 0 1 1 0 0 14 0 1 1 0 1 1 0 0 1 0 1 1 1 1 0 0 0 0 1 0 1 1 0 1 0 1 1 1 0 15 1 1 0 1 1 0 0 0 1 1 1 1 1 0 0 0 0 0 0 0 0 1 0 0 0 1 0 1 0 16 1 0 0 0 0 0 0 1 1 0 1 1 1 1 0 1 0 0 0 0 1 1 0 0 0 1 0 0 0 07 0 1 0 1 1 1 0 0 1 1 1 1 1 1 0 0 0 0 0 1 1 1 0 0 0 1 1 0 0 18 0 1 1 0 0 1 0 0 1 1 0 0 1 1 0 1 1 0 0 0 0 0 1 0 0 0 1 1 0 19 1 0 1 1 1 1 1 0 1 0 0 0 0 0 0 1 1 0 0 0 0 1 1 1 0 0 1 0 0 0
10 0 0 0 1 0 0 0 0 0 0 0 1 1 0 0 1 0 1 1 1 0 0 0 1 0 0 1 1 0 011 0 1 0 1 0 0 0 0 1 0 1 1 1 0 1 0 0 0 0 0 1 0 1 0 0 1 0 1 1 012 1 1 0 1 1 1 1 1 1 1 0 0 1 1 0 0 0 0 0 0 1 1 0 1 0 1 0 1 0 013 0 1 1 0 1 0 0 1 0 1 0 0 0 1 1 1 1 0 1 1 1 1 0 0 0 0 0 0 0 114 1 0 0 1 1 1 0 0 1 0 1 0 0 1 1 0 0 1 0 1 0 0 0 1 0 1 0 0 0 015 0 1 1 1 1 0 1 1 1 1 0 1 1 1 1 0 0 1 0 0 1 1 0 0 0 0 1 0 0 016 0 1 0 1 0 1 0 0 1 0 0 1 0 1 1 1 0 0 1 0 1 1 1 1 1 1 1 0 0 017 0 1 0 1 1 1 0 1 1 0 0 0 0 0 1 1 0 0 1 0 0 0 0 1 0 1 1 1 1 018 0 0 1 0 1 0 1 1 1 0 0 1 0 0 1 0 0 0 1 0 1 1 1 0 1 1 1 0 0 019 1 1 0 1 0 1 1 1 0 1 1 1 1 0 0 1 0 0 0 0 1 0 0 0 0 1 0 0 0 120 1 0 1 1 0 0 0 1 1 1 1 0 1 0 0 0 1 1 0 0 1 1 0 1 1 0 0 1 1 121 1 1 0 0 0 0 0 1 1 0 0 1 1 1 0 1 1 0 0 0 0 1 0 0 0 1 0 1 0 022 1 1 0 1 0 0 0 0 0 1 0 1 0 1 0 0 1 0 0 0 1 1 0 0 0 1 1 0 1 123 0 1 1 0 0 0 1 0 0 1 0 1 0 0 0 1 0 1 0 1 0 1 0 1 0 1 1 0 0 124 1 1 0 1 0 0 1 1 0 1 0 0 1 1 1 1 1 0 0 1 1 0 0 0 0 0 0 0 0 025 0 1 1 1 0 1 0 1 1 1 1 0 1 1 1 1 1 0 1 1 0 0 0 0 1 0 0 0 0 0

134
26 0 0 1 0 1 0 0 0 1 0 1 1 0 0 0 0 0 0 0 0 0 0 1 1 0 1 0 0 0 0
27 1 0 1 0 0 0 0 0 1 0 1 0 1 0 1 0 1 0 1 0 1 0 0 0 1 0 1 1 1 128 0 1 0 1 1 1 0 0 1 0 1 1 1 1 1 0 0 1 0 0 1 0 0 0 1 1 0 0 1 129 0 1 1 1 0 0 0 0 1 0 0 0 0 1 1 1 1 0 0 0 0 0 1 1 0 0 1 1 0 030 1 0 0 0 1 1 0 0 1 0 0 0 0 1 0 0 0 0 0 0 0 1 0 1 0 1 1 0 0 031 0 1 0 0 0 0 0 0 1 1 0 1 1 1 1 0 0 0 1 0 1 1 1 1 0 1 0 0 0 032 0 1 1 0 1 0 1 0 0 0 0 1 0 1 0 0 0 1 0 1 0 0 0 1 0 0 0 1 0 033 0 1 0 0 0 0 0 0 0 1 1 0 0 1 1 0 0 0 0 0 1 1 1 1 0 1 0 1 0 134 0 1 0 0 1 0 0 0 0 1 0 1 1 1 0 0 0 0 0 0 1 0 1 0 0 1 0 0 0 135 1 0 0 1 0 1 0 0 0 1 0 0 1 0 1 0 0 0 0 0 1 0 0 0 0 1 1 0 1 036 0 0 1 0 1 1 0 0 0 1 0 1 0 1 0 1 0 1 1 0 0 0 1 0 0 0 1 1 0 137 0 0 1 0 1 0 0 1 1 1 0 1 0 1 1 1 0 0 1 1 1 1 0 1 0 1 0 0 0 038 0 1 0 1 1 1 0 0 1 1 0 1 0 0 1 1 1 0 0 1 0 0 0 1 0 0 0 1 1 039 1 1 0 1 0 0 1 0 1 0 0 1 0 0 1 0 0 1 0 0 1 0 0 1 1 1 0 1 1 140 1 1 0 1 1 0 0 0 1 0 1 1 0 1 1 0 0 0 0 0 0 1 0 1 0 1 1 0 0 041 0 1 0 1 1 1 0 1 1 1 1 1 1 1 1 0 1 0 0 1 1 1 0 0 0 1 0 0 0 042 0 0 1 0 1 0 0 0 1 0 1 0 1 0 0 1 0 1 0 1 0 0 0 1 1 1 0 0 1 143 1 1 0 1 1 0 0 0 0 1 0 1 1 0 1 1 1 0 0 1 0 0 1 1 1 0 1 0 0 144 1 0 1 0 1 1 0 1 0 1 0 1 1 1 0 1 1 1 0 0 0 0 0 0 1 0 0 0 1 045 0 0 1 0 0 0 0 0 1 0 0 0 0 0 0 1 1 0 0 0 0 1 0 1 0 1 1 0 1 046 0 1 0 1 0 0 0 0 0 0 0 0 0 0 1 0 0 0 0 0 0 0 1 1 0 0 0 1 0 047 0 1 0 0 1 1 0 0 1 1 0 1 0 1 0 0 0 0 0 1 1 1 0 1 0 1 1 0 1 048 0 1 0 1 1 0 0 0 1 0 1 1 0 1 1 0 1 1 1 0 1 1 1 1 0 0 0 1 0 049 0 1 0 0 0 0 0 0 1 1 1 0 0 0 0 1 0 1 1 1 0 0 1 0 1 0 1 1 0 150 0 1 0 1 0 1 0 1 1 0 1 0 1 0 0 0 1 0 0 1 0 1 1 1 0 1 1 1 1 1
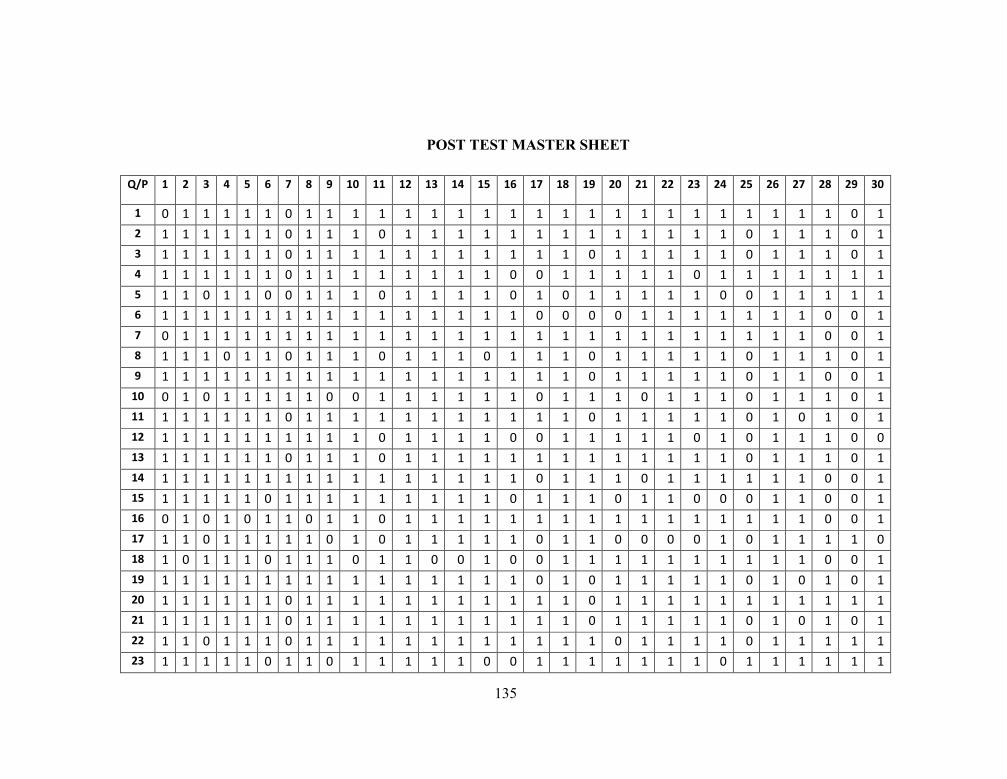
135
POST TEST MASTER SHEET
Q/P 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30
1 0 1 1 1 1 1 0 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 0 12 1 1 1 1 1 1 0 1 1 1 0 1 1 1 1 1 1 1 1 1 1 1 1 1 0 1 1 1 0 13 1 1 1 1 1 1 0 1 1 1 1 1 1 1 1 1 1 1 0 1 1 1 1 1 0 1 1 1 0 14 1 1 1 1 1 1 0 1 1 1 1 1 1 1 1 0 0 1 1 1 1 1 0 1 1 1 1 1 1 15 1 1 0 1 1 0 0 1 1 1 0 1 1 1 1 0 1 0 1 1 1 1 1 0 0 1 1 1 1 16 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 0 0 0 0 1 1 1 1 1 1 1 0 0 17 0 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 0 0 18 1 1 1 0 1 1 0 1 1 1 0 1 1 1 0 1 1 1 0 1 1 1 1 1 0 1 1 1 0 19 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 0 1 1 1 1 1 0 1 1 0 0 1
10 0 1 0 1 1 1 1 1 0 0 1 1 1 1 1 1 0 1 1 1 0 1 1 1 0 1 1 1 0 111 1 1 1 1 1 1 0 1 1 1 1 1 1 1 1 1 1 1 0 1 1 1 1 1 0 1 0 1 0 112 1 1 1 1 1 1 1 1 1 1 0 1 1 1 1 0 0 1 1 1 1 1 0 1 0 1 1 1 0 013 1 1 1 1 1 1 0 1 1 1 0 1 1 1 1 1 1 1 1 1 1 1 1 1 0 1 1 1 0 114 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 0 1 1 1 0 1 1 1 1 1 1 0 0 115 1 1 1 1 1 0 1 1 1 1 1 1 1 1 1 0 1 1 1 0 1 1 0 0 0 1 1 0 0 116 0 1 0 1 0 1 1 0 1 1 0 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 0 0 117 1 1 0 1 1 1 1 1 0 1 0 1 1 1 1 1 0 1 1 0 0 0 0 1 0 1 1 1 1 018 1 0 1 1 1 0 1 1 1 0 1 1 0 0 1 0 0 1 1 1 1 1 1 1 1 1 1 0 0 119 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 0 1 0 1 1 1 1 1 0 1 0 1 0 120 1 1 1 1 1 1 0 1 1 1 1 1 1 1 1 1 1 1 0 1 1 1 1 1 1 1 1 1 1 121 1 1 1 1 1 1 0 1 1 1 1 1 1 1 1 1 1 1 0 1 1 1 1 1 0 1 0 1 0 122 1 1 0 1 1 1 0 1 1 1 1 1 1 1 1 1 1 1 1 0 1 1 1 1 0 1 1 1 1 123 1 1 1 1 1 0 1 1 0 1 1 1 1 1 0 0 1 1 1 1 1 1 1 0 1 1 1 1 1 1
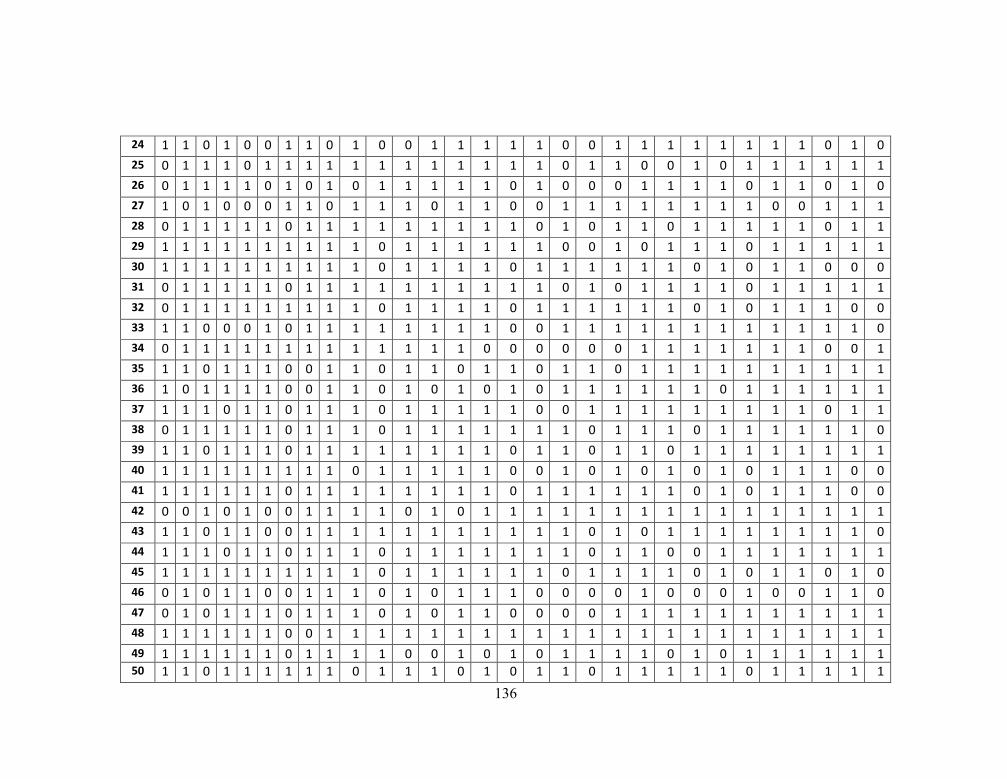
136
24 1 1 0 1 0 0 1 1 0 1 0 0 1 1 1 1 1 0 0 1 1 1 1 1 1 1 1 0 1 025 0 1 1 1 0 1 1 1 1 1 1 1 1 1 1 1 1 0 1 1 0 0 1 0 1 1 1 1 1 126 0 1 1 1 1 0 1 0 1 0 1 1 1 1 1 0 1 0 0 0 1 1 1 1 0 1 1 0 1 027 1 0 1 0 0 0 1 1 0 1 1 1 0 1 1 0 0 1 1 1 1 1 1 1 1 0 0 1 1 128 0 1 1 1 1 1 0 1 1 1 1 1 1 1 1 1 0 1 0 1 1 0 1 1 1 1 1 0 1 129 1 1 1 1 1 1 1 1 1 1 0 1 1 1 1 1 1 0 0 1 0 1 1 1 0 1 1 1 1 130 1 1 1 1 1 1 1 1 1 1 0 1 1 1 1 0 1 1 1 1 1 1 0 1 0 1 1 0 0 031 0 1 1 1 1 1 0 1 1 1 1 1 1 1 1 1 1 0 1 0 1 1 1 1 0 1 1 1 1 132 0 1 1 1 1 1 1 1 1 1 0 1 1 1 1 0 1 1 1 1 1 1 0 1 0 1 1 1 0 033 1 1 0 0 0 1 0 1 1 1 1 1 1 1 1 0 0 1 1 1 1 1 1 1 1 1 1 1 1 034 0 1 1 1 1 1 1 1 1 1 1 1 1 1 0 0 0 0 0 0 1 1 1 1 1 1 1 0 0 135 1 1 0 1 1 1 0 0 1 1 0 1 1 0 1 1 0 1 1 0 1 1 1 1 1 1 1 1 1 136 1 0 1 1 1 1 0 0 1 1 0 1 0 1 0 1 0 1 1 1 1 1 1 0 1 1 1 1 1 137 1 1 1 0 1 1 0 1 1 1 0 1 1 1 1 1 0 0 1 1 1 1 1 1 1 1 1 0 1 138 0 1 1 1 1 1 0 1 1 1 0 1 1 1 1 1 1 1 0 1 1 1 0 1 1 1 1 1 1 039 1 1 0 1 1 1 0 1 1 1 1 1 1 1 1 0 1 1 0 1 1 0 1 1 1 1 1 1 1 140 1 1 1 1 1 1 1 1 1 0 1 1 1 1 1 0 0 1 0 1 0 1 0 1 0 1 1 1 0 041 1 1 1 1 1 1 0 1 1 1 1 1 1 1 1 0 1 1 1 1 1 1 0 1 0 1 1 1 0 042 0 0 1 0 1 0 0 1 1 1 1 0 1 0 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 143 1 1 0 1 1 0 0 1 1 1 1 1 1 1 1 1 1 1 0 1 0 1 1 1 1 1 1 1 1 044 1 1 1 0 1 1 0 1 1 1 0 1 1 1 1 1 1 1 0 1 1 0 0 1 1 1 1 1 1 145 1 1 1 1 1 1 1 1 1 1 0 1 1 1 1 1 1 0 1 1 1 1 0 1 0 1 1 0 1 046 0 1 0 1 1 0 0 1 1 1 0 1 0 1 1 1 0 0 0 0 1 0 0 0 1 0 0 1 1 047 0 1 0 1 1 1 0 1 1 1 0 1 0 1 1 0 0 0 0 1 1 1 1 1 1 1 1 1 1 148 1 1 1 1 1 1 0 0 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 149 1 1 1 1 1 1 0 1 1 1 1 0 0 1 0 1 0 1 1 1 1 0 1 0 1 1 1 1 1 150 1 1 0 1 1 1 1 1 1 0 1 1 1 0 1 0 1 1 0 1 1 1 1 1 0 1 1 1 1 1
Related Documents











