Al-Azhar university - Gaza Deanship of Postgraduate Studies & scientific research Biology Department M.Sc. Program in Biological Sciences Effect of antioxidant "taurine" addition on the reliability of complete blood count (CBC) and red cell indices of whole blood specimens stored at room temperature and at 4 C o up to 7 days Submitted in Partial fulfillment of requirements for the Degree of Master of science (biological sciences) Submitted By /Heba A. Al Sarraj (B.Sc. in microbiology) Supervisor Co-supervisor Dr. Mahmoud Sirdah Dr. Abdel Nasser Abushahla November 2010

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
-
Al-Azhar university - Gaza
Deanship of Postgraduate Studies & scientific research
Biology Department
M.Sc. Program in Biological Sciences
Effect of antioxidant "taurine" addition on the
reliability of complete blood count (CBC) and red cell indices of whole blood� specimens stored at room
temperature and at 4 Co up to 7 days
Submitted in Partial fulfillment of requirements for the Degree of Master
of science (biological sciences)
Submitted By /Heba A. Al Sarraj
(B.Sc. in microbiology)
Supervisor Co-supervisor
Dr. Mahmoud Sirdah Dr. Abdel Nasser Abushahla
��November 2010��
id21029765 pdfMachine by Broadgun Software - a great PDF writer! - a great PDF creator! - http://www.pdfmachine.com http://www.broadgun.com
-
i
-
ii
��
��DEDICATED��
��
��
��
��
To����
My great parents who love me, who raised me, supported me, and taught me everything I know.
��
��
��
My brother Rajab and nephews. ��
��
��
My sisters and niece. ��
��
��
��
��
��
��
��
-
iii
��
Acknowledgements����
My deepest and profound acknowledgments are to my supervisor Dr. Mahmoud
Sirdah for his continuous support, generous help, and fruitful and constructive
suggestions. Without his assistance and guidance this work could not be done. I
would like also to express my sincere gratitude to my Co- Supervisor Dr. Abdel
Nasser Abushahla for his support and constructive suggestions throughout this work.
My appreciation and thanks are extended to the staff of Biology department and the
staff of Biology laboratory in Faculty of Science at Al-Azhar university- Gaza, and
the stuff of Balsam laboratory for their help and support specially, Mr. Mohamed
Abdel Majeed.
My special deep and sincere gratitude goes to my parents, brother, sisters especially
Rana, and my friends for their continuous support, help, and encouragement.
Finally, thanks are extended to everyone who has helped in this work.��
��
��
��
��
��
��
-
iv
Table of Contents����
��
Page
i����
ii
- Approval sheet .
- Dedication
iii iv��
- Acknowledgments ...
- Table of content
vii - List of Tables ....
ix - List of Figures....
x - List of Abbreviations ....
xi ��
xiii
- Abstract ....
- Abstract in Arabic..
1 I. Introduction ..
5 II. Review of Literature ...
5����
6
II.1. CBC and its hematological indice
II.2. Storage time and CBC.
7 II.3.Temperature and CBC .
9 II.4. The Anticoagulant EDTA ............
12 II.5. Taurine ..
12�� II.5.1. About Taurine
13 II.5.2.Taurine Biosynthesis ..
14 II.5.3. Actions of Taurine .
-
v
14 II.5.3.1. Bile Acid Conjugation and Cholesterol Excretion .
15�� II.5.3.2. Detoxification By Taurine ...
17�� II.5.3.3. Membrane Stabilization of Taurine .
24 III. Materials and Methods ..
24 III.1. Study design.................
24 III.2 Target population .
24 III.3. Chemicals and equipments
24 III.4. Methods
24 III.4.1. Sampling .
26 III.4.2. Study Groups .
26 III.5. Statistical analysis .
28 IV.Results ..
28 IV.1. Baseline values of the samples ..
31 IV.2. Reliability of the CBC Parameters and Indices .
31 IV.2.1. Platelets Count (PLT) ..
36 IV.2.2. Mean Platelets Volume (MPV)
40 IV.2.3. Red cell distribution width (RDW) .
44 IV.2.4. Red blood cell count (RBC)
48 IV.2.5. Mean Corpuscular Volume (MCV) .
52 IV.2.6. Mean Corpuscular Hemoglobin (MCH) ..
56 IV.2.7. Mean Corpuscular Hemoglobin Concentration (MCHC)
-
vi
60 IV.2.8. Hematocrit Concentration (Hct) ..
64 IV.2.9. Hemoglobin concentration (Hb) ..
68 IV.2.10. White Blood Cell Count (WBC)
72 V.Discussion ...
73 V.1. Baseline values of the samples .
74 V.1.1. Platelets Count (PLT) .
75 V.1.2. Mean Platelets Volume (MPV) ..
76 V.1.3. Red Cell Distribution Width (RDW)
76 V.1.4. Red blood cell count (RBC) ..
77 V.1.5. Mean Corpuscular Volume (MCV) ...
78 V.1.6. Mean Corpuscular Hemoglobin (MCH)
78 V.1.7. Mean Corpuscular Hemoglobin Concentration (MCHC) ..
79�� V.1.8. Hematocrit Concentration (Hct)
79 V.1.9. Hemoglobin concentration (Hb)
80 V.1.10. White Blood Cell Count (WBC) .
81����
81����
83 84
V.I.Summary and Conclusion .
VI.1. Summary.
VI.2. Conclusions.........................................................................................
VII. Recommendations.
86��V.III.References
-
vii
��
List of Tables��
��
Page ��
��Table
29 Mean and SD of the baseline values (2-3 hours from collection) of CBC parameters of the blood samples at room temperature
Table1.
30 Mean and SD of the baseline values (2-3 hours from collection) of CBC parameters of the blood samples at 4 oC refrigerator
��
Table 2.
33 PLT count for samples at Room Temperature ..
Table 3.��
34 PLT count for samples at Refrigerator . ���
Table 4.��
35 Mean Percentage changes of PLT ... ��
Table 5.��
37 MPV for samples at Room Temperature ...
Table 6.��
38 MPV for samples at Refrigerator . ��
Table 7.��
39 Mean Percentage changes of MPV . ��
Table 8.��
41 RDW for samples at Room Temperature . ��
Table 9.��
42 RDW for samples at Refrigerator .. ��
Table 10.��
43 Mean Percentage changes of RDW ��
Table 11.��
45 RBC count for samples at Room Temperature ��
Table 12.��
46 RBC count for samples at Refrigerator ��
Table 13.��
47 Mean Percentage changes of RBC .. ��
Table 14.��
49 MCV for samples at Room Temperature .. ��
Table 15.��
50 MCV for samples at Refrigerator . ��
Table 16.��
51 Mean Percentage changes of MCV . ��
Table 17.��
53 MCH for samples at Room Temperature . ��
Table 18.��
54 MCH for samples at Refrigerator . ��
Table 19.��
55 Mean Percentage changes of MCH .
Table 20.��
57
MCHC for samples at Room Temperature . Table 21.��
-
viii
58 MCHC for samples at Refrigerator .. ��
Table 22.����
59 Mean Percentage changes of MCHC .. ��
Table 23.��
61 Hct for samples at Room Temperature .. ��
Table 24.��
62 Hct for samples at Refrigerator ... ��
Table 25.��
63 Mean Percentage changes of Hct .. ��
Table 26.��
65 Hb concentration for samples at Room Temperature .. ��
Table 27.��
66 Hb concentration for samples at Refrigerator ... ��
Table 28.��
67 Mean Percentage changes of Hb ��
Table 29.��
69 WBC count for samples at Room Temperature ... ��
Table 30.��
70 WBC count for samples at Refrigerator .. ��
Table 31.��
71 Mean Percentage changes of WBC .
Table 32.��
��
��
��
��
��
��
��
��
��
��
-
ix
List of Figures�� ��
Page ��
��Figure
12 Structure of taurine
Figure 1.
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
-
x
List of Abbreviations:�����
Full word��Abbreviation 2,2'-Azobis(2-amidinopropane) dihydrochloride��AAPH��Hepatic alpha-Smooth Muscle Actin��alpha -SMA Complete Blood Count CBC��Carbon Tetrachloride��CCl4��Cysteine Sulfinic Acid Decarboxylase��CSAD��Differential Leucocyte Count��DLC��5,5-dimethylpyrroline-N-oxide��DMPO Ethylene Diamine Tetra Acetic Acid��EDTA Electron Paramagnetic Resonance��EPR Haemoglobin Hb Haematocrit Hct Hepatic Damage��HD Hypochlorous acid��HOCl��Hepatic stellate cells ��HSC��International Council for standardization in Haematology��ICSH��intraperitoneal��i.p.��Tripotassium Ethylene Diamine Tetra Acetic Acid��K3 EDTA��Low density Lipoprotein��LDL Low density Lipoprotein_Cholesterol��LDL-CHO��Lipid Peroxidation��LP Lipopolysaccharide��LPS��Mitogen Activated Protein kinase��MAP-kinase��Malondialdehyde��MDA��Mean Corpuscular Haemoglobin MCH Mean Corpuscular Haemoglobin Concentration MCHC Mean Corpuscular Volume MCV Mean Platelet Volume MPV National Committee for Clinical Laboratory Standards��NCCLS��8-hydroxy-2\- deoxyguanosine ��8-OHdG��Photoreceptor terminals ��P1��Platelets Count PLT Optical platelet count��PLTo��Red Blood Cell RBC Recommended Daily Allowance��RDA��Red Cell Distribution Width RDW Monochlorotaurine��TauNHCl��Taurocholic acid��TCA Total Cholesterol��T-CHO��Triglyceride ��TG��Thepatic cytokine transforming growth factor-beta��TGF-â1 mRNA��Tauroursodeoxycholic��TUDCA��United Kingdom��UK United States��USA Very Low density Lipoprotein��VLDL��Very Low density Lipoprotein_Cholesterol��VLDL-CHO��White Blood Cell WBC��
-
xi
Abstract
Complete blood count (CBC) and its associated hematological indices are one of the
most common and routine laboratory tests. the present study aimed at the evaluation
of possible effects of adding antioxidant taurine on reliability and stability of
complete blood count parameters and its related cell indices of whole blood stored in
vitro at room temperature and 4oC refrigerator up to 7 days.
Random venous blood samples (20 ml each) were collected in K3-EDTA tubes
from 25 apparently healthy nonsmoker male students. The collected blood was
distributed almost equally into 2 sets of K3-EDTA tubes, each set of 4 tubes. One set
of EDTA tubes was kept at the ambient room temperature (23 ± 2 oC) while the other
set was kept at 4oC. For each temperature set, the four EDTA tubes correspond to:
control with zero taurine, 2.5 g/l taurine, 5 g/l taurine, and 10 g/l taurine
concentrations. For each group, CBC analysis was performed at collection time and
then daily for 7 successive days after collection and storage. Statistical comparisons
of data were carried out using the paired t-test, and one-way analysis of variance
(ANOVA). In addition, Mean Percentage changes were calculated and compared.
PLT count was significantly affected by storage temperature and time. Storage of
EDTA blood with taurine at room temperature considerably enhanced the stability of
PLT count over 7 days of storage, while taurine at 4oC showed no remarkable effect
on the stability of PLT count. Neither storage temperature nor incubation with taurine
at the different concentrations stabilize MPV of blood samples, with mean percentage
change increased considerably per time and reached values of 25.4 and 28.1 % at
room temperature and at 4oC, respectively on the 7th day.
-
xii
RDW readings were stabilized with taurine addition at the different concentrations for
48 hours at room temperature, and for 72 hours with 5 g/l taurine at 4oC refrigerator.
RBC count showed instability over time at the different temperatures, while taurine at
10 g/l exerted some stabilizing effect on RBC at room temperature over the first 5
days of the storage period. The MCV readings were stable for 2 days both at room
temperature and at 4oC refrigerator, and taurine did not enhance the stability of MCV
neither at room temperature nor at 4oC refrigerator. On the other hand, MCH readings
were found to be unstable along the 7 days both at room temperature and at 4oC
refrigerator, but addition of taurine to these samples exerted some stability on the
MCH readings both at room temperature for 5 days and for 4 days at 4oC refrigerator.
MCHC readings were unstable and exhibited a significantly decreasing trend
with time despite of temperature or addition of taurine. Also, Hct values were
unstable and exhibited an increasing pattern at room temperature and at 4oC
refrigerator even in the presence of taurine. The values of Hb concentration showed
stable values over the 7 days at both temperatures, with no advantage of taurine on the
stability of Hb values. While WBC count revealed different stabilities at room
temperature and at 4oC refrigerator which lasted for 7 days and 4 days respectively.
However, at room temperature taurine at 5.0 and 10.0 g/l reduced the stability to 3 and
2 days, respectively.
It was concluded that: the different CBC parameters and its related indices
exhibited variable stability patterns in terms of the storage temperature, the time
period and the addition of taurine. Therefore, it is worthwhile for each laboratory to
consider what conditions to be adopted when preserving EDTA blood according to
what laboratory tests are of concern and intended to be performed.
Keywords: Taurine, antioxidant, CBC, K3-EDTA, ANOVA and PLT.
-
xiii
κΨϠϤϟ
�ΓΪδϛϷ�ΩΎπϣ�ΔϓΎο·�ήϴΛ΄Η�ϦϳέϮΗ���ϭ�ϞϣΎϜϟ�ϡΪϟ�ΩΪόΗ�Ε˯ήϗ�ΔϴϗΪμϣ�ϰϠϋ
�ΔΟέΩ�ϭ�Δϓήϐϟ�ΓέήΣ�ΓέήΣ�ΔΟέΩ�ϰϠϋ�ΔχϮϔΤϣ�ϡΩ�ΕΎϨϴόϟ�ϪΗήηΆϣ��ϡΎϳ�ΔόΒγ�ϰΘΣ�ΔϳϮΌϣ
���������ϞѧϣΎϜϟ�ϡΪѧϟ�ΎѧϳϼΧ�ΩΪόΗ�ήΒΘόϳ��CBC����������������ΔѧϴϠϤόϤϟ�ΕέΎѧΒΘΧϹ�Ϣѧϫ�Ϧѧϣ�˵ΪѧΣϭ�ϪѧΑ�ΔѧτΒΗήϤϟ�ϪΗήѧηΆϣϭ
��������������Ϧѧϣ�ΩΪѧΤϤϟ�ΖѧϗϮϟ�ϝϼѧΧ�ϢѧΗ�Ύѧϣ�Ϋ·�ΕΎϨϴόϟ�κΤϓϭ�ϲϟϵ�ϞϴϠΤΘϟ�ΓΰϬΟ�έϮτΗ�Ϟχ�ϲϓ�Ύ˵λϮμΧ�ˬ�ΎϋϮϴη�ήΜϛϷ
ΔόϨμϤϟ�Δϛήθϟ�ϞΒϗ��ΕήΒΘΨϤϟ�ϲϓ��ϑϮϟ΄Ϥϟ�Ϧϣϭ�ϦϴΑ�ΔϴϨϣί�ΓήΘϓ�ϝϼΧ�ϡΪϟ�ΕΎϨϴϋ�ϝΎΒϘΘγ��������ΔϋΎγ����
� ��˰ѧѧѧϟ�ΔϓΎѧѧѧο·�ήϴΛ΄ѧѧѧΗ�ϯΪѧѧѧϣ�ϢϴѧѧѧϴϘΗ�ϰѧѧѧϟ·�ΔѧѧѧϴϟΎΤϟ�ΎϨΘѧѧѧγέΩ�ϑΪѧѧѧϬΗ�taurine���ΞΎѧѧѧΘϧ�έήϘΘѧѧѧγ�ϰѧѧѧϠϋ�CBC��
���������ϭ�Δѧϓήϐϟ�ΓέήѧΣ�ϲѧΘΟέΩ�ϊѧϗϮΑ�ήѧΒΘΨϤϟ�ϲѧϓ�ΎѧϬϨϳΰΨΗ�ϢѧΗ�ΕΎϨϴϋ�ϡΪΨΘγΎΑ�ϪΑ�ΔτΒΗήϤϟ�ϪΗήηΆϣϭ�ϡo
���ΔѧΟϼΜϟ�ϲѧϓ�
Ύϳ�ΔόΒγ�έΪϣ�ϰϠϋϡ���
� ��������ΖϠϤѧη�ΔϴϮθѧϋ�ϱΪѧϳέϭ�ϡΩ�ΕΎϨϴϋ�ϊϤΟ�ϢΗ�Ϛϟάϟ�ΎϘϴϘΤΗϭ���������˯ΎΤѧλϷϭ�ϦϴϨΧΪѧϤϟ�ήѧϴϏ�Ϧѧϣ�ήѧϛΫ�ΎѧΒϟΎσ�
����ήϫίϷ�ΔόϣΎΠΑ�ΎϳήϫΎχ±����ϊѧϗϮΑ�ΓΰϏ���������������ΐѧϴΑΎϧ�Ϧѧϣ�ϦϴΘϋϮѧϤΠϣ�ϰѧϟ·�ϡΪѧϟ�ϢϴδѧϘΗ�ϢѧΗϭ�ˬ�ΐѧϟΎσ�Ϟѧϛ�Ϧѧϣ�Ϟѧϣ��K3-
EDTA��������������������ϲѧϓ�ϦϴΘϋϮѧϤΠϤϟ�ϯΪѧΣ·�φѧϔΣ�ϢѧΗ�ΪѧϘϟϭ�ˬ�ΐѧϴΑΎϧ�ΔѧόΑέ�Ϧѧϣ�ΔϋϮϤΠϣ�Ϟϛ�ΖϧϮϜΗϭ����Δѧϓήϐϟ�ΓέήѧΣ�ΔѧΟέΩ�
��ΎϫέΪϘϣϭ�����ϡ�o
�����������ΎϫέΪѧϘϣ�ΓέήѧΣ�ΔѧΟέΪΑ�ΔѧΟϼΜϟ�ϲѧϓ�ΔѧϴϧΎΜϟ�ΔѧϋϮϤΠϤϟ�φѧϔΣ�ϢѧΗ�ϦϴΣ�ϲϓ��ϡ�o�����Ζѧϋίϭ�ΪѧϘϟϭ
��������˰ϟ�ΰϴϛήΗ�ΐδΣ�ΔϋϮϤΠϣ�Ϟϛ�ϲϓ�ΔόΑέϷ�ΐϴΑΎϧϷ�taurine�����ϲϟΎѧΘϟ�ϮѧΤϨϟ�ϰϠϋ����������ΔϓΎѧο·�ϥϭΪѧΑ�ϢѧϜΤΗ�ΔѧΑϮΒϧ�
�taurine���Ώ�ˬ��������ϡήΟ���ϟΘ������˰ѧϟ�Ϧѧϣ�ή�taurine��Ν������ϡήѧΟ�������˰ѧϟ�Ϧѧϣ�ήѧΘϟ�taurine��Ω�ˬ������ϡήѧΟ�����ήѧΘϟ
���˰ϟ�Ϧϣ�taurine����������˯ήΟ·�ϢΗ�Ϛϟάϟ�ΔϓΎοϹΎΑ�CBC����������Ϛϟάѧϛϭ�ΔϨϴόϟ�ΐΤγ�ΔψΤϟ�ϚϟΫϭ�ϦϴΗέϮϛάϤϟ�ϦϴΘϋϮϤΠϤϠϟ
����ΔϴϟΎΘΘϣ�ϡΎϳ�ΔόΒγ�έΪϣ�ϰϠϋ������ϝϼѧΧ�Ϧѧϣ�ΎѧϬϴϟ·�ΎϨϠѧλϮΗ�ϲΘϟ�ΞΎΘϨϟ�˯Ϯο�ϰϠϋϭ�κѧΤϓ��CBC����˯ήΟΈѧΑ�ΎѧϨϤϗ�ϖΑΎδѧϟ�
������έΎΒΘΧ�ϡΪΨΘγΎΑ�ΕΎϧΎϴΒϠϟ�ΔϴΎμΣϹ�ΕΎϧέΎϘϤϟ�t����������ΪѧΣϭ�ϩΎΠΗ�ϲϓ�ϦϳΎΒΘϟ�ϞϴϠΤΗϭ�ϥέΎϘϤϟ�ANOVA����ΏΎδѧΣϭ
�ΔϳϮΌϤϟ�ΔΒδϨϟ�ςγϮΘϣ���
�����ΔϳϮϣΪϟ�Ύϔμϟ�ΩΪϋ�ϥ�ΎϨψΣϻϭ�PLT������������ΔϧΎπѧΣ�ϥϭ�ˬ�ϪѧΗΪϣϭ�ϦϳΰѧΨΘϟ�ΓέήѧΣ�ΔѧΟέΪΑ�υϮѧΤϠϣ�ϞϜθѧΑ�ήΛ΄ѧΗ�ΪѧϘϟ
�ςϠΠΘϟ�ϊϧΎϣ�ϊϣ�ϡΪϟ�K3 EDATA���˰ϟϭ�taurine��δ˴Σ�Δϓήϐϟ�ΓέήΣ�ΔΟέΩ�Ϟχ�ϲϓ�Ύϔμϟ�ΔϳέήϘΘγ�Ϧϣ�Ϧ
���ϝϼΧ�ΔϳϮϣΪϟ��������������ΔϓΎѧο·�ΪѧϨϋ�υϮѧΤϠϣ�ήϴΛ΄ѧΗ�ϱ�ΙΪѧΤϳ�Ϣϟ�ΎϤϨϴΑ�ϡΎϳ��taurine���������ϲѧϓ�ΎѧϬϨϳΰΨΗ�ϢѧΗ�ϲѧΘϟ�ΕΎѧϨϴόϟ�ϰѧϠϋ
��˰ѧѧϟ�ΰѧѧϴϛήΘϟ�ϻϭ�ϦϳΰѧѧΨΘϟ�ΓέήѧѧΤϟ�ήϴΛ΄ѧѧΗ�ϱ�ΪѧѧΟϮϳ�ϻ�ΎѧϤϛ�ˬ�ΔѧѧϳϮϣΪϟ�Ύϔμѧѧϟ�έήϘΘѧѧγ�ϰѧѧϠϋ�ΔѧѧΟϼΜϟ�ΓέήѧѧΣ�ΔѧΟέΩ�
-
xiv
�taurine�������˰ϟ�ΔϳέήϘΘγ�ϰϠϋ�ΔϔϠΘΨϤϟ�MPV�������ϰϠϋ�ΓήϤΘδϣ�ΓΩΎϳί�ήϴϐΘϠϟ�ΔϳϮΌϤϟ�ΔΒδϨϟ�ςγϮΘϣ�ΪϬη�ϦϴΣ�ϲϓ�ˬ
�����ϝΩΎόΗ�ϪΘϤϴϗ�ΖϧΎϛϭ�ˬ�ΔόΒδϟ�ϡΎϳϷ�έΪϣ����������ϭ�Δѧϓήϐϟ�ΓέήѧΣ�ΔѧΟέΩ�ϲϓ�����������ΔѧΟϼΜϟ�ΓέήѧΣ�ΔѧΟέΩ�ϲѧϓ
��ϊΑΎδϟ�ϡϮϴϟ�ϲϓ���Ε˯ήϗ�ΕήϘΘγ�ΎϤϛ�RDW������ѧϟ�ϊѧϣ�ϪѧϨϳΰΨΗ�ΪѧϨϋ�˰�taurine�������ΓΪѧϤϟ�ΔѧΗϭΎϔΘϣ�ΕΰѧϴϛήΗ�ϲѧϓ���
������ΓΪϤϟϭ�ˬ�Δϓήϐϟ�ΓέήΣ�ΔΟέΩ�ϲϓ�ΔϋΎγ������ΰѧϴϛήΗ�ϊѧϣ�ΔϋΎѧγ���ϢѧΟ����������ΕήѧϬχ�ΎѧϤϨϴΑ�ΔѧΟϼΜϟ�ΓέήѧΣ�ΔѧΟέΩ�ϲѧϓ�ήѧΘϟ
������˯ήѧϤΤϟ�ϡΪѧϟ�ΎѧϳϼΧ�ΩΪѧόΗ�Ε˯ήѧϗ�RBC�����������ΓέήѧѧΤϟ�ϲΘΟέΪѧΑ�ΎѧϬψϔΣ�˯ΎѧϨΛ�ΔόΒδѧϟ�ϡΎѧϳϷ�ϝϼѧΧ�ΎϫέήϘΘѧγ�ϡΪѧϋ
���ΰϴϛήΗ�ΪϨϋ�ΎϤϨϴΑ�ϦϴΘϘΑΎδϟ���ϢΟ�����������ϡΎѧϳϷ�ϝϼѧΧ�Δѧϓήϐϟ�ΓέήѧΣ�ΔѧΟέΩ�ΪѧϨϋ�Ε˯ήѧϘϟ�ϩάϬϟ�ΎϴΒδϧ�έήϘΘγ�ΎϧΪΟϭ�ήΘϟ
�����ϦϳΰΨΘϟ�Ϧϣ�ϰϟϭϷ�ΔδϤΨϟ�����Ε˯ήϘϟ�ΔΒδϨϟΎΑϭ�MCV�����������������ϲѧΘΟέΩ�ϲѧϓ�ϲϧΎѧΜϟϭ�ϝϭϷ�ϦϴϣϮѧϴϟ�ϲѧϓ�ΓήϘΘδѧϣ�ΖѧϧΎϜϓ
����������˰Ϡϟ�ήϴΛ΄Η�ϱ�ΪΟϮϳ�ϻ�Ϫϧ�ΎϤϛ�ˬ�ΓέήΤϟ�taurine�����Ε˯ήѧϗ�ϰϠϋ�MCV�����ΘΟέΪѧϟ�ϲѧΘϠϛ�ϲѧϓϦϴ������Ε˯ήѧϗ�Ϧѧϋ�Ύѧϣ
�MCH����������˰ѧѧϟ�ΔϓΎѧѧο·�ΪѧѧϨϋ�ϦѧѧϜϟϭ�ˬ�ϦϴΘΟέΪѧѧϟ�ϲѧѧΘϠϛ�ϲѧѧϓ�ϊΒδѧѧϟ�ϡΎѧѧϳϷ�ϝϼѧѧΧ�έήϘΘѧѧγ�ϱ�ϯήѧѧΧϷ�ϲѧѧϫ�ΪϬθѧѧΗ�ϢѧѧϠϓ
�taurine����ΓέήѧѧΣ�ΔѧѧΟέΩ�ϲѧѧϓ�ϡΎѧѧϳ�ΔѧѧόΑέϷϭ�ϡΎѧѧϳ�ΔδѧѧϤΧ�ΓΪѧѧϤϟ�Δѧѧϓήϐϟ�ΓέήѧѧΣ�ΔѧѧΟέΩ�ΪѧѧϨϋ�έήϘΘѧѧγϻ�ξѧѧόΑ�ΙΪѧѧΣ
ΔΟϼΜϟ�������Ε˯ήϗ�ιϮμΨΑϭMCHC)������Θϣϭ�ΓήϘΘδϣ�ήϴϏ�ΖϧΎϛ�ΪϘϓ���������Ϟѧϛ�ϲѧϓ�υϮѧΤϠϣ�ϞϜθѧΑ�νΎѧϔΨϧϻ�ϮΤϧ�ΔϬΠ
����ΖϗϮϟ�έϭήϤΑ�ϑϭήψϟ�����Ε˯ήϗ�ΖϧΎϛ�ΪϘϓ�ήϴΧϭ�Hct�����������ϲѧϓ�ΓΩΎѧϳΰϟ�ϮѧΤϧ�ΎѧϫΎΠΗ�ΕήѧϬχϭ�Ύπѧϳ�ΓήϘΘδѧϣ�ήѧϴϏ
������˰ϟ�ΔϓΎο·�ΪϨϋϭ�ϦϴΘΟέΪϟ�ϲΘϠϛ�taurine������������ϡΪѧϟ�ΏΎπѧΧ�ΰϴϛήΗ�Ϣϴϗ�ϥ�ΎϤϛ�ˬ��HB���������ϡΎѧϳϷ�ϝϼѧΧ�ΓήϘΘδѧϣ�ΖѧϧΎϛ
��ϼπѧѧϓ�ϦϴΘΟέΪѧѧϟ�ϲѧѧΘϠϛ�ϲѧѧϓ�ΔόΒδѧѧϟ��˰ѧѧϟ�ήϴΛ΄ѧѧΗ�ϡΪѧѧόϧ�Ϧѧѧϋ��taurine���ΎѧѧϬϴϠϋ���Ε˯ήѧѧϗ�ΎѧѧϤϨϴΑ��WBC����ΕήѧѧϬχ
�ΔϋϮϤΠϣ�Ϟϛ�ΐδΤΑ�ΎϨϳΎΒΘϣ�έήϘΘγ���
� �����������ϞѧϣΎϜϟ�ϡΪϟ�ΎϳϼΧ�ΩΪόΗ�ϥ�ϰϟ·�ήϴθϧ�ΎϣΎΘΧϭ�CBC��������������ΐδѧΣ�ϩέήϘΘѧγ�ϒѧϠΘΨϳ�ϪѧΑ�ΔѧτΒΗήϤϟ�ϪΗήѧηΆϣϭ
��������˰ϟ�ΰϴϛήΗ�ΔΒδϧϭ�ϪΗΪϣϭ�ϦϳΰΨΘϟ�ΓέήΣ�ΔΟέΩ�taurine����ΰΨΗ�ϲϓ�ϡΪΨΘδϤϟ���ϡΪϟ�ΕΎϨϴϋ�Ϧϳ�����ϞѧϜϟ�ΪѧϴϔϤϟ�ϦϤϓ�Ϛϟάϟ
����������������ϱϮѧϨϳ�ϲѧΘϟ�ΔѧϳήΒΨϤϟ�ΕΎѧλϮΤϔϟ�ϊѧϣ�ϖѧϓϮΘΗ�ϲѧϜϟ�ϞѧϣΎϜϟ�ϡΪѧϟ�ΕΎѧϨϴϋ�φѧϔΤϳ�ϦϴѧΣ�ΔϤϼϣ�ρϭήη�ϊπϳ�ϥ�ήΒΘΨϣ
�ΎϬήΟ·����
-
�
I. Introduction
Complete blood count (CBC) and its associated hematological indices are one
of the most common and routine laboratory tests that are requested as the first step to
diagnose an illness or clinical presentation. With the development of the automated
hematological analyzers or counters, the CBC test has become an easy, quick, and
reliable test that can give valuable information to physicians leading to provisional
diagnosis or to further testing (England et al., 1984; Buttarello, 2004).
Most clinical laboratories are equipped now with modern automated analyzers
that are capable of processing large number of hematological tests in an efficient and
timely manner. These tests include CBC [red blood cell (RBC), haemoglobin (Hb),
haematocrit (Hct), white blood cell (WBC), and platelets (PLT) counts] and its
related indices [mean corpuscular volume (MCV), mean corpuscular haemoglobin
(MCH), mean corpuscular haemoglobin concentration (MCHC), red cell distribution
width (RDW), and mean platelet volum (MPV)].
To ensure reliability of the results generated by the instrument, it is imperative
that the specimens are collected appropriately in a suitable anticoagulant and analyzed
on a properly calibrated instrument within the time frame considered appropriate or
recommended by the manufacturer (International Council for standardization in
Haematology (ICSH), 1993; Lewis, 1999; Macey et al., 2002).
However, the recent trends towards large centralized laboratories, and changes
in laboratory organizations, have brought redistribution activity to a new perspective.
-
�
Laboratories now test specimens that have been dispatched over a long distance; as a
result, testing is often delayed by 1224 hours or more after veinpuncture. Moreover,
on weekends, this interval may exceed 36 hours. Therefore, When such a specimen
arrives, the laboratory must decide whether to accept or reject the specimen (Gulati et
al., 2002). The laboratory must then decide whether to perform all of the tests ordered
or only those deemed appropriate given the age of the specimen, and what comments
should be appended to the reported results regarding the reliability or limitations of
the analysis. Although laboratories should still give reliable results, excessive delays
in processing might affect the reliability, accuracy and imprecision analysis
(Buttarello 2004).
Taurine has been demonstrated to function as a direct or indirect antioxidant.
Directly, taurine performs its antioxidant effect by scavenging or quenching reactive
oxygen species and other free radicals, especially for the hypochlorite ion (Wright et
al., 1985) and inhibiting lipid peroxidation by reducing the production of
malondialdehyde (MDA), an end-product of lipid peroxidation, from the unsaturated
membrane lipids (Huxtable, 1992). However, the indirect antioxidant effect of
taurine is thought to be due to its ability to stabilize biomembranes structure and
function by preventing the increase in membrane permeability from oxidants effects
(Wright et al., 1985).
A lot of studies about the effect of taurine as antioxidant in different tissues
have been performed and confirmed the potent antioxidant activity of taurine
(Nakashima et al., 1982; Milei et al., 1992). Taurine has been demonstrated to act as
-
�
both a primary antioxidant that scavenges free radicals and as a secondary antioxidant
that attenuates oxidant-induced changes in biomembranes stability (Koyama et al.,
1992). It seems likely that taurine is involved in membrane stabilization at several
levels and that this action accounts for many of its physiological effects. Taurine's
ability to stabilize cell membranes may be attributed to one or more of its action:
antioxidation (Nakamori et al., 1990; Vissers et al., 1994), osmoregulation (Ozasa
&. Gould 1982), and its ability to maintain of intracellular ions homeostasis (Qi, et
al., 1995), its ability to inhibit membrane proteins phosphorylation (Lombardini,
1985), its ability to prevent lipid peroxidation (Pasantes-Morales & Cruz, 1985),
and its ability to form conjugated compounds (Hino et al., 1993).
Different studies have revealed that whole blood samples become more stable
when stored at low temperature or when an anticoagulant is used in preserving the
collected whole blood samples (McShine et al., 1990; Chen et al., 1999; Macey et
al., 2002; Buttarello, 2004; Mahmoodi et al., 2006).
Objectives of the study
The general objective was to evaluate the possible effects of adding the
antioxidant taurine on the stability and reliability of complete blood count and red cell
indices of whole blood stored in vitro at room temperature and at 4 oC for up to 7
days.
-
�
The specific objectives were
To assess the effect of storage temperature (4 oC and room temperature) on the
stability and reliability of CBC and red cell indices of whole blood.
To test the effect of taurine addition at different concentrations on the stability
and reliability of CBC and red cell indices of whole blood.
To find any relationship between taurine concentration and stability and
reliability of CBC and red cell indices of whole blood.
To determine the best running period for each test of interest that provides
stable and reliable results.
��
��
��
��
��
��
��
��
��
��
-
�
II. Review of Literature
The main objective of any laboratory determination is to produce results that
are accurate and precise enough for clinical use (Buttarello, 2004).
In clinical laboratories, the cycles of each test starts with the preparation of
patient, and continues with biologic sample collection, preparation and storage of the
sample under suitable conditions and finally finishes by reporting the result. It is
sometimes necessary to repeat a test to obtain a reliable result. Sometimes there is a
period of time between sample collection and doing or repeating a test. In this
situation the stability of the sample is very important. Since blood tests are more
common than the other biologic fluids, therefore using the standard methods for
sample collection, and storage, and the role of environmental factors that may affect
the bloods indices should be considered (Mahmoodi et al., 2006).
II.1. CBC and its hematological indices
The complete blood count (CBC) with its indices is one of the most common
laboratory tests performed nowadays. It gives information about the production of all
blood cells and identifies the patient's oxygen-carrying capacity through the
evaluation of red blood cell indices, hemoglobin, and hematocrit. It also gives
information about the immune system through the evaluation of the differential white
blood cell count. These tests are useful in diagnosing anemia, certain cancers,
infection, acute hemorrhagic states, allergies, and immunodeficiencies as well as
monitoring the side effects of certain drugs that cause blood dyscrasias (George-Gay
and Parker, 2003).
-
�
Clinical laboratories equipped with modern automated analyzers are capable
of processing large number of hematological tests in an efficient and timely manner.
These tests include CBC , RBC, Hb, Hct, WBC, and PLT and its related indices
MCV, MCH, MCHC, RDW, and MPV. To ensure reliability of the results generated
by the instrument, it is imperative that the specimens are collected appropriately in a
suitable anticoagulant and analyzed by a properly calibrated instrument within the
time frame considered appropriate or recommended by the manufacturer (ICSH,
1993; Lewis, 1999; Macey et al.; 2002).
II.2. Storage time and CBC
The recent trends towards large centralized laboratories, and changes in
laboratory organizations have brought redistribution activity to a new perspective. In
fact, delayed sample analysis is not rare in clinical or laboratory routine, especially
when blood samples are shipped, under poorly controlled conditions to distant
centralized laboratories (Lippi et al., 2005). So clinical laboratory professionals are
familiar with the scenario whereby a blood specimen is collected on a Friday but not
delivered to the laboratory for processing until the following Monday or even later.
When such a specimen arrives to the laboratory, the staff needs to decide whether to
accept or reject it; and if accepted, whether to perform all of the requested tests or
only those deemed appropriate based on the age of the specimen; and what
comments, if any, should be appended to the reported results regarding their reliability
or unreliability. Such decision making requires the lab. technician to be familiar with
changes known to occur in blood specimens during storage. The manufacturers of
automated analyzers and the published literature often cite that blood specimens kept
-
�
at either room temperature or at 4 oC (refrigerated) for up to 24 hours, generally yield
reliable results for complete blood cell count (CBC) (Gulati et al., 2002). However,
recent studies showed that specific information concerning the suitability, stability,
and reliability of whole blood specimens older than 1 day for various automated
hematologic tests are limited, particularly in the recent literature (Buttarello, 2004;
Hedberg & Lehto, 2009).
Mahmoodi et al., (2006) in their study entitled "survey of changes in
complete blood count and red cell indices of whole blood incubated in vitro at
different temperatures up to 48 hours" showed that delay in doing the CBC test can
lead to changes in some parameters, therefore the blood samples should not be left in
the laboratory and the test should be done on blood samples as soon as possible.
In Philadelphia Gulati et al., (2002) suggested that clinically reliable results
may be obtained for some CBC parameters, from specimens older than 1 day, when
analyzed on the Coulter Gen.S (Beckman Coulter, Miami, Fla). For example, Hb,
RBC, and MCH values are stable for samples of 7 days old, WBC value is stable for
samples of 3 days old, and platelets value is stable for samples of 4 days of storage at
room temperature, While WBC differential value is not stable or reliable for samples
of more than one day old.
II.3. Temperature and CBC
Different studies have showed that whole blood samples become more stable
when stored at low temperature or when an anticoagulant is used in preserving the
-
�
collected whole blood samples (Vogelaar et al., 2002; Lippi et al., 2005; Hedberg &
Lehto, 2009).
In Italy Lippi et al., (2005) evaluated the stability of conventional and new
hematologic parameters in blood specimens stored for as long as 24 hours at 4°C. Of
the 21 hematologic parameters tested with the use of the Advia 120 hematologic
analyzer (Bayer Diagnostics), means for paired samples of specimens differed
significantly over the 24-hours storage period for Hct, MCV, percentage of
macrocytes, PLT count, MPV, reticulocyte count and percentage, and reticulocyte
hemoglobin content (all P
-
�
of impedance platelet count yielded more reliable results than the routine PLTo. WBC
differential parameters, except eosinophils, were stable for up to 48 hours at +23 ± 2
oC. CBC parameters were stable for 72 hours, except MPV, which slightly increased
between 48 and 72 hours at +4 oC. WBC differentials were stable for 4872 hours,
with a slight decrease observed in absolute neutrophils and lymphocytes at +4 oC. The
authors concluded that CBC and differential parameters should be analyzed as soon as
possible after collection. If analysis is delayed for a longer period of time specimens
should preferably be maintained at +4 oC. The date and time collection should be
clearly indicated and, in cases where a delay in analysis does not enable accurate
results, the corresponding parameter should be omitted and substituted by a comment.
II.4. The anticoagulant EDTA
Ethylene Diamine Tetra Acetic Acid (EDTA) is the most commonly used
anticoagulant in evacuated tubes since 1950s. It inhibits the clotting process by
removing calcium from the blood. It has certain advantages over other anticoagulants;
it does not distort blood cells, making it ideal for hematology use. So EDTA is the
anticoagulant recommended for full blood cell counts and white blood cell differential
analysis by the NCCLS (National Committee for Clinical Laboratory Standards),
principally for its cell preservation properties (Macey et al., 2002).
Potassium EDTA is the most soluble salt among the three other EDTA salts
Na2EDTA, K2EDTA and K3EDTA (England et al., 1993). Tripotassium Ethylene
Diamine Tetra Acetic Acid (K3 EDTA) is dispensed as a liquid and thus causes a
slight dilution of the specimen. This salt also affects the red blood cell size at
-
��
increased concentrations and on storage than the dipotassium salt (Hedberg and
lehto 2009).
Nowdays the International Council for Standardization in Hematology
recommends the dipotassium salt of EDTA as the anticoagulant for full blood counts .
In Europe and Japan, it is the preferred anticoagulant, whereas in the United States
(USA) and the United Kingdom (UK) the tripotassium salt of EDTA is more
commonly used. Under optimal conditions (appropriate anticoagulant concentration
and analysis within 14 hours after veinpuncture), the choice of dipotassium EDTA or
tripotassium EDTA have insignificant effect on the results of full blood cell counts
and white blood cell differential analyses (Macey et al., 2002).
In Netherlands McShine et al., (1990) observed that platelet counts in citrated
blood samples were lower than those in EDTA and highlighted the necessity to
present citrated samples mixed with dried EDTA when characterization or quality
control of blood and blood components is required, and they suggested that a small
population of platelets may form microaggregates within 1 to 4 hours in the blood
collected in citrate-containing anticoagulant- solutions. This leads to an erroneous
evaluation of the platelet count. Mixing these samples with dried EDTA before
platelet counting will ensure a correct platelet count, if an EDTA sample itself is not
available (McShine et al., 1990 ).
In China Chen et al., (1999) found that values of Hb, Hct, MCV and
lymphocyte percentage collected in Na2 EDTA tubes were significantly higher than
-
��
those collected in K3 EDTA (P 0.05 for Hb and lymphocyte percentage, and P all
0.01 for others ), While values of MCHC collected in Na2 EDTA were significantly
lower than those collected in K3 EDTA tubes ( P 0.05). for underfilling for blood
sample, values of Hct and MCV with 2 ml blood volume (both P 0.01 ), while
values of MCHC with 2 ml blood volume were significantly higher than those with
5ml blood volume ( P < 0.01 ). When the collection blood volume was increased to
3.5 ml, there were no significant difference between values for 3.5 ml and 5 ml blood
volume (P all > 0.05). in the storage stability study, there was a significant sequential
increase of Hct and MCV between 1 hour, 8 hours and 12 hours (P < 0.05 and < 0.01,
respectively, for 8 hours, P all < 0.01 for 12 hours). There was also a significant
sequential decrease of neutrophil percentage between 1 hour and 4, 8, 12 hours'
storage at room temperature (P all
-
��
Figure 1: Structure of Taurine
analytical goals based on the state of the art are acceptable while for bias this is
satisfactory only for some parameters.
II.5. Taurine
I.5.1. About taurine
Taurine was first isolated from ox bile in 1827 and was named (Gallen-
Asparagin). After that, it was named Bos taurus, after the ox (Bos taurus is the Latin
name of ox). In 1838, the term taurine first appeared in the literature . Although
taurine was discovered more than 184 years ago, it is just only in the past three
decades that the significance of taurine in human nutrition and disorders has really
been investigated and identified (Sirdah, 2006).
Initial interest in taurine was generated during both World Wars, when naval
doctors had administered taurine to their soldiers to enhance their night vision and
relieve fatigue. Taurine is believed to be an all-round medicine (Sirdah, 2006) .
Taurine (2-aminoethanesulfonic acid
NH2CH2CH2SO3H), is a naturally-occurring ß-
sulfonated amino acid, its molecular weight is
125.2 and has two acidic dissociation constants
(pKa) values (at 25°C) of 1.5 and 8.82. Along
with methionine, cystine and cysteine, taurine is a sulfur amino acid (Sirdah, 2006).
Taurine zwitterionic nature gives it high water solubility and low lipophilicity
(Huxtable, 1992).
-
��
Taurine occurs in the body as a free molecule or in simple peptides and is not
incorporated into muscle proteins. Taurine, one of the lesser-known amino acids, it
has many important and beneficial effects on the human body. It has been implicated
in many physiological functions, pharmacological actions and pathological conditions
(Sirdah, 2006).
For a long time, taurine was considered a nonessential nutrient for humans.
Recently, it has become clear that taurine is a very important amino acid involved in a
large number of metabolic processes and become essential under certain
circumstances (conditionally essential amino acid). When it is given in nutritional or
therapeutic dose, taurine has not been consistently linked with any toxicity or severe
adverse effects, it is thought to be quite safe (Sirdah, 2006).
II.5.2.Taurine biosynthesis :
Taurine biosynthesis was outlined by Jacobsen and Smith (Jacobsen and
Smith, 1968). There are a number of possible pathways through which taurine may be
generated, and these include:
1) the oxidation of cysteine to cysteine sulfinic acid and subsequently to
cysteic acid, which is decarboxylated to taurine.
2) oxidation of cysteine to cysteine sulfinic acid with subsequent
decarboxylation to hypotaurine, which is oxidized to taurine. The rate limiting step is
the conversion of cysteine sulfinic acid to hypotaurine catalyzed by cysteine sulfinic
acid decarboxylase (CSAD). This is a pyridoxal phosphate requiring enzyme, and
-
��
therefore vitamin B6 deficiency can lead to a reduction in endogenous taurine.
Generally humans have an inherent capacity to maintain endogenous taurine levels
within a wide normal range from dietary methionine and cysteine. Because of this no
Recommended Daily Allowance (RDA) has been established for taurine (Redmond
et al., 1998).
The physiologic normal plasma taurine concentration is in the range between
35 and 60 mol/L, with any excess being readily excreted via the kidneys in the urine
(Trautwein and Hayes, 1990). Normal whole blood taurine in humans ranges
between 160 and 320 mol/L (Trautwein and Hayes, 1990).
II.5.3. Actions of taurine
Taurine has a lot of important and beneficial effects on the human body. It has
been implicated in many physiological functions, pharmacological actions and
pathological conditions (Sirdah, 2006).
II.5.3.1. Bile acid conjugation and cholesterol excretion
Bile acids, primarily cholic acid and chenodeoxycholic� acid, result from
cholesterol metabolism in the liver and are involved in�emulsification and absorption
of lipids and fat-soluble vitamins. In order for�this to occur, bile acids must be bound
to either glycine or taurine, forming�bile salt conjugates. The conjugation of bile acids
by taurine results in� increased cholesterol solubility and excretion (Hardison and
Grundy, 1983). In Japan Mizushima et al., (1996) had investigated the effects of oral
-
��
taurine supplementation on lipids and sympathetic nerve tone in healthy young men
on experimental high fat and cholesterol diets. They found that oral taurine
supplementation attenuated increases in Total Cholesterol (T-CHO), Low density
Lipoprotein Cholesterol (LDL-CHO) and Low density Lipoprotein (LDL) in healthy
men on high fat cholesterol diets but induced significant increases in very Low
density Lipoprotein Cholesterol (VLDL-CHO), very Low density Lipoprotein
(VLDL) and triglyceride (TG), which could be explained by a possible effect of
taurine on lipoprotein lipase. Significantly lower urinary norepinephrine excretion
observed by the taurine administration implies the suppression of the sympathetic
nervous system.
II.5.3.2. Detoxification by taurine
Taurine has been demonstrated to function as a direct or indirect antioxidant.
Directly, taurine performes its antioxidant effect by scavenging or quenching reactive
oxygen species and other free radicals, especially for the hypochlorite ion (Wright et
al., 1985) and inhibiting lipid peroxidation by reducing the production of
malondialdehyde (MDA), an end-product of lipid peroxidation, from the unsaturated
membrane lipids (Huxtable, 1992). However, the indirect antioxidant effect of
taurine is thought to be due to its ability to stabilize biomembranes structure and
function by preventing the increase in membrane permeability due to oxidantation
effects (Wright et al., 1985).
A lot of studies about the effect of taurine as antioxidant in different tissues
have been performed and these studies confirmed the potent antioxidant activity of
taurine.
-
��
Nakashima et al., (1982) investigated the effect of taurine on hepatic lipid
peroxide level following carbon tetrachloride (CCl4) administration in rats. To
determine the therapeutic efficacy of taurine administration on liver injury, to CCl4
intoxicated rats (CCl4, 2 ml/kg, intraperitoneal (i.p.)), 3 ml of a 10% aqueous solution
of taurine was administered after CCl4 administration (at 12, 16, and 20 hours after),
and rats were sacrificed at 24 hours after CCl4 administration in order to estimate the
level of lipid peroxides in the liver. The decrease of hepatic lipid peroxidation induced
by CCl4 was noticed in the taurine-treated rats. Taurine had no effect on mixed
function oxidase activity in hepatic microsomes nor on hepatic antioxidant content in
the CCl4-intoxicated rats. Hepatic taurine content decreased significantly 12 and 24
hours after CCl4 administration, whereas oral administration of taurine to CCl4-
intoxicated rats was able to protect these rats from hepatic taurine depletion. These
results suggest that hepatic taurine may play a critical role on the protection of
hepatocytes against hepatotoxins such as CCl4 and the administration of taurine may
be useful in the treatment of hepatotoxin-induced liver injury.
Miyazaki et al., (2005) examined the effects of taurine on hepatic fibrogenesis
and in isolated hepatic stellate cells (HSC). Rats of the hepatic damage (HD) group
were administered carbon tetracholoride (CCl4) for 5 weeks and a subgroup received,
in addition, a 2% taurine containing diet for 6 weeks (HDT). The HSC were isolated
from normal rats and cultured for 4 days. They found that hepatic taurine
concentration was decreased in the HD group. This loss and the hepatic histological
damage and fibrosis, were reduced following taurine treatment. Furthermore, the
hepatic alpha-smooth muscle actin (alpha-SMA), lipid hydroperoxide and 8-hydroxy-
2\- deoxyguanosine (8-OHdG) levels in serum and liver, as well as hepatic cytokine
-
��
transforming growth factor-beta1 (TGF-â1 mRNA) and hydroxyproline levels were
significantly increased in the HD group, and most of these parameters were
significantly reduced following taurine treatment. In contrast to the mitogen activated
protein kinase (MAP-kinase) and Akt expressions, which remained unchanged, the
lipid hydroperoxide and hydroxyproline concentrations, as well as (TGF- â1 mRNA)
levels were significantly reduced by taurine in activated HSC. So oral taurine
administration enhances hepatic taurine accumulation, reduces oxidative stress and
prevents progression of hepatic fibrosis in CCl4-induced HD rats, as well as inhibits
transformation of the HSC.
A striking finding about the antioxidant action of taurine was reported by
Anitha Nandhini et al., (2002) who investigated the effect of taurine on the
susceptibility of the aorta to lipid peroxidation and on the activities of enzymatic and
non-enzymatic antioxidants in animal model. The study concluded that: not only
taurine supplementation reduces lipid perodxaition but it also raised the activities of
the antioxidant enzymes significantly (Anitha Nandhini et al., 2002; Sirdah, 2006).
II.5.3.3. Membrane stabilization of taurine��
Taurine ability to stabilize cell membranes may be�attributed to several
mechanisms. Taurine has been shown to regulate osmotic�pressure in the cell,
maintain homeostasis of intracellular ions, inhibit�phosphorylation of membrane
proteins, and prevent lipid peroxidation. As an�osmotic regulator, it has been
suggested that taurine, along with glutamic acid, act as an instrument in the transport
of metabolically-generated water from the�brain (Van Gelder, 1990).
-
��
The antioxidation effects of taurine was investigated by many investigators as
Nakamori K. et al., (1990) who investigated the effect of taurine in protecting
biomembrane attacked by hypochlorous acid (HOCl) using canine erythrocytes which
had been pre-treated with HOCl. In the treatment, most of the HOCl was consumed as
a result of its reaction with a number of electrophilic substances, such as free amino
groups (-NH2) in the membrane, whereas hemoglobin inside the cells was not
oxidized. The lysis of HOCl-treated erythrocytes was dependent on the concentration
of HOCl and on the storage time at 37 °C. Taurine inhibited the lysis at 37 °C in a
dose dependent manner. During the storage of HOCl-treated erythrocytes with
taurine, an appreciable amount of monochlorotaurine (TauNHCl) was detected in the
supernate. This suggests that taurine might remove the oxidized chlorine from HOCl-
treated erythrocytes, resulting in the production of TauNHCl. The effect of taurine on
the removal of Cl+� moiety was further examined using Sepharose gel with free amino
groups. Taurine removed Cl+ moiety from HOCl-treated Sepharose gel, and the yield
of TauNHCl depended on the concentration of taurine and the storage time. These
results indicate that taurine might inhibit the hemolysis by scavenging the oxidized
chlorine moiety from the HOCl-treated erythrocytes.
Milei et al., (1992) investigated the possible free-radical scavenging action of
taurine during coronary artery bypass grafting, twelve patients were randomly divided
into two equal groups. One to 3 hours before surgery, they received a rapid
intravenous infusion of either placebo (group 1) or taurine (5 gm) (group 2). During
surgery, biopsy samples were taken before ischemia (preischemic samples) and after
10 minutes of reperfusion (reperfusion samples). Lipoperoxidation was determined by
hydroperoxide-initiated chemiluminescence of heart homogenates, and myocardial
-
��
cell damage was assessed by electron microscopy. The values for chemiluminescence
in preischemic and reperfusion samples from group 1 were 7500 +/- 1600 and 18,600
+/- 4600 cpm/mg of protein, respectively (p less than 0.03). This difference was not
observed in group 2 where the values were 10,050 +/- 2700 and 11,800 +/- 4200
cpm/mg of protein, for preischemic and reperfusion samples, respectively. The
number of severely damaged mitochondria (grades 3 and 4) in reperfusion samples
from group 1 increased significantly compared to preischemic samples (25 +/- 8% vs
12 +/- 3%, p less than 0.01). Conversely no differences were observed between the
number of severely damaged mitochondria in reperfusion and preischemic samples
from group 2 (8 +/- 3% vs 8 +/- 2%). The number of damaged and necrotic myocytes
increased in group 1 after reperfusion from 22 +/- 9% to 34 +/- 10% (p less than 0.03)
and from 10 +/- 7% to 26 +/- 20% (p = NS), respectively. No differences were
observed between reperfusion and preischemic samples in group 2. Treatment with
taurine seems to reduce lipoperoxidation and decrease cell damage at the time of
reperfusion.
The effect of taurine in protecting biomembrane against oxygen radicals was
investigated by Nakamura T. et al., (1993) using canine erythrocytes 2,2'-Azobis(2-
amidinopropane) dihydrochloride (AAPH), a water-soluble azo-compound, was used
as the oxygen-radical generator. Taurine suppressed erythrocyte hemolysis more
effectively than alpha-alanine, used for comparison. To clarify the relationship to the
lipid peroxidation, the amount of lipid peroxide was measured using liposomes
prepared with egg yolk lecithin. However, the peroxidation was not suppressed by
taurine. When intact erythrocytes were subjected to hemolysis by hyposmotic
solutions, taurine suppressed the osmotic hemolysis more effectively than alpha-
-
��
alanine. These results suggest that taurine does not have an antioxidative effect like
vitamin E, but interacts with the biomembrane, and helps to protect it against damage
caused by AAPH.
The study of Mankovskaya et al., (2000) in Ukraine was undertaken to
elucidate the effects of taurine on lipid peroxidation (LP) intensity and membrane
Na+, K+-ATPase activity in a hypoxic rat model. It was shown that 3 intraperitoneal
(i.p.) injections of 200 mg/kg of taurine prevented hypoxia-induced lactate
accumulation and LP in brain, liver, and heart tissues and prevented the decrease of
Na+, K+-ATPase activity in the liver. It is suggested that the effect of taurine on LP
could be due to the taurine antiacidotic action as well as to its membrane stabilizing
activity.
The effect of taurine on chimpanzee spermatozoa placed under hyperosmotic
stress was studied by Ozasa and Gould, (1982). The lethal effect of osmotic stress on
spermatozoa was partially alleviated by treating the cells with 2 mM taurine, whereas
the viability of unstressed cells was not affected by this treatment. Ultrastructurally,
exposure of spermatozoa to osmotic stress was accompanied by an increase in cells
with disintegrated plasma and outer acrosomal membranes. Treatment of stressed
spermatozoa with taurine partially prevented this increase with a concomitant
enhancement of cell viability. These results suggest that taurine plays an
osmoregulatory role in chimpanzee spermatozoa, which possibly involves
stabilization of the cell membrane.
-
��
Membrane disorganization and swelling was induced by exposing the isolated
frog rod outer segments to light (5000 lux) in Pasantes-Morales and Cruz, (1985)
experiment . An increase of about 50% on lipid peroxidation, measured by the extent
of malonaldehyde formation, accompanied the light-induced damage. Taurine and
hypotaurine (25 mM) prevented the increase in lipid peroxidation, and provided an
entire protection of rod outer segment structure.
The maintenance of intracellular ions homeostasis by taurine was investigated
by Yamauchi-Takihara et al., (1988). The study was on chick heart and was
designed to investigate whether oral pretreatment with taurine or taurine added
directly to the perfusate has any effect on calcium paradox-induced heart failure. In
both protocols, taurine significantly reduced the mechanical dysfunction resulting
from the calcium paradox. Taurine pretreatment partially inhibited the excess
accumulation of calcium in the myocardium that occurs upon calcium repletion, and
microscopy revealed almost normal structure. This protective effect of taurine was
accompanied by: (a) reduction of the gain of sodium content that occurs during
calcium depletion. (b) reduction of the late gain in calcium that occurs during calcium
repletion. It is proposed that taurine plays a role in the regulation of calcium
homeostasis and membrane stabilization.
Qi et al., (1995) investigated the interrelationship between taurine and
erythrocyte-membrane Na-K ATPase activity. A comparison was conducted to test
whether taurine or uric acid (a water-soluble scavenger of free radicals) prevents or
recovers the depletion in membrane ouabain-sensitive Na-K ATPase activity resulting
-
��
from ozone exposure or cholesterol enrichment of the erythrocyte membrane. A
depletion of 44% and 27% in ouabain-sensitive Na-K ATPase activity was
respectively caused by ozone exposure and cholesterol enrichment. Taurine like uric
acid partially prevented the activity loss from ozone exposure and taurine at high
concentrations (from 1.5 to 4.5 mM) restored the depletion of erythrocyte-membrane
Na-K ATPase activity due to ozone exposure and prevented the depletion of the
enzyme activity due to cholesterol enrichment. In contrast, although the same high
concentrations were used, uric acid failed to show any of the above effects. These
results suggest that taurine acts (1.5-4.5 mM) polyvalently as an antioxidizing agent
and as a membrane stabilizer to maintain the functions of membrane Na-K ATPase.
Lombardini, (1985) showed that taurine (20 mM) stimulates ATP-dependent
calcium ion uptake by two fold in crude retinal homogenates. On the other hand, it
inhibits the phosphorylation of specific membrane proteins as shown by acrylamide
gel electrophoresis and autoradiography. The close structural analogue of taurine, 2-
aminoethylhydrogen sulfate demonstrated similar effects whereas isethionic acid and
guanidinoethanesulfonate showed no effect. A photoreceptor terminals (P1) (P1)
subcellular fraction of the retinal membrane preparation that contains photoreceptor
cell synaptosomes has a higher specific activity for the uptake of calcium ions.
Phosphorylation of specific proteins in the P1 fraction is also inhibited by the addition
of 20 mM taurine. Taurine is not affect on retinal ATPase activities or on phosphatase
activity, thus suggesting that it directly affects a kinase system.
Hino et al., (1993) studied the effect of lipopolysaccharide (LPS) and/or bile
acids on rat erythrocyte membranes in vitro. Addition of LPS isolated from E. coli
-
��
into the erythrocyte resulted in a decrease of membrane fluidity as determined by spin
labelling using electron paramagnetic resonance (EPR). This was accompanied by
membrane fragility. Hydroxyl radicals were generated from erythrocytes treated with
LPS by using 5,5-dimethylpyrroline-N-oxide (DMPO) spin trapping. However,
pretreatment of erythrocytes with taurine-conjugated bile acids was found to modify
the membrane response induced by LPS. Taurocholic acid (TCA) and
tauroursodeoxycholic acid (TUDCA) prevented the decrease of membrane fluidity
induced by LPS, and, as a result, the membrane integrity was maintained and no
significant changes were observed in the amount of hydroxyl radicals produced by
LPS addition. However, taurochenodeoxycholic acid (TCDCA) exhibited little
beneficial effect on the dynamic properties and the function of the erythrocyte
membranes, although the hydroxyl radical declined markedly in the erythrocytes.
Therefore, it is suggested that TCA and TUDCA have a protective effect against LPS-
induced membrane fragility by modulating membrane fluidity.
-
��
III. Materials and Methods
III.1. Study design
The present work was performed according to the experimental research design,
where case-control groups were compared and statistically analyzed for significant
differences of the study variables.
III.2. Target population
The target population of the present work was apparently healthy nonsmoker male
students (18-20) years old at Al-Azhar University Gaza.
III.3. Chemicals and equipments
Vacationer 5ml Tri-potassium Ethylene diamine tetra acetic acid (K3-EDTA) tubes
purchased from DISPO company, Amman-Jordan., while Taurine (99.5 % purity) was
purchased from Sigma Aldrich USA. The measurements were undertaken using an
Abbot CELLDYN 1800 Sapphire Hematology Analyzer ( Abbott Diagnostics, Santa
Clara, CA, USA ).
III.4. Methods
III.4.1. Sampling:
After the formal consent and approval of the project by the Biology
Department Council and the Deanship of Postgraduate Studies and Scientific
-
��
Research at Al-Azhar university-Gaza, the male students of the faculty of science at
Al-Azhar University-Gaza were informed and invited to participate in the study.
Twenty five students 18-20 years old were involved and all subjects were informed
about the objective and scope of the study. They accepted to participate and all
signed consent forms about the study providing their acceptance to be enrolled in the
venous blood withdrawal procedure .
Random venous blood samples (20 ml each) were collected in K3-EDTA tubes
from 25 apparently healthy nonsmoker male students at the faculty of science, Al-
Azhar university-Gaza. The collected blood was distributed almost equally into 2 sets
of K3-EDTA tubes. One set was kept at the ambient room temperature (23 ± 2 oC)
while the other set was kept at 4oC refrigerator. Each set contains four tubes. Each
tube represented a study group therefore four study groups (one control and 3
different taurine groups) were included in each set of the present study.
For each group, CBC analysis was performed and including the following
parameters and indices CBC (RBC, Hb, Hct, WBC, and PLT counts) and its related
indices (MPV, MCV, MCH, MCHC, and RDW).
CBC was performed at collection time and then daily for 7 successive days after
collection and storage. For convenient sampling, testing and retesting, 8-10 blood
samples were withdrawn in each session that extend to 7 days. This led to performing
448-560 CBC tests /8- 10 blood samples of each session.
-
��
III.4.2. Study groups
The four groups of each set were as follows:
Group I: 2.5 ml of venous blood is collected in K3-EDTA tube, and incubated
with 50 µl of normal saline solution, no addition of taurine (control group) .
Group II: 2.5 ml of venous blood is collected in K3-EDTA tube, with the
addition of 50 µl of 2.5 g/l taurine solution. (to increase taurine concentration
to 5 folds of the normal plasma taurine concentration)
Group III: 2.5 ml of venous blood is collected in K3-EDTA tube, with the
addition of 50 µl of 5 g/l taurine solution. (to increase taurine concentration to
10 folds of the normal plasma taurine concentration).
Group IV: 2.5 ml of venous blood is collected in K3-EDTA tube, with the
addition of 50 µl of 10 g/l taurine solution. (to increase taurine concentration
to 20 folds of the normal plasma taurine concentration).
Where the physiologic normal plasma taurine concentration is in the range between
35 and 60 mol/L (Trautwein and Hayes, 1990).
III.5. Statistical analysis
The results of CBC were grouped, tabulated, encoded and statistically
analyzed using the Statistical Package for the Social Sciences (SPSS) version 13.
Statistical comparison of data was carried out using the paired t-test, and one-way
analysis of variance (ANOVA). Any 2-tailed p value less than 0.05 was considered to
be statistically significant. In addition, for each parameter and indices the mean
-
��
percentage changes (mean value mean baseline value / mean baseline value x100)
was calculated and compared.
-
��
IV. Results
IV.1. Baseline values of the samples
The present work included 25 blood samples which were withdrawn from
apparently healthy, never smoker, male university students, aging 18-20 years old.
The blood from samples were divided into eight EDTA tubes, four were kept at room
temperature and the other four were kept at 4oC refrigerator. For each temperature, the
four EDTA tubes correspond to: control with zero taurine, 2.5 g/l taurine, 5 g/l
taurine, and 10 g/l taurine concentrations. The mean and standard deviation for all
CBC parameters and indices are mentioned in Table 1 for those samples stored at
room temperature and in Table 2 for those samples stored at 4oC refrigerator.
According to the ANOVA statistical test, non of these CBC parameters and indices
showed any significant differences neither as compared to the control group nor
among the taurine groups, with p-value > 0.05.
-
��
Table 1: Mean and SD of the baseline values (2-3 hours from collection) of CBC
parameters of the blood samples at room temperature**
Stored at Room temperature
Parameter Control
n= 25
2.5 g/l taurine
n= 25
5 g/l taurine
n=25
10 g/l taurine
n=25
mean SD mean SD mean SD mean SD
PLT(K�uL) 220.08 51.20 228.20 65.52 214.88 50.84 228.08 54.66
MPV(fL) 8.77 0.74 8.84 1.03 8.57 0.52 8.97 0.99
RDW (%) 13.87 1.46 13.93 1.47 13.95 1.60 13.94 1.43
RBC (M�uL) 5.04 0.70 5.04 0.66 5.01 0.66 5.05 0.67
MCV (fL) 75.10 9.65 74.94 9.52 74.63 9.54 74.80 9.78
MCH (pg) 27.61 4.06 27.48 3.92 27.59 3.95 27.42 4.07
MCHC(g�dL) 36.64 0.98 36.57 0.82 36.92 0.92 36.56 0.88
HCT (%) 37.23 2.19 37.19 2.23 36.84 2.50 37.24 2.16
HB (g�dL) 13.65 0.98 13.60 0.94 13.66 1.04 13.62 0.96
WBC (K�uL) 5.55 1.44 5.49 1.33 5.52 1.33 5.53 1.31
PLT: platelets counts, MPV: mean platelet volum, RDW: red cell distribution width, RBC:
red blood cell, MCV: mean corpuscular volume, MCH: mean corpuscular haemoglobin,
MCHC: mean corpuscular haemoglobin concentration, Hct: haematocrit, Hb: haemoglobin,
WBC: white blood cell.
** Non of these CBC parameters and indices showed any significant differences neither as
compared to the control group nor among the taurine groups, with P-value > 0.05.
-
��
Table 2 : Mean and SD of the baseline values (2-3 hours from collection) of
CBC parameters of the blood samples at 4 oC refrigerator **
Stored at 4 oC Refrigerator
Parameter Control
n= 25
2.5 g/l taurine
n= 25
5 g/l taurine
n=25
10 g/l taurine
n=25
mean SD mean SD mean SD mean SD
PLT (K�uL) 222.96 57.16 229.48 62.09 229.48 62.09 236.12 51.70
MPV (fL) 8.81 0.59 8.81 0.70 8.81 0.70 8.89 0.70
RDW (%) 13.68 1.40 13.82 1.79 13.82 1.79 13.56 1.48
RBC (M�uL) 5.05 0.75 5.10 0.74 5.10 0.74 5.07 0.75
MCV (fL) 75.23 9.85 74.41 9.93 74.41 9.93 74.69 9.70
MCH (pg) 27.69 4.24 27.43 4.17 27.43 4.17 27.53 4.08
MCHC(g�dL) 36.70 1.08 36.75 0.97 36.75 0.97 36.75 1.00
HCT (%) 37.34 2.66 37.30 2.41 37.30 2.410 37.26 2.61
HB (g�dL) 13.70 1.03 13.70 0.96 13.70 0.96 13.69 1.00
WBC (K�uL) 5.73 1.43 5.59 1.40 5.59 1.40 5.63 1.36
PLT: platelets counts, MPV: mean platelet volum, RDW: red cell distribution width, RBC:
red blood cell, MCV: mean corpuscular volume, MCH: mean corpuscular haemoglobin,
MCHC: mean corpuscular haemoglobin concentration, Hct: haematocrit, Hb: haemoglobin,
WBC: white blood cell.
** Non of these CBC parameters and indices showed any significant differences neither as
compared to the control group nor among the taurine groups, with P-value > 0.05.
-
��
IV.2. Reliability of the CBC parameters and indices
In the following sections, the effect of the different storage temperatures
(Room temperature and 4 oC refrigerator) and the storage of the EDTA blood samples
with (2.5, 5, and 10 g/l) taurine on the different CBC parameters and indices are
presented. The reliability of the different CBC parameters and indices were evaluated
in term of the stability of these parameters and indices from the baseline values. Non
significant differences or changes from the baseline values indicated a stable and so
reliable parameter or indices. The mean ± SD for all parameters and were presented
and compared to the baseline corresponding values. Moreover, for each parameter the
mean percentage changes was calculated at the different storage temperatures (Room
temperature and 4oC refrigerator) and the storage of the EDTA blood samples with
(2.5, 5, and 10 g/l) taurine along the 7 days. The mean percentage change could be
used to describe the level of precision of the reading as compared to baseline values.
So when a precision level of 5 % is acceptable this reflect a mean percentage change
of ± 5 %.
IV.2.1. Platelets count (PLT)
Tables 3 and 4 show the effect of storage temperature, storage time, and the
storage with taurine at different concentrations on the stability of platelets count.
Platelets count was significantly changed and affected by the storage temperature and
storage time. However, the storage of the EDTA blood with taurine at room
temperature considerably enhanced the stability of PLT count over the 7 days of
storage and there were no significant differences in PLT count from the 1st day values
and the 7 days of storage at room temperature. While, the storage of the EDTA blood
-
��
with taurine at 4 oC refrigerator showed no remarkable effect toward the stability of
PLT count, with some dispersed trend for storage with 5 g/l taurine. The mean
percentage changes in PLT count at the different temperature and taurine
concentrations are mentioned in Table 5. Except for the 7th day at room temperature
(11.8 %), all the values of mean percentage changes in PLT count were within ±10%.
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
-
��
��
Table 3: PLT count for samples at room temperature
Parameter Day1 Day 2 Day 3 Day 4 Day5 Day 6 Day 7
Mean SD Mean SD Mean SD Mean SD Mean SD Mean SD Mean SD
control 220.08 51.20 235.68 57.79 237.00 55.49 233.64 54.08 232.48 56.92 225.04 60.13 244.20 54.78
2.5 g/l taurine 228.20 65.52 236.96* 66.98 240.48* 76.92 232.68* 72.38 227.24* 79.36 227.64* 72.99 240.64* 68.91
5 g/l taurine 214.88 50.84 231.80 58.19 228.16* 63.31 223.60* 65.79 217.96* 67.74 214.52* 62.83 228.00* 69.92
10 g/l taurine 228.08 54.66 230.52* 65.06 233.84* 64.16 234.12* 66.97 227.96* 62.23 220.44* 64.01 241.32* 69.53
* No significant changes were reported as compared to 1st day value.
-
��
Table 4: PLT count for samples at refrigerator
Parameter Day1 Day 2 Day 3 Day 4 Day5 Day 6 Day 7
Mean SD Mean SD Mean SD Mean SD Mean SD Mean SD Mean SD
control 222.96 57.16 232.28 60.60 226.52 54.36 243.20 62.18 234.76 65.07 243.44 70.86 228.12 59.73
2.5 g/l taurine 225.76 60.36 231.32 57.28 238.20 61.68 235.16 59.34 233.16 61.81 240.68 67.47 222.32 60.85
5 g/l taurine 229.48 62.09 229.52* 58.14 232.76* 56.86 241.04 62.34 234.40* 58.51 249.48 72.92 220.32* 63.28
10 g/l taurine
236.12 51.70 244.92 48.95 244.68 48.00 248.84 47.67 243.80 46.40 246.92 50.89 228.08 55.57
* No significant changes were reported as compared to 1st day value.
-
��
Table 5: Mean percentage changes of PLT count compared to the 1st day values
Room temperature 4oC
Day2 Day3 Day4 Day5 Day6 Day7 Day2 Day3 Day4 Day5 Day6 Day7
PLT0 6.8 7.6 6.3 5.6 1.6 11.8 4.2 2.3 9.5 4.8 8.4 2.5
PLT2.5 4.3 5.8 2.3 -0.4 0.4 7.6 3.2 5.8�� 4.7�� 3.4�� 6.4 -1.5��
PLT5 8.4 6.8 4.5 1.4 0.3 6.7 0.7 2.3 5.6 2.8 8.3 -4.0
PLT10 1.0 3.2 2.8 1.3 -3.0 6.8 4.3 4.3 6.2 4.1 5.1 -3.7
-
��
��
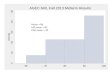
IV.2.2. Mean platelets volume (MPV)
Tables 6 and 7 showed the effect of storage temperature, storage time, and the
storage with taurine at different concentrations on the stability of mean platelets
volume (MPV). Neither the storage temperature nor the storage with taurine at the
different concentrations stabilize the MPV of the blood samples. The ANOVA
statistical test showed significant changes of MPV along the 7 days of storage, with a
trend towards an increase in the MPV of these samples. The mean percentage
changes in MPV at the different temperature and taurine concentrations are presented
in Table 8. The mean percentage change in MPV increased considerably per time and
at the 7th day it reached values of 25.4 and 28.1 % at room temperature and at 4oC
refrigerator, respectively.
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
-
��
Table 6: MPV** for samples at room temperature
Parameter Day1 Day 2 Day 3 Day 4 Day5 Day 6 Day 7
Mean SD Mean SD Mean SD Mean SD Mean SD Mean SD Mean SD
control 8.77 0.74 9.31 0.81 9.77 0.88 9.84 0.74 10.28 0.93 10.79 1.36 10.96 1.32
2.5 g/l taurine
8.84 1.03 9.23 0.66 9.72 0.49 9.91 0.72 10.18 0.84 10.41 1.64 10.45 1.18
5 g/l taurine
8.57 0.52 9.19 0.72 9.66 0.69 10.17 0.80 10.67 1.21 11.12 1.51 10.53 0.54
10 g/l taurine
8.97 0.99 9.53 0.61 9.81 1.01 9.81 0.62 10.86 2.02 10.43 0.92 11.51 2.09
** All readings are significantly different from the corresponding 1st day value.
-
��
Table 7: MPV** for samples at refrigerator
Parameter Day1 Day 2 Day 3 Day 4 Day5 Day 6 Day 7
Mean SD Mean SD Mean SD Mean SD Mean SD Mean SD Mean SD
control 8.81 0.59 9.44 0.70 9.90 0.85 10.16 1.04 10.58 1.18 11.11 1.57 11.33 1.10
2.5 g/l taurine
8.77 0.73 9.53 0.81 10.12 0.83 10.19 0.72 10.47 0.98 10.66 1.33 10.53 0.93
5 g/l taurine
8.81 0.70 9.36 0.77 10.07 0.84 9.73 0.58 10.44 0.84 10.73 1.02 11.09 0.73
10 g/l taurine 8.89 0.70 9.34 0.52 9.83 0.68 10.10 0.73 10.68 1.10 10.73 1.65 11.14 1.06
** All readings are significantly different from the corresponding 1st day value.
-
��
Table 8: Mean percentage changes of MPV compared to the 1st day values
Room temperature 4oC
Day2 Day3 Day4 Day5 Day6 Day7 Day2 Day3 Day4 Day5 Day6 Day7
MPV0 6.2 13.1 13.9 19.1 24.5 25.4 7.1 12.3 14.5 19.7 25.7 28.1
MPV2.5 7.6 13.4 15.6 18.9 20.8 24.8 8.9�� 15.7 16.6 20.0 21.5 20.4
MPV5 7.3 12.7 18.7 24.3 29.3 23.1 6.3 14.3 10.7 18.7 21.8 27.2
MPV10 9.5 12.4 12.6 24.0 19.9 31.6 5.4 10.9 13.8 20.4 20.5 25.8
��
��
��
��
-
��
��
IV.2.3. Red cell distribution width (RDW)
The possible effects of storage temperature and storage with taurine on the
RDW are illustrated in Tables 9 and 10. Table 9 showed that at room temperature the
RDW changed significantly over time stating from the second day readings. However,
the storage with taurine at the different concentrations stabilized the RDW readings
for the 48 hours from collection. While after that taurine has no stabilizing effect on
RDW at Room temperature, and all the RDW readings after the second day are
significantly differ from the baseline values.
At 4 oC refrigerator (Table 10), the RDW value is stable for 48 hours with and without
the effect of taurine. However, the storage with taurine at 5g/l enhanced the stability
of RDW value for additional 24 hours making it non-significantly changed from the
baseline value for 72 hours. On the other hand, the mean percentage changes on the
RDW are presented in Table 11, which revealed less than 10 % changes at room
temperature for the 1st 3 days, and less than 10 % changes at 4oC refrigerator for 5
days.
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
-
��
Table 9: RDW for samples at room temperature
Parameter Day1 Day 2 Day 3 Day 4 Day5 Day 6 Day 7
Mean SD Mean SD Mean SD Mean SD Mean SD Mean SD Mean SD
control 13.87 1.46 14.33 1.60 14.75 1.42 15.62 1.70 15.93 1.28 15.49 1.28 15.53 1.43
2.5 g/l taurine
13.93 1.47 14.06* 1.70 15.25 1.40 15.66 1.27 15.20 1.73 15.29 1.57 15.32 1.55
5 g/l taurine
13.95 1.60 14.12* 1.49 15.07 1.16 15.68 1.44 15.47 1.24 15.54 1.34 15.38 1.43
10 g/l taurine
13.94 1.43 13.91* 1.71 15.13 1.60 15.69 1.55 15.54 1.27 15.41 1.34 15.63 0.98
* No significant changes were reported as compared to 1st day value.
-
��
Table 10: RDW for samples at refrigerator
Parameter Day1 Day 2 Day 3 Day 4 Day5 Day 6 Day 7
Mean SD Mean SD Mean SD Mean SD Mean SD Mean SD Mean SD
control 13.68 1.40 13.83* 1.52 14.26 1.60 14.52 1.29 14.91 1.15 15.37 1.34 15.98 0.85
2.5 g/l taurine 13.81 1.42 13.77* 1.61 14.26 1.42 14.51 1.29 14.83 1.15 15.39 1.29 15.62 1.01
5 g/l taurine 13.82 1.79 13.52* 1.30 13.88* 1.35 14.36 1.40 14.93 1.25 15.54 1.48 15.63 1.32
10 g/l taurine 13.56 1.48 13.78* 1.75 14.22 1.32 14.35 1.37 15.00 1.27 15.63 1.10 15.70 1.17
* No significant changes were reported as compared to 1st day value.
-
��
Table 11: Mean percentage changes of RDW compared to the 1st day values
Room temperature 4oC
Day2 Day3 Day4 Day5 Day6 Day7 Day2 Day3 Day4 Day5 Day6 Day7
RDW0 3.4 6.5 12.7 15.2 12.1 12.3 1.2 4.3 6.3 9.4 12.7 17.6
RDW2.5 0.9 9.7 12.8 9.2 10.0 10.1 -0.4 3.4 5.2 7.8 11.8 13.8
RDW5
1.3 8.5 12.9 11.5 11.9 10.6 -1.7 0.9 4.5 9.0 13.3 13.8
RDW10 -0.1 8.7 12.8 11.8 10.8 12.7 1.6 5.2 6.2 11.2 15.9 16.5
��
��
-
��
��
��
IV.2.4. Red blood cell count (RBC)
Tables 12 and 13 show the effects of the different factors (storage time,
temperature, and addition of taurine) on the red blood cell count of the study samples.
Table 12 showed the instability of the RBC over time and the values were
significantly different from the baseline( p-value 0.05). Furthermore, Table 14, showed that the mean percentage changes in
RBC count is almost 3 % and 2.2 % at room and 4 oC refrigerator temperatures at the
7th day, respectively. While the addition of 2.5 g/l taurine reduces these mean
percentage changes to 1.6 and 1.2%, respectively.
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
-
��
Table 12: RBC count for samples at room temperature
Parameter Day1 Day 2 Day 3 Day 4 Day5 Day 6 Day 7
Mean SD Mean SD Mean SD Mean SD Mean SD Mean SD Mean SD
control 5.04 0.70 5.13 0.70 5.13 0.73 5.13 0.72 5.13 0.72 5.06 0.76 5.19 0.72
2.5 g/l taurine
5.04 0.66 5.09 0.67 5.14 0.68 5.08 0.70 5.09 0.73 4.99 0.72 5.12 0.71
5 g/l taurine
5.01 0.66 5.10 0.69 5.14 0.72 5.13 0.71 5.11 0.75 5.01 0.72 5.15 0.72
10 g/l taurine
5.05 0.67 5.09* 0.72 5.12 0.72 5.09* 0.74 5.06* 0.71 4.96 0.71 5.15 0.74
* No significant changes were reported as compared to 1st day value.
-
��
Table 13: RBC count for samples at refrigerator
Parameter Day1 Day 2 Day 3 Day 4 Day5 Day 6 Day 7
Mean SD Mean SD Mean SD Mean SD Mean SD Mean SD Mean SD
control 5.05 0.75 5.10 0.74 5.13 0.75 5.13 0.75 5.16 0.77 5.08 0.81 5.16 0.77
2.5 g/l taurine
5.11 0.76 5.16 0.73 5.16 0.72 5.19 0.72 5.19 0.73 5.09 0.75 5.17 0.77
5 g/l taurine
5.10 0.74 5.17 0.73 5.16 0.70 5.22 0.73 5.23 0.71 5.10 0.75 5.20 0.73
10 g/l taurine 5.07 0.75 5.16 0.73 5.17 0.72 5.21 0.73 5.21 0.73 5.05 0.71 5.17 0.74
* No significant changes were reported as compared to 1st day value.
-
��
Table 14: Mean percentage changes of RBC compared to the 1st day values
Room temperature 4oC
Day2 Day3 Day4 Day5 Day6 Day7 Day2 Day3 Day4 Day5 Day6 Day7
RBC0 1.9 1.9 1.9 1.9 0.3 3.0 1.1 1.6 1.7 2.1 0.4 2.2
RBC2.5 1.1 2.1 0.8 0.9 -1.1 1.6 1.2 1.3 1.8 1.8 -0.2 1.2
RBC5 1.9 2.6 2.4 1.9 -0.1 2.9 1.5 1.5 2.5 2.8 0.1 2.1
RBC10 0.7 1.3 0.6 0.0 -1.9 1.8 1.8 2.1 2.9 2.8 -0.4 2.1
��
��
��
��
-
��
��
IV.2.5. Mean corpuscular volume (MCV)
The stability of mean corpuscular volume (MCV) over the 7 days is summarized in
Table 15 for those samples kept at room temperature and in Table 16 for samples kept
at 4oC refrigerator. At all the investigated concentrations, taurine did not enhance the
stability of MCV neither at room temperature nor at 4oC refrigerator. However, MCV
reading itself was stable for 2 days both at room temperature and at 4oC refrigerator,
with no significant differences between the 1st and 2nd days readings. Moreover, the
mean percentage changes of MCV values (Table 17) were found to be increased by
time but these changes were lower when samples are at 4oC refrigerator, with value of
almost 10 % at day 7.
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
��
-
��
Table 15: MCV for samples at room temperature
Parameter Day1 Day 2 Day 3 Day 4 Day5 Day 6 Day 7
Mean SD Mean SD Mean SD Mean SD Mean SD Mean SD Mean SD
control 75.10 9.65 76.36* 10.05 78.00 10.06 80.93 10.51 83.42 11.29 84.58 11.43 85.85 11.78
2.5 g/l taurine 74.94 9.52 75.62 9.49 77.92 10.03 81.13 10.52 83.29 11.03 84.54 11.34 85.64 11.69
5 g/l taurine 74.63 9.54 75.62 9.51 78.02 9.88 81.12 10.50 83.48 11.04 84.87 11.48 85.78 11.82
10 g/l taurine 74.80 9.78 76.21 9.89 78.02 9.91 81.12 10.62 83.45 11.19 84.76 11.48 85.66 11.61
* No significant changes were reported as compared to 1st day value.
-
��
Table 16 : MCV for samples at refrigerator
Parameter Day1 Day 2 Day 3 Day 4 Day5 Day 6 Day 7
Mean SD Mean SD Mean SD Mean SD Mean SD Mean SD Mean SD
control 75.23 9.85 75.28 10.11 76.00 10.01 78.97 11.29 78.17 10.14 80.62 10.42 82.82 10.93
2.5 g/l taurine
74.30 9.99 74.97 9.58 75.35 9.88 76.65 9.98 78.02 9.99 80.36 10.27 82.44 10.52
5 g/l taurine
74.41 9.93 74.50 9.35 75.49 9.86 76.52 10.06 77.90 10.00 80.32 10.20 82.25 10.56
10 g/l taurine 74.69 9.70 74.54 9.58 75.24 9.71 76.40 9.90 77.88 10.21 80.37 10.51 82.38 10.79
* No significant changes were reported as compared to 1st day value.
-
��
Table 17: Mean percentage changes of MCV compared to 1st day values
Room temperature 4oC
Day2 Day3 Day4 Day5 Day6 Day7 Day2 Day3 Day4 Day5 Day6 Day7
MCV0 1.7 3.9 7.7 11.0 12.5 14.2 0.0 1.0 5.2 3.9 7.2 10.1
MCV2.5 0.9 4.0 8.2 11.1 12.7 14.1 1.0 1.5 3.3 5.1 8.3 11.1
MCV5 1.4 4.6 8.7 11.8 13.6 14.8 0.2 1.5 2.9 4.8 8.1 10.6
MCV10 1.9 4.4 8.4 11.5 13.2 14.4 -0.2 0.8 2.3 4.3 7.6 10.3
��
��
��
��
��
-
��
��
IV.2.6. Mean corpuscular hemoglobin (MCH)
Mean corpuscular hemoglobin readings were found to be unstable along the
7days both at room temperature and at 4oC refrigerator, (Tables 18 and 19,
respectively). But, the addition of taurine to these samples was found to exert some
stability on the MCH readings both at room temperature and at 4oC refrigerator. At
room temperature storage EDTA blood with 10 g/l taurine enhances the stability of
MCH over 5 days f
Related Documents