NICKEL (ine patients with moderate ~d adequate sensation ",:ere .~mity. The results of f:xof temonstrate that reasonable ke patients. fiou and Treatment of the Upper : 69-93, 1969¯ nsplan~ and Its Use in CerebrM u)r-Pronator Origin for Flexion 15." of Eighteen Cases. J. Bone and ent Status of Intraneural ’i::,.~.ol Thomas, 19,57. ure in the Forearm. J. Bone and Clin. North America, 48: ll~- net Surgetj-. Philadelphia, d. B. ec ~nstruction of the Amputated Finger Tip with a Triangular Volar Flap A NEW SURGICAL PROCEDURE* BY ERDOGAN ATASOY~ M.:D.~ EVANGELOS IOAKIMIDIS~ M.D.S, RIORTON L. KASDAN, R’I.D.~, JOSEPH E. KUTZ, ~I.D.~, AND HAROLD E. KLEINERT~ M.]).~ LOUISVILLE, KENTUCKY F~’om the Deparlment of Surgery, University of Lmdsville School of Medicine, Louisville .pWca~ion of the finger tip is a common iniury a~d good judgmentin surgical onseruetion is needed to preserve maximum function and to minimize loss of time work. The ideal procedure should maintaitt length and cover the defect wi~h , well padded skin with normal sensation. Previously described methods provide good padding and coverage but without normal sensation~-~! Even Kutler’s procedure, it is not uncommon to find diminished or absent sensation the smaller lateral triangles. OF BONE AND JOINT Transverse Oblique Dorsal Fro. I C Oblique Palmar:/ Three commonest types of finger-tip amputations. procedure we describe here, called the triangular volar flap, was developed ration whenthe distal phalam,~ is amputated and the bone is exposed. It be applied to most finger4ip amputations, except those in which ~he soft-fissile ~s extensive and the plane of amputation is inclined volarward~an oblique amputation (Fig. 1). Occasionally, the remaining part of the phalanx has i shortened a few millimeters in order to facilitate the procedure. Amputations the middle or proximal phalanx can be treated by this method in order to maximum length. The proc, edure provides good contour and padding Read at the Annual Meeting of the American Society for Surgery of the Hand~ Chicago, 17, 1970. Department of Surgery, Univm~ity of Louisville School of Medicine, Louisville, Kentucky :~ Former Fellow in Surgery of the Hand, University of Louisville School of Medicine. Reprint. requests should be directed to Dr. Atasoy, 1001DoctorsBuilding, Louisville, ¯ 40202. 5~-.~., .NO. 5. JULY I970 921

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
NICKEL
(ine patients with moderate~d adequate sensation ",:ere.~mity. The results of f:xoftemonstrate that reasonableke patients.
fiou and Treatment of the Upper: 69-93, 1969¯
nsplan~ and Its Use in CerebrM
u)r-Pronator Origin for Flexion15." of Eighteen Cases. J. Bone and
ent Status of Intraneural ’i::,.~.ol
Thomas, 19,57.ure in the Forearm. J. Bone and
Clin. North America, 48: ll~-
net Surgetj-. Philadelphia, d. B.
ec ~nstruction of the Amputated Finger Tip with a
Triangular Volar FlapA NEW SURGICAL PROCEDURE*
BY ERDOGAN ATASOY~ M.:D.~ EVANGELOS IOAKIMIDIS~ M.D.S,
RIORTON L. KASDAN, R’I.D.~, JOSEPH E. KUTZ, ~I.D.~, AND
HAROLD E. KLEINERT~ M.]).~ LOUISVILLE, KENTUCKY
F~’om the Deparlment of Surgery, University of Lmdsville School of Medicine, Louisville
.pWca~ion of the finger tip is a common iniury a~d good judgment in surgicalonseruetion is needed to preserve maximum function and to minimize loss of time
work. The ideal procedure should maintaitt length and cover the defect wi~h, well padded skin with normal sensation. Previously described methods
provide good padding and coverage but without normal sensation~-~! EvenKutler’s procedure, it is not uncommon to find diminished or absent sensation
the smaller lateral triangles.
OF BONE AND JOINT
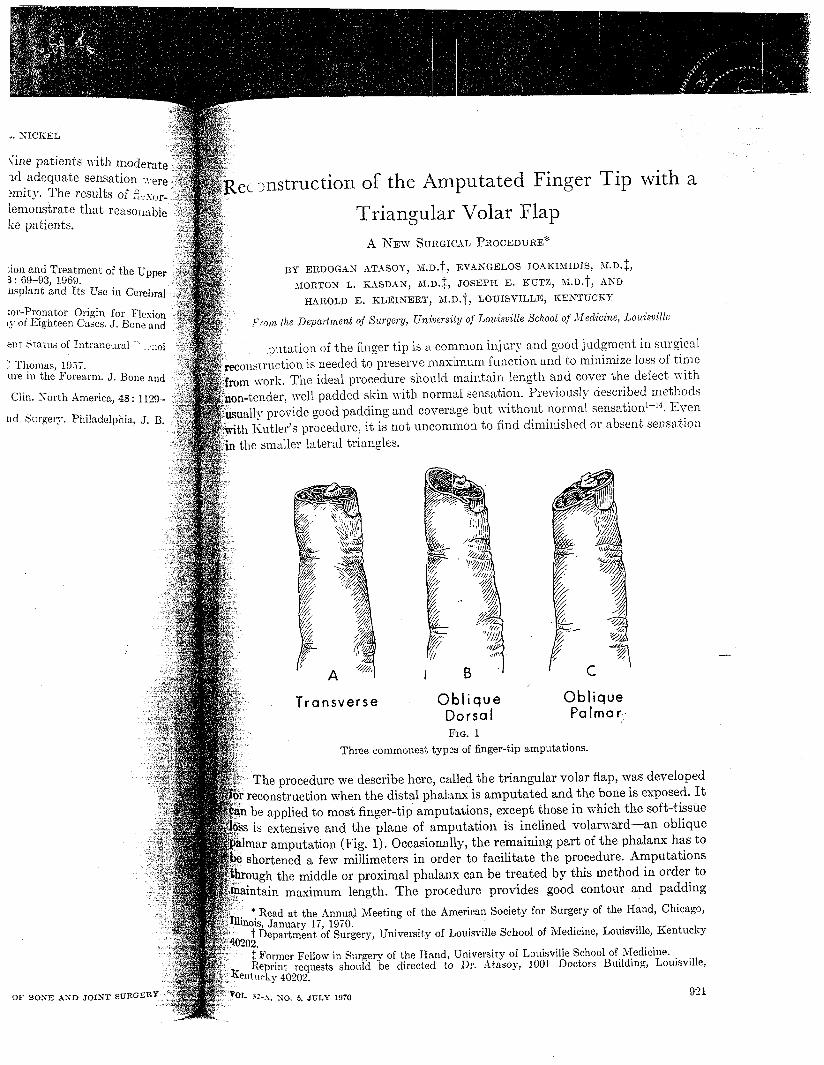
Transverse ObliqueDorsalFro. I
C
ObliquePalmar:/
Three commonest types of finger-tip amputations.
procedure we describe here, called the triangular volar flap, was developedration when the distal phalam,~ is amputated and the bone is exposed. It
be applied to most finger4ip amputations, except those in which ~he soft-fissile~s extensive and the plane of amputation is inclined volarward~an oblique
amputation (Fig. 1). Occasionally, the remaining part of the phalanx has i shortened a few millimeters in order to facilitate the procedure. Amputations
the middle or proximal phalanx can be treated by this method in order tomaximum length. The proc, edure provides good contour and padding
Read at the Annual Meeting of the American Society for Surgery of the Hand~ Chicago,17, 1970.
Department of Surgery, Univm~ity of Louisville School of Medicine, Louisville, Kentucky
:~ Former Fellow in Surgery of the Hand, University of Louisville School of Medicine.Reprint. requests should be directed to Dr. Atasoy, 1001 Doctors Building, Louisville,
4̄0202.
5~-.~., .NO. 5. JULY I970 921
922
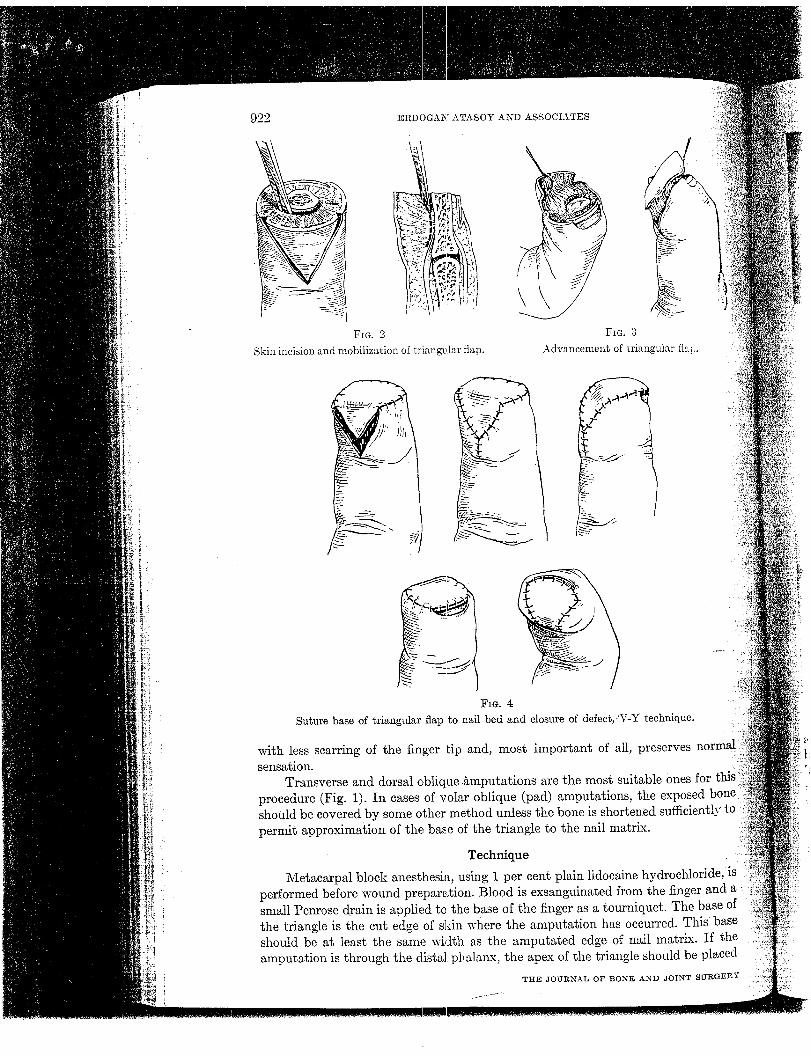
Fro. 2Skin incision and mobilization of triangular flap.
ERDOGAN ATASO¥ AND A$SOCL~TES
F~. 3Advancement of triangular
FIG.Suture base of triangular flap to nail bed and closure of defect,)V-Y technique.
with less scarring of the finger tip and, most important of all, preservessensation.
Transverse and dorsal oblique .~mputations are the most suitable ones for thig’procedure (Fig. 1). In eases of volar oblique (pad) amputations, the exposedshould be covered by some other method unless the bone is shortened sufficiently topermit approximation of the base of the triangle to the nail matrix.
Technique
Metacarpal block anesthesia, using 1 per cent plain lidocaine hydrochloride, ~sperformed before wound preparation. Blood is exsanguinated from the finger and asmall Penrose drain is applied to the base of the finger as a tourniquet. The base o~the triangle is the cut edge of skin wipers the amputation has occurred. This baseshould be at least the same width as the amputated edge of nail matrix. If theamputation is through the distal phalamx, the apex of the triangle should be placed
TIlE JOUI~AL OF BONE AND JOINT SuRGEBY
~ of triangular flap.
V-Y technique.
:I1, preserves normal
~uitable ones forthe exposed
~tened sufficiently~trix.
:ne hydrochloride, is¯ om the finger and a.miquet. The base ofoccurred. This basenail matrix. If the
~le should be placed
[E AND JOINT SURGER~"
RECONSTRUCTION OF THE AMPUTATED FINGER TIP
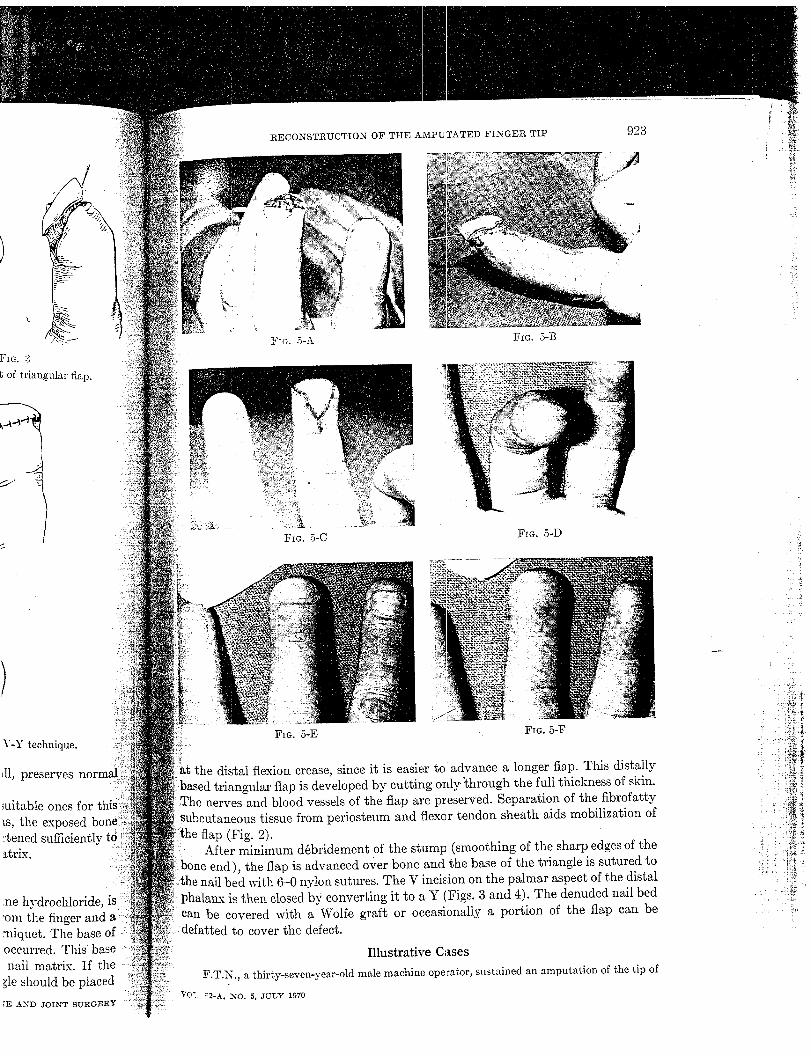
FIG. 5-A
923
FIG. 5-D
FIG. 5-E FIG. 5-F
the distal flexion crease, since it is easier to advance a longer flap. This distallyangular flap is developed by cutting only’through the full thickness of sldn.
nerves and blood vessels of the flap are preserved. Separation of the fibrofatty:subcutaneous tissue from periosteum and flexor tendon sheath aids mobilization of
flap (Fig. 2).: After minimum d~bridement of the stump (smoothing of the sharp edges of thei: bone end), the flap is advanced over bone and the base of the triangle is sutured to
bed with 6-0 nylon sutures. The V incision on the palmar aspect of the distalphalamx is then closed by converting it to a Y (.Figs. 3 and 4). The denuded nail bedcan be covered with a Wolfe graf~ or occasionally a portion of the flap can bedefatted to cover ~he defect.
Illustrative Cases
F.T.N., ~ thirty-seven-year-old male m~chine operator, sustained an ~mput~tion of the tip of
VOi 52-A, NO. 5, JULY 1970
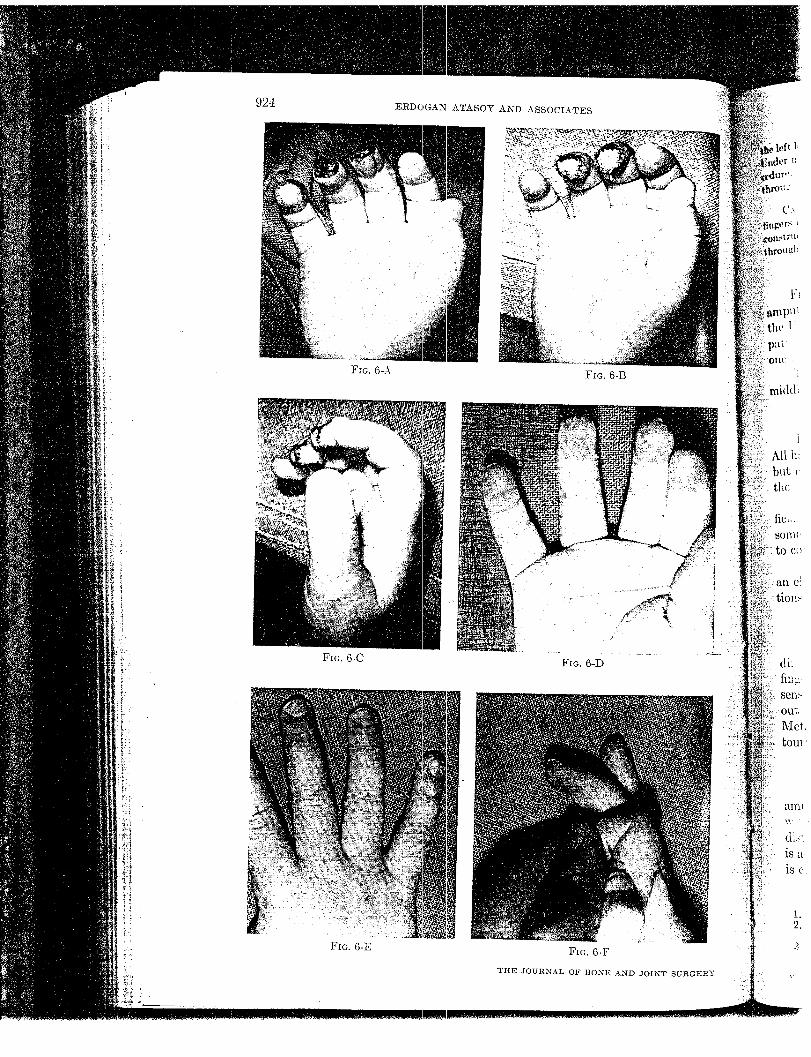
F~s. 6-A
ERDOGAN ATASO¥ AND ASSOCIATES
FIG. 6-B
FiG. 6-C
FIG. 6-E
FiG. 6-])
FIG. 6-F
TItE JOURNAL OF BONE AND JOIR’T
Fro. 6-B
925I~ECONSTRUCTION OF THE AMPUTATED FINGER TIP
left ~,~n~ finger by a shear machine on Augus~ 20,1968, and los~ one4hird of the dis~al phalanx.:: ~acarpM block anesthesia, the tip was reconstructed wi~h ~he triangular volar flap pro--...~sadon in the finger tip and the cosmetic resul~ a~ follow-up were excellen~ (Figs.~-F).
C,~s~ 2. D. K., ~ ~hree-ye~r-old girl, ~mput~ted the dist~I one-third of the righ~ long and ringin a door ~ home on August 5, 1969. Under :~xillary block anesthesia, the tips were re-
meted by using the triangular volar-flap procedure. The result was excellent (Figs. 6-A
Material
l:rom September 1967 to October 1969, sixty-one patients wi~h sixty-four finger.~:~. dons at different levels had their fingers reconstructed bj this procedure at
.erslt~ of Louisville l\Iedieal Center and affiliated hospitals. The VOUl~o~estwas fourteen months and the oldest eighty-five ?,ears old. There were forty-
male and seventeen female patients.The procedure was performed on the distal phalan-x fifty-four times, on the
phalamx five times, and on the proximal phalamx five times.
Results
Fifty-six of the sixty-one patients were ~vailable for evaluation at follow-up.had normal sensation except for two in whom finger sensation was initially lost’-<er gradually returned to nearly normal. All patients had normal motion and
;~.earanee of the finger was excellent./itere were no serious complications. Two patients had a small area of super-skin necrosis at the edge of the flap whidh later epithelized. Three patients hadsympathetic dystrophy with hypersensitivity of the finger tip. This responded
conservative treatment and within a few weeks the hyperesthesia had subsided.Not included in this study are eases in which the V-Y procedure was utilized as
elective method of reconstructing old unsalisfaetory painful finger-tip amputa-
In these eases, the end result was also excellent.
Advantages of the V-Y procedure
J_~. is simple to perform. Sear is minimurn and less painful since it is not locatedover the end of the finger. Cosraetieally, the result is excellent with good
contour and padding. Most important, the procedure preserves normal
of the finger tip. Only a simple finger dressing and guard is requi~ed with-immobilization as in other flaps and grafts, thereby lessening joint stiffness.
)al block anesthesia is adequate and a small Penrose drain suffices as
uet.
Summa:ry"
A triangular volar flap has been used successfully for the reconstruction ofrotated finger tips. It can be applied to most finger amputations except those
extensive soft-tissue loss on the volar side of the amputated finger tip. Thebased triangular flap, carefully prepared with intac~ nerve and blood supply,
over exposed bone and approximated to the nail matrix. The V incisionis closed by converting it to a Y.
ReferencesB.a~CL~Y, T. L.: The Late Results of Finger-Tip Iniuries. British J. Plash. Surg., 8 : 38-43, 1956.
2. B~ASlmY, R. W.: Reeonsl;rue~ion of Amputated Finger Tips. Plasg. and ReeonstrucL Surg.,44: 349-352, 1969. ̄
~. CaoN~x, T. D.: The Cross Finger Flap: A New Method of Repair. Am. Surgeon., 17: 419-425,~951.
V,’)L 52-A, NO. 5, JULY 1970
926 ERDOGAN ATASOY AND ASSOCIATES
4. DEJoNG~, EDWIN: A Sirnple Plastic Procedure of Fingers for Conserving Bony TissueForming a Soft Tissue Pad. Am. J. Surg., 57:346 347, 1942.
5. FISHER, R. H.: The Kutler ~Iethod of Repair of Finger-Tip Amputations. J. Bone and JoiSm’g., 49-A: 317-321, Mar. 19~37.
6. FLATT, A. E.: The Thenar Flap. J. Bone and Joint Surg., 39-B: 80-85, Feb. 1957.7. GURDtN, ~’[ICHAEL, and PANGY.(AN, ~.~. J.: The Repair of Surface Defects of Fingers by "2ran
digital Flaps. Plast. and Reconstruct. Surg., 5: 36~-371, 1950.S. HADDAD, R.. J., JR.: The Kutler Repair of Fingertip Amputation. Southern 5Ied. J., 61
t26i-1267, 1968.9. HOLMES, J. L.: Repair of Traumatic Finger Tip Amputations. U. S. Armed Forces Med. J.,
4 : 877-882, 1953.10. KEIM, H. A., and GRANTHAM, S. A.: Volar-Flap Advancement for Thumb and Finger Tip In-.
juries. Clin. Orthop., 66: 109-112, 1969.11. KLEINERT, H. E.: Finger Tip Injuries and Their Management, Am. Surgeon, 25 : 41-51,12. I~LEINERT, H. E. ; DESIMONE, I~ENNETH ; GASPAR, ~I. E. ; ARNOLD, R. E. ; a~lod KASDAN, "~I. L.:
Regional Anesthesia for Upper Extremity Surgerv. J. Trauma, 3 : 3-12, 196o. ¯13. I(CTLER, WILLIAM: A New ~Iethod for Finger Tip’Amputation J Am Zied Assn, 133" o9-30,
14. Sxow, J. %V.: The Use of a Volar Flap for Repair of Fingertip Amputations: A PreliminaryI{eport. Plast. and Reconstruct. Surg., 40: 163-168, 1967. "
DISCUSSIONDR. WILLI.aM NIETC.aLF, BRONX:, NEW YO~K: Dr. Atasoy and his associates have demonstrated
another useful application to hand surgery of the well known and well tried V-Y principle insurgery. It is an imaginative adaptation of Dr. :Kutler’s bilateral triangular-flap repair, having thesame basic principle and application which he described in the Journal of the American NIedicalAssociation in 1947 and discussed at one of our meetings iust a few years ago.
They have treated a sizeable series of cases, and they have presented the series briefly, succinct-ly, and with clear diagrams and photographs. The local complication rate has been at a minimumand the follow-up results are eminently satisfactory. The advantages claimed by the attthors are ¯weil substantiated by their results, have been clearly stated, and do not need repetition. A maioradvantage not stated by the authors is that the method obviates the need for split-graft coverageof residual skin defects required by other methods of repair. One disadvantage, freely admitted bythe authors, is the inapplicability of ~he method to volar oblique loss of tissue, and, I might add, tolateral or medial oblique losses.
I would like to indicate methods of using local tissue to repair such defects. For volar obliqueloss incisions in each paronychial sulcus allow the two resulting flaps to be interdigitated cove~ing :the bone end and reconstituting the finger tip; the small proximal residual skin defect, about onecentimeter in diameter, is covered with a split graft. For the dorsal oblique tissue loss, shorteningof the bone by only three to five mil].l~neters allows direct approximation to the nail base and thismethod may be as effective as the one presented by the authors. For the lateral oblique tissueincluding part of the nail, the V--Y procedure again is not applicable. Here an incision in the sulcusopposite the iniury allows development of a flap to cover the bone (after trimming the littlexpikc)and a small graft completes the repair.
In a crushing injury, resulting in the loss of the nail, the pulp, nail base, and the bone tuft, "careful d~bridement resulted in two flaps which were interdigitated and supported the remainingn̄ail base. A split graft covered the small residual defect. The result about ten weeks later wasregrown nail and nicely contoured finger tip.
T~’E JOUP~NAL OF BONE AND JOINT SURGERY

Do not mark this box!Document: 11000260

No. 1Giant cell lesion of boneHAND
cases may belassification
:s observedng factor.12
a the cellular
me hesitation,:ion. At a, the above,preciated andfor connectivestrating the
tomenclature~ phalangeal:oma were ::sed3o broad a term~¢e prefer the3up ofisorders
,,rved normai
:ation of the~tures atypical:al picturefence of aaluation.history and therill be
s not"atypical giant~the criteria of
o is best~URG 2:25 I-2,;J: Giant-cell~URO 5:39-50,neppen O:iegreendings. Ugeskr
ranuloma,~us) dysplasia:3os temporalLaryngol 83:95
ative:ia and reviewbed in the
’4Giant cell
of ethmoid concurrent with carcinoma ofsinuses. Ear Nose Throat J 55:38-41, 1976
SA. Eisenstein R, Wallner LJ: Giant cell le-invo!ving the nasal accessory sinuses. Laryngo-
7~ "~3-76. 1969RS, Schuknecht HF: Reparative granuloma fol-
btapedectomy. Ann Otol 76:1008-17, 1967t CC. Malik SRK, Gupta DK, Kahar PK: Reparative
~ma of the orbit. Am J Ophthamol 63:524-7, 1967
111.Abrams B, Shear M: A histological comparison of thegiant cells in the central giant cell granuloma of the jawsand the giant cell tumor of long bone. J Oral Pathol3:217-23, 1974
12. Davis GB, Tideman H: Multiple recurrent central giantcell granulomas of the jaws. J Max-Fac Surg 5:127-9,1977
13. Zook EG: Extensive giant cell tumor of the finger: A casehistory. J HAND SURG 2:267-8, 1977
,eatment of nail bed avulsions withsplit-thickness nail bed grafts
Experimental studies with squirrel monkeys indicated the feasibility of split-thickness grafting of
segments of the nail bed. Thin grafts, when takeu from the nail bed, achieved excellent take over
of the avulsed areas. Thirty-one patients with avulsion of segments of the nail bed were treatedwith split-thickness nail bed grafts. The injured nail bed had sufficient residual nail bed to serve
donor site in 24 patients. The remaining seven patients required split-thickness grafts fromthe lateral one third of the great toe. Of the 131 treated nail beds, there was a total of fivedeformities in which there was either nonadherence of the nail or irregularity of the nail surface.Twenty-six had nails with no deformity. No deformities occurred in the graft donor area. The
nail bed graft offers the advantage of frequent availability of tissue on the sameinjured digit and the absence of donor site deformity, whether on the same injured digit or adonor great toe. (J HAND SURG 8:49-54, 1983.)
H. Shepard, M.D., F.A.C.S., Newport, News, Va.
¯ " frequently result in avul-
of the nail bed. These injuries haveirregular, thickened nails and
to adhere to the injured surface,x-e Aof treatment of this injury have
When the avulsed segment was avail-replacement and suture, Schiller~
developing nails. Full-thickness nailsecond or third toe to the injured
reported by McCash,4 Berson, ~ andresults were obtained with the injured
digits were left with nail defor-skin grafting of the avulsed nail
advocated by Flatt, ~ Hanrahan,8 and
Laboratory for Microvascular Research,Newport News, Va.
Feb. 16, 1982.Dr. Glenn H. Shepard, 314 Main St., Newport
Stewart) Nonadherence of the growing nail to the skingraft is the common deformity. Kleinert et al. ~° advo-cated the use of dermal grafts and noted adherence_inall but the distal portion of the nail.
Personal clinical observations of nail bed avulsionsindicated deficiencies in available methods of treat-
ment. These deficiencies inspire d experimental evalua-tJ.on of operative procedures. As a result of these stud-ies, a technique of split-thickness nail bed grafting wasdeveloped. The purpose of this paper is to review lab-oratory experience and an 8-year clinical experience inthe management of nail bed avulsions.
Experimental study
The squirrel monkey (Saimiri) was used. The nailstructure resembles that of human nails grossly andmicroscopicaily. Complete nail regeneration in thisspecies occurs within 3 weeks, while it takes humannails 4 to 5 months. The initial phase of the experi-ments involved creation of a model in which a de-formed nail could be consistently reproduced by de-
+06500.60/0 © 1983 American Society for Surgery of the Hand THE JOURNAL OF HAND SURGERY 49
5O ShepardThe Journal
HAND SURGE
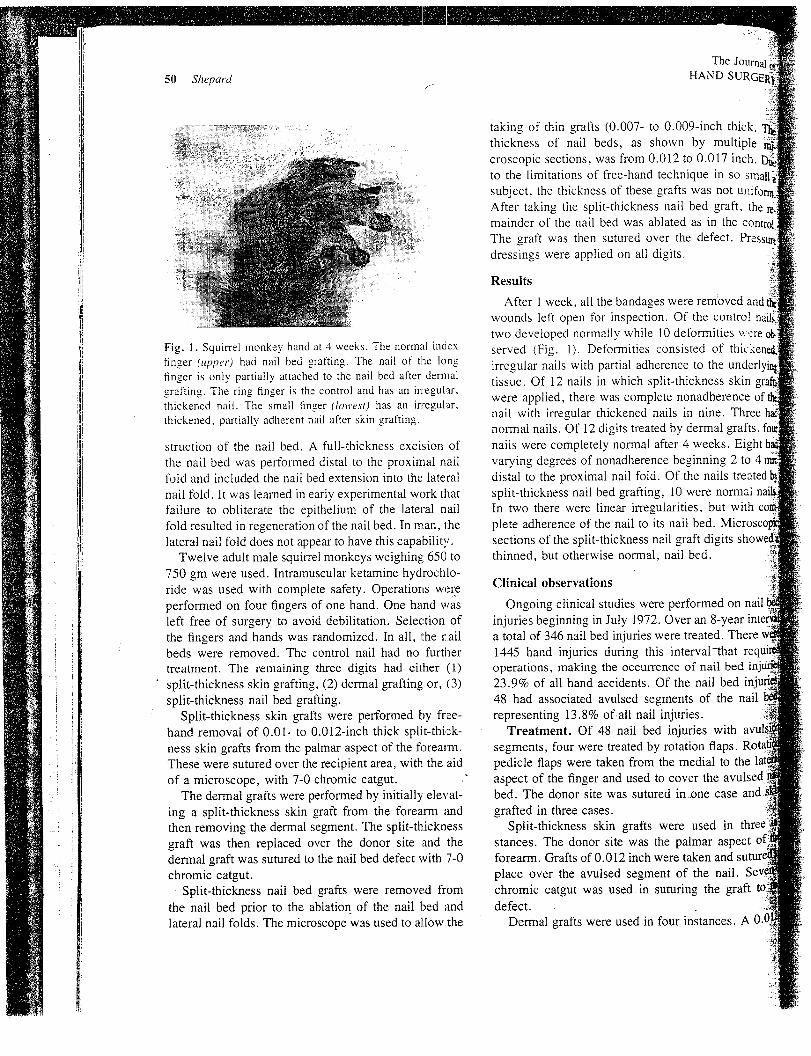
Fig. 1. Squirrel monkey’ hand at 4 weeks. The normal indexfinger (upper) had nail bed grafting. The nail of the longfinger is only partially attached to the nail bed after dermalgrafting. The ring finger is the control and has an in:egular,thickened nail. The small finger (lowest) has an irregular,thickened, partially adherent nail after skin grafting.
struction of the nail bed. A full-thickness excision ofthe nail bed was performed distal to the proximal nailfold and included the nail bed extension into the lateralnail fold. It was learned in early experimental work thatfailure to obliterate the epithelium of the lateral nailfold resulted in regeneration of the nail bed. In man, thelateral nail fold does not appear to have this capability.
Twelve adult male squirrel monkeys weighing 650 to750 gm were used. Intramuscular ketamine hydrochlo-ride was used with complete safety. Operations wereperformed on four fingers of one hand. One hand wasleft free of surgery to avoid debilitation. Selection ofthe fingers and hands was randomized. In all, the r~ailbeds were removed. The control nail had no furthertreatment. The remaining three digits had either (I)
" split-thickness skin grafting, (2) dermal grafting or, (3)split-thickness nail bed grafting.
¯ Split-thickness skin grafts were performed by free-hand removal of 0.01- to 0.012-inch thick split-thick-ness skin grafts from the palmar aspect of the forearm.These were sutured over the recipient area, with the aidof a microscope, with 7-0 chromic catgut. ."
The dermal grafts were performed by initially elevat-ing a split-thickness skin graft from the forearm andthen removing the dermal segment. The split-thicknessgraft was then replaced over the donor site and thedermal graft was sutured to the nail bed defect with 7-0chromic catgut.
Split-thickness nail bed grafts were removed fromthe nail bed prior to the ablation of the nail bed andlateral nail folds. The microscope was used to aIlow the
taking of thin grafts (0.007- to 0.009-inch thick.thickness of nail beds, as shown by multiplecroscopic sections, was from 0.012 to 0.017 inch.to the limitations of free-hand technique in so sinaisubject, the thickness of these grafts was not unifo~After taking the split-thickness nail bed graft, themainder of the nail bed was ablated as in theThe graft was then sutured over the defect. Pressu~dressings were applied on all digits.
Results
After 1 week, all the bandages were removed andwounds left open for inspection. Of the controltwo developed normally while I0 deformities wereserved (Fig. 1). Deformities consisted of thick~irregular nails with partial adherence to the underl,tissue. Of 12 nails in which split-thickness skinwere applied, there was complete nonadherence ofnail with irregular thickened nails in nine. Threenormal nails. Of 12 digits treated by dermal grafts,nails were completely normal after 4 weeks. Eightvarying degrees of nonadherence beginning 2 todistal to the proximal nail fold. Of the nailssplit-thickness nail bed grafting, 10 were normalIn two there were linear irregularities, but withplete adherence of the nail to its nail bed.sections of the split-thickness nail graft digitsthinned, but otherwise normal, nail bed.
Clinical observations
Ongoing clinical studies were performed on nailinjuries beginning in July 1972. Over an 8-yeara total of 346 nail bed injuries were treated.1445 hand injuries during this interval~hat recoperations, making the occurrence of nail bed in23.9% of all hand accidents. Of the nail bed in48 had associated avulsed segments of the nailrepresenting 13.8% of’all nail injuries.
Treatment. Of 48 nail bed injuries withsegments, four were treated by rotation flaps.pedicle flaps were taken from the medial to theaspect of the finger and used to cover the avulsedbed. The donor site was sutured in.one case andgrafted in three cases.
Split-thickness skin grafts were used instances. The donor site was the palmar aspectforearm. Grafts of 0.012 inch were takenplace over the avulsed segment of the nail.chromic catgut was used in suturing the graftdefect.
Dermal grafts were used in four instances. A

The JournalND SURGERy
NO. 1
1983Split-thickness grafts for nail bed avulsions 51
~ch thick. Themultiple
.017 inch. Due!: in so small a.s not uniform.t graft, the re.in the control.elect. Pressure
,.moved and the: control nails.nities were
of thickened.the underlying~ess skin graf~:lherence of theine. Three hadrnal grafts, four~eks. Eight hadring 2 to 4 mmnails treated b~’¯ e normal nails.but with corn-d. Microscopic:tigits showed~l.
ned¯ 8-year:ed.~1 that recail bed infil bedf the nail
’, with avulsii
Fig. 2. A, Diagrammatical representation of full-thickness nail bed avulsion. B, Technique ofremoving a split-thickness nail bed graft. Magnification is used. C, Split-thickness nail bed graftsutured over defect with 7-0 chromic catgut. D, The nail, when available, is replaced over the defect~:d a pressure dressing is applied. E, When the nail is not available, a single thickness of Betadine:auze (Purdue Frederick Co., Norwalk, Conn.) is placed over the defect with the proximal portionslipped under the proximal nail fold.
skin graft was elevated fromaspect of the forearm. The underlying der-
~,~,/~,gment was excised. A split-thickness skin graftsutured over the donor site w~th 6-0 nylon
~:and a pressure dressing was applied. The der-~ _~af.ts were then defatted and sutured ~n place over~.i ~bed with 7-0 chromic catgut. The removed
~I was sutured over the graft and a pressureg~was applied.i~tients a full-thickness nail bed graft from the©:was taken. The donor defect was treated by
afll ~,otati~ent of the lateral nail fold and primary closure~PoSlh~ late~~f~eu~The full-thickness grafts from the toe
he avulsed ~~ red in place over the avulsive segmentse case ana~ ~,~~~:~-~~ith 7-0 chromic catgut. The removed nail’ was
:~red over the defect and a pressure dressing was,~d in three ~~i.-,~fient
tr as-ect of ~jiP " s avulsed segments of the nail bed weren an~sutur~~~ split-thickness grafts of the nail bed. Sub-~vu,sed se~ment~ of the na~l:he graft ~a. ~ ted by this me~od (Fig. 2). In 24 cases
adjacent to the injured segment was large
tnces. A~ Novide sufficient graft to cover the d~fect. In
Fig. 3. Technique of removing split-thickness toe nail bedgrafts. One third of the nail is removed. A split thickness ofthe underlying nail bed is removed. The defect is coveredwitl~ a single thickness of Betadine gauze (Purdue Frederick),which is left in place until the advancing nail elevates it.

The Jo~HAND SU52 Shepard
Fig. 4. A. "Mix-Master" injury of index finger showing exposed bone and near total avulsion ofnail bed. Matrix was intact. This was treated by full-thickness toenail bed graft. B, Full-thicknesstoe nail bed graft sutured to avulsed fingernail bed. C, Normal nail after 6 months. D, Deformity ofdonor toe nail after 6 months.
Fig. 5. A, Lawn mower avulsion of great toenail bed. B, Taking of split-thickness nail bed graftlateral to avulsed defect. C: Split-thickness nail bed gr~tft sutured with. 7-0 chromic catgut. D, Resultat 1 year.

The Journal,HAND
t Split-thickness gratis for nail bed avldsions 53
ion of:knessfity of
A. Avulsion of nail bed segment by punch press. B,at 6 months.
¯ :: ’?:ickness great toe nail bed grafts were~:g. 3). The grafts were taken with a free-
technique with magnification. These were taken . ....thin and measured approximately 0.009 inch in
an attempt was made to make them of uni ............thickness. When observed through the micro-there were obvious variations in thickness of
~ graft despite careful excision technique¯split-thickness nail bed grafts were then used to
¯the avulsed segments. Seven-0 chromic catgutusc~! , suture the graft in place. After careful
,~ ~z graft slightly larger than the avulsive de-the nail, when available, was sutured in place over
and a pressure dressing was applied. Whennail was not available, Betadine gauze (Purdue
Co., Norwalk, Conn.) was inserted under thenail fold and used to cover the remainder of
bed.
of the nail were present in all of the fourpedicle flaps. Abnormal growth of the nail be-
pedicle flaps required reoperation in twofour dermal grafts, there was nonadher-
as judged by 6-month follow-up, in alltime, the nail had completely regrown to
finger, but was not adhering to the under-bed in the segment corresponding to the
In all cases in which split-thicknesswere used to cover the defect, there were
¯ and thickened nails and there was partial non-
to the nail bed in all cases.six patients with full-thickness toenail grafts,
nails were normal (Fig. 4). An obviouswas present in all toe donor areas (Fig. 4, D).
Fig. 7. A, Jointer-saw injury with defect of nail and nail bed.B, Result at 6 months.
FEXTENSOR TENDON ~MATRIX/ ~PROXIMAL /rNAIL BED
// NAIL FOLD
~/FPERIOSTEUM
""
/ /
-,, NAIL PLATE
Fig. 8. Anatomy of the nail mechanism, as demonstratedby Zais. ~’
Of 31 nail beds treated by split-thickness nail bedgrafts, there were a total of five deformities in which
there was either nonadherence of the nail or irregularityof the nail surface. Twenty-six (84%) had normal ap-
pearing nails with no obvious deformity (Figs. 5-7).
The Journ54 Shepard HAND SU
the six toenails that served as split-thickness nail beddonors, none had subsequent deformities. In the digitsthat had nail deformities after this technique, the de-formities appeared to be in the area of avulsion ratherthan the area of the nail bed donor site.
Discussion
Anatomical and physiological features of the :nailmechanism have been given a diversity of designationsand descriptions. The terminology of Zais~" 1., is usedin this paper (Fig. 8). The present study confirms thereports in the literature that success of nail bed re-placement is inconsistent when tissues other than thoseof the nail bed are used. The nail bed represents a
highly specialized tissue performing the very particularfunction of shaping and adhering to the advancing nailplate.l:~, i4 "Like tissue" appears to be the only satis-factory replacement for this complex tissue. Full-thick-ness toenail grafts serve quite nicely as replacement.The only disadvantage of this procedure is the defect ofthe donor area. Split-thickness nail bed grafts takenfrom the toenail have proven successful in areas whereinsufficient nail bed has been available on the injureddigit. Since no deformities of the donor toe have beenobserved, this procedure has merit. The advantage ofusing, where available, nail bed grafts from the inju!~eddigit is that there is no additional temporary disabilityto another part of the body and a second local anestheticis not required.
The role of the microscope in this study must beemphasized. If microscopic evaluation of the injureddigit indicates that the avulsion is of partial thickness,as in tangential lacerations by sharp objects, grafting isnot necessary because the regeneration of a functionalnail bed will occur without the aid of grafts. In ~:heexperimental animal there is a limitation as to ~:hethickness to which grafts can be taken; in man there canbe a considerable variation in thickness of grafts har-vested from a nail bed. The question "how thick can
split nail bed grafts be taken and still permit the
eration of the donor nail bed?" has not beenby these studies. Certainly when thin grafts are t&i:sufficient tissue to restore function to the lostment is provided without functional losses by the dor, inail bed.
REFERENCES
1. Buncke JH, Gonzalez RI: Fingernail reconstrucPlast Reconstr Surg 30:452-60, 1962
2. Tajima T: Treatment of open crushing type injuryhand and forearm: Degloving, open circumferential,press and nail bed injuries. J Trauma 14:995-1011,
3. Schiller C: Nail replacement in fingertip injuries.Reconstr Surg 19:521-30. 1957
4. McCash CR: Free nail grafting. Br J Plast Surg ~’,: 19-3.~ iI956
5. Berson MI: Reconstruction of the index fingertransplantation. Surgery 27:594-9, 1950
6. Swanker WA: Reconstructive surgery of the inAm J Surg 74:341-5, 1947
7. Flatt AE: Nail bed injuries. Br J Plast Surg 8:34-7,8. Hanrahan EM: The split thickness skin graft as a
ing following removal of a fingernail. Surgery400, 1946
9. Stewart JH: Surgical treatment of deformities of thelux by skin grafting. Br Med J 2:329-31, 1946
10. Kleinert HE, Putcha SM, Ashbell S, Kutz JE: The,formed fingernail, a frequent result of a failurenail bed injuries. J Trauma 7: 177-90, 1967
11. Zais N: The regeneration of the primatein the squirrel monkey, Saimiri. J Invest44:107-17, 1965
12. Zais N: The formation of the primate nail plate. An,itoradiographic study in squirrel monkey. Jmatol 51:120-36, 1968
13. Lewis BL: Microscopic studies of the fgfal andnail and surrounding soft tissue. Arch Dermatol70:732-47, 1954
14. Zais N: The movement of the nail bed. J Invest48:402-6, 1966
Related Documents











