EBS Microvascular Decompression for Hemi Facial Spasm After Excision of Acoustic Neuroma Macquarie Neurosurgery Evidence Based Surgery presentation Date: 25/2/16 By Dr Chris Davidoff

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

EBS
Microvascular Decompression for Hemi Facial Spasm After Excision of Acoustic Neuroma
Macquarie Neurosurgery
Evidence Based Surgery presentationDate: 25/2/16
By Dr Chris Davidoff

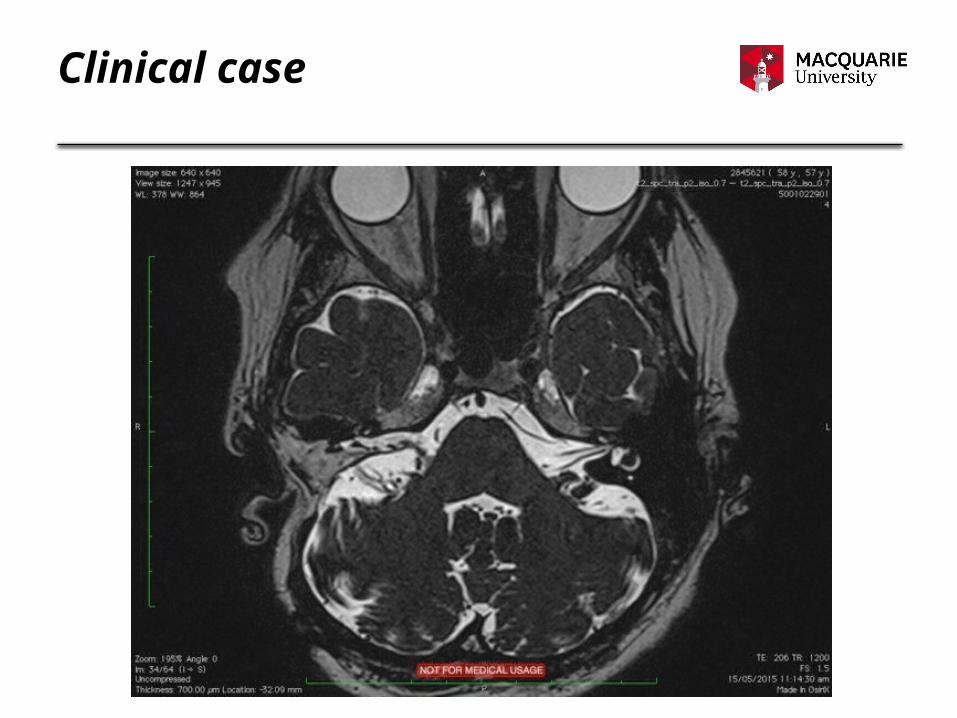
Clinical case
58yr old enrolled nurse presents with right sided facial spasms
• removal of right sided acoustic neuroma in 2005
• started having right sided facial spasms and tinnitus in 2012
• progress scans showed no recurrence of tumour
• reviewed by neurologist and multiple medical therapies trialled
• trialled botox therapy twice without relief
• ongoing severe spasm and tinnitus, starting to affect her ability to work
• desperate to undergo microvascular decompression
Clinical case

Searchable question (PICO format)
P – Patients who have hemifacial spasm after resection of a cerebellopontine angle lesion
I – microvascular decompression or surgical management
C – none
O – surgical success rate and/or complication rate
Question: “What is the role of surgery for hemi facial spasm after excision of a cerebellopontine angle lesion?”

Search strategy
• Medline• Embase• Scopus• Cochrane Library

Search results
Initial Medline search

Search results
Medline search

Search results
Embase search

Search results
Scopus search

Search results
Cochrane Search

Prisma Flow Diagram
Medline 18 articles Embase 48 articles Scopus 111 articles Cochrane 1 article
143 Abstracts reviewed
5 Articles retrieved
138 Excluded- 137 irrelevant- 1 inaccessible
0 Papers reviewed
5 excluded

Summary of papers
• retrieved as it was a case series of HFS caused by CP angle tumours• aimed to investigate the possibility that one of the cases had received an
operation prior to GK

Summary of papers
• single case report study• retrieved to see if there was a relevant cross over between HFS and
hemimasticatory spasm• reviewed to ascertain how the spasm was managed in the post-
operative period

Summary of papers
• case series of 9 patients with HFS as the result of CP angle tumours • retrieved to ascertain if any of the patients’ HFS did not resolve as the
result of surgery• 2 cases had HFS recur – 1 as a result of subtotal resction of AN, 1 due
to thickened arachnoid due to “inflammatory changes”• no comment made as to whether re-operation was attemped

Summary of papers
• retrospective cohort study of 652 patients undergoing surgical resection of AN
• 61 patients had HFS at 3 months post-op – this improved in 45 patients at 24 months and persisted in 16 patients
• 17 patients developed HFS between 3-24 months post-op• showed a 13% chance of developing HFS in the post-op period, with a
42% chance it would resolved in 24 months

Summary of papers
• single case study on HFS and AN being treated by a single GK exposure
• retrieved to investigate the possibility that HFS was treated after AN received GK therapy
• reported that the HFS was likely secondary to AN and that GK therapy resolved the HFS

Further Search
Further Search

Difficulties of search
• Difficult to construct a search delineating MVD for HFS after AN resection
• Re-operation search strategies focused on failure of MVD surgery, not for MVD after previous surgery
• Relative paucity of papers on HFS
• Broadening search to include CP angle tumours netted multiple papers focusing on gamma knife surgery
• Looking for individual case results resulted in having to read throughmany abstracts and papers

Conclusions
• 13% chance of developing HFS after surgical resection of AN
• 42% chance it will resolve in 24 months
• no reports of anyone operating for persisting HFS after previous surgery
Related Documents











