Review Educational interventions aiming at improving adherence to treatment recommendations in type 2 diabetes A sub-analysis of a systematic review of randomised controlled trials Johan Wens a, *, Etienne Vermeire a,b , Hilary Hearnshaw c , Antje Lindenmeyer c , Yves Biot a , Paul Van Royen a a Department of General Practice, Interdisciplinary Health Care and Geriatrics, University of Antwerp, Belgium b Department of Nursing and Midwifery, University of Antwerp, Belgium c Centre for Primary Health Care Studies, University of Warwick, UK diabetes research and clinical practice 79 (2008) 377–388 article info Article history: Received 13 February 2007 Accepted 16 June 2007 Published on line 23 July 2007 Keywords: Type 2 diabetes mellitus Patient education Adherence Self-management Systematic review abstract Objective: In the management of type 2 diabetes, a complex interaction takes place between medical professionals’ treatment goals and patients’ health beliefs about the disease and its treatment options. The contribution of self-management education to adherence in general or even more specifically to medicine taking is not known. We assessed educational interventions aimed at improving adherence to medical treatment recommendations, other than lifestyle advice. Study design: Systematic literature review. Setting: This paper represents an analysis of eight articles describing an educational inter- vention as a subgroup of a Cochrane Review [E. Vermeire, J. Wens, P. Van Royen, Y. Biot, H. Hearnshaw, A. Lindenmeyer, Interventions for improving adherence to treatment recom- mendations in people with type 2 diabetes mellitus, Cochrane Database of Systematic Reviews 2005, Issue 2, Art. No.: CD003638, doi:10.1002/14651858.CD003638.pub2] on inter- ventions to improve adherence to treatment recommendations in people with type 2 diabetes. Results: Four studies reported interventions using face-to-face education, two reported on the effects of group education and two on distance education by telemedicine. Due to poor quality of study designs, a variety of heterogeneous outcome measures in different time intervals, unclear definitions of adherence, and difficulties in evaluating different aspects of education performed, general conclusions could not be drawn. Conclusion: Consistent conclusions about the effectiveness of educational interventions on adherence to treatment recommendations were hard to be drawn. There is an urgent need for well-designed intervention studies on the effect of different aspects of education on adherence to treatment recommendations. # 2007 Elsevier Ireland Ltd. All rights reserved. * Corresponding author at: University of Antwerp, Faculty of Medicine, Department of General Practice, Interdisciplinary Health Care and Geriatrics, Universiteitsplein 1, 2610 Wilrijk, Antwerp, Belgium. Tel.: +32 3 820 25 29; fax: +32 3 820 25 26. E-mail address: [email protected] (J. Wens). available at www.sciencedirect.com journal homepage: www.elsevier.com/locate/diabres 0168-8227/$ – see front matter # 2007 Elsevier Ireland Ltd. All rights reserved. doi:10.1016/j.diabres.2007.06.006

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Review
Educational interventions aiming at improving adherenceto treatment recommendations in type 2 diabetesA sub-analysis of a systematic review of randomisedcontrolled trials
Johan Wens a,*, Etienne Vermeire a,b, Hilary Hearnshaw c, Antje Lindenmeyer c,Yves Biot a, Paul Van Royen a
aDepartment of General Practice, Interdisciplinary Health Care and Geriatrics, University of Antwerp, BelgiumbDepartment of Nursing and Midwifery, University of Antwerp, BelgiumcCentre for Primary Health Care Studies, University of Warwick, UK
d i a b e t e s r e s e a r c h a n d c l i n i c a l p r a c t i c e 7 9 ( 2 0 0 8 ) 3 7 7 – 3 8 8
a r t i c l e i n f o
Article history:
Received 13 February 2007
Accepted 16 June 2007
Published on line 23 July 2007
Keywords:
Type 2 diabetes mellitus
Patient education
Adherence
Self-management
Systematic review
a b s t r a c t
Objective: In the management of type 2 diabetes, a complex interaction takes place between
medical professionals’ treatment goals and patients’ health beliefs about the disease and its
treatment options.
The contribution of self-management education to adherence in general or even more
specifically to medicine taking is not known. We assessed educational interventions aimed
at improving adherence to medical treatment recommendations, other than lifestyle advice.
Study design: Systematic literature review.
Setting: This paper represents an analysis of eight articles describing an educational inter-
vention as a subgroup of a Cochrane Review [E. Vermeire, J. Wens, P. Van Royen, Y. Biot, H.
Hearnshaw, A. Lindenmeyer, Interventions for improving adherence to treatment recom-
mendations in people with type 2 diabetes mellitus, Cochrane Database of Systematic
Reviews 2005, Issue 2, Art. No.: CD003638, doi:10.1002/14651858.CD003638.pub2] on inter-
ventions to improve adherence to treatment recommendations in people with type 2
diabetes.
Results: Four studies reported interventions using face-to-face education, two reported on
the effects of group education and two on distance education by telemedicine. Due to poor
quality of study designs, a variety of heterogeneous outcome measures in different time
intervals, unclear definitions of adherence, and difficulties in evaluating different aspects of
education performed, general conclusions could not be drawn.
Conclusion: Consistent conclusions about the effectiveness of educational interventions on
adherence to treatment recommendations were hard to be drawn. There is an urgent need
for well-designed intervention studies on the effect of different aspects of education on
adherence to treatment recommendations.
avai lab le at www.sc iencedi rec t .com
journal homepage: www.e lsev ier .com/ locate /d iabres
# 2007 Elsevier Ireland Ltd. All rights reserved.
* Corresponding author at: University of Antwerp, Faculty of Medicine, Department of General Practice, Interdisciplinary Health Care andGeriatrics, Universiteitsplein 1, 2610 Wilrijk, Antwerp, Belgium. Tel.: +32 3 820 25 29; fax: +32 3 820 25 26.
E-mail address: [email protected] (J. Wens).
0168-8227/$ – see front matter # 2007 Elsevier Ireland Ltd. All rights reserved.doi:10.1016/j.diabres.2007.06.006

d i a b e t e s r e s e a r c h a n d c l i n i c a l p r a c t i c e 7 9 ( 2 0 0 8 ) 3 7 7 – 3 8 8378
Contents
1. Introduction. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 378
2. Materials and methods . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 378
2.1. Systematic literature search . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 378
2.2. Study selection . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 379
2.3. Data collection, quality assessment and analysis. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 379
3. Results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 380
3.1. Methodological quality . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 380
3.2. Kind of interventions. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 380
3.3. Quantitative synthesis. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 386
4. Discussion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 386
5. Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 387
Conflicts of interests . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 387
Acknowledgements . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 387
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 387
1. Introduction
The global burden of diabetes has been estimated at many
occasions [2,3]. WHO estimated 135 million people to be
affected in 1995, their number reaching 299 million by the year
2025 [4]. Over the last 30 years, type 2 diabetes has changed
from being considered a relatively mild ailment associated
with ageing, to one of the major contemporary causes of
premature mortality and morbidity worldwide [5]. Diabetes is
ranked among the leading causes of blindness, renal failure
and lower limb amputation [6], and is one of the major causes
of cardiovascular death.
To date there is strong evidence that the vigorous
treatment of type 2 diabetes can decrease morbidity and
mortality [7–10]. However, treatment outcomes in many
people with diabetes remain unsatisfactory. Since these
outcomes may be improved by a number of – usually complex
– interventions, full benefits of medication cannot be realized
at currently achievable levels of adherence [11]. Non-adher-
ence with therapeutic regimens therefore has been a
continuing problem for health care providers and a major
concern for public health [12,13].
Rather than the health care provider, the person living with
the disease seems to be the key to successful management
[14]. In addition, interventions focusing on modifying the
behaviour of people living with diabetes seem to have better
outcomes than those focusing on modifying clinician’s
behaviour [15].
Earlier quantitative research on the use of formal diabetes
education as a therapeutic tool, to promote self-management
in adults with type 2 diabetes, did not produce consistent
results in terms of improved metabolic control and of reduced
risks for cardiovascular disease. Positive effects on patient
knowledge, self-care behaviour, metabolic control, and psy-
chological outcomes were reported in reviews on the effec-
tiveness of education in type 2 diabetes [16–19]. However, in
these reviews, a complete and adequate description of the
interventions often is lacking. In general, comprehensive
interventions combining cognitive, behavioural, and educa-
tional components are more effective than single-focus
interventions [20]. Self-management education in patients
with type 2 diabetes mellitus, especially interventions invol-
ving active participation, may have short-term effectiveness
for improving diabetes knowledge, self-monitoring of blood
glucose levels, self-reported dietary habits, and glycemic
control [21]. However, the long-term outcomes of diabetes
education, aiming at the promotion of self-management and
adherence in adults with type 2 diabetes still have to be
established.
Diabetes self-management appears to be among the most
difficult of all chronic illnesses’ self-management regimes
[22,23]. Where quantitative studies failed to, the findings of
qualitative studies contributed to a deeper understanding of
the context in which diabetes education should be applied, in
order to be successful in promoting self-management beha-
viours in adults with type 2 diabetes [24]. By setting self-care
goals themselves, people may be more likely to adhere to
treatment plans [14,25–27]. Therapeutic patient education
may contribute to the adherence process by providing people
with the information they need for priority setting and
problem solving, assisting them in identifying realistic targets
for behavioural changes, and providing ongoing emotional
support and encouragement in their self-management plans.
We performed a systematic review of published articles to
identify the effectiveness of interventions aimed at improving
adherence to medical treatment recommendations in people
with type 2 diabetes mellitus, not lifestyle changes, diet nor
exercise [1]. This paper reports a synthesis of studies of
educational interventions that are a subgroup of studies
included in the Cochrane Review.
2. Materials and methods
2.1. Systematic literature search
A systematic literature search [28] was conducted to identify
interventions containing information on improving adher-
ence to medical treatment recommendations, not oriented to
other aspects such as exercise, attendance at clinic nor diet.
Search terms consisted of the Cochrane Metabolic and
Endocrine Disorders Group search strategy for type 2 diabetes

d i a b e t e s r e s e a r c h a n d c l i n i c a l p r a c t i c e 7 9 ( 2 0 0 8 ) 3 7 7 – 3 8 8 379
mellitus and a combination of MESH terms: patient compli-
ance, health behaviour, health education, self-care, patient
education, patient satisfaction, educational status, patient
dropouts, physician–patient relations and delivery of health
care, all with subheadings and categories included. In
addition, truncations of compliance, concordance and adher-
ence were used besides word searches on self-care or self-
management. The full search strategy is described in the
original Cochrane publication [1].
We searched electronically the Cochrane Library including
the Cochrane Controlled Trials Register (CCTR) and the
Database of reviews of effectiveness (DARE), the Metabolic
and Endocrine Disorders Group Specialized Register, MEDLINE
(1966 to November 2002), EMBASE (1980 to November 2002),
Psych Info (1987 to November 2002), CINAHL (1982 to November
2002), Dissertation Abstracts (1961 to November 2002), ERIC
(to November 2002), and furthermore Sociological Abstracts,
Digital Dissertations Proquest, the National Library of Medicine
Gateway and Current Controlled Trials. Besides these databases
Internet search engines were used exhaustively. The reference
lists of relevant articles were investigated too.
2.2. Study selection (see Plate 1)
Studies in primary care, outpatient, community settings and
hospital settings were included. Randomized and quasi-
randomized controlled trials, controlled before and after
studies, observational studies and cohort studies were
appropriate for inclusion. Two researchers (E.V. and J.W.)
independently selected articles for review based on abstracts.
Plate 1 – Progress of th
Full articles were retrieved for further assessment if the
information given suggested that the study:
1. i
e s
ncluded patients with type 2 diabetes mellitus,
2. a
ssessed adherence to medical treatment, not to exercisenor to diet,
3. m
easured an outcome of an intervention intended toenhance adherence,
4. a
imed at patients as well as health care providers,5. u
sed a design as described in the inclusion criteria for studydesign.
For the purpose of this study, adherence was defined in a
broader way than WHO that considers adherence as the extent
to which a person’s behaviour corresponds with agreed
recommendations from a health care provider [29]. Also
articles mentioning compliance, concordance or related
aspects in title or abstract were included. For the purpose of
this analysis the included papers were re-examined (Plate 1).
2.3. Data collection, quality assessment and analysis
Two teams of reviewers (E.V. and J.W., P.V.R. and Y.B.)
independently assessed all trials identified for inclusion.
Three teams of two reviewers (H.H. and A.L. in addition to
the two previous teams), assessed trial quality and extracted
the data required. Researchers were not blinded about
information on authors and journals. The quality of an
individual trial was assessed by scoring a list of nine topics:
randomisation, concealment of allocation, patient blinding,
tudy selection.

d i a b e t e s r e s e a r c h a n d c l i n i c a l p r a c t i c e 7 9 ( 2 0 0 8 ) 3 7 7 – 3 8 8380
blinding of administrator of treatment, blinding of outcome
assessment, description of losses to follow-up/withdrawals,
intention to treat analysis, similarity of groups at the start of
the study and groups equally provided of care. Quality
assessment was done individually by every individual
researcher by scoring on these questions where answers
were compared afterwards. Overall quality was graded as A
(good), B (medium) or C (poor) by mutual agreement.
Whenever reviewers disagreed, consensus was obtained
through discussion or by a referee’s decision (PVR).
The extracted data were entered in a structured Excel sheet
adapted from the Cochrane Metabolic and Endocrine Disorder
Group data extraction sheet. Studies with comparable inter-
ventions were grouped and the results were synthesised in a
narrative way. HbA1c was considered a common outcome
measure which allowed performing a meta-analysis to
calculate pooled weighted mean differences (WMD). Because
of clinical heterogeneity a random effects model was used. For
this purpose the Cochrane review manager (RevMan) software
package version 4.2 was used.
3. Results
This paper summarizes the results of eight educational
interventions aimed at improving adherence to medication.
A total of 4387 references were identified of which only 74
studies met selection criteria and were assessed in full text of
which 21 articles were include in the review. The selection
process was done by two teams or reviewers assessing
studies independently. The inter observer agreement of the
first team (P.V.R. and Y.B.) expressed as a kappa was 0.526
(S.E. 0.085), that of the second team (E.V. and J.W.) was 0.827
(S.E. 0.032).
The studies in this sub-analysis contain data of 772
patients. A summary of the study characteristics, methodo-
logical quality and outcome is shown in Table 1.
Of the included studies six were randomized controlled
trials (RCTs) (ordered alphabetically Jaber [30], Krier [31],
Mease [32], Piette [33], Rachmani [34], White [35] and two
studies were studies controlling before and after (CBAs)
(Coast-Senior [36] and Jiang [37]).
3.1. Methodological quality
The overall quality of the included studies was medium to low.
The most frequent shortcomings were found in the conceal-
ment of allocation and the blinding procedures. Randomiza-
tion was adequate in all six RCTs while concealment of
allocation and blinding procedures were estimated as ade-
quate in only one study [33]. In seven trials, groups were
similar at the start of the study, in one study [34] data were
missing. Intervention and control groups were equally
provided of care in four studies [31,32,34,35], in one study
[30] this was not the case and data were missing or unclear in
three other studies [32,36,37]. Two studies did not describe
losses to follow-up [34,37], six adequately described these
losses. Only in four studies, it was clear that the authors
performed an intention-to-treat analysis [32–35].
It is striking that not one author mentioned details about
the calculation of the statistical power of the study. Moreover,
not one of the studies included assessed any economical
aspect of the interventions.
3.2. Kind of interventions
The different educational intervention studies were grouped
by the kind of intervention: (1) face-to-face education, (2)
group education and (3) telemedicine education.
(1) Face-to-face education
Two studies [30,36] assessed the effect of pharmacist-
led interventions (pill count, Micro-Electro-Mechanical
Systems (MEMS), comprehensive care, treatment adjust-
ments or prescription refill reminders) on self-reported
adherence, medication prescription refill, and metabolic
parameters. The latter are indirect measurements of
adherence. One paper [30] studied the impact of a
pharmacist-delivered comprehensive care model on
under-served urban African–Americans. Patients in the
intervention group were offered diabetes education,
medication counselling and evaluation, plus adjustment
of their hypoglycaemic regimen. A significant improve-
ment of HbA1c levels, from 11.5 � 2.9% to 9.2 � 2.1%
(p = 0.003), was obtained in the intervention group. Renal
function parameters, fasting blood glucose, blood pressure
and lipids were also outcome measures, but it remains
unclear, based on the published data, whether differences
were found between intervention and control groups. More
hypoglycaemic episodes, reported as mild to moderate,
occurred in the intervention group than the control group
(17 versus 2, p = not mentioned). Health status and Quality
of Life were not significantly improved in the intervention
group. The second paper [36] reported the outcomes of a
program of direct pharmacist involvement in initiating
insulin treatment in the care of older veterans. A change
from 11.1 � 1.6% to 8.9 � 1.4% (p = 0.00004) in glycated
haemoglobin was reported after 12 months in the inter-
vention group of 23 veterans.
The effect of quarterly visits of a diabetes educator was
assessed versus usual care after 3, 6 and 9 months on
HbA1c, different metabolic parameters, blood pressure and
self-reported compliance with diet and medication [31]. A
multivariate analysis using repeated measures technique
showed no differences on HBA1c, on weight and adherence
values using the initial value as a covariate. The compar-
isons over time and between groups showed no significant
differences. Barriers were the small sample population
(n = 39) and the poor adherence among both groups due to
poor motivation and to lack of financial support to afford
their medications.
The effect of standard consultations was compared
with a patient participating program in which patients
shared therapeutic responsibilities with a follow-up of 48
months [34]. HbA1c, blood pressure, LDL and the number of
cardiovascular events (total mortality, cerebrovascular
mortality, non-fatal vascular events, non-fatal acute
myocardial infarction, non-fatal stroke and coronary
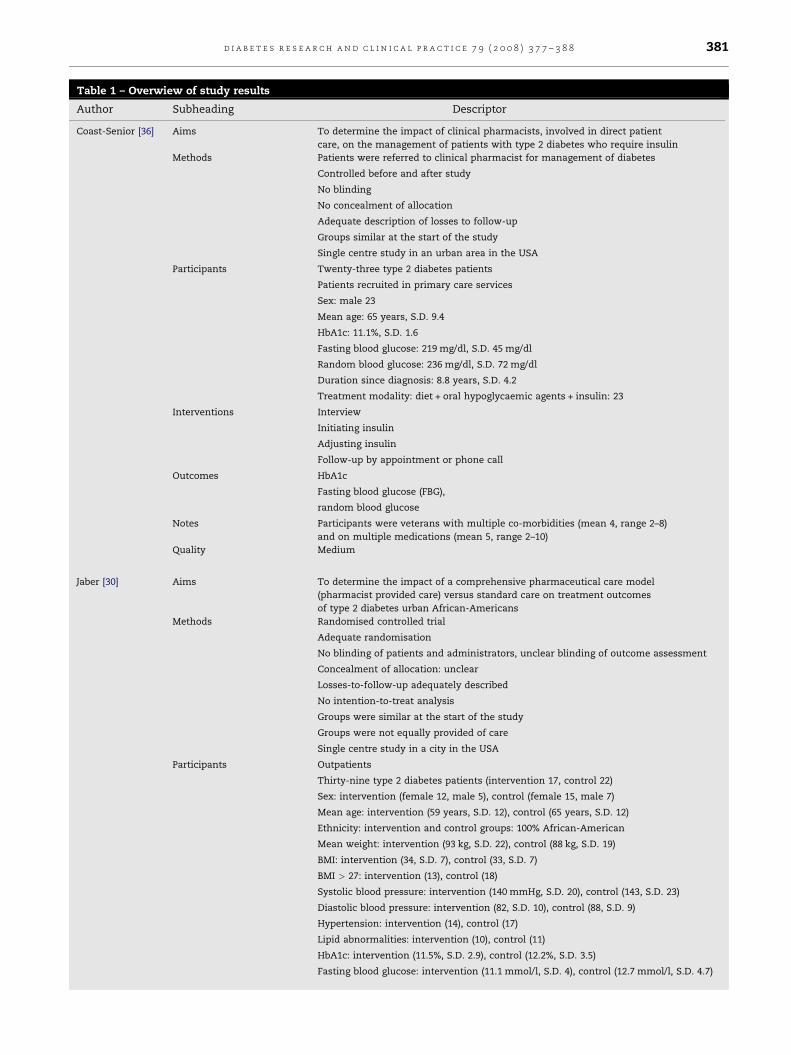
Table 1 – Overwiew of study results
Author Subheading Descriptor
Coast-Senior [36] Aims To determine the impact of clinical pharmacists, involved in direct patient
care, on the management of patients with type 2 diabetes who require insulin
Methods Patients were referred to clinical pharmacist for management of diabetes
Controlled before and after study
No blinding
No concealment of allocation
Adequate description of losses to follow-up
Groups similar at the start of the study
Single centre study in an urban area in the USA
Participants Twenty-three type 2 diabetes patients
Patients recruited in primary care services
Sex: male 23
Mean age: 65 years, S.D. 9.4
HbA1c: 11.1%, S.D. 1.6
Fasting blood glucose: 219 mg/dl, S.D. 45 mg/dl
Random blood glucose: 236 mg/dl, S.D. 72 mg/dl
Duration since diagnosis: 8.8 years, S.D. 4.2
Treatment modality: diet + oral hypoglycaemic agents + insulin: 23
Interventions Interview
Initiating insulin
Adjusting insulin
Follow-up by appointment or phone call
Outcomes HbA1c
Fasting blood glucose (FBG),
random blood glucose
Notes Participants were veterans with multiple co-morbidities (mean 4, range 2–8)
and on multiple medications (mean 5, range 2–10)
Quality Medium
Jaber [30] Aims To determine the impact of a comprehensive pharmaceutical care model
(pharmacist provided care) versus standard care on treatment outcomes
of type 2 diabetes urban African-Americans
Methods Randomised controlled trial
Adequate randomisation
No blinding of patients and administrators, unclear blinding of outcome assessment
Concealment of allocation: unclear
Losses-to-follow-up adequately described
No intention-to-treat analysis
Groups were similar at the start of the study
Groups were not equally provided of care
Single centre study in a city in the USA
Participants Outpatients
Thirty-nine type 2 diabetes patients (intervention 17, control 22)
Sex: intervention (female 12, male 5), control (female 15, male 7)
Mean age: intervention (59 years, S.D. 12), control (65 years, S.D. 12)
Ethnicity: intervention and control groups: 100% African-American
Mean weight: intervention (93 kg, S.D. 22), control (88 kg, S.D. 19)
BMI: intervention (34, S.D. 7), control (33, S.D. 7)
BMI > 27: intervention (13), control (18)
Systolic blood pressure: intervention (140 mmHg, S.D. 20), control (143, S.D. 23)
Diastolic blood pressure: intervention (82, S.D. 10), control (88, S.D. 9)
Hypertension: intervention (14), control (17)
Lipid abnormalities: intervention (10), control (11)
HbA1c: intervention (11.5%, S.D. 2.9), control (12.2%, S.D. 3.5)
Fasting blood glucose: intervention (11.1 mmol/l, S.D. 4), control (12.7 mmol/l, S.D. 4.7)
d i a b e t e s r e s e a r c h a n d c l i n i c a l p r a c t i c e 7 9 ( 2 0 0 8 ) 3 7 7 – 3 8 8 381
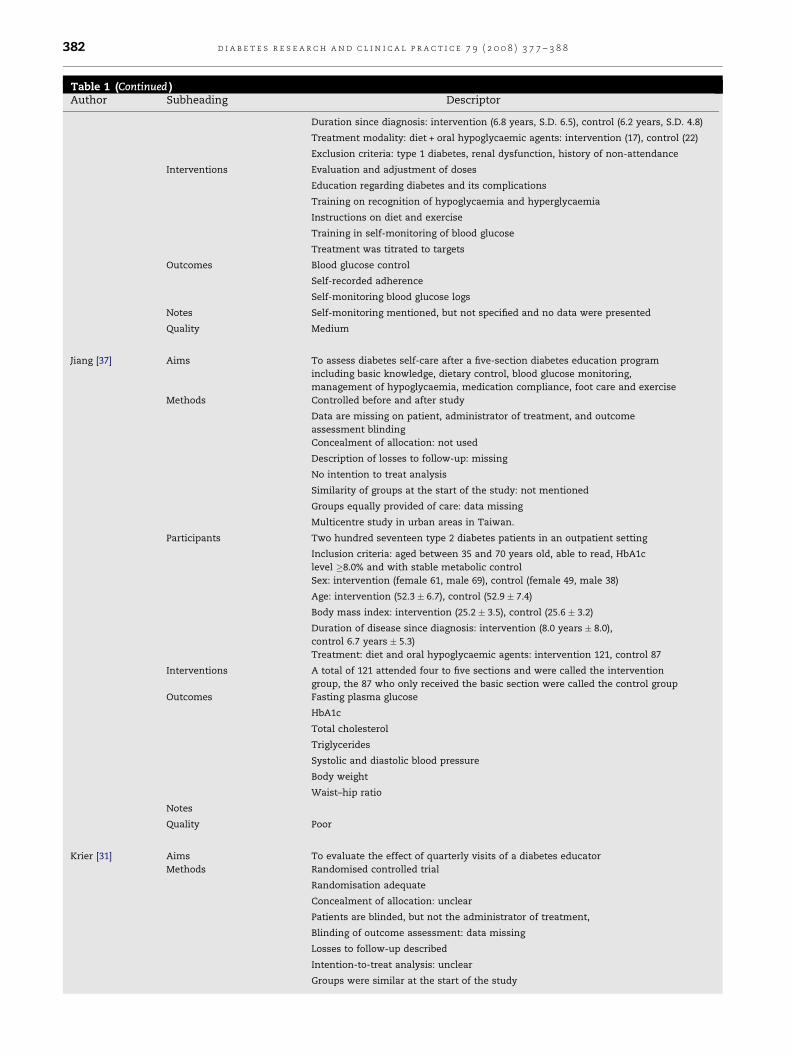
Table 1 (Continued )Author Subheading Descriptor
Duration since diagnosis: intervention (6.8 years, S.D. 6.5), control (6.2 years, S.D. 4.8)
Treatment modality: diet + oral hypoglycaemic agents: intervention (17), control (22)
Exclusion criteria: type 1 diabetes, renal dysfunction, history of non-attendance
Interventions Evaluation and adjustment of doses
Education regarding diabetes and its complications
Training on recognition of hypoglycaemia and hyperglycaemia
Instructions on diet and exercise
Training in self-monitoring of blood glucose
Treatment was titrated to targets
Outcomes Blood glucose control
Self-recorded adherence
Self-monitoring blood glucose logs
Notes Self-monitoring mentioned, but not specified and no data were presented
Quality Medium
Jiang [37] Aims To assess diabetes self-care after a five-section diabetes education program
including basic knowledge, dietary control, blood glucose monitoring,
management of hypoglycaemia, medication compliance, foot care and exercise
Methods Controlled before and after study
Data are missing on patient, administrator of treatment, and outcome
assessment blinding
Concealment of allocation: not used
Description of losses to follow-up: missing
No intention to treat analysis
Similarity of groups at the start of the study: not mentioned
Groups equally provided of care: data missing
Multicentre study in urban areas in Taiwan.
Participants Two hundred seventeen type 2 diabetes patients in an outpatient setting
Inclusion criteria: aged between 35 and 70 years old, able to read, HbA1c
level �8.0% and with stable metabolic control
Sex: intervention (female 61, male 69), control (female 49, male 38)
Age: intervention (52.3 � 6.7), control (52.9 � 7.4)
Body mass index: intervention (25.2 � 3.5), control (25.6 � 3.2)
Duration of disease since diagnosis: intervention (8.0 years � 8.0),
control 6.7 years � 5.3)
Treatment: diet and oral hypoglycaemic agents: intervention 121, control 87
Interventions A total of 121 attended four to five sections and were called the intervention
group, the 87 who only received the basic section were called the control group
Outcomes Fasting plasma glucose
HbA1c
Total cholesterol
Triglycerides
Systolic and diastolic blood pressure
Body weight
Waist–hip ratio
Notes
Quality Poor
Krier [31] Aims To evaluate the effect of quarterly visits of a diabetes educator
Methods Randomised controlled trial
Randomisation adequate
Concealment of allocation: unclear
Patients are blinded, but not the administrator of treatment,
Blinding of outcome assessment: data missing
Losses to follow-up described
Intention-to-treat analysis: unclear
Groups were similar at the start of the study
d i a b e t e s r e s e a r c h a n d c l i n i c a l p r a c t i c e 7 9 ( 2 0 0 8 ) 3 7 7 – 3 8 8382
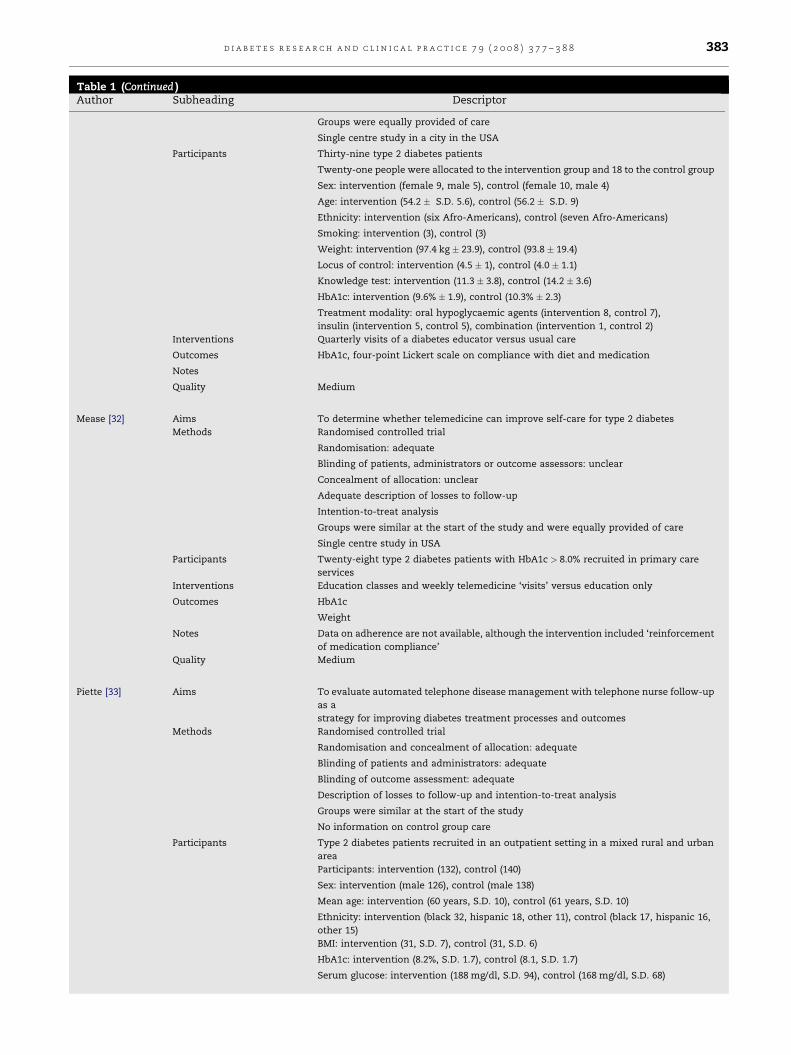
Table 1 (Continued )Author Subheading Descriptor
Groups were equally provided of care
Single centre study in a city in the USA
Participants Thirty-nine type 2 diabetes patients
Twenty-one people were allocated to the intervention group and 18 to the control group
Sex: intervention (female 9, male 5), control (female 10, male 4)
Age: intervention (54.2 � S.D. 5.6), control (56.2 � S.D. 9)
Ethnicity: intervention (six Afro-Americans), control (seven Afro-Americans)
Smoking: intervention (3), control (3)
Weight: intervention (97.4 kg � 23.9), control (93.8 � 19.4)
Locus of control: intervention (4.5 � 1), control (4.0 � 1.1)
Knowledge test: intervention (11.3 � 3.8), control (14.2 � 3.6)
HbA1c: intervention (9.6% � 1.9), control (10.3% � 2.3)
Treatment modality: oral hypoglycaemic agents (intervention 8, control 7),
insulin (intervention 5, control 5), combination (intervention 1, control 2)
Interventions Quarterly visits of a diabetes educator versus usual care
Outcomes HbA1c, four-point Lickert scale on compliance with diet and medication
Notes
Quality Medium
Mease [32] Aims To determine whether telemedicine can improve self-care for type 2 diabetes
Methods Randomised controlled trial
Randomisation: adequate
Blinding of patients, administrators or outcome assessors: unclear
Concealment of allocation: unclear
Adequate description of losses to follow-up
Intention-to-treat analysis
Groups were similar at the start of the study and were equally provided of care
Single centre study in USA
Participants Twenty-eight type 2 diabetes patients with HbA1c > 8.0% recruited in primary care
services
Interventions Education classes and weekly telemedicine ‘visits’ versus education only
Outcomes HbA1c
Weight
Notes Data on adherence are not available, although the intervention included ‘reinforcement
of medication compliance’
Quality Medium
Piette [33] Aims To evaluate automated telephone disease management with telephone nurse follow-up
as a
strategy for improving diabetes treatment processes and outcomes
Methods Randomised controlled trial
Randomisation and concealment of allocation: adequate
Blinding of patients and administrators: adequate
Blinding of outcome assessment: adequate
Description of losses to follow-up and intention-to-treat analysis
Groups were similar at the start of the study
No information on control group care
Participants Type 2 diabetes patients recruited in an outpatient setting in a mixed rural and urban
area
Participants: intervention (132), control (140)
Sex: intervention (male 126), control (male 138)
Mean age: intervention (60 years, S.D. 10), control (61 years, S.D. 10)
Ethnicity: intervention (black 32, hispanic 18, other 11), control (black 17, hispanic 16,
other 15)
BMI: intervention (31, S.D. 7), control (31, S.D. 6)
HbA1c: intervention (8.2%, S.D. 1.7), control (8.1, S.D. 1.7)
Serum glucose: intervention (188 mg/dl, S.D. 94), control (168 mg/dl, S.D. 68)
d i a b e t e s r e s e a r c h a n d c l i n i c a l p r a c t i c e 7 9 ( 2 0 0 8 ) 3 7 7 – 3 8 8 383
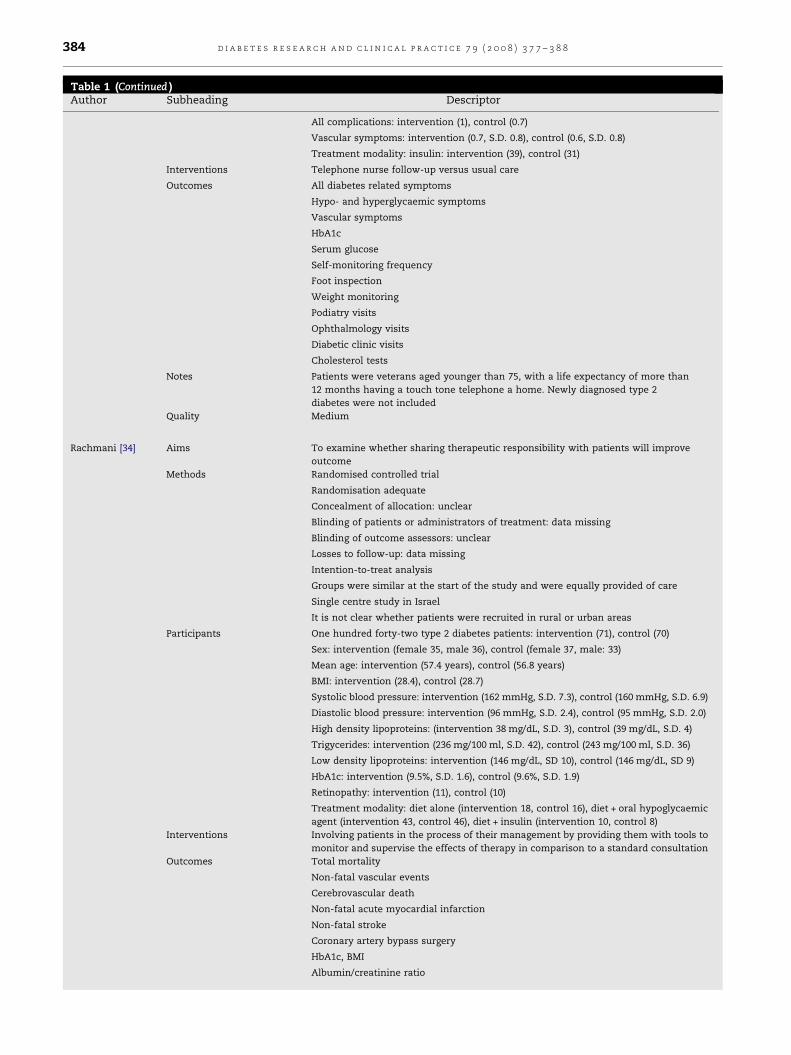
Table 1 (Continued )Author Subheading Descriptor
All complications: intervention (1), control (0.7)
Vascular symptoms: intervention (0.7, S.D. 0.8), control (0.6, S.D. 0.8)
Treatment modality: insulin: intervention (39), control (31)
Interventions Telephone nurse follow-up versus usual care
Outcomes All diabetes related symptoms
Hypo- and hyperglycaemic symptoms
Vascular symptoms
HbA1c
Serum glucose
Self-monitoring frequency
Foot inspection
Weight monitoring
Podiatry visits
Ophthalmology visits
Diabetic clinic visits
Cholesterol tests
Notes Patients were veterans aged younger than 75, with a life expectancy of more than
12 months having a touch tone telephone a home. Newly diagnosed type 2
diabetes were not included
Quality Medium
Rachmani [34] Aims To examine whether sharing therapeutic responsibility with patients will improve
outcome
Methods Randomised controlled trial
Randomisation adequate
Concealment of allocation: unclear
Blinding of patients or administrators of treatment: data missing
Blinding of outcome assessors: unclear
Losses to follow-up: data missing
Intention-to-treat analysis
Groups were similar at the start of the study and were equally provided of care
Single centre study in Israel
It is not clear whether patients were recruited in rural or urban areas
Participants One hundred forty-two type 2 diabetes patients: intervention (71), control (70)
Sex: intervention (female 35, male 36), control (female 37, male: 33)
Mean age: intervention (57.4 years), control (56.8 years)
BMI: intervention (28.4), control (28.7)
Systolic blood pressure: intervention (162 mmHg, S.D. 7.3), control (160 mmHg, S.D. 6.9)
Diastolic blood pressure: intervention (96 mmHg, S.D. 2.4), control (95 mmHg, S.D. 2.0)
High density lipoproteins: (intervention 38 mg/dL, S.D. 3), control (39 mg/dL, S.D. 4)
Trigycerides: intervention (236 mg/100 ml, S.D. 42), control (243 mg/100 ml, S.D. 36)
Low density lipoproteins: intervention (146 mg/dL, SD 10), control (146 mg/dL, SD 9)
HbA1c: intervention (9.5%, S.D. 1.6), control (9.6%, S.D. 1.9)
Retinopathy: intervention (11), control (10)
Treatment modality: diet alone (intervention 18, control 16), diet + oral hypoglycaemic
agent (intervention 43, control 46), diet + insulin (intervention 10, control 8)
Interventions Involving patients in the process of their management by providing them with tools to
monitor and supervise the effects of therapy in comparison to a standard consultation
Outcomes Total mortality
Non-fatal vascular events
Cerebrovascular death
Non-fatal acute myocardial infarction
Non-fatal stroke
Coronary artery bypass surgery
HbA1c, BMI
Albumin/creatinine ratio
d i a b e t e s r e s e a r c h a n d c l i n i c a l p r a c t i c e 7 9 ( 2 0 0 8 ) 3 7 7 – 3 8 8384

Table 1 (Continued )Author Subheading Descriptor
Blood pressure
Retinopathy
Glomerular filtration rate
Notes
Quality Medium
White [35] Aims To compare the effect of group management versus an advice-educational technique
Methods Randomised controlled trial
Randomisation: adequate
Concealment of allocation: inadequate
Blinding of patient, administrator of treatment, and of outcome assessment: data
missing
Losses to follow-up clearly described
Intention-to-treat analysis
Groups were similar at the start of the study
Groups were equally provided of care
Participants Thirty-two type 2 diabetes outpatients
Inclusion criteria: less than satisfactory control (FBG > 140 mg/dl), infrequent
hypoglycaemic reactions (<1/mol), no history of ketoacidosis, body weight >15%
above the mean value for height, no history of alcohol abuses or severe personality
disorder, and no current use of glucocorticoids
Sex: men only
Age: intervention (62.4 years � 5.5), control (60.7 years � 6.4)
Percentage of weight excess: intervention (36.3% � 21.0), control (44.3% � 21.0)
Duration since diagnosis: intervention (10.2 years � 12.9), control (13.6 years � 9.6)
Interventions Group management versus an advice-educational technique
Outcomes HbA1c
Notes
Quality Poor
d i a b e t e s r e s e a r c h a n d c l i n i c a l p r a c t i c e 7 9 ( 2 0 0 8 ) 3 7 7 – 3 8 8 385
artery bypass surgery) were evaluated in both groups.
HbA1c improved by from 9.5 � 1.6% before to 8.2 � 1.5%
after the patient participation program (p < 0.05 versus
standard care group).
(2) G
roup educationGroup education was compared with a usually used
management technique, based on advice and education
over 6 months in 32 veterans [35]. The advice-education
control group format was designed to minimize subject
interaction by having a nurse and a dietician give lectures
on the disease and is management. The experimental
management group was divided in three smaller groups of
less than eight members which met separately with a
clinical psychologist experienced in small group manage-
ment. An endocrinologist served as a consultant on call for
the psychologist during and between experimental group
sessions. Subjects in the experimental group were encour-
aged to interact and assessed their own and their peers’
progress towards managing their diabetes by sharing
ideas, advice, and support. There was a 10% decline in
HbA1c levels (p < 0.05) during the first 3 months of the
study in both groups, The effect, however, did not persist
until the end of the study.
The effect of a five-section education program inter-
vention over 4 months was compared with a basic course
(control) by measuring of fasting blood glucose, HbA1c,
serum cholesterol, triglycerides, blood pressure and body
weight [37]. The educational program covered the defini-
tion of diabetes mellitus, dietary control and meal plan,
urine and blood glucose testing, action of insulin and oral
hypoglycaemic agents, symptoms and treatment of hypo-
glycaemia and uncontrolled hyperglycaemia, foot care and
exercise. Those who attended only Section 1, the basics of
diabetes mellitus, were considered the control group.
Those who attended four to five were designed as the
experimental group. In both the experimental and the
control groups, the decline in HbA1c levels was statistically
significant (from 9.4 � 1.2% to 8.7 � 1.4% p < 0.001, versus
from 9.3 � 1.4% to 9.0 � 1.5%, p = 0.008). In the experi-
mental group, the decline in fasting plasma glucose, total
cholesterol, systolic blood pressure, body weight and
waist–hip ratio was also statistically significant. The effect
on drug adherence, though assessed by a questionnaire,
was not reported separately.
(3) T
elemedicine educationThe comparison of the effectiveness of education
classes plus a weekly nurse telemedicine ‘home visit’
versus usual care showed a statistically significant reduc-
tion in mean HbA1c level of 14% (from 9.5 (8.1–12.6)% to 8.2
(5.7–10.2)%, p < 0.05) over a period of 3 months [32]. The
mean weight reduction was limited and there were no
significant changes on a Diabetes Quality of Life scale or on

d i a b e t e s r e s e a r c h a n d c l i n i c a l p r a c t i c e 7 9 ( 2 0 0 8 ) 3 7 7 – 3 8 8386
the Medical Outcome Health Survey SF-36 scale. Some
metabolic parameters such as micro-albuminuria, serum
creatinin and serum lipids did not improve during the
study period. Physicians and case managers considered
telemedicine to have a high benefit, but technological
problems were a major obstacle.
A nurse-led automated telephone management inter-
vention, with weekly follow-up nurse calls about self-care,
medication adherence and symptoms, showed a small but
statistically significant (p = 0.04) lowering of glycated
haemoglobin for patients with an initial level of �8%(33).
Patients in the intervention group also reported more
frequent glucose self-monitoring and foot inspections and
a 10% reduction in diabetes related symptoms. However,
there was no significant lowering of glycated haemoglobin
levels for the entire intervention group. Finally there were
no differences between groups in the proportion of
patients reporting one or more medication adherence
problems.
3.3. Quantitative synthesis
Studies assessing educational interventions ranging from
offering education individually [30,31,33,36] over group educa-
tion [35,37] to education on distance [32,33] were pooled
statistically. Since comparable assessments on medication
taking were not available in the different studies, the HbA1c
was used as a common outcome measure. The weighted mean
difference (WMD) of the studies evaluating the effect of
education offered individually on the short (3–6 months) and
medium term (9–12 months) was calculated. It was not
surprising that the I2 test exceeded 70%, indicating consider-
able levels of heterogeneity [38] thus making statistical pooling
almost unacceptable.
4. Discussion
This subgroup analysis of a Cochrane Systematic Review could
not draw clear and consistent conclusions on the effect of
educational interventions aimed at improving adherence in
medication taking in people living with type 2 diabetes. A
slightly positive overall effect is shown, but this leaves us with
the question whether a small statistical significant effect
entails clinical relevant effects. Moreover, even when an effect
has been shown it remains unclear which intervention or
which part of a complex educational intervention contributed
the most to the perceived effect. A second conclusion of this
review is that there is an urgent need for high quality
interventional and observational studies on the relation
between education in people living with type 2 diabetes and
adherence to medicine taking or even self management as a
whole, assessing effectiveness and efficiency of the performed
interventions. Finally, authors should clearly define adher-
ence and should search for valid methods to measure the
adherence as they define it.
Though the review process was performed according to the
Cochrane Metabolic and Endocrine Diseases Collaborative
Review Group recommendations, there are some limitations.
First, on the one hand a comprehensive search in different
electronic databases and by hand searching was performed,
but on the other hand one may assume that in this area of
research many studies may be unpublished. Unfortunately,
funnel plots could not be calculated to assess publication bias
because of the high clinical heterogeneity. Second, only eight
studies could be included in this analysis. The most important
reason for exclusion was the low quality of retrieved studies
which main shortcomings were the unclear or missing
concealment of allocation and the blinding procedures.
Moreover, the lack of appropriate operational definitions of
adherence contributed to a high exclusion rate. In a majority of
articles, although compliance or adherence was mentioned to
be the topic of research, it merely was diabetes care in general
or self-care in particular that was assessed. Many authors
even did not feel the need to define adherence nor did they
make no clear distinction between compliance, adherence or
concordance [12]. The authors’ lack of definition of adherence
was the most disturbing factor in this reviewing process. At
least authors could lay upon Glasgow and Anderson [25] who
state that the constructs of ‘compliance’ and ‘adherence’
might be replaced by ‘collaborative goal-setting’ and ‘on-going
self-management support’. Third, as a result of the lack of
definition, valid measurement instruments and valid outcome
measures are missing. Since HbA1c was shown in most of the
included studies this outcome measure was used as a proxy
for adherence. Fourth, this review was not able to explore
which educational interventions or which part of complex
interventions contributed most to the overall effect size. Fifth
is the sample size that may limit the synthesis and its
conclusions. Most of the studies included rather small
numbers of participants limiting statistical procedures and
hence preventing from doing comparisons between groups
and subgroups. Sixth, no economic aspects were studied. This
is quite surprising because, although better diabetes outcomes
are aimed at by governments, managed care organizations,
caregivers and by patients themselves, no economic con-
sequences of interventions were considered.
Seventh, the literature review was completed in November
2002 and trials published since then may differ in their results,
although they would be unlikely to substantially change the
conclusions drawn from the eight trials included in this
review. An update of the review will be performed in 2008.
Besides the mentioned limitations and weaknesses, a
number of strengths are to be stressed. The review’s
conclusions are consistent with a UK Health Technology
Assessment systematic review [39] which concludes that
education, as part of an intensification of treatment, produces
improvement in diabetic control in type 1 diabetes, which has
not consistently been shown in type 2 though. For people with
type 2 diabetes, a meta-analysis assessing the role of
education shows overall modest improvements in glycaemic
control too [40]. The problems that were faced in the reviewing
process seem to be common to reviewing adherence issues in
medical care in general. Authors of different systematic
reviews of adherence to treatment for blood pressure lowering
medication [41], lipid lowering drugs [42] or even medication
adherence as a whole for chronic health problems [11]
described exactly the same problems and pitfalls. In general
clear conclusions were hard to be drawn.

d i a b e t e s r e s e a r c h a n d c l i n i c a l p r a c t i c e 7 9 ( 2 0 0 8 ) 3 7 7 – 3 8 8 387
The importance of education on improving adherence to
medication has been stressed earlier [43]. The relation between
adherence to medications (based on pharmacy claims) and
clinical outcomes has been shown for type 2 diabetes, since a
10% decrease in adherence to metformin and statins was
associated with an increase of 0.14% of HbA1c [44]. It has to be
stressed that clinical outcomes are not always consistently
related to the magnitude of adherence results [45].
The complexity of adherence has prevented the develop-
ment of a gold standard method of measurement [46]. Direct
and indirect measurements are being used, but serious
obstacles remain in generating valid and reliable estimates of
the extent of adherence [12]. Aiming at understanding better
and improving more adherences, a focus on reliability and
validity of adherence measurement is urgently needed [47].
Moreover, it is challenging to decide which outcomes of
educational interventions should be considered. Adherence to
treatment recommendations is to be found in physical
activity, eating, medication taking, monitoring of blood
glucose, problem solving as for sick days, reducing risks for
diabetes complications and psychosocial adaptation [48].
Further research into this area is desperately needed. It is
striking that in such an ‘epidemic disease’ with a high human
and financial burden so little high quality research on
improving adherence has been executed. Though everybody
claims that education is an essential part of the management
of diabetes, the effectiveness of educational interventions on
adherence and the relation between adherence and clinical
outcomes still need clarification. Also, the efficiency of
different educational interventions such as group sessions,
education on distance and the use of new information
technology need to be studied more profoundly, not omitting
economic assessments [21,49,50].
5. Conclusions
The question whether educational interventions aiming at
improving adherence to medication in people living with type
2 diabetes are effective remains unanswered.
In spite of a high number of abstracts fitting the search
strategy only eight studies could be included in this subgroup
analysis of a systematic review. Though the term ‘adherence’
is often mentioned in titles or abstracts, adherence itself is not
the subject of the research presented.
It is important though to state that this review did not show
evidence that educational interventions may be ineffective or
even harmful. Finally, this review process point at how
trustworthy research in the future should be conducted.
Conflicts of interests
None.
Acknowledgement
The research project was made possible by an unconditional
grant of Primary Care Diabetes Europe ivzw/inpo.
r e f e r e n c e s
[1] E. Vermeire, J. Wens, P. Van Royen, Y. Biot, H. Hearnshaw,A. Lindenmeyer, Interventions for improving adherence totreatment recommendations in people with type 2 diabetesmellitus, Cochrane Database of Systematic Reviews 2005,Issue 2, Art. No.: CD003638, doi:10.1002/14651858.CD003638.pub2.
[2] International Diabetes Federation, Triennial Report (1991–1994) and Directory, Brussels, 1994.
[3] A. Amos, D.P.Z. McCarty, The rising global burden ofdiabetes and its complications: estimates and projectionsto the year 2010, Diab. Med. 14 (1997) S1–S85.
[4] H. King, R.E. Aubert, W.H. Herman, Global burden ofdiabetes, 1995–2025: prevalence, numerical estimates, andprojections, Diab. Care 21 (9) (1998) 1414–1431.
[5] G. Roglic, N. Unwin, P.H. Bennett, C. Mathers, J. Tuomilehto,S. Nag, et al., The burden of mortality attributable todiabetes: realistic estimates for the year 2000, Diab. Care 28(9) (2005) 2130–2135.
[6] American Diabetes A, Standards of medical care indiabetes—2007, Diab. Care 30 (Suppl. 1) (2007)S4–S41.
[7] UK Prospective Diabetes Study Group, Intensive bloodglucose control with sulphonylureas or insulin comparedwith conventional treatment and risk of complications inpatients with type 2 diabetes (UKPDS 33), Lancet 352 (1998)837–853.
[8] UK Prospective Diabetes Study Group, Effect of intensiveblood glucose control with metformin on complications inoverweight patients with type 2 diabetes (UKPDS 34),Lancet 352 (1998) 854–865.
[9] UK Prospective Diabetes Study Group, Tight blood pressurecontrol and risk of macro vascular and micro vascularcomplications in type 2 diabetes (UKPDS 38), BMJ 317 (1998)703–713.
[10] UK Prospective Diabetes Study Group, Efficacy of atenololand captopril in reducing risk of both macro vascular andmicro vascular complications in type 2 diabetes (UKPDS 39),BMJ 317 (1998) 73–720.
[11] R.B. Haynes, X. Yao, A. Degani, S. Kripalani, A. Garg, H.P.McDonald, Interventions for enhancing medicationadherence. Cochrane Database of Systematic Reviews 2005,Issue 4, Art. No.: CD000011, doi:10.1002/14651858.CD000011.pub2.
[12] E. Vermeire, H. Hearnshaw, P. Van Royen, J. Denekens,Patient adherence to treatment: three decades of research.A comprehensive review, J. Clin. Pharm. Ther. 26 (5) (2001)331–342.
[13] M. Nagasawa, M.C. Smith, J.H.J.R. Barnes, J.E. Fincham,Meta-analysis of correlates of diabetes patients’compliance with prescribed medications, The Diab.Educator 16 (3) (1990) 192–200.
[14] E. Vermeire, P. Van Royen, S. Coenen, J. Wens, J. Denekens,The adherence of type 2 diabetes patients to theirtherapeutic regimens: a qualitative study from the patient’sperspective, Pract. Diab. Int. 20 (6) (2003) 209–214.
[15] H. Van Dam, F. Van der Horst, B. Van den Borne, R.Ryckman, H. Crebolder, Provider–patient interaction indiabetes care: effects on patient self-care and outcomes. Asystematic review, Patient Educ. Couns. 51 (2003) 17–28.
[16] S.E. Ellis, T. Speroff, R.S. Dittus, A. Brown, J.W. Pichert, T.A.Elasy, Diabetes patient education: a meta-analysis andmeta-regression, Patient Educ. Couns. 52 (1) (2004)91–105.
[17] S. Brown, Effects of educational interventions indiabetes care: a meta-analysis of findings, Nurs. Res. 37(1988) 223–230.
d i a b e t e s r e s e a r c h a n d c l i n i c a l p r a c t i c e 7 9 ( 2 0 0 8 ) 3 7 7 – 3 8 8388
[18] D. Padgett, Meta-analysis of the effects of educational andpsychosocial interventions on management of diabetesmellitus, J. Clin. Epidemiol. 41 (1988) 1007–1030.
[19] S. Brown, Meta-analysis of diabetes patient educationresearch: variations in intervention effects across studies,Res. Nurs. Health 15 (1992) 409–419.
[20] D.L. Roter, J.A. Hall, R. Merisca, B. Nordstrom, D. Cretin, B.Svarstad, Effectiveness of interventions to improve patientcompliance: a meta-analysis, Med. Care 36 (8) (1998) 1138–1161.
[21] S.L. Norris, M.M. Engelgau, K.M. Venkat Narayan,Effectiveness of self-management training in type 2diabetes: a systematic review of randomized controlledtrials, Diab. Care 24 (3) (2001) 561–587.
[22] International Diabetes Federation, Diabetes Atlas/DiabetesEducation, second ed., IDF, Brussels, 2003, Chapter 6, p.208.
[23] S.A. Brown, Interventions to promote diabetes self-management: state of the science, The Diab. Educator 25 (6Suppl.) (1999) 52–61.
[24] P. Corabian, C. Harstall, Patient diabetes education in themanagement of adult type 2 diabetes: Centre for Reviewsand Dissemination. Database of Abstracts of Reviews ofEffects (DARE); 2001.
[25] R.E. Glasgow, R.M. Anderson, In diabetes care, moving fromcompliance to adherence is not enough. Something entirelydifferent is needed, Diab. Care 22 (12) (1999) 2090–2092.
[26] R.M. Anderson, M.M. Funnell, Compliance and adherenceare dysfunctional concepts in diabetes care, The Diab.Educator 26 (4) (2000) 597–604.
[27] Olivarius NdF, H. Beck-Nielsen, A.H. Andreasen, M. Horder,P.A. Pedersen, Randomised controlled trial of structuredpersonal care of type 2 diabetes mellitus, BMJ 323 (7319)(2001) 970.
[28] J. Wens, E. Vermeire, P. Van Royen, H. Hearnshaw, Asystematic review of adherence with medications fordiabetes: response to cramer, Diab. Care 27 (9) (2004), 2284-.
[29] World Health Organisation (WHO), Adherence to long-termtherapies. Evidence for action, World Health Organisation(WHO), Geneva, 2003, Chapter 1, Defining adherence, pp. 3–7.
[30] L.A. Jaber, H. Halapy, M. Fernet, S. Tummalapalli, H.Diwakaran, Evaluation of a pharmaceutical care model ondiabetes management, The Ann. Pharmacother. 30 (1996)238–243.
[31] B.P. Krier, R.D. Parker, D. Grayson, G. Byrd, Effect of diabeteseducation on glucose control, J. La State Med. Soc. 151(1999) 87–92.
[32] A. Mease, W.L. Whitlock, A. Brown, K. Moore, H. Pavliscsak,A. Dingbaum, et al., Telemedicine improved diabeticmanagement, Mil. Med. 165 (8) (2000) 579–584.
[33] J.D. Piette, M. Weinberger, F.B. Kraemer, S.J. McPhee,Impact of automated calls with nurse follow-up on diabetestreatment outcomes in a department of veterans affairsHealth Care System, Diab. Care 24 (2) (2001) 202–208.
[34] R. Rachmani, Z. Levi, I. Slavachevski, M. Avin, M. Ravid,Teaching patients to monitor their risk factors retards theprogression of vascular complications in high-risk patients
with Type 2 diabetes mellitus. A randomized prospectivestudy, Diab. Med. 19 (2002) 385–392.
[35] N. White, J. Carnahan, C.A. Nugent, T. Iwaoka, M.A.Dodson, Management of obese patients with diabetesmellitus: comparison of advice education with groupmanagement, Diab. Care 9 (5) (1986) 490–496.
[36] E.A. Coast-Senior, B.A. Kroner, C.L. Kelley, L.E. Trilli,Management of patients with type 2 diabetes bypharmacists in primary care clinics, The Ann.Pharmacother. 32 (1998) 636–641.
[37] Y.-D. Jiang, L.-M. Chuang, H.-P. Wu, S.-J. Shiau, C.-H. Wang,Y.-J. Lee, et al., Assessment of the function and effect ofdiabetes education programs in Taiwan, Diab. Res. Clin.Pract. 46 (1999) 177–182.
[38] Available from: http://www.cochrane-net.org/openlearning/HTML/mod13.htm.
[39] E. Loveman, C. Cave, C. Green, P. Royle, N. Dunn, N. Waugh,The clinical and cost-effectiveness of patient educationmodels for diabetes: a systematic review and economicevaluation, Health Technol. Assess. 7 (22) (2003) 1–202.
[40] T.L. Gary, J.M. Genkinger, E. Guallar, M. Peyrot, F.L. Brancati,Meta-analysis of randomized educational and behavioralinterventions in type 2 diabetes, The Diab. Educator 29 (3)(2003) 488–501.
[41] K. Schroeder, T. Fahey, S. Ebrahim, Interventions forimproving adherence to treatment in patients with highblood pressure in ambulatory settings, Cochrane Databaseof Systematic Reviews 2004, Issue 3, Art. No.: CD004804,doi:10.1002/14651858.CD004804.
[42] A. Schedlbauer, K. Schroeder, T.J. Peters, T. Fahey,Interventions to improve adherence to lipid loweringmedication, Cochrane Database of Systematic Reviews2004, Issue 4, Art. No.: CD004371, doi:10.1002/14651858.CD004371.pub2.
[43] G. Rutten, Diabetes patient education: time for a new era,Diab. Med. 22 (6) (2005) 671–673.
[44] M. Pladevall, L.K. Williams, L.A. Potts, G. Divine, H. Xi, J.Elston Lafata, Clinical outcomes and adherence tomedications measured by claims data in patients withdiabetes, Diab. Care 27 (12) (2004) 2800–2805.
[45] S. Kripalani, X. Yao, R.B. Haynes, Interventions to enhancemedication adherence in chronic medical conditions: asystematic review, Arch. Intern. Med. 167 (6) (2007) 540–549.
[46] K.C. Farmer, Methods for measuring and monitoringmedication regimen adherence in clinical trials and clinicalpractice, Clin. Ther. 21 (1999) 1074–1090.
[47] M.R. DiMatteo, Variations in patients’ adherence to medicalrecommendations: a quantitative review of 50 years ofresearch, Med. Care 42 (3) (2004) 200–209.
[48] American Association of Diabetes E, Standards foroutcomes measurement of diabetes self-managementeducation, The Diab. Educator 29 (5) (2003) 804–816.
[49] D.C. Klonoff, D.M. Schwartz, An economic analysis ofinterventions for diabetes, Diab. Care 23 (3) (2000)390–404.
[50] R.M. Kaplan, W.K. Davis, Evaluating the costs and benefitsof outpatient diabetes education and nutrition counseling,Diab. Care 9 (1) (1986) 81–86.
Related Documents











