Early Mobilization of Patients in Critical Care Poramed Chayaratanasin, PhD, MD Rehabilitation Medicine Department, Faculty of Medicine Ramathibodi Hospital, Mahidol University

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Early Mobilization of Patients in Critical Care
Poramed Chayaratanasin, PhD, MD
Rehabilitation Medicine Department,
Faculty of Medicine Ramathibodi Hospital,
Mahidol University

Outline
• Immobilization syndrome
• Post ICU syndrome
• Benefit of early mobilization
• Safety
• How
• Barrier
• Assisting aid/ technology

Effects of immobilization on body systems
• Musculoskeletal system
• Cardiovascular system
• Pulmonary system
• Integumentary system
• Genitourinary system
• Gastrointestinal system
• Metabolic and endocrine systems
• Cognitive and behavioral systems

Disuse atrophy
• Size of muscle fibers & muscle mass↓
• Generalized and more prominent in antigravity muscles
• Muscle protein synthesis ↓

Disuse atrophy
• Atrophy of type I and IIa muscle fibers > IIb
• Rate of muscle wasting: slow during the 1st
and 2nd days but becomes rapid thereafter
• Muscle wt. loss 50% at 10thday

Loss of Strength
• Myofibrils per fiber volume↓
• Size and number of mitochondria↓
• Sarcomeres ↓
• Strength loss 50% at 4thwk

Loss of Endurance
• ↓ATP & glycogen storage
• Muscle type I and IIa↓

Joint contracture
Prolonged joint immobilization
• Resting flexing muscle length
• Collagen synthesis ↓
(but proportional less than protein synthesis)
• Capsular or soft tissue tightness

Disuse osteoporosis
• Maintenance of skeletal mass depends on mechanical loading (muscle pull and gravity)
• Loss of Ca and hydroxyproline from cancellous portion of long bone (epiphyses and metaphyses) and cortical bone near bone marrow

Immobilization hypercalciuria(± hypercalcemia)
• Urinary calcium excretion above the normal level on 2nd - 3rd day and max loss in 4th -5th wk
• Hypercalcemia may show in young adults (SCI)

Immobilization hypercalciuria(± hypercalcemia)
• Symptoms: anorexia, abd. pain, N/V, constipation, confusion, coma
• Decrease in total Ca can last for months or years (even after resumption of physical act.)

Effects in cardiovascular & pulmonary systems

Redistribution of body fluid
• Lying down : 500-700 ml. of blood shifts to thorax --> CO ↑ & HR ↓
• ↓ secretion of ADH (compensatory diuresis)
• reduction in blood volume and CO
• blood vol. loss max day 14th (20%)

Postural hypotension
• Blood shift
• Venous compliance and intravascular depletion
• Inadequate sympathetic response

Postural hypotension
• Postural CVS responses may completely lost after 3 wk of bed rest in healthy people
• Restoration take 20-72 days

Cardiac deconditioning at rest
• resting HR ↑ 1 bpm every 2 days
(immobization tachycardia)
When resuming submax. activity
• After 3 days of bed rest: HR↑ 32%
• After 7 days of bed rest: HR↑ 62%
• After 21 days of bed rest: HR↑ 89%

Redistribution of body fluid
• Plasma volume ↓ more than RBC mass
→ blood viscosity↑
→ thromboembolic phenomena

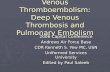
Deep venous thrombosis
• Virchow’s triad : venous stasis
↑blood coagulability
injury to the vessel wall

Deep venous thrombosis
• Immobility: exposes two factor
– venous stasis: decrease pumping of calf m.
– ↑blood coagulability: ↑blood viscosity
• May develop pulmonary embolism

Effect on respiratory system
2% 7%
19%
30%
• Diaphragm movement ↓
• Chest excursion ↓
• ROM of costovertebral and costochondral joints↓

Effect on respiratory system
• In recumbency, secretions pool in the dependent part, whereas the upper part is dry and the ciliary function is impaired so the secretion clearance
• Changes in ventilation-perfusion ratio in the dependent part leads to lowered arterial oxygenation

Effect on respiratory system
• ↑Risk of atelectasis and pneumonia
• Diaphram thickness↓in 72 hr of invasive ventilation

Effects of immobilization on Integumentary systems
• Pressure injury
• Dependent edema

Effect on gastrointestinal system
• Loss of appetite
• ↓rate of absorption
• Distaste protein rich food: hypoproteinemia

Effect on gastrointestinal system
• ↓Bowel motility: GE reflux
• Constipation
- ↑adrenergic activity; inh. peristalsis + ↑sphincter contraction
- Plasma vol. loss and dehydration
- Defecate in nonphysiological position

Effects on Genitourinary systems
• Bladder/renal stones & UTI
• Hypercalciuria, ↑urinary phosphorus excretion
• Void in supine position → incomplete bladder emptying → urinary retention
(abdominal weakness, ↓intraab. pressure)

Effects of immobilization on metabolism and endocrine systems
• ↓ lean body mass but ↑ body fat content
• ↓ metabolic activity of muscle → utilization of O2 and glucose↓ → insulin resistance (Glucose intolerance)

Effects of immobilization on metabolism and endocrine systems
• Electrolyte imbalance (Na, K, phosphorus)
• ↑ parathyroid hormone production & other hormones alterations

Effects of immobilization on Cognitive and behavioral systems
• Sensory deprivation
• Confusion and disorientation
• Anxiety and depression
• ↓ intellectual capacity
• Impaired balance and coordination

Post ICU Care Syndrome (PICS)
• New or worsening impairment in physical, cognitive or mental health status arising after critical illness and persisting beyond discharge form the acute care settings

Post ICU Care Syndrome (PICS)
• Symptoms: generalized weakness, fatigue, mobility ↓, anxious/depressed mood, sexual dysfn, sleep disturbances, cognitive issues
• Symptoms can last for few months to many years post recovery

Post ICU Care Syndrome (PICS)
Cognitive impairment
• Incidence 25-75%
• Memory disturbance/loss, slow mental processing, poor concentration, thinking and judgement impairment
• Risk factors: delirium duration, brain dysfn, hypoxia, hypotension, glucose dysregulation, respiratory failure (mech. ventilation), severe sepsis, renal replacement therapy, ARDS, prior cognitive impairment

Post ICU Care Syndrome (PICS)
Psychiatric illnessess
• Incidence 1-62%
• Depression, anxiety, PTSD
• Risk factors: female, lower educational level, preexisting disability, use of sedation and analgesia, other as cognitive risk

Post ICU Care Syndrome (PICS)
Physical impairment
• Incidence > 25%
• ICU-acquired weakness, fatigue, poor mobility, recurrent falls
• Risk factors: prolonged mech. ventilation (>7 days), sepsis, multisystem organ failure, prolonged duration of deep sedation

PICS-F (family)
• acute and chronic psychological effects of critical illness on family of pt. includes symptoms that are experienced during critical illness and those that occur following death or D/C form ICU
• Symptoms: sleep deprivation, anxiety, depression, PTSD
• Risk factors: poor communication, decision-making role, lower education level, having loved one who died/close to death

ABCDE bundle
“Prevention is better than cure”
• Awakening (light/minimal sedation)
• Breathing (spontaneous breathing trial)
• Coordination of care and communication among various disciplines
• Delirium monitoring, assessment, Mx
• Early ambulation in ICU

Early Mobilization

Early Mobilization
• Proposed in 1975 and growing
• “the application of physical activity within the first 2 to 5 days of critical illness or injury”

Early Mobilization
Benefits (esp. start W/I 72 hr)
• prevent ICUAW
• ↑ventilator free days
• ↓ Delirium duration
• ↓ ICU and hospital LOS
• improve functional outcome at D/C (6MWD, independent ambulation)
• Feeling of well-being (SF-36)

Early Mobilization
Consideration
• But recent systematic review showed minimal effect on fn recovery or QoL
• No assoc. bt EM and short-/long-term mortality

Early Mobilization
Limitation of evidence
• Heterogeneity of ICU patient
• Lack of consensus around terms of early mobilization (intensity, duration, freq.)
• Variation in standard pt. care
• Inconsistency in outcome measurement

Early Mobilization
Core set of outcomes measures
• EQ-5D
• HADS (the hospital anxiety and depression scale)
• IES-R (Impact of Events Scale-Revised)
• Survival
• Others – not consensus (MoCA, 6MWT, MMT/grip strength)

Early Mobilization
Large variety of interventions
• PROM
• NMES
• Cycle ergometers
• Tilt tables
• Active assistive exercise
• Strengthening exercise
• Functional mobilization

Early Mobilization
Mobilizing pt
• Screen pt.
• Vital signs and status
• Environment, Cables, instrument
• Titrate with monitor
• Be prepared for all situations
• Enough staffs

Early Mobilization
Titrate mobility
• Bed rolling
• Upright with support (legs on bed)
• Dangling
• Pivot to chair
• Standing
• Marching
• Ambulation

Safety
Event ? %

Safety
• Potential safety event 2.6% (mostly BP change and O2 desat (self resolved))
• Significant complication 0.6%

Safety

Barrier
• Patient factor
• Structural barrier
• Process barrier
• Cultural barrier

Barrier
Patient factor

Barrier
Patient factor

Barrier
Patient factor

Barrier

Barrier

Barrier

Early Mobilization
Management
• Multidisciplinary team
• Team education
• Mobility champions/teams
• Stepwise approach to mobility

Take home message
• Immobility is terrible
• EM start within the first 72 hr may improve outcomes
• Safe and feasible
• Prevention is better than cure
Related Documents