Effectiveness of bisphosphonate therapy in a community setting ☆ Adrianne C. Feldstein a,b, ⁎, Derek Weycker c , Gregory A. Nichols a , Gerry Oster c , Gabriela Rosales a , David L. Boardman b , Nancy Perrin a a Center for Health Research, Kaiser Permanente Northwest, Portland OR, USA b Northwest Permanente, Portland, OR, USA c Policy Analysis, Inc. (PAI), Brookline, Massachusetts, USA abstract article info Article history: Received 4 March 2008 Revised 25 July 2008 Accepted 5 September 2008 Available online 26 September 2008 Edited by: M. McClung Keywords: Post-menopausal osteoporosis Bisphosphonate Fracture risk Background: Osteoporosis is a major cause of morbidity and mortality. Clinical trials have shown the effectiveness of bisphosphonates, the most commonly prescribed treatments, in reducing fracture risk. The population-based effectiveness of bisphosphonates in clinical practice is uncertain. Methods: This retrospective cohort study used a matched design that compared time to clinical fracture in at- risk community women who initiated a bisphosphonate medication between 7/1/1996 and 6/30/2006 to those who did not. The study was conducted in an HMO in Oregon and Washington. Clinical electronic databases provided data. Eligible members were newly treated women aged ≥ 55 years with either a BMD T- score of ≤− 2.0 or a prior qualifying clinical fracture. They did not have contraindications for bisphosphonate therapy or a diagnosis associated with secondary osteoporosis (n =1829). They were matched to a similar comparison group (n =1829; total N = 3658). The primary outcome was the first new incident fracture validated through chart review (closed clinical fracture of any bone except face, skull, finger, or toe or pathological fracture secondary to malignancy) during follow-up. An intention-to-treat analysis used Cox proportional hazards models to estimate the hazard ratio of fracture for treated relative to comparison patients, adjusting for differences in potential confounders. Results: Treated and comparison patients were similar in mean age (72.0 years) and history of fracture (about 45%). The treated group had more women with T-scores of ≤− 2.5 (67.3% vs. 54.7%) and a lower mean weight (146.6 lb vs.151.8 lb). Only about 45% of treated patients had a bisphosphonate medication possession ratio (MPR) of ≥ 0.80. During follow-up, 198 (10.8%) of patients in the treated group had incident fractures, vs.179 (9.8%) of patients in the comparison group. After adjustments, patients in the treated group were 0.91 (95% CI 0.74–1.13) as likely to have an incident fracture as the comparison patients (p = 0.388). The treatment effect remained non-significant after accounting for MPR. Conclusions: In this analysis of a community cohort of post-menopausal women at risk, the fracture risk of patients who received bisphosphonates did not differ significantly from those who did not. An enhanced understanding of this lack of treatment effect is urgently needed. © 2008 Elsevier Inc. All rights reserved. Introduction Osteoporosis is a major cause of morbidity and mortality and is of growing importance as the population ages [1,2]. Osteoporosis is estimated to have resulted in more than 2 million new fractures in the United States in 2005, at a cost of $17 billion. By 2025, annual fractures and costs are projected to increase by more than 50% [2]. In women, the mortality rate from osteoporotic fractures is higher than that of breast and ovarian cancers combined [3]. In controlled clinical trials, anti-resorptive medications and parathyroid hormone derivatives have been shown to reduce risk of fracture by 12–65% in persons with osteoporosis, depending upon the specific population and agent studied [4]. Bisphosphonates, the most commonly prescribed treatments for osteoporosis, reduce the risk of vertebral and non-vertebral fractures in women with pre-existing vertebral fractures and low bone mineral density (BMD) [5], in those with BMD-confirmed osteoporosis [6–8], and in those with a prior hip fracture [9]. The advent of bisphosphonates markedly improved treatment options for patients at risk for osteoporotic fractures. However, the oral bisphosphonates are complex for patients to take and often result in gastrointestinal intolerability; adherence and persistence have been low outside of the clinical trial setting [10]. Observational studies of osteoporosis medications have reported 1–2 year persistence rates of below 25% [11–13] and adherence to therapy (medication possession Bone 44 (2009) 153–159 ☆ This project was supported by Policy Analysis Inc. (PAI) through a research contract with Amgen. ⁎ Corresponding author. Center for Health Research, Kaiser Permanente, 3800 N Interstate Avenue, Portland OR 97227, USA. Fax: +1503 335 6311. E-mail address: [email protected] (A.C. Feldstein). 8756-3282/$ – see front matter © 2008 Elsevier Inc. All rights reserved. doi:10.1016/j.bone.2008.09.006 Contents lists available at ScienceDirect Bone journal homepage: www.elsevier.com/locate/bone

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Bone 44 (2009) 153–159
Contents lists available at ScienceDirect
Bone
j ourna l homepage: www.e lsev ie r.com/ locate /bone
Effectiveness of bisphosphonate therapy in a community setting☆
Adrianne C. Feldstein a,b,⁎, Derek Weycker c, Gregory A. Nichols a, Gerry Oster c,Gabriela Rosales a, David L. Boardman b, Nancy Perrin a
a Center for Health Research, Kaiser Permanente Northwest, Portland OR, USAb Northwest Permanente, Portland, OR, USAc Policy Analysis, Inc. (PAI), Brookline, Massachusetts, USA
☆ This project was supported by Policy Analysis Inc. (Pwith Amgen.⁎ Corresponding author. Center for Health Research
Interstate Avenue, Portland OR 97227, USA. Fax: +1 503E-mail address: [email protected] (A.C
8756-3282/$ – see front matter © 2008 Elsevier Inc. Aldoi:10.1016/j.bone.2008.09.006
a b s t r a c t
a r t i c l e i n f oArticle history:
Background: Osteoporosis Received 4 March 2008Revised 25 July 2008Accepted 5 September 2008Available online 26 September 2008Edited by: M. McClung
Keywords:Post-menopausal osteoporosisBisphosphonateFracture risk
is a major cause of morbidity and mortality. Clinical trials have shown theeffectiveness of bisphosphonates, the most commonly prescribed treatments, in reducing fracture risk. Thepopulation-based effectiveness of bisphosphonates in clinical practice is uncertain.Methods: This retrospective cohort study used a matched design that compared time to clinical fracture in at-risk community women who initiated a bisphosphonate medication between 7/1/1996 and 6/30/2006 tothose who did not. The study was conducted in an HMO in Oregon and Washington. Clinical electronicdatabases provided data. Eligible members were newly treated women aged ≥55 years with either a BMD T-score of ≤−2.0 or a prior qualifying clinical fracture. They did not have contraindications for bisphosphonatetherapy or a diagnosis associated with secondary osteoporosis (n=1829). They were matched to a similarcomparison group (n=1829; total N=3658). The primary outcome was the first new incident fracturevalidated through chart review (closed clinical fracture of any bone except face, skull, finger, or toe orpathological fracture secondary to malignancy) during follow-up. An intention-to-treat analysis used Coxproportional hazards models to estimate the hazard ratio of fracture for treated relative to comparisonpatients, adjusting for differences in potential confounders.Results: Treated and comparison patients were similar in mean age (72.0 years) and history of fracture (about45%). The treated group had more women with T-scores of ≤−2.5 (67.3% vs. 54.7%) and a lower mean weight(146.6 lb vs. 151.8 lb). Only about 45% of treated patients had a bisphosphonate medication possession ratio(MPR) of ≥0.80. During follow-up, 198 (10.8%) of patients in the treated group had incident fractures, vs. 179(9.8%) of patients in the comparison group. After adjustments, patients in the treated group were 0.91 (95% CI0.74–1.13) as likely to have an incident fracture as the comparison patients (p=0.388). The treatment effectremained non-significant after accounting for MPR.Conclusions: In this analysis of a community cohort of post-menopausal women at risk, the fracture risk ofpatients who received bisphosphonates did not differ significantly from those who did not. An enhancedunderstanding of this lack of treatment effect is urgently needed.
© 2008 Elsevier Inc. All rights reserved.
Introduction
Osteoporosis is a major cause of morbidity and mortality and is ofgrowing importance as the population ages [1,2]. Osteoporosis isestimated to have resulted in more than 2 million new fractures in theUnited States in 2005, at a cost of $17 billion. By 2025, annual fracturesand costs are projected to increase by more than 50% [2]. In women,the mortality rate from osteoporotic fractures is higher than that ofbreast and ovarian cancers combined [3].
AI) through a research contract
, Kaiser Permanente, 3800 N335 6311.. Feldstein).
l rights reserved.
In controlled clinical trials, anti-resorptive medications andparathyroid hormone derivatives have been shown to reduce risk offracture by 12–65% in persons with osteoporosis, depending upon thespecific population and agent studied [4]. Bisphosphonates, the mostcommonly prescribed treatments for osteoporosis, reduce the risk ofvertebral and non-vertebral fractures in women with pre-existingvertebral fractures and low bone mineral density (BMD) [5], in thosewith BMD-confirmed osteoporosis [6–8], and in those with a prior hipfracture [9].
The advent of bisphosphonates markedly improved treatmentoptions for patients at risk for osteoporotic fractures. However, theoral bisphosphonates are complex for patients to take and often resultin gastrointestinal intolerability; adherence and persistence have beenlow outside of the clinical trial setting [10]. Observational studies ofosteoporosis medications have reported 1–2 year persistence rates ofbelow 25% [11–13] and adherence to therapy (medication possession

Fig. 1. Study population flow. HMO members eligible for the study were newly treatedwomen aged N55 years with a BMD T-score of b−2.0 or a prior qualifying clinicalfracture, without contraindications for bisphosphonate therapy or a diagnosisassociated with secondary osteoporosis (n=1829). They were matched to a similarcomparison group (n=1829; total N=3658).
154 A.C. Feldstein et al. / Bone 44 (2009) 153–159
ratio (MRP) ≥80%) of 25–45% [12–15]. Studies from administrativedatabases have also reported that reduced adherence results indiminished fracture reduction efficacy [11,12,14,16,17].
These prior studies were limited by their combined evaluation ofmultiple types of osteoporosis medications; the use of administrativedata and minimal access to clinical information, such as BMD andweight; and resulting inability to compare fracture risk in bispho-sphonate-treated and untreated patients. Given the adherence andlowered efficacy concerns raised by other observational studies[11,12,14,16,17], the effectiveness of bisphosphonates in clinicalpractice may be less than that reported in randomized controlledtrials. We used electronic medical record data from a large group-model health maintenance organization (HMO) and chart reviewvalidation of fracture outcomes to examine the effectiveness ofbisphosphonate therapy in reducing the risk of fractures in at-riskpost-menopausal women.
Methods
Study design overview
Thiswas a retrospective cohort study that used amatched design tocompare risk of clinical fracture in at-riskwomen (thosewith lowBMDor a prior fracture) who had received a bisphosphonate medication(the treated group) to those who did not (the comparison group). Thestudy period was 7/1/1995 through 12/31/2006, and the patientaccrual periodwas 7/1/1996 through 6/30/2006. The primary outcomewas the incidence of a new closed clinical fracture of any bone exceptface, skull, finger, or toe or pathological fracture from a neoplasm. Anintention-to-treat analysis used Cox proportional hazards models toestimate the hazard ratio of fracture for treated relative to comparisonpatients, adjusting for differences in potential confounders.
The study design and procedures were approved by the studyHMO's Institutional Review Board. The need for informed consent waswaived.
Study site and data sources
The study was conducted in a not-for-profit group-model HMOwith about 480,000 members in Oregon and Washington. Planmembers are similar in age, sex, ethnicity, and economic status tothe overall local community [18]. The HMO has used an electronicmedical record since 1996. Comprehensive electronic databases storepatient demographics, weight and height, inpatient and outpatientICD-9 clinician-documented encounter and problem list diagnoses,outside claims and referrals, BMD screening results, radiology reports,and dispensed medications. Patient records are linked through theunique health record number of each HMO member. All BMDmeasures are performed using dual energy X-ray absorptiometry(DXA) by a single diagnostic center under contract with the HMO [19].Measurements include BMD of the hip (femoral neck and total) andlumbar spine (L1–L4). DXA was performed on a Lunar DPX-L (GEMedical Systems, MadisonWI) until April 1999 and on a Lunar ProdigyDXA (GE Medical Systems, Madison WI) after that time. The HMOdatabases capture over 95% of the medical care and pharmacy servicesmembers receive [18].
The HMO has had internal clinical practice guidelines for theprevention and management of post-menopausal osteoporosis since1998. Pharmacologic treatment was recommended for women withclear clinical osteoporosis, those with a T-score of b−2.5, and thosewith a T-score between −2.0 and −2.5 and two or more additional riskfactors. Treatment recommendations were consistent with prevailingnational guidelines, with estrogen removed as a recommended first-line treatment option in August 2002. Reflecting trends in thecommunity, DXA screening and treatment became more frequent inthe last several years of the study period.
Source population
Fig. 1 reveals the study design and participant flow. We aimed toidentify a source population of women with a probable indication forosteoporosis medication treatment (for post-menopausal osteopeniaor osteoporosis) and no absolute contraindication to bisphosphonatemedication use [20]. Thus, we identified women aged 55 years andolder who had evidence of at least one of two qualifying “clinicalindications”: low BMD (a T-score of ≤−2.0 at lumbar spine or hip[femoral neck or total hip]) or a prior clinical fracture (any closedfracture, except a pathologic fracture from neoplasm and those of thefingers, toes, skull, and face [ICD-9 codes available upon request]) from7/1/96 through 6/30/2006 (n=20,593). We excluded 3352 patients(16.3%) with one or more of the following in the 12 months beforetheir clinical indication: 1) conditions or medication use associatedwith secondary osteoporosis or osteomalacia [21,22] (hyperthyroid-ism, n=115; hyperparathyroidism, n=71; Cushings disease, n=17;chronic kidney disease, n=416; malabsorption or malnutrition,n=189; vitamin D deficiency, n=37; “chronic” glucocorticosteroiduse [dispense/s of more than a 90-day supply], n=14; any dispense ofthe anti-convulsant medications phenobarbital, phenytoin, or carba-mazepine, n=483); 2) other bone conditions treated with bispho-sphonates (Paget's disease, n=11); 3) risk indicators for pathologicfractures from malignancy (malignant neoplasms except for non-melanoma skin malignancy, n=1912); and 4) contraindications forbisphosphonate use (diagnoses of peptic or esophageal ulcers or

155A.C. Feldstein et al. / Bone 44 (2009) 153–159
strictures, n=424) in the one year prior to their clinical indication.After those exclusions, n=17,241.
Sequential matching
Beginning with the first month of the patient accrual period, weidentified “treated patients”—women in the source population whoinitiated bisphosphonate therapy in that month and had a qualifyingclinical indication in the prior six-month period. Bisphosphonatesincluded oral alendronate sodium, risedronate sodium, and ibandro-nate sodium. The date of the first dispense of bisphosphonate therapywas designated as the “index date” for each patient. We limited thegroup to those who had 12 months of HMO membership including adrug benefit prior to the index date and excluded those who had anyprior (back to 1995) dispenses of bisphosphonates or other osteo-porosis medications (calcitonin, estrogen, selective estrogen receptormodulator, and teriparatide) during the prior 12 months (N=2120).
We grouped those with prior fractures into “higher risk” forosteoporosis (fractures of the vertebra, hip, pelvis, humerus or wrist)or “lower risk” (all remaining fractures) [23]. On a monthly basis, wematched each treated patient to awoman similar in age and qualifyingclinical indication in the preceding six months. These “comparisonpatients” did not initiate bisphosphonate therapy in that month or thenext 6 months (although they may have subsequently) and met thesame eligibility criteria (membership and prior medication history) astheir matched treated patient. Eligible comparison patients were theclosest in age within 5 years and had the same qualifying clinicalindication in the prior 6 months as treated patients: either low BMD(closest match within T-score of 0.25 at the same site) or clinicalfracture group (high or low risk).
Each comparison patient was assigned the same index date as theintervention patient to whom she was matched. Once matched, theintervention patient and the comparison patient were removed fromthe source population, and the same process was repeated for eachsubsequent calendarmonth of the patient accrual period.Wematched1829 treated patients to 1829 comparison patients; total studyN=3658.
Follow-up began on the day after the index date and ended on thedate of fracture, disenrollment from the HMO, death, or December 31,2006 (the end of the study period), whichever occurred first. In thecase of the comparison group, we also included the date of first receiptof any bisphosphonate medication as a censoring criterion.
Primary outcome and covariates
The primary outcome was incidence during follow-up of a newclosed clinical fracture that has been associated with osteoporosis[23]—i.e., a closed clinical fracture of any bone except face, skull,finger, or toe or pathological fractures secondary to malignancy.Qualifying fractures were extracted from electronic records based onencounter diagnoses and were considered as possible new incidentfractures if there was no recorded fracture of that body part in theprior 6 months. Qualifying fractures were reviewed by an expertchart reviewer blinded to patient treatment status. Only thosefractures that were validated as new qualifying fractures through aconfirmatory radiology report or orthopedic specialist review wereincluded in the analyses.
Explanatory variables included age and other factors associatedwith fracture risk (osteoporosis and falls), overall medication/diseaseburden, other factors that could be associated with the likelihood ofreceipt of bisphosphonate therapy, and measures of adherence. Agewas assessed at the index date. Osteoporosis risk-related measuresincluded 1) the BMD T-score and stratum (based upon the lowestmeasure at any site from the most recent measurement during the24months prior to index); 2) prior fracture (any recorded in a problemlist or encounter diagnosis in the 12 months prior to index); 3)
hypothyroidism (in the 12months prior to index); 4) diabetes mellitus(in the 12 months prior to index) 5) weight (continuous), weightb127 lb, and body mass index (BMI) in kg/m2 using the most recentweight in the 12 months prior to index and any available height; 6)current smoking (any indicator in the 12 months prior to index) 7)thiazolidinedione, 8) proton pump inhibitor and 9) selective serotoninreuptake inhibitors dispense in the 12 months prior to index [20,24–27]. Conditions or medications associated with the risk of falls [28]included osteoarthritis, rheumatoid arthritis, Parkinson's disease,Alzheimer's disease and other dementias (based upon a problem listor encounter diagnosis in the 12 months prior to index), and anydispense of longer-acting benzodiazepines (chlordiazepoxide, clora-zepate, diazepam, flurazepam, triazolam) or tertiary tricyclic anti-depressants (amitriptyline, imipramine, doxepin) [28] during the12 months prior to index.
Factors that may be associated with a reduced likelihood of receiptof bisphosphonate therapy included esophageal and peptic disorders(except for peptic or esophageal ulcers or strictures that served asstudy exclusions), which we ascertained based upon a problem list orencounter diagnosis in the 12 months prior to index. As a measure ofpatient medication and disease burden [29], we determined the meannumber of unique generic drugs (exclusive of the bisphosphonates)dispensed for each participant during the 12-month pre-period.
As a measure of medication adherence, we calculated the bispho-sphonatemedication possession ratio for treated patients by summingthe days of medication dispensed during follow-up divided by theduration of follow-up in days. We stratified the bisphosphonate MPRinto b20%, 20%–39%, 40%–59%, 60%–79%, ≥80% and additionally into≥80% and b80% of covered days. The proportion of treated andcomparison patients with any dispense and number of therapy dayswith other non-bisphosphonate osteoporosis drug therapy (estrogen,calcitonin, raloxifene) were ascertained beginning on the day of firstdispense for the corresponding drug through the end of follow-up.
Statistical analysis
We compared baseline characteristics of the treated and compar-ison patients using the Wilcoxon signed rank test for continuousvariables and McNemar's test for categorical variables.
The primary analysis employed intention-to-treat principles andincluded all matched treated (regardless of duration of bispho-sphonate therapy) and comparison patients. We used a Cox propor-tional hazards model (SAS/9.1, SAS Institute, Cary NC) to estimate therelative hazard of fracture for intervention patients vs. comparisonpatients, adjusting for differences in potential confounders. Weexamined whether treated patients who were adherent with bispho-sphonate therapy were less likely to fracture than those whowere notadherent to therapy by including a term for bisphosphonate MPR(≥80%, vs. the referent b80%). All covariates (except BMD which wasavailable in only 62.1%) were retained in the final model. We assessedthe impact on results of accounting for matching in the Coxproportional hazards model by employing a stratified analyticapproach (i.e., stratified analysis by matched pair) and by includinga variable identifying each matched pair. We ran several additionalmodels: one that did not censor for the initiation of bisphosphonatesin the comparison group; another that censored treated andcomparison patients on the date of initiation of any other osteoporosisdrug therapy during follow-up; one that limited the study populationto those with a BMD T-score of ≤−2.5 or a prior high-risk fracture andone that included only those patients who had a BMD and thatcontrolled for prior high-risk fracture and BMD T-score (as acontinuous measure). All statistical tests were two-sided and wereperformed at a significance level of α=0.05.
Using retrospective data and data from clinical trials of bispho-sphonates [5,6] we estimated that with an annual risk of fracture inthe comparison group of 4.0%, a mean duration of follow-up of 4 years,
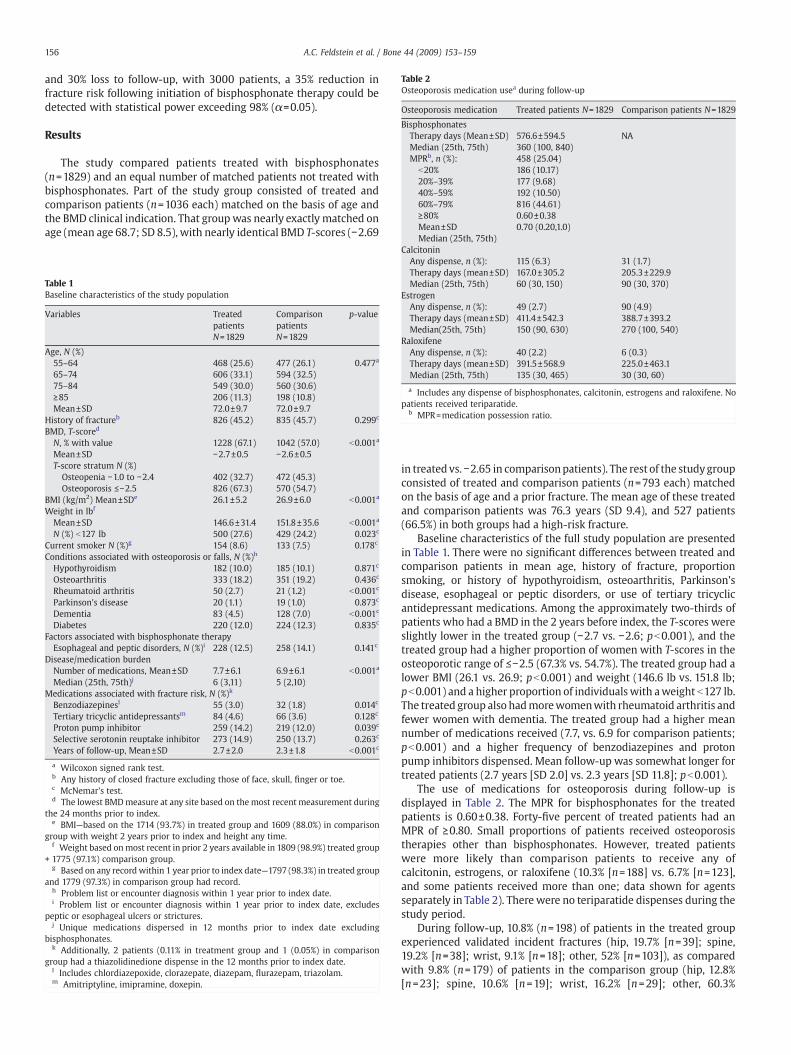
Table 2Osteoporosis medication usea during follow-up
Osteoporosis medication Treated patients N=1829 Comparison patients N=1829
BisphosphonatesTherapy days (Mean±SD) 576.6±594.5 NAMedian (25th, 75th) 360 (100, 840)MPRb, n (%): 458 (25.04)
b20% 186 (10.17)20%–39% 177 (9.68)40%–59% 192 (10.50)60%–79% 816 (44.61)≥80% 0.60±0.38Mean±SD 0.70 (0.20,1.0)Median (25th, 75th)
156 A.C. Feldstein et al. / Bone 44 (2009) 153–159
and 30% loss to follow-up, with 3000 patients, a 35% reduction infracture risk following initiation of bisphosphonate therapy could bedetected with statistical power exceeding 98% (α=0.05).
Results
The study compared patients treated with bisphosphonates(n=1829) and an equal number of matched patients not treated withbisphosphonates. Part of the study group consisted of treated andcomparison patients (n=1036 each) matched on the basis of age andthe BMD clinical indication. That group was nearly exactly matched onage (mean age 68.7; SD 8.5), with nearly identical BMD T-scores (−2.69
Table 1Baseline characteristics of the study population
Variables TreatedpatientsN=1829
ComparisonpatientsN=1829
p-value
Age, N (%)55–64 468 (25.6) 477 (26.1) 0.477a
65–74 606 (33.1) 594 (32.5)75–84 549 (30.0) 560 (30.6)≥85 206 (11.3) 198 (10.8)Mean±SD 72.0±9.7 72.0±9.7
History of fractureb 826 (45.2) 835 (45.7) 0.299c
BMD, T-scored
N, % with value 1228 (67.1) 1042 (57.0) b0.001a
Mean±SD −2.7±0.5 −2.6±0.5T-score stratum N (%)
Osteopenia −1.0 to −2.4 402 (32.7) 472 (45.3)Osteoporosis ≤−2.5 826 (67.3) 570 (54.7)
BMI (kg/m2) Mean±SDe 26.1±5.2 26.9±6.0 b0.001a
Weight in lbf
Mean±SD 146.6±31.4 151.8±35.6 b0.001a
N (%) b127 lb 500 (27.6) 429 (24.2) 0.023c
Current smoker N (%)g 154 (8.6) 133 (7.5) 0.178c
Conditions associated with osteoporosis or falls, N (%)h
Hypothyroidism 182 (10.0) 185 (10.1) 0.871c
Osteoarthritis 333 (18.2) 351 (19.2) 0.436c
Rheumatoid arthritis 50 (2.7) 21 (1.2) b0.001c
Parkinson's disease 20 (1.1) 19 (1.0) 0.873c
Dementia 83 (4.5) 128 (7.0) b0.001c
Diabetes 220 (12.0) 224 (12.3) 0.835c
Factors associated with bisphosphonate therapyEsophageal and peptic disorders, N (%)i 228 (12.5) 258 (14.1) 0.141c
Disease/medication burdenNumber of medications, Mean±SD 7.7±6.1 6.9±6.1 b0.001a
Median (25th, 75th)j 6 (3,11) 5 (2,10)Medications associated with fracture risk, N (%)k
Benzodiazepinesl 55 (3.0) 32 (1.8) 0.014c
Tertiary tricyclic antidepressantsm 84 (4.6) 66 (3.6) 0.128c
Proton pump inhibitor 259 (14.2) 219 (12.0) 0.039c
Selective serotonin reuptake inhibitor 273 (14.9) 250 (13.7) 0.263c
Years of follow-up, Mean±SD 2.7±2.0 2.3±1.8 b0.001c
a Wilcoxon signed rank test.b Any history of closed fracture excluding those of face, skull, finger or toe.c McNemar's test.d The lowest BMDmeasure at any site based on the most recent measurement during
the 24 months prior to index.e BMI—based on the 1714 (93.7%) in treated group and 1609 (88.0%) in comparison
group with weight 2 years prior to index and height any time.f Weight based onmost recent in prior 2 years available in 1809 (98.9%) treated group
+ 1775 (97.1%) comparison group.g Based on any recordwithin 1 year prior to index date—1797 (98.3%) in treated group
and 1779 (97.3%) in comparison group had record.h Problem list or encounter diagnosis within 1 year prior to index date.i Problem list or encounter diagnosis within 1 year prior to index date, excludes
peptic or esophageal ulcers or strictures.j Unique medications dispersed in 12 months prior to index date excluding
bisphosphonates.k Additionally, 2 patients (0.11% in treatment group and 1 (0.05%) in comparison
group had a thiazolidinedione dispense in the 12 months prior to index date.l Includes chlordiazepoxide, clorazepate, diazepam, flurazepam, triazolam.m Amitriptyline, imipramine, doxepin.
CalcitoninAny dispense, n (%): 115 (6.3) 31 (1.7)Therapy days (mean±SD) 167.0±305.2 205.3±229.9Median (25th, 75th) 60 (30, 150) 90 (30, 370)
EstrogenAny dispense, n (%): 49 (2.7) 90 (4.9)Therapy days (mean±SD) 411.4±542.3 388.7±393.2Median(25th, 75th) 150 (90, 630) 270 (100, 540)
RaloxifeneAny dispense, n (%): 40 (2.2) 6 (0.3)Therapy days (mean±SD) 391.5±568.9 225.0±463.1Median (25th, 75th) 135 (30, 465) 30 (30, 60)
a Includes any dispense of bisphosphonates, calcitonin, estrogens and raloxifene. Nopatients received teriparatide.
b MPR=medication possession ratio.
in treated vs. −2.65 in comparisonpatients). The rest of the studygroupconsisted of treated and comparison patients (n=793 each) matchedon the basis of age and a prior fracture. The mean age of these treatedand comparison patients was 76.3 years (SD 9.4), and 527 patients(66.5%) in both groups had a high-risk fracture.
Baseline characteristics of the full study population are presentedin Table 1. There were no significant differences between treated andcomparison patients in mean age, history of fracture, proportionsmoking, or history of hypothyroidism, osteoarthritis, Parkinson'sdisease, esophageal or peptic disorders, or use of tertiary tricyclicantidepressant medications. Among the approximately two-thirds ofpatients who had a BMD in the 2 years before index, the T-scores wereslightly lower in the treated group (−2.7 vs. −2.6; pb0.001), and thetreated group had a higher proportion of women with T-scores in theosteoporotic range of ≤−2.5 (67.3% vs. 54.7%). The treated group had alower BMI (26.1 vs. 26.9; pb0.001) and weight (146.6 lb vs. 151.8 lb;pb0.001) and a higher proportion of individualswith aweight b127 lb.The treated group also hadmorewomenwith rheumatoid arthritis andfewer women with dementia. The treated group had a higher meannumber of medications received (7.7, vs. 6.9 for comparison patients;pb0.001) and a higher frequency of benzodiazepines and protonpump inhibitors dispensed. Mean follow-up was somewhat longer fortreated patients (2.7 years [SD 2.0] vs. 2.3 years [SD 11.8]; pb0.001).
The use of medications for osteoporosis during follow-up isdisplayed in Table 2. The MPR for bisphosphonates for the treatedpatients is 0.60±0.38. Forty-five percent of treated patients had anMPR of ≥0.80. Small proportions of patients received osteoporosistherapies other than bisphosphonates. However, treated patientswere more likely than comparison patients to receive any ofcalcitonin, estrogens, or raloxifene (10.3% [n=188] vs. 6.7% [n=123],and some patients received more than one; data shown for agentsseparately in Table 2). There were no teriparatide dispenses during thestudy period.
During follow-up, 10.8% (n=198) of patients in the treated groupexperienced validated incident fractures (hip, 19.7% [n=39]; spine,19.2% [n=38]; wrist, 9.1% [n=18]; other, 52% [n=103]), as comparedwith 9.8% (n=179) of patients in the comparison group (hip, 12.8%[n=23]; spine, 10.6% [n=19]; wrist, 16.2% [n=29]; other, 60.3%

Fig. 2. Time to first fracture after index date in treated and comparison patients. During follow-up, 198 (10.8%) of patients in the treated group had incident fractures, vs. 179 (9.8%) ofpatients in the comparison group. After adjustments, patients in the treated group were .91 (95% CI 0.74–1.12) as likely to have an incident fracture as the comparison patients(p=0.388). The treatment effect remained non-significant after accounting for MPR.
157A.C. Feldstein et al. / Bone 44 (2009) 153–159
[n=108]). Fig. 2 presents Kaplan–Meier estimates of time to firstfracture for the treated and comparison group patients. The time tofirst fracture is not statistically different between the two groups(p= .474).
Table 3 presents hazard ratios, 95% confidence intervals, and p-values for the Cox proportional hazards model, adjusted forconfounders. Patients in the treated group were 0.91 (95% CI 0.74–1.13) as likely to have an incident fracture as the comparison patients,
Table 3Adjusted risk of fracture during follow-up (multivariate Cox proportional hazardsmodel)
Variables Hazard ratio 95% CI p-value
Treated group 0.91 0.74–1.13 0.390Age 1.04 1.03–1.05 b .001Weight b127 lba 1.22 0.97–1.55 0.093History of fractureb 1.04 0.82–1.32 0.748Current smokerc 1.34 0.92–1.96 0.131Hypothyroidismd 1.03 0.75–1.42 0.846Osteoarthritisd 1.32 1.03–1.68 0.026Rheumatoid arthritisd 1.15 0.62–2.14 0.656Parkinson's diseased 2.34 1.19–4.59 0.013Dementiad 0.87 0.55–1.37 0.552Esophageal and peptic disordersd,e 1.18 0.87–1.60 0.290Benzodiazepamsf 0.73 0.34–1.55 0.410Tertiary tricyclic antidepressantsg 1.29 0.83–1.99 0.260Number of medicationsh 1.02 0.99–1.04 0.060Diabetesd 1.16 0.84–1.59 0.370Proton pump inhibitori 1.21 0.87–1.68 0.253Selective serotonin reuptake inhibitori 1.49 1.12–2.0 0.007
Model based on 3522 (96.3%) patients with a weight measure and tobacco useascertainment record.
a Weight based onmost recent in prior 2 years available in 1809 (98.9%) treated group1775 (97.1%) comparison group.
b Any history of closed fracture excluding those of face, skull, finger, or toe.c Based on any record within 1 year prior to index date; 1797 (98.3%) in treated group
and 1779 (97.3%) in comparison group had record.d Problem list or encounter diagnosis within 1 year prior to index date.e Excludes peptic or esophageal ulcers or strictures.f Includes chlordiazepoxide, clorazepate, diazepam, flurazepam, triazolam.g Amitriptyline, imipramine, doxepin.h Unique medications dispersed in 12 months prior to index date, excluding
bisphosphonates.i Dispensed in 12 months prior to index date.
but the finding was not significant (p=0.390). Four covariates wereindependently significantly related to time to fracture. For each 1-yearincrease in patient age, patients were 4% more likely to fracture. Thosewith osteoarthritis were 1.32 times more likely (p=0.026), and thosewith Parkinson's disease were 2.34 times more likely (p=0.013) tofracture than those without those conditions. Patients takingdispensed a selective serotonin reuptake inhibitor (HR 1.49;p=0.007) were also more likely to fracture.
When the treated group was stratified into persons with MPRs forbisphosphonate therapy ≥80% vs. b80% during follow-up, the effect oftreatment on fracture risk remained non-significant.
Results were not substantively changed in othermodels: those thataccounted for matching, censoring for the initiation of non-bispho-sphonate osteoporosis medications, not censoring for the initiation ofbisphosphonates in the comparison group, limiting the studypopulation to those with BMD T-scores of ≤−2.5 or those with priorhigh-risk fractures or to only those who had a BMD.
Discussion
In a community cohort of post-menopausal women at similar riskof osteoporotic fractures, we found in an intention-to-treat analysisthat bisphosphonate therapy did not significantly reduce fracture risk.Although a number of observational studies have evaluated therelationship of fracture risk to use of anti-resorptives, includingbisphosphonates [11,12,15–17], we are not aware of any other studythat has adopted an approach similar to ours—namely, comparingfracture risk in clinical practice among persons prescribed bispho-sphonates to those who were not prescribed these agents. Given themorbidity and mortality associated with osteoporosis [1], our findingthat the effectiveness of bisphosphonates in the general community isfar below that found in clinical trials [7,8], and the fact thatconclusions about the cost-effectiveness studies of osteoporosistreatment are predicated on a 35% reduction in clinical fractureincidence [30], an enhanced understanding of this lack of treatmenteffect is urgently needed.
There are multiple possible explanations for the lack of treatmenteffect that we observed. First, prior studies of bisphosphonates haveconsistently demonstrated a lack of treatment effect for post-menopausal women who do not have BMD-confirmed osteoporosis

158 A.C. Feldstein et al. / Bone 44 (2009) 153–159
[6–8] or a prior vertebral or hip fracture [5,9]. Whenwe restricted ouranalyses to patients with a BMD T-score of ≤−2.5 or a prior high-riskfracture, the hazard ratio dropped to 0.82 for the treated group, butthe results remained non-significant (p=0.13). Second, prior bispho-sphonate studies revealed a greater treatment effect on the incidenceof vertebral, hip, and wrist fractures when compared to any clinicalfracture [5,6,8,31,32]. Our study was not powered to be able toevaluate the effect of treatment on these fracture subgroups.
The lack of a significant treatment effect may also be due to lowtreatment adherence. Using our intent-to-treat definition (those withany bisphosphonate dispense were included in the treatment group),we found that the bisphosphonate adherence of the treated womenwas low. Less than one-half of women in the treated group (44.6%) hadan MPR ≥80%, and a quarter had an MPR b20%.
This result is in contrast to the adherence observed in clinical trialsof bisphosphonate therapy. For example, in the Fracture InterventionTrial (FIT), which assessed the effect of alendronate on the risk offracture in women with low bone density, 96% of participants took atleast 75% of their pills [6]. Prior work among users of all medicationsfor osteoporosis found that a consistently high level of adherence(N90%) is needed to minimize fracture risk [15], that a year ofuninterrupted therapy reduced the risk of hip and vertebral fractures[11], and that poorer treatment adherence and lack of supplementa-tion with calcium and vitamin D were significantly associated withinadequate clinical response [16]. The only study limited to bispho-sphonate users found that only 43% of participants had an MPR N80%and that the association between refill compliance and fracture riskreduction was progressive, commencing at an MPR of about 50% [12].We believe that the lack of a treatment effect in our study owes largelyto low adherence, but we were unable to confirm this with our data.
Finally, subjects in our study may have been different from thosewho agree to participate in clinical trials of osteoporosis medications.Mean age in our study was 72 years, and we had no upper age limit(N10% were ≥85 years). The annual rate of fractures was about 4%, ascompared to 3.5% in the FIT trial [6]. Nearly two-thirds of the womenhad a BMD T-score of ≤−2.5, and about 45% had a prior fracture. Theseresults also are in contrast to the FIT trial [6], where the mean age ofparticipants was about 68 years and women age N80 years were notenrolled. In FIT, closer to a third of study subjects had a BMD T-score of≤−2.5, 35% had a prior fracture, and there were multiple comorbidityexclusions. Other authors have also noted a higher prevalence ofindividuals with prior fractures, more severe osteoporosis, and ahigher incidence of fractures in patients in clinical practice comparedwith those in clinical trials of anti-resorptive medications [16]. Otherillness or shorter life expectancy may diminish patient benefit fromtreatment.
This study has several additional limitations. As an observational–rather than experimental–study, there are several well-knownpotential biases [33]. Most importantly, treated patients may differfrom untreated patients, as was borne out in this study. We were ableto control for many but not all differences in important risk factors forfracture between treated and comparison patients. For example,although the mean BMD T-score was similar for the treatment andcomparison groups, the latter had a slightly lower risk, with a smallerproportion of women with T-scores ≤−2.5; we could not control forthis difference due to missing data. BMD measurement was availablein only about two-thirds of our study population, and the study wasnot powered for either this or the high-risk fracture subgroup.We alsocould not control for differences in use of supplements or otherlifestyle factors.
The overall follow-up time for patients in this studymay be shorterthan is optimal given that alendronate significantly reduced theincidence of non-vertebral fractures only after the first 2 years [34].Also, the comparison group had shorter follow-up time (mostly due tothe initiation of bisphosphonates), which could mean that they hadless opportunity to fracture, thereby biasing the difference between
their fracture risk and that of the treatment group toward the null.Although the Cox models adjust for these follow-up differences,patients with very short follow-up periods may not have a clinicallyreasonable amount of time to fracture.
The study was conducted at one site; membership is 92% white,which is not representative of other communities and practices withdifferent patient mixes. The data were limited in that they werecollected in the course of normal clinical care as opposed to in aresearch setting. Thus, data were collected at more varying intervals,and critical datawere not available, including BMD and other importantpredictors of fracture risk, such as family history, frailty and vision.
The study is strengthened by access to clinician-entered diagnos-tic, physiologic, and treatment data on many women at risk availablein an electronic medical record. In contrast to other reportedobservational studies in this area, we validated all incident fractures.Despite the inherent designweaknesses, the study provides importantinformation on the community effectiveness of bisphosphonates andidentifies areas for further research, in particular the effectiveness ofbisphosphonates in other community settings and among diversepatients. It would be useful to include more patients who have BMDmeasurement in future studies so that important risk subgroups couldbe evaluated. BMD ascertainment will be particularly important infurther evaluating the relationship of adherence to fracture risk; wefound that patients with lower BMDs were more adherent.
Future research should seek to further elucidate the relationship ofadherence to fracture outcomes (particularly threshold for response).Intermittent or inconsistent therapy may be acceptable in some cases,as previous studies have demonstrated persistence of an effect onbone turnover following discontinuation of alendronate therapy [35],vertebral fracture risk reduction that persisted during the first yearfollowing discontinuation of risedronate therapy inwomenwith post-menopausal osteoporosis [36], and a 5-year time period for post-treatment BMD to fall to pre-treatment levels after cessation ofalendronate [37]. In other cases, low adherence will diminishtreatment effectiveness unacceptably. We need to better identifyoptimal strategies for patient selection and support for treatment.
In summary, in this analysis of a community cohort of post-menopausal women at risk, the fracture risk of patients whoreceived bisphosphonates did not differ significantly from thosewho did not. Further work is necessary to elucidate and interveneupon the major contributors to reduced population effectiveness ofbisphosphonates.
Acknowledgments
This project was supported by Policy Analysis Inc. through aresearch contract with Amgen. The funding organization reviewedand approved the research design but was not involved in the conductof the research; the collection, management, analysis, or interpreta-tion of the data; or the preparation or approval of this manuscript. Thefunder had an opportunity to review the manuscript and providecomments prior to publication. The authors thank Sepideh S. Farivar,PhD; David Macarios, MBA; and Sacha Satram-Hoang, PhD, of AmgenInc. for their valuable comments on the study design and themanuscript. Dr. Feldstein had full access to all of the data in thestudy and takes responsibility for the integrity of the data and theaccuracy of the data analysis. Wewould like to thankMartha Swain forher editorial assistance and Debra Burch and Chalinya Bruce for theiradministrative support.
References
[1] Cummings SR, Melton LJ. Epidemiology and outcomes of osteoporotic fractures.Lancet 2002;359:1761–7.
[2] Burge R, Dawson-Hughes B, Solomon DH, Wong JB, King A, Tosteson A. Incidenceand economic burden of osteoporosis-related fractures in the United States, 2005–2025. J Bone Miner Res 2007;22:465–75.

159A.C. Feldstein et al. / Bone 44 (2009) 153–159
[3] Hanley DA, Josse RG. Prevention and management of osteoporosis: consensusstatements from the Scientific Advisory Board of the Osteoporosis Society ofCanada. 1. Introduction. CMAJ 1996;155:921–3.
[4] McCarus DC. Fracture prevention in postmenopausal osteoporosis: a review oftreatment options. Obstet Gynecol Surv 2006;61:39–50.
[5] Black DM, Cummings SR, Karpf DB, Cauley JA, Thompson DE, Nevitt MC, Bauer DC,Genant HK, Haskell WL, Marcus R, Ott SM, Torner JC, Quandt SA, Reiss TF, EnsrudKE. Randomised trial of effect of alendronate on risk of fracture in women withexisting vertebral fractures. Fracture Intervention Trial Research Group. Lancet1996;348:1535–41.
[6] Cummings SR, Black DM, Thompson DE, Applegate WB, Barrett-Connor E,Musliner TA, Palermo L, Prineas R, Rubin SM, Scott JC, Vogt T, Wallace R, YatesAJ, LaCroix AZ. Effect of alendronate on risk of fracture in women with low bonedensity but without vertebral fractures: results from the Fracture InterventionTrial. JAMA 1998;280:2077–82.
[7] Cranney A, Guyatt G, Griffith L, Wells G, Tugwell P, Rosen C. Meta-analyses oftherapies for postmenopausal osteoporosis. IX: Summary of meta-analyses oftherapies for postmenopausal osteoporosis. Endocr Rev 2002;23:570–8.
[8] Boonen S, Laan RF, Barton IP, Watts NB. Effect of osteoporosis treatments on risk ofnon-vertebral fractures: review and meta-analysis of intention-to-treat studies.Osteoporos Int 2005;16:1291–8.
[9] Lyles KW, Colon-Emeric CS, Magaziner JS, Adachi JD, Pieper CF, Mautalen C,Hyldstrup L, Recknor C, Nordsletten L, Moore KA, Lavecchia C, Zhang J, MesenbrinkP, Hodgson PK, Abrams K, Orloff JJ, Horowitz Z, Eriksen EF, Boonen S. Zoledronicacid and clinical fractures and mortality after hip fracture. N Engl J Med 2007;357:1799–809.
[10] Ettinger B, Pressman AR, Schein J, Chan J, Silver P, Connolly N. Alendronate useamong 812 women: prevalence of gastrointestinal complaints, non-compliancewith patient instructions, and discontinuation. J Manag Care Pharm 1998;4:488–92.
[11] McCombs JS, Thiebaud P, Laughlin-Miley C, Shi J. Compliance with drugtherapies for the treatment and prevention of osteoporosis. Maturitas 2004;48:271–87.
[12] Siris ES, Harris ST, Rosen CJ, Barr CE, Arvesen JN, Abbott TA, Silverman S. Adherenceto bisphosphonate therapy and fracture rates in osteoporotic women: relationshipto vertebral and nonvertebral fractures from 2 US claims databases. Mayo Clin Proc2006;81:1013–22.
[13] Weycker D, Macarios D, Edelsberg J, Oster G. Compliance with drug therapy forpostmenopausal osteoporosis. Osteoporos Int 2006;17:1645–52.
[14] Huybrechts KF, Ishak KJ, Caro JJ. Assessment of compliance with osteoporosistreatment and its consequences in a managed care population. Bone 2006;38:922–8.
[15] Caro JJ, Ishak KJ, Huybrechts KF, Raggio G, Naujoks C. The impact of compliancewith osteoporosis therapy on fracture rates in actual practice. Osteoporos Int2004;15:1003–8.
[16] Adami S, Isaia G, Luisetto G, Minisola S, Sinigaglia L, Gentilella R, Agnusdei D, Iori N,Nuti R. Fracture incidence and characterization in patients on osteoporosistreatment: the ICARO study. J Bone Miner Res 2006;21:1565–70.
[17] Weycker D, Macarios D, Edelsberg J, Oster G. Compliance with osteoporosis drugtherapy and risk of fracture. Osteoporos Int 2007;18:271–7.
[18] Freeborn DK, Pope C. Promise and performance in managed care: the prepaidgroup practice model. Baltimore, MD: Johns Hopkins University Press; 1994.
[19] Feldstein AC, Elmer PJ, Orwoll E, Herson M, Hillier T. Bone mineral densitymeasurement and treatment for osteoporosis in older individuals withfractures: a gap in evidence-based practice guideline. Arch Intern Med 2003;163:2165–72.
[20] National Osteoporosis Foundation. Physicians guide to prevention and treatmentof osteoporosis. Washington, DC: National Osteoporosis Foundation; 2000. RefType: Report.
[21] Melton III LJ, Achenbach SJ, O'FallonWM, Khosla S. Secondary osteoporosis and therisk of distal forearm fractures in men and women. Bone 2002;31:119–25.
[22] NIH Consensus Development Panel on Osteoporosis Prevention DaT. Osteoporosisprevention, diagnosis, and therapy. JAMA 2001;285:785–95.
[23] Seeley DG, Browner WS, Nevitt MC, Genant HK, Scott JC, Cummings SR. Whichfractures are associated with low appendicular bone mass in elderly women? TheStudy of Osteoporotic Fractures Research Group. Ann Intern Med 1991;115:837–42.
[24] Cummings SR, Nevitt MC, BrownerWS, Stone K, Fox KM, Ensrud KE, Cauley J, BlackD, Vogt TM. Risk factors for hip fracture in white women. Study of OsteoporoticFractures Research Group. N Engl J Med 1995;332:767–73.
[25] Schwartz AV, Sellmeyer DE. Effect of thiazolidinediones on skeletal health inwomen with Type 2 diabetes. Expert Opin Drug Saf 2008;7:69–78.
[26] Weng MY, Lane NE. Medication-induced osteoporosis. Curr Osteoporos Rep2007;5:139–45.
[27] Allport J. Incidence and prevalence of medication-induced osteoporosis: evidence-based review. Curr Opin Rheumatol 2008;20:435–41.
[28] Tinetti ME, Speechley M, Ginter SF. Risk factors for falls among elderly personsliving in the community. N Engl J Med 1988;319:1701–7.
[29] Schneeweiss S,Walker AM, Glynn RJ,MaclureM, Dormuth C, Soumerai SB. Outcomesof reference pricing for angiotensin-converting-enzyme inhibitors. N Engl J Med2002;346:822–9.
[30] Tosteson AN, Melton III LJ, wson-Hughes B, Baim S, Favus MJ, Khosla S, Lindsay RL.Cost-effective osteoporosis treatment thresholds: the United States perspective.Osteoporos Int 2008;19:437–47.
[31] Harris ST, Watts NB, Genant HK, McKeever CD, Hangartner T, Keller M, Chesnut IIICH, Brown J, Eriksen EF, Hoseyni MS, Axelrod DW, Miller PD. Effects of risedronatetreatment on vertebral and nonvertebral fractures in women with postmenopau-sal osteoporosis: a randomized controlled trial. Vertebral Efficacy With Risedro-nate Therapy (VERT) Study Group. JAMA 1999;282:1344–52.
[32] Black DM, Delmas PD, Eastell R, Reid IR, Boonen S, Cauley JA, Cosman F, Lakatos P,Leung PC, Man Z, Mautalen C, Mesenbrink P, Hu H, Caminis J, Tong K, Rosario-Jansen T, Krasnow J, Hue TF, Sellmeyer D, Eriksen EF, Cummings SR. Once-yearlyzoledronic acid for treatment of postmenopausal osteoporosis. N Engl J Med2007;356:1809–22.
[33] Laupacis A, Mamdani M. Observational studies of treatment effectiveness: somecautions. Ann Intern Med 2004;140:923–4.
[34] Black DM, Thompson DE, Bauer DC, Ensrud K, Musliner T, HochbergMC, Nevitt MC,Suryawanshi S, Cummings SR. Fracture risk reduction with alendronate in womenwith osteoporosis: the Fracture Intervention Trial. FIT Research Group. J ClinEndocrinol Metab 2000;85:4118–24.
[35] Wasnich RD, Bagger YZ, Hosking DJ, McClung MR, Wu M, Mantz AM, Yates JJ, RossPD, Alexandersen P, Ravn P, Christiansen C, Santora AC. Changes in bone densityand turnover after alendronate or estrogen withdrawal. Menopause 2004;11:622–30.
[36] Watts NB, Chines A, Olszynski WP, McKeever CD, McClung MR, Zhou X, Grauer A.Fracture risk remains reduced one year after discontinuation of risedronate.Osteoporos Int 2008;19(3):365–72. Electronic Publication 2007, Oct. 16.
[37] Ensrud KE, Barrett-Connor EL, Schwartz A, Santora AC, Bauer DC, Suryawanshi S,Feldstein A, Haskell WL, Hochberg MC, Torner JC, Lombardi A, Black DM.Randomized trial of effect of alendronate continuation versus discontinuation inwomen with low BMD: results from the Fracture Intervention Trial long-termextension. J Bone Miner Res 2004;19:1259–69.
Related Documents











