Effective transcatheter valve implantation after pulmonary homograft failure: A new perspective on the Ross operation Johannes Nordmeyer a , Philipp Lurz a , Victor T. Tsang a , Louise Coats a , Fiona Walker b , Andrew M. Taylor a , Sachin Khambadkone a , Marc R. de Leval a , and Philipp Bonhoeffer a,∗ Johannes Nordmeyer: ; Philipp Lurz: ; Victor T. Tsang: ; Louise Coats: ; Fiona Walker: ; Andrew M. Taylor: ; Sachin Khambadkone: ; Marc R. de Leval: ; Philipp Bonhoeffer: [email protected] a UCL Institute of Child Health and Great Ormond Street Hospital for Children, London, United Kingdom. b The Heart Hospital, London, United Kingdom. Abstract Objective—The Ross procedure offers good autograft function and low reoperation rates for the neoaortic valve; however, the rate of conduit dysfunction in the right ventricular outflow tract remains a concern. This study assessed percutaneous pulmonary valve implantation in this setting. Methods—We retrospectively analyzed outcomes of 12 patients (mean age 28 ± 5 years) referred for percutaneous pulmonary valve implantation to treat right ventricle–pulmonary artery conduit failure 11.1 ± 3.3 years after Ross procedure. Results—Percutaneous pulmonary valve implantation was feasible in all 12 patients, with no procedural complications (procedure time 99 ± 16 minutes, fluoroscopy time 21 ± 6 minutes). Right ventricular outflow tract gradient during catheterization and pulmonary regurgitant fraction on magnetic resonance imaging fell after valve implantation (gradient 34 ± 6 to 14 ± 3 mm Hg, P < . 01, regurgitant fraction 20% ± 6% to 2% ± 1%, P < .05). After restoration of right ventricular outflow tract function, indexed right ventricular end-diastolic volume decreased (91 ± 13 to 78 ± 12 mL · beat −1 · m −2 , P < .01) and maximal cardiopulmonary exercise performance improved (peak oxygen consumption 25.4 ± 2.3 to 30.8 ± 3.0 mL · kg −1 · min −1 , P < .01). During follow-up (18.8 ± 4.6 months), there was 1 device explantation (restenosis). The probabilities of freedom from right ventricular outflow tract reoperation were 100% at 1 year and 90% at 3 years. Conclusions—Percutaneous pulmonary valve implantation provides an effective transcatheter treatment strategy to prolong the lifespan of right ventricle–pulmonary artery conduits after the Ross procedure, reducing the reoperation burden on patients with aortic valve disease. © 2009 Mosby, Inc.. This document may be redistributed and reused, subject to certain conditions. ∗Address for reprints: Philipp Bonhoeffer, MD, Cardiothoracic Unit, Great Ormond Street Hospital for Children, Great Ormond St, London WC1N 3JH, UK. [email protected]. This document was posted here by permission of the publisher. At the time of deposit, it included all changes made during peer review, copyediting, and publishing. The U.S. National Library of Medicine is responsible for all links within the document and for incorporating any publisher-supplied amendments or retractions issued subsequently. The published journal article, guaranteed to be such by Elsevier, is available for free, on ScienceDirect. Supported by the British Heart Foundation (RG/03/006). P.L. is funded by the European Union (Health e Child Initiative); L.C. was funded by the British Heart Foundation; and A.M.T. is funded by the Higher Education Funding Council for England. Sponsored document from The Journal of Thoracic and Cardiovascular Surgery Published as: J Thorac Cardiovasc Surg. 2009 July ; 138(1): 84–88. Sponsored Document Sponsored Document Sponsored Document

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Effective transcatheter valve implantation after pulmonaryhomograft failure: A new perspective on the Ross operation
Johannes Nordmeyera, Philipp Lurza, Victor T. Tsanga, Louise Coatsa, Fiona Walkerb,Andrew M. Taylora, Sachin Khambadkonea, Marc R. de Levala, and Philipp Bonhoeffera,∗Johannes Nordmeyer: ; Philipp Lurz: ; Victor T. Tsang: ; Louise Coats: ; Fiona Walker: ; Andrew M. Taylor: ; SachinKhambadkone: ; Marc R. de Leval: ; Philipp Bonhoeffer: [email protected] Institute of Child Health and Great Ormond Street Hospital for Children, London, UnitedKingdom.bThe Heart Hospital, London, United Kingdom.
AbstractObjective—The Ross procedure offers good autograft function and low reoperation rates for theneoaortic valve; however, the rate of conduit dysfunction in the right ventricular outflow tract remainsa concern. This study assessed percutaneous pulmonary valve implantation in this setting.
Methods—We retrospectively analyzed outcomes of 12 patients (mean age 28 ± 5 years) referredfor percutaneous pulmonary valve implantation to treat right ventricle–pulmonary artery conduitfailure 11.1 ± 3.3 years after Ross procedure.
Results—Percutaneous pulmonary valve implantation was feasible in all 12 patients, with noprocedural complications (procedure time 99 ± 16 minutes, fluoroscopy time 21 ± 6 minutes). Rightventricular outflow tract gradient during catheterization and pulmonary regurgitant fraction onmagnetic resonance imaging fell after valve implantation (gradient 34 ± 6 to 14 ± 3 mm Hg, P < .01, regurgitant fraction 20% ± 6% to 2% ± 1%, P < .05). After restoration of right ventricular outflowtract function, indexed right ventricular end-diastolic volume decreased (91 ± 13 to 78 ± 12 mL ·beat−1 · m−2, P < .01) and maximal cardiopulmonary exercise performance improved (peak oxygenconsumption 25.4 ± 2.3 to 30.8 ± 3.0 mL · kg−1 · min−1, P < .01). During follow-up (18.8 ± 4.6months), there was 1 device explantation (restenosis). The probabilities of freedom from rightventricular outflow tract reoperation were 100% at 1 year and 90% at 3 years.
Conclusions—Percutaneous pulmonary valve implantation provides an effective transcathetertreatment strategy to prolong the lifespan of right ventricle–pulmonary artery conduits after the Rossprocedure, reducing the reoperation burden on patients with aortic valve disease.
© 2009 Mosby, Inc..This document may be redistributed and reused, subject to certain conditions.
∗Address for reprints: Philipp Bonhoeffer, MD, Cardiothoracic Unit, Great Ormond Street Hospital for Children, Great Ormond St,London WC1N 3JH, UK. [email protected] document was posted here by permission of the publisher. At the time of deposit, it included all changes made during peer review,copyediting, and publishing. The U.S. National Library of Medicine is responsible for all links within the document and for incorporatingany publisher-supplied amendments or retractions issued subsequently. The published journal article, guaranteed to be such by Elsevier,is available for free, on ScienceDirect.Supported by the British Heart Foundation (RG/03/006). P.L. is funded by the European Union (Health e Child Initiative); L.C. wasfunded by the British Heart Foundation; and A.M.T. is funded by the Higher Education Funding Council for England.
Sponsored document fromThe Journal of Thoracic andCardiovascular Surgery
Published as: J Thorac Cardiovasc Surg. 2009 July ; 138(1): 84–88.
Sponsored Docum
ent Sponsored D
ocument
Sponsored Docum
ent
Abbreviations and AcronymsCPEX, cardiopulmonary exercise; MRI, magnetic resonance imaging; PA, pulmonary artery; PPVI,percutaneous pulmonary valve implantation; RV, right ventricle; RVOT, right ventricular outflowtract
The pulmonary autograft replacement of aortic valve (Ross procedure) represents an attractivesurgical option for aortic valve disease, especially for younger patients. Because it uses thepatient's own pulmonary valve as an aortic autograft, advantages include a favorablehemodynamic profile, the potential for adaptive growth, and the avoidance of anticoagulationtherapy and its associated risks. In addition, the autograft function has been shown to beacceptable in several studies reporting midterm outcomes for this procedure in different patientpopulations. A major drawback of this procedure, however, is that the necessary placement ofa conduit from the right ventricle (RV) to the pulmonary artery (PA) converts “single-valvedisease” into “two-valve disease.” Although the orthotopic positioning of the RV-PA conduitmay provide a reasonable longevity, the rate of RV-PA conduit dysfunction remains asignificant concern, with an estimated freedom from reoperation or restenosis (peak RVoutflow tract [RVOT] gradient exceeding 30 mm Hg) of only 64% at 6 years in a pediatriccohort. We report our experience with percutaneous pulmonary valve implantation (PPVI) asa transcatheter treatment option for RV-PA conduit dysfunction in this setting.
Materials and MethodsPatients
Of the 176 patients who underwent PPVI with the current device design (January 2003–November 2007), we retrospectively examined the outcomes of 13 patients who had RV-PAconduit dysfunction after the Ross procedure. One patient with repaired complex leftventricular outflow tract obstruction (coarctation with valvular and supravalvular aorticstenosis) was excluded from the analysis, because PPVI was performed only as part of apalliative strategy in the context of multiorgan failure. Most of the remaining patients (10/12)had the Ross procedure performed outside our institutions. Clinical indications for PPVIincluded RV hypertension with significant RVOT obstruction, significant pulmonaryinsufficiency, and RV dilatation or failure as described previously.
PPVI was performed under general anesthesia at Great Ormond Street Hospital for Children,The Heart Hospital, and Harley Street Clinic (London, UK). The ethics committees at theseinstitutions approved the study protocol, and written, informed consent was obtained frompatients and parents as appropriate.
EchocardiographyOn echocardiography, peak RVOT gradient and RV systolic pressure (estimated from tricuspidregurgitant jet velocities) were obtained from continuous-wave Doppler traces (VIVID 7; GE,Medical Systems, Milwaukee, Wis). Color flow mapping of the RVOT and branch pulmonaryarteries was used for qualitative grading of the degree of pulmonary regurgitation (0 absent, 1trivial, 2 mild, 3 moderate, and 4 severe).
Cardiopulmonary Exercise TestingTen of 12 patients underwent cardiopulmonary exercise (CPEX) testing before and early afterPPVI (median 20 days after PPVI, range 2–381 days). The remaining 2 patients did not undergoCPEX testing because of pulmonary hypertension (n = 1) and nonmedical reasons (n = 1). Aramp protocol was performed on a mechanically braked bicycle ergometer (ergometrics ER
Nordmeyer et al. Page 2
Published as: J Thorac Cardiovasc Surg. 2009 July ; 138(1): 84–88.
Sponsored Docum
ent Sponsored D
ocument
Sponsored Docum
ent
900 PC; ergoline GmbH, Bitz, Germany). Peak oxygen consumption was derived fromrespiratory gas analysis during CPEX testing.
Cardiac Magnetic Resonance ImagingCardiac magnetic resonance imaging (MRI) was performed for 10 of 12 patients before andearly after PPVI (median 7 days after PPVI, range 1–364 days). The remaining 2 patients didnot undergo cardiac MRI because they had pacemakers inserted. The MRI scans wereperformed at 1.5 T (Symphony Maestro Series and Avanto; Siemens Medical Systems,Erlangen, Germany). Retrospective gated steady-state free-precession cine images of the heartand arterial flow data with a flow-sensitive gradient echo sequence were acquired. Thereafter,ventricular volumes, pulmonary and aortic regurgitant fractions were calculated with the Argusanalysis work package (Siemens Medical Systems).
Follow-up AssessmentDuring structured follow-up, echocardiographic and chest radiographic investigations wereperformed immediately after PPVI and at 1 month, 3 months, 6 months, 1 year, and yearlythereafter. Echocardiography was used to assess the hemodynamic situation; chest radiographywas used to screen for structural integrity of the stent.
Statistical AnalysisData are expressed as mean ± SEM unless otherwise specified. Two paired samples wereanalyzed with paired Student t tests or Wilcoxon matched pairs tests as appropriate. Multiplecomparisons were performed with repeated measures analysis of variance and subsequent posthoc analysis (Bonferroni correction) as appropriate. Probability of freedom from reinterventionwas obtained by use of Kaplan–Meier plots. Statistical testing and data analysis were performedwith SPSS version 11 (SPSS Inc, Chicago, Ill) and GraphPad InStat 3 Demo (GraphpadSoftware, Inc, La Jolla, Calif).
ResultsBaseline Characteristics
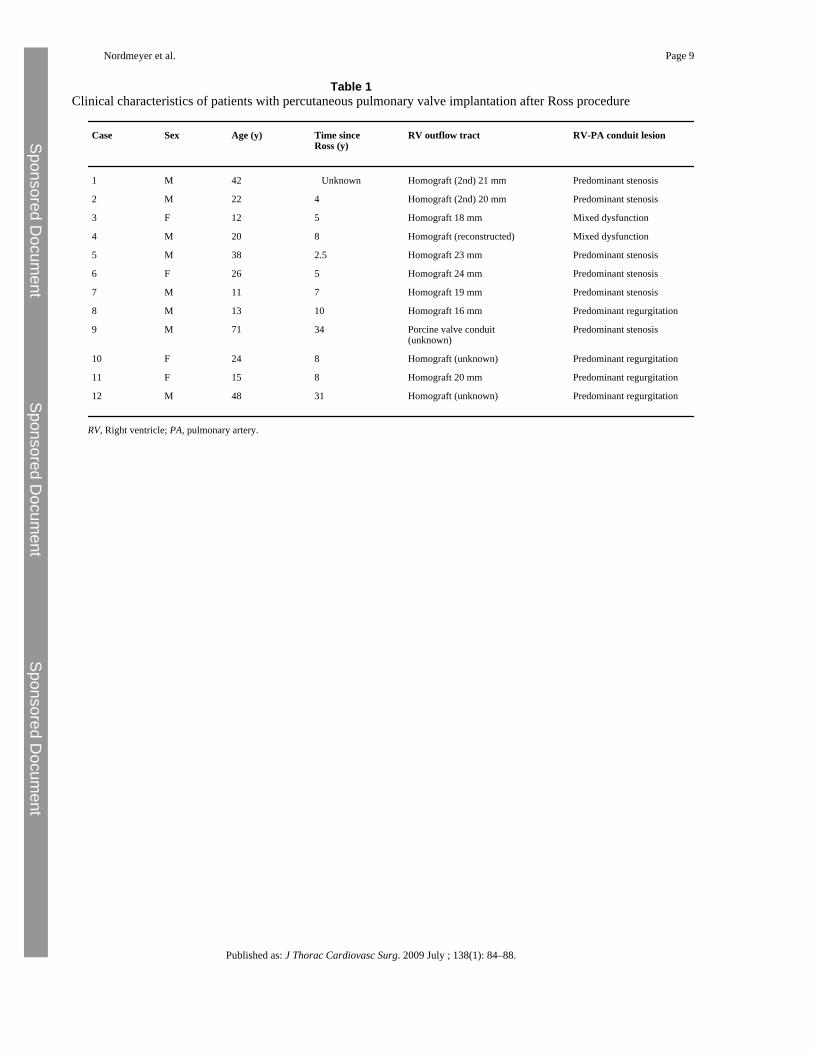
Twelve patients (28 ± 5 years old, 21–98 kg) underwent PPVI for RV-PA conduit failure 11.1± 3.3 years after Ross procedure (Table 1). The indications for PPVI were predominant RV-PA conduit stenosis in 6 of 12 patients (50%), predominant conduit regurgitation in 4 of 12(33%), and mixed conduit dysfunction in 2 of 12 (17%) (Table 1). The failed conduitscomprised homografts in 11 of 12 cases (92%, first homograft n = 8, reconstructed firsthomograft n = 1, second homograft n = 2) and a porcine valve conduit in the remaining case(8%).
In the aortic position, 11 of 12 patients (92%) had the original autograft in place with nosignificant incompetence (median aortic regurgitant fraction 3%, range 0%–17%). One patient(8%) had a 19-mm St Jude mechanical valve (St Jude Medical, Inc, St Paul, Minn), which wasinserted because of early autograft failure 1 year after the Ross procedure.
Procedural DetailsPPVI was successful in 12 of 12 patients (100%; Figure 1), with no procedural complications(procedure time 99 ± 16 minutes; fluoroscopy time 21 ± 6 minutes). Prestenting with a bare-metal stent (Max LD; ev3 Endovascular, Inc, Peripheral Vascular, Plymouth, Minn) wasperformed in 2 of 12 patients (17%), particularly in the context of early second homograftfailure, 1.5 years and 3.5 years after surgery.
Nordmeyer et al. Page 3
Published as: J Thorac Cardiovasc Surg. 2009 July ; 138(1): 84–88.
Sponsored Docum
ent Sponsored D
ocument
Sponsored Docum
ent
Hemodynamic OutcomeAfter PPVI, the invasively measured peak RVOT gradient, and RV-systemic pressure ratio fellacutely (RVOT gradient 34 ± 6 to 14 ± 3 mm Hg, P < .01, RV–SP ratio 0.68 ± 0.07 to 0.42 ±0.03, P < .01). Likewise, pulmonary regurgitant fraction measured on cardiac MRI fell afterPPVI (20% ± 6% to 2% ± 1%, P < .05).
On cardiac MRI, the indexed RV end-diastolic volume decreased (91 ± 13 to 78 ± 12 mL ·beat−1 · m−2, P < .01; Table 2). Other parameters did not show statistically significantdifferences from before to after PPVI (Table 2).
Functional OutcomeCPEX testing revealed improved indices of maximal cardiopulmonary exercise performance(peak oxygen consumption 25.4 ± 2.3 to 30.8 ± 3.0 mL · kg−1 · min−1, P < .01, maximumworkload achieved 128 ± 11 to 150 ± 13 W, P < .01; Table 2). In addition, the anaerobicthreshold increased after restoration of RVOT function (13.6 ± 1.3 to 15.0 ± 1.3 mL · kg−1 ·min−1, P < .05; Table 2).
Reintervention and ReoperationDuring a mean follow-up of 18.8 ± 4.6 months, 2 of 12 patients (17%) had further events. Bothpatients had a good initial result from PPVI but had RVOT obstruction recur because of stentfractures and were treated with second PPVI at 4 and 7 months, respectively. Subsequently, 1of the 2 patients required third PPVI at 3 years, when further hemodynamically relevant stentfractures occurred. The other patient had restenosis in the context of medically treatedendocarditis; however, the actual cause of restenosis could not be unequivocally identified.This patient underwent reoperation and device explantation at 13 months at another institution.In this series, the probabilites of freedom from RVOT reintervention were 81.5% at 1 and 3years (Figure 2, A), respectively, and the freedoms from RVOT reoperation were 100% at 1year and 90% at 3 years (Figure 2, B).
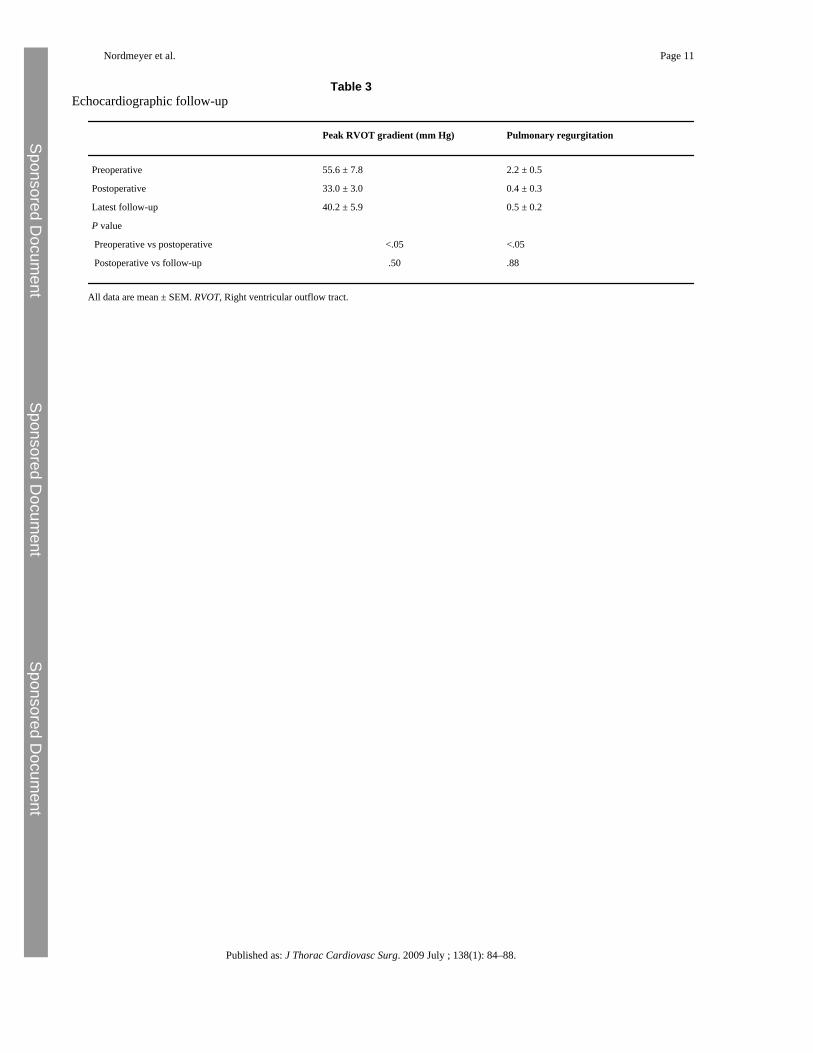
In all other patients (10 of 12, 83%), there was sustained hemodynamic improvement at latestfollow-up relative to immediate postprocedural results. This improvement was demonstratedby echocardiography, which also showed preserved pulmonary valve competence (Table 3).
DiscussionThe search for the optimal surgical treatment for aortic valve lesions in young patients remainsa significant challenge. Ideally, a replacement valve should offer native hemodynamicperformance, the potential for adaptive growth, freedom from anticoagulation therapy (whichhas important implications for patient compliance), and good longevity. In this respect, theautograft valve comes close to the ideal, and it is superior to such other current options asbioprosthetic and mechanical valves. The Ross procedure continues to be questioned as atreatment option for patients with aortic valve disease, however, because of the potential forautograft dilatation or failure but in particular because of the need for RV-PA conduit. Thisstudy showed PPVI to provide a novel, effective transcatheter treatment strategy to prolongthe lifespan of surgically placed RV-PA conduits in this scenario. Such a minimally invasivetreatment for managing conduit dysfunction justifies a further review of the Ross procedure,particularly for young patients, who probably benefit most from the advantages of the autograftoption.
In this series, we had good procedural success and did not see procedural complications withPPVI. This finding is related to the advantageous anatomic substrate in patients after the Rossprocedure of circumferential RV-PA conduits placed into undistorted anatomy of the RVOT
Nordmeyer et al. Page 4
Published as: J Thorac Cardiovasc Surg. 2009 July ; 138(1): 84–88.
Sponsored Docum
ent Sponsored D
ocument
Sponsored Docum
ent
and the PAs. These anatomic features compare favorably with our experience with congenitalright heart lesions, in which the underlying RVOT anatomy often makes device implantationchallenging, and in very rare cases even impossible. From a technical perspective, most patientswith RV-PA conduit failure after the Ross procedure therefore qualify for PPVI. Particularcare should be taken to prevent damage to the reimplanted coronary arteries, because theirproximal course could be at risk from external compression during percutaneous valvedeployment, although we have not seen this in our own experience. Careful preproceduralimaging assessment of the reimplanted coronary arteries in relation to the RVOT shouldtherefore be performed. This imaging should involve noninvasive 3-dimensional imagingmodalities (eg, cardiac magnetic resonance or computed tomography) in addition to standardangiography during catheterization.
Importantly, RVOT function was restored in all patients after PPVI, with significant reductionsin pulmonary stenosis and regurgitation. A slight residual gradient across the RVOT may befound with this technique, however, because the device cannot always be expanded to itsintended dimensions as a result of the varying geometry and distensibility of the failed RV-PAconduits (eg, the impact of asymmetric calcifications). The mean size of the original RV-PAconduits in this series revealed no evidence supporting patient–prosthesis mismatch;nonetheless, this possibility cannot be fully excluded. It is important to note that use of thecurrent device is restricted to RV-PA conduits larger than 14 × 14 mm11 to achieve a sufficientvalve orifice area. Therefore, patients who have received RV-PA conduits smaller than thesuggested dimension (eg, those operated on at a very young age) thus do not qualify for PPVI.In our overall experience of PPVI, prestenting with bare-metal stents and postdilatation withhigh-pressure balloons has resulted in less residual gradients, leading to lower reinterventionrates.
The restoration of RVOT function was accompanied by changes in MRI and CPEX parameters,suggesting an objective improvement in cardiac function after relief of adverse RV loadingconditions. These data represent the first description of early functional outcome after RVOTreintervention in the Ross population without the confounding effects of cardiopulmonarybypass. Long-term ventricular response and other outcome parameters, however, cannot beforeseen at present.
The only indication for reintervention in this series of PPVI was recurrent RVOT obstruction.Overall, 3 repeated PPVI were performed in 2 patients and was an effective treatment optionfor early device failure caused by stent fracture, the most common follow-up complication inour experience, resulting in further prolongation of the lifespan of surgically placedconduits. RVOT reoperation was performed in 1 patient, 13 months after PPVI. The surgerywas performed at another institution for what was described as restenosis after medicaltreatment of endocarditis, although the actual cause of the gradient across the device could notbe unequivocally identified at surgery.
LimitationsOur study highlights an important treatment option for patients after the Ross procedure;however, it represents a retrospective analysis in a relatively small patient population. Mostpatients were referred to us from different institutions. All follow-up investigations wereperformed and read in an unblinded fashion. Although our study has demonstrated immediatefunctional benefits from this procedure, its long-term utility remains to be investigated.
ConclusionsRV-PA conduit dysfunction after the Ross procedure can be successfully treated with PPVI.This may help decrease the cumulative surgical burden in the lifetime management of left
Nordmeyer et al. Page 5
Published as: J Thorac Cardiovasc Surg. 2009 July ; 138(1): 84–88.
Sponsored Docum
ent Sponsored D
ocument
Sponsored Docum
ent
ventricular outflow tract lesions and thus justifies a further review of the Ross operation,particularly for young patients.
References1. Ross D.N. Replacement of the aortic and mitral valves with a pulmonary autograft. Lancet 1967;2:956–
959. [PubMed: 4167516]2. Simon P. Aschauer C. Moidl R. Marx M. Keznickl F.P. Eigenbauer E. Growth of the pulmonary
autograft after the Ross operation in childhood. Eur J Cardiothorac Surg 2001;19:118–121. [PubMed:11167098]
3. Kouchoukos N.T. Dávila-Román V.G. Spray T.L. Murphy S.F. Perrillo J.B. Replacement of the aorticroot with a pulmonary autograft in children and young adults with aortic-valve disease. N Engl J Med1994;330:1–6. [PubMed: 8259138]
4. Sievers H.H. Hanke T. Stierle U. Bechtel M.F. Graf B. Robinson D.R. A critical reappraisal of theRoss operation: renaissance of the subcoronary implantation technique? Circulation 2006;114(1Suppl):I504–I511. [PubMed: 16820628]
5. Hanke T. Stierle U. Boehm J.O. Botha C.A. Matthias Bechtel J.F. Erasmi A. Autograft regurgitationand aortic root dimensions after the Ross procedure: the German Ross Registry experience. Circulation2007;116(11 Suppl):I251–I258. [PubMed: 17846313]
6. Böhm J.O. Botha C.A. Horke A. Hemmer W. Roser D. Blumenstock G. Is the Ross operation still anacceptable option in children and adolescents? Ann Thorac Surg 2006;82:940–947. [PubMed:16928513]
7. McMullan D.M. Oppido G. Davies B. Kawahira Y. Cochrane A.D. d'Udekem d'Acoz Y. Surgicalstrategy for the bicuspid aortic valve: tricuspidization with cusp extension versus pulmonary autograft.J Thorac Cardiovasc Surg 2007;134:90–98. [PubMed: 17599491]
8. Selamet Tierney E.S. Gersony W.M. Altmann K. Solowiejczyk D.E. Bevilacqua L.M. Khan C.Pulmonary position cryopreserved homografts: durability in pediatric Ross and non-Ross patients. JThorac Cardiovasc Surg 2005;130:282–286. [PubMed: 16077388]
9. Bonhoeffer P. Boudjemline Y. Saliba Z. Merckx J. Aggoun Y. Bonnet D. Percutaneous replacementof pulmonary valve in a right-ventricle to pulmonary-artery prosthetic conduit with valve dysfunction.Lancet 2000;356:1403–1405. [PubMed: 11052583]
10. Khambadkone S. Coats L. Taylor A. Boudjemline Y. Derrick G. Tsang V. Percutaneous pulmonaryvalve implantation in humans: results in 59 consecutive patients. Circulation 2005;112:1189–1197.[PubMed: 16103239]
11. Lurz P. Coats L. Khambadkone S. Nordmeyer J. Boudjemline Y. Schievano S. Percutaneouspulmonary valve implantation: impact of evolving technology and learning curve on clinicaloutcome. Circulation 2008;117:1964–1972. [PubMed: 18391109]
12. Coats L. Khambadkone S. Derrick G. Sridharan S. Schievano S. Mist B. Physiological and clinicalconsequences of relief of right ventricular outflow tract obstruction late after repair of congenitalheart defects. Circulation 2006;113:2037–2044. [PubMed: 16636174]
13. Nordmeyer J. Khambadkone S. Coats L. Schievano S. Lurz P. Parenzan G. Risk stratification,systematic classification, and anticipatory management strategies for stent fracture after percutaneouspulmonary valve implantation. Circulation 2007;115:1392–1397. [PubMed: 17339542]
14. Nordmeyer J. Coats L. Lurz P. Lee T.Y. Rees P. Cullen S. Percutaneous pulmonary valve-in-valveimplantation: a successful treatment concept for early device failure. Eur Heart J 2008;29:810–815.[PubMed: 18316357]
Nordmeyer et al. Page 6
Published as: J Thorac Cardiovasc Surg. 2009 July ; 138(1): 84–88.
Sponsored Docum
ent Sponsored D
ocument
Sponsored Docum
ent
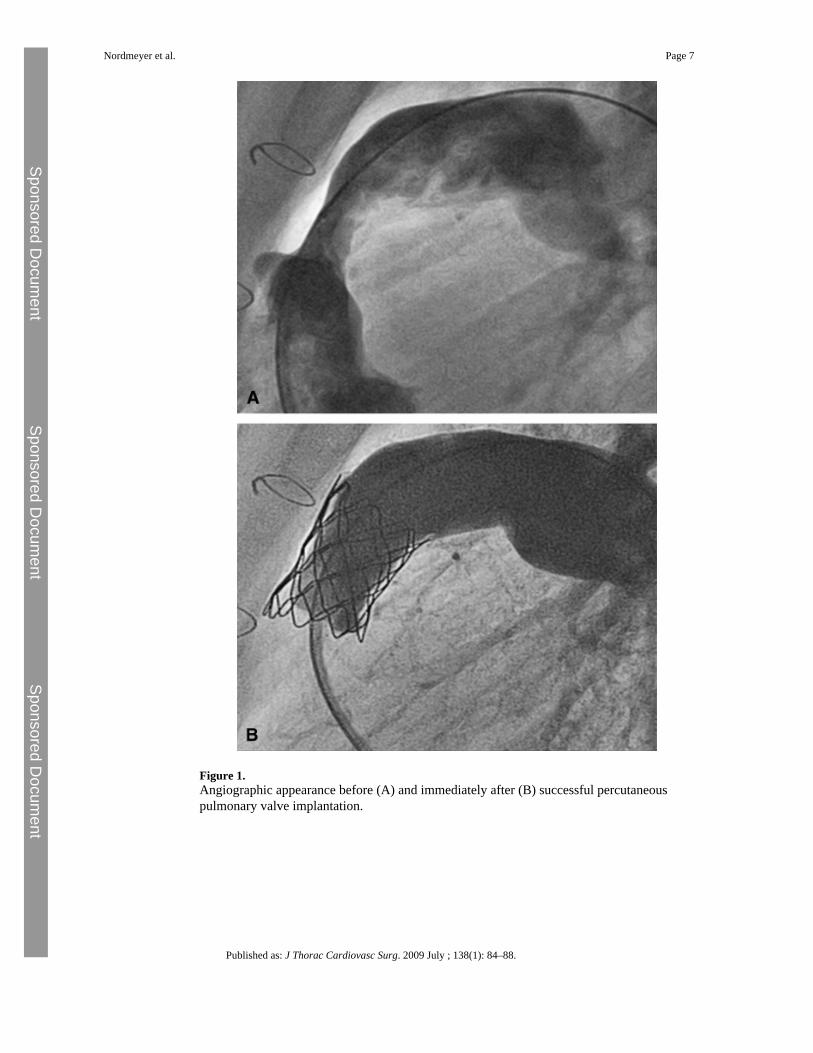
Figure 1.Angiographic appearance before (A) and immediately after (B) successful percutaneouspulmonary valve implantation.
Nordmeyer et al. Page 7
Published as: J Thorac Cardiovasc Surg. 2009 July ; 138(1): 84–88.
Sponsored Docum
ent Sponsored D
ocument
Sponsored Docum
ent
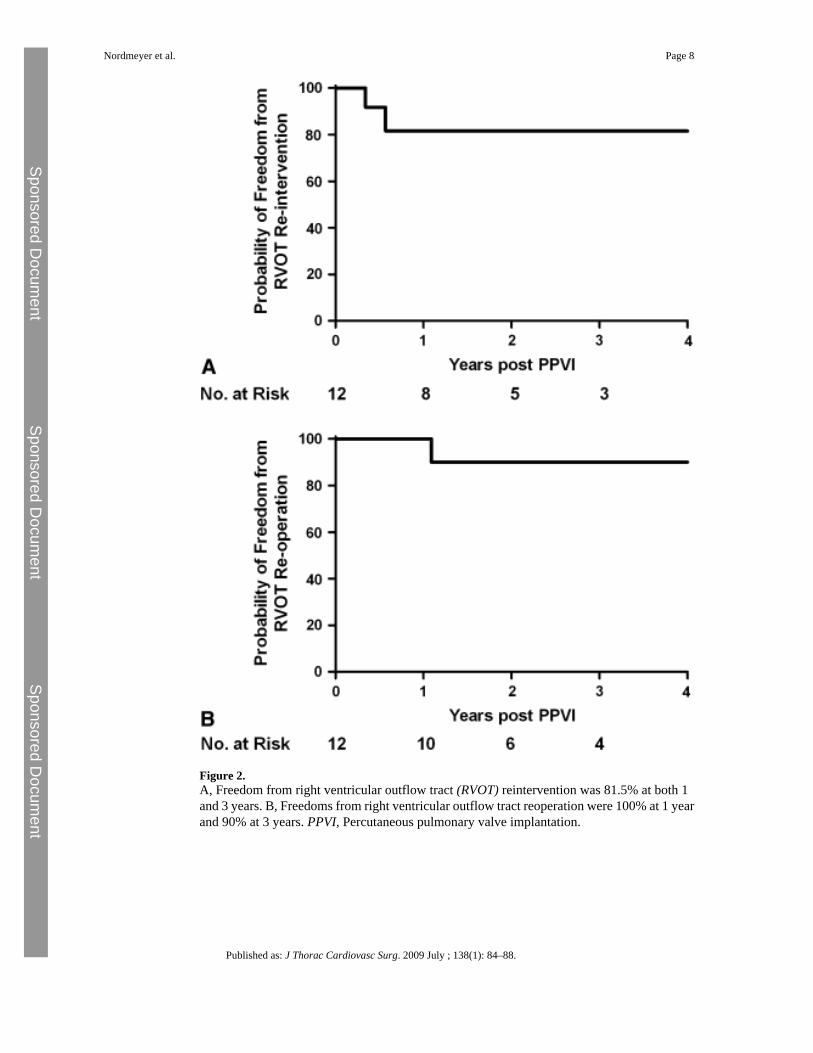
Figure 2.A, Freedom from right ventricular outflow tract (RVOT) reintervention was 81.5% at both 1and 3 years. B, Freedoms from right ventricular outflow tract reoperation were 100% at 1 yearand 90% at 3 years. PPVI, Percutaneous pulmonary valve implantation.
Nordmeyer et al. Page 8
Published as: J Thorac Cardiovasc Surg. 2009 July ; 138(1): 84–88.
Sponsored Docum
ent Sponsored D
ocument
Sponsored Docum
ent
Sponsored Docum
ent Sponsored D
ocument
Sponsored Docum
ent
Nordmeyer et al. Page 9
Table 1Clinical characteristics of patients with percutaneous pulmonary valve implantation after Ross procedure
Case Sex Age (y) Time sinceRoss (y)
RV outflow tract RV-PA conduit lesion
1 M 42 Unknown Homograft (2nd) 21 mm Predominant stenosis
2 M 22 4 Homograft (2nd) 20 mm Predominant stenosis
3 F 12 5 Homograft 18 mm Mixed dysfunction
4 M 20 8 Homograft (reconstructed) Mixed dysfunction
5 M 38 2.5 Homograft 23 mm Predominant stenosis
6 F 26 5 Homograft 24 mm Predominant stenosis
7 M 11 7 Homograft 19 mm Predominant stenosis
8 M 13 10 Homograft 16 mm Predominant regurgitation
9 M 71 34 Porcine valve conduit(unknown)
Predominant stenosis
10 F 24 8 Homograft (unknown) Predominant regurgitation
11 F 15 8 Homograft 20 mm Predominant regurgitation
12 M 48 31 Homograft (unknown) Predominant regurgitation
RV, Right ventricle; PA, pulmonary artery.
Published as: J Thorac Cardiovasc Surg. 2009 July ; 138(1): 84–88.

Sponsored Docum
ent Sponsored D
ocument
Sponsored Docum
ent
Nordmeyer et al. Page 10
Table 2Functional outcome
Parameter Before After P value
Cardiac magnetic resonance imaging
Pulmonary regurgitant fraction (%) 20 ± 6 2 ± 1 <.05
RV end-diastolic volume (mL · beat−1 · m−2) 91 ± 13 78 ± 12 <.01
RV end-systolic volume (mL · beat−1 · m−2) 41 ± 10 34 ± 11 .06
Effective RV stroke volume (mL · beat−1 · m−2) 39 ± 3 43 ± 2 .11
RV ejection fraction (%) 59 ± 4 62 ± 5 .43
Cardiopulmonary exercise testing
Peak oxygen consumption (mL · kg−1 · min−1) 25.4 ± 2.3 30.8 ± 3.0 <.01
Maximum workload (W) 128 ± 11 150 ± 13 <.01
Anaerobic threshold (mL · kg−1 · min−1) 13.6 ± 1.3 15.0 ± 1.3 <.05
Respiratory exchange ratio 1.10 ± 0.04 1.10 ± 0.02 .95
All data are mean ± SEM. RV, Right ventricle.
Published as: J Thorac Cardiovasc Surg. 2009 July ; 138(1): 84–88.
Sponsored Docum
ent Sponsored D
ocument
Sponsored Docum
ent
Nordmeyer et al. Page 11
Table 3Echocardiographic follow-up
Peak RVOT gradient (mm Hg) Pulmonary regurgitation
Preoperative 55.6 ± 7.8 2.2 ± 0.5
Postoperative 33.0 ± 3.0 0.4 ± 0.3
Latest follow-up 40.2 ± 5.9 0.5 ± 0.2
P value
Preoperative vs postoperative <.05 <.05
Postoperative vs follow-up .50 .88
All data are mean ± SEM. RVOT, Right ventricular outflow tract.
Published as: J Thorac Cardiovasc Surg. 2009 July ; 138(1): 84–88.
Related Documents











