28 April 2018, RACV City Club, Melbourne Education event: COPD & its comorbidities Activity no: 125314

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

28 April 2018, RACV City Club, Melbourne
Education event: COPD & its comorbidities
Activity no: 125314
Before we begin
Emergency exists Rest rooms Mobile phones

OPC Support and Collaborations
Gold Sponsors Partner
Agenda – part 1
Time Presentation / Activity Presenter
9.45 – 10.00 am Introduction - Prof David Price
10.00 – 10.30 amGOLD and Australian COPDX guidelines, Australian Best Practice Guidelines for
Diabetes, Guidelines for the prevention, detection and management of chronic heart
failure in Australia: considering recent evidence
- Prof Peter Frith - Dr Anita Sharma -Prof Merlin Thomas
10.30 – 10.45 am Common co-morbidities of COPD, Heart Failure and Diabetes - Prof Peter Frith
10.45 – 11:00 amExacerbations of COPD: current state of the art in terms of differential diagnosis (vs HF),
treatment and prevention- Prof David Price
11.00 – 11.30 am Review of delegate pre-disposing activity (COPD with a co-morbidity) – Morning tea
- Prof David Price - Prof Peter Frith - Dr
Anita Sharma - Dr Kerry Hancock - Prof
Merlin Thomas
11.30 – 11.45 am Psychological factors in COPD - Dr Kerry Hancock
11.45 – 12.15 pmPanel Discussion – Inadequate and over treatment of COPD, Heart Failure and Diabetes
and implications for clinical practice.
Prof David Price - Prof Peter Frith - Dr
Anita Sharma - Dr Kerry Hancock -
Prof Merlin Thomas
12.15 – 12.45 pmGroup Discussion -Continue review of delegate pre-disposing activity (COPD, Heart
Failure, Diabetes case studies) in light of panel discussion
Prof David Price - Prof Peter Frith
- Dr Anita Sharma - Dr Kerry Hancock
- Prof Merlin Thomas
12:45 – 1.15 pm Lunch
Agenda – part 2
Time Presentation / Activity Presenter
1.15 – 1.45 pmPanel Discussion
Referrals and Investigations for COPD, Heart Failure and Diabetes. When to refer,
appropriate use of tests and biomarkers for guiding treatment (stepping up and down)
- Prof David Price - Prof Peter Frith -
Dr Anita Sharma - Dr Kerry Hancock -
Prof Merlin Thomas
1.45 – 2.45 pm
Workshop 1: Inhaler technique in COPD
………………………………………………………...………………………………………………...
Workshop 2: Interpreting spirometry
- W1: Prof David Price + nurses (LFA)
- W2: Prof Peter Frith + Dr Kerry Hancock
2.45 – 3.30 pm
Case studies
Case study 1: COPD and heart failure (role of rehab)
Case study 2: COPD and Diabetes
- Dr Anita Sharma + Prof David Price
- Dr Merlin Thomas + Prof David Price
3.30 – 3.45 pm Afternoon Tea
3.45 – 4.30 pm Discussions of learnings from meeting and post meeting follow-ups- Prof David Price
4.30 pm Event close – Exit Venue

Introduction

Our panel
Kerry Hancock
Anita Sharma Merlin ThomasPeter Frith
David Price
Dr Kerry Hancock - Principal, Chandlers Hill Surgery, Happy Valley SA;
Executive member COPD National Program, Lung Foundation Australia;
Chair, RACGP Respiratory Medicine Specific Interest Network
Prof Merlin Thomas - physician scientist in the Department of Diabetes,
Monash University, Melbourne, Australia
Prof David Price - Professor David Price is the founder and director of
OPC (Australia and UK)
Dr Peter Frith - Professor in Respiratory Medicine at Flinders University
in Adelaide, Adjunct Professor in Health Sciences at University of South
Australia, and he serves on the Boards of Directors of GOLD and of Lung
Foundation Australia (LFA)
Dr Anita Sharma - principal at Platinum Medical Centre
What COPD Looks Like Today
OPC Collaborations

Guidelines: COPD, Diabetes and Heart Failure
Chair of session: Peter Frith

Heart Failure Guidelines For Primary Care in 2018
Dr Anita Shama MBBS FRACGP

Heart Failure
HF: heart failure https://www.escardio.org/Guidelines/Clinical-Practice-Guidelines/Acute-and-Chronic-Heart-Failure
• HF is complex syndrome, often underdiagnosed and undertreated due in part to
the non specific nature of presentation and presence of other co-morbidities that
compete for attention.
• HF is however ‘A SILENT KILLER’ associated with high mortality, reduced quality-
of-life, and high cost to the community.
• Mortality from HF parallels or even exceeds some cancer associated mortality:
50% of HF patients are dead at 5 years!
Heart Failure
https://www.escardio.org/Guidelines/Clinical-Practice-Guidelines/Acute-
and-Chronic-Heart-Failure
• Optimum HF management involves both non-pharmacological and pharmacological
therapies and a patient centred mulit-disciplinary plan, coordinated by the GP, and
ideally involving other HCPs such as HF specialists (cardiologists/HF nurses),
dietitians, exercise therapists, social workers, psychologists and pharmacists.
• HF is commonly classified according to assessment of LVEF. Patients are generally
described as having HF with normal or preserved LVEF (HFpEF) [LVEF ≥50%] or HF
reduced LVEF (HFrEF) [LVEF of <40%]. There is now also an entity HFmEF that
refers to patients with EF in the grey zone (40-49%)
EF: ejection fraction; GP: general practitioner; HCP: health care practitioner; HF:
heart failure; HFmEF: heart failure and midrange ejection fraction; HFpEF: heart
failure with preserved ejection fraction; LVEF: left ventricular ejection fraction
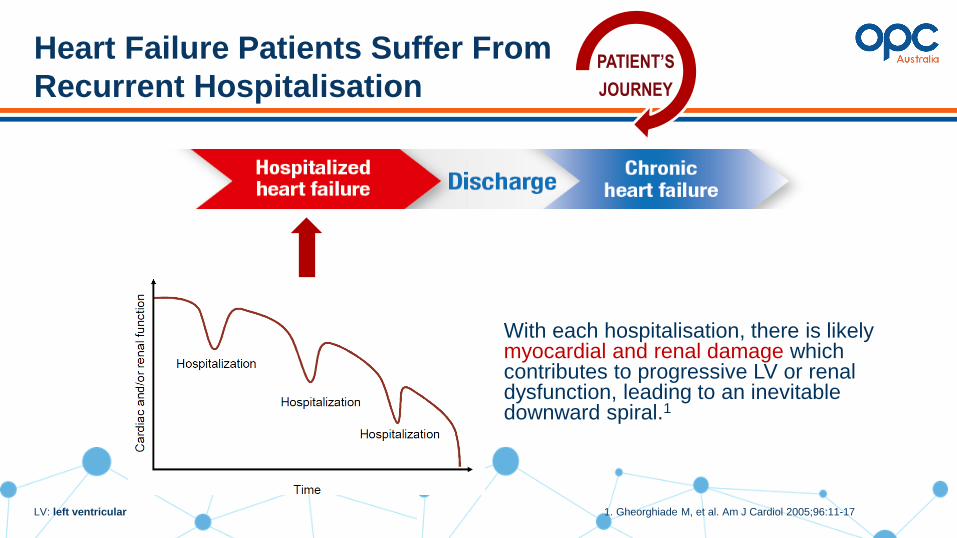
Heart Failure Patients Suffer From
Recurrent Hospitalisation
1. Gheorghiade M, et al. Am J Cardiol 2005;96:11-17LV: left ventricular
PATIENT’S
JOURNEY
With each hospitalisation, there is likely myocardial and renal damage which contributes to progressive LV or renal dysfunction, leading to an inevitable downward spiral.1

Diagnostic
Algorithm for CHF
BNP: B-type natriuretic peptide; CHF: congestive heart failure;
JVP: jugular venous pressure; LVEF: left ventricular ejection
fraction; MI: myocardial infarction; PND: paroxysmal nocturnal
dyspnoea

HF Current Guidelines in Australia (LVEF<40%)
Heart foundation guidelines for
the prevention, detection and
management of CHF in
Australia from October 2011
NYHA IVNYHA II to III
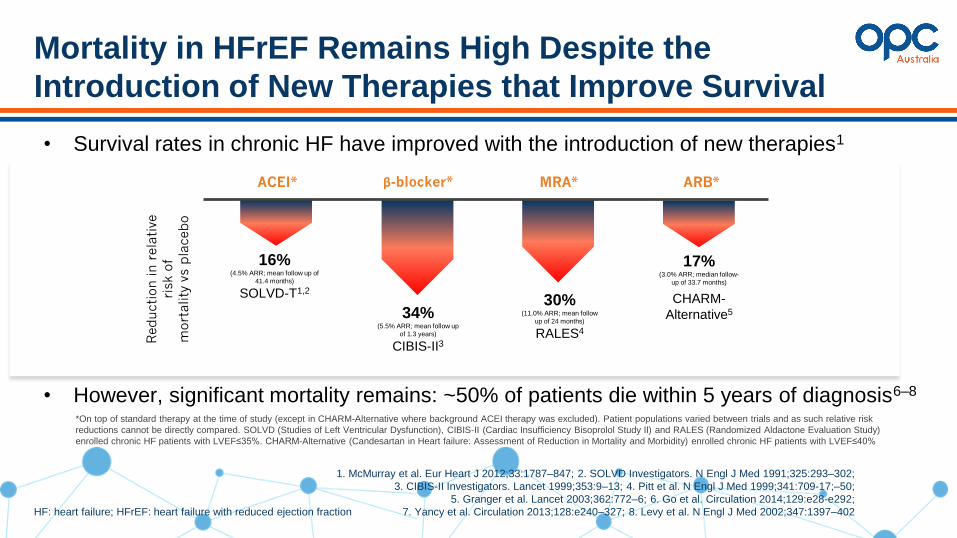
Mortality in HFrEF Remains High Despite the
Introduction of New Therapies that Improve Survival
1. McMurray et al. Eur Heart J 2012;33:1787–847; 2. SOLVD Investigators. N Engl J Med 1991;325:293–302;
3. CIBIS-II Investigators. Lancet 1999;353:9–13; 4. Pitt et al. N Engl J Med 1999;341:709-17;–50;
5. Granger et al. Lancet 2003;362:772–6; 6. Go et al. Circulation 2014;129:e28-e292;
7. Yancy et al. Circulation 2013;128:e240–327; 8. Levy et al. N Engl J Med 2002;347:1397–402HF: heart failure; HFrEF: heart failure with reduced ejection fraction
• Survival rates in chronic HF have improved with the introduction of new therapies1
16%(4.5% ARR; mean follow up of
41.4 months)
SOLVD-T1,2
34%(5.5% ARR; mean follow up
of 1.3 years)
CIBIS-II3
Reducti
on in r
ela
tive
risk o
f
mort
ality
vs p
lacebo
30%(11.0% ARR; mean follow
up of 24 months)
RALES4
17%(3.0% ARR; median follow-
up of 33.7 months)
CHARM-
Alternative5
ACEI* β-blocker* MRA* ARB*
• However, significant mortality remains: ~50% of patients die within 5 years of diagnosis6–8
*On top of standard therapy at the time of study (except in CHARM-Alternative where background ACEI therapy was excluded). Patient populations varied between trials and as such relative risk
reductions cannot be directly compared. SOLVD (Studies of Left Ventricular Dysfunction), CIBIS-II (Cardiac Insufficiency Bisoprolol Study II) and RALES (Randomized Aldactone Evaluation Study)
enrolled chronic HF patients with LVEF≤35%. CHARM-Alternative (Candesartan in Heart failure: Assessment of Reduction in Mortality and Morbidity) enrolled chronic HF patients with LVEF≤40%

Take Home Message
HF: heart failure; NYHA: New York Heart Association https://www.escardio.org/Guidelines/Clinical-Practice-Guidelines/Acute-and-Chronic-Heart-Failure
• Diagnose HF early (targeted approach) and start treatment in early stage of
disease (NYHA II and early NYHA III)
• Optimise background therapies Ace-I, b-blockers, diuretics, MRAs
• Consider option of ARNI if symptoms persist- ‘STABLE’ is not good enough
• Do not forget lifestyle measures (fluid/salt balance, nutrition, exercise,
psychological support, etc.)
• HF patients are ‘fragile’, and at risk of sudden decompensation hospitalisation,
and sudden death
Diabetes Guidelines
Professor Merlin Thomas
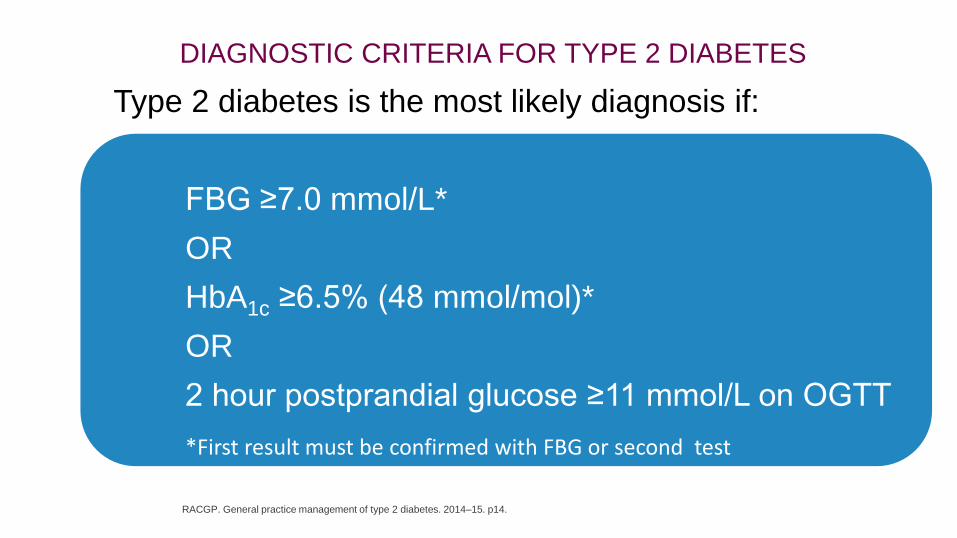
Type 2 diabetes is the most likely diagnosis if:
FBG ≥7.0 mmol/L*
OR
HbA1c ≥6.5% (48 mmol/mol)*
OR
2 hour postprandial glucose ≥11 mmol/L on OGTT
*First result must be confirmed with FBG or second test
DIAGNOSTIC CRITERIA FOR TYPE 2 DIABETES
RACGP. General practice management of type 2 diabetes. 2014–15. p14.


Diabetes* increases the risk of CV events
Emerging Risk Factors Collaboration, Lancet 2010;375:2215–2222.
Coronary heart disease
Coronary death
Non-fatal MI
Cerebrovascular disease
Ischaemic stroke
Haemorrhagic stroke
Unclassified stroke
Other vascular deaths
2.00 (1.83–2.19)
2.31 (2.05–2.60)
1.82 (1.64–2.03)
2.27 (1.95–2.65)
1.56 (1.19–2.05)
1.84 (1.59–2.13)
1.73 (1.51–1.98)
HR (95% CI)
26,505
11,556
14,741
3799
1183
4973
3826
Cases (n)
1 2 4Hazard ratio (diabetes vs no diabetes)
Outcome
2
* independent to age, smoking status, body mass index and systolic blood pressure
DM

Does the patient have macrovascular disease?
− Cardiac ischemia (silent or overt)
− Peripheral arterial disease
− Cerebrovascular/carotid disease
AND if the patient is NOT at glycemic target
Does the patient have
microvascular disease?
− Retinopathy
− Kidney disease (ACR≥2.0)
− Neuropathy
Is the patient...
− age ≥55 with additional CV risk factors?
− age ≥40?− age ≥30, and diabetes >15 years?
− warranted for statin therapy based on the Canadian
Statin1
+
ACEi/ARB2
+
ASA3
Liraglutide, Empagliflozin or Canagliflozin4
Statin1
+
ACEi/ARB2
Statin1
YES
YES
YES
NO
N
O
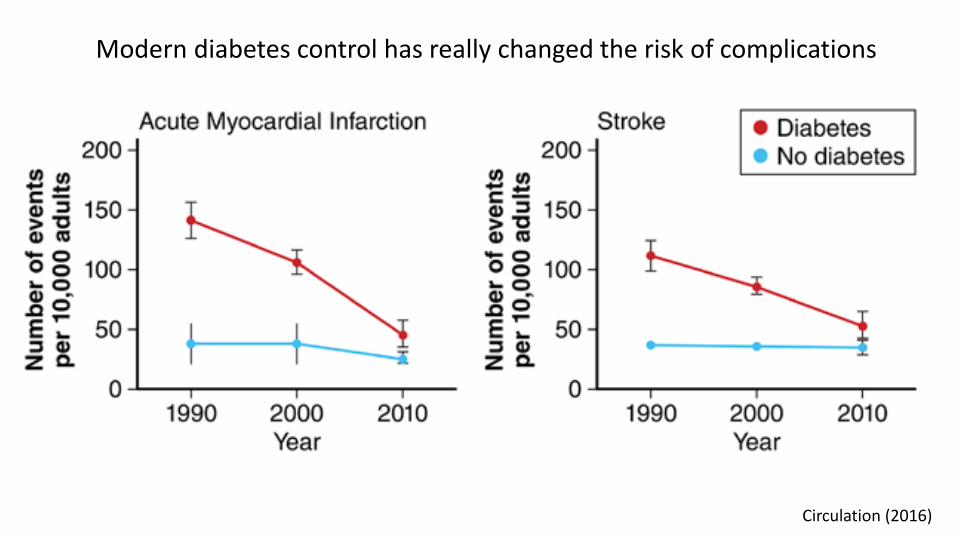
Circulation (2016)
Modern diabetes control has really changed the risk of complications

STENO-2
7.8 years
∆Median
survival
7.9 years
Gæde, et al Diabetologia (2016)
Intensive
Standard
Years since randomisation
Cu
mu
lati
ve
Mo
rta
lity

In some countries, older adults are clearly in the majority
0
50
100
150
200
250
300
350
20-24 25-29 30-34 35-39 40-44 45-49 50-54 55-59 60-64 65-69 70-74 75-79 80-84 85+Tho
usa
nd
s
>50% of adults
with diabetes are 65+
Australia

In the aged, the choice of agent should focus on drug safety, especially
protecting against hypoglycaemia, heart failure, renal dysfunction, bone
fractures and drug interactions. Strategies specifically minimising the
risk of low blood glucose may be preferred.

Common comorbidities of COPD – Heart
Failure & Diabetes
Chair of session: Peter Frith

COPD & its Comorbiditiesfor OPC Australia
Peter Frith
Lung Foundation Australia
Global Initiative for chronic Obstructive Lung Disease
Flinders University College of Medicine & Public Health
University of South Australia Health Sciences Faculty
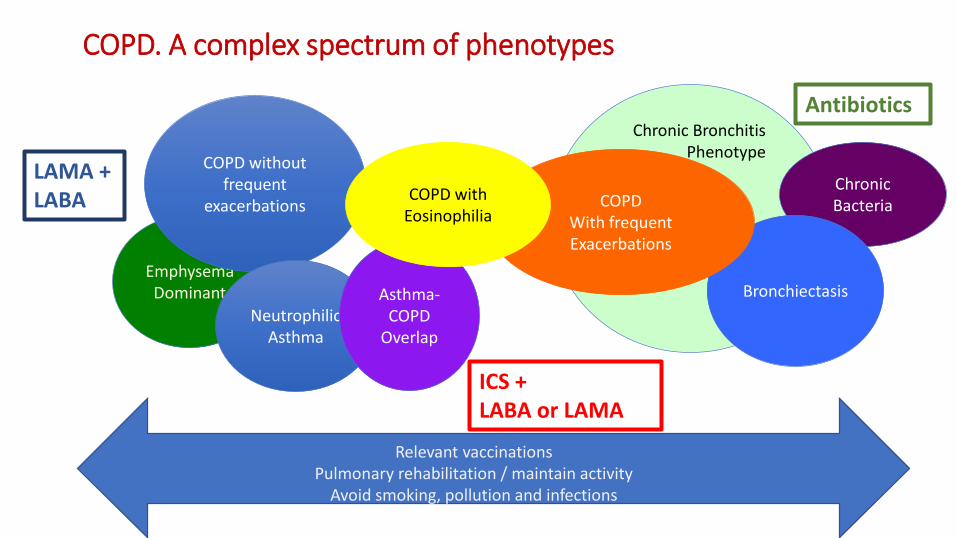
EmphysemaDominant
Chronic Bacteria
Bronchiectasis
COPDWith frequentExacerbations
COPD. A complex spectrum of phenotypes
COPD withoutfrequent
exacerbations
NeutrophilicAsthma
Chronic BronchitisPhenotype
Asthma-COPD
Overlap
COPD with Eosinophilia
LAMA + LABA
ICS + LABA or LAMA
Antibiotics
Relevant vaccinationsPulmonary rehabilitation / maintain activity
Avoid smoking, pollution and infections
COPD & Comorbid diseases
• COPD is very common (1 in 7 of Australians over age 45)
• Other chronic conditions are also common• Cardiovascular and cerebrovascular diseases
• Diabetes mellitus and endocrine disorders
• Osteoporosis and degenerative joint diseases
• Asthma
• Sleep breathing disorders
• Lifestyle factors are shared across some of these
• COPD has not only shared prevalence but also has systemic effects

COPD is not all smoking-relatedPrimary and secondary prevention are not uniform Comorbidities are not uniform
Agusti A & Faner R. Lancet Respir Med 2018 Feb 26
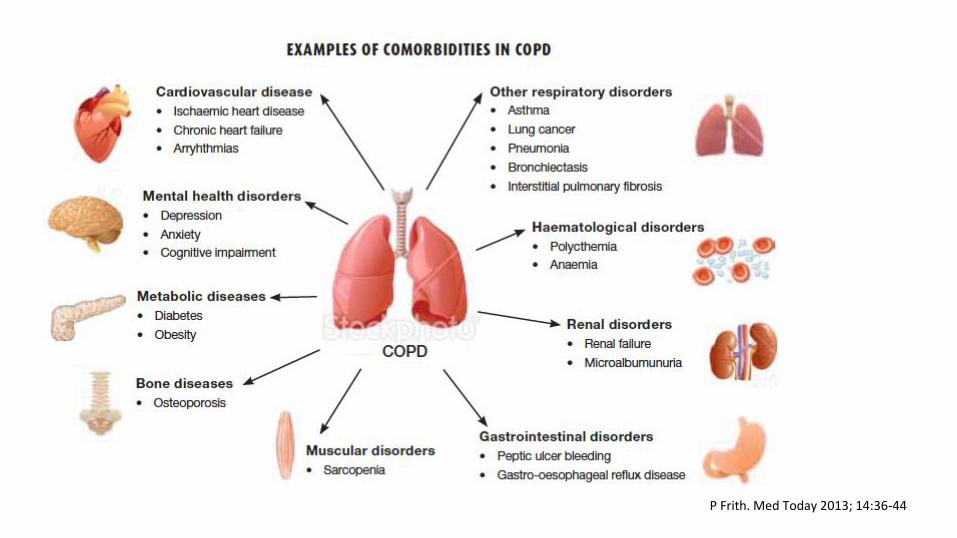
P Frith. Med Today 2013; 14:36-44

Comorbidities measured in COPD patients
MC Smith, JP Wrobel. Internat J COPD 2014; 9:871-888
Comorbidities can occur with any COPD severityA Agusti, et al. Respir Res 2010; 11:122
Co-occurrence worsens outcomes in most conditionsD Mascarenhas, et al. Am Heart J 2008; 155:521-525
Exacerbation risk and severity increase with comorbidityJA Westerik, et al. Respir Res 2017; 18:31
Principles of managing COPD
• Primary prevention• Target all smoking• Reduce home and atmospheric air pollution
• Detect COPD in all who really have it• Targeted screening• Confirm and quantify airways obstruction with spirometry• Clarify comorbid symptom confusion
• Control symptoms• Optimise bronchodilators (drugs and devices) for the individual• Enhance exercise capacity and willingness to be active
• Reduce risks of deterioration• Prevent and reduce impact of exacerbations• Detect and treat exacerbations early and well• Prolong life• Avoid harm (respiratory and comorbidities)
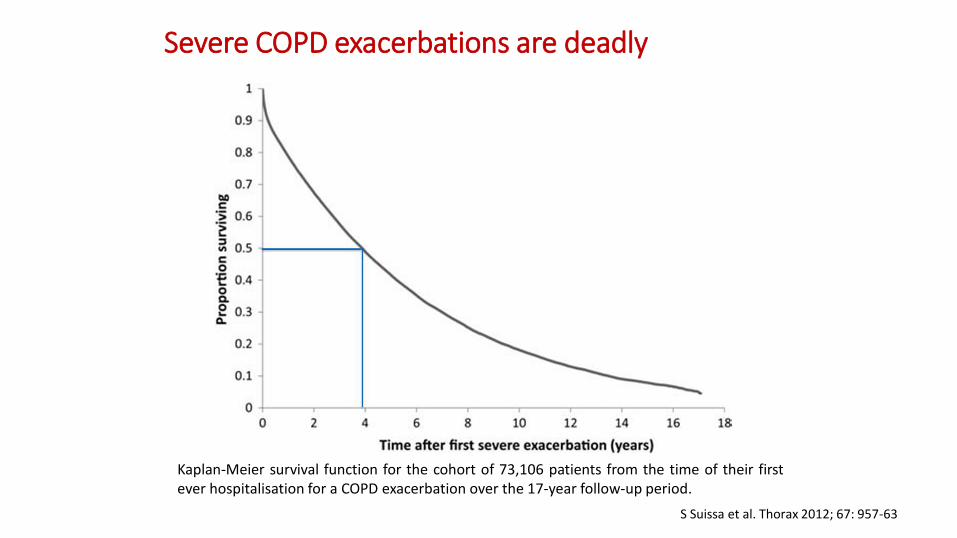
Severe COPD exacerbations are deadly
S Suissa et al. Thorax 2012; 67: 957-63
Kaplan-Meier survival function for the cohort of 73,106 patients from the time of their firstever hospitalisation for a COPD exacerbation over the 17-year follow-up period.
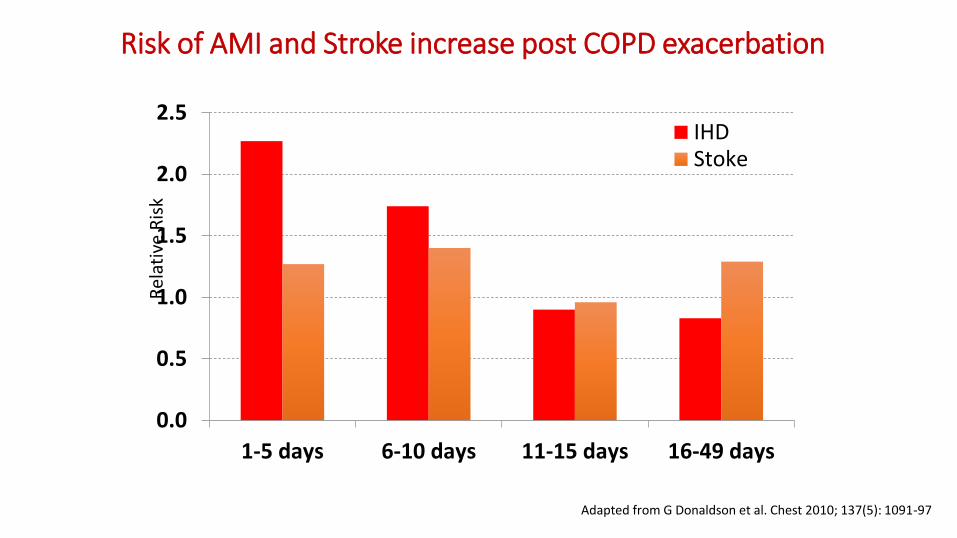
Risk of AMI and Stroke increase post COPD exacerbation
0.0
0.5
1.0
1.5
2.0
2.5
1-5 days 6-10 days 11-15 days 16-49 days
IHDStoke
Rel
ativ
e R
isk
Adapted from G Donaldson et al. Chest 2010; 137(5): 1091-97

COPD and Chronic Heart Failure have similar symptoms
DJA Janssen et al. J Pall Med 2011;14:735-743
(n=105) (n=80)
Mean age=66.3[SD 9.2], 61.9% male Mean age=76.2[SD 8.3], 67.5% male
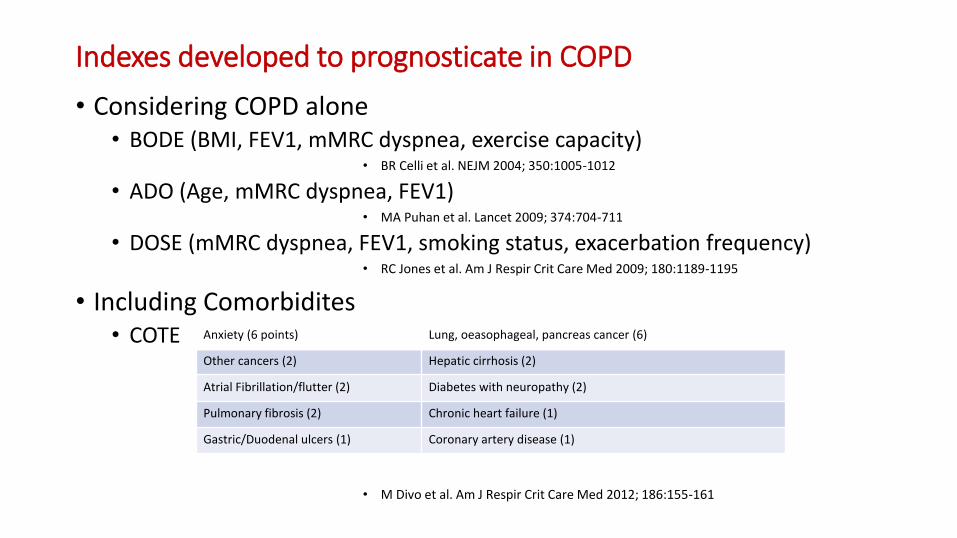
Indexes developed to prognosticate in COPD
• Considering COPD alone• BODE (BMI, FEV1, mMRC dyspnea, exercise capacity)
• BR Celli et al. NEJM 2004; 350:1005-1012
• ADO (Age, mMRC dyspnea, FEV1)• MA Puhan et al. Lancet 2009; 374:704-711
• DOSE (mMRC dyspnea, FEV1, smoking status, exacerbation frequency)• RC Jones et al. Am J Respir Crit Care Med 2009; 180:1189-1195
• Including Comorbidites• COTE
• M Divo et al. Am J Respir Crit Care Med 2012; 186:155-161
Anxiety (6 points) Lung, oeasophageal, pancreas cancer (6)
Other cancers (2) Hepatic cirrhosis (2)
Atrial Fibrillation/flutter (2) Diabetes with neuropathy (2)
Pulmonary fibrosis (2) Chronic heart failure (1)
Gastric/Duodenal ulcers (1) Coronary artery disease (1)
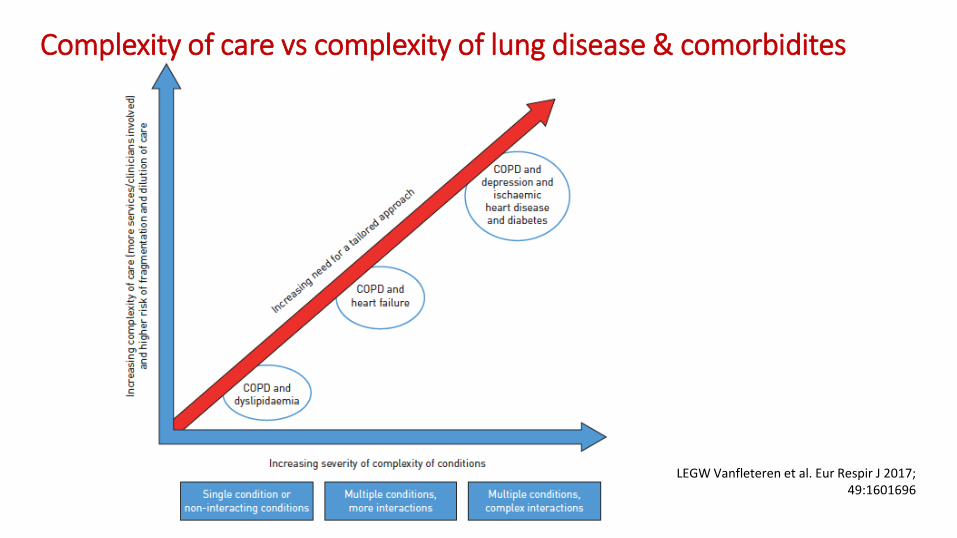
Complexity of care vs complexity of lung disease & comorbidites
LEGW Vanfleteren et al. Eur Respir J 2017; 49:1601696
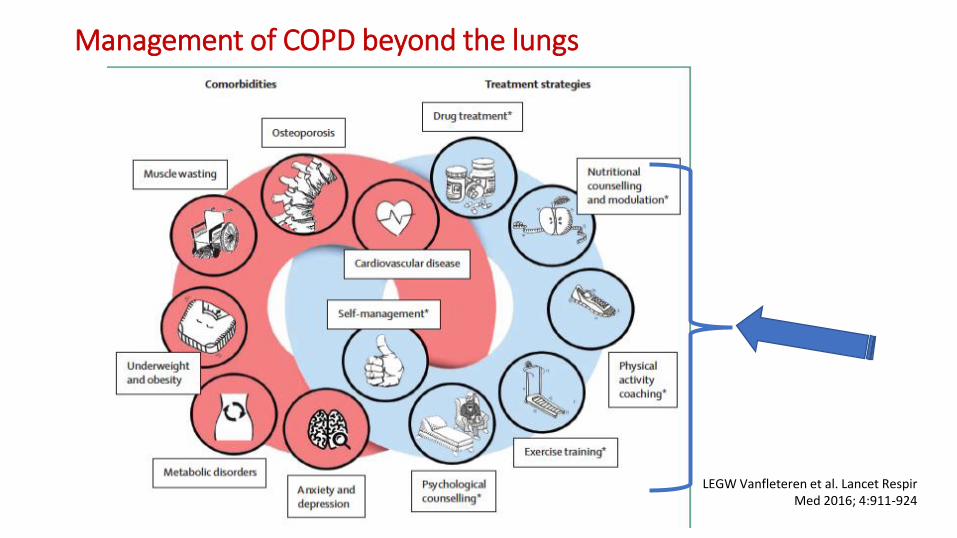
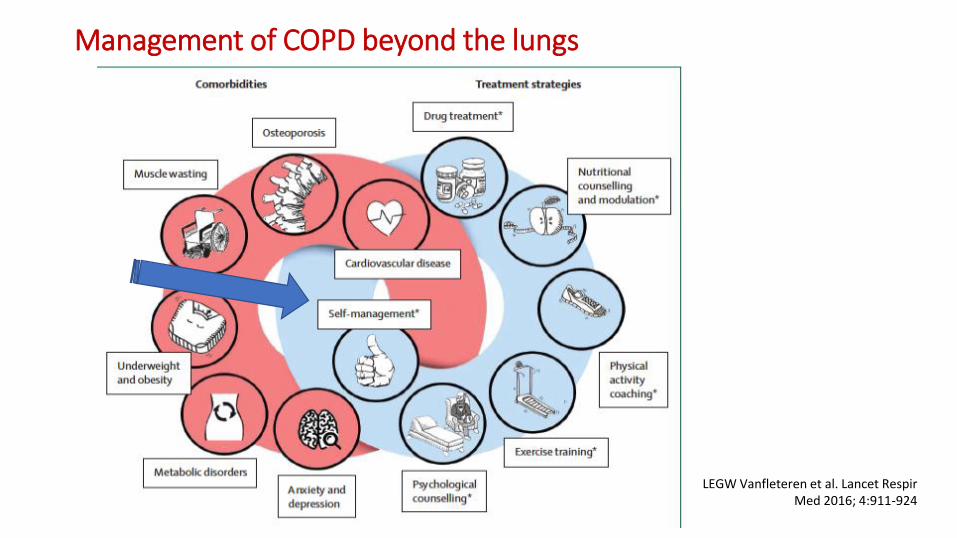
Management of COPD beyond the lungs
LEGW Vanfleteren et al. Lancet Respir Med 2016; 4:911-924
Management of COPD beyond the lungs
LEGW Vanfleteren et al. Lancet Respir Med 2016; 4:911-924

Self management interventions for COPD DO NOT reduce exacerbations of COPD
Odds Ratio = 0.01 (-0.28, 0.29) A Lenferink et al. Cochrane Database Syst Rev 2015; 10.1002/12651858.CD011682
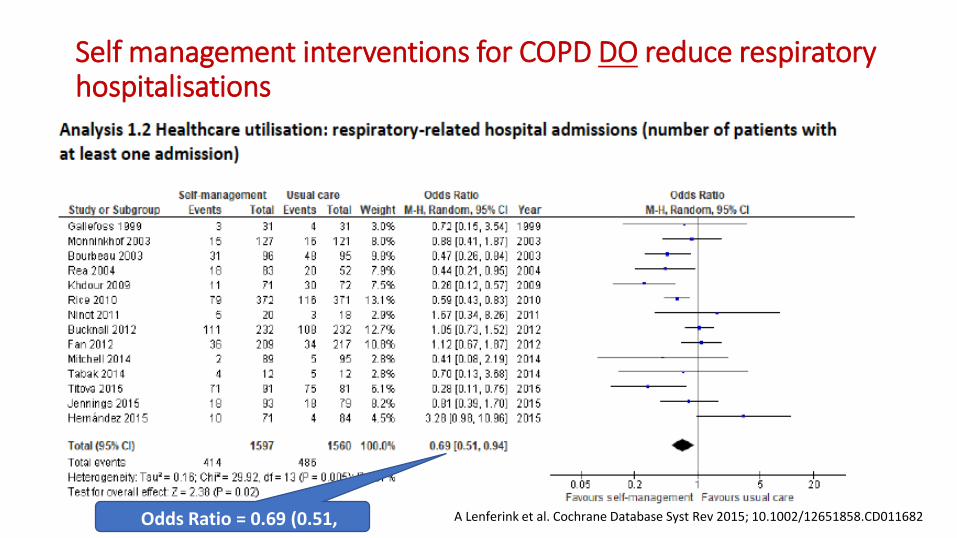
Self management interventions for COPD DO reduce respiratory hospitalisations
Odds Ratio = 0.69 (0.51, 0.94)
A Lenferink et al. Cochrane Database Syst Rev 2015; 10.1002/12651858.CD011682
Medication regimen complexity affects outcomes in COPD combined with non-COPD diagnoses
• Dosage, device complexity and timing of respiratory medications
• Dosage, timing and routes of non-COPD medications
• Medication regimen complexity index (MRCI)• J George et al. Ann Pharmacother 2004; 38:1369-1376
• RECOMMENDATIONS
• Minimise multiple dosing frequencies
• Minimise numbers of and harmonise inhaler devices
• Time non-COPD medications with COPD medication dosing
• NA Negewo et al. Internat J COPD 2017; 12:2929-2942

Biomarkers for patients with COPD in primary care
• ‘C’ - Diagnosis & differential (acute and stable phase symptoms)• Spirometry; spirometry reversibility
• Blood eosinophils; FeNO
• BNP, procalcitonin, CRP, low interleukin-15, high interleukin-8
• ‘O’ - Management• Future risk - History of moderate and severe exacerbations; blood eosinophils
• Current impact - Level of symptom impact (mMRC; CAT; CCQ; SGRQ; CRQ)
• Comorbidities
• ‘P’ - Prognosis• Spirometry; pO2; pCO2; BODE Index; ADO; DOSE; AKPS; fibrinogen
• Comorbidities
• ‘X’ - Exacerbation • Symptom increment

What to look out for at a 14-day post-discharge check-up to predict early unplanned readmission &/or refer to specialist
• COPD severity scores
• Symptoms out of proportion to spirometry or unusual/unexpected• Heart failure / heart disease• Anaemia• Asthma• Lung cancer
• Blood eosinophil count (>350)
• Adherence to prescribed bronchodilators & correct use of device
• Exacerbations in the previous year
• Possession & use of action plans
• Pack-years and duration of smoking and ongoing smoking
• Level of airways obstruction (FEV1 % predicted)
Exacerbations of COPD and Heart Failure: current state of the art in terms of differential diagnosis, treatment
and prevention
Chair of session: David Price
Exacerbations of COPD: current state of the art in terms of differential diagnosis vs heart
failure, treatment and prevention
Chair of session: David Price

CI: confidence interval; OR: odds ratio
Jones R, et al. Lancet Respir Med 2014;2:267-276;
Wedzicha JA, Seemungal TA. Lancet 2007;370:786-96
‘Exacerbations’ Before Diagnosis to After Diagnosis
OR (95% CI)
N = 38, 859
First year after diagnosis 3.16 (3.01, 3.32)*
Second year after diagnosis 2.81 (2.67, 2.96)**
* Adjusted for age, gender, place of diagnosis & year of diagnosis
** Adjusted for age, gender & year of diagnosis
Patients with frequent exacerbations
Higher mortality
Greater airway
inflammation
Poorer quality
of life
Faster decline
in lung function
More hospital
admissions
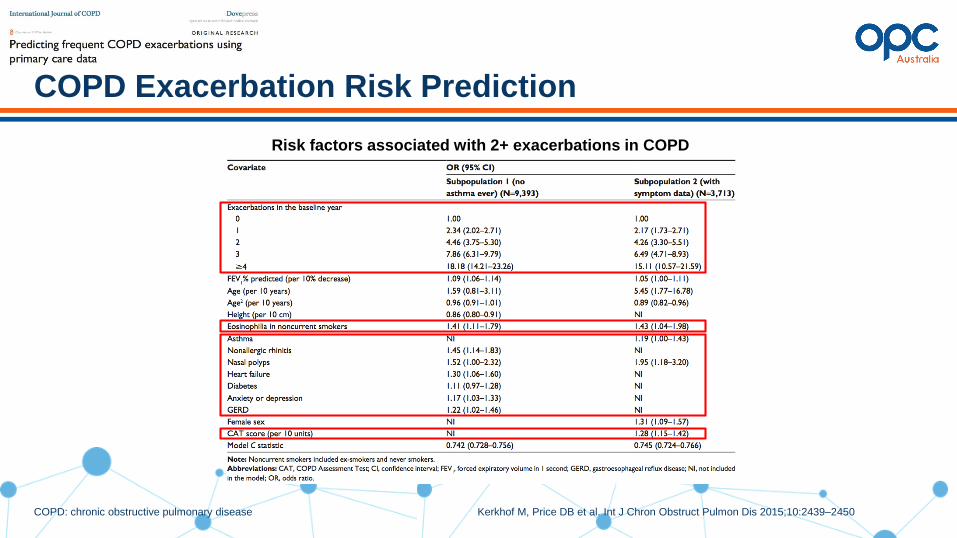
COPD: chronic obstructive pulmonary disease Kerkhof M, Price DB et al. Int J Chron Obstruct Pulmon Dis 2015;10:2439–2450
COPD Exacerbation Risk Prediction
Risk factors associated with 2+ exacerbations in COPD

MRC: medical research council Price D, et al. Unpublished data
Patients with COPD and HF are More Breathless
than Patients with COPD Alone
Study endpoint: time to first LABA or LAMA prescription after COPD diagnosis
Patients are censored at the end of patient records (extraction or leaving practice), death, or heart failure diagnosis after COPD diagnosis in the COPD only cohort

COPD: chronic obstructive pulmonary disease; HF: heart failure Lipworth B, Price D et al. Heart 2016; 102(23): 1934
Underuse of Beta-Blockers in Patients with HF and COPD
Prescription of BB and ACEI/ARB for patients with HF and COPD according to inhaler therapy
Prescription of BB and ACEI/ARB for patients with HF alone versus patients with HF and COPD
ICS: inhaled corticosteroid; LABA: long-acting β2-agonist;
LAMA: long-acting muscarinic antagonist
1. Yang et al., The COPD-X Plan 2016, Version 2.46; Lung Foundation Australia
2. Australian Pharmaceutical Benefits Scheme, 2017 http://www.pbs.gov.au/pbs/home
3. Harrison et al. Intern Med J., 2017;47:1310–13
COPD and ICS in Australia
COPD and ICS indication in Australia
Inhaled corticosteroids should be considered in patients:• with post-bronchodilator FEV1 <50% predicted and who experience >2 exacerbations in 12 months 1,2
ICS monotherapy is not indicated in COPD 1,2
In patients with coexisting asthma and COPD, ICS monotherapy can sometimes be used together with LAMA, LABA or LAMA/LABA fixed dose combination inhalers (as the ICS would be indicated for asthma) 1,2
But in reality...Of 707 COPD patients identified from the lung function test database at a tertiary Australian hospital;
52.4% of patients with a post-bronchodilator FEV1 ≥50% were prescribed an ICS 3
...inappropriate use of ICS in Australia?
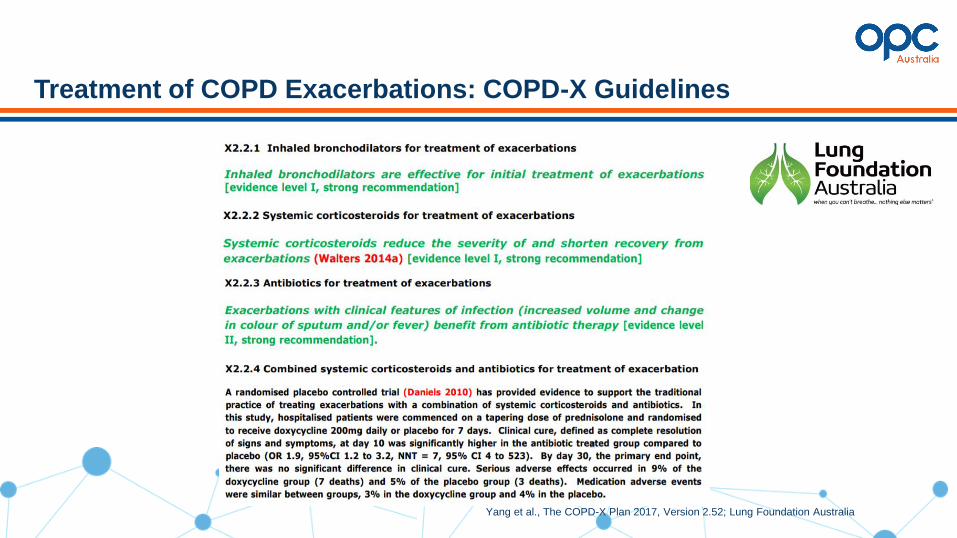
Yang et al., The COPD-X Plan 2017, Version 2.52; Lung Foundation Australia
Treatment of COPD Exacerbations: COPD-X Guidelines
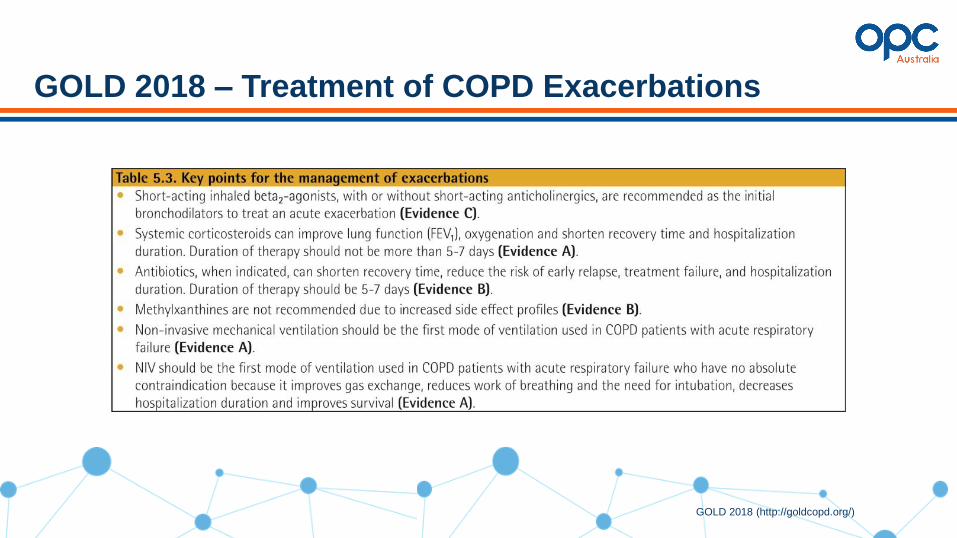
GOLD 2018 – Treatment of COPD Exacerbations
GOLD 2018 (http://goldcopd.org/)
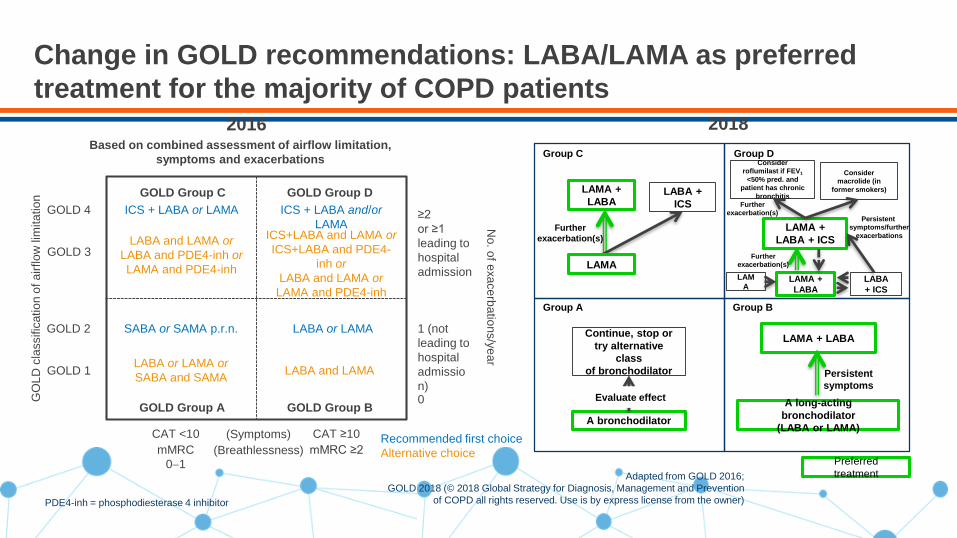
Change in GOLD recommendations: LABA/LAMA as preferred
treatment for the majority of COPD patients
PDE4-inh = phosphodiesterase 4 inhibitor
Adapted from GOLD 2016;
GOLD 2018 (© 2018 Global Strategy for Diagnosis, Management and Prevention
of COPD all rights reserved. Use is by express license from the owner)
GOLD 1
GOLD 2
GOLD 3
GOLD 4
CAT ≥10
mMRC ≥2
CAT <10
mMRC
0−1N
o. o
f exa
ce
rba
tion
s/y
ea
r
≥2
or ≥1
leading to
hospital
admission
Based on combined assessment of airflow limitation,
symptoms and exacerbations
0
1 (not
leading to
hospital
admissio
n)
ICS + LABA or LAMA ICS + LABA and/or
LAMA
LABA and LAMA or
LABA and PDE4-inh or
LAMA and PDE4-inh
ICS+LABA and LAMA or
ICS+LABA and PDE4-
inh or
LABA and LAMA or
LAMA and PDE4-inh
SABA or SAMA p.r.n. LABA or LAMA
LABA or LAMA or
SABA and SAMA LABA and LAMA
Recommended first choice
Alternative choice
(Symptoms)
(Breathlessness)
GO
LD
cla
ssific
atio
n o
f a
irflo
w lim
ita
tio
n GOLD Group C GOLD Group D
GOLD Group A GOLD Group B
Group A Group B
Group C Group D
A bronchodilator
Continue, stop or
try alternative
class
of bronchodilator
Evaluate effectA long-acting
bronchodilator
(LABA or LAMA)
LAMA + LABA
Persistent
symptoms
LAMA +
LABA
Further
exacerbation(s)
LABA +
ICS
LAMA +
LABA
Consider
roflumilast if FEV1
<50% pred. and
patient has chronic
bronchitis
Further
exacerbation(s)
Consider
macrolide (in
former smokers)
LAM
ALABA
+ ICS
LAMA +
LABA + ICS
Further
exacerbation(s)
Persistent
symptoms/further
exacerbations
LAMA
2016 2018
Preferred
treatment
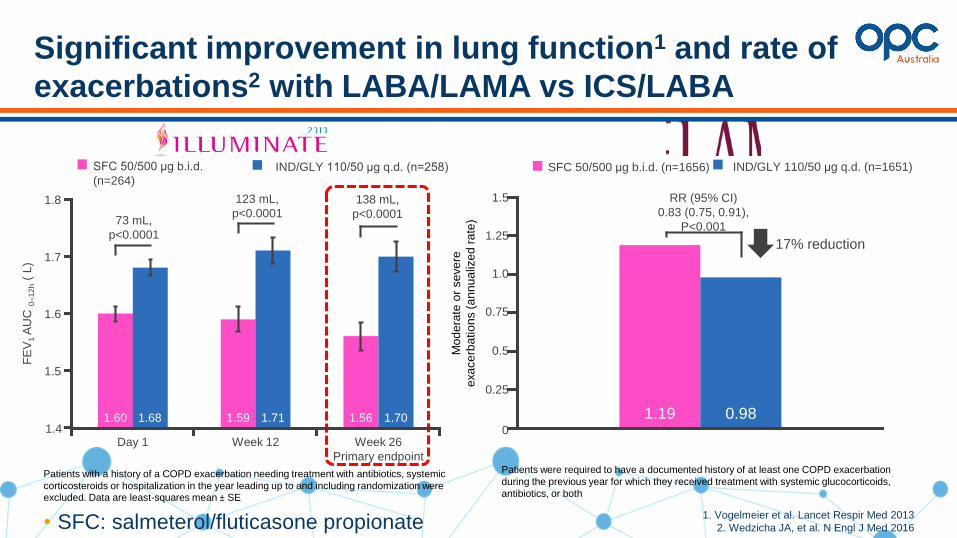
Significant improvement in lung function1 and rate of
exacerbations2 with LABA/LAMA vs ICS/LABA
• SFC: salmeterol/fluticasone propionate1. Vogelmeier et al. Lancet Respir Med 2013
2. Wedzicha JA, et al. N Engl J Med 2016
73 mL,
p<0.0001
123 mL,
p<0.0001 138 mL,
p<0.0001
1.60 1.59 1.561.68 1.71 1.70
FE
V1
AU
C 0
–1
2h
( L
)
Day 1 Week 12 Week 26
Primary endpoint
1.7
1.6
1.5
1.4
1.8
1.60 1.68 1.59 1.71 1.56 1.70
SFC 50/500 μg b.i.d.
(n=264)IND/GLY 110/50 μg q.d. (n=258)
Patients with a history of a COPD exacerbation needing treatment with antibiotics, systemic
corticosteroids or hospitalization in the year leading up to and including randomization were excluded. Data are least-squares mean ± SE
1.19 0.98
RR (95% CI)
0.83 (0.75, 0.91),
P<0.001
IND/GLY 110/50 μg q.d. (n=1651)SFC 50/500 μg b.i.d. (n=1656)
17% reduction
1.5
Mo
de
rate
or
se
ve
re
exa
ce
rba
tio
ns (
an
nu
aliz
ed
ra
te)
0.75
1.0
1.25
0.5
0.25
0
Patients were required to have a documented history of at least one COPD exacerbation
during the previous year for which they received treatment with systemic glucocorticoids,
antibiotics, or both
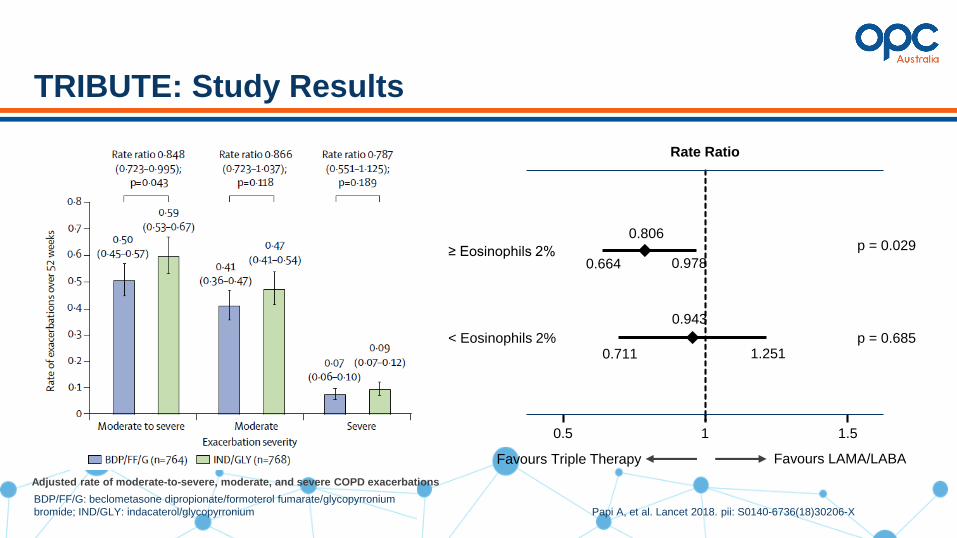
BDP/FF/G: beclometasone dipropionate/formoterol fumarate/glycopyrronium
bromide; IND/GLY: indacaterol/glycopyrronium Papi A, et al. Lancet 2018. pii: S0140-6736(18)30206-X
TRIBUTE: Study Results
Favours Triple Therapy Favours LAMA/LABA
≥ Eosinophils 2%
0.5 1 1.5
Rate Ratio
< Eosinophils 2%
0.664 0.978
0.806
0.711 1.251
0.943
p = 0.685
p = 0.029
Adjusted rate of moderate-to-severe, moderate, and severe COPD exacerbations
Lipson DA, et al. N Engl J Med 2018
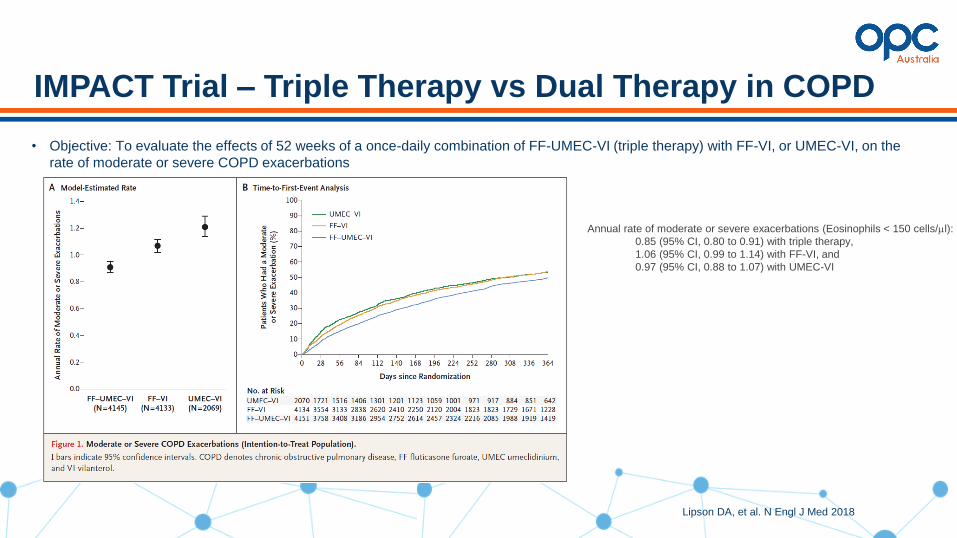
IMPACT Trial – Triple Therapy vs Dual Therapy in COPD
• Objective: To evaluate the effects of 52 weeks of a once-daily combination of FF-UMEC-VI (triple therapy) with FF-VI, or UMEC-VI, on the
rate of moderate or severe COPD exacerbations
Annual rate of moderate or severe exacerbations (Eosinophils < 150 cells/ml):
0.85 (95% CI, 0.80 to 0.91) with triple therapy,
1.06 (95% CI, 0.99 to 1.14) with FF-VI, and
0.97 (95% CI, 0.88 to 1.07) with UMEC-VI
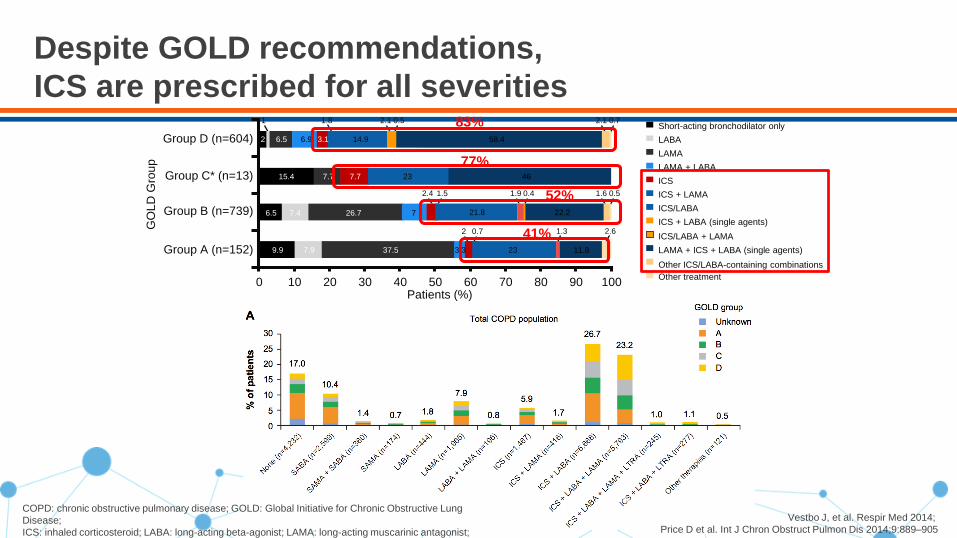
Despite GOLD recommendations,
ICS are prescribed for all severities
Patients (%)0 10 20 30 40 50 60 70 80 90 100
Group C* (n=13) 46237.77.715.4
Group D (n=604)
2.1 0.72.11.81 0.5
58.414.93.16.96.52
Group B (n=739)
Group A (n=152)
1.6 0.5
2 0.7 2.61.3
1.9 0.42.4 1.5
6.5 7.4 26.7 7
11.8
22.221.8
233.337.57.99.9
GO
LD
Gro
up
52%
41%
77%
83% Short-acting bronchodilator only
LABA
LAMA
LAMA + LABA
ICS
ICS + LAMA
ICS/LABA
ICS + LABA (single agents)
Other ICS/LABA-containing combinations
ICS/LABA + LAMA
LAMA + ICS + LABA (single agents)
Other treatment
Vestbo J, et al. Respir Med 2014;
Price D et al. Int J Chron Obstruct Pulmon Dis 2014;9:889–905
COPD: chronic obstructive pulmonary disease; GOLD: Global Initiative for Chronic Obstructive Lung
Disease;
ICS: inhaled corticosteroid; LABA: long-acting beta-agonist; LAMA: long-acting muscarinic antagonist;
LTRA: leukotriene receptor antagonist; SABA: short-acting beta-agonist; SAMA: short acting muscarinic
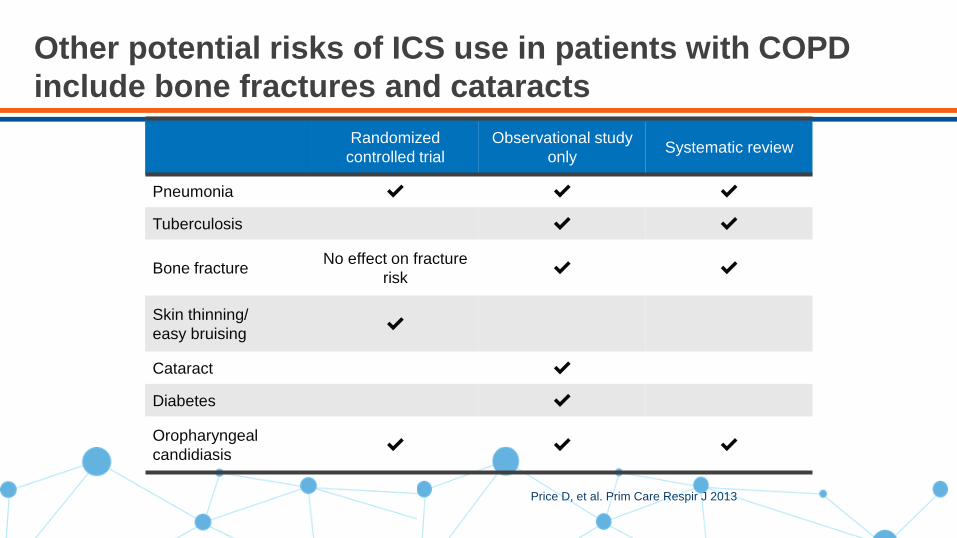
Other potential risks of ICS use in patients with COPD
include bone fractures and cataracts
Price D, et al. Prim Care Respir J 2013
Randomized
controlled trial
Observational study
onlySystematic review
Pneumonia ✔ ✔ ✔
Tuberculosis ✔ ✔
Bone fractureNo effect on fracture
risk✔ ✔
Skin thinning/
easy bruising✔
Cataract ✔
Diabetes ✔
Oropharyngeal
candidiasis✔ ✔ ✔

ICS* Dose in COPD and Onset of Diabetes/Osteoporosis
HR for ICS* vs. non-ICS, diabetes onset, stratified by GOLD
groups
Effect sizes of the different dosing strata
Study design: Historical matched cohort study utilising primary care medical record data from CPRD and OPCRD.
Inclusion criteria: Clinician-diagnosed COPD; Age ≥ 40 years;
ICS* cohort: ≥ 2 ICS* prescriptions per year; Non-ICS cohort: ≥ 2 LABA, LAMA and/or LAMA/LABA prescriptions per year
CPRD: ICS*, n=10395; LAMA/LABA, n=3543
OPCRD: ICS*, n=14,983; LAMA/LABA, n=5,013
CPRD: ICS*, n=11098; LAMA/LABA, n=3928
OPCRD: ICS*, n=15722; LAMA/LABA, n=5406
* *
Voorham J, Price D et al. Unpublished Data

• 1 year, multinational, randomised, double-blind, parallel-group and active-controlled study
• 6-week run-in period on triple therapy (tiotropium 18mcg OD, salmeterol 50mcg BID, fluticasone 500mcg BID)
• 1:1 allocation into double blind phase that contains active control and stepwise step-down from 500 mcg fluticasone to
250mcg, 100mcg and placebo - Stepwise reduction was done at every 6 weeks
Magnussen H, et al. Respir Med 2014;108(4):593-9
WISDOM: Study Design
Sc
ree
nin
g Triple
TherapyTio - 18µg QD
Sal - 50µg BD
Flu - 500µg BD
Week
Visit
-7
1
-6
2
Ra
nd
om
iza
tio
n (
1:1
)
0
3
6
4
12
5
18
6
52
13
Run-in
ICS (remained in triple therapy from run-in)
Stepwise ICS withdrawal (remained on standard dose of
tiotropium and Salmeterol )
250µg BD 100µg BD 0µg BD (placebo) Stable Treatment500µg BD
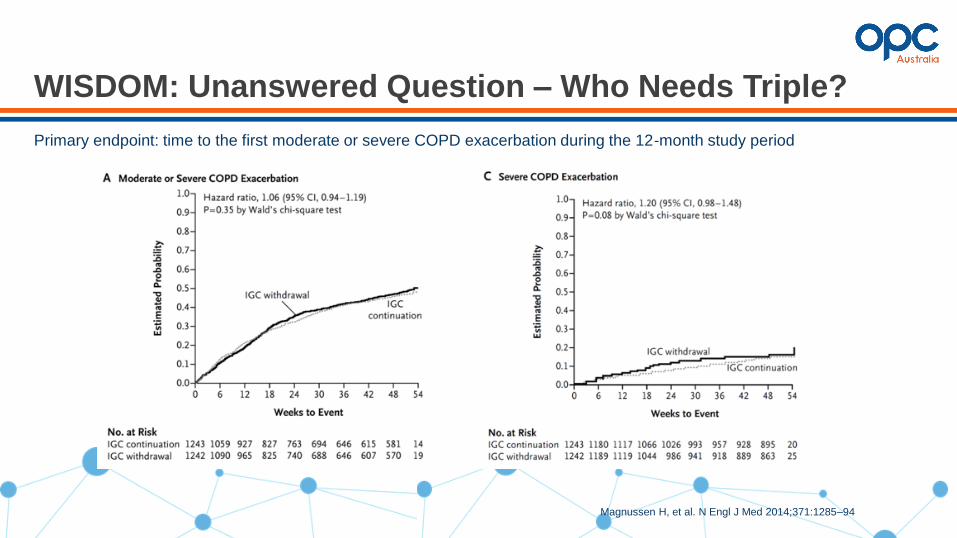
Primary endpoint: time to the first moderate or severe COPD exacerbation during the 12-month study period
Magnussen H, et al. N Engl J Med 2014;371:1285–94
WISDOM: Unanswered Question – Who Needs Triple?
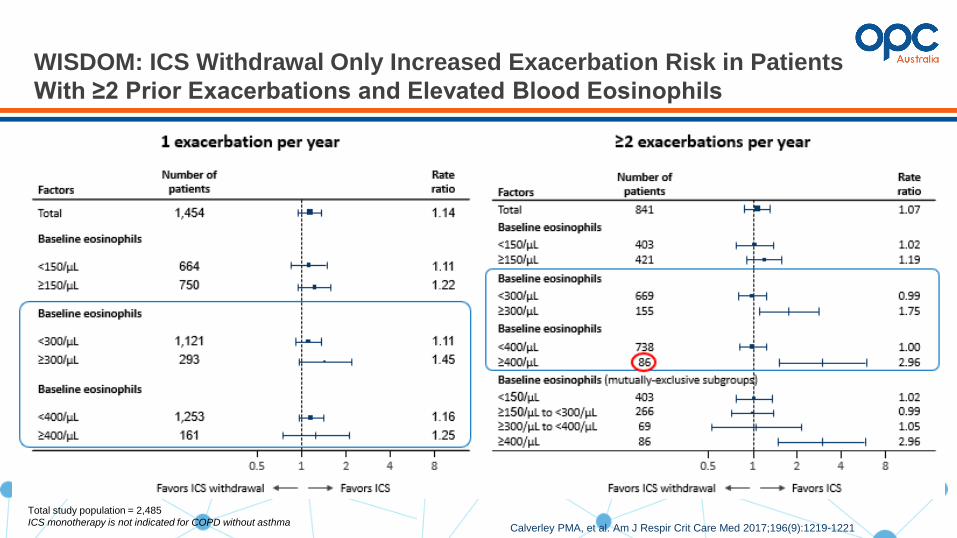
Calverley PMA, et al. Am J Respir Crit Care Med 2017;196(9):1219-1221
WISDOM: ICS Withdrawal Only Increased Exacerbation Risk in Patients
With ≥2 Prior Exacerbations and Elevated Blood Eosinophils
Total study population = 2,485
ICS monotherapy is not indicated for COPD without asthma
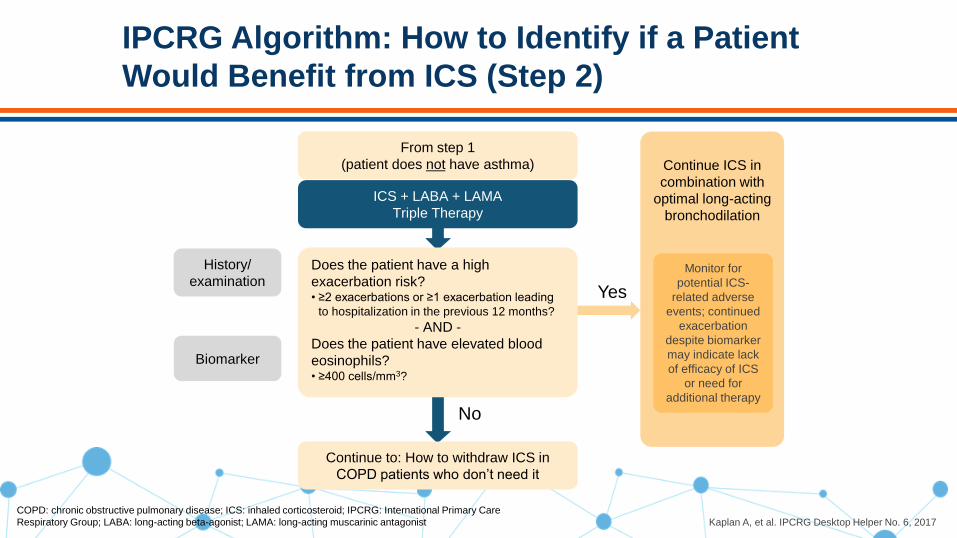
IPCRG Algorithm: How to Identify if a Patient
Would Benefit from ICS (Step 2)
Kaplan A, et al. IPCRG Desktop Helper No. 6, 2017
ICS + LABA + LAMA
Triple Therapy
Does the patient have a high
exacerbation risk?• ≥2 exacerbations or ≥1 exacerbation leading
to hospitalization in the previous 12 months?
- AND -
Does the patient have elevated blood
eosinophils?• ≥400 cells/mm3?
Continue ICS in
combination with
optimal long-acting
bronchodilation
Yes
No
From step 1
(patient does not have asthma)
History/
examination
Continue to: How to withdraw ICS in
COPD patients who don’t need it
Biomarker
Monitor for
potential ICS-
related adverse
events; continued
exacerbation
despite biomarker
may indicate lack
of efficacy of ICS
or need for
additional therapy
COPD: chronic obstructive pulmonary disease; ICS: inhaled corticosteroid; IPCRG: International Primary Care
Respiratory Group; LABA: long-acting beta-agonist; LAMA: long-acting muscarinic antagonist

IPCRG Algorithm: How to Identify if a Patient
Would Benefit from ICS (Step 1)
ICS + LABAICS + LABA +
LAMA
(Triple Therapy)
Does the patient have asthma?• Documented history of asthma, with or without
atopy, diagnosed before the age of 40 years,
or family history of asthma?
• A large degree of reversibility of airflow
limitation (>15% and 400 mL in post-
bronchodilator FEV1)?
Continue ICS in
combination with
optimal long-acting
bronchodilation
Monitor for
potential ICS-
related adverse
events; continued
exacerbation
despite biomarker
may indicate lack
of efficacy of ICS
or need for
additional therapy
Yes
No No
Continue to:
Step 2
Treatment at
assessment
consultation
History/
examination
Continue to:
How to withdraw
ICS in COPD
patients who
don’t need it
Kaplan A, et al. IPCRG Desktop Helper No. 6, 2017
COPD: chronic obstructive pulmonary disease; FEV1: forced expiratory volume in one second; ICS: inhaled
corticosteroid;
IPCRG: International Primary Care Respiratory Group; LABA: long-acting beta-agonist; LAMA: long-acting muscarinic
antagonist

Review of delegate pre-disposing activity
Psychological factors in COPD
Presenter: Dr Kerry Hancock
Rationale
• The 2017 GOLD report proposed a revised assessment scheme for patients with COPD.
• We examined the prevalence of common comorbidities in patients with an established diagnosis and those started on maintenance therapy for the first time by GOLD group.
83Halpin DMG, Price D, et al. Unpublished data
Methods
• Study population:− 6940 patients with a recorded diagnosis of COPD on 1/1/2014 in the Optimum
Patient Care Research Database (ALL), and− 876 patients newly initiated on maintenance therapy (NMT) in 2014 with a two
year follow-up were studied.
• Both cohorts had data on comorbidities, the number of exacerbations in the previous 12 months, and mMRC & FEV1 in the year 2014.
84Halpin DMG, Price D, et al. Unpublished data
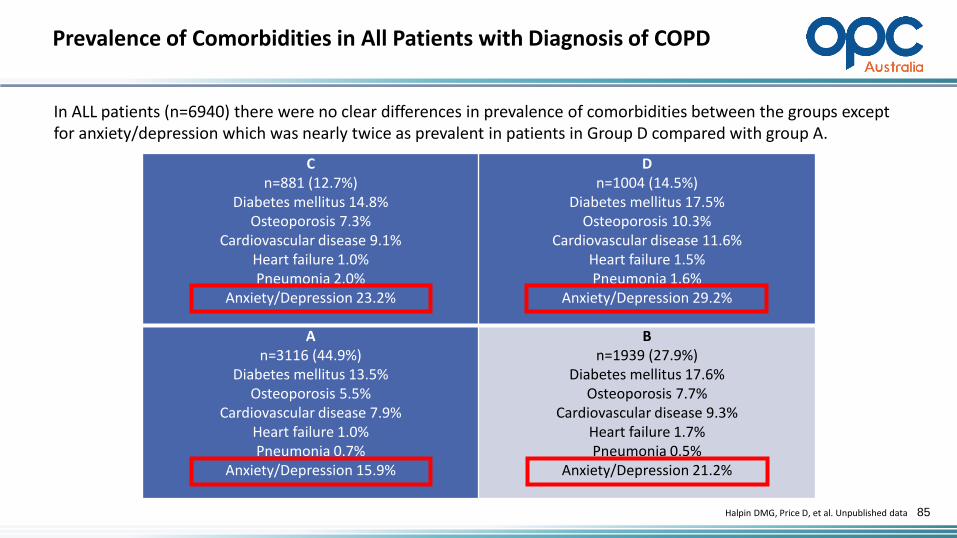
Prevalence of Comorbidities in All Patients with Diagnosis of COPD
85
Cn=881 (12.7%)
Diabetes mellitus 14.8%Osteoporosis 7.3%
Cardiovascular disease 9.1%Heart failure 1.0%Pneumonia 2.0%
Anxiety/Depression 23.2%
Dn=1004 (14.5%)
Diabetes mellitus 17.5%Osteoporosis 10.3%
Cardiovascular disease 11.6%Heart failure 1.5%Pneumonia 1.6%
Anxiety/Depression 29.2%
An=3116 (44.9%)
Diabetes mellitus 13.5%Osteoporosis 5.5%
Cardiovascular disease 7.9%Heart failure 1.0%Pneumonia 0.7%
Anxiety/Depression 15.9%
Bn=1939 (27.9%)
Diabetes mellitus 17.6%Osteoporosis 7.7%
Cardiovascular disease 9.3%Heart failure 1.7%Pneumonia 0.5%
Anxiety/Depression 21.2%
Halpin DMG, Price D, et al. Unpublished data
In ALL patients (n=6940) there were no clear differences in prevalence of comorbidities between the groups except for anxiety/depression which was nearly twice as prevalent in patients in Group D compared with group A.

Prevalence of Comorbidities in Patients with Diagnosis of COPD Initiating Maintenance Therapy
86Halpin DMG, Price D, et al. Unpublished data
In NMT patients (n=876) there were also no clear differences in prevalence of comorbidities between the groups except for osteoporosis which was more common in patients in groups B & D.
Cn=120 (13.7%)
Diabetes mellitus 12.5%Osteoporosis 4.2%
Cardiovascular disease 11.7%Heart failure 2.5%Pneumonia 1.7%
Anxiety/Depression 29.2%
Dn=79 (9.0%)
Diabetes mellitus 16.5%Osteoporosis 8.9%
Cardiovascular disease 7.6%Heart failure 2.5%Pneumonia 3.8%
Anxiety/Depression 24.1%
An=424 (48.4%)
Diabetes mellitus 13.2%Osteoporosis 2.8%
Cardiovascular disease 6.6%Heart failure 0.5%Pneumonia 0.5%
Anxiety/Depression 16.5%
Bn=253 (28.9%)
Diabetes mellitus 17.0%Osteoporosis 6.3%
Cardiovascular disease 10.3%Heart failure 2.4%Pneumonia 1.6%
Anxiety/Depression 19.8%

Conclusion
• Comorbidities are common in people with COPD and many are already present at the time maintenance therapy is initiated.
87Halpin DMG, Price D, et al. Unpublished data

Contact Our Team
88
www.optimumpatientcare.org/australia
@optimumpatientcareaustralia
@OPCare
https://www.linkedin.com/company/
optimum-patient-care


• One that provides information not already available from the clinical assessment
• Aids in clinical decision making
• Has a short turnaround time
• Is inexpensive
What is a good bio-marker?

What is BNP and NT-proBNP
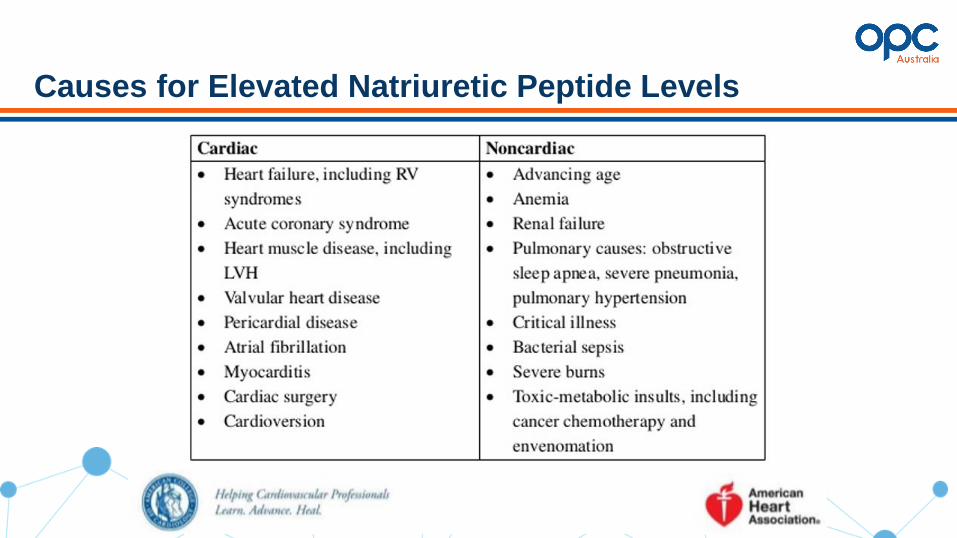
Causes for Elevated Natriuretic Peptide Levels
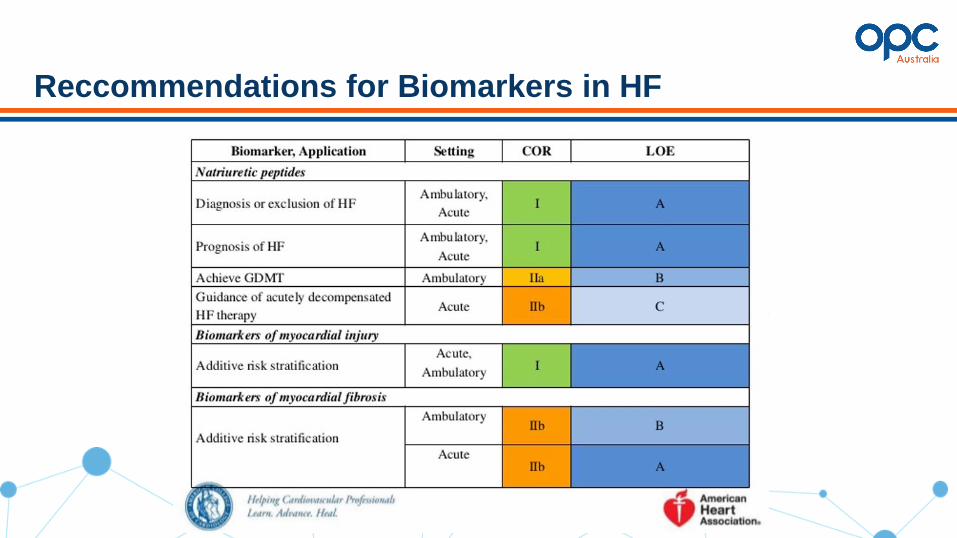
Reccommendations for Biomarkers in HF

BNP Consensus Algorithm
Medicare Reimbursement of BNP testing in Australia
Latest recommendations from Cardiac Society of Australia and New Zealand ( CSANZ ) state that GPs should consider BNP testing in the following scenarios:
• to diagnose, rule out or to differentiate heart failure from other potential clinical conditions in a patient presenting with dyspnoea , and access to an echo is unavailable or delayed.
BNP testing is however not reimbursed in primary care settings and out of pocket cost should be discussed with the patient.
Dr Garry Jennings, Chief Medical Advisor, National Heart Foundation

Workshops

Who really has COPD? Spirometry Interpretation for GPs (in 25 minutes!)
Dr Kerry Hancock
Professor Peter Frith April 28th 2018, Melbourne
Declarations - Dr Kerry Hancock
• Pharmaceutical companies who undertake research , develop and / or market medicines prescribed to patients with COPD
• Advisory Board fees, Leadership Forum attendances, presentation fees
• Spirometry Learning Module
• LFA Executive National COPD Program Coordinating Committee

COPD is confirmed by the presence of persistent airflow limitation
(post-bd FEV1/FVC <0.7)
• pre and post-bronchodilator spirometry
• use proper technique
• post-bd FEV1/FVC ratio <0.7 and FEV1 <80% predicted
• airflow limitation that isn’t fully reversible
• interpret borderline spirometry results with caution
• particularly in older (>65yr) and younger patients (<45yr)
• those without a history of smoking or exposure to occupational/environmental pollutants or dust
• if borderline spirometry, consider alternative diagnoses and investigate appropriately

COPD: Under - diagnosis and Mis - diagnosis
• Under-diagnosis is high (50%)
• Misclassification COPD
• Tas 31% in 31 practices (Walters 2011)
• 18% normal
• NSW 42% in 44 practices (Zwar 2011)
• 20% normal
• Vic 37% in 41 practices (Laing 2018 )
• 31% normal

Are we good at interpreting spirometry?
• Sydney 36 practices (Zwar 2016) • case finding
• 10,234 patients invited, 1641 spiro tests
• PNs trained in spirometry + mentoring/feedback
→ 75% traces met quality standards
• decision support via interpretive tool kit
• GPs on-line training COPD guidelines
• 287 “new cases COPD” / 1641 spiro tests (18%)
• 78 (27%) did NOT have FEV1/FVC < 0.7
Early intervention for chronic obstructive pulmonary disease by practice nurse and GP teams: a cluster randomized trial (PELICAN study)Nicholas A Zwar,et al. Family Practice, Volume 33, Issue 6, 1 December 2016, pp 663–670
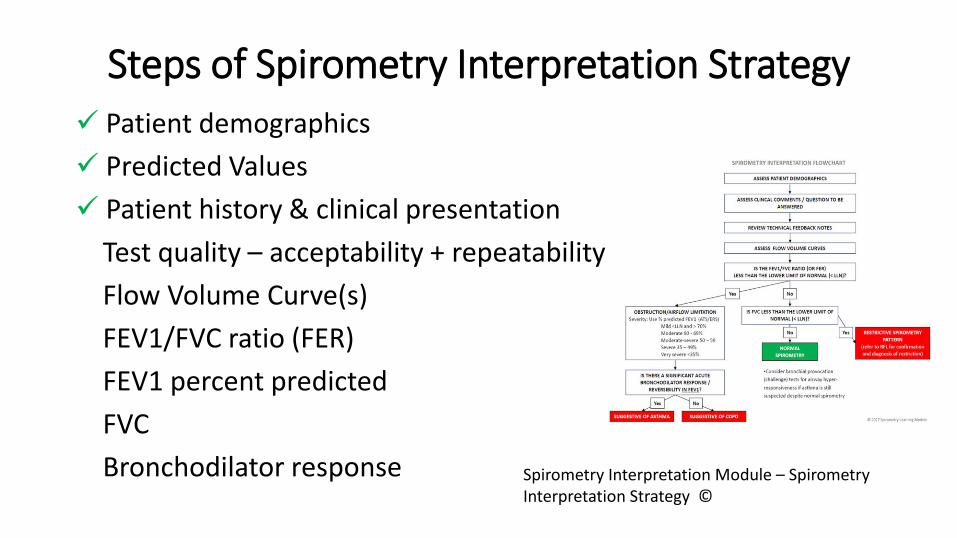
Steps of Spirometry Interpretation Strategy✓ Patient demographics
✓ Predicted Values
✓ Patient history & clinical presentation
Test quality – acceptability + repeatability
Flow Volume Curve(s)
FEV1/FVC ratio (FER)
FEV1 percent predicted
FVC
Bronchodilator response Spirometry Interpretation Module – Spirometry Interpretation Strategy ©
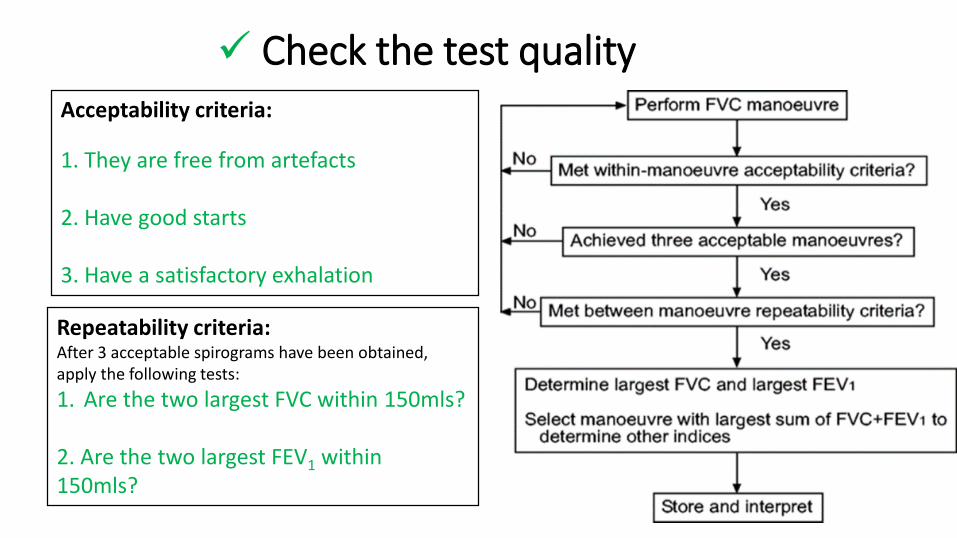
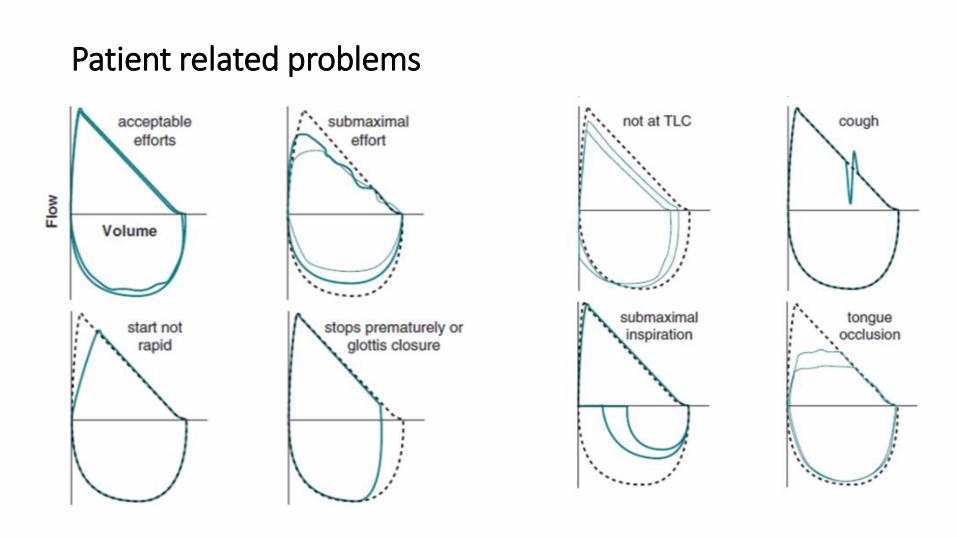
✓ Check the test qualityAcceptability criteria:
1. They are free from artefacts
2. Have good starts
3. Have a satisfactory exhalation
Repeatability criteria:After 3 acceptable spirograms have been obtained, apply the following tests:
1. Are the two largest FVC within 150mls?
2. Are the two largest FEV1 within 150mls?
ADVOCACY | AWARENESS | EDUCATION | SUPPORT | RESEARCH
Patient related problems
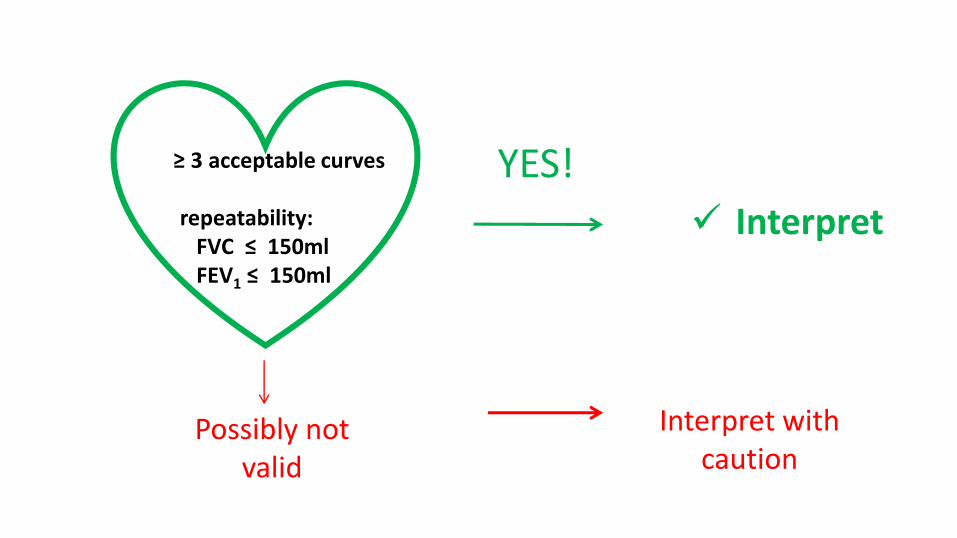
≥ 3 acceptable curves
repeatability:FVC ≤ 150ml FEV1 ≤ 150ml
Possibly not valid
YES!
Interpret with caution
✓ Interpret
Flo
w
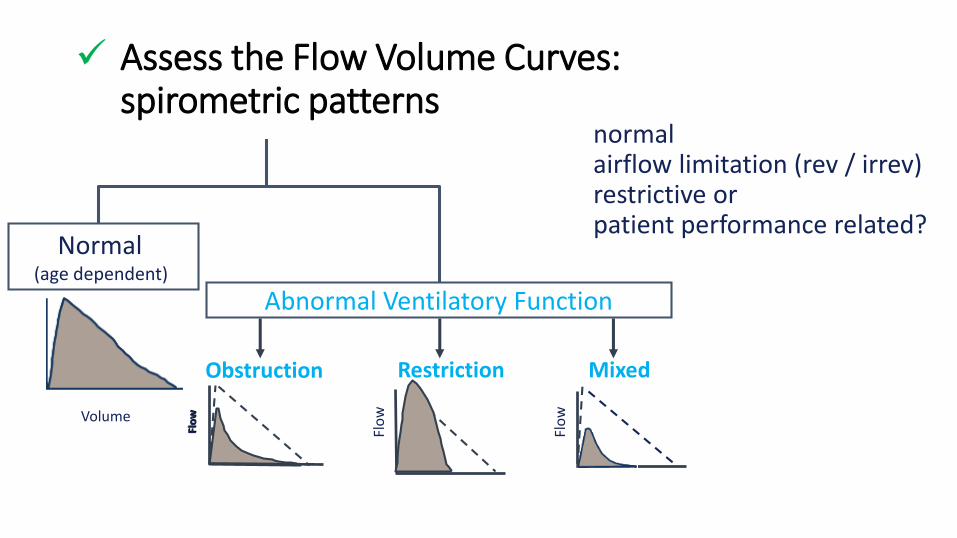
RestrictionObstruction Mixed
Abnormal Ventilatory Function
Normal (age dependent)
Volume
Flo
w
Flo
w
normalairflow limitation (rev / irrev) restrictive or patient performance related?
✓ Assess the Flow Volume Curves: spirometric patterns
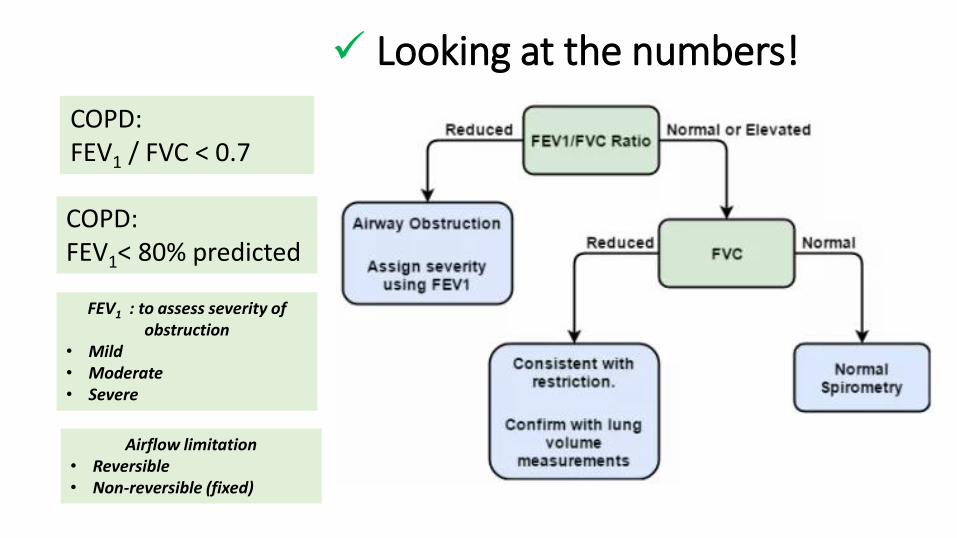
FEV1 : to assess severity of obstruction
• Mild • Moderate • Severe
RESTRICTION
OBSTRUCTION
Airflow limitation • Reversible• Non-reversible (fixed)
COPD: FEV1 / FVC < 0.7
COPD: FEV1< 80% predicted
✓ Looking at the numbers!
✓ Is FVC reduced ?Is there a restrictive pattern?
• consider suboptimal patient performance
• early test termination
• failure to inspire completely
• if ‘true’ restrictive pattern (i.e. 3 acceptable and repeatable trials) refer to accredited laboratory for confirmation by measurement of total lung capacity
• is there a mixed obstructive/restrictive pattern ?
• ratio and FVC < LLN
• early airway closure may mirror a restrictive pattern
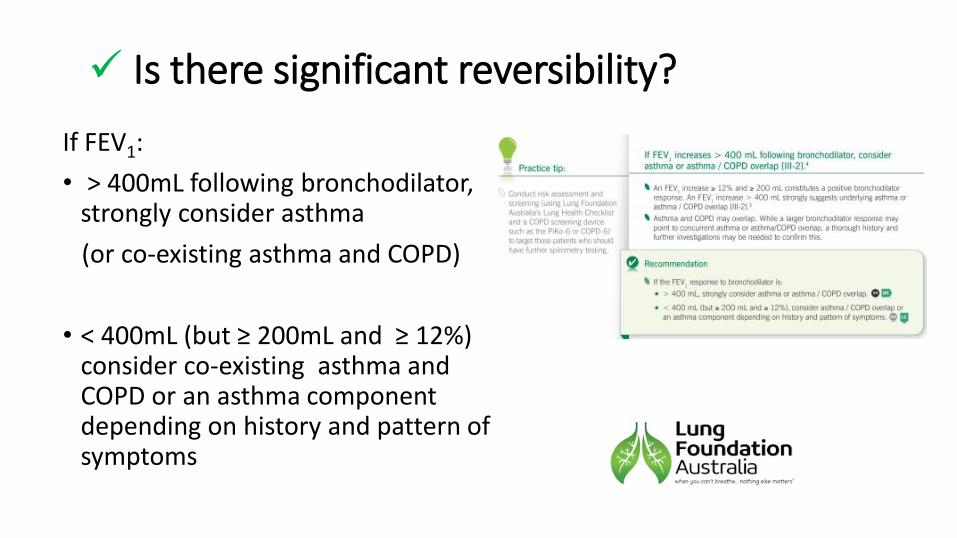
✓ Is there significant reversibility?
If FEV1:
• > 400mL following bronchodilator, strongly consider asthma
(or co-existing asthma and COPD)
• < 400mL (but ≥ 200mL and ≥ 12%) consider co-existing asthma and COPD or an asthma component depending on history and pattern of symptoms
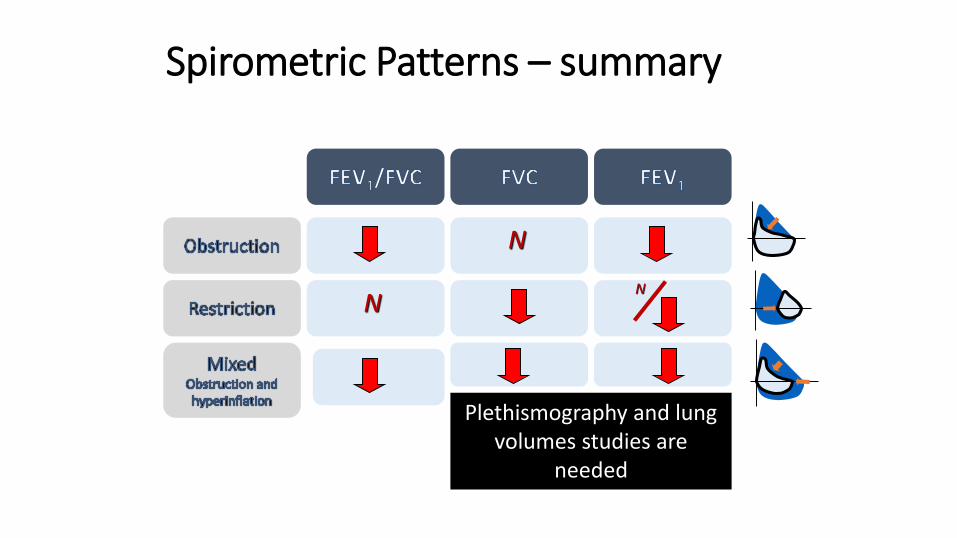
N
Plethismography and lung volumes studies are
needed
NN
Spirometric Patterns – summary

Spirometry Training Courses
• National Asthma Council
• Asthma Australia
• The Lung Health Promotion Centre (Alfred) https://www.lunghealth.org/
• Queensland Health
• Indigenous Respiratory Outreach Care (IROC) Program
• Spirometry Training Professionals
• A list of registered training organisations offering spirometry can be found on the Australian Government Department of Education and Training website.

Resources for Performance and Interpretation of Spirometry
ATS / ERS Guidelines:
Pellegrino R, Viegi G, Brusasco V, et al Interpretive strategies for lung function tests. Eur Respir J. 2005;26(5):948-968..
Miller MR, et al. Standardisation of spirometry. Eur Respir J 2005: 26(2): 319-338
Australian Resources:
Johns DP , Burton D, and Swanney MP. Spirometer Users’ and Buyers Guide; Melbourne: National Asthma Council Australia, 2013. Revised 2015
https://www.nationalasthma.org.au/living-with-asthma/how-to-videos/performing-spirometry-in-primary-care
https://www.nationalasthma.org.au/living-with-asthma/resources/health-professionals/information-paper/spirometry-quick-reference-guide
Johns DP and Pierce R. Pocket Guide to Spirometry, 3rd edition. Sydney: McGraw-Hill Australia, 2011 ISBN 9780071716193
Abramson M, et. al. COPD-X Concise Guide for Primary Care. Brisbane. Lung Foundation Australia. 2014

In pairs …..
- consider the following case study - assess and interpret the two spirometry tests using the spirometry assessment tool

Mr DD
• 62 yo male truck driver
• T2DM
• IHD/ CABVG
• Childhood pneumonia & “bronchitis”
• Current smoker – approx 50PY
• Recent increase in cough
• CXR – “mild hyperinflation”, no sinister abnormalities
• Spirometry 2010 and 2015



Group activity: Case Studies
Case Study 2
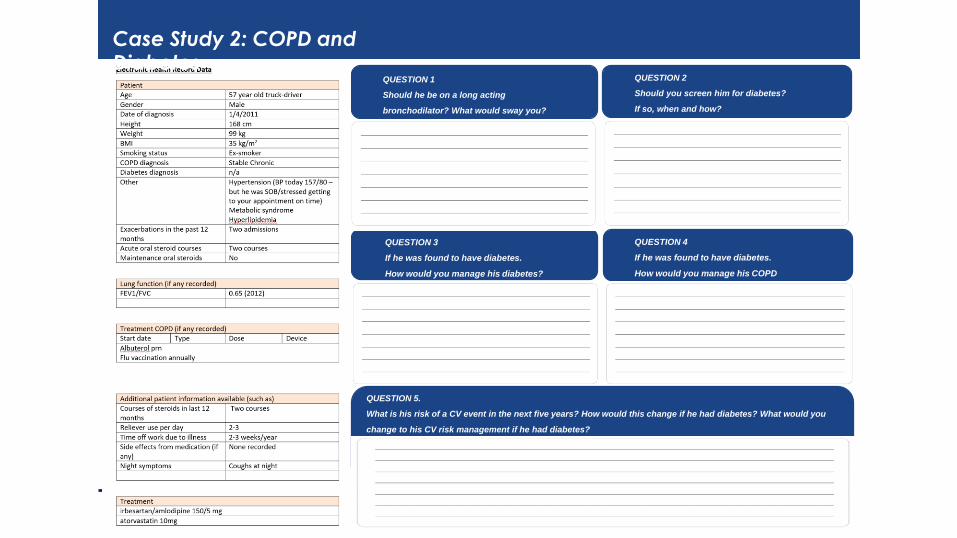
QUESTION 3
If he was found to have diabetes.
How would you manage his diabetes?
QUESTION 1
Case Study 2: COPD and Diabetes
QUESTION 1
Should he be on a long acting
bronchodilator? What would sway you?
QUESTION 3
If he was found to have diabetes, how
would you treat his diabetes?
QUESTION 2
Should you screen him for diabetes?
If so, when and how?
QUESTION 4
If he was found to have diabetes.
How would you manage his COPD
differently?
QUESTION 5.
What is his risk of a CV event in the next five years? How would this change if he had diabetes? What would you
change to his CV risk management if he had diabetes?

Case Study 1: COPD HF
QUESTION 2
What would you do?
• Short term
• Long term
QUESTION 1
What are your considerations?
What do you do in terms of investigations?
QUESTION 3
What would you amend in terms of treatment?
QUESTION 4
What are your review plans and what would trigger
you to refer the patient?
Anne presents for scripts and says ‘feeling fine but have shortened my daily walk with the dog’

Thank you
Related Documents











