nature publishing group 1350 The American Journal of GASTROENTEROLOGY VOLUME 109 | SEPTEMBER 2014 www.amjgastro.com REVIEW CLINICAL AND SYSTEMATIC REVIEWS INTRODUCTION Irritable bowel syndrome (IBS) is one of the commonest functional gastrointestinal disorders worldwide, with a prev- alence of between 5 and 20%, depending on the criteria used to define its presence (1). Although the condition is more common in women and in younger individuals, evidence for the effect of socioeconomic status on prevalence is conflict- ing (2). Patients with IBS take more sickness-related absences from work than those without bowel symptoms (3). A recent burden-of-illness study in the United States estimated that IBS cost almost $1 billion in direct costs and another $50 million in indirect costs (4). In addition, patients with IBS Effect of Antidepressants and Psychological Therapies, Including Hypnotherapy, in Irritable Bowel Syndrome: Systematic Review and Meta-Analysis Alexander C. Ford, MBChB, MD 1,2 , Eamonn M.M. Quigley , MD, FRCP, FACP, FACG, FRCPI 3 , Brian E. Lacy, MD, PhD 4 , Anthony J. Lembo 5 , Yuri A. Saito 6 , Lawrence R. Schiller , MD, MSHS, RFF, FACG, AGAF 7 , Edy E. Soffer 8 , Brennan M.R. Spiegel, MD, MSHS, RFF, FACG, AGAF 9 and Paul Moayyedi, MBChB, PhD, MPH, FACG 10 OBJECTIVES: Irritable bowel syndrome (IBS) is a chronic functional gastrointestinal disorder. Evidence relating to the treatment of this condition with antidepressants and psychological therapies continues to accumulate. METHODS: We performed an updated systematic review and meta-analysis of randomized controlled trials (RCTs). MEDLINE, EMBASE, and the Cochrane Controlled Trials Register were searched (up to December 2013). Trials recruiting adults with IBS, which compared antidepressants with placebo, or psychological therapies with control therapy or “usual management,” were eligible. Dichotomous symptom data were pooled to obtain a relative risk (RR) of remaining symptomatic after therapy, with a 95% confidence interval (CI). RESULTS: The search strategy identified 3,788 citations. Forty-eight RCTs were eligible for inclusion: thirty-one compared psychological therapies with control therapy or “usual management,” sixteen compared antidepressants with placebo, and one compared both psychological therapy and antidepressants with placebo. Ten of the trials of psychological therapies, and four of the RCTs of antidepressants, had been published since our previous meta-analysis. The RR of IBS symptom not improving with antidepressants vs. placebo was 0.67 (95% CI = 0.58–0.77), with similar treatment effects for both tricyclic antidepressants and selective serotonin reuptake inhibitors. The RR of symptoms not im- proving with psychological therapies was 0.68 (95% CI = 0.61–0.76). Cognitive behavioral therapy, hypnotherapy, multicomponent psychological therapy, and dynamic psychotherapy were all beneficial. CONCLUSIONS: Antidepressants and some psychological therapies are effective treatments for IBS. Despite the considerable number of studies published in the intervening 5 years since we last examined this issue, the overall summary estimates of treatment effect have remained remarkably stable. Am J Gastroenterol 2014; 109:1350–1365; doi:10.1038/ajg.2014.148; published online 17 June 2014 1 Leeds Gastroenterology Institute, St James’s University Hospital, Leeds, UK; 2 Leeds Institute of Biomedical and Clinical Sciences, University of Leeds, Leeds, UK; 3 Division of Gastroenterology and Hepatology, Department of Medicine, Houston Methodist Hospital, Houston, Texas, USA; 4 Dartmouth-Hitchcock Medical Center, Gastroenterology , Lebanon, New Hampshire, USA; 5 The Beth Israel Deaconess Medical Center , Boston, Massachusetts, USA; 6 Division of Gastroenterology and Hepatology, Mayo Clinic, Rochester, Minnesota, USA; 7 Digestive Health Associates of Texas, Baylor University Medical Center , Dallas, Texas, USA; 8 Division of Gastroenterology at Cedars-Sinai, University of Southern California, Los Angeles, Califoria, USA; 9 Department of Gastroenterology, VA Greater Los Angeles Healthcare System, Los Angeles, California, USA; 10 Division of Gastroenterology, McMaster University, Health Sciences Center , Hamilton, Ontario, Canada. Correspondence: Alexander C. Ford, MBChB, MD, Leeds Gastroenterology Institute, St James’s University Hospital, Beckett Street, Room 125, 4th Floor, Bexley Wing, Leeds LS9 7TF UK. E-mail: [email protected] Received 25 February 2014; accepted 29 April 2014 CME

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

nature publishing group1350
The American Journal of GASTROENTEROLOGY VOLUME 109 | SEPTEMBER 2014 www.amjgastro.com
see related editorial on page x
REV
IEW
CLINICAL AND SYSTEMATIC REVIEWS
INTRODUCTION Irritable bowel syndrome (IBS) is one of the commonest functional gastrointestinal disorders worldwide, with a prev-alence of between 5 and 20 % , depending on the criteria used to define its presence ( 1 ). Although the condition is more common in women and in younger individuals, evidence for
the effect of socioeconomic status on prevalence is conflict-ing ( 2 ). Patients with IBS take more sickness-related absences from work than those without bowel symptoms ( 3 ). A recent burden-of-illness study in the United States estimated that IBS cost almost $ 1 billion in direct costs and another $ 50 million in indirect costs ( 4 ). In addition, patients with IBS
Effect of Antidepressants and Psychological Therapies, Including Hypnotherapy, in Irritable Bowel Syndrome: Systematic Review and Meta-Analysis Alexander C. Ford , MBChB, MD 1 , 2 , Eamonn M.M. Quigley , MD, FRCP, FACP, FACG, FRCPI 3 , Brian E. Lacy , MD, PhD 4 , Anthony J. Lembo 5 , Yuri A. Saito 6 , Lawrence R. Schiller , MD, MSHS, RFF, FACG, AGAF 7 , Edy E. Soff er 8 , Brennan M.R. Spiegel , MD, MSHS, RFF, FACG, AGAF 9 and Paul Moayyedi , MBChB, PhD, MPH, FACG 10
OBJECTIVES: Irritable bowel syndrome (IBS) is a chronic functional gastrointestinal disorder. Evidence relating to the treatment of this condition with antidepressants and psychological therapies continues to accumulate.
METHODS: We performed an updated systematic review and meta-analysis of randomized controlled trials (RCTs). MEDLINE, EMBASE, and the Cochrane Controlled Trials Register were searched (up to December 2013). Trials recruiting adults with IBS, which compared antidepressants with placebo, or psychological therapies with control therapy or “ usual management, ” were eligible. Dichotomous symptom data were pooled to obtain a relative risk (RR) of remaining symptomatic after therapy, with a 95 % confi dence interval (CI).
RESULTS: The search strategy identifi ed 3,788 citations. Forty-eight RCTs were eligible for inclusion: thirty-one compared psychological therapies with control therapy or “ usual management, ” sixteen compared antidepressants with placebo, and one compared both psychological therapy and antidepressants with placebo. Ten of the trials of psychological therapies, and four of the RCTs of antidepressants, had been published since our previous meta-analysis. The RR of IBS symptom not improving with antidepressants vs. placebo was 0.67 (95 % CI = 0.58 – 0.77), with similar treatment effects for both tricyclic antidepressants and selective serotonin reuptake inhibitors. The RR of symptoms not im-proving with psychological therapies was 0.68 (95 % CI = 0.61 – 0.76). Cognitive behavioral therapy, hypnotherapy, multicomponent psychological therapy, and dynamic psychotherapy were all benefi cial.
CONCLUSIONS: Antidepressants and some psychological therapies are effective treatments for IBS. Despite the considerable number of studies published in the intervening 5 years since we last examined this issue, the overall summary estimates of treatment effect have remained remarkably stable.
Am J Gastroenterol 2014; 109:1350–1365; doi: 10.1038/ajg.2014.148; published online 17 June 2014
1 Leeds Gastroenterology Institute, St James ’ s University Hospital , Leeds , UK ; 2 Leeds Institute of Biomedical and Clinical Sciences, University of Leeds , Leeds , UK ; 3 Division of Gastroenterology and Hepatology, Department of Medicine, Houston Methodist Hospital , Houston , Texas , USA ; 4 Dartmouth-Hitchcock Medical Center, Gastroenterology , Lebanon, New Hampshire, USA ; 5 The Beth Israel Deaconess Medical Center , Boston , Massachusetts , USA ; 6 Division of Gastroenterology and Hepatology, Mayo Clinic , Rochester , Minnesota , USA ; 7 Digestive Health Associates of Texas, Baylor University Medical Center , Dallas , Texas , USA ; 8 Division of Gastroenterology at Cedars-Sinai, University of Southern California , Los Angeles , Califoria , USA ; 9 Department of Gastroenterology, VA Greater Los Angeles Healthcare System , Los Angeles , California , USA ; 10 Division of Gastroenterology, McMaster University, Health Sciences Center , Hamilton , Ontario , Canada . Correspondence: Alexander C. Ford, MBChB, MD , Leeds Gastroenterology Institute, St James ’ s University Hospital , Beckett Street , Room 125, 4th Floor, Bexley Wing, Leeds LS9 7TF UK . E-mail: [email protected] Received 25 February 2014; accepted 29 April 2014
CME

© 2014 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY
1351
REV
IEW
Antidepressants and Psychological Therapies in IBS
consume > 50 % more health-care resources than matched controls without IBS ( 5 ).
Eff ective treatment of IBS is therefore extremely important for the individual, health-care systems, and society as a whole. However, the cause of IBS remains obscure, meaning that there is no single unifying explanation for the symptoms toward which therapy can be targeted. Patients with IBS demonstrate visceral hypersensitivity to painful stimuli ( 6,7 ), abnormal cen-tral processing of pain ( 8 ), and higher levels of psychological comorbidity compared with healthy controls without IBS ( 9,10 ). As a result, antidepressants, which have pain-modifying proper-ties ( 11,12 ), and psychological therapies have been proposed as potential treatments for IBS.
Despite the fact that the use of antidepressants in IBS is wide-spread ( 13 ), until recently the evidence for their effi cacy was dis-puted, partly owing to the fact that previous systematic reviews and meta-analyses that had examined this issue had limitations ( 14 ). In addition, despite the fact that the use of psychological therapies is recommended for the management of IBS by previ-ous guidelines ( 15,16 ), access to these interventions is limited in some countries, and there may also be a reluctance on the part of physicians to consider referral ( 17 ). In our previous systematic review and meta-analysis ( 18 ), conducted to inform the American College of Gastroenterology ’ s monograph on the management of IBS ( 15 ), we summarized all available evidence for both antide-pressants and psychological therapies up to 2009. However, in the intervening 5 years, there has been a considerable amount of evi-dence published. We have therefore re-examined this issue.
METHODS Search strategy and study selection We updated our previous systematic review and meta-analy-sis ( 18 ). A search of the medical literature was conducted using MEDLINE (1946 to December 2013), EMBASE, and EMBASE Classic (1947 to December 2013), and the Cochrane central register of controlled trials. Randomized controlled trials (RCT) examining the eff ect of antidepressants and psychological thera-pies in adult patients (over the age of 16 years) with IBS were eligible for inclusion ( Box 1 ). Th e fi rst period of crossover RCTs, before crossover to the second treatment, were also eligible for inclusion. In the case of antidepressant trials, the control arms were required to receive placebo, whereas for studies of psycho-logical therapies the control arm could receive placebo, symptom monitoring (including waiting list control), or a physician ’ s “ usual management. ”
Duration of therapy had to be at least 7 days. Th e diagnosis of IBS could be based on either a physician ’ s opinion or symptom-based diagnostic criteria, supplemented by the results of investiga-tions to exclude organic disease, where the investigators deemed this necessary. Subjects were required to be followed up for at least 1 week, and studies had to report either a global assessment of IBS symptom cure or improvement, or abdominal pain cure or improvement, aft er completion of therapy, preferably as reported by the patient, but if this was not recorded then as documented by
the investigator or via questionnaire data. Where studies included patients with IBS among patients with other functional gastroin-testinal disorders, or did not report these types of dichotomous data but were otherwise eligible for inclusion in the systematic review, we attempted to contact the original investigators in order to obtain further information.
Th e literature search was performed as part of a broader exer-cise to inform an update of the American College of Gastroen-terology ’ s monograph on the management of IBS. Specifi cally, studies on IBS were identifi ed with the terms irritable bowel syndrome and functional diseases, colon (both as medical sub-ject heading and free text terms), and IBS , spastic colon , irri-table colon , or functional adj5 bowel (as free text terms). Th ese were combined using the set operator AND with studies identi-fi ed with the following terms: psychotropic drugs , antidepressive agents , antidepressive agents (tricyclic) , desipramine , imipramine , trimipramine , doxepin, dothiepin, nortriptyline , amitriptyline , selective serotonin reuptake inhibitors , paroxetine, sertraline, fl uoxetine, citalopram, venlafaxine, cognitive therapy, psychother-apy, behavior therapy, relaxation techniques, or hypnosis (both as medical subject heading terms and free text terms). Th e fol-lowing free text terms were used: behavioral therapy , relaxation therapy , or hypnotherapy .
Th ere were no language restrictions, and abstracts of the papers identifi ed by the initial search were evaluated by the lead reviewer for appropriateness to the study question, and all potentially rel-evant papers were obtained and evaluated in detail. Foreign lan-guage papers were translated where necessary. Abstract books of conference proceedings between 2001 and 2013 were hand-searched to identify potentially eligible studies published only in abstract form. Th e bibliographies of all identifi ed relevant studies were used to perform a recursive search of the literature. Articles were independently assessed by two reviewers using predesigned eligibility forms, according to the prospectively defi ned eligibility criteria. Any disagreement between investigators was resolved by consensus.
Box 1. Eligibility criteria
Randomized controlled trials. Adults (participants aged > 16 years). Diagnosis of IBS based on either a clinician ’ s opinion or meeting specifi c diagnostic criteria * , supplemented by negative investigations where trials deemed this necessary. Comparison of antidepressants with placebo, or psychological therapies with a control therapy, including a physician ’ s “ usual management, ” symptom monitoring, supportive therapy, or placebo . Minimum duration of therapy 7 days. Minimum duration of follow-up 7 days. Dichotomous assessment of response to therapy in terms of effect on global IBS symptoms or abdominal pain following therapy. † * Manning, Kruis score, Rome I, II, or III. † Preferably patient-reported, but if this was not available then as assessed by a physician or questionnaire data.

The American Journal of GASTROENTEROLOGY VOLUME 109 | SEPTEMBER 2014 www.amjgastro.com
1352R
EVIE
W Ford et al.
Data synthesis and statistical analysis Data were pooled using a random-effects model ( 20 ), to give a more conservative estimate of the effect of antidepressants and psychological therapies, allowing for any heterogeneity between studies. The impacts of different interventions were expressed as a relative risk (RR) of global IBS symptoms or abdominal pain not improving with intervention compared with control with 95 % confidence intervals (CIs). Adverse events data were also summarized with RRs. The number needed to treat (NNT) and the number needed to harm, with 95 % CIs, were calculated from the reciprocal of the risk differ-ence of the meta-analysis.
Heterogeneity, which is variation between individual study results arising as a result of either diff erences in study partici-pants or methodology, was assessed using both the I 2 statistic with a cutoff of ≥ 50 % , and the χ 2 test with a P -value < 0.10, used to defi ne a signifi cant degree of heterogeneity ( 21 ). Where the degree of statistical heterogeneity was greater than this between-trial results in this meta-analysis, possible explanations were investigated using subgroup analyses according to the type of antidepressant or psychological therapy used, trial setting, cri-teria used to defi ne IBS, whether method of randomization or concealment of allocation were reported, level of blinding, risk of bias of included trials, and, for trials of psychological therapies, method of handling of the control arm. We compared individual RRs between these analyses using the Cochran Q statistic. Th ese were exploratory analyses only, and they may explain some of the observed variability, but the results should be interpreted with caution.
Review Manager version 5.1.4 (RevMan for Windows 2008, the Nordic Cochrane Centre, Copenhagen, Denmark) and Stats-Direct version 2.7.7 (StatsDirect, Cheshire, England) were used to generate Forest plots of pooled RRs and risk diff erences for primary and secondary outcomes with 95 % CIs, as well as fun-nel plots. Th e latter were assessed for evidence of asymmetry, and therefore possible publication bias or other small study eff ects, using the Egger test ( 22 ), if there were suffi cient (10 or more) eli-gible studies included in the meta-analysis, in line with recent recommendations ( 23 ).
RESULTS Th e search strategy identifi ed a total of 3,788 citations, of which 92 published articles appeared to be relevant and were retrieved for further assessment ( Figure 1 ). Of these 92 articles, 46 were excluded for various reasons, leaving 46 eligible articles, 29 of which compared psychological therapies with control therapy in the form of symptom monitoring, physician ’ s “ usual manage-ment, ” or supportive therapy, 16 compared antidepressants with placebo, and one compared both psychological therapies and antidepressants with placebo. Agreement between reviewers for assessment of trial eligibility was excellent (kappa statistic = 0.93). Ten of the trials of psychological therapies, and four of the RCTs of antidepressants, had been published since our previous meta-analysis.
Outcome assessment Th e primary outcomes assessed were the eff ects of antidepressants compared with placebo, and the eff ects of psychological therapies compared with control therapy or a physician ’ s “ usual manage-ment, ” on global IBS symptoms or abdominal pain aft er cessation of therapy. Secondary outcomes included assessing effi cacy accord-ing to a specifi c type of antidepressant or psychological therapy, and adverse events occurring as a result of therapy.
Data extraction All data were extracted independently by two reviewers on to a Microsoft Excel spreadsheet (XP professional edition; Microsoft , Redmond, WA) as dichotomous outcomes (global IBS symp-toms unimproved, or abdominal pain unimproved; Box 2 ). In addition, the following clinical data were extracted for each trial: setting (primary, secondary, or tertiary care-based), number of centers, country of origin, dose of antidepressant or number of sessions of psychological therapy administered, duration of therapy, total number of adverse events reported, criteria used to defi ne IBS, primary outcome measure used to defi ne symp-tom improvement or cure following therapy, duration of follow-up, proportion of female patients, and proportion of patients according to predominant stool pattern. We also recorded the handling of the control arm for trials of psychological therapies. Data were extracted as intention-to-treat analyses, with all drop-outs assumed to be treatment failures, wherever trial reporting allowed this.
Assessment of risk of bias Th is was performed independently by two investigators, with disagreements resolved by discussion. Risk of bias was assessed as described in the Cochrane handbook ( 19 ), by recording the method used to generate the randomization schedule and conceal allocation, whether blinding was implemented, what proportion of patients completed follow-up, whether an intention-to-treat analysis was extractable, and whether there was evidence of selective reporting of outcomes.
Box 2. Data extraction methodology
Outcome of interest: Improvement in global IBS symptoms preferable; if this was not reported then improvement in abdominal pain. Reporting of outcomes: Patient-reported was preferable; if this was not available then investigator-reported. Time of assessment: Upon completion of therapy. Denominator used: True intention-to-treat analysis; if this was not available then all evaluable patients. Cutoff used for dichotomization: Any improvement in global IBS symptoms or abdominal pain for Likert-type scales, investigator-defi ned improvement for continuous scales; if no investigator defi nition was available then we used ≥ 1 s.d. decrease in symptom score from baseline to completion of therapy (we assessed if the use of any decrease in symp-tom score from baseline to completion of therapy altered our analysis).

© 2014 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY
1353
REV
IEW
Antidepressants and Psychological Therapies in IBS
Effi cacy of antidepressants in the treatment of IBS In total, there were 17 RCTs comparing antidepressants with placebo in the treatment of IBS ( 24 – 40 ), which evaluated 1,084 patients, 592 of whom received active therapy and 492 received placebo. Ten trials used tricyclic antidepressants (TCAs) ( 24 – 26,28,29,34 – 38 ), six used selective serotonin reuptake inhibi-tor (SSRIs) ( 27,30,31,33,39,40 ), and one studied both ( 32 ). Only three of the RCTs were at a low risk of bias ( 36,38,39 ). Th e propor-tion of female patients recruited by trials ranged from 42 to 100 % . Th e majority of trials did not diff erentiate between the type of IBS patients recruited, with only seven studies providing data on this ( 27,30,31,33 – 35,39 ), one of which recruited only IBS-C patients ( 33 ) and another recruited only IBS-D patients ( 34 ). Detailed characteristics of individual RCTs are provided in Table 1 .
Overall, 260 (43.9 % ) of 592 patients assigned to antidepressant therapy reported unimproved IBS symptoms following therapy, compared with 330 (65.0 % ) of 508 patients allocated to placebo. Th e RR of IBS symptoms not improving aft er treatment with anti-depressant therapy vs. placebo was 0.67 (95 % CI = 0.58 – 0.77), with marginally signifi cant heterogeneity detected between studies
( I 2 = 37 % , P = 0.06; Figure 2 ). Th ere was statistically signifi cant asymmetry in the funnel plot (Egger test, P = 0.05), suggesting publication bias or other small study eff ects; however, this was driven by the TCA arm of one small study ( 32 ) and disappeared with its exclusion from the analysis (Egger test, P = 0.13). Th e NNT with antidepressants was 4 (95 % CI = 3 – 6).
Subgroup analyses were conducted ( Table 2 ). Treatment eff ect appeared to be increased in secondary care-based studies, studies that did not state the method of generation of the randomization schedule or method of concealment of allocation, and studies at a high or unclear risk of bias. A statistically signifi cant diff erence in treatment eff ect was detected for study setting and level of blind-ing only.
Th e eff ect of antidepressant therapy on abdominal pain was reported by seven RCTs ( 26,27,30,33 – 35,38 ), with 87 (47.8 % ) of 182 patients receiving antidepressants having no improvement in abdominal pain following treatment, compared with 123 (72.8 % ) of 169 subjects allocated to placebo, and the RR of abdominal pain not improving was 0.62 (95 % CI = 0.43 – 0.88), with considerable heterogeneity between studies ( I 2 = 72.4 % , P = 0.001).
Effi cacy of TCAs in the treatment of IBS . Eleven RCTs compared TCAs with placebo, including a total of 744 patients ( 24 – 26,28,29,32,34 – 38 ). Of 416 patients receiving active therapy, 180 (43.3 % ) had no improvement in symptoms aft er treatment, compared with 209 (63.7 % ) of 328 receiving placebo. Th e RR of IBS symptoms not improving with TCAs compared with placebo was 0.66 (95 % CI = 0.56 – 0.79), with no statistically signifi cant hetero-geneity detected between studies ( I 2 = 35 % , P = 0.12; Figure 2 ), and evidence of funnel plot asymmetry (Egger test, P = 0.02). Again, this was driven by one study ( 32 ), and when this was removed from the analysis there was no longer statistically signifi cant publication bias (Egger test, P = 0.06). Th e NNT with TCAs was 4 (95 % CI = 3 – 6).
Effi cacy of SSRIs in the treatment of IBS . Seven trials compared SSRIs with placebo in a total of 356 patients ( 27,30 – 33,39,40 ). In all, 80 (45.5 % ) of 176 patients allocated to SSRIs had no improve-ment in symptoms following therapy, compared with 121 (67.2 % ) of 180 placebo patients . Th e RR of IBS symptoms not improving with SSRIs compared with placebo was 0.68 (95 % CI = 0.51 – 0.91), but with statistically signifi cant heterogeneity between studies ( I 2 = 49 % , P = 0.07; Figure 2 ). Th e NNT with SSRIs was 4 (95 % CI = 2.5 – 20).
Adverse events with antidepressant therapy Only seven trials reported on overall adverse events with antide-pressants vs. placebo ( 25 – 28,31,35,37 ). In total, 65 (31.3 % ) of 208 patients assigned to antidepressants experienced adverse events, compared with 33 (16.5 % ) of 200 patients allocated to placebo. When data were pooled, the incidence of adverse events was signifi cantly higher among those taking antidepressants (RR of experiencing any adverse event = 1.63; 95 % CI = 1.18 – 2.25). Th e number needed to harm was 9 (95 % CI = 5 – 111). Th ere were no serious adverse events. Drowsiness and dry mouth were more
Excluded (n=46) because:
•
•
••
•
•
•
•
•
No dichotomous data reported=10
Dual publication=9
Not the control intervention ofinterest=5
Cross-over study with noextractable data=4
No placebo or comparator arm=4
Not randomized=3
Review article=2
Study protocol only=1
Studies identified in literaturesearch (n=3,788)
Studies retrieved for evaluation(n=92)
Excluded (title and abstract revealednot appropriate) (n=3,696)
Outcome of interest not reported=8
Eligible studies (n=46):Psychologicaltherapies=29Antidepressants=16Psychologicaltherapies andantidepressants=1
•
••
Figure 1 . Flow diagram of assessment of studies identifi ed in the updated systematic review and meta-analysis.

The American Journal of GASTROENTEROLOGY VOLUME 109 | SEPTEMBER 2014 www.amjgastro.com
1354R
EVIE
W Ford et al.
Tabl
e 1 .
Cha
ract
eris
tics
of r
ando
miz
ed c
ontr
olle
d tr
ials
of
antid
epre
ssan
ts v
s. p
lace
bo in
IB
S
Stud
y Co
untr
y Se
ttin
g
Dia
gnos
tic
crite
ria u
sed
for
IBS
Crite
ria u
sed
to d
efi n
e sy
mpt
om im
prov
emen
t fo
llow
ing
ther
apy
Sam
ple
size
( %
fem
ale)
An
tidep
ress
ant
used
D
urat
ion
of
ther
apy
Met
hodo
logy
Hee
fner
( 26 )
U
SA
Terti
ary
care
Cl
inic
al
diag
nosi
s an
d in
vest
igat
ions
Patie
nt-r
epor
ted
impr
ove-
men
t in
abdo
min
al p
ain
44 (N
ot
repo
rted)
D
esip
ram
ine
150
mg
o.d.
2
Mon
ths
Met
hod
of ra
ndom
izat
ion
and
conc
ealm
ent o
f al-
loca
tion
not s
tate
d. D
oubl
e-bl
ind.
Unc
lear
if o
ther
IB
S m
edic
atio
ns a
llow
ed
Myr
en ( 2
8 )
Nor
way
Se
cond
ary
care
Cl
inic
al
diag
nosi
s an
d in
vest
igat
ions
Patie
nt-r
epor
ted
impr
ove-
men
t in
glob
al s
ympt
oms
61 (5
5)
Trim
ipra
min
e 50
mg
o.d.
4
Wee
ks
Met
hod
of ra
ndom
izat
ion
and
conc
ealm
ent o
f al
loca
tion
not s
tate
d. D
oubl
e-bl
ind.
No
othe
r IB
S m
edic
atio
ns a
llow
ed
Nig
am ( 2
9 )
Indi
a Se
cond
ary
care
Cl
inic
al
diag
nosi
s an
d in
vest
igat
ions
Patie
nt-r
epor
ted
impr
ove-
men
t in
glob
al s
ympt
oms
42 (N
ot
repo
rted)
Am
itrip
tylin
e 12
.5 m
g o.
d.
12 W
eeks
M
etho
d of
rand
omiz
atio
n an
d co
ncea
lmen
t of a
l-lo
catio
n no
t sta
ted.
Dou
ble-
blin
d. U
ncle
ar if
oth
er
IBS
med
icat
ions
allo
wed
Boe
rner
( 25 )
G
erm
any
Seco
ndar
y ca
re
Clin
ical
di
agno
sis
and
inve
stig
atio
ns
Patie
nt-r
epor
ted
impr
ove-
men
t in
glob
al s
ympt
oms
83 (N
ot
repo
rted)
D
oxep
in 5
0 m
g o.
d.
8 W
eeks
M
etho
d of
rand
omiz
atio
n an
d co
ncea
lmen
t of a
l-lo
catio
n no
t sta
ted.
Dou
ble-
blin
d. U
ncle
ar if
oth
er
IBS
med
icat
ions
allo
wed
Ber
gman
n ( 2
4 )
Ger
man
y Se
cond
ary
care
Cl
inic
al
diag
nosi
s an
d in
vest
igat
ions
Patie
nt-r
epor
ted
impr
ove-
men
t in
glob
al s
ympt
oms
35 (8
7)
Trim
ipra
min
e 50
mg
o.d.
3
Mon
ths
Met
hod
of ra
ndom
izat
ion
and
conc
ealm
ent o
f al-
loca
tion
not s
tate
d. B
lindi
ng n
ot s
tate
d. N
o ot
her
IBS
med
icat
ions
allo
wed
Vij (
35 )
Indi
a Se
cond
ary
care
Cl
inic
al
diag
nosi
s an
d in
vest
igat
ions
Patie
nt-r
epor
ted
impr
ove-
men
t in
glob
al s
ympt
oms
50 (N
ot
repo
rted)
D
oxep
in 7
5 m
g o.
d.
6 W
eeks
M
etho
d of
rand
omiz
atio
n st
ated
. Met
hod
of c
on-
ceal
men
t of a
lloca
tion
not s
tate
d. D
oubl
e-bl
ind.
U
ncle
ar if
oth
er IB
S m
edic
atio
ns a
llow
ed
Dro
ssm
an ( 3
6 )
USA
and
Ca
nada
Te
rtiar
y ca
re
Rom
e I
≥ Sco
re o
f 28
on tr
eatm
ent
satis
fact
ion
ques
tionn
aire
17
2 (1
00)
Des
ipra
min
e 50
mg
o.d.
for 1
wee
k, th
en
100
mg
o.d.
for 1
w
eek,
then
150
mg
o.d.
ther
eafte
r
12 W
eeks
M
etho
d of
rand
omiz
atio
n an
d co
ncea
lmen
t of
allo
catio
n st
ated
. Dou
ble-
blin
d. U
ncle
ar if
oth
er
IBS
med
icat
ions
allo
wed
Kui
ken
( 27 )
H
olla
nd
Terti
ary
care
R
ome
I and
in
vest
igat
ions
Pa
tient
-rep
orte
d im
prov
e-m
ent i
n gl
obal
sym
ptom
s 40
(55)
Fl
uoxe
tine
20 m
g o.
d.
6 W
eeks
M
etho
d of
rand
omiz
atio
n an
d co
ncea
lmen
t of
allo
catio
n st
ated
. Dou
ble-
blin
d. U
ncle
ar if
oth
er
IBS
med
icat
ions
allo
wed
Taba
s ( 3
0 )
USA
Te
rtiar
y ca
re
Rom
e I
Patie
nt-r
epor
ted
impr
ove-
men
t in
wel
l-bei
ng
90 (7
4)
Paro
xetin
e 10
mg,
in
crea
sing
to 2
0 m
g th
en 4
0 m
g if
no
impr
ovem
ent
12 W
eeks
M
etho
d of
rand
omiz
atio
n an
d co
ncea
lmen
t of
allo
catio
n st
ated
Dou
ble-
blin
d. H
igh
fi ber
die
t. U
ncle
ar if
oth
er IB
S m
edic
atio
ns a
llow
ed
Vahe
di ( 3
3 )
Iran
Seco
ndar
y ca
re
Rom
e II
and
inve
stig
atio
ns
Patie
nt-r
epor
ted
impr
ove-
men
t in
abdo
min
al p
ain
44 (6
1)
Fluo
xetin
e 20
mg
o.d.
12
Wee
ks
Met
hod
of ra
ndom
izat
ion
stat
ed. M
etho
d of
con
-ce
alm
ent o
f allo
catio
n no
t sta
ted.
Dou
ble-
blin
d.
Unc
lear
if o
ther
IBS
med
icat
ions
allo
wed
Tack
( 31 )
B
elgi
um
Terti
ary
care
R
ome
II an
d in
vest
igat
ions
Pa
tient
-rep
orte
d 50
%
decr
ease
in d
ays
with
sy
mpt
oms
23 (7
8)
Cita
lopr
am 2
0 m
g o.
d. fo
r 3 w
eeks
in
crea
sing
to 4
0 m
g o.
d. fo
r nex
t 3 w
eeks
6 W
eeks
M
etho
d of
rand
omiz
atio
n an
d co
ncea
lmen
t of
allo
catio
n st
ated
. Dou
ble-
blin
d. N
o ot
her I
BS
med
icat
ions
allo
wed
Talle
y ( 3
2 )
Aust
ralia
Te
rtiar
y ca
re
Rom
e II
and
inve
stig
atio
ns
Patie
nt-r
epor
ted
adeq
uate
re
lief o
f sym
ptom
s 51
(61)
Im
ipra
min
e 50
mg
o.d.
or c
italo
pram
40
mg
o.d.
12 W
eeks
M
etho
d of
rand
omiz
atio
n an
d co
ncea
lmen
t of
allo
catio
n st
ated
. Dou
ble-
blin
d. N
o ot
her I
BS
med
icat
ions
allo
wed
Tabl
e 1
cont
inue
d on
follo
win
g pa
ge

© 2014 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY
1355
REV
IEW
Antidepressants and Psychological Therapies in IBS
common in patients randomized to TCAs than those receiving placebo.
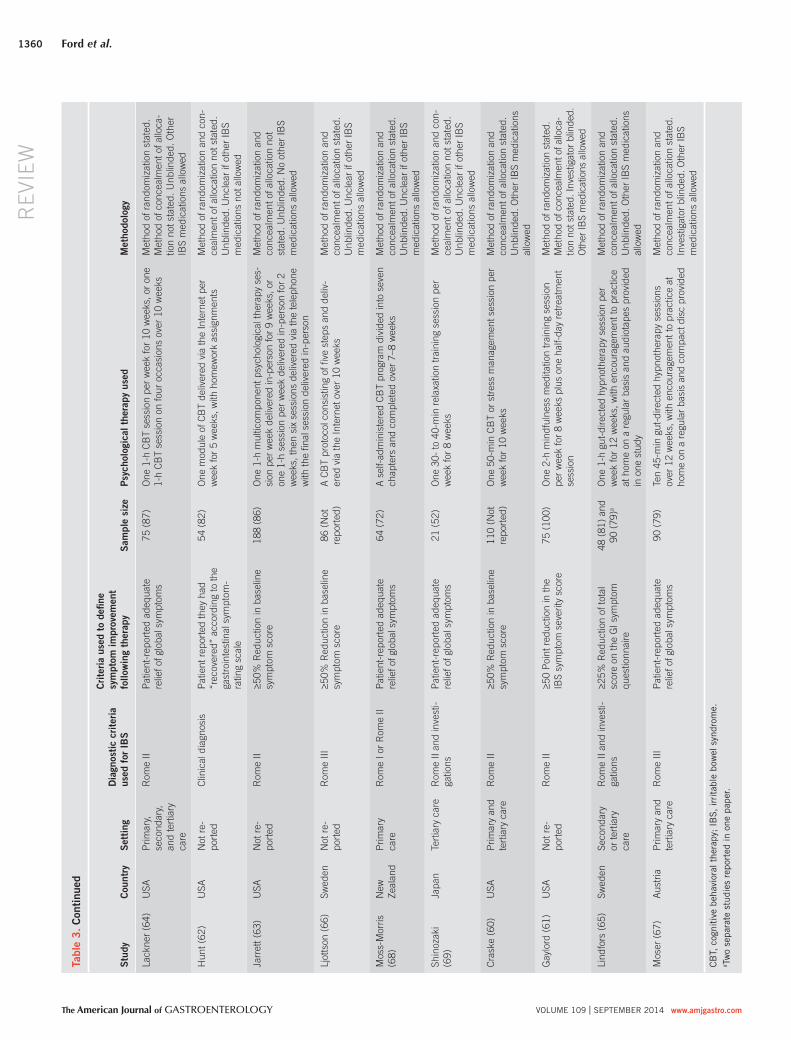
Effi cacy of psychological therapies in the treatment of IBS Th ere were a total of 30 articles, reporting on 32 separate RCTs, comparing various psychological therapies with control therapy in the form of symptom monitoring, physician ’ s “ usual manage-ment, ” supportive therapy, or placebo for the treatment of IBS in a total of 2,189 patients ( 36,41 – 69 ). Six RCTs used cognitive behav-ioral therapy (CBT) ( 36,46,50,53,57,59 ); fi ve trials used relaxation training or therapy ( 42,49,51,58,69 ); fi ve RCTs, reported in four separate articles, used hypnotherapy ( 45,56,65,67 ); four trials, reported in three separate articles, used multicomponent psycho-logical therapy ( 41,48,52 ); two RCTs used self-administered or minimal-contact CBT ( 54,68 ); two trials used Internet-delivered CBT ( 62,66 ); two RCTs used dynamic psychotherapy ( 44,47 ); one trial used mindfulness meditation training ( 61 ); one RCT used stress management ( 55 ); one trial used stress management or CBT ( 60 ); one RCT used CBT or self-administered CBT ( 64 ); one trial used multicomponent psychological therapy delivered in-person or mainly via the telephone ( 63 ); and one RCT used CBT or relax-ation therapy ( 43 ).
Th e control arm received symptom monitoring in 16 RCTs, reported in 15 articles ( 41,42,45,46,49,51 – 54,57,59,60,62,64,66 ); usual care in 13 trials, reported in 12 articles ( 43,44,47,48,50,55,58,63,65,67 – 69 ); supportive therapy in 2 RCTs ( 56,61 ); and placebo in 1 trial ( 36 ). None of the trials were at a low risk of bias, owing to the inability to blind participants to the nature of the intervention received. Th e proportion of female patients recruited by trials ranged from 52 to 100 % . Detailed character-istics of individual trials are provided in Table 3 . Adverse events data were poorly reported by included RCTs, precluding any meaningful analysis.
Overall, IBS symptoms did not improve in 639 (51.9 % ) of 1,232 patients receiving psychological therapies, compared with 839 (76.1 % ) of 1,102 receiving control in the form of symptom moni-toring, physician ’ s “ usual management, ” supportive therapy, or pla-cebo. Th e RR of IBS symptoms not improving with psychological therapies was 0.68 (95 % CI = 0.61 – 0.76; Figure 3 ), with consider-able heterogeneity detected between studies ( I 2 = 71 % , P < 0.001), and evidence of funnel plot asymmetry, or other small study eff ects (Egger test, P < 0.001), with a lack of small studies showing no eff ect of psychological therapies on the symptoms of IBS ( Figure 4 ). Th e NNT with psychological therapies was 4 (95 % CI = 3 – 5).
Subgroup analyses were conducted ( Table 4 ). Treatment eff ect appeared to be increased in tertiary care-based studies, RCTs that used clinical criteria to defi ne IBS, studies that did not state the method of generation of the randomization schedule or method of concealment of allocation, unblinded studies, and studies that used waiting list control as the comparison. A statistically signifi -cant diff erence in treatment eff ect was detected for concealment of allocation and level of blinding only.
Effi cacy of CBT in IBS . Nine trials compared CBT with control therapy in 610 patients ( 36,43,46,50,53,57,59,60,64 ). Symptoms Ta
ble
1 . C
ontin
ued
Stud
y Co
untr
y Se
ttin
g
Dia
gnos
tic
crite
ria u
sed
for
IBS
Crite
ria u
sed
to d
efi n
e sy
mpt
om im
prov
emen
t fo
llow
ing
ther
apy
Sam
ple
size
( %
fem
ale)
An
tidep
ress
ant
used
D
urat
ion
of
ther
apy
Met
hodo
logy
Vahe
di ( 3
4 )
Iran
Seco
ndar
y ca
re
Rom
e II
and
inve
stig
atio
ns
Patie
nt-r
epor
ted
impr
ove-
men
t in
glob
al s
ympt
oms
54 (4
4)
Amitr
ipty
line
10 m
g o.
d.
2 M
onth
s M
etho
d of
rand
omiz
atio
n st
ated
. Met
hod
of c
on-
ceal
men
t of a
lloca
tion
not s
tate
d. D
oubl
e-bl
ind.
U
ncle
ar if
oth
er IB
S m
edic
atio
ns a
llow
ed
Abdu
l-Bak
i ( 3
7 )
Leba
non
Prim
ary,
se
cond
ary,
and
te
rtiar
y ca
re
Rom
e II
Patie
nt-r
epor
ted
relie
f of
glob
al s
ympt
oms
107
(42)
Im
pira
min
e 25
mg
o.d.
titra
ted
up to
b.
i.d.
12 W
eeks
M
etho
d of
rand
omiz
atio
n an
d co
ncea
lmen
t of
allo
catio
n st
ated
. Dou
ble-
blin
d. N
o ot
her I
BS
med
icat
ions
allo
wed
Mas
and
( 40 )
U
SA
Terti
ary
care
R
ome
II an
d in
vest
igat
ions
Pa
tient
-rep
orte
d im
prov
e-m
ent i
n gl
obal
sym
ptom
s 72
(88)
Pa
roxe
tine
12.5
mg
o.d.
incr
ease
d to
50
mg
o.d.
12 W
eeks
M
etho
d of
rand
omiz
atio
n an
d co
ncea
lmen
t of
allo
catio
n no
t sta
ted.
Dou
ble-
blin
d. N
o ot
her I
BS
med
icat
ions
allo
wed
Lada
baum
( 3
9 )
USA
Pr
imar
y,
seco
ndar
y, a
nd
terti
ary
care
Rom
e II
and
inve
stig
atio
ns
Patie
nt-r
epor
ted
adeq
uate
re
lief o
f glo
bal s
ympt
oms
54 (8
2)
Cita
lopr
am 2
0 m
g o.
d. fo
r 4 w
eeks
th
en 4
0 m
g o.
d. fo
r 4
wee
ks
8 W
eeks
M
etho
d of
rand
omiz
atio
n an
d co
ncea
lmen
t of
allo
catio
n st
ated
. Dou
ble-
blin
d. F
iber
and
lope
ra-
mid
e al
low
ed
Gha
dir (
38 )
Iran
Seco
ndar
y ca
re
Rom
e III
Pa
tient
-rep
orte
d im
prov
e-m
ent i
n ab
dom
inal
pai
n 62
(Not
re
porte
d)
Dox
epin
or n
ortip
tyl-
ine
10 m
g o.
d.
2 M
onth
s M
etho
d of
rand
omiz
atio
n an
d co
ncea
lmen
t of
allo
catio
n st
ated
. Dou
ble-
blin
d. U
ncle
ar if
oth
er
IBS
med
icat
ions
allo
wed
b.i.d
., tw
ice-
daily
; o.d
., on
ce-d
aily
; IB
S, ir
ritab
le b
owel
syn
drom
e.

The American Journal of GASTROENTEROLOGY VOLUME 109 | SEPTEMBER 2014 www.amjgastro.com
1356R
EVIE
W Ford et al.
no signifi cant heterogeneity detected between studies ( I 2 = 0 % , P = 0.43). Th e NNT with hypnotherapy was 4 (95 % CI = 3 – 8).
Effi cacy of multicomponent psychological therapy in IBS . Five separate RCTs, again reported in four articles ( 41,48,52,63 ), compared multicomponent psychological therapy with control therapy in 335 patients. Symptoms of IBS were not improved in 96 (57.1 % ) of 168 patients randomized to multicomponent psy-chological therapy, compared with 135 (80.8 % ) of 167 receiving control. Th e RR of IBS symptoms not improving was 0.72 (95 % CI = 0.62 – 0.83; Figure 3 ), with no signifi cant heterogeneity de-tected between studies ( I 2 = 0 % , P = 0.64). Th e NNT with multi-component psychological therapy was 4 (95 % CI = 3 – 7).
Effi cacy of self-administered or minimal-contact CBT in IBS . Th ree trials, involving 144 patients, used self-administered or min-imal-contact CBT ( 54,64,68 ). Overall, 34 (46.6 % ) of 73 patients allocated to receive self-administered or minimal-contact CBT reported no improvement in symptoms, compared with 63 (88.7 % ) of 71 assigned to control. Th e RR of IBS symptoms not improving with self-administered or minimal-contact CBT was 0.53 (95 % CI = 0.17 – 1.66), with signifi cant heterogeneity detected between individual study results ( I 2 = 96 % , P < 0.001).
of IBS did not improve in 145 (41.5 % ) of 349 patients assigned to CBT, compared with 166 (63.6 % ) of 261 patients allocated to control, with an RR of 0.60 (95 % CI = 0.44 – 0.83; Figure 3 ), and statistically signifi cant heterogeneity between studies ( I 2 = 70 % , P < 0.001). Th e NNT with CBT was 3 (95 % CI = 2 – 6).
Effi cacy of relaxation training or therapy in IBS . Six RCTs compared relaxation training or therapy with control therapy in 255 patients ( 42,43,49,51,58,69 ). IBS symptoms did not improve in 96 (72.2 % ) of 133 patients randomized to relaxation training or therapy, compared with 107 (87.7 % ) of 122 patients receiving con-trol therapy. Overall, no benefi t of relaxation training or therapy in IBS was detected (RR of symptoms not improving = 0.77; 95 % CI = 0.57 – 1.04; Figure 3 ), and there was statistically signifi cant heterogeneity between studies ( I 2 = 71 % , P = 0.004).
Effi cacy of hypnotherapy in IBS . Five separate trials, reported in four articles ( 45,56,65,67 ), compared hypnotherapy with con-trol therapy in 278 patients. IBS symptoms did not improve in 77 (54.6 % ) of 141 patients assigned to hypnotherapy, compared with 106 (77.4 % ) of 137 allocated to control therapy. Overall, hypnotherapy was of benefi t in IBS, and the RR of symptoms not improving was 0.74 (95 % CI = 0.63 – 0.87; Figure 3 ), with
1.1.1 Tricyclic antidepressants
1.1.2 Selective serotonin re-uptake inhibitors
Heefner, 1978 105
1416
51460
80
3414
925
655
1515
80
260592
330508
19442211173627
176
21462212163627
180
12361911
52612
121
180 209
223021421925
11527185938
416 328
1210211914203616
53620
22 4.5% 19781982198419881991199120032008200820092011
0.83 (0.46, 1.51)0.52 (0.20, 1.33)0.67 (0.50, 0.92)0.82 (0.50, 1.36)0.30 (0.14, 0.65)0.70 (0.47, 1.04)0.83 (0.63, 1.08)0.50 (0.26, 0.97)0.08 (0.00, 1.36)0.77 (0.58, 1.01)0.44 (0.28, 0.70)0.66 (0.56, 0.79)
0.83 (0.45, 1.51) 2003200420052006200820092010
0.73 (0.54, 0.98)0.32 (0.16, 0.64)0.50 (0.25, 0.97)0.94 (0.33, 2.65)0.58 (0.37, 0.89)1.25 (0.73, 2.15)0.68 (0.51, 0.91)
0.67 [0.58, 0.77]
2.1%9.8%5.6%3.0%7.5%
11.0%3.8%0.3%
10.7%6.5%
4.4%10.0%
3.5%3.7%1.8%6.8%5.1%
35.3%
0.1
Favorsantidepressants
Favors placebo0.2 0.5 1 2 5 10
100.0%
64.7%
31214116255727164824
Myren, 1982Nigam, 1984Boerner, 1988Bergmann, 1991Vij, 1991Drossman, 2003Vahedi, 2008Talley, 2008Abdul-Baki, 2009Ghadir, 2011
Kuiken 2003Tabas 2004Vahedi 2005Tack 2006Talley 2008Masand 2009Ladabaum 2010
Total events
Total events
Subtotal (95% Cl)
Subtotal (95% Cl)Total eventsHeterogeneity: !2 = 0.03; "2 = 15.31, d.f. = 10 (P = 0.12); l2 = 35%Test for overall effect: Z = 4.61 (P < 0.00001)
Heterogeneity: !2 = 0.07; "2 = 11.85, d.f. = 6 (P = 0.07); l2 = 49%
Heterogeneity: !2 = 0.03; "2 = 27.09, d.f. = 17 (P = 0.06); l2 = 37%
Test for overall effect: Z = 2.57 (P = 0.01)
Test for overall effect: Z = 5.39 (P = 0.00001)Test for subgroup differences: "2 = 0.02, d.f. = 1 (P = 0.88), l2 = 0%
Total (95% Cl)
Study or subgroupAntidepressants Placebo
Events Total Events Total Weight M-H, Random, 95% Cl M-H, Random, 95% ClRisk ratio Risk ratio
Year
Figure 2 . Forest plot of randomized controlled trials of antidepressants vs. placebo in irritable bowel syndrome.

© 2014 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY
1357
REV
IEW
Antidepressants and Psychological Therapies in IBS
Effi cacy of CBT delivered via the Internet in IBS . Th ere were two trials that delivered CBT via the Internet, containing 140 patients ( 62,66 ). Among 71 patients randomized to CBT via the Internet, 51 (71.8 % ) reported no improvement in symptoms. Th is compared with 68 (98.6 % ) of 69 allocated to control therapy. Th e RR of IBS symptoms not improving with CBT via the Inter-net was 0.75 (95 % CI = 0.48 – 1.17), with signifi cant heterogeneity between the two RCTs ( I 2 = 90 % , P = 0.002).
Effi cacy of dynamic psychotherapy in IBS . Two RCTs compared dynamic psychotherapy with control therapy in 273 patients ( 44,47 ). No improvement in IBS symptoms was reported by 61 (44.2 % ) of 138 patients randomized to dynamic psycho therapy, compared with 95 (70.4 % ) of 135 patients receiving control; the RR of symptoms not improving was 0.60 (95 % CI = 0.39 – 0.93; Figure 3 ), and the NNT was 3.5 (95 % CI = 2 – 25 ). Again there was signifi cant heterogeneity between studies ( I 2 = 72 % , P = 0.06).
Effi cacy of stress management in IBS . Th ere were two trials using this therapy ( 55,60 ), involving 98 patients. Overall, 24 (40.7 % ) of 59 patients assigned to stress management reported no improvement in IBS symptoms, compared with 23 (59.0 % ) of 39 allocated to control. Th ere was no benefi cial eff ect detected for
stress management in IBS (RR = 0.63; 95 % CI = 0.19 – 2.08), and there was signifi cant heterogeneity between studies ( I 2 = 83 % , P = 0.02).
Effi cacy of multicomponent psychological therapy mainly via the telephone or mindfulness meditation training in IBS . Th ere was only one study that used each of these treatment modalities ( 61,63 ). Multicomponent psychological therapy mainly via the telephone appeared to be benefi cial in IBS (RR of symp-toms not improving = 0.78; 95 % CI = 0.64 – 0.93) ( 63 ), but there was no benefi t with mindfulness meditation training (RR = 0.57; 95 % CI = 0.32 – 1.01) ( 61 ).
DISCUSSION Th is updated systematic review and meta-analysis has demon-strated that antidepressants and psychological therapies are eff ec-tive treatments for IBS. Th e NNT for both TCA s and SSRIs was 4, although in the latter instance there was signifi cant heterogeneity between studies and widening of the 95 % CI of eff ect. Adverse events were signifi cantly higher among those taking antidepres-sants, with a number needed to harm of 9. When all psycho-logical therapies, including hypnotherapy, were considered the NNT was again 4. Cognitive behavioral therapy, hypnotherapy,
Table 2 . Subgroup analyses of randomized controlled trials of antidepressants vs. placebo in IBS
Number of
trials Number of patients
Relative risk of IBS symptoms not improving (95 % confi dence interval)
P value for the difference I 2 ( P value)
Setting
Secondary care 8 431 0.55 (0.43 – 0.70) 0.04 39 % (0.12)
Tertiary care 8 508 0.74 (0.63 – 0.86) 0 % (0.51)
Criteria used to defi ne IBS
Rome 12 785 0.66 (0.55 – 0.81) 0.92 48 % (0.03)
Clinical diagnosis 6 315 0.67 (0.54 – 0.83) 12 % (0.34)
Method of randomization
Stated 11 740 0.69 (0.57 – 0.85) 0.53 48 % (0.04)
Not stated 7 360 0.63 (0.51 – 0.77) 8 % (0.37)
Concealment of allocation
Stated 6 518 0.76 (0.61 – 0.94) 0.13 47 % (0.09)
Not stated 12 582 0.61 (0.50 – 0.73) 23 % (0.21)
Blinding
Double 17 1,065 0.69 (0.60 – 0.79) 0.04 28 % (0.38)
Not stated 1 35 0.30 (0.14 – 0.65) NA
Risk of bias
Low 3 288 0.76 (0.46 – 1.27) 0.60 78 % (0.01)
Unclear or high 15 812 0.66 (0.57 – 0.76) 18 % (0.26)
IBS, irritable bowel syndrome; NA, not applicable.

The American Journal of GASTROENTEROLOGY VOLUME 109 | SEPTEMBER 2014 www.amjgastro.com
1358R
EVIE
W Ford et al.
Tabl
e 3 .
Cha
ract
eris
tics
of r
ando
miz
ed c
ontr
olle
d tr
ials
of
psyc
holo
gica
l the
rapi
es v
s. c
ontr
ol in
IB
S
Stud
y
Coun
try
Sett
ing
Dia
gnos
tic c
riter
ia
used
for
IB
S
Crite
ria u
sed
to d
efi n
e sy
mpt
om im
prov
emen
t fo
llow
ing
ther
apy
Sam
ple
size
Ps
ycho
logi
cal t
hera
py u
sed
Met
hodo
logy
Nef
f ( 52
) U
SA
Terti
ary
care
Cl
inic
al d
iagn
osis
≥ 5
0 % R
educ
tion
in b
asel
ine
sym
ptom
sco
re
19 (7
9)
Mul
ticom
pone
nt p
sych
olog
ical
ther
apy
cons
istin
g of
two
1-h
sess
ions
per
wee
k fo
r 4 w
eeks
of a
com
-bi
natio
n of
rela
xatio
n th
erap
y, th
erm
al b
iofe
edba
ck,
educ
atio
n an
d tra
inin
g in
stre
ss c
opin
g st
rate
gies
th
en o
ne s
essi
on p
er w
eek
for a
furth
er 4
wee
ks
Met
hod
of ra
ndom
izat
ion
and
con-
ceal
men
t of a
lloca
tion
not s
tate
d.
Unb
linde
d. U
ncle
ar if
oth
er IB
S m
edic
atio
ns a
llow
ed
Lync
h ( 5
1 )
Cana
da
Terti
ary
care
Cl
inic
al d
iagn
osis
≥ 5
0 % R
educ
tion
in d
iary
ra
ting
of s
ympt
oms
21 (6
7)
One
2-h
rela
xatio
n th
erap
y se
ssio
n pe
r wee
k fo
r 8
wee
ks, w
ith a
udio
tape
s to
pra
ctic
e re
laxa
tion
tech
niqu
es tw
ice
daily
Met
hod
of ra
ndom
izat
ion
and
con-
ceal
men
t of a
lloca
tion
not s
tate
d.
Unb
linde
d. U
ncle
ar if
oth
er IB
S m
edic
atio
ns a
llow
ed
Gut
hrie
( 47 )
En
glan
d Te
rtiar
y ca
re
Clin
ical
dia
gnos
is
and
inve
stig
atio
ns
Patie
nt-r
epor
ted
impr
ove-
men
t in
glob
al s
ympt
oms
102
(75)
O
ne 2
-h d
ynam
ic p
sych
othe
rapy
ses
sion
follo
wed
by
six
furth
er s
essi
ons
over
3 m
onth
s, a
nd a
rela
xa-
tion
audi
otap
e pr
ovid
ed fo
r use
at h
ome
Met
hod
of ra
ndom
izat
ion
and
con-
ceal
men
t of a
lloca
tion
not s
tate
d.
Unb
linde
d. N
o ne
w IB
S m
edic
a-tio
ns a
llow
ed b
ut c
ould
con
tinue
on
cur
rent
ther
apy
Shaw
( 55 )
W
ales
Te
rtiar
y ca
re
Clin
ical
dia
gnos
is
and
inve
stig
atio
ns
Patie
nt-r
epor
ted
over
all
bene
fi t fr
om tr
eatm
ent
35 (5
7)
One
40-
min
stre
ss m
anag
emen
t tec
hniq
ue s
essi
on
per w
eek
for a
t lea
st 4
wee
ks (t
otal
num
ber o
f ses
-si
ons
was
fl ex
ible
)
Met
hod
of ra
ndom
izat
ion
and
con-
ceal
men
t of a
lloca
tion
not s
tate
d.
Unb
linde
d. U
ncle
ar if
oth
er IB
S m
edic
atio
ns a
llow
ed
Bla
ncha
rd
( 41 )
U
SA
Terti
ary
care
Cl
inic
al d
iagn
osis
an
d in
vest
igat
ions
≥ 5
0 % R
educ
tion
in b
asel
ine
sym
ptom
sco
re
20 (8
5) a
nd
77 (6
6) a
Mul
ticom
pone
nt p
sych
olog
ical
ther
apy
cons
istin
g of
two
1-h
sess
ions
per
wee
k fo
r 4 w
eeks
of a
com
-bi
natio
n of
rela
xatio
n th
erap
y, th
erm
al b
iofe
edba
ck,
educ
atio
n an
d tra
inin
g in
stre
ss c
opin
g st
rate
gies
th
en o
ne s
essi
on p
er w
eek
for a
furth
er 4
wee
ks
Met
hod
of ra
ndom
izat
ion
and
con-
ceal
men
t of a
lloca
tion
not s
tate
d.
Unb
linde
d. U
ncle
ar if
oth
er IB
S m
edic
atio
ns a
llow
ed
Bla
ncha
rd
( 42 )
U
SA
Terti
ary
care
Cl
inic
al d
iagn
osis
an
d in
vest
igat
ions
≥
50 %
Red
uctio
n in
bas
elin
e sy
mpt
om s
core
23
(78)
Tw
o pr
ogre
ssiv
e m
uscl
e re
laxa
tion
sess
ions
per
w
eek
for 2
wee
ks th
en o
ne s
essi
on p
er w
eek
for a
fu
rther
6 w
eeks
, with
regu
lar h
ome
prac
tice
emph
a-si
zed
(at l
east
25
min
per
day
)
Met
hod
of ra
ndom
izat
ion
and
con-
ceal
men
t of a
lloca
tion
not s
tate
d.
Unb
linde
d. O
ther
IBS
med
icat
ions
“ d
isco
urag
ed ”
Gre
ene
( 46 )
U
SA
Terti
ary
care
Cl
inic
al d
iagn
osis
an
d in
vest
igat
ions
≥ 5
0 % R
educ
tion
in b
asel
ine
sym
ptom
sco
re
20 (7
5)
Two
1-h
CBT
sess
ions
per
wee
k fo
r 2 w
eeks
then
on
e se
ssio
n pe
r wee
k fo
r a fu
rther
6 w
eeks
M
etho
d of
rand
omiz
atio
n an
d co
n-ce
alm
ent o
f allo
catio
n no
t sta
ted.
U
nblin
ded.
Unc
lear
if o
ther
IBS
med
icat
ions
allo
wed
Payn
e ( 5
3 )
USA
Te
rtiar
y ca
re
Rom
e I a
nd in
vest
i-ga
tions
≥ 5
0 % R
educ
tion
in b
asel
ine
sym
ptom
sco
re
22 (8
2)
Two
1-h
CBT
sess
ions
per
wee
k fo
r 2 w
eeks
then
on
e se
ssio
n pe
r wee
k fo
r a fu
rther
6 w
eeks
M
etho
d of
rand
omiz
atio
n an
d co
n-ce
alm
ent o
f allo
catio
n no
t sta
ted.
U
nblin
ded.
Unc
lear
if o
ther
IBS
med
icat
ions
allo
wed
Gal
ovsk
i ( 45
) U
SA
Terti
ary
care
Cl
inic
al d
iagn
osis
≥ 5
0 % R
educ
tion
in b
asel
ine
sym
ptom
sco
re
12 (8
3)
One
30-
min
to 1
-h g
ut-d
irect
ed h
ypno
ther
apy
ses-
sion
per
wee
k fo
r 6 w
eeks
M
etho
d of
rand
omiz
atio
n an
d co
n-ce
alm
ent o
f allo
catio
n no
t sta
ted.
U
nblin
ded.
Unc
lear
if o
ther
IBS
med
icat
ions
allo
wed
Vollm
er ( 5
9 )
USA
Te
rtiar
y ca
re
Rom
e I a
nd in
vest
i-ga
tions
≥ 5
0 % R
educ
tion
in b
asel
ine
sym
ptom
sco
re
34 (7
6)
One
1-h
ses
sion
of i
ndiv
idua
l CB
T pe
r wee
k fo
r 10
wee
ks, o
r one
90-
min
ses
sion
of g
roup
CB
T pe
r w
eek
for 1
0 w
eeks
Met
hod
of ra
ndom
izat
ion
and
con-
ceal
men
t of a
lloca
tion
not s
tate
d.
Unb
linde
d. U
ncle
ar if
oth
er IB
S m
edic
atio
ns a
llow
ed
Tabl
e 3
cont
inue
d on
follo
win
g pa
ge

© 2014 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY
1359
REV
IEW
Antidepressants and Psychological Therapies in IBS
Tabl
e 3
cont
inue
d on
follo
win
g pa
ge
Tabl
e 3 .
Con
tinue
d
Stud
y
Coun
try
Sett
ing
Dia
gnos
tic c
riter
ia
used
for
IB
S
Crite
ria u
sed
to d
efi n
e sy
mpt
om im
prov
emen
t fo
llow
ing
ther
apy
Sam
ple
size
Ps
ycho
logi
cal t
hera
py u
sed
Met
hodo
logy
Keef
er ( 4
9 )
USA
Te
rtiar
y ca
re
Clin
ical
dia
gnos
is
≥ 50 %
Red
uctio
n in
bas
elin
e sy
mpt
om s
core
15
(Not
re
porte
d)
One
30-
min
rela
xatio
n re
spon
se m
edita
tion
sess
ion
per w
eek
for 6
wee
ks
Met
hod
of ra
ndom
izat
ion
and
con-
ceal
men
t of a
lloca
tion
not s
tate
d.
Unb
linde
d. U
ncle
ar if
oth
er IB
S m
edic
atio
ns a
llow
ed
Boy
ce ( 4
3 )
Aust
ralia
Te
rtiar
y ca
re
Rom
e I a
nd in
vest
i-ga
tions
≥ 1
Sta
ndar
d de
viat
ion
de-
crea
se in
bas
elin
e sy
mpt
om
scor
e
105
(81)
O
ne 1
-h C
BT
sess
ion
per w
eek
for 8
wee
ks, o
r one
30
-min
rela
xatio
n th
erap
y se
ssio
n pe
r wee
k fo
r 8
wee
ks
Met
hod
of ra
ndom
izat
ion
and
conc
ealm
ent o
f allo
catio
n st
ated
. In
vest
igat
or b
linde
d. N
o ot
her I
BS
med
icat
ions
allo
wed
Cree
d ( 4
4 )
Engl
and
Terti
ary
care
R
ome
I Pa
tient
-rep
orte
d im
prov
e-m
ent i
n gl
obal
sym
ptom
s 17
1 (7
9)
One
2-h
and
sev
en 4
5-m
in p
sych
odyn
amic
inte
r-pe
rson
al th
erap
y se
ssio
ns o
ver 3
mon
ths
Met
hod
of ra
ndom
izat
ion
and
conc
ealm
ent o
f allo
catio
n st
ated
. In
vest
igat
or b
linde
d. U
ncle
ar if
ot
her I
BS
med
icat
ions
allo
wed
Dro
ssm
an
( 36 )
U
SA
and
Cana
da
Terti
ary
care
R
ome
I ≥ S
core
of 2
8 on
trea
tmen
t sa
tisfa
ctio
n qu
estio
nnai
re
169
(100
) O
ne 1
-h C
BT
sess
ion
per w
eek
for 1
2 w
eeks
M
etho
d of
rand
omiz
atio
n an
d co
ncea
lmen
t of a
lloca
tion
stat
ed.
Inve
stig
ator
blin
ded.
Unc
lear
if
othe
r IB
S m
edic
atio
ns a
llow
ed
Tkac
huk
( 57 )
Ca
nada
Te
rtiar
y ca
re
Rom
e I a
nd in
vest
i-ga
tions
Pa
tient
-rep
orte
d im
prov
e-m
ent i
n gl
obal
sym
ptom
s 28
(96)
Tw
o 90
-min
gro
up C
BT
sess
ions
per
wee
k fo
r 1
wee
k th
en o
ne s
essi
on p
er w
eek
for 8
wee
ks
Met
hod
of ra
ndom
izat
ion
and
con-
ceal
men
t of a
lloca
tion
not s
tate
d.
Unb
linde
d. U
ncle
ar if
oth
er IB
S m
edic
atio
ns a
llow
ed
Hei
tkem
per
( 48 )
U
SA
Terti
ary
care
R
ome
I ≥ 5
0 % R
educ
tion
in s
ympt
om
scor
e 95
(100
) O
ne 1
-h w
eekl
y m
ultic
ompo
nent
psy
chol
ogic
al
ther
apy
sess
ion
per w
eek
for 8
wee
ks
Met
hod
of ra
ndom
izat
ion
and
con-
ceal
men
t of a
lloca
tion
not s
tate
d.
Unb
linde
d. O
ther
IBS
med
icat
ions
al
low
ed
Sim
ren
( 56 )
Sw
eden
Te
rtiar
y ca
re
Rom
e II
and
inve
sti-
gatio
ns
Patie
nt-r
epor
ted
impr
ove-
men
t in
glob
al s
ympt
oms
28 (6
8)
One
1-h
gut
-dire
cted
hyp
noth
erap
y se
ssio
n pe
r w
eek
for 1
2 w
eeks
M
etho
d of
rand
omiz
atio
n st
ated
. M
etho
d of
con
ceal
men
t of a
lloca
-tio
n no
t sta
ted.
Unb
linde
d. N
o ot
her I
BS
med
icat
ions
allo
wed
Kenn
edy
( 50 )
En
glan
d Pr
imar
y ca
re
Clin
ical
dia
gnos
is
Impr
ovem
ent i
n sy
mpt
om
seve
rity
band
ing
by o
ne b
and
(gra
ded
seve
re to
non
e on
a
four
-poi
nt L
iker
t-sca
le)
149
(not
re
porte
d)
One
50-
min
CB
T se
ssio
n pe
r wee
k fo
r 6 w
eeks
M
etho
d of
rand
omiz
atio
n st
ated
. M
etho
d of
con
ceal
men
t of a
lloca
-tio
n no
t sta
ted.
Unb
linde
d. N
o ne
w
IBS
med
icat
ions
allo
wed
Sand
ers
( 54 )
U
SA
Terti
ary
care
R
ome
II an
d in
vest
i-ga
tions
≥ 5
0 % re
duct
ion
in b
asel
ine
sym
ptom
sco
re
28 (7
9)
Self-
adm
inis
tere
d CB
T m
aile
d as
fi ve
mod
ules
ove
r 10
wee
ks
Met
hod
of ra
ndom
izat
ion
stat
ed.
Met
hod
of c
once
alm
ent o
f al-
loca
tion
not s
tate
d. U
nblin
ded.
U
ncle
ar if
oth
er IB
S m
edic
atio
ns
allo
wed
van
der V
eek
( 58 )
H
olla
nd
Terti
ary
care
R
ome
II R
elia
ble
chan
ge in
dex
≥ 1.9
6 (p
re-th
erap
y sc
ore
min
us
post
-ther
apy
scor
e di
vide
d by
sta
ndar
d er
ror o
f the
di
ffere
nce)
105
(Not
re
porte
d)
One
90-
min
rela
xatio
n tra
inin
g se
ssio
n pe
r wee
k fo
r 4
wee
ks w
ith o
ne b
oost
er s
essi
on a
fter 3
mon
ths
Met
hod
of ra
ndom
izat
ion
not
stat
ed. M
etho
d of
con
ceal
men
t of
allo
catio
n st
ated
. Unb
linde
d. O
ther
IB
S m
edic
atio
ns a
llow
ed
The American Journal of GASTROENTEROLOGY VOLUME 109 | SEPTEMBER 2014 www.amjgastro.com
1360R
EVIE
W Ford et al.
Tabl
e 3 .
Con
tinue
d
Stud
y
Coun
try
Sett
ing
Dia
gnos
tic c
riter
ia
used
for
IB
S
Crite
ria u
sed
to d
efi n
e sy
mpt
om im
prov
emen
t fo
llow
ing
ther
apy
Sam
ple
size
Ps
ycho
logi
cal t
hera
py u
sed
Met
hodo
logy
Lack
ner (
64 )
USA
Pr
imar
y,
seco
ndar
y,
and
terti
ary
care
Rom
e II
Patie
nt-r
epor
ted
adeq
uate
re
lief o
f glo
bal s
ympt
oms
75 (8
7)
One
1-h
CB
T se
ssio
n pe
r wee
k fo
r 10
wee
ks, o
r one
1-
h CB
T se
ssio
n on
four
occ
asio
ns o
ver 1
0 w
eeks
M
etho
d of
rand
omiz
atio
n st
ated
. M
etho
d of
con
ceal
men
t of a
lloca
-tio
n no
t sta
ted.
Unb
linde
d. O
ther
IB
S m
edic
atio
ns a
llow
ed
Hun
t ( 62
) U
SA
Not
re-
porte
d Cl
inic
al d
iagn
osis
Pa
tient
repo
rted
they
had
“ r
ecov
ered
” ac
cord
ing
to th
e ga
stro
inte
stin
al s
ympt
om-
ratin
g sc
ale
54 (8
2)
One
mod
ule
of C
BT
deliv
ered
via
the
Inte
rnet
per
w
eek
for 5
wee
ks, w
ith h
omew
ork
assi
gnm
ents
M
etho
d of
rand
omiz
atio
n an
d co
n-ce
alm
ent o
f allo
catio
n no
t sta
ted.
U
nblin
ded.
Unc
lear
if o
ther
IBS
med
icat
ions
not
allo
wed
Jarr
ett (
63 )
USA
N
ot re
-po
rted
Rom
e II
≥ 50 %
Red
uctio
n in
bas
elin
e sy
mpt
om s
core
18
8 (8
6)
One
1-h
mul
ticom
pone
nt p
sych
olog
ical
ther
apy
ses-
sion
per
wee
k de
liver
ed in
-per
son
for 9
wee
ks, o
r on
e 1-
h se
ssio
n pe
r wee
k de
liver
ed in
-per
son
for 2
w
eeks
, the
n si
x se
ssio
ns d
eliv
ered
via
the
tele
phon
e w
ith th
e fi n
al s
essi
on d
eliv
ered
in-p
erso
n
Met
hod
of ra
ndom
izat
ion
and
conc
ealm
ent o
f allo
catio
n no
t st
ated
. Unb
linde
d. N
o ot
her I
BS
med
icat
ions
allo
wed
Ljot
tson
( 66 )
Sw
eden
N
ot re
-po
rted
Rom
e III
≥ 5
0 % R
educ
tion
in b
asel
ine
sym
ptom
sco
re
86 (N
ot
repo
rted)
A
CBT
prot
ocol
con
sist
ing
of fi
ve s
teps
and
del
iv-
ered
via
the
Inte
rnet
ove
r 10
wee
ks
Met
hod
of ra
ndom
izat
ion
and
conc
ealm
ent o
f allo
catio
n st
ated
. U
nblin
ded.
Unc
lear
if o
ther
IBS
med
icat
ions
allo
wed
Mos
s-M
orris
( 6
8 )
New
Ze
alan
d Pr
imar
y ca
re
Rom
e I o
r Rom
e II
Patie
nt-r
epor
ted
adeq
uate
re
lief o
f glo
bal s
ympt
oms
64 (7
2)
A se
lf-ad
min
iste
red
CBT
prog
ram
div
ided
into
sev
en
chap
ters
and
com
plet
ed o
ver 7
– 8 w
eeks
M
etho
d of
rand
omiz
atio
n an
d co
ncea
lmen
t of a
lloca
tion
stat
ed.
Unb
linde
d. U
ncle
ar if
oth
er IB
S m
edic
atio
ns a
llow
ed
Shin
ozak
i ( 6
9 )
Japa
n Te
rtiar
y ca
re
Rom
e II
and
inve
sti-
gatio
ns
Patie
nt-r
epor
ted
adeq
uate
re
lief o
f glo
bal s
ympt
oms
21 (5
2)
One
30-
to 4
0-m
in re
laxa
tion
train
ing
sess
ion
per
wee
k fo
r 8 w
eeks
M
etho
d of
rand
omiz
atio
n an
d co
n-ce
alm
ent o
f allo
catio
n no
t sta
ted.
U
nblin
ded.
Unc
lear
if o
ther
IBS
med
icat
ions
allo
wed
Cras
ke ( 6
0 )
USA
Pr
imar
y an
d te
rtiar
y ca
re
Rom
e II
≥ 50 %
Red
uctio
n in
bas
elin
e sy
mpt
om s
core
11
0 (N
ot
repo
rted)
O
ne 5
0-m
in C
BT
or s
tress
man
agem
ent s
essi
on p
er
wee
k fo
r 10
wee
ks
Met
hod
of ra
ndom
izat
ion
and
conc
ealm
ent o
f allo
catio
n st
ated
. U
nblin
ded.
Oth
er IB
S m
edic
atio
ns
allo
wed
Gay
lord
( 61 )
U
SA
Not
re-
porte
d R
ome
II ≥ 5
0 Po
int r
educ
tion
in th
e IB
S sy
mpt
om s
ever
ity s
core
75
(100
) O
ne 2
-h m
indf
ulne
ss m
edita
tion
train
ing
sess
ion
per w
eek
for 8
wee
ks p
lus
one
half-
day
retre
atm
ent
sess
ion
Met
hod
of ra
ndom
izat
ion
stat
ed.
Met
hod
of c
once
alm
ent o
f allo
ca-
tion
not s
tate
d. In
vest
igat
or b
linde
d.
Oth
er IB
S m
edic
atio
ns a
llow
ed
Lind
fors
( 65 )
Sw
eden
Se
cond
ary
or te
rtiar
y ca
re
Rom
e II
and
inve
sti-
gatio
ns
≥ 25 %
Red
uctio
n of
tota
l sc
ore
on th
e G
I sym
ptom
qu
estio
nnai
re
48 (8
1) a
nd
90 (7
9) a
One
1-h
gut
-dire
cted
hyp
noth
erap
y se
ssio
n pe
r w
eek
for 1
2 w
eeks
, with
enc
oura
gem
ent t
o pr
actic
e at
hom
e on
a re
gula
r bas
is a
nd a
udio
tape
s pr
ovid
ed
in o
ne s
tudy
Met
hod
of ra
ndom
izat
ion
and
conc
ealm
ent o
f allo
catio
n st
ated
. U
nblin
ded.
Oth
er IB
S m
edic
atio
ns
allo
wed
Mos
er ( 6
7 )
Aust
ria
Prim
ary
and
terti
ary
care
R
ome
III
Patie
nt-r
epor
ted
adeq
uate
re
lief o
f glo
bal s
ympt
oms
90 (7
9)
Ten
45-m
in g
ut-d
irect
ed h
ypno
ther
apy
sess
ions
ov
er 1
2 w
eeks
, with
enc
oura
gem
ent t
o pr
actic
e at
ho
me
on a
regu
lar b
asis
and
com
pact
dis
c pr
ovid
ed
Met
hod
of ra
ndom
izat
ion
and
conc
ealm
ent o
f allo
catio
n st
ated
. In
vest
igat
or b
linde
d. O
ther
IBS
med
icat
ions
allo
wed
CBT,
cog
nitiv
e be
havi
oral
the
rapy
; IB
S, ir
ritab
le b
owel
syn
drom
e.
a Tw
o se
para
te s
tudi
es r
epor
ted
in o
ne p
aper
.

© 2014 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY
1361
REV
IEW
Antidepressants and Psychological Therapies in IBS
Psychological therapies ControlStudy or Subgroup1.1.1 Cognitive behavioural therapy
1.1.2 Relaxation training or therapy
1.1.3 Hypnotherapy
1.1.4 Multi-component psychological therapy
1.1.5 Self-administered / minimal contact cognitive behavioural therapy
1.1.6 Cognitive behavioural therapy via internet
1.1.7 Dynamic psychotherapy
1.1.8 Stress management
1.1.9 Multi-component psychological therapy via telephone
1.1.10 Mindfulness meditation training
Greene 1994 23
110
51
4103
3146
34
281923
4224
2541
96
16108
34
2526
284371
2642
264369
6851
1725
7331
1027
63
26
11273371
1038104862
168
8 1.4% 0.45 (0.20, 0.99) 19871992199220042009
200720082010
0.78 (0.56, 1.08)0.50 (0.22, 1.14)0.70 (0.51, 0.96)0.75 (0.61, 0.91)0.72 (0.62, 0.83)
1.04 (0.83, 1.29)0.41 (0.26, 0.66)0.33 (0.18, 0.61)
0.90 (0.78, 1.04) 200920100.62 (0.48, 0.79)
0.75 (0.48, 1.17)
0.53 (0.17, 1.66)
3.6%1.4%3.7%4.5%
14.5%
4.3%2.7%2.0%9.0%
4.8%4.2%8.9%
2041
61
5385
138
3956
4986
135
95
0.47 (0.33, 0.69) 199120030.74 (0.57, 0.97)
0.60 (0.39, 0.93)
0.34 (0.16, 0.73) 19912011
2009
1.13 (0.62, 2.07)0.63 (0.19, 2.08)
0.78 (0.64, 0.93)0.78 (0.64, 0.93)
20110.57 (0.32, 1.01)0.57 (0.32, 1.01)
0.68 (0.61, 0.76)
0.1 0.2
Favors psychological Favors control
0.5 1 2 5 10
3.3%4.0%7.3%
519
24
44
44
11
639
1232
839
1102
11
3636
21
21
3939
64 55
55
626264
184159
149
172239
23
1.5%2.1%3.6%
4.5%4.5%
2.2%2.2%
100.0%
298
3555
939104762
167135
77
6 69
402031
6 1.5%1.2%4.1%4.0%3.3%
14.1%
0.54 (0.25, 1.16) 19982004201220122013
0.44 (0.18, 1.11)0.70 (0.55, 0.90)0.87 (0.67, 1.15)0.71 (0.49, 1.03)0.74 (0.63, 0.87)
14452349
137106
14452551
141
2
1114
7365411
1087
25507
10 1.6% 0.39 (0.19, 0.82) 198919932001200320072010
0.80 (0.54, 1.20)0.49 (0.20, 1.20)1.17 (0.92, 1.49)0.87 (0.77, 0.98)0.26 (0.07, 0.97)0.77 (0.57, 1.04)
3.1%1.2%4.2%4.9%0.6%
15.6%
98
345110
122107
13396
27249
18
10122414
112357223
349166145
47
9996
362536279
10 0.7% 0.22 (0.06, 0.78) 199419951998200320032003200520082011
0.28 (0.10, 0.76)0.51 (0.31, 0.82)0.08 (0.00, 1.25)0.72 (0.54, 0.96)1.05 (0.80, 1.38)0.71 (0.48, 1.07)0.40 (0.25, 0.66)0.94 (0.50, 1.74)0.60 (0.44, 0.83)
1.0%2.7%0.2%3.9%4.0%3.1%2.6%2.0%
20.1%
1010145734772722
261
Payne 1995Vollmer 1998Tkachuk 2003Drossman 2003Boyce 2003Kennedy 2005Lackner 2008Craske 2011Subtotal (95% Cl)Total events
Lynch 1989Blanchard 1993Keefer 2001Boyce 2003Van der Veek 2007Shinozaki 2010Subtotal (95% Cl)Total events
Galovski 1998Simren 2004Lindfors 2012aLindfors 2012bMoser 2013Subtotal (95% Cl)Total events
Neff 1987Blanchard 1992bBlanchard 1992aHeitkemper 2004Jarrett 2009Subtotal (95% Cl)Total events
Total events
Total events
Total events
Total events
Total events
Total events
Gaylord 2011
Total (95% Cl)
Jarrett 2009
Total events
Sanders 2007Lackner 2008
Hunt 2009
Guthrie 1991Creed 2003
Shaw 1991Craske 2011
Ljotsson 2010Subtotal (95% Cl)
Subtotal (95% Cl)
Subtotal (95% Cl)
Subtotal (95% Cl)
Subtotal (95% Cl)
Moss-Morris 2010Subtotal (95% Cl)
Heterogeneity: !2 = 0.00; "2 = 2.53, d.f. = 4 (P = 0.64); l 2 = 0%
Heterogeneity: !2 = 0.97; "2 = 44.54, d.f. = 2 (P < 0.00001); l 2 = 96%
Heterogeneity: !2 = 0.09; "2 = 9.56, d.f. = 1 (P = 0.002); l 2 = 90%
Heterogeneity: !2 = 0.07; "2 = 3.62, d.f. = 1 (P = 0.006); l 2 = 72%
Heterogeneity: !2 = 0.61; "2 = 5.87, d.f. = 1 (P = 0.02); l 2 = 83%
Heterogeneity: !2 = 0.06; "2 = 119.98, d.f. = 35 (P < 0.00001); l 2 = 71
Heterogeneity: Not applicable
Heterogeneity: Not applicable
Test for overall effect: Z = 4.43 (P < 0.00001)
Test for overall effect: Z = 1.09 (P = 0.27)
Test for overall effect: Z = 1.27 (P = 0.20)
Test for overall effect: Z = 2.26 (P = 0.02)
Test for overall effect: Z = 0.75 (P = 0.45)
Test for overall effect: Z = 6.66 (P < 0.00001)Test for subgroup differences: "2 = 3.74, d.f. = 9 (P = 0.93), l 2 = 0%
Test for overall effect: Z = 2.66 (P = 0.008)
Test for overall effect: Z = 1.94 (P = 0.05)
Heterogeneity: !2 = 0.14; "2 = 26.47, d.f. = 8 (P = 0.0009); l 2 = 70%
Heterogeneity: !2 = 0.07; "2 = 17.08, d.f. = 5 (P = 0.004); l 2 = 71%
Heterogeneity: !2 = 0.00; "2 = 3.84, d.f. = 4 (P = 0.43); l 2 = 0%Test for overall effect: Z = 3.74 (P = 0.0002)
Test for overall effect: Z = 3.12 (P = 0.002)
Test for overall effect: Z = 1.73 (P = 0.08)
Events EventsTotal WeightRisk ratio
M-H, Random, 95% ClRisk ratio
M-H, Random, 95% ClYearTotal
Figure 3 . Forest plot of randomized controlled trials of psychological therapies vs. control in irritable bowel syndrome.

The American Journal of GASTROENTEROLOGY VOLUME 109 | SEPTEMBER 2014 www.amjgastro.com
1362R
EVIE
W Ford et al.
via the Internet were of no benefi t, it should be noted that in most cases the proportions with an improvement in symptoms were higher with active therapy, and the number of included individu-als in the eligible trials was small. Adverse events data were poorly reported among trials of psychological therapies. Th e assumption that the administration of psychological therapies is without the potential for adverse events is probably unrealistic. In the future, RCTs should report these data more completely.
A strength of this systematic review and meta-analysis is our use of rigorous methodology. We reported our search strategy, which included searching the “ gray ” literature, and assessment of eligibility and data extraction was performed independently by two reviewers. We also used an intention-to-treat analysis and pooled data with a random-eff ects model to minimize the likeli-hood that treatment eff ect would be overestimated. We included non-English RCTs in the analysis, and contacted investigators of potentially eligible studies to either obtain dichotomous data or to exclude patients with other functional gastrointestinal disorders from the analysis. Th is inclusive approach has pro-vided us with access to data for > 1,000 IBS patients treated with antidepressants vs. placebo, and > 2,100 patients randomized to psychological therapies vs. control. We also performed sub-group analyses to explore the reasons for heterogeneity between studies, and to assess treatment eff ect according to individual therapy used, study setting, criteria used to defi ne IBS, and
multicomponent psychological therapy, either in person or mainly via the telephone, and dynamic psychotherapy were all more eff ective than control therapy, with NNTs of between 3 and 4, and there was a trend toward a benefi t of mindfulness medita-tion training. Although relaxation training, stress management, self-administered or minimal-contact CBT, and CBT delivered
Bias assessment plot
–4.0 –2.4 –0.8 0.8 2.4 4.0 5.61.5
1.0
0.5
0.0
Log(relative risk)
Sta
ndar
d er
ror
Figure 4 . Funnel plot of randomized controlled trials of psychological therapies vs. control in irritable bowel syndrome.
Table 4 . Subgroup analyses of randomized controlled trials of psychological therapies vs. control in IBS
Number of
trials Number of patients
Relative risk of IBS symptoms not improving (95 % confi dence interval)
P value for the difference I 2 ( P value)
Setting
Tertiary care 22 1,103 0.65 (0.55 – 0.78) 0.53 75 % ( < 0.001)
Other 14 1,231 0.70 (0.60 – 0.81) 65 % ( < 0.001)
Criteria used to defi ne IBS
Rome 24 1,787 0.72 (0.63 – 0.81) 0.16 72 % ( < 0.001)
Clinical diagnosis 12 547 0.58 (0.44 – 0.76) 73 % ( < 0.001)
Method of randomization
Stated 18 1,411 0.75 (0.65 – 0.87) 0.06 74 % ( < 0.001)
Not stated 18 923 0.60 (0.50 – 0.71) 67 % ( < 0.001)
Concealment of allocation
Stated 12 1,104 0.80 (0.70 – 0.93) 0.007 67 % ( < 0.001)
Not stated 24 1,230 0.59 (0.50 to 0.70) 73 % ( < 0.001)
Blinding
Investigator 6 654 0.83 (0.67 – 1.04) 0.05 68 % (0.008)
Unblinded 30 1,680 0.64 (0.56 – 0.73) 73 % ( < 0.001)
Handling of control arm
Waiting list control 18 693 0.61 (0.49 – 0.76) 0.17 76 % ( < 0.001)
Usual management / supportive 17 1,472 0.73 (0.63 – 0.83) 71 % ( < 0.001)
IBS, irritable bowel syndrome.

© 2014 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY
1363
REV
IEW
Antidepressants and Psychological Therapies in IBS
study methodology and design. Finally, we extracted and pooled adverse events data, where reported.
Th ere are limitations to this systematic review and meta-analy-sis, which arise from the nature of the studies available for syn-thesis. Th ere were very few trials at a low risk of bias, and there was evidence of heterogeneity between RCTs in many of our analyses, although not for TCAs, hypnotherapy, or multicompo-nent psychological therapy. In addition, the diff erence in favor of antidepressants was no longer statistically signifi cant when trials at high or unclear risk of bias were excluded from the analysis, although there were only three studies at a low risk of bias, con-taining 288 patients. Th ere was evidence of publication bias, or other small study eff ects, for both antidepressants and psycho-logical therapies. For antidepressants, this disappeared when one small outlying RCT was excluded from the analysis. Subgroup analyses demonstrated that treatment eff ect was generally lower in studies that reported the method of generation of the rand-omization schedule and concealment of allocation, which is in line with reports from the systematic review literature in gen-eral ( 70 ). Th ese issues may mean that the true treatment eff ect of both antidepressants and psychological therapies has been overestimated.
Our previous meta-analysis examining this issue demonstrated similar fi ndings, in terms of the effi cacy of both antidepressants and psychological therapies ( 18 ). Despite the addition of 4 trials of antidepressants ( 37 – 40 ), and 10 studies of psychological therapies ( 60 – 69 ), since its publication, the overall estimates of the effi cacy of these treatments remain almost identical. However, more trials of antidepressants now report adverse events than previously, and these were signifi cantly more common with active therapy than with placebo, which was not the case previously. In addition, there was a signifi cant eff ect of antidepressant therapy on abdominal pain, an outcome that was reported by more RCTs in this updated meta-analysis ( 26,27,30,33 – 35,38 ).
It remains unclear whether antidepressants or psychological therapies are eff ective for the treatment of IBS in primary care, with only two of the RCTs we identifi ed conducted entirely within this setting ( 50,68 ). Th e effi cacy of these therapies according to predominant stool pattern reported by the patient has also not been well studied. TCAs have been shown to prolong orocecal and whole gut transit times, whereas SSRIs decreases orocecal transit time ( 71 ). It would therefore seem biologically plausible that TCAs would be more eff ective in diarrhea-predominant IBS, and SSRIs of greater benefi t in constipation-predominant IBS, but this has only been assessed in two studies to date ( 33,34 ).
In addition, whether the benefi t of antidepressants arises from the treatment of coexistent depression is controversial ( 72 ). Th ree studies reported that there was no signifi cant relationship between depression scores and improvement in IBS symptoms ( 30,31,35 ), and one RCT showed that treatment eff ect with desipramine was greater in those without evidence of coexistent depression ( 36 ). Overall, in our meta-analysis, there appeared to be a benefi t of antidepressants in IBS, but there was signifi cant heterogeneity between studies of SSRIs. However, in one RCT of citalopram, the authors screened for and excluded depressed individuals from the
study, and in this trial there was no benefi t of active therapy over placebo ( 39 ), leading to the conclusion that there was only weak evidence that citalopram was superior to placebo in achieving response in nondepressed patients with IBS. For SSRIs, this theory is plausible, as the doses used in treatment trials for IBS are very similar to those used to treat depression; however, this would seem less likely for TCAs, where the doses used are considerably lower than the therapeutic range considered as eff ective for the treatment of mood disorders.
Th ere remains, therefore, a clear need for larger trials of both anti-depressants and psychological therapies, perhaps in combination, that use rigorous methodology, are conducted among IBS patients in primary care, recruit patients based on predominant stool pat-tern, either exclude depressed or anxious individuals, or stratify for co-existent depression, anxiety, and other co-morbidities, and which use outcome measures in accordance with recommendations for the design of treatment trials for the functional gastrointesti-nal disorders from the Rome committee ( 73 ), or Food and Drug Administration-approved end points. It would also be insightful to understand more about the exact mechanisms by which these therapies have their benefi cial eff ects in IBS. Functional magnetic resonance imaging studies have demonstrated that hypnotherapy appears to lead to normalization of abnormal central pain process-ing ( 74 ), and that amitriptyline reduces brain activation during painful rectal distension ( 75 ), but there are a few other studies that advance our understanding of how antidepressants and other psy-chological therapies may improve the symptoms of IBS patients.
In summary, this updated systematic review and meta-analysis has demonstrated that TCAs, SSRIs, CBT, hypnotherapy, multi-component psychological therapy, either in person or mainly via the telephone, and dynamic psychotherapy are all eff ective treat-ments for IBS. Despite the considerable number of studies pub-lished in the intervening 5 years since we last examined this issue, the overall summary estimates of treatment eff ect have remained almost identical. Th e fi nding that antidepressants, as well as many of the psychological therapies we studied, are benefi cial in IBS has implications for the management of a condition that clinicians oft en fi nd challenging, and should encourage increased use of anti-depressants by gastroenterologists and promote eff orts to improve access for both patients and physicians to psychological therapies.
ACKNOWLEDGMENTS Th is study was performed to inform the American College of Gastroenterology Monograph on irritable bowel syndrome. We are grateful to Payman Moayedi for translation of foreign language arti-cles, and Dr Maxine Lewis for assistance with interpretation of RCTs of psychological therapies in IBS.
CONFLICTS OF INTEREST Guarantor of the article: Alexander C. Ford, MBChB, MD. Specifi c author contributions: A.C.F., E.M.M.Q., B.E.L., A.J.L., Y.A.S., L.R.S., E.E.S., B.M.R.S., and P.M. conceived the study. A.C.F. and P.M. collected all data, analyzed and interpreted the data. A.C.F. draft ed the manuscript. All authors commented on draft s of the paper. All authors have approved the fi nal draft of the manuscript.

The American Journal of GASTROENTEROLOGY VOLUME 109 | SEPTEMBER 2014 www.amjgastro.com
1364R
EVIE
W Ford et al.
25 . Boerner D , Eberhardt R , Metz K et al. Wirksamkeit Und Vertraglichkeit Eines Antidepressivuns Beim Colon Irritabile . Th erapiewoche 1988 ; 38 : 201 – 8 .
26 . Heefner JD , Wilder RM , Wilson ID . Irritable colon and depression . Psycho-somatics 1978 ; 19 : 540 – 7 .
27 . Kuiken SD , Tytgat GNJ , Boeckxstaens GEE . Th e selective serotonin reuptake inhibitor fl uoxetine does not change rectal sensitivity and symptoms in patients with irritable bowel syndrome: A Double-Blind, Randomized, Placebo-Controlled Study . Clin Gastroenterol Hepatol 2003 ; 1 : 219 – 28 .
28 . Myren J , Groth H , Larssen SE et al. Th e eff ect of trimipramine in patients with the irritable bowel syndrome: a double-blind study . Scand J Gastro-enterol 1982 ; 17 : 871 – 5 .
29 . Nigam P , Kapoor KK , Rastog CK et al. Diff erent therapeutic regimens in irritable bowel syndrome . J Assoc Physicians India 1984 ; 32 : 1041 – 4 .
30 . Tabas G , Beaves M , Wang J et al. Paroxetine to treat irritable bowel syn-drome not responding to high fi ber diet: A Double-Blind Placebo-Control-led Trial . Am J Gastroenterol 2004 ; 99 : 914 – 20 .
31 . Tack J , Broekaert D , Fischler B et al. A controlled crossover study of the selective serotonin reuptake inhibitor citalopram in irritable bowel syndrome . Gut 2006 ; 55 : 1095 – 103 .
32 . Talley NJ , Kellow JE , Boyce P et al. Antidepressant Th erapy (Imipramine And Citalopram) For Irritable Bowel Syndrome: A Double-Blind, Rand-omized, Placebo-Controlled Trial . Dig Dis Sci 2008 ; 53 : 108 – 15 .
33 . Vahedi H , Merat S , Rashidioon A et al. Th e eff ect of fl uoxetine in patients with pain and constipation-predominant irritable bowel syndrome: a double-blind randomized-controlled study . Aliment Pharmacol Th er 2005 ; 22 : 381 – 5 .
34 . Vahedi H , Merat S , Momtahen S et al. Clinical trial: the eff ect of amitriptyl-ine in patients with diarrhea-predominant irritable bowel syndrome . Aliment Pharmacol Th er 2008 ; 27 : 678 – 84 .
35 . Vij JC , Jiloha RC , Kumar N et al. Eff ect of antidepressant drug (Doxepin) on irritable bowel syndrome patients . Indian J Psychiatry 1991 ; 33 : 243 – 6 .
36 . Drossman DA , Toner BB , Whitehead WE et al. Cognitive-behavioral therapy versus education and desipramine versus placebo for moderate to severe functional bowel disorders . Gastroenterology 2003 ; 125 : 19 – 31 .
37 . Abdul-Baki H , El Hajj II , Elzahabi L et al. A randomized controlled trial of imipramine in patients with irritable bowel syndrome . World J Gastro-enterol 2009 ; 15 : 3636 – 42 .
38 . Ghadir MR , Habibinejad H , Heidari A et al. Doxepin is more eff ective than nortriptyline and placebo for the treatment of diarrhea-predominant irritable bowel syndrome: a randomized triple-blind placebo-controlled trial . Tehran Univ Med J 2011 ; 69 : 352 – 8 .
39 . Ladabaum U , Sharabidze A , Levin TR et al. Citalopram is not eff ective therapy for nondepressed patients with irritable bowel syndrome . Clin Gastroenterol Hepatol 2010 ; 8 : 42 – 8 .
40 . Masand PS , Pae C - U , Krulewicz S et al. A double-blind, randomized, placebo-controlled trial of paroxetine controlled-release in irritable bowel Syndrome . Psychosomatics 2009 ; 50 : 78 – 86 .
41 . Blanchard EB , Schwarz SP , Suls JM et al. Two controlled evaluations of mul-ticomponent psychological treatment of irritable bowel syndrome . Behav Res Th er 1992 ; 30 : 175 – 89 .
42 . Blanchard EB , Greene B , Scharff L et al. Relaxation training as a treatment for irritable bowel syndrome . Biofeedback Self Regul 1993 ; 18 : 125 – 31 .
43 . Boyce PM , Talley NJ , Balaam B et al. A randomized controlled trial of cognitive behavior therapy, relaxation training, and routine clinical care for the irritable bowel syndrome . Am J Gastroenterol 2003 ; 98 : 2209 – 18 .
44 . Creed F , Fernandes L , Guthrie E et al. Th e cost-eff ectiveness of psycho-therapy and paroxetine for severe irritable bowel syndrome . Gastro-enterology 2003 ; 124 : 303 – 17 .
45 . Galovski TE , Blanchard EB . Th e treatment of irritable bowel syndrome with hypnotherapy . Appl Psychophysiol Biofeedback 1998 ; 23 : 219 – 32 .
46 . Greene B , Blanchard EB . Cognitive therapy for irritable bowel syndrome . J Consult Clin Psychol 1994 ; 62 : 576 – 82 .
47 . Guthrie E , Creed F , Dawson D et al. A controlled trial of psycho-logical treatment for the irritable bowel syndrome . Gastroenterology 1991 ; 100 : 450 – 7 .
48 . Heitkemper M , Jarrett ME , Levy RL et al. Self-management for women with irritable bowel syndrome . Clin Gastroenterol Hepatol 2004 ; 2 : 585 – 96 .
49 . Keefer L , Blanchard EB . Th e eff ects of relaxation response meditation on the symptoms of irritable bowel syndrome: results of a controlled treatment study . Behav Res Th er 2001 ; 39 : 801 – 11 .
Financial support: Th is work was supported by American College of Gastroenterology. Potential competing interests: None.
REFERENCES 1 . Lovell RM , Ford AC . Global prevalence of, and risk factors for, irritable
bowel syndrome: a meta-analysis . Clin Gastroenterol Hepatol 2012 ; 10 : 712 – 21 .
2 . Lovell RM , Ford AC . Prevalence of gastro-esophageal refl ux-type symptoms in individuals with irritable bowel syndrome in the community: a meta-analysis . Am J Gastroenterol 2012 ; 107 : 1793 – 801 .
3 . Drossman DA , Li Z , Andruzzi E et al. US householder survey of functional gastrointestinal disorders prevalence, sociodemography, and health impact . Dig Dis Sci 1993 ; 38 : 1569 – 80 .
4 . Everhart JE , Ruhl CE . Burden of digestive diseases in the united states part i: overall and upper gastrointestinal diseases . Gastroenterology 2009 ; 136 : 376 – 86 .
5 . Inadomi JM , Fennerty MB , Bjorkman D . Systematic review: the economic impact of irritable bowel syndrome . Aliment Pharmacol Th er 2003 ; 18 : 671 – 82 .
6 . Moriarty KJ , Dawson AM . Functional abdominal pain: further evidence that whole gut is aff ected . Br Med J 1982 ; 284 : 1670 – 2 .
7 . Trimble KC , Farouk R , Pryde A et al. Heightened visceral sensation in func-tional gastrointestinal disease is not site-specifi c. Evidence for a generalized disorder of gut sensitivity . Dig Dis Sci 1995 ; 40 : 1607 – 13 .
8 . Tillisch K , Mayer EA , Labus JS . Quantitative meta-analysis identifi es brain regions activated during rectal distension in irritable bowel syndrome . Gastroenterology 2011 ; 140 : 91 – 100 .
9 . Osterberg E , Blomquist L , Krakau I et al. A population study on irritable bowel syndrome and mental health . Scand J Gastroenterol 2000 ; 35 : 264 – 8 .
10 . Whitehead WE , Palsson O , Jones KR . Systematic review of the comorbidity of irritable bowel syndrome with other disorders: what are the causes and implications? Gastroenterology 2002 ; 122 : 1140 – 56 .
11 . Mcquay HJ , Tramer M , Nye BA et al. A systematic review of antidepressants in neuropathic pain . Pain 1996 ; 68 : 217 – 27 .
12 . Saarto T , Wiff en PJ . Antidepressants for neuropathic pain . Cochrane Database Syst Rev 2007 ; 17 : Cd005454 .
13 . Ladabaum U , Boyd E , Zhao WK et al. Diagnosis, comorbidities, and management of irritable bowel syndrome in patients in a large health main-tenance organization . Clin Gastroenterol Hepatol 2012 ; 10 : 37 – 45 .
14 . Ford AC , Guyatt GH , Talley NJ et al. Errors in the conduct of systematic reviews of pharmacological interventions for irritable bowel syndrome . Am J Gastroenterol 2010 ; 105 : 280 – 8 .
15 . Brandt LJ , Chey WD , Foxx-Orenstein AE et al. An evidence-based systematic review on the management of irritable bowel syndrome . Am J Gastroenterol 2009 ; 104 (Suppl I) : S8 – S35 .
16 . National Institute For Health And Clinical Excellence . Irritable bowel syn-drome in adults: diagnosis and management of irritable bowel syndrome in primary care . http://www.nice.org.uk/nicemedia/live/11927/39622/39622.pdf . 2008 .
17 . Harkness EF , Harrington V , Hinder S et al. Gp perspectives of irritable bowel syndrome--an accepted illness, but management deviates from guidelines: a qualitative study . Bmc Fam Pract 2013 ; 14 : 92 .
18 . Ford AC , Talley NJ , Schoenfeld PS et al. Effi cacy of antidepressants and psychological therapies in irritable bowel syndrome: systematic review and meta-analysis . Gut 2009 ; 58 : 367 – 78 .
19 . Higgins JPT , Green S . Cochrane handbook for systematic reviews of inter-ventions: Version 5.0.2 . http://www.cochrane-handbook.org . 2009 .
20 . Dersimonian R , Laird N . Meta-analysis in clinical trials . Control Clin Trials 1986 ; 7 : 177 – 88 .
21 . Higgins JPT , Th ompson SG , Deeks JJ et al. Measuring inconsistency in meta-analyses . Br Med J 2003 ; 327 : 557 – 60 .
22 . Egger M , Davey-Smith G , Schneider M et al. Bias in meta-analysis detected by a simple, graphical test . Br Med J 1997 ; 315 : 629 – 34 .
23 . Sterne JA , Sutton AJ , Ioannidis JP et al. Recommendations for examining and interpreting funnel plot asymmetry in meta-analyses of randomised controlled trials . Br Med J 2011 ; 343 : D4002 .
24 . Bergmann M , Heddergott A , Schlosser T . Die Th erapie Des Colon Irritabile Mit Trimipramin (Herphonal) - Eine Kontrollierte Studie . Z Klin Med 1991 ; 46 : 1621 – 8 .

© 2014 by the American College of Gastroenterology The American Journal of GASTROENTEROLOGY
1365
REV
IEW
Antidepressants and Psychological Therapies in IBS
50 . Kennedy T , Jones R , Darnley S et al. Cognitive behaviour therapy in addition to antispasmodic treatment for irritable bowel syndrome in primary care: randomised controlled trial . Br Med J 2005 ; 331 : 435 – 7 .
51 . Lynch PM , Zamble E . A controlled behavioral treatment study of irritable bowel syndrome . Behav Th er 1989 ; 20 : 509 – 23 .
52 . Neff DF , Blanchard EB . A multi-component treatment for irritable bowel syndrome . Behav Th er 1987 ; 18 : 70 – 83 .
53 . Payne A , Blanchard EB . A controlled comparison of cognitive therapy and self-help support groups in the treatment of irritable bowel syndrome . J Consult Clin Psychol 1995 ; 63 : 779 – 86 .
54 . Sanders KA , Blanchard EB , Sykes MA . Preliminary study of a self-admin-istered treatment for irritable bowel syndrome: comparison to a wait list control group . Appl Psychophysiol Biofeedback 2007 ; 32 : 111 – 9 .
55 . Shaw G , Srivastava ED , Sadlier M et al. Stress management for irritable bowel syndrome: a controlled trial . Digestion 1991 ; 50 : 36 – 42 .
56 . Simren M , Ringstrom G , Bjornsson ES et al. Treatment with hypnotherapy reduces the sensory and motor component of the gastrocolonic response in irritable bowel syndrome . Psychosom Med 2004 ; 66 : 233 – 8 .
57 . Tkachuk GA , Graff LA , Martin GL et al. Randomized controlled trial of cognitive-behavioral group therapy for irritable bowel syndrome in a medi-cal setting . J Clin Psychol Med Settings 2003 ; 10 : 57 – 69 .
58 . Van Der Veek PPJ , Van Rood YR et al. Clinical trial: short- and long-term benefi t of relaxation training for irritable bowel syndrome . Aliment Phar-macol Th er 2007 ; 26 : 943 – 52 .
59 . Vollmer A , Blanchard EB . Controlled comparison of individual ver-sus group cognitive therapy for irritable bowel syndrome . Behav Th er 1998 ; 29 : 19 – 33 .
60 . Craske MG , Wolitzky-Taylor KB , Labus J et al. A cognitive-behavioral treat-ment for irritable bowel syndrome using interoceptive exposure to visceral sensations . Behav Res Th er 2011 ; 49 : 413 – 21 .
61 . Gaylord SA , Palsson OS , Garland EL et al. Mindfulness training reduces the severity of irritable bowel syndrome in women: results of a randomized controlled trial . Am J Gastroenterol 2011 ; 106 : 1678 – 88 .
62 . Hunt MG , Moshier S , Milonova M . Brief cognitive-behavioral internet therapy for irritable bowel syndrome . Behav Res Th er 2009 ; 47 : 797 – 802 .
63 . Jarrett ME , Cain KC , Burr RL et al. Comprehensive self-management for irritable bowel syndrome: randomized trial of in-person vs. combined in-person and telephone sessions . Am J Gastroenterol 2009 ; 104 : 3004 – 14 .
64 . Lackner JM , Jaccard J , Krasner SS et al. Self-administered cognitive behavior therapy for moderate to severe irritable bowel syndrome: clinical effi cacy, tolerability, feasibility . Clin Gastroenterol Hepatol 2008 ; 6 : 899 – 906 .
65 . Lindfors P , Unge P , Arvidsson P et al. Eff ects of gut-directed hypnotherapy on ibs in diff erent clinical settings - results from two randomized, control-led trials . Am J Gastroenterol 2012 ; 107 : 276 – 85 .
66 . Ljotsson B , Falk L , Wibron Vesterlund A et al. Internet-delivered exposure and mindfulness based therapy for irritable bowel syndrome - a rand-omized controlled trial . Behav Res Th er 2010 ; 48 : 531 – 9 .
67 . Moser G , Tragner S , Elwira Gajowniczek E et al. Long-term success of gut-directed group hypnosis for patients with refractory irritable bowel syndrome: a randomized controlled trial . Am J Gastroenterol 2013 ; 108 : 602 – 9 .
68 . Moss-Morris R , Mcalpine L , Didsbury LP et al. A randomized control-led trial of a cognitive behavioural therapy-based self-management intervention for irritable bowel syndrome in primary care . Psychol Med 2010 ; 40 : 85 – 94 .
69 . Shinozaki M , Kanazawa M , Kano M et al. Eff ect of autogenic training on general improvement in patients with irritable bowel syndrome: a rand-omized controlled trial . Appl Psychophysiol Biofeedback 2010 ; 35 : 189 – 98 .
70 . Juni P , Altman DG , Egger M . Assessing the quality of controlled clinical trials . Br Med J 2001 ; 323 : 42 – 6 .
71 . Gorard DA , Libby GW , Farthing MJ . Infl uence of antidepressants on whole gut orocaecal transit times in health and irritable bowel syndrome . Aliment Pharmacol Th er 1994 ; 8 : 159 – 66 .
72 . Camilleri M , Mayer EA . Developing irritable bowel syndrome guidelines through meta-analyses: does the emperor really have new clothes? Gastro-enterology 2009 ; 137 : 766 – 9 .
73 . Design Of Treatment Trials Committee Irvine EJ ## Whitehead WE , Chey WD et al. Design of treatment trials for functional gastrointestinal disor-ders . Gastroenterology 2006 ; 130 : 1538 – 51 .
74 . Lowen MB , Mayer EA , Sjoberg M et al. Eff ect of hypnotherapy and educa-tional intervention on brain response to visceral stimulus in the irritable bowel syndrome . Aliment Pharmacol Th er 2013 ; 37 : 1184 – 97 .
75 . Morgan V , Pickens D , Gautam S et al. Amitriptyline reduces rectal pain related activation of the anterior cingulate cortex in patients with irritable bowel syndrome . Gut 2005 ; 54 : 601 – 7 .
Related Documents