EEG network connectivity changes in mild cognitive impairment — Preliminary results Brigitta Tóth a,c, ⁎, Bálint File f , Roland Boha a , Zsófia Kardos a,c , Zoltán Hidasi d , Zsófia Anna Gaál a , Éva Csibri d , Pál Salacz d , Cornelis Jan Stam b , Márk Molnár a,e a Institute of Cognitive Neuroscience and Psychology, RCNS, HAS, Hungary b Department of Clinical Neurophysiology, VU University Medical Centre, Amsterdam, Netherlands c Department of Cognitive Science, Institute of Psychology, Eötvös Loránd University, Budapest, Hungary d Department of Psychiatry and Psychotherapy, Faculty of Medicine, Semmelweis University, Budapest, Hungary e Psychophysiology Unit, Institute of Psychology, Eötvös Loránd University, Budapest, Hungary f Faculty of Information Technology, Pázmány Péter Catholic University, Budapest, Hungary abstract article info Article history: Received 6 August 2013 Received in revised form 31 January 2014 Accepted 1 February 2014 Available online 6 February 2014 Keywords: Mild cognitive impairment Functional connectivity Phase synchronization EEG Follow-up study Resting state EEGs were compared between patients with amnestic subtype of mild cognitive impairment (aMCI) and matched elderly controls at two times over a one year period. The study aimed at investigating the role of functional connectivity between and within different brain regions in relation to the progression of cognitive def- icit in MCI. The EEG was recorded in two sessions during eyes closed and eyes open resting conditions. Functional brain connectivity was investigated based on the measurement of phase synchronization in different frequency bands. Delta and theta synchronization characteristics indicated decreased level of local and large-scale connec- tivity in the patients within the frontal, between the frontal and temporal, and frontal and parietal brain areas which was more pronounced 1 year later. As a consequence of opening the eyes connectivity in the alpha1 band within the parietal lobe decreased compared to the eyes closed condition but only in the control group. The lack of alpha1 band reactivity following eye opening could reliably differentiate patients from controls. Our preliminary results support the notion that the functional disconnection between distant brain areas is a characteristic feature of MCI, and may prove to be predictive in terms of the progression of this condition. © 2014 Elsevier B.V. All rights reserved. 1. Introduction The term “mild cognitive impairment” (MCI) conventionally applies to a condition in which the decline of cognitive abilities is more appar- ent than that seen in normal aging, but it still does not satisfy the criteria of dementia. Individuals with predominating memory problems are re- ferred to as amnestic MCI (aMCI) (Petersen et al., 2001). While MCI may be regarded as a transitional state from which Alzheimer disease (AD) may develop (“MCI-converters”), this conversion does not occur in all MCI patients (“MCI-nonconverters”, or “stable MCI” patients) (Decarli, 2003). Eckerström et al. (2008) suggested that the left hippocampal vol- ume loss was predictive for the possible development of AD and non-AD dementia in individuals with MCI. The practical importance of a predic- tive biomarker by which conversion from aMCI to AD is emphasized by the fact that the rate of conversion to AD is much higher in MCI than in normal aging individuals (Petersen et al., 2001; Petersen, 2004). There- fore, the investigation of a neurophysiological marker which is sensitive to the progression of MCI or conversion into AD is of crucial importance. Despite the obvious importance of the functional disconnection of brain regions in MCI and AD, there are only few longitudinal studies in which the relationship between the progression of MCI and changes of func- tional connectivity characteristics was considered from this perspective (Giannakopoulos et al., 2009; Fernández et al., 2012). The present study aimed for the first time at investigating the role of functional connectiv- ity of brain regions in relation to the progression of cognitive deficit in MCI. Since neurodegenerative diseases such as AD or aMCI are considered to be disconnection syndromes, functional connectivity analysis would seem to be an optimal approach for the purpose of their investigation (Missonnier et al., 2007; Buscema et al., 2007). Functional connectivity is defined as the temporal interdependence of neuronal activity of ana- tomically separated brain regions (reflected by hemodynamic and/or electrophysiological responses), and its analysis enables the quantifica- tion of the interaction between and within different neural systems (Rodriguez et al., 1999). Recent findings indicate disturbed network or- ganization in aMCI and AD: reduced level of functional communication between distant brain regions and altered patterns of functional brain organization were observed, already apparent during resting state, and not just under high cognitive load (Bokde et al., 2009). Resting state (Raichle et al., 2001) denotes a state in which an individual is awake and alert, but is not actively involved in an attention demanding or goal directed task (“psychological baseline”). Neuroimaging studies International Journal of Psychophysiology 92 (2014) 1–7 ⁎ Corresponding author at: H-1117 Budapest, Magyar Tudósok körútja 2., P.O.B. 286 H- 1519, Budapest, Hungary. Tel.: +36 1 382 6812. E-mail address: [email protected] (B. Tóth). 0167-8760/$ – see front matter © 2014 Elsevier B.V. All rights reserved. http://dx.doi.org/10.1016/j.ijpsycho.2014.02.001 Contents lists available at ScienceDirect International Journal of Psychophysiology journal homepage: www.elsevier.com/locate/ijpsycho

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

International Journal of Psychophysiology 92 (2014) 1–7
Contents lists available at ScienceDirect
International Journal of Psychophysiology
j ourna l homepage: www.e lsev ie r .com/ locate / i jpsycho
EEG network connectivity changes in mild cognitive impairment —Preliminary results
Brigitta Tóth a,c,⁎, Bálint File f, Roland Boha a, Zsófia Kardos a,c, Zoltán Hidasi d, Zsófia Anna Gaál a, Éva Csibri d,Pál Salacz d, Cornelis Jan Stam b, Márk Molnár a,e
a Institute of Cognitive Neuroscience and Psychology, RCNS, HAS, Hungaryb Department of Clinical Neurophysiology, VU University Medical Centre, Amsterdam, Netherlandsc Department of Cognitive Science, Institute of Psychology, Eötvös Loránd University, Budapest, Hungaryd Department of Psychiatry and Psychotherapy, Faculty of Medicine, Semmelweis University, Budapest, Hungarye Psychophysiology Unit, Institute of Psychology, Eötvös Loránd University, Budapest, Hungaryf Faculty of Information Technology, Pázmány Péter Catholic University, Budapest, Hungary
⁎ Corresponding author at: H-1117 Budapest, Magyar T1519, Budapest, Hungary. Tel.: +36 1 382 6812.
E-mail address: [email protected] (B. Tóth).
0167-8760/$ – see front matter © 2014 Elsevier B.V. All rihttp://dx.doi.org/10.1016/j.ijpsycho.2014.02.001
a b s t r a c t
a r t i c l e i n f oArticle history:Received 6 August 2013Received in revised form 31 January 2014Accepted 1 February 2014Available online 6 February 2014
Keywords:Mild cognitive impairmentFunctional connectivityPhase synchronizationEEGFollow-up study
Resting state EEGswere comparedbetween patientswith amnestic subtype ofmild cognitive impairment (aMCI)and matched elderly controls at two times over a one year period. The study aimed at investigating the role offunctional connectivity between andwithin different brain regions in relation to the progression of cognitive def-icit inMCI. The EEGwas recorded in two sessions during eyes closed and eyes open resting conditions. Functionalbrain connectivity was investigated based on the measurement of phase synchronization in different frequencybands. Delta and theta synchronization characteristics indicated decreased level of local and large-scale connec-tivity in the patients within the frontal, between the frontal and temporal, and frontal and parietal brain areaswhich was more pronounced 1 year later. As a consequence of opening the eyes connectivity in the alpha1band within the parietal lobe decreased compared to the eyes closed condition but only in the control group.The lack of alpha1 band reactivity following eye opening could reliably differentiate patients from controls.Our preliminary results support the notion that the functional disconnection between distant brain areas is acharacteristic feature of MCI, and may prove to be predictive in terms of the progression of this condition.
© 2014 Elsevier B.V. All rights reserved.
1. Introduction
The term “mild cognitive impairment” (MCI) conventionally appliesto a condition in which the decline of cognitive abilities is more appar-ent than that seen in normal aging, but it still does not satisfy the criteriaof dementia. Individuals with predominating memory problems are re-ferred to as amnesticMCI (aMCI) (Petersen et al., 2001).WhileMCImaybe regarded as a transitional state from which Alzheimer disease (AD)may develop (“MCI-converters”), this conversion does not occur in allMCI patients (“MCI-nonconverters”, or “stable MCI” patients) (Decarli,2003). Eckerström et al. (2008) suggested that the left hippocampal vol-ume losswaspredictive for thepossible development of ADandnon-ADdementia in individuals with MCI. The practical importance of a predic-tive biomarker by which conversion from aMCI to AD is emphasized bythe fact that the rate of conversion to AD is much higher in MCI than innormal aging individuals (Petersen et al., 2001; Petersen, 2004). There-fore, the investigation of a neurophysiological marker which is sensitiveto the progression of MCI or conversion into AD is of crucial importance.Despite the obvious importance of the functional disconnection of brain
udósok körútja 2., P.O.B. 286 H-
ghts reserved.
regions in MCI and AD, there are only few longitudinal studies in whichthe relationship between the progression of MCI and changes of func-tional connectivity characteristics was considered from this perspective(Giannakopoulos et al., 2009; Fernández et al., 2012). The present studyaimed for the first time at investigating the role of functional connectiv-ity of brain regions in relation to the progression of cognitive deficit inMCI.
Since neurodegenerative diseases such as ADor aMCI are consideredto be disconnection syndromes, functional connectivity analysis wouldseem to be an optimal approach for the purpose of their investigation(Missonnier et al., 2007; Buscema et al., 2007). Functional connectivityis defined as the temporal interdependence of neuronal activity of ana-tomically separated brain regions (reflected by hemodynamic and/orelectrophysiological responses), and its analysis enables the quantifica-tion of the interaction between and within different neural systems(Rodriguez et al., 1999). Recent findings indicate disturbed network or-ganization in aMCI and AD: reduced level of functional communicationbetween distant brain regions and altered patterns of functional brainorganization were observed, already apparent during resting state,and not just under high cognitive load (Bokde et al., 2009). Restingstate (Raichle et al., 2001) denotes a state in which an individual isawake and alert, but is not actively involved in an attention demandingor goal directed task (“psychological baseline”). Neuroimaging studies

2 B. Tóth et al. / International Journal of Psychophysiology 92 (2014) 1–7
up till now described around eight networks of anatomically distinctbrain regions that show a high level of functional connectivity duringrest, including the so-called default mode network (DMN), consistingof the precuneus, the medial frontal, inferior parietal and temporalregions. The DMN is assumed to be exclusively crucial for the mainte-nance of cognitive functioning and is presumably altered in mentaldisorders (Broyd et al., 2009). In functional neuroimaging (fMRI —functional magnetic resonance imaging) studies peculiar features ofthe DMN were observed in MCI subjects distinguishing this conditionfrom healthy aging (Qi et al., 2010; Liu et al., 2012). A consistent patternof deactivation was observed in DMN during cognitive processes(Raichle et al., 2001).
Since the EEG signal represents directly the ongoing neural activityfrom which both global and local properties characterizing physiologi-cal and/or pathological function can be extracted this method is appro-priate for the investigation of resting state networks related to variousoscillatory frequency bands. EEG oscillations are generated locally in dif-ferent brain regions and mediate coordinated interactions within andbetween different neuronal systems (Rodriguez et al., 1999). Functionalconnections are reflected by the temporal correlation – synchrony –
between the oscillatory firing patterns of neuronal assemblies. Numer-ous EEG studies reported lower EEG synchrony (indicating decreasedfunctional connectivity) in MCI and AD patients in resting conditioncompared to age matched control subjects (Koenig et al., 2005; Stam,2010; Park et al., 2008). Babiloni et al. (2010) found characteristicchanges in MCI and AD patients with respect to sources of the delta,theta and alpha1 and alpha2 bands when compared to healthy elderly.Delta oscillation (related to large-scale cortical integrationwith homeo-static processes and also to attentional processes) sensitively reflectsbrain structural damage (lesions) and a wide range of neurodegenera-tive disorders (Parkinson's disease, AD, and schizophrenia depression(for review see Knyazev, 2012)). Pathological changes of theta oscilla-tion are mainly reported in association with memory deficits (impor-tant for a variety of cognitive functions such as declarative memoryand attentional control processes). Low alpha rhythm as a characteristicoscillation of resting state (the “idling rhythm”, but which may alsohave a role in inhibiting neural task irrelevant regions) is shown to beabnormal in dementia and AD and MCI (Scheeringa et al., 2012).
The observed loss of synchrony was interpreted as functional dis-connection between different cortical regions which cannot simply bedue to the loss of cortical neurons (Jeong et al., 2001; Schliebs andArendt, 2011). Interestingly, in the few studies when the EEG of MCIand AD patients was analyzed in conditions with cognitive load suchas a working memory task a frequency band dependent increase ofEEG synchrony was found in the patient groups (Jiang and Zheng,2006; Pijnenburg et al., 2004). The results obtained by the computation-al neural mass model of de Haan et al. (2012) used for the investigationof the relation between the level of neural activity and hub vulnerabilityin Alzheimer's disease supported these latter findings. The model pre-dicted a range of AD hallmarks (loss of spectral power and long-rangesynchronization, hub vulnerability, disrupted functional network topol-ogy) and reproduced the transient increase of functional connectivity inpreclinical AD patients followed by subsequent breakdownof functionalconnections in definite AD. In healthy adults, corroborating the abovementioned neuroimaging findings on DMN sensory activation, atten-tional focusing was found to be associated with decreases in alphapower in the corresponding sensory area (Niedermeyer, 1999).
In the present preliminary study functional connectivity was inves-tigated with respect to the progression of aMCI status as an attempt toidentify reliable electrophysiological markers that are able to capturethe decline of MCI patients. As a putative electrophysiological markerthe spatial distribution of EEG phase synchronization (phase lag index,a method that eliminates the distorting bias of volume conduction),(Stam et al., 2007) was analyzed to characterize the longitudinal patho-physiological changes in aMCI. EEG data of aMCI patients and agematched control subjects were recorded in two sessions (one year in
between) in eyes closed and eyes open resting conditions. First, aMCIpatients and elderly controls were compared to assess the differencesof functional connectivity between and within different brain regions.The difference of these connectivity characteristics between the two re-cording sessions was used to identify pathophysiological changes ofaMCI over time. Discrimination analysis was applied in order to deter-mine which of the electrophysiological connectivity characteristics thebest predictors of aMCI status are. Furthermore, the effect of sensorystimulation (due to opening the eyes) on resting state functional con-nectivity was investigated by the comparison of eyes closed and eyesopen resting conditions. It was hypothesized that connectivity mea-sures will be sensitive indices of 1) deterioration of connectivity and2) decline of reactivity in aMCI which, compared to healthy controls,was supposed to increase with elapsing time.
2. Methods
2.1. Participants
Elderly adults (N = 14; women 8; age: 64.8, ±2.5) and patients(N = 9;women 6; age: 67.5, ±3.2)with the diagnosis of amnestic sub-type of MCI (aMCI) took part in the study. The participants signed awritten informed consent form and received financial compensationfor taking part in the study that was approved by the relevantinstitutional ethical committee. None of the control subjects had anyneurological or mental disorders. Dementia, sedative medication andantipsychotic-based medical treatment were exclusion criteria in bothgroups. The aMCI patients were recruited from the Department ofPsychiatry and Psychotherapy in Budapest. The diagnosis of aMCI wasbased on neurological and psychiatric examination and neuroimagingscans, including subjectively reported and neuropsychologicallyassessed memory impairment (Petersen's criteria standard clinical pro-tocol, Petersen, 2004). The test results in the patients were the follow-ing: Mini Mental State Examination (MMSE) mean 1 session: 27.4;SD: ±1.8, 2. session: 26.9; SD: ±2.2; Addebrooke's Cognitive Testmean: 83.0; SD: ±8.6; Global Deterioration Scale mean: 3.0; SD: ±0.The MCI diagnosis of the patients was confirmed one year later by thesame clinical department. Follow-up electrophysiological and behavior-al data collection was performed in the patients andmatched (age, sex)elderly controls in the Institute of Cognitive Neuroscience and Psychol-ogy. Prior to the EEG recordings in all participants the IQ (WechslerAdult Intelligence Scale [WAIS]) was tested and the Mini Mental StateExamination was performed in the aMCI patients. The IQ and MMSEresults were used to assess possible cognitive decline over time in theaMCI patients by taking it two times over a one-year period.
The participants were seated in an acoustically attenuated and elec-trically shielded room. The EEG was recorded with 33 Ag/AgCl elec-trodes (positioned according to the international 10–20 system) usingNeuroscan software and amplifiers (Scan 4.3., Nuamps, bandpass: DC-70 Hz, FIR, sampling rate: 1000 Hz). Vertical and horizontal eye move-ments were recorded. The tip of the nose was used as reference andan electrode placed between Cz and Fz as ground. The EEG data of elder-ly adults and patients with aMCI were recorded two times over a one-year period. The time between the two recording sessions in the elderlygroupwas 13.2 (SD: 2.1)months, and in the case of the aMCI group 12.6(SD: 4.1) months. 4 min of spontaneous EEG was recorded both in eyesclosed (EC) and also in eyes open (EO) conditions.
2.2. Data analysis
The EEG epochs recorded at the two sessions (session 1, session 2) inEC and EO conditions were analyzed separately. A single epoch lengthwas2048data points (2048ms). The EEG epochswerefiltered in six fre-quency bands (delta: 0.5–4 Hz, theta: 4–8 Hz, alpha1: 8–10 Hz, alpha2:10–13Hz, beta: 13–30Hz, gamma: 30–45Hz). Visual screening, and ICA(using EEGLab 10.2.5.8b ADJUST plugin) were used to exclude blinks

Table 1Results of the psychological tests (Wechsler Adult Intelligence Scale [WAIS], Mini MentalState Examination, [MMSE]).
Patient Elderly
1. session 2. session 1. session 2. session
IQ 109.5 ±9.8 110.8 ±8.62 118.2 ±9.2 122.1 ±6.7Verbal IQ 110.7 ±9.1 113.5 ±8.52 115.9 ±8.6 120.25 ±9.2Performance IQ 107.1 ±12.5 108.5 ±12.57 119.9 ±9.1 121.5 ±6.1
3B. Tóth et al. / International Journal of Psychophysiology 92 (2014) 1–7
and other kind of artifacts. There was no significant difference betweenthe average numbers of epochs in the different conditions categories.The average number of EEG epochs included in the final analysis inthe aMCI group was 97.44 (SD: 29.9), and in the elderly control groupwas 89.77 (SD: 31.02).
2.3. Functional connectivity measures
Characteristics of functional brain networks were analyzed by mea-suring the phase lag index (PLI) in five frequency bands calculated in allthe EEG epochs. PLI is a measure of the asymmetry of the distribution ofinstantaneous phase differences between two signals quantifying theconsistency of phase relation of the signals (Stam et al., 2007). PLI wascalculated by using the Brainwave 0.9.58. software (http://home.kpn.nl/stam7883/brainwave.html). PLIs are expressed as values between 0(symmetric phase distribution) and 1 (distribution with constant,non-zero phase difference indicating maximum strength of functionalconnectivity). The assessment of PLI between and within brain regionsprovides information about the large-scale and local connectivitystrength. For the regional analysis of PLI the EEG channelswere groupedinto regions of interest (ROIs): frontal, temporal, parietal (right and left,respectively). The average PLIs were calculated for all channels within aregion (local connectivity) or between two regions (long distance con-nectivity: left and right fronto-temporal, left and right fronto-parietal,left and right temporo-parietal). Electrodes making up the differentROIs were the following: right frontal (FP2, F8 and F4); left frontal(FP1, F7 and F3); right temporal (T8, FT10 and TP10); left temporal(T7, FT9 and TP9); right parietal (CP2, CP6, P4 and P8); left parietal(CP1, CP5, P7 and P3). In the present study the prioritywas for the selec-tion of EEG channels into ROIs tomeasure changes of functional connec-tivity characteristics not only in each cerebral lobe (frontal, temporal,parietal, and occipital) but also to differentiate these characteristics be-tween right and left hemispheres (for example left and right frontallobes). Therefore, the EEG signals recorded by fronto-central electrodeswere excluded from further analysis.
2.4. Statistical analysis
The statistical analyses of the PLI data between 1) control and aMCI,2) EO and EC conditions and 3) first and second recording sessionswereperformed by ANOVA for repeated measures by using the Statistica 9.1software for each frequency band and ROIs separately where groupwasthe between subject factor, session and conditions were thewithin sub-ject factors. No condition (EC, EO) effects were found for the delta andtheta bands, therefore, the statistical analyses of the PLI data between1) control and aMCI, and 2) first and second recording sessions wereperformed separately for the EO and EC conditions. The Tukey's testwasused for post hoc analyses. All test variables consideredhad approx-imately normal distribution, as verified by the Kolmogorov–Smirnovtest.
Discriminant function analysis (DAwhich has the same assumptionsas linear regression analysis but is appropriate for categorical predictorvariables)was applied to determinewhether a set of functional connec-tivity parameter variables was effective in predicting categorymember-ship (aMCI and control). Discriminant function analysis (DA) was usedto determine 1) the overall predictive power of functional connectivityparameters which discriminate between the aMCI and control groupsand 2) which of these were the best predictors of aMCI status.
3. Results
3.1. Behavioral assessment
The patients showed decreased performance on the subtests ofperformance IQ such as Symbol-Coding and Picture Completion test(p = 0.044; p= 0.032 respectively) compared to controls. No significant
difference was observed regarding the level of IQ and MMSE in the aMCIgroup between the two recording sessions (Table 1).
3.2. Electrophysiological data
Results with regard to significant group differences of connectivitystrength are presented. Consistent group differences in PLI wereobserved in the delta, theta, and alpha1 bands. Significant differencesare shown in Fig. 1 (delta band), Fig. 2 (theta band) and Fig. 3 (alpha1band).
3.2.1. Delta band
3.2.1.1. Control–aMCI group differences in PLI (main effects of groups)
3.2.1.1.1. Intra-regional connectivity. A significant decrease of PLIwithin regions was present in aMCI patients. Compared to healthy con-trols, aMCI patients showed significantly lower level of local connectiv-ity within the left and right frontal regions (F1. 22 = 4.25, p = 0.052;F1. 22 = 6.97, p = 0.015, respectively) in the EO condition.
3.2.1.1.2. Inter-regional connectivity. A difference of PLI between re-gions was found between the control and aMCI group. Compared tohealthy controls, aMCI patients showed significantly lower level of con-nectivity between the left frontal and temporal areas (F1. 22 = 5.22.p = 0.033), and also between frontal and parietal areas in bothhemispheres (left F1. 22 = 8.16. p = 0.009; right F1. 22 = 7.25.p = 0.014) but only in the EO condition.
3.2.1.2. Group and recording session interaction effects
3.2.1.2.1. Intra-regional connectivity. A significant difference with re-spect to recording session was found only in aMCI. PLI was lower inthe EC condition within the left and right frontal regions in the secondsession compared to the first (left: F1. 22 = 10.94, p = 0.003, posthoc p = 0.005; right: F1. 22 = 5.66, p = 0.027, post hoc p = 0.013).
3.2.1.2.2. Inter-regional connectivity. Fronto-temporal PLI tended todecrease as a function of time only in the aMCI group. This differencewas more pronounced in the right hemisphere (left F1. 22 = 3.82,p = 0.064, post hoc p = 0.012; right F1. 22 = 5.65, p = 0.027, posthoc p = 0.046). Fronto-parietal PLI showed a similar decline as a func-tion of time in the aMCI patients in the right (F1. 22 = 4.52. p = 0.046,post hoc p = 0.017) and left (F1. 22 = 4.38. p = 0.049, post hocp = 0.039) hemisphere as well.
3.2.2. Theta band
3.2.2.1. Group and recording session interaction effects
3.2.2.1.1. Intra-regional connectivity. Interaction of recording sessionand group was found in the right parietal region (F1. 22 = 6.29,p = 0.022, post hoc p = 0.065) in the EO condition: PLI decreased asa function of time only in the aMCI group.
3.2.2.1.2. Inter-regional connectivity. Fronto-parietal PLI decreased asa function of time in the aMCI patients in the right (F1. 22 = 13.46,p = 0.002, post hoc p = 0.015) and left (F1. 22 = 14.12, p = 0.002,post hoc p b 0.001) hemispheres as well.

Fig. 1. Delta band functional network characteristics in aMCI. PLI measured within the frontal (a) and between the fronto-temporal (b) and fronto-parietal regions (c) in eyes closed(EC) and eyes open (EO) conditions (first and second recording sessions). Horizontal lines corresponding to the diagrams indicate significant differences.
4 B. Tóth et al. / International Journal of Psychophysiology 92 (2014) 1–7
3.2.3. Alpha1 band
3.2.3.1. Control–aMCI group differences in PLI (main effects of groups)
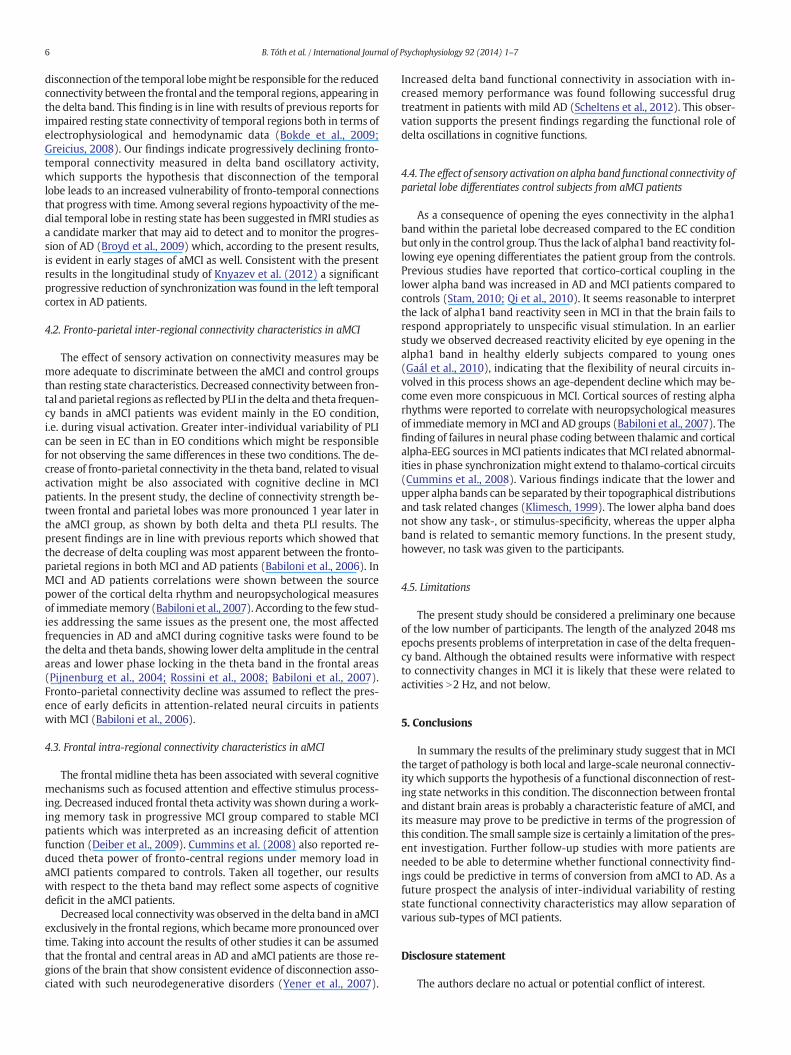
3.2.3.1.1. Intra-regional connectivity. A significant group differencewas found in the right parietal region but only in the EO condition.Higher level of connectivity was observed in the aMCI group comparedto the healthy elderly group (F1. 22 = 4.65, p = 0.042).
3.2.3.2. Difference between EC and EO conditions
3.2.3.2.1. Intra-regional connectivity. A trend of condition–group in-teraction was found in the apha1 band (F1. 22 = 3.737, p = 0.066).PLI decreased within the parietal regions in the EO condition comparedto the EC condition (p = 0.001) but only in the control group. This dif-ference was evident in both the left (p b 0.001) and the right parietalareas (p b 0.001).
3.2.4. Predictive validity of functional connectivity strengthThe variables (inter- and intra-regional connectivity strength) of
the second sessions showing significant group differences were usedas predictor variables in DA. The discriminant function revealed asignificant association between groups and all predictors (Wilks'Lambda = 0.027, p = 0.002) accounting for 97.2% of between group
variability. The structure matrix revealed that the best predictors ofaMCI status could be identified in the EO condition, namely frontal con-nectivity in thedelta band (left: 0.442, right: 0.214), fronto-parietal con-nectivity in the theta band (left: 0.276, right: 0.341) and parietalconnectivity in the alpha1 band (left: −0.372, right: −0.309). Thecross validated classification showed that in 69.7% of the overall casesthe participants were correctly identified as one that belonged to theaMCI or to the normal control group.
4. Discussion
The present longitudinal preliminary study attempted to exploreresting state EEG functional connectivity characteristics in aMCI as afunction of time. Although the results must be taken as preliminaryones, it seems likely that the analysis of connectivity strength may pro-vide new insights as to which brain regions and what EEG frequencybands are important to be considered from this perspective. The resultssuggest that cortical functional couplingmechanisms of delta, theta andalpha rhythms are impaired in aMCI patients. The observed changes inconnectivity represent evidence of altered resting state neural networkschanging as a function of time in these patients. In the aMCI patientgroup decreased level of intra and inter-regional connectivity was ob-served, as reflected by PLI changes in the delta and theta bands withinthe frontal, between the frontal and temporal, and between the frontaland parietal areas. Although the use of 2048ms epochs was not optimal
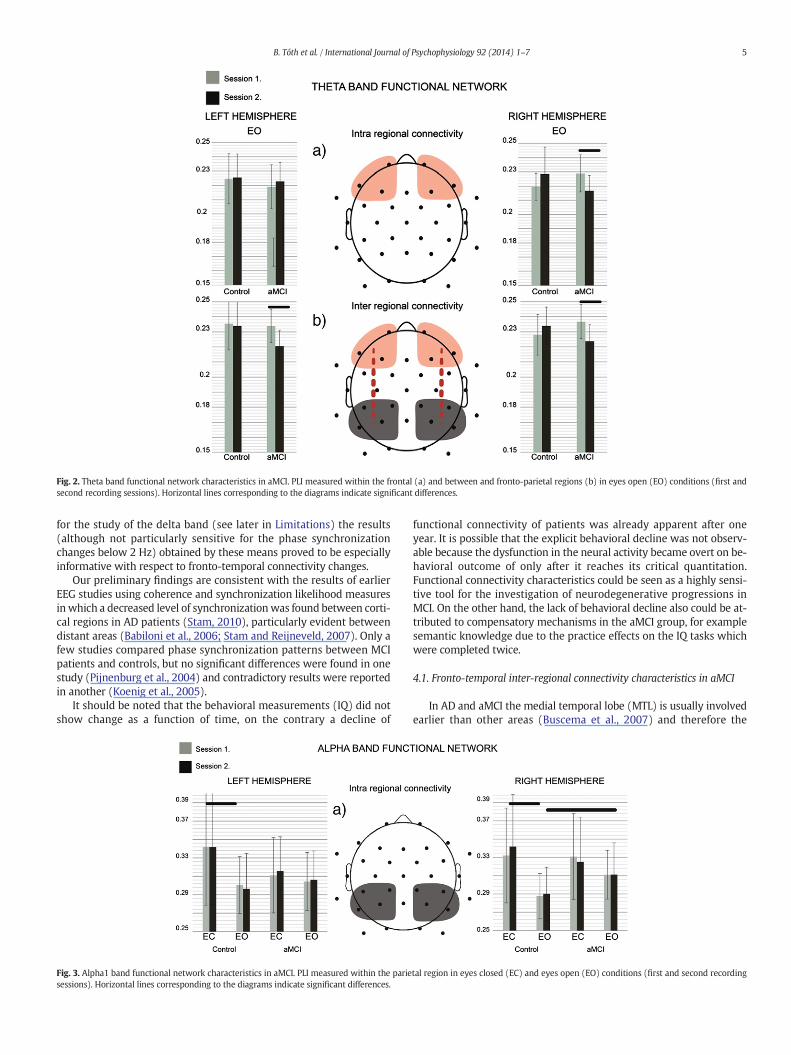
Fig. 2. Theta band functional network characteristics in aMCI. PLI measured within the frontal (a) and between and fronto-parietal regions (b) in eyes open (EO) conditions (first andsecond recording sessions). Horizontal lines corresponding to the diagrams indicate significant differences.
5B. Tóth et al. / International Journal of Psychophysiology 92 (2014) 1–7
for the study of the delta band (see later in Limitations) the results(although not particularly sensitive for the phase synchronizationchanges below 2 Hz) obtained by these means proved to be especiallyinformative with respect to fronto-temporal connectivity changes.
Our preliminary findings are consistent with the results of earlierEEG studies using coherence and synchronization likelihood measuresin which a decreased level of synchronizationwas found between corti-cal regions in AD patients (Stam, 2010), particularly evident betweendistant areas (Babiloni et al., 2006; Stam and Reijneveld, 2007). Only afew studies compared phase synchronization patterns between MCIpatients and controls, but no significant differences were found in onestudy (Pijnenburg et al., 2004) and contradictory results were reportedin another (Koenig et al., 2005).
It should be noted that the behavioral measurements (IQ) did notshow change as a function of time, on the contrary a decline of
Fig. 3. Alpha1 band functional network characteristics in aMCI. PLI measured within the pariesessions). Horizontal lines corresponding to the diagrams indicate significant differences.
functional connectivity of patients was already apparent after oneyear. It is possible that the explicit behavioral decline was not observ-able because the dysfunction in the neural activity became overt on be-havioral outcome of only after it reaches its critical quantitation.Functional connectivity characteristics could be seen as a highly sensi-tive tool for the investigation of neurodegenerative progressions inMCI. On the other hand, the lack of behavioral decline also could be at-tributed to compensatory mechanisms in the aMCI group, for examplesemantic knowledge due to the practice effects on the IQ tasks whichwere completed twice.
4.1. Fronto-temporal inter-regional connectivity characteristics in aMCI
In AD and aMCI the medial temporal lobe (MTL) is usually involvedearlier than other areas (Buscema et al., 2007) and therefore the
tal region in eyes closed (EC) and eyes open (EO) conditions (first and second recording
6 B. Tóth et al. / International Journal of Psychophysiology 92 (2014) 1–7
disconnection of the temporal lobemight be responsible for the reducedconnectivity between the frontal and the temporal regions, appearing inthe delta band. This finding is in line with results of previous reports forimpaired resting state connectivity of temporal regions both in terms ofelectrophysiological and hemodynamic data (Bokde et al., 2009;Greicius, 2008). Our findings indicate progressively declining fronto-temporal connectivity measured in delta band oscillatory activity,which supports the hypothesis that disconnection of the temporallobe leads to an increased vulnerability of fronto-temporal connectionsthat progress with time. Among several regions hypoactivity of the me-dial temporal lobe in resting state has been suggested in fMRI studies asa candidate marker that may aid to detect and to monitor the progres-sion of AD (Broyd et al., 2009) which, according to the present results,is evident in early stages of aMCI as well. Consistent with the presentresults in the longitudinal study of Knyazev et al. (2012) a significantprogressive reduction of synchronizationwas found in the left temporalcortex in AD patients.
4.2. Fronto-parietal inter-regional connectivity characteristics in aMCI
The effect of sensory activation on connectivity measures may bemore adequate to discriminate between the aMCI and control groupsthan resting state characteristics. Decreased connectivity between fron-tal and parietal regions as reflected by PLI in the delta and theta frequen-cy bands in aMCI patients was evident mainly in the EO condition,i.e. during visual activation. Greater inter-individual variability of PLIcan be seen in EC than in EO conditions which might be responsiblefor not observing the same differences in these two conditions. The de-crease of fronto-parietal connectivity in the theta band, related to visualactivation might be also associated with cognitive decline in MCIpatients. In the present study, the decline of connectivity strength be-tween frontal and parietal lobes was more pronounced 1 year later inthe aMCI group, as shown by both delta and theta PLI results. Thepresent findings are in line with previous reports which showed thatthe decrease of delta coupling was most apparent between the fronto-parietal regions in both MCI and AD patients (Babiloni et al., 2006). InMCI and AD patients correlations were shown between the sourcepower of the cortical delta rhythm and neuropsychological measuresof immediatememory (Babiloni et al., 2007). According to the few stud-ies addressing the same issues as the present one, the most affectedfrequencies in AD and aMCI during cognitive tasks were found to bethe delta and theta bands, showing lower delta amplitude in the centralareas and lower phase locking in the theta band in the frontal areas(Pijnenburg et al., 2004; Rossini et al., 2008; Babiloni et al., 2007).Fronto-parietal connectivity decline was assumed to reflect the pres-ence of early deficits in attention-related neural circuits in patientswith MCI (Babiloni et al., 2006).
4.3. Frontal intra-regional connectivity characteristics in aMCI
The frontal midline theta has been associated with several cognitivemechanisms such as focused attention and effective stimulus process-ing. Decreased induced frontal theta activity was shown during a work-ing memory task in progressive MCI group compared to stable MCIpatients which was interpreted as an increasing deficit of attentionfunction (Deiber et al., 2009). Cummins et al. (2008) also reported re-duced theta power of fronto-central regions under memory load inaMCI patients compared to controls. Taken all together, our resultswith respect to the theta band may reflect some aspects of cognitivedeficit in the aMCI patients.
Decreased local connectivity was observed in the delta band in aMCIexclusively in the frontal regions, which becamemore pronounced overtime. Taking into account the results of other studies it can be assumedthat the frontal and central areas in AD and aMCI patients are those re-gions of the brain that show consistent evidence of disconnection asso-ciated with such neurodegenerative disorders (Yener et al., 2007).
Increased delta band functional connectivity in association with in-creased memory performance was found following successful drugtreatment in patients with mild AD (Scheltens et al., 2012). This obser-vation supports the present findings regarding the functional role ofdelta oscillations in cognitive functions.
4.4. The effect of sensory activation on alpha band functional connectivity ofparietal lobe differentiates control subjects from aMCI patients
As a consequence of opening the eyes connectivity in the alpha1band within the parietal lobe decreased compared to the EC conditionbut only in the control group. Thus the lack of alpha1 band reactivity fol-lowing eye opening differentiates the patient group from the controls.Previous studies have reported that cortico-cortical coupling in thelower alpha band was increased in AD and MCI patients compared tocontrols (Stam, 2010; Qi et al., 2010). It seems reasonable to interpretthe lack of alpha1 band reactivity seen in MCI in that the brain fails torespond appropriately to unspecific visual stimulation. In an earlierstudy we observed decreased reactivity elicited by eye opening in thealpha1 band in healthy elderly subjects compared to young ones(Gaál et al., 2010), indicating that the flexibility of neural circuits in-volved in this process shows an age-dependent decline which may be-come even more conspicuous in MCI. Cortical sources of resting alpharhythms were reported to correlate with neuropsychological measuresof immediate memory inMCI and AD groups (Babiloni et al., 2007). Thefinding of failures in neural phase coding between thalamic and corticalalpha-EEG sources inMCI patients indicates that MCI related abnormal-ities in phase synchronization might extend to thalamo-cortical circuits(Cummins et al., 2008). Various findings indicate that the lower andupper alpha bands can be separated by their topographical distributionsand task related changes (Klimesch, 1999). The lower alpha band doesnot show any task-, or stimulus-specificity, whereas the upper alphaband is related to semantic memory functions. In the present study,however, no task was given to the participants.
4.5. Limitations
The present study should be considered a preliminary one becauseof the low number of participants. The length of the analyzed 2048 msepochs presents problems of interpretation in case of the delta frequen-cy band. Although the obtained results were informative with respectto connectivity changes in MCI it is likely that these were related toactivities N2 Hz, and not below.
5. Conclusions
In summary the results of the preliminary study suggest that in MCIthe target of pathology is both local and large-scale neuronal connectiv-ity which supports the hypothesis of a functional disconnection of rest-ing state networks in this condition. The disconnection between frontaland distant brain areas is probably a characteristic feature of aMCI, andits measure may prove to be predictive in terms of the progression ofthis condition. The small sample size is certainly a limitation of the pres-ent investigation. Further follow-up studies with more patients areneeded to be able to determine whether functional connectivity find-ings could be predictive in terms of conversion from aMCI to AD. As afuture prospect the analysis of inter-individual variability of restingstate functional connectivity characteristics may allow separation ofvarious sub-types of MCI patients.
Disclosure statement
The authors declare no actual or potential conflict of interest.

7B. Tóth et al. / International Journal of Psychophysiology 92 (2014) 1–7
Acknowledgments
This research was supported by the Hungarian Research Fund OTKA77750 and 104332. The authors thank E. Várkonyi for the technicalassistance.
References
Babiloni, C., Cassetta, E., Binetti, G., Tombini, M., Del Percio, C., Ferreri, F., Ferri, R., Frisoni,G., Lanuzza, B., Nobili, F., Parisi, L., Rodriguez, G., Frigerio, L., Gurzì, M., Prestia, A.,Vernieri, F., Eusebi, F., Rossini, P.M., 2007. Resting EEG sources correlate with atten-tional span in mild cognitive impairment and Alzheimer's disease. Eur. J. Neurosci.25, 3742–3757.
Babiloni, C., Ferri, R., Binetti, G., Cassarino, A., Dal Forno, G., Ercolani, M., Ferreri, F., Frisoni,G.B., Lanuzza, B., Miniussi, C., Nobili, F., Rodriguez, G., Rundo, F., Stam, C.J., Musha, T.,Vecchio, F., Rossini, P.M., 2006. Fronto-parietal coupling of brain rhythms in mildcognitive impairment: a multicentric EEG study. Brain Res. Bull. 69, 63–73.
Babiloni, C., Visser, P.J., Frisoni, G., De Deyn, P.P., Bresciani, L., Jelic, V., Nagels, G.,Rodriguez, G., Rossini, P.M., Vecchio, F., Colombo, D., Verhey, F., Wahlund, L.-O., Nobili,F., 2010. Cortical sources of resting EEG rhythms in mild cognitive impairment andsubjective memory complaint. Neurobiol. Aging 31, 1787–1798.
Bokde, A.L.W., Ewers, M., Hampel, H., 2009. Assessing neuronal networks: understandingAlzheimer's disease. Prog. Neurobiol. 89, 125–133.
Broyd, S.J., Demanuele, C., Debener, S., Helps, S.K., James, C.J., Sonuga-Barke, E.J.S., 2009.Default-mode brain dysfunction in mental disorders: a systematic review. Neurosci.Biobehav. Rev. 33, 279–296.
Buscema, M., Rossini, P., Babiloni, C., Grossi, E., 2007. The IFAST model, a novel parallel non-linear EEG analysis technique, distinguishesmild cognitive impairment and Alzheimer'sdisease patients with high degree of accuracy. Artif. Intell. Med. 40, 127–141.
Cummins, T.D.R., Broughton, M., Finnigan, S., 2008. Theta oscillations are affected byamnestic mild cognitive impairment and cognitive load. Int. J. Psychophysiol. 70, 75–81.
Decarli, C., 2003. Reviews mild cognitive impairment: prevalence, prognosis, aetiology,and treatment. Lancet Neurol. 2, 15–21.
Deiber, M.-P., Ibañez, V., Missonnier, P., Herrmann, F., Fazio-Costa, L., Gold, G.,Giannakopoulos, P., 2009. Abnormal-induced theta activity supports early directed-attention network deficits in progressive MCI. Neurobiol. Aging 30, 1444–1452.
Eckerström, C., Olsson, E., Borga, M., Ekholm, S., Ribbelin, S., Rolstad, S., Starck, G., Edman,a, Wallin, a, Malmgren, H., 2008. Small baseline volume of left hippocampus is asso-ciated with subsequent conversion of MCI into dementia: the Göteborg MCI study.J. Neurol. Sci. 272, 48–59.
Fernández, A., Gil Gregorio, P., Maestú, F., 2012. Spontaneous electroencephalographicand magneto-encephalographic activity as a marker of Alzheimer's disease andmild cognitive impairment. Rev. Esp. Geriatr. Gerontol. 47 (1), 27–32.
Niedermeyer, E., 1999. Electroencephalography: Basic Principles, Clinical Applications,and Related Fields, 4th ed. Williams & Wilkins, Baltimore, MD.
Gaál, Z.A., Boha, R., Stam, C.J., Molnár, M., 2010. Age-dependent features of EEG-reactivity—spectral, complexity, and network characteristics. Neurosci. Lett. 479, 79–84.
Giannakopoulos, P., Missonnier, P., Kövari, E., Gold, G., Michon, A., 2009. Electrophysiolog-ical markers of rapid cognitive decline in mild cognitive impairment. Front. Neurol.Neurosci. 24, 39–46.
Greicius, M., 2008. Resting-state functional connectivity in neuropsychiatric disorders.Curr. Opin. Neurol. 21, 424–430.
Jeong, J., Gore, J.C., Peterson, B.S., 2001. Mutual information analysis of the EEG in patientswith Alzheimer's disease. Clin. Neurophysiol. 112 (5), 827–835.
Jiang, Z., Zheng, L., 2006. Inter- and intra-hemispheric EEG coherence in patients withmild cognitive impairment at rest and during working memory task. J. ZhejiangUniv. Sci. B 7, 357–364.
Klimesch,W., 1999. EEG alpha and theta oscillations reflect cognitive andmemory perfor-mance: a review and analysis. Brain research. Brain research reviews 29 (2–3),169–195.
Knyazev, M.G., Carmeli, C., Khadivi, A., Ghika, J., Meuli, R., Frackowiak, R.S., 2012. Evolutionof source EEG synchronization in early Alzheimer's disease. Neurobiol. Aging 34 (3),694–705.
Knyazev, G.G., 2012. EEG delta oscillations as a correlate of basic homeostatic andmotiva-tional processes. Neurosci. Biobehav. Rev. 36 (1), 677–695.
Koenig, T., Prichep, L., Dierks, T., Hubl, D., Wahlund, L.O., John, E.R., Jelic, V., 2005.Decreased EEG synchronization in Alzheimer's disease and mild cognitive impair-ment. Neurobiol. Aging 26, 165–171.
Liu, Z., Zhang, Y., Yan, H., Bai, L., Dai, R., Wei, W., Zhong, C., Xue, T., Wang, H., Feng, Y., You,Y., Zhang, X., Tian, J., 2012. Altered topological patterns of brain networks inmild cog-nitive impairment and Alzheimer's disease: a resting-state fMRI study. PsychiatryRes. 202, 118–125.
Missonnier, P., Deiber, M.-P., Gold, G., Herrmann, F.R., Millet, P., Michon, a, Fazio-Costa, L.,Ibañez, V., Giannakopoulos, P., 2007. Working memory load-related electroencepha-lographic parameters can differentiate progressive from stable mild cognitive impair-ment. Neuroscience 150, 346–356.
Park, Y.-M., Che, H.-J., Im, C.-H., Jung, H.-T., Bae, S.-M., Lee, S.-H., 2008. Decreased EEGsynchronization and its correlation with symptom severity in Alzheimer's disease.Neurosci. Res. 62, 112–117.
Petersen, R.C., 2004. Mild cognitive impairment as a diagnostic entity. J. Intern. Med. 256,183–194.
Petersen, A., Kurz, R.C., D.R., et al., 2001. Current concepts in mild cognitive impairment.Arch. Neurol. 58, 1985–1992.
Pijnenburg, Y.A.L., vd Made, Y., van Cappellen van Walsum, A.M., Knol, D.L., Scheltens, P.,Stam, C.J., 2004. EEG synchronization likelihood in mild cognitive impairment andAlzheimer's disease during a working memory task. Clin. Neurophysiol. 115,1332–1339.
Qi, Z., Wu, X., Wang, Z., Zhang, N., Dong, H., Yao, L., Li, K., 2010. Impairment andcompensation coexist in amnestic MCI default mode network. NeuroImage 50,48–55.
Raichle, M.E., MacLeod, A.M., Snyder, A.Z., Powers, W.J., Gusnard, D.A., Shulman,G.L., 2001. A default mode of brain function. Proc. Natl. Acad. Sci. U. S. A. 98,676–682.
Rodriguez, E., George, N., Lachaux, J.P., Martinerie, J., Renault, B., Varela, F.J., 1999. Percep-tion' s shadow: long-distance synchronization of human brain activity. Nature 397(6718), 430–433 (4).
Rossini, P.M., Buscema, M., Capriotti, M., Grossi, E., Rodriguez, G., Del Percio, C., Babiloni,C., 2008. Is it possible to automatically distinguish resting EEG data of normal elderlyvs. mild cognitive impairment subjects with high degree of accuracy? Clin.Neurophysiol. 119, 1534–1545.
Scheltens, P., Twisk, J.W.R., Blesa, R., Scarpini, E., von Arnim, C.A.F., Bongers, A., Harrison, J.,Swinkels, S.H.N., Stam, C.J., de Waal, H., Wurtman, R.J., Wieggers, R.L., Vellas, B.,Kamphuis, P.J.G.H., 2012. Efficacy of Souvenaid in mild Alzheimer's disease: resultsfrom a randomized, controlled trial. J. Alzheimers Dis. 31, 225–236.
Scheeringa, R., Petersson, K.M., Kleinschmidt, A., Jensen, O., Bastiaansen, M.C.M., 2012.EEG α power modulation of fMRI resting-state connectivity. Brain Connectivity 2(5), 254-.
Schliebs, R., Arendt, T., 2011. The cholinergic system in aging and neuronal degeneration.Behav. Brain Res. 221, 555–563.
Stam, C.J., 2010. Use of magnetoencephalography (MEG) to study functional brainnetworks in neurodegenerative disorders. J. Neurol. Sci. 289, 128–134.
Stam, C.J., Nolte, G., Daffertshofer, A., 2007. Phase lag index: assessment of functional con-nectivity from multichannel EEG and MEG with diminished bias from commonsources. Hum. Brain Mapp. 28, 1178–1193.
Stam, C.J., Reijneveld, J.C., 2007. Graph theoretical analysis of complex networks in thebrain. Nonlinear Biomed. Phys. 1, 3.
Yener, G.G., Güntekin, B., Oniz, a, Başar, E., 2007. Increased frontal phase-locking of event-related theta oscillations in Alzheimer patients treated with cholinesterase inhibitors.Int. J. Psychophysiol. 64, 46–52.
de Haan, W., van der Flier, W.M., Koene, T., Smits, L.L., Scheltens, P., Stam, C.J., 2012.Disrupted modular brain dynamics reflect cognitive dysfunction in Alzheimer'sdisease. NeuroImage 59, 3085–3093.
Related Documents











