H Mehdian MD , FRCS Consultant Spinal Surgeon The Centre for Spinal Studies and Surgery, Queen’s Medical Centre, Nottingham Management of Paediatric Spinal Deformity

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
H Mehdian MD , FRCS
Consultant Spinal Surgeon
The Centre for Spinal Studies and Surgery, Queen’s Medical
Centre, Nottingham
Management of Paediatric Spinal
Deformity

Paediatric Spinal Deformity
1) Early Onset Scoliosis
2) Late Onset Scoliosis
a) Idiopathic Scoliosis
b) Neuromuscular Scoliosis
c) Congenital Scoliosis
d) Syndromic Scoliosis

Classification
Idiopathic Scoliosis
Old Classification
Infantile Onset < 3 yrs Age
Juvenile Onset 3-10 yrs Age
Adolescent Onset > 10 yrs Age
New Classification
Early onset Onset < 8 yrs Age
Late onset Onset > 8 yrs Age
Approximately 80% of patients with scoliosis have
idiopathic scoliosis
Classification
Early Onset Scoliosis
Definition Curves greater than 10 degrees in a child under the age of five years are defined as early onset scoliosis, this umbrella term includes:
1) Idiopathic Scoliosis
2) Neuromuscular Scoliosis
3) Congenital Scoliosis
1) Syndromic Scoliosis
The first five years of life are crucial as the lungs
are still growing dramatically
Constriction of the chest cavity as a result of a
spinal deformity significantly restricts lung
growth and may contribute to serious pulmonary
complications
Early Onset Scoliosis
Early Onset Scoliosis
Scoliosis
New classification reflects the importance of
lung development up to age 7
At birth 20 million alveoli
Age 5 300 million alveoli
Early Onset
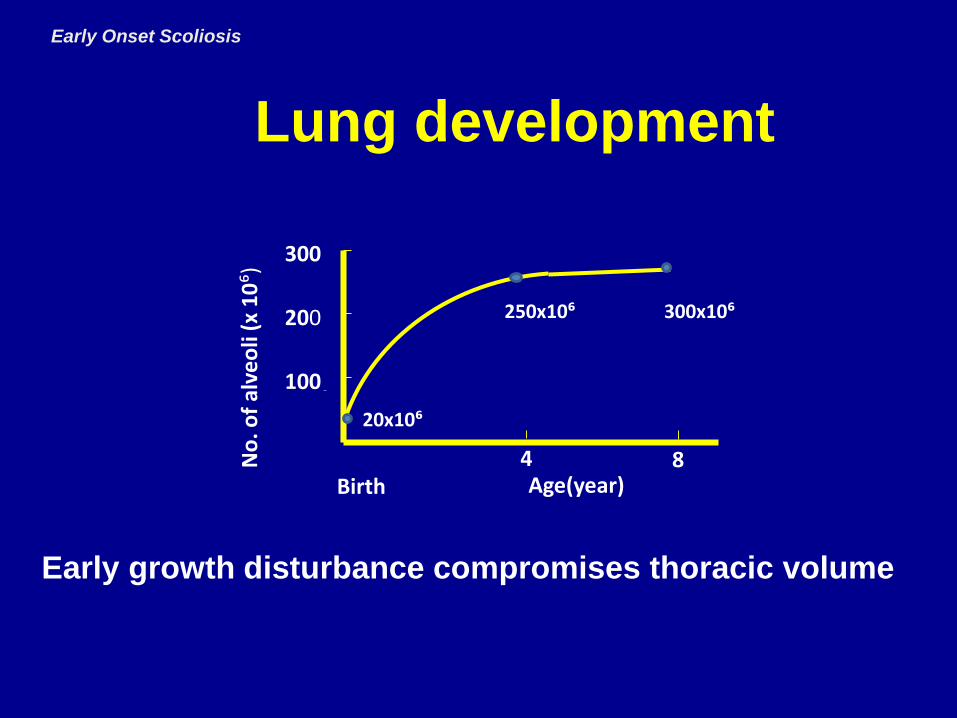
Lung development
4 8
300
250x10⁶200
100
Age(year)Birth
No
. of
alve
oli
(x 1
0⁶)
300x10⁶
20x10⁶
Early growth disturbance compromises thoracic volume
Early Onset Scoliosis
Idiopathic Scoliosis
75% of the curves , resolve spontaneously
25% of the curves, progress very rapidly
(malignant)
• Identify the malignant curves, prevent
development of respiratory compromise
Features
• Male
• Left sided Thoracic curve
Early Onset Scoliosis
Early Onset
Early onset
Idiopathic Scoliosis
Predicting Progression
Early Onset Scoliosis
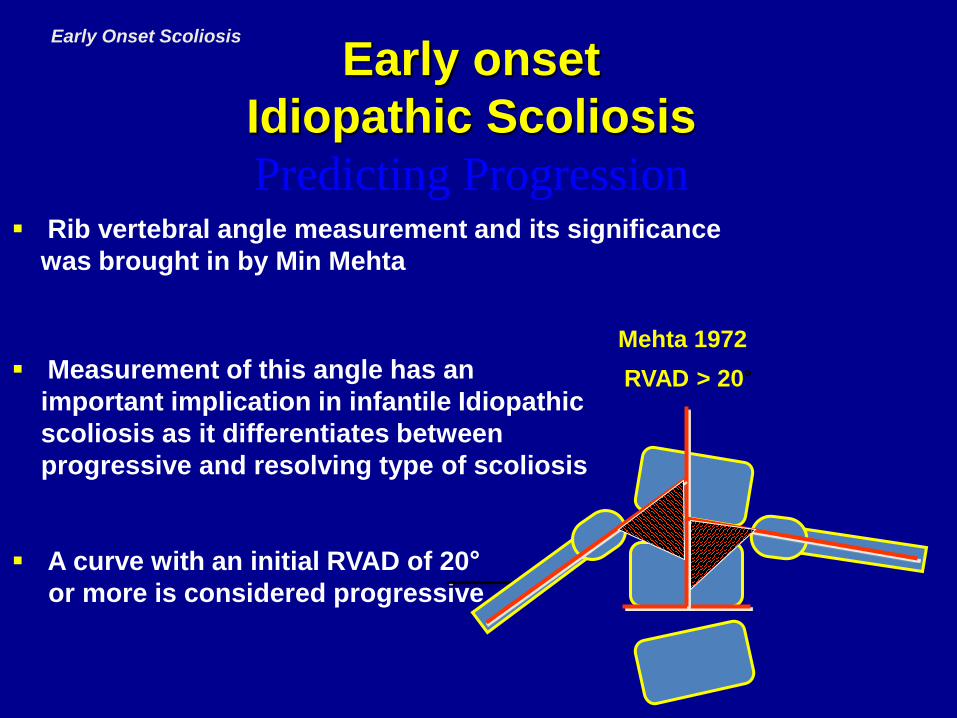
Rib vertebral angle measurement and its significance
was brought in by Min Mehta
Measurement of this angle has an
important implication in infantile Idiopathic
scoliosis as it differentiates between
progressive and resolving type of scoliosis
A curve with an initial RVAD of 20°
or more is considered progressive
RVAD > 20°
Mehta 1972

Predicting Progression
RVAD > 20°
Mehta 1972
Convex RVA < 68°
Kristmundsdottir 198080% 85%

Observation• Differentiate between Resolving Curves, progressive
Bracing, serial casting• Is an attempt to stop progression of the curve but does
not improve the curve.
Early onset
Idiopathic Scoliosis
Treatment
Early Onset Scoliosis

Operative Treatment
• Convex Stapling Smith 1954
• Posterior Fusion Scott 1956
• Unilateral Growth Arrest Roaf 1963
• Concave Costoplasty Piggott 1971
• Convex Epiphysiodesis Roaf 1977
• Segmental Instrumentation Luque 1980
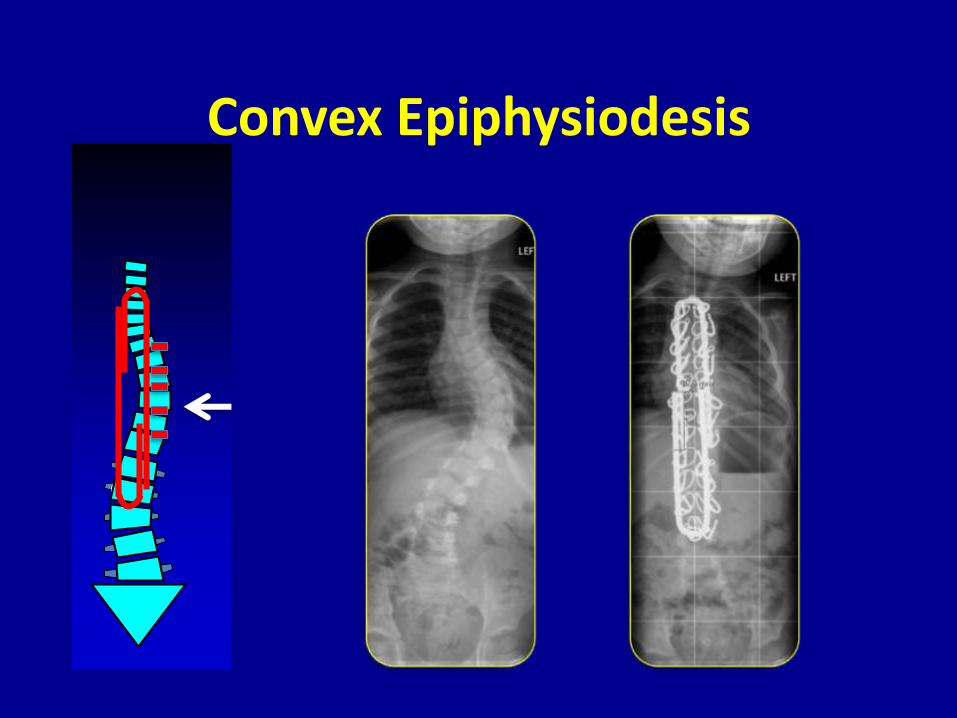
Convex Epiphysiodesis

Early Onset Scoliosis
Convex Epiphysiodesis & Luque trolley

46.5mm27.3mm
Age at 3 yrs Age at 9 yrsAge 3
Spinal Growth 2 cm
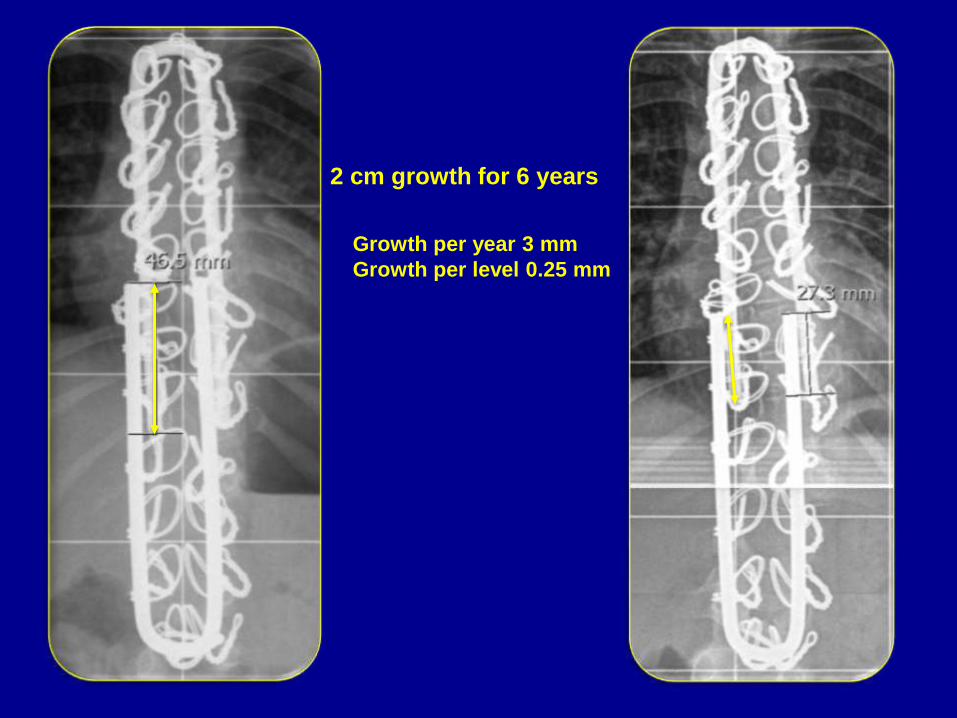
2 cm growth for 6 years
27.3mm
46.5mmGrowth per year 3 mm
Growth per level 0.25 mm

Conclusion
• It appears that convex epiphysiodesis has
a tethering effect on growth phenomenon
and therefore should be avoided when
growing constructs are used.
Surgery
progressive curves (Growing construct)
Spinal fusion is not an option, because the thoracic height
would cease to develop and lung development would be
restricted
Early onset
Idiopathic Scoliosis
Treatment
Early Onset Scoliosis
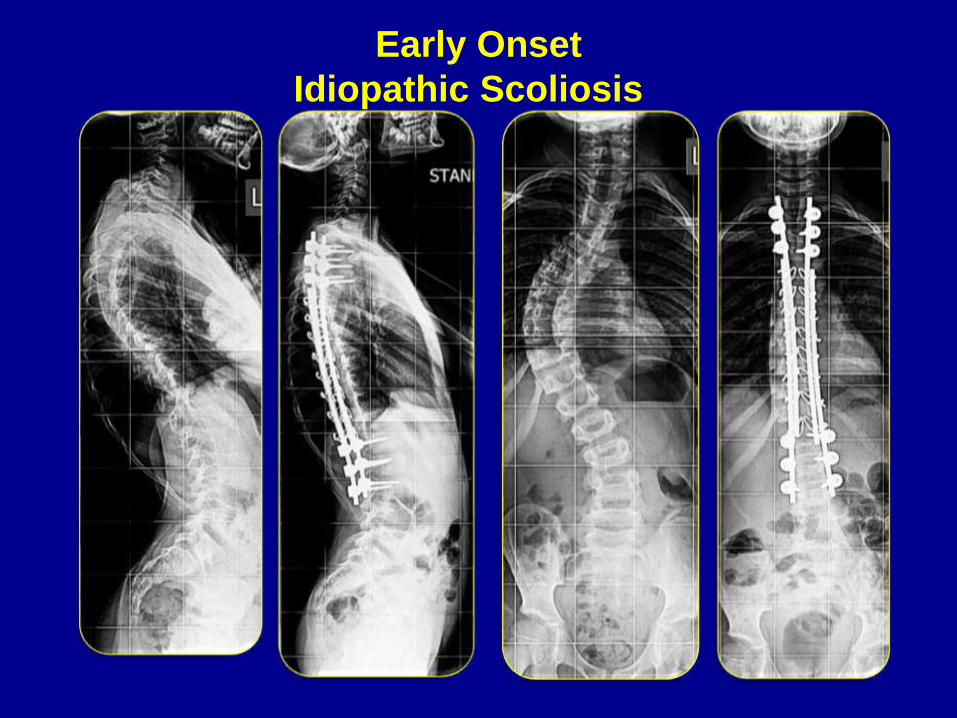
Consequences of Premature Spinal Fusion in a Case of Early Onset Scoliosis
Centre for Spinal Studies and Surgery Nottingham
15 year old female
4 months Serial Casting
3 years Uninstrumented
Convex Epiphysiodesis
7 years Post Fusion T3-L3
Residual spinal deformity
Back pain & costo-pelvic impingement
Breathlessness & difficulty of ambulation
Disproportionately small thorax
FVC 17% of predicted value
Centre for Spinal Studies and Surgery Nottingham
Main Complaints & Clinical Examination

Centre for Spinal Studies and Surgery Nottingham
Casting
Failed to control progression of the deformity
Premature fusion
Resulted in thoracic & respiratory insufficiency
Surgical options now
Too late for surgery to effect respiratory function?
Will respiratory function permit further surgery?
Outcome is premature death
• A
• SSSurgi Centre for Spinal Studies and Surgery Nottingham
What to do next, if anything?

Early Onset Scoliosis
Double Growing Rod Construct
VEPTERThoracic insufficiency syndrome , cog chest
Wall deformities
ShillaConstruct
Hybrid Construct
H Bar Construct
Growing Rod Constructs
Vertical ExpandableProsthetic Titanium Rib
Distraction Growth Guided
Early Onset
Idiopathic Scoliosis

Early Onset
Idiopathic Scoliosis

Early Onset
Idiopathic Scoliosis

Early Onset
Idiopathic Scoliosis

Early Onset
Neuromuscular Scoliosis
Neuromuscular
Spinal deformity develops in majority of the
Patients with neuromuscular disease
Deformity Early in life
Progression Common

Classification (SRS)EONMS
Upper Motor Neuron
Cerebral Palsy
Syringomyelia
Spinal Cord Trauma
Spinal Cord Tumour
Spinocerebellar Degeneration
Neuropathic
CP
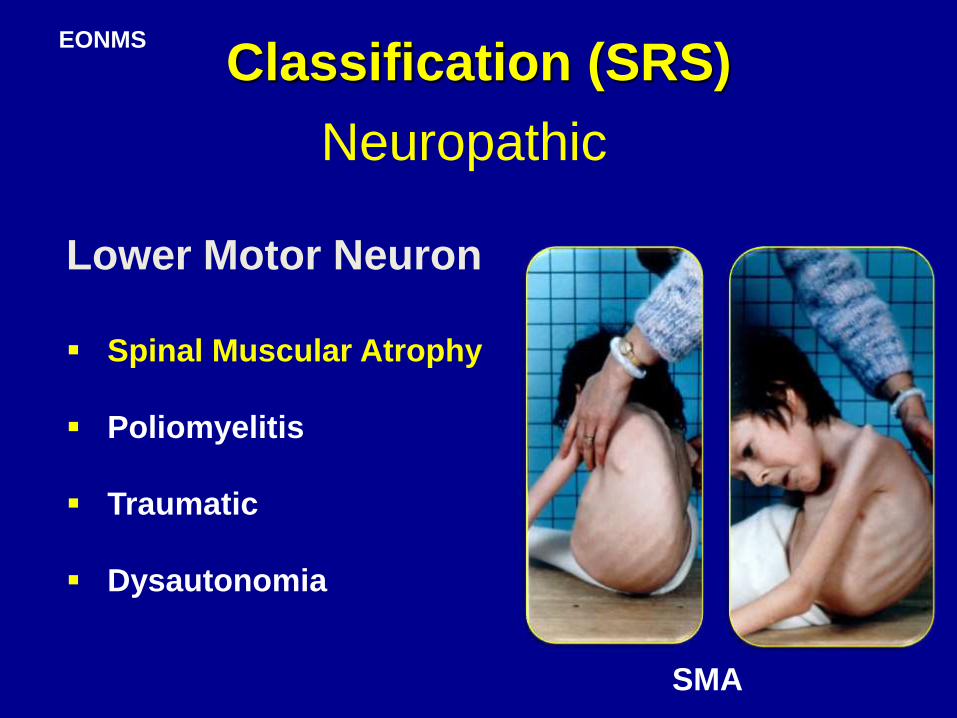
Classification (SRS)EONMS
Neuropathic
Lower Motor Neuron
Spinal Muscular Atrophy
Poliomyelitis
Traumatic
Dysautonomia
SMA
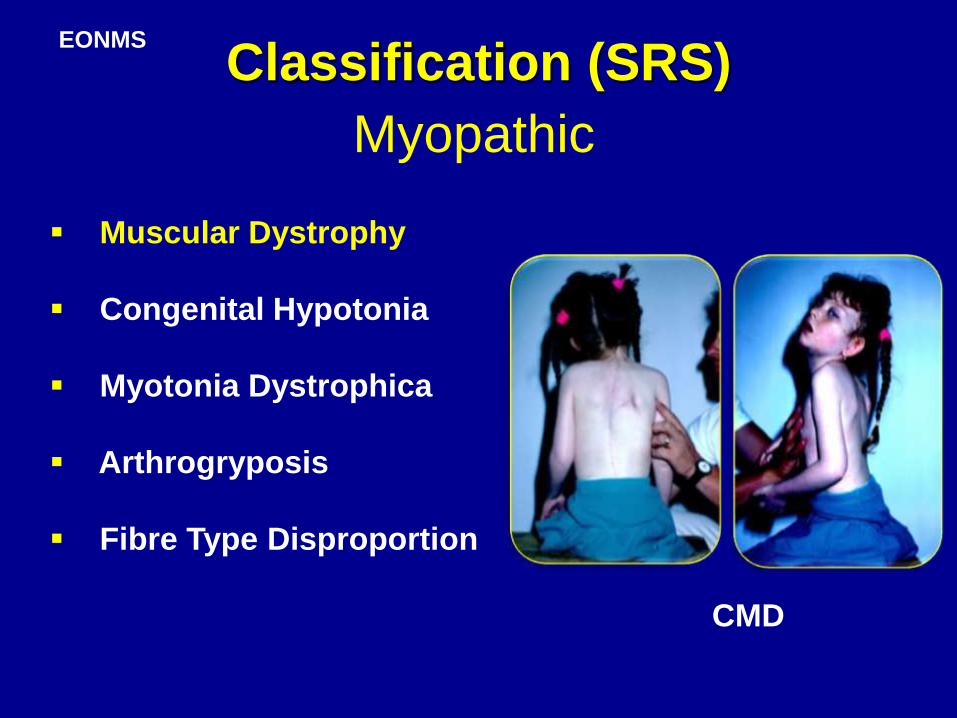
Classification (SRS)EONMS
Myopathic
Muscular Dystrophy
Congenital Hypotonia
Myotonia Dystrophica
Arthrogryposis
Fibre Type Disproportion
CMD
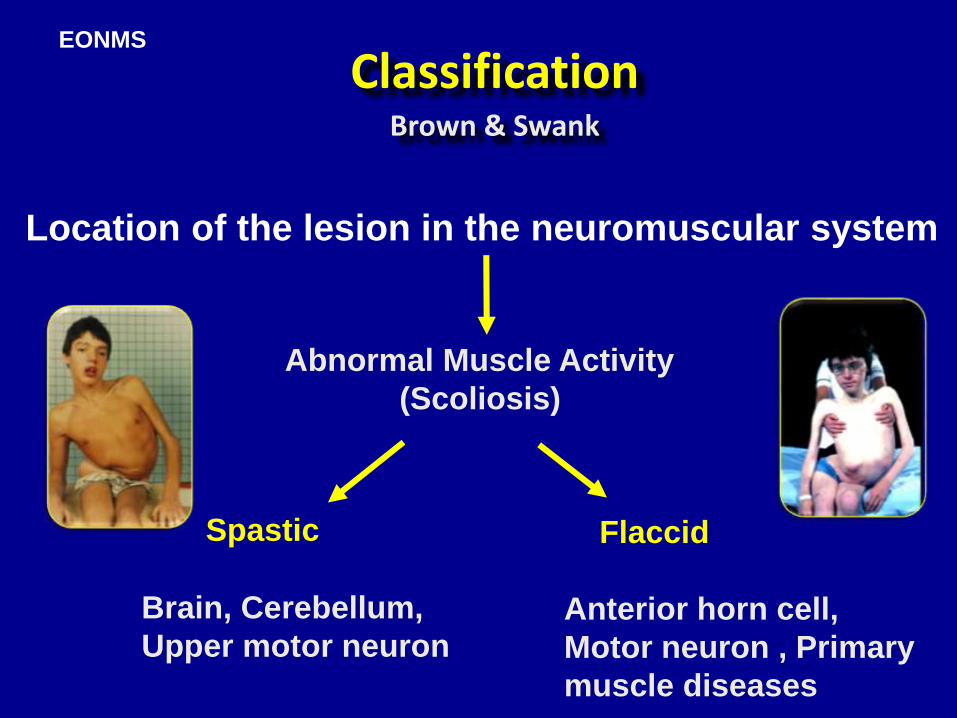
ClassificationBrown & Swank
Location of the lesion in the neuromuscular system
Abnormal Muscle Activity
(Scoliosis)
Spastic
Brain, Cerebellum,
Upper motor neuron
Flaccid
Anterior horn cell,
Motor neuron , Primary
muscle diseases
EONMS
General PrinciplesNeuromuscular
Progression
Pulmonary dysfunction
Cardiomyopathy
Urinary tract disease
Pressure sore
Hip dislocation
Patients with neuromuscular scoliosis present
with significantly different and more complicated
problems than those with idiopathic scoliosis
Neuromuscular
Osteoporosis
External support
Post-operative ventilatory support
Post-operative management
Blood loss
The management of these patients by surgical
means may be associated with much greater risk
Surgical Risks
Neuromuscular
Correction of the spinal deformity
Maintain the correction during the growth period
Allow spinal growth and lung development
Prevent progressive deterioration of P.F.
Avoid the need for definitive fusion at an early age
Goals of Surgery

Neuromuscular
Observation
Orthosis
Operation
The modalities of treatment in neuromuscular
scoliosis are similar to those of idiopathic
scoliosis
Treatment
Neuromuscular
Attempts at prophylactic or early bracing
have not prevented curve development and
progression.
An immediate effect of this will be to cause
difficulty breathing and restrict growth
of the chest wall in the longer term.
Orthosis & Seating Systems
Arterial and central lines
Urinary catheter
Temperature probe
Blood warmer
Heating blanket
Controlled hypotension
Cell saver
Spinal cord monitoring
Experienced anaesthetic input is essential in
major spinal surgery
Surgery
Neuromuscular
Pre-op Assessment
Chest Physician
Neurologist
Anaesthetist
Physiotherapist
Spinal Surgeon
Multidisciplinary review
Early Onset
Neuromuscular Scoliosis

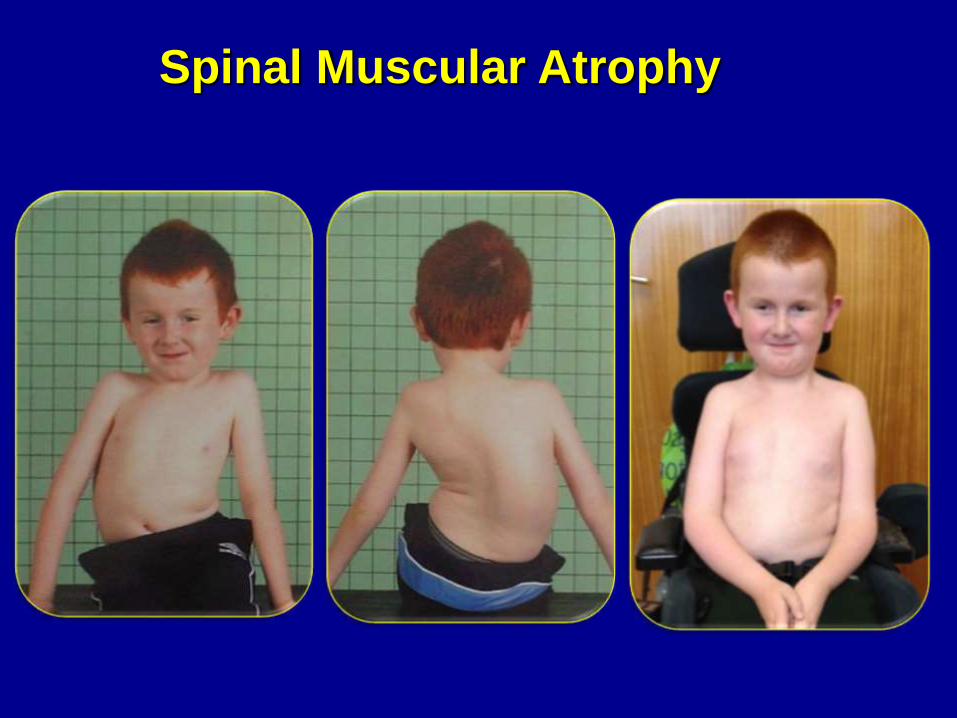
Spinal Muscular Atrophy
Autosomal recessive
Degeneration of anterior horn cells
Single gene responsible (chromosome 5)
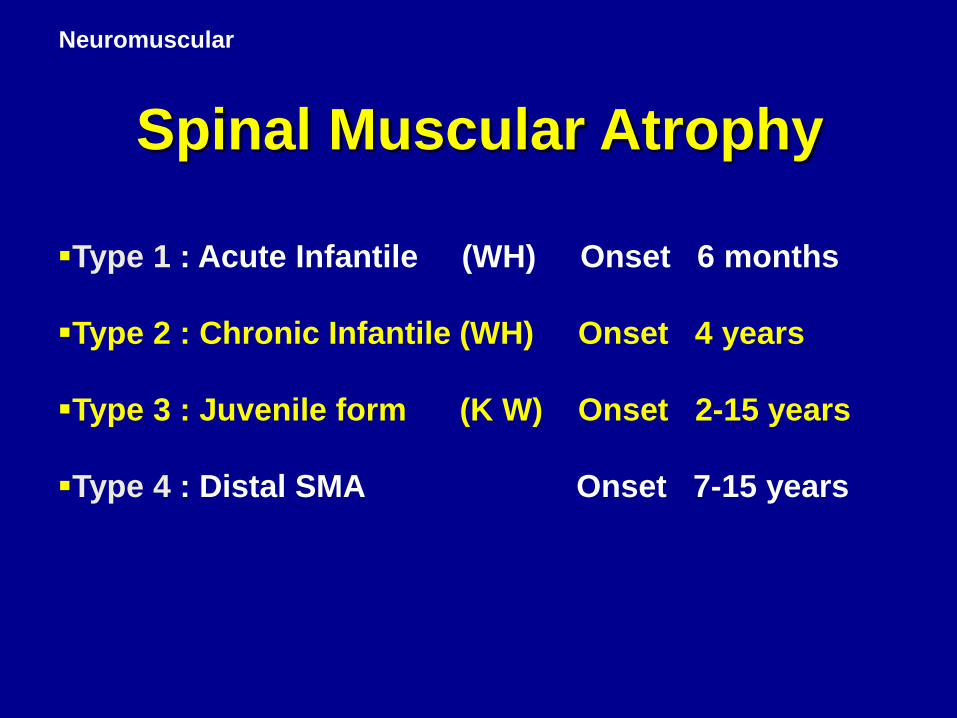
Scoliosis is present in more than 70% of
patients with SMA. Those with type 2 and 3
are the most common group presenting to
spinal surgeons and often present at a
young age.
Neuromuscular
Type 1 : Acute Infantile (WH) Onset 6 months
Type 2 : Chronic Infantile (WH) Onset 4 years
Type 3 : Juvenile form (K W) Onset 2-15 years
Type 4 : Distal SMA Onset 7-15 years
Spinal Muscular Atrophy

Various surgical techniques have been employed
to treat EONMS
Limitations :
Lack of segmental control
Loss of sagittal balance
Multiple surgeries
High rate of complications
EARLY ONSET NEUROMUSCULAR SCOLIOSIS
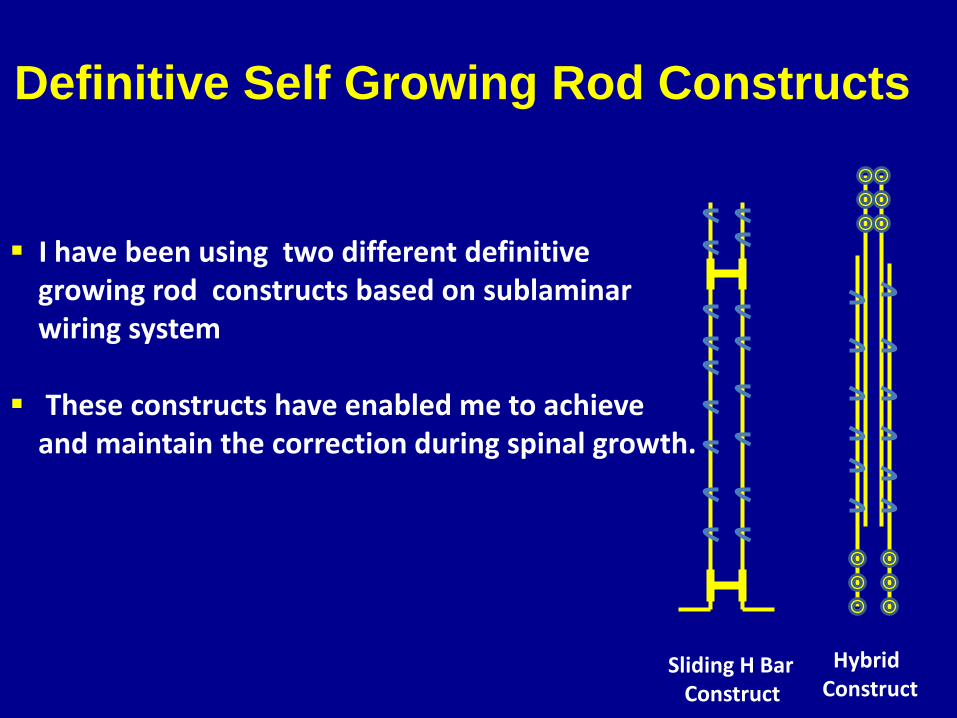
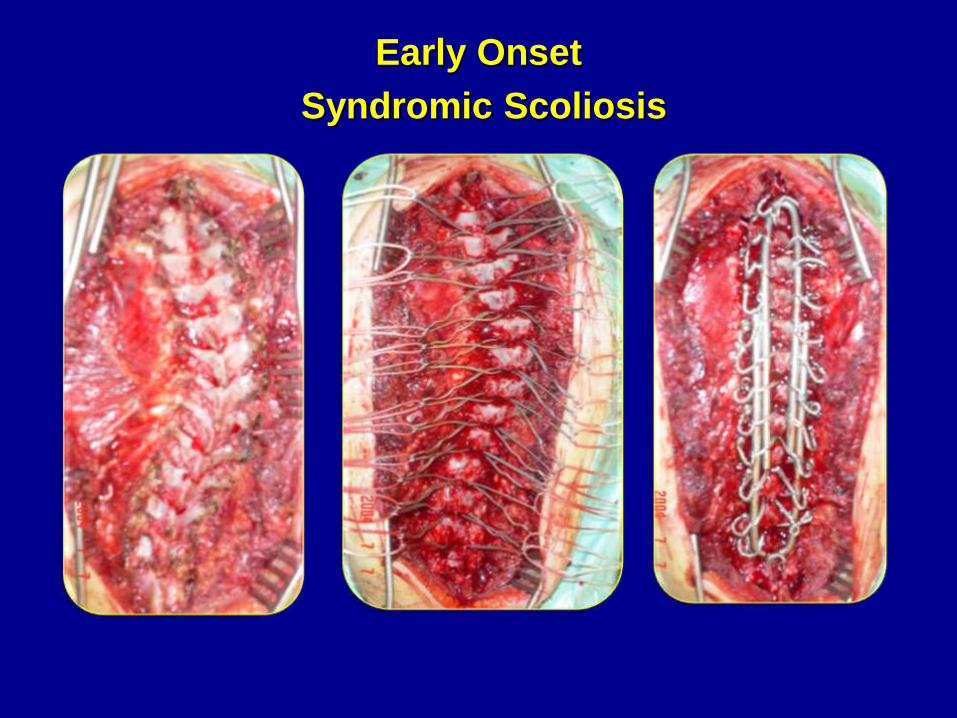
I have been using two different definitivegrowing rod constructs based on sublaminarwiring system
These constructs have enabled me to achieveand maintain the correction during spinal growth.
Sliding H Bar Construct
Hybrid Construct
Definitive Self Growing Rod Constructs

Screw + Wire Construct
Sliding H Bar Construct
Self Growing Rod Constructs

Neuromuscular
Segmental Spinal Instrumentation using short closed wire loops
H Mehdian, Clinical Orthopaedics, 1989, 247
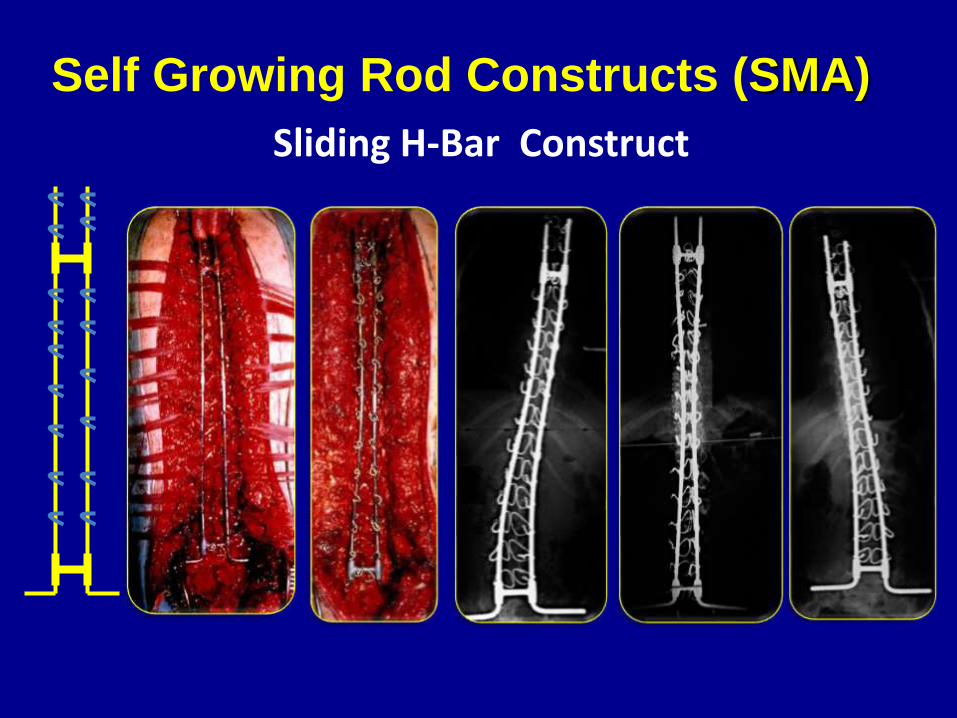
Sliding H-Bar Construct
Self Growing Rod Constructs (SMA)
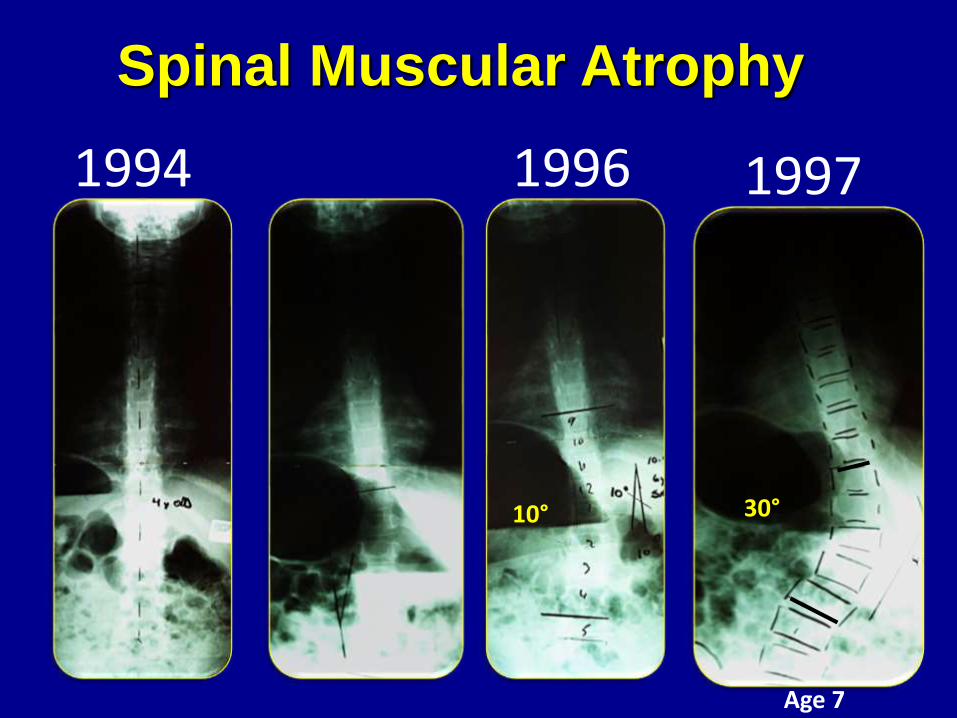
1994
Spinal Muscular Atrophy
1996 1997
30°10°
Age 7
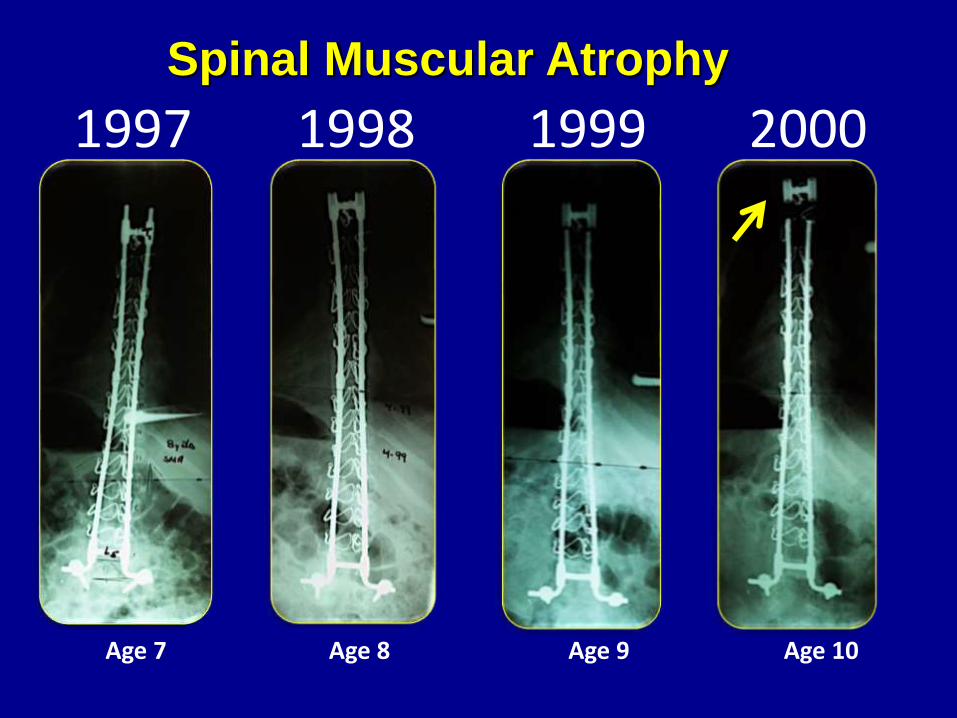
19981997 1999 2000
Age 7 Age 9Age 8 Age 10
Spinal Muscular Atrophy
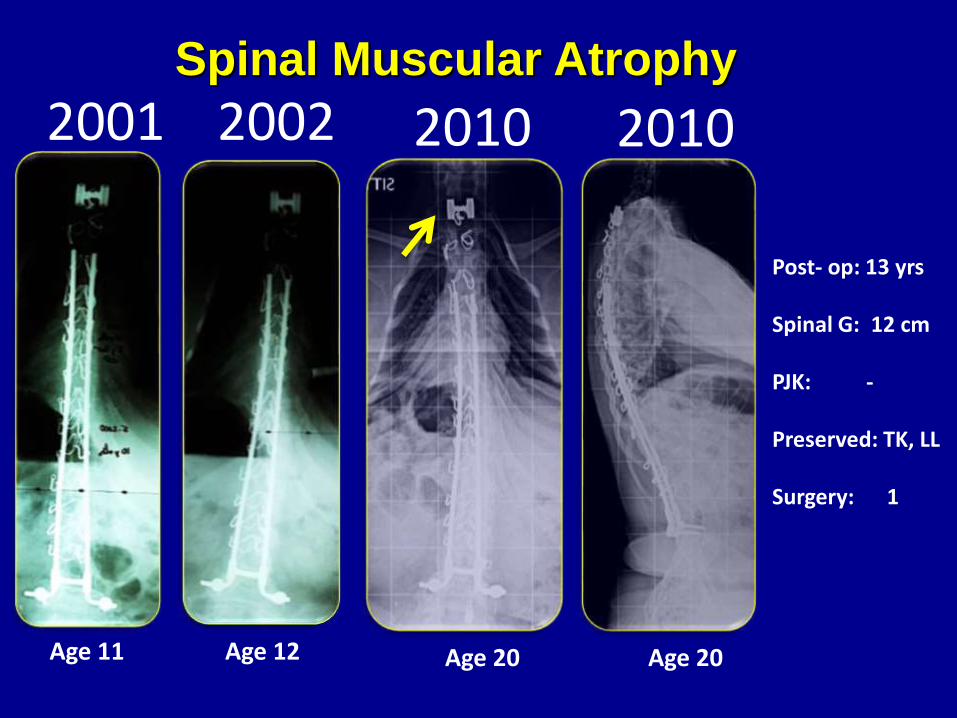
2001 2002 2010 2010
Age 11 Age 20Age 12 Age 20
Post- op: 13 yrs
Spinal G: 12 cm
PJK: -
Preserved: TK, LL
Surgery: 1
Spinal Muscular Atrophy

19981997 1999 2000 2001 2002 2010 2010
Spinal growth ( 12cm)
Age 7 Age 8 Age 9 Age 10 Age 11 Age 12 Age 20 Age 20
Spinal Muscular Atrophy
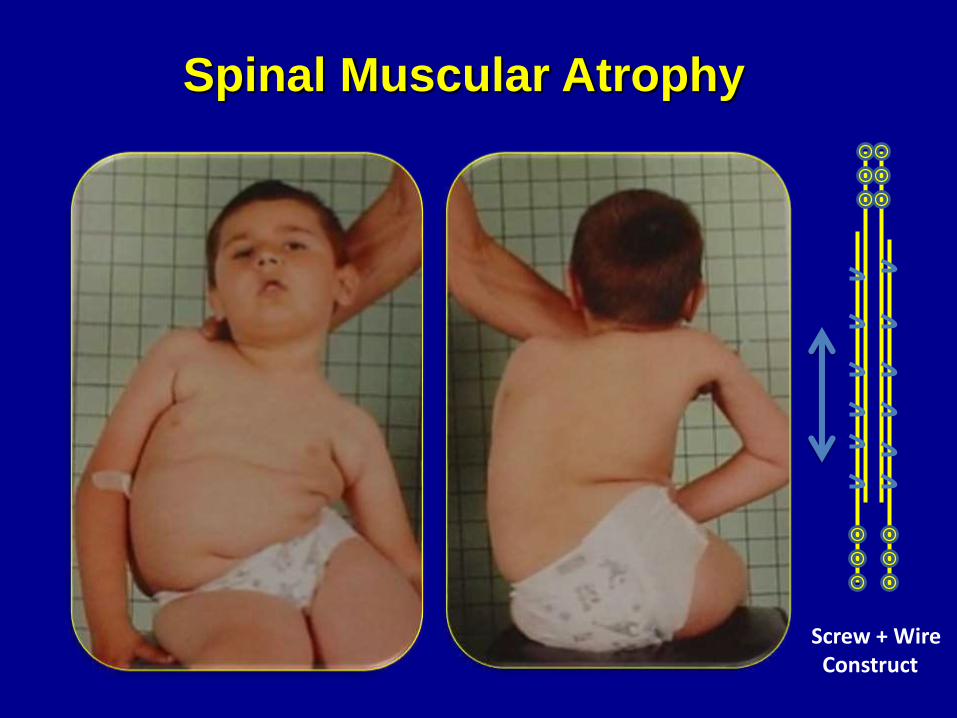
Screw + Wire Construct
Spinal Muscular Atrophy
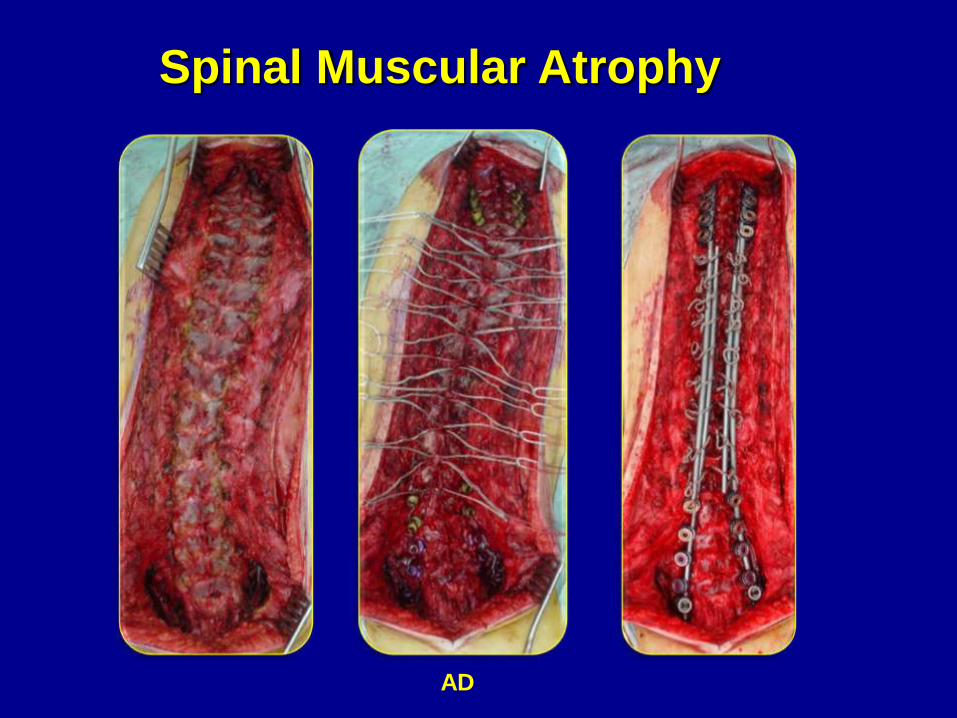
AD
Spinal Muscular Atrophy

90˚ 80˚
A D
Spinal Muscular Atrophy
Spinal Muscular Atrophy
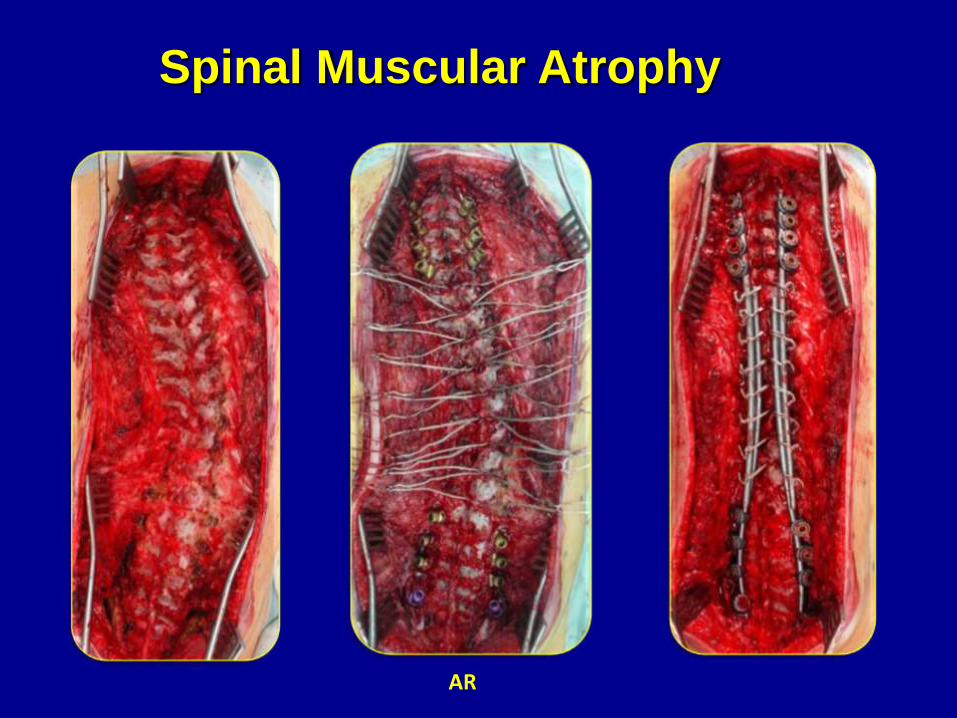
AR
Spinal Muscular Atrophy
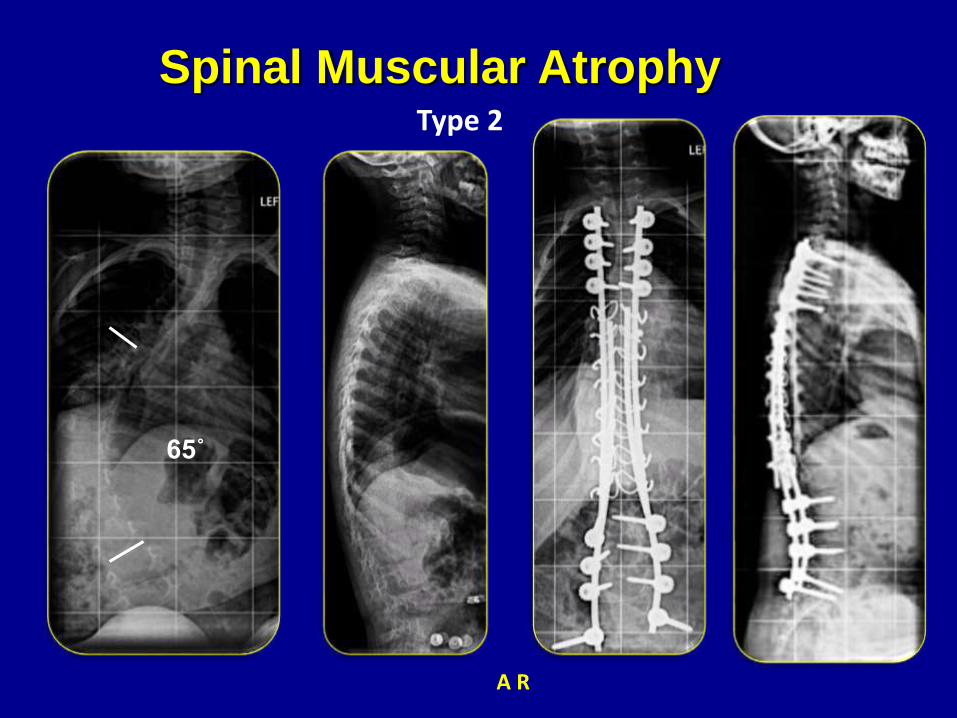
65˚
Type 2
A R
Spinal Muscular Atrophy

07.10.2009
18.3 mm
19.03.2012
44.7 mm
26.4 mm 2½ years
Spinal Growth

TC
Congenital Hypotonia

T C
Congenital Hypotonia
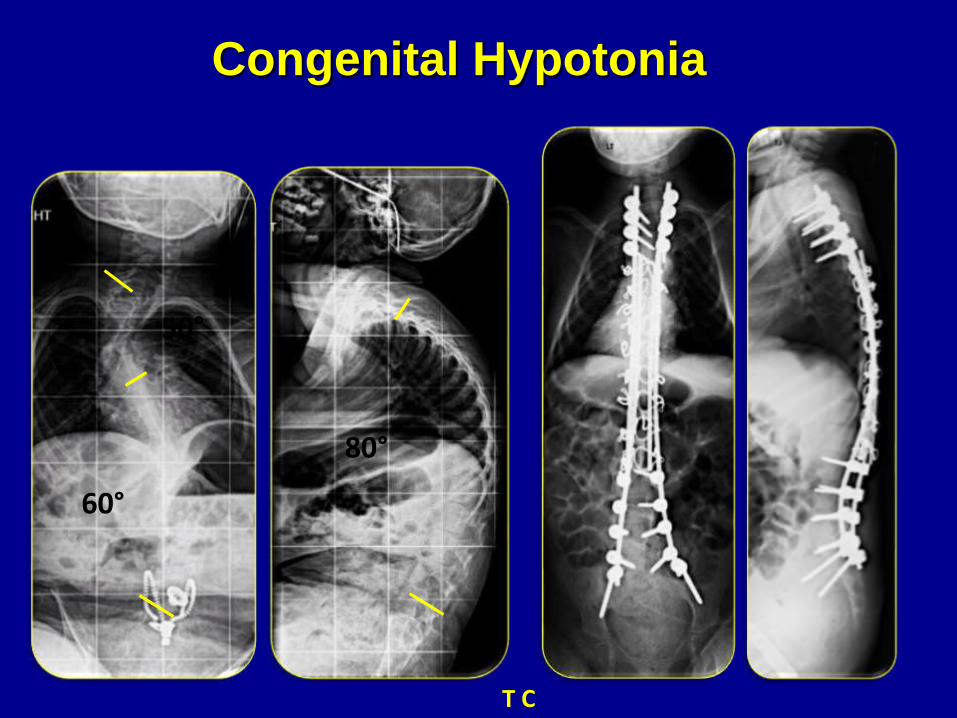
50°
60°
80°
T C
Congenital Hypotonia

A & S B
Congenital Muscular dystrophy

AB
Congenital Muscular dystrophy
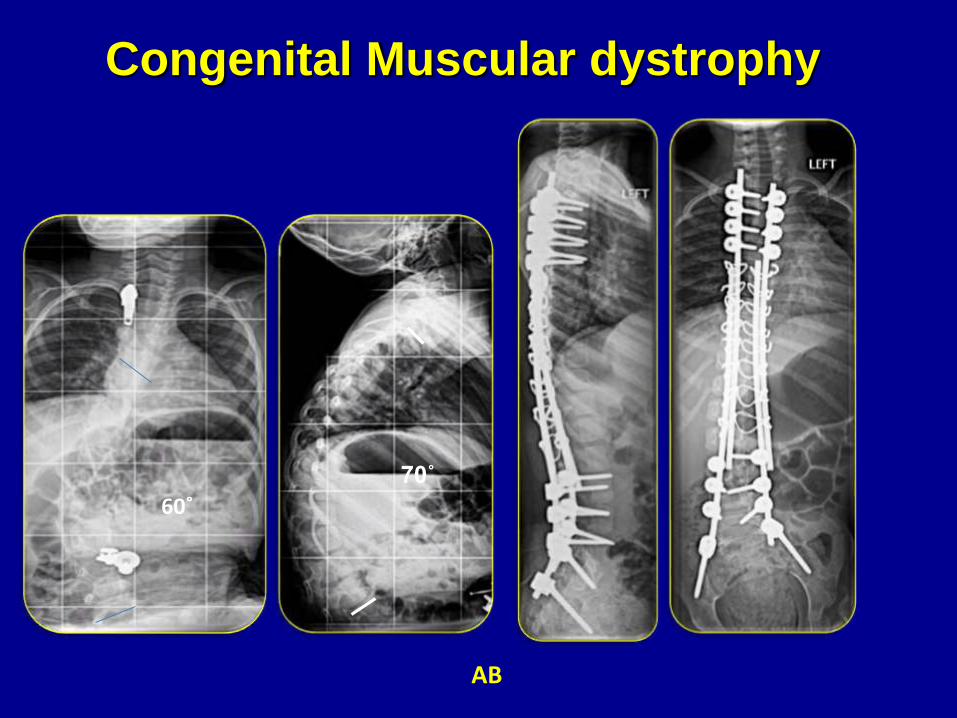
AB
70˚
60˚
Congenital Muscular dystrophy

SB
Congenital Muscular dystrophy
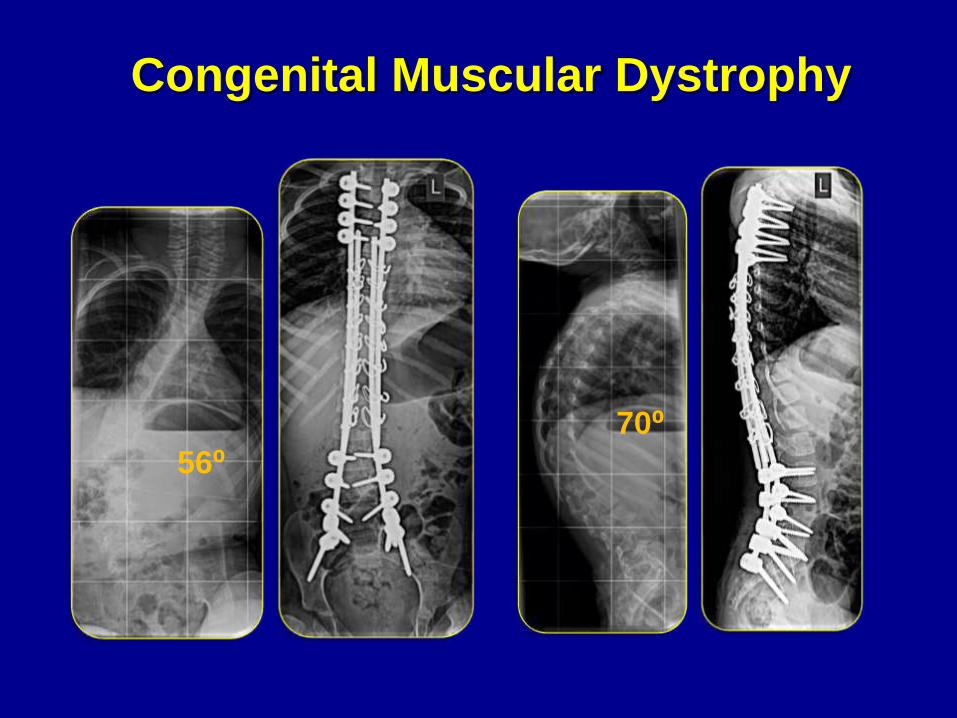
56⁰70⁰
Congenital Muscular Dystrophy
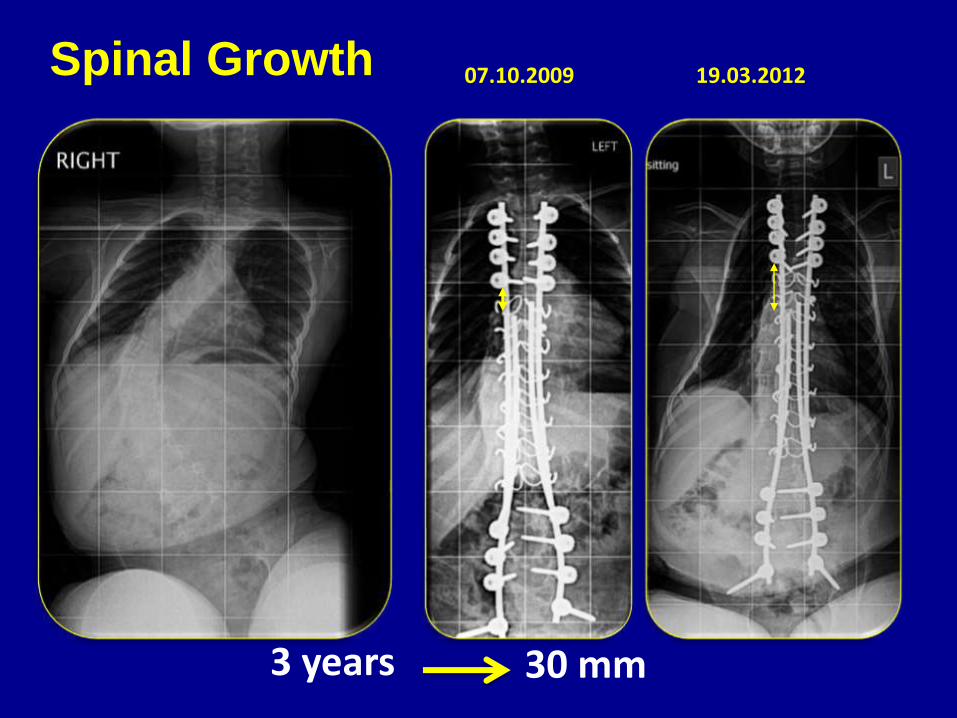
07.10.2009 19.03.2012Spinal Growth
30 mm 3 years

07.10.2009 15.09.2012
Spinal Growth
30 mm 3 years
22mm 52mm

4 Years 4 cm Growth

29.09.2008 20.01.2014
4 Years and 8 months 5 cm Growth
Definitive growing construct appears to be more
advantageous over other systems in patients with
early onset neuromuscular scoliosis, it eliminates the
need for further surgeries
The ideal design of implants for the treatment of
patients with EOS should have the following
characteristics:
Eliminates the need for recurrent lengthening
Provides good fixation
Maintains sagittal curvature of the spine
Conclusion

6th International Congress on
Early Onset Scoliosis & Growing Spine
November 15-16, 2012- Dublin, Ireland
Best Paper



Early Onset
Congenital Scoliosis
The spinal column develop at the same time as several
other major organ systems such as the bladder, kidneys
and heart.

Cong Scoliosis
Classification
Centre for Spinal Studies and Surgery Nottingham
Based on the embryological development
of the spine
Defects of Formation
Defects of Segmentation
Mixed

• MRI shows abnormalities in 26%
• Syrinx
• Chiari Malformation
• Tether cord
• Diastomatomyelia
• Single kidny
Imaging / Associations
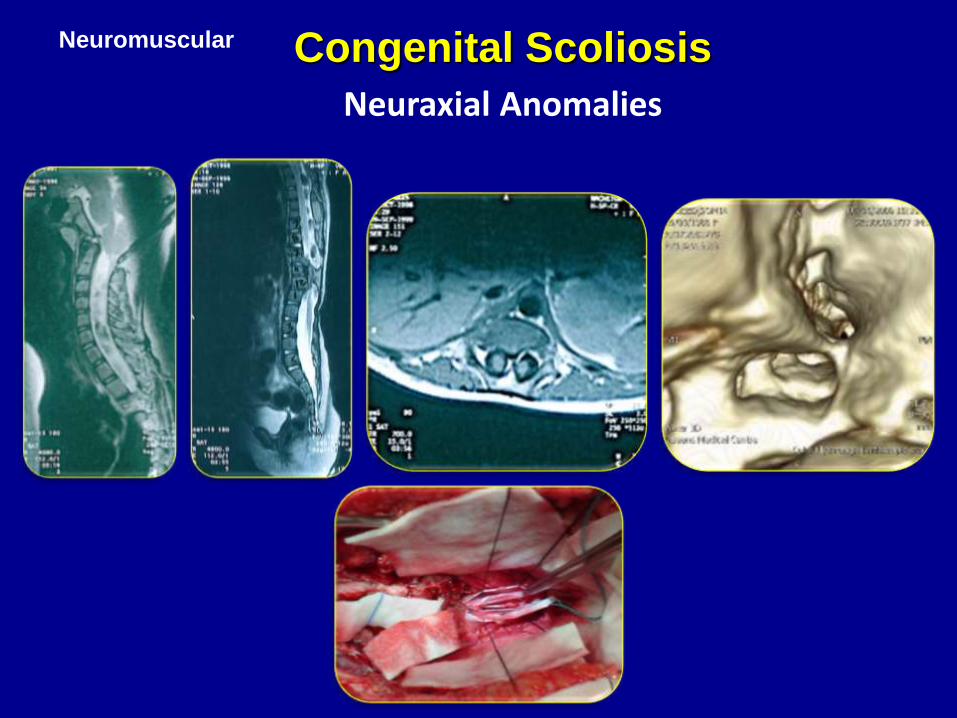
Neuromuscular Congenital Scoliosis
Neuraxial Anomalies
Bracing
• Proven little value for congenital curves
Indication for Surgery
• Unacceptable deformity
• Bar + contralateral hemivertebra
• Progression >10° in one year

Surgical Options
• Posterior fusion
• Anterior and posterior fusion
• Convex hemiepiphyseodesis
• Posterior vertebral resection
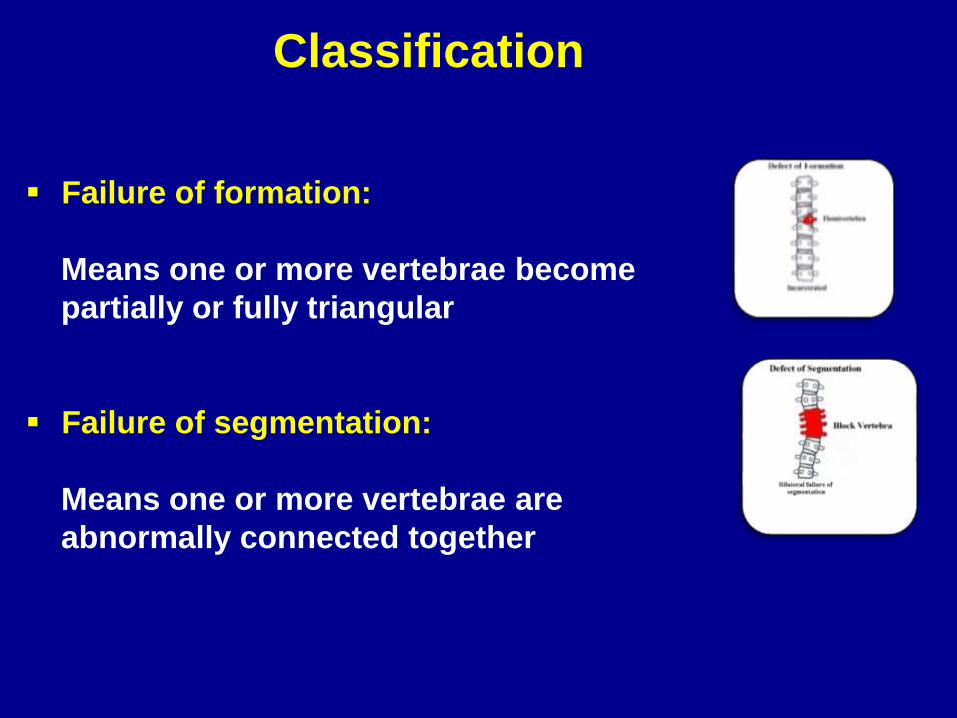
Classification
Failure of formation:
Means one or more vertebrae become
partially or fully triangular
Failure of segmentation:
Means one or more vertebrae are
abnormally connected together

Failure of formation
Fully SegmentedIncarceratedNonsegmented
Semi
Segmented
Wedge Vertebra

Failure of Segmentation
Bilateral Failure of
Segmentation
Unilateral Failure of
Segmentation,unsegmented bar
Unilateral Failure of
Segmentation, unsegmented
bar + contralateral hemi
vertebra

Cong Scoliosis
Centre for Spinal Studies and Surgery Nottingham
Defects of Formation
A lateral defect of vertebral formation can vary from
mild wedging to the complete absence of half of the
vertebra (Hemivertebra)
A hemivertebra is one of the most common causes
of congenital scoliosis
Hemivetebra consists of half of the vertebral body, a
single pedicle, and hemi-lamina

Cong Scoliosis
Centre for Spinal Studies and Surgery Nottingham
Defects of Formation
Hemivertebra
Four different types of hemivertebrae
Fully Segmented Most common
Semi segmented Less common
Non-segmented Least common
Incarcerated Least common

Cong Scoliosis
Centre for Spinal Studies and Surgery Nottingham
Defects of Formation
Fully Segmented Hemivertebra
At the thoracolumbar region the deformity
can exceed 45⁰ at skeletal maturity
Cosmetic deformity is moderate
At the lumbosacral junction, cosmetic deformity
is major

Cong Scoliosis
Centre for Spinal Studies and Surgery Nottingham
Defects of FormationFully Segmented Hemivertebra
Two fully segmented hemivertebrae on the
same side of the spine are less common
All exceed 50⁰ by 10 years of age
Without treatment these could reach 70⁰ byskeletal maturity
Two opposing fully segmented hemivertebraeare more common
Cong Scoliosis
Centre for Spinal Studies and Surgery Nottingham
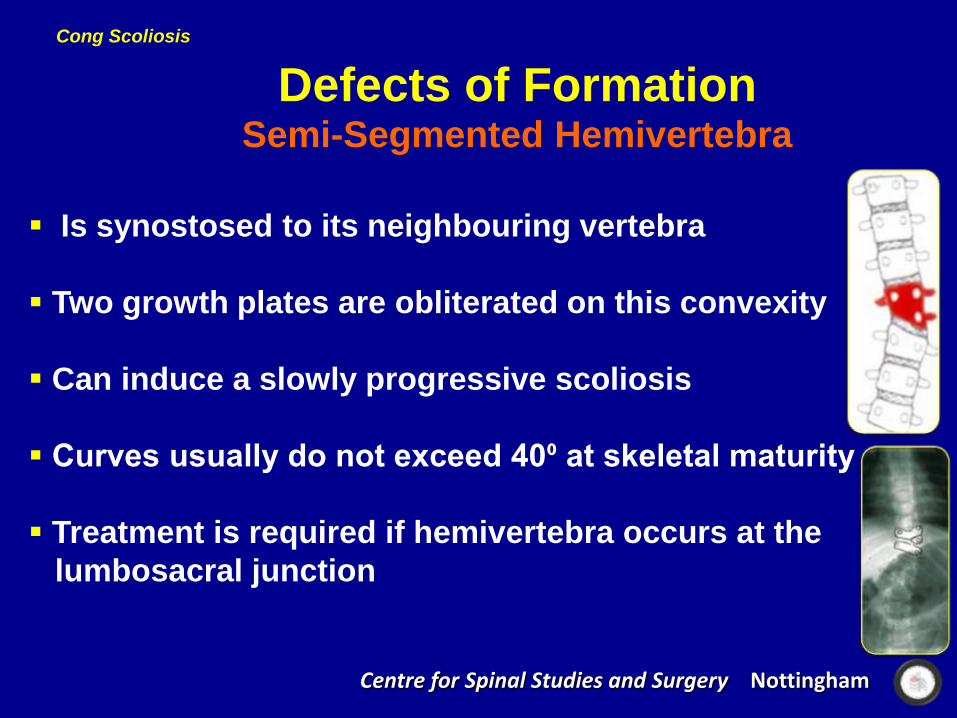
Defects of FormationSemi-Segmented Hemivertebra
Is synostosed to its neighbouring vertebra
Two growth plates are obliterated on this convexity
Can induce a slowly progressive scoliosis
Curves usually do not exceed 40⁰ at skeletal maturity
Treatment is required if hemivertebra occurs at the
lumbosacral junction
Cong Scoliosis
Centre for Spinal Studies and Surgery Nottingham
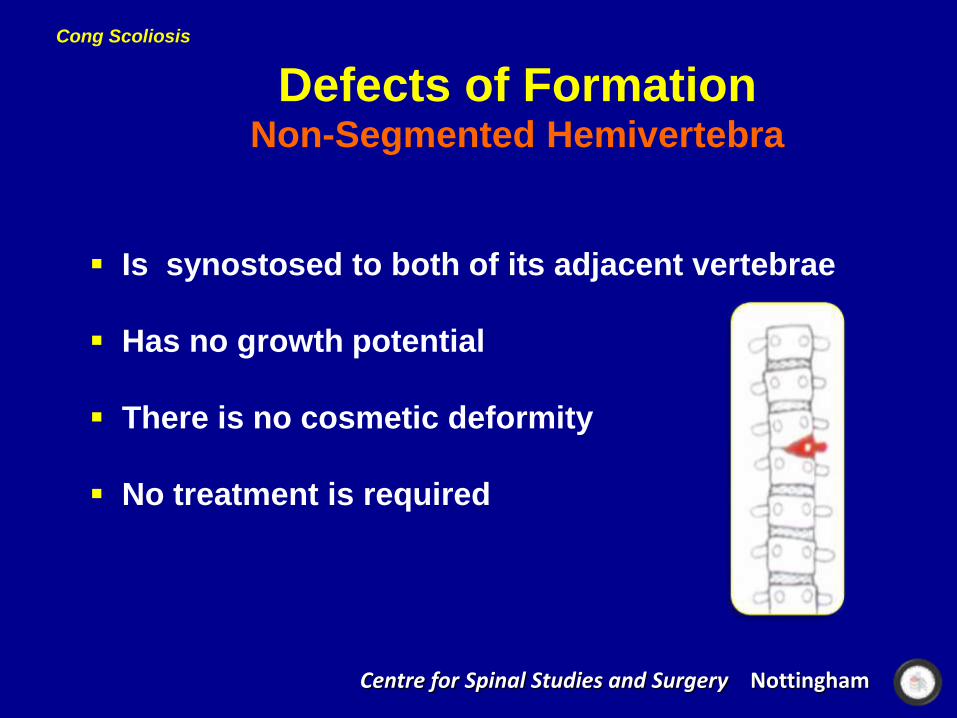
Defects of FormationNon-Segmented Hemivertebra
Is synostosed to both of its adjacent vertebrae
Has no growth potential
There is no cosmetic deformity
No treatment is required
Cong Scoliosis
Centre for Spinal Studies and Surgery Nottingham
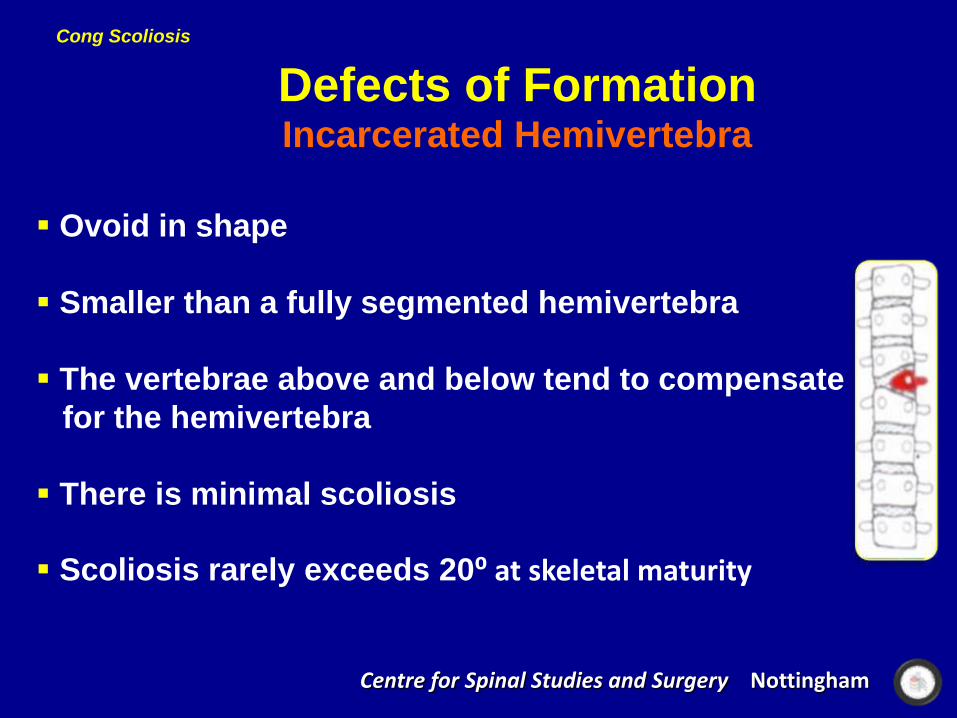
Defects of FormationIncarcerated Hemivertebra
Ovoid in shape
Smaller than a fully segmented hemivertebra
The vertebrae above and below tend to compensate
for the hemivertebra
There is minimal scoliosis
Scoliosis rarely exceeds 20⁰ at skeletal maturity

Cong Scoliosis
Centre for Spinal Studies and Surgery Nottingham
Defects of FormationWedge-vertebra
Rare cause of congenital scoliosis
Partial failure of a vertebra to form on one side
Scoliosis deteriorates relatively slowly
Surgical treatment may occasionally be required
Cong Scoliosis
Centre for Spinal Studies and Surgery Nottingham
Associated Deforming Features
Upper thoracic curve:
Significant cosmetic deformity
A 30⁰ curve upper limit of acceptability
Cong Scoliosis
Centre for Spinal Studies and Surgery Nottingham
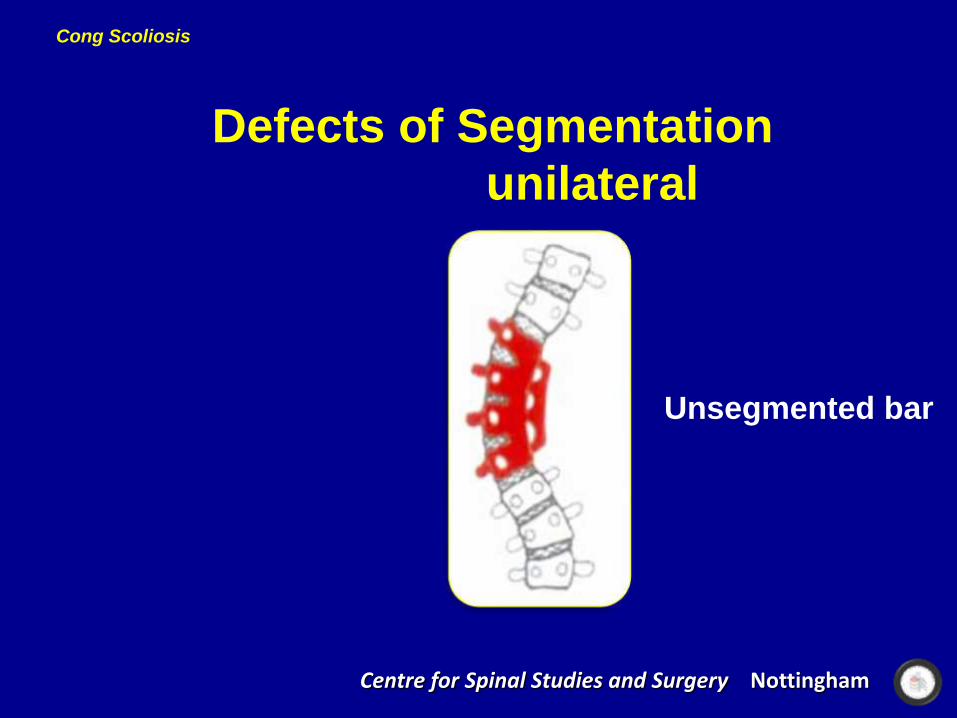
Defects of Segmentation
unilateral
Unsegmented bar

Cong Scoliosis
Defects of Segmentation
Centre for Spinal Studies and Surgery Nottingham
The unsegmented bar does not contain growth plates
Some degree of growth continues on the opposite side
Rib fusions are often seen adjacent to the unsegmented
bar
Unilateral unsegmented bar
Cong Scoliosis
Centre for Spinal Studies and Surgery Nottingham
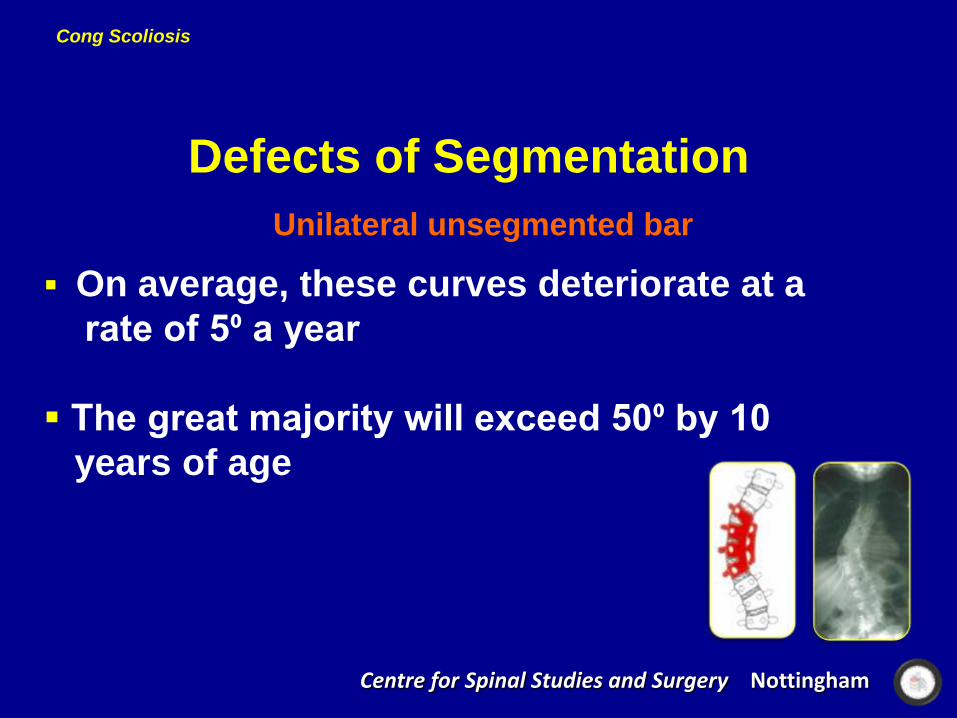
Defects of Segmentation
Unilateral unsegmented bar
On average, these curves deteriorate at a
rate of 5⁰ a year
The great majority will exceed 50⁰ by 10
years of age
Cong Scoliosis
Centre for Spinal Studies and Surgery Nottingham
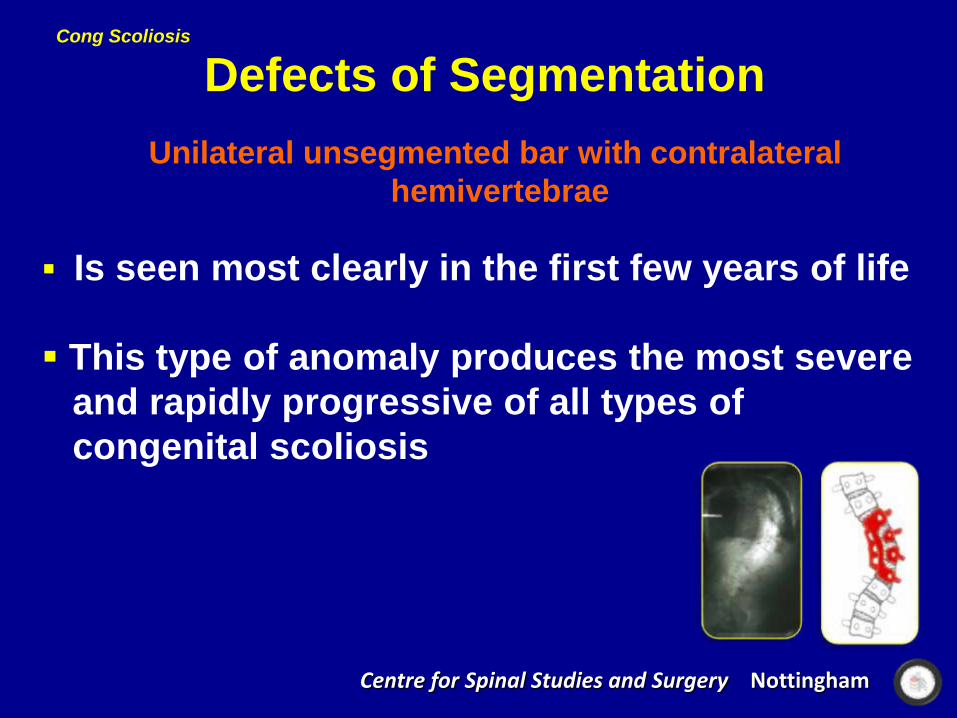
Defects of Segmentation
Unilateral unsegmented bar with contralateral
hemivertebrae
Is seen most clearly in the first few years of life
This type of anomaly produces the most severe
and rapidly progressive of all types of
congenital scoliosis

Cong Scoliosis
Centre for Spinal Studies and Surgery Nottingham
Defects of Segmentation
Unilateral unsegmented bar with contralateral
Hemivertebrae
On average, these curves deteriorate 6⁰ or
more a year
All exceed 50⁰ by 4 years of age
If untreated, at an early age can lead to
cor pulmonale
Cong Scoliosis
Centre for Spinal Studies and Surgery Nottingham
Treatment
Defects of Segmentation
Unilateral unsegemented bar with or without contralateral
hemivertebrae
Fusion should be performed as soon as the anomaly
is recognized
The best results are achieved when surgery is performed
before the age of 2 years

Cong Scoliosis
Centre for Spinal Studies and Surgery Nottingham
Defects of Segmentation
Bilateral
Block Vertebra

Congenital Kyphosis
• Type I: Failure of formation (hemivertebra)
• Rapidly progressive
• May produce paraplegia
• Type II: Failure of segmentation (bar)
• Less progressive
• Does not produce paraplegia

Congenital EO Scoliosis

Congenital Early Onset Scoliosis
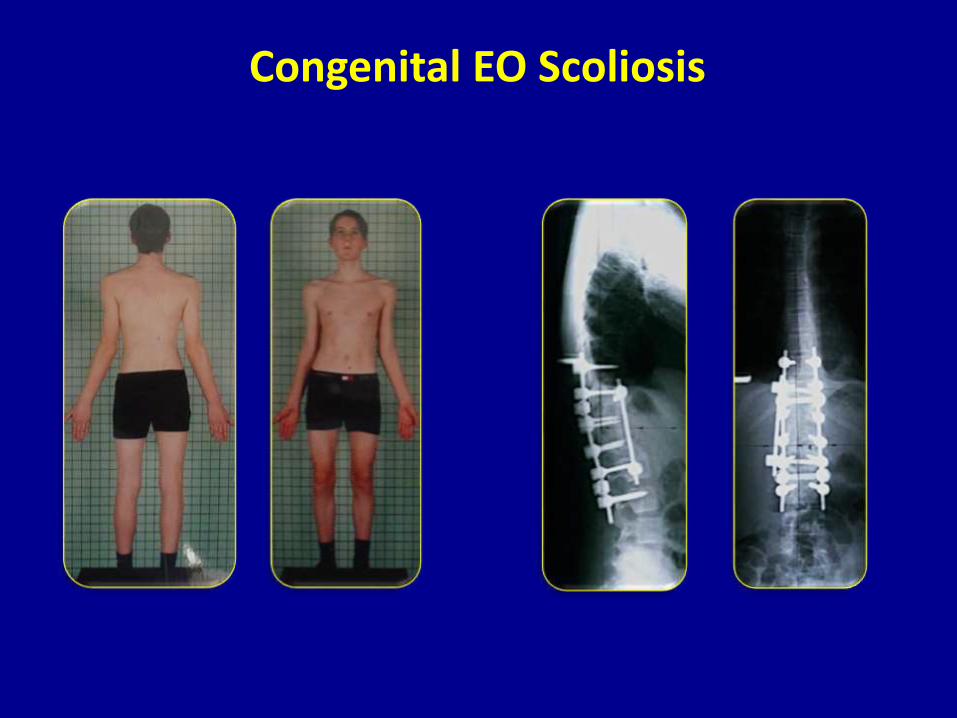
Congenital EO Scoliosis

Congenital Kyphosis
Prognosis
• Most patients have slight short stature
• 70% risk of progression
• Progression greatest after 10 years of age
• May cause cor pulmonale
• Congenital kyphosis may cause paralysis

Congenital Kyphosis

Neuromuscular
Management of Kyphosis (Kyphectomy)
Kyphectomy

Congenital Early onset Scoliosis
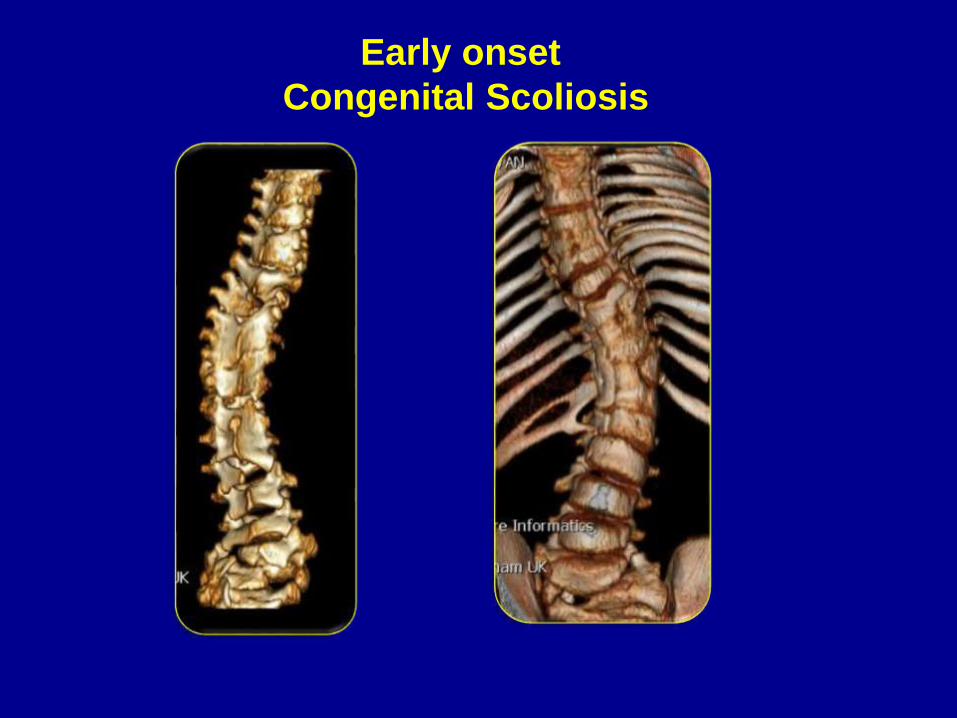
Early onset
Congenital Scoliosis
Spinal Growth
• Averages 0.07 cm/year per segment
• Anomalous segments will never have this
degree of growth
• Spinal growth is two thirds complete
by age 6

Early onset
Congenital Scoliosis

Early onset
Congenital Scoliosis


Rhys Hart, 12 y/o MK1738918
10 cm
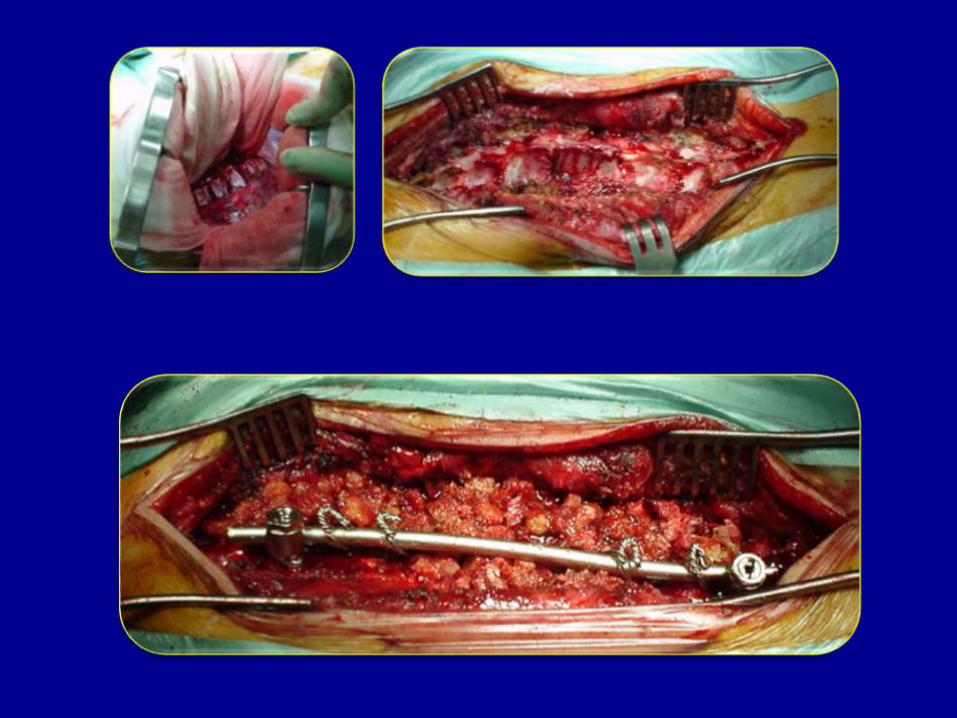
T11 PVCRT2–Ileum segmentalinstrumented fusion











120º
72º

The Segmental Self Growing Rod Construct
is a powerful, definitive technique for the
management of early onset scoliosis
Construct Advantages:
Excellent correction
Maintain the correction during growth period
PJK is prevented
Sagittal contour of the spine is well preserved
Maximum spinal growth and thoracic
development is achieved just with one surgery
Conclusion

Adolescent Idiopathic Scoliosis
Natural History
• Progression related to maturity and curve size
• Risk of progression increases strongly at in an
immature patients
• Curves> 45° should be considered for surgery
• Pulmonary compromise > 75° to 100°

Initial Evaluation
Whole Spine X-rays (curve measurement)
Regular outpatient review

Progression more than 5° in curves between
20°-25° in patients with ( Risser 0-3)
Brace treatment for curves > 40° to 45° has very
lower success rate
Brace Indications
Brace Types
• Thoracolumbosacral (TLSO) TLC
• Milwaukee Brace high thoracic curves
• Charleston Night Brace Single curves 25°

Preoperative assessment
MRI indicated if:
Left Lower thoracic curve
Significant back or neck pain
Neurological abnormality
Less than 10 years of age

Late Onset ScoliosisLenke Classification
The Lenke Classification is a complex, accurate and reproducible . It relies onmeasurements taken from standard x-rays
X-rays of the patient from the AP, LAT,and in bending positions are measuredand evaluated
Each scoliosis curve is then classified in three ways

Late Onset ScoliosisLenke Classification
Curve type (1-6) : proximal thoracic, main thoracic and
thoracolumbar/lumbar
Lumbar modifier (A, B, C) lumbar
modifier based on the distance of
the center of the lumbar spine to
the midline

Late Onset ScoliosisLenke Classification
Sagittal thoracic modifier (-, N, +)
Sagittal thoracic modifier based on the
amount of thoracic kyphosis
The most common type is a 1AN curve

Type 1 B,N ( Main Thoracic)
Seg Screw Fixation
68º
Type 1 B,N (Main Thoracic)
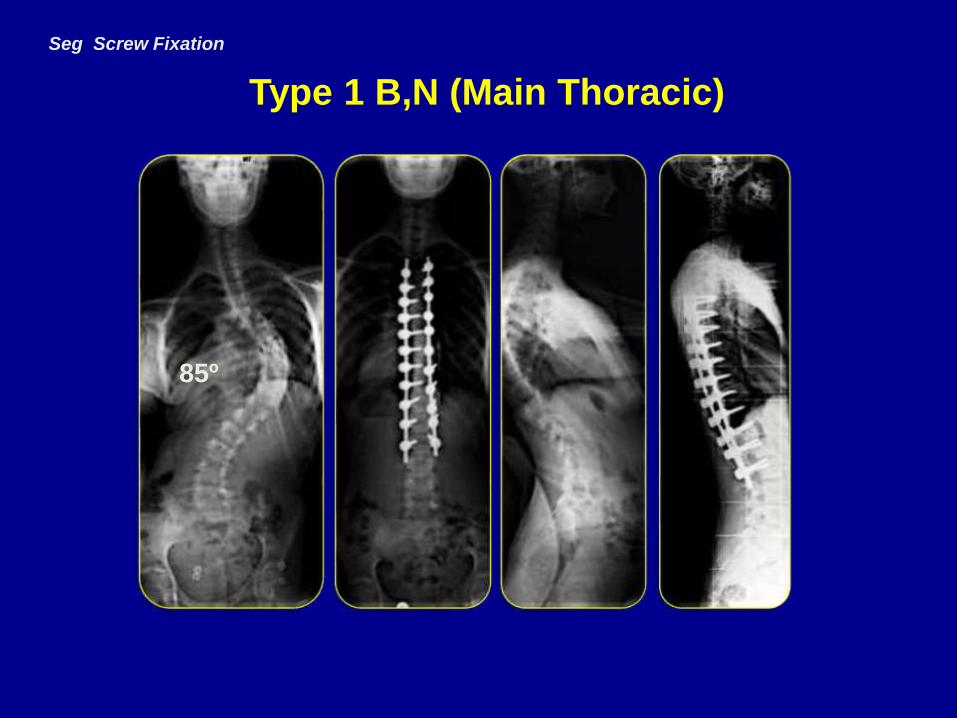
Seg Screw Fixation
85º

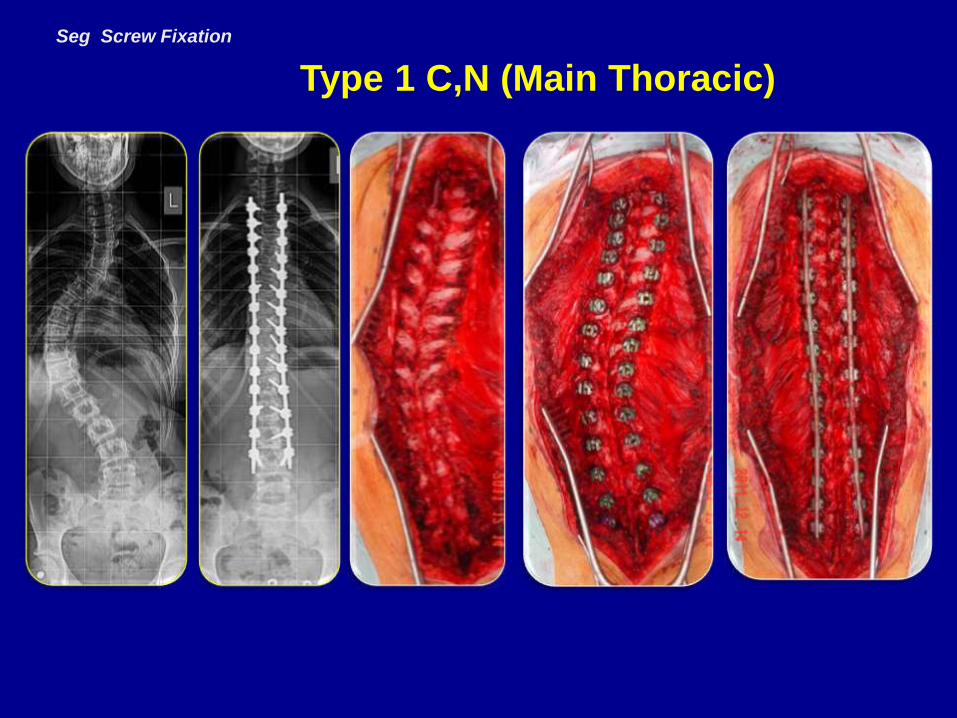
Type 1C,N (Main Thoracic )
Seg Screw Fixation
90º
60º
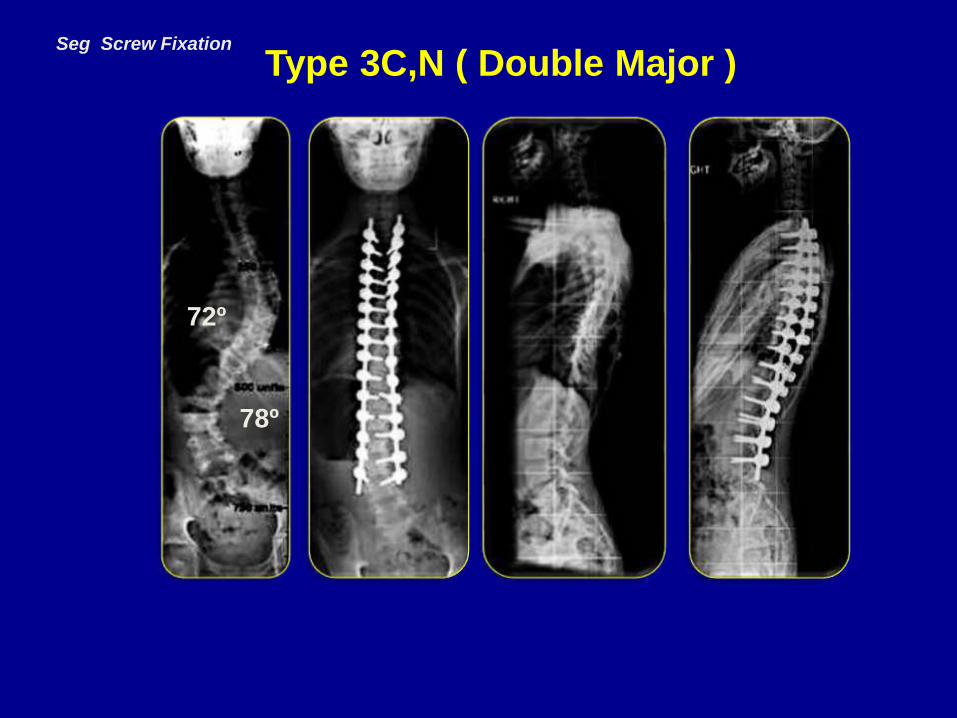
Type 3C,N ( Double Major )Seg Screw Fixation
78º
72º
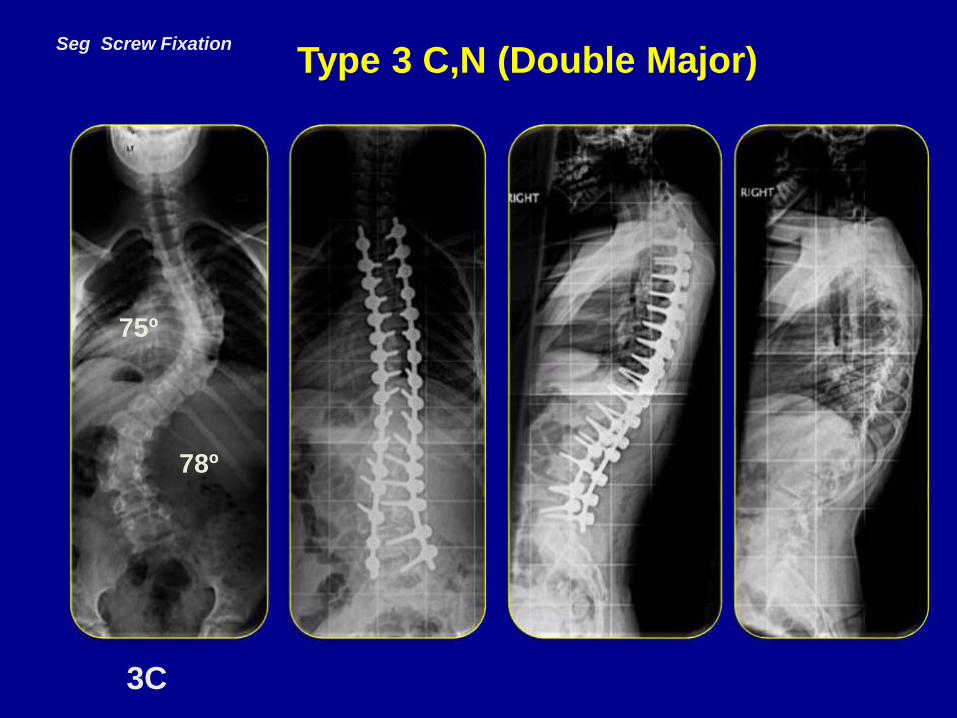
Type 3 C,N (Double Major)
3C
Seg Screw Fixation
78º
75º

Type 6C,N (Thoracolumbar)
Seg Screw Fixation
85º
75º

Image Free technique
Type 6C,N (Thoracolumbar)

Seg Screw Fixation Type 3C,N ( Double Major )
80º
78º
Seg Screw Fixation
Type 1 C,N (Main Thoracic)
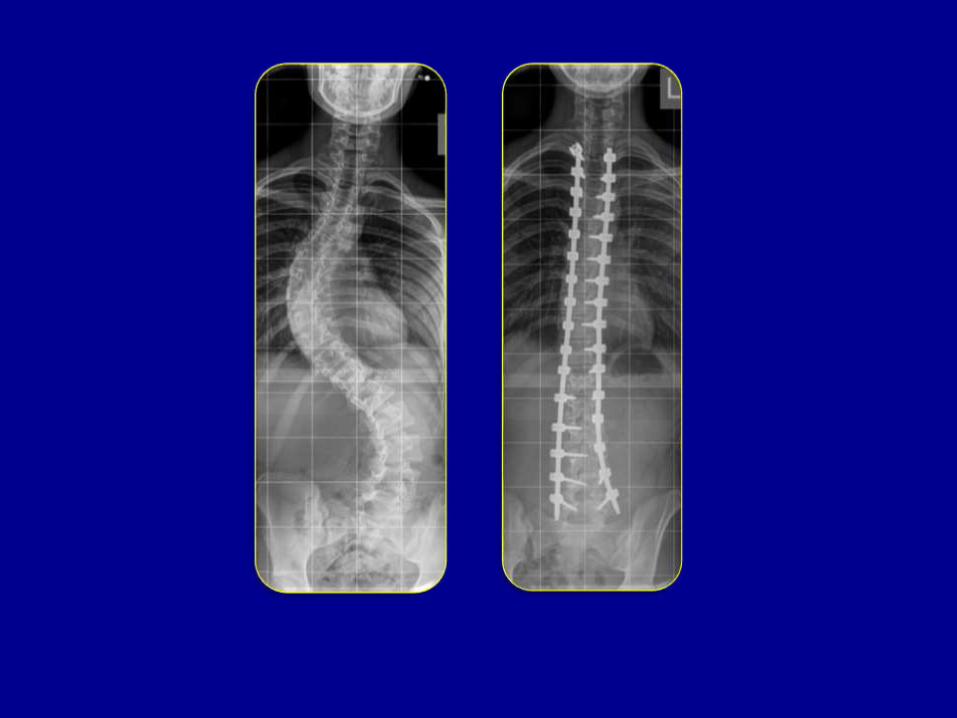



Seg Screw Fixation

Seg Screw Fixation

Seg Screw Fixation

Paediatric spinal deformity surgery should be
performed in a specialist centre where a high
volume of procedures are performed
Good medical support staff, including
experienced paediatric anaesthetists, are an
essential part of the team dealing with these
children with deformity
Conclusion
Centre for Spinal Studies and Surgery Nottingham

EOS TO REMAIN NORMAL
• Weight: 40 kg
• T1-T12= 22 cm
• VC: more than 50%

Early Onset
Syndromic Scoliosis
Prader willi Syndrome

Early Onset
Syndromic Scoliosis
Early Onset
Syndromic Scoliosis
Related Documents











