Page 1 of 100 ECTOR COUNTY INDEPENDENT SCHOOL DISTRICT REQUEST FOR PROPOSAL; PROPOSAL INSTRUCTIONS; GENERAL CONDITIONS AND SPECIFICATIONS/REQUIREMENTS FOR: PHARMACY BENEFIT MANAGER FOR RETAIL, AND MAIL ORDER SERVICES, ON SITE/NEAR SITE CLINIC MANAGEMENT SERVICES, EMPLOYEE ASSISTANCE PROGRAMS, TELE-MEDICINE PROVIDER EMPLOYEE BENEFIT ADMINISTRATION RFP #20-07 PROPOSAL DEADLINE: April 20th, 2020 2:00 PM CDST

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

PPaaggee 11 ooff 110000
ECTOR COUNTY
INDEPENDENT
SCHOOL DISTRICT
REQUEST FOR PROPOSAL; PROPOSAL INSTRUCTIONS;
GENERAL CONDITIONS AND
SPECIFICATIONS/REQUIREMENTS FOR:
PHARMACY BENEFIT MANAGER FOR RETAIL, AND MAIL ORDER SERVICES,
ON SITE/NEAR SITE CLINIC MANAGEMENT SERVICES, EMPLOYEE ASSISTANCE PROGRAMS,
TELE-MEDICINE PROVIDER
EEMMPPLLOOYYEEEE BBEENNEEFFIITT AADDMMIINNIISSTTRRAATTIIOONN RFP #20-07
PROPOSAL DEADLINE:
April 20th, 2020
22::0000 PPMM CCDDSSTT

PPaaggee 22 ooff 110000
PROPOSAL REQUIREMENTS Proposers must complete all forms and fill in all information asked for in the blanks provided under each item. Failure to comply may result in rejection of the proposal at ECTOR COUNTY ISD (the District)’s option. The total for each proposal submitted must include any applicable taxes. Although the District is exempt from most City, State and Federal taxes, this is not true in all cases. It is suggested that taxes, if any, be separately identified, itemized and stated on each proposal. The District cannot determine for the proposer whether the proposal is taxable to the District. The proposer, through the proposer’s attorney or tax consultant, must make such determination. Bills submitted for taxes after the proposals are awarded will not be honored. Proposals deposited with the District cannot be withdrawn before the time set for Proposal Deadline. Request for non-consideration of proposals must be made in writing to the Purchasing Officer and received by the District before the time set for pending proposals. After other proposals are opened, the proposal for which non-consideration is requested may be returned unopened. The proposal may not be withdrawn after the proposals have been received, and the proposer, in submitting the same, warrants and guarantees that this proposal has been carefully reviewed and checked and that it is in all things true and accurate and free of mistakes and that such proposal will not and cannot be withdrawn because of any mistake or mistaken assumption of fact committed by the Proposer. Proposals will not be publicly opened. Proposals will be tabulated for comparison based on the proposal prices and guaranties shown in the proposal. Until final award of the Contract, the District reserves the right to reject any or all proposals, to waive technicalities, to request new proposals, or proceed to do the work otherwise in the best interest of the District. Proposals will be considered irregular if they show any omissions, alteration of form, additions or conditions not called for, unauthorized alternate proposals or irregularities of any kind. However, the District reserves the right to waive any irregularities and to make the award in the best interest of the District. The District reserves the right to reject any or all proposals in whole or in part, to waive any informality in any proposal, to declare inadequate or inappropriate any proposer failing to meet the specifications, and to accept the proposal which, in its discretion, is in the best interest of the District, and all proposals submitted are subject to this reservation. Proposals may be rejected, among other reasons, for any of the following specific reasons:
1. Proposals received after the time limit for receiving proposals as stated in the advertisement;
2. Proposal containing any irregularities;
3. Unbalanced value of any items; and/or

PPaaggee 33 ooff 110000
4. Failure to comply with the enclosed contract language.
Proposers may be disqualified, and their proposals not considered, among other reasons, for any of the following specific reasons:
1. Reason for believing collusion exists among the proposers;
2. Reasonable grounds for believing that any proposer is interested in more than one proposal for the work contemplated;
3. The proposer being interested in any litigation against the District;
4. The proposer being in arrears on any existing contract or having defaulted on a previous contract;
5. Lack of competency as revealed by a financial statement, experience and equipment, questionnaires, etc.;
6. Uncompleted work that, in the judgment of the District, will prevent or hinder the prompt completion of additional work if awarded; and/or
7. Failure to comply with the enclosed contract language.
The successful proposal/proposer may not assign his rights and duties under the award without the written consent of the District’s Director of Purchasing. Such consent shall not relieve the assignor of liability in event of default by his assignee. Proposals will be received only at the following address: BY E-MAIL BY E-MAIL Albert Valencia Eric Smith Director of Purchasing Managing Partner ECISD Purchasing Department Smith & Associates Consulting 802 N Sam Houston P.O. Box 92398 Odessa, TX 79761 Southlake, TX 76092 [email protected] [email protected]
All proposals must be at the above address by April 20, 2020 at 2:00 p.m. CDST. All proposals received after the prescribed deadline, regardless of the mode of delivery, shall be returned unopened.
All proposers must include a financial statement audited by an independent third party.

PPaaggee 44 ooff 110000
All proposers must clearly mark cost proposal sections and place them at the front of the proposal. If you have any technical questions about the specifications, please put all questions in writing to the attention of Eric Smith via e-mail at [email protected].
PPaaggee 55 ooff 110000
AFFIDAVIT STATE OF ________________) § COUNTY OF _____________)
__________________________________________, of lawful age, being first duly sworn, on
oath says, that she/he is the agent authorized by the proposal to submit the attached proposal.
Affiant further states that the proposal has not been a party to any collusion among
proposals/proposers in restraint of freedom of competition by agreement to proposal at a fixed
price or to refrain from proposing; or with any state official, ESC Employee, ESC Board Member
or Benefit consultant as to quantity, quality, or price in the prospective contract, or any other
terms of said prospective contract, or in any discussions or actions between
proposals/proposers and any state official, ESC employee, ESC Board Member, or Benefit
consultant concerning exchange of money or other things of value for special consideration in
the letting of this contract.
_______________________________________
(Signature) Subscribed and sworn to before me this ______ day of ______________________, 2020 _____________________________________________ (Notary Public)
State of _______________________________________
My Commission Expires:__________________________
Carrier/Administrator: ______________________________________________
Vendor: __________________________________________________________
PPaaggee 66 ooff 110000
STATEMENT OF COMPLIANCE
Please submit as a part of your proposal the following information:
RE: ECTOR COUNTY INDEPENDENT SCHOOL DISTRICT We hereby acknowledge receipt of Request for Proposal for Pharmacy Benefit Manager Retail/Mail Order, Employee Assistance Program, Tele-Medicine Provider, Near Site/On site Clinic Management Services, and certify that our proposal conforms to the RFP except as detailed below: ____________________________ ________________________________ Organization Signature ____________________________ ________________________________ Date Title

PPaaggee 77 ooff 110000
CONFLICT OF INTEREST
Effective January 1, 2006, Chapter 176 of the Texas Local Government Code requires that persons, or their agents, who seek to contract for the sale or purchase of property, goods, or services with the District, shall file a completed conflict of interest questionnaire with the District Secretary not later than the seventh (7th) business day after the date that the person: (1) begins contract discussions or negotiations with the District; or (2) submits to the District an application, response to a request for bid or proposal, correspondence, or another writing related to a potential agreement with the District. The Conflict of Interest questionnaire form is available below or from the Texas Ethics Commission at www.ethics.state.tx.us. Completed questionnaires may be mailed or delivered to the Office of the District Secretary. If mailing a completed questionnaire, mail to: Albert Valencia, 802 N Sam Houston, Odessa TX, 79761
SEE BELOW

PPaaggee 88 ooff 110000
CONFLICT OF INTEREST QUESTIONNAIRE For vendor or other person doing business with local governmental entity
FORM CIQ
This questionnaire reflects changes made to the law by H.B. 1491, 80th Leg., Regular
Session.
This questionnaire is being filed in accordance with Chapter 176, Local Government Code by a person who has a business relationship as defined by Section 176.001(1-a) with a local governmental entity and the person meets requirements under Section 176.006(a).
By law this questionnaire must be filed with the records administrator of the local governmental entity not later than the 7th business day after the date the person becomes aware of facts that require the statement to be filed. See Section 176.006, Local Government Code.
A person commits an offense if the person knowingly violates Section 176.006, Local Government Code. An offense under this section is a Class C misdemeanor.
OFFICE USE ONLY
Date Received
Name of person who has a business relationship with local governmental entity. 11
Check this box if you are filing an update to a previously filed questionnaire.
(The law requires that you file an updated completed questionnaire with the appropriate filing authority not
later than the 7th business day after the date the originally filed questionnaire becomes incomplete or inaccurate.)
22
Name of local government officer with whom filer has employment or business relationship.
Name of Officer
This section (item 3 including subparts A, B, C & D) must be completed for each officer with whom the filer has an employment or other business relationship as defined by Section 176.001(1-a), Local Government Code. Attach additional pages to this Form CIQ as necessary.
A. Is the local government officer named in this section receiving or likely to receive taxable income, other than investment income, from the filer of the questionnaire?
Yes No
B. Is the filer of the questionnaire receiving or likely to receive taxable income, other than investment income, from or at the direction of the local government officer named in this section AND the taxable income is not received from the local governmental entity?
Yes No
C. Is the filer of this questionnaire employed by a corporation or other business entity with respect to which the local government officer serves as an officer or director, or holds an ownership of 10 percent or more?
Yes No
D. Describe each employment or business relationship with the local government officer named in this section.
33
Signature of person doing business with the governmental entity Date
44
Adopted 06/29/2007

PPaaggee 99 ooff 110000
FELONY CONVICTION NOTICE Statutory citation covering notification of criminal history of contractor is found in the Texas Education Code Section 44.034. Following is an example of a felony conviction notice:
FELONY CONVICTION NOTICE
State of Texas Legislative Senate Bill No. 1, Section 44.034, Notification of Criminal History, Subsection (a), states “a person or business entity that enters into a contract with a public entity must give advance notice to the public entity if the person or an owner or operator of the business entity has been convicted of a felony. The notice must include a general description of the conduct resulting in the conviction of a felony.” Subsection (b) states “a public entity may terminate a contract with a person or business entity if the public entity determines that the person or business entity failed to give notice as required by Subsection (a) or misrepresented the conduct resulting in the conviction. The public entity must compensate the person or business entity for services performed before the termination of the contract.”
THIS NOTICE IS NOT REQUIRED OF A PUBLICLY-HELD CORPORATION
I, the undersigned agent for the firm named below, certify that the information concerning notification of felony convictions has been reviewed by me and the following information furnished is true to the best of my knowledge. VENDOR’S NAME: AUTHORIZED COMPANY OFFICIAL’S NAME (PRINTED): A. My firm is a publicly held corporation; therefore, this reporting requirement is not
applicable. Signature of Company Official: B. My firm is not owned nor operated by anyone who has been convicted of a felony: Signature of Company Official: C. My firm is owned or operated by the following individual(s) who has/have been
convicted of a felony: Name of Felon(s):
Detail of Conviction(s):
Signature of Company Official:

PPaaggee 1100 ooff 110000
RECOMMENDED TIMETABLE
for
Ector County Independent School District
PROPOSAL SPECIFICATIONS
Mail Specifications March 22nd, 2020 Deadline for Proposals April 20th, 2020
2:00 pm CDST
Proposal Analysis April 21st, 2020 through
April 24th, 2020
Tentative Interviews April 27th- May 1st, 2020
Board Approval May 2020
Effective Date January 1st 2021

PPaaggee 1111 ooff 110000
TABLE OF CONTENTS
Section A Background Information Section B General Carrier Requirements Section C Pharmacy Benefit Manager Retail/Mail Order Section D On Site/Near Site Clinic
Management Services Section E Employee Assistance Program Section F Tele-Medicine Provider
Section G Claims Experience

PPaaggee 1122 ooff 110000
SECTION A
BACKGROUND INFORMATION

PPaaggee 1133 ooff 110000
SECTION A: BACKGROUND INFORMATION
Ector County Independent School District has a self-insured Medical Benefit Plan administrated by Blue Cross Blue Shield. Embedded in the District’s offering from Blue Cross Blue Shield is a tele-medicine benefit offered by Web MD. The District currently offers three medical plans; two of the plans are standard deductible/co-insurance type plans and one is an HSA Plan. The prescription drugs are administered by ESI. As of September 30, 2019, there were 2281 employees enrolled on the plan with the $1300 deductible, there were 388 on the plan with the $1900 deductible, and there were 294 employees enrolled in the HSA Plan. The District also offers a Hospital Indemnity plan for those employees who do not enroll in a medical plan with 688 employees enrolled. The District Employee Assistance provider is Centers for Children & Families. The employee assistance programs offered to all the 4000 eligible employees. Currently the District does not have an onsite/near site clinic provider. It is the District intent to hire a firm or provider(s) to administer at a minimum of two locations with a 40 hour per week practitioner at each location. Whether or not each practitioner is a MD/DO, or a mid-level provider has not been decided upon at this time. The bulk of this RFP is for: . Pharmacy Benefit Manager Retail/Mail Order . Employee Assistance Program . Tele-Medicine Provider . On-Site/ Near Site clinic management The District does not have the staff to increase their job functions being performed currently. Therefore, any carrier must be willing to meet all the stated current services as a minimum and clearly outlined in his or her proposal any deviations from those stated in the administrative services section of this RFP. Should you have standard products that do not in their entirety meet the RFP, please feel free to respond based upon your standard package. However, you must specify any and all deviations in your proposal and the RFP on the “Statement of Compliance”. It will be assumed that your proposal is in compliance if deviations are not noted in the "Statement of Compliance”. Administrative services are specific, and deviations will not be accepted. This RFP has outlined the services the District expects as a minimum requirement. Any proposer will be responsible for having qualified personnel and computerized systems capable of handling a case of this size and the flexible plan of benefits. The proposer must provide references and proof of the provider’s ability to serve satisfactory to the District. This contract will not be based upon cost alone but will place equal importance on ability to pay claims timely and accurately, and on the ability of the provider to administer cost containment programs selected by the District. Sealed Proposals will be received only at the following address:
PPaaggee 1144 ooff 110000
BY E-MAIL BY E-MAIL Albert Valencia Eric Smith Director of Purchasing Managing Partner ECISD Purchasing Department Smith & Associates Consulting 802 N Sam Houston P.O. Box 92398 Odessa, TX 79761 Southlake, TX 76092 [email protected] [email protected]
All sealed proposals must be at the above address by MARCH 31st, 2020 at 2:00 p.m. CDST. All proposals received after the prescribed deadline, regardless of the mode of delivery, shall be returned unopened.
All proposers must include a financial statement audited by an independent third party. If you have any technical questions about the specifications, please put all questions in writing to the attention of Eric Smith via e-mail at [email protected].

PPaaggee 1155 ooff 110000
SECTION B
GENERAL CARRIER REQUIREMENTS

PPaaggee 1166 ooff 110000
SECTION B: GENERAL CARRIER REQUIREMENTS
1. Transitional Process
The selected company shall be responsible for all claims incurred on/or after January 1, 2021. It is imperative that any exclusions, limitations or any other deviation be clearly outlined and discussed. A proposer is expected to explain, in detail, any limitations.
2. Commission
No commissions or service fees shall be paid to any party without full disclosure.
3. Compliance with the Request for Proposal
All responses are to be prepared according to the Request for Proposal. Any item(s) your company cannot accommodate are to be disclosed in writing on the Statement of Compliance Form. After a commitment has been made by the District, the carrier will be held responsible for all items contained in the specifications.
4. Effective Date
The effective date of the new contract(s) will be. January 1, 2021.
5. Enrollment The selected carrier will be responsible for enrollment support and informational meetings at the District during open enrollment to be held during the month of October-November
7. Quoted Rates
A minimum rate guarantee of 36 (thirty-six) months is required. Please confirm this guarantee in your response to the proposal and denote any additional guarantees your company may wish to extend to the District. It is the Region’s intent to establish three (3) one-year contracts with the new carrier provided renewal rates are given in a capped % and are provided with your proposal. The proposal must clearly state: a) The guaranteed period of time. Any adjustments on an annual basis must have an
acceptable negotiable cap; and b) Must include a clause retaining the Region’s continuing right to terminate the
contract at the end of the Region’s budget period; and c) A clause conditioning the continuation of the contract on the Region’s best efforts to
appropriate funds for the payment of the contract.

PPaaggee 1177 ooff 110000
8. Renewal Rates
The selected carrier is required to deliver a rate adjustment no later than 90 days before the anniversary date each year.
9. Ownership of Records
All records, member files and miscellaneous data necessary to administer the plan shall be the property of the District. The selected carrier will be asked to transfer records to the District within 30 days of notice of termination.
10. Master Contract
The master contract and/or summary plan descriptions shall be provided to the District no later than 30 days before effective date. Please confirm your ability to provide this service and meet the deadline in your bid response.
11. Plan Changes and Amendments
If changes in the plan of benefits or servicing requirements are needed, such changes will be made in writing and deemed as an amendment to the contract.
12. Carrier Selection
The selection of the carrier/admisrator will be made on or before May 31st , 2020
13. Right to Audit
The District or District member reserves the right to audit the claim records and other financial records of its insurers/providers, as they pertain to the employee benefit program whenever it is deemed appropriate. Such audits may be performed by the Region’s personnel or by outside auditors selected by the District. Claim data tapes/CDs may be requested for time periods of a year or more to be used in conjunction with an audit. These will be furnished within 10 calendar days of a written request at the Administrator’s expense along with an applicable record file layout and/or any other file specifications deemed necessary to “read” the data on the tape/CD. The requested tape/CD will contain the data specified in the written request.
14. Data Caveat
The data contained in this section has been gathered and coordinated by the consultant and reviewed as to accuracy on a "best effort" manner. This request for proposal is qualified to the extent the data provided is accurate.
PPaaggee 1188 ooff 110000
15. Qualification Provisions
The selected Carrier/Administrator must meet the following criteria:
I. Must have been rated by A.M. Best for at least the past three (3) years as an A
rated company; II. Insurance Company(s) are published in the current listing of insurance companies
authorized to transact business in Texas; and III. Will consider waiving the Employee Actively at Work/Dependent Non-Confined
underwriting provision. IV. Third Party Administrators must be licensed in the State of Texas.
16. Biography
Please provide a brief biography or relevant experience on key personnel in management, claims, eligibility and data processing.
17. Client Information
The Administrator data needed:
. 3 termed clients within last 5 years
. 2 new clients within last year
. 5 existing clients with that Administrator for 3 or more years
18. Awards
The award to the successful proposer will be based upon responses to questions outlined in these specifications and an estimate of the quality and effectiveness of each proposer’s services in the following areas:
1. Experience in servicing self-insured governmental entities; 2. Claims adjudication service(s) offered; 3. Quality of risk management information services and report capabilities; 4. Internal and external claims audit reports; and 5. Written and oral presentations and representations.
In addition, the District may also consider: 1. The purchase price; 2. The reputation of the vendor and the vendor’s goods or services; 3. The quality of the vendor’s goods or services; 4. The extent to which the goods or services meet the Region’s needs; 5. The vendor’s past relationship with the District; 6. The impact on the ability of the District to comply with laws and rules relating to
historically underutilized businesses;

PPaaggee 1199 ooff 110000
7. The total long-term cost to the District to acquire the vendor’s goods or services; and
8. Any other relevant factor that a private business entity would consider in selecting a vendor.
20. Graded Evaluation Factor
The following graded evaluation factors will be used to determine how well a proposer(s) meet(s) the desired performance: Factors Points Price 40 Personnel & Management Experience 15 Computer System and Report Generation 15 Location and Market Access 10 Proposal Responsibilities 10 School District Experience 10

PPaaggee 2200 ooff 110000
SECTION C
PHARMACY BENEFITS MANAGER RETAIL/MAIL ORDER

PPaaggee 2211 ooff 110000
SECTION C: PHARMACY BENEFIT MANAGER RETAIL / MAIL ORDER To assist you in developing your response, we have summarized the criteria that will be used to evaluate your proposal. The successful organization will exhibit the following critical elements:
General Program Characteristics
. Ability to interface with the District Medical TPA Blue Cross Blue Shield
. Ability to administer an electronically integrated POS retail and mail service program;
. Proven experience in administering integrated managed prescription drugs and DUR programs:
. Ability and willingness to administer plan design exactly as specified;
. Ability to offer on-line access to transfer of eligibility information;
. Ability to interface with medical claims payors and utilization review organizations as necessary;
. Proactive, responsive, and effective account management;
. Professional, complete, and timely response to RFP; and
. Favorable input from client references.
. Employees will need to have the ability to get Mail Order Prescriptions at certain Retail Pharmacy’s at the Mail Order Co-pay. Do you have this capability?
Retail Network Considerations
. Access to retail network providers;
. Ability to provide on-line, electronic POS capability to:
- Verify eligibility;
- Verify plan design;
- Submit and adjudicate claims;
- Perform concurrent DUR; and
- Collect cost and utilization data.
. Acceptable plan for transition from current mail service provider (if necessary).
Mail Service Characteristics
. Acceptable level of dispensing accuracy;
. Acceptable prescription turnaround time;
. Ability to provide on-line, electronic POS capability to:

PPaaggee 2222 ooff 110000
- Verify eligibility;
- Verify plan design;
- Submit claims;
- Perform concurrent DUR;
- Collect cost and utilization data; and
. Acceptable plan for transition from current mail service provider (if necessary).
DUR Programs
. Timely integration of mail service and retail data;
. Ability to offer comprehensive concurrent and retrospective programs;
. Extensive evaluation criteria and frequent product enhancement;
. Ability to monitor concurrent and retrospective review outcomes; and
. Ability to provide measurable results.
Quality Assurance Measures
. Thorough retail network provider credentialing including:
- Professional qualifications;
- Appropriate state and federal licensure;
- Adequate malpractice insurance;
- Disciplinary history; and
- Re-credentialing/contract re-negotiation.
Customer/Client Services (Applicable to Both Retail and Mail Service)
. Access to Customer Service Representative (CSR);
. Favorable CSR responsiveness:
- Average speed of answer;
- Abandonment rate;
- Inquiry/complaint resolution;
. Ability to monitor customer service performance measures on a client-specific basis;
. Access to registered pharmacist;
. Access to electronically integrated mail service and retail cost and utilization data (on-line, real time);

PPaaggee 2233 ooff 110000
. Extensive, flexible reporting capabilities;
. Ability to provide on-line access to claims database; and
. Assistance in developing a broad range of education/introductory program materials/services.
Financial Considerations
. Stability of organization;
. Competitive administrative costs;
. Significant provider discounts; and
. Ability to negotiate network pharmacy reimbursement based upon the lesser of the pharmacy’s usual and customary retail price, the negotiated contract price or Maximum Allowable Cost (MAC) pricing.
PROGRAM MANAGEMNT AND OR ADDITIONAL CLINICAL PROGRAMS
The District is interested in various alternatives to control pharmacy costs. Organizations who may not be primary Pharmacy Benefit Managers but do provide consulting, contract analysis or who offer clinical management programs to control pharmacy spend are encouraged to describe the programs and pricing in this section.
Please be advised that other criteria may be employed during the evaluation process. Consequently, your organization should feel free to address other issues that may be deemed crucial to the competitiveness of your proposal.

PPaaggee 2244 ooff 110000
FEE QUOTATION EXHIBITS
Please contact Eric Smith at [email protected] for a copy of the claims file.
Administrative Service Fees
Please show your administrative service fees on the enclosed Rate/Fee Sheet for both the retail and mail service portions of the plan. Additionally, consider the following:
. Administrative fee quotations are to be provided on a per claim basis for a traditional model or via PEPM fee for pass thru model.
. District is highly interested in a reinvestment of rebates in lieu of AWP discounts pricing model.
. Please note any additional administrative fees not accounted for in the quoted base rate (e.g., data integration, etc.); and
. Fees would be guaranteed for a minimum of three years. Please indicate if your guarantee will differ.
. . Use of voluntary formulary program to help drive drug product selection;
. All claims incurred by eligible participants on or after January 1, 2021, will be covered under these arrangements; and
. Fees should be guaranteed for a minimum of three (3) years. Please indicate if your guarantee will differ.
If you are unwilling to meet these requirements, please note variations and include them along with your quotation.
Drug Costs
Please quote retail and mail service drug costs assuming existing benefit design. Additionally, assume:
. Lesser of U&C price, MAC price, or negotiated contract rate for reimbursement.
. A generic enforcement program whereby patients refusing a generic substitute when available and appropriate, will be required to pay the difference between brand and generic prices in addition to the applicable co-payment. This program will apply for both retail and mail service prescription purchases;
PPaaggee 2255 ooff 110000
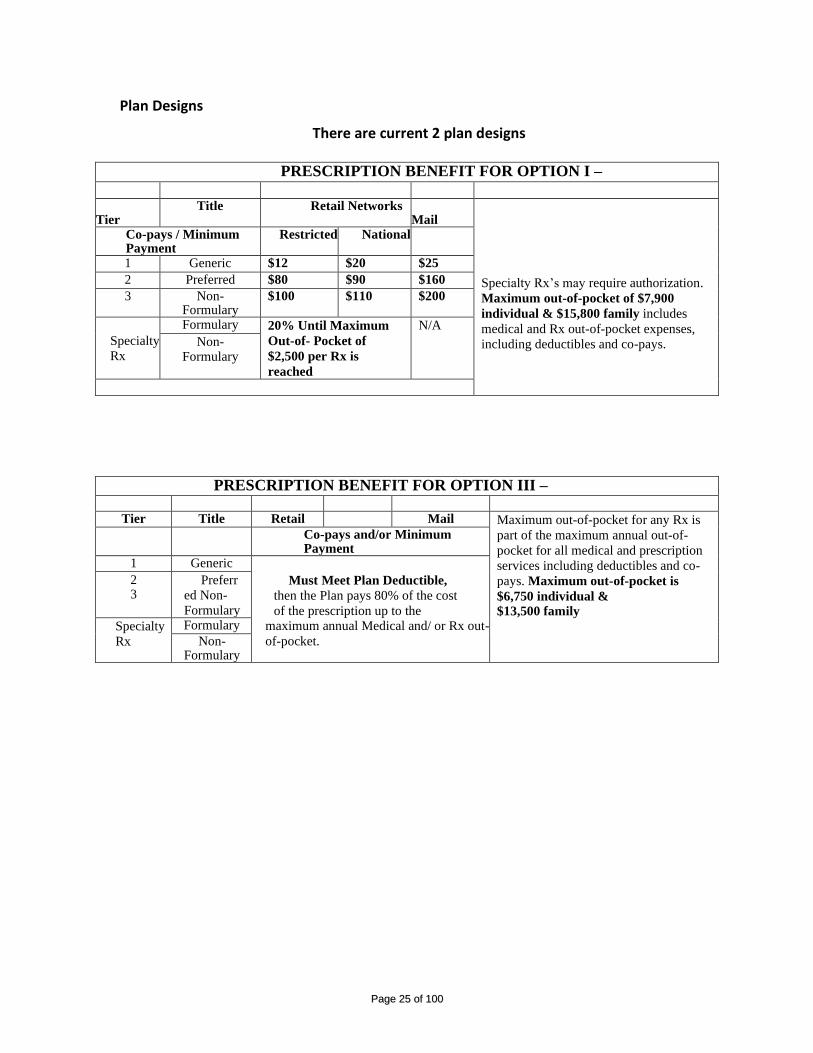
Plan Designs
There are current 2 plan designs
PRESCRIPTION BENEFIT FOR OPTION I –
Tier
Title Retail Networks Mail
Specialty Rx’s may require authorization.
Maximum out-of-pocket of $7,900
individual & $15,800 family includes
medical and Rx out-of-pocket expenses,
including deductibles and co-pays.
Co-pays / Minimum Payment
Restricted National
1 Generic $12 $20 $25
2 Preferred $80 $90 $160
3 Non-Formulary
$100 $110 $200
Specialty
Rx
Formulary 20% Until Maximum
Out-of- Pocket of
$2,500 per Rx is
reached
N/A
Non-Formulary
PRESCRIPTION BENEFIT FOR OPTION III –
Tier Title Retail Mail Maximum out-of-pocket for any Rx is
part of the maximum annual out-of-
pocket for all medical and prescription
services including deductibles and co-
pays. Maximum out-of-pocket is
$6,750 individual &
$13,500 family
Co-pays and/or Minimum Payment
1 Generic
Must Meet Plan Deductible,
then the Plan pays 80% of the cost
of the prescription up to the maximum annual Medical and/ or Rx out-
of-pocket.
2 3
Preferr
ed Non-
Formulary
Specialty
Rx
Formulary
Non-Formulary
PPaaggee 2266 ooff 110000
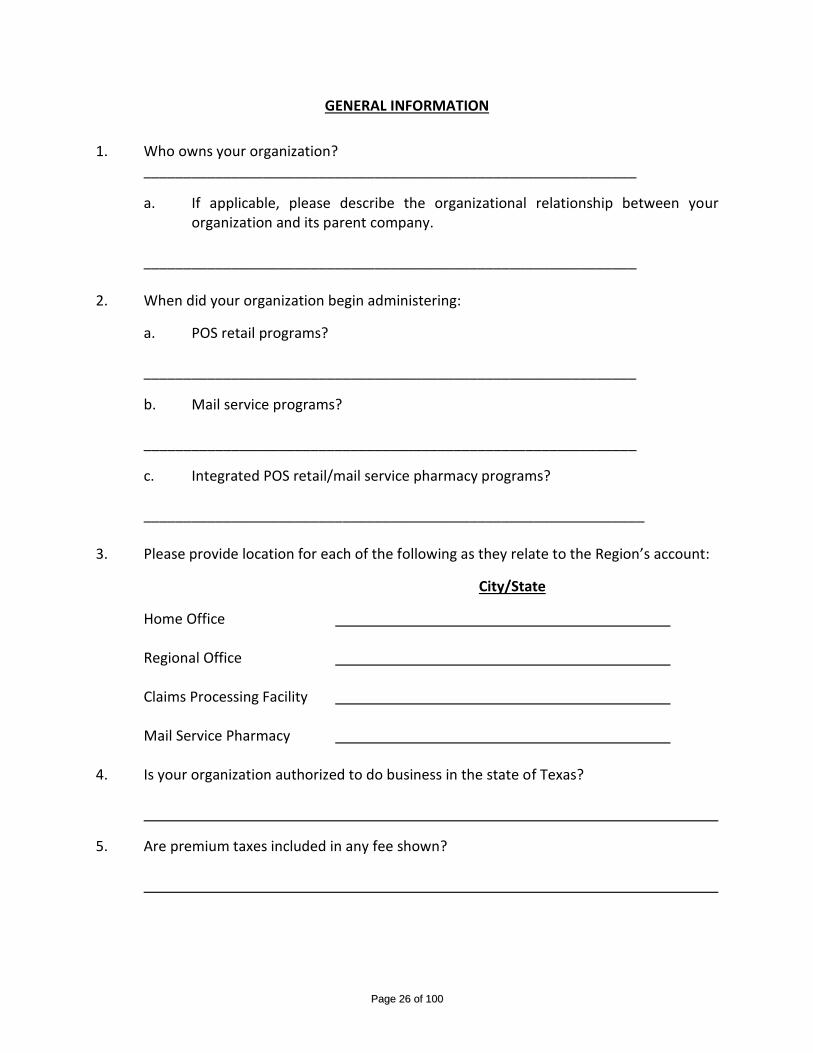
GENERAL INFORMATION
1. Who owns your organization? ______________________________________________________________
a. If applicable, please describe the organizational relationship between your organization and its parent company.
______________________________________________________________ 2. When did your organization begin administering:
a. POS retail programs? ______________________________________________________________
b. Mail service programs? ______________________________________________________________
c. Integrated POS retail/mail service pharmacy programs? _______________________________________________________________ 3. Please provide location for each of the following as they relate to the Region’s account:
City/State
Home Office Regional Office Claims Processing Facility Mail Service Pharmacy 4. Is your organization authorized to do business in the state of Texas?
5. Are premium taxes included in any fee shown?

PPaaggee 2277 ooff 110000
6. Do the fees provided include any level of commissions? 7. Does your organization agree that all records, member files and miscellaneous data
used in administration of this plan shall remain the property of the District? _____________________________________________________________ 8. Can you provide a paid claim file to the District’s Third-Party Administrator at least once
a month, preferable daily or weekly? This file must show the members paid portion at retail pharmacies.
9. Does your organization have access to our or have you formed your own
Biotechnical/Specialty Network? If so, please explain in detail how it would function and the costs of these drugs.
10. Please describe in detail all your cost containment services. (i.e. Step Therapy, Prior
Authorization, etc) and the costs associated with these services, if any. 11. Can you administer a 90-day prescription at certain retail pharmacies for the mail order co-pay? 12. Please review the attached plan changes in Section M and verify your ability to
administer a program such as the 13. Please give some suggested cost control measures that you fill the District should consider. 14. Can you administer a co-insurance plan for Retail Rx instead of co-pays? 15. How do you typical administer/process manufacturer coupons? 16. Can you administer any plan saving initiatives regarding manufacturer coupons?

PPaaggee 2288 ooff 110000
17. Describe in detail manufacturer rebates and how they will be calculated and
reimbursed to the plan? 18. Based on your review of the claims file please project the districts saving by switching to
your organization, and are there any changes to the formulary you would recommend? 19. Please provide three (3) references consisting of both current and terminated clients. Name Company Telephone # # of EE Lives Name Company Telephone # # of EE Lives Name Company Telephone # # of EE Lives

PPaaggee 2299 ooff 110000
Financial Proposal - Traditional / Pass Through
Year One Year Two Year Three
Retail 30 Generic Guaranteed Discount
Retail 30 Generic Guaranteed Dispensing Fee
Retail 30 Brand Guaranteed Discount
Retail 30 Brand Guaranteed Dispensing Fee
Retail 90 Generic Guaranteed Discount
Retail 90 Generic Guaranteed Dispensing Fee
Retail 90 Brand Guaranteed Discount
Retail 90 Brand Guaranteed Dispensing Fee
Mail Order Generic Guaranteed Discount
Mail Order Generic Guaranteed Dispensing Fee
Mail Order Brand Guaranteed Discount
Mail Order Brand Guaranteed Dispensing Fee
Specialty Generic Guaranteed Discount
Specialty Generic Guaranteed Dispensing Fee
Specialty Brand Guaranteed Discount
Specialty Brand Guaranteed Dispensing Fee
Pharmaceutical Manufacturer Rebates - Traditional Year One Year Two Year Three
Minimum Retail Per Brand Guarantee
Minimum Retail 90 Per Brand Guarantee
Minimum Mail Order Per Brand Guarantee
Minimum Specialty Per Brand Guarantee
Projected Network
Performance
Pharmacy Network Pricing - Pass Through / Transparent Year One Year Two Year Three Year One
Year Two
Year Three
Retail 30 Generic Minimum Guaranteed Discount
Retail 30 Generic Minimum Guaranteed Dispensing Fee
Retail 30 Brand Minimum Guaranteed Discount
Retail 30 Brand Minimum Guaranteed Dispensing Fee
Retail 90 Generic Minimum Guaranteed Discount
Retail 90 Generic Minimum Guaranteed Dispensing Fee
Retail 90 Brand Minimum Guaranteed Discount
Retail 90 Brand Minimum Guaranteed Dispensing Fee
Mail Order Generic Minimum Guaranteed Discount
Mail Order Generic Minimum Guaranteed Dispensing Fee
Mail Order Brand Minimum Guaranteed Discount
Mail Order Brand Minimum Guaranteed Dispensing Fee
Specialty Generic Minimum Guaranteed Discount
Specialty Generic Minimum Guaranteed Dispensing Fee
Specialty Brand Minimum Guaranteed Discount
Specialty Brand Minimum Guaranteed Dispensing Fee

PPaaggee 3300 ooff 110000
This sheet must be completed in order to be considered
Projected Performance
Pharmaceutical Manufacturer Rebates - Pass Through / Transparent Year One Year Two Year Three Year One
Year Two
Year Three
Minimum Retail Per Brand Guarantee
Minimum Retail 90 Per Brand Guarantee
Minimum Mail Order Per Brand Guarantee
Minimum Specialty Per Brand Guarantee
Administrative / Service Fees
Proposed Administrative Fees (Pass Through / Transparent Offering) Year One Year Two Year Three
All-In Administrative Fee (Preferred) - PMPM
All-In Administrative Fee (Preferred) - Per Paid Claim
Prospective Partner Allowances Year One Year Two Year Three
District Management Fees 2% of AWP 2% of AWP 2% of AWP
Pharmacy Management Fund
*Any supporting caveats to the Prospective Partner pricing must be disclosed in a separate supplement document signed by the Company Executive.
*Any traditional contract is assumed to include any/all administrative fees.

PPaaggee 3311 ooff 110000
SECTION D
ONSITE/NEAR SITE CLINIC MANAGEMENT SERVICES

PPaaggee 3322 ooff 110000
SECTION D: ONSITE/NEAR SITE CLINIC MANAGEMENT SERVICES SCOPE OF SERVICES
I. SCOPE OF SERVICES
The selected organization will be responsible for managing the day-to-day operations of an employee Clinic, including the care and treatment of employees, as well as providing enhanced health awareness, education and follow-up on employee health issues. Dues to the unique nature of the District pricing will need to be broken down into 8-hour sections. Assume 8 hours of clinic time per 1000 employees. Specifically, the following core services are expected to be delivered in the center, in conjunction with the current programs in place;
1. Conduct pre-employment physicals as requested;
.
2. Give inoculations and vaccinations including flu shots, tetanus, etc. as desired or promoted by the District or during wellness related health screenings and events.
3. Provide minor care for injured employees, in accordance with state law, and case management.
a. Prompt Treatment – injuries to receive preferred service (no waiting periods) by a licensed physician.
b. Communication with the District: The Physician shall contact the designated Human Resource staff member with the employee’s condition, treatment, prognosis, and return to work status.
c. Case Management to include loss control, peer to peer review and computerized tracking.
4. Provide primary medical care for employees who have non-occupational illness or injuries.
5. Provide state of the art technology to support scheduling requirements for employees and online check-in.
6. Support wellness initiatives in conjunction with the District’s wellness program,
including but not limited to conducting: a. Health Screening – Blood Pressure checks, HDL/LDL Cholesterol, Blood
Sugar, Total BMI and other screenings as requested during the year. b. Supply the District with an electronic file on a month basis with participation
in the Health Assessments. This allows the District to accurately apply the premium incentives.
c. Provide employee follow-up and wellness education. d. Offer comprehensive Health Risk Assessments (with reports back to
individuals and to the District on an overview of our total risks, what to
PPaaggee 3333 ooff 110000
focus on to reduce risks. All reporting should be in compliance with HIPAA requirements).
e. Chronic disease management and monitoring and employee education f. Coordination with the District’s wellness representative to support wellness
related activities. g. Assist the District in developing wellness initiatives that have a direct impact
on potentially reducing identified health risks in the District.
7. It is the District’s intent that the Clinic will provide pharmacy benefits if the cost and implementation is determined to be a benefit to the District and its employees. This will be considered as an option during the review of this Clinic’s feasibility study. If these services are offered, please provide detailed pricing information.
8. Provide Pediatric services by a Pediatrician on a limited basis.
II. CLINIC HOURS
The Clinic is expected to operate initially during normal business hours of 8:00 am to 8:00 pm.
Alternate hours or extended hours may be proposed as options but should be quoted in addition to the standard operating hours. Hours may be extended after the Clinic is operational, based on demand, demonstrated success in meeting the District’s expectations and quality of care. After-hours, weekend and emergency care will be provided through established Urgent Care Centers and ER Facilities. If the Clinic is to be staffed by someone other than an MD/DO during the evening hours or Saturday hours, please explain the licensure of the individual you expect to fulfill those hours. A Nurse Practitioner is acceptable to the District during these hours.
III. REPORTING
The selected vendor will deliver management reports on an agreed upon timeframe (quarterly, etc.) to include:
a. Clinic census data (employees seen/day; time/visit; etc) b. Financial performance data c. Employee satisfaction data d. Referral data e. Cost savings f. Wellness initiatives and efforts
In addition to the above-mentioned reporting requirements, the District is also requesting that member specific disease states are transmitted to the designated Disease Management Company on a monthly basis.

PPaaggee 3344 ooff 110000
IV. CLINIC MANAGEMENT AND OPERATIONS
a. The selected vendor will operate the Clinic on a day-to-day basis to include, but not limited to, the following components:
i. Staffing of medical, technical and support staff that demonstrate strong interpersonal skills, exceptional service philosophy and passion for the treatment, care and recovery of patients;
ii. Supply and inventory management; iii. Medical administration of patient care including patient management and referral
management; iv. Maintain communications with District officials regarding patient status within
HIPAA and ADA guidelines; v. Maintain employee records in a secured environment and efficient matter and in
compliance with HIPAA regulations; vi. Actively manage the District’s employee health by deploying target wellness and
chronic disease management initiatives with internal or subcontracted vendors; vii. Maintain open dialogue with the District’s medical providers and District officials in
charge of those functions to balance the employee’s recovery; viii. Assist and actively engage in cost savings management initiatives;
ix. Provide regularly scheduled reports to the District that sufficiently describe the program impact, cost impact, employee satisfaction, and other parameters as agreed upon with the District;
x. Manage and dispense prescription drugs, to include specialty pharmacy and biotech medicines, etc.;
xi. Refer members to cost effective, local providers who are in the District’s PPO Network.
b. Clinic Start-up
The selected vendor will be expected to engage in development work leading to an efficient and successful Clinic. To that extent, the vendor, in tandem with District officials, or District designated representatives, will extend any of its purchasing benefits, resources, networking contracts, or additional opportunities to minimize cost and optimize resources. The Clinic is to be furnished and maintained in the most professional and efficient manner possible.
c. Communications and Promotion of the Clinic
The vendor will provide resources and expertise to ensure an optimal and positive positioning of the Clinic at time of opening. The District values the high employee’s endorsement received from the surveys and interviews and expects that to translate into high participation volumes. In recognition of that, the vendor will coordinate its marketing and promotional efforts with District interests.
d. Quality Assurance and Liability i. The selected vendor will provide proof of high patient service quality through its
patient satisfaction program, patient complaint handling and its conformance with regulatory requirements. Given the oversight by Risk Management and Employee Benefits, this aspect will be emphasized during the selection process.
ii. The vendor will clearly state the extent to which it will accept liability for the services provided and the extent to which the District will be liable. The vendor will

PPaaggee 3355 ooff 110000
provide any examples of liability cases that it may be aware of to assist the District in determining its potential liability.
e. Add-On Services
The vendor, with individual District approval, will recommend additional services on an as-needed basis. Such services will be evaluated on medical and cost aspects as well as overall impact to the individual District’s. This will not be a cookie cutter approach flexibility and fluidity will be extremely important for the selected entity.
V. EXPERIENCE AND HISTORY
The vendor shall provide a demonstrated history of successful Clinic design, start-up and management. The vendor shall provide detail to outline projected steps in Clinic startup and provide at least one site visit for 2-3 District staff of a recently implemented and operational Clinic similar in scope to what the District is requesting. References of the proposer’s Clinics shall include: a Clinic in operation in excess of 5 years, less than 5 years and newly implemented. It is important that the District obtains a comfort level with the vendor for the quality of work proposed as well as the conceptual fit of the Clinic with the District’s intent to manage cost and optimize employee relations. Further, the proposer must disclose how they will find staff to work in the Clinic that fit the District’s organizational culture of care and service delivery expected of a world-class organization.
Scope of Services Questionnaire
The District seeks a company to offer on-site medical services to its member District’s employees and dependents to include but not limited to primary care, health risk assessments, call support, immunizations, injections, new hire physicals, exams and screenings (including random and required drug testing), prescriptions, pharmaceuticals, disease management, and primary care case management. In addition to on-site healthcare the Entity’s desires the on-site medical services to provide health risk assessments and handle on-the-job injury services including treatment of injuries and case management. The District is also interested to know if the proposer can offer disease management services driven by its health plans medical and pharmacy claims data so it can reach members who don’t access the Clinic. The provider will work with the District’s existing wellness program to provide educational, intervention and incentive programs. The company must comply with all guidelines and regulations set forth in the Health Insurance Portability and Accountability Act (HIPAA).
PPaaggee 3366 ooff 110000
So that the District can fully understand your services, please answer the following questions as thoroughly and succinctly as possible:
Primary Care:
1. How are appointments scheduled?
2. How many appointments per day are you estimating?
3. Clearly explain:
a. What level of staff you are projecting (P.A., Nurse, MD, etc)
b. Their normal projected salary
c. Their projected hours per day at the Clinic
4. Is the appointment scheduling process available online?
5. Describe the types of problems that can be addressed on-site.
6. Describe if you support implementing a pharmacy on-site or recommend this as a 2nd
phase.
7. What hours of operation are you proposing?
8. What if a disease process escalates?
9. Will your physician(s) have hospital privileges? If so, where?
10. Describe the primary care case management process.
11. What if the medical team is not available on the day the care is needed?
12. How will you refer after hours issues?
13. The District will expect some pediatric coverage at the Clinic, please explain how you
can and will address this coverage.
Pharmacy:
1. Please explain your methodology for dispensing prescription drugs through the Clinic.
2. Please explain in detail how you propose to handle the inventory of Prescription drugs.
3. What guarantees are you willing to put in place, assuring the District they will not be at
risk for Out of Date Prescriptions?
4. Please explain how your ability to supply specialty and biotech drugs through the Clinic.
5. How would you propose getting prescriptions to members who live a great distance
from the Clinic?

PPaaggee 3377 ooff 110000
Communication Plan & Member Services: Please provide a proposed communication plan for introducing the on-site healthcare and wellness program and reference the on-going communication process. Outline your company’s responsibilities in these processes. Please include copies of your educational materials and timelines for distribution.
1. How can employees communicate with the medical team?
2. How do you determine locations of service and standard hours of operations for
member services?
3. Will you utilize existing resources for Clinics?
4. What staffing do you envision?
5. What days and hours of operation do you recommend?
6. Describe your ability to provide health care on nights and weekends.
7. Is your health risk assessment available both on-line and off-line?
8. Can your website be linked with the District’s website?
9. Describe your ability to communicate with an employee population that is
geographically dispersed. Provide examples if appropriate.
10. Discuss the frequency and type of communications that eligible persons will receive
throughout the program period.
11. How can an employee access your company for Member Services after hours?
12. Provide your web address and any access codes needed to explore your services.
13. Are you willing to let the District use its own branding on communication and program
materials?
Identification of High-Risk Individuals: Understanding that there are a variety of methodologies for implementing a HRA/targeted intervention process, please explain in detail the HRA/targeted intervention model that your organization would recommend be implemented. Explain the rationale behind your recommendation. Please keep in mind that this needs to be a confidential process following all HIPAA guidelines.
1. How would your company identify high-risk members?

PPaaggee 3388 ooff 110000
2. Please describe your methodology for tracking and intervening with high-risk members
on an on-going basis.
3. Do you stratify members by severity of risk for complication? Please elaborate.
4. What Health Risk Assessment (HRA) do you use and how long have you used it? List all
risk factors you identify in your profile. Please provide a sample HRA in your response.
5. How often do you recommend that the members have an HRA?
6. Please describe turn-a-round time for each of the following areas:
a. Providing the HRA results to individuals;
b. Contacting individuals for possible interventions;
c. Providing the District with a summary report of the initial HRA results.
7. Please describe how your organization would provide a system to assist HRA
participants in completion of their questionnaires and in the interpretation of their
personal profile.
8. What level of participation can we expect in year one, two and three of this program?
9. Describe how your organization will set and reach participation goals?
10. Do you recommend using incentives? If so, please describe the incentives your
organization recommends.
11. Please describe your plan to involve new employees in the HRA process.
12. Please describe your capabilities to update an individuals HRA record while conducting
follow-up calls.
13. How does your HRA monitor and report individual changes from year to year?
14. Describe in detail how Clinic data gathered at the Clinic will be shared with the District’s
Case Management/Disease Management vendor.
15. Describe how you envision working collectively with the District’s Case Management /
Disease Management Vendor.
PPaaggee 3399 ooff 110000
Intervention
Please describe a typical intervention conversation.
1. Are telephone conversations monitored for quality assurance? If so, how?
2. Describe the process for engaging the targeted individual.
3. Describe the process for persons you are unable to reach.
4. Describe and provide samples of any support materials used with the intervention.
5. Describe the process for documentation and tracking of each conversation.
6. Describe and provide samples of any management reports on intervention activity.
7. How do you link to on-site or community programs (Employee Assistance Programs,
Wellness Screenings, etc.)?
8. Describe your methods for ensuring confidentiality of caller information.
9. Indicate what type of provider interventions and education your plan provides and the
results of these interventions.
Measurement Tools & Results: Provide a copy of your quality assurance program. This should include standard measurement criteria for on-site healthcare activities, costs, outcomes, HRA, disease management, member services, member intervention and educational materials.
1. How would you propose measuring the outcomes and success of the overall program?
2. Describe your standard management reports. Describe your custom reporting
capabilities and the associated costs. Please provide a recommendation and examples
of reports that you would provide the District.
3. Provide examples of the following:
a. On-site healthcare activity report
b. HRA and member profile
c. Member participation
d. Member intervention
e. Financial summary/savings report
f. Are management reports available on-line?
PPaaggee 4400 ooff 110000
4. Describe how your plan specifically evaluates the effectiveness of primary care case
management. Include any results of the evaluation as an attachment.
5. Provide all Clinic indicators used to track the success of the program and the results, if
any, by year since inception of the program.
6. Describe specifically how records for individuals with both personal health and job injury
Clinic experience will be managed.
HIPAA Compliance:
1. Is your firm HIPAA compliant?
2. Describe your system for the assurance of personal health data security.
3. Has your network security systems ever been breached? If so, please explain in detail.
Proposed Program Costs: It is the District’s intention to provide on-site health care and population health management services including health risk assessment to every employee and their dependents on our self-funded medical plan. Please include the following in your detailed pricing qualifications:
1. Fees broken out for each recommended key component of making the Clinic
operational:
a. Average cost per visit
b. Hours per day per staff
c. Salaries of Staff
d. Supply costs
e. Expected number of visits per day
f. Any other estimated costs

PPaaggee 4411 ooff 110000
SECTION E
EMPLOYEE ASSISTANCE PROGRAM

PPaaggee 4422 ooff 110000
SECTION E: EMPLOYEE ASSISTANCE PROGRAM
TThhee DDiissttrriicctt iiss llooookkiinngg ttoo ooffffeerr aann EEmmppllooyyeeee AAssssiissttaannccee PPrrooggrraamm ((EEAAPP)) ttoo pprroovviiddee IInnddiivviidduuaall,,
MMaarriittaall,, FFaammiillyy,, PPllaayy,, aanndd GGrroouupp CCoouunnsseelliinngg ffoorr DDiissttrriicctt eemmppllooyyeeeess aanndd tthheeiirr ffaammiilliieess..,, ffoorr aannyy ooff
tthhee ffoolllloowwiinngg nneeeeddss::
--DDeepprreessssiioonn --WWoorrkkppllaaccee DDiiffffiiccuullttiieess
--AAnnxxiieettyy --SSttrreessss MMaannaaggeemmeenntt
--AAnnggeerr MMaannaaggeemmeenntt --BBiippoollaarr DDiissoorrddeerr
--MMaarriittaall DDiissccoorrdd --FFaammiillyy CCoonnfflliicctt//VViioolleennccee
--DDoommeessttiicc VViioolleennccee --SSuubbssttaannccee AAbbuussee
--GGrriieeff//LLoossss --SSkkiillll BBuuiillddiinngg ffoorr PPaarreennttss
--PPeeeerr DDiiffffiiccuullttiieess --BBeehhaavviioorraall AAccttiinngg OOuutt iinn CChhiillddrreenn
--TThhoouugghhttss ooff SSuuiicciiddee --EEaattiinngg DDiissoorrddeerrss
--DDiivvoorrccee//BBlleennddeedd FFaammiilliieess --CCoommppuullssiivvee SSeexxuuaall BBeehhaavviioorrss//IInntteerrnneett AAddddiiccttiioonnss
--PPrreemmaarriittaall CCoouunnsseelliinngg --RReeffeerrrraall ttoo CCoommmmuunniittyy RReessoouurrcceess
EEmmppllooyyeeeess wwiillll rreecceeiivvee uupp ttoo 66 ccoouunnsseelliinngg sseessssiioonnss aatt nnoo cchhaarrggee.. SShhoouulldd lloonnggeerr--tteerrmm ccaarree bbee
nneeeeddeedd,, pprroovviiddeerrss sshhoouulldd aacccceepptt IInnssuurraannccee,, MMeeddiiccaaiidd aanndd CCHHIIPPss aass wweellll aass ooffffeerriinngg aa sslliiddiinngg ffeeee
ssccaallee..
AAnn aafftteerr hhoouurr,, oonn ccaallll sseerrvviiccee iiss rreeqquueesstteedd ffoorr eemmoottiioonnaall//bbeehhaavviioorraall ccrriissiiss..
PPaaggee 4433 ooff 110000
EAP QUESTIONNAIRE
. Maximum of three (3) or six (6) sessions per employee and dependent per incident
every 12 months. . Training for both employee and supervisors. . Reports upon request. 1. Do you provide a toll-free number for customer service?
2. What are your business hours? 3. Do you provide an afterhours call-in system? How does it work?
4. What is the average return call time?
5. Briefly summarize the history of your organization and identify the owner.
6. List the academic and professional experience of your staff.
7. List areas of counseling (individual and family) you are prepared to offer.
8. How does your organization handle client confidentiality?

PPaaggee 4444 ooff 110000
9. Are you equipped to stagger the scheduling of employees in order to maintain their confidentiality? Please explain.
10. How do you provide comprehensive follow-up care?
11. Explain your referral process.
12. What are your liability insurance levels?
13. Provide addresses of locations where counseling will be available.
14. Has your organization ever worked with an employee group that has a PPO? If so, describe how you interact with a PPO system.
15. Will your organization provide educational materials to the District for employees? Is there an extra cost for materials provided?
16. What are your procedures for management and employee training? How much training
is provided?
17. Do you have a provider network? If so, state your financial interest, if any, in the network.
18. What reports are provided and how often are they available? What are your fees for additional reports?
PPaaggee 4455 ooff 110000
19. Are you able, if requested, to provide seminars or assistance to management in how to confront troubled employees for possible referral to the program? Is this an extra charge?
20. Provide a list of companies/references and a contact name for each that utilize your services.
21. Provide one company/reference that has terminated your services in the last six
months.
22. Basic Program EAP only: 3 Day Visit 6 Day Visit Annual Cost $______________ $___________ Monthly Cost Per Employee $______________ $___________
Start Up Cost $______________ $___________ PPO Access Fee (if any) $______________ $___________
23. Managed Mental Health/ 3 Day Visit 6 Day Visit Annual Cost $______________ $___________ Monthly Cost Per Employee $______________ $___________
Start Up Cost $______________ $___________ PPO Access Fee (if any) $______________ $___________ 26. How long will your fee remain firm? 27. Do you offer Work Life resources? (Childcare, Elder Care, Financial, Nutrition, etc.) If so,
please provide a complete list of services & details. 27. Other Comments:

PPaaggee 4466 ooff 110000
SECTION F
TELE-MEDICINE PROVIDER
PPaaggee 4477 ooff 110000
SECTION F: TELE-MEDICINE PROVIDER
TELE-MEDICINE QUESTIONNAIRE 1. Do you provide a toll-free number for customer service?
4. What are your business hours? 5. Do you provide an afterhours call-in system? How does it work?
4. What is the average return call time?
5. Briefly summarize the history of your organization.
6. List the academic and professional experience of your staff.
7. List types of medical consults you perform.
8. Do you offer Mental Nervous Consults’? If so at an additional cost??
9. Do you offer Dermatology consults? If so at what costs?
10. How do you provide comprehensive follow-up care?

PPaaggee 4488 ooff 110000
11. Do you have mobile App?
12. What services are available on the App??
13. Will your organization provide educational materials to the District for employees? Is
there an extra cost for materials provided? 14. What are your procedures for management and employee training? How much training
is provided?
15. How large is your provider Network? Mental Nervous Network? Dermatology Network?
16. What reports are provided and how often are they available?
17. What I your average utilization across you book of business. 18. Provide a list of companies/references for 5 clients. 19. Provide one company/reference that has terminated your services in the last six
months. 20. Can you file claims with a client’s third-party administrator? 21. Basic Tele-Medicine Program with: $40 Consult Fee $0 Consult Fee Annual Cost $______________ $___________ Monthly Cost Per Employee $______________ $___________
Start Up Cost $______________ $___________
PPaaggee 4499 ooff 110000
22. Basic Program with Mental Nervous: $80 Consult Fee $0 Consult Fee
Annual Cost $______________ $___________ Monthly Cost Per Employee $______________ $___________
23. How long will your fee remain firm?

SECTION G
CCLLAAIIMMSS EEXXPPEERRIIEENNCCEE//SSAAMMPPLLEE AAGGRREEEEMMEENNTTSS

SSaammppllee PPBBMM AAggrreeeemmeenntt
Sample PHARMACY BENEFIT MANAGEMENT SERVICES AGREEMENT
REGION 12 EMPLOYEE BENEFIT DISTRICT This Pharmacy Benefit Management Services Agreement (“Agreement”) is effective as of <INSERT DATE> (the “Effective Date”) by and between <INSERT PBM> (“<INSERT PBM NAME>”), and <INSERT CLIENT NAME> (“Client”).
RECITALS
Whereas, Client provides its employees and their dependents with medical benefits including benefits for prescription drugs and certain devices and supplies dispensed by pharmacists; and Whereas, <INSERT PBM NAME> provides its clients services in connection with the healthcare operations and payment of claims on behalf of their Plans; and Whereas, <INSERT PBM NAME> provides its services using either a zero-spread, transparent, full pass-through business model, where all of the discounts and rebates received from pharmacies and pharmaceutical manufacturers are provided to its clients, or a traditional reimbursement model where <INSERT PBM NAME> contracts with participating pharmacies and pharmaceutical manufacturers on behalf of the Client. <INSERT PBM NAME> may retain the difference of any price improvements negotiated with manufacturers or pharmacies during the contract term; and Whereas, Client and <INSERT PBM NAME> desire to establish this Agreement for the management of the pharmacy benefits sponsored by Client; Now therefore, in consideration of the mutual promises set forth herein, the sufficiency of which is hereby acknowledged, <INSERT PBM NAME> and Client agree as follows:
Article I DEFINITIONS
The terms below, including their single and plural forms, shall have the meanings set forth in this Article I: Account means a depository account maintained by Client at a federal or state-chartered bank, savings and loan association or savings bank. Average Wholesale Price or AWP means the average wholesale price of a prescription drug published and updated by Medi-Span, or another nationally-recognized reporting service purchased or licensed by <INSERT PBM NAME>. Brand Covered Product or Brand means a Covered Product where the Medi-Span Multi-Source Indicator for the Covered Product reported by Medi-Span contains an “M” (co-branded product), “O” (originator brand) or an “N” (single source brand) for the Covered Product on the date dispensed except where the claim is submitted with a DAW code of “3”, “5”, or “6”, in which case it shall be considered a Generic Drug. Business Associate means a person assisting a Covered Entity in connection with its payment, treatment or health care operations, as more fully defined in 45 CFR §160.103.
Cardmember means one of Client’s active employees, and, if so indicated on the signature page below retired employees, who satisfy all the eligibility criteria necessary to receive pharmacy benefits under Client’s Plan and are identified by Client to <INSERT PBM NAME> in accordance with the provisions of this Agreement as eligible for such benefits. For purposes of clarification, any Eligible Person who is a “Dependent,” as defined below, is not a “Cardmember” for purposes of this Agreement. CFR means the Code of Federal Regulations. Claim means: (a) a contractual payment request submitted by a Participating Pharmacy dispensing one or more prescription drugs and transmitted in accordance with the electronic transaction standards set forth in 45 CFR Parts 160, 162 and 164, as amended from time to time; or (b) a Direct Reimbursement Claim submitted by a Participating Pharmacy, another provider, an Eligible Person or such Eligible Person’s representative in connection with one or more prescription drugs dispensed to such Eligible Person. Coinsurance means that portion of the charge for Covered Products, calculated as a percentage of the charge, which is to be paid by Eligible Persons pursuant to Client’s Plan Guidelines (or for certain Participating Pharmacies, if less, the U&C of the Covered Products). Confidential Information has the meaning given in Section 9.03 of this Agreement. Contract Administrator, if any, means the person so indicated on the signature page below. District, means the <INSERT DISTRICT NAME>. District Consultant, means the pharmacy consulting firm delegated by the District to deliver pharmacy consulting services to all participants of the District. Coordination of Benefits means claims administration when Eligible Persons are covered by more than one pharmacy benefit plan. Co-payment means a fixed dollar portion of the charge for Covered Products which is to be paid by Eligible Persons pursuant to Client’s Plan Guidelines (or for certain Participating Pharmacies, if less, the U&C of the Covered Products). Covered Entity means a health plan, a health care clearinghouse or a health care provider, as more fully defined in 45 CFR §160.103. Covered Products means those prescription drugs and ancillary devices and supplies that are covered under Client’s Plan Guidelines. Deductible means a predetermined amount of money that an Eligible Person must pay before benefits are eligible for payment as indicated in Client’s Plan Guidelines. The deductible applies to each Eligible Person each contract year. Dependent means an individual who satisfies all the eligibility criteria through a Cardmember necessary to receive pharmacy benefits under Client’s Plan and is identified by Client to <INSERT PBM NAME> in accordance with the provisions of this Agreement as eligible for such benefits. For purposes of clarification, any Eligible Person who is a “Cardmember,” as defined above, is not a “Dependent” for purposes of this Agreement. Direct Reimbursement Claim means a request for reimbursement for the cost of one or more Covered Products dispensed by a pharmacy and submitted by a Participating Pharmacy, a Non-Participating Pharmacy, or an Eligible Person in a pre-printed universal claim form acceptable to <INSERT PBM NAME>
Eligible Person means each Cardmember and Dependent. ERISA means the Employee Retirement Income Security Act of 1974, and regulations promulgated thereunder, as amended from time to time. FDA means the United States Food and Drug Administration. Formulary means the list of FDA-approved Covered Products developed by <INSERT PBM NAME>’ Pharmacy and Therapeutics Committee, subject to Client’s Plan Guidelines and coverage decisions. Generic Covered Product or Generic means a Covered Product for which there is an approved application under § 505(j) of the Federal Food Drug and Cosmetic Act (21 USC 355(j)) and the Medi-Span Multi-Source Indicator for the Covered Product is a “Y” on the date dispensed. Claims submitted with a Multi-Source Code, as defined by Medi-Span, of “O” and also submitted with a DAW code of “3”, “5”, or “6” shall also be considered a Generic Drug. If a drug product approval is based upon an abbreviated new drug application (ANDA), that drug is a Generic Covered Product. Single-source Generic Covered Products are included in the definition of “Generic Covered Products.” HIPAA means the Health Insurance Portability and Accountability Act of 1996, and regulations promulgated thereunder, as amended from time to time. HIPAA Privacy Rule means the federal regulations related to the use and disclosure of patients’ Protected Health Information under 45 CFR Parts 160, 162 and 164, as amended from time to time. HIPAA Rules mean the medical records, privacy, security, and standard transaction regulations under 45 CFR Parts 160 and 164. Initial Term means the initial term of this Agreement as defined in Section 12.01 of this Agreement. Mail Service Pharmacy means a pharmacy where prescriptions are filled and delivered to Eligible Persons via the United States Postal Service, United Parcel Service or other delivery service, and which has entered into an agreement with <INSERT PBM NAME> to dispense Covered Products. Material Breach means a breach such that a reasonable person in the position of the non-breaching party would wish to terminate this agreement because of that breach. Member means the same as “Eligible Person,” and the two terms may be used interchangeably. <INSERT PBM NAME> Maximum Allowable Cost (“MAC”) means the maximum allowable cost determined by <INSERT PBM NAME> and updated at least quarterly based upon review and analysis of current pricing in the marketplace. Non-Participating Pharmacy means a pharmacy that does not have an agreement with <INSERT PBM NAME> to dispense Covered Products to the Eligible Persons receiving benefits under this Agreement. Participating Pharmacy means a pharmacy, or a company authorized to represent one or more subsidiary, affiliated, or franchised pharmacies, which has entered into an agreement with <INSERT PBM NAME> to dispense Covered Products. For purposes of this Agreement, a "Participating Pharmacy" will not be considered a representative, subcontractor, or agent of <INSERT PBM NAME> and may include the Mail Service Pharmacy and the Specialty Pharmacy.

Pass-Through means that all Claims are invoiced to Client at the net amount <INSERT PBM NAME> pays the Participating Pharmacy for such Claims, and Rebates are provided to Client in accordance with Article IV, below, and <INSERT PBM NAME> does not retain any Rebates or any other direct financial benefits from drug manufacturers or pharmacies, and pays all such amounts to Client. Plan means Client’s insured or self-funded benefit plan, which provides pharmacy benefits to Eligible Persons. Plan Guidelines means a description of Client’s Plan related to pharmacy benefits and limitations thereto, including the framework of policies, interpretations, rules, practices and procedures applicable to such benefits, required and signed by Client and submitted to <INSERT PBM NAME>. The Plan Guidelines shall not include any amendments except as provided in Section 3.02 of this Agreement. PPACA means the Patient Protection and Affordable Care Act and the Health Care Education and Reconciliation Act of 2010 and their accompanying regulations, as amended from time to time. Practitioner means a physician or other health care provider authorized to prescribe medication to Eligible Persons. Prior Authorization means a prospective review to verify that certain criteria required by Client are satisfied for specific Covered Products prior to processing the claim for such Covered Products. Protected Health Information or PHI has the meaning set forth in 45 CFR §164.501 and includes individually identifiable health information related to the physical or mental health or condition, the provision of health care, or the payment for the provision of health care to an Eligible Person or otherwise deemed confidential under federal or state law. Rebates means rebates or discounts received by <INSERT PBM NAME> pursuant to a contract with a pharmaceutical manufacturer, and directly attributable to the Formulary and Covered Product utilization by Eligible Persons. Renewal Term means the time period as defined in Section 12.01 of this Agreement. Specialty Pharmaceuticals means those biotech and other Covered Products identified as specialty pharmaceuticals from time to time. A then-current list of Specialty Pharmaceuticals may be obtained at any time by contacting <INSERT PBM NAME>. Specialty Pharmacy means a pharmacy that has entered into an agreement with <INSERT PBM NAME> to dispense Covered Products including Specialty Pharmaceuticals to Eligible Persons. Usual and Customary Price or U&C means the retail price, including any minimum price, charged by a Non-Participating Pharmacy or a Participating Pharmacy for a Covered Product in a cash or uninsured transaction on the date such product is dispensed. Wholesaler Acquisition Cost or WAC means the wholesale acquisition cost pricing data for a given pharmaceutical product, as published by Medi-Span or another nationally recognized drug database reporting service used by <INSERT PBM NAME>. Year 1 means <INSERT APPLICABLE CONTRACT YEAR>. Year 2 means <INSERT APPLICABLE CONTRACT YEAR>. Year 3 means <INSERT APPLICABLE CONTRACT YEAR>.

Article II <INSERT PBM NAME>’ RESPONSIBILITIES
Section 2.01. General Description of Duties and Obligations. <INSERT PBM NAME> will process Claims, render clinical and Formulary services and provide Client standard management reports and consultative services, all in connection with Eligible Persons’ Covered Product utilization and as more fully set forth in this Agreement. In connection with these services, <INSERT PBM NAME> will evaluate the status and performance of Client’s pharmacy benefit program and advise Client on a regular basis of the results of such evaluation. Section 2.02. Implementation Services. <INSERT PBM NAME> will assign dedicated personnel to Client in order to implement the services provided under this Agreement. The <INSERT PBM NAME> implementation team will facilitate the implementation of all aspects of the Client pharmacy benefit program and will provide Client the following standard implementation services: (a) loading eligibility files that do not require conversion to be in <INSERT PBM NAME>’ standard format; (b) encoding Client’s Plan Guidelines within the <INSERT PBM NAME> information services and claims processing systems; (c) creating and encoding Client’s Plan Guidelines within the Participating Pharmacy network active in the <INSERT PBM NAME> system; (d) initiating for Client a standard reporting package, without modification, from <INSERT PBM NAME>’ standard report library; (e) implementing standard <INSERT PBM NAME> system edits; (f) producing standard laminated identification cards with <INSERT PBM NAME> logo, or providing files to Client for production of a combined identification card by Client; (g) enabling Client’s connectivity through a virtual private network or file transfer protocol to <INSERT PBM NAME>’ system; (h) implementing standard Prior Authorization guidelines required by Client (when prior authorization services are purchased without customization); and (i) producing standard prior authorization letters, from <INSERT PBM NAME>’ standard library (when prior authorization services are purchased without customization). Section 2.03. Client Services. <INSERT PBM NAME> will assign to Client an account manager to direct Client’s pharmacy benefit program following implementation. The account manager, assisted by pharmacists and other <INSERT PBM NAME> personnel, will respond to general inquiries and requests from Client’s benefit group and will provide general support and consultative services related to Plan design, Covered Products utilization and charges, Participating Pharmacy network changes, Eligible Person communications and Formulary management and support. Section 2.04. Customer Service Call Centers. <INSERT PBM NAME> will maintain call centers, which will be accessible through a toll-free telephone line, responsible for responding to inquiries from Participating Pharmacies, other providers, and Eligible Persons regarding the services provided by <INSERT PBM NAME> under this Agreement. Call center personnel will respond to questions related to eligibility of individuals, Plan Guidelines, Deductible status, Coinsurance and Co-payment levels, maximum benefit status, direct reimbursement, and in the case of Participating Pharmacies, online adjudication instruction. <INSERT PBM NAME>’ toll-free help line shall be available to Client and all Participating Pharmacies and Providers during <INSERT PBM NAME>’ regular hours of business. <INSERT PBM NAME> customer service will be available twenty-four hours a day, seven days a week, excluding Christmas Day and Thanksgiving Day. <INSERT PBM NAME> reserves the right to change such hours of operation and <INSERT PBM NAME> shall notify Client and the Participating Pharmacies prior to any such changes; provided that any such changes will comply with applicable law. Section 2.05. Cardmember Materials. <INSERT PBM NAME> will provide and mail an identification card for each Cardmember, unless provided by a third party designated by Client or by Client directly. If Client elects to use a third party to provide the identification card or to provide it directly, the cost will be the responsibility of the Client. <INSERT PBM NAME> will also provide Direct Reimbursement Claim forms. Section 2.06. Pharmacy Network. <INSERT PBM NAME> has created and will maintain a network of Participating Pharmacies that will perform pharmacy services for Eligible Persons according to their Participating Pharmacy agreement. Although the composition of the Participating Pharmacy network may change due to the addition or

withdrawal of specific Participating Pharmacies, <INSERT PBM NAME> will use commercially reasonable efforts to ensure that the network includes Participating Pharmacies such that the network will provide reasonable access and availability to the Eligible Persons. (a) Listing of Participating Pharmacies. <INSERT PBM NAME> will make available an up-to-date list of Participating Pharmacies in its network on-line via its website. In addition, <INSERT PBM NAME> shall make printed versions of the list of Participating Pharmacies or relevant portions of the list available upon request to Eligible Persons through its Customers Service Call Center representatives.
(b) Mail Service. Upon Client’s request, <INSERT PBM NAME> will provide Client a mail service program through which the Mail Service Pharmacy will fill prescriptions for Eligible Persons and will mail such prescriptions to Eligible Persons subject to the terms set forth in Exhibit 2.
(c) Specialty Pharmacy. Upon Client’s request, <INSERT PBM NAME> will provide Client a Specialty Pharmaceutical program which provides a distribution channel for certain Covered Products that are generally biotechnological in nature, are given by injection, or otherwise require special handling. The Specialty Pharmacy will dispense Specialty Pharmaceuticals to Eligible Persons subject to the terms set forth in Exhibit 2.
(d) Pharmacy Audits. <INSERT PBM NAME> shall maintain a pharmacy audit program, the criteria of which may be amended from time to time. The audit may be conducted by <INSERT PBM NAME>' internal auditors or its outside auditors at the Participating Pharmacy or at <INSERT PBM NAME> by a review of electronically submitted Claims. Any overpayments made to a Participating Pharmacy attributable to Client's Claims will be offset against future payments to that Participating Pharmacy or Non-Participating Pharmacy from Client's account. If offset is not available, then any overpayment recovered from the Participating Pharmacy will be promptly remitted to Client. <INSERT PBM NAME> will promptly use commercially reasonable efforts to recover any overpayment from a Participating Pharmacy or Non-Participating Pharmacy. <INSERT PBM NAME> will not be required to commence any litigation to recover any such overpayments if, in <INSERT PBM NAME>’ reasonable discretion, it deems such actions not to be economically feasible. In addition, if <INSERT PBM NAME> commences litigation to recover such amounts, then all expenses incurred by <INSERT PBM NAME> with regard to such litigation may be offset against any amounts recovered.
Section 2.07. Claim Processing. (a) General. <INSERT PBM NAME> will process Claims with dates of fill on or after the Effective Date, through and including Claims with dates of fill prior to the termination of this Agreement. <INSERT PBM NAME> will process all Claims according to the Prescription Pricing Schedule in Exhibit 2, Client’s Plan Guidelines and HIPAA-required transaction code sets. Notwithstanding the foregoing, if Client requests that <INSERT PBM NAME> encourage a pharmacy to become a Participating Pharmacy by offering such pharmacy reimbursement rates that exceed the rates set forth in Exhibit 2, then <INSERT PBM NAME> shall use such revised reimbursement rates for such pharmacy; provided, however, <INSERT PBM NAME> may refuse to add pharmacies to its network if they do not meet <INSERT PBM NAME>’ minimum credentialing criteria or are owned by, or under common control with, a direct competitor of <INSERT PBM NAME>. <INSERT PBM NAME> will review all contractual Claims transmitted by Participating Pharmacies and notify such providers on-line of the reason or reasons for denial of such Claims, including, but not limited to missing or erroneous information. Likewise, <INSERT PBM NAME> will report to submitting persons the status of all denied Direct Reimbursement Claims in accordance with ERISA rules and regulations. Client will maintain an appeals process for review of Claims that have been denied by <INSERT PBM NAME> and appealed by an Eligible Person after such Eligible Person has exhausted available appeals processes maintained by <INSERT PBM NAME>. Subject to the terms and conditions herein, Client shall make the final determination regarding payment of all submitted Claims. Additionally, if Client notifies <INSERT PBM NAME> that an Eligible Person has a primary insurer other than the Plan, then <INSERT PBM NAME> will pay Claims for such Eligible Person as a secondary payor rather than as a primary payor. <INSERT PBM NAME> does not assume responsibility for establishing coordination of benefits filing order for subsequent coverages,

nor responsibility for coordination of benefits investigational efforts, subrogation, or coordination with Worker’s Compensation.
Client hereby delegates to <INSERT PBM NAME> the authority, responsibility and discretion to (i) determine eligibility and enrollment for coverage under the Plan according to the information provided by the Client; (ii) make factual determinations and to interpret the provisions of the Plan to make coverage determinations on claims for Plan Benefits;(iii) conduct a full and fair review of each claim which has been denied as required by ERISA; (iv) conduct the initial level of appeal determinations for all “Urgent Care,” “Concurrent,” “Pre-service,” and “Post-service” claims (as those terms are defined in ERISA) and notify the Eligible Person or the Eligible Person’s authorized representative of its decision. Client shall conduct final level(s) of appeal determinations for all “Urgent Care,” “Concurrent,” “Pre-service,” and “Post-service” claims (as those terms are defined in ERISA) upon request by the Eligible Person following the initial appeal determination. Client will ensure that all summary plan description materials provided to Eligible Persons reflect this delegation.
(b) Direct Member Reimbursement. Upon request, <INSERT PBM NAME> will provide an Eligible Person with a <INSERT PBM NAME>-approved claim form that must be used when submitting a Claim for reimbursement for Covered Products provided by a Participating or Non-Participating Pharmacy. When such a Claim is submitted on the approved form, <INSERT PBM NAME> will process the Claim according to the Plan Guidelines and in the amount approved by the Client for payment. The Claim forms should be sent to: <INSERT PBM NAME> with addresses at <INSERT PBM ADDRESS>, or such other address designated by <INSERT PBM NAME> upon written notice.
Section 2.08. Collection of Deductible, Co-payment, or Coinsurance by Pharmacies. <INSERT PBM NAME> will contractually require Participating Pharmacies to collect from Eligible Persons or their representatives the amount of any applicable Coinsurance, Co-payment, or Deductible communicated by the online adjudication processing system prior to providing such persons any Covered Products to which such Eligible Person is or may be entitled. <INSERT PBM NAME> also will contractually require Participating Pharmacies to agree not to recover from Eligible Persons any unpaid balances due from <INSERT PBM NAME> and/or the Plan. Section 2.09. Client Claims File. <INSERT PBM NAME> will provide Client with an electronic file in <INSERT PBM NAME> standard format of all paid Claims for the Client prescription drug program on a quarterly basis or such other time frame agreed upon by the parties. Such data may also be provided from time to time, at the request of Client, to a Client designee for purposes of assisting in the implementation and management of disease management programs or other programs desired by Client. Section 2.10. Clinical and Other Services. <INSERT PBM NAME> in partnership with District Consultant will provide Client and its Eligible Persons certain clinical and ancillary services to facilitate Eligible Persons’ appropriate utilization of Covered Products. (a) Concurrent Drug Utilization Review. <INSERT PBM NAME> in partnership with District Consultant will provide concurrent on-line drug utilization review to Participating Pharmacies for all Claims submitted on-line. Participating Pharmacies transmitting Claims will receive advisory messages identifying potential drug interactions and other circumstances, which may be indicative of inappropriate drug utilization.
(b) Retrospective Drug Utilization Review. <INSERT PBM NAME> in partnership with District Consultant will retrospectively review previously approved Claims for potential fraud or abuse, and clinical appropriateness. <INSERT PBM NAME> in partnership with District Consultant will analyze Eligible Persons’ drug profiles and review one or more specific therapeutic categories or issues. Automatic algorithms will be employed to identify Eligible Persons receiving the profiling and targeted drug therapy. <INSERT PBM NAME> also will contact Practitioners and Participating Pharmacies as needed to discuss therapeutic issues and to offer suggestions for alternative therapy.
(c) Treatment Alternatives. Client agrees that consistent with the HIPAA Privacy Rule, <INSERT PBM NAME> in partnership with District Consultant may contact Eligible Persons to provide refill reminders or information about treatment alternatives, including, but not limited to, Brand and Generic drugs, or other health-related benefits and services that may be of interest to such Eligible Persons. In connection with these services, <INSERT PBM NAME> in partnership with District Consultant also may provide Participating Pharmacies and Practitioners information, electronic messaging, and communications about such alternatives and services. Client further agrees that Participating Pharmacies and Practitioners may contact Eligible Persons regarding refill reminders or information about treatment alternatives, provided that such action is not inconsistent with applicable medical standards of care or any limitation imposed by applicable law.
(d) Prior Authorizations. <INSERT PBM NAME> will, as required by Client, confirm with Practitioners whether certain Covered Products are prescribed for medical conditions consistent with FDA-approved indications and labeling. In providing any or all such services, <INSERT PBM NAME> may rely upon information provided by the Eligible Person or such person’s representative, the Practitioner, the dispensing pharmacist and other sources deemed reliable by <INSERT PBM NAME>. <INSERT PBM NAME> will not determine medical necessity or appropriateness of treatment, although <INSERT PBM NAME> may rely upon protocols established and maintained by its Pharmacy and Therapeutics Committee (consisting of pharmacists and physicians) based upon factors such as safety, availability, potential for misuse and cost in its review of Claims submitted for payment of such prescription drugs. The standard <INSERT PBM NAME> prior authorization list will be made available to Client along with <INSERT PBM NAME>-approved criteria for use. This list may change from time to time based upon the clinical determination of the <INSERT PBM NAME> Pharmacy and Therapeutics Committee and such changes will be communicated in advance to Client. Any customization or additions to the standard <INSERT PBM NAME> Prior Authorization list may result in additional fees payable to <INSERT PBM NAME> by the Client. <INSERT PBM NAME> will notify Client of the anticipated amounts of such additional fees, which will be reasonably determined promptly following receipt of Client’s request for such customizations or additions, and the parties will negotiate in good faith regarding changes to the list and any accompanying additional fees. Client acknowledges that <INSERT PBM NAME> may suspend processing of Claims for Covered Products subject to Prior Authorization in the event the Practitioner fails to provide missing information necessary for the processing of such Claims in compliance with such protocols.
(e) Formulary Management. <INSERT PBM NAME> in partnership with District Consultant shall provide a recommended drug formulary to Client. Client agrees to implement, administer, and cooperate with <INSERT PBM NAME> and to facilitate Eligible Persons’ utilization of the Formulary.
(f) Formulary Support Programs. <INSERT PBM NAME> in partnership with District Consultant will offer Client Formulary support programs intended to assist in the transition of Client’s Eligible Persons from their current drug utilization mix to a new mix of utilized products that are therapeutically equivalent and are better aligned with the <INSERT PBM NAME> Formulary.
(g) Treatment Decisions. Subject to Client’s Plan Guidelines and the Prior Authorization process set forth in this Agreement, the decisions, in all circumstances, to prescribe and dispense any prescription drug shall be made solely by the prescribing physician or health care provider and the dispensing pharmacist, respectively. A Participating Pharmacy will not be deemed to be a representative, subcontractor, or agent of <INSERT PBM NAME> or Client based solely on this Agreement.
(h) Ninety Day at Retail. <INSERT PBM NAME> will provide Client, should it so choose in Exhibit 2, a ninety (90) day at retail program through which retail pharmacies will fill prescriptions for Eligible Persons subject to the terms set forth in Exhibit 2.
(i) Additional Services. In the event that Client requests <INSERT PBM NAME> to provide services other than those described herein including, but not limited to, special research projects, reports, consultative services (e.g., HIPAA compliance consultation), <INSERT PBM NAME> system changes to accommodate changes in Client’s pharmacy program

or system, or other tasks to be specifically performed for or on behalf of Client, Client shall pay to <INSERT PBM NAME> an additional charge as set forth in Exhibit 1 or as otherwise mutually agreed upon by the parties in writing before the services are provided. Section 2.11. Eligibility and Claim Files. <INSERT PBM NAME> will establish and maintain claim and eligibility files related to Eligible Persons and their Covered Product utilization. Maintenance of eligibility files (additions, terminations and updates) will be performed within two business days of <INSERT PBM NAME>’ receipt of Client’s submission of such additions, terminations, and updates to files, provided that the information received from Client conforms with the specifications for such information reasonably requested by <INSERT PBM NAME>. Until expiration of such time period, Client will remain responsible for all Claims submitted on behalf of such affected individuals. Section 2.12. Core Reports. <INSERT PBM NAME> shall prepare and deliver to Client core reports no later than 30 days from the close of the month or quarter, as applicable. Client will receive <INSERT PBM NAME>' Standard Report Package. “<INSERT PBM NAME> Standard Report Package” will include reports and data files generally available to <INSERT PBM NAME>’ clients, with information necessary for Client to manage and oversee its Plan. Additional or customized reports shall incur costs to Client as described in Exhibit 1. Upon receipt of Client’s request for an ad hoc report, the parties will negotiate in good faith to agree on a due date for such ad hoc report.
Article III CLIENT RESPONSIBILITIES
Section 3.01. Plan and Other Information. Client agrees to provide <INSERT PBM NAME> all information reasonably required by <INSERT PBM NAME> to fulfill its duties and obligations under this Agreement. Client agrees to review and analyze information provided by <INSERT PBM NAME> in a timely fashion and notify <INSERT PBM NAME> of any errors or omissions. Client represents and warrants that all information provided shall be true, accurate and complete and consistent with the Plan benefits available to Eligible Persons. <INSERT PBM NAME> may rely on all information provided by Client in providing services hereunder. Section 3.02. Plan Guidelines. Client represents and warrants that its Plan Guidelines are true, accurate and complete descriptions of the pharmacy benefits available to Eligible Persons and acknowledges its status as the plan administrator for purposes of this Agreement. Client shall retain its discretionary authority to manage, control and interpret its Plan and may, at any time, alter or amend the Plan Guidelines, provided, Client notifies <INSERT PBM NAME> in writing of all such changes not less than 30 days prior to the effective date of any changes. <INSERT PBM NAME> will advise Client of the anticipated implementation dates of the proposed benefit changes, and the benefits that are implemented shall be deemed incorporated into this Agreement as of the date of implementation. Charges, as agreed upon by <INSERT PBM NAME> and Client in writing, for programming to implement any customized edits shall be borne by Client unless otherwise agreed by the parties. If Client modifies its Plan Guidelines in a manner that materially affects <INSERT PBM NAME>’ duties, obligations or cost of performance under this Agreement, then at the request of <INSERT PBM NAME>, the parties will work toward a mutually acceptable modification of this Agreement, including, but not limited to, adjustments to the administrative charges in Exhibit 1 or the Prescription Pricing Schedule in Exhibit 2 of this Agreement. If Client and <INSERT PBM NAME> are unable to agree upon mutually acceptable modifications of this Agreement, then a final and binding decision on the modifications shall be made by a third party acceptable to both parties. Section 3.03. Eligibility. Client represents that each individual’s eligibility for benefits is determined by reference to criteria in its Plan. Client will provide <INSERT PBM NAME> eligibility information identifying each individual eligible for pharmacy benefits under Client’s Plan. Such information shall include all information identified by <INSERT PBM NAME> so as to enable <INSERT PBM NAME> to process Claims in accordance with HIPAA and shall be provided in a mutually acceptable format. Client will provide <INSERT PBM NAME> regular updates of subsequent changes in enrollment, including, but not limited to, changes in eligibility status, additions and deletions of Eligible Persons, and termination of benefits, together with the effective date of any such changes if such changes occur after the effective date of this
Agreement. If Client retroactively changes an Eligible Person’s status under the Plan, Client shall be responsible for payment of all Claims related to such Eligible Person that are processed prior to <INSERT PBM NAME> processing the notification of the retroactive termination. Section 3.04. Eligible Person Authorizations and Consents. Client represents and warrants that it has or shall obtain the Eligible Persons’ consents and authorizations if required for the services provided in connection with this Agreement and for Protected Health Information to be released to Client if so required. Section 3.05. Contract Administrator. If Client appoints a Contract Administrator, Client represents and warrants that the Contract Administrator is and shall be authorized to act as Client’s agent and representative on any and all matters in connection with this Agreement, including, but not limited to (a) additions, deletions, and modifications of eligibility listings provided to <INSERT PBM NAME>; (b) payment to <INSERT PBM NAME> of claims, services and fees; (c) plan design and coverage decisions; and (d) the provision and receipt of contractually required or permitted notices. Client acknowledges and agrees that <INSERT PBM NAME> shall be entitled to rely upon any and all such acts and omissions by Contract Administrator and, further, that any and all such acts and omissions shall be binding upon Client.
Article IV FORMULARY PROGRAM AND REBATES
Section 4.01. Cooperation. Client agrees to approve the Formulary and to allow <INSERT PBM NAME> to communicate with, and make available, Formulary-related literature to, Participating Pharmacies, Practitioners and Eligible Persons. Client agrees to cooperate with <INSERT PBM NAME> in the maintenance of the Formulary and to facilitate Eligible Persons’ utilization of the Formulary. Section 4.02. Rebate Submissions. Client further agrees that, consistent with the HIPAA Privacy Rule, <INSERT PBM NAME> will submit Eligible Persons’ Protected Health Information to pharmaceutical manufacturers in exchange for Rebates. Client acknowledges that Rebates are intended to be paid only once by manufacturers on Covered Product utilization and agrees not to participate in any other formulary, Rebate or discount program related to Covered Product utilization by Eligible Persons in connection with this Agreement. Client agrees that if any manufacturer’s audit reveals that Client has submitted Covered Product utilization in a duplicitous manner to pharmaceutical manufacturers for purposes of Rebates or calculating Rebates, then Client shall be solely responsible for the reimbursement of any Rebates improperly made based on such utilization and <INSERT PBM NAME> may terminate Client’s participation in the Rebate program. Section 4.03. Rebate Calculations. <INSERT PBM NAME> will calculate Client’s share of Rebates on Covered Products. Client’s share of Rebates will be in proportion to its pharmacy utilization of Covered Products as compared to all other <INSERT PBM NAME> clients with similar Plans, and as specified by the criteria established by the pharmaceutical manufacturer. Client will then be eligible to elect between the following rebate payment options:
1. ____ Elect to receive 100% of the specified manufacturer dollars received by <INSERT PBM NAME> specific to Client’s claims utilization on a pass-through basis per the standard turnaround timeline. <INSERT PBM NAME>’ payment to Client for Rebates will be on a quarterly basis and will include Client’s portion of any Rebates collected and validated for accuracy during the applicable calendar quarter. <INSERT PBM NAME> agrees to pay Client its portion of received rebates within 30 business days following the end of each calendar quarter in which such amounts are received, after final audit and validation of accuracy. Client acknowledges and agrees that it will not have a right to interest on any Rebate payments received by <INSERT PBM NAME>, or to other manufacturer monies received by <INSERT PBM NAME> and not directly attributable to Covered Product utilization of Eligible Persons. Amounts due and owing Client in connection with such Rebates may be offset by <INSERT PBM NAME> against Client’s overdue, outstanding balances; or,
2. ____ Elect to instruct <INSERT PBM NAME> to reinvest the total sum of all expected rebates at point of
sale, buying down pharmacy discounts which result in lower point of sale pharmacy costs to the member;
Any claims for which <INSERT PBM NAME> is unable to submit and collect rebates (e.g. 340B, GPO pricing, hospital or government pharmacies), including any claims that may qualify for rebates under any government program (e.g. Managed Medicaid rebate discounts), are not eligible for Rebates. Claims submitted directly by Eligible Persons may not be eligible for Rebates. Client acknowledges that its eligibility to receive payments for Rebates may change over time due to changes in laws governing prescription drug pricing (including Rebates), or changes in <INSERT PBM NAME>’ contracts with pharmaceutical manufacturers. Client agrees that <INSERT PBM NAME> shall not have any liability or obligation to Client or its Eligible Persons for any failure by any manufacturer to pay any Rebates, any breach of an agreement related to the transactions contemplated by this Agreement by any manufacturer, or any negligence or willful misconduct of any manufacturer.
Article V COMPENSATION; CLAIMS BILLINGS AND PAYMENTS
Section 5.01. Compensation. Client acknowledges that it has had an opportunity to review <INSERT PBM NAME>’ qualifications and services in relation to the marketplace and Client’s Covered Product expenditures and has determined the reasonableness of <INSERT PBM NAME>’ compensation in connection with the services provided under this Agreement. Client further acknowledges and agrees that <INSERT PBM NAME>, and third parties contracted to <INSERT PBM NAME>, may retain interest earnings not in excess of market rates pending clearance of electronic transfers and checks in connection with the payment of Covered Product claims under this Agreement. Section 5.02. Payments to <INSERT PBM NAME>. Client agrees to pay <INSERT PBM NAME> the administrative charges as set forth in Exhibit 1 to this Agreement. Client also agrees to fund the payment of Covered Product Claims in accordance with the Prescription Pricing Schedule in Exhibit 2 to this Agreement and all applicable gross receipts, provider, sales, use and similar taxes. Client assumes all financial responsibility for funding the payment of Covered Product Claims submitted to <INSERT PBM NAME> with regard to Client’s Eligible Persons, whether by Participating Pharmacies or Eligible Persons. <INSERT PBM NAME> will invoice Client for Claims at the amount <INSERT PBM NAME> pays for those Claims. (a) Timing of Payment. <INSERT PBM NAME> will submit invoices to Client between seven and ten days after the end of each invoice cycle, and Client agrees to pay <INSERT PBM NAME> for amounts owed thereunder within five business days after the date of invoice. Alternatively, upon Client’s request and <INSERT PBM NAME>’ consent, Client may advance to, and maintain with, <INSERT PBM NAME> an amount equal to the sum of one month's estimated Covered Product Claims and one month's estimated administrative charges not later than 15 days prior to the Effective Date of this Agreement. If Client maintains such an amount with <INSERT PBM NAME>, payment in full will be due 15 days after the date of invoice, instead of five days from the date of the invoice as set forth above.
(b) Payment Methodology. The parties will cooperate in good faith to establish a mutually agreed upon methodology for ACH transfers related to payments as identified by Client during implementation of the services hereunder where either Client or <INSERT PBM NAME> will initiate ACH transfers from Client’s account to <INSERT PBM

NAME> when due. Client shall be solely responsible for depositing funds and verifying that the account has sufficient funds to pay Covered Product Claims and <INSERT PBM NAME>' administrative charges. Client acknowledges and agrees that <INSERT PBM NAME>' account(s) into which money from Client's bank account is transferred is no longer a Plan asset. Client agrees that <INSERT PBM NAME>. Section 5.03. Failure to Make Funds Available. In the event that for any reason funds are not available on the date due and Client fails to provide the required funds within three business days after that failure is brought to the attention of Client, <INSERT PBM NAME> may terminate this Agreement immediately and may provide notice of such termination to Participating Pharmacies and Eligible Persons. In the event that Client has at any time failed to make funds available to pay claims for Covered Products or has failed to pay 2%to <INSERT PBM NAME>, in addition to any other remedies, <INSERT PBM NAME> will have the right to offset any unpaid amounts against any amounts owed to Client by <INSERT PBM NAME>, or any entity affiliated with <INSERT PBM NAME>.
Section 5.04. Collections; Interest. Client shall be responsible for all costs and expenses of collection of amounts due from Client to <INSERT PBM NAME>, and enforcement of judgments, and agrees to reimburse <INSERT PBM NAME> for such costs and expenses, including reasonable attorneys’ fees. Any amounts not paid by the due date thereof shall bear the interest rate of 6% per annum; however, this interest rate shall not exceed the maximum rate allowed by applicable laws. The rights and remedies set forth in this paragraph are in addition to other rights and remedies available to <INSERT PBM NAME> under law or in equity. Section 5.05. Performance Guarantees. Final compensation to <INSERT PBM NAME> may be adjusted based upon assessments incurred for failure to meet performance guarantees as described in Exhibit 3. Unless otherwise set forth in Exhibit 3, <INSERT PBM NAME> shall provide a report to Client on all applicable performance guarantees on a quarterly basis, no later than one month after the end of each quarter; however, assessments for any failure to meet a performance guarantee shall be determined on an annual basis, based on the average of the results reported quarterly.
Article VI TERMINATION
Section 6.01. Mutual Agreement. This Agreement may be terminated at any time by mutual written consent of the parties. If Client terminates this Agreement prior to the end of the then-current term, then Client shall pay <INSERT PBM NAME> and District Consultant an amount equal to fees set forth in Exhibit 1. Section 6.02. For Cause. (a) Either Client or <INSERT PBM NAME> may terminate this Agreement, at any time, upon not less than 90 days’ written notice if: (1) the other party makes an assignment for the benefit of creditors, is the subject of a voluntary or involuntary petition for bankruptcy or is adjudged to be insolvent or bankrupt, or a receiver or trustee is appointed for any portion of its property; or (2) the other party commits a Material Breach of this Agreement, unless the breach is cured prior to the expiration of such notice; or (3) a change in law occurs, as provided in Section 11.08 of this Agreement. (b) <INSERT PBM NAME> may terminate this Agreement immediately, in accordance with Section 5.03 of this Agreement. Section 6.03. Effect of Termination; Other Remedies. Termination of this Agreement shall not affect Client’s financial responsibility for Covered Product claims and <INSERT PBM NAME>’ administrative charges pertaining to the period prior to termination. A party’s right to terminate this Agreement shall not be exclusive of any other remedies available to such party under this Agreement, at law or in equity.
Section 6.04. No Consent; Notice to Third Parties. This Agreement may be terminated without the consent of, or notice to, any Eligible Person, any Participating Pharmacy or other third parties. Notwithstanding the foregoing, <INSERT PBM NAME> may advise Participating Pharmacies and pharmaceutical manufacturers of a pending or actual termination of this Agreement. Section 6.05. Run-Out Period. Client shall continue to assume full responsibility for the funding of Covered Product Claims incurred prior to the effective date of termination of this Agreement and for the payment of <INSERT PBM NAME>’ administrative charges. Client’s obligation for payment for these services will continue as long as claims are being processed by <INSERT PBM NAME>, not to exceed a run-out period of 90 days on the effective date of termination. Administrative service fees for the run-out period will be based on per-transaction charges, calculated on the basis of the actual transactions related to the actual administrative service fees incurred in the last full month prior to the termination of this Agreement. <INSERT PBM NAME> will return to Client any unapplied deposits, overpayments or advances previously received from Client within 30 days following such run-out period.
Article VII LIABILITY, INDEMNIFICATION, AND WARRANTY
Section 7.01. Limited Warranty. <INSERT PBM NAME> warrants that it will perform the services described in this Agreement in accordance with the practices and standards generally established in the pharmacy benefits management industry. <INSERT PBM NAME> guarantees that Claims will be processed with at least 95% accuracy based upon number of Claims processed. Except as expressly set forth herein, <INSERT PBM NAME> makes no representation or warranty of any kind whatsoever, express or implied, and expressly disclaims any and all such warranties, including, but not limited to, any implied warranties of merchantability or fitness for a particular purpose with respect to the products or services provided hereunder. <INSERT PBM NAME> does not warrant that its services will be uninterrupted or error free. Section 7.02. Role of the Parties. Client acknowledges that <INSERT PBM NAME> will administer Client’s Plan on behalf of Client. <INSERT PBM NAME> does not underwrite or insure liability of Client in connection with its prescription drug benefits, and Client retains the ultimate responsibility and final authority for its Plan. For purposes of applicable state and federal legislation, Client is, and shall be deemed, the Plan sponsor of any applicable prescription drug benefit. Nothing in this Agreement is intended by the parties, or shall be construed, to confer upon <INSERT PBM NAME> the status of a fiduciary of Client or any benefit plan maintained by Client as “Plan fiduciary” is defined under applicable law. The parties agree <INSERT PBM NAME> is not a fiduciary, except to the extent <INSERT PBM NAME> exercises discretion with regard to the services provided hereunder. Section 7.03. Insurance. <INSERT PBM NAME> agrees, at its sole expense, to maintain commercial general liability insurance coverage in amounts not less than $1,000,000 per occurrence and $2,000,000 in aggregate. <INSERT PBM NAME> also agrees to maintain errors and omissions insurance with coverage of $5,000,000 in aggregate and security and data insurance with coverage of $5,000,000 in aggregate. Finally, <INSERT PBM NAME> warrants and represents that it has in place and will maintain any Workers' Compensation insurance required by applicable law. Section 7.04. Limitation of Liability for Covered Products. (a) Client agrees and acknowledges that the services provided by <INSERT PBM NAME> herein are not intended to substitute for or supplement the knowledge, expertise, skill, and judgment of physicians, pharmacists, or other health care professionals in prescribing or suggesting pharmaceuticals or other products.
(b) <INSERT PBM NAME> shall under no circumstances be liable (regardless of the basis for the action) to Client, any Eligible Person, or consumers of pharmaceutical products for any damages, injuries, losses, claims, costs, or lawsuits, including any attorney’s fees, arising from any actions, failure to act, or violations of any applicable standard of care or applicable law by pharmacies, pharmaceutical manufacturers, pharmaceutical distributors, or any health care providers

arising out of the sale, compounding, dispensing, manufacturing, or use of any prescription product or services in connection with this Agreement.
Section 7.05. Limitations of Liability. (a) In no event shall <INSERT PBM NAME>’ total liability for the entire term of this Agreement, regardless of the cause or form of action upon which any such liability is based, exceed the greater of:
(i) the amount of any applicable liability covered by <INSERT PBM NAME>’ insurance coverage or the actual and direct damages incurred by Client.
(b) In no event shall either party be liable to the other party for any indirect, special, incidental, consequential, or punitive damages or lost profits, arising out of, or related to, the performance of this Agreement or a breach of this Agreement, even if advised of the possibility of such damages or lost profits.
(c) Any claim for negligence or other tort liability arising out of, or related to, this Agreement, even if a breach is the result of acts or omissions that may arguably be characterized as negligence or other tortious conduct must be brought as a claim for breach of contract rather than as a claim for tortious conduct.
(d) Any controversy or claim arising out of, or relating to, this Agreement, regardless of the basis of the claim, must be filed within the applicable statute of limitations or one year after the date on which the factual basis for the claim arose, whichever time period is shorter. Failure to file such a claim within that time period shall bar a party from asserting that claim.
Section 7.06. Indemnification. Subject to the other limitations in this Article VII and in consideration of Client’s covenants, representations and warranties in this Agreement, <INSERT PBM NAME> agrees to indemnify, defend and hold Client harmless from any and all actions or claims arising from a material breach by <INSERT PBM NAME> of this Agreement. In consideration of <INSERT PBM NAME>’ covenants, representations and warranties in this Agreement, Client agrees to indemnify, save, defend and hold <INSERT PBM NAME> harmless from any and all actions or claims arising from (a) a material breach by Client of this Agreement; (b) Client’s plan design; (c) Client’s coverage decisions. <INSERT PBM NAME> also will not be responsible for the payment of fraudulent claims or filling of fraudulent prescriptions if the fraud is committed by an Eligible Person, or any party other than <INSERT PBM NAME>. The above indemnifications shall survive termination of this Agreement. A party seeking indemnification hereunder will promptly notify the indemnifying party of any claim subject to indemnification hereunder. Such party will reasonably cooperate with the indemnifying party in such defense.
Article VIII COMPLIANCE WITH LAW
Section 8.01. Compliance. <INSERT PBM NAME> agrees to comply with all applicable state and federal regulations, rules and laws, including, but not limited to, those related to the licensure and registration of third party administrators, HIPAA, and ERISA, if applicable to Client’s Plan. Client acknowledges that if its Plan is an employee welfare Plan for purposes of applicable state or federal law, Client is responsible for its own activities and duties (such as its duties as Plan Administrator) in connection with its Plan. Client acknowledges and agrees that it is responsible for disclosing to Eligible Persons all benefit information legally required to be disclosed, including information related to the calculation of Coinsurance, Co-payments, and Deductibles; coverages and exclusions; eligibility requirements; and Rebates it receives in connection with this Agreement. Client will not identify or represent <INSERT PBM NAME> as a Plan administrator or a named fiduciary of Client’s Plan as those terms are used in state or federal law. Section 8.02. Business Associate Agreement. The parties acknowledge that they have signed, or are signing contemporaneously with this Agreement, a Business Associate Agreement in compliance with HIPAA.

Article IX
RECORDS; CONFIDENTIALITY Section 9.01. Maintenance of Records; Audits. <INSERT PBM NAME> agrees that it will provide Client with access to all of its records; contracts with drug manufacturers; participating pharmacies, and any subcontractor and such other book and records as may be reasonably required to audit <INSERT PBM NAME> performance under this Agreement. <INSERT PBM NAME> agrees to maintain true and correct books and records of Client’s Covered Product expenditures in the standard <INSERT PBM NAME> format and for a period of not less than seven years from the date payment is made. Client may audit such books and records, using an auditor and methodology that is mutually agreed upon by the parties, upon reasonable prior written notice and during <INSERT PBM NAME>’ normal business hours consistent with privacy and other limitations of applicable federal and state laws, rules and regulations and the provisions of this Agreement; provided, however, that any claims against <INSERT PBM NAME> related to such audits must be made within six months of the termination of this Agreement. The parties shall require any third-party auditor to execute a confidentiality agreement in a form that is reasonably acceptable to both parties, and which contains provisions intended to protect each party’s Confidential Information that are substantially the same as the provisions set forth herein. Any release to the other party of records and data reviewed during such audit, whether electronically or in any other mutually agreeable format, will be in accordance with the terms of this Agreement and applicable law. Notwithstanding the foregoing, <INSERT PBM NAME> acknowledges that state and federal rules, regulations and laws will govern audits conducted by regulatory agencies with jurisdiction over Client’s Plan. Section 9.02. Use and Disclosure of Protected Health Information. Client acknowledges that Protected Health Information will be obtained by <INSERT PBM NAME> and such Protected Health Information will be obtained from and/or distributed to Client, Participating Pharmacies, the Mail Service Pharmacy, Specialty Pharmacies, and Eligible Persons’ Practitioners for drug utilization review and other purposes related to the services provided in connection with this Agreement. Subject to the remaining provisions of this Agreement and to the terms of the Business Associate Agreement, Client hereby permits <INSERT PBM NAME> to use and disclose such PHI in performance of its duties and obligations in connection with this Agreement. Client grants <INSERT PBM NAME> permission during and after the term of this Agreement to use de-identified Protected Health Information for quality improvement projects and the development of clinical programs. Such projects and programs may be included in services provided to prospective and existing clients. <INSERT PBM NAME> shall retain full ownership rights over all resultant data. Notwithstanding anything else in this Agreement, <INSERT PBM NAME> will not sell any PHI to any third party without Client’s permission. Section 9.03. Confidential Information. (a) Definition. "Confidential Information" means non-public information, in any form, medium, or format that a party disclosing the information (a “Disclosing Party”) discloses to another party hereunder (a “Receiving Party”) unless the Disclosing Party expressly designates such information as not being confidential. “Confidential Information” includes, without limitation: (i) financial, customer, product, technical, and business information, including, but not limited to, financial statements, strategic plans, intellectual property, customer lists and other customer information, marketing plans, business plans, product plans, software, forms, processes, strategies, service methods, personnel information, trade secrets, pricing and know-how; (ii) any confidential information of a third party used by, held by, or otherwise in the possession of a party; and (iii) any protected health information or other information protected by HIPAA or any other state or federal law. (b) Protection of Confidential Information. Client, District, District Consultant, and <INSERT PBM NAME> agree to take all reasonably necessary steps to protect and not to disclose the other party's Confidential information (as defined below) to any third party, during or after the termination of this Agreement, and shall not use the Confidential Information of another party hereunder, except (a) as specifically contemplated by this Agreement; (b) with the other's prior written consent; (c) as required by local, state or federal law, rule or regulation, including any judicial or

administrative interpretation thereof; or (d) to the extent such information becomes generally available to the public, through no action or fault of the Receiving Party. (c) Use after Termination. Client, District, District Consultant, and <INSERT PBM NAME> shall cease using the other parties' Confidential Information upon termination of this Agreement; provided, however, that District, District Consultant, and <INSERT PBM NAME> may retain records and use information as set forth herein, and each Receiving Party may retain Confidential Information for back-up, legal, and archival purposes, provided that such retained Confidential Information shall remain subject to the terms and conditions of this Agreement, and provided that the Confidential Information shall be destroyed or returned as soon as reasonably practicable. (d) Disclosures to Third Parties. Each Receiving Party shall not disclose or communicate, or permit the disclosure or communication of any such Confidential Information to any third party without the prior written consent of the Disclosing Party and a written agreement with such third party. Such written agreement will include terms substantially the same as those set forth in this Agreement. Each Receiving Party shall also take reasonable and prudent steps to avoid the inadvertent or intentional disclosure or misuse of any Confidential Information by any of its current or former directors, officers, employees, agents, or affiliates (“Representatives”); provided, however, that it may disclose Confidential Information to its Representatives for the sole purpose of complying with its obligations under this Agreement, subject to the confidentiality obligations herein.
(e) Injunctive Relief. Each party acknowledges that a breach or threatened breach of this Section of this Agreement may cause immediate and irreparable harm to the Disclosing Party. To protect against such harm, the Disclosing Party may seek from a court of competent jurisdiction the issuance of a restraining order or injunction to prohibit any threatened disclosure or misuse of the Disclosing Party’s Confidential Information. Such an action for a restraining order or injunction is in addition to and does not limit all other remedies provided by law or in equity or by agreement between the Parties.
(f) Ownership of Information. All Confidential Information is and shall remain the property of the Disclosing Party. Disclosure of Confidential Information by the Disclosing Party to the Receiving Party does not grant to the Receiving Party any express or implied right to the Disclosing Party’s Confidential Information.
(g) Legal Process. In the event a Receiving Party is served with any subpoena or other legal process requiring or purporting to require the disclosure of any Confidential Information of the Disclosing Party, the Receiving Party shall promptly notify the Disclosing Party in writing and shall reasonably cooperate with the Disclosing Party and its legal counsel so that the Disclosing Party may seek a protective order, confidential treatment or other appropriate remedy to the extent deemed appropriate by the Disclosing Party. If the Disclosing Party elects not to seek or is unsuccessful in obtaining any such protective order or other remedy, then the Receiving Party may disclose such Confidential Information to the extent legally required.
Section 9.04. Conflicts of Interest. Upon Client’s request and consistent with <INSERT PBM NAME>’ transparent business model, <INSERT PBM NAME> will share with Client: (a) the existence of organizational arrangements, if any, that could potentially create a conflict of interest in making clinical or financial decisions; (b) sources of revenue as they relate to the Client's contract; and (c) the pricing structure for pharmacy benefit management services including rebate structure and administrative fees.
Article X DISPUTE RESOLUTION PROCEDURES
Section 10.01. Resolution of Disputes. The parties agree to work in good faith toward resolution of disputes arising during the term of this Agreement. If they are unable to resolve the dispute through informal discussions, either party may submit a written objection to the other party describing and proposing a manner of resolving that dispute. The

party receiving such objection shall respond by accepting, rejecting, or modifying such proposal, in writing, within 30 days of the date that it receives the proposal. If the proposal is accepted, then the acceptance shall be deemed an agreement between the parties. If the proposal is rejected or modified, then the parties shall resume good faith efforts to resolve the dispute for a period of 30 days after notice of the rejection or modification is given. Except for actions requesting equitable relief, no lawsuit or other adverse proceeding may be commenced until expiration of that 30 day period. Section 10.02. Arbitration. If the parties are unable to resolve their dispute after complying with Section 10.01 above, then, as the exclusive means of resolving through alternative dispute resolution any disputes arising out of this Agreement, a party may demand that the dispute be resolved by arbitration administered by the American Arbitration Association in accordance with its commercial arbitration rules including provisions for interim relief, and each party hereby consents to the dispute being so resolved. Any arbitration hearings will be conducted in Texas or such other location mutually agreed upon by the parties. Judgment on any award rendered in any such arbitration may be entered in any court with competent jurisdiction over the party that is the subject of such action.
Article XI MISCELLANEOUS
Section 11.01. Notices. Communications in the ordinary course of performance of this Agreement, including communications regarding payment, may be conducted by any reasonable means, including, but not limited to, telephone, facsimile, or electronic mail. Any formal notice to be given in connection with this Agreement must be in writing and will be deemed to have been given and effective if and when sent by: (a) personal delivery or commercial courier; (b) certified or registered mail, return receipt requested with overnight or two-day guaranteed delivery, postage prepaid; (c) electronic mail message, where delivery is confirmed by recipient; or (d) a nationally recognized overnight delivery service, and addressed to:
<INSERT PBM NAME> Client: see signature page
Attn:
Phone:
Fax:
E-mail:
With a copy to: <INSERT PBM NAME> Attn: Either Client or <INSERT PBM NAME> may change its address for receipt of such notice by providing like written notice to the other party. Section 11.02. Entire Agreement. This Agreement, its Exhibits, the Plan Guidelines and any other documents incorporated by reference constitute the entire and complete understanding between the parties regarding the subject matter hereof and supersede all discussions, representations, proposals, offers, counteroffers, and writings between the parties that may have occurred before entering into this Agreement. There are no other agreements or undertakings, written or oral, in effect between the parties relating to the subject matter herein.

Section 11.03. Force Majeure. The performance obligations of <INSERT PBM NAME> or Client respectively hereunder shall be suspended to the extent that all or part of this Agreement cannot be performed due to causes that are outside the control of <INSERT PBM NAME> and/or Client. Without limiting the generality of the foregoing, such causes include acts of God, acts of a public enemy, acts of any person engaged in a subversive or terrorist activity or sabotage, wars, fires, floods, earthquakes, explosions, strikes, slow-downs, freight embargoes, market fluctuations, pricing generally available to <INSERT PBM NAME>, and comparable causes. The foregoing shall not be considered to be a waiver of any continuing obligations under this Agreement, and as soon as said conditions abate sufficiently to allow the resumption of operations, the party affected thereby shall fulfill its obligations as set forth under this Agreement. Section 11.04. Exclusivity. Client agrees that <INSERT PBM NAME> shall be the exclusive provider to the Client of the type of administrative services described in this Agreement. The Parties will mutually agree upon the Mail Service Pharmacy and Specialty Pharmacy, which will generally not include any entity owned by a direct competitor of <INSERT PBM NAME> unless otherwise agreed. Section 11.05. Intellectual Property. Except as expressly otherwise provided herein, <INSERT PBM NAME> retains all rights, title, and interest in and reserves the right to use and control the use of its intellectual property rights in its assets including, but not limited to, its software, reporting packages, user documentation, operations, procedures, and trademarks and service marks. Client agrees not to use any such items except as expressly allowed under this Agreement and also not to refer to <INSERT PBM NAME> or its trade name or marks in any publication without the prior written approval of <INSERT PBM NAME>. Section 11.06. No Third-Party Beneficiaries. This Agreement is not intended, and shall not be construed, to create third-party beneficiary rights in any person, including, but not limited to, any pharmacy or other provider or Eligible Person. Section 11.07. Governing Law. This Agreement shall be governed by and construed in accordance with applicable federal laws, rules and regulations, including PPACA, ERISA and HIPAA. To the extent such laws, rules and regulations do not apply or are not controlling, the internal laws of the State of Texas will govern all claims arising out of or relating to this Agreement regardless of the basis of any such claims. Section 11.08. Change in Law. In the event of any change in federal, state or local laws, rules or regulations, including any judicial or administrative interpretation thereof, which materially alters the rights, duties, obligations or cost of performance of either party under this Agreement, the parties will work in good faith toward mutually acceptable modifications of this Agreement, which may include, but are not limited to, changes in benefit design and drug coverage. To the extent that these modifications agreed to by the parties vary the cost of performance, the parties will negotiate in good faith toward the adjustment of the administrative charges to reflect this variation. If Client and <INSERT PBM NAME> have worked in good faith, but are unable to agree upon mutually acceptable modifications, then either Client or <INSERT PBM NAME> may terminate this Agreement upon not less than 60 days’ prior written notice. Section 11.09. Relationship of Parties. This Agreement is not intended, and shall not be construed, to create any relationship between Client and <INSERT PBM NAME> other than that of independent contractors. Neither Client nor <INSERT PBM NAME> shall be construed to be the agent, partner, employee, fiduciary or representative of the other, and neither party shall have the right to make any representations concerning the duties, obligations or services of the other except as consistent with the express terms of this Agreement or as otherwise authorized in writing by the other party. Section 11.10. Changes to Pricing Methodology. At any time during the term of this Agreement, upon an industry-wide event or industry-wide circumstance outside <INSERT PBM NAME>’ control that makes necessary or desirable a conversion of pricing methodology with respect to AWP and/or wholesale acquisition cost pricing and discounts, <INSERT PBM NAME> may request, upon 30 days’ notice to Client, to convert the pricing methodology used under this

Agreement and set forth in Exhibit 2, to another payment methodology that is economically equivalent, as reasonably determined by <INSERT PBM NAME>. However, if the nature of the industry-wide event or circumstance makes a 30 day notice unfeasible, <INSERT PBM NAME> shall give notice as soon as reasonably possible. <INSERT PBM NAME> shall review the need for the conversion, the details of the conversion, and its economic equivalency with Client, and shall not implement the conversion without the prior written approval of Client, which approval shall not be unreasonably withheld; provided, however, that <INSERT PBM NAME> may implement such change in pricing methodology, immediately, if it reasonably determines that there is no other way to process Claims hereunder. Section 11.11. Amendment; Waiver. This Agreement may be amended or modified solely through a writing signed by authorized persons on behalf of both parties. The failure of either party to insist upon the strict observation or performance of any term or provision of this Agreement or to exercise any right or remedy will not impair or waive any such right or remedy or constitute a waiver of any subsequent breach of the same term or provision or any other term or provision hereof. Section 11.12. Effect of Invalidity In the event a provision of this Agreement is rendered invalid or unenforceable by state or federal statute or regulations or declared null and void by any court or agency of competent jurisdiction, that provision will be deemed stricken, and the remaining provisions of this Agreement will remain in full force and effect. Section 11.13. Assignment. No party may assign or transfer its rights or obligations under this Agreement, in whole or in part, without the other party’s prior written consent, which shall not be unreasonably qualified or delayed. Any attempted assignment without that consent shall be void. Notwithstanding the forgoing, <INSERT PBM NAME> may assign this Agreement to any parent company or affiliate. Section 11.14. Construction. This Agreement will be construed and interpreted neutrally and without regard to the party that drafted it. The headings in this Agreement are used solely for the purpose of convenience and will not be considered in the construction of any provision in this Agreement.
ARTICLE XII NOTICE REGARDING AUTOMATIC RENEWAL
Section 12.01. Term of Agreement; Automatic Renewal. This Agreement is effective as of the Effective Date above and will continue in full force and effect for a period of three years (“Initial Term”). After the Initial Term has ended, this Agreement will continue from year to year (“Renewal Term”) unless sooner terminated as described in Article VI of this Agreement. Any additional Renewal Terms shall be subject to termination rights as otherwise provided in this Agreement. Section 12.02. Deadline and Action Required to Decline Renewal. This Agreement will not renew for a Renewal Term if Client notifies <INSERT PBM NAME> or <INSERT PBM NAME> notifies Client of its intent to renew this Agreement at least 180 days before the end of the then-current term. If declining renewal, Client shall notify <INSERT PBM NAME> in writing by (a) regular U.S. mail, registered or certified mail; (b) fax; (c) e-mail; or (d) recognized overnight courier service.
Section 12.03. Increase in Administrative Fees. As provided in Exhibit 1, “ADMINISTRATIVE SERVICES FEE SCHEDULE,” attached hereto, at the beginning of the second full year of the Agreement and at the beginning of each full year thereafter, whether in the Initial Term or a Renewal Term, the amount of the administrative charge may increase by zero to three percent for inflation and other business-related expenses. Section 12.04. Notice of Change in Administrative Fees. After the Initial Term or any Renewal Term for which administrative fees have been expressly set forth in this Agreement, <INSERT PBM NAME> may change the administrative fees hereunder upon not less than 90 days prior written notice to Client. If any revision in the administrative fees is not acceptable, then Client shall so notify <INSERT PBM NAME> in writing not less than 60 days

prior to the expiration of the 90-day notice period. In the event the parties cannot agree on the compensation adjustment on or before the expiration of the 90-day notice period, then Client may terminate this Agreement upon 60 days written notice to <INSERT PBM NAME>, provided such termination shall not be effective until after the end of the 90-day notice period. IN WITNESS WHEREOF, Client has acknowledged its understanding and agreement regarding the automatic renewal notice above, and the parties have entered into this Agreement on the day first written above.
<CLIENT> <INSERT PBM NAME>
By: By:
Name: Name:
Title: Title:
Variables: “Cardmember” will / will not [strike one] include retired employees. Contract Administrator: None or Name: ________________________________. Notices to Client (12.01): Attn: __________________________________ __ Address: _________________________________ _________________________________________ Phone: ___________________________________ Fax: _____________________________________ E-mail: ___________________________________

Exhibit 1 ADMINISTRATIVE SERVICES FEE SCHEDULE
Client authorizes <INSERT PBM NAME> to pay Smith and Associates a monthly administrative fee equal to 1% of Client’s calculated AWP for ongoing management of the District and delegated District Consulting Services, and when chosen by the member District a fee of 1% of the Client’s calculated AWP to the PBM consultant as defined here in. The administrative fee does not include fees for certain additional services provided by <INSERT PBM NAME>. <INSERT PBM NAME>’s administrative fee will include the following services, which are independent from the District and are outlined as follows:
Administrative Services Service Fee
Implementation & Plan Set-up
Pre-Implementation Claims Analysis
Pre-Implementation Guided Discovery
Requirements Approval Process
Dedicated Implementation Project Manager
Status and Communication Frequency - Weekly
Pre-Implementation and Go-Live Staffing
Dedicated and Secure Client Web Portal
Post-Implementation Review
Program Consultation and Customization
Standard Coordination of Benefits (COB)
Member Fulfillment
Member print materials, including postage
Individual Mailing of Welcome Letter
Pharmacy ID Card Replacement.
Claims Management
Point-of-Service Claims Processing
Direct Member Reimbursement (paper claims)
Manual Pharmacy-Submitted Claims Processing
Eligibility Management
Pharmacy Network Services
<INSERT PBM NAME> Network Management
Pharmacy Network Credentialing & Compliance
Mail Service Program Management
Specialty Program (<INSERT PBM NAME> SpecialtyRx) Clinical Management
Maximum Allowable Cost (MAC) Program Administration
Pharmacy Reimbursement
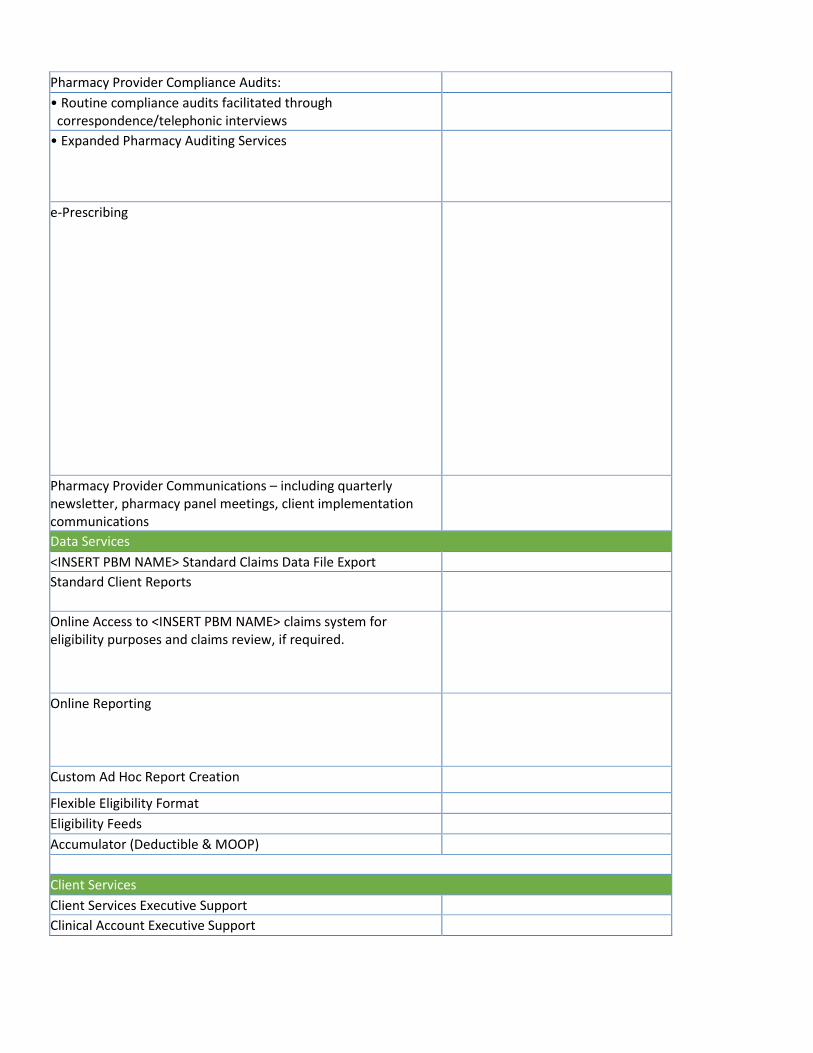
Pharmacy Provider Compliance Audits:
• Routine compliance audits facilitated through correspondence/telephonic interviews
• Expanded Pharmacy Auditing Services
e-Prescribing
Pharmacy Provider Communications – including quarterly newsletter, pharmacy panel meetings, client implementation communications
Data Services
<INSERT PBM NAME> Standard Claims Data File Export
Standard Client Reports
Online Access to <INSERT PBM NAME> claims system for eligibility purposes and claims review, if required.
Online Reporting
Custom Ad Hoc Report Creation
Flexible Eligibility Format
Eligibility Feeds
Accumulator (Deductible & MOOP)
Client Services
Client Services Executive Support
Clinical Account Executive Support

Consultative Review
Operational Meetings
Health Fair & Employee Meeting Support
Customer Care
Integrated Call Center with LIVE Representative Service: Member & Pharmacy Help Desk
Formulary and Rebate Services
<INSERT PBM NAME> Formulary Management
P&T Committee Review & Support
Pharmaceutical Manufacturer Contracting and Management
Safety, Drug Price and Volume Management
Online Concurrent DUR
Administrative/Non-Clinical Prior Authorization
Clinical Prior Authorization
Electronic Prior Authorization
ERISA Appeal Support for Claim re-determinations.
Prism Patient Management & Therapy Adherence $1.75 PMPM
Step Therapy Care and Quantity Limits
Retrospective DUR - Safety (RDUR)
• Controlled Substance Monitoring • Multi-Prescriber • Multi-Prescription • Expanded Fraud, Waste & Abuse • Duplicate Therapy

Exhibit 2 TRADITIONAL PRESCRIPTION PRICING SCHEDULE
Client acknowledges that the discount rates and dispensing fees set forth below are guaranteed discounts established for the pricing distribution channels necessary to meet access requirements. Client acknowledges that the pricing set forth below will be delivered to Client from the participating pharmacies. <INSERT PBM NAME> agrees to negotiate to achieve these guaranteed rates. Any discounts obtained by <INSERT PBM NAME> that exceed the targets stated below may be passed through to client or retained by <INSERT PBM NAME>. <INSERT PBM NAME> negotiates aggressive discounts with network pharmacies and rebates with pharmaceutical manufacturers on behalf of Client. <INSERT PBM NAME> may from time to time assess network fees and earn revenue from the pharmacies that participate in its network. <INSERT PBM NAME> will deliver the contracted discount to the participating pharmacy, which may be different than what has been contracted to the Client. The network guarantees are representative pharmacy reimbursement amounts (including AWP discount and MAC) and dispensing fees. Under the <INSERT PBM NAME> Traditional Prescription Pricing Schedule, Client pays the reimbursement rate (discounts and dispense fees) outlined in the Pricing Grid outlined below, less the Member copay or coinsurance. Guarantees represent the average performance of all participating pharmacies. AWP/WAC pricing for all Claims is based on the 11-digit National Drug Code (NDC) as of the date of service, and as reported and verifiable by Medi-Span, a national pricing source. Medi-Span is <INSERT PBM NAME>’ only source of drug pricing data and is utilized for all Claims adjudication. All guarantees are based on use of the <INSERT PBM NAME> Formulary and are subject to change in response to formulary and/or plan design changes. <INSERT PBM NAME> will manage the pharmacy network, will determine which pharmacies are to be included in the network, and will negotiate all pharmacy pricing and terms. Network participation will vary, and <INSERT PBM NAME> does not guarantee the number of participating pharmacies. As a result of various states’ most-favored nation Medicaid pricing formulas and historically premium status, various providers have negotiated region-specific pricing with <INSERT PBM NAME>. Claims originating from pharmacies subject to region-specific pricing may be excluded from network discounts and fees. Network discounts and fees may also exclude Claims originating from non-traditional providers, such as long-term-care pharmacies, home infusion providers, military pharmacies, rural pharmacies, Indian Tribal pharmacies, specialty pharmacies, pharmacies deemed by Client as necessary to include in the network but which do not meet <INSERT PBM NAME> discount or credential standards, and pharmacies that hold a direct agreement with Client. Network rates may be modified if more than 5% of Claims are incurred in Massachusetts, Georgia, Hawaii, Alaska, or Puerto Rico, or any U.S. Territory. Additional exclusions from retail network discounts include compound Claims, secondary Claims, 340B Claims, vaccination Claims, pharmaceutical care incentive (PCI) Claims (if applicable) and Member submitted Claims. Specialty guarantees are applicable for specialty pharmacy Claims originating at <INSERT PBM SPECIALTY PHARMACY> as the primary specialty pharmacy provider. <INSERT PBM SPECIALTY PHARMACY>. <INSERT PBM NAME> will deliver the entire value of the proposed network reimbursement terms pricing and manufacturer rebates set forth below. In accordance with Exhibit 2 Traditional Prescription Pricing Schedule, should a discount performance shortfall occur <INSERT PBM NAME> will pay dollar for dollar at 100% for any shortfall or missed performance guarantee. Retail 30 pricing applies to Claims between 1 and 83 days' supply, Retail 90 pricing applies to Claims greater than 83 days’ supply.

A. Network Rates. Reimbursement for each Branded Covered Product, not requiring compounding, dispensed by a
Participating Pharmacy will be based upon the lower of (1) AWP, less an average of the applicable percentage in the below table, plus an average dispensing fee of the applicable dispensing fee in the below table; (2) such pharmacy's Usual and Customary Price; or (3) the amount submitted by the pharmacy. Reimbursement for each Generic Covered Product dispensed by a Participating Pharmacy will be the lower of (1) the <INSERT PBM NAME> MAC plus a dispensing fee, if applicable; (2) each Participating Pharmacy’s respective contracted price for such Covered Product, including a discount plus a dispensing fee; (3) such pharmacy's Usual and Customary Price; or (4) the amount submitted; The average effective discount performance for generic Covered Product is AWP minus the applicable percentage in the below table plus an average dispense fee of the applicable dispensing fee in the below table.
B. Rebates. <INSERT PBM NAME> guarantees that during the Initial Term of the Agreement rebates per Brand Claim will meet the following guarantees:
Pharmaceutical Manufacturer Rebates - Traditional Year One Year Two Year Three
Minimum Retail Per Brand Guarantee
Minimum Retail 90 Per Brand Guarantee
Minimum Mail Order Per Brand Guarantee
Minimum Specialty Per Brand Guarantee
Pharmacy Network Pricing Proposal - Traditional Year One Year Two Year Three
Retail 30 Generic Guaranteed Discount
Retail 30 Generic Guaranteed Dispensing Fee
Retail 30 Brand Guaranteed Discount
Retail 30 Brand Guaranteed Dispensing Fee
Retail 90 Generic Guaranteed Discount
Retail 90 Generic Guaranteed Dispensing Fee
Retail 90 Brand Guaranteed Discount
Retail 90 Brand Guaranteed Dispensing Fee
Mail Order Generic Guaranteed Discount
Mail Order Generic Guaranteed Dispensing Fee
Mail Order Brand Guaranteed Discount
Mail Order Brand Guaranteed Dispensing Fee
Specialty Generic Guaranteed Discount
Specialty Generic Guaranteed Dispensing Fee
Specialty Brand Guaranteed Discount
Specialty Brand Guaranteed Dispensing Fee

Rebate Guarantees and Expected performance are on a per Brand Claim basis.
C. Re-Invested Rebate Network Rates. If Client selects the option of Reinvesting rebates into increasing network discount guarantees, Client will
not receive individual rebate payments, and will instead be accountable to the following considerations: a. Reimbursement for each Branded Covered Product, not requiring compounding, dispensed by a
Participating Pharmacy will be based upon the lower of (1) AWP, less an average of the applicable percentage in the below table, plus an average dispensing fee of the applicable dispensing fee in the below table; (2) such pharmacy's Usual and Customary Price; or (3) the amount submitted by the pharmacy. Reimbursement for each Generic Covered Product dispensed by a Participating Pharmacy will be the lower of (1) the <INSERT PBM NAME> MAC plus a dispensing fee, if applicable; (2) each Participating Pharmacy’s respective contracted price for such Covered Product, including a discount plus a dispensing fee; (3) such pharmacy's Usual and Customary Price; or (4) the amount submitted; The average effective discount performance for generic Covered Product is AWP minus the applicable percentage in the below table plus an average dispense fee of the applicable dispensing fee in the below table.
Pharmacy Network Pricing Proposal – Traditional / REINVESTED REBATES
Year One Year Two Year Three
Retail 30 Generic Guaranteed Discount
Retail 30 Generic Guaranteed Dispensing Fee
Retail 30 Brand Guaranteed Discount
Retail 30 Brand Guaranteed Dispensing Fee
Retail 90 Generic Guaranteed Discount
Retail 90 Generic Guaranteed Dispensing Fee
Retail 90 Brand Guaranteed Discount
Retail 90 Brand Guaranteed Dispensing Fee
Mail Order Generic Guaranteed Discount
Mail Order Generic Guaranteed Dispensing Fee
Mail Order Brand Guaranteed Discount
Mail Order Brand Guaranteed Dispensing Fee
Specialty Generic Guaranteed Discount
Specialty Generic Guaranteed Dispensing Fee
Specialty Brand Guaranteed Discount
Specialty Brand Guaranteed Dispensing Fee

Exhibit 3 PASS THROUGH PRESCRIPTION PRICING SCHEDULE
Client acknowledges that the discount rates and dispensing fees set forth below are minimum guaranteed discounts established for the pricing distribution channels necessary to meet access requirements. Client acknowledges that 100% of the pricing will be passed through to Client from the participating pharmacies. <INSERT PBM NAME> agrees to negotiate to achieve or exceed these guaranteed rates. Any discounts obtained by <INSERT PBM NAME> that exceed the targets stated below will be passed through to Client. It is acknowledged by both parties that individual contracts may vary from the targeted rate based upon negotiation. <INSERT PBM NAME> passes through all pharmacy discounts to Client. <INSERT PBM NAME> does not assess network fees or any other forms of revenue from the pharmacies that participate in its network. <INSERT PBM NAME> will pass through the amount paid to the participating pharmacy, which will be the same amount that is invoiced Client. The network guarantees are representative pharmacy reimbursement amounts (including AWP discount and MAC) and dispensing fees. Under the <INSERT PBM NAME> transparent, full pass-through model, Client pays the actual reimbursement rate (discounts and dispense fees) paid to the pharmacy from which the Claim originates, less the Member copay or coinsurance. The contracted discount for each participating pharmacy will vary, causing the actual reimbursement paid to each participating pharmacy to be greater or less than the guarantees identified. Guarantees represent the average performance of all participating pharmacies. AWP/WAC pricing for all Claims is based on the 11-digit National Drug Code (NDC) as of the date of service, and as reported and verifiable by Medi-Span, a national pricing source. Medi-Span is <INSERT PBM NAME>’ only source of drug pricing data and is utilized for all Claims adjudication. All guarantees are based on use of the <INSERT PBM NAME> Formulary and are subject to change in response to formulary and/or plan design changes. <INSERT PBM NAME> will manage the pharmacy network, will determine which pharmacies are to be included in the network, and will negotiate all pharmacy pricing and terms. Network participation will vary, and <INSERT PBM NAME> does not guarantee the number of participating pharmacies. As a result of various states’ most-favored nation Medicaid pricing formulas and historically premium status, various providers have negotiated region-specific pricing with <INSERT PBM NAME>. Claims originating from pharmacies subject to region-specific pricing may be excluded from network discounts and fees. Network discounts and fees may also exclude Claims originating from non-traditional providers, such as long-term-care pharmacies, home infusion providers, military pharmacies, rural pharmacies, Indian Tribal pharmacies, specialty pharmacies, pharmacies deemed by Client as necessary to include in the network but which do not meet <INSERT PBM NAME> discount or credential standards, and pharmacies that hold a direct agreement with Client. Network rates may be modified if more than 5% of Claims are incurred in Massachusetts, Georgia, Hawaii, Alaska, or Puerto Rico, or any U.S. Territory. Additional exclusions from retail network discounts include compound Claims, secondary Claims, 340B Claims, vaccination Claims, pharmaceutical care incentive (PCI) Claims (if applicable) and Member submitted Claims. Specialty guarantees are applicable for specialty pharmacy Claims originating at <INSERT PBM SPECIALTY PHARMACY> as the primary specialty pharmacy provider. <INSERT PBM SPECIALTY PHARMACY>. <INSERT PBM NAME> will deliver the entire value of the proposed network reimbursement terms pricing and manufacturer rebates set forth below, including all upside performance. In accordance with a full pass-through model, the financial performance of overage in one area may be used to offset a shortfall in another area, limited to the retail network, mail service, and manufacturer rebates. Should a shortfall occur after applying this methodology, <INSERT PBM NAME> will pay dollar for dollar at 100% for any shortfall or missed performance guarantee.
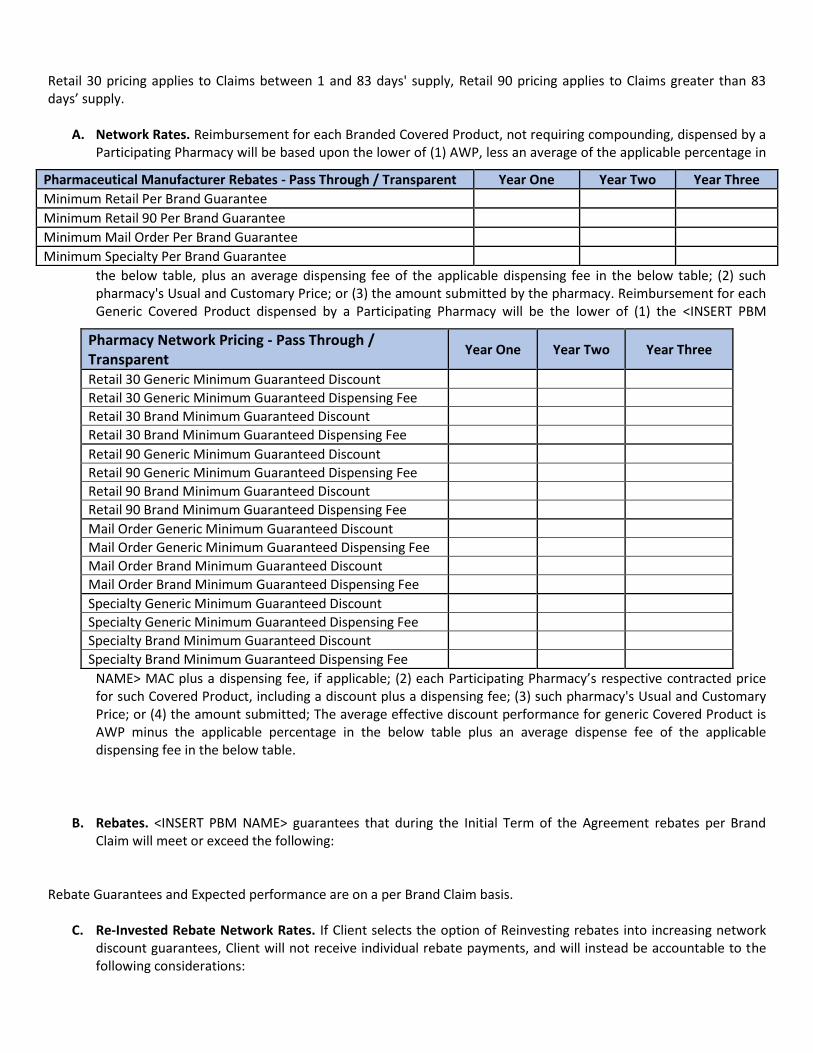
Retail 30 pricing applies to Claims between 1 and 83 days' supply, Retail 90 pricing applies to Claims greater than 83 days’ supply.
A. Network Rates. Reimbursement for each Branded Covered Product, not requiring compounding, dispensed by a Participating Pharmacy will be based upon the lower of (1) AWP, less an average of the applicable percentage in
the below table, plus an average dispensing fee of the applicable dispensing fee in the below table; (2) such pharmacy's Usual and Customary Price; or (3) the amount submitted by the pharmacy. Reimbursement for each Generic Covered Product dispensed by a Participating Pharmacy will be the lower of (1) the <INSERT PBM
NAME> MAC plus a dispensing fee, if applicable; (2) each Participating Pharmacy’s respective contracted price for such Covered Product, including a discount plus a dispensing fee; (3) such pharmacy's Usual and Customary Price; or (4) the amount submitted; The average effective discount performance for generic Covered Product is AWP minus the applicable percentage in the below table plus an average dispense fee of the applicable dispensing fee in the below table.
B. Rebates. <INSERT PBM NAME> guarantees that during the Initial Term of the Agreement rebates per Brand
Claim will meet or exceed the following: Rebate Guarantees and Expected performance are on a per Brand Claim basis.
C. Re-Invested Rebate Network Rates. If Client selects the option of Reinvesting rebates into increasing network discount guarantees, Client will not receive individual rebate payments, and will instead be accountable to the following considerations:
Pharmacy Network Pricing - Pass Through / Transparent
Year One Year Two Year Three
Retail 30 Generic Minimum Guaranteed Discount
Retail 30 Generic Minimum Guaranteed Dispensing Fee
Retail 30 Brand Minimum Guaranteed Discount
Retail 30 Brand Minimum Guaranteed Dispensing Fee
Retail 90 Generic Minimum Guaranteed Discount
Retail 90 Generic Minimum Guaranteed Dispensing Fee
Retail 90 Brand Minimum Guaranteed Discount
Retail 90 Brand Minimum Guaranteed Dispensing Fee
Mail Order Generic Minimum Guaranteed Discount
Mail Order Generic Minimum Guaranteed Dispensing Fee
Mail Order Brand Minimum Guaranteed Discount
Mail Order Brand Minimum Guaranteed Dispensing Fee
Specialty Generic Minimum Guaranteed Discount
Specialty Generic Minimum Guaranteed Dispensing Fee
Specialty Brand Minimum Guaranteed Discount
Specialty Brand Minimum Guaranteed Dispensing Fee
Pharmaceutical Manufacturer Rebates - Pass Through / Transparent Year One Year Two Year Three
Minimum Retail Per Brand Guarantee
Minimum Retail 90 Per Brand Guarantee
Minimum Mail Order Per Brand Guarantee
Minimum Specialty Per Brand Guarantee

a. Reimbursement for each Branded Covered Product, not requiring compounding, dispensed by a Participating Pharmacy will be based upon the lower of (1) AWP, less an average of the applicable percentage in the below table, plus an average dispensing fee of the applicable dispensing fee in the below table; (2) such pharmacy's Usual and Customary Price; or (3) the amount submitted by the pharmacy. Reimbursement for each Generic Covered Product dispensed by a Participating Pharmacy will be the lower of (1) the <INSERT PBM NAME> MAC plus a dispensing fee, if applicable; (2) each Participating Pharmacy’s respective contracted price for such Covered Product, including a discount plus a dispensing fee; (3) such pharmacy's Usual and Customary Price; or (4) the amount submitted; The average effective discount performance for generic Covered Product is AWP minus the applicable percentage in the below table plus an average dispense fee of the applicable dispensing fee in the below table.
Exhibit 4
PERFORMANCE GUARANTEES
<INSERT PBM NAME> will provide the following performance guarantees, placing up to <INSERT RISK THRESHOLD IN DOLLARS> at risk for the applicable time frame, with assessments as described for non-compliance. The proposed assessments set forth below are expressed as a percentage of the administrative fees at risk.
Category Performance Standard Measurement Assessment
Mail Order Dispensing Accuracy Rate
Mail Order Claims Turnaround - Clean Claims (no intervention)
Pharmacy Network Pricing - Pass Through / Transparent – REINVESTED REBATES
Year One Year Two Year Three
Retail 30 Generic Minimum Guaranteed Discount
Retail 30 Generic Minimum Guaranteed Dispensing Fee
Retail 30 Brand Minimum Guaranteed Discount
Retail 30 Brand Minimum Guaranteed Dispensing Fee
Retail 90 Generic Minimum Guaranteed Discount
Retail 90 Generic Minimum Guaranteed Dispensing Fee
Retail 90 Brand Minimum Guaranteed Discount
Retail 90 Brand Minimum Guaranteed Dispensing Fee
Mail Order Generic Minimum Guaranteed Discount
Mail Order Generic Minimum Guaranteed Dispensing Fee
Mail Order Brand Minimum Guaranteed Discount
Mail Order Brand Minimum Guaranteed Dispensing Fee
Specialty Generic Minimum Guaranteed Discount
Specialty Generic Minimum Guaranteed Dispensing Fee
Specialty Brand Minimum Guaranteed Discount
Specialty Brand Minimum Guaranteed Dispensing Fee

Category Performance Standard Measurement Assessment
Mail Order Claims Turnaround - Claims Requiring Administrative or Clinical Intervention
Customer Care - Abandonment Rate
Customer Care - Telephone Service Factor (TSF) TSF is a literal count of all calls answered within the specified threshold. TSF is reported as a percentage.
Customer Care - Average Speed to Answer (ASTA) ASTA is the average amount of time all calls are held before being answered. ASTA is reported in seconds.
Customer Care - Written Inquiries
Financial Accuracy
Information Management - Standard Reports
Claims Processing System Availability
Overall On-Time Program Implementation

SSaammppllee TTPPAA AAggrreeeemmeenntt
AADDMMIINNIISSTTRRAATTIIVVEE SSEERRVVIICCEESS
AAGGRREEEEMMEENNTT
TTHHIISS AAddmmiinniissttrraattiivvee SSeerrvviicceess AAggrreeeemmeenntt ((hheerreeiinnaafftteerr ““AAggrreeeemmeenntt””)),, eeffffeeccttiivvee ffoorr aann iinniittiiaall ppeerriioodd ooff tthhiirrttyy--ssiixx ((3366))

mmoonntthhss bbeeggiinnnniinngg JJaannuuaarryy 11,, 22001122,, aanndd eennddiinngg DDeecceemmbbeerr 3311,, 22001144,, aanndd ccoonnttiinnuuiinngg tthheerreeaafftteerr,, ffoorr aa mmaaxxiimmuumm ooff ttwwoo
aaddddiittiioonnaall ttwweellvvee ((1122)) mmoonntthh ppeerriiooddss,, aass pprroovviiddeedd bbyy tthhiiss AAggrreeeemmeenntt,, iiss eenntteerreedd iinnttoo bbyy tthhee ““CClliieenntt”” ,, aa lleeggaall eennttiittyy dduullyy
oorrggaanniizzeedd aanndd eexxiissttiinngg uunnddeerr tthhee llaawwss ooff tthhee SSttaattee ooff TTeexxaass,, ((hheerreeiinnaafftteerr rreeffeerrrreedd ttoo aass tthhee ““PPllaann SSppoonnssoorr””)),, aanndd TTPPAA,,
IINNCC..,, aa ccoorrppoorraattiioonn dduullyy oorrggaanniizzeedd aanndd eexxiissttiinngg uunnddeerr tthhee llaawwss ooff tthhee SSttaattee ooff AAnnyywwhheerree ((hheerreeiinnaafftteerr rreeffeerrrreedd ttoo aass tthhee ““TTPPAA””))..
WWHHEERREEAASS,, tthhee PPllaann SSppoonnssoorr ssppoonnssoorrss aa sseellff--ffuunnddeedd eemmppllooyyeeee wweellffaarree bbeenneeffiitt ppllaann ((tthhee ““PPllaann””));;
WWHHEERREEAASS,, tthhee PPllaann SSppoonnssoorr ddeessiirreess ttoo mmaakkee aavvaaiillaabbllee aa pprrooggrraamm ooff hheeaalltthh ccaarree bbeenneeffiittss uunnddeerr tthhee PPllaann;;
WWHHEERREEAASS,, tthhee PPllaann SSppoonnssoorr wwiisshheess ttoo ccoonnttrraacctt wwiitthh aann iinnddeeppeennddeenntt tthhiirrdd ppaarrttyy aaddmmiinniissttrraattoorr ttoo ppeerrffoorrmm cceerrttaaiinn
aaddmmiinniissttrraattiivvee sseerrvviicceess wwiitthh rreessppeecctt ttoo tthhee PPllaann aass ddeessccrriibbeedd hheerreeiinn;;
WWHHEERREEAASS,, tthhee TTPPAA ddeessiirreess ttoo ccoonnttrraacctt wwiitthh tthhee PPllaann SSppoonnssoorr ttoo ppeerrffoorrmm cceerrttaaiinn aaddmmiinniissttrraattiivvee sseerrvviicceess wwiitthh rreessppeecctt ttoo tthhee PPllaann aass ddeessccrriibbeedd hheerreeiinn;; aanndd
TTHHEERREEFFOORREE,, iinn ccoonnssiiddeerraattiioonn ooff tthhee pprroommiisseess aanndd mmuuttuuaall ccoovveennaannttss ccoonnttaaiinneedd hheerreeiinn,, tthhee PPllaann SSppoonnssoorr aanndd tthhee TTPPAA
eenntteerr iinnttoo tthhiiss AAggrreeeemmeenntt ffoorr aaddmmiinniissttrraattiivvee sseerrvviicceess ffoorr tthhee PPllaann..
AARRTTIICCLLEE II:: DDEEFFIINNIITTIIOONNSS
FFoorr tthhee ppuurrppoosseess ooff tthhiiss AAggrreeeemmeenntt,, tthhee ffoolllloowwiinngg wwoorrddss
aanndd pphhrraasseess hhaavvee tthhee mmeeaanniinnggss sseett ffoorrtthh bbeellooww,, uunnlleessss
tthhee ccoonntteexxtt cclleeaarrllyy iinnddiiccaatteess ootthheerrwwiissee aanndd,, wwhheerreevveerr
aapppprroopprriiaattee,, tthhee ssiinngguullaarr sshhaallll iinncclluuddee tthhee pplluurraall aanndd tthhee
pplluurraall sshhaallll iinncclluuddee tthhee ssiinngguullaarr..
11..11 ““CCllaaiimm”” mmeeaannss eeaacchh bbiillll,, iinnvvooiiccee,, ccllaaiimm ffoorrmm oorr
ootthheerr ddooccuummeenntt rreepprreesseennttiinngg aa rreeqquueesstt ffoorr
ppaayymmeenntt ffoorr mmeeddiiccaall,, ddeennttaall oorr vviissiioonn sseerrvviicceess,,
wwhhiicchh iiss rreecceeiivveedd bbyy tthhee TTPPAA.. EEaacchh ssuucchh
ddooccuummeenntt wwiillll bbee ccoonnssiiddeerreedd ttoo bbee oonnee ““ccllaaiimm””,,
rreeggaarrddlleessss ooff tthhee nnuummbbeerr ooff iitteemmiizzeedd lliinneess oonn tthhee ddooccuummeenntt aanndd rreeggaarrddlleessss ooff wwhheetthheerr tthhee
ddooccuummeenntt iiss aa dduupplliiccaattee ooff pprreevviioouuss ddooccuummeennttss oorr
wwhheetthheerr tthhee sseerrvviicceess iinnddiiccaatteedd oonn tthhee ddooccuummeenntt
aarree eelliiggiibbllee ffoorr ccoovveerraaggee uunnddeerr tthhee aapppplliiccaabbllee
PPllaann..
11..22 ““CCllaaiimmaanntt”” mmeeaannss aa CCoovveerreedd PPeerrssoonn oorr eennttiittyy oonn
bbeehhaallff ooff aa CCoovveerreedd PPeerrssoonn,, ssuubbmmiittttiinngg eexxppeennsseess
ffoorr ppaayymmeenntt oorr rreeiimmbbuurrsseemmeenntt ffrroomm tthhee PPllaann..
11..33 ““CCllaaiimmss PPaayymmeenntt AAccccoouunntt”” mmeeaannss aann aaccccoouunntt
uuttiilliizzeedd bbyy tthhee PPllaann SSppoonnssoorr ffoorr ppaayymmeenntt oorr
rreeiimmbbuurrsseemmeenntt ffoorr CCoovveerreedd SSeerrvviicceess,, wwhhiicchh
aaccccoouunntt bbaallaanncceess sshhaallll ccoonnssttiittuuttee aasssseettss ooff tthhee
PPllaann SSppoonnssoorr aanndd nnoott tthhee PPllaann..
11..44 ““CCOOBBRRAA”” mmeeaannss tthhee CCoonnssoolliiddaatteedd OOmmnniibbuuss
BBuuddggeett RReeccoonncciilliiaattiioonn AAcctt ooff 11998855 oorr tthhee PPuubblliicc
HHeeaalltthh SSeerrvviiccee AAcctt,, aass aammeennddeedd,, ttooggeetthheerr wwiitthh aallll
rreegguullaattiioonnss aapppplliiccaabbllee tthheerreettoo..
11..55 ““CCOOBBRRAA PPaarrttiicciippaanntt”” mmeeaannss aannyy ppeerrssoonn wwhhoo iiss
pprrooppeerrllyy eennrroolllleedd ffoorr aanndd eennttiittlleedd ttoo bbeenneeffiittss ffrroomm
tthhee PPllaann ppoolliiccyy,, ppuurrssuuaanntt ttoo CCOOBBRRAA ccoonnttiinnuuaattiioonn
ccoovveerraaggee..
11..66 ““CCoommpplleettee CCllaaiimm”” mmeeaannss aa ccllaaiimm ffoorr bbeenneeffiittss ffoorr aa
CCoovveerreedd PPeerrssoonn tthhaatt hhaass bbeeeenn ssuubbmmiitttteedd bbyy aa
lliicceennsseedd HHeeaalltthh CCaarree PPrroovviiddeerr oorr tthhee CCoovveerreedd
PPeerrssoonn,, vvooiidd ooff aannyy oommiissssiioonnss ooff ppeerrttiinneenntt iinnffoorrmmaattiioonn,, ccoooorrddiinnaattiioonn ooff bbeenneeffiittss oorr lliiaabbiilliittyy
iissssuueess,, iinn aa ffoorrmm ssaattiissffaaccttoorryy ttoo TTPPAA aanndd wwiitthh
ssuuffffiicciieenntt ddooccuummeennttaattiioonn ttoo ssuubbssttaannttiiaattee tthhee
ccllaaiimm ffoorr bbeenneeffiittss uunnddeerr tthhee PPllaann tthhaatt iiss nneecceessssaarryy
oorr rreeqquuiirreedd aaccccoorrddiinngg ttoo iinndduussttrryy ssttaannddaarrddss oorr
rreeqquuiirreemmeennttss iinn oorrddeerr ffoorr tthhee TTPPAA ttoo mmaakkee aa
ddeetteerrmmiinnaattiioonn ooff bbeenneeffiittss uunnddeerr tthhee PPllaann..
11..77 ““CCoovveerreedd PPeerrssoonn”” iiss aa ppeerrssoonn wwhhoo iiss pprrooppeerrllyy
eennrroolllleedd aanndd eennttiittlleedd ttoo bbeenneeffiittss ffrroomm tthhee PPllaann..
11..88 ““CCoovveerreedd SSeerrvviicceess”” mmeeaannss tthhee ccaarree,, ttrreeaattmmeennttss,,
sseerrvviicceess oorr ssuupppplliieess ddeessccrriibbeedd iinn tthhee PPllaann
DDooccuummeenntt aass eelliiggiibbllee ffoorr ppaayymmeenntt oorr
rreeiimmbbuurrsseemmeenntt ffrroomm tthhee PPllaann..

11..99 ““CCrreeddiittaabbllee CCoovveerraaggee”” mmeeaannss hheeaalltthh oorr mmeeddiiccaall
ccoovveerraaggee uunnddeerr wwhhiicchh aa CCoovveerreedd PPeerrssoonn wwaass
ccoovveerreedd pprriioorr ttoo eennrroollllmmeenntt uunnddeerr tthhiiss PPllaann wwhhiicchh
pprriioorr ccoovveerraaggee wwaass uunnddeerr aannyy ooff tthhee ffoolllloowwiinngg::
((aa)) AA ggrroouupp hheeaalltthh ppllaann;;
((bb)) HHeeaalltthh IInnssuurraannccee ccoovveerraaggee;;
((cc)) PPaarrtt AA,, PPaarrtt BB oorr PPaarrtt CC ooff TTiittllee
XXVVIIIIII ooff tthhee SSoocciiaall SSeeccuurriittyy AAcctt ((MMeeddiiccaarree));;
((dd)) TTiittllee XXIIXX ooff tthhee SSoocciiaall SSeeccuurriittyy AAcctt,,
ootthheerr tthhaann ccoovveerraaggee ccoonnssiissttiinngg ssoolleellyy ooff
bbeenneeffiittss uunnddeerr §§11992288 ((MMeeddiiccaaiidd));;
((ee)) CChhaapptteerr 5555 ooff TTiittllee 1100,, UUnniitteedd
SSttaatteess CCooddee ((aaccttiivvee mmiilliittaarryy aanndd CCHHAAMMPPUUSS));;
((ff)) AA mmeeddiiccaall ccaarree pprrooggrraamm ooff tthhee
IInnddiiaann HHeeaalltthh SSeerrvviiccee oorr aa ttrriibbaall
oorrggaanniizzaattiioonn;;
((gg)) AA ssttaattee hheeaalltthh bbeenneeffiittss rriisskk ppooooll;;
((hh)) AA hheeaalltthh ppllaann ooffffeerreedd uunnddeerr
CChhaapptteerr 8899 ooff TTiittllee 55,, UUnniitteedd SSttaatteess CCooddee
((FFeeddeerraall EEmmppllooyyeeee HHeeaalltthh BBeenneeffiittss));;
((ii)) AA ppuubblliicc hheeaalltthh ppllaann;; oorr
((jj)) AA hheeaalltthh bbeenneeffiitt ppllaann uunnddeerr §§55((ee))
ooff tthhee PPeeaaccee CCoorrppss AAcctt..
((kk)) AA ssttaattee CChhiillddrreenn’’ss HHeeaalltthh
IInnssuurraannccee PPrrooggrraamm ((CCHHIIPP))
11..1100 ““EEmmppllooyyeerr”” mmeeaannss tthhee PPllaann SSppoonnssoorr aanndd aannyy
ssuucccceessssoorr oorrggaanniizzaattiioonn oorr aaffffiilliiaattee ooff ssuucchh
EEmmppllooyyeerr wwhhiicchh aassssuummeess tthhee oobblliiggaattiioonnss ooff tthhee
PPllaann aanndd tthhiiss AAggrreeeemmeenntt..
11..1111 ““EERRIISSAA”” mmeeaannss tthhee EEmmppllooyyeeee RReettiirreemmeenntt IInnccoommee SSeeccuurriittyy AAcctt ooff 11997744,, aass aammeennddeedd,, ttooggeetthheerr wwiitthh
aallll rreegguullaattiioonnss aapppplliiccaabbllee tthheerreettoo..
11..1122 ““FFeeee SScchheedduullee”” mmeeaannss tthhee lliissttiinngg ooff ffeeeess oorr
cchhaarrggeess ffoorr sseerrvviicceess pprroovviiddeedd uunnddeerr tthhiiss
AAggrreeeemmeenntt.. TThhiiss FFeeee SScchheedduullee mmaayy bbee mmooddiiffiieedd
ffrroomm ttiimmee ttoo ttiimmee iinn wwrriittiinngg bbyy tthhee mmuuttuuaall
aaggrreeeemmeenntt ooff tthhee ppaarrttiieess.. TThhee FFeeee SScchheedduullee iiss
ccoonnttaaiinneedd iinn AAppppeennddiixx AA aanndd iiss aa ppaarrtt ooff tthhiiss
AAggrreeeemmeenntt..
11..1133 ““HHeeaalltthh CCaarree PPrroovviiddeerrss”” mmeeaannss pphhyyssiicciiaannss,,
ddeennttiissttss,, hhoossppiittaallss,, oorr ootthheerr hheeaalltthh ccaarree
pprraaccttiittiioonneerrss oorr hheeaalltthh ccaarree ffaacciilliittiieess tthhaatt aarree dduullyy
lliicceennsseedd aanndd aauutthhoorriizzeedd ttoo rreecceeiivvee ppaayymmeenntt oorr
rreeiimmbbuurrsseemmeenntt ffoorr CCoovveerreedd SSeerrvviicceess iinn
aaccccoorrddaannccee wwiitthh tthhee tteerrmmss ooff tthhee PPllaann..
11..1144 ““HHIIPPAAAA”” mmeeaannss tthhee HHeeaalltthh IInnssuurraannccee PPoorrttaabbiilliittyy
aanndd AAccccoouunnttaabbiilliittyy AAcctt ooff 11999966,, aass aammeennddeedd,, ttooggeetthheerr wwiitthh aallll aapppplliiccaabbllee rreegguullaattiioonnss tthheerreettoo..
11..1155 ““PPaaiidd CCllaaiimmss”” mmeeaannss ccllaaiimmss ffoorr bbeenneeffiittss uunnddeerr tthhee
PPllaann tthhaatt hhaavvee bbeeeenn pprroocceesssseedd ffoorr ppaayymmeenntt bbyy
tthhee TTPPAA,, hhaavvee bbeeeenn ffuunnddeedd iinn UU..SS.. DDoollllaarrss bbyy tthhee
PPllaann oorr tthhee PPllaann SSppoonnssoorr,, aanndd ffoorr wwhhiicchh ppaayymmeenntt
oorr eelleeccttrroonniicc ppaayymmeenntt hhaass bbeeeenn iissssuueedd aanndd
ttrraannssmmiitttteedd ttoo tthhee CCllaaiimmaanntt oorr aassssiiggnneeee..
11..1166 ““PPllaann”” mmeeaannss tthhee sseellff--ffuunnddeedd hheeaalltthh aanndd wweellffaarree bbeenneeffiitt ppllaann wwhhiicchh iiss tthhee ssuubbjjeecctt ooff tthhiiss
AAggrreeeemmeenntt aanndd wwhhiicchh tthhee PPllaann SSppoonnssoorr hhaass
eessttaabblliisshheedd ppuurrssuuaanntt ttoo tthhee PPllaann DDooccuummeenntt..
11..1177 ““PPllaann AAddmmiinniissttrraattoorr”” mmeeaannss tthhee ppeerrssoonn oorr eennttiittyy,,
iinncclluuddiinngg aann iinnssuurraannccee ccoommppaannyy,, ddeessiiggnnaatteedd bbyy
tthhee PPllaann SSppoonnssoorr ttoo mmaannaaggee tthhee PPllaann aanndd mmaakkee aallll
ddiissccrreettiioonnaarryy ddeecciissiioonnss rreeggaarrddiinngg PPllaann tteerrmmss aanndd
mmaannaaggiinngg PPllaann aasssseettss..
11..1188 ““PPllaann DDooccuummeenntt”” mmeeaannss tthhee iinnssttrruummeenntt oorr
iinnssttrruummeennttss tthhaatt sseett ffoorrtthh aanndd ggoovveerrnn tthhee dduuttiieess
ooff tthhee PPllaann SSppoonnssoorr aanndd eelliiggiibbiilliittyy aanndd bbeenneeffiitt
pprroovviissiioonnss ooff tthhee PPllaann,, wwhhiicchh pprroovviiddee ffoorr tthhee
ppaayymmeenntt oorr rreeiimmbbuurrsseemmeenntt ooff CCoovveerreedd SSeerrvviicceess..
11..1199 ““PPllaann PPaarrttiicciippaanntt”” iiss aannyy eemmppllooyyeeee,, rreettiirreeee oorr
CCOOBBRRAA bbeenneeffiicciiaarryy wwhhoo iiss pprrooppeerrllyy eennrroolllleedd aanndd
eelliiggiibbllee oorr bbeenneeffiittss uunnddeerr tthhee PPllaann..
11..2200 ““PPllaann YYeeaarr”” mmeeaannss tthhee ttwweellvvee--mmoonntthh ppeerriioodd ooff
ttiimmee bbeeggiinnnniinngg wwiitthh tthhee eeffffeeccttiivvee ddaattee ooff tthhee PPllaann
aass ssppeecciiffiieedd iinn tthhee PPllaann DDooccuummeenntt..
11..2211 ““QQuuaalliiffiieedd BBeenneeffiicciiaarryy”” mmeeaannss aa CCoovveerreedd PPeerrssoonn
uunnddeerr tthhee PPllaann SSppoonnssoorr’’ss PPllaann,, wwhhoo iiss eelliiggiibbllee ttoo
ccoonnttiinnuuee ccoovveerraaggee uunnddeerr tthhee PPllaann ppoolliiccyy iinn
aaccccoorrddaannccee wwiitthh tthhee aapppplliiccaabbllee pprroovviissiioonnss ooff TTiittllee
XX ooff CCOOBBRRAA oorr §§660099((aa)) ooff EERRIISSAA rreeggaarrddiinngg
QQuuaalliiffiieedd MMeeddiiccaall CChhiilldd SSuuppppoorrtt OOrrddeerrss,, oorr iinn
aaccccoorrddaannccee wwiitthh aannyy ssiimmiillaarr aapppplliiccaabbllee ssttaattee llaaww..
QQuuaalliiffiieedd BBeenneeffiicciiaarryy aallssoo mmeeaannss aa cchhiilldd bboorrnn ttoo,,
aaddoopptteedd oorr ppllaacceedd ffoorr aaddooppttiioonn wwiitthh aa PPaarrttiicciippaanntt
oorr ffoorrmmeerr PPaarrttiicciippaanntt,, wwhhoo iiss aa CCOOBBRRAA ppaarrttiicciippaanntt,,
aatt aannyy ttiimmee dduurriinngg aaccttiivvee CCOOBBRRAA ccoonnttiinnuuaattiioonn
ccoovveerraaggee ooff tthhaatt PPaarrttiicciippaanntt oorr ffoorrmmeerr PPaarrttiicciippaanntt..

11..2222 ““QQuuaalliiffyyiinngg EEvveenntt”” mmeeaannss::
((aa)) WWiitthh rreessppeecctt ttoo aann eelliiggiibbllee PPaarrttiicciippaanntt::
11.. TThhee tteerrmmiinnaattiioonn
((ootthheerr tthhaann bbyy rreeaassoonn ooff ggrroossss
mmiissccoonndduucctt)) ooff tthhee ccoovveerreedd
PPaarrttiicciippaanntt’’ss eemmppllooyymmeenntt;; oorr
22.. TThhee rreedduuccttiioonn iinn
hhoouurrss ooff tthhee ccoovveerreedd PPaarrttiicciippaanntt’’ss
eemmppllooyymmeenntt ccaauussiinngg tthhee
PPaarrttiicciippaanntt ttoo bbeeccoommee iinneelliiggiibbllee
ffoorr ccoovveerraaggee..
((bb)) WWiitthh rreessppeecctt ttoo ccoovveerreedd
DDeeppeennddeennttss::
11.. DDeeaatthh ooff tthhee
ccoovveerreedd PPaarrttiicciippaanntt;;
22.. TTeerrmmiinnaattiioonn ooff
tthhee ccoovveerreedd PPaarrttiicciippaanntt’’ss
eemmppllooyymmeenntt;;
33.. RReedduuccttiioonn iinn
hhoouurrss ooff tthhee ccoovveerreedd PPaarrttiicciippaanntt’’ss
eemmppllooyymmeenntt ccaauussiinngg tthhee
PPaarrttiicciippaanntt ttoo bbeeccoommee iinneelliiggiibbllee
ffoorr ccoovveerraaggee;;
44.. TThhee ddiivvoorrccee oorr
lleeggaall sseeppaarraattiioonn ooff tthhee ccoovveerreedd
PPaarrttiicciippaanntt ffrroomm hhiiss oorr hheerr
ssppoouussee;;
55.. TThhee ccoovveerreedd
PPaarrttiicciippaanntt’’ss eennttiittlleemmeenntt ttoo MMeeddiiccaarree;; oorr
66.. AA ccoovveerreedd
DDeeppeennddeenntt cchhiilldd cceeaasseess ttoo bbee aa
DDeeppeennddeenntt aass ddeeffiinneedd bbyy tthhee
PPllaann..
((cc)) QQuuaalliiffyyiinngg EEvveennttss ffoorr rreettiirreedd
PPaarrttiicciippaannttss,, ffoorr ppuurrppoosseess ooff tthhiiss
sseeccttiioonn,, aarree::
11.. BBaannkkrruuppttccyy,, iiff tthhee
ccoovveerreedd PPaarrttiicciippaanntt rreettiirreedd oonn oorr
bbeeffoorree tthhee ddaattee ooff aannyy ssuubbssttaannttiiaall
eelliimmiinnaattiioonn ooff ggrroouupp hheeaalltthh
ccoovveerraaggee dduuee ttoo bbaannkkrruuppttccyy..
((dd)) QQuuaalliiffyyiinngg EEvveennttss ffoorr tthhee
DDeeppeennddeennttss ooff rreettiirreedd ccoovveerreedd
PPaarrttiicciippaannttss,, ffoorr ppuurrppoosseess ooff tthhiiss sseeccttiioonn,,
aarree::
11.. BBaannkkrruuppttccyy,, iiff tthhee
DDeeppeennddeenntt wwaass aa ccoovveerreedd
DDeeppeennddeenntt ooff aa ccoovveerreedd rreettiirreeee
oonn oorr bbeeffoorree tthhee ddaayy bbeeffoorree tthhee
bbaannkkrruuppttccyy QQuuaalliiffyyiinngg EEvveenntt..
11..2233 ““SSttoopp LLoossss oorr EExxcceessss LLoossss IInnssuurraannccee”” mmeeaannss aann
iinnssuurraannccee ppoolliiccyy oobbttaaiinneedd bbyy tthhee PPllaann oorr tthhee PPllaann
SSppoonnssoorr ttoo pprroovviiddee ccoovveerraaggee ffoorr iinnddiivviidduuaall ccllaaiimmss aatt aa ssppeecciiffiieedd ssttoopp lloossss lliimmiitt aanndd//oorr ggrroouupp ccllaaiimmss
aatt aann aaggggrreeggaattee ssttoopp lloossss lliimmiitt tthhaatt aarree iinnccuurrrreedd
aanndd ppaaiidd dduurriinngg aa ddeeffiinneedd ppeerriioodd ooff ttiimmee bbyy tthhee
iinnssuurraannccee ppoolliiccyy..
11..2244 ““SSuummmmaarryy PPllaann DDeessccrriippttiioonn”” mmeeaannss tthhee ddooccuummeenntt
tthhaatt ddeessccrriibbeess tthhee tteerrmmss aanndd ccoonnddiittiioonnss uunnddeerr
wwhhiicchh tthhee PPllaann ooppeerraatteess..
11..2255 ““UUttiilliizzaattiioonn MMaannaaggeemmeenntt”” mmeeaannss tthhee eevvaalluuaattiioonn
ooff mmeeddiiccaall nneecceessssiittyy aanndd aapppprroopprriiaatteenneessss ooff tthhee
uussee ooff hheeaalltthh ccaarree sseerrvviicceess,, pprroocceedduurreess,, aanndd
ffaacciilliittiieess uuttiilliizzeedd bbyy aa CCoovveerreedd PPeerrssoonn uunnddeerr tthhee
tteerrmmss ooff tthhee PPllaann..
11..2266 ““WWoorrkkiinngg DDaayyss”” sshhaallll mmeeaann aa rreegguullaarr bbuussiinneessss
ddaayy,, wwhhiicchh iiss nnoott aa rreeccooggnniizzeedd ffeeddeerraall oorr bbaannkkiinngg
hhoolliiddaayy,, aanndd ssppeecciiffiiccaallllyy eexxcclluuddiinngg aannyy SSaattuurrddaayy oorr
SSuunnddaayy..
AARRTTIICCLLEE IIII.. RREELLAATTIIOONNSSHHIIPP OOFF TTHHEE PPAARRTTIIEESS
22..11 TThhee PPllaann SSppoonnssoorr aacckknnoowwlleeddggeess tthhaatt tthhee TTPPAA iiss aann
iinnddeeppeennddeenntt ccoonnttrraaccttoorr ffoorr ppuurrppoosseess ooff tthhiiss
AAggrreeeemmeenntt.. AAss ssuucchh,, tthhee TTPPAA iiss nnoott aann aaggeenntt oorr
eemmppllooyyeeee ooff tthhee PPllaann SSppoonnssoorr aanndd ddooeess nnoott
aassssuummee aannyy lliiaabbiilliittyy oorr rreessppoonnssiibbiilliittyy ffoorr aannyy
bbrreeaacchh ooff dduuttyy oorr aacctt ooff oommiissssiioonn bbyy tthhee PPllaann
SSppoonnssoorr.. TThhee PPllaann SSppoonnssoorr ddeelleeggaatteess ttoo tthhee TTPPAA
oonnllyy nnoonn--ddiissccrreettiioonnaarryy aauutthhoorriittyy wwiitthh rreessppeecctt ttoo
aassssiissttiinngg PPllaann SSppoonnssoorr iinn tthhee ddeevveellooppmmeenntt,,
mmaaiinntteennaannccee aanndd aaddmmiinniissttrraattiioonn ooff tthhee PPllaann aass
ssppeecciiffiiccaallllyy ddeessccrriibbeedd iinn tthhiiss AAggrreeeemmeenntt.. AAnnyy
ffuunnccttiioonn nnoott ssppeecciiffiiccaallllyy ddeelleeggaatteedd bbyy PPllaann
SSppoonnssoorr ttoo,, aanndd aaggrreeeedd ttoo bbee aassssuummeedd bbyy tthhee TTPPAA
iinn wwrriittiinngg ppuurrssuuaanntt ttoo tthhiiss AAggrreeeemmeenntt sshhaallll

rreemmaaiinn tthhee ssoollee rreessppoonnssiibbiilliittyy ooff tthhee PPllaann SSppoonnssoorr..
TThhee PPllaann SSppoonnssoorr sshhaallll rreettaaiinn aallll ddiissccrreettiioonnaarryy
aauutthhoorriittyy,, ccoonnttrrooll aanndd rreessppoonnssiibbiilliittyy ffoorr tthhee
ooppeerraattiioonn aanndd aaddmmiinniissttrraattiioonn ooff tthhee PPllaann..
22..22 TThhee ppaarrttiieess aacckknnoowwlleeddggee tthhaatt::
((aa)) TThhiiss iiss aa ccoonnttrraacctt ffoorr
aaddmmiinniissttrraattiivvee sseerrvviicceess oonnllyy aass ssppeecciiffiiccaallllyy
sseett ffoorrtthh hheerreeiinn;;
((bb)) TThhee TTPPAA sshhaallll nnoott bbee oobblliiggaatteedd ttoo
ddiissbbuurrssee mmoorree iinn ppaayymmeenntt ffoorr CCllaaiimmss oorr
ootthheerr oobblliiggaattiioonnss aarriissiinngg uunnddeerr tthhee PPllaann tthhaann tthhee PPllaann SSppoonnssoorr sshhaallll hhaavvee mmaaddee
aavvaaiillaabbllee iinn tthhee CCllaaiimmss PPaayymmeenntt AAccccoouunntt;;
((cc)) TThhiiss AAggrreeeemmeenntt sshhaallll nnoott bbee
ddeeeemmeedd aa ccoonnttrraacctt ooff iinnssuurraannccee uunnddeerr
aannyy llaawwss oorr rreegguullaattiioonnss.. TThhee TTPPAA ddooeess
nnoott iinnssuurree,, gguuaarraanntteeee oorr uunnddeerrwwrriittee tthhee
lliiaabbiilliittyy ooff tthhee PPllaann SSppoonnssoorr uunnddeerr tthhee
PPllaann.. TThhee TTPPAA hhaass nnoo rreessppoonnssiibbiilliittyy aanndd
tthhee PPllaann SSppoonnssoorr hhaass ttoottaall rreessppoonnssiibbiilliittyy
ffoorr ppaayymmeenntt ooff CCllaaiimmss uunnddeerr tthhee PPllaann aanndd
aallll eexxppeennsseess iinncciiddeennttaall ttoo tthhee PPllaann;; aanndd
((dd)) TThhee TTPPAA iiss nnoott tthhee ppllaann
aaddmmiinniissttrraattoorr,, ppllaann ssppoonnssoorr oorr ppllaann
ffiidduucciiaarryy aanndd tthhee PPllaann SSppoonnssoorr wwiillll nnoott
iiddeennttiiffyy tthhee TTPPAA oorr aannyy ooff iittss aaffffiilliiaatteess aass
ssuucchh.. TThhee PPllaann SSppoonnssoorr aacckknnoowwlleeddggeess
aanndd aaggrreeeess tthhaatt iitt iiss tthhee ppllaann ssppoonnssoorr,,
ppllaann aaddmmiinniissttrraattoorr aanndd nnaammeedd ffiidduucciiaarryy aass ssuucchh tteerrmmss aarree ddeeffiinneedd bbyy EERRIISSAA..
22..33 EExxcceepptt aass ssppeecciiffiiccaallllyy sseett ffoorrtthh hheerreeiinn,, tthhiiss
AAggrreeeemmeenntt sshhaallll iinnuurree ttoo tthhee bbeenneeffiitt ooff aanndd bbee
bbiinnddiinngg uuppoonn tthhee ppaarrttiieess hheerreettoo aanndd tthheeiirr
rreessppeeccttiivvee lleeggaall ssuucccceessssoorrss pprroovviiddeedd,, hhoowweevveerr,,
tthhaatt nneeiitthheerr ppaarrttyy mmaayy aassssiiggnn tthhiiss AAggrreeeemmeenntt
wwiitthhoouutt tthhee pprriioorr wwrriitttteenn ccoonnsseenntt ooff tthhee ootthheerr,,
wwhhiicchh ccoonnsseenntt sshhaallll nnoott bbee uunnrreeaassoonnaabbllyy
wwiitthhhheelldd..
22..44 IItt iiss aaggrreeeedd bbyy tthhee ppaarrttiieess ttoo tthhiiss AAggrreeeemmeenntt tthhaatt
aannyy ccaauussee ooff aaccttiioonn bbrroouugghhtt bbyy eeiitthheerr ppaarrttyy ttoo tthhiiss
ccoonnttrraacctt mmuusstt bbee mmaaddee wwiitthhiinn ffoouurr((44)) yyeeaarrss ooff tthhee
ddaattee ooff ooccccuurrrreennccee ooff aannyy aalllleeggeedd bbrreeaacchh,,
iinnffrraaccttiioonn oorr ddiissppuuttee,, oorr wwiitthhiinn ffoouurr((44)) yyeeaarrss ooff
tthhee tteerrmmiinnaattiioonn ddaattee ooff tthhiiss AAggrreeeemmeenntt,,
wwhhiicchheevveerr ooccccuurrss ffiirrsstt..
22..55 TThhee PPllaann SSppoonnssoorr aacckknnoowwlleeddggeess aanndd aaggrreeeess tthhaatt
tthhee TTPPAA wwiillll nnoott bbee ddeeeemmeedd ttoo bbee aa lleeggaall oorr ttaaxx
aaddvviissoorr ffoorr tthhee PPllaann oorr tthhee PPllaann SSppoonnssoorr aass aa
rreessuulltt ooff tthhee ppeerrffoorrmmaannccee ooff iittss dduuttiieess uunnddeerr tthhiiss
AAggrreeeemmeenntt.. TThhee TTPPAA mmaakkeess nnoo rreepprreesseennttaattiioonn ttoo
tthhee PPllaann SSppoonnssoorr ccoonncceerrnniinngg ffeeddeerraall,, ssttaattee,, oorr
llooccaall llaawwss,, rruulleess oorr rreegguullaattiioonnss aapppplliiccaabbllee ttoo tthhee
PPllaann.. CCoommppaannyy mmuusstt sseeeekk iittss oowwnn ccoouunnsseell ffoorr
lleeggaall aaddvviiccee aanndd gguuiiddaannccee.. IInn nnoo eevveenntt sshhaallll tthhee
TTPPAA bbee lliiaabbllee ffoorr ssppeecciiaall oorr ccoonnsseeqquueennttiiaall ddaammaaggeess,, eevveenn iiff tthhee TTPPAA wwaass aaddvviisseedd ooff tthhee
ppoossssiibbiilliittyy ooff ssuucchh ddaammaaggeess..
22..66 TThhee TTPPAA mmaayy sseeccuurree tthhee sseerrvviicceess ooff aaccttuuaarriieess,,
ccoommppuutteerr ssooffttwwaarree ccoommppaanniieess,, ccoommppuutteerr sseerrvviiccee
ffiirrmmss,, iinnssuurraannccee ccoonnssuullttaannttss aanndd pprroodduucceerrss,, lleeggaall
ccoouunnsseell,, aaccccoouunnttaannttss,, uuttiilliizzaattiioonn mmaannaaggeemmeenntt
ccoonnssuullttaannttss,, pphhaarrmmaaccyy bbeenneeffiitt mmaannaaggeemmeenntt
ccoommppaanniieess,, pprreeffeerrrreedd pprroovviiddeerr oorrggaanniizzaattiioonnss,,
ccllaaiimmss nneeggoottiiaattiioonn ccoommppaanniieess,, ssuubbrrooggaattiioonn ffiirrmmss,,
aanndd aannyy ootthheerr eennttiittiieess tthhaatt iitt ddeeeemmss nneecceessssaarryy iinn
tthhee ppeerrffoorrmmaannccee ooff iittss oobblliiggaattiioonnss uunnddeerr tthhiiss
AAggrreeeemmeenntt.. AAtt tthhee ddiissccrreettiioonn ooff tthhee TTPPAA,, ssuucchh
sseerrvviicceess mmaayy bbee ppeerrffoorrmmeedd ddiirreeccttllyy bbyy tthhee TTPPAA,,
wwhhoollllyy oorr iinn ppaarrtt,, tthhrroouugghh aa ssuubbssiiddiiaarryy oorr aaffffiilliiaattee
ooff TTPPAA oorr uunnddeerr aann aaggrreeeemmeenntt wwiitthh aann
oorrggaanniizzaattiioonn,, aaggeenntt,, aaddvviissoorr oorr ootthheerr ppeerrssoonn ooff iittss
cchhoooossiinngg.. AAnnyy ssuucchh sseerrvviicceess rreessuullttiinngg iinn aa ffeeee nnoott
aaggrreeeedd ttoo iinn tthhee FFeeee SScchheedduullee,, AAppppeennddiixx AA,, mmuusstt
ffiirrsstt bbee aauutthhoorriizzeedd iinn wwrriittiinngg bbyy tthhee PPllaann SSppoonnssoorr..
22..77 TThhee TTPPAA aaggrreeeess ttoo bbee dduullyy lliicceennsseedd aass aa TThhiirrdd
PPaarrttyy AAddmmiinniissttrraattoorr ttoo tthhee eexxtteenntt rreeqquuiirreedd uunnddeerr
aapppplliiccaabbllee llaaww aanndd aaggrreeeess ttoo mmaaiinnttaaiinn ssuucchh
lliicceennssuurree tthhrroouugghhoouutt tthhee tteerrmm ooff tthhiiss AAggrreeeemmeenntt..
22..88 TThhee TTPPAA wwiillll ppoosssseessss tthhrroouugghh tthhee tteerrmm ooff tthhiiss
AAggrreeeemmeenntt aann iinn--ffoorrccee ffiiddeelliittyy bboonndd oorr ootthheerr
iinnssuurraannccee aass mmaayy bbee rreeqquuiirreedd bbyy ssttaattee aanndd ffeeddeerraall
llaawwss ffoorr tthhee pprrootteeccttiioonn ooff iittss cclliieennttss.. AAddddiittiioonnaallllyy,,
tthhee TTPPAA aaggrreeeess ttoo ccoommppllyy wwiitthh aannyy ssttaattee oorr
ffeeddeerraall ssttaattuutteess oorr rreegguullaattiioonnss rreeggaarrddiinngg iittss
ooppeerraattiioonnss..
22..99 TThhee TTPPAA sshhaallll bbee eennttiittlleedd ttoo rreellyy uuppoonn,, wwiitthhoouutt
iinnvveessttiiggaattiioonn oorr iinnqquuiirryy,, aannyy wwrriitttteenn oorr oorraall

iinnffoorrmmaattiioonn oorr ccoommmmuunniiccaattiioonn ooff tthhee PPllaann
SSppoonnssoorr oorr aaggeennttss,, iinncclluuddiinngg bbuutt nnoott lliimmiitteedd ttoo
ccoonnssuullttaannttss,, aaccttuuaarriieess,, aattttoorrnneeyyss,, aaccccoouunnttaannttss,,
aauuddiittoorrss,, mmaannaaggeedd ccaarree oorrggaanniizzaattiioonnss,, pprreeffeerrrreedd pprroovviiddeerr oorrggaanniizzaattiioonnss,, pphhaarrmmaaccyy bbeenneeffiitt
mmaannaaggeemmeenntt ccoommppaanniieess,, mmeennttaall hheeaalltthh ccaarree
mmaannaaggeemmeenntt ccoommppaanniieess oorr bbrrookkeerrss rreettaaiinneedd bbyy
tthhee PPllaann SSppoonnssoorr..
22..1100 TThhee TTPPAA wwiillll iinnddeemmnniiffyy,, ddeeffeenndd,, ssaavvee aanndd hhoolldd tthhee
PPllaann SSppoonnssoorr hhaarrmmlleessss ffrroomm aanndd aaggaaiinnsstt aannyy aanndd
aallll ccllaaiimmss,, ssuuiittss,, lliiaabbiilliittiieess,, lloosssseess,, ppeennaallttiieess oorr
ddaammaaggeess iinncclluuddiinngg ccoouurrtt ccoossttss aanndd aattttoorrnneeyyss’’ ffeeeess
wwiitthh rreessppeecctt ttoo tthhee PPllaann wwhhiicchh ddiirreeccttllyy rreessuulltt ffrroomm oorr aarriissee oouutt ooff tthhee ddiisshhoonneesstt,, ffrraauudduulleenntt,, ggrroossssllyy
nneegglliiggeenntt oorr ccrriimmiinnaall aaccttss ooff tthhee TTPPAA oorr iittss
eemmppllooyyeeeess,, eexxcceepptt ffoorr aannyy aaccttss ttaakkeenn aatt tthhee
ssppeecciiffiicc ddiirreeccttiioonn ooff tthhee PPllaann SSppoonnssoorr..
22..1111 TThhee PPllaann SSppoonnssoorr aacccceeppttss aallll lleeggaall aanndd ffiinnaanncciiaall
lliiaabbiilliittyy ffoorr iittss oowwnn aaccttiioonnss oorr iinnaaccttiioonnss aass wweellll aass
tthhee aaccttiioonnss oorr iinnaaccttiioonnss ooff iittss aauutthhoorriizzeedd
rreepprreesseennttaattiivveess.. TThhee PPllaann SSppoonnssoorr sshhaallll eennssuurree
tthhaatt nnoo ssuucchh lleeggaall oorr ffiinnaanncciiaall lliiaabbiilliittiieess sshhaallll bbee
bboorrnnee bbyy tthhee TTPPAA..
AARRTTIICCLLEE IIIIII.. TTHHEE TTPPAA’’SS RREESSPPOONNSSIIBBIILLIITTIIEESS
TThhee TTPPAA wwiillll pprroovviiddee tthhee ffoolllloowwiinngg PPllaann AAddmmiinniissttrraattiivvee
sseerrvviicceess ffoorr tthhee PPllaann SSppoonnssoorr::
33..11 MMaaiinnttaaiinn PPllaann rreeccoorrddss bbaasseedd oonn eelliiggiibbiilliittyy
iinnffoorrmmaattiioonn ssuubbmmiitttteedd bbyy tthhee PPllaann SSppoonnssoorr aass ttoo
tthhee ddaatteess oonn wwhhiicchh aa CCoovveerreedd PPeerrssoonn’’ss ccoovveerraaggee ccoommmmeenncceess aanndd tteerrmmiinnaatteess..
MMaaiinnttaaiinn PPllaann rreeccoorrddss ooff PPllaann ccoovveerraaggee aapppplliiccaabbllee
ttoo eeaacchh CCoovveerreedd PPeerrssoonn bbaasseedd oonn iinnffoorrmmaattiioonn
ssuubbmmiitttteedd bbyy tthhee PPllaann SSppoonnssoorr..
MMaaiinnttaaiinn PPllaann rreeccoorrddss rreeggaarrddiinngg ppaayymmeenntt ooff
CCllaaiimmss,, ddeenniiaall ooff CCllaaiimmss,, aanndd CCllaaiimmss ppeennddeedd..
33..22 AAddmmiinniisstteerr eennrroollllmmeenntt ooff CCoovveerreedd PPeerrssoonnss,, ccrreeaattee
aanndd ddiissttrriibbuuttee eennrroollllmmeenntt ffoorrmmss aanndd aannsswweerr
iinnqquuiirriieess,, ccrreeaattee aanndd mmaaiinnttaaiinn eennrroollllmmeenntt rreeccoorrddss
ffoorr CCoovveerreedd PPeerrssoonnss,, aanndd ddiissttrriibbuuttee iiddeennttiiffiiccaattiioonn
ccaarrddss ttoo tthhee PPllaann SSppoonnssoorr iinn aaccccoorrddaannccee wwiitthh
AAppppeennddiixx AA,, tthhee FFeeee SScchheedduullee..
33..33 PPrroocceessss CCoommpplleettee CCllaaiimmss ssuubbmmiitttteedd bbyy CCoovveerreedd
PPeerrssoonnss oorr HHeeaalltthh CCaarree PPrroovviiddeerrss aaccccoorrddiinngg ttoo tthhee
tteerrmmss ooff tthhee PPllaann DDooccuummeenntt aass ccoonnssttrruueedd bbyy tthhee
PPllaann SSppoonnssoorr.. TThheessee CCllaaiimmss wwiillll bbee pprroocceesssseedd iinn aaccccoorrddaannccee wwiitthh pprreevvaaiilliinngg iinndduussttrryy pprraaccttiicceess aanndd
tthhee TTPPAA wwiillll uussee aann iinndduussttrryy--rreeccooggnniizzeedd mmeetthhoodd
ooff ddeetteerrmmiinniinngg uussuuaall,, ccuussttoommaarryy,, aanndd rreeaassoonnaabbllee
cchhaarrggeess oorr tthhee pprreevvaaiilliinngg ffeeee aalllloowwaannccee aass
ddeetteerrmmiinneedd bbyy tthhee PPllaann SSppoonnssoorr iinn tthhee PPllaann..
TThhee TTPPAA wwiillll nnoott bbee rreeqquuiirreedd bbyy tthhee PPllaann SSppoonnssoorr
ttoo aalltteerr iittss ssttaannddaarrdd ccllaaiimmss pprroocceesssseess,, pprroocceedduurreess
oorr rreegguullaarr mmaaiill ddaatteess ttoo mmaanniippuullaattee tthhee PPaaiidd
CCllaaiimmss ddaattee ffoorr aannyy ppuurrppoossee..
TThhee TTPPAA wwiillll pprroocceessss ccllaaiimmss rreecceeiivveedd oonn aa bbaassiiss
ccoonnssiisstteenntt wwiitthh pprreevvaaiilliinngg iinndduussttrryy pprraaccttiiccee ffoorr
ttiimmeelliinneessss aanndd aaccccuurraaccyy,, iinn aaccccoorrddaannccee wwiitthh tthhee
tteerrmmss ooff tthhee PPllaann DDooccuummeenntt aass ccoonnssttrruueedd bbyy tthhee
PPllaann SSppoonnssoorr,, aanndd ccoonnssiisstteenntt mmeeddiiccaall iinnffoorrmmaattiioonn
ffoorrmmss,, pprree--eexxiissttiinngg ccoonnddiittiioonnss rreeqquuiirreemmeennttss,,
ddiissaabbiilliittyy ddeetteerrmmiinnaattiioonnss aanndd ccoooorrddiinnaattiioonn ooff
bbeenneeffiittss ssiittuuaattiioonnss.. UUnnlleessss ssppeecciiffiiccaallllyy aaggrreeeedd bbyy
tthhee ppaarrttiieess iinn wwrriittiinngg,, tthhee TTPPAA’’ss dduuttiieess wwiitthh
rreessppeecctt ttoo ssuubbrrooggaattiioonn ssiittuuaattiioonnss sshhaallll bbee lliimmiitteedd
ttoo iinnffoorrmmiinngg tthhee PPllaann SSppoonnssoorr tthhaatt ssuubbrrooggaattiioonn
rriigghhttss mmaayy eexxiisstt.. TThhee tteerrmmss,, ccoonnddiittiioonnss aanndd ffeeeess
ffoorr aannyy aaddddiittiioonnaall aaggrreeeemmeenntt rreeggaarrddiinngg
ssuubbrrooggaattiioonn aarree aass ssttaatteedd iinn tthhee aattttaacchheedd
SSuubbrrooggaattiioonn SSeerrvviicceess AAppppeennddiixx,, iiff aapppplliiccaabbllee..
TThhee TTPPAA wwiillll pprroocceessss CCllaaiimmss oorr rreeqquueesstt aaddddiittiioonnaall
iinnffoorrmmaattiioonn iinn oorrddeerr ttoo bbee aabbllee ttoo pprroocceessss aa
CCoommpplleettee CCllaaiimm wwiitthhiinn aann aavveerraaggee ooff ffoouurrtteeeenn ((1144)) WWoorrkkiinngg DDaayyss ffrroomm tthhee ddaattee tthhee CCoommpplleettee
CCllaaiimm iiss rreecceeiivveedd bbyy tthhee TTPPAA..
IIff aaddddiittiioonnaall iinnffoorrmmaattiioonn iiss nneeeeddeedd ffoorr aa CCoommpplleettee
CCllaaiimm,, tthhee TTPPAA wwiillll sseenndd tthhrroouugghh tthhee UU..SS.. MMaaiill ttoo
tthhee aapppprroopprriiaattee ppeerrssoonnss ((wwiitthh aa ccooppyy ttoo tthhee PPllaann
PPaarrttiicciippaanntt)) aa ffoollllooww--uupp rreeqquueesstt ffoorr tthhee rreeqquuiirreedd
iinnffoorrmmaattiioonn ffoorr aa CCoommpplleettee CCllaaiimm rreeqquueessttiinngg aa
rreessppoonnssee ttoo tthhee rreeqquueesstt ffoorr aaddddiittiioonnaall
iinnffoorrmmaattiioonn ffoorr aa CCoommpplleettee CCllaaiimm wwiitthhiinn aa
mmaaxxiimmuumm ooff ffoorrttyy--ffiivvee ((4455)) ddaayyss.. TThhee ffoollllooww--uupp
rreeqquueesstt wwiillll iinnddiiccaattee tthhaatt nnoo aaddddiittiioonnaall rreeqquueessttss
ffoorr iinnffoorrmmaattiioonn wwiillll bbee sseenntt aanndd tthhee ffiillee wwiillll bbee
cclloosseedd,, aanndd tthhee iinniittiiaall iinnccoommpplleettee ccllaaiimm wwiillll bbee
ddeenniieedd,, iiff tthhee rreeqquueesstteedd iinnffoorrmmaattiioonn iiss nnoott
pprroovviiddeedd wwiitthhiinn tthhee ssppeecciiffiieedd ttiimmee..
WWhheenn aallll nneecceessssaarryy ddooccuummeennttss aanndd CCllaaiimm
iinnffoorrmmaattiioonn hhaavvee bbeeeenn rreecceeiivveedd ttoo ccoonnssttiittuuttee aa
CCoommpplleettee CCllaaiimm aanndd tthhee CCoommpplleettee CCllaaiimm hhaass bbeeeenn aapppprroovveedd,, aa CCllaaiimm cchheecckk oorr ddrraafftt wwiillll bbee rreemmiitttteedd
oonn tthhee nneexxtt PPaaiidd CCllaaiimmss bbaattcchh ddiissbbuurrssaall ddaattee
pprroovviiddeedd tthhaatt tthhee PPllaann SSppoonnssoorr hhaass pprroovviiddeedd
ffuunnddss ffoorr ssuucchh CCoommpplleettee CCllaaiimmss oorr aaddvvaannccee
ffuunnddiinngg hhaass bbeeeenn pprroovviiddeedd bbyy tthhee SSttoopp LLoossss oorr
EExxcceessss LLoossss iinnssuurraannccee ccoommppaannyy.. AAllll CCoommpplleettee
CCllaaiimmss wwiillll rreemmaaiinn iinn aa pprroocceesssseedd bbuutt ppeennddeedd
ssttaattuuss uunnttiill ffuunnddeedd bbyy tthhee PPllaann SSppoonnssoorr oorr iittss SSttoopp
LLoossss oorr EExxcceessss LLoossss iinnssuurraannccee ccoommppaannyy.. TThhee PPllaann
SSppoonnssoorr mmuusstt pprroovviiddee ffuunnddiinngg ooff aallll CCoommpplleettee CCllaaiimmss wwiitthhiinn ffiivvee ((55)) WWoorrkkiinngg DDaayyss ooff rreecceeiipptt ooff
rreeqquueesstt ffoorr ffuunnddiinngg ffrroomm tthhee TTPPAA..
CCuussttoommeerr SSeerrvviiccee RReepprreesseennttaattiivveess ooff tthhee TTPPAA wwiillll
iinnffoorrmm aannyy PPllaann PPaarrttiicciippaanntt oorr HHeeaalltthh CCaarree
PPrroovviiddeerr wwhhoo iinnqquuiirreess aabboouutt aannyy CCllaaiimm wwhhiicchh iiss
ppeennddeedd ffoorr llaacckk ooff ffuunnddss tthhaatt ssuucchh CCllaaiimm hhaass bbeeeenn
rreecceeiivveedd aanndd pprroocceesssseedd aanndd iiss ppeennddiinngg rreecceeiipptt ooff
ffuunnddss.. NNoo ffuurrtthheerr eexxppllaannaattiioonn wwiillll bbee rreeqquuiirreedd ooff
tthhee TTPPAA bbyy tthhee PPllaann SSppoonnssoorr uunnddeerr ssuucchh
cciirrccuummssttaanncceess..
UUnnlleessss ootthheerrwwiissee aaddvviisseedd bbyy tthhee PPllaann SSppoonnssoorr,, tthhee
PPllaann SSppoonnssoorr aaggrreeeess tthhaatt tthhee oorrddeerr ooff ccllaaiimmss
ppaayymmeenntt bbyy TTPPAA ooff nneeww ccllaaiimmss ssuubbmmiitttteedd uunnddeerr
tthhee PPllaann sshhaallll bbee bbaasseedd oonn pprroocceessssiinngg ffiirrsstt tthhee
oollddeesstt ccllaaiimmss wwiitthh ccoommpplleettee mmeeddiiccaall,,
rreepprriicciinngg//ddiissccoouunntt,, aanndd ootthheerr nneecceessssaarryy
iinnffoorrmmaattiioonn wwiitthh ppeerrmmiitttteedd eexxcceeppttiioonnss ffoorr tthhoossee
ccllaaiimmss iiddeennttiiffiieedd wwiitthh eexxcceessss lloossss iinnssuurraannccee rreeiimmbbuurrsseemmeenntt ppootteennttiiaall oorr wwhhiicchh ffaaccee lloossss ooff aannyy
aavvaaiillaabbllee ddiissccoouunnttss ffoorr tthhee mmeeddiiccaall sseerrvviicceess ssoo
rreennddeerreedd.. AAnnyy ppaayymmeenntt bbyy TTPPAA iiss ccoonnttiinnggeenntt
uuppoonn tthhee aavvaaiillaabbiilliittyy aaddeeqquuaattee ffuunnddiinngg bbyy tthhee PPllaann
SSppoonnssoorr.. IIff tthhee ffuunnddss pprroovviiddeedd bbyy tthhee PPllaann
SSppoonnssoorr aarree iinnssuuffffiicciieenntt ttoo ppaayy aallll aaddjjuuddiiccaatteedd
ccllaaiimmss,, tthheenn,, aatt tthhee ssppeecciiffiicc ddiirreeccttiioonn ooff PPllaann
SSppoonnssoorr,, tthhee ffuunnddss wwiillll bbee aapppplliieedd ttoo ppaayy ccllaaiimmss aass
nnootteedd aabboovvee ttoo tthhee eexxtteenntt ffuunnddss aarree aavvaaiillaabbllee
eexxcceepptt tthhaatt llaarrggee ccllaaiimmss tthhaatt ccaannnnoott bbee ffuunnddeedd bbyy
tthhee tthheenn aavvaaiillaabbllee ffuunnddiinngg wwiillll bbee sskkiippppeedd iinn ffaavvoorr
ooff mmoorree rreecceenntt ccllaaiimmss tthhaatt ccaann bbee ccoovveerreedd wwiitthh
tthheenn aavvaaiillaabbllee ffuunnddiinngg.. FFuurrtthheerr,, aallll ccllaaiimmss ffoorr aa
ppaarrttiicciippaanntt aanndd hhiiss oorr hheerr ccoovveerreedd ddeeppeennddeennttss
ssuubbsseeqquueenntt ttoo tthhee ffiirrsstt ccllaaiimm tthhaatt ccaannnnoott bbee
ffuunnddeedd dduuee ttoo iinnssuuffffiicciieenntt ffuunnddiinngg ffrroomm tthhee PPllaann
SSppoonnssoorr sshhaallll bbee sskkiippppeedd iinn ffaavvoorr ooff mmoorree rreecceenntt
ccllaaiimmss ffrroomm ootthheerr ppaarrttiicciippaannttss aanndd//oorr tthheeiirr
ddeeppeennddeennttss iiff tthhee PPllaann SSppoonnssoorr ffuunnddiinngg iiss nnoott
ssuuffffiicciieenntt ttoo ccoovveerr aallll aaddjjuuddiiccaatteedd ccllaaiimmss ffoorr tthhee ppaarrttiicciippaanntt aanndd//oorr hhiiss oorr hheerr ddeeppeennddeenntt..
33..44 AAfftteerr aa pprreelliimmiinnaarryy rreevviieeww ttoo ddeetteerrmmiinnee tthhaatt tthhee
CCllaaiimm wwaass ccoorrrreeccttllyy pprroocceesssseedd,, tthhee TTPPAA wwiillll rreeffeerr
aannyy ddoouubbttffuull,, ddiissppuutteedd oorr aappppeeaalleedd CCllaaiimmss ttoo tthhee
PPllaann SSppoonnssoorr ffoorr aa ffiinnaall ddeecciissiioonn.. TThhee TTPPAA wwiillll
pprroovviiddee iinniittiiaall ccllaaiimmss aaddjjuuddiiccaattiioonn aanndd aassssiisstt tthhee
PPllaann AAddmmiinniissttrraattoorr wwiitthh aappppeeaallss.. TThhee PPllaann wwiillll
ppaayy tthhee aaccttuuaall ccoosstt ooff aannyy eexxppeerrtt mmeeddiiccaall
ccoonnssuullttaattiioonn rreeqquuiirreedd ttoo ddeetteerrmmiinnee ccllaaiimmss eelliiggiibbiilliittyy uunnddeerr tthhee PPllaann aass aa ccllaaiimmss ccoosstt..
33..55 PPrroocceessss,, iissssuuee aanndd ddiissttrriibbuuttee CCllaaiimmss cchheecckkss,, ddrraaffttss
oorr eelleeccttrroonniicc ffuunnddss ttrraannssffeerr,, aass iinnssttrruucctteedd bbyy tthhee
PPllaann SSppoonnssoorr ttoo PPllaann PPaarrttiicciippaannttss,, HHeeaalltthh CCaarree
PPrroovviiddeerrss,, oorr ootthheerrss aass mmaayy bbee aapppplliiccaabbllee..
EEvveerryy wweeeekk tthhee TTPPAA wwiillll nnoottiiffyy tthhee PPllaann SSppoonnssoorr ooff
tthhee CCllaaiimmss bbaattcchh aammoouunntt rreeqquuiirreedd ttoo bbee
pprroossppeeccttiivveellyy ddeeppoossiitteedd ttoo tthhee CCllaaiimmss PPaayymmeenntt
AAccccoouunntt ttoo ppaayy tthhee CCllaaiimmss lliiaabbiilliittyy aafftteerr tthheessee
CCllaaiimmss aarree pprroocceesssseedd ffoorr ppaayymmeenntt..
TThhee TTPPAA sshhaallll eessttaabblliisshh aanndd mmaaiinnttaaiinn ccuussttoommaarryy
iinnvveessttiiggaattiivvee bbeenneeffiitt aanndd CCllaaiimmss rreevviieeww
pprroocceedduurreess wwiitthhiinn tthhee pprreevvaaiilliinngg ssttaannddaarrdd ooff ccaarree
iinn tthhee TTPPAA iinndduussttrryy.. TThhee TTPPAA wwiillll nnoottiiffyy tthhee PPllaann
SSppoonnssoorr ooff tthhee ddiissccoonnttiinnuuaannccee ooff ssuucchh pprroocceedduurreess
oorr aannyy ssiiggnniiffiiccaanntt oorr mmaatteerriiaall cchhaannggeess tthheerreeiinn..
TThhee TTPPAA sshhaallll ttaakkee rreeaassoonnaabbllee mmeeaassuurreess aanndd pprreeccaauuttiioonnss ttoo pprreevveenntt tthhee aalllloowwaannccee aanndd
ppaayymmeenntt ooff iimmpprrooppeerr bbeenneeffiittss aanndd CCllaaiimmss.. TThhee
TTPPAA sshhaallll nnoott bbee lliiaabbllee ffoorr ffrraauudd bbyy aannyy HHeeaalltthh
CCaarree PPrroovviiddeerr oorr CCoovveerreedd PPeerrssoonn oorr ffoorr eerrrroorrss iinn
CCllaaiimm ppaayymmeenntt mmaaddee ttoo CCoovveerreedd PPeerrssoonnss oorr
ddeessiiggnnaatteedd aassssiiggnneeeess iinn ggoooodd ffaaiitthh.. TThhee TTPPAA sshhaallll
nnoott bbee lliiaabbllee ffoorr aannyy lloossss ooff ddiissccoouunntt oorr iinnccrreeaassee iinn
cchhaarrggeess aarriissiinngg ffrroomm aa CCllaaiimm dduuee ttoo aa ddeellaayy iinn tthhee
ppaayymmeenntt ooff aa CCllaaiimm.. IIff aa CCllaaiimm ppaayymmeenntt eerrrroorr iiss
ddiissccoovveerreedd,, tthhee HHeeaalltthh CCaarree PPrroovviiddeerr oorr CCoovveerreedd
PPeerrssoonn wwiillll bbee nnoottiiffiieedd aanndd rreeqquueesstteedd ttoo rreeffuunndd
ppaayymmeenntt.. IInn tthhee eevveenntt tthhaatt tthhee CCoovveerreedd PPeerrssoonn oorr
hhiiss//hheerr aassssiiggnneeee ddooeess nnoott rreessppoonndd ttoo tthhee rreeffuunndd
rreeqquueesstt oorr rreeffuusseess ppaayymmeenntt,, tthhee PPllaann SSppoonnssoorr wwiillll
bbee nnoottiiffiieedd.. TThhee PPllaann SSppoonnssoorr sshhaallll hhaavvee tthhee rriigghhtt
ttoo bbrriinngg aaccttiioonn aaggaaiinnsstt aannyy eemmppllooyyeeee oorr pprroovviiddeerr

ooff sseerrvviiccee wwhhoo ddooeess nnoott vvoolluunnttaarriillyy aaggrreeee ttoo rreeppaayy
tthhee PPllaann ffoorr ppaayymmeennttss mmaaddee iinn eerrrroorr.. TThhee TTPPAA
sshhaallll nnoott bbee lliiaabbllee ffoorr mmiissrreepprreesseennttaattiioonnss,, iinnffllaatteedd
cchhaarrggeess,, oommiissssiioonnss,, eerrrroorrss oorr ffrraauudd bbyy aannyy HHeeaalltthh CCaarree PPrroovviiddeerr oorr CCoovveerreedd PPeerrssoonn wwhhiicchh mmaayy rreessuulltt
iinn aannyy iinneelliiggiibbllee oorr eexxcceessssiivvee CCllaaiimm ppaayymmeennttss..
33..66 NNoottiiffyy CCoovveerreedd PPeerrssoonnss iinn wwrriittiinngg tthhrroouugghh tthhee
UU..SS.. MMaaiill ooff iinneelliiggiibbllee CCllaaiimmss rreecceeiivveedd.. TThhee
ccoommppuutteerriizzeedd EExxppllaannaattiioonn ooff BBeenneeffiittss ffoorrmm ((EEOOBB))
sshhaallll iinnddiiccaattee tthhee ggeenneerraall rreeaassoonn wwhhyy ssuucchh CCllaaiimm
iiss iinneelliiggiibbllee ffoorr ppaayymmeenntt.. TThhee EEOOBB sshhaallll aallssoo
ccoonnttaaiinn nnoottiiccee ooff tthhee wwrriitttteenn CCllaaiimmss rreevviieeww aanndd
aappppeeaall pprroocceedduurree iinn tthhee PPllaann.. TThhiiss nnoottiiffiiccaattiioonn wwiillll bbee mmaaddee wwiitthhiinn aann aavveerraaggee ooff ffoouurrtteeeenn ((1144))
WWoorrkkiinngg DDaayyss ooff tthhee ddaattee tthhee TTPPAA rreecceeiivveess tthhee
CCoommpplleettee CCllaaiimm ddooccuummeennttaattiioonn aanndd aannyy PPllaann
iinntteerrpprreettaattiioonnss bbyy tthhee PPllaann SSppoonnssoorr..
33..77 RReessppoonndd ttoo CCllaaiimmss iinnqquuiirriieess bbyy aa CCoovveerreedd PPeerrssoonn,,
tthhee eessttaattee ooff aa CCoovveerreedd PPeerrssoonn,, aann aauutthhoorriizzeedd
mmeemmbbeerr ooff aa CCoovveerreedd PPeerrssoonn’’ss ffaammiillyy uunniitt,, tthhee
CCoovveerreedd PPeerrssoonn’’ss aauutthhoorriizzeedd lleeggaall rreepprreesseennttaattiivvee
oorr aann aauutthhoorriizzeedd HHeeaalltthh CCaarree PPrroovviiddeerr..
33..88 MMaaiinnttaaiinn llooccaall tteelleepphhoonnee sseerrvviiccee aanndd ttoollll--ffrreeee
tteelleepphhoonnee lliinneess dduurriinngg rreegguullaarr bbuussiinneessss hhoouurrss ffoorr
iinnqquuiirriieess mmaaddee bbyy CCoovveerreedd PPeerrssoonnss rreeggaarrddiinngg tthhee
ssttaattuuss ooff tthheeiirr CCllaaiimmss.. SSuucchh tteelleepphhoonnee lliinneess mmaayy
bbee rreeccoorrddeedd bbyy tthhee TTPPAA..
33..99 MMaaiinnttaaiinn aann IInntteerrnneett IInnqquuiirryy ssiittee ffoorr PPaaiidd CCllaaiimmss,,
pprroocceesssseedd ccllaaiimmss aanndd rreellaatteedd iinnffoorrmmaattiioonn..
MMaaiinnttaaiinn aann iinntteerraaccttiivvee vvooiiccee rreessppoonnssee ssyysstteemm aanndd ffaaxx bbaacckk sseerrvviiccee ffoorr tthhee ccoonnvveenniieennccee ooff
CCoovveerreedd PPeerrssoonnss aanndd HHeeaalltthh CCaarree PPrroovviiddeerrss ffoorr
CCllaaiimm oorr ccoovveerraaggee iinnqquuiirriieess..
33..1100 MMaaiinnttaaiinn iinnffoorrmmaattiioonn tthhaatt iiddeennttiiffiieess aa CCoovveerreedd
PPeerrssoonn iinn aa ccoonnffiiddeennttiiaall mmaannnneerr.. TThhee TTPPAA aaggrreeeess
ttoo ttaakkee aallll rreeaassoonnaabbllee pprreeccaauuttiioonnss ttoo pprreevveenntt
ddiisscclloossuurree oorr uussee ooff CCllaaiimmss iinnffoorrmmaattiioonn ffoorr aa
ppuurrppoossee uunnrreellaatteedd ttoo tthhee aaddmmiinniissttrraattiioonn ooff tthhee
PPllaann.. TTPPAA sshhaallll nnoott bbee lliiaabbllee ffoorr ffrraauudd,, ddeecceeiitt,,
mmiissrreepprreesseennttaattiioonn oorr aannyy ootthheerr ffaallssee,, mmiisslleeaaddiinngg
oorr eerrrroonneeoouuss rreepprreesseennttaattiioonnss mmaaddee bbyy tthhee PPllaann
SSppoonnssoorr,, aannyy CCoovveerreedd PPeerrssoonn,, aannyy HHeeaalltthh CCaarree
PPrroovviiddeerr oorr aannyy ootthheerr ppeerrssoonn ppeerrttaaiinniinngg ttoo aannyy
ccoonnffiiddeennttiiaall,, ppeerrssoonnaall oorr pprrootteecctteedd hheeaalltthh
iinnffoorrmmaattiioonn oorr ccllaaiimm rreeqquueesstt.. TThhee TTPPAA wwiillll oonnllyy
rreelleeaassee nnoonn--pprrootteecctteedd hheeaalltthh oorr CCllaaiimmss
iinnffoorrmmaattiioonn ffoorr cceerrttiiffiiccaattee ooff nneeeedd rreevviieewwss;; ffoorr
mmeeddiiccaall nneecceessssiittyy ddeetteerrmmiinnaattiioonnss;; ttoo sseett uunniiffoorrmm
ddaattaa ssttaannddaarrddss;; ttoo uuppddaattee rreellaattiivvee vvaalluueess ssccaalleess;; ttoo uussee iinn ccllaaiimmss aannaallyyssiiss;; ttoo ffuurrtthheerr ccoosstt
ccoonnttaaiinnmmeenntt pprrooggrraammss;; ttoo vveerriiffyy eelliiggiibbiilliittyy;; ttoo
ccoommppllyy wwiitthh ffeeddeerraall,, ssttaattee oorr llooccaall llaawwss;; ffoorr
ccoooorrddiinnaattiioonn ooff bbeenneeffiittss;; ffoorr ssuubbrrooggaattiioonn;; iinn
rreessppoonnssee ttoo aa cciivviill oorr ccrriimmiinnaall aaccttiioonn uuppoonn
iissssuuaannccee ooff aa ssuubbppooeennaa,, oorr wwiitthh tthhee wwrriitttteenn
ccoonnsseenntt ooff tthhee CCoovveerreedd PPeerrssoonn oorr hhiiss oorr hheerr lleeggaall
rreepprreesseennttaattiivvee..
33..1111 PPrroovviiddee aanndd mmaaiinnttaaiinn aa ssppeecciimmeenn PPllaann DDooccuummeenntt aanndd SSuummmmaarryy PPllaann DDeessccrriippttiioonn iinn aa ffoorrmmaatt
aacccceeppttaabbllee ttoo tthhee TTPPAA ffoorr rreevviieeww aanndd ffiinnaall
aapppprroovvaall bbyy tthhee PPllaann SSppoonnssoorr aanndd tthhee PPllaann
SSppoonnssoorr’’ss lleeggaall ccoouunnsseell.. UUppoonn aapppprroovvaall ooff tthhee
PPllaann DDooccuummeenntt ffrroomm tthhee PPllaann SSppoonnssoorr,, tthhee TTPPAA
wwiillll ffoorrwwaarrdd ccooppiieess ooff ppllaann ddooccuummeenntt aanndd
aammeennddmmeennttss,, iiff aannyy,, ttoo tthhee SSttoopp LLoossss oorr EExxcceessss
LLoossss iinnssuurraannccee ccoommppaannyy..
TThhee TTPPAA wwiillll ffuurrnniisshh aa mmaasstteerr SSuummmmaarryy PPllaann
DDeessccrriippttiioonn ttoo tthhee PPllaann SSppoonnssoorr,, eeiitthheerr
eelleeccttrroonniiccaallllyy ((PPDDFF ffoorrmmaatt)),, oorr iinn pprriinntteedd ffoorrmm,,
aanndd SSuummmmaarryy PPllaann DDeessccrriippttiioonn bbooookklleettss iinn TTPPAA’’ss
ffoorrmmaatt ffoorr tthhee ffeeeess ssttaatteedd iinn AAppppeennddiixx AA..
TThhee TTPPAA wwiillll mmaaiinnttaaiinn aann eelleeccttrroonniicc CCllaaiimmss ffiillee oonn
eevveerryy CCllaaiimm rreeppoorrtteedd ttoo iitt bbyy tthhee CCoovveerreedd
PPeerrssoonnss.. TThhee TTPPAA sshhaallll rreettaaiinn ssuucchh ffiilleess aanndd aallll
PPllaann--rreellaatteedd iinnffoorrmmaattiioonn ffoorr aa ppeerriioodd ooff ssiixx ((66))
yyeeaarrss.. CCooppiieess ooff ssuucchh rreeccoorrddss sshhaallll bbee mmaaddee aavvaaiillaabbllee ttoo tthhee PPllaann SSppoonnssoorr ffoorr iinnssppeeccttiioonn
dduurriinngg aa rreegguullaarrllyy sscchheedduulleedd WWoorrkkiinngg DDaayy aatt tthhee
ooffffiiccee ooff tthhee TTPPAA ffoorr ccoonnssuullttaattiioonn,, rreevviieeww aanndd
aauuddiitt uuppoonn aaddvvaannccee nnoottiiccee ooff aa mmiinniimmuumm ooff
ffoouurrtteeeenn ((1144)) WWoorrkkiinngg DDaayyss..
TThhee PPllaann SSppoonnssoorr sshhaallll ppaayy ffoorr aannyy aauuddiitt mmaaddee aatt
iittss rreeqquueesstt..
IInn tthhee eevveenntt tthhiiss AAggrreeeemmeenntt iiss tteerrmmiinnaatteedd,, tthhee
PPllaann SSppoonnssoorr sshhaallll hhaavvee aa ccoonnttiinnuuiinngg oobblliiggaattiioonn
aanndd lliiaabbiilliittyy ttoo ppaayy tthhee TTPPAA ffoorr aallll ccoossttss aanndd
pprrooffeessssiioonnaall,, eexxeeccuuttiivvee,, mmaannaaggeerriiaall aanndd cclleerriiccaall
ttiimmee eexxppeennddeedd bbyy tthhee TTPPAA aanndd iittss eemmppllooyyeeeess ffoorr
aannyy aauuddiitt ccoonndduucctteedd bbyy tthhee PPllaann SSppoonnssoorr oorr iittss
SSttoopp LLoossss oorr EExxcceessss LLoossss iinnssuurraannccee ccoommppaannyy,, aanndd

tthhiiss oobblliiggaattiioonn aanndd lliiaabbiilliittyy sshhaallll ssuurrvviivvee aanndd
ccoonnttiinnuuee bbeeyyoonndd tthhee tteerrmmiinnaattiioonn ooff tthhiiss
AAggrreeeemmeenntt.. TThhee PPllaann SSppoonnssoorr sshhaallll ppaayy aann
aaddvvaannccee rreettaaiinneerr ttoo tthhee TTPPAA ffoorr aannyy aauuddiitt aassssiissttaannccee aatt aannyy ttiimmee tthhee TTPPAA rreecceeiivveess nnoottiiccee
ffrroomm tthhee PPllaann SSppoonnssoorr oorr iittss SSttoopp LLoossss oorr EExxcceessss
LLoossss iinnssuurraannccee ccoommppaannyy ooff aann aauuddiitt ttoo bbee
ccoonndduucctteedd aafftteerr tthhee tteerrmmiinnaattiioonn ddaattee ooff tthhiiss
AAggrreeeemmeenntt.. TThhee aaddvvaannccee rreettaaiinneerr sshhaallll bbee iinn aann
aammoouunntt ttoo bbee ddeetteerrmmiinneedd bbyy tthhee TTPPAA iinn
eessttiimmaattiioonn ooff tthhee eexxttrraa ttiimmee rreeqquuiirreedd ffoorr tthhee
ssccooppee ooff tthhee aauuddiitt tthhaatt iiss rreeqquueesstteedd.. IInn nnoo eevveenntt
sshhaallll tthhee aauuddiitt rreettaaiinneerr ffeeee bbee lleessss tthhaann TTwwoo
TThhoouussaanndd FFiivvee HHuunnddrreedd aanndd nnoo//110000 DDoollllaarrss (($$22,,550000..0000)).. TThhee TTPPAA wwiillll nnoott bbee rreeqquuiirreedd bbyy tthhee
PPllaann SSppoonnssoorr ttoo pprroovviiddee aacccceessss ttoo iittss rreeccoorrddss,, nnoorr
wwiillll aannyy ooff tthhee TTPPAA’’ss eemmppllooyyeeeess pprroovviiddee
aassssiissttaannccee ttoo aannyy aauuddiittoorr uunnttiill rreecceeiipptt bbyy tthhee TTPPAA
ooff tthhee rreeqquuiirreedd aauuddiitt rreettaaiinneerr ffeeee..
AAnnyy aauuddiitt sshhaallll bbee ccoonndduucctteedd bbyy aann aauuddiittoorr
mmuuttuuaallllyy aacccceeppttaabbllee ttoo tthhee PPllaann SSppoonnssoorr aanndd tthhee
TTPPAA aanndd tthhee aauuddiitt sshhaallll iinncclluuddee,, bbuutt nnoott
nneecceessssaarriillyy bbee lliimmiitteedd ttoo,, pprroodduucciinngg pphhoottooccooppiieess
ooff CCllaaiimmss aanndd ffuunnddiinngg iinnffoorrmmaattiioonn iinn tthhee TTPPAA’’ss
eexxiissttiinngg ffoorrmmaatt((ss)),, aa rreevviieeww ooff pprroocceedduurraall
ccoonnttrroollss,, aa rreevviieeww ooff ssyysstteemm ccoonnttrroollss,, aa rreevviieeww ooff
PPllaann pprroovviissiioonnss,, aa rreevviieeww ooff ssaammpplleedd CCllaaiimmss,, aanndd
ccoommppaarriissoonn ooff rreessuullttss ttoo TTPPAA iinndduussttrryy
ppeerrffoorrmmaanncceess ssttaannddaarrddss oorr aannyy ssttaattiissttiiccaall mmooddeellss
pprreevviioouussllyy aaggrreeeedd ttoo bbyy tthhee PPllaann SSppoonnssoorr aanndd tthhee
TTPPAA iinn wwrriittiinngg..
NNootthhiinngg iinn tthhiiss AAggrreeeemmeenntt,, eexxpprreesssseedd oorr iimmpplliieedd,, sshhaallll rreeqquuiirree tthhee TTPPAA ddiisscclloossee aannyy pprroopprriieettaarryy
iinnffoorrmmaattiioonn,, iinncclluuddiinngg,, bbuutt nnoott lliimmiitteedd,, ffiillee llaayyoouutt
oorr rreeccoorrdd ffoorrmmaattss ooff iittss CCllaaiimmss pprroocceessssiinngg ssyysstteemm
oorr pprroocceedduurreess.. FFuurrtthheerr,, eexxcceepptt ffoorr tthhoossee rreeppoorrttss
aanndd ddaattaa eexxttrraaccttss aaggrreeeedd ttoo sseeppaarraatteellyy iinn wwrriittiinngg,,
nnootthhiinngg iinn tthhiiss AAggrreeeemmeenntt,, eexxpprreesssseedd oorr iimmpplliieedd
sshhaallll rreeqquuiirree TTPPAA ttoo pprroovviiddee rreeccoorrddss oorr
iinnffoorrmmaattiioonn iinn aa ffoorrmmaatt nnoott iinn uussee bbyy tthhee TTPPAA,, oorr
ttoo ccrreeaattee uunniiqquuee iinnffoorrmmaattiioonn ffoorrmmaattss ssoolleellyy ffoorr
tthhee uussee ooff tthhee aauuddiittoorr((ss)),, ccoonnssuullttaanntt((ss)),, aaggeenntt((ss))
oorr bbrrookkeerr((ss)) ffoorr tthhee PPllaann SSppoonnssoorr wwiitthhoouutt mmuuttuuaall
aaggrreeeemmeenntt oorr wwiitthhoouutt ppaayymmeenntt ooff ffeeeess aatt tthhee
nnoorrmmaall hhoouurrllyy rraattee cchhaannggeedd ffoorr ssuucchh sseerrvviicceess aass
nnootteedd iinn AAppppeennddiixx AA..
33..1122 UUppoonn rreeqquueesstt ooff tthhee PPllaann SSppoonnssoorr,, pprroovviiddee CCOOBBRRAA
ccoonnttiinnuuaattiioonn ccoovveerraaggee sseerrvviicceess tthhrroouugghh aa rreellaatteedd
ccoorrppoorraattiioonn,, AAlllleeggiiaannccee CCOOBBRRAA SSeerrvviicceess,, IInncc..
((AACCSSII)).. AA sseeppaarraattee ffeeee wwiillll bbee cchhaarrggeedd ffoorr CCOOBBRRAA
ccoonnttiinnuuaattiioonn sseerrvviicceess,, wwhhiicchh ffeeee iiss sseett oouutt iinn aa CCOOBBRRAA SSeerrvviicceess AAggrreeeemmeenntt.. IIff tthhee PPllaann SSppoonnssoorr
ddooeess nnoott rreeqquueesstt CCOOBBRRAA ccoonnttiinnuuaattiioonn sseerrvviicceess
ffrroomm AACCSSII,, aallll rreessppoonnssiibbiilliittyy aanndd lliiaabbiilliittyy ffoorr
aaddmmiinniissttrraattiioonn ooff CCOOBBRRAA ccoonnttiinnuuaattiioonn sshhaallll
rreemmaaiinn wwiitthh tthhee PPllaann SSppoonnssoorr,, aanndd nneeiitthheerr tthhee
TTPPAA nnoorr AACCSSII wwiillll hhaavvee aannyy oobblliiggaattiioonn oorr
rreessppoonnssiibbiilliittyy ffoorr pprroovviiddiinngg ssuucchh sseerrvviicceess oorr
ccoonnssuullttaattiioonn rreeggaarrddiinngg ssuucchh sseerrvviicceess..

33..1133 PPrroovviiddee tthhee ffoolllloowwiinngg rreeppoorrttss::
((aa)) mmoonntthhllyy ssuummmmaarryy ooff bbeenneeffiittss
ppaaiidd aannaallyyssiiss bbyy ttyyppee ooff CCllaaiimm aanndd ttoottaall ddoollllaarr aammoouunnttss;;
((bb)) mmoonntthhllyy cchheecckk rreeggiisstteerr;;
((cc)) mmoonntthhllyy ccuummuullaattiivvee aaggggrreeggaattee
ddeedduuccttiibbllee ttoo ppaaiidd CCllaaiimmss rreeppoorrtt;;
((dd)) aannnnuuaall ssuummmmaarryy mmaannaaggeemmeenntt
rreeppoorrtt wwiitthhiinn ssiixxttyy ((6600)) ddaayyss aafftteerr tthhee
cclloossee ooff tthhee PPllaann YYeeaarr;;
((ee)) aannnnuuaall lloossss aannaallyyssiiss rreeppoorrtt;; aanndd
((ff)) ssppeecciiaall rreeppoorrttss rreeqquueesstteedd bbyy tthhee
PPllaann SSppoonnssoorr wwhhiicchh tthhee TTPPAA aaggrreeeess ttoo pprroodduuccee,, aanndd ssuubbjjeecctt ttoo aa ffeeee aaddddrreesssseedd
iinn AAppppeennddiixx AA..
33..1155 IIff aapppplliiccaabbllee::
((aa)) NNoottiiffyy tthhee SSttoopp LLoossss oorr EExxcceessss
LLoossss iinnssuurraannccee ccoommppaannyy ooff aannyy ppootteennttiiaall
llaarrggee CCllaaiimmss,, wwhhiicchh mmaayy bbeeccoommee aa CCllaaiimm
uunnddeerr tthhee SSttoopp LLoossss oorr EExxcceessss LLoossss
ccoovveerraaggee..
((bb)) OOnn bbeehhaallff ooff tthhee PPllaann SSppoonnssoorr,,
tthhee TTPPAA wwiillll ffiillee wwiitthh tthhee iinnssuurraannccee
ccoommppaannyy oorr iittss ddeessiiggnneeee aannyy CCoommpplleettee
CCllaaiimmss ffoorr ccoonnssiiddeerraattiioonn ffoorr
rreeiimmbbuurrsseemmeenntt uunnddeerr tthhee SSttoopp LLoossss oorr
EExxcceessss LLoossss ppoolliicciieess..
((cc)) PPrroommppttllyy ffoorrwwaarrdd ttoo tthhee PPllaann
SSppoonnssoorr aannyy pprreemmiiuumm,, ccllaaiimm
rreeiimmbbuurrsseemmeenntt,, SSttoopp LLoossss oorr EExxcceessss LLoossss
oorr ootthheerr nnoottiicceess rreecceeiivveedd ffrroomm tthhee SSttoopp LLoossss oorr EExxcceessss LLoossss iinnssuurraannccee ccaarrrriieerr
ccoonncceerrnniinngg tthhee ppoolliiccyy..
33..1166 IIff aapppplliiccaabbllee,, ccoonndduucctt uuttiilliizzaattiioonn rreevviieeww ffoorr tthhee
PPllaann,, iinncclluuddiinngg pprree--cceerrttiiffiiccaattiioonn ooff hhoossppiittaall ssttaayyss,,
ccoonnccuurrrreenntt rreevviieeww ooff hhoossppiittaall ssttaayyss,, ddiisscchhaarrggee
ppllaannnniinngg,, pprreelliimmiinnaarryy rreevviieeww ffoorr ppootteennttiiaall hhoossppiittaall
bbiillll aauuddiittss,, llaarrggee ccaassee mmaannaaggeemmeenntt oorr aannyy ootthheerr
mmaannaaggeedd ccaarree pprrooggrraammss aass aaggrreeeedd ttoo bbeettwweeeenn
tthhee PPllaann SSppoonnssoorr aanndd tthhee TTPPAA.. AA sseeppaarraattee ffeeee wwiillll
bbee cchhaarrggeedd ffoorr tthheessee sseerrvviicceess aass ssttaatteedd iinn
AAppppeennddiixx AA..
33..1177 MMaaiinnttaaiinn wwoorrkkiinngg rreellaattiioonnsshhiippss wwiitthh nneettwwoorrkkss ooff
HHeeaalltthh CCaarree PPrroovviiddeerrss tthhrroouugghh PPrreeffeerrrreedd PPrroovviiddeerr
OOrrggaanniizzaattiioonnss ((PPPPOO)) ccoonnttrraacctteedd bbyy tthhee PPllaann
SSppoonnssoorr oorr aarrrraannggeedd bbyy tthhee TTPPAA.. TThhee TTPPAA sshhaallll bbee
eennttiittlleedd ttoo rreellyy uuppoonn aannyy aanndd aallll rreepprreesseennttaattiioonnss
mmaaddee bbyy HHeeaalltthh CCaarree PPrroovviiddeerrss//PPPPOO rreeggaarrddiinngg
tthheeiirr qquuaalliiffiiccaattiioonnss aass HHeeaalltthh CCaarree PPrroovviiddeerrss,, aanndd sshhaallll hhaavvee nnoo oobblliiggaattiioonn oorr lliiaabbiilliittyy ttoo oobbttaaiinn,,
vveerriiffyy oorr mmoonniittoorr ssuucchh qquuaalliiffiiccaattiioonnss oorr
ccrreeddeennttiiaallss..
IIff aapppplliiccaabbllee,, aa sseeppaarraattee ffeeee wwiillll bbee cchhaarrggeedd ffoorr
PPPPOO nneettwwoorrkk sseerrvviicceess,, TTPPAA ccoooorrddiinnaattiioonn aanndd
ssyysstteemm mmaaiinntteennaannccee ffoorr PPPPOO nneettwwoorrkkss,, aass ssttaatteedd
iinn FFeeee SScchheedduullee,, AAppppeennddiixx AA..
TThhee TTPPAA wwiillll nnoott bbee rreessppoonnssiibbllee ffoorr aannyy sseerrvviicceess
pprroovviiddeedd ((oorr aannyy ffaaiilluurree ttoo pprroovviiddee sseerrvviicceess)) bbyy aa ppaarrttiicciippaattiinngg PPPPOO oorr HHeeaalltthh CCaarree PPrroovviiddeerrss aanndd
ssppeecciiffiiccaallllyy mmaakkeess nnoo rreepprreesseennttaattiioonn,, wwaarrrraannttyy oorr
gguuaarraanntteeee wwhhaattssooeevveerr rreeggaarrddiinngg aannyy ssuucchh PPPPOO,,
HHeeaalltthh CCaarree PPrroovviiddeerrss,, oorr tthheeiirr rreepprreesseennttaattiioonnss,,
qquuaalliiffiiccaattiioonnss oorr ccrreeddeennttiiaallss..
33..1188 IIff cchheecckkeedd aass aann iinncclluuddeedd sseerrvviiccee iinn AAppppeennddiixx AA,,
tthhee TTPPAA wwiillll pprroovviiddee ccoooorrddiinnaattiioonn ooff sseerrvviicceess ffoorr
wweellllnneessss aanndd hheeaalltthh aasssseessssmmeenntt tthhrroouugghh aa tthhiirrdd
ppaarrttyy vveennddoorr,, BBeehhaavviioorraall HHeeaalltthh CCaarree OOppttiioonnss,, IInncc..
33..1199 PPrroovviiddee,, wwiitthhiinn tthhiirrttyy ((3300)) ddaayyss aafftteerr tteerrmmiinnaattiioonn
ooff tthhiiss AAggrreeeemmeenntt,, aa ssuummmmaarryy ppaaiidd CCllaaiimm rreeppoorrtt
ooff aallll CCllaaiimmss ppaaiidd ttwweennttyy--ffoouurr ((2244)) mmoonntthhss pprriioorr ttoo
tthhee ddaattee ooff tteerrmmiinnaattiioonn,, ccooppiieess ooff aannyy
ggoovveerrnnmmeennttaall rreeppoorrttss,, aanndd ootthheerr ppllaann
ddooccuummeennttaattiioonn ttoo tthhee PPllaann SSppoonnssoorr.. UUnnttiill tthhaatt
ttiimmee,, tthheessee rreeccoorrddss wwiillll bbee mmaaiinnttaaiinneedd aatt tthhee
TTPPAA’’ss pprriinncciippaall aaddmmiinniissttrraattiivvee ooffffiiccee.. CCllaaiimm ffiilleess
wwiillll bbee kkeepptt iinn sseeccuurree ssttoorraaggee ffaacciilliittiieess oorr eelleeccttrroonniicc mmeeddiiaa ffoorr aatt lleeaasstt ssiixx ((66)) yyeeaarrss ffoolllloowwiinngg
tthhee tteerrmmiinnaattiioonn ooff tthhee PPllaann YYeeaarr.. CCooppiieess ooff aannyy
mmaatteerriiaallss iinn ssttoorraaggee wwiillll bbee aavvaaiillaabbllee ttoo tthhee PPllaann
SSppoonnssoorr ffoorr aa ccooppyy ffeeee ooff ffiifftteeeenn (($$..1155)) cceennttss ppeerr
ppaaggee ccooppiieedd pplluuss aa rreettrriieevvaall ffeeee ooff TTeenn DDoollllaarrss
(($$1100..0000)) ppeerr bbooxx oorr eelleeccttrroonniicc mmeeddiiaa aacccceessss.. AAtt
tthhee eenndd ooff tthhee ssiixx ((66)) yyeeaarr ppeerriioodd oorr tteerrmmiinnaattiioonn
ooff tthhiiss AAggrreeeemmeenntt,, iiff eeaarrlliieerr,, tthhee TTPPAA sshhaallll nnoottiiffyy
tthhee PPllaann SSppoonnssoorr tthhaatt tthheessee rreeccoorrddss wwiillll bbee
ddeessttrrooyyeedd..
UUppoonn tteerrmmiinnaattiioonn ooff tthhiiss AAggrreeeemmeenntt,, pprroovviiddee aallll
nnoottiicceess aanndd ddooccuummeennttss ttoo tthhee PPllaann SSppoonnssoorr aanndd
ttoo tthhee TTeexxaass DDeeppaarrttmmeenntt ooff IInnssuurraannccee aass aarree
rreeqquuiirreedd uunnddeerr AApppplliiccaabbllee TTeexxaass ssttaattuutteess aanndd
rreegguullaattiioonnss..

33..2200 PPrroovviiddee CCeerrttiiffiiccaatteess ooff CCrreeddiittaabbllee CCoovveerraaggee aanndd
ootthheerr CCrreeddiittaabbllee CCoovveerraaggee sseerrvviicceess aass rreeqquuiirreedd bbyy
HHIIPPAAAA ffoorr eemmppllooyyeeeess ooff tthhee PPllaann SSppoonnssoorr aanndd tthheeiirr eelliiggiibbllee ddeeppeennddeennttss..
33..2211 PPrroovviiddee MMeeddiiccaarree,, MMSSPP,, aanndd §§111111 rreeppoorrttiinngg
sseerrvviicceess..
33..2222 PPrroovviiddee nnoonn--pprroopprriieettaarryy iinnffoorrmmaattiioonn aanndd
ddooccuummeennttss aass rreeqquueesstteedd bbyy tthhee PPllaann SSppoonnssoorr ttoo
rreepprreesseennttaattiivveess ddeessiiggnnaatteedd bbyy tthhee PPllaann SSppoonnssoorr..
HHoowweevveerr,, iiff tthhee PPllaann SSppoonnssoorr hhaass eenntteerreedd iinnttoo aann
aaggrreeeemmeenntt wwiitthh aannyy nneeww rreepprreesseennttaattiivvee,, aanndd tthhee TTPPAA hhaass nnoottiiccee ooff tthhee ssaammee,, tthhee TTPPAA sshhaallll nnoott bbee
rreeqquuiirreedd ttoo pprroovviiddee aannyy iinnffoorrmmaattiioonn oorr
ddooccuummeennttaattiioonn ttoo ootthheerr rreepprreesseennttaattiivveess uunnlleessss oorr
uunnttiill tthhee PPllaann SSppoonnssoorr hhaass tteerrmmiinnaatteedd tthhee oorriiggiinnaall
rreepprreesseennttaattiivvee aaggrreeeemmeenntt aanndd nnoottiiffiieedd tthhee
oorriiggiinnaall rreepprreesseennttaattiivvee ooff tthhee tteerrmmiinnaattiioonn.. TThhee
TTPPAA sshhaallll hhaavvee tthhee eexxpprreessss rriigghhtt ttoo ccoonnttaacctt aannyy
rreepprreesseennttaattiivvee ttoo vveerriiffyy tthhee rreepprreesseennttaattiivvee
aaggrreeeemmeenntt hhaass bbeeeenn tteerrmmiinnaatteedd.. AA sseeppaarraattee ffeeee
wwiillll bbee cchhaarrggeedd ffoorr tthhiiss sseerrvviiccee aass ssttaatteedd iinn
AAppppeennddiixx AA..
33..2233 FFoorr PPllaann SSppoonnssoorrss wwhhiicchh hhaavvee ddeessiiggnnaatteedd
ssuubbssiiddiiaarriieess,, ddiivviissiioonnss,, oorr wwhhiicchh aarree aa MMuullttiippllee
EEmmppllooyyeerr WWeellffaarree AArrrraannggeemmeenntt ((MMEEWWAA)):: wwhheenn
aannyy ddeessiiggnnaatteedd ssuubbssiiddiiaarryy,, ddiivviissiioonn oorr mmeemmbbeerr
eemmppllooyyeerr ooff aa MMEEWWAA tteerrmmiinnaatteess ccoovveerraaggee uunnddeerr
tthhee ppllaann tthhaatt iiss tthhee ssuubbjjeecctt ooff tthhiiss AAggrreeeemmeenntt,, tthhee
TTPPAA wwiillll aauuttoommaattiiccaallllyy ppeerrffoorrmm rruunn--oouutt sseerrvviicceess
ffoorr aa ppeerriioodd ooff tthhrreeee ((33)) mmoonntthhss aafftteerr tthhee ddaattee ooff ssuucchh tteerrmmiinnaattiioonn ffoorr ssuucchh ddeessiiggnnaatteedd ssuubbssiiddiiaarryy,,
ddiivviissiioonn oorr mmeemmbbeerr eemmppllooyyeerr,, uunnlleessss ddiirreecctteedd nnoott
ttoo ddoo ssoo bbyy tthhee PPllaann SSppoonnssoorr iinn wwrriittiinngg.. TThhee ffeeee
ffoorr eeaacchh mmoonntthh ooff rruunn--oouutt sseerrvviicceess wwiillll bbee eeqquuaall
ttoo tthhee ccllaaiimmss pprroocceessssiinngg ffeeee((ss)) ssttaatteedd iinn AAppppeennddiixx
AA,, bbaasseedd uuppoonn tthhee ddeessiiggnnaatteedd ssuubbssiiddiiaarryy’’ss,,
ddiivviissiioonn’’ss oorr MMEEWWAA mmeemmbbeerr eemmppllooyyeerr’’ss nnuummbbeerr
ooff eennrroolllleedd PPllaann PPaarrttiicciippaannttss ffoorr tthhee mmoonntthh
iimmmmeeddiiaatteellyy pprriioorr ttoo tthhee ddaattee ooff tteerrmmiinnaattiioonn ooff
ccoovveerraaggee.. PPllaann SSppoonnssoorr wwiillll aallssoo ppaayy tthhee TTPPAA rruunn--
oouutt sseerrvviicceess ffeeeess ffoorr aannyy eennrroolllleedd PPllaann
PPaarrttiicciippaannttss wwhhoo wweerree llaaiidd--ooffff oorr ootthheerrwwiissee
tteerrmmiinnaatteedd ffrroomm tthhee rroollllss ooff tthhee PPllaann dduurriinngg tthhee
tteerrmm ooff tthhiiss AAggrreeeemmeenntt iiff tthhee ttoottaall nnuummbbeerr ooff
ssuucchh llaaiidd--ooffff oorr tteerrmmiinnaatteedd PPllaann PPaarrttiicciippaannttss
eexxcceeeeddss ffiivvee ((55%%)) ppeerrcceenntt ooff tthhee ttoottaall nnuummbbeerr ooff
eennrroolllleedd PPllaann PPaarrttiicciippaannttss dduurriinngg tthhee ffiirrsstt mmoonntthh
ooff tthhiiss AAggrreeeemmeenntt.. FFiinnaall rreeccoonncciilliiaattiioonn ooff rruunn--oouutt
sseerrvviicceess ffeeeess wwiillll bbee mmaaddee wwiitthhiinn nniinneettyy ((9900)) ddaayyss
ooff tthhee eenndd ooff tthhiiss AAggrreeeemmeenntt..
33..2244 FFeeeess ffoorr tthhee sseerrvviicceess ddeessccrriibbeedd iinn AArrttiiccllee IIIIII aarree sseett
oouutt iinn AAppppeennddiixx AA hheerreettoo.. SSuucchh ffeeeess aarree ffiixxeedd ffoorr
tthhee iinniittiiaall tteerrmm ooff tthhiiss AAggrreeeemmeenntt eexxcceepptt tthhaatt
uuppoonn ssiixxttyy ((6600)) ddaayyss pprriioorr nnoottiiccee ttoo PPllaann SSppoonnssoorr,,
tthhee ffeeeess aarree ssuubbjjeecctt ttoo cchhaannggee uunnddeerr tthhee ffoolllloowwiinngg
ccoonnddiittiioonnss::
((aa)) iiff tthhee PPllaann SSppoonnssoorr’’ss cceennssuuss ooff
eennrroolllleedd eemmppllooyyeeeess iinnccrreeaasseess oorr ddeeccrreeaasseess bbyy mmoorree tthhaann tteenn ((1100%%))
ppeerrcceenntt ffrroomm tthhee nnuummbbeerr ooff eemmppllooyyeeeess
tthhaatt wweerree eennrroolllleedd oonn tthhee ccoommmmeennccee ooff
tthhiiss AAggrreeeemmeenntt;;
((bb)) iiff tthhee PPllaann SSppoonnssoorr ssiiggnniiffiiccaannttllyy
aalltteerrss tthhee ddeessiiggnn oorr ccoommpplleexxiittyy ooff iittss
hheeaalltthh bbeenneeffiitt ppllaann;; oorr
((cc)) rreegguullaarrllyy rreeqquueessttiinngg aanndd
oobbttaaiinniinngg eexxttrraa--ccoonnttrraaccttuuaall sseerrvviicceess ffrroomm
tthhee TTPPAA..
33..2255 TThhee TTPPAA wwiillll ccoommppllyy wwiitthh tthhee aapppplliiccaabbllee
llaawwss aanndd rruulleess ffoorr tthhee ssttoorraaggee,, ttrraannssmmiissssiioonn aanndd
rreelleeaassee ooff aannyy ““pprrootteecctteedd hheeaalltthh iinnffoorrmmaattiioonn””
((uusseedd hheerreeiinn aass ssuucchh ddeeffiinneedd iinn HHIIPPAAAA))..
NNoottwwiitthhssttaannddiinngg aannyy ootthheerr pprroovviissiioonn ooff tthhiiss
AAggrreeeemmeenntt,, tthhee TTPPAA sshhaallll nnoott bbee rreeqquuiirreedd ttoo ddoo
aannyy aacctt wwhhiicchh iinn iittss jjuuddggmmeenntt vviioollaatteess tthhee HHIIPPAAAA
AAddmmiinniissttrraattiivvee SSiimmpplliiffiiccaattiioonn oorr HHii TTeecchh SSeeccuurriittyy
rruulleess..
33..2266 TThhee TTPPAA wwiillll pprroovviiddee ccoonnssoolliiddaatteedd bbiilllliinngg
sseerrvviicceess iiff cchheecckkeedd aass aann iinncclluuddeedd sseerrvviiccee iinn
AAppppeennddiixx AA.. SSppeecciiffiiccaallllyy,, tthhee TTPPAA wwiillll bbiillll ffeeeess aanndd
pprreemmiiuummss ffoorr ootthheerr eemmppllooyyeeee bbeenneeffiittss iinncclluuddiinngg,,
bbuutt nnoott lliimmiitteedd ttoo,, ggrroouupp lliiffee,, ggrroouupp AADD&&DD aanndd//oorr
ggrroouupp sshhoorrtt tteerrmm aanndd lloonngg tteerrmm ddiissaabbiilliittyy ttoo tthhee
PPllaann SSppoonnssoorr,, aanndd wwiillll rreemmiitt tthhee pprreemmiiuumm
ccoolllleecctteedd ttoo tthhee aapppplliiccaabbllee ccaarrrriieerr..
AARRTTIICCLLEE IIVV::
TTHHEE PPLLAANN SSPPOONNSSOORR’’SS RREESSPPOONNSSIIBBIILLIITTIIEESS
TThhee PPllaann SSppoonnssoorr oorr EEmmppllooyyeerr wwiillll::
44..11 EEssttaabblliisshh tthhee PPllaann ttooggeetthheerr wwiitthh aa ffrraammeewwoorrkk ooff

ppoolliicciieess,, iinntteerrpprreettaattiioonnss aanndd rruulleess,, wwhhiicchh sshhaallll bbee
tthhee bbaassiiss ffoorr tthhee TTPPAA’’ss ppeerrffoorrmmaannccee ooff iittss dduuttiieess
uunnddeerr tthhiiss AAggrreeeemmeenntt..
MMaaiinnttaaiinn ccuurrrreenntt aanndd aaccccuurraattee PPllaann eelliiggiibbiilliittyy aanndd
ccoovveerraaggee rreeccoorrddss,, vveerriiffyy CCoovveerreedd PPeerrssoonn eelliiggiibbiilliittyy
aanndd ssuubbmmiitt eelliiggiibbiilliittyy aanndd ccoovveerraaggee iinnffoorrmmaattiioonn
mmoonntthhllyy,, oorr mmoorree oofftteenn iiff rreeqquueesstteedd bbyy tthhee TTPPAA,,
ttoo tthhee TTPPAA aatt iittss ddeessiiggnnaatteedd eelleeccttrroonniicc oorr ppoossttaall
aaddddrreessss..
TThhiiss iinnffoorrmmaattiioonn sshhaallll bbee pprroovviiddeedd iinn aa ffoorrmmaatt
aacccceeppttaabbllee ttoo tthhee TTPPAA aanndd sshhaallll iinncclluuddee tthhee
ffoolllloowwiinngg ffoorr eeaacchh CCoovveerreedd PPeerrssoonn:: nnaammee aanndd aaddddrreessss,, SSoocciiaall SSeeccuurriittyy nnuummbbeerr,, ddaattee ooff bbiirrtthh,,
ttyyppee ooff ccoovveerraaggee,, sseexx,, rreellaattiioonnsshhiipp ttoo eemmppllooyyeeee,,
cchhaannggeess iinn ccoovveerraaggee,, ddaattee ccoovveerraaggee bbeeggiinnss oorr
eennddss,, aanndd aannyy ootthheerr iinnffoorrmmaattiioonn aass nneecceessssaarryy ttoo
ddeetteerrmmiinnee eelliiggiibbiilliittyy aanndd ccoovveerraaggee uunnddeerr tthhee PPllaann..
TThhee PPllaann SSppoonnssoorr aassssuummeess tthhee rreessppoonnssiibbiilliittyy ffoorr
aanndd wwiillll hhoolldd tthhee TTPPAA hhaarrmmlleessss ffrroomm tthhee
eerrrroonneeoouuss ddiissbbuurrsseemmeenntt ooff bbeenneeffiittss bbyy tthhee TTPPAA iinn
tthhee eevveenntt ooff eerrrroorr oorr nneegglleecctt bbyy tthhee PPllaann SSppoonnssoorr
oorr EEmmppllooyyeerr iinn pprroovviiddiinngg eelliiggiibbiilliittyy aanndd ccoovveerraaggee
iinnffoorrmmaattiioonn ttoo tthhee TTPPAA,, iinncclluuddiinngg,, bbuutt nnoott lliimmiitteedd
ttoo,, ffaaiilluurree ttoo ggiivvee ttiimmeellyy nnoottiiffiiccaattiioonn iiff iinneelliiggiibbiilliittyy
oorr tteerrmmiinnaattiioonn ooff aa ffoorrmmeerr CCoovveerreedd PPeerrssoonn,, oorr
ffrraauudduulleenntt eennrroollllmmeenntt aanndd//oorr ccoonnttiinnuuaattiioonn ooff
ccoovveerraaggee..
44..22 TThhee TTPPAA sshhaallll mmaakkee rreeccoommmmeennddaattiioonnss rreeggaarrddiinngg
CCllaaiimmss ddeetteerrmmiinnaattiioonnss.. TThhee SSppoonnssoorr sshhaallll hhaavvee
tthhee ssoollee aauutthhoorriittyy ttoo rreessoollvvee aallll PPllaann aammbbiigguuiittiieess aanndd iinntteerrpprreettaattiioonnss,, qquueessttiioonnss aanndd ddiissppuutteess
rreellaattiinngg ttoo tthhee PPllaann eelliiggiibbiilliittyy ooff aa CCoovveerreedd PPeerrssoonn,,
PPllaann ccoovveerraaggee aanndd ddeenniieedd CCllaaiimmss..
TThhee PPllaann SSppoonnssoorr sshhaallll hhaavvee tthhee ssoollee aauutthhoorriittyy ttoo
mmaakkee ddeetteerrmmiinnaattiioonnss rreeggaarrddiinngg aappppeeaall ooff ddeenniieedd
CCllaaiimmss.. TThhee PPllaann SSppoonnssoorr wwiillll rreessppoonndd ttoo aannyy
wwrriitttteenn rreeqquueesstt ffoorr iinnffoorrmmaattiioonn mmaaddee bbyy tthhee TTPPAA
wwiitthhiinn tteenn ((1100)) WWoorrkkiinngg DDaayyss ooff rreecceeiipptt ooff tthhee
rreeqquueesstt..
RReessoollvvee aallll PPllaann aammbbiigguuiittiieess,, qquueessttiioonnss aanndd
ddiissppuutteess rreellaattiinngg ttoo tthhee PPllaann eelliiggiibbiilliittyy ooff aa
CCoovveerreedd PPeerrssoonn,, PPllaann ccoovveerraaggee,, ddeenniiaall ooff CCllaaiimmss
oorr ddeecciissiioonnss rreeggaarrddiinngg aappppeeaall oorr ddeenniiaall ooff CCllaaiimmss,,
oorr aannyy ootthheerr PPllaann iinntteerrpprreettaattiioonn qquueessttiioonnss.. TThhee
PPllaann SSppoonnssoorr wwiillll rreessppoonndd ttoo aannyy wwrriitttteenn rreeqquueesstt
mmaaddee bbyy tthhee TTPPAA wwiitthhiinn tteenn ((1100)) WWoorrkkiinngg DDaayyss ooff
rreecceeiipptt ooff tthhee rreeqquueesstt..
TThhee TTPPAA wwiillll aaddmmiinniisstteerr aanndd pprroocceessss CCllaaiimmss iinn
aaccccoorrddaannccee wwiitthh AArrttiiccllee IIIIII iiff tthhee PPllaann DDooccuummeenntt
aanndd SSuummmmaarryy PPllaann ddeessccrriippttiioonn aarree cclleeaarr aanndd
uunnaammbbiigguuoouuss aass ttoo tthhee vvaalliiddiittyy ooff tthhee CCllaaiimmss aanndd
tthhee CCoovveerreedd PPeerrssoonn’’ss eelliiggiibbiilliittyy ffoorr ccoovveerraaggee
uunnddeerr tthhee PPllaann.. TThhee TTPPAA wwiillll hhaavvee nnoo
ddiissccrreettiioonnaarryy aauutthhoorriittyy ttoo iinntteerrpprreett tthhee PPllaann oorr
aaddjjuuddiiccaattee CCllaaiimmss.. IIff pprroocceessssiinngg aa bbeenneeffiitt CCllaaiimm
rreeqquuiirreess iinntteerrpprreettaattiioonn ooff aammbbiigguuoouuss PPllaann
llaanngguuaaggee,, aanndd tthhee PPllaann SSppoonnssoorr hhaass nnoott pprreevviioouussllyy iinnddiiccaatteedd ttoo tthhee TTPPAA tthhee pprrooppeerr iinntteerrpprreettaattiioonn ooff
tthhee llaanngguuaaggee,, tthheenn tthhee PPllaann SSppoonnssoorr wwiillll bbee
rreessppoonnssiibbllee ffoorr rreessoollvviinngg tthhee aammbbiigguuiittyy oorr aannyy
ootthheerr ddiissppuuttee..
IInn aannyy eevveenntt,, tthhee TTPPAA sshhaallll rreellyy uuppoonn tthhee PPllaann
SSppoonnssoorr’’ss ddeecciissiioonn aass ttoo aannyy CCllaaiimm ((wwhheetthheerr oorr
nnoott iitt iinnvvoollvveess aa PPllaann aammbbiigguuiittyy oorr ootthheerr ddiissppuuttee))
aanndd ssuucchh ddeecciissiioonn bbyy tthhee PPllaann SSppoonnssoorr sshhaallll bbee
ffiinnaall aanndd bbiinnddiinngg uunnlleessss mmooddiiffiieedd oorr rreevveerrsseedd bbyy aa
ccoouurrtt oorr rreegguullaattoorryy aaggeennccyy hhaavviinngg jjuurriissddiiccttiioonn
oovveerr ssuucchh CCllaaiimm mmaatttteerr..
44..33 FFuullllyy ffuunndd tthhee CCllaaiimmss PPaayymmeenntt AAccccoouunntt eevveerryy
wweeeekk bbaasseedd uuppoonn tthhee CCllaaiimmss bbaattcchh rreeppoorrtt
pprroovviiddeedd bbyy tthhee TTPPAA..
44..44 SSeett ffuunnddiinngg lleevveellss ffoorr tthhee PPllaann aatt aa mmiinniimmuumm lleevveell
nneecceessssaarryy ttoo ccoovveerr tthhee eexxppeecctteedd CCllaaiimmss ccoossttss,,
aaddmmiinniissttrraattiivvee eexxppeennsseess aanndd iinnccuurrrreedd bbuutt nnoott rreeppoorrtteedd CCllaaiimmss lliiaabbiilliittyy aanndd ffuunndd tthhee PPllaann aatt ssuucchh
lleevveell..
44..55 NNoott rreeqquueesstt oorr rreeqquuiirree tthhee TTPPAA,, uunnddeerr aannyy
cciirrccuummssttaanncceess,, ttoo iissssuuee CCllaaiimmss ddrraaffttss ffoorr CCllaaiimmss,,
ssttoopp lloossss oorr eexxcceessss lloossss iinnssuurraannccee pprreemmiiuummss,, oorr
aannyy ootthheerr ccoossttss aarriissiinngg oouutt ooff tthhee ssuubbjjeecctt mmaatttteerr
ooff tthhiiss AAggrreeeemmeenntt,, uunnlleessss tthhee PPllaann SSppoonnssoorr hhaass ssoo
aauutthhoorriizzeedd aanndd hhaass pprreevviioouussllyy ddeeppoossiitteedd ssuuffffiicciieenntt
ffuunnddss ttoo ccoovveerr ssuucchh CCoommpplleettee CCllaaiimmss oorr ootthheerr
PPllaann eexxppeennssee oobblliiggaattiioonnss aanndd ppaayymmeenntt((ss))..
44..66 PPrroovviiddee tthhee TTPPAA wwiitthh ccooppiieess ooff aannyy aanndd aallll
rreevviissiioonnss oorr cchhaannggeess ttoo tthhee PPllaann aatt lleeaasstt ffiivvee ((55))
WWoorrkkiinngg DDaayyss pprriioorr ttoo tthhee eeffffeeccttiivvee ddaattee ooff tthhee
cchhaannggeess.. FFaaiilluurree ttoo pprroovviiddee ttiimmeellyy nnoottiiccee mmaayy

rreessuulltt iinn aaddddiittiioonnaall ccllaaiimmss pprroocceessssiinngg ffeeeess aass sseett
ffoorrtthh iinn AAppppeennddiixx AA..
44..77 PPrroovviiddee,, aanndd ttiimmeellyy ddiissttrriibbuuttee,, aallll nnoottiicceess aanndd iinnffoorrmmaattiioonn rreeqquuiirreedd ttoo bbee ggiivveenn ttoo CCoovveerreedd
PPeerrssoonnss,, iinncclluuddiinngg SSuummmmaarryy AAnnnnuuaall RReeppoorrttss..
MMaaiinnttaaiinn aanndd ooppeerraattee tthhee PPllaann iinn aaccccoorrddaannccee wwiitthh
aapppplliiccaabbllee llaaww.. MMaaiinnttaaiinn aallll rreeccoorrddkkeeeeppiinngg aanndd
ffiillee aallll ffoorrmmss rreellaattiivvee tthheerreettoo ppuurrssuuaanntt ttoo aannyy
ffeeddeerraall,, ssttaattee oorr llooccaall llaaww,, uunnlleessss tthhiiss AAggrreeeemmeenntt
ssppeecciiffiiccaallllyy aassssiiggnnss ssuucchh dduuttiieess ttoo tthhee TTPPAA..
44..88 AAcckknnoowwlleeddggee tthhaatt iitt iiss tthhee PPllaann SSppoonnssoorr,, PPllaann
AAddmmiinniissttrraattoorr,, aanndd NNaammeedd FFiidduucciiaarryy.. AAss ssuucchh,, tthhee PPllaann SSppoonnssoorr rreettaaiinnss ffuullll ddiissccrreettiioonnaarryy ccoonnttrrooll aanndd
aauutthhoorriittyy aanndd ddiissccrreettiioonnaarryy rreessppoonnssiibbiilliittyy iinn tthhee
ooppeerraattiioonn aanndd aaddmmiinniissttrraattiioonn ooff tthhee PPllaann..
44..99 PPaayy aannyy ttaaxxeess,, aasssseessssmmeennttss ffoorr ffeeeess aarriissiinngg ssoolleellyy
oouutt ooff tthhee ooppeerraattiioonnss ooff tthhee PPllaann oorr tthhee sseerrvviicceess
pprroovviiddeedd uunnddeerr tthhiiss AAggrreeeemmeenntt tthhaatt aarree lleevviieedd
aaggaaiinnsstt tthhee PPllaann oorr aaggaaiinnsstt tthhee TTPPAA bbyy aannyy
ggoovveerrnnmmeennttaall eennttiittyy wwhheetthheerr ffeeddeerraall,, ssttaattee oorr
llooccaall,, oorr aannyy ppoolliittiiccaall ssuubbddiivviissiioonnss oorr
iinnssttrruummeennttaalliittyy tthheerreeooff.. TTaaxxeess bbaasseedd oonn TTPPAA’’ss nneett
iinnccoommee oorr lliicceennsseess TTPPAA iiss rreeqquuiirreedd ttoo mmaaiinnttaaiinn ttoo
pprroovviiddee tthhee sseerrvviicceess uunnddeerr tthhiiss AAggrreeeemmeenntt sshhaallll
bbee tthhee ssoollee rreessppoonnssiibbiilliittyy ooff TTPPAA..
44..1100 TThhee PPllaann SSppoonnssoorr uunnddeerrssttaannddss aanndd aaggrreeeess tthhaatt
tthhee TTPPAA aanndd iittss aaffffiilliiaatteess aarree nnoott oobblliiggaatteedd ttoo
sshhaarree pprroopprriieettaarryy aanndd ccoonnffiiddeennttiiaall iinnffoorrmmaattiioonn..
NNeevveerrtthheelleessss,, iinn tthhee eevveenntt TTPPAA oorr iittss aaffffiilliiaatteess
aaggrreeee ttoo pprroovviiddee pprroopprriieettaarryy aanndd ccoonnffiiddeennttiiaall iinnffoorrmmaattiioonn,, tthhee PPllaann SSppoonnssoorr uunnddeerrssttaannddss aanndd
aacckknnoowwlleeddggeess tthhaatt tthhaatt TTPPAA oorr iittss aaffffiilliiaattee wwiillll
aasssseerrtt,, iinn aa bbrriieeff ttoo tthhee TTeexxaass AAttttoorrnneeyy GGeenneerraall,,
tthhaatt tthhee pprroopprriieettaarryy aann ccoonnffiiddeennttiiaall iinnffoorrmmaattiioonn
wwoouulldd bbee eexxeemmpptt ffrroomm ppuubblliicc ddiisscclloossuurree uunnddeerr
tthhee TTeexxaass PPuubblliicc IInnffoorrmmaattiioonn AAcctt ccooddiiffiieedd aatt
CChhaapptteerr 555522 ooff tthhee TTeexxaass GGoovveerrnnmmeenntt CCooddee,, aanndd
tthhaatt ssuucchh iinnffoorrmmaattiioonn sshhoouulldd nnoott bbee rreelleeaasseedd ttoo aa
rreeqquueessttoorr uunnddeerr tthhee TTeexxaass PPuubblliicc IInnffoorrmmaattiioonn AAcctt
wwiitthhoouutt tthhee pprriioorr wwrriitttteenn ccoonnsseenntt ooff tthhee TTPPAA oorr iittss
aaffffiilliiaattee.. TThhee PPllaann SSppoonnssoorr hheerreebbyy aaggrreeeess ttoo
nnoottiiffyy tthhee TTPPAA,, iinn wwrriittiinngg,, wwiitthhiinn tthhrreeee ((33))
bbuussiinneessss ddaayyss ooff PPllaann SSppoonnssoorr’’ss rreecceeiipptt ooff aannyy
ssuucchh ppuubblliicc iinnffoorrmmaattiioonn rreeqquueesstt ffoorr tthhee
pprroopprriieettaarryy aanndd ccoonnffiiddeennttiiaall iinnffoorrmmaattiioonn.. FFaaiilluurree
ttoo pprroovviiddee ssuucchh nnoottiiccee ttoo tthhee TTPPAA sshhaallll ccoonnssttiittuuttee
aa mmaatteerriiaall bbrreeaacchh ooff tthhiiss AAggrreeeemmeenntt
44..1111 PPaayy,, iinn aaccccoorrddaannccee wwiitthh tthhee FFeeee SScchheedduullee,,
AAppppeennddiixx AA,, tthhee TTPPAA’’ss ffeeeess ffoorr sseerrvviicceess rreennddeerreedd uunnddeerr tthhiiss AAggrreeeemmeenntt.. TThhee TTPPAA iiss eexxpprreessssllyy
ddiirreecctteedd bbyy tthhee PPllaann SSppoonnssoorr ttoo ppaayy aannyy eexxcceessss
lloossss iinnssuurraannccee pprreemmiiuummss ((wwhheerree aapppplliiccaabbllee)),, ffeeee,,
ccoosstt oorr cchhaarrggee tthheenn dduuee ttoo tthhee TTPPAA pprriioorr ttoo
aapppplliiccaattiioonn ooff ffuunnddss ttoo ppaayymmeenntt ooff CCllaaiimmss oorr aannyy
ootthheerr ccoossttss aarriissiinngg oouutt ooff tthhee PPllaann oorr ssuubbjjeecctt
mmaatttteerr ooff tthhiiss AAggrreeeemmeenntt.. TThhee PPllaann SSppoonnssoorr
ssppeecciiffiiccaallllyy ddiirreeccttss tthhaatt aallll ffuunnddss pprroovviiddeedd ttoo TTPPAA
uunnddeerr tthhiiss AAggrreeeemmeenntt wwiillll bbee ddiissbbuurrsseedd iinn tthhee
ffoolllloowwiinngg oorrddeerr:: FFiirrsstt ttoo ppaayy eexxcceessss lloossss iinnssuurraannccee pprreemmiiuummss wwhheerree aapppplliiccaabbllee,, ccllaaiimmss
aaddmmiinniissttrraattiioonn ffeeeess,, ccoossttss aanndd rreellaatteedd eexxppeennsseess
iinnccuurrrreedd bbyy TTPPAA aanndd sseeccoonndd,, ttoo ppaayy bbeenneeffiitt
ccllaaiimmss aarriissiinngg uunnddeerr tthhee PPllaann..
44..1122 MMaaiinnttaaiinn aannyy ffiiddeelliittyy bboonndd oorr ootthheerr iinnssuurraannccee aass
mmaayy bbee rreeqquueesstteedd bbyy ssttaattee oorr ffeeddeerraall llaaww ffoorr tthhee
pprrootteeccttiioonn ooff tthhee PPllaann aanndd CCoovveerreedd PPeerrssoonnss..
44..1133 NNoottiiffyy tthhee TTPPAA iiff tthhee PPllaann SSppoonnssoorr cceeaasseess ttoo
mmaaiinnttaaiinn SSttoopp LLoossss oorr EExxcceessss LLoossss iinnssuurraannccee wwiitthh
aann aaddmmiitttteedd iinnssuurraannccee ccoommppaannyy iinn tthhee aammoouunntt
sseett ffoorrtthh iinn tthhee FFeeee SScchheedduullee,, AAppppeennddiixx AA..
44..1144 PPrroommppttllyy nnoottiiffyy tthhee TTPPAA ooff aannyy tteerrmmiinnaattiioonn
nnoottiiccee,, eexxppiirraattiioonn llaappssee,, oorr mmooddiiffiiccaattiioonn ooff SSttoopp
LLoossss oorr EExxcceessss LLoossss iinnssuurraannccee,, lliiffee iinnssuurraannccee,,
ddiissaabbiilliittyy iinnssuurraannccee,, ccoonnvveerrssiioonn iinnssuurraannccee oorr aannyy
ootthheerr iinnssuurraannccee ppuurrcchhaasseedd iinn ccoonnjjuunnccttiioonn wwiitthh
tthhee PPllaann..
44..1155 EEnnssuurree tthhaatt tthheerree iiss aaddeeqquuaattee rreelleeaassee aanndd
aauutthhoorriizzaattiioonn ffrroomm eeaacchh ppaarrttiicciippaanntt aanndd//oorr
bbeenneeffiicciiaarryy uunnddeerr tthhee PPllaann ppeerrmmiittttiinngg HHeeaalltthh CCaarree
PPrroovviiddeerrss ttoo sshhaarree wwiitthh TTPPAA aanndd TTPPAA ttoo sshhaarree wwiitthh
HHeeaalltthh CCaarree PPrroovviiddeerrss aanndd ootthheerr sseerrvviiccee pprroovviiddeerrss
ttoo tthhee PPllaann aannyy aanndd aallll iinnffoorrmmaattiioonn,, wwhheetthheerr
pprrootteecctteedd oorr iinnddiivviidduuaallllyy iiddeennttiiffiiaabbllee,, wwhhiicchh mmaayy
bbee nneecceessssaarryy ttoo ppeerrffoorrmm tthhee sseerrvviicceess aannttiicciippaatteedd
bbyy tthhiiss AAggrreeeemmeenntt aanndd aannyy AAppppeennddiicceess hheerreettoo..
TTPPAA mmaayy iinn iittss ssoollee ddiissccrreettiioonn,, rreeqquuiirree ppaarrttiicciippaannttss
aanndd//oorr bbeenneeffiicciiaarriieess ooff tthhee PPllaann ttoo eexxeeccuuttee
aaddddiittiioonnaall rreelleeaasseess aanndd aauutthhoorriizzaattiioonnss ffoorr tthhee uussee
aanndd ddiisscclloossuurree ooff ssuucchh iinnffoorrmmaattiioonn.. TTPPAA mmaayy
rreeffuussee ttoo rreelleeaassee pprrootteecctteedd oorr ootthheerr iinnddiivviidduuaallllyy
iiddeennttiiffiiaabbllee hheeaalltthh ccaarree iinnffoorrmmaattiioonn ttoo PPllaann

SSppoonnssoorr,, iittss aaggeennttss aanndd ddeessiiggnneeeess iiff ssuucchh
aauutthhoorriizzaattiioonnss aanndd//oorr rreelleeaasseess aarree nnoott pprroovviiddeedd..
44..1166 HHaavvee tthhee ssoollee rreessppoonnssiibbiilliittyy ffoorr rreeppoorrttiinngg aanndd ddiisscclloossuurree,, iinncclluuddiinngg bbuutt nnoott lliimmiitteedd ttoo ppllaann
ddooccuummeennttss,, ssuummmmaarryy ppllaann ddeessccrriippttiioonnss,,
ssuummmmaarriieess ooff mmaatteerriiaall mmooddiiffiiccaattiioonnss,, ppaarrttiicciippaanntt
ccoommmmuunniiccaattiioonnss,, pprree--rreettiirreemmeenntt ccoouunnsseelliinngg ttoo
ppaarrttiicciippaannttss,, bboonnddiinngg ffiilliinnggss oorr ootthheerr ccoommpplliiaannccee
rreeqquuiirreedd ooff,, bbyy oorr ffoorr tthhee PPllaann,, tthheeiirr ppaarrttiicciippaannttss
aanndd bbeenneeffiicciiaarriieess,, oorr tthhee PPllaann SSppoonnssoorr bbyy EERRIISSAA,,
tthhee IInntteerrnnaall RReevveennuuee CCooddee,, oorr aannyy ootthheerr rreellaatteedd
aanndd//oorr aapppplliiccaabbllee ffeeddeerraall,, ssttaattee oorr llooccaall llaawwss,,
rruulleess oorr rreegguullaattiioonnss..
44..1177 SShhaallll bbee ssoolleellyy rreessppoonnssiibbllee ffoorr ppaayyiinngg aallll ffeeeess,,
eexxppeennsseess,, oorr ccoossttss aattttrriibbuuttaabbllee ttoo aannyy lleeggaall aaccttiioonn
oorr pprroocceeeeddiinngg bbrroouugghhtt ttoo rreeccoovveerr aa ccllaaiimm ffoorr
bbeenneeffiittss uunnddeerr tthhee PPllaann.. TTPPAA sshhaallll,, hhoowweevveerr,,
mmaakkee aavvaaiillaabbllee ttoo tthhee PPllaann SSppoonnssoorr aanndd iittss
ccoouunnsseell,, ssuucchh eevviiddeennccee wwhhiicchh rreellaatteess ttoo oorr iiss
rreelleevvaanntt ttoo ssuucchh aaccttiioonn oorr pprroocceeeeddiinngg aass TTPPAA mmaayy
hhaavvee aass aa rreessuulltt ooff tthhee ppeerrffoorrmmaannccee ooff tthhee
sseerrvviicceess sseett ffoorrtthh iinn tthhiiss AAggrreeeemmeenntt.. TTPPAA sshhaallll
pprroommppttllyy nnoottiiffyy tthhee PPllaann SSppoonnssoorr iinn wwrriittiinngg ooff aannyy
lleeggaall aaccttiioonnss ooff wwhhiicchh iitt bbeeccoommeess aawwaarree tthhaatt
iinnvvoollvvee tthhee PPllaann oorr tthhee PPllaann SSppoonnssoorr.. TThhee TTPPAA wwiillll
bbee rreessppoonnssiibbllee ffoorr iittss oowwnn aattttoorrnneeyy’’ss ffeeeess aanndd
ccoossttss bbuutt,, oonnllyy ttoo tthhee eexxtteenntt tthhaatt tthhee TTPPAA iiss ffoouunndd
ttoo bbee lliiaabbllee ffoorr ssuucchh ffeeeess aanndd ccoossttss....
44..1188 PPrroovviiddee ttiimmeellyy,, aaccccuurraattee aanndd ccoommpplleettee
iinnffoorrmmaattiioonn rreeqquuiirreedd bbyy TTPPAA ttoo pprroovviiddee tthhee
sseerrvviicceess tthhaatt TTPPAA hhaass aaggrreeeedd ttoo ppeerrffoorrmm uunnddeerr tthhiiss AAggrreeeemmeenntt.. TTPPAA sshhaallll hhaavvee tthhee rriigghhtt ttoo rreellyy
oonn ssuucchh iinnffoorrmmaattiioonn.. SSuucchh iinnffoorrmmaattiioonn sshhaallll
iinncclluuddee bbuutt nnoott bbee lliimmiitteedd ttoo aallll nneecceessssaarryy
eelliiggiibbiilliittyy eennrroollllmmeenntt aanndd ppaarrttiicciippaanntt ddaattaa;; aanndd
ccooppiieess ooff aallll ggoovveerrnniinngg ddooccuummeennttss ooff tthhee PPllaann aanndd
aannyy aammeennddmmeennttss tthheerreettoo,, iinncclluuddiinngg aannyy wwrriitttteenn
ppoolliicciieess,, iinntteerrpprreettaattiioonnss,, rruulleess,, pprraaccttiicceess oorr
pprroocceedduurree ccoonncceerrnniinngg ssaammee.. SSuucchh iinnffoorrmmaattiioonn
sshhaallll bbee pprroovviiddeedd uuppoonn eexxeeccuuttiioonn ooff tthhiiss
AAggrreeeemmeenntt aanndd iimmmmeeddiiaatteellyy ffoolllloowwiinngg
mmooddiiffiiccaattiioonn oorr aammeennddmmeenntt.. TTPPAA sshhaallll hhaavvee tthhee
rriigghhtt ttoo aassssuummee tthhaatt aallll ssuucchh iinnffoorrmmaattiioonn iiss
aaccccuurraattee aanndd ccoommpplleettee aanndd TTPPAA sshhaallll bbee uunnddeerr nnoo
dduuttyy ttoo qquueessttiioonn ssuucchh iinnffoorrmmaattiioonn.. PPllaann SSppoonnssoorr
sshhaallll rreeiimmbbuurrssee TTPPAA aatt iittss ssttaannddaarrdd hhoouurrllyy rraatteess
ffoorr TTPPAA’’ss ccoossttss iinnccuurrrreedd ffoorr eeffffoorrttss eexxppeennddeedd ttoo
rreemmeeddyy ddaattaa oorr iinnffoorrmmaattiioonn iinnaaccccuurraacciieess aass wweerree
pprroovviiddee bbyy tthhee PPllaann SSppoonnssoorr..
AARRTTIICCLLEE VV:: DDUURRAATTIIOONN OOFF AAGGRREEEEMMEENNTT
55..11 TThhiiss AAggrreeeemmeenntt sshhaallll ccoommmmeennccee aanndd eenndd oonn tthhee
ddaatteess ffiirrsstt wwrriitttteenn aabboovvee,, uunnlleessss tteerrmmiinnaatteedd
eeaarrlliieerr iinn aaccccoorrddaannccee wwiitthh tthhiiss AArrttiiccllee.. TThhiiss
AAggrreeeemmeenntt sshhaallll aauuttoommaattiiccaallllyy rreenneeww ffoorr aa
mmaaxxiimmuumm ooff ttwwoo aaddddiittiioonnaall 1122 mmoonntthh ppeerriiooddss
((JJaannuuaarryy 11,, 22001155 tthhrroouugghh DDeecceemmbbeerr 3311,, 22001155 aanndd
JJaannuuaarryy 11,, 22001166 tthhrroouugghh DDeecceemmbbeerr 3311,, 22001166))
uuppoonn tthhee tteerrmmss aanndd ffoorr tthheessee ssttaatteedd iinn tthhee FFeeee
AAppppeennddiixx hheerreettoo,, uunnlleessss tteerrmmiinnaatteedd aass ootthheerrwwiissee ssttaatteedd iinn tthhiiss AArrttiiccllee..
55..22 AAtt aannyy ttiimmee dduurriinngg tthhee tteerrmm ooff tthhiiss AAggrreeeemmeenntt,,
eeiitthheerr tthhee PPllaann SSppoonnssoorr oorr tthhee TTPPAA mmaayy aammeenndd oorr
cchhaannggee tthhee pprroovviissiioonnss ooff tthhiiss AAggrreeeemmeenntt.. TThheessee
aammeennddmmeennttss oorr cchhaannggeess mmuusstt bbee aaggrreeeedd uuppoonn iinn
aaddvvaannccee iinn wwrriittiinngg bbyy bbootthh tthhee PPllaann SSppoonnssoorr aanndd
tthhee TTPPAA.. IIff aannyy ssuucchh aammeennddmmeenntt iinnccrreeaasseess tthhee
aannttiicciippaatteedd CCllaaiimmss eexxppeerriieennccee uunnddeerr tthhee PPllaann oorr
tthhee TTPPAA’’ss ccoosstt ooff aaddmmiinniisstteerriinngg tthhee PPllaann,, tthhee PPllaann
SSppoonnssoorr aaggrreeeess ttoo ppaayy aannyy iinnccrreeaassee iinn CCllaaiimmss
eexxppeennsseess,, aass wweellll aass iinnccrreeaasseess iinn aaddmmiinniissttrraattiivvee
ffeeeess oorr ootthheerr ccoossttss wwhhiicchh tthhee TTPPAA rreeaassoonnaabbllyy
eexxppeeccttss ttoo iinnccuurr aass aa rreessuulltt ooff ssuucchh mmooddiiffiiccaattiioonn..
AAnnyy aammeennddmmeenntt wwhhiicchh aaffffeeccttss oonnllyy tthhee FFeeee
SScchheedduullee,, AAppppeennddiixx AA,, mmaayy bbee mmaaddee,, iinn wwrriittiinngg,,
ssiiggnneedd bbyy aallll ppaarrttiieess,, aanndd wwiitthhoouutt ootthheerr ffoorrmmaall
aammeennddmmeenntt ooff tthhiiss AAggrreeeemmeenntt.. AAllll ffeeee qquuootteess
aacccceepptteedd bbyy tthhee PPllaann SSppoonnssoorr ffoorr rreenneewwaallss ooff tthhiiss AAggrreeeemmeenntt wwiillll bbee iinnccoorrppoorraatteedd iinnttoo tthhiiss
AAggrreeeemmeenntt aass aammeennddmmeennttss ttoo tthhee FFeeee SScchheedduullee,,
AAppppeennddiixx AA..
55..33 EEiitthheerr tthhee PPllaann SSppoonnssoorr oorr tthhee TTPPAA mmaayy tteerrmmiinnaattee
tthhiiss AAggrreeeemmeenntt aatt aannyy ttiimmee,, bbyy ggiivviinngg ssiixxttyy ((6600))
ddaayyss aaddvvaannccee wwrriitttteenn nnoottiiccee ttoo tthhee ootthheerr ppaarrttyy
uunnlleessss bbootthh ppaarrttiieess aaggrreeee ttoo wwaaiivvee ssuucchh aaddvvaannccee
nnoottiiccee.. AAtt tthhee ooppttiioonn ooff tthhee ppaarrttyy iinniittiiaattiinngg tthhee
tteerrmmiinnaattiioonn,, tthhee ootthheerr ppaarrttyy mmaayy bbee ppeerrmmiitttteedd aa
ccuurree ppeerriioodd ((ooff aa lleennggtthh ddeetteerrmmiinneedd bbyy tthhee ppaarrttyy
iinniittiiaattiinngg tthhee tteerrmmiinnaattiioonn)) ttoo ccuurree aannyy ddeeffaauulltt..
55..44 TThhee TTPPAA mmaayy,, aatt iittss ssoollee ooppttiioonn,, tteerrmmiinnaattee tthhiiss
AAggrreeeemmeenntt wwiitthh tthhiirrttyy ((3300)) ddaayyss wwrriitttteenn nnoottiiccee
uuppoonn tthhee ooccccuurrrreennccee ooff aannyy oonnee oorr mmoorree ooff tthhee

ffoolllloowwiinngg eevveennttss ppeerrttaaiinniinngg ttoo tthhee PPllaann SSppoonnssoorr::
((aa)) TThhee PPllaann SSppoonnssoorr ffaaiillss ttoo ffuunndd tthhee
CCllaaiimmss PPaayymmeenntt aaccccoouunntt;; ((bb)) TThhee PPllaann SSppoonnssoorr ffaaiillss ttoo ppaayy
aaddmmiinniissttrraattiioonn ffeeeess oorr ootthheerr ffeeeess ffoorr tthhee
TTPPAA’’ss sseerrvviicceess uuppoonn pprreesseennttaattiioonn ffoorr
ppaayymmeenntt aanndd iinn aaccccoorrddaannccee wwiitthh tthhee FFeeee
SScchheedduullee,, AAppppeennddiixx AA;;
((cc)) TThhee PPllaann SSppoonnssoorr ffaaiillss ttoo ccoommppllyy
wwiitthh aannyy ffeeddeerraall,, ssttaattee oorr ootthheerr
ggoovveerrnnmmeenntt ssttaattuuttee,, rruullee oorr rreegguullaattiioonn;;
((dd)) TThhee PPllaann SSppoonnssoorr,, tthhrroouugghh iittss
aaccttss,, pprraaccttiicceess,, oorr ooppeerraattiioonnss,, eexxppoosseess tthhee TTPPAA ttoo aannyy eexxiissttiinngg oorr ppootteennttiiaall
iinnvveessttiiggaattiioonn oorr lliittiiggaattiioonn..
((ee)) TThhee PPllaann SSppoonnssoorr ppeerrmmiittss iittss ssttoopp
lloossss oorr eexxcceessss lloossss iinnssuurraannccee ttoo llaappssee,,
wwhheetthheerr bbyy ffaaiilluurree ttoo ppaayy pprreemmiiuummss oorr
ootthheerrwwiissee;;
((ff)) TThhee PPllaann SSppoonnssoorr lloosseess iittss
lliicceennssuurree oorr cceerrttiiffiiccaattiioonn,, iiff rreeqquuiirreedd bbyy
llaaww,, ttoo ccoonnttiinnuuee tthhee PPllaann;;
((gg)) IInnssoollvveennccyy ooff tthhee PPllaann;;
((hh)) CCoouurrtt aappppooiinnttmmeenntt ooff aa
ppeerrmmaanneenntt rreecceeiivveerr ffoorr ssuubbssttaannttiiaallllyy aallll ooff
tthhee PPllaann SSppoonnssoorr’’ss aasssseettss;;
((ii)) AA ggeenneerraall aassssiiggnnmmeenntt ffoorr tthhee
bbeenneeffiitt ooff ccrreeddiittoorrss bbyy tthhee PPllaann SSppoonnssoorr;;
oorr
((jj)) TThhee ffiilliinngg ooff aa vvoolluunnttaarryy oorr
iinnvvoolluunnttaarryy ppeettiittiioonn ooff bbaannkkrruuppttccyy,, iiff ssuucchh
ppeettiittiioonn iiss nnoott ddiissmmiisssseedd wwiitthhiinn ffoorrttyy--ffiivvee
((4455)) ddaayyss ooff tthhee ddaattee ooff ffiilliinngg,, pprroovviiddeedd tthhaatt aann oorrddeerr ffoorr rreelliieeff ffrroomm aauuttoommaattiicc
ssttaayy hhaass bbeeeenn oobbttaaiinneedd,, oorr wwiitthh rreessppeecctt ttoo
aa CChhaapptteerr 1111 pprroocceeeeddiinngg,, tthhaatt tthhee
bbaannkkrruupptt oorr BBaannkkrruuppttccyy TTrruusstteeee ffaaiillss ttoo
rreeaaffffiirrmm tthhiiss AAggrreeeemmeenntt aanndd pprroovviiddee
aaddeeqquuaattee aassssuurraanncceess ppuurrssuuaanntt ttoo 1111 UUSSCC
336655..
DDuurriinngg tthhee tthhiirrttyy--ddaayy nnoottiiccee ppeerriioodd TTPPAA’’ss
oobblliiggaattiioonnss uunnddeerr tthhiiss AAggrreeeemmeenntt aanndd aannyy
ppeerrffoorrmmaannccee gguuaarraanntteeeess rreellaatteedd tthheerreettoo sshhaallll bbee
ssuussppeennddeedd..
55..55 TThhee PPllaann SSppoonnssoorr mmaayy,, aatt iittss ooppttiioonn,, tteerrmmiinnaattee
tthhiiss AAggrreeeemmeenntt wwiitthh tthhiirrttyy ((3300)) ddaayyss wwrriitttteenn
nnoottiiccee uuppoonn tthhee ooccccuurrrreennccee ooff aannyy oonnee oorr mmoorree ooff
tthhee ffoolllloowwiinngg eevveennttss ppeerrttaaiinniinngg ttoo tthhee TTPPAA::
((aa)) CCoouurrtt aappppooiinnttmmeenntt ooff aa
ppeerrmmaanneenntt rreecceeiivveerr ffoorr aallll oorr ssuubbssttaannttiiaallllyy aallll ooff tthhee TTPPAA’’ss aasssseettss;;
((bb)) AA ggeenneerraall aassssiiggnnmmeenntt ffoorr tthhee
bbeenneeffiitt ooff ccrreeddiittoorrss bbyy tthhee TTPPAA;;
((cc)) TThhee ffiilliinngg ooff aa vvoolluunnttaarryy oorr
iinnvvoolluunnttaarryy ppeettiittiioonn ooff bbaannkkrruuppttccyy,, iiff ssuucchh
ppeettiittiioonn iiss nnoott ddiissmmiisssseedd wwiitthhiinn ffoorrttyy--ffiivvee
((4455)) ddaayyss ooff tthhee ddaattee ooff ffiilliinngg,, pprroovviiddeedd
tthhaatt aann oorrddeerr ffoorr rreelliieeff ffrroomm aauuttoommaattiicc
ssttaayy hhaass bbeeeenn oobbttaaiinneedd,, oorr wwiitthh rreessppeecctt ttoo
aa CChhaapptteerr 1111 pprroocceeeeddiinngg,, tthhaatt tthhee bbaannkkrruupptt oorr BBaannkkrruuppttccyy TTrruusstteeee ffaaiillss ttoo
rreeaaffffiirrmm tthhiiss AAggrreeeemmeenntt aanndd pprroovviiddee
aaddeeqquuaattee aassssuurraanncceess ppuurrssuuaanntt ttoo 1111 UUSSCC
336655;;
((dd)) TThhee TTPPAA lloosseess iittss lliicceennssuurree oorr
cceerrttiiffiiccaattiioonn rreeqquuiirreedd bbyy llaaww ttoo ccoonnttiinnuuee
iittss bbuussiinneessss oorr ccoonnttiinnuuee aass tthhiirrdd ppaarrttyy
aaddmmiinniissttrraattoorr;; oorr
((ee)) TThhee TTPPAA ffaaiillss ttoo ccoommppllyy wwiitthh aannyy
ffeeddeerraall,, ssttaattee oorr ootthheerr ggoovveerrnnmmeennttaall
ssttaattuuttee,, rruullee oorr rreegguullaattiioonnss..
((ff)) TThhee TTPPAA,, tthhrroouugghh iittss aaccttss,,
pprraaccttiicceess,, oorr ooppeerraattiioonnss,, eexxppoosseess tthhee TTPPAA
ttoo aannyy eexxiissttiinngg oorr ppootteennttiiaall iinnvveessttiiggaattiioonn
oorr lliittiiggaattiioonn..
DDuurriinngg tthhee tthhiirrttyy--ddaayy nnoottiiccee ppeerriioodd TTPPAA’’ss
oobblliiggaattiioonnss uunnddeerr tthhiiss AAggrreeeemmeenntt aanndd aannyy
ppeerrffoorrmmaannccee gguuaarraanntteeeess rreellaatteedd tthheerreettoo sshhaallll bbee
ssuussppeennddeedd..
55..66 AAtt tthhee wwrriitttteenn rreeqquueesstt ooff tthhee PPllaann SSppoonnssoorr aanndd
ssuubbjjeecctt ttoo tthhee PPllaann SSppoonnssoorr’’ss ccoonnttiinnuuiinngg
oobblliiggaattiioonn ttoo ffuunndd tthhee CCllaaiimmss PPaayymmeenntt AAccccoouunntt,,
aanndd ttoo ttiimmeellyy ppaayy aannyy oouuttssttaannddiinngg aammoouunnttss dduuee
aanndd ppaayyaabbllee ttoo tthhee TTPPAA uunnddeerr tthhee tteerrmmss ooff tthhiiss
AAggrreeeemmeenntt,, tthhee TTPPAA mmaayy,, aatt iittss ssoollee ddiissccrreettiioonn,,
aaggrreeee ttoo pprroocceessss iinnccuurrrreedd bbuutt nnoott rreeppoorrtteedd CCllaaiimmss
aafftteerr tthhee tteerrmmiinnaattiioonn ooff tthhiiss AAggrreeeemmeenntt ((RRuunn--OOuutt
SSeerrvviicceess)).. TThhee wwrriitttteenn rreeqquueesstt ooff tthhee PPllaann
SSppoonnssoorr mmuusstt bbee rreecceeiivveedd ssiimmuullttaanneeoouussllyy wwiitthh
tthhee nnoottiiccee ooff tteerrmmiinnaattiioonn rreeqquuiirreedd bbyy ssuubbsseeccttiioonn
55..33 ooff tthhiiss AAggrreeeemmeenntt.. SSuucchh aaggrreeeemmeenntt ((RRuunn--OOuutt
SSeerrvviicceess AAggrreeeemmeenntt)),, iiff aannyy,, sshhaallll bbee iinn wwrriittiinngg
aanndd aa sseeppaarraattee ffeeee wwiillll bbee cchhaarrggeedd ffoorr tthhiiss sseerrvviiccee..
TTPPAA wwiillll nnoott rreeffuussee ttoo pprroovviiddee RRuunn--oouutt SSeerrvviicceess
eexxcceepptt iiff tthhee PPllaann SSppoonnssoorr hhaass mmaatteerriiaallllyy
bbrreeaacchheedd tthhiiss AAggrreeeemmeenntt,, tthhee PPllaann SSppoonnssoorr
tteerrmmiinnaatteess tthhiiss AAggrreeeemmeenntt wwiitthhoouutt pprrooppeerr nnoottiiccee,, oorr iiff tthhiiss AAggrreeeemmeenntt iiss tteerrmmiinnaatteedd aass aa rreessuulltt ooff
aannyy ooff tthhee eevveennttss sseett oouutt iinn ppaarraaggrraapphhss 55..44 oorr 55..55
ooff tthhiiss AAggrreeeemmeenntt.. AAddddiittiioonnaallllyy,, iiff tthhee PPllaann
SSppoonnssoorr tteerrmmiinnaatteess tthhiiss aaggrreeeemmeenntt eeaarrllyy,, tthheerree
sshhaallll bbee aaddddiittiioonnaall ffeeeess ffoorr rruunn oouutt sseerrvviicceess aass
ssttaatteedd iinn AAppppeennddiixx AA hheerreettoo..
55..77 IIff tthhiiss AAggrreeeemmeenntt tteerrmmiinnaatteess ffoorr aannyy rreeaassoonn aanndd
nnoo RRuunn--OOuutt SSeerrvviiccee AAggrreeeemmeenntt iiss rreeqquueesstteedd,, oorr iiff
tthhee TTPPAA ddeecclliinneess ttoo pprroovviiddee RRuunn--OOuutt SSeerrvviicceess,, tthhee TTPPAA sshhaallll hhaavvee nnoo oobblliiggaattiioonn ttoo::
((aa)) CCoommpplleettee tthhee pprroocceessssiinngg ooff aannyy
ccllaaiimm rreeqquueessttss tthhaatt wweerree ppeennddiinngg oorr
ootthheerrwwiissee nnoott CCoommpplleettee CCllaaiimmss oorr
ccoommpplleettee tthhee pprroocceessssiinngg ooff aannyy CCoommpplleettee
CCllaaiimmss iiff tthhee PPllaann SSppoonnssoorr hhaass ffaaiilleedd ttoo
pprroovviiddee ffuunnddss ffoorr tthhee ppaayymmeennttss ooff aannyy
bbeenneeffiittss dduuee;;
((bb)) AAcccceepptt oorr pprroocceessss rreeqquueessttss ffoorr
ccllaaiimm ppaayymmeennttss pprreesseenntteedd ttoo iitt aafftteerr
tteerrmmiinnaattiioonn ooff tthhiiss AAggrreeeemmeenntt
iirrrreessppeeccttiivvee ooff wwhheenn ssuucchh ccllaaiimm wwaass
iinnccuurrrreedd;;
((cc)) IIssssuuee ccllaaiimmss cchheecckkss aafftteerr tthhee
tteerrmmiinnaattiioonn ddaattee ooff tthhiiss AAggrreeeemmeenntt ffoorr
aannyy rreeqquueesstt ffoorr ccllaaiimmss ppaayymmeennttss rreellaattiivvee
ttoo ccoonnddiittiioonnss eexxiissttiinngg bbeeffoorree,, oonn oorr aafftteerr
ssuucchh aa ddaattee..
((dd)) PPrroovviiddee oonnggooiinngg ccuussttoommeerr sseerrvviiccee ttoo PPllaann PPaarrttiicciippaannttss oorr HHeeaalltthh CCaarree
PPrroovviiddeerrss;; oorr
((ee)) PPeerrffoorrmm aannyy ootthheerr ttaasskk oorr
rreeqquuiirreemmeenntt ooff tthhiiss AAggrreeeemmeenntt,, eexxcceepptt
ffoorr tthhoossee rreeqquuiirreemmeennttss tthhaatt ssppeecciiffiiccaallllyy
ssuurrvviivvee tteerrmmiinnaattiioonn ooff tthhiiss AAggrreeeemmeenntt..
55..88 IIff tthhee PPllaann SSppoonnssoorr tteerrmmiinnaatteess tthhiiss AAggrreeeemmeenntt oonn
oorr bbeeffoorree tthhee eexxpprreesssseedd eexxppiirraattiioonn ddaattee ooff tthhiiss
AAggrreeeemmeenntt,, bbuutt aafftteerr ssuucchh tteerrmmiinnaattiioonn ddaattee
bbeeccoommeess eennttiittlleedd ttoo aannyy rreeiimmbbuurrsseemmeenntt((ss))
ppuurrssuuaanntt ttoo tthhee pprroovviissiioonnss ooff tthhee PPllaann SSppoonnssoorr’’ss
SSttoopp LLoossss oorr EExxcceessss LLoossss iinnssuurraannccee ppoolliiccyy
aaggggrreeggaattee oorr ssppeecciiffiicc lloossss rreeiimmbbuurrsseemmeenntt
pprroovviissiioonnss,, aanndd nnoo sseeppaarraattee RRuunn--OOuutt SSeerrvviicceess
AAggrreeeemmeenntt iiss eexxeeccuutteedd,, tthhee PPllaann SSppoonnssoorr sshhaallll
ppaayy ttoo tthhee TTPPAA aann hhoouurrllyy ffeeee ooff OOnnee HHuunnddrreedd aanndd
nnoo//110000 DDoollllaarrss (($$110000..0000)) ppeerr hhoouurr ffoorr aallll sseerrvviicceess
rreennddeerreedd bbyy tthhee TTPPAA aafftteerr tteerrmmiinnaattiioonn ooff tthhiiss
AAggrreeeemmeenntt rreeggaarrddiinngg ssuucchh rreeiimmbbuurrsseemmeenntt((ss)) rreeqquueesstt mmaaddee ttoo oorr ccllaaiimmss ppaaiidd bbyy aa SSttoopp LLoossss oorr
EExxcceessss LLoossss iinnssuurraannccee ccoommppaannyy..
55..99 IInn tthhee eevveenntt tthhiiss AAggrreeeemmeenntt iiss tteerrmmiinnaatteedd ffoorr aannyy
rreeaassoonn aanndd PPllaann SSppoonnssoorr ccaannnnoott bbee llooccaatteedd
ffoolllloowwiinngg rreeaassoonnaabbllee eeffffoorrttss bbyy TTPPAA,, TTPPAA sshhaallll
cchhaarrggee aa $$5500..0000 ppeerr cchheecckk aaddmmiinniissttrraattiivvee cchhaarrggee
ffoorr iittss eeffffoorrttss ttoo rreettuurrnn aannyy ssttaallee ddaatteedd ffuunnddss
((ddeeffiinneedd aass aa cchheecckk wwiitthh aann oorriiggiinnaall iissssuuee ddaattee
ggrreeaatteerr tthhaann 118800 ddaayyss)) bbeelloonnggiinngg ttoo PPllaann SSppoonnssoorr oorr bbeelloonnggiinngg ttoo aa ppllaann ppaarrttiicciippaanntt wwhhoo,, lliikkeewwiissee,,
ccaannnnoott bbee llooccaatteedd.. TThhee aaddmmiinniissttrraattiivvee cchhaarrggee mmaayy
bbee ppaaiidd ffrroomm aannyy ffuunnddss ooff tthhee PPllaann SSppoonnssoorr hheelldd
bbyy TTPPAA,, oorr bbiilllleedd ddiirreeccttllyy ttoo tthhee PPllaann SSppoonnssoorr.. TThhiiss
pprroovviissiioonn sshhaallll ssuurrvviivvee tteerrmmiinnaattiioonn ooff tthhiiss
AAggrreeeemmeenntt..
55..1100 TThhee PPllaann SSppoonnssoorr ssppeecciiffiiccaallllyy aacckknnoowwlleeddggeess tthhaatt
tthhee TTPPAA iinnccuurrss oonnggooiinngg ccoossttss ffoorr ssttaaffffiinngg,, lloonngg
tteerrmm ppllaannnniinngg,, mmaaiinntteennaannccee ooff ccuussttoommeerr sseerrvviiccee
ssuuppppoorrtt aanndd ootthheerr ccoossttss ccoonnnneecctteedd wwiitthh pprroovviiddiinngg
sseerrvviicceess ttoo PPllaann SSppoonnssoorr’’ss PPllaann,, aanndd tthhaatt tthhee
nnoottiiccee ooff tteerrmmiinnaattiioonn aanndd tteerrmmiinnaattee ddaattee
pprroovviissiioonnss ooff tthhiiss AAggrreeeemmeenntt pprroovviiddee aaddeeqquuaattee
nnoottiiccee ttoo tthhee TTPPAA ssoo tthhaatt uunnnneecceessssaarryy ccoossttss aarree
nnoott iinnccuurrrreedd bbyy tthhee TTPPAA iiff tthhee PPllaann SSppoonnssoorr
tteerrmmiinnaatteess tthhiiss AAggrreeeemmeenntt.. IInn tthhaatt rreeggaarrdd,, iitt iiss
ssppeecciiffiiccaallllyy aaggrreeeedd bbyy tthhee PPllaann SSppoonnssoorr tthhaatt iinn tthhee
eevveenntt tthhaatt tthhee PPllaann SSppoonnssoorr eeiitthheerr ffaaiillss ttoo pprroovviiddee
tthhee aaddvvaannccee nnoottiiccee ffoorr tteerrmmiinnaattiioonn rreeqquuiirreedd bbyy tthhiiss AAggrreeeemmeenntt,, oorr tteerrmmiinnaatteess tthhiiss AAggrreeeemmeenntt
ootthheerr tthhaann oonn iittss eexxpprreessss eexxppiirraattiioonn ddaattee,, tthhee PPllaann
SSppoonnssoorr sshhaallll ppaayy ttoo tthhee TTPPAA aa ffeeee eeqquuaall ttoo ttwwoo
ttiimmeess tthhee aammoouunntt ooff PPllaann SSppoonnssoorr’’ss
aaddmmiinniissttrraattiivvee ffeeeess ppaayyaabbllee ttoo tthhee TTPPAA ffoorr tthhee
mmoonntthh iimmmmeeddiiaatteellyy pprriioorr ttoo tthhee ddaattee nnoottiiccee ooff
tteerrmmiinnaattiioonn iiss rreecceeiivveedd.. TThhee aammoouunntt ppaayyaabbllee
uunnddeerr tthhiiss pprroovviissiioonn sshhaallll bbee aass lliiqquuiiddaatteedd
ddaammaaggeess iinnccuurrrreedd bbyy tthhee TTPPAA ffoorr tthhee ccoossttss rreecciitteedd
iinn tthhiiss ssuubbsseeccttiioonn,, iinn lliieeuu ooff ssppeecciiffiicc ccaallccuullaattiioonn ooff
tthhee ssaammee,, aanndd nnoott aass aa ppeennaallttyy.. TThhee lliiqquuiiddaatteedd
ddaammaaggeess wwiillll bbee iinn aaddddiittiioonn ttoo aannyy ootthheerr ffeeeess
rreeqquuiirreedd uunnddeerr tthhiiss AAggrreeeemmeenntt oorr aannyy ssuubbsseeqquueenntt
RRuunn--OOuutt SSeerrvviicceess AAggrreeeemmeenntt bbeettwweeeenn tthhee ppaarrttiieess..
AARRTTIICCLLEE VVII:: MMIISSCCEELLLLAANNEEOOUUSS

66..11 TThhiiss AAggrreeeemmeenntt,, ttooggeetthheerr wwiitthh aallll aaddddeennddaa,,
eexxhhiibbiittss aanndd aappppeennddiicceess,, ssuuppeerrsseeddeess aannyy aanndd aallll
pprriioorr rreepprreesseennttaattiioonnss,, ccoonnddiittiioonnss,, wwaarrrraannttiieess,, uunnddeerrssttaannddiinnggss,, pprrooppoossaallss oorr ootthheerr aaggrreeeemmeennttss
bbeettwweeeenn tthhee PPllaann SSppoonnssoorr aanndd tthhee TTPPAA hheerreettoo,,
oorraall oorr wwrriitttteenn,, iinn rreellaattiioonn ttoo tthhee sseerrvviicceess aanndd
ssyysstteemmss ooff tthhee TTPPAA,, wwhhiicchh aarree rreennddeerreedd oorr aarree ttoo
bbee rreennddeerreedd iinn ccoonnnneeccttiioonn wwiitthh iittss aassssiissttaannccee ttoo
tthhee PPllaann SSppoonnssoorr iinn tthhee aaddmmiinniissttrraattiioonn ooff tthhee
PPllaann..
66..22 TThhiiss AAggrreeeemmeenntt,, ttooggeetthheerr wwiitthh tthhee aaffoorreessaaiidd
aaddddeennddaa,, eexxhhiibbiittss,, aanndd aappppeennddiicceess,, ccoonnssttiittuutteess tthhee eennttiirree AAddmmiinniissttrraattiivvee SSeerrvviicceess AAggrreeeemmeenntt ooff
wwhhaattssooeevveerr kkiinndd oorr nnaattuurree eexxiissttiinngg bbeettwweeeenn oorr
aammoonngg tthhee ppaarrttiieess..
66..33 TThhee ppaarrttiieess hheerreettoo,, hhaavviinngg rreeaadd aanndd uunnddeerrssttoooodd
tthhiiss eennttiirree AAggrreeeemmeenntt,, aacckknnoowwlleeddggee aanndd aaggrreeee
tthhaatt tthheerree aarree nnoo ootthheerr rreepprreesseennttaattiioonnss,,
ccoonnddiittiioonnss,, pprroommiisseess,, aaggrreeeemmeennttss,,
uunnddeerrssttaannddiinnggss oorr wwaarrrraannttiieess tthhaatt eexxiisstt oouuttssiiddee
tthhiiss AAggrreeeemmeenntt wwhhiicchh hhaavvee bbeeeenn mmaaddee bbyy eeiitthheerr
ooff tthhee ppaarrttiieess hheerreettoo,, wwhhiicchh hhaavvee iinndduucceedd eeiitthheerr
ppaarrttyy oorr hhaavvee lleedd ttoo tthhee eexxeeccuuttiioonn ooff tthhiiss
AAggrreeeemmeenntt bbyy eeiitthheerr ppaarrttyy.. AAnnyy ssttaatteemmeennttss,,
pprrooppoossaallss,, rreepprreesseennttaattiioonnss,, ccoonnddiittiioonnss,,
wwaarrrraannttiieess,, uunnddeerrssttaannddiinnggss oorr aaggrreeeemmeennttss wwhhiicchh
mmaayy hhaavvee bbeeeenn hheerreettooffoorree mmaaddee bbyy eeiitthheerr ooff tthhee
ppaarrttiieess hheerreettoo,, aanndd wwhhiicchh aarree nnoott eexxpprreessssllyy
ccoonnttaaiinneedd oorr iinnccoorrppoorraatteedd bbyy rreeffeerreennccee hheerreeiinn,,
aarree vvooiidd aanndd ooff nnoo eeffffeecctt..
66..44 EExxcceepptt aass pprroovviiddeedd iinn AArrttiiccllee VV,, nnoo cchhaannggeess iinn oorr
aaddddiittiioonnss ttoo tthhiiss AAggrreeeemmeenntt sshhaallll bbee rreeccooggnniizzeedd
uunnlleessss aanndd uunnttiill mmaaddee iinn wwrriittiinngg aanndd ssiiggnneedd bbyy aallll
ppaarrttiieess hheerreettoo..
66..55 IInn tthhee eevveenntt aannyy pprroovviissiioonn ooff tthhiiss AAggrreeeemmeenntt iiss
hheelldd ttoo bbee iinnvvaalliidd,, iilllleeggaall oorr uunneennffoorrcceeaabbllee ffoorr aannyy
rreeaassoonn aanndd iinn aannyy rreessppeecctt,, ssuucchh iinnvvaalliiddiittyy,,
iilllleeggaalliittyy oorr uunneennffoorrcceeaabbiilliittyy sshhaallll iinn nnoo eevveenntt
aaffffeecctt,, pprreejjuuddiiccee oorr ddiissttuurrbb tthhee vvaalliiddiittyy ooff tthhee
rreemmaaiinnddeerr ooff tthhiiss AAggrreeeemmeenntt,, wwhhiicchh sshhaallll rreemmaaiinn
iinn aaccccoorrddaannccee wwiitthh iittss tteerrmmss..
66..66 TThhee ppaarrttiieess hheerreettoo wwiillll eeaacchh nnoottiiffyy tthhee ootthheerr,,
wwiitthhiinn tteenn ((1100)) WWoorrkkiinngg DDaayyss ooff aannyy iinnqquuiirryy mmaaddee
bbyy aannyy CCoovveerreedd PPeerrssoonn oorr aauutthhoorriizzeedd
rreepprreesseennttaattiivvee ooff aannyy CCoovveerreedd PPeerrssoonn rreellaatteedd ttoo
PPllaann DDooccuummeennttss,, PPllaann RReeccoorrddss,, CCllaaiimmss,, CCllaaiimmss
AAppppeeaallss,, CCllaaiimmss DDiissppuutteess,, tthhrreeaatteenneedd lliittiiggaattiioonn,,
llaawwssuuiittss ppeerrttaaiinniinngg ttoo tthhee PPllaann oorr aannyy iinnqquuiirryy
mmaaddee bbyy ffeeddeerraall oorr ssttaattee aauutthhoorriittyy rreeggaarrddiinngg tthhee PPllaann..
66..77 IInn tthhee eevveenntt tthhaatt eeiitthheerr ppaarrttyy iiss uunnaabbllee ttoo ppeerrffoorrmm
aannyy ooff iittss oobblliiggaattiioonnss uunnddeerr tthhiiss AAggrreeeemmeenntt
bbeeccaauussee ooff nnaattuurraall ddiissaasstteerr,, ffiirree,, fflloooodd,, wwiinndd
ssttoorrmm,, ppoowweerr oouuttaaggee,, llaabboorr uunnrreesstt,, cciivviill
ddiissoobbeeddiieennccee,, aaccttss ooff wwaarr ((ddeeccllaarreedd oorr
uunnddeeccllaarreedd)),, oorr aaccttiioonnss oorr ddeeccrreeeess ooff
ggoovveerrnnmmeennttaall bbooddiieess oorr aannyy eevveenntt wwhhiicchh iiss
rreeffeerrrreedd ttoo aass aa ““FFoorrccee MMaajjeeuurree EEvveenntt””,, tthhee ppaarrttyy wwhhoo hhaass bbeeeenn ssoo aaffffeecctteedd sshhaallll iimmmmeeddiiaatteellyy nnoottiiffyy
tthhee ootthheerr ppaarrttyy aanndd sshhaallll ddoo eevveerryytthhiinngg ppoossssiibbllee
ttoo rreessuummee ppeerrffoorrmmaannccee..
UUppoonn rreecceeiipptt ooff ssuucchh nnoottiiccee,, aallll oobblliiggaattiioonnss uunnddeerr
tthhiiss AAggrreeeemmeenntt sshhaallll bbee iimmmmeeddiiaatteellyy ssuussppeennddeedd..
IIff tthhee ppeerriioodd ooff nnoonn--ppeerrffoorrmmaannccee eexxcceeeeddss
ffoouurrtteeeenn ((1144)) WWoorrkkiinngg DDaayyss ffrroomm tthhee rreecceeiipptt ooff
nnoottiiccee ooff tthhee FFoorrccee MMaajjeeuurree EEvveenntt,, tthhee ppaarrttyy
wwhhoossee aabbiilliittyy ttoo ppeerrffoorrmm hhaass nnoott bbeeeenn ssoo aaffffeecctteedd
mmaayy tteerrmmiinnaattee tthhiiss AAggrreeeemmeenntt bbyy ggiivviinngg tthhiirrttyy
((3300)) ccaalleennddaarr ddaayyss’’ wwrriitttteenn nnoottiiccee..
66..88 AAllll nnoottiicceess rreeqquuiirreedd ttoo bbee ggiivveenn ttoo eeiitthheerr ppaarrttyy bbyy
tthhiiss AAggrreeeemmeenntt sshhaallll,, uunnlleessss ootthheerrwwiissee ssppeecciiffiieedd
iinn wwrriittiinngg,, bbee ddeeeemmeedd ttoo hhaavvee bbeeeenn ggiivveenn tthhrreeee
((33)) ddaayyss aafftteerr ddeeppoossiitt iinn tthhee UU..SS.. MMaaiill,, ffiirrsstt ccllaassss
ppoossttaaggee pprreeppaaiidd,, cceerrttiiffiieedd mmaaiill,, rreettuurrnn rreecceeiipptt
rreeqquueesstteedd..
AAnnyy ooffffiicciiaall nnoottiiccee ttoo tthhee TTPPAA wwiillll bbee mmaaiilleedd ttoo tthhee
aatttteennttiioonn ooff:: PPrreessiiddeenntt aanndd GGeenneerraall MMaannaaggeerr,,
22880066 SSoouutthh GGaarrffiieelldd SStt..,, MMiissssoouullaa,, MMTT 5599880011..
AAnnyy ooffffiicciiaall nnoottiiccee ttoo tthhee PPllaann SSppoonnssoorr wwiillll bbee
mmaaiilleedd ttoo tthhee aatttteennttiioonn ooff::
66..99
EEmmppllooyyeeeess hhiirreedd bbyy tthhee TTPPAA aarree hhiirreedd oonn tthhee bbaassiiss
ooff mmeerriitt aanndd qquuaalliiffiiccaattiioonnss,, aanndd tthheerree iiss nnoo
ddiissccrriimmiinnaattiioonn oonn tthhee bbaassiiss ooff rraaccee,, ccoolloorr,, rreelliiggiioouuss
ccrreeeedd,, ppoolliittiiccaall iiddeeaass,, sseexx,, aaggee,, mmaarriittaall ssttaattuuss,,
pphhyyssiiccaall hhaannddiiccaapp,, nnaattiioonnaall oorriiggiinn oorr aanncceessttrryy bbyy
ppeerrssoonnss ppeerrffoorrmmiinngg tthhiiss AAggrreeeemmeenntt..
QQuuaalliiffiiccaattiioonnss mmeeaann ssuucchh aabbiilliittiieess aass aarree ggeennuuiinneellyy
rreellaatteedd ttoo ccoommppeetteenntt ppeerrffoorrmmaannccee ooff tthhee
ppaarrttiiccuullaarr ooccccuuppaattiioonnaall ttaasskk..
66..1100 TThhiiss AAggrreeeemmeenntt sshhaallll bbee iinntteerrpprreetteedd aanndd ccoonnssttrruueedd iinn aaccccoorrddaannccee wwiitthh tthhee llaawwss ooff tthhee
ssttaattee ooff TTeexxaass eexxcceepptt ttoo tthhee eexxtteenntt ssuuppeerrsseeddeedd bbyy
ffeeddeerraall llaaww.. AAnnyy lliittiiggaattiioonn rreellaatteedd ttoo tthhee
iinntteerrpprreettaattiioonn oorr ppeerrffoorrmmaannccee ooff tthhiiss aaggrreeeemmeenntt
sshhaallll bbee ccoonndduucctteedd iinn aa TTeexxaass ssttaattee oorr ffeeddeerraall
ccoouurrtt wwiitthh jjuurriissddiiccttiioonn,, iinn HHaarrrriiss CCoouunnttyy,, TTeexxaass..
66..1111 TThhee ppaarrttiieess aaggrreeee ttoo uussee aanndd ddiisscclloossee pprrootteecctteedd
hheeaalltthh iinnffoorrmmaattiioonn aabboouutt aa CCoovveerreedd PPeerrssoonn iinn
aaccccoorrddaannccee wwiitthh tthhee tteerrmmss ooff aa sseeppaarraatteellyy pprroovviiddeedd BBuussiinneessss AAssssoocciiaattee AAggrreeeemmeenntt..
66..1122 TThhee TTPPAA sshhaallll ccoommppllyy wwiitthh tthhee AAnnyywwhheerree
WWoorrkkeerrss’’ CCoommppeennssaattiioonn AAcctt wwhhiillee ppeerrffoorrmmiinngg iittss
oobblliiggaattiioonnss uunnddeerr tthhiiss AAggrreeeemmeenntt iinn aaccccoorrddaannccee
wwiitthh §§§§3399--7711--112200,, 3399--7711--440011 aanndd 3399--7711--440055,,
AAnnyywwhheerree CCooddee AAnnnnoottaatteedd.. PPrrooooff ooff ccoommpplliiaannccee
sshhaallll bbee iinn tthhee ffoorrmm ooff wwoorrkkeerrss’’ ccoommppeennssaattiioonn
iinnssuurraannccee,, aann iinnddeeppeennddeenntt ccoonnttrraaccttoorr’’ss
eexxeemmppttiioonn oorr ddooccuummeennttaattiioonn ooff ccoorrppoorraattee ooffffiicceerr
ssttaattuuss.. SSuucchh iinnssuurraannccee//eexxeemmppttiioonn sshhaallll bbee vvaalliidd
aanndd iinn ffoorrccee ffoorr tthhee dduurraattiioonn ooff tthhiiss AAggrreeeemmeenntt..
TThhee TTPPAA sshhaallll aallssoo ccoommppllyy wwiitthh tthhee wwoorrkkeerr’’ss
ccoommppeennssaattiioonn llaawwss oorr ootthheerr ssiimmiillaarr llaawwss ooff aannyy
ootthheerr ssttaattee tthhaatt mmaayy aappppllyy..
66..1133 TThhee TTPPAA mmaayy eenntteerr iinnttoo aarrrraannggeemmeennttss wwiitthh aa
HHeeaalltthh CCaarree PPrroovviiddeerr oorr ggrroouupp ooff HHeeaalltthh CCaarree
PPrroovviiddeerrss ttoo oobbttaaiinn ddiissccoouunnttss iinn cchhaarrggeess ffoorr
CCoovveerreedd SSeerrvviicceess.. TTPPAA mmaakkeess nnoo rreepprreesseennttaattiioonnss tthhaatt ssuucchh ddiissccoouunnttss wwiillll ccoonnttiinnuuee ffoorr aannyy ppeerriioodd ooff
ttiimmee oorr wwiillll aappppllyy iinn aannyy ppaarrttiiccuullaarr ffaaccttuuaall ccoonntteexxtt..
IInn nnoo eevveenntt wwiillll TTPPAA bbee rreessppoonnssiibbllee ffoorr tthhee lloossss ooff
aannyy ssuucchh ddiissccoouunnttss eexxcceepptt iinn tthhee ssoollee eevveenntt tthhaatt
ssuucchh lloossss iiss ddiirreeccttllyy ccaauussee bbyy ccoommmmiissssiioonnss oorr
oommiissssiioonnss ooff TTPPAA wwhhiicchh ccoonnssttiittuuttee ggrroossss
nneegglliiggeennccee..
66..1144 NNoo ffoorrbbeeaarraannccee oorr nneegglleecctt oonn tthhee ppaarrtt ooff eeiitthheerr
ppaarrttyy ttoo eennffoorrccee oorr iinnssiisstt uuppoonn aannyy ooff tthhee
pprroovviissiioonnss ooff tthhiiss AAggrreeeemmeenntt sshhaallll bbee ccoonnssttrruueedd aass
aa wwaaiivveerr,, aalltteerraattiioonn oorr mmooddiiffiiccaattiioonn ooff tthhee
AAggrreeeemmeenntt..
66..1155 SShhoouulldd TTPPAA’’ss ppeerrffoorrmmaannccee ooff iittss dduuttiieess uunnddeerr tthhiiss
AAggrreeeemmeenntt bbee mmaaddee mmaatteerriiaallllyy mmoorree bbuurrddeennssoommee
oorr eexxppeennssiivvee dduuee ttoo aann iinnccrreeaassee iinn UUSS PPoossttaall
SSeerrvviiccee rraatteess oorr dduuee ttoo aa cchhaannggee iinn ffeeddeerraall,, ssttaattee
oorr llooccaall llaawwss oorr iimmppoossiittiioonn ooff ffeeeess tthheerree uunnddeerr,,
aannyy ssuucchh aaddddiittiioonnaall ffeeeess sshhaallll bbee ppaaiidd bbyy PPllaann SSppoonnssoorr.. TThhee TTPPAA wwiillll nnoottiiffyy tthhee CCiittyy aanndd ggeett tthheeiirr
aapppprroovvaall bbeeffoorree aannyy iinnccrreeaassee iinn ffeeeess aassssoocciiaatteedd
wwiitthh tthhiiss sseeccttiioonn..
66..1166 TThhee TTPPAA aanndd tthhee PPllaann SSppoonnssoorr ssppeecciiffiiccaallllyy ssttaattee,,
aacckknnoowwlleeddggee aanndd aaggrreeee tthhaatt iitt iiss tthheeiirr iinntteenntt tthhaatt
nnoo ootthheerr ppaarrttiieess iinncclluuddiinngg,, bbuutt nnoott lliimmiitteedd ttoo,, aallll
ppeerrssoonnss eelliiggiibbllee ffoorr bbeenneeffiittss uunnddeerr tthhee PPllaann,, aallll
ccoovveerreedd eemmppllooyyeeeess,, aanndd tthheeiirr aassssiiggnneeeess sshhaallll bbee
tthhiirrdd ppaarrttyy bbeenneeffiicciiaarriieess ooff tthhiiss AAggrreeeemmeenntt.. TThhee ppaarrttiieess ffuurrtthheerr aaggrreeee tthhaatt nnootthhiinngg hheerreeiinn sshhaallll bbee
ddeeeemmeedd ttoo iimmppoossee oonn tthhee TTPPAA aannyy oobblliiggaattiioonn ttoo
aannyy ootthheerr ppaarrttyy iinncclluuddiinngg,, bbuutt nnoott lliimmiitteedd ttoo,, aallll
ppeerrssoonnss eelliiggiibbllee ffoorr bbeenneeffiittss uunnddeerr tthhee PPllaann,, aallll
ccoovveerreedd eemmppllooyyeeeess,, aanndd tthheeiirr aassssiiggnneeeess..
66..1177 TThhee PPllaann SSppoonnssoorr aacckknnoowwlleeddggeess tthhaatt tthhee TTPPAA sshhaallll
hhaavvee nnoo rreessppoonnssiibbiilliittyy oorr lliiaabbiilliittyy ffoorr aannyy ffiinneess oorr
ppeennaallttiieess aasssseesssseedd tthhee IInntteerrnnaall RReevveennuuee SSeerrvviiccee
aass aa rreessuulltt ooff tthhee iissssuuaannccee ooff aannnnuuaall 11009999 ffoorrmmss ttoo
mmeeddiiccaall sseerrvviiccee pprroovviiddeerrss ssoo lloonngg aass tthhee TTPPAA hhaass
iissssuueedd tthhee 11009999 ttoo tthhee ssaammee nnaammee,, aaddddrreessss aanndd
TTIINN aass bbiilllleedd bbyy tthhee mmeeddiiccaall sseerrvviicceess pprroovviiddeerr aatt
tthhee ppooiinntt ooff ccllaaiimm ssuubbmmiissssiioonn..

IINN WWIITTNNEESSSS WWHHEERREEOOFF,, tthhee ppaarrttiieess hhaavvee ccaauusseedd tthhiiss AAggrreeeemmeenntt ttoo bbee eexxeeccuutteedd oonn tthheeiirr bbeehhaallff bbyy tthheeiirr
dduullyy aauutthhoorriizzeedd rreepprreesseennttaattiivveess’’ ssiiggnnaattuurreess,, eeffffeeccttiivvee aass ooff tthhee ddaattee ffiirrsstt wwrriitttteenn aabboovvee..
CClliieenntt CCoommppaannyyTTPPAA,, IINNCC..
BByy:: ______________________________________________________________________ BByy:: NNaammeeTTiittllee
BByy:: ______________________________________________________________________ BByy:: ________________________________________________________________________
((SSiiggnnaattuurree)) ((SSiiggnnaattuurree))
DDaattee:: __________________________________________________________________ DDaattee::
____________________________________________________________________

Related Documents











