EFFECT OF HEALTH EDUCATION ON ANXIETY OF ADULT PATIENTS UNDERGOING CRANIOTOMY PROJECT REPORT Submitted in partial fulfillment of the requirements for the DIPLOMA IN NEURO NURSING Submitted by ASHA GOPI G.S CODE N0.5784 SREE CHITRA TIRUNAL INSTITUTE FOR MEDICAL SCIENCES AND TECHNOLOGY TRIVANDRUM NOVEMER 2008

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
EFFECT OF HEALTH EDUCATION ON
ANXIETY OF ADULT PATIENTS UNDERGOING
CRANIOTOMY
PROJECT REPORT
Submitted in partial fulfillment of the requirements
for the DIPLOMA IN NEURO NURSING
Submitted by
ASHA GOPI G.S CODE N0.5784
SREE CHITRA TIRUNAL INSTITUTE FOR MEDICAL SCIENCES AND TECHNOLOGY
TRIVANDRUM
NOVEMER 2008

CERTIFICATE FROM SUPERVISORY GUIDE
This is to certify that Miss. ASHA GOPI G.S has completed the project
work on EFFECT OF HEALTH EDUCATION ON ANXIETY OF ADULT
PATIENT UNDER GOING CRANIOTOMY under my direct supervision for
the partial fulfillment for the Diploma in Neuro Nursing in the University of
Sree Chitra Thirunal Institute for Medical Sciences and Technology,
Trivandrum.
It is also certified that no part of this report has been included in any otherthesis
for processing any other degree by the candidate.
Trivandrum
NOVEMBER 2008
Mrs. SARAMMA P.P
Lecturer in nursing
SCTIMST
Trivandrum-695011
CERTIFICATE FROM CANDIDATE
This is to certify that the Project on EFFECT OF HEALTH
EDUCATION ON ANXIETY OF ADULT PATIENT UNDERGOING
CRANIOTOMY is a genuine work done by me at Sree Chitra Tirunal Institute
For Sciences and Technology, Trivandrum under the guidance of Mrs. Saramma
P. P. It is also certified that this work has not been presented previously to any
university for award of degree, diploma or other recognition.
Trivandrum
November 2008
Asha Gopi G. S
Roll: 5784
SCTIMST
Trivandrum-6950 11
APPROVAL SHEET
This is to certify that Miss. ASHA GOPI G.S bearing Roll no - 5784
has been admitted to the Diploma in Neuro Nursing in January 2008
and she undertaken the project entitled, EFFECT OF HEALTH
EDUCATION ON ANXIETY OF ADULT PATIENT UNDERGOING
CRANIOTOMY, which is approved for the Diploma in Neuro Nursing
awarded by the Sree Chitra Tirunal Institute For Medical Sciences
andTechnology, Trivandrum, as it is found satisfactory.
Trivandrum
November 2008
Examiners
1)-------------------
2)------------~------
Guide(s)
1)-------------~------
2)--------------------
ACKNOWLEDGEMENT
First of all let me thank God of almighty for the unending love, care and blessing especially during the tenure if this study.
I take this opportunity to express my sincere gratitude to Mrs.Saramma. P.P, Lecturer in Nursing, Sree Chitra Thirunal Institute for Medical Sciences and Technology, Trivandrum. For the guidance, she provided for executing this study. Her advices regarding the concept, basic guidelines, and analysis of data were very much encouraging. Her contributions and suggestion have been of great help for which I am extremely grateful, with profound sentiments and gratitude the investigator acknowledge the encouragement and help received from the following person for the successful completion of this study.
I am thankful to Dr Suresh Nair HOD, Department of Neuro Surgery for this constant support and encouragement.
All staffs and Departmental head of Neuro Surgical Intensive Care Unit and Ncuro Surgical Ward were helped for the completion of this study.
Special thanks to library staff of STIMST for granting permission to utilize the library facility.
The investigator investigator wishes to express heartful thanks to parents and near ones for their prayer , encouragement and help throughout this project .
The investigator also takes this opportunity to express the sincere gratitude to all patients who co-operated during the time of data collection.
Asha Gopi.G.S

ABSTRACT
Effect of health education on anxiety of adult patient under going craniotomy.
Craniotomy is an elective neuro surgical procedure.Majority of people
have fear about surgery,post operative complication and out come. Many
studies have shown that pre operative health education reduce post operative
anxiety. Objectives of the study was to find out (1) effect of health education on
anxiety of adult patient undergoing craniotomy and (2) relationship between
anxity and selected variables such as age , sex , level of education , occupation,
and income. The study was conducted in Neuro surgical ICU and Neuro
surgical ward in SCTIMST ,Trivandrum. Sampling technique was alternate
sampling. The sample size was 34. Patients were randomly assigned to
Intervention (patients those seeking health education) and Control group (not
seeking health education). In this study the investigator used standardized
Malayalam version of Speilberger's State Trait Anxiety Inventory , for
assessing the anxiety. Two group pre test and post test design was used.
Individual health education using a self prepared pamphlet was given after
initial assessment. Major finding of the study was patients in the Intervention
group the State anxiety level was reduced both in male and female after surgery
compared than control group.The results support the existing knowledge that
pre operative health education reduces post operative anxiety.

Chapter
1 I
2 II
3 III
4 IV
5 v
6 VI
7 VII
CONTENTS
Title
Introduction
Review of Literature
Methodology
Analysis and Interpretation
Summary, Conclusion, Limitation, Recommendations
References
Appendix

CHAPTER 1
Introduction
No Title Page no
1.1 Introduction 1
1.2 Back ground of the study 2-4
1.3 Need and significant of the study 4 ccc c c cc c c~c~ c•cCc-~cc••••'• """~'~ c cccc•c ccc cwcc we cc c ccc c •~cwcccwcwccc c ccc ccc.ccccccc . .w.cc"~'·'''""'~~····"'"=~·-==·~~-· ccc.c .• ccccccccMcc=cccc~··~··c1·
1.4 ,Statement of the problem 4
1.5 Objectives 4
5
6
6
1.10 Delimitations 7
1.11 rganization of the report 7
2.1 :Studies for redu
CHAPTER 11
Review of literature
cing anxiety by pre -operative education.
.3 Studies on cran iotomy
2.3 Key terms
8-15
15-18
19
CHAPTER 111
Methodology
3.1 Research approach 20
3.2 I Research design 20
3.3 1 Settings 21
3.4 Sampling and sampling technique 21
3.5 Inclusion criteria 21
3.6 Exclusion criteria 21
3.7 Development of tool 21
3.8 Description of tool 22
3.9 Pilot study 23
3.10 Data collection 23-24
3.11 Plan of analysis 24
3.12 Summary 24
CHAPTER 1V
Analysis and interpretation of data
4.1 Distribution of sample according to the demographic 26-32 variables
4.2 Mean, standard deviation and P-value of pre 32-33 operative state anxiety
4.3 Mean, standard deviation and P-value of pre 34-35 operative state anxiety
4.4 Summary 35

5.1
5.2
5.3
SA 5.5
CHAPTER V
Summary, Conclusions, Discussion and Recommendations
!Summary
JMajor findings
!Limitation """"":' ,,,,.,,,,,,,, .. , .. , .. , •.. ~,"'"' ... ,,,,,, ''''"'' . "''""''""'"'''"~' ········~· ...... ··~"'"''·'·"'·"''~'''''~+ ........... ~ ...•
:Discussion ~ -~~'"" ,~. -----'~"""~W---~~~~'"•'••--w--~"'"• ' - .. - ' ''
Recommendation
Reference
Appendix 42-46 ·~~····~······~~···~~'··~~~~~ ..... ~~ ..... ~--~~~····---·«----=-·~-~~.~~-~¥-

CHAPTER -1
INTRODUCTION
1.1 . INTRODUCTION
Craniotomy is the surgical opemng of the skull to gam access to
intracranial structures. This procedure is done to remove a space- occupying
abnormality such as tumor, cyst or vascular malformation. This procedure may
also be needed on an emergency basis to evacuate a hematoma ,relive
intracranial pressure and reverse a herniation syndrome. In this procedure, a
skull incision is made, the bone flap is elevated , dura is opened , and the tumor
is subjected to biopsy or resection. (Hickey, 2003).
Craniotomy is indicated for the diagnosis or treatment of intracranial
lesions demonstrated by neuroradiology , where there is adequate clinical .
indication with modem diagnostic facilities, truly exploratory procedures will
rarely be needed.
Contra - indication may be the nature of lesion, the speed of progression
symptoms and also the patients age and fitness. The few absolute
contraindications include overwhelming infections or abnormalities of blood
coagulation. Poor neurological condition of the patient need to be a
contraindication, since surgical treatment of an intracranial mass will usually be
required before improvement can occur.
1.2. Background of the study
There are many reasons for performing a craniotomy. It may be done as
an emergency following a head injury or brain hemorrhage. This is to remove
blood clots, which are pressing on the brain. As a planned procedure , a
craniotomy may be essential to remove a tumor or to clip an aneurysm. All
operations carry some risks. Proper assessment of the postoperative status of the
patients requires an awareness of the patient's symptoms, so that a comparison
may be made between the pre operative and postoperative conditions. In case of
craniotomy the complications occurs intra -operatively, during the immediate
and late postoperative period. The complications after craniotomy includes
increased intra cranial pressure, vasospasm, cerebral infraction, hydrocephalus,
pneumonia, pulmonary embolism, diabetic insipidus, syndrome of inappropriate
anti diuretic hormone (SIADH) , wound infectios meningitis , seizure, cranial
nerve damage and functional disability. The late post operative complications
includes wound infections, seizure, meningitis, and functional disabilities . Most
2

of the patients are very much anxious due to complications. So reduction of pre
operative anxiety is widely accepted as part of nursing care. (Johnson 1971).
SCTIMST is one of the major center in India where craniotomy is done
successfully. More than 100 cases were done in a month.
Johnson (1971) suggested that accurate pre operative information builds
accurate expectation of surgery which will infact reduce emotional arousal
during surgery. Anxiety is one of the most common emotions seen in health
care setting. Care of anxious client is one of the grater challenges as nurses.
Anxiety is a universal experience and an unavoidable aspect of everyone
life. Mainly anxiety is three types that are mild, moderate, and severe. The
responsibility for giving pre operative information o reduce anxiety is
recognized as a necessary and ongoing responsibility of the nurse as a source of
emotional support ( Oakely 1984)
Anxiety is one of the maJor problem in psychology and result in
considerable functional impairment. State and trait anxiety is one of the most
common features of anxiety. State anxiety refers to emotional reaction
characterized by subjective conscious feeling . of tension, apprehension,
nervousness and worry. In contrast , Trait anxiety deals with individual
difference in the dangerous, and in the frequency that state anxiety is
experienced. Statistics very widely but most agree that anxiety disorders are
3
more common in women than in men. Medical illness and invasive procedure
are often associated with anxiety.
The most common used psychometric self-report inventory is probably
Speilberger's State Trait Anxiety Inventory (STAI - Speilberger's eta1.,1970
).State and Trait anxiety are analogus in certain respect to kinetic and potential
energy. People who differ in trait anxiety will show corresponding difference in
state anxiety depending on the extent to which each of them perceives a specific
situation as psychologically dangerous or threatening and this is greatly
influenced by each individual's past experienced.
1.3. Need and significance of study
Patients who are admitted for craniotomy are found to be more anxious
about the outcome of surgery . These patients also fear about the complications
and are in high emotional stress before surgery. The patient's anxiety level is an
indication of post operative problem . Pre operative anxiety increase the chance
of post operative pain, analgesic consumption, and hospital stay and recovery.
In this situation pre operative teaching plays an important role in
relieving anxiety and reducing anxiety related complications. The patients ask
too many questions about surgery, ICU staying, complications follow up
recovery etc. Hence the investigator felt the need to conduct the study about the
effectiveness of preoperative teaching on anxiety.
4
1.4. Statement of the problem
A study to assess the effectiveness of pre operative teaching on the
anxiety level of patients undergoing craniotomy.
1.5. Objectives
craniotomy.
1. To find out effect of health education on anxiety of adult patients
undergoing craniotomy.
2. To find out relationship between anxiety and selected variables such
as sex, age, education , occupation , and income
1.6 . Operational Definitions
Pre operative teaching :- In this study pre operative teachings describes an
interactive process of providing in formations about surgical process, expected
patients behavior and anticipated sensations and providing appropriate
reassurance and therapeutic listening to patients who are about to under gone
surgrey.
Anxiety :- It is a state of emotion and is measured by using Speilberger's State
Trait Anxiety Scale.
5
Craniotomy: - Is a surgical openmg of the skull to provide access to the
intracranial content for reasons such as removel of tumor, clipping of an
aneurysm , or repair of a cerebral injury , relive elevated ICP , evacuate a blood
clot and control hemorrhage.
1.7. Methodology
Settings Neurosurgical ICU and Neurosurgical Ward in
SCTIMST.
Study design : Pre test and post test design. One group received health
education (intervention group) and other group (control group) not received
health education.
Pre test done before the day of surgery.
Posttest done before the day of discharge.
Sample technique : Alternate sampling.
Exclusion criteria : Children below the age of 18yrs.
1.8. Tool
The investigator assessed the anxiety level of patient by usmg
Speilberger's State Trait Anxiety Inventory standardized Malayalam version.
After assessing the anxiety level the investigator gives health education by
using self prepared pamphlet. The content of health education includes the
6

disease condition, surgery, need for surgery, out come, ICU staying and follow
up. The experts in neurology department in SCTIMST validated this content.
1.9. De limitations
1 . The patients who speak Malayalam.
2. The patients who are conscious , oriented and co operative.
1.10. Organization of the report
Chapter 1 deals with introduction, back ground of the study, need and
significance of the study, statement of the problem, objectives, operational
definition and delimitations. Chapter II deals with review of literature, Chapter
III deals with the methodology, and Chapter IV presents analysis and inter
pretation of data and Capter V include summary, discussion, Conclusion and
recommendation, reference and appendices are given towards the end.
7
CHAPTER 11
REVIEW OF LITERATURE
Review of literature is an important aspect of any research project from
beginning to end. It gives character insight in to the problem and helps in
selecting methodology, developing and also analyzing data. With these in view
an intensive review of literature has been done.
The review of literature relevant to this study IS presented m the
following section.
2.1 Studies for reducing anxiety by pre operative education.
2.2 Studies on craniotomy.
2.1 Studies for reducing anxiety by pre operative education.
Andrews et al;(l999) investigated the impact of treatment information
package on patients being monitored for possible surgical treatment for
temporal lobe Epilepsy.! 00 patients were randomly assigned to eighter a high or
low information preparation condition. Level of anxiety were tested soon after
admission. by using the Hospital Anxiety and Depression Scale (HADS). The
State -Trait Anxiety Inventory(STAI),and a newly devised questionnaire to
assess specific concern and anxieties of epilepsy patients presenting for
monitoring and surgery. Patients assigned to the high- information condition
8
were exposed to an intervention package ,which included v1ewmg a video
depicting two separate interviews with patients who had undergone surgery as
vvell as an information package ,which described the various tests that the
patient would undergo in the course of the monitoring procedure . Patients
assigned to the low - information group were given information that the hospital
provided to all patients in there care. All subjects were then retested on anxiety
levels a few days later. Those in the high - information group showed a
significant in anxiety and depression levels compared with those in low
information group.
Sjoling et al; (2003) observed that specific information given prior to
surgery can help patients obtain better pain relief after total knee
arthroplasty(TKE). Objectives were to study the impact of pre- operative
information on state and trait anxiety,satisfaction with pain management and
satisfaction with nursing care. The study was an intervention study with two
group of equal size (n=30) . The intervention group was given specific
information , while control group received routine information. Pain
assessments were made pre operatively and first three post operative days using
Visual Analogue Scale(VAS). The result of this study suggested that
information influenced the experience of pain after surgery and related
psychological factors. The post operative pain declined more rapidly for
9
patients in the treatment group, the degree of pre operative state anxiety was
lower and they were more satisfied with the post operative pain management.
Asilioglu and Celik ;(2004) the purpose of this experimental study was to
evaluate the effect of pre operative teaching method on anxiety levels of the
patients. This study consisted of 100 patients having open cardiac surgery.Of
1 00 patients 50 were interventional group and remaining 50 were in the control
group. The patients in the interventional group were given a planned teaching
according to the patient education booklet. Patients in the control group were
informed about only pre and post operative routine, by the purpose . of
comparing anxiety level of the patients in the interventional group and control
group. Anxiety of both group were measured on the 3rd day after the operation
by using Self Evaluating questionnaire for state and trait anxiety inventory
scale. The mean post operative state and trait anxiety score in the control group
was slightly higher than the mean ofthe patients in the intervention group.
Deyirmenjian et al ; (2006) assessed the impact of pre operative patients
education on anxiety and recovery of patients undergoing open heart surgery.
This quasi- experimental study the patients were randomly assigned to a
experimental (n=57) on a control group (n=53) group. The patients in the
experimental group received special education and the control group followed
the routine hospital protocol. Anxiety was assessed using the Beck Anxiety
Inventory Scale (BAIS).Borderline statistical significance was noted for the
10
experimental group in terms of pre operative and post operative anxiety. It is
also reported that the experimental group had a shorter time from awaking to
extubation.
Vanzurren et al ; (2006) studied the potential beneficial effect of an
information brochure on patients undergoing a gastrointestinal endoscopy for
the first time. Patients were randomly assigned to an experimental group
receiving the brochure at least 1st day before the gastroscopy (n=4 7) , or control
group not receiving the brochure (n=48) . The result showed that all
experimental sujects , those receiving the brochure experienced less anxiety
before the gastroscopy and after wards they reported grater satisfaction. Low
bunters (those not seeking information) as compared to high blunters showed
extra reduced anxiety after reading the brochure. High moitores (those seeking
information) receiving the brochure showed reduced anxiety during the
gastroscopy as compared to low monitores.
Nemi-Murola et al ; (2007) studied about patients often suffer from
inadequate treatment of post operative pain. The purpose of this study was to
survey the factors affecting patients · satisfaction with post operative pain
management . A questionnaire with 41 items given on the 3rd postoperative day
to 102 patients undergoing major orthopedic or vascular surgery. Intensity of
pain was assessed using a 10-cm visual analogue scale (VAS) and given
analgesics were recorded. Nurse (n=74) working on the ward received a
11
questionnaire concernmg attitudes towards management of pam. The
questionnaire were returned by 75.5% of the patients and 86.3% of the nurses.
28% of the patients agreed having hard pain during the day of operation and
39.3% during the 1st post operative night. 80% of the patients were satisfied
with pain management their satisfaction correlated significantly with received
the pre operative information. Pre operative interview is very important tool to
receive and give information concerning post operative pain management.
Beapupre et al ; (2004) observed that the effectiveness of a pre operative
exercise\ education program following primary total knee arthroplasty (TKE) .
I 31 subjects were randomized to either the control (n=66) or treatment (n=65)
group 6weeks before TKE surgery. Patients in the treatment group underwent a
4 week exercise \educational program before surgery. All subjects were
assessed 6 weeks pre operatively (before the exercise \education intervention)
immediately pre operatively (after the exercise \education! intervention) ,and
3,6andl2 months after surgery utilizing the western Ontario McMaster
osteoarthritis Index. Subjects were similar in demographic characteristics and
all measures at the baseline assessment.
Davis et al ; (1994) to examine the effects of coping style and type of
preparatory informational treatment on cardiac catheterization patient anxiety.
Pre test - post test randomized control group design. 145 adult patients (107
men and 38 women) scheduled for their first cardiac catheterization. Age range
12
was from 34 to 78 yrs. Patients randomly assigned to monitoring (information
seeking) or blunting (information avoiding ) . Subject's coping style was
assessed by mans of Miller's Behavioral Style Scale. Subjects anxiety was
assessed by means of Speilberger's A-Trait and A-State Inventory.Sbjects
anxiety was assessed before and after intervention (timel&time2) and before
and after catheterization (time3& time4) . Monitors who received the procedural
--sensory modeling video treatment and blunters who received the procedural
modeling video treatment reported significant reductions in A-State anxiety .At
time 4 monitors and blunters in each of the treatment group reported a
significant decrease in A-State anxiety. Female monitors and blunters reported
significantly higher A-State anxiety level than male .
Blay and Donoghue (2005) observed the objectives of randomized
controlled study were to determine if pre admission patients education affects
post- operative pain levels , domiciliary self care capacity and patient recall
following a laproscopic cholecystectomy (LC) .Sampling is 93 elective
Lcpatients. Participents were randomized to receive the standard pre admission
program (SP) or an individualized , education intervention (EI). A pre -
operative questionnaire was administered in the pre admission clinic to
determine participants' knowledge of LC and post operative management.
Telephone follow-up and postoperative questionnaire were conducted
approximately 14 days post discharge. EI participants experienced lower pain
13
levels and significantly grater recall of provided information . However no
significant difference were found between the control and intervention group for
domiciliary self-care. Pre education intervention helps reduce post operative
pain levels following LC and significantly increases patients' knowledge of self
care and complication mnagement.
Lilja et al ; (2003) evaluate the effects of extended pre operative
information , given by anesthetic nurses, on pre operative stress in patients
operated on for breast cancer or total hip replacement (THR) .46 consecutive
patients scheduled for surgery for breast cancer and 55 for THR , were
randomized in to two groups which were given different modes of pre operative
information . Patients in the controlled group were informed about pre and post
operative routine by ward nurse . Patients in the intervention group were given
extend formalized information by an anesthetic nurse . Wilcoxon rank sum test
was used to show relations between variables . There were no significant
differences between the intervention group and control group for patients with
breast cancer or for the patient with THR . Breast cancer patients in the
intervention group were significantly more anxious than THR patients in the
intervention group (p<O.Ol). Breast cancer patients in the intervention group
showed the highest anxiety scores on the Hospital Anxiety and Depression
Scale (HADS) on the day of surgery . This information may reflect an increased
level of anxiety due to the extend information given pre operatively . The
14
information may have negative effect on breast cancer patients , resulting in an
increased state of anxiety.
2.2 Studies on Craniotomy.
Brackmann et al ; (2007) conducted a to evaluate the long-term facial
function of patients after translabyrinthine vestibular schwannoma [VS] surgery
and identify factors that influence these outcomes. A retrospective review was
performed that included 580 consecutive patients who underwent
translabyrinthine craniotomy for removal of VS. A total of 512 patients who
underwent primary microsurgical treatment of sporadic unilateral VS met
inclusion criteria. Patient and tumor characteristics as well as perioperative
complications are described. Perioperative and long-term facial function were
evaluated in 392 patients who had at least 1-year follow-up. Complication rates
after translabyrinthine craniotomy for VS are low. Patients with smaller tumors
have significantly better postoperative facial function than those with larger
tumors. Excellent long-term facial function can be expected in the majority of
patients who undergo microsurgical removal of VS via the translabyrinthine
approach. Alternative treatment strategies may need to be developed for the
treatment ofVS > 3.5 em in orderto maximize postoperative facial function.
Kourbeti et al ; (2007) conducted a retrospective cohort study to
determine the incidence, bacteriological features, and risk factors for
postcraniotomy meningitis. Patients older than 18 years who underwent
15
nonstereotactic craniotomies between January 1996 and March 2000 and who
survived for more than 7 days were included. Operations for placement of burr
holes and shunts were excluded. Records of the first 30 postoperative days were
abstracted. Host factors, types of craniotomy, and pre- and postoperative
variables were evaluated as risk factors for meningitis. Among 453 patients,
there were 25 cases of meningitis. Eight out of 12 culture-positive cases were ·
the result of gram-positive cocci. 420 (92%) patients received antibiotic
prophylaxis, most commonly a first-generation cephalosporin. In multivariate
analysis, the risk of meningitis was increased by surgery that entered a sinus ,
and increases in the number of days of external ventricular drainage and
intracranial pressure monitoring. Access of upper airway bacteria to the surgical
wound, host factors as expressed by the American Society of Anesthesiologists
score, and duration of device-related postoperative communication of the
cerebrospinal fluid and the environment are major risk factors for postoperative
meningitis after craniotomy.
Curry et al ; (2005) conducted a study was to determine the risk of
adverse outcomes after contemporary surgical treatment of meningiomas in the
US and trends in patient outcomes and patterns of care. The study were
performed a retrospective cohort study by using the Nationwide Inpatient
Sample covering the period of 1988 to 2000. Multivariate regression models
with disposition end points of death and hospital discharge were used to test
16

patient, surgeon, and hospital characteristics, including volume of care, as
outcome predictors. Multivariate analyses revealed that larger-volume centers
had lower mortality rates for patients who underwent craniotomy for
meningioma. Adverse discharge disposition was also less likely at high-, and a
significantly less frequent adverse discharge disposition. In-hospital mortality
rates decreased 61%, from 4.5% in 1988 to 1.8% in 2000. Reductions in the
mortality rates were largest at high-volume centers (a 72% reduction in the
relative mortality rate at largest-volume-quintile centers, compared with a 6%
increase in the relative mortality rate at lowest-volume-quintile centers). The
number of US hospitals where craniotomies were performed for meningiomas
increased slightly. The mortality and adverse hospital discharge disposition
rates were lower when meningioma surgery was performed by high-volume
providers.
Mark Bernstein ; (200 1) observed that routinely performed awake
craniotomy for intra-axial brain tumors with low complication rate and low
resource utilization. A pilot study was initiated to assess the feasibility of
performing craniotomy for tumor resection as an outpatient procedure. A
rigorous protocol was developed and adhered to, based around the patient's
arrival at hospital at 6:00 am, undergoing image-guided awake craniotomy with
cortical mapping, and being discharged by 6:00 p.m. During the 48 month
period from December 1996 to December 2000, 245 awake craniotomies were
17
performed and of those, 46 patients were entered into the outpatient craniotomy
protocol. Pathology in the 46 intent-to-treat group was: 21 metastasis, 19
glioma, and six miscellaneous. Four patients required conversion to inpatients
and one patient was readmitted later the same evening due to headache. Thus
41146 patients successfully completed the protocol (89%). There were five
complications in the 46 intent-to-treat group (10.9%). Outpatient craniotomy for
brain tumor is a feasible option which appears safe and effective for selected
patients, the procedure may be psychologically less traumatic to patients than
standard craniotomy for brain tumor.
The key terms used for search.
http://www.ncbi.nlm.nih.gov\pubmed
Table 2.1
Key terms used for literature search
Key Terms No of articles Effect of health education on anxiety of patients under gone surgery.
123 Craniotomy studies on 2000.
1023 Study related to effect of pre operative and post operative health education. 123
18

CHAPTER 111
METHODOLOGY
This chapter deals with research approach, research design,
Setting, the sample and sample technique, development of tool, description of
tool , pilot study , data collection and plan of analysis.
The aim of the study was:-
• To find out the effect of health education on anxiety of adult patients
undergoing craniotomy.
.. To find out relationship between anxiety and selected variables such us
sex, age, education level, occupation , income etc.
3.1 Research approach
3.2 Research design
Pre experimental study
For full filJing the objective of the study one group pre test- Post test was
used. The schematic representation shown in figure 3 .1. In the figure 01
represent pre test , 1 represent is the health education , 02 represent the post
test.
01 I 02
19

Figure 3.1 Two - group pretest posttest design
3.3 Settings:
The study was conducted in the Neuro surgical ICU and Neuro surgical
ward at SCTIMST; Trivandrum. The rationale for selecting this hospital was
that this is one of the superspeciality hospital in India doing craniotomy. In this
hospital on an average, 100 craniotomy cases are done every month on a regular
basis. More over, the investigator was familiar with this hospital.
3.4 Sample and sampling technique:
Alternate sampling technique was used for selecting the sample. All the
patients who met the inclusion criteria were selected. The total duration of the
study period was September- October 2008.
3.5 Inclusion criteria :
• Both male and female patients undergone craniotomy.
• Those patients who are co operative, conscious and oriented.
• Those patients who know Malayalam.
3.6 Exclusion criteria :
Children below the age of 18 yrs.
3. 7 Development of tool
An extensive review and study of literature helped in preparing a health
education pamphlet and it was scrutinized and approved by experts in Sree
20
Chitra Thirunal Institute Of Medical Science and Technology. In this study the
investigator used standardized Malayalam version of Speilberger's State Trait
Anxiety Inventory of assessing pre operative anxiety and to assess post
operative anxiety which contain 36 questions.
3.8. Description on tool :
The tool used in present study consists of the following parts:
Part -1
This part contains demographic data including age, sex, education, occupation
and income.
Part -11
It consists of Speilberger' s State Trait Anxiety Inventory which is popular
instrument for measuring anxiety. It has been. used previously in many
researches to assess emotional reaction to surgical procedure. This inventory
. consists of 36 self reporting items and has two parts. The State anxiety and Trait
anxiety.
Part -111
Patients were randomly assigned to experimental and intervention group.
After assessing the anxiety level, health education was given to the intervention .
group. The health education pamphlet contains details about the disease
condition,Surgery, need for surgery and ICU stay.
21
3.7 Pilot study :
Pilot study was conducted from September 15th to 25th, 2008. The aim of
the study was to assess the effect of health education on anxiety of adult patients
undergoing craniotomy. The study was conducted among five patients, both
male and female between the age group of 18 to 60 yrs. The tool used is State
Trait Anxiety Inventory (STAI) with 36 questions. The questions were asked in
Malayalam. Total time period required was 30 minutes for a patient. Pilot study
reveled that post test anxiety score was lower than pre test anxiety. After
making necessary correction in the scoring part of the tool the main study was
conducted.
3.8 Data collection :
For data collection formal permission was obtained from the authorities. Period
of data collection from September 2008 to October 2008. Data was collected
from patients in the Neurosurgical ward and Neurosurgical ICU.
The investigator first introduced herself and explained need and purpose study
to the patients. After getting consent from the patients, anxiety level of the
patients was assessed with the help of Speilberger's State Trait Anxiety
Inventory. After this health education was given to patients in the intervention
group by using self-preparing health education pamphlet. The patients were also
given the opportunities to clear their doubts. In case of experimental group
22

health education is not received. On the 1st post operative day, both groups
(Intervention and control group) anxiety were assessed by using the same
structured anxiety scale, to find out the effectiveness of health education in
reducing the anxiety level .
3.9 Plan of analysis :
A plan of data analysis was developed by the investigator after the pilot
study. A master sheet was prepared with the score obtained in the STAI.
(Descriptive statistics is used to analyses the data).
3.10 Summary :
This chapter deals with research approach, the study design, setting of the
study, sample and sampling technique, development of tool, data collection
and plan of analyze.
23
CHAPTER IV
Analyse and interpretation of data
This chapter presents the analysis and interpretation of data collected
from 34 patients who underwent craniotomy at SCTIMST , Trivandrum.
Analysis is a process of organizing and synthesizing in such a way that project
elicit meaning from collected data. The aim of the research study was to assess
pre operative anxiety of patients undergoing craniotomy and to assess the effect
of pre operative teaching on the anxiety level of patients undergoing
craniotomy.
Interpretation refers to the process of making sense of the results and of
examining the implication of the findings with in a broder content.
The data were coded , entered in Microsoft excel and analysed using epi info
version 3.2 .
The finding of the study were arranged and analyzed under the following
section.
4.1 Distribution of Sample according to the demographic
variables.
4.2 . Mean , standard deviation and P. value of pre -operative
anxiety.
24

4.3. Mean, standard deviation and P. value of post- operative
state anxiety.
4.1 . Distribution of sample according to the Demographic
variables.
( 1 ) Distribution of sample according to sex.
Table 4.1
Sex Male
14 41.2%
Total 34 100%
The data given in table 4.1 shown that 58.8%of sample consisted of male.
25
4.1 The same data gives • f p n
35
30
25
20
15
10
-rT
• 3-D Column 1 • 3-D Column 2 • 3-D Column 3 • Male • Female • Total
FREQUANCY
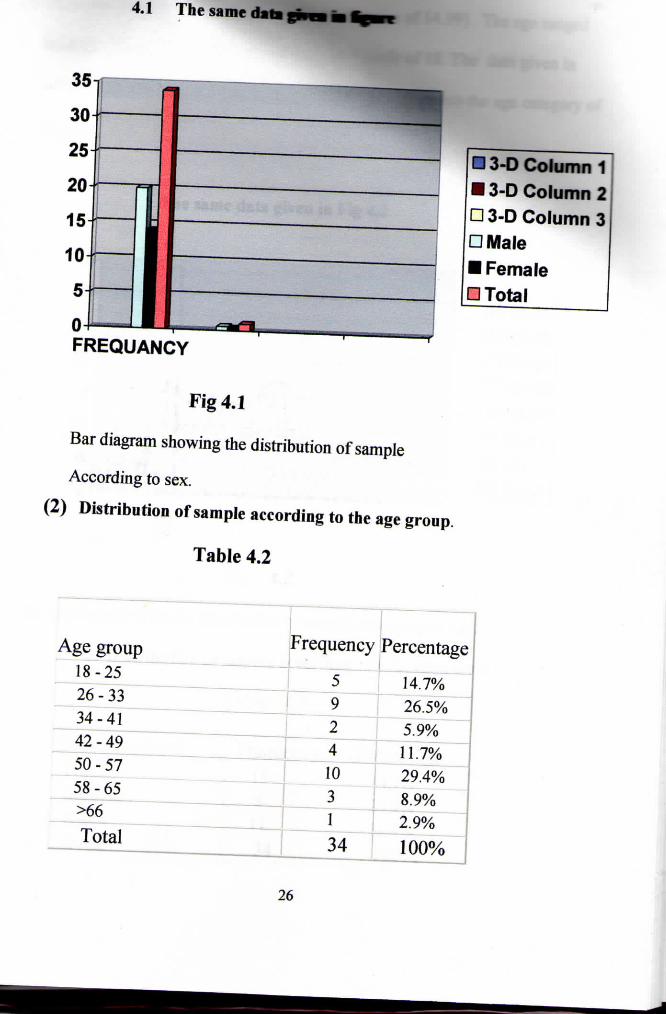
Fig 4.1
Bar diagram showing the distribution of sample
According to sex.
(2) Distribution of sample according to the age group.
Table 4.2
Age group Frequency Percentage
18-25 5 14.7% 26-33 9 26.5% 34-41 2 5.9% 42-49 4 11.7% 50-57 10 29.4% 58-65 3 8.9% >66 1 2.9% Total 34 100%
26

The mean age of the sample was 41.71 (with mean of 14.99). The age ranged
between 18 to 75. With medial age of 42 and mode of 18. The data given in
table 4.2 shown that 29.4 percentage of subjects belonged to the age category of
50 to 57.
The same data given in Fig 4.2
35
30
25
20
15
10
5
0
j j
-j
m II .i .i frequancy
Fig 4.2
• 18-25 • 26-33 • 34-41 • 42-49 • 50-57 • 58-65 • >66 • Total
Bar diagram showing the distribution of sample according to age.
3. Distribution of sample according to education level.
Table 4.3
Education level Frequency Percentage Primary 15 44.1% Secondary 8 23.5% Higher 11 32.4% Total 34 100%
27
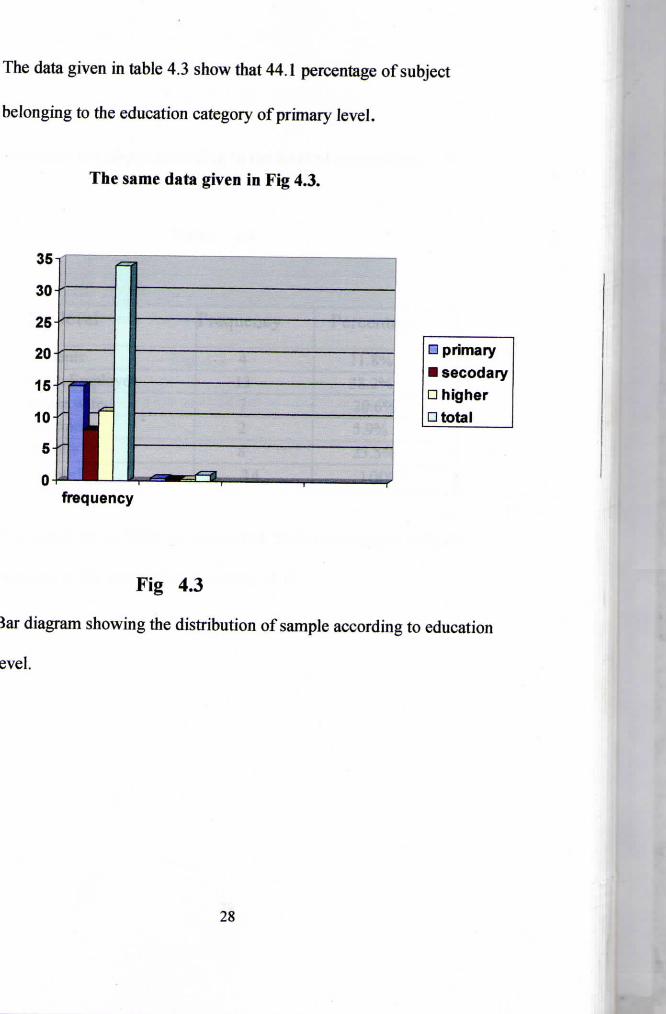
The data given in table 4.3 show that 44.1 percentage of subject
belonging to the education category of primary level.
The same data given in Fig 4.3.
• primary • secodary • higher • total
frequency
Fig 4.3
Bar diagram showing the distribution of sample according to education
level.
28
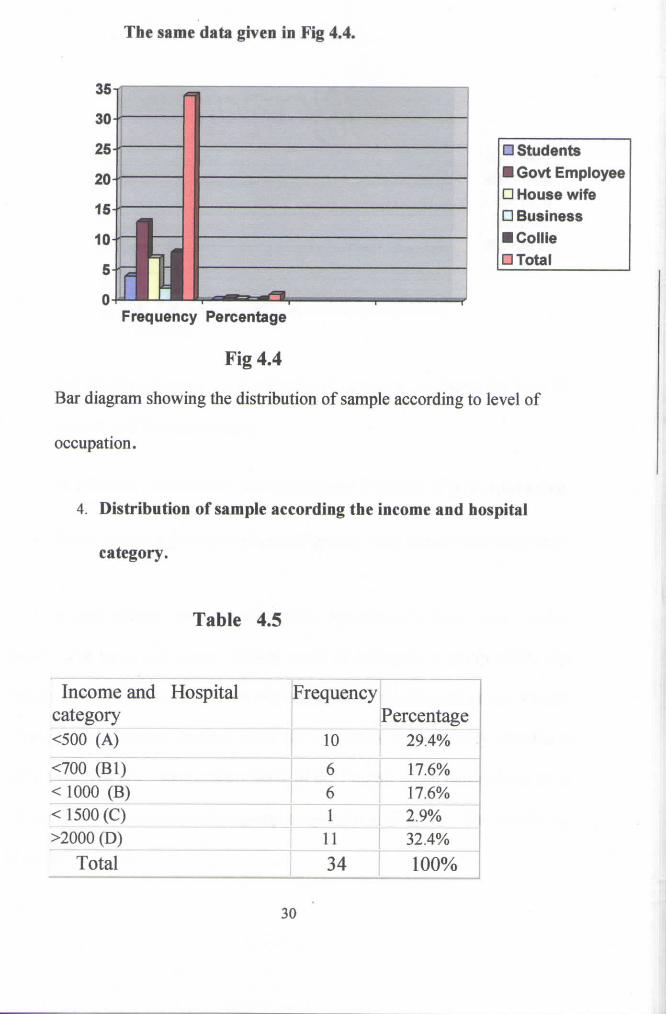
The same data given in Fig 4.4,
• Students • Govt Employee • House wife • Business • Collie • Total
Frequency Percentage
Fig 4.4
Bar diagram showing the distribution of sample according to level of
occupation.
4. Distribution of sample according the income and hospital
category.
Table 4.5
Income and Hospital category
Frequency Percentage
<500 (A) 10 29.4%
<700 (Bl) 6 17.6% <1000 (B) 6 17.6% < 1500 (C) 1 2.9% >2000 (D) 11 32.4%
Total 34 100%
30

The same data given in Fig 4.5
3 5 —̂_
30
25
20 -
15
Frequency
Bar diagram showing the distribution of sample according to the level of
income and hospital category
4.2 Mean , standard deviation and P value of pre-operative
State anxiety score of Control group and Interventiongroup.
The state anxiety was measured using Speilberger's State Trait Anxiety
Scale . The mean pre - state anxiety score of Intervention group (47.7) was
higher than the mean pre - state anxiety score of the Control group (44.63).
However an unpaired students t-test did not show a statistically significant
difference. The pre - state anxiety score of the Control group ranged from 29 to
64 and that of the Intervention group ranged from 27 to 62. The details are
given in Table 4.6.
31
• A<500 • BK700 • B<1000 • C<2000 • D>2000 • total
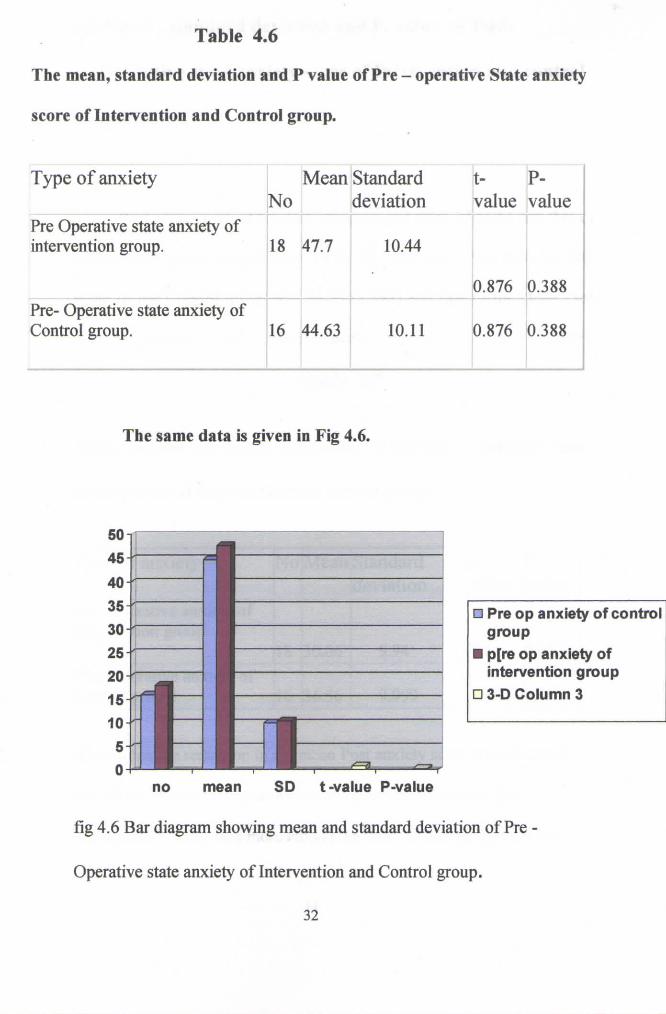
Table 4.6
The mean, standard deviation and P value of Pre
score of Intervention and Control group.
- operative State anxiety
Type o f anxiety No
Mean Standard deviation
t-value
P-value
Pre Operative state anxiety of intervention group. 18 47.7 10.44
0.876 0.388 Pre- Operative state anxiety of Control group. 16 44.63 10.11 0.876 0.388
The same data is given in Fig 4.6.
• Pre op anxiety of control group
• p[re op anxiety of intervention group
• 3-D Column 3
no mean SD t-value P-value
fig 4.6 Bar diagram showing mean and standard deviation of Pre -
Operative state anxiety of Intervention and Control group.
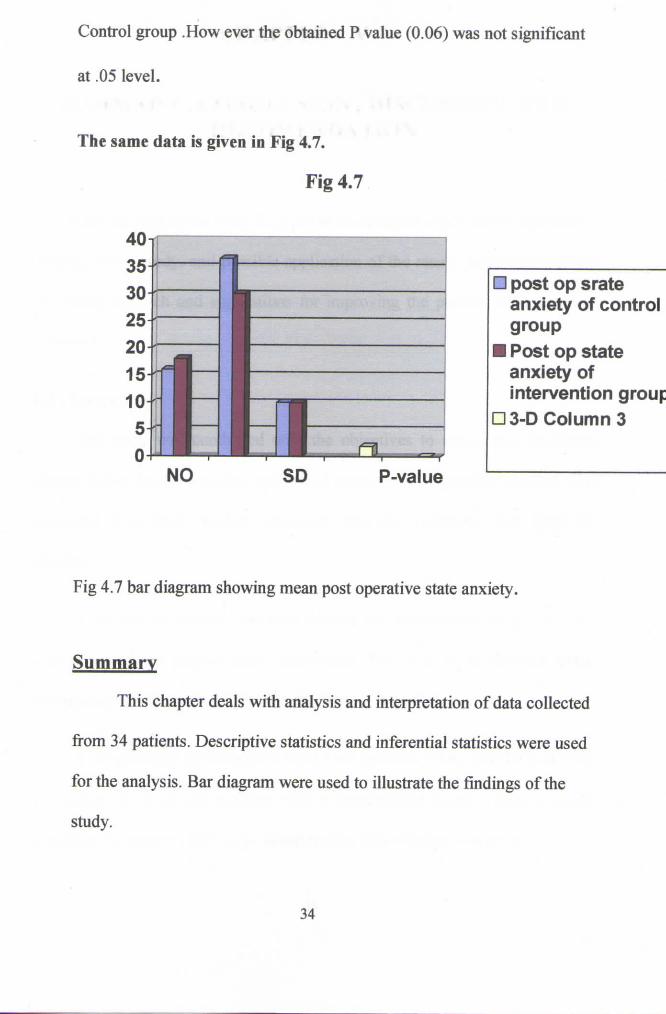
Control group .How ever the obtained P value (0.06) was not significant
at .05 level.
The same data is given in Fig 4.7.
Fig 4.7
-rr
l-i-^-NO S D P-value
• post op srate anxiety of control group
• Post op state anxiety of intervention group
• 3-D Column 3
Fig 4.7 bar diagram showing mean post operative state anxiety.
Summary
This chapter deals with analysis and interpretation of data collected
from 34 patients. Descriptive statistics and inferential statistics were used
for the analysis. Bar diagram were used to illustrate the findings of the
study.
34
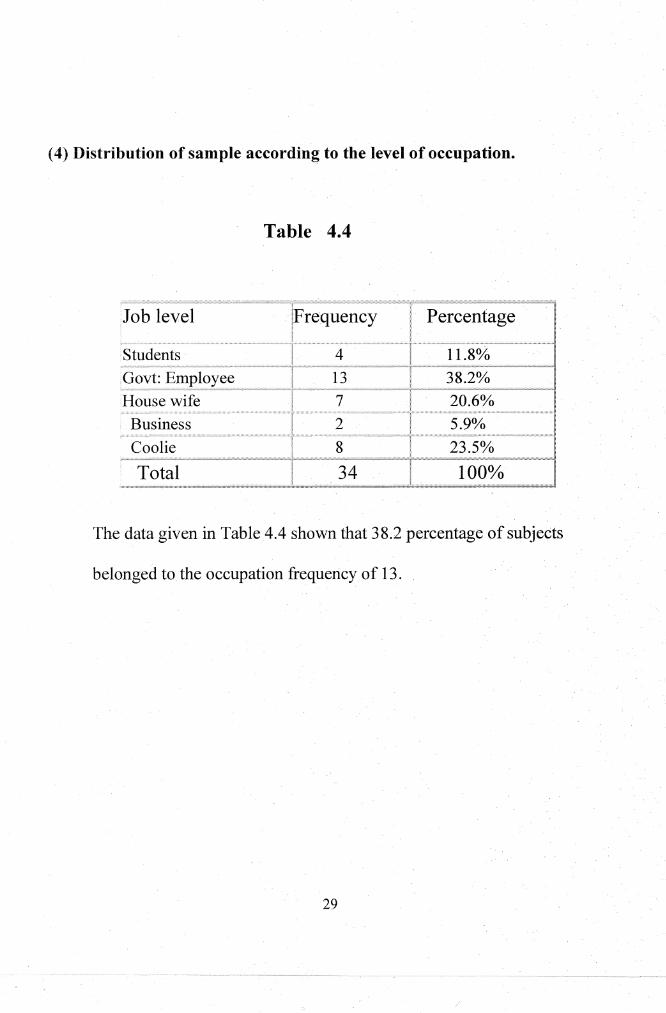
( 4) Distribution of sample according to the level of occupation.
Table 4.4
m-~~'"''"''c'"'~~'"""'""'''~ w• ''••••·~----';,;,,,,,;-~,;"""'""'• ....... IF~~q~~~~y· I. Job level Percentage [
Students 4 11.8% Govt: Employee 13 J8.2% House wife 7 20.6% Business 2 5.9% Coolie 8 23.5%
Total 34 100%
The data given in Table 4.4 shown that 3 8.2 percentage of subjects
belonged to the occupation frequency of 13.
29

4.3 Mean , standard deviation and P. value of Post-
Operative state anxiety score of Intervention and control
group.
Post state score of Control group ranged from 22 to 53 and that of
Intervention group ranged from 19 to 53. The mean Post state anxiety
score of the Control group was 36.56 (9.999) and that of the mean Post
state anxiety· of Intervention group 30.06 (9.94).
Table 4.7
Mean, standard deviation and P.value of the Post operativ~ state
anxiety score of Intervention and control group.
Type of ar.xiety jNotrvfeaniStandard lt-1 ' ;
: jdeviation lvalue . . .. ..... ... . .. .. ............. . -····r----·· .... _;c---c·""--"··------•: ........... ~-----·····--···· -- ................ _._, _______ _ Post Operative anxiety of I11tcrvention group
118 ]30.06 : 9.94 ;1.9 J0.067 ...................... ,.. . .. ........ . ... ' ............ :i"'"'" ................. ,................. . ........................ " ........................ .
Post-Operative anxiety of . . • l ~
~S?tr~!J?l~~:~~-~M-······· ...... ................ -~-~--~·--~~-~~~~--J ...... -~~?.-~~----··-~%ili~NJJ _· ~----~··--j~_;g67 _ J
A considerable reduction in the mean Post anxiety score was observed
among the Control group as well as the Intervention group. The
r9ductionof am:iety was.: more among the Intervention group than the
CHAPTER- V
SUMMARY , CONCLUSION , DISCUSSION AND RECOMENDATION
A brief account of the study is given in this chapter which cover objectives,
findings of the study, and possible application of the result. Recommendations
for future research and suggestions for improving the present study are also
presented.
5.1 . Summary
The study was conducted with the objectives to assess pre- operative
anxiety before health teaching and and to assess post - operative anxiety. The
structured State-Trait Anxiety Inventory was for collecting data from 34
samples.
A review of related literature helped the investigator to get a clear
concept about the project topic undertaken , as well as to develop tools,
methodology of the study and decide the plan for data analysis.
A standardized Speilberger's State Trait Inventory was used for assessing
the anxiety level of the patients with a standardized questionnaire , health
education on surgery, ICU stay, complication and outcome was given.
35

The study was conducted in SCTIMST , Trivandrum ,during the period
of Sep - Oct 2008. The sample comprised of 34 patients, both males and
females. Between the age group of 18 -75 years. Tool used for data collection
patients demographic data, Speilberger's State Trait Anxiety Inventory. State
anxiety scale consisted of 18 questions and Trait anxiety scale consisted of 18
questions.
5.2. The major findings of the study
The study results showed that there was a statistically significant
reduction in the mean post state craniotomy anxiety of the samples .
5.3. Limitation
1. Study was limited to the SCTIMST ,Trivandrum
2. Study was conducted in a single group of patients admitted for craniotomy.
3. The study was conducted only among patients who could read Malayalam.
5.4 . Discussion
Assessment of anxiety level of patients who undergoing craniotomy is
very impmiant , because these patients are anxious about surgery, ICU stay ,
complication, outcome etc.
According to Andrewes et al ; (1999) Asilioglu and Celik (2004)
VanZuuren et al ; (2006) Nemi-Murola et al ;(2007) pre operatively patients had
36
higher level of anxiety than post operatively. The findings of the present study
is comparable to these results. The present study showed that health education
seemed to decrease the anxiety level post operatively
5.5. Recommendations
The following recommendations are made on the basis of present study.
• Similar study can be reported by increasing the sample size.
• True experimental study to assess the effectiveness of pre operative
teaching on anxiety level of patients before and after surgery can done.
5.6 . Conclusion
Based on the findings of the study , the following conclusion were drawn.
With this limited number of patients it is not possible to generalize
findings.
There is need for study studies involving more number ofpatients
validate the findings.
37

REFERANCE
1. Patient satisfaction with post operative Hickey , J.V.(2003) The
clinical practice of Neurological and Neurosurgical Nursing . (51h ed),
USA Lippincott Williams and Wilkins.
2. Andrewes , D., Camp , K., Kilpatrick ,C.,Cook,M. (1999), The
assessment and treatment of concerns and anxiety in patients undergoing
pre surgical monitoring for epilepsy. Epilepsia, 40(11), 15.35-42.
3. Sjoling , M., Nordhal, G., Olofsson , N., Asplund,K.(2003) , The
impact of pre operative information on state anxiety , post operative pain
and satisfaction with pain management. The patient Educ Couns, 51(2),
169-76.
4. Asilioglu , K., Celik , S.S. (2004) , The effect of pre operative
education on anxiety of open cardiac surgery patients. Patient Educ
Couns, 53(1), 65-70.
5. Deyirmenjian, M., Karam, N., Salameh, p.(2006), Pre operative
patient education for open- heart patients :a source of anxiety?. Patient
Educ Couns, 62(1), 111-7.
6. VanZuuren , F.J., Grypdonck , M." Crevits ,E., Vande Walle , C.,
Defloor , T. (2006), The effect of an information brochure on patient
38
under going gastro intestinal endoscopy ; a randomized controlled study.
Patient Educ Couns ,64(1-3), 173-82.
7. Niemi"'Murola, L., Poyhia , R., Onkinen,K., Rhen,B., Makela ,A.,
Niemi , T.T. (2007), pain management- effect of pre operative factors.
Pain manag Nurs, 8(3), 122-9.
8. Beaupre, L.A., Lier, D., Davies , D.M., Johnston,D.B.(2004), The
effect of a pre operative exercise and education program on functional
recovery , health related quality of life, and health service utilization
following primary total knee arthroplasty.lRheumatol, 31(6),1166-73.
9. Davis ,T.M., Maquire ,T.O., Haraphongse , M. (1994) , Prepadng
adult patient for cardiac catheterization : informational treatment and
coping style interactions. Heart Lung, 23 (2), 130-9.
10. Blay ,N., Donoghue,]. (2005) , The effect of pre admission
education on domiciliary recovery following laproscopic
cholecystectomy. Aust J Adv Nurs, 22(4), 14-9.
11. Lilja , Y., Ryden , S., Fridlund , B. (2003), Effect of extend pre
operative information on Peri operative stress: an anesthetic nurse
intervention for patients with breast cancer and total hip replacement.
Patient Educ Couns, 50(2), 108-11.
39
12. Brackmann D., Cullen, R.D., Fisher , L.M.(2007), Facial nerve
function after translabyrinthine vestibular schwannoma surgery.
Otolaryngol Head neck surgery,136(5), 773-7.
13. Kourbeti , I,S., Jacobs , A.V., Koslow, M., Karabetsos ,D.,
Holzman,R.S.(2007), Risk · factor associated with post craniotomy
meningitis. Neurosurgery, 60(2), 317-25.
14. Curry , W.T., Me Dermott, M.W., Carter,B.S., Barker, F.J.(2005),
Craniotomy for menmgwma in the US between 1999 and 2000.
Decreasing rate of mortality and the effect of provider caseload.
Neurosurgery, 102(6), 997-86. s
15. MarkBevnstein , A.(200 1 ), Out patient craniotomy for brain tumor:
A pilot feasibility study in 46 patients. The Canadian Journal of
Neurological science, 28(2), 120-124.
40
APPENDIX

LaD c u.u w E§<.9 Eill9LW 5P> ® · o ~ lrorv <.9 o ~aD '€P ~ Q) w \¥) C€P ~ u.u ~ Q) 0 ra lJ" L s l C€P ~ L w QW
o ~a:D'€P~s® ( [J"lCW ~Lf&cft u.D ~<9G'L(f)Ca:Dg)fU~WL<IDUD ~Q)(Q) ~u.D ~Q)0 S<.9liCJLrillQ)<Q19)
ICJ~WC~'€P ~La:D'€P<.9<.9 S<.9~E§Em9LW (lS~lgqlS~my) WS~CmJg) u.D~<9Gla:D0
~8cmg,ts,(Q) gl)A>UOg)~CE9
·o~cg>C2JJ9~ S<.9l'€P S<.9~E§Effi9LW o~o8£WLCW
o~E§<9G'~m.DIU9 Q)<.9ru ~<IDUD ~8c0 ~ICJg)L08a:Dts,<ID ~FOUOg)ftc~ E§<.9Effi9LW ·'€P~a:Doru
~CUJg)LOf&Lcw oQ)ruLru <Q.w ~L'ffi2.U9<.9~ cftg)LS<ID 'crag)lJULOCrv<.9 SPWIClonJJ
w £CD rv <.9 ~R>te'l1!il9 ® ·o ~ lrorv <.9 o ~aD '€P ~ Q)(Q) ~LaD '€P<.9 <.9 s <.9 ~ E§Em9 LW ~R>te' mil9 ®
£WCCTU g) f\1) S<.9 ~<.9L<99'LSC ({1) g) IU91s, ~ <Q.w OFI)U Qf) g)~ WL<ID QJJ2) . ~(ill~ (99l La:DC (JU(U) ~ c ({1) s (Q)
mcrtl9~ill9QW 5P>® "Oill9<99'LE§~'€P f&L(f)Ca:Dg)fU~ ( ~Lcruc8ts,IU9) o~ru<.9 ~u.D~Q)0
oFI)UQI)g) ~WL<IDQW { o ~lrorv<.9 o(99lts,UJ o ~ru0CQ)g)tSC<ID o ~a:DQI)Is,0 ~WC0~FOU ~ Q) ~ru)
· ~ u.u ~ lrorv<.9 o(99lts, w caD g)C 0 '€P 1s, (f) c 2.1 'caD g) c 0<.Q.l.Q)C 0<.9 LS ~ 0 <.Q.lQ) <.9 (f) c 2.1 u.u ~ lrorv <.9
a:DL C€P1<ID1 ,(WQI) ~La:DICJ(Q) ICJ <.9LrDCQ)L(Q)Qlf)) O(U)rDL8 s <.9 ~ ({1) a:DL '€P1(Q) 1 ,(WQI)
o CU> ru LEI @ & t ru got trJ t <9e> em L CEJ~l (Q)l £ill QJ)
·~<.Ll)~sft<.9ru2J~WQW rDLUDUJu ocwc~w~ru ~L(Q.lQ)8c0~Q)ru<.9 ·~~0LCW~IU9
~C<9G'LQ)C cwocw too ~<99'ra 1119 ~ WLICJ c '€P f& La:DQI) 1 <Q.w w <.9 L<ID u.u ill9<.9 c <.Q.lQ) (f) c 2.1
~ w IDu ~LOCf'U g) ra <ID m ~ 0 ·o aD Is, ill9 FOU ra L2> QW 9J9C aD a:DL '€P1<ID1 £W Qf)
~\¥)'€Pm~0 ICJ<.9LOCf'Ug)ICJ(Q) o~<99'\¥)'€PL(f)CQ)g) %06 l0SCa:Dg)LUJ'€Jl1g) 9J9CaDL'€Pl<IDl,(WQI)
u.u ~ lrorv<.9 ~La:DICJ w ~ L<ID u.u ~ <99'1s, w 1¥) '€P a>~ 0 ~ ~ (Q1Q) '€P<99' £CD raw
(Locs~cw LtrJSC«Dg)LWCEJ~lg) )guR>Oog)~CE9 10<9L«<Ho(Q) 9J9CW(f}u
· o ~ <99'La:Dcuucw ~c <9G' £CD o ~ '€P o ~aD CffiQI) <Q.w o ~ aDLSru g) s <.9 ~ E§ Effi9 LW
W')Effi9 ~ Q) c CEP u.u ~ a:Doru m<.9 c <ID ·o ~aDo~ '€P 5P> ® Q)<.9 ru LffiL Q) ru ~ Q) ~ ~c CQ.lQl9 o L QW
WJEffi9~Q)C'€P ~~ o~rwu-u o~ru~~0 ~a:DLCEP1<ID1£WQI) ·o~ill9C'€P o~({l)CffiQI)(Qm}
o ~ aDLSru g) \¥) c rw g)~ <99'\¥) '€Jlg) ~ (ll)(l}u a:DL '€P1<ID1 £W Qf) o ~ <99'.1¥) '€PL(f) c Q) g) c ~ UJu
w> afl9 r Q) cca> aug (99)g) LO> L<n.Ull9 o LQ.W> w> cg> LUJ c Q) g)
J:Ugl)~llJ (LlllSCCCDIDLWce>liD) ~RPOID~CE9 10<9LCCDIO(Q)

-~(Q)(il)l(9G>L8rDlWQW WJCW.9Cce> o'(emQ)g)<Qm) ~(9(99JliTWIU9
WJCrillg)l(9e:>LQ)Lem<fuf» ~LrD"lemlruYUJu<9 OliOClWlQ)LlWUJu ·~C(Q)(il)l(99JLQ)C(U)O(U)
ws~Cffi)g) ~C~g)(99JliTWIU9 f&LOl(99Jem<910LUJ)(f)CQ)g)<Qm) S<9l~009LW OlrtJ(U)rDL8
c~UJu ·ol8c0 ~IOg)LCTUWCrD ~<9009LW oR)UQJ)g)lUJL(QlQ)(U)rDL8 C2lJ9g)Q) 'ClWg)t9
·~cwlW l8c0
owl'lm ~@ ~t)s tQ)t9 ~CWLW<2W ·~L8ru WJC(99JL<fiClV<9Wl'lm em<9LWW ~WJE.ill.9LW
~cwLwemclVlVQJ)lLru ~wtru ·o'((99JLQ)LemcwlW'CQ)w o~ru<9 WJcru'C(99JLS'CCfP
~WJE.ill.9LW ~L~lWLOl(9G>LW9lV s-v L8ClV ~t)s <Qw ·o'Cce>cat9~ lW<9W ~Lemcru
S<9l~Eill9LW ~t)s <Qw QJ<9rDlWlWlce>CWC(99JL(U)rQJ) em<9LWW ·~LrDCUJC(9G>LQJC(U)O(U)
~WJE.ill.9LW ~CWLW<2W ·o'((9G>LQ)LemCat9~ ~t)s lQ)t9 LemCWLWlWl(99JL(U)rQJ)
~Lemcru S<9l~009LW ·o'Cce>Cat9lSlJUlr\siCI-u ~lVg) S<9l~009LW WJce>liU9l)S emLOfV<9
101.,1" LcmC WLW(ll) 'C emLOQ.liD rDLlW UJu o8 Q>IZIZl (U) (Q)9J Q) 'f'GLSL lV em 8 ~ uu s <9l ~ Eill9 LW
"Ol(99JLQ)Lem<Qml ~LrD"leml(U)"(.f]u(9 WJCrillg)lQ)W.9~ WJ009LW ~L<fice> LO~Q>(U)
·o'Cce>cat9~ o'(Q)ClVQ>fillL(U) 'o'(Q)ClVWS~CCTUg) f&L2JIO
OUJIOI.,QJ)LQ)fU oce>)wmul 'o l~009WCffiLrDO(U) CfPLW 'Cm<fuf» ~lWLWlW l(99JLRroJ[.,QJLW
WJ009W (QlQ)Q)rurul o 'C8m o 'C emW;g) L (lllQ) QJ) c CfPg)(U)C rQJ) 'o '( emW><9L (QlQ) em 8 ~ uu
S<9LrD<2W ·o'C8ma ~rcmLrD C~LW9'lem Q>emCfP<9 J::U[.,MWJW;® ~(9G>L~Q>(U) cog)t)w) fl:JISN ~<9009LW OR>UQJ)g) ~emLCfPlWlDJJQJ) ·'ClWl(9G>LemcuuM WJC009o~
17 E l t ,?19 ~ UJ.J t UJ.J c (Q) ~ o \" Q) m <.9<.9 Qlf)) ~ L w UJu 'tt
17 E l t ,?19 rill) r s FU (9 m2! ~ (D Qlf)) 0 C\.U c r QJ) LW l(lQ) <Qw ~ LW (flu 'Ot
17 E l t .?J9 rill) rill) c (Q) ~ o ll9 r cw ~ L w UJu '6
17 E l t ,?19 t UJ.J t s FU <.9 m 2! t w Qlf)) o YJ9 <tP 5PJ@ ~ LW UJu ·g
17 E l t .?l9 ~ill) r s FU (9 m 2! r w Qlf))
umc(Q)f'UL2!1"B omQJ)lLm ~LWUJu 'L
17 E l t .?J9 rill) rill) c (Q) ~ WJ c FU ~ L <9€P L w UJu (j)JJ lJ"' ro r '€1' <Qw
~rru LO t<9€P§<.9 8Jl9\" (f) c2JwLw UJ.J~rocQJrv:D tUJ.Jm ·g
17 E l t .?J9 t UJ.J ~ s FU <.9 m 2! t w Qlf)) (Q) 0\U) r cw Qlf)) ~ L w UJu ·s
17 E l t ,?19 t UJ.J t UJ.J c (Q) ~ o cw c r QJ) <Qw ~L w UJu '17
17 E l t ,?19ZOC'€J'C2U9@ OEJQJ0'lJC\.UCW:D!l'J ~LWUJu '£
17 E l t ,?19 t UJ.J t UJ.J c (Q) ~ o r(Q) (Q) Lwe> QJ t cw ~ L w UJu ·z
17 E l t ,?19 t UJ.J t s F'6<.9 m 2! t w Qlf)) (Q) (J)JJ c QJ) ~ L w UJu .,
ot&cFU~cmcffiUJu otocm<9€PL!l'J of&cFU~ffim ffiLmfro<9€PLQJf.9 WIUC(Q),(Wrul ~rww ]
· · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · WJ (,Q) L uu c ru LrD QJ.f)) I WJ (,Q) L uu o ru LrD
· · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · · ~ Lm o (,Q) <9
· · · · · · ·• ·· · ·· · · · · · ·· · · · · · · · ·· · · · ·· · · · ·· · · · · · · · · · o(\.Jj o ~::v o ~ EJLrD
.. , ............................. "WJRP ~Q) ~ru I ~(.Q)/ ,(W
···········································~emru
''9' ~ce>~LW W')tm9 Q) rDLrD WJ ~em o ru Oi<90(.Q)
~L(Q.lQ)ill9VOUrDg)(f) ~ocilliDu ·~LWJ0<9ill9ce>~W 9Jf'Ug) S<9~E§tm9LW ~LemLroruo~EJOfV[l cu@
· ~ c (,Q) WJ ~ <9B' LR;ce> t (\.Jj Lem o 0 ~ (\.Jj uu Q) 0 Q) ru W')E.Ul9
Q) (Q.lQ)@ s <9 ~ E§ tm9 LW · ce> ~ <9B' L()t) QJ) 1 o ce> ~ (.Q) g) ru 1 WJ o ru ~ (.Q) ~ Oi IDu o Q) (Q.lQ) @ o ~ <9B' W') tm9 ~ EJ o rv g) o ~ IDu
· ce> ~ (Q.lQ) ~ s ft <9 ro Q) g) o ill9 Q) ce> L (Q) ru l (Q.lQ) <9 ~ EJ CQw WJ ~ WJ o (.Q) g) W1 o rw g) ~ <9B' Lem o ru o f ru \" EJ o rv :n c Q) g) o t9
(.Q) <9 c em E§ ce> o em 0 ruJ ~ (Q) 'C s t ce> fU L w 
1 mcruro LoJm3anorum 6Hll1.00 8.lJ 12l1~ ru~C:?;jO\l'&o m1.ooruoo&o n{j)~OWC:?;jO\l'&o
12. n{j) m1c£l6) oJ1ro1m & o& .ooo arrom & c;: ru 6l?;JS& <m & 6T1i 2 3 4
13. n{j) m 1 c£l6) ru1L Ulll2l o am m & c;: ru 6l ?d s J <m J 6T1i 2 3 4
'!4. n{j) m 1 c£l6) ffi! o an~ n1 roll a: an o <m & 6TE 2 3 4
15. n{j) m 1 c£l6) m1 roo Ull c: an o <m 6 <m & 6T1i 2 3 4
16. 6\ll) 0 m 6) oJ 6l§ m) rul .a, 0 <ll a: c6rl:1 0 @: Clml) 1m
am s 1 m 6l ?d s J <m & 6T1i 2 3 4
17. n{j) m 1 c£l6) aJ'l0 m m o a: an o <m 6 <m & 6T1i 2 3 4
18. n{j) m 1 c£l6) LoJ mJ <man a: an o <m & <m), 6T1i 2 3 4
m1 m a: '3 (/!) 6!m un
6l6lBffioB1m ~'lru1<IDClmll1arn alTclffiJ @:OJ 6l?;jSOOJ~ !l...l18J <fhO<ll.),6lffiuB <ID06l\!'6l<fhOSJ Clmll1<ll1.00J <m&. alTclOJ mJOWO
ro 6TIJ wocw1 m16lffiuBc£l6)' n{i)l<ID C:Clml'JO@o arrom& c;:ru 6l?;JS& <m & @rum) @ !l...l1<ID mowan1m& c:m6l<ll x arras m>o@ Clmll18Jl6lS C:<ll6l.J
6) ?d s 6 Clml) 6 .a, .
19. n{j) m 1 c£l6) m m mJ 3 6l.J o a: an o <m & <m & 6T1i 2 3 4
20. n{j) m 1 c£l6) 6l oJ 6l3 m) c6rl:1'l6TIJ o am m & c;: ru 6l ?d s o o & 6T1i 2 3 4
21. n{j) m 1 c£l6) .a, ro w 6TIJ 6ll2l m) a: an o <m & <m 3 6T1i 2 3 4
22. mg& ~ ru 6l<ll C:?;J06l8J mJC:(Tij)On9o:11~1ro1.ooom6~
al'l0l en nD o n{j) m1.oo 6 6T1i 2 3 4
23. 6loJ6l§m) <ID'l<ll612l0ffi6lffiuB n{j)S6.00;jOJOCT3
mJOW1.ooOClmll<ID612ll8Jo nJ8J m~S6lffi@&o
n{j)m1.oo& 6'1"'150<fh00& Gni. 2 3 4
24. n{j)m1c£l6) ru1LUlll2lo arrom& c;: ru 6l?;JSO o;~ 6T1i 2 3 4
25 n{j) m 1 c£l6) mJ J m.l1J an w & o Ull o (Tij) an w & o
alTclffiJ @:OJ 6l?;jSOO&Gni 2 3 4
26. n{j)m1c£l6) ru1n9o:112l<ID<fhuB rurorw1.oo&<fhm>&o alTclOJ6lm>
<ID<ll6TIJo 6l!l...l<Bj&ruom .a,w1m>o6l<mm>&o rurooo&Gni 2 3 4
27. m1C'(;ldo ro.a, oro .,1, 6lffi 6l@ .oo& o1~ 6llllOCT3
!l...l1(Tij)O<fhJ 8JffiO<fhOOJ Gni. 2 3 4
28. n{j)m1c£l6) mJC:(Tij)On9o:112l&Gni 2 3 4
29. ffiJ ow o ro6TIJ .a, O<ll.), 6lffiuB .a,o1 m l2l o m>16l§ s;~ .oo & <m
l oJ ru 6TIJ an n{j) m1.oo & 6T1i 2 3 4
30. n{j) m 1 c£l6) mJ & ro c6rl:11 an <IDJ o a: an o <m o o & 6T1i 2 3 4
31. n{j)m1c£l6) mlrooUll @6'1"'15:J<fh:JO),Gni 2 3 4
32. n{j) m1 c£l6) ffiJ o an~ n1 an 1 a: an o <m o o), 6T1i 2 3 4
33, aJTOLnJW::lffil2l::lCW rul8J rulmllcfhOO ng)6liTD
rulrili 01 ?;j1&>l::l o~ 61li
34, §<'10J1®6l6lm (()::l{f(),\ 6m3u8 Ul'DCOQJnJ),IDC]d 6l0 5), &>l), ITD),
Qlffi cwlarnmlm) ((ffi)QJ@Clll 0::lg6 ru::>oil c£h\l'1cwool~
36, =s& = cfh::> eJm nffl6l~ cruocors 6m3 6l~ cfh), 012J&o <m::>eJ' nJCO ,\6m3 6l~&>l), Ol2J& o ama:eJ::>rul&>l), a:cru::>u8
ng)m1<f16l 00:m ::> CfU 12!2lcOI3 0),6115 ::> c£h), ITDJ,
2
2
2
2
3 4
3 4
3 4
3 4
n{f)6lrrg <"2roa(f)@C"1YT'IDQ;jg1w&~ arroo1ru n.JC01<"2uoaw1c66);J.cm<m1m&o n{f)6loR awm
m.J 1 <fh m 1 flJ arro ~ c66) 6 em <ID 1m J o e2 OJ 61151, 6® am nJ l m 6pJ 0 a w1 cru l2l2l <m 1.3;~!1 ro 1 c66) J cm 6.
gQ ® 63 ro ~ nJ o m C"1YT'ID 16l erg cs a (f) 0 a m). gQ rn nJ o m C"1YT'ID 1 m ~ e2 OJ 61151 6® am cru n.o d3:> ro 1
-21 ~ @ d3:> a ~ a 6l 0 en)" cru l2l2."l <m 1 cOO 6 cm & .

SCORE
State Anxiety Trait Anxiety
No s c 0 r e No s c 0 r e
1 4 3 2 1 19 4 3 2 I
2. 4 3 2 1 20. 1 2 3 4
3. 1 ..,
3 4 21. 1 2 3 4 L.
4. 4 3 2 1 22. 4 3 2 l
5. l 2 3 4 23. 1 2 3 4
6. l 2 3 4 24. 4 3 2 I
7. 4 " 2 1 25. 4 3 2 1 .)
8. 1 2 3 4 26. 1 2 3 4
9. 4 3 2 1 27. I 2 3 4
10. 4 3 2 1 28 4 3 2 I
11. 1 2 3 4 29. I 2 3 4
12. 1 2 3 4 30. 4 3 2 I
13. 4 " 2 I 31. I 2 3 4 .)
14. 4 3 2 I 32. 4 3 2 I
15. I 2 3 4 33. I 2 3 4
16. 1 2 3 4 34. I 2 3 4
17. 4 3 2 1 35. 4 3 2 I
18. 4 3 2 I 36. 1 2 3 4
Related Documents











