http://acc.sagepub.com/ Care European Heart Journal: Acute Cardiovascular http://acc.sagepub.com/content/early/2014/07/29/2048872614540094 The online version of this article can be found at: DOI: 10.1177/2048872614540094 published online 30 July 2014 European Heart Journal: Acute Cardiovascular Care Escribano, Antonio Bayes-Genis, Domingo Pascual-Figal, Francisco J Chorro and Juan Sanchis Julio Núñez, Sergio Garcia, Eduardo Núñez, Clara Bonanad, Vicent Bodí, Gema Miñana, Enrique Santas, David cardio-renal syndrome revisited Early serum creatinine changes and outcomes in patients admitted for acute heart failure: the Published by: European Society of Cardiology ESC Working Group on Acute Cardiac Care and http://www.sagepublications.com can be found at: European Heart Journal: Acute Cardiovascular Care Additional services and information for http://acc.sagepub.com/cgi/alerts Email Alerts: http://acc.sagepub.com/subscriptions Subscriptions: http://www.sagepub.com/journalsReprints.nav Reprints: http://www.sagepub.com/journalsPermissions.nav Permissions: What is This? - Jul 30, 2014 OnlineFirst Version of Record >> by guest on August 2, 2014 acc.sagepub.com Downloaded from by guest on August 2, 2014 acc.sagepub.com Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
http://acc.sagepub.com/Care
European Heart Journal: Acute Cardiovascular
http://acc.sagepub.com/content/early/2014/07/29/2048872614540094The online version of this article can be found at:
DOI: 10.1177/2048872614540094
published online 30 July 2014European Heart Journal: Acute Cardiovascular CareEscribano, Antonio Bayes-Genis, Domingo Pascual-Figal, Francisco J Chorro and Juan Sanchis
Julio Núñez, Sergio Garcia, Eduardo Núñez, Clara Bonanad, Vicent Bodí, Gema Miñana, Enrique Santas, Davidcardio-renal syndrome revisited
Early serum creatinine changes and outcomes in patients admitted for acute heart failure: the
Published by:
European Society of Cardiology
ESC Working Group on Acute Cardiac Care
and http://www.sagepublications.com
can be found at:European Heart Journal: Acute Cardiovascular CareAdditional services and information for
http://acc.sagepub.com/cgi/alertsEmail Alerts:
http://acc.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
What is This?
- Jul 30, 2014OnlineFirst Version of Record >>
by guest on August 2, 2014acc.sagepub.comDownloaded from by guest on August 2, 2014acc.sagepub.comDownloaded from
European Heart Journal: Acute Cardiovascular Care 1 –11© The European Society of Cardiology 2014Reprints and permissions: sagepub.co.uk/journalsPermissions.navDOI: 10.1177/2048872614540094acc.sagepub.com
EUROPEANSOCIETY OFCARDIOLOGY ®
Introduction
Approximately 20%–40% of patients admitted for acute decompensated heart failure (ADHF) develop worsening
renal function (WRF).1–3 The pathophysiology of WRF in ADHF is complex, multifactorial and not completely
Early serum creatinine changes and outcomes in patients admitted for acute heart failure: the cardio-renal syndrome revisited
Julio Núñez1, Sergio Garcia1, Eduardo Núñez1, Clara Bonanad1, Vicent Bodí1, Gema Miñana2, Enrique Santas1, David Escribano1, Antonio Bayes-Genis3, Domingo Pascual-Figal4, Francisco J Chorro1 and Juan Sanchis1
AbstractBackground: The changes in renal function that occurred in patients with acute decompensated heart failure (ADHF) are prevalent, and have multifactorial etiology and dissimilar prognosis. To what extent the prognostic role of such changes may vary according to the presence of renal insufficiency at admission is not clear. Accordingly, we sought to determine whether early creatinine changes (ΔCr) (admission to 48–72 hours) had an effect on 1-year mortality relative to the presence of renal insufficiency at admission.Methods: We included 705 consecutive patients admitted with the diagnosis of ADHF. Admission renal insufficiency was defined as serum creatinine ≥1.4mg/dl (A-RIcr) or estimated glomerular filtration rate <60ml/min/1.73m2 (A-RIGFR). Appropriate survival regression techniques were used.Results: The mean age was 72.9±11.4 years and 51.2% were males. Patients with admission renal insufficiency (24.7% and 42.8% for A-RIcr and A-RIGFR, respectively) had higher prevalence of extreme values in ΔCr in either direction (increasing/decreasing). At 1-year follow-up, 114 (16.2%) deaths were registered. The multivariable analysis showed a significant interaction between admission renal insufficiency and ΔCr (p=0.004 and p=0.019 for A-RIcr and A-RIGFR, respectively). In the presence of renal insufficiency, the continuum of ΔCr followed a positive and almost linear relationship with mortality risk. Conversely, in patients without renal insufficiency, those changes adopted a ‘J-shape’ trajectory with increased mortality at both ends of the curve distribution.Conclusions: In patients with ADHF the effect of ΔCr on 1-year mortality varied according to its magnitude and the presence of admission renal insufficiency. There was a graded-association with mortality when renal insufficiency was present on admission.
Keywordsabsolute creatinine changes, acute decompensated heart failure, mortality, renal failure, worsening renal function
Received: 15 Apr 2014; Accepted: 24 May 2014
1 Servicio de Cardiología, Hospital Clínico Universitario, INCLIVA, Universitat de Valencia, Spain
2Servicio de Cardiología, Hospital de Manises, Valencia, Spain3 Servicio de Cardiología, Hospital Universitari Germas Trias i Pujol, Badalona, Spain
540094 ACC0010.1177/2048872614540094European Heart Journal: Acute Cardiovascular CareNúñez et al.research-article2014
Original scientific paper
4 Servicio de Cardiología, Hospital Virgen de la Arrixaca, Universidad de Murcia, Murcia, Spain
Corresponding author:Julio Núñez, Servicio de Cardiología, Hospital Clínico Universitario, Avda. Blasco Ibáñez 17, 46010 Valencia, Spain. Email: [email protected]
by guest on August 2, 2014acc.sagepub.comDownloaded from

2 European Heart Journal: Acute Cardiovascular Care
understood.4 Historically, WRF has been attributed to reduced cardiac output and, consequently, renal under-perfusion (prerenal azotemia), especially after an aggres-sive use of loop diuretics.5,6 Nevertheless, recent evidence have brought into consideration other factors, such as structural tubular damage,7 systemic venous conges-tion,5,7–9 neurohormonal activation10 and elevated intra-abdominal pressure.11,12
Classically, developing WRF in the setting of chronic heart failure and ADHF has shown to increase the prognos-tic burden of this disease.1–3 Nevertheless, recent observa-tions have shown that it may also operate as a surrogate for decongestion, a condition related to response to treatment and better outcomes.13–16 Intriguingly, most of these studies have shown that patients who experienced hemoconcentra-tion showed better renal function compared to those that did not fulfill this criteria.13–16 In an attempt to conciliate both postulates, we speculate that, in ADHF, the prognostic implications for those renal function changes are differen-tially influenced by the status of renal function on admis-sion. In addition, some caveats still prevail around this topic: a) the current WFR definitions came from non-heart failure scenarios,17 and no specific threshold have been validated/inferred for patients with ADHF18 and, b) there is scarce information regarding the prognostic meaning of a decrease in serum creatinine (sCr).
We aimed to evaluate the association of these early changes in sCr (ΔCr) and the risk of 1-year all-cause mor-tality and whether this association is modified by the pres-ence of admission renal insufficiency (A-RI). As secondary endpoint, we sought to evaluate the clinical determinants of ΔCr.
Methods
Study group and protocol
We studied a consecutive cohort of 705 patients admitted for ADHF in the Cardiology department of a third-level center (Hospital Clínico Universitario de Valencia) from 1 July 2010 to 31 December 2012. ADHF was defined as the rapid onset of symptoms and signs secondary to abnormal cardiac function and the presence of objective evidence of structural or functional abnormality of heart at rest (cardio-megaly, third heart sound, cardiac murmur, abnormality of the echocardiogram or raised natriuretic peptides).6,19 Patients with a final diagnosis of pneumonia, sepsis, acute coronary syndrome or end-stage renal failure on dialysis or imminent need of dialysis were excluded from this study. Demographic data, medical history, vital signs, 12-lead electrocardiogram and laboratory data were routinely deter-mined during hospitalization following pre-established reg-istry questionnaires. Left ventricular ejection fraction was assessed by echocardiography (Agilent Sonos 5500; Phillips) during index hospitalization. Treatment was
individualized following established guidelines.6,19 The protocol was approved by the ethical committee of our cen-tre in accordance with the principles of the Declaration of Helsinki and national regulations. All patients signed the informed consent, in accordance with the principles of the Declaration of Helsinki and national regulations.
Exposure
The absolute difference in sCr between patient’s admission and the following 48–72 hours constitutes the main focus of this study. Those patients who had only one measure-ment due to an early death were excluded by design (n=14). In simple terms, our goal was to test the interaction between A-RI and ΔCr against 1-year mortality.
RF was defined by two clinically accepted cut points: sCr ≥1.4 mg/dl (A-RIcr) and eGFR <60 ml/min/1.73m2 (A-RIGFR). Estimated glomerular filtration rate (eGFR) was estimated from the 4-variable Modification of Diet in Renal Disease study equation.20 For comparability purpose, WRF was defined as ΔCr >0.3 mg/dl (WRF0.3) and ΔCr >0.5 mg/dl (WRF0.5). Because we were also interested in looking for any prognostic trend across the severity of cardio-renal injury, the KDIGO17 classification (Stage 1 to 3) was esti-mated as follows: Stage 1 ≥1.5-fold of baseline sCr or ΔCr≥0.3 mg/dl; Stage 2 ≥2-fold of baseline sCr; Stage 3 ≥3-fold of baseline sCr or ΔCr ≥4.0 mg/dl.
Endpoints
The primary endpoint for this study was all-cause mortality with the cohort censored at 1-year follow-up. The second-ary endpoint was to determine the clinical predictors of ΔCr in this population.
Statistical analysis
Continuous variables are presented as mean ±1 standard deviation (SD) or median, interquartile range (IQR) when appropriate, and were compared among the indicators of renal insufficiency by the Fisher-exact test or Wilcoxon rank-sum test when appropriate. Discrete variables were presented as percentages and compared with Chi2 test.
Prognostic evaluation of ΔCr. These analyses were addressed by using a parametric proportional hazard regression which is a part of the Royston-Parmar models.21 According to our working hypothesis, we forced in every model the interac-tion between renal insufficiency status and ΔCr. As a com-mon building-strategy, the selection of covariates was conducted by backward elimination using a multivariable fractional polynomial algorithm.22 The set of covariates used for 1-year mortality were: age (years), etiology, Charlson score, serum sodium (mEq/l), NT-proBNP (pg/ml), high-sensitivity troponin T (ng/ml), systolic blood
by guest on August 2, 2014acc.sagepub.comDownloaded from

Núñez et al. 3
pressure (mmHg), progressive worsening of known chronic heart failure, anemia, and the interaction between A-RI and ΔCr. In the models, the baseline hazard function was mod-eled with 4-degrees of freedom restricted cubic splines. Estimates are presented as hazard ratios with their respec-tive 95% CIs, or as event-rates when appropriate.
Clinical predictors of ΔCr. Multivariable linear regression analysis was performed to determine the risk factors that predict ΔCr.
A 2-sided p-value of <0.05 was considered to be statisti-cally significant for all analyses. All analyses were per-formed using Stata 13.1 (StataCorp. 2011. Stata Statistical Software: Release 12. College).
Results
Differences in baseline characteristics according to A-RI status
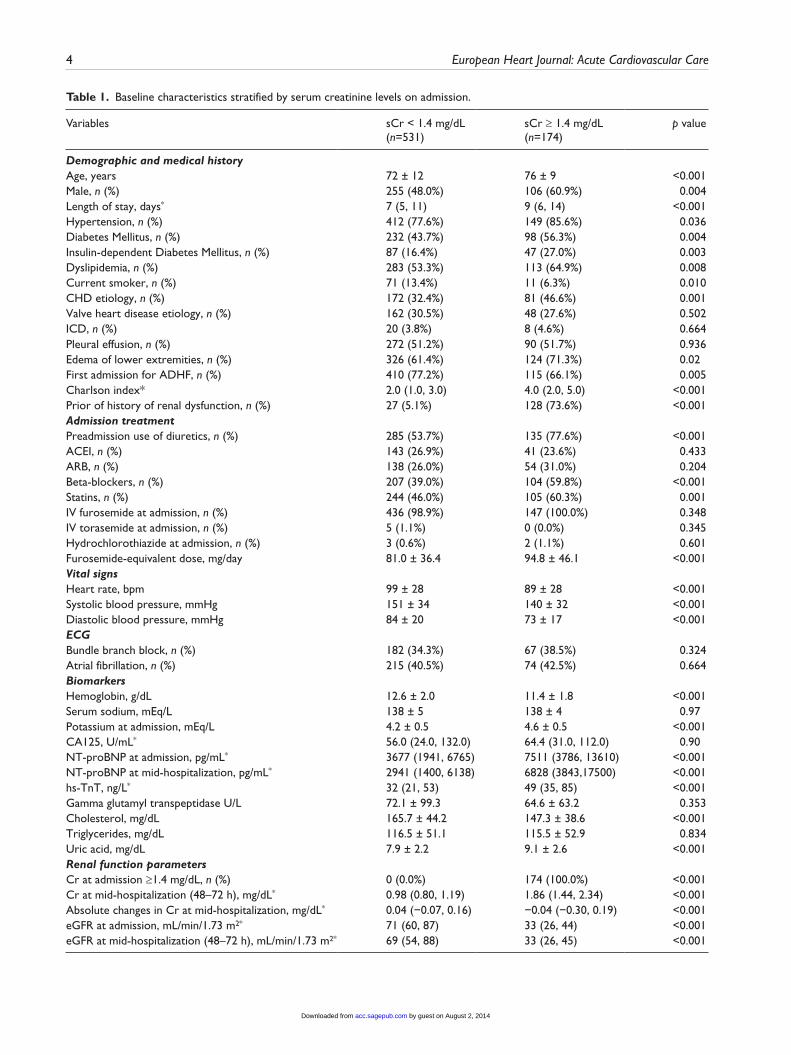
The prevalence of A-RI varied from 24.7% (n=174) to 42.8% (n=302) if the criteria used to define it was sCr (A-RIcr) or eGFR (A-RIGFR), respectively. The means eGFR for males and females patients with A-RIcr were 37.8±10.8 ml/min/1.73m2 and 27.1±7.0 ml/min/1.73m2, respectively). Except for gender distribution, differences between patients with and without renal insufficiency were in the same direction, no matter which definition of A-RI was used. Overall, patients with A-RI were older and had higher prevalence of comorbid conditions such as ischemic heart disease, hypertension, diabetes, dyslipidemia and anemia. At the examination, patients with A-RI had more peripheral edema and lower systolic blood pressure, diastolic blood pressure and heart rate. Patients with A-RI were more frequently receiving loop diuretics, beta-blockers, and statins prior to admission and, once admitted, these patients were treated with higher dose of intravenous loop diuretics. No sig-nificant differences between A-RI/non-A-RI were documented in other baseline characteristics.
ΔCr according to A-RIcrPatients with A-RIcr had a decrease in the median ΔCr but also displayed higher prevalence of extreme values in ΔCr in either direction (increasing/decreasing) (0.04 mg/dl [−0.07, 0.16] and −0.04 mg/dl [−0.30, 0.19], p<0.001 for non-A-RIcr and A-RIcr, respectively). The prevalence of WRF0.3 and WRF0.5 was higher for patients with A-RIcr (p<0.05 for both comparisons). A trend to higher acute kid-ney injury across KDIGO classification was found for those with A-RIcr (see Table 1).
ΔCr according to A-RIGFR
There was an increase in the median of ΔCr for both groups which was greater, however, for patients with non-A-RIGFR
(0.04 mg/dl [−0.06, 0.16] and 0.01 mg/dl [−0.20, 0.19], p=0.009, for non-A-RIGFR and A-RIGFR, respectively). Likewise, extreme values for ΔCr were more frequent in those with A-RIGFR. The prevalence of WRF0.5 was higher for patients with A-RIGFR at admission (p=0.002). A trend was noticed for WRF0.3 (p=0.085). A-RIGFR was not associ-ated to acute kidney injury according KDIGO classifica-tion. (Table 2).
Clinical outcomes
In the whole population, we registered 24 (3.4%) in- hospital deaths and 114 (16.2%) deaths at 1-year follow-up. In a stratified analysis by A-RI status and independently of the criteria used, A-RI was a marker for worst clinical out-comes (Supplementary Table 1). No significant differences were present in the bivariate association between ΔCr and 1-year mortality (0.03 mg/dl [−0.09, 0.18] vs. 0.01 mg/dl [−0.18, 0.15], p=0.101) in all patients. By grading the cohort on severity of acute kidney injury (KDIGO criteria), we found, in a bivariate analysis, no association with 1-year mortality. Similarly, WRF0.3 was not associated to higher 1-year mortality. Only WRF0.5 was related to higher rates of 1-year mortality (Table 3).
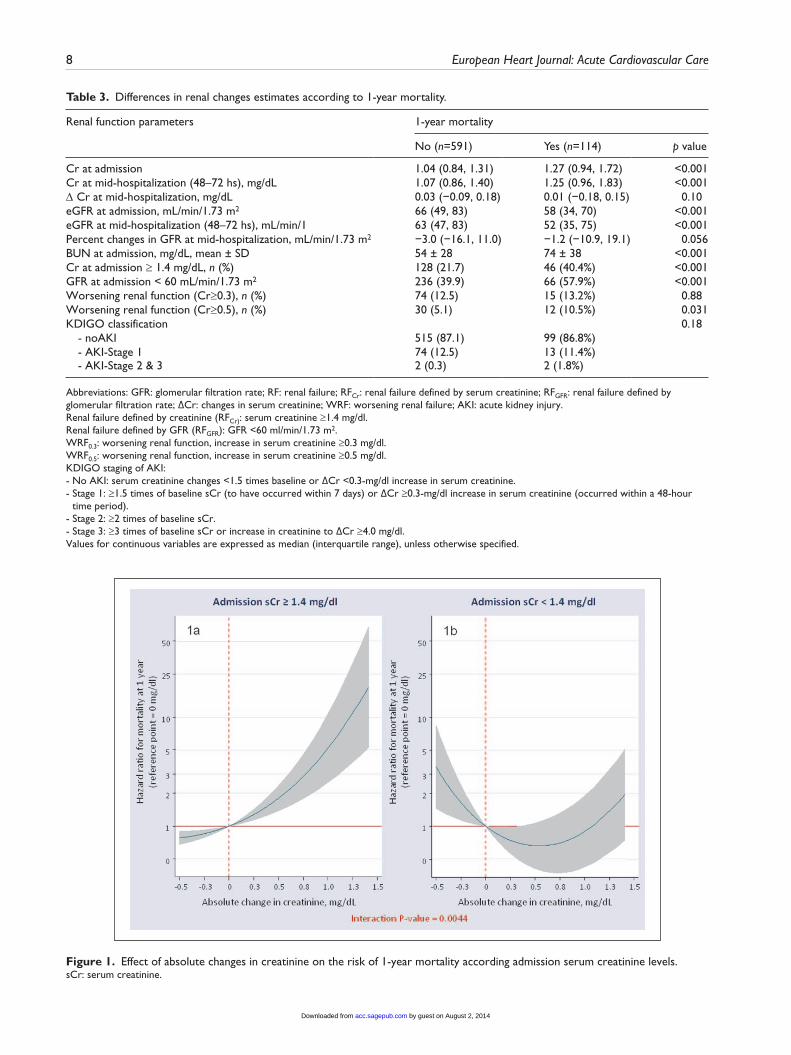
In a multivariable setting for 1-year mortality, there was a significant interaction between A-RIcr and ΔCr (p=0.004) (Figure 1). In summary, we can identify very distinctive patterns of the association between ΔCr and the risk of mortality according to A-RIcr status. In the presence of A-RIcr, the continuum of ΔCr followed an almost linear relationship with the risk of mortality (Figure 1a). Thus, WRF (>0.3 mg/dl and >0.5 mg/dl com-pared to no changes) was related to an increase risk of 1-year death (HRs: 1.36; CI 95% = 1.18–1.56 and 1.8; CI 95% = 1.38–2.35, respectively). However, the associa-tion pattern for non-A-RIcr showed a marginal U-shaped association with the risk of death with increasing risk at both ends of ΔCr distribution (Figure 1b). In this sub-group of patients, the use of the traditional thresholds for defining WRF (>0.3 mg/dl and >0.5 mg/dl) vs. patients with no changes were not significantly associated to worse outcomes and even, a trend to improve prognosis was documented for values around 0.3 mg/dl. However, a deleterious effect on mortality was noticed with impor-tant increase of but also small decrease in ΔCr (Figure 1b). The C-statistics estimated from this model was 0.77. By censoring the cohort at 6-month and 60-days follow-up, similar results were obtained (Supplementary Figures 1 and 2, respectively).
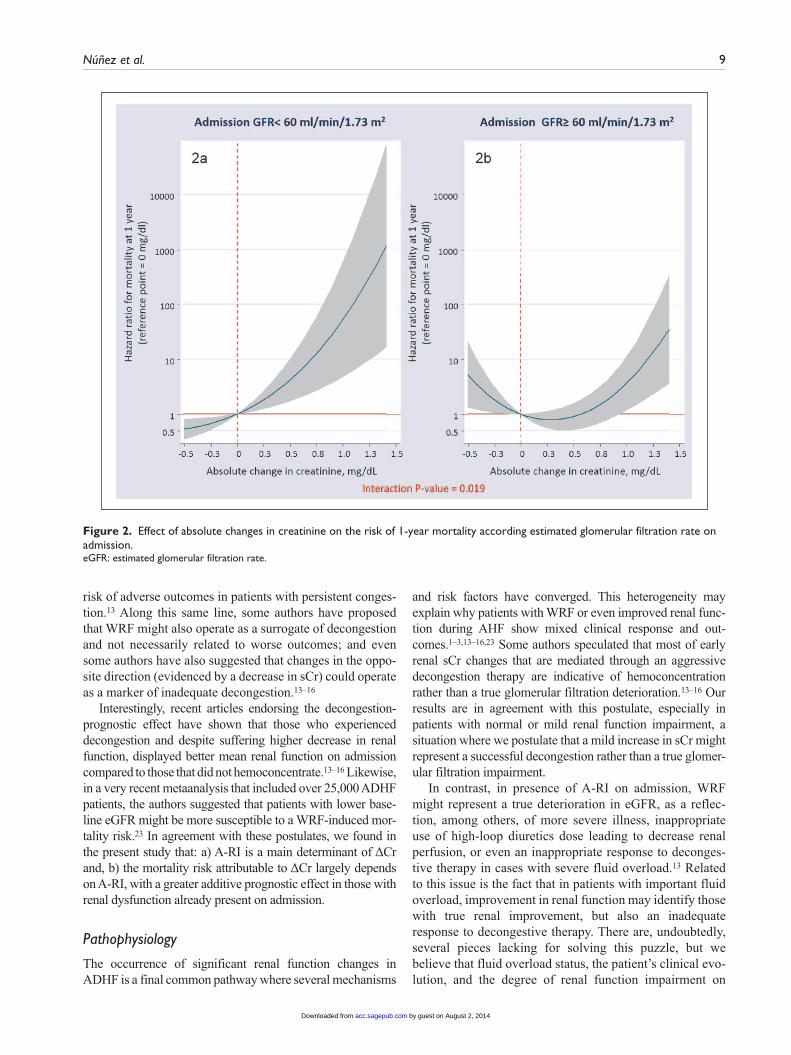
A similar pattern of association was documented when renal insufficiency at baseline was defined as eGFR <60 ml/min/1.73m2 (p=0.019). A linear and positive signifi-cant association was observed for ΔCr in patients with A-RIGFR (Figure 2a) whereas in patients with non-A-RIGRF, a significant increase in risk was only observed
by guest on August 2, 2014acc.sagepub.comDownloaded from
4 European Heart Journal: Acute Cardiovascular Care
Table 1. Baseline characteristics stratified by serum creatinine levels on admission.
Variables sCr < 1.4 mg/dL (n=531)
sCr ≥ 1.4 mg/dL (n=174)
p value
Demographic and medical historyAge, years 72 ± 12 76 ± 9 <0.001Male, n (%) 255 (48.0%) 106 (60.9%) 0.004Length of stay, days* 7 (5, 11) 9 (6, 14) <0.001Hypertension, n (%) 412 (77.6%) 149 (85.6%) 0.036Diabetes Mellitus, n (%) 232 (43.7%) 98 (56.3%) 0.004Insulin-dependent Diabetes Mellitus, n (%) 87 (16.4%) 47 (27.0%) 0.003Dyslipidemia, n (%) 283 (53.3%) 113 (64.9%) 0.008Current smoker, n (%) 71 (13.4%) 11 (6.3%) 0.010CHD etiology, n (%) 172 (32.4%) 81 (46.6%) 0.001Valve heart disease etiology, n (%) 162 (30.5%) 48 (27.6%) 0.502ICD, n (%) 20 (3.8%) 8 (4.6%) 0.664Pleural effusion, n (%) 272 (51.2%) 90 (51.7%) 0.936Edema of lower extremities, n (%) 326 (61.4%) 124 (71.3%) 0.02First admission for ADHF, n (%) 410 (77.2%) 115 (66.1%) 0.005Charlson index* 2.0 (1.0, 3.0) 4.0 (2.0, 5.0) <0.001Prior of history of renal dysfunction, n (%) 27 (5.1%) 128 (73.6%) <0.001Admission treatmentPreadmission use of diuretics, n (%) 285 (53.7%) 135 (77.6%) <0.001ACEI, n (%) 143 (26.9%) 41 (23.6%) 0.433ARB, n (%) 138 (26.0%) 54 (31.0%) 0.204Beta-blockers, n (%) 207 (39.0%) 104 (59.8%) <0.001Statins, n (%) 244 (46.0%) 105 (60.3%) 0.001IV furosemide at admission, n (%) 436 (98.9%) 147 (100.0%) 0.348IV torasemide at admission, n (%) 5 (1.1%) 0 (0.0%) 0.345Hydrochlorothiazide at admission, n (%) 3 (0.6%) 2 (1.1%) 0.601Furosemide-equivalent dose, mg/day 81.0 ± 36.4 94.8 ± 46.1 <0.001Vital signsHeart rate, bpm 99 ± 28 89 ± 28 <0.001Systolic blood pressure, mmHg 151 ± 34 140 ± 32 <0.001Diastolic blood pressure, mmHg 84 ± 20 73 ± 17 <0.001ECGBundle branch block, n (%) 182 (34.3%) 67 (38.5%) 0.324Atrial fibrillation, n (%) 215 (40.5%) 74 (42.5%) 0.664BiomarkersHemoglobin, g/dL 12.6 ± 2.0 11.4 ± 1.8 <0.001Serum sodium, mEq/L 138 ± 5 138 ± 4 0.97Potassium at admission, mEq/L 4.2 ± 0.5 4.6 ± 0.5 <0.001CA125, U/mL* 56.0 (24.0, 132.0) 64.4 (31.0, 112.0) 0.90NT-proBNP at admission, pg/mL* 3677 (1941, 6765) 7511 (3786, 13610) <0.001NT-proBNP at mid-hospitalization, pg/mL* 2941 (1400, 6138) 6828 (3843,17500) <0.001hs-TnT, ng/L* 32 (21, 53) 49 (35, 85) <0.001Gamma glutamyl transpeptidase U/L 72.1 ± 99.3 64.6 ± 63.2 0.353Cholesterol, mg/dL 165.7 ± 44.2 147.3 ± 38.6 <0.001Triglycerides, mg/dL 116.5 ± 51.1 115.5 ± 52.9 0.834Uric acid, mg/dL 7.9 ± 2.2 9.1 ± 2.6 <0.001Renal function parametersCr at admission ≥1.4 mg/dL, n (%) 0 (0.0%) 174 (100.0%) <0.001Cr at mid-hospitalization (48–72 h), mg/dL* 0.98 (0.80, 1.19) 1.86 (1.44, 2.34) <0.001Absolute changes in Cr at mid-hospitalization, mg/dL* 0.04 (−0.07, 0.16) −0.04 (−0.30, 0.19) <0.001eGFR at admission, mL/min/1.73 m2* 71 (60, 87) 33 (26, 44) <0.001eGFR at mid-hospitalization (48–72 h), mL/min/1.73 m2* 69 (54, 88) 33 (26, 45) <0.001
by guest on August 2, 2014acc.sagepub.comDownloaded from
Núñez et al. 5
Variables sCr < 1.4 mg/dL (n=531)
sCr ≥ 1.4 mg/dL (n=174)
p value
Percent changes in eGFR at mid-hospitalization, mL/min/1.73 m2*
−4.1 (−16.9, 9.5) 3.0 (−11.2, 21.0) <0.001
Urea at admission, mg/dL 46 ± 17 92 ± 35 <0.001Worsening renal function (Cr≥0.3), n (%) 58 (10.9%) 31 (17.8%) 0.020Worsening renal function (Cr≥0.5), n (%) 21 (4.0%) 21 (12.1%) <0.001KDIGO classification, n (%) 0.056 - No AKI 471 (88.7) 143 (82.2) - AKI Stage 1 56 (10.5) 31 (17.8) - AKI Stage 2 3 (0.6) 0 (0.0) - AKI Stage 3 1 (0.2) 0 (0.0) EchocardiographyLVEF, % 47.8 ± 16.2 47.9 ± 15.8 0.952Left atrium diameter, mm 42.8 ± 8.6 43.5 ± 7.3 0.331TAPSE, mm* 18.0 (16.0, 21.0) 18.0 (15.0, 21.0) 0.570Treatments at dischargeFurosemide, n (%) 415 (80.7%) 148 (90.8%) 0.003Torsemide, n (%) 91 (17.7%) 15 (9.2%) 0.009Hydrochlorothiazide, n (%) 22 (4.1%) 10 (5.7%) 0.401ACEI, n (%) 224 (43.1%) 39 (24.7%) <0.001ARB, n (%) 156 (30.1%) 42 (26.6%) 0.432Beta-blockers, n (%) 414 (79.6%) 123 (77.4%) 0.583Nitrates, n (%) 57 (11.0%) 30 (18.9%) 0.011Digoxin, n (%) 106 (20.5%) 19 (12.1%) 0.021Spironolactone, n (%) 137 (26.6%) 21 (13.5%) <0.001Eplerenone, n (%) 73 (23.9%) 23 (22.3%) 0.791Statins, n (%) 304 (58.6%) 104 (65.4%) 0.144Allopurinol, n (%) 57 (11.0%) 55 (34.6%) <0.001Antiarrhythmics, n (%) 39 (7.3%) 22 (12.6%) 0.042Calcium channel blocker, n (%) 88 (16.6%) 50 (28.7%) <0.001Oral anticoagulants, n (%) 250 (48.3%) 72 (45.6%) 0.596
Abbreviations: CHD: coronary heart disease; ICD: implantable cardioverter defibrillator; ADHF: acute decompensate heart failure; ACEI: angiotensin converting enzyme inhibitors; ARB: angiotensin II receptor blockers; CA125: antigen carbohydrate 125; NT-proBNP: amino-terminal pro-brain natriuretic peptide; hs-TnT: high-sensitive troponin T; Cr: serum creatinine; eGFR: estimated glomerular filtration rate; KDIGO: Kidney Disease Improving Global Outcomes; AKI: acute kidney injury; LVEF: left ventricular ejection fraction; TAPSE: tricuspid annular plane systolic excursion.Values for continuous variables are expressed as mean (SD), unless otherwise specified; categorical variables are presented as percentages.*Value presented as the median (interquartile range).
Table 1. (Continued)
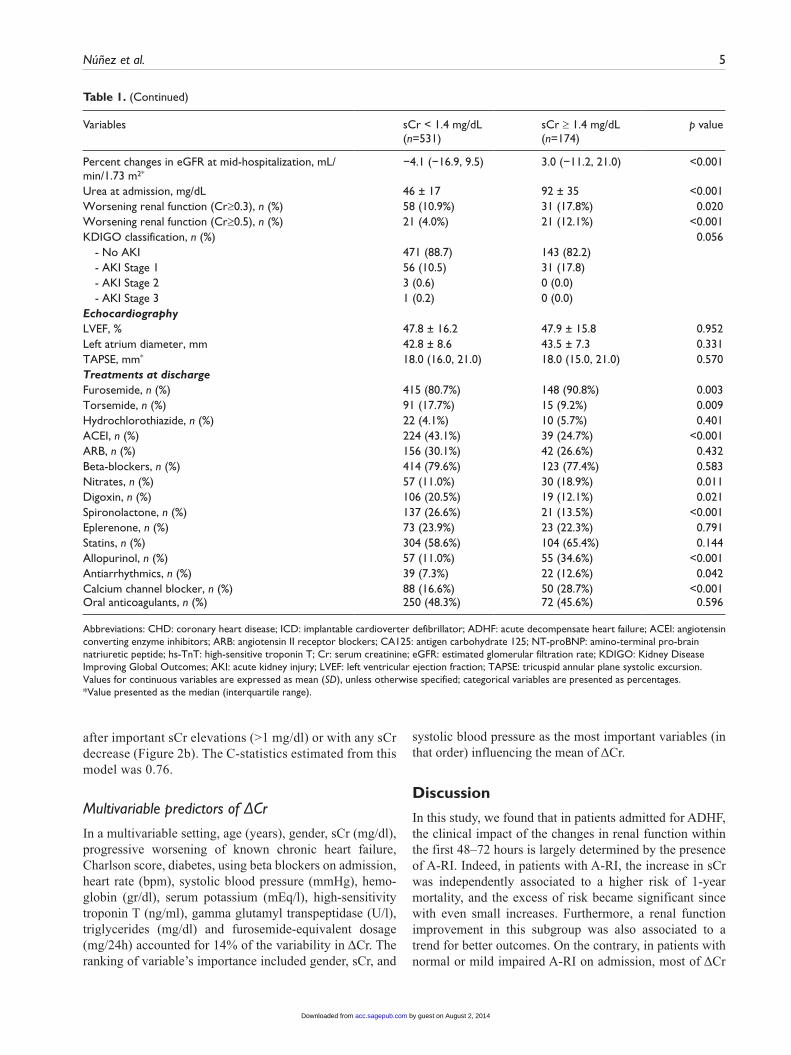
after important sCr elevations (>1 mg/dl) or with any sCr decrease (Figure 2b). The C-statistics estimated from this model was 0.76.
Multivariable predictors of ΔCr
In a multivariable setting, age (years), gender, sCr (mg/dl), progressive worsening of known chronic heart failure, Charlson score, diabetes, using beta blockers on admission, heart rate (bpm), systolic blood pressure (mmHg), hemo-globin (gr/dl), serum potassium (mEq/l), high-sensitivity troponin T (ng/ml), gamma glutamyl transpeptidase (U/l), triglycerides (mg/dl) and furosemide-equivalent dosage (mg/24h) accounted for 14% of the variability in ΔCr. The ranking of variable’s importance included gender, sCr, and
systolic blood pressure as the most important variables (in that order) influencing the mean of ΔCr.
Discussion
In this study, we found that in patients admitted for ADHF, the clinical impact of the changes in renal function within the first 48–72 hours is largely determined by the presence of A-RI. Indeed, in patients with A-RI, the increase in sCr was independently associated to a higher risk of 1-year mortality, and the excess of risk became significant since with even small increases. Furthermore, a renal function improvement in this subgroup was also associated to a trend for better outcomes. On the contrary, in patients with normal or mild impaired A-RI on admission, most of ΔCr
by guest on August 2, 2014acc.sagepub.comDownloaded from
6 European Heart Journal: Acute Cardiovascular Care
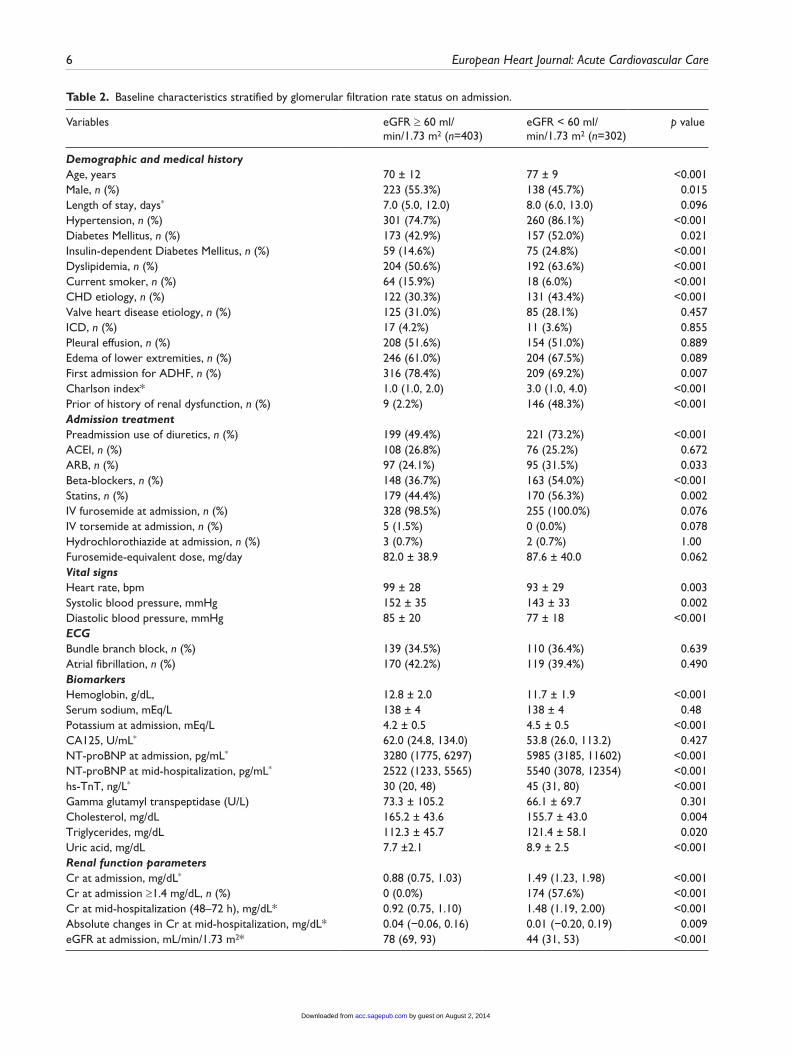
Table 2. Baseline characteristics stratified by glomerular filtration rate status on admission.
Variables eGFR ≥ 60 ml/min/1.73 m2 (n=403)
eGFR < 60 ml/min/1.73 m2 (n=302)
p value
Demographic and medical historyAge, years 70 ± 12 77 ± 9 <0.001Male, n (%) 223 (55.3%) 138 (45.7%) 0.015Length of stay, days* 7.0 (5.0, 12.0) 8.0 (6.0, 13.0) 0.096Hypertension, n (%) 301 (74.7%) 260 (86.1%) <0.001Diabetes Mellitus, n (%) 173 (42.9%) 157 (52.0%) 0.021Insulin-dependent Diabetes Mellitus, n (%) 59 (14.6%) 75 (24.8%) <0.001Dyslipidemia, n (%) 204 (50.6%) 192 (63.6%) <0.001Current smoker, n (%) 64 (15.9%) 18 (6.0%) <0.001CHD etiology, n (%) 122 (30.3%) 131 (43.4%) <0.001Valve heart disease etiology, n (%) 125 (31.0%) 85 (28.1%) 0.457ICD, n (%) 17 (4.2%) 11 (3.6%) 0.855Pleural effusion, n (%) 208 (51.6%) 154 (51.0%) 0.889Edema of lower extremities, n (%) 246 (61.0%) 204 (67.5%) 0.089First admission for ADHF, n (%) 316 (78.4%) 209 (69.2%) 0.007Charlson index* 1.0 (1.0, 2.0) 3.0 (1.0, 4.0) <0.001Prior of history of renal dysfunction, n (%) 9 (2.2%) 146 (48.3%) <0.001Admission treatmentPreadmission use of diuretics, n (%) 199 (49.4%) 221 (73.2%) <0.001ACEI, n (%) 108 (26.8%) 76 (25.2%) 0.672ARB, n (%) 97 (24.1%) 95 (31.5%) 0.033Beta-blockers, n (%) 148 (36.7%) 163 (54.0%) <0.001Statins, n (%) 179 (44.4%) 170 (56.3%) 0.002IV furosemide at admission, n (%) 328 (98.5%) 255 (100.0%) 0.076IV torsemide at admission, n (%) 5 (1.5%) 0 (0.0%) 0.078Hydrochlorothiazide at admission, n (%) 3 (0.7%) 2 (0.7%) 1.00Furosemide-equivalent dose, mg/day 82.0 ± 38.9 87.6 ± 40.0 0.062Vital signsHeart rate, bpm 99 ± 28 93 ± 29 0.003Systolic blood pressure, mmHg 152 ± 35 143 ± 33 0.002Diastolic blood pressure, mmHg 85 ± 20 77 ± 18 <0.001ECGBundle branch block, n (%) 139 (34.5%) 110 (36.4%) 0.639Atrial fibrillation, n (%) 170 (42.2%) 119 (39.4%) 0.490BiomarkersHemoglobin, g/dL, 12.8 ± 2.0 11.7 ± 1.9 <0.001Serum sodium, mEq/L 138 ± 4 138 ± 4 0.48Potassium at admission, mEq/L 4.2 ± 0.5 4.5 ± 0.5 <0.001CA125, U/mL* 62.0 (24.8, 134.0) 53.8 (26.0, 113.2) 0.427NT-proBNP at admission, pg/mL* 3280 (1775, 6297) 5985 (3185, 11602) <0.001NT-proBNP at mid-hospitalization, pg/mL* 2522 (1233, 5565) 5540 (3078, 12354) <0.001hs-TnT, ng/L* 30 (20, 48) 45 (31, 80) <0.001Gamma glutamyl transpeptidase (U/L) 73.3 ± 105.2 66.1 ± 69.7 0.301Cholesterol, mg/dL 165.2 ± 43.6 155.7 ± 43.0 0.004Triglycerides, mg/dL 112.3 ± 45.7 121.4 ± 58.1 0.020Uric acid, mg/dL 7.7 ±2.1 8.9 ± 2.5 <0.001Renal function parametersCr at admission, mg/dL* 0.88 (0.75, 1.03) 1.49 (1.23, 1.98) <0.001Cr at admission ≥1.4 mg/dL, n (%) 0 (0.0%) 174 (57.6%) <0.001Cr at mid-hospitalization (48–72 h), mg/dL* 0.92 (0.75, 1.10) 1.48 (1.19, 2.00) <0.001Absolute changes in Cr at mid-hospitalization, mg/dL* 0.04 (−0.06, 0.16) 0.01 (−0.20, 0.19) 0.009eGFR at admission, mL/min/1.73 m2* 78 (69, 93) 44 (31, 53) <0.001
by guest on August 2, 2014acc.sagepub.comDownloaded from
Núñez et al. 7
Variables eGFR ≥ 60 ml/min/1.73 m2 (n=403)
eGFR < 60 ml/min/1.73 m2 (n=302)
p value
eGFR at mid-hospitalization (48–72 h), mL/min/1.73 m2* 77 (63, 92) 43 (31, 53) <0.001Percent changes in eGFR at mid-hospitalization, mL/min/1.73 m2*
−4.3 (−17.7, 8.4) −1.1 (−13.1, 17.2) <0.001
eGFR at admission <60 mL/min/1.73 m2 0 (0.0%) 302 (100.0%) <0.001Urea at admission, mg/dL 42 ± 16 77 ± 34 <0.001Worsening renal function (Cr≥0.3), n (%) 43 (10.7%) 46 (15.2%) 0.083Worsening renal function (Cr≥0.5), n (%) 14 (3.5%) 28 (9.3%) 0.002KDIGO classification, n (%) 0.262 - No AKI 358 (88.8) 256 (84.8) - AKI Stage 1 42 (10.4) 45 (14.9) - AKI Stage 2 2 (0.5) 1 (0.3) - AKI Stage 3 1 (0.2) 0 (0.0) EchocardiographyLVEF, % 47.3 ± 16.3 48.4 ± 15.8 0.378Left atrium diameter, mm 42.9 ± 8.6 43.1 ± 7.8 0.841TAPSE, mm* 18.0 (16.0, 21.0) 18.0 (15.5, 21.0) 0.205Treatment at dischargeFurosemide, n (%) 313 (80.3%) 250 (87.1%) 0.021Torasemide, n (%) 70 (17.9%) 36 (12.5%) 0.078Hydrochlorothiazide, n (%) 18 (4.5%) 14 (4.6%) 1.00ACEI, n (%) 173 (43.7%) 90 (31.9%) 0.002ARB, n (%) 116 (29.4%) 82 (29.1%) 1.00Beta-blockers, n (%) 312 (78.8%) 225 (79.5%) 0.85Nitrates, n (%) 35 (8.9%) 52 (18.4%) <0.001Digoxin, n (%) 78 (19.8%) 47 (16.8%) 0.370Spironolactone, n (%) 103 (26.3%) 55 (19.6%) 0.055Eplerenone, n (%) 58 (24.7%) 38 (22.0%) 0.564Statins, n (%) 222 (56.2%) 186 (65.7%) 0.019Allopurinol, n (%) 39 (9.9%) 73 (25.8%) <0.001Antiarrhythmics, n (%) 29 (7.2%) 32 (10.6%) 0.146Calcium channel blocker, n (%) 68 (16.9%) 70 (23.2%) 0.044Oral anticoagulants, n (%) 192 (48.9%) 130 (45.9%) 0.481
Abbreviations: CHD: coronary heart disease; ICD: implantable cardioverter defibrillator; ADHF: acute decompensate heart failure; ACEI: angiotensin converting enzyme inhibitors; ARB: angiotensin II receptor blockers; CA125: antigen carbohydrate 125; NT-proBNP: amino-terminal pro-brain natriuretic peptide; hs-TnT: high-sensitive troponin T; Cr: serum creatinine; eGFR: estimated glomerular filtration rate; KDIGO: Kidney Disease Improving Global Outcomes; AKI: acute kidney injury; LVEF: left ventricular ejection fraction; TAPSE: tricuspid annular plane systolic excursion.Values for continuous variables are expressed as mean (SD), unless otherwise specified; categorical variables are presented as percentages.*Value presented as the median (interquartile range).
Table 2. (Continued)
seen in daily practice were not significantly associated with mortality and only important ΔCr increases (greater than 1 mg) were related to worse outcomes. Interestingly, in this subgroup of patients, a decrease in ΔCr was associated to worse outcomes. Thus, we believe our results pointed out to the importance for accounting for renal function on admis-sion when interpreting the clinical implications of early renal changes in the setting of ADHF.
Previous studies
Several studies have endorsed the deleterious prognostic effect of WRF in ADHF in regard to the risk of death,
rehospitalization, and length of stay.1–3 In addition, a recent meta-analysis concluded that: a) chronic kidney disease was an independent predictor for WRF during hospitalization; and b) WRF was consistently associated with long-term mortality.23 Moreover, recent studies have also shown that renal changes may also operate as surrogate of response to decongestive therapy, suggesting that the prognostic effect of renal changes during AHF are influenced, at least in part, by fluid-overload status and response to decongestive ther-apy.13–16 For instance, Metra et al. reported in 599 consecu-tive patients with ADHF that, in the absence of clinical signs of congestion, any increase in sCr did not have prognostic value; meanwhile, WRF was strongly associated to a higher
by guest on August 2, 2014acc.sagepub.comDownloaded from
8 European Heart Journal: Acute Cardiovascular Care
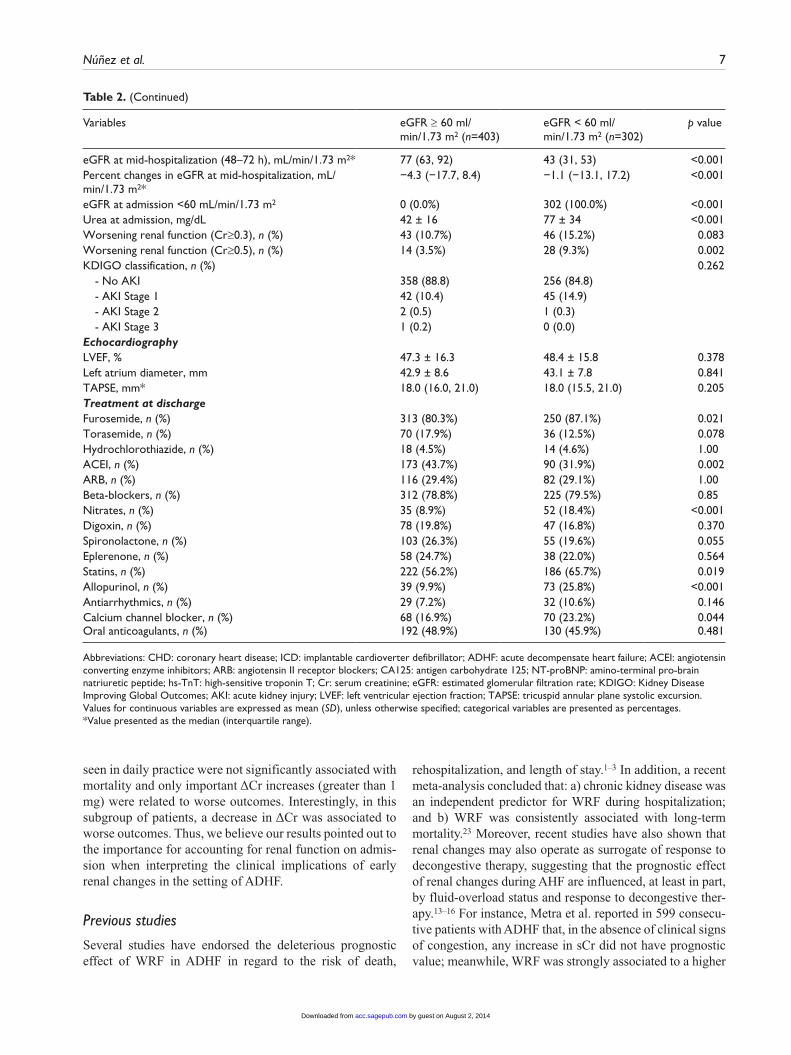
Figure 1. Effect of absolute changes in creatinine on the risk of 1-year mortality according admission serum creatinine levels.sCr: serum creatinine.
Table 3. Differences in renal changes estimates according to 1-year mortality.
Renal function parameters 1-year mortality
No (n=591) Yes (n=114) p value
Cr at admission 1.04 (0.84, 1.31) 1.27 (0.94, 1.72) <0.001Cr at mid-hospitalization (48–72 hs), mg/dL 1.07 (0.86, 1.40) 1.25 (0.96, 1.83) <0.001Δ Cr at mid-hospitalization, mg/dL 0.03 (−0.09, 0.18) 0.01 (−0.18, 0.15) 0.10eGFR at admission, mL/min/1.73 m2 66 (49, 83) 58 (34, 70) <0.001eGFR at mid-hospitalization (48–72 hs), mL/min/1 63 (47, 83) 52 (35, 75) <0.001Percent changes in GFR at mid-hospitalization, mL/min/1.73 m2 −3.0 (−16.1, 11.0) −1.2 (−10.9, 19.1) 0.056BUN at admission, mg/dL, mean ± SD 54 ± 28 74 ± 38 <0.001Cr at admission ≥ 1.4 mg/dL, n (%) 128 (21.7) 46 (40.4%) <0.001GFR at admission < 60 mL/min/1.73 m2 236 (39.9) 66 (57.9%) <0.001Worsening renal function (Cr≥0.3), n (%) 74 (12.5) 15 (13.2%) 0.88Worsening renal function (Cr≥0.5), n (%) 30 (5.1) 12 (10.5%) 0.031KDIGO classification 0.18 - noAKI 515 (87.1) 99 (86.8%) - AKI-Stage 1 74 (12.5) 13 (11.4%) - AKI-Stage 2 & 3 2 (0.3) 2 (1.8%)
Abbreviations: GFR: glomerular filtration rate; RF: renal failure; RFCr: renal failure defined by serum creatinine; RFGFR: renal failure defined by glomerular filtration rate; ΔCr: changes in serum creatinine; WRF: worsening renal failure; AKI: acute kidney injury.Renal failure defined by creatinine (RFCr): serum creatinine ≥1.4 mg/dl.Renal failure defined by GFR (RFGFR): GFR <60 ml/min/1.73 m2.WRF0.3: worsening renal function, increase in serum creatinine ≥0.3 mg/dl.WRF0.5: worsening renal function, increase in serum creatinine ≥0.5 mg/dl.KDIGO staging of AKI:- No AKI: serum creatinine changes <1.5 times baseline or ΔCr <0.3-mg/dl increase in serum creatinine.- Stage 1: ≥1.5 times of baseline sCr (to have occurred within 7 days) or ΔCr ≥0.3-mg/dl increase in serum creatinine (occurred within a 48-hour
time period).- Stage 2: ≥2 times of baseline sCr.- Stage 3: ≥3 times of baseline sCr or increase in creatinine to ΔCr ≥4.0 mg/dl.Values for continuous variables are expressed as median (interquartile range), unless otherwise specified.
by guest on August 2, 2014acc.sagepub.comDownloaded from
Núñez et al. 9
risk of adverse outcomes in patients with persistent conges-tion.13 Along this same line, some authors have proposed that WRF might also operate as a surrogate of decongestion and not necessarily related to worse outcomes; and even some authors have also suggested that changes in the oppo-site direction (evidenced by a decrease in sCr) could operate as a marker of inadequate decongestion.13–16
Interestingly, recent articles endorsing the decongestion-prognostic effect have shown that those who experienced decongestion and despite suffering higher decrease in renal function, displayed better mean renal function on admission compared to those that did not hemoconcentrate.13–16 Likewise, in a very recent metaanalysis that included over 25,000 ADHF patients, the authors suggested that patients with lower base-line eGFR might be more susceptible to a WRF-induced mor-tality risk.23 In agreement with these postulates, we found in the present study that: a) A-RI is a main determinant of ΔCr and, b) the mortality risk attributable to ΔCr largely depends on A-RI, with a greater additive prognostic effect in those with renal dysfunction already present on admission.
Pathophysiology
The occurrence of significant renal function changes in ADHF is a final common pathway where several mechanisms
and risk factors have converged. This heterogeneity may explain why patients with WRF or even improved renal func-tion during AHF show mixed clinical response and out-comes.1–3,13–16,23 Some authors speculated that most of early renal sCr changes that are mediated through an aggressive decongestion therapy are indicative of hemoconcentration rather than a true glomerular filtration deterioration.13–16 Our results are in agreement with this postulate, especially in patients with normal or mild renal function impairment, a situation where we postulate that a mild increase in sCr might represent a successful decongestion rather than a true glomer-ular filtration impairment.
In contrast, in presence of A-RI on admission, WRF might represent a true deterioration in eGFR, as a reflec-tion, among others, of more severe illness, inappropriate use of high-loop diuretics dose leading to decrease renal perfusion, or even an inappropriate response to deconges-tive therapy in cases with severe fluid overload.13 Related to this issue is the fact that in patients with important fluid overload, improvement in renal function may identify those with true renal improvement, but also an inadequate response to decongestive therapy. There are, undoubtedly, several pieces lacking for solving this puzzle, but we believe that fluid overload status, the patient’s clinical evo-lution, and the degree of renal function impairment on
Figure 2. Effect of absolute changes in creatinine on the risk of 1-year mortality according estimated glomerular filtration rate on admission.eGFR: estimated glomerular filtration rate.
by guest on August 2, 2014acc.sagepub.comDownloaded from

10 European Heart Journal: Acute Cardiovascular Care
admission are the pivotal pathophysiological factors that need to be researched for unraveling the clinical meaning of renal function changes in patients with ADHF.
Clinical implications
In agreement with our results, baseline renal function should be taken into account when interpreting renal change in AHF setting. A clinical awareness should be guided by the magnitude of ΔCr, particularly in cases with renal dysfunction. Our results advocate for a thor-oughly diagnostic work-up, close follow-up and, poten-tial therapeutic modifications when WRF occurs in patients where renal dysfunction was already present on admission; conversely, in patients without renal dysfunc-tion, a mild-moderate creatinine increase might be a proxi for decongestion.
In this regard, our data are in agreement with the results obtained from randomized Pre-RELAX and RELAX-AHF where the therapeutic effect of Serelaxin in 1161 patients admitted for ADHF and concomitant renal dysfunction on admission was evaluated.24,25 In a RELAX-AHF trial, WRF (creatinine increase ≥0.3mg/dl and cystatin-C increase ≥0.3mg/l at 2 days) was associated to higher risk of 180-days mortality (HR=1.76 [1.11–2.82] and 2.10 [1.38–3.20]), respectively. Promisingly, Serelaxin administration was associated with a lower incidence of WRF at day 2, lower serum creatinine, and plasma cystatin-C values in the first 5 days after enrollment, and a reduction in the risk of 180-days mortality.26 These results reinforce the potential role of these new therapeutic avenues aimed to avoid organ-damage, and consequently to decrease the morbimortality following an episode of decompensation.
Limitations
This is an observational study where causality cannot be inferred; moreover, various additional limitations should be stated: a) sCr may not be the most accurate and sensi-tive parameter for detecting early renal function changes,27 b) we did not routinely assessed other markers of decon-gestion during hospitalization; variables that may operate as confounders or might better dissect this complex inter-action, c) late-hospitalization renal status was not system-atically evaluated, d) the effect of pharmacological treatment on renal status, and indirectly on prognostic could not be assessed with this design and, e) the lack of longitudinal assessment of renal function, particularly pre and post hospitalization, precludes to dissect more pre-cisely the trajectories of renal function and its clinical implications following an admission for ADHF.
Conclusions
In patients admitted for ADHF, the prognostic implications of early ΔCr are differentially influenced by renal function
on admission. Based on our results, these changes had greater prognostic impact in those patients with A-RI.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding sources
This work was supported in part by grants from Instituto de Salud Carlos III, Red de Investigación Cardiovascular, Programa 7 (RD12/0042/0010) FEDER, PI11/02323, Prometeo/2013/007 and Novartis.
Supplementary Material
The online figures are available at http://acc.sagepub.com/supplemental-data
References
1. Butler J, Chirovsky D, Phatak H, et al. Renal function, health outcomes, and resource utilization in acute heart failure: a systematic review. Circ Heart Fail 2010; 3: 726–745.
2. Maeder MT, Rickli H, Pfisterer ME, et al; TIME-CHF Investigators. Incidence, clinical predictors, and prognostic impact of worsening renal function in elderly patients with chronic heart failure on intensive medical therapy. Am Heart J 2012; 163: 407–414.
3. Damman K, Navis G, Voors AA, et al. Worsening renal func-tion and prognosis in heart failure: systematic review and meta-analysis. J Card Fail 2007; 13: 599–608.
4. Testani JM and Damman K. Venous congestion and renal function in heart failure … it’s complicated. Eur J Heart Fail 2013; 15: 599–601.
5. Ljungman S, Laragh JH and Cody RJ. Role of the kidney in congestive heart failure. Relationship of cardiac index to kidney function. Drugs 1990; 39 Suppl 4: 10–21; discussion 22–24.
6. McMurray JJ, Adamopoulos S, Anker SD, et al; ESC Committee for Practice Guidelines. ESC Guidelines for the diagnosis and treatment of acute and chronic heart fail-ure 2012: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association (HFA) of the ESC. Eur Heart J 2012; 33: 1787–1847.
7. Damman K, Ng Kam Chuen MJ, MacFadyen RJ, et al. Volume status and diuretic therapy in systolic heart failure and the detection of early abnormalities in renal and tubular function. J Am Coll Cardiol 2011; 57: 2233–2241.
8. Mullens W, Abrahams Z, Francis GS, et al. Importance of venous congestion for worsening of renal function in advanced decompensated heart failure. J Am Coll Cardiol 2009; 53: 589–596.
9. Ross EA. Congestive renal failure: the pathophysiology and treatment of renal venous hypertension. J Card Fail 2012; 18: 930–938.
10. Paterna S, Parrinello G, Cannizzaro S, et al. Medium term effects of different dosage of diuretic, sodium, and fluid administration on neurohormonal and clinical outcome in patients with recently compensated heart failure. Am J Cardiol 2009; 103: 93–102.
by guest on August 2, 2014acc.sagepub.comDownloaded from
Núñez et al. 11
11. Mullens W, Abrahams Z, Francis GS, et al. Prompt reduction in intra-abdominal pressure following large-volume mechan-ical fluid removal improves renal insufficiency in refractory decompensated heart failure. J Card Fail 2008; 14: 508–514.
12. Mullens W, Abrahams Z, Skouri HN, et al. Elevated intra-abdominal pressure in acute decompensated heart failure: a potential contributor to worsening renal function? J Am Coll Cardiol 2008; 51: 300–306.
13. Metra M, Davison B, Bettari L, et al. Is worsening renal function an ominous prognostic sign in patients with acute heart failure? The role of congestion and its interaction with renal function. Circ Heart Fail 2012; 5: 54–62.
14. Testani JM, Chen J, McCauley BD, et al. Potential effects of aggressive decongestion during the treatment of decompen-sated heart failure on renal function and survival. Circulation 2010; 122: 265–272.
15. Greene SJ, Gheorghiade M, Vaduganathan M, et al; EVEREST Trial investigators. Haemoconcentration, renal function, and post-discharge outcomes among patients hos-pitalized for heart failure with reduced ejection fraction: insights from the EVEREST trial. Eur J Heart Fail 2013; 112: 1763–1769.
16. van der Meer P, Postmus D, Ponikowski P, et al. The predic-tive value of short-term changes in hemoglobin concentra-tion in patients presenting with acute decompensated heart failure. J Am Coll Cardiol 2013; 61: 1973–1981.
17. Roy AK, Mc Gorrian C, Treacy C, et al. A comparison of tra-ditional and novel definitions (RIFLE, AKIN, and KDIGO) of acute kidney injury for the prediction of outcomes in acute decompensated heart failure. Cardiorenal Med 2013; 3: 26–37.
18. Sheerin NJ, Newton PJ, Macdonald PS, et al. Worsening renal function in heart failure: The need for a consensus definition. Int J Cardiol. Epub ahead of print 21 April 2014. pii: S0167-5273(14)00842-0. DOI: 10.1016/j.ijcard.2014.04.162.
19. Dickstein K, Cohen-Solal A, Filippatos G, et al; ESC Committee for Practice Guidelines (CPG). ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure 2008: the Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2008 of the European
Society of Cardiology. Developed in collaboration with the Heart Failure Association of the ESC (HFA) and endorsed by the European Society of Intensive Care Medicine (ESICM). Eur Heart J 2008; 29: 2388–2442.
20. Levey AS, Coresh J, Greene T, et al. Chronic Kidney Disease Epidemiology Collaboration. Using standardized serum cre-atinine values in the modification of diet in renal disease study equation for estimating glomerular filtration rate. Ann Intern Med 2006; 145: 247–254.
21. Royston P and Parmar MK. Flexible parametric proportional-hazards and proportional-odds models for censored survival data, with application to prognostic modelling and estima-tion of treatment effects. Stat Med 2002; 21: 2175–2197.
22. Sauerbrei W, Royston P and Binder H. Selection of impor-tant variables and determination of functional form for con-tinuous predictors in multivariable model building. Stat Med 2007; 26: 5512–5528.
23. Damman K, Valente MA, Voors AA, et al. Renal impairment, worsening renal function, and outcome in patients with heart failure: an updated meta-analysis. Eur Heart J 2014; 35: 455–469.
24. Teerlink JR, Metra M, Felker GM, et al. Relaxin for the treatment of patients with acute heart failure (Pre-RELAX-AHF): a multicentre, randomised, placebo-controlled, parallel-group, dose-finding phase IIb study. Lancet 2009; 373: 1429–1439.
25. Teerlink JR, Cotter G, Davison BA, et al; RELAX in in Acute Heart Failure (RELAX-AHF) Investigators. Serelaxin, recombinant human relaxin-2, for treatment of acute heart failure (RELAX-AHF): a randomised, placebo-controlled trial. Lancet 2013; 381: 29–39.
26. Metra M, Cotter G, Davison BA, et al; RELAX-AHF Investigators. Effect of serelaxin on cardiac, renal, and hepatic biomarkers in the Relaxin in Acute Heart Failure (RELAX-AHF) development program: correlation with out-comes. J Am Coll Cardiol 2013; 61: 196–206.
27. Taub PR, Borden KC, Fard A, et al. Role of biomarkers in the diagnosis and prognosis of acute kidney injury in patients with cardiorenal syndrome. Expert Rev Cardiovasc Ther 2012; 10: 657–667.
by guest on August 2, 2014acc.sagepub.comDownloaded from
Related Documents











