Published: December 28, 2012 DOI: 10.1371/journal.pone.0052986 Clinical Manifestations and Case Managemen Caused by a Newly Identified Virus Strain, Bun Paul Roddy Natasha Howard, Maria D. Van Kerkhove, Julius Lutwama, Joseph Wa Esther Sterk, Benjamin Jeffs, Michel Van Herp, Matthias Borchert Abstract A confirmed Ebola haemorrhagic fever (EHF) outbreak in Bundibugyo, Uganda, Novemb (Bundibugyo ebolavirus). It included 93 putative cases, 56 laboratory-confirmed cases, manifestations and case management for 26 hospitalised laboratory-confirmed EHF pa infections. The most frequently experienced symptoms were non-bloody diarrhoea (81 reported or were observed with haemorrhagic symptoms, six of whom died. Ebola care infection-control procedures required. However, quality data collection is essential to e improvement in future epidemics. Organizations usually involved in EHF case managem Figures Citation: Roddy P, Howard N, Van Kerkhove MD, Lutwama J, Wamala J, et al. (2012) Fever Caused by a Newly Identified Virus Strain, Bundibugyo, Uganda, 2007–2008. Editor: Malcolm Gracie Semple, University of Liverpool, United Kingdom Received: August 31, 2012; Accepted: November 23, 2012; Published: December 2 Copyright: © 2012 Roddy et al. This is an open-access article distributed under the unrestricted use, distribution, and reproduction in any medium, provided the origina Funding: MDVK acknowledges funding from the Medical Research Council UK and th design, data collection and analysis, decision to publish, or preparation of the manu Competing interests: The authors have declared that no competing interests exist. Introduction Filoviridae family members are characterised by filamentous enveloped particles with a genera, Ebolavirus and Marburgvirus, respectively causing Ebola and Marburg haemorr Affiliation: Department of Clinica Medicine Antwerp and Departm Medicine, University of Antwerp

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
-
Published: December 28, 2012 DOI: 10.1371/journal.pone.0052986
Clinical Manifestations and Case Management of Ebola HaemorrhagicCaused by a Newly Identified Virus Strain, Bundibugyo, Uganda, 2007Paul Roddy , Natasha Howard, Maria D. Van Kerkhove, Julius Lutwama, Joseph Wamala,Esther Sterk, Benjamin Jes, Michel Van Herp, Matthias Borchert
AbstractA conrmed Ebola haemorrhagic fever (EHF) outbreak in Bundibugyo, Uganda, November 2007February 20(Bundibugyo ebolavirus). It included 93 putative cases, 56 laboratory-conrmed cases, and 37 deaths (CFR =manifestations and case management for 26 hospitalised laboratory-conrmed EHF patients. Clinical ndinginfections. The most frequently experienced symptoms were non-bloody diarrhoea (81%), severe headache reported or were observed with haemorrhagic symptoms, six of whom died. Ebola care remains dicult due tinfection-control procedures required. However, quality data collection is essential to evaluate case denitionimprovement in future epidemics. Organizations usually involved in EHF case management have a particular
Figures
Citation: Roddy P, Howard N, Van Kerkhove MD, Lutwama J, Wamala J, et al. (2012) Clinical ManifestationFever Caused by a Newly Identied Virus Strain, Bundibugyo, Uganda, 20072008. PLoS ONE 7(12): e52
Editor: Malcolm Gracie Semple, University of Liverpool, United Kingdom
Received: August 31, 2012; Accepted: November 23, 2012; Published: December 28, 2012
Copyright: 2012 Roddy et al. This is an open-access article distributed under the terms of the Creativeunrestricted use, distribution, and reproduction in any medium, provided the original author and source a
Funding: MDVK acknowledges funding from the Medical Research Council UK and the Bill and Melinda Gadesign, data collection and analysis, decision to publish, or preparation of the manuscript.
Competing interests: The authors have declared that no competing interests exist.
IntroductionFiloviridae family members are characterised by lamentous enveloped particles with a negative-sense singlegenera, Ebolavirus and Marburgvirus, respectively causing Ebola and Marburg haemorrhagic fever (EHF, MHF
Aliation: Department of Clinical Sciences, Institute oMedicine Antwerp and Department of Epidemiology aMedicine, University of Antwerp, Antwerp, Belgium
-
haemorrhagic fever (FHF) outbreaks are characterised by secondary transmission and high case fatality (CFR) vary considerably: Zaire ebolavirus (ZEBOV; 8090%) [2], [4], [5], Sudan ebolavirus[6][8], Cte d'Ivoire ebolavirus (CIEBOV; 0%; based on a single patient) [9][11], Reston ebolavirus[12][16], and Lake Victoria marburgvirus (MARV; 2088%) [17][20]. To date, 35 FHF outbreaks are knownMHF), all in or originating from sub-Saharan Africa [2], [21][27].
Suspect and laboratory-conrmed patient categorisationIn sub-Saharan Africa, when a medical professional suspects a lovirus infection, the patient's blood sample(BSL-4) laboratory for diagnostic conrmation. If positive, an outbreak is declared and an international respocontact tracing, with isolation and treatment of suspect and laboratory-conrmed patients in a lovirus wardDue to delays between outbreak onset, recognition, and response, some individuals potentially infected with to follow-up before having their blood sampled for disease conrmation. Likewise, if clinical disease and outcfunctionality, not all patients are hospitalised and treated on a lovirus ward. Outbreaks therefore habitually conrmed patient categorisations, with only some patients receiving supportive treatment on a lovirus wardOnce case identication and contact tracing activities commence, individuals matching epidemiological and clovirus ward for clinical assessment and, when appropriate, categorised as a suspected FHF patient while aconrmation. Diagnostic results are typically available within four hours from an on-site laboratory, 48 hoursweek for samples sent abroad [33], [34]. Patients with negative test results are discharged and assessed forre-tested if FHF clinical suspicion remains. Laboratory-conrmed patients remain hospitalised on the loviru
Standard case managementIn the absence of specic antiloviral therapy, lovirus ward clinicians provide suspect and laboratory-conradministered during the 1995 EHF outbreak in Kikwit, Democratic Republic of the Congo and subsequent outrehydration, nutritional supplementation, and psychosocial support [26], [29][31]. Oral medication includeas nausea and vomiting (e.g. metoclopramide and promethazine), dyspepsia (e.g. aluminium hydroxide, cimeagitation, or confusion (e.g. diazepam, chlorpromazine), and pain (e.g. paracetamol, tramadol, and morphineoral artemether/lumefantrine for uncomplicated malaria and an oral antibiotic (e.g. amoxicillin, cotrimoxazoladministered due to the customary absence of an on-site laboratory capable of safely processing biological sexpanded, supportive care may also include prevention and treatment of dehydration via intravenous (IV) usupplementation, and IV administration of medication for optimum drug delivery when clinically indicated
Improving knowledge of human clinical manifestations and case managementLimited quality FHF clinical data from human outbreaks have been collected, analysed, and published, partly paper-based clinical records outside the lovirus ward [26]. Records have been destroyed as potential fomiteresult, most detailed descriptions of clinical manifestation have been from laboratory-based studies of non-hhuman patients (e.g. ZEBOV [28], [40][52], SEBOV [53][56], CIEBOV [9], and MARV Substantial uncertainties remain regarding human FHF incubation periods and symptom frequency, onset, andata are of questionable validity and reliability due to reporting and recall biases [41], symptom frequency and duration [9], [19], [40], [49], [53], [55], numerous others yielded only frequency daand period prevalence of symptoms (e.g. at admission to the lovirus ward, during hospital stay) fail to docuhuman FHF symptomatology is crucial for advancing outbreak control measures and administering supportivdisease severity [33].Although anecdotal evidence suggests supportive treatment increases FHF survival, its eectiveness has not[46]. More data on human clinical manifestations and treatment eectiveness are needed to improve respons
The 20072008 Bundibugyo outbreak
-
On 29 November 2007, the Uganda Ministry of Health (MoH) and the World Health Organization (WHO) conwestern Uganda, and responded in collaboration with Mdecins Sans Frontires (MSF), the Uganda Virus Resfor Disease Control and Prevention (CDC), and others [68]. On 20 February 2008, the outbreak concluded wi(30 of whom were hospitalised) and 37 deaths, yielding a 25% CFR [69], [70]. Most cases originated from B16,000 and 5,700 inhabitants respectively. Bundibugyo is situated at the base of the Rwenzori Mountains, anwas set up and maintained at each location throughout the outbreak response [70]. Genetic sequencing of vthe virus causing the Bundibugyo outbreak diered from any known ebolavirus (EBOV) species and was, althproposed as a new EBOV species provisionally named Bundibugyo ebolavirus (BEBOV)
Study rationale and objectivesThis outbreak is the rst known observation of human disease caused by this putatively novel EBOV species. BEBOV infection furthers knowledge of human FHF symptomatology, while describing the implemented FHF cshortcomings, a baseline imperative for improving and assessing the eectiveness of supportive case managthis may be the only way for future patients to receive better care. The objectives of this secondary analysis odemographics and contact histories; (ii) document symptoms from onset to clinical outcome; (iii) describe carecommend strategies for improving data collection in future FHF outbreaks.
MethodsEthics statementThe Uganda National Health Research Organization and the Ethics Review Boards of Mdecins Sans FrontireMedicine provided ethics approval for a posteriori analyses of the outbreak's anonymous and routinely collecadditional data were collected for research purposes and all data were anonymous before analysis, the ethicconsent.
Study population and data collectionStudy subjects were patients hospitalised on Bundibugyo or Kikyo Ebola wards with subsequent EHF laboratosuspected EHF cases in Bundibugyo District were: (i) an epidemiological link to an individual potentially infec(i.e. asthenia, anorexia, myalgia/arthralgia, diarrhoea, abdominal pain, nausea, vomiting, headache, dysphag(ii) fever plus at least three of the general symptoms listed above; or (iii) fever plus unexplained haemorrhagaccompanied to an Ebola ward and clinically assessed. Suspected cases further corroborated by clinical assedrawn and sent to the UVRI/CDC laboratory in Entebbe, Uganda for biological conrmation by polymerase chlinked immunosorbent assay (ELISA), or IgM-capture ELISA [69], [71]. Laboratory results were available thrThe makeshift Bundibugyo and Kikyo Ebola wards became fully functional following implementation of WHO a[3], [31]. Study subjects were hospitalised on (i) a makeshift ward for the entirety of their stay; (ii) a makeshstay; or (iii) a fully functional ward for the entirety of their stay. Dierences between fully functional and makmanagement as described in the introduction, and standardised data collection [48]. Data were recorded by MSF sta on fully functional wards (Figure 1).
-
Figure 1. Filovirus ward clinicians administering supportive treatment while concurrently recording clin200708 Ebola haemorrhagic fever outbreak.Photo by Claude Mahoudeau.doi:10.1371/journal.pone.0052986.g001
Study variables and data analysisData were collected on patient demographics, contact history, symptoms (self-reported from disease onset uhealthcare workers from admission until clinical outcome), treatment, patient monitoring, and clinical outcomDemographic variables were age, gender, residence, occupation, and Ebola ward. Contact history with an indcategorized as none, indirect (i.e. via fomite), direct, and direct during funeral practices Supportive treatment was categorised as EHF-related symptom alleviation, antibiotics, antimalarials, and dehpsychosocial support data were not collected. Patient monitoring data were axillary body temperature (i.e. feCelsius), heart rate (beats per minute), respiratory rate (breaths per minute), and blood pressure (mmHg). Cdischarge from the Ebola ward.Data were analysed using Microsoft Excel and Stata 11.0 (StataCorp Texas) to describe symptom frequencassociations between demographics, symptoms, or treatment and clinical outcome using exact logistic regreregression was used to determine probability of death by number of symptoms. Fisher's exact p-values of
-
Table 1. Self-reported demographics, days before seeking treatment at an Ebola ward, and contact histEbola haemorrhagic fever, Bundibugyo District, Uganda (November 2007February 2008).doi:10.1371/journal.pone.0052986.t001
Course of disease and clinical manifestationsEleven of the 26 patients died (CFR = 42%). The median duration of disease was 9 days (range 3 to 20) frompatients and 9.9 days (range 2 to 21) from self-reported onset to last recorded symptom prior to discharge fEbola ward after a mean self-reported delay of 3.5 days (range 0 to 8) following symptom onset. Available daincreased probability of death (e.g. dierences were not signicant for patients who died after being admittethree days (4/13; 31%) after symptoms reportedly commenced [Fisher's exact p-value 0.66; Table 2 presents all recorded patient symptoms. The left side shows frequency, usual day of onset, and mean15 patients. The most frequently reported general symptoms were fever, nausea/vomiting and non-bloody di(9/15; 60%), and conjunctivitis (5/15; 33%). Each self-reported symptom was experienced for a median of no individual self-reported symptom was associated with clinical outcome (Fisher's exact p-value range 0.23signicantly doubled the odds of death (OR 2.14; 95%CI: 1.028.18).
Table 2. Self-reported symptoms (15 patients), clinically observed symptoms (21 patients), and combihospitalised laboratory-conrmed EHF patients with known clinical outcome for whom data were recor2007February 2008).doi:10.1371/journal.pone.0052986.t002
The centre of Table 2 presents frequency, pattern (continuous versus intermittent), and mean duration in daypatients, from presentation to the Ebola ward until clinical outcome. Frequent symptoms included severe heamyalgia (16/21; 76%), dysphagia and appetite loss (15/21; 71% each), and non-bloody diarrhoea (14/21; 3.58 days (range 113). Less frequent clinically observed general symptoms (conjunctivitis, chest pain, cou
-
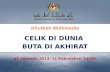
protracted duration (mean 47 days). Of ten patients whose body temperature was recorded at least once wfever for one day.The right of Table 2 and Figure 2 present symptom frequency from self-reported onset to clinical outcome (i.study-patients. The most frequently experienced symptoms were non-bloody diarrhoea (81%), severe headapresents their median duration.
Figure 2. Frequency of non-haemorrhagic symptoms from self-reported day of symptom onset to clinicpercentages, among symptomatic (9 deceased and 12 surviving) laboratory-conrmed Ebola haemorrUganda, November 2007February 2008.Note changes in denominator between self-reported and clinically observed sections.doi:10.1371/journal.pone.0052986.g002
Figure 3. Median duration in days of symptoms from self-reported onset until clinical outcome among 2haemorrhagic fever patients, Bundibugyo District, Uganda (November 2007February 2008).Blue and red bars indicate general and haemorrhagic symptoms, respectively. *Day 0 = presentation to thduration of the self-reported symptoms prior to presentation to the Ebola ward for patient observations >clinician-assessed symptoms at presentation to and during hospitalisation on the Ebola ward for patient o
-
patients only (n = 9).doi:10.1371/journal.pone.0052986.g003
No self-reported or clinically observed symptom or combination of symptoms, other than any haemorrhage (clinical outcome (Fisher's exact p-value range: 0.371.00). However, similarly to self-reported symptoms, foodds of death increased by approximately 31% (OR 1.31; 95%CI: 1.041.82).
Haemorrhagic symptomsSeven patients experienced self-reported and/or clinically observed haemorrhagic symptoms, six of whom dtimes greater odds of dying than those not experiencing any haemorrhagic symptom (86% versus 33%; OR Three patients self-reported haemorrhagic symptoms prior to admission while ve patients were clinically obhospitalisation. The one surviving patient self-reported and was clinically observed with epistaxis (and later died, one reported melaena, while the other reported haematemesis, epistaxis, and postpartum blehaemorrhagic symptoms clinically observed during hospitalisation. Of the three patients who self-reported award within 24 hours of self-reported bleeding onset, while one tolerated melaena for three days prior to preself-reported median of one day of fever prior to Ebola ward presentation.Clinically observed haemorrhagic symptoms (Table 2; Figure 4) included melaena and prolonged bleeding athaematemesis, bleeding gums, haemoptysis, haematuria, haematoma, and postpartum vaginal bleeding (1/2clinically observed with haemorrhagic symptoms, the rst was observed with bleeding gums; the second withthird with melaena, haematemesis, and prolonged bleeding from an injection site; and the fourth with melaenpostpartum bleeding. Petechiae were not observed.
Figure 4. Frequency of haemorrhagic symptoms from self-reported day of symptom onset to clinical ouamong symptomatic (9 deceased and 12 surviving) laboratory-conrmed Ebola haemorrhagic fever paNovember 2007February 2008.Note changes in denominator between self-reported and clinically observed sections.doi:10.1371/journal.pone.0052986.g004
Case managementOf the 19 laboratory-conrmed patients with treatment details recorded, 18 (95%) were administered paracreceived cimetidine for dyspepsia (Table 3). No other medication was administered to alleviate Ebola-relatedpatients (37%) for potential concomitant infections. Antimalarials were administered to 11 patients (58%), borderline signicant positive association between antimalarial administration and fatal outcome (OR 5.93, 9However, two of these patients received quinine, indicating more severe infection. When these two were remo
-
patients receiving presumptive artemether/lumefantrine, the dierence in clinical outcome was no longer sigwas administered to 16 patients (84%), while four patients (21%) received IV-uids. Vitamin supplementatiantimalarial treatment, there was no signicant dierence in clinical outcome for any treatment component (
Table 3. Treatment recorded for 19 hospitalised laboratory-conrmed Ebola haemorrhagic fever patiendoi:10.1371/journal.pone.0052986.t003
Of the ten patients whose axillary body temperature was recorded at least once during hospitalisation, ve (5daily for 80% of their stay, while seven (70%) had their temperature recorded at least once daily for 50% ofrate, and blood pressure were not recorded for any patients.
DiscussionThis study documents clinical manifestations of human BEBOV infection among hospitalised patients and desclinical manifestations from a putatively novel EBOV species furthers knowledge of human lovirus infection,for improvement and accentuates the need to assess eectiveness of supportive treatment in future outbrea
Case fatality ratioTo date, the 25% crude CFR of the 20072008 Bundibugyo outbreak is the lowest of recorded major humanlaboratory-conrmed patients the CFR increases to 42%, similar to that found by MacNeil and colleagues forand observed consistently in SEBOV [53][55], [72] and occasionally in ZEBOV [41], [73]among putative cases [8] or more accurate due to inclusion of less severe cases who did not attend hospitalspecies merits caution, as disease recognition often requires a functioning surveillance system and case-fataspecies, including route and dose of infection, genetic susceptibility, and underlying prevalence of immunode
Patient demographics and contact historiesSimilar to some previous lovirus outbreaks, this study population only comprised adults (2066 years) reported direct contact (11/14) or direct contact with a potentially infected corpse during funeral practices opportunities for disease transmission in previous lovirus outbreaks [33], [49], [75]contact history. This may be due to non-rigorous patient interviews during high-workload periods on the Ebowere missing (e.g. 54%, or 14/26 of study subjects did not have their occupation recorded), indicating shortunnoticed secondary transmission could have occurred. Available data preclude decisive conclusions.Regrettably, incubation periods were not measured for this study population. Albeit challenging to establish with a source case, it is possible to obtain quality contact history and incubation-period data Contact history data facilitate outbreak control eorts and further understanding of transmission patterns
-
understanding of disease course in humans [35], [80]. Without complete and accurate data, interpretation odicult. Authors are, for example, precluded from explaining why 73% of the study population were male.
Clinical manifestationsEbola-ward clinicians working on the fully functional ward employed a standardised prospective case reportiprioritised data transfer outside the ward [19], [81], [82]. Subsequent analyses (Tables 2human disease caused by this putatively novel EBOV species and further knowledge of FHF clinical manifestaobserved and reported from human ZEBOV [28], [40][52], SEBOV [53][55], CIEBOV clinical data. A more detailed comparison is not feasible due to substantial variations in FHF reporting methoAs lovirus ward clinicians often use personal discretion to decide whether an individual should proceed to acommunity [33], these documented BEBOV clinical manifestations could potentially assist future FHF clinicalsupposed lovirus disease hallmarks (fever plus haemorrhage) were observed relatively infrequently (3/26; 1prior to hospitalization reported fever plus haemorrhage, no individual whose axillary temperature was recorand one or more haemorrhagic symptom was observed in only ve hospitalised patients. The most frequent population (i.e. severe headache, asthenia, myalgia) are subjective and could equally indicate typhoid, shigelsettings, authors recommend continued rigorous study of human FHF clinical manifestations to increase the crucial aspect of outbreak control [28][33]. Further improvements to diagnostic accuracy beyond that achirequire the consistent and timely dispatch of eld laboratories to lovirus outbreak settings and an eventual test).Comprehensive documentation and understanding of FHF clinical manifestations is needed, as the administrapresentation, anticipated symptomatology, and disease severity. Authors recommend that future clinical repoform, further justication of which is delineated below [19].
Case managementData indicate that components of standard treatment were not comprehensively administered and monitorinshould have received antibiotics and antimalarials, but these were recorded for only 27% and 42% of patienthis was warranted or rather demonstrate sub-standard treatment, incomplete data recording, or both. Lack 74% increased odds of death, suggesting a possible relationship between data recording and outcome, thou1.74; 95%CI: 0.2315.06).Measurement of axillary body temperature, a basic non-invasive procedure, was recorded sporadically, if at atemperature recorded at least once per day for 80% of their hospital stay. This indication of sub-standard panding that only one patient developed fever for one day during hospitalisation. It is questionable whether thinfection, which seems likely to have been more frequent than data indicate. Sub-standard patient monitoringrespiratory rate, blood pressure and laboratory-based biochemical patient monitoring data. Since the use of prevented by safety concerns, it is important to develop a protocol for safe usage of such basic monitoring tohigh-biosafety eld laboratory to be located near-by future outbreak epicentres so that diagnostic results aredesirable if laboratory testing additionally included the monitoring of patient's biochemical parameters. Patietreatment regimens are to incorporate additional elements of intensive care (e.g. correcting electrolyte and mhaemodynamics, supplementing oxygen, and mitigating strong inammatory responses and disseminated intevaluation.While antibiotics and antimalarial administration and standard patient monitoring are deliverables for all patias indicated by symptomatology or disease severity. However, as in other data collection initiatives 69% of patients experience mild pain and appropriately receive paracetamol for its alleviation, or did other prelief? This diculty in interpretation also applies to administration of cimetidine, IV-uids, and ORS receivedOrganizations responsible for lovirus patient management should, prior to the next outbreak, consider thescollection accordingly.
Study limitations
-
Data were collected from laboratory-conrmed EBOV hospitalised patients on the two Ebola wards and not fridentied in the community [69]. Individuals receiving hospital care may dier from those not seeking and reless severe disease and survive more frequently, thus explaining the overall lower CFR compared to the one opatients (25% versus 42%). Moreover, limited data were collected from patients hospitalised early in the outAuthors were limited to describing administered treatment rather than assessing its impact on clinical outcommonitoring data precluded adjusting for potential confounding (e.g. by disease severity) of any association binstance, the borderline association of antimalarial treatment with fatal outcome could be explained by patiewith malaria or Ebola than those who did not.
Recommendations for improving data collection in lovirus outbreaksLikely reasons for incomplete patient monitoring and possible sub-standard treatment delivery include: (i) nocollection due to heavy workloads, particularly during the height of the outbreak, (ii) recording of patient datlikelihood of data mismanagement or loss, and (iii) lack of sta awareness of the importance and reasons formanagement during lovirus outbreaks. Organizations responsible for lovirus patient management thus neesupplies to improve data collection and case management components, similar to those used for intensive caThose responsible for lovirus case management must ensure that sucient supplies and equipment (e.g. thstethoscope, and sphygmomanometer, as used for previous lovirus patients [9], [19], available at outbreak response initiation. Together with appropriate training and comprehensive supportive tclinicians' eorts to deliver optimal care to future patients and enhance analyses of accurate epidemiologicaoutbreak control and treatment eorts for poorly understood lovirus diseases.Finally, laboratory tests (e.g. haemoglobin, complete and white blood cell counts) performed in past outbreaincluded in routine lovirus patient monitoring. On-site laboratory capacity would greatly facilitate case mandiagnostic and patient status results. The authors recommend on-site diagnostic and biochemical laboratory[29], [33], [34].
ConclusionsAuthors did not nd important dierences between the symptomatology of BEBOV and other FHF strains. fatality reported initially [8], but are similar to MacNeil and colleague's ndings among conrmed BEBOV cassignicantly increased the probability of patient death. Each additional symptom increased the odds of deathfactor.Recordkeeping and data collection were poor in both makeshift and fully functional Ebola wards. Standardisirecordkeeping on Ebola wards will help address the uncertainties discussed in this paper. Improved documenintensifying supportive care in future outbreaks. Safety protocols should be reviewed where they appear to csignicantly improving safety.
AcknowledgmentsFor their invaluable contributions to outbreak containment, authors thank the Uganda Ministry of Health, UgOutbreak Alert and Response Network (GOARN), Mdecins Sans Frontires, Uganda Virus Research Institute,African Field Epidemiology Network, International Federation of Red Cross and Red Crescent Societies (IFRCWorld Food Programme (WFP).
Author ContributionsPerformed the experiments: PR NH MDVK PPP ES BJ JL JW ZY RC MVH MB. Analyzed the data: PR NH MDVK M
-
1.
2.
3.
4.
View Article PubMed/NCBI Google Scholar
5.
View Article PubMed/NCBI Google Scholar
6.
7.
8.
9.
View Article PubMed/NCBI Google Scholar
10.
View Article PubMed/NCBI Google Scholar
11.
View Article PubMed/NCBI Google Scholar
12.
View Article PubMed/NCBI Google Scholar
13.
View Article PubMed/NCBI Google Scholar
14.
View Article PubMed/NCBI Google Scholar
PR NH MDVK PPP ES BJ JL JW ZY RC MVH MB. Wrote the paper: PR NH MDVK PPP ES BJ JL JW ZY RC MVH MB.
ReferencesFeldmann H, Geisbert T, Jahrling P, Klenk H, Netesov S, et al.. (2004) Filoviridae In: C.MFauquet MAM,Taxonomy, VIIIth Report of the ICTV. London: Elsevier/Academic Press. pp. 645653.
Kuhn J (2008) Filoviruses: a compendium of 40 years of epidemiological, clinical, and laboratory stud
WHO, CDC (1998) Infection Control for Viral Haemorrhagic Fevers in the African Health Care Setting./publications/ebola/WHO_EMC_ESR_98_2_EN/en/. Accessed 13 November 2012. Geneva: WHO.
Formenty P, Libama F, Epelboin A, Allarangar Y, Leroy E, et al. (2003) [Outbreak of Ebola hemorrhagicstrategy?]. Med Trop (Mars) 63: 291295. doi: 10.1086/503836
Leroy EM, Rouquet P, Formenty P, Souquiere S, Kilbourne A, et al. (2004) Multiple Ebola virus transmiwildlife. Science 303: 387390. doi: 10.1126/science.1092528
CDC (2007) Ebola Hemorrhagic Fever Outbreak in Uganda. Available: http://www.cdc.gov/ncidod/dvNovember 2012. Outbreak Postings.
CDC (2010) Known Cases and Outbreaks of Ebola Hemorrhagic Fever, in Chronological Order. Availabes/dispages/ebola/ebolatable.htm. [Accessed 13/11/2012]. CDC Special Pathogens Branch.
WHO (2008) Ebola outbreak contained in Uganda. Available: http://www.who.int/features/2008/ebo
Formenty P, Hatz C, Le Guenno B, Stoll A, Rogenmoser P, et al. (1999) Human infection due to Ebola vpresentation. J Infect Dis 179 Suppl 1S4853. doi: 10.1086/514285
Le Guenno B, Formenty P, Wyers M, Gounon P, Walker F, et al. (1995) Isolation and partial characteris12711274. doi: 10.1016/s0140-6736(95)90925-7
WHO (1995) Ebola virus Available at: http: whqlibdoc.who.int wer = WHO_WER_1995. [Accessed 22/1Epidemiologique Hebdomadaire 70: 137.
Fisher-Hoch SP, Brammer TL, Trappier SG, Hutwagner LC, Farrar BB, et al. (1992) Pathogenic potentihost and virus strain. J Infect Dis 166: 753763. doi: 10.1093/infdis/166.4.753
Becker S, Feldmann H, Will C, Slenczka W (1992) Evidence for occurrence of lovirus antibodies in hulovirus infections occur worldwide? Med Microbiol Immunol 181: 4355. doi: 10.1007/bf00193395
Rollin PE, Williams RJ, Bressler DS, Pearson S, Cottingham M, et al. (1999) Ebola (subtype Reston) virimported from the Philippines to the United States. J Infect Dis 179 Suppl 1: S108114. doi: 10.1086
-
15.
View Article PubMed/NCBI Google Scholar
16.
View Article PubMed/NCBI Google Scholar
17.
18.
View Article PubMed/NCBI Google Scholar
19.
View Article PubMed/NCBI Google Scholar
20.
View Article PubMed/NCBI Google Scholar
21.
View Article PubMed/NCBI Google Scholar
22.
23.
24.View Article PubMed/NCBI Google Scholar
25.View Article PubMed/NCBI Google Scholar
26.
View Article PubMed/NCBI Google Scholar
27.
28.
View Article PubMed/NCBI Google Scholar
29.
View Article PubMed/NCBI Google Scholar
30.
Miranda ME, Ksiazek TG, Retuya TJ, Khan AS, Sanchez A, et al. (1999) Epidemiology of Ebola (subtype179 Suppl 1: S115119. doi: 10.1086/514314
Bausch DG, Feldmann H, Geisbert TW, Bray M, Sprecher AG, et al. (2007) Outbreaks of lovirus hemoInfect Dis 196 Suppl 2: S136141. doi: 10.1086/520542
WHO (2005) Marburg haemorrhagic fever in Angola - update 25 (August 24, 2005). Available: Accessed 13 November 2012. Geneva.
Bausch DG, Borchert M, Grein T, Roth C, Swanepoel R, et al. (2003) Risk factors for Marburg hemorrhEmerg Infect Dis 9: 15311537. doi: 10.3201/eid0912.030355
Colebunders R, Tshomba A, Van Kerkhove MD, Bausch DG, Campbell P, et al. (2007) Marburg hemorrhRepublic of the Congo: clinical documentation, features of illness, and treatment. J Infect Dis 196 Sup
Bausch DG, Nichol ST, Muyembe-Tamfum JJ, Borchert M, Rollin PE, et al. (2006) Marburg hemorrhagicvirus. N Engl J Med 355: 909919. doi: 10.1056/nejmoa051465
Bausch DG, Sprecher AG, Jes B, Boumandouki P (2008) Treatment of Marburg and Ebola hemorrhagvaccines under outbreak conditions. Antiviral Res 78: 150161. doi: 10.1016/j.antiviral.2008.01.152
WHO (2008) Case of Marburg Haemorrhagic Fever imported into the Netherlands from Uganda. Avail/index.html. Accessed 13 November 2012. Geneva.
WHO (2008) Ebola haemorrhagic fever in the Democratic Republic of the Congo. Available: Accessed 13 November 2012. Geneva.
CDC (2009) Imported case of Marburg hemorrhagic fever Colorado 2008. Morbidity and Mortality W
Tus A (2009) Experimental vaccine may have saved Hamburg scientist from Ebola fever. BMJ 338: b1
Roddy P, Colebunders R, Lim M (in preparation) Filovirus hemorrhagic fever outbreak case managemeoptions. Journal of Infectious Disease doi: 10.1093/infdis/jir297
WHO (2011) Ebola in Uganda. Available: http://www.who.int/csr/don/2011_05_18/en
Ndambi R, Akamituna P, Bonnet MJ, Tukadila AM, Muyembe-Tamfum JJ, et al. (1999) Epidemiologic anMosango, Democratic Republic of the Congo, 1995. J Infect Dis 179 Suppl 1: S810. doi: 10.1086/51
Jes B, Roddy P, Weatherill D, de la Rosa O, Dorion C, et al. (2007) The Medecins Sans Frontieres inteepidemic, Uige, Angola, 2005. I. Lessons learned in the hospital. J Infect Dis 196 Suppl 2: S154161
Baert B (2001) Ebola outbreak preparedness and management. Brussels: Mdecins Sans Frontires B
-
31.
32.
View Article PubMed/NCBI Google Scholar
33.
View Article PubMed/NCBI Google Scholar
34.
View Article PubMed/NCBI Google Scholar
35.View Article PubMed/NCBI Google Scholar
36.
View Article PubMed/NCBI Google Scholar
37.
View Article PubMed/NCBI Google Scholar
38.
View Article PubMed/NCBI Google Scholar
39.
View Article PubMed/NCBI Google Scholar
40.
View Article PubMed/NCBI Google Scholar
41.
View Article PubMed/NCBI Google Scholar
42.
View Article PubMed/NCBI Google Scholar
43.
View Article PubMed/NCBI Google Scholar
44.
View Article PubMed/NCBI Google Scholar
45.
Sterk E (2008) Filovirus haemorrhagic fever guidelines. Barcelona: Mdecins Sans Frontires Operati
Casillas AM, Nyamathi AM, Sosa A, Wilder CL, Sands H (2003) A current review of Ebola virus: pathogassessment. Biol Res Nurs 4: 268275. doi: 10.1177/1099800403252603
Roddy P, Thomas SL, Jes B, Nascimento Folo P, Pablo Palma P, et al. (2010) Factors associated with from Uige, Angola. J Infect Dis 201: 19091918. doi: 10.1086/652748
Grolla A, Jones SM, Fernando L, Strong JE, Stroher U, et al. (2011) The Use of a Mobile Laboratory UnEpidemiological Surveillance during the 2005 Marburg Outbreak in Angola. PLoS Negl Trop Dis 5: e11
Bray M, Mahanty S (2003) Ebola hemorrhagic fever and septic shock. J Infect Dis 188: 16131617. d
Stroher U, Feldmann H (2006) Progress towards the treatment of Ebola haemorrhagic fever. Expert O10.1517/13543784.15.12.1523
Zaki SR, Goldsmith CS (1999) Pathologic features of lovirus infections in humans. Curr Top Microbio10.1007/978-3-642-59949-1_7
Davis KJ, Anderson AO, Geisbert TW, Steele KE, Geisbert JB, et al. (1997) Pathology of experimental EInvolvement of broblastic reticular cells. Arch Pathol Lab Med 121: 805819.
Jaax NK, Davis KJ, Geisbert TJ, Vogel P, Jaax GP, et al. (1996) Lethal experimental infection of rhesus moral and conjunctival route of exposure. Arch Pathol Lab Med 120: 140155.
Sureau PH (1989) Firsthand clinical observations of hemorrhagic manifestations in Ebola hemorrhagiS790793. doi: 10.1093/clinids/11.supplement_4.s790
Georges AJ, Leroy EM, Renaut AA, Benissan CT, Nabias RJ, et al. (1999) Ebola hemorrhagic fever outbhealth control issues. J Infect Dis 179 Suppl 1: S6575. doi: 10.1086/514290
Leroy EM, Souquiere S, Rouquet P, Drevet D (2002) Re-emergence of ebola haemorrhagic fever in Gab10.1016/s0140-6736(02)07796-6
Kalongi Y, Mwanza K, Tshisuaka M, Lusiama N, Ntando E, et al. (1999) Isolated case of Ebola hemorrhKinshasa, Democratic Republic of the Congo. J Infect Dis 179 Suppl 1: S1517. doi: 10.1086/514301
Kibadi K, Mupapa K, Kuvula K, Massamba M, Ndaberey D, et al. (1999) Late ophthalmologic manifestain Kikwit, Democratic Republic of the Congo. J Infect Dis 179 Suppl 1: S1314. doi: 10.1086/514288
Mupapa K, Mukundu W, Bwaka MA, Kipasa M, De Roo A, et al. (1999) Ebola hemorrhagic fever and pre
-
View Article PubMed/NCBI Google Scholar
46.
View Article PubMed/NCBI Google Scholar
47.
View Article PubMed/NCBI Google Scholar
48.
View Article PubMed/NCBI Google Scholar
49.View Article PubMed/NCBI Google Scholar
50.
51.
52.
View Article PubMed/NCBI Google Scholar
53.View Article PubMed/NCBI Google Scholar
54.
View Article PubMed/NCBI Google Scholar
55.View Article PubMed/NCBI Google Scholar
56.
View Article PubMed/NCBI Google Scholar
57.
View Article PubMed/NCBI Google Scholar
58.View Article PubMed/NCBI Google Scholar
59.
View Article PubMed/NCBI Google Scholar
60.
10.1086/514289
Mupapa K, Massamba M, Kibadi K, Kuvula K, Bwaka A, et al. (1999) Treatment of Ebola hemorrhagic fpatients. International Scientic and Technical Committee. J Infect Dis 179 Suppl 1: S1823. doi: 10.
Bonnet MJ, Akamituna P, Mazaya A (1998) Unrecognized Ebola hemorrhagic fever at Mosango HospitRepublic of the Congo. Emerg Infect Dis 4: 508510. doi: 10.3201/eid0403.980349
Bwaka MA, Bonnet MJ, Calain P, Colebunders R, De Roo A, et al. (1999) Ebola hemorrhagic fever in Kiobservations in 103 patients. J Infect Dis 179 Suppl 1: S17. doi: 10.1086/514308
WHO (1978) Ebola haemorrhagic fever in Zaire, 1976. Bull World Health Organ 56: 271293.
Isaacson M, Sureau P, Courteille G, Pattyn S (1978) Clinical aspects of Ebola virus disease at the Ngaeditor. Ebola virus hemorrhagic fever. Amsterdam: Elsevier/North Holland. pp. 1520.
Piot P, Sureau P, Breman G (1978) Clinical aspects of Ebola virus infection in Yambuku area, Zaire, 19fever: Elsevier/North-Holland. pp. 714.
Heymann DL, Weisfeld JS, Webb PA, Johnson KM, Cairns T, et al. (1980) Ebola hemorrhagic fever: Tandoi: 10.1093/infdis/142.3.372
WHO (1978) Ebola haemorrhagic fever in Sudan, 1976. Report of a WHO/International Study Team. B
Baron RC, McCormick JB, Zubeir OA (1983) Ebola virus disease in southern Sudan: hospital disseminOrgan 61: 9971003.
Emond RT, Evans B, Bowen ET, Lloyd G (1977) A case of Ebola virus infection. Br Med J 2: 541544. d
Mupere E, Kaducu OF, Yoti Z (2001) Ebola haemorrhagic fever among hospitalised children and adoleclinical observations. Afr Health Sci 1: 6065.
Siegert R, Shu HL, Slenczka W, Peters D, Muller G (1967) [On the etiology of an unknown human infecWochenschr 92: 23412343. doi: 10.1055/s-0028-1106144
Martini GA (1969) Marburg agent disease: in man. Trans R Soc Trop Med Hyg 63: 295302.
Martini GA, Knau HG, Schmidt HA, Mayer G, Baltzer G (1968) A hitherto unknown infectious diseasedisease. Ger Med Mon 13: 457470.
Martini G (1971) Marburg virus disease. Clinical syndrome. Marburg Virus Disease. New York: Springe
-
61.
62.
63.
64.
65.
View Article PubMed/NCBI Google Scholar
66.
View Article PubMed/NCBI Google Scholar
67.
View Article PubMed/NCBI Google Scholar
68.
69.
View Article PubMed/NCBI Google Scholar
70.
71.
View Article PubMed/NCBI Google Scholar
72.
73.
74.
View Article PubMed/NCBI Google Scholar
75.View Article PubMed/NCBI Google Scholar
76.
View Article PubMed/NCBI Google Scholar
Egbring R, Slenczka W, Baltzer G (1971) Clinical manifestations and mechanism of the haemorrhagicDisease. Berlin: Springer-Verlag. pp. 4249.
Stille W, Bohle E (1971) Clinical course and prognosis of Marburg virus (Green Monkey) disease. M1018.
Todorovitch K, Mocitch M, Klasnja R (1971) Clinical picture of two patients infected by the Marburg veVerlag. pp. 1923.
Nikiforov VV, Turovskii Iu I, Kalinin PP, Akinfeeva LA, Katkova LR, et al.. (1994) [A case of a laboratoryEpidemiol Immunobiol: 104106.
Johnson ED, Johnson BK, Silverstein D, Tukei P, Geisbert TW, et al. (1996) Characterization of a new MKenya. Arch Virol Suppl 11: 101114. doi: 10.1007/978-3-7091-7482-1_10
Smith DH, Johnson BK, Isaacson M, Swanapoel R, Johnson KM, et al. (1982) Marburg-virus disease in10.1016/s0140-6736(82)91871-2
Gear JS, Cassel GA, Gear AJ, Trappler B, Clausen L, et al. (1975) Outbreak of Marburg virus disease in10.1136/bmj.4.5995.489
WHO (2007) Ebola haemorrhagic fever in Uganda. Available: http://www.who.int/csr/don/2007_11_Geneva.
MacNeil A, Farnon EC, Wamala J, Okware S, Cannon DL, et al. (2010) Proportion of deaths and clinicaUganda. Emerg Infect Dis 16: 19691972. doi: 10.3201/eid1612.100627
WHO (2007) End of Ebola outbreak in Uganda. Available: http://www.who.int/csr/don/2007_02_20bGeneva.
Towner JS, Sealy TK, Khristova ML, Albarino CG, Conlan S, et al. (2008) Newly discovered ebola virusUganda. PLoS Pathog 4: e1000212. doi: 10.1371/journal.ppat.1000212
WHO (2004) WHO announces end of Ebola outbreak in southern Sudan. Available: 13 November 2012. Geneva.
WHO (2008) End of Ebola outbreak in the Democratic Republic of the Congo. Available: Accessed 13 November 2012. Geneva.
Borchert M, Muyembe-Tamfum JJ, Colebunders R, Libande M, Sabue M, et al. (2002) Short communican infant. Trop Med Int Health 7: 902906. doi: 10.1046/j.1365-3156.2002.00945.x
Dowell SF (1996) Ebola hemorrhagic fever: why were children spared? Pediatr Infect Dis J 15: 1891
Roels TH, Bloom AS, Bungton J, Muhungu GL, Mac Kenzie WR, et al. (1999) Ebola hemorrhagic feverisk factors for patients without a reported exposure. J Infect Dis 179 Suppl 1: S9297. doi: 10.1086
-
77.
View Article PubMed/NCBI Google Scholar
78.View Article PubMed/NCBI Google Scholar
79.
View Article PubMed/NCBI Google Scholar
80.View Article PubMed/NCBI Google Scholar
81.
View Article PubMed/NCBI Google Scholar
82.
Francesconi P, Yoti Z, Declich S, Onek PA, Fabiani M, et al. (2003) Ebola hemorrhagic fever transmissiInfect Dis 9: 14301437. doi: 10.3201/eid0911.030339
Hewlett BS, Amola RP (2003) Cultural contexts of Ebola in northern Uganda. Emerg Infect Dis 9: 124
Conrad JL, Isaacson M, Smith EB, Wul H, Crees M, et al. (1978) Epidemiologic investigation of MarbuMed Hyg 27: 12101215.
Bray M, Murphy FA (2007) Filovirus research: knowledge expands to meet a growing threat. J Infect D
Bausch DG, Towner JS, Dowell SF, Kaducu F, Lukwiya M, et al. (2007) Assessment of the risk of Ebola Infect Dis 196 Suppl 2: S142147. doi: 10.1086/520545
Buhler S (2008) Health care workers' experiences and preferences regarding documentation of clinicMarburg wards (MSc thesis). London: London School of Hygiene & Tropical Medicine.
Related Documents