Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Early diagnosis of AKI
Presented byDrYHaghdar saheli
Assistant Professor of GUMSNephrologist
bull AKI remains a common and significant problem in the last decade Between 5 and 20 of critically ill patients in the ICU have an episode of AKI with ATN accounting for about 75 of cases
bull Despite significant advances in both critical care and nephrology the mortality rate of hospitalized patients with AKI has remained relatively unchanged at around 50 over the past few decades
bull The most common causes of AKI are septic shock ischemia and nephrotoxins
bull The loss of kidney function in AKI is most easily detected by measurement of the serum creatinine
bull Although the serum creatinine is widely used in diagnosing the presence of AKI it is a suboptimal biomarker
bull It is a lagging marker of change in kidney function therefore it has poor sensitivity for the early diagnosis of AKI and it is unable to differentiate among the various causes of AKI
bull The rise in serum creatinine is slow following the onset of AKI
bull By the time a change is observed in the serum creatinine a critical therapeutic window may have been missed particularly among those with ATN
bull A number of factors may contribute to a lag in rise of serum creatinine after AKI including dilutional effect of fluid administration and decrease in creatinine generation
bull novel biomarkers are potential to reflect physiologic and pathophysiologic processes of the injured kidney
bull Some biomarkers are detected in the urine of patients without a diagnostic increase in serum creatinine which defines a group of patients with subclinical AKI who are at risk for adverse outcomes
bull Biomarkers are used in clinical investigation to facilitate early randomization to different treatment arms
bull For instance sepsis-associated AKI may have a biomarker profile that is distinctly different from that of nephrotoxin-associated AKI
bull Clinicians need tools that are not influenced by other clinical parameters or patient characteristics and that can identify losses in GFR soon after occurence
bull the ideal biomarker of AKI would be a substance that the kidney releases immediately in response to injury and that can be detected in the blood or urine without significant metabolism
bull This biomarker would be highly sensitive and specific for injury to the kidney
bull Novel AKI biomarkers would be detect injury prior to changes in kidney function and potentially to aid in the differential diagnosis of AKI
Traditional biomarkers
Urine output
bull Urine output (UO) in AKI can vary from states of oliguria (lt400 mL24 h) to anuria (lt100 mL24 h) to extreme polyuria
bull While severe AKI can exist despite normal UO changes in UO can occur long before any biochemicalchanges are apparent As such UO is one of the criteria for defining AKI
bull UO often decreases before serum creatinine (SCr) concentration increases making it a more time-sensitive marker of GFR
bull However UO is not nearly as specific for GFR While it is true that if there is no UO in the absence of obstruction there can be no GFR not all reductions in UO signal AKI
bull Furthermore while sustained oliguria is invariably associated with AKI the timeliness of UO as an early indicator is lost in this case
Urine dipstick and microscopic examination
bull Routine dipstick and microscopic examinations of urine are often helpful in determining the cause of AKI
bull While granular or epithelial casts in urine are increased in acute tubular necrosis (ATN) they lack sufficient sensitivity specificity and predictive power for routine clinical use
Urinary indices
bull Diagnostic urinary indices of AKI are the fractional excretion of sodium (FENa) urea (FEurea) uric acid urine sodium and urine osmolality
bull Reduced effective circulating volume stimulates anti-diuretic hormone (ADH) release which results in increased distal water and urea reabsorption Thus low FEurea (lt35) is more sensitive and specific than FENa in differentiating between prerenal and renal causes of AKI especially when diuretics have been administered
bull FEurea and FENa have low diagnostic sensitivity in distinguishing azotemia associated with renal vasoconstriction and intact tubular function from established AKI with tubular dysfunction
Urinary tubular enzymes
bull Traditional urinary biomarkers including low- and high-molecular-weight proteins (a1-microglobulin b2- microglobulin retinol-binding proteins) brush border antigens (NaH exchanger isoform-3) urinary enzymes (a-glutathione S-transferase c-glutamyl transpeptidase N-acetyl-b-D-glucosaminidase) and Tamm-Horsfallprotein
bull have not entered clinical routine for AKI patients due to the lack of sufficient validation lack of standardized assays
Urinary tubular enzymes
bull Urinary tubular enzymes consist of proximal renal tubular epithelial antigen (HRTE-1) alpha-glutathione S-transferase (alpha-GST) glutamyltranspeptidase(gamma-GT) alanine aminopeptidase (AAP) lactate dehydrogenase (LDH) N-acetyl-beta-glucosaminidase(NAG) and alkaline phosphatase (ALP)
bull Most of these are released from proximal tubular epithelial cells within 12 hours and four days earlier than a detectable rise in serum creatinine
bull No validated cut-off points currently exist to help distinguish prerenal disease from ATN
Urinary low-molecular-weight proteins
bull Alpha1-microglobulin (alpha1-m) beta2-microglobulin (beta2-m) retinol-binding protein (RBP) adenosine deaminase-binding protein (ABP) and urinary cystatin C are urinary lowmolecular- weight proteins
bull They are produced at different sites filtered at the glomerulus and reabsorbed at the proximal tubule with no secretion
bull Although promising prognostically and to help distinguish prerenal disease from ATN increased levels may be observed after reversible and mild dysfunction and may not necessarily be associated with persistent or irreversible damage
Functional biomarkersSerum creatinine
bull Currently the standard diagnostic tools for AKI detection are SCrconcentration and UO both of which are markers of renal function but not kidney injury
bull SCr is an integrator of various intra- and extra-renal functions and its concentration indicates the balance between creatinine generation and excretion
bull Unfortunately due to the non-linear relationship between GFR and sCr the increase of creatinine may be within the reference range in early phase of AKI and may overlooked
bull SCr does not indicate the severity of the injury until a steady state has been reached in AKI Therefore SCr is a delayed and insensitive biomarker of changes in kidney function moreover its concentration does not differentiate between structural kidney damage and functional hemodynamic triggers and it could be affected by many factors
bull Especially in intensive care unit patients creatinine-based definitions of AKI can be influenced by baseline creatinine estimation fluid overload malnourishment and muscle wasting
Cystatin-C
bull Cystatin-C is produced at a constant rate by nucleated cells filtered by the glomerular cells almost completely reabsorbed and catabolized (but not secreted) in the proximal tubule It is a polypeptide chain with 120 amino acid residues
bull In this way some of the limitations of serum creatinine effect of muscle mass diet gender and tubular secretion may not be a problem with cystatin C and appear to rise one to two days earlier than serum creatinine
bull Cystatin C is better marker of GFR than serum creatinine as demonstrated in several studies
bull Over the past decade Cystatin C (CyC) a serum measure of renal function is a stronger predictor of the risk of death and cardiovascular events in elderly persons than is creatinine
bull Koyner et al demonstrated that urinary CyC was superior to SCr and plasma CyC in the early diagnosis of acute kidney injury following adult cardiac surgery
bull Roos et al performed a systematic review comparing the diagnostic accuracy of plasma and urine CyC with SCr in patients undergoing cardiac surgery They concluded that the diagnostic accuracy for impaired renal function favors urine CyC
bull However while Cys-C levels are a more precise indicator of kidney function than SCr concentration they seem to be influenced by old age large doses of corticosteroids hyperthyroidism inflammation neoplasia smoking and alcohol consumption
bull Currently it is unclear whether the value of Cys-C is generalizable to all forms of AKI or specific to particular populations
Damage biomarkers
Neutrophil Gelatinase-Associated Lipocalin(NGAL)
bull Human NGAL is a 25 kDa protein firstly identified bound to gelatinase in specific granules of the neutrophil NGAL is a critical component of innate immunity to bacterial infection and is expressed by immune cells hepatocytes and renal tubular cells in various disease states
bull Its resistance to proteolysis further enhanced potential suitability as a clinical biomarker
bull In healthy kidneys it is barel detectable in either plasma or urine
bull However in the setting of acute tubular injury NGAL undergoes rapid and profound upregulation with large increases in both urine and plasma
bull Distinct from traditional markers of function such as creatinine this rapid response enables NGAL to potentially identify injured kidney much earlier than was previously possible The endogenous role of NGAL remains unclear It seems to be involved with iron transportation to and from the proximal tubular epithelial cells and animal studies demonstrate a renoprotective effect of exogenously administered NGAL in the setting of acute ischemic injury
bull NGAL was also detected in the urine of mice in the early stage of cisplatin-induced nephrotoxicity
bull These animal studies demonstrated that NGAL may represent an early sensitive and noninvasive urinary biomarker for ischemic and nephrotoxic kidney injury
bull NGAL is markedly upregulated and abundantly expressed in the kidney after renal ischemia
bull In this setting NGAL may function to dampen toxicity by reducing apoptosis and increasing the normal proliferation of kidney tubule cells
bull following ischemia reperfusion as evidenced by a rise in creatinine the kidneys illuminate indicating NGAL production at the site of injury
bull Interestingly following maneuvers that lead to significant prerenal disease there was no NGAL illumination indicating that prerenal disease does not induce NGAL expression
bull Thus NGAL may potentially be useful in differentiating prerenal disease from ATN
bull In these studies the average sensitivity and specificity of NGAL measured one to three days prior to AKI diagnosis was 76 and 77 percent respectively for cardiac surgery patients and 73 and 80 percent respectively for patients admitted to the intensive care unit (ICU)
bull NGAL may also represent early sensitive biomarker of AKI after contrast administrations for coronary angiography
bull NGAL was measured in the serum and urine before and at 2 4 12 24 and 48 h after contrast administration they found a significant rise in serum NGAL 2 and 4 h after PCI and a rise in urinary NGAL 4 and 12 h after PCI
bull A similar study of 25 patients with normal serum creatinine undergoing PCI due to unstable angina There was a significant rise in serum NGAL after 2 and 4 hours Urinary NGAL and urinary L-FABP followed the same pattern Both markers increased significantly after 4 hours and remained elevated up to 48 hours after PCI
bull Urine and plasma NGAL levels also represent early biomarkers of AKI in ICU
bull A multicenter study of serum NGAL was performed in 143 critically ill children with systemic inflammatory response syndrome (SIRS) or septic shock during the first 24 h of admission to the ICU there was a significant difference in serum NGAL between healthy children ill children with SIRS and septic shock the study was concluded that serum NGAL is a highly sensitive but nonspecific predictor of acute kidney injury in critically ill children with septic shock
bull A 2010 study evaluated 88 ICU patient and found that an NGAL level of ge150 nmolL predicted AKI with 82 sensitivity and 97 specificity
bull A recent study had 98 patients who were divided in two groups depending on the presence of sepsis Fifty-six patients had sepsis while forty-two patients were nonseptic Among septic patients subjects who developed AKI showed signi1048853 cant higher levels of NGAL
bull A more study of 65 patients with septic shock were found that urine NGAL levels 12 hours before AKI diagnosis were a good predictor of AKI
Kidney Injury Molecule-1 (KIM-1)
bull KIM-1 mRNA and protein are expressed at a low level in normal kidney but are increased dramatically in postischemic kidney
bull KIM-1 has been identified as the first nonmyeloidphosphatidylserine receptor that confers a phagocytic phenotype on injured epithelial cells both in vivo and in vitro
bull Urinary KIM-1 has been found to be an early indicator of AKI that compares favorably to a number of conventional biomarkers and tubular enzymes
bull KIM-1 is also a tissue and urinary biomarker for nephrotoxicant-induced kidney injury
bull Tissue and urinary expressions were measured with different nephrotoxic doses of cisplatin folic acide cadmium gentamycin mercury
bull As early as 1 day after cisplatin treatment positive KIM- 1 immunostaining observed in the outer medulla of the kidney and changes in urinary clusterin indicated the onset of proximal tubular injury in the absence of functional effects
bull Tissue KIM-1 was the most sensitive biomarker for detection of cisplatin-induced kidney damage
bull KIM-1 is a biomarker of AKI in humans bull Urine samples were collected from 32 patients with various
acute and chronic kidney diseases as well as from eight normal controls there was extensive expression of KIM-1 in proximal tubule cells in kidney biopsies from six patients with biopsy confirmed acute tubular necrosis (ATN)
bull Urinary KIM-1 levels were significantly higher in patients with ischemic ATN compared to levels in patients with other forms of acute renal failure or chronic renal disease
bull Adjusted for age gender and length of time delay between the initial insult and sampling of the urine a one-unit increase in normalized KIM-1 was associated with a greater than 12-fold risk for the presence of ATN
bull In hospital patients with AKI urinary levels of KIM-1 that higher levels correlated with a higher odds ratio for dialysis requirement or hospital death
bull this study demonstrated that urinary biomarker of AKI such as KIM-1 can predict adverse clinical outcomes in patients with AKI
bull Both renal and urinary KIM-1 correlate with kidney damage and negatively with renal function but not with proteinuria
bull A recent study has explored urinary KIM-1correlated with kidney function in kidney allograft recipients Kidney transplant recipients showed significantly higher KIM-1 values than the healthy volunteers this study concluded that even a successful kidney transplantation is associated with kidney injury as reflected by elevated urinary KIM-1
bull A rapid direct 15-minute assay for the detection of urinary human KIM-1 has been developed Using this assay more urinary KIM-1 was detected in the urine of patients with AKI than in the urine from healthy volunteers
Urinary interleukin-18
bull Interleukin18 (IL-18) is a 22 kDa pro-inflammatory cytokine that increases in the kidney after ischemia-reperfusion injury in a caspase- 1-dependent manner
bull Patients with ATN had significantly greater urinary IL-18 concentrations than those with other conditions (healthy controls patients with pre-renal azotemia urinary tract infection CKD and nephrotic syndrome)
bull urinary IL-18 concentrations measured in the first 24 h after kidney transplantation were higher in patients who received a cadaveric kidney that developed delayed graft function compared to patients who received a cadaveric kidney with prompt graft function and patients who received a kidney with prompt graft function from a living donor
bull However the performance of urinary IL-18 measured 1 day before AKI was modest
bull Its predictive utility for AKI following cardiac surgery could not be demonstrated in one prospective observational study of 100 adult patients
bull In addition in a large study population of 1439 critically ill patients IL-18 had a poor-to-moderate ability to predict AKI renal replacement therapy (RRT) or 90-day mortality
Liver-Type Fatty Acid Binding Protein(L-FABP)
bull Liver-type fatty acid-binding protein (L-FABP) is a 14 kDa protein from the large super- family of lipidbinding proteins
bull The 14-kD L-FABP protein can be localized predominantly in the proximal tubule
bull Noiri et al demonstrated that increase of urinary L-FABP was observed at 1 h after ischemia even in the 5-min IRI group and urinary L-FABP was superior to BUN and urinary NAG for early and accurate detection of acute tubular necrosis in different models of animal AKI
bull urinary L-FABP may be a promising biomarker for early detection of AKI and prediction of dialysis requirement and in-hospital mortality
bull Urinary excretion of urinary liver-type fatty acid-binding protein (L-FABP) reflects stress of proximal tubular epithelial cells and correlates with severity of ischemic tubular injury
bull A meta-analysis of 15 prospective cohort studies demonstrated that in hospitalndashbased cohorts of patients at risk of AKI L-FABP can discriminate for the diagnosis of AKI and predict the need for dialysis and in-hospital mortality
bull It was correlated with the degree of tubulointerstitial damage in a folic acid induced nephropathy
bull In ischemic and cisplatin-induced AKI L-FABP was increased in the urine before the increase in BUN
bull In cisplatin-induced AKI urinary L-FABP levels increased exponentially even in the lowest dose group as early as 2 hours whereas BUN levels increased at 48 hours
bull L-FABP was measured in 80 critically ill patients Urinary L-FABP levels in patients with septic shock were significantly higher than severe sepsis without shock Serum L-FABP levels did not have significant differences between patients with septic shock severe sepsis and healthy
bull Another study was evaluated 145 septic shock patients complicated with established AKI Urinary L-FABP measured at admission was significantly higher in the nonsurvivors of septic shock with established acute kidney injury than in the survivors
Failure of the TRIBE-AKI study
bull The Translational Research Investigating Biomarker Endpoints in AKI (TRIBE-AKI) study evaluated the performance of urinary c-glutamyltranspeptidase ( c-GTP) alkaline phosphatase NGAL Cys-C KIM-1 and IL-18 in AKI diagnosis
bull The results of four novel urine biomarkers and one plasma biomarker (urine NGAL IL-18 KIM-1 and L-FABP and plasma NGAL) were provided Of all the novel biomarkers only urine IL-18 and plasma NGAL in adults were helpful in predicting progression of AKI when measured on the day of clinical AKI diagnosis
bull Combinations of three biomarkers in adults from two different time points and combinations of two biomarkers in children from two time points were found to be able to increase the ROC for AKI up to 078
bull In summary the clinical use of single damage biomarkers in AKI prediction remains unclear because large prospective multicenter trials such as the TRIBE-AKI study (nfrac141530) have failed to demonstrate troponin-like diagnostic performance
Various clinical scenarios of AKI based onfunction damage and stress
bull Over the last decade a number of novel damage biomarkers have been evaluated for their capacity to detect kidney damage and predict the development of AKI However the relationship between decreasing function and increasing damage is not as straightforward as might be assumed
bull The characteristic pattern whereby damage precedes loss of function (panel A) may be seen in some cases of AKI and affords an opportunity to detect ldquosubclinicalrdquo AKI before function start to fall Unfortunately other patterns might also occur For example functional decline may start to occur alongside damage (panel B) and in some cases function may start to decline even before damage (panel C)
bull This makes damage markers difficult to use for predicting AKI However other markers might actually measure the ldquostressrdquo occurring at the cellular level before damage or loss of function
Paradigm shift to pre-injury phase biomarkers
bull Katz et al proposed that the pre-injury phase that leads to AKI can be described as ldquoacute kidney stressrdquo (AKS) after the report of the identification of cell cycle arrest biomarkers that signal the potential development of AKI is part of an evolution in the molecular diagnosis and understanding of AKI
bull These biomarkers are released by kidney cells along a path which may lead to AKI during a pre-injury phase
bull AKS is defined as the increased-risk phase (pre-injury phase) that leads to AKI
bull This ldquoAKSrdquo may or may not lead to damage and functional declinebull But it is the earliest possible the process of AKI can be detected
Pre-injury phase biomarkers
Stress biomarkersbull In 2013 Kashani et al reported the results of a prospective international
observational investigation (the Sapphire study) of tissue inhibitor of metalloproteinases- 2 (TIMP-2) and insulin-like growth factor-binding protein 7 (IGFBP7) in a heterogeneous group of critically ill patients [TIMP-2][IGFBP7] was significantly superior to all previously described markers of AKI (plt0002)
bull Next the Opal and Topaz study showed the cut-off value and risk assessment using the urinary[TIMP-2] [IGFBP7]
bull The urine [IGFBP7][TIMP2] biomarker is already FDA approved and commercially available in the United States
bull Falsepositive results are common and they will be magnified if the test is used inappropriately in low-risk patients In addition this biomarker should not be used in ambulatory practices and it is not beneficial in patients with established AKI
microRNAsbull microRNAs (miRNAs) are endogenous single-stranded non-coding
mRNAs of about 19-23 nucleotides bull In the past years researchers have begun to investigate the
relevance of miRNAs to AKI with many miRNAs being implicated bull Some of them contribute to pathogenesis by regulating apoptosis
and inflammation amplifying or reducing acute injury responses while others regulate fibrosis and angiogenesis participating in renal recovery or progression to fibrosis
bull Certain miRNAs have been investigated for their potential as novel biomarkers for the early detection or prognostication of AKI
Hemojuvelinbull Hemojuvelin (HJV) a glycophosphatidylinositol (GPI)- linked
membrane protein is highly expressed in liver and skeletal musclesbull The molecular weight of HJV is 42 kDa for the soluble form (sHJV)
and can be passed through glomerular filtration and reabsorbed by the renal tubules Increased iron content in the kidney and urine is observed in human and animal models of AKI and increased iron load can induce renal tubular cell injury
bull There is evidence that the increased expression of the hemojuvelin-hepcidin ferroportin pathway is an intrinsic response to iron overload conditions during AKI
bull Therefore urine HJV (uHJV) has the potential to be an early AKI biomarker in response to iron homeostasis during AKI
Combination of functional and damage biomarkers
bull While new biomarkers are being validated functional biomarkers (serum creatinine serum urea and urine output) continue to be utilized in the diagnosis and staging of AKI In the future existing or newer damage biomarkers will likely be combined with the use of functional biomarkers to enhance the ability of RIFLE AKIN
bull A study of 345 children after cardiopulmonary bypass surgery demonstrated that the composite of functional biomarker such as plasma cystatin C and urinary NGAL was superior to changes in serum creatinine to predict AKI
PROGNOSTIC BIOMARKERS
bull Most of the biomarkers described above allow early detection of acute kidney injury but do not predict severe AKI
Urinary renin and angiotensinogen
bull Urinary renin angiotensinogen and plasma NGAL may predict the development of severe AKI
bull Among 99 consecutively enrolled patients who developed AKI the ratio of urinary angiotensinogen to urinary creatinine (uAnCR expressed as ng per mg creatinine)calculated Patients with the highest uAnCR had a higher risk of worsening AKI compared with patients with the lowest uAnCR An elevated uAnCR predicted a longer hospital stay
bull Among 204 patients who developed Acute Kidney Injury Network (AKIN) stage 1 following cardiac surgery the urinary renin-to-creatinine ratio and the angiotensinogen-to-creatinine ratio predicted a composite outcome of death or AKIN stage 3 or death
Plasma NGAL
bull In a prospective cohort study in which 616 patients admitted from the emergency department were classified by clinical criteria as AKI transient azotemia stable CKD or normal kidney function plasma NGAL discriminated AKI from normal function and from transient azotemia
bull Higher concentrations of NGAL were associated with more severe AKI
Thanks for your attention
bull AKI remains a common and significant problem in the last decade Between 5 and 20 of critically ill patients in the ICU have an episode of AKI with ATN accounting for about 75 of cases
bull Despite significant advances in both critical care and nephrology the mortality rate of hospitalized patients with AKI has remained relatively unchanged at around 50 over the past few decades
bull The most common causes of AKI are septic shock ischemia and nephrotoxins
bull The loss of kidney function in AKI is most easily detected by measurement of the serum creatinine
bull Although the serum creatinine is widely used in diagnosing the presence of AKI it is a suboptimal biomarker
bull It is a lagging marker of change in kidney function therefore it has poor sensitivity for the early diagnosis of AKI and it is unable to differentiate among the various causes of AKI
bull The rise in serum creatinine is slow following the onset of AKI
bull By the time a change is observed in the serum creatinine a critical therapeutic window may have been missed particularly among those with ATN
bull A number of factors may contribute to a lag in rise of serum creatinine after AKI including dilutional effect of fluid administration and decrease in creatinine generation
bull novel biomarkers are potential to reflect physiologic and pathophysiologic processes of the injured kidney
bull Some biomarkers are detected in the urine of patients without a diagnostic increase in serum creatinine which defines a group of patients with subclinical AKI who are at risk for adverse outcomes
bull Biomarkers are used in clinical investigation to facilitate early randomization to different treatment arms
bull For instance sepsis-associated AKI may have a biomarker profile that is distinctly different from that of nephrotoxin-associated AKI
bull Clinicians need tools that are not influenced by other clinical parameters or patient characteristics and that can identify losses in GFR soon after occurence
bull the ideal biomarker of AKI would be a substance that the kidney releases immediately in response to injury and that can be detected in the blood or urine without significant metabolism
bull This biomarker would be highly sensitive and specific for injury to the kidney
bull Novel AKI biomarkers would be detect injury prior to changes in kidney function and potentially to aid in the differential diagnosis of AKI
Traditional biomarkers
Urine output
bull Urine output (UO) in AKI can vary from states of oliguria (lt400 mL24 h) to anuria (lt100 mL24 h) to extreme polyuria
bull While severe AKI can exist despite normal UO changes in UO can occur long before any biochemicalchanges are apparent As such UO is one of the criteria for defining AKI
bull UO often decreases before serum creatinine (SCr) concentration increases making it a more time-sensitive marker of GFR
bull However UO is not nearly as specific for GFR While it is true that if there is no UO in the absence of obstruction there can be no GFR not all reductions in UO signal AKI
bull Furthermore while sustained oliguria is invariably associated with AKI the timeliness of UO as an early indicator is lost in this case
Urine dipstick and microscopic examination
bull Routine dipstick and microscopic examinations of urine are often helpful in determining the cause of AKI
bull While granular or epithelial casts in urine are increased in acute tubular necrosis (ATN) they lack sufficient sensitivity specificity and predictive power for routine clinical use
Urinary indices
bull Diagnostic urinary indices of AKI are the fractional excretion of sodium (FENa) urea (FEurea) uric acid urine sodium and urine osmolality
bull Reduced effective circulating volume stimulates anti-diuretic hormone (ADH) release which results in increased distal water and urea reabsorption Thus low FEurea (lt35) is more sensitive and specific than FENa in differentiating between prerenal and renal causes of AKI especially when diuretics have been administered
bull FEurea and FENa have low diagnostic sensitivity in distinguishing azotemia associated with renal vasoconstriction and intact tubular function from established AKI with tubular dysfunction
Urinary tubular enzymes
bull Traditional urinary biomarkers including low- and high-molecular-weight proteins (a1-microglobulin b2- microglobulin retinol-binding proteins) brush border antigens (NaH exchanger isoform-3) urinary enzymes (a-glutathione S-transferase c-glutamyl transpeptidase N-acetyl-b-D-glucosaminidase) and Tamm-Horsfallprotein
bull have not entered clinical routine for AKI patients due to the lack of sufficient validation lack of standardized assays
Urinary tubular enzymes
bull Urinary tubular enzymes consist of proximal renal tubular epithelial antigen (HRTE-1) alpha-glutathione S-transferase (alpha-GST) glutamyltranspeptidase(gamma-GT) alanine aminopeptidase (AAP) lactate dehydrogenase (LDH) N-acetyl-beta-glucosaminidase(NAG) and alkaline phosphatase (ALP)
bull Most of these are released from proximal tubular epithelial cells within 12 hours and four days earlier than a detectable rise in serum creatinine
bull No validated cut-off points currently exist to help distinguish prerenal disease from ATN
Urinary low-molecular-weight proteins
bull Alpha1-microglobulin (alpha1-m) beta2-microglobulin (beta2-m) retinol-binding protein (RBP) adenosine deaminase-binding protein (ABP) and urinary cystatin C are urinary lowmolecular- weight proteins
bull They are produced at different sites filtered at the glomerulus and reabsorbed at the proximal tubule with no secretion
bull Although promising prognostically and to help distinguish prerenal disease from ATN increased levels may be observed after reversible and mild dysfunction and may not necessarily be associated with persistent or irreversible damage
Functional biomarkersSerum creatinine
bull Currently the standard diagnostic tools for AKI detection are SCrconcentration and UO both of which are markers of renal function but not kidney injury
bull SCr is an integrator of various intra- and extra-renal functions and its concentration indicates the balance between creatinine generation and excretion
bull Unfortunately due to the non-linear relationship between GFR and sCr the increase of creatinine may be within the reference range in early phase of AKI and may overlooked
bull SCr does not indicate the severity of the injury until a steady state has been reached in AKI Therefore SCr is a delayed and insensitive biomarker of changes in kidney function moreover its concentration does not differentiate between structural kidney damage and functional hemodynamic triggers and it could be affected by many factors
bull Especially in intensive care unit patients creatinine-based definitions of AKI can be influenced by baseline creatinine estimation fluid overload malnourishment and muscle wasting
Cystatin-C
bull Cystatin-C is produced at a constant rate by nucleated cells filtered by the glomerular cells almost completely reabsorbed and catabolized (but not secreted) in the proximal tubule It is a polypeptide chain with 120 amino acid residues
bull In this way some of the limitations of serum creatinine effect of muscle mass diet gender and tubular secretion may not be a problem with cystatin C and appear to rise one to two days earlier than serum creatinine
bull Cystatin C is better marker of GFR than serum creatinine as demonstrated in several studies
bull Over the past decade Cystatin C (CyC) a serum measure of renal function is a stronger predictor of the risk of death and cardiovascular events in elderly persons than is creatinine
bull Koyner et al demonstrated that urinary CyC was superior to SCr and plasma CyC in the early diagnosis of acute kidney injury following adult cardiac surgery
bull Roos et al performed a systematic review comparing the diagnostic accuracy of plasma and urine CyC with SCr in patients undergoing cardiac surgery They concluded that the diagnostic accuracy for impaired renal function favors urine CyC
bull However while Cys-C levels are a more precise indicator of kidney function than SCr concentration they seem to be influenced by old age large doses of corticosteroids hyperthyroidism inflammation neoplasia smoking and alcohol consumption
bull Currently it is unclear whether the value of Cys-C is generalizable to all forms of AKI or specific to particular populations
Damage biomarkers
Neutrophil Gelatinase-Associated Lipocalin(NGAL)
bull Human NGAL is a 25 kDa protein firstly identified bound to gelatinase in specific granules of the neutrophil NGAL is a critical component of innate immunity to bacterial infection and is expressed by immune cells hepatocytes and renal tubular cells in various disease states
bull Its resistance to proteolysis further enhanced potential suitability as a clinical biomarker
bull In healthy kidneys it is barel detectable in either plasma or urine
bull However in the setting of acute tubular injury NGAL undergoes rapid and profound upregulation with large increases in both urine and plasma
bull Distinct from traditional markers of function such as creatinine this rapid response enables NGAL to potentially identify injured kidney much earlier than was previously possible The endogenous role of NGAL remains unclear It seems to be involved with iron transportation to and from the proximal tubular epithelial cells and animal studies demonstrate a renoprotective effect of exogenously administered NGAL in the setting of acute ischemic injury
bull NGAL was also detected in the urine of mice in the early stage of cisplatin-induced nephrotoxicity
bull These animal studies demonstrated that NGAL may represent an early sensitive and noninvasive urinary biomarker for ischemic and nephrotoxic kidney injury
bull NGAL is markedly upregulated and abundantly expressed in the kidney after renal ischemia
bull In this setting NGAL may function to dampen toxicity by reducing apoptosis and increasing the normal proliferation of kidney tubule cells
bull following ischemia reperfusion as evidenced by a rise in creatinine the kidneys illuminate indicating NGAL production at the site of injury
bull Interestingly following maneuvers that lead to significant prerenal disease there was no NGAL illumination indicating that prerenal disease does not induce NGAL expression
bull Thus NGAL may potentially be useful in differentiating prerenal disease from ATN
bull In these studies the average sensitivity and specificity of NGAL measured one to three days prior to AKI diagnosis was 76 and 77 percent respectively for cardiac surgery patients and 73 and 80 percent respectively for patients admitted to the intensive care unit (ICU)
bull NGAL may also represent early sensitive biomarker of AKI after contrast administrations for coronary angiography
bull NGAL was measured in the serum and urine before and at 2 4 12 24 and 48 h after contrast administration they found a significant rise in serum NGAL 2 and 4 h after PCI and a rise in urinary NGAL 4 and 12 h after PCI
bull A similar study of 25 patients with normal serum creatinine undergoing PCI due to unstable angina There was a significant rise in serum NGAL after 2 and 4 hours Urinary NGAL and urinary L-FABP followed the same pattern Both markers increased significantly after 4 hours and remained elevated up to 48 hours after PCI
bull Urine and plasma NGAL levels also represent early biomarkers of AKI in ICU
bull A multicenter study of serum NGAL was performed in 143 critically ill children with systemic inflammatory response syndrome (SIRS) or septic shock during the first 24 h of admission to the ICU there was a significant difference in serum NGAL between healthy children ill children with SIRS and septic shock the study was concluded that serum NGAL is a highly sensitive but nonspecific predictor of acute kidney injury in critically ill children with septic shock
bull A 2010 study evaluated 88 ICU patient and found that an NGAL level of ge150 nmolL predicted AKI with 82 sensitivity and 97 specificity
bull A recent study had 98 patients who were divided in two groups depending on the presence of sepsis Fifty-six patients had sepsis while forty-two patients were nonseptic Among septic patients subjects who developed AKI showed signi1048853 cant higher levels of NGAL
bull A more study of 65 patients with septic shock were found that urine NGAL levels 12 hours before AKI diagnosis were a good predictor of AKI
Kidney Injury Molecule-1 (KIM-1)
bull KIM-1 mRNA and protein are expressed at a low level in normal kidney but are increased dramatically in postischemic kidney
bull KIM-1 has been identified as the first nonmyeloidphosphatidylserine receptor that confers a phagocytic phenotype on injured epithelial cells both in vivo and in vitro
bull Urinary KIM-1 has been found to be an early indicator of AKI that compares favorably to a number of conventional biomarkers and tubular enzymes
bull KIM-1 is also a tissue and urinary biomarker for nephrotoxicant-induced kidney injury
bull Tissue and urinary expressions were measured with different nephrotoxic doses of cisplatin folic acide cadmium gentamycin mercury
bull As early as 1 day after cisplatin treatment positive KIM- 1 immunostaining observed in the outer medulla of the kidney and changes in urinary clusterin indicated the onset of proximal tubular injury in the absence of functional effects
bull Tissue KIM-1 was the most sensitive biomarker for detection of cisplatin-induced kidney damage
bull KIM-1 is a biomarker of AKI in humans bull Urine samples were collected from 32 patients with various
acute and chronic kidney diseases as well as from eight normal controls there was extensive expression of KIM-1 in proximal tubule cells in kidney biopsies from six patients with biopsy confirmed acute tubular necrosis (ATN)
bull Urinary KIM-1 levels were significantly higher in patients with ischemic ATN compared to levels in patients with other forms of acute renal failure or chronic renal disease
bull Adjusted for age gender and length of time delay between the initial insult and sampling of the urine a one-unit increase in normalized KIM-1 was associated with a greater than 12-fold risk for the presence of ATN
bull In hospital patients with AKI urinary levels of KIM-1 that higher levels correlated with a higher odds ratio for dialysis requirement or hospital death
bull this study demonstrated that urinary biomarker of AKI such as KIM-1 can predict adverse clinical outcomes in patients with AKI
bull Both renal and urinary KIM-1 correlate with kidney damage and negatively with renal function but not with proteinuria
bull A recent study has explored urinary KIM-1correlated with kidney function in kidney allograft recipients Kidney transplant recipients showed significantly higher KIM-1 values than the healthy volunteers this study concluded that even a successful kidney transplantation is associated with kidney injury as reflected by elevated urinary KIM-1
bull A rapid direct 15-minute assay for the detection of urinary human KIM-1 has been developed Using this assay more urinary KIM-1 was detected in the urine of patients with AKI than in the urine from healthy volunteers
Urinary interleukin-18
bull Interleukin18 (IL-18) is a 22 kDa pro-inflammatory cytokine that increases in the kidney after ischemia-reperfusion injury in a caspase- 1-dependent manner
bull Patients with ATN had significantly greater urinary IL-18 concentrations than those with other conditions (healthy controls patients with pre-renal azotemia urinary tract infection CKD and nephrotic syndrome)
bull urinary IL-18 concentrations measured in the first 24 h after kidney transplantation were higher in patients who received a cadaveric kidney that developed delayed graft function compared to patients who received a cadaveric kidney with prompt graft function and patients who received a kidney with prompt graft function from a living donor
bull However the performance of urinary IL-18 measured 1 day before AKI was modest
bull Its predictive utility for AKI following cardiac surgery could not be demonstrated in one prospective observational study of 100 adult patients
bull In addition in a large study population of 1439 critically ill patients IL-18 had a poor-to-moderate ability to predict AKI renal replacement therapy (RRT) or 90-day mortality
Liver-Type Fatty Acid Binding Protein(L-FABP)
bull Liver-type fatty acid-binding protein (L-FABP) is a 14 kDa protein from the large super- family of lipidbinding proteins
bull The 14-kD L-FABP protein can be localized predominantly in the proximal tubule
bull Noiri et al demonstrated that increase of urinary L-FABP was observed at 1 h after ischemia even in the 5-min IRI group and urinary L-FABP was superior to BUN and urinary NAG for early and accurate detection of acute tubular necrosis in different models of animal AKI
bull urinary L-FABP may be a promising biomarker for early detection of AKI and prediction of dialysis requirement and in-hospital mortality
bull Urinary excretion of urinary liver-type fatty acid-binding protein (L-FABP) reflects stress of proximal tubular epithelial cells and correlates with severity of ischemic tubular injury
bull A meta-analysis of 15 prospective cohort studies demonstrated that in hospitalndashbased cohorts of patients at risk of AKI L-FABP can discriminate for the diagnosis of AKI and predict the need for dialysis and in-hospital mortality
bull It was correlated with the degree of tubulointerstitial damage in a folic acid induced nephropathy
bull In ischemic and cisplatin-induced AKI L-FABP was increased in the urine before the increase in BUN
bull In cisplatin-induced AKI urinary L-FABP levels increased exponentially even in the lowest dose group as early as 2 hours whereas BUN levels increased at 48 hours
bull L-FABP was measured in 80 critically ill patients Urinary L-FABP levels in patients with septic shock were significantly higher than severe sepsis without shock Serum L-FABP levels did not have significant differences between patients with septic shock severe sepsis and healthy
bull Another study was evaluated 145 septic shock patients complicated with established AKI Urinary L-FABP measured at admission was significantly higher in the nonsurvivors of septic shock with established acute kidney injury than in the survivors
Failure of the TRIBE-AKI study
bull The Translational Research Investigating Biomarker Endpoints in AKI (TRIBE-AKI) study evaluated the performance of urinary c-glutamyltranspeptidase ( c-GTP) alkaline phosphatase NGAL Cys-C KIM-1 and IL-18 in AKI diagnosis
bull The results of four novel urine biomarkers and one plasma biomarker (urine NGAL IL-18 KIM-1 and L-FABP and plasma NGAL) were provided Of all the novel biomarkers only urine IL-18 and plasma NGAL in adults were helpful in predicting progression of AKI when measured on the day of clinical AKI diagnosis
bull Combinations of three biomarkers in adults from two different time points and combinations of two biomarkers in children from two time points were found to be able to increase the ROC for AKI up to 078
bull In summary the clinical use of single damage biomarkers in AKI prediction remains unclear because large prospective multicenter trials such as the TRIBE-AKI study (nfrac141530) have failed to demonstrate troponin-like diagnostic performance
Various clinical scenarios of AKI based onfunction damage and stress
bull Over the last decade a number of novel damage biomarkers have been evaluated for their capacity to detect kidney damage and predict the development of AKI However the relationship between decreasing function and increasing damage is not as straightforward as might be assumed
bull The characteristic pattern whereby damage precedes loss of function (panel A) may be seen in some cases of AKI and affords an opportunity to detect ldquosubclinicalrdquo AKI before function start to fall Unfortunately other patterns might also occur For example functional decline may start to occur alongside damage (panel B) and in some cases function may start to decline even before damage (panel C)
bull This makes damage markers difficult to use for predicting AKI However other markers might actually measure the ldquostressrdquo occurring at the cellular level before damage or loss of function
Paradigm shift to pre-injury phase biomarkers
bull Katz et al proposed that the pre-injury phase that leads to AKI can be described as ldquoacute kidney stressrdquo (AKS) after the report of the identification of cell cycle arrest biomarkers that signal the potential development of AKI is part of an evolution in the molecular diagnosis and understanding of AKI
bull These biomarkers are released by kidney cells along a path which may lead to AKI during a pre-injury phase
bull AKS is defined as the increased-risk phase (pre-injury phase) that leads to AKI
bull This ldquoAKSrdquo may or may not lead to damage and functional declinebull But it is the earliest possible the process of AKI can be detected
Pre-injury phase biomarkers
Stress biomarkersbull In 2013 Kashani et al reported the results of a prospective international
observational investigation (the Sapphire study) of tissue inhibitor of metalloproteinases- 2 (TIMP-2) and insulin-like growth factor-binding protein 7 (IGFBP7) in a heterogeneous group of critically ill patients [TIMP-2][IGFBP7] was significantly superior to all previously described markers of AKI (plt0002)
bull Next the Opal and Topaz study showed the cut-off value and risk assessment using the urinary[TIMP-2] [IGFBP7]
bull The urine [IGFBP7][TIMP2] biomarker is already FDA approved and commercially available in the United States
bull Falsepositive results are common and they will be magnified if the test is used inappropriately in low-risk patients In addition this biomarker should not be used in ambulatory practices and it is not beneficial in patients with established AKI
microRNAsbull microRNAs (miRNAs) are endogenous single-stranded non-coding
mRNAs of about 19-23 nucleotides bull In the past years researchers have begun to investigate the
relevance of miRNAs to AKI with many miRNAs being implicated bull Some of them contribute to pathogenesis by regulating apoptosis
and inflammation amplifying or reducing acute injury responses while others regulate fibrosis and angiogenesis participating in renal recovery or progression to fibrosis
bull Certain miRNAs have been investigated for their potential as novel biomarkers for the early detection or prognostication of AKI
Hemojuvelinbull Hemojuvelin (HJV) a glycophosphatidylinositol (GPI)- linked
membrane protein is highly expressed in liver and skeletal musclesbull The molecular weight of HJV is 42 kDa for the soluble form (sHJV)
and can be passed through glomerular filtration and reabsorbed by the renal tubules Increased iron content in the kidney and urine is observed in human and animal models of AKI and increased iron load can induce renal tubular cell injury
bull There is evidence that the increased expression of the hemojuvelin-hepcidin ferroportin pathway is an intrinsic response to iron overload conditions during AKI
bull Therefore urine HJV (uHJV) has the potential to be an early AKI biomarker in response to iron homeostasis during AKI
Combination of functional and damage biomarkers
bull While new biomarkers are being validated functional biomarkers (serum creatinine serum urea and urine output) continue to be utilized in the diagnosis and staging of AKI In the future existing or newer damage biomarkers will likely be combined with the use of functional biomarkers to enhance the ability of RIFLE AKIN
bull A study of 345 children after cardiopulmonary bypass surgery demonstrated that the composite of functional biomarker such as plasma cystatin C and urinary NGAL was superior to changes in serum creatinine to predict AKI
PROGNOSTIC BIOMARKERS
bull Most of the biomarkers described above allow early detection of acute kidney injury but do not predict severe AKI
Urinary renin and angiotensinogen
bull Urinary renin angiotensinogen and plasma NGAL may predict the development of severe AKI
bull Among 99 consecutively enrolled patients who developed AKI the ratio of urinary angiotensinogen to urinary creatinine (uAnCR expressed as ng per mg creatinine)calculated Patients with the highest uAnCR had a higher risk of worsening AKI compared with patients with the lowest uAnCR An elevated uAnCR predicted a longer hospital stay
bull Among 204 patients who developed Acute Kidney Injury Network (AKIN) stage 1 following cardiac surgery the urinary renin-to-creatinine ratio and the angiotensinogen-to-creatinine ratio predicted a composite outcome of death or AKIN stage 3 or death
Plasma NGAL
bull In a prospective cohort study in which 616 patients admitted from the emergency department were classified by clinical criteria as AKI transient azotemia stable CKD or normal kidney function plasma NGAL discriminated AKI from normal function and from transient azotemia
bull Higher concentrations of NGAL were associated with more severe AKI
Thanks for your attention

bull The loss of kidney function in AKI is most easily detected by measurement of the serum creatinine
bull Although the serum creatinine is widely used in diagnosing the presence of AKI it is a suboptimal biomarker
bull It is a lagging marker of change in kidney function therefore it has poor sensitivity for the early diagnosis of AKI and it is unable to differentiate among the various causes of AKI
bull The rise in serum creatinine is slow following the onset of AKI
bull By the time a change is observed in the serum creatinine a critical therapeutic window may have been missed particularly among those with ATN
bull A number of factors may contribute to a lag in rise of serum creatinine after AKI including dilutional effect of fluid administration and decrease in creatinine generation
bull novel biomarkers are potential to reflect physiologic and pathophysiologic processes of the injured kidney
bull Some biomarkers are detected in the urine of patients without a diagnostic increase in serum creatinine which defines a group of patients with subclinical AKI who are at risk for adverse outcomes
bull Biomarkers are used in clinical investigation to facilitate early randomization to different treatment arms
bull For instance sepsis-associated AKI may have a biomarker profile that is distinctly different from that of nephrotoxin-associated AKI
bull Clinicians need tools that are not influenced by other clinical parameters or patient characteristics and that can identify losses in GFR soon after occurence
bull the ideal biomarker of AKI would be a substance that the kidney releases immediately in response to injury and that can be detected in the blood or urine without significant metabolism
bull This biomarker would be highly sensitive and specific for injury to the kidney
bull Novel AKI biomarkers would be detect injury prior to changes in kidney function and potentially to aid in the differential diagnosis of AKI
Traditional biomarkers
Urine output
bull Urine output (UO) in AKI can vary from states of oliguria (lt400 mL24 h) to anuria (lt100 mL24 h) to extreme polyuria
bull While severe AKI can exist despite normal UO changes in UO can occur long before any biochemicalchanges are apparent As such UO is one of the criteria for defining AKI
bull UO often decreases before serum creatinine (SCr) concentration increases making it a more time-sensitive marker of GFR
bull However UO is not nearly as specific for GFR While it is true that if there is no UO in the absence of obstruction there can be no GFR not all reductions in UO signal AKI
bull Furthermore while sustained oliguria is invariably associated with AKI the timeliness of UO as an early indicator is lost in this case
Urine dipstick and microscopic examination
bull Routine dipstick and microscopic examinations of urine are often helpful in determining the cause of AKI
bull While granular or epithelial casts in urine are increased in acute tubular necrosis (ATN) they lack sufficient sensitivity specificity and predictive power for routine clinical use
Urinary indices
bull Diagnostic urinary indices of AKI are the fractional excretion of sodium (FENa) urea (FEurea) uric acid urine sodium and urine osmolality
bull Reduced effective circulating volume stimulates anti-diuretic hormone (ADH) release which results in increased distal water and urea reabsorption Thus low FEurea (lt35) is more sensitive and specific than FENa in differentiating between prerenal and renal causes of AKI especially when diuretics have been administered
bull FEurea and FENa have low diagnostic sensitivity in distinguishing azotemia associated with renal vasoconstriction and intact tubular function from established AKI with tubular dysfunction
Urinary tubular enzymes
bull Traditional urinary biomarkers including low- and high-molecular-weight proteins (a1-microglobulin b2- microglobulin retinol-binding proteins) brush border antigens (NaH exchanger isoform-3) urinary enzymes (a-glutathione S-transferase c-glutamyl transpeptidase N-acetyl-b-D-glucosaminidase) and Tamm-Horsfallprotein
bull have not entered clinical routine for AKI patients due to the lack of sufficient validation lack of standardized assays
Urinary tubular enzymes
bull Urinary tubular enzymes consist of proximal renal tubular epithelial antigen (HRTE-1) alpha-glutathione S-transferase (alpha-GST) glutamyltranspeptidase(gamma-GT) alanine aminopeptidase (AAP) lactate dehydrogenase (LDH) N-acetyl-beta-glucosaminidase(NAG) and alkaline phosphatase (ALP)
bull Most of these are released from proximal tubular epithelial cells within 12 hours and four days earlier than a detectable rise in serum creatinine
bull No validated cut-off points currently exist to help distinguish prerenal disease from ATN
Urinary low-molecular-weight proteins
bull Alpha1-microglobulin (alpha1-m) beta2-microglobulin (beta2-m) retinol-binding protein (RBP) adenosine deaminase-binding protein (ABP) and urinary cystatin C are urinary lowmolecular- weight proteins
bull They are produced at different sites filtered at the glomerulus and reabsorbed at the proximal tubule with no secretion
bull Although promising prognostically and to help distinguish prerenal disease from ATN increased levels may be observed after reversible and mild dysfunction and may not necessarily be associated with persistent or irreversible damage
Functional biomarkersSerum creatinine
bull Currently the standard diagnostic tools for AKI detection are SCrconcentration and UO both of which are markers of renal function but not kidney injury
bull SCr is an integrator of various intra- and extra-renal functions and its concentration indicates the balance between creatinine generation and excretion
bull Unfortunately due to the non-linear relationship between GFR and sCr the increase of creatinine may be within the reference range in early phase of AKI and may overlooked
bull SCr does not indicate the severity of the injury until a steady state has been reached in AKI Therefore SCr is a delayed and insensitive biomarker of changes in kidney function moreover its concentration does not differentiate between structural kidney damage and functional hemodynamic triggers and it could be affected by many factors
bull Especially in intensive care unit patients creatinine-based definitions of AKI can be influenced by baseline creatinine estimation fluid overload malnourishment and muscle wasting
Cystatin-C
bull Cystatin-C is produced at a constant rate by nucleated cells filtered by the glomerular cells almost completely reabsorbed and catabolized (but not secreted) in the proximal tubule It is a polypeptide chain with 120 amino acid residues
bull In this way some of the limitations of serum creatinine effect of muscle mass diet gender and tubular secretion may not be a problem with cystatin C and appear to rise one to two days earlier than serum creatinine
bull Cystatin C is better marker of GFR than serum creatinine as demonstrated in several studies
bull Over the past decade Cystatin C (CyC) a serum measure of renal function is a stronger predictor of the risk of death and cardiovascular events in elderly persons than is creatinine
bull Koyner et al demonstrated that urinary CyC was superior to SCr and plasma CyC in the early diagnosis of acute kidney injury following adult cardiac surgery
bull Roos et al performed a systematic review comparing the diagnostic accuracy of plasma and urine CyC with SCr in patients undergoing cardiac surgery They concluded that the diagnostic accuracy for impaired renal function favors urine CyC
bull However while Cys-C levels are a more precise indicator of kidney function than SCr concentration they seem to be influenced by old age large doses of corticosteroids hyperthyroidism inflammation neoplasia smoking and alcohol consumption
bull Currently it is unclear whether the value of Cys-C is generalizable to all forms of AKI or specific to particular populations
Damage biomarkers
Neutrophil Gelatinase-Associated Lipocalin(NGAL)
bull Human NGAL is a 25 kDa protein firstly identified bound to gelatinase in specific granules of the neutrophil NGAL is a critical component of innate immunity to bacterial infection and is expressed by immune cells hepatocytes and renal tubular cells in various disease states
bull Its resistance to proteolysis further enhanced potential suitability as a clinical biomarker
bull In healthy kidneys it is barel detectable in either plasma or urine
bull However in the setting of acute tubular injury NGAL undergoes rapid and profound upregulation with large increases in both urine and plasma
bull Distinct from traditional markers of function such as creatinine this rapid response enables NGAL to potentially identify injured kidney much earlier than was previously possible The endogenous role of NGAL remains unclear It seems to be involved with iron transportation to and from the proximal tubular epithelial cells and animal studies demonstrate a renoprotective effect of exogenously administered NGAL in the setting of acute ischemic injury
bull NGAL was also detected in the urine of mice in the early stage of cisplatin-induced nephrotoxicity
bull These animal studies demonstrated that NGAL may represent an early sensitive and noninvasive urinary biomarker for ischemic and nephrotoxic kidney injury
bull NGAL is markedly upregulated and abundantly expressed in the kidney after renal ischemia
bull In this setting NGAL may function to dampen toxicity by reducing apoptosis and increasing the normal proliferation of kidney tubule cells
bull following ischemia reperfusion as evidenced by a rise in creatinine the kidneys illuminate indicating NGAL production at the site of injury
bull Interestingly following maneuvers that lead to significant prerenal disease there was no NGAL illumination indicating that prerenal disease does not induce NGAL expression
bull Thus NGAL may potentially be useful in differentiating prerenal disease from ATN
bull In these studies the average sensitivity and specificity of NGAL measured one to three days prior to AKI diagnosis was 76 and 77 percent respectively for cardiac surgery patients and 73 and 80 percent respectively for patients admitted to the intensive care unit (ICU)
bull NGAL may also represent early sensitive biomarker of AKI after contrast administrations for coronary angiography
bull NGAL was measured in the serum and urine before and at 2 4 12 24 and 48 h after contrast administration they found a significant rise in serum NGAL 2 and 4 h after PCI and a rise in urinary NGAL 4 and 12 h after PCI
bull A similar study of 25 patients with normal serum creatinine undergoing PCI due to unstable angina There was a significant rise in serum NGAL after 2 and 4 hours Urinary NGAL and urinary L-FABP followed the same pattern Both markers increased significantly after 4 hours and remained elevated up to 48 hours after PCI
bull Urine and plasma NGAL levels also represent early biomarkers of AKI in ICU
bull A multicenter study of serum NGAL was performed in 143 critically ill children with systemic inflammatory response syndrome (SIRS) or septic shock during the first 24 h of admission to the ICU there was a significant difference in serum NGAL between healthy children ill children with SIRS and septic shock the study was concluded that serum NGAL is a highly sensitive but nonspecific predictor of acute kidney injury in critically ill children with septic shock
bull A 2010 study evaluated 88 ICU patient and found that an NGAL level of ge150 nmolL predicted AKI with 82 sensitivity and 97 specificity
bull A recent study had 98 patients who were divided in two groups depending on the presence of sepsis Fifty-six patients had sepsis while forty-two patients were nonseptic Among septic patients subjects who developed AKI showed signi1048853 cant higher levels of NGAL
bull A more study of 65 patients with septic shock were found that urine NGAL levels 12 hours before AKI diagnosis were a good predictor of AKI
Kidney Injury Molecule-1 (KIM-1)
bull KIM-1 mRNA and protein are expressed at a low level in normal kidney but are increased dramatically in postischemic kidney
bull KIM-1 has been identified as the first nonmyeloidphosphatidylserine receptor that confers a phagocytic phenotype on injured epithelial cells both in vivo and in vitro
bull Urinary KIM-1 has been found to be an early indicator of AKI that compares favorably to a number of conventional biomarkers and tubular enzymes
bull KIM-1 is also a tissue and urinary biomarker for nephrotoxicant-induced kidney injury
bull Tissue and urinary expressions were measured with different nephrotoxic doses of cisplatin folic acide cadmium gentamycin mercury
bull As early as 1 day after cisplatin treatment positive KIM- 1 immunostaining observed in the outer medulla of the kidney and changes in urinary clusterin indicated the onset of proximal tubular injury in the absence of functional effects
bull Tissue KIM-1 was the most sensitive biomarker for detection of cisplatin-induced kidney damage
bull KIM-1 is a biomarker of AKI in humans bull Urine samples were collected from 32 patients with various
acute and chronic kidney diseases as well as from eight normal controls there was extensive expression of KIM-1 in proximal tubule cells in kidney biopsies from six patients with biopsy confirmed acute tubular necrosis (ATN)
bull Urinary KIM-1 levels were significantly higher in patients with ischemic ATN compared to levels in patients with other forms of acute renal failure or chronic renal disease
bull Adjusted for age gender and length of time delay between the initial insult and sampling of the urine a one-unit increase in normalized KIM-1 was associated with a greater than 12-fold risk for the presence of ATN
bull In hospital patients with AKI urinary levels of KIM-1 that higher levels correlated with a higher odds ratio for dialysis requirement or hospital death
bull this study demonstrated that urinary biomarker of AKI such as KIM-1 can predict adverse clinical outcomes in patients with AKI
bull Both renal and urinary KIM-1 correlate with kidney damage and negatively with renal function but not with proteinuria
bull A recent study has explored urinary KIM-1correlated with kidney function in kidney allograft recipients Kidney transplant recipients showed significantly higher KIM-1 values than the healthy volunteers this study concluded that even a successful kidney transplantation is associated with kidney injury as reflected by elevated urinary KIM-1
bull A rapid direct 15-minute assay for the detection of urinary human KIM-1 has been developed Using this assay more urinary KIM-1 was detected in the urine of patients with AKI than in the urine from healthy volunteers
Urinary interleukin-18
bull Interleukin18 (IL-18) is a 22 kDa pro-inflammatory cytokine that increases in the kidney after ischemia-reperfusion injury in a caspase- 1-dependent manner
bull Patients with ATN had significantly greater urinary IL-18 concentrations than those with other conditions (healthy controls patients with pre-renal azotemia urinary tract infection CKD and nephrotic syndrome)
bull urinary IL-18 concentrations measured in the first 24 h after kidney transplantation were higher in patients who received a cadaveric kidney that developed delayed graft function compared to patients who received a cadaveric kidney with prompt graft function and patients who received a kidney with prompt graft function from a living donor
bull However the performance of urinary IL-18 measured 1 day before AKI was modest
bull Its predictive utility for AKI following cardiac surgery could not be demonstrated in one prospective observational study of 100 adult patients
bull In addition in a large study population of 1439 critically ill patients IL-18 had a poor-to-moderate ability to predict AKI renal replacement therapy (RRT) or 90-day mortality
Liver-Type Fatty Acid Binding Protein(L-FABP)
bull Liver-type fatty acid-binding protein (L-FABP) is a 14 kDa protein from the large super- family of lipidbinding proteins
bull The 14-kD L-FABP protein can be localized predominantly in the proximal tubule
bull Noiri et al demonstrated that increase of urinary L-FABP was observed at 1 h after ischemia even in the 5-min IRI group and urinary L-FABP was superior to BUN and urinary NAG for early and accurate detection of acute tubular necrosis in different models of animal AKI
bull urinary L-FABP may be a promising biomarker for early detection of AKI and prediction of dialysis requirement and in-hospital mortality
bull Urinary excretion of urinary liver-type fatty acid-binding protein (L-FABP) reflects stress of proximal tubular epithelial cells and correlates with severity of ischemic tubular injury
bull A meta-analysis of 15 prospective cohort studies demonstrated that in hospitalndashbased cohorts of patients at risk of AKI L-FABP can discriminate for the diagnosis of AKI and predict the need for dialysis and in-hospital mortality
bull It was correlated with the degree of tubulointerstitial damage in a folic acid induced nephropathy
bull In ischemic and cisplatin-induced AKI L-FABP was increased in the urine before the increase in BUN
bull In cisplatin-induced AKI urinary L-FABP levels increased exponentially even in the lowest dose group as early as 2 hours whereas BUN levels increased at 48 hours
bull L-FABP was measured in 80 critically ill patients Urinary L-FABP levels in patients with septic shock were significantly higher than severe sepsis without shock Serum L-FABP levels did not have significant differences between patients with septic shock severe sepsis and healthy
bull Another study was evaluated 145 septic shock patients complicated with established AKI Urinary L-FABP measured at admission was significantly higher in the nonsurvivors of septic shock with established acute kidney injury than in the survivors
Failure of the TRIBE-AKI study
bull The Translational Research Investigating Biomarker Endpoints in AKI (TRIBE-AKI) study evaluated the performance of urinary c-glutamyltranspeptidase ( c-GTP) alkaline phosphatase NGAL Cys-C KIM-1 and IL-18 in AKI diagnosis
bull The results of four novel urine biomarkers and one plasma biomarker (urine NGAL IL-18 KIM-1 and L-FABP and plasma NGAL) were provided Of all the novel biomarkers only urine IL-18 and plasma NGAL in adults were helpful in predicting progression of AKI when measured on the day of clinical AKI diagnosis
bull Combinations of three biomarkers in adults from two different time points and combinations of two biomarkers in children from two time points were found to be able to increase the ROC for AKI up to 078
bull In summary the clinical use of single damage biomarkers in AKI prediction remains unclear because large prospective multicenter trials such as the TRIBE-AKI study (nfrac141530) have failed to demonstrate troponin-like diagnostic performance
Various clinical scenarios of AKI based onfunction damage and stress
bull Over the last decade a number of novel damage biomarkers have been evaluated for their capacity to detect kidney damage and predict the development of AKI However the relationship between decreasing function and increasing damage is not as straightforward as might be assumed
bull The characteristic pattern whereby damage precedes loss of function (panel A) may be seen in some cases of AKI and affords an opportunity to detect ldquosubclinicalrdquo AKI before function start to fall Unfortunately other patterns might also occur For example functional decline may start to occur alongside damage (panel B) and in some cases function may start to decline even before damage (panel C)
bull This makes damage markers difficult to use for predicting AKI However other markers might actually measure the ldquostressrdquo occurring at the cellular level before damage or loss of function
Paradigm shift to pre-injury phase biomarkers
bull Katz et al proposed that the pre-injury phase that leads to AKI can be described as ldquoacute kidney stressrdquo (AKS) after the report of the identification of cell cycle arrest biomarkers that signal the potential development of AKI is part of an evolution in the molecular diagnosis and understanding of AKI
bull These biomarkers are released by kidney cells along a path which may lead to AKI during a pre-injury phase
bull AKS is defined as the increased-risk phase (pre-injury phase) that leads to AKI
bull This ldquoAKSrdquo may or may not lead to damage and functional declinebull But it is the earliest possible the process of AKI can be detected
Pre-injury phase biomarkers
Stress biomarkersbull In 2013 Kashani et al reported the results of a prospective international
observational investigation (the Sapphire study) of tissue inhibitor of metalloproteinases- 2 (TIMP-2) and insulin-like growth factor-binding protein 7 (IGFBP7) in a heterogeneous group of critically ill patients [TIMP-2][IGFBP7] was significantly superior to all previously described markers of AKI (plt0002)
bull Next the Opal and Topaz study showed the cut-off value and risk assessment using the urinary[TIMP-2] [IGFBP7]
bull The urine [IGFBP7][TIMP2] biomarker is already FDA approved and commercially available in the United States
bull Falsepositive results are common and they will be magnified if the test is used inappropriately in low-risk patients In addition this biomarker should not be used in ambulatory practices and it is not beneficial in patients with established AKI
microRNAsbull microRNAs (miRNAs) are endogenous single-stranded non-coding
mRNAs of about 19-23 nucleotides bull In the past years researchers have begun to investigate the
relevance of miRNAs to AKI with many miRNAs being implicated bull Some of them contribute to pathogenesis by regulating apoptosis
and inflammation amplifying or reducing acute injury responses while others regulate fibrosis and angiogenesis participating in renal recovery or progression to fibrosis
bull Certain miRNAs have been investigated for their potential as novel biomarkers for the early detection or prognostication of AKI
Hemojuvelinbull Hemojuvelin (HJV) a glycophosphatidylinositol (GPI)- linked
membrane protein is highly expressed in liver and skeletal musclesbull The molecular weight of HJV is 42 kDa for the soluble form (sHJV)
and can be passed through glomerular filtration and reabsorbed by the renal tubules Increased iron content in the kidney and urine is observed in human and animal models of AKI and increased iron load can induce renal tubular cell injury
bull There is evidence that the increased expression of the hemojuvelin-hepcidin ferroportin pathway is an intrinsic response to iron overload conditions during AKI
bull Therefore urine HJV (uHJV) has the potential to be an early AKI biomarker in response to iron homeostasis during AKI
Combination of functional and damage biomarkers
bull While new biomarkers are being validated functional biomarkers (serum creatinine serum urea and urine output) continue to be utilized in the diagnosis and staging of AKI In the future existing or newer damage biomarkers will likely be combined with the use of functional biomarkers to enhance the ability of RIFLE AKIN
bull A study of 345 children after cardiopulmonary bypass surgery demonstrated that the composite of functional biomarker such as plasma cystatin C and urinary NGAL was superior to changes in serum creatinine to predict AKI
PROGNOSTIC BIOMARKERS
bull Most of the biomarkers described above allow early detection of acute kidney injury but do not predict severe AKI
Urinary renin and angiotensinogen
bull Urinary renin angiotensinogen and plasma NGAL may predict the development of severe AKI
bull Among 99 consecutively enrolled patients who developed AKI the ratio of urinary angiotensinogen to urinary creatinine (uAnCR expressed as ng per mg creatinine)calculated Patients with the highest uAnCR had a higher risk of worsening AKI compared with patients with the lowest uAnCR An elevated uAnCR predicted a longer hospital stay
bull Among 204 patients who developed Acute Kidney Injury Network (AKIN) stage 1 following cardiac surgery the urinary renin-to-creatinine ratio and the angiotensinogen-to-creatinine ratio predicted a composite outcome of death or AKIN stage 3 or death
Plasma NGAL
bull In a prospective cohort study in which 616 patients admitted from the emergency department were classified by clinical criteria as AKI transient azotemia stable CKD or normal kidney function plasma NGAL discriminated AKI from normal function and from transient azotemia
bull Higher concentrations of NGAL were associated with more severe AKI
Thanks for your attention

bull The rise in serum creatinine is slow following the onset of AKI
bull By the time a change is observed in the serum creatinine a critical therapeutic window may have been missed particularly among those with ATN
bull A number of factors may contribute to a lag in rise of serum creatinine after AKI including dilutional effect of fluid administration and decrease in creatinine generation
bull novel biomarkers are potential to reflect physiologic and pathophysiologic processes of the injured kidney
bull Some biomarkers are detected in the urine of patients without a diagnostic increase in serum creatinine which defines a group of patients with subclinical AKI who are at risk for adverse outcomes
bull Biomarkers are used in clinical investigation to facilitate early randomization to different treatment arms
bull For instance sepsis-associated AKI may have a biomarker profile that is distinctly different from that of nephrotoxin-associated AKI
bull Clinicians need tools that are not influenced by other clinical parameters or patient characteristics and that can identify losses in GFR soon after occurence
bull the ideal biomarker of AKI would be a substance that the kidney releases immediately in response to injury and that can be detected in the blood or urine without significant metabolism
bull This biomarker would be highly sensitive and specific for injury to the kidney
bull Novel AKI biomarkers would be detect injury prior to changes in kidney function and potentially to aid in the differential diagnosis of AKI
Traditional biomarkers
Urine output
bull Urine output (UO) in AKI can vary from states of oliguria (lt400 mL24 h) to anuria (lt100 mL24 h) to extreme polyuria
bull While severe AKI can exist despite normal UO changes in UO can occur long before any biochemicalchanges are apparent As such UO is one of the criteria for defining AKI
bull UO often decreases before serum creatinine (SCr) concentration increases making it a more time-sensitive marker of GFR
bull However UO is not nearly as specific for GFR While it is true that if there is no UO in the absence of obstruction there can be no GFR not all reductions in UO signal AKI
bull Furthermore while sustained oliguria is invariably associated with AKI the timeliness of UO as an early indicator is lost in this case
Urine dipstick and microscopic examination
bull Routine dipstick and microscopic examinations of urine are often helpful in determining the cause of AKI
bull While granular or epithelial casts in urine are increased in acute tubular necrosis (ATN) they lack sufficient sensitivity specificity and predictive power for routine clinical use
Urinary indices
bull Diagnostic urinary indices of AKI are the fractional excretion of sodium (FENa) urea (FEurea) uric acid urine sodium and urine osmolality
bull Reduced effective circulating volume stimulates anti-diuretic hormone (ADH) release which results in increased distal water and urea reabsorption Thus low FEurea (lt35) is more sensitive and specific than FENa in differentiating between prerenal and renal causes of AKI especially when diuretics have been administered
bull FEurea and FENa have low diagnostic sensitivity in distinguishing azotemia associated with renal vasoconstriction and intact tubular function from established AKI with tubular dysfunction
Urinary tubular enzymes
bull Traditional urinary biomarkers including low- and high-molecular-weight proteins (a1-microglobulin b2- microglobulin retinol-binding proteins) brush border antigens (NaH exchanger isoform-3) urinary enzymes (a-glutathione S-transferase c-glutamyl transpeptidase N-acetyl-b-D-glucosaminidase) and Tamm-Horsfallprotein
bull have not entered clinical routine for AKI patients due to the lack of sufficient validation lack of standardized assays
Urinary tubular enzymes
bull Urinary tubular enzymes consist of proximal renal tubular epithelial antigen (HRTE-1) alpha-glutathione S-transferase (alpha-GST) glutamyltranspeptidase(gamma-GT) alanine aminopeptidase (AAP) lactate dehydrogenase (LDH) N-acetyl-beta-glucosaminidase(NAG) and alkaline phosphatase (ALP)
bull Most of these are released from proximal tubular epithelial cells within 12 hours and four days earlier than a detectable rise in serum creatinine
bull No validated cut-off points currently exist to help distinguish prerenal disease from ATN
Urinary low-molecular-weight proteins
bull Alpha1-microglobulin (alpha1-m) beta2-microglobulin (beta2-m) retinol-binding protein (RBP) adenosine deaminase-binding protein (ABP) and urinary cystatin C are urinary lowmolecular- weight proteins
bull They are produced at different sites filtered at the glomerulus and reabsorbed at the proximal tubule with no secretion
bull Although promising prognostically and to help distinguish prerenal disease from ATN increased levels may be observed after reversible and mild dysfunction and may not necessarily be associated with persistent or irreversible damage
Functional biomarkersSerum creatinine
bull Currently the standard diagnostic tools for AKI detection are SCrconcentration and UO both of which are markers of renal function but not kidney injury
bull SCr is an integrator of various intra- and extra-renal functions and its concentration indicates the balance between creatinine generation and excretion
bull Unfortunately due to the non-linear relationship between GFR and sCr the increase of creatinine may be within the reference range in early phase of AKI and may overlooked
bull SCr does not indicate the severity of the injury until a steady state has been reached in AKI Therefore SCr is a delayed and insensitive biomarker of changes in kidney function moreover its concentration does not differentiate between structural kidney damage and functional hemodynamic triggers and it could be affected by many factors
bull Especially in intensive care unit patients creatinine-based definitions of AKI can be influenced by baseline creatinine estimation fluid overload malnourishment and muscle wasting
Cystatin-C
bull Cystatin-C is produced at a constant rate by nucleated cells filtered by the glomerular cells almost completely reabsorbed and catabolized (but not secreted) in the proximal tubule It is a polypeptide chain with 120 amino acid residues
bull In this way some of the limitations of serum creatinine effect of muscle mass diet gender and tubular secretion may not be a problem with cystatin C and appear to rise one to two days earlier than serum creatinine
bull Cystatin C is better marker of GFR than serum creatinine as demonstrated in several studies
bull Over the past decade Cystatin C (CyC) a serum measure of renal function is a stronger predictor of the risk of death and cardiovascular events in elderly persons than is creatinine
bull Koyner et al demonstrated that urinary CyC was superior to SCr and plasma CyC in the early diagnosis of acute kidney injury following adult cardiac surgery
bull Roos et al performed a systematic review comparing the diagnostic accuracy of plasma and urine CyC with SCr in patients undergoing cardiac surgery They concluded that the diagnostic accuracy for impaired renal function favors urine CyC
bull However while Cys-C levels are a more precise indicator of kidney function than SCr concentration they seem to be influenced by old age large doses of corticosteroids hyperthyroidism inflammation neoplasia smoking and alcohol consumption
bull Currently it is unclear whether the value of Cys-C is generalizable to all forms of AKI or specific to particular populations
Damage biomarkers
Neutrophil Gelatinase-Associated Lipocalin(NGAL)
bull Human NGAL is a 25 kDa protein firstly identified bound to gelatinase in specific granules of the neutrophil NGAL is a critical component of innate immunity to bacterial infection and is expressed by immune cells hepatocytes and renal tubular cells in various disease states
bull Its resistance to proteolysis further enhanced potential suitability as a clinical biomarker
bull In healthy kidneys it is barel detectable in either plasma or urine
bull However in the setting of acute tubular injury NGAL undergoes rapid and profound upregulation with large increases in both urine and plasma
bull Distinct from traditional markers of function such as creatinine this rapid response enables NGAL to potentially identify injured kidney much earlier than was previously possible The endogenous role of NGAL remains unclear It seems to be involved with iron transportation to and from the proximal tubular epithelial cells and animal studies demonstrate a renoprotective effect of exogenously administered NGAL in the setting of acute ischemic injury
bull NGAL was also detected in the urine of mice in the early stage of cisplatin-induced nephrotoxicity
bull These animal studies demonstrated that NGAL may represent an early sensitive and noninvasive urinary biomarker for ischemic and nephrotoxic kidney injury
bull NGAL is markedly upregulated and abundantly expressed in the kidney after renal ischemia
bull In this setting NGAL may function to dampen toxicity by reducing apoptosis and increasing the normal proliferation of kidney tubule cells
bull following ischemia reperfusion as evidenced by a rise in creatinine the kidneys illuminate indicating NGAL production at the site of injury
bull Interestingly following maneuvers that lead to significant prerenal disease there was no NGAL illumination indicating that prerenal disease does not induce NGAL expression
bull Thus NGAL may potentially be useful in differentiating prerenal disease from ATN
bull In these studies the average sensitivity and specificity of NGAL measured one to three days prior to AKI diagnosis was 76 and 77 percent respectively for cardiac surgery patients and 73 and 80 percent respectively for patients admitted to the intensive care unit (ICU)
bull NGAL may also represent early sensitive biomarker of AKI after contrast administrations for coronary angiography
bull NGAL was measured in the serum and urine before and at 2 4 12 24 and 48 h after contrast administration they found a significant rise in serum NGAL 2 and 4 h after PCI and a rise in urinary NGAL 4 and 12 h after PCI
bull A similar study of 25 patients with normal serum creatinine undergoing PCI due to unstable angina There was a significant rise in serum NGAL after 2 and 4 hours Urinary NGAL and urinary L-FABP followed the same pattern Both markers increased significantly after 4 hours and remained elevated up to 48 hours after PCI
bull Urine and plasma NGAL levels also represent early biomarkers of AKI in ICU
bull A multicenter study of serum NGAL was performed in 143 critically ill children with systemic inflammatory response syndrome (SIRS) or septic shock during the first 24 h of admission to the ICU there was a significant difference in serum NGAL between healthy children ill children with SIRS and septic shock the study was concluded that serum NGAL is a highly sensitive but nonspecific predictor of acute kidney injury in critically ill children with septic shock
bull A 2010 study evaluated 88 ICU patient and found that an NGAL level of ge150 nmolL predicted AKI with 82 sensitivity and 97 specificity
bull A recent study had 98 patients who were divided in two groups depending on the presence of sepsis Fifty-six patients had sepsis while forty-two patients were nonseptic Among septic patients subjects who developed AKI showed signi1048853 cant higher levels of NGAL
bull A more study of 65 patients with septic shock were found that urine NGAL levels 12 hours before AKI diagnosis were a good predictor of AKI
Kidney Injury Molecule-1 (KIM-1)
bull KIM-1 mRNA and protein are expressed at a low level in normal kidney but are increased dramatically in postischemic kidney
bull KIM-1 has been identified as the first nonmyeloidphosphatidylserine receptor that confers a phagocytic phenotype on injured epithelial cells both in vivo and in vitro
bull Urinary KIM-1 has been found to be an early indicator of AKI that compares favorably to a number of conventional biomarkers and tubular enzymes
bull KIM-1 is also a tissue and urinary biomarker for nephrotoxicant-induced kidney injury
bull Tissue and urinary expressions were measured with different nephrotoxic doses of cisplatin folic acide cadmium gentamycin mercury
bull As early as 1 day after cisplatin treatment positive KIM- 1 immunostaining observed in the outer medulla of the kidney and changes in urinary clusterin indicated the onset of proximal tubular injury in the absence of functional effects
bull Tissue KIM-1 was the most sensitive biomarker for detection of cisplatin-induced kidney damage
bull KIM-1 is a biomarker of AKI in humans bull Urine samples were collected from 32 patients with various
acute and chronic kidney diseases as well as from eight normal controls there was extensive expression of KIM-1 in proximal tubule cells in kidney biopsies from six patients with biopsy confirmed acute tubular necrosis (ATN)
bull Urinary KIM-1 levels were significantly higher in patients with ischemic ATN compared to levels in patients with other forms of acute renal failure or chronic renal disease
bull Adjusted for age gender and length of time delay between the initial insult and sampling of the urine a one-unit increase in normalized KIM-1 was associated with a greater than 12-fold risk for the presence of ATN
bull In hospital patients with AKI urinary levels of KIM-1 that higher levels correlated with a higher odds ratio for dialysis requirement or hospital death
bull this study demonstrated that urinary biomarker of AKI such as KIM-1 can predict adverse clinical outcomes in patients with AKI
bull Both renal and urinary KIM-1 correlate with kidney damage and negatively with renal function but not with proteinuria
bull A recent study has explored urinary KIM-1correlated with kidney function in kidney allograft recipients Kidney transplant recipients showed significantly higher KIM-1 values than the healthy volunteers this study concluded that even a successful kidney transplantation is associated with kidney injury as reflected by elevated urinary KIM-1
bull A rapid direct 15-minute assay for the detection of urinary human KIM-1 has been developed Using this assay more urinary KIM-1 was detected in the urine of patients with AKI than in the urine from healthy volunteers
Urinary interleukin-18
bull Interleukin18 (IL-18) is a 22 kDa pro-inflammatory cytokine that increases in the kidney after ischemia-reperfusion injury in a caspase- 1-dependent manner
bull Patients with ATN had significantly greater urinary IL-18 concentrations than those with other conditions (healthy controls patients with pre-renal azotemia urinary tract infection CKD and nephrotic syndrome)
bull urinary IL-18 concentrations measured in the first 24 h after kidney transplantation were higher in patients who received a cadaveric kidney that developed delayed graft function compared to patients who received a cadaveric kidney with prompt graft function and patients who received a kidney with prompt graft function from a living donor
bull However the performance of urinary IL-18 measured 1 day before AKI was modest
bull Its predictive utility for AKI following cardiac surgery could not be demonstrated in one prospective observational study of 100 adult patients
bull In addition in a large study population of 1439 critically ill patients IL-18 had a poor-to-moderate ability to predict AKI renal replacement therapy (RRT) or 90-day mortality
Liver-Type Fatty Acid Binding Protein(L-FABP)
bull Liver-type fatty acid-binding protein (L-FABP) is a 14 kDa protein from the large super- family of lipidbinding proteins
bull The 14-kD L-FABP protein can be localized predominantly in the proximal tubule
bull Noiri et al demonstrated that increase of urinary L-FABP was observed at 1 h after ischemia even in the 5-min IRI group and urinary L-FABP was superior to BUN and urinary NAG for early and accurate detection of acute tubular necrosis in different models of animal AKI
bull urinary L-FABP may be a promising biomarker for early detection of AKI and prediction of dialysis requirement and in-hospital mortality
bull Urinary excretion of urinary liver-type fatty acid-binding protein (L-FABP) reflects stress of proximal tubular epithelial cells and correlates with severity of ischemic tubular injury
bull A meta-analysis of 15 prospective cohort studies demonstrated that in hospitalndashbased cohorts of patients at risk of AKI L-FABP can discriminate for the diagnosis of AKI and predict the need for dialysis and in-hospital mortality
bull It was correlated with the degree of tubulointerstitial damage in a folic acid induced nephropathy
bull In ischemic and cisplatin-induced AKI L-FABP was increased in the urine before the increase in BUN
bull In cisplatin-induced AKI urinary L-FABP levels increased exponentially even in the lowest dose group as early as 2 hours whereas BUN levels increased at 48 hours
bull L-FABP was measured in 80 critically ill patients Urinary L-FABP levels in patients with septic shock were significantly higher than severe sepsis without shock Serum L-FABP levels did not have significant differences between patients with septic shock severe sepsis and healthy
bull Another study was evaluated 145 septic shock patients complicated with established AKI Urinary L-FABP measured at admission was significantly higher in the nonsurvivors of septic shock with established acute kidney injury than in the survivors
Failure of the TRIBE-AKI study
bull The Translational Research Investigating Biomarker Endpoints in AKI (TRIBE-AKI) study evaluated the performance of urinary c-glutamyltranspeptidase ( c-GTP) alkaline phosphatase NGAL Cys-C KIM-1 and IL-18 in AKI diagnosis
bull The results of four novel urine biomarkers and one plasma biomarker (urine NGAL IL-18 KIM-1 and L-FABP and plasma NGAL) were provided Of all the novel biomarkers only urine IL-18 and plasma NGAL in adults were helpful in predicting progression of AKI when measured on the day of clinical AKI diagnosis
bull Combinations of three biomarkers in adults from two different time points and combinations of two biomarkers in children from two time points were found to be able to increase the ROC for AKI up to 078
bull In summary the clinical use of single damage biomarkers in AKI prediction remains unclear because large prospective multicenter trials such as the TRIBE-AKI study (nfrac141530) have failed to demonstrate troponin-like diagnostic performance
Various clinical scenarios of AKI based onfunction damage and stress
bull Over the last decade a number of novel damage biomarkers have been evaluated for their capacity to detect kidney damage and predict the development of AKI However the relationship between decreasing function and increasing damage is not as straightforward as might be assumed
bull The characteristic pattern whereby damage precedes loss of function (panel A) may be seen in some cases of AKI and affords an opportunity to detect ldquosubclinicalrdquo AKI before function start to fall Unfortunately other patterns might also occur For example functional decline may start to occur alongside damage (panel B) and in some cases function may start to decline even before damage (panel C)
bull This makes damage markers difficult to use for predicting AKI However other markers might actually measure the ldquostressrdquo occurring at the cellular level before damage or loss of function
Paradigm shift to pre-injury phase biomarkers
bull Katz et al proposed that the pre-injury phase that leads to AKI can be described as ldquoacute kidney stressrdquo (AKS) after the report of the identification of cell cycle arrest biomarkers that signal the potential development of AKI is part of an evolution in the molecular diagnosis and understanding of AKI
bull These biomarkers are released by kidney cells along a path which may lead to AKI during a pre-injury phase
bull AKS is defined as the increased-risk phase (pre-injury phase) that leads to AKI
bull This ldquoAKSrdquo may or may not lead to damage and functional declinebull But it is the earliest possible the process of AKI can be detected
Pre-injury phase biomarkers
Stress biomarkersbull In 2013 Kashani et al reported the results of a prospective international
observational investigation (the Sapphire study) of tissue inhibitor of metalloproteinases- 2 (TIMP-2) and insulin-like growth factor-binding protein 7 (IGFBP7) in a heterogeneous group of critically ill patients [TIMP-2][IGFBP7] was significantly superior to all previously described markers of AKI (plt0002)
bull Next the Opal and Topaz study showed the cut-off value and risk assessment using the urinary[TIMP-2] [IGFBP7]
bull The urine [IGFBP7][TIMP2] biomarker is already FDA approved and commercially available in the United States
bull Falsepositive results are common and they will be magnified if the test is used inappropriately in low-risk patients In addition this biomarker should not be used in ambulatory practices and it is not beneficial in patients with established AKI
microRNAsbull microRNAs (miRNAs) are endogenous single-stranded non-coding
mRNAs of about 19-23 nucleotides bull In the past years researchers have begun to investigate the
relevance of miRNAs to AKI with many miRNAs being implicated bull Some of them contribute to pathogenesis by regulating apoptosis
and inflammation amplifying or reducing acute injury responses while others regulate fibrosis and angiogenesis participating in renal recovery or progression to fibrosis
bull Certain miRNAs have been investigated for their potential as novel biomarkers for the early detection or prognostication of AKI
Hemojuvelinbull Hemojuvelin (HJV) a glycophosphatidylinositol (GPI)- linked
membrane protein is highly expressed in liver and skeletal musclesbull The molecular weight of HJV is 42 kDa for the soluble form (sHJV)
and can be passed through glomerular filtration and reabsorbed by the renal tubules Increased iron content in the kidney and urine is observed in human and animal models of AKI and increased iron load can induce renal tubular cell injury
bull There is evidence that the increased expression of the hemojuvelin-hepcidin ferroportin pathway is an intrinsic response to iron overload conditions during AKI
bull Therefore urine HJV (uHJV) has the potential to be an early AKI biomarker in response to iron homeostasis during AKI
Combination of functional and damage biomarkers
bull While new biomarkers are being validated functional biomarkers (serum creatinine serum urea and urine output) continue to be utilized in the diagnosis and staging of AKI In the future existing or newer damage biomarkers will likely be combined with the use of functional biomarkers to enhance the ability of RIFLE AKIN
bull A study of 345 children after cardiopulmonary bypass surgery demonstrated that the composite of functional biomarker such as plasma cystatin C and urinary NGAL was superior to changes in serum creatinine to predict AKI
PROGNOSTIC BIOMARKERS
bull Most of the biomarkers described above allow early detection of acute kidney injury but do not predict severe AKI
Urinary renin and angiotensinogen
bull Urinary renin angiotensinogen and plasma NGAL may predict the development of severe AKI
bull Among 99 consecutively enrolled patients who developed AKI the ratio of urinary angiotensinogen to urinary creatinine (uAnCR expressed as ng per mg creatinine)calculated Patients with the highest uAnCR had a higher risk of worsening AKI compared with patients with the lowest uAnCR An elevated uAnCR predicted a longer hospital stay
bull Among 204 patients who developed Acute Kidney Injury Network (AKIN) stage 1 following cardiac surgery the urinary renin-to-creatinine ratio and the angiotensinogen-to-creatinine ratio predicted a composite outcome of death or AKIN stage 3 or death
Plasma NGAL
bull In a prospective cohort study in which 616 patients admitted from the emergency department were classified by clinical criteria as AKI transient azotemia stable CKD or normal kidney function plasma NGAL discriminated AKI from normal function and from transient azotemia
bull Higher concentrations of NGAL were associated with more severe AKI
Thanks for your attention

bull novel biomarkers are potential to reflect physiologic and pathophysiologic processes of the injured kidney
bull Some biomarkers are detected in the urine of patients without a diagnostic increase in serum creatinine which defines a group of patients with subclinical AKI who are at risk for adverse outcomes
bull Biomarkers are used in clinical investigation to facilitate early randomization to different treatment arms
bull For instance sepsis-associated AKI may have a biomarker profile that is distinctly different from that of nephrotoxin-associated AKI
bull Clinicians need tools that are not influenced by other clinical parameters or patient characteristics and that can identify losses in GFR soon after occurence
bull the ideal biomarker of AKI would be a substance that the kidney releases immediately in response to injury and that can be detected in the blood or urine without significant metabolism
bull This biomarker would be highly sensitive and specific for injury to the kidney
bull Novel AKI biomarkers would be detect injury prior to changes in kidney function and potentially to aid in the differential diagnosis of AKI
Traditional biomarkers
Urine output
bull Urine output (UO) in AKI can vary from states of oliguria (lt400 mL24 h) to anuria (lt100 mL24 h) to extreme polyuria
bull While severe AKI can exist despite normal UO changes in UO can occur long before any biochemicalchanges are apparent As such UO is one of the criteria for defining AKI
bull UO often decreases before serum creatinine (SCr) concentration increases making it a more time-sensitive marker of GFR
bull However UO is not nearly as specific for GFR While it is true that if there is no UO in the absence of obstruction there can be no GFR not all reductions in UO signal AKI
bull Furthermore while sustained oliguria is invariably associated with AKI the timeliness of UO as an early indicator is lost in this case
Urine dipstick and microscopic examination
bull Routine dipstick and microscopic examinations of urine are often helpful in determining the cause of AKI
bull While granular or epithelial casts in urine are increased in acute tubular necrosis (ATN) they lack sufficient sensitivity specificity and predictive power for routine clinical use
Urinary indices
bull Diagnostic urinary indices of AKI are the fractional excretion of sodium (FENa) urea (FEurea) uric acid urine sodium and urine osmolality
bull Reduced effective circulating volume stimulates anti-diuretic hormone (ADH) release which results in increased distal water and urea reabsorption Thus low FEurea (lt35) is more sensitive and specific than FENa in differentiating between prerenal and renal causes of AKI especially when diuretics have been administered
bull FEurea and FENa have low diagnostic sensitivity in distinguishing azotemia associated with renal vasoconstriction and intact tubular function from established AKI with tubular dysfunction
Urinary tubular enzymes
bull Traditional urinary biomarkers including low- and high-molecular-weight proteins (a1-microglobulin b2- microglobulin retinol-binding proteins) brush border antigens (NaH exchanger isoform-3) urinary enzymes (a-glutathione S-transferase c-glutamyl transpeptidase N-acetyl-b-D-glucosaminidase) and Tamm-Horsfallprotein
bull have not entered clinical routine for AKI patients due to the lack of sufficient validation lack of standardized assays
Urinary tubular enzymes
bull Urinary tubular enzymes consist of proximal renal tubular epithelial antigen (HRTE-1) alpha-glutathione S-transferase (alpha-GST) glutamyltranspeptidase(gamma-GT) alanine aminopeptidase (AAP) lactate dehydrogenase (LDH) N-acetyl-beta-glucosaminidase(NAG) and alkaline phosphatase (ALP)
bull Most of these are released from proximal tubular epithelial cells within 12 hours and four days earlier than a detectable rise in serum creatinine
bull No validated cut-off points currently exist to help distinguish prerenal disease from ATN
Urinary low-molecular-weight proteins
bull Alpha1-microglobulin (alpha1-m) beta2-microglobulin (beta2-m) retinol-binding protein (RBP) adenosine deaminase-binding protein (ABP) and urinary cystatin C are urinary lowmolecular- weight proteins
bull They are produced at different sites filtered at the glomerulus and reabsorbed at the proximal tubule with no secretion
bull Although promising prognostically and to help distinguish prerenal disease from ATN increased levels may be observed after reversible and mild dysfunction and may not necessarily be associated with persistent or irreversible damage
Functional biomarkersSerum creatinine
bull Currently the standard diagnostic tools for AKI detection are SCrconcentration and UO both of which are markers of renal function but not kidney injury
bull SCr is an integrator of various intra- and extra-renal functions and its concentration indicates the balance between creatinine generation and excretion
bull Unfortunately due to the non-linear relationship between GFR and sCr the increase of creatinine may be within the reference range in early phase of AKI and may overlooked
bull SCr does not indicate the severity of the injury until a steady state has been reached in AKI Therefore SCr is a delayed and insensitive biomarker of changes in kidney function moreover its concentration does not differentiate between structural kidney damage and functional hemodynamic triggers and it could be affected by many factors
bull Especially in intensive care unit patients creatinine-based definitions of AKI can be influenced by baseline creatinine estimation fluid overload malnourishment and muscle wasting
Cystatin-C
bull Cystatin-C is produced at a constant rate by nucleated cells filtered by the glomerular cells almost completely reabsorbed and catabolized (but not secreted) in the proximal tubule It is a polypeptide chain with 120 amino acid residues
bull In this way some of the limitations of serum creatinine effect of muscle mass diet gender and tubular secretion may not be a problem with cystatin C and appear to rise one to two days earlier than serum creatinine
bull Cystatin C is better marker of GFR than serum creatinine as demonstrated in several studies
bull Over the past decade Cystatin C (CyC) a serum measure of renal function is a stronger predictor of the risk of death and cardiovascular events in elderly persons than is creatinine
bull Koyner et al demonstrated that urinary CyC was superior to SCr and plasma CyC in the early diagnosis of acute kidney injury following adult cardiac surgery
bull Roos et al performed a systematic review comparing the diagnostic accuracy of plasma and urine CyC with SCr in patients undergoing cardiac surgery They concluded that the diagnostic accuracy for impaired renal function favors urine CyC
bull However while Cys-C levels are a more precise indicator of kidney function than SCr concentration they seem to be influenced by old age large doses of corticosteroids hyperthyroidism inflammation neoplasia smoking and alcohol consumption
bull Currently it is unclear whether the value of Cys-C is generalizable to all forms of AKI or specific to particular populations
Damage biomarkers
Neutrophil Gelatinase-Associated Lipocalin(NGAL)
bull Human NGAL is a 25 kDa protein firstly identified bound to gelatinase in specific granules of the neutrophil NGAL is a critical component of innate immunity to bacterial infection and is expressed by immune cells hepatocytes and renal tubular cells in various disease states
bull Its resistance to proteolysis further enhanced potential suitability as a clinical biomarker
bull In healthy kidneys it is barel detectable in either plasma or urine
bull However in the setting of acute tubular injury NGAL undergoes rapid and profound upregulation with large increases in both urine and plasma
bull Distinct from traditional markers of function such as creatinine this rapid response enables NGAL to potentially identify injured kidney much earlier than was previously possible The endogenous role of NGAL remains unclear It seems to be involved with iron transportation to and from the proximal tubular epithelial cells and animal studies demonstrate a renoprotective effect of exogenously administered NGAL in the setting of acute ischemic injury
bull NGAL was also detected in the urine of mice in the early stage of cisplatin-induced nephrotoxicity
bull These animal studies demonstrated that NGAL may represent an early sensitive and noninvasive urinary biomarker for ischemic and nephrotoxic kidney injury
bull NGAL is markedly upregulated and abundantly expressed in the kidney after renal ischemia
bull In this setting NGAL may function to dampen toxicity by reducing apoptosis and increasing the normal proliferation of kidney tubule cells
bull following ischemia reperfusion as evidenced by a rise in creatinine the kidneys illuminate indicating NGAL production at the site of injury
bull Interestingly following maneuvers that lead to significant prerenal disease there was no NGAL illumination indicating that prerenal disease does not induce NGAL expression
bull Thus NGAL may potentially be useful in differentiating prerenal disease from ATN
bull In these studies the average sensitivity and specificity of NGAL measured one to three days prior to AKI diagnosis was 76 and 77 percent respectively for cardiac surgery patients and 73 and 80 percent respectively for patients admitted to the intensive care unit (ICU)
bull NGAL may also represent early sensitive biomarker of AKI after contrast administrations for coronary angiography
bull NGAL was measured in the serum and urine before and at 2 4 12 24 and 48 h after contrast administration they found a significant rise in serum NGAL 2 and 4 h after PCI and a rise in urinary NGAL 4 and 12 h after PCI
bull A similar study of 25 patients with normal serum creatinine undergoing PCI due to unstable angina There was a significant rise in serum NGAL after 2 and 4 hours Urinary NGAL and urinary L-FABP followed the same pattern Both markers increased significantly after 4 hours and remained elevated up to 48 hours after PCI
bull Urine and plasma NGAL levels also represent early biomarkers of AKI in ICU
bull A multicenter study of serum NGAL was performed in 143 critically ill children with systemic inflammatory response syndrome (SIRS) or septic shock during the first 24 h of admission to the ICU there was a significant difference in serum NGAL between healthy children ill children with SIRS and septic shock the study was concluded that serum NGAL is a highly sensitive but nonspecific predictor of acute kidney injury in critically ill children with septic shock
bull A 2010 study evaluated 88 ICU patient and found that an NGAL level of ge150 nmolL predicted AKI with 82 sensitivity and 97 specificity
bull A recent study had 98 patients who were divided in two groups depending on the presence of sepsis Fifty-six patients had sepsis while forty-two patients were nonseptic Among septic patients subjects who developed AKI showed signi1048853 cant higher levels of NGAL
bull A more study of 65 patients with septic shock were found that urine NGAL levels 12 hours before AKI diagnosis were a good predictor of AKI
Kidney Injury Molecule-1 (KIM-1)
bull KIM-1 mRNA and protein are expressed at a low level in normal kidney but are increased dramatically in postischemic kidney
bull KIM-1 has been identified as the first nonmyeloidphosphatidylserine receptor that confers a phagocytic phenotype on injured epithelial cells both in vivo and in vitro
bull Urinary KIM-1 has been found to be an early indicator of AKI that compares favorably to a number of conventional biomarkers and tubular enzymes
bull KIM-1 is also a tissue and urinary biomarker for nephrotoxicant-induced kidney injury
bull Tissue and urinary expressions were measured with different nephrotoxic doses of cisplatin folic acide cadmium gentamycin mercury
bull As early as 1 day after cisplatin treatment positive KIM- 1 immunostaining observed in the outer medulla of the kidney and changes in urinary clusterin indicated the onset of proximal tubular injury in the absence of functional effects
bull Tissue KIM-1 was the most sensitive biomarker for detection of cisplatin-induced kidney damage
bull KIM-1 is a biomarker of AKI in humans bull Urine samples were collected from 32 patients with various
acute and chronic kidney diseases as well as from eight normal controls there was extensive expression of KIM-1 in proximal tubule cells in kidney biopsies from six patients with biopsy confirmed acute tubular necrosis (ATN)
bull Urinary KIM-1 levels were significantly higher in patients with ischemic ATN compared to levels in patients with other forms of acute renal failure or chronic renal disease
bull Adjusted for age gender and length of time delay between the initial insult and sampling of the urine a one-unit increase in normalized KIM-1 was associated with a greater than 12-fold risk for the presence of ATN
bull In hospital patients with AKI urinary levels of KIM-1 that higher levels correlated with a higher odds ratio for dialysis requirement or hospital death
bull this study demonstrated that urinary biomarker of AKI such as KIM-1 can predict adverse clinical outcomes in patients with AKI
bull Both renal and urinary KIM-1 correlate with kidney damage and negatively with renal function but not with proteinuria
bull A recent study has explored urinary KIM-1correlated with kidney function in kidney allograft recipients Kidney transplant recipients showed significantly higher KIM-1 values than the healthy volunteers this study concluded that even a successful kidney transplantation is associated with kidney injury as reflected by elevated urinary KIM-1
bull A rapid direct 15-minute assay for the detection of urinary human KIM-1 has been developed Using this assay more urinary KIM-1 was detected in the urine of patients with AKI than in the urine from healthy volunteers
Urinary interleukin-18
bull Interleukin18 (IL-18) is a 22 kDa pro-inflammatory cytokine that increases in the kidney after ischemia-reperfusion injury in a caspase- 1-dependent manner
bull Patients with ATN had significantly greater urinary IL-18 concentrations than those with other conditions (healthy controls patients with pre-renal azotemia urinary tract infection CKD and nephrotic syndrome)
bull urinary IL-18 concentrations measured in the first 24 h after kidney transplantation were higher in patients who received a cadaveric kidney that developed delayed graft function compared to patients who received a cadaveric kidney with prompt graft function and patients who received a kidney with prompt graft function from a living donor
bull However the performance of urinary IL-18 measured 1 day before AKI was modest
bull Its predictive utility for AKI following cardiac surgery could not be demonstrated in one prospective observational study of 100 adult patients
bull In addition in a large study population of 1439 critically ill patients IL-18 had a poor-to-moderate ability to predict AKI renal replacement therapy (RRT) or 90-day mortality
Liver-Type Fatty Acid Binding Protein(L-FABP)
bull Liver-type fatty acid-binding protein (L-FABP) is a 14 kDa protein from the large super- family of lipidbinding proteins
bull The 14-kD L-FABP protein can be localized predominantly in the proximal tubule
bull Noiri et al demonstrated that increase of urinary L-FABP was observed at 1 h after ischemia even in the 5-min IRI group and urinary L-FABP was superior to BUN and urinary NAG for early and accurate detection of acute tubular necrosis in different models of animal AKI
bull urinary L-FABP may be a promising biomarker for early detection of AKI and prediction of dialysis requirement and in-hospital mortality
bull Urinary excretion of urinary liver-type fatty acid-binding protein (L-FABP) reflects stress of proximal tubular epithelial cells and correlates with severity of ischemic tubular injury
bull A meta-analysis of 15 prospective cohort studies demonstrated that in hospitalndashbased cohorts of patients at risk of AKI L-FABP can discriminate for the diagnosis of AKI and predict the need for dialysis and in-hospital mortality
bull It was correlated with the degree of tubulointerstitial damage in a folic acid induced nephropathy
bull In ischemic and cisplatin-induced AKI L-FABP was increased in the urine before the increase in BUN
bull In cisplatin-induced AKI urinary L-FABP levels increased exponentially even in the lowest dose group as early as 2 hours whereas BUN levels increased at 48 hours
bull L-FABP was measured in 80 critically ill patients Urinary L-FABP levels in patients with septic shock were significantly higher than severe sepsis without shock Serum L-FABP levels did not have significant differences between patients with septic shock severe sepsis and healthy
bull Another study was evaluated 145 septic shock patients complicated with established AKI Urinary L-FABP measured at admission was significantly higher in the nonsurvivors of septic shock with established acute kidney injury than in the survivors
Failure of the TRIBE-AKI study
bull The Translational Research Investigating Biomarker Endpoints in AKI (TRIBE-AKI) study evaluated the performance of urinary c-glutamyltranspeptidase ( c-GTP) alkaline phosphatase NGAL Cys-C KIM-1 and IL-18 in AKI diagnosis
bull The results of four novel urine biomarkers and one plasma biomarker (urine NGAL IL-18 KIM-1 and L-FABP and plasma NGAL) were provided Of all the novel biomarkers only urine IL-18 and plasma NGAL in adults were helpful in predicting progression of AKI when measured on the day of clinical AKI diagnosis
bull Combinations of three biomarkers in adults from two different time points and combinations of two biomarkers in children from two time points were found to be able to increase the ROC for AKI up to 078
bull In summary the clinical use of single damage biomarkers in AKI prediction remains unclear because large prospective multicenter trials such as the TRIBE-AKI study (nfrac141530) have failed to demonstrate troponin-like diagnostic performance
Various clinical scenarios of AKI based onfunction damage and stress
bull Over the last decade a number of novel damage biomarkers have been evaluated for their capacity to detect kidney damage and predict the development of AKI However the relationship between decreasing function and increasing damage is not as straightforward as might be assumed
bull The characteristic pattern whereby damage precedes loss of function (panel A) may be seen in some cases of AKI and affords an opportunity to detect ldquosubclinicalrdquo AKI before function start to fall Unfortunately other patterns might also occur For example functional decline may start to occur alongside damage (panel B) and in some cases function may start to decline even before damage (panel C)
bull This makes damage markers difficult to use for predicting AKI However other markers might actually measure the ldquostressrdquo occurring at the cellular level before damage or loss of function
Paradigm shift to pre-injury phase biomarkers
bull Katz et al proposed that the pre-injury phase that leads to AKI can be described as ldquoacute kidney stressrdquo (AKS) after the report of the identification of cell cycle arrest biomarkers that signal the potential development of AKI is part of an evolution in the molecular diagnosis and understanding of AKI
bull These biomarkers are released by kidney cells along a path which may lead to AKI during a pre-injury phase
bull AKS is defined as the increased-risk phase (pre-injury phase) that leads to AKI
bull This ldquoAKSrdquo may or may not lead to damage and functional declinebull But it is the earliest possible the process of AKI can be detected
Pre-injury phase biomarkers
Stress biomarkersbull In 2013 Kashani et al reported the results of a prospective international
observational investigation (the Sapphire study) of tissue inhibitor of metalloproteinases- 2 (TIMP-2) and insulin-like growth factor-binding protein 7 (IGFBP7) in a heterogeneous group of critically ill patients [TIMP-2][IGFBP7] was significantly superior to all previously described markers of AKI (plt0002)
bull Next the Opal and Topaz study showed the cut-off value and risk assessment using the urinary[TIMP-2] [IGFBP7]
bull The urine [IGFBP7][TIMP2] biomarker is already FDA approved and commercially available in the United States
bull Falsepositive results are common and they will be magnified if the test is used inappropriately in low-risk patients In addition this biomarker should not be used in ambulatory practices and it is not beneficial in patients with established AKI
microRNAsbull microRNAs (miRNAs) are endogenous single-stranded non-coding
mRNAs of about 19-23 nucleotides bull In the past years researchers have begun to investigate the
relevance of miRNAs to AKI with many miRNAs being implicated bull Some of them contribute to pathogenesis by regulating apoptosis
and inflammation amplifying or reducing acute injury responses while others regulate fibrosis and angiogenesis participating in renal recovery or progression to fibrosis
bull Certain miRNAs have been investigated for their potential as novel biomarkers for the early detection or prognostication of AKI
Hemojuvelinbull Hemojuvelin (HJV) a glycophosphatidylinositol (GPI)- linked
membrane protein is highly expressed in liver and skeletal musclesbull The molecular weight of HJV is 42 kDa for the soluble form (sHJV)
and can be passed through glomerular filtration and reabsorbed by the renal tubules Increased iron content in the kidney and urine is observed in human and animal models of AKI and increased iron load can induce renal tubular cell injury
bull There is evidence that the increased expression of the hemojuvelin-hepcidin ferroportin pathway is an intrinsic response to iron overload conditions during AKI
bull Therefore urine HJV (uHJV) has the potential to be an early AKI biomarker in response to iron homeostasis during AKI
Combination of functional and damage biomarkers
bull While new biomarkers are being validated functional biomarkers (serum creatinine serum urea and urine output) continue to be utilized in the diagnosis and staging of AKI In the future existing or newer damage biomarkers will likely be combined with the use of functional biomarkers to enhance the ability of RIFLE AKIN
bull A study of 345 children after cardiopulmonary bypass surgery demonstrated that the composite of functional biomarker such as plasma cystatin C and urinary NGAL was superior to changes in serum creatinine to predict AKI
PROGNOSTIC BIOMARKERS
bull Most of the biomarkers described above allow early detection of acute kidney injury but do not predict severe AKI
Urinary renin and angiotensinogen
bull Urinary renin angiotensinogen and plasma NGAL may predict the development of severe AKI
bull Among 99 consecutively enrolled patients who developed AKI the ratio of urinary angiotensinogen to urinary creatinine (uAnCR expressed as ng per mg creatinine)calculated Patients with the highest uAnCR had a higher risk of worsening AKI compared with patients with the lowest uAnCR An elevated uAnCR predicted a longer hospital stay
bull Among 204 patients who developed Acute Kidney Injury Network (AKIN) stage 1 following cardiac surgery the urinary renin-to-creatinine ratio and the angiotensinogen-to-creatinine ratio predicted a composite outcome of death or AKIN stage 3 or death
Plasma NGAL
bull In a prospective cohort study in which 616 patients admitted from the emergency department were classified by clinical criteria as AKI transient azotemia stable CKD or normal kidney function plasma NGAL discriminated AKI from normal function and from transient azotemia
bull Higher concentrations of NGAL were associated with more severe AKI
Thanks for your attention
bull Clinicians need tools that are not influenced by other clinical parameters or patient characteristics and that can identify losses in GFR soon after occurence
bull the ideal biomarker of AKI would be a substance that the kidney releases immediately in response to injury and that can be detected in the blood or urine without significant metabolism
bull This biomarker would be highly sensitive and specific for injury to the kidney
bull Novel AKI biomarkers would be detect injury prior to changes in kidney function and potentially to aid in the differential diagnosis of AKI
Traditional biomarkers
Urine output
bull Urine output (UO) in AKI can vary from states of oliguria (lt400 mL24 h) to anuria (lt100 mL24 h) to extreme polyuria
bull While severe AKI can exist despite normal UO changes in UO can occur long before any biochemicalchanges are apparent As such UO is one of the criteria for defining AKI
bull UO often decreases before serum creatinine (SCr) concentration increases making it a more time-sensitive marker of GFR
bull However UO is not nearly as specific for GFR While it is true that if there is no UO in the absence of obstruction there can be no GFR not all reductions in UO signal AKI
bull Furthermore while sustained oliguria is invariably associated with AKI the timeliness of UO as an early indicator is lost in this case
Urine dipstick and microscopic examination
bull Routine dipstick and microscopic examinations of urine are often helpful in determining the cause of AKI
bull While granular or epithelial casts in urine are increased in acute tubular necrosis (ATN) they lack sufficient sensitivity specificity and predictive power for routine clinical use
Urinary indices
bull Diagnostic urinary indices of AKI are the fractional excretion of sodium (FENa) urea (FEurea) uric acid urine sodium and urine osmolality
bull Reduced effective circulating volume stimulates anti-diuretic hormone (ADH) release which results in increased distal water and urea reabsorption Thus low FEurea (lt35) is more sensitive and specific than FENa in differentiating between prerenal and renal causes of AKI especially when diuretics have been administered
bull FEurea and FENa have low diagnostic sensitivity in distinguishing azotemia associated with renal vasoconstriction and intact tubular function from established AKI with tubular dysfunction
Urinary tubular enzymes
bull Traditional urinary biomarkers including low- and high-molecular-weight proteins (a1-microglobulin b2- microglobulin retinol-binding proteins) brush border antigens (NaH exchanger isoform-3) urinary enzymes (a-glutathione S-transferase c-glutamyl transpeptidase N-acetyl-b-D-glucosaminidase) and Tamm-Horsfallprotein
bull have not entered clinical routine for AKI patients due to the lack of sufficient validation lack of standardized assays
Urinary tubular enzymes
bull Urinary tubular enzymes consist of proximal renal tubular epithelial antigen (HRTE-1) alpha-glutathione S-transferase (alpha-GST) glutamyltranspeptidase(gamma-GT) alanine aminopeptidase (AAP) lactate dehydrogenase (LDH) N-acetyl-beta-glucosaminidase(NAG) and alkaline phosphatase (ALP)
bull Most of these are released from proximal tubular epithelial cells within 12 hours and four days earlier than a detectable rise in serum creatinine
bull No validated cut-off points currently exist to help distinguish prerenal disease from ATN
Urinary low-molecular-weight proteins
bull Alpha1-microglobulin (alpha1-m) beta2-microglobulin (beta2-m) retinol-binding protein (RBP) adenosine deaminase-binding protein (ABP) and urinary cystatin C are urinary lowmolecular- weight proteins
bull They are produced at different sites filtered at the glomerulus and reabsorbed at the proximal tubule with no secretion
bull Although promising prognostically and to help distinguish prerenal disease from ATN increased levels may be observed after reversible and mild dysfunction and may not necessarily be associated with persistent or irreversible damage
Functional biomarkersSerum creatinine
bull Currently the standard diagnostic tools for AKI detection are SCrconcentration and UO both of which are markers of renal function but not kidney injury
bull SCr is an integrator of various intra- and extra-renal functions and its concentration indicates the balance between creatinine generation and excretion
bull Unfortunately due to the non-linear relationship between GFR and sCr the increase of creatinine may be within the reference range in early phase of AKI and may overlooked
bull SCr does not indicate the severity of the injury until a steady state has been reached in AKI Therefore SCr is a delayed and insensitive biomarker of changes in kidney function moreover its concentration does not differentiate between structural kidney damage and functional hemodynamic triggers and it could be affected by many factors
bull Especially in intensive care unit patients creatinine-based definitions of AKI can be influenced by baseline creatinine estimation fluid overload malnourishment and muscle wasting
Cystatin-C
bull Cystatin-C is produced at a constant rate by nucleated cells filtered by the glomerular cells almost completely reabsorbed and catabolized (but not secreted) in the proximal tubule It is a polypeptide chain with 120 amino acid residues
bull In this way some of the limitations of serum creatinine effect of muscle mass diet gender and tubular secretion may not be a problem with cystatin C and appear to rise one to two days earlier than serum creatinine
bull Cystatin C is better marker of GFR than serum creatinine as demonstrated in several studies
bull Over the past decade Cystatin C (CyC) a serum measure of renal function is a stronger predictor of the risk of death and cardiovascular events in elderly persons than is creatinine
bull Koyner et al demonstrated that urinary CyC was superior to SCr and plasma CyC in the early diagnosis of acute kidney injury following adult cardiac surgery
bull Roos et al performed a systematic review comparing the diagnostic accuracy of plasma and urine CyC with SCr in patients undergoing cardiac surgery They concluded that the diagnostic accuracy for impaired renal function favors urine CyC
bull However while Cys-C levels are a more precise indicator of kidney function than SCr concentration they seem to be influenced by old age large doses of corticosteroids hyperthyroidism inflammation neoplasia smoking and alcohol consumption
bull Currently it is unclear whether the value of Cys-C is generalizable to all forms of AKI or specific to particular populations
Damage biomarkers
Neutrophil Gelatinase-Associated Lipocalin(NGAL)
bull Human NGAL is a 25 kDa protein firstly identified bound to gelatinase in specific granules of the neutrophil NGAL is a critical component of innate immunity to bacterial infection and is expressed by immune cells hepatocytes and renal tubular cells in various disease states
bull Its resistance to proteolysis further enhanced potential suitability as a clinical biomarker
bull In healthy kidneys it is barel detectable in either plasma or urine
bull However in the setting of acute tubular injury NGAL undergoes rapid and profound upregulation with large increases in both urine and plasma
bull Distinct from traditional markers of function such as creatinine this rapid response enables NGAL to potentially identify injured kidney much earlier than was previously possible The endogenous role of NGAL remains unclear It seems to be involved with iron transportation to and from the proximal tubular epithelial cells and animal studies demonstrate a renoprotective effect of exogenously administered NGAL in the setting of acute ischemic injury
bull NGAL was also detected in the urine of mice in the early stage of cisplatin-induced nephrotoxicity
bull These animal studies demonstrated that NGAL may represent an early sensitive and noninvasive urinary biomarker for ischemic and nephrotoxic kidney injury
bull NGAL is markedly upregulated and abundantly expressed in the kidney after renal ischemia
bull In this setting NGAL may function to dampen toxicity by reducing apoptosis and increasing the normal proliferation of kidney tubule cells
bull following ischemia reperfusion as evidenced by a rise in creatinine the kidneys illuminate indicating NGAL production at the site of injury
bull Interestingly following maneuvers that lead to significant prerenal disease there was no NGAL illumination indicating that prerenal disease does not induce NGAL expression
bull Thus NGAL may potentially be useful in differentiating prerenal disease from ATN
bull In these studies the average sensitivity and specificity of NGAL measured one to three days prior to AKI diagnosis was 76 and 77 percent respectively for cardiac surgery patients and 73 and 80 percent respectively for patients admitted to the intensive care unit (ICU)
bull NGAL may also represent early sensitive biomarker of AKI after contrast administrations for coronary angiography
bull NGAL was measured in the serum and urine before and at 2 4 12 24 and 48 h after contrast administration they found a significant rise in serum NGAL 2 and 4 h after PCI and a rise in urinary NGAL 4 and 12 h after PCI
bull A similar study of 25 patients with normal serum creatinine undergoing PCI due to unstable angina There was a significant rise in serum NGAL after 2 and 4 hours Urinary NGAL and urinary L-FABP followed the same pattern Both markers increased significantly after 4 hours and remained elevated up to 48 hours after PCI
bull Urine and plasma NGAL levels also represent early biomarkers of AKI in ICU
bull A multicenter study of serum NGAL was performed in 143 critically ill children with systemic inflammatory response syndrome (SIRS) or septic shock during the first 24 h of admission to the ICU there was a significant difference in serum NGAL between healthy children ill children with SIRS and septic shock the study was concluded that serum NGAL is a highly sensitive but nonspecific predictor of acute kidney injury in critically ill children with septic shock
bull A 2010 study evaluated 88 ICU patient and found that an NGAL level of ge150 nmolL predicted AKI with 82 sensitivity and 97 specificity
bull A recent study had 98 patients who were divided in two groups depending on the presence of sepsis Fifty-six patients had sepsis while forty-two patients were nonseptic Among septic patients subjects who developed AKI showed signi1048853 cant higher levels of NGAL
bull A more study of 65 patients with septic shock were found that urine NGAL levels 12 hours before AKI diagnosis were a good predictor of AKI
Kidney Injury Molecule-1 (KIM-1)
bull KIM-1 mRNA and protein are expressed at a low level in normal kidney but are increased dramatically in postischemic kidney
bull KIM-1 has been identified as the first nonmyeloidphosphatidylserine receptor that confers a phagocytic phenotype on injured epithelial cells both in vivo and in vitro
bull Urinary KIM-1 has been found to be an early indicator of AKI that compares favorably to a number of conventional biomarkers and tubular enzymes
bull KIM-1 is also a tissue and urinary biomarker for nephrotoxicant-induced kidney injury
bull Tissue and urinary expressions were measured with different nephrotoxic doses of cisplatin folic acide cadmium gentamycin mercury
bull As early as 1 day after cisplatin treatment positive KIM- 1 immunostaining observed in the outer medulla of the kidney and changes in urinary clusterin indicated the onset of proximal tubular injury in the absence of functional effects
bull Tissue KIM-1 was the most sensitive biomarker for detection of cisplatin-induced kidney damage
bull KIM-1 is a biomarker of AKI in humans bull Urine samples were collected from 32 patients with various
acute and chronic kidney diseases as well as from eight normal controls there was extensive expression of KIM-1 in proximal tubule cells in kidney biopsies from six patients with biopsy confirmed acute tubular necrosis (ATN)
bull Urinary KIM-1 levels were significantly higher in patients with ischemic ATN compared to levels in patients with other forms of acute renal failure or chronic renal disease
bull Adjusted for age gender and length of time delay between the initial insult and sampling of the urine a one-unit increase in normalized KIM-1 was associated with a greater than 12-fold risk for the presence of ATN
bull In hospital patients with AKI urinary levels of KIM-1 that higher levels correlated with a higher odds ratio for dialysis requirement or hospital death
bull this study demonstrated that urinary biomarker of AKI such as KIM-1 can predict adverse clinical outcomes in patients with AKI
bull Both renal and urinary KIM-1 correlate with kidney damage and negatively with renal function but not with proteinuria
bull A recent study has explored urinary KIM-1correlated with kidney function in kidney allograft recipients Kidney transplant recipients showed significantly higher KIM-1 values than the healthy volunteers this study concluded that even a successful kidney transplantation is associated with kidney injury as reflected by elevated urinary KIM-1
bull A rapid direct 15-minute assay for the detection of urinary human KIM-1 has been developed Using this assay more urinary KIM-1 was detected in the urine of patients with AKI than in the urine from healthy volunteers
Urinary interleukin-18
bull Interleukin18 (IL-18) is a 22 kDa pro-inflammatory cytokine that increases in the kidney after ischemia-reperfusion injury in a caspase- 1-dependent manner
bull Patients with ATN had significantly greater urinary IL-18 concentrations than those with other conditions (healthy controls patients with pre-renal azotemia urinary tract infection CKD and nephrotic syndrome)
bull urinary IL-18 concentrations measured in the first 24 h after kidney transplantation were higher in patients who received a cadaveric kidney that developed delayed graft function compared to patients who received a cadaveric kidney with prompt graft function and patients who received a kidney with prompt graft function from a living donor
bull However the performance of urinary IL-18 measured 1 day before AKI was modest
bull Its predictive utility for AKI following cardiac surgery could not be demonstrated in one prospective observational study of 100 adult patients
bull In addition in a large study population of 1439 critically ill patients IL-18 had a poor-to-moderate ability to predict AKI renal replacement therapy (RRT) or 90-day mortality
Liver-Type Fatty Acid Binding Protein(L-FABP)
bull Liver-type fatty acid-binding protein (L-FABP) is a 14 kDa protein from the large super- family of lipidbinding proteins
bull The 14-kD L-FABP protein can be localized predominantly in the proximal tubule
bull Noiri et al demonstrated that increase of urinary L-FABP was observed at 1 h after ischemia even in the 5-min IRI group and urinary L-FABP was superior to BUN and urinary NAG for early and accurate detection of acute tubular necrosis in different models of animal AKI
bull urinary L-FABP may be a promising biomarker for early detection of AKI and prediction of dialysis requirement and in-hospital mortality
bull Urinary excretion of urinary liver-type fatty acid-binding protein (L-FABP) reflects stress of proximal tubular epithelial cells and correlates with severity of ischemic tubular injury
bull A meta-analysis of 15 prospective cohort studies demonstrated that in hospitalndashbased cohorts of patients at risk of AKI L-FABP can discriminate for the diagnosis of AKI and predict the need for dialysis and in-hospital mortality
bull It was correlated with the degree of tubulointerstitial damage in a folic acid induced nephropathy
bull In ischemic and cisplatin-induced AKI L-FABP was increased in the urine before the increase in BUN
bull In cisplatin-induced AKI urinary L-FABP levels increased exponentially even in the lowest dose group as early as 2 hours whereas BUN levels increased at 48 hours
bull L-FABP was measured in 80 critically ill patients Urinary L-FABP levels in patients with septic shock were significantly higher than severe sepsis without shock Serum L-FABP levels did not have significant differences between patients with septic shock severe sepsis and healthy
bull Another study was evaluated 145 septic shock patients complicated with established AKI Urinary L-FABP measured at admission was significantly higher in the nonsurvivors of septic shock with established acute kidney injury than in the survivors
Failure of the TRIBE-AKI study
bull The Translational Research Investigating Biomarker Endpoints in AKI (TRIBE-AKI) study evaluated the performance of urinary c-glutamyltranspeptidase ( c-GTP) alkaline phosphatase NGAL Cys-C KIM-1 and IL-18 in AKI diagnosis
bull The results of four novel urine biomarkers and one plasma biomarker (urine NGAL IL-18 KIM-1 and L-FABP and plasma NGAL) were provided Of all the novel biomarkers only urine IL-18 and plasma NGAL in adults were helpful in predicting progression of AKI when measured on the day of clinical AKI diagnosis
bull Combinations of three biomarkers in adults from two different time points and combinations of two biomarkers in children from two time points were found to be able to increase the ROC for AKI up to 078
bull In summary the clinical use of single damage biomarkers in AKI prediction remains unclear because large prospective multicenter trials such as the TRIBE-AKI study (nfrac141530) have failed to demonstrate troponin-like diagnostic performance
Various clinical scenarios of AKI based onfunction damage and stress
bull Over the last decade a number of novel damage biomarkers have been evaluated for their capacity to detect kidney damage and predict the development of AKI However the relationship between decreasing function and increasing damage is not as straightforward as might be assumed
bull The characteristic pattern whereby damage precedes loss of function (panel A) may be seen in some cases of AKI and affords an opportunity to detect ldquosubclinicalrdquo AKI before function start to fall Unfortunately other patterns might also occur For example functional decline may start to occur alongside damage (panel B) and in some cases function may start to decline even before damage (panel C)
bull This makes damage markers difficult to use for predicting AKI However other markers might actually measure the ldquostressrdquo occurring at the cellular level before damage or loss of function
Paradigm shift to pre-injury phase biomarkers
bull Katz et al proposed that the pre-injury phase that leads to AKI can be described as ldquoacute kidney stressrdquo (AKS) after the report of the identification of cell cycle arrest biomarkers that signal the potential development of AKI is part of an evolution in the molecular diagnosis and understanding of AKI
bull These biomarkers are released by kidney cells along a path which may lead to AKI during a pre-injury phase
bull AKS is defined as the increased-risk phase (pre-injury phase) that leads to AKI
bull This ldquoAKSrdquo may or may not lead to damage and functional declinebull But it is the earliest possible the process of AKI can be detected
Pre-injury phase biomarkers
Stress biomarkersbull In 2013 Kashani et al reported the results of a prospective international
observational investigation (the Sapphire study) of tissue inhibitor of metalloproteinases- 2 (TIMP-2) and insulin-like growth factor-binding protein 7 (IGFBP7) in a heterogeneous group of critically ill patients [TIMP-2][IGFBP7] was significantly superior to all previously described markers of AKI (plt0002)
bull Next the Opal and Topaz study showed the cut-off value and risk assessment using the urinary[TIMP-2] [IGFBP7]
bull The urine [IGFBP7][TIMP2] biomarker is already FDA approved and commercially available in the United States
bull Falsepositive results are common and they will be magnified if the test is used inappropriately in low-risk patients In addition this biomarker should not be used in ambulatory practices and it is not beneficial in patients with established AKI
microRNAsbull microRNAs (miRNAs) are endogenous single-stranded non-coding
mRNAs of about 19-23 nucleotides bull In the past years researchers have begun to investigate the
relevance of miRNAs to AKI with many miRNAs being implicated bull Some of them contribute to pathogenesis by regulating apoptosis
and inflammation amplifying or reducing acute injury responses while others regulate fibrosis and angiogenesis participating in renal recovery or progression to fibrosis
bull Certain miRNAs have been investigated for their potential as novel biomarkers for the early detection or prognostication of AKI
Hemojuvelinbull Hemojuvelin (HJV) a glycophosphatidylinositol (GPI)- linked
membrane protein is highly expressed in liver and skeletal musclesbull The molecular weight of HJV is 42 kDa for the soluble form (sHJV)
and can be passed through glomerular filtration and reabsorbed by the renal tubules Increased iron content in the kidney and urine is observed in human and animal models of AKI and increased iron load can induce renal tubular cell injury
bull There is evidence that the increased expression of the hemojuvelin-hepcidin ferroportin pathway is an intrinsic response to iron overload conditions during AKI
bull Therefore urine HJV (uHJV) has the potential to be an early AKI biomarker in response to iron homeostasis during AKI
Combination of functional and damage biomarkers
bull While new biomarkers are being validated functional biomarkers (serum creatinine serum urea and urine output) continue to be utilized in the diagnosis and staging of AKI In the future existing or newer damage biomarkers will likely be combined with the use of functional biomarkers to enhance the ability of RIFLE AKIN
bull A study of 345 children after cardiopulmonary bypass surgery demonstrated that the composite of functional biomarker such as plasma cystatin C and urinary NGAL was superior to changes in serum creatinine to predict AKI
PROGNOSTIC BIOMARKERS
bull Most of the biomarkers described above allow early detection of acute kidney injury but do not predict severe AKI
Urinary renin and angiotensinogen
bull Urinary renin angiotensinogen and plasma NGAL may predict the development of severe AKI
bull Among 99 consecutively enrolled patients who developed AKI the ratio of urinary angiotensinogen to urinary creatinine (uAnCR expressed as ng per mg creatinine)calculated Patients with the highest uAnCR had a higher risk of worsening AKI compared with patients with the lowest uAnCR An elevated uAnCR predicted a longer hospital stay
bull Among 204 patients who developed Acute Kidney Injury Network (AKIN) stage 1 following cardiac surgery the urinary renin-to-creatinine ratio and the angiotensinogen-to-creatinine ratio predicted a composite outcome of death or AKIN stage 3 or death
Plasma NGAL
bull In a prospective cohort study in which 616 patients admitted from the emergency department were classified by clinical criteria as AKI transient azotemia stable CKD or normal kidney function plasma NGAL discriminated AKI from normal function and from transient azotemia
bull Higher concentrations of NGAL were associated with more severe AKI
Thanks for your attention

Traditional biomarkers
Urine output
bull Urine output (UO) in AKI can vary from states of oliguria (lt400 mL24 h) to anuria (lt100 mL24 h) to extreme polyuria
bull While severe AKI can exist despite normal UO changes in UO can occur long before any biochemicalchanges are apparent As such UO is one of the criteria for defining AKI
bull UO often decreases before serum creatinine (SCr) concentration increases making it a more time-sensitive marker of GFR
bull However UO is not nearly as specific for GFR While it is true that if there is no UO in the absence of obstruction there can be no GFR not all reductions in UO signal AKI
bull Furthermore while sustained oliguria is invariably associated with AKI the timeliness of UO as an early indicator is lost in this case
Urine dipstick and microscopic examination
bull Routine dipstick and microscopic examinations of urine are often helpful in determining the cause of AKI
bull While granular or epithelial casts in urine are increased in acute tubular necrosis (ATN) they lack sufficient sensitivity specificity and predictive power for routine clinical use
Urinary indices
bull Diagnostic urinary indices of AKI are the fractional excretion of sodium (FENa) urea (FEurea) uric acid urine sodium and urine osmolality
bull Reduced effective circulating volume stimulates anti-diuretic hormone (ADH) release which results in increased distal water and urea reabsorption Thus low FEurea (lt35) is more sensitive and specific than FENa in differentiating between prerenal and renal causes of AKI especially when diuretics have been administered
bull FEurea and FENa have low diagnostic sensitivity in distinguishing azotemia associated with renal vasoconstriction and intact tubular function from established AKI with tubular dysfunction
Urinary tubular enzymes
bull Traditional urinary biomarkers including low- and high-molecular-weight proteins (a1-microglobulin b2- microglobulin retinol-binding proteins) brush border antigens (NaH exchanger isoform-3) urinary enzymes (a-glutathione S-transferase c-glutamyl transpeptidase N-acetyl-b-D-glucosaminidase) and Tamm-Horsfallprotein
bull have not entered clinical routine for AKI patients due to the lack of sufficient validation lack of standardized assays
Urinary tubular enzymes
bull Urinary tubular enzymes consist of proximal renal tubular epithelial antigen (HRTE-1) alpha-glutathione S-transferase (alpha-GST) glutamyltranspeptidase(gamma-GT) alanine aminopeptidase (AAP) lactate dehydrogenase (LDH) N-acetyl-beta-glucosaminidase(NAG) and alkaline phosphatase (ALP)
bull Most of these are released from proximal tubular epithelial cells within 12 hours and four days earlier than a detectable rise in serum creatinine
bull No validated cut-off points currently exist to help distinguish prerenal disease from ATN
Urinary low-molecular-weight proteins
bull Alpha1-microglobulin (alpha1-m) beta2-microglobulin (beta2-m) retinol-binding protein (RBP) adenosine deaminase-binding protein (ABP) and urinary cystatin C are urinary lowmolecular- weight proteins
bull They are produced at different sites filtered at the glomerulus and reabsorbed at the proximal tubule with no secretion
bull Although promising prognostically and to help distinguish prerenal disease from ATN increased levels may be observed after reversible and mild dysfunction and may not necessarily be associated with persistent or irreversible damage
Functional biomarkersSerum creatinine
bull Currently the standard diagnostic tools for AKI detection are SCrconcentration and UO both of which are markers of renal function but not kidney injury
bull SCr is an integrator of various intra- and extra-renal functions and its concentration indicates the balance between creatinine generation and excretion
bull Unfortunately due to the non-linear relationship between GFR and sCr the increase of creatinine may be within the reference range in early phase of AKI and may overlooked
bull SCr does not indicate the severity of the injury until a steady state has been reached in AKI Therefore SCr is a delayed and insensitive biomarker of changes in kidney function moreover its concentration does not differentiate between structural kidney damage and functional hemodynamic triggers and it could be affected by many factors
bull Especially in intensive care unit patients creatinine-based definitions of AKI can be influenced by baseline creatinine estimation fluid overload malnourishment and muscle wasting
Cystatin-C
bull Cystatin-C is produced at a constant rate by nucleated cells filtered by the glomerular cells almost completely reabsorbed and catabolized (but not secreted) in the proximal tubule It is a polypeptide chain with 120 amino acid residues
bull In this way some of the limitations of serum creatinine effect of muscle mass diet gender and tubular secretion may not be a problem with cystatin C and appear to rise one to two days earlier than serum creatinine
bull Cystatin C is better marker of GFR than serum creatinine as demonstrated in several studies
bull Over the past decade Cystatin C (CyC) a serum measure of renal function is a stronger predictor of the risk of death and cardiovascular events in elderly persons than is creatinine
bull Koyner et al demonstrated that urinary CyC was superior to SCr and plasma CyC in the early diagnosis of acute kidney injury following adult cardiac surgery
bull Roos et al performed a systematic review comparing the diagnostic accuracy of plasma and urine CyC with SCr in patients undergoing cardiac surgery They concluded that the diagnostic accuracy for impaired renal function favors urine CyC
bull However while Cys-C levels are a more precise indicator of kidney function than SCr concentration they seem to be influenced by old age large doses of corticosteroids hyperthyroidism inflammation neoplasia smoking and alcohol consumption
bull Currently it is unclear whether the value of Cys-C is generalizable to all forms of AKI or specific to particular populations
Damage biomarkers
Neutrophil Gelatinase-Associated Lipocalin(NGAL)
bull Human NGAL is a 25 kDa protein firstly identified bound to gelatinase in specific granules of the neutrophil NGAL is a critical component of innate immunity to bacterial infection and is expressed by immune cells hepatocytes and renal tubular cells in various disease states
bull Its resistance to proteolysis further enhanced potential suitability as a clinical biomarker
bull In healthy kidneys it is barel detectable in either plasma or urine
bull However in the setting of acute tubular injury NGAL undergoes rapid and profound upregulation with large increases in both urine and plasma
bull Distinct from traditional markers of function such as creatinine this rapid response enables NGAL to potentially identify injured kidney much earlier than was previously possible The endogenous role of NGAL remains unclear It seems to be involved with iron transportation to and from the proximal tubular epithelial cells and animal studies demonstrate a renoprotective effect of exogenously administered NGAL in the setting of acute ischemic injury
bull NGAL was also detected in the urine of mice in the early stage of cisplatin-induced nephrotoxicity
bull These animal studies demonstrated that NGAL may represent an early sensitive and noninvasive urinary biomarker for ischemic and nephrotoxic kidney injury
bull NGAL is markedly upregulated and abundantly expressed in the kidney after renal ischemia
bull In this setting NGAL may function to dampen toxicity by reducing apoptosis and increasing the normal proliferation of kidney tubule cells
bull following ischemia reperfusion as evidenced by a rise in creatinine the kidneys illuminate indicating NGAL production at the site of injury
bull Interestingly following maneuvers that lead to significant prerenal disease there was no NGAL illumination indicating that prerenal disease does not induce NGAL expression
bull Thus NGAL may potentially be useful in differentiating prerenal disease from ATN
bull In these studies the average sensitivity and specificity of NGAL measured one to three days prior to AKI diagnosis was 76 and 77 percent respectively for cardiac surgery patients and 73 and 80 percent respectively for patients admitted to the intensive care unit (ICU)
bull NGAL may also represent early sensitive biomarker of AKI after contrast administrations for coronary angiography
bull NGAL was measured in the serum and urine before and at 2 4 12 24 and 48 h after contrast administration they found a significant rise in serum NGAL 2 and 4 h after PCI and a rise in urinary NGAL 4 and 12 h after PCI
bull A similar study of 25 patients with normal serum creatinine undergoing PCI due to unstable angina There was a significant rise in serum NGAL after 2 and 4 hours Urinary NGAL and urinary L-FABP followed the same pattern Both markers increased significantly after 4 hours and remained elevated up to 48 hours after PCI
bull Urine and plasma NGAL levels also represent early biomarkers of AKI in ICU
bull A multicenter study of serum NGAL was performed in 143 critically ill children with systemic inflammatory response syndrome (SIRS) or septic shock during the first 24 h of admission to the ICU there was a significant difference in serum NGAL between healthy children ill children with SIRS and septic shock the study was concluded that serum NGAL is a highly sensitive but nonspecific predictor of acute kidney injury in critically ill children with septic shock
bull A 2010 study evaluated 88 ICU patient and found that an NGAL level of ge150 nmolL predicted AKI with 82 sensitivity and 97 specificity
bull A recent study had 98 patients who were divided in two groups depending on the presence of sepsis Fifty-six patients had sepsis while forty-two patients were nonseptic Among septic patients subjects who developed AKI showed signi1048853 cant higher levels of NGAL
bull A more study of 65 patients with septic shock were found that urine NGAL levels 12 hours before AKI diagnosis were a good predictor of AKI
Kidney Injury Molecule-1 (KIM-1)
bull KIM-1 mRNA and protein are expressed at a low level in normal kidney but are increased dramatically in postischemic kidney
bull KIM-1 has been identified as the first nonmyeloidphosphatidylserine receptor that confers a phagocytic phenotype on injured epithelial cells both in vivo and in vitro
bull Urinary KIM-1 has been found to be an early indicator of AKI that compares favorably to a number of conventional biomarkers and tubular enzymes
bull KIM-1 is also a tissue and urinary biomarker for nephrotoxicant-induced kidney injury
bull Tissue and urinary expressions were measured with different nephrotoxic doses of cisplatin folic acide cadmium gentamycin mercury
bull As early as 1 day after cisplatin treatment positive KIM- 1 immunostaining observed in the outer medulla of the kidney and changes in urinary clusterin indicated the onset of proximal tubular injury in the absence of functional effects
bull Tissue KIM-1 was the most sensitive biomarker for detection of cisplatin-induced kidney damage
bull KIM-1 is a biomarker of AKI in humans bull Urine samples were collected from 32 patients with various
acute and chronic kidney diseases as well as from eight normal controls there was extensive expression of KIM-1 in proximal tubule cells in kidney biopsies from six patients with biopsy confirmed acute tubular necrosis (ATN)
bull Urinary KIM-1 levels were significantly higher in patients with ischemic ATN compared to levels in patients with other forms of acute renal failure or chronic renal disease
bull Adjusted for age gender and length of time delay between the initial insult and sampling of the urine a one-unit increase in normalized KIM-1 was associated with a greater than 12-fold risk for the presence of ATN
bull In hospital patients with AKI urinary levels of KIM-1 that higher levels correlated with a higher odds ratio for dialysis requirement or hospital death
bull this study demonstrated that urinary biomarker of AKI such as KIM-1 can predict adverse clinical outcomes in patients with AKI
bull Both renal and urinary KIM-1 correlate with kidney damage and negatively with renal function but not with proteinuria
bull A recent study has explored urinary KIM-1correlated with kidney function in kidney allograft recipients Kidney transplant recipients showed significantly higher KIM-1 values than the healthy volunteers this study concluded that even a successful kidney transplantation is associated with kidney injury as reflected by elevated urinary KIM-1
bull A rapid direct 15-minute assay for the detection of urinary human KIM-1 has been developed Using this assay more urinary KIM-1 was detected in the urine of patients with AKI than in the urine from healthy volunteers
Urinary interleukin-18
bull Interleukin18 (IL-18) is a 22 kDa pro-inflammatory cytokine that increases in the kidney after ischemia-reperfusion injury in a caspase- 1-dependent manner
bull Patients with ATN had significantly greater urinary IL-18 concentrations than those with other conditions (healthy controls patients with pre-renal azotemia urinary tract infection CKD and nephrotic syndrome)
bull urinary IL-18 concentrations measured in the first 24 h after kidney transplantation were higher in patients who received a cadaveric kidney that developed delayed graft function compared to patients who received a cadaveric kidney with prompt graft function and patients who received a kidney with prompt graft function from a living donor
bull However the performance of urinary IL-18 measured 1 day before AKI was modest
bull Its predictive utility for AKI following cardiac surgery could not be demonstrated in one prospective observational study of 100 adult patients
bull In addition in a large study population of 1439 critically ill patients IL-18 had a poor-to-moderate ability to predict AKI renal replacement therapy (RRT) or 90-day mortality
Liver-Type Fatty Acid Binding Protein(L-FABP)
bull Liver-type fatty acid-binding protein (L-FABP) is a 14 kDa protein from the large super- family of lipidbinding proteins
bull The 14-kD L-FABP protein can be localized predominantly in the proximal tubule
bull Noiri et al demonstrated that increase of urinary L-FABP was observed at 1 h after ischemia even in the 5-min IRI group and urinary L-FABP was superior to BUN and urinary NAG for early and accurate detection of acute tubular necrosis in different models of animal AKI
bull urinary L-FABP may be a promising biomarker for early detection of AKI and prediction of dialysis requirement and in-hospital mortality
bull Urinary excretion of urinary liver-type fatty acid-binding protein (L-FABP) reflects stress of proximal tubular epithelial cells and correlates with severity of ischemic tubular injury
bull A meta-analysis of 15 prospective cohort studies demonstrated that in hospitalndashbased cohorts of patients at risk of AKI L-FABP can discriminate for the diagnosis of AKI and predict the need for dialysis and in-hospital mortality
bull It was correlated with the degree of tubulointerstitial damage in a folic acid induced nephropathy
bull In ischemic and cisplatin-induced AKI L-FABP was increased in the urine before the increase in BUN
bull In cisplatin-induced AKI urinary L-FABP levels increased exponentially even in the lowest dose group as early as 2 hours whereas BUN levels increased at 48 hours
bull L-FABP was measured in 80 critically ill patients Urinary L-FABP levels in patients with septic shock were significantly higher than severe sepsis without shock Serum L-FABP levels did not have significant differences between patients with septic shock severe sepsis and healthy
bull Another study was evaluated 145 septic shock patients complicated with established AKI Urinary L-FABP measured at admission was significantly higher in the nonsurvivors of septic shock with established acute kidney injury than in the survivors
Failure of the TRIBE-AKI study
bull The Translational Research Investigating Biomarker Endpoints in AKI (TRIBE-AKI) study evaluated the performance of urinary c-glutamyltranspeptidase ( c-GTP) alkaline phosphatase NGAL Cys-C KIM-1 and IL-18 in AKI diagnosis
bull The results of four novel urine biomarkers and one plasma biomarker (urine NGAL IL-18 KIM-1 and L-FABP and plasma NGAL) were provided Of all the novel biomarkers only urine IL-18 and plasma NGAL in adults were helpful in predicting progression of AKI when measured on the day of clinical AKI diagnosis
bull Combinations of three biomarkers in adults from two different time points and combinations of two biomarkers in children from two time points were found to be able to increase the ROC for AKI up to 078
bull In summary the clinical use of single damage biomarkers in AKI prediction remains unclear because large prospective multicenter trials such as the TRIBE-AKI study (nfrac141530) have failed to demonstrate troponin-like diagnostic performance
Various clinical scenarios of AKI based onfunction damage and stress
bull Over the last decade a number of novel damage biomarkers have been evaluated for their capacity to detect kidney damage and predict the development of AKI However the relationship between decreasing function and increasing damage is not as straightforward as might be assumed
bull The characteristic pattern whereby damage precedes loss of function (panel A) may be seen in some cases of AKI and affords an opportunity to detect ldquosubclinicalrdquo AKI before function start to fall Unfortunately other patterns might also occur For example functional decline may start to occur alongside damage (panel B) and in some cases function may start to decline even before damage (panel C)
bull This makes damage markers difficult to use for predicting AKI However other markers might actually measure the ldquostressrdquo occurring at the cellular level before damage or loss of function
Paradigm shift to pre-injury phase biomarkers
bull Katz et al proposed that the pre-injury phase that leads to AKI can be described as ldquoacute kidney stressrdquo (AKS) after the report of the identification of cell cycle arrest biomarkers that signal the potential development of AKI is part of an evolution in the molecular diagnosis and understanding of AKI
bull These biomarkers are released by kidney cells along a path which may lead to AKI during a pre-injury phase
bull AKS is defined as the increased-risk phase (pre-injury phase) that leads to AKI
bull This ldquoAKSrdquo may or may not lead to damage and functional declinebull But it is the earliest possible the process of AKI can be detected
Pre-injury phase biomarkers
Stress biomarkersbull In 2013 Kashani et al reported the results of a prospective international
observational investigation (the Sapphire study) of tissue inhibitor of metalloproteinases- 2 (TIMP-2) and insulin-like growth factor-binding protein 7 (IGFBP7) in a heterogeneous group of critically ill patients [TIMP-2][IGFBP7] was significantly superior to all previously described markers of AKI (plt0002)
bull Next the Opal and Topaz study showed the cut-off value and risk assessment using the urinary[TIMP-2] [IGFBP7]
bull The urine [IGFBP7][TIMP2] biomarker is already FDA approved and commercially available in the United States
bull Falsepositive results are common and they will be magnified if the test is used inappropriately in low-risk patients In addition this biomarker should not be used in ambulatory practices and it is not beneficial in patients with established AKI
microRNAsbull microRNAs (miRNAs) are endogenous single-stranded non-coding
mRNAs of about 19-23 nucleotides bull In the past years researchers have begun to investigate the
relevance of miRNAs to AKI with many miRNAs being implicated bull Some of them contribute to pathogenesis by regulating apoptosis
and inflammation amplifying or reducing acute injury responses while others regulate fibrosis and angiogenesis participating in renal recovery or progression to fibrosis
bull Certain miRNAs have been investigated for their potential as novel biomarkers for the early detection or prognostication of AKI
Hemojuvelinbull Hemojuvelin (HJV) a glycophosphatidylinositol (GPI)- linked
membrane protein is highly expressed in liver and skeletal musclesbull The molecular weight of HJV is 42 kDa for the soluble form (sHJV)
and can be passed through glomerular filtration and reabsorbed by the renal tubules Increased iron content in the kidney and urine is observed in human and animal models of AKI and increased iron load can induce renal tubular cell injury
bull There is evidence that the increased expression of the hemojuvelin-hepcidin ferroportin pathway is an intrinsic response to iron overload conditions during AKI
bull Therefore urine HJV (uHJV) has the potential to be an early AKI biomarker in response to iron homeostasis during AKI
Combination of functional and damage biomarkers
bull While new biomarkers are being validated functional biomarkers (serum creatinine serum urea and urine output) continue to be utilized in the diagnosis and staging of AKI In the future existing or newer damage biomarkers will likely be combined with the use of functional biomarkers to enhance the ability of RIFLE AKIN
bull A study of 345 children after cardiopulmonary bypass surgery demonstrated that the composite of functional biomarker such as plasma cystatin C and urinary NGAL was superior to changes in serum creatinine to predict AKI
PROGNOSTIC BIOMARKERS
bull Most of the biomarkers described above allow early detection of acute kidney injury but do not predict severe AKI
Urinary renin and angiotensinogen
bull Urinary renin angiotensinogen and plasma NGAL may predict the development of severe AKI
bull Among 99 consecutively enrolled patients who developed AKI the ratio of urinary angiotensinogen to urinary creatinine (uAnCR expressed as ng per mg creatinine)calculated Patients with the highest uAnCR had a higher risk of worsening AKI compared with patients with the lowest uAnCR An elevated uAnCR predicted a longer hospital stay
bull Among 204 patients who developed Acute Kidney Injury Network (AKIN) stage 1 following cardiac surgery the urinary renin-to-creatinine ratio and the angiotensinogen-to-creatinine ratio predicted a composite outcome of death or AKIN stage 3 or death
Plasma NGAL
bull In a prospective cohort study in which 616 patients admitted from the emergency department were classified by clinical criteria as AKI transient azotemia stable CKD or normal kidney function plasma NGAL discriminated AKI from normal function and from transient azotemia
bull Higher concentrations of NGAL were associated with more severe AKI
Thanks for your attention

Urine dipstick and microscopic examination
bull Routine dipstick and microscopic examinations of urine are often helpful in determining the cause of AKI
bull While granular or epithelial casts in urine are increased in acute tubular necrosis (ATN) they lack sufficient sensitivity specificity and predictive power for routine clinical use
Urinary indices
bull Diagnostic urinary indices of AKI are the fractional excretion of sodium (FENa) urea (FEurea) uric acid urine sodium and urine osmolality
bull Reduced effective circulating volume stimulates anti-diuretic hormone (ADH) release which results in increased distal water and urea reabsorption Thus low FEurea (lt35) is more sensitive and specific than FENa in differentiating between prerenal and renal causes of AKI especially when diuretics have been administered
bull FEurea and FENa have low diagnostic sensitivity in distinguishing azotemia associated with renal vasoconstriction and intact tubular function from established AKI with tubular dysfunction
Urinary tubular enzymes
bull Traditional urinary biomarkers including low- and high-molecular-weight proteins (a1-microglobulin b2- microglobulin retinol-binding proteins) brush border antigens (NaH exchanger isoform-3) urinary enzymes (a-glutathione S-transferase c-glutamyl transpeptidase N-acetyl-b-D-glucosaminidase) and Tamm-Horsfallprotein
bull have not entered clinical routine for AKI patients due to the lack of sufficient validation lack of standardized assays
Urinary tubular enzymes
bull Urinary tubular enzymes consist of proximal renal tubular epithelial antigen (HRTE-1) alpha-glutathione S-transferase (alpha-GST) glutamyltranspeptidase(gamma-GT) alanine aminopeptidase (AAP) lactate dehydrogenase (LDH) N-acetyl-beta-glucosaminidase(NAG) and alkaline phosphatase (ALP)
bull Most of these are released from proximal tubular epithelial cells within 12 hours and four days earlier than a detectable rise in serum creatinine
bull No validated cut-off points currently exist to help distinguish prerenal disease from ATN
Urinary low-molecular-weight proteins
bull Alpha1-microglobulin (alpha1-m) beta2-microglobulin (beta2-m) retinol-binding protein (RBP) adenosine deaminase-binding protein (ABP) and urinary cystatin C are urinary lowmolecular- weight proteins
bull They are produced at different sites filtered at the glomerulus and reabsorbed at the proximal tubule with no secretion
bull Although promising prognostically and to help distinguish prerenal disease from ATN increased levels may be observed after reversible and mild dysfunction and may not necessarily be associated with persistent or irreversible damage
Functional biomarkersSerum creatinine
bull Currently the standard diagnostic tools for AKI detection are SCrconcentration and UO both of which are markers of renal function but not kidney injury
bull SCr is an integrator of various intra- and extra-renal functions and its concentration indicates the balance between creatinine generation and excretion
bull Unfortunately due to the non-linear relationship between GFR and sCr the increase of creatinine may be within the reference range in early phase of AKI and may overlooked
bull SCr does not indicate the severity of the injury until a steady state has been reached in AKI Therefore SCr is a delayed and insensitive biomarker of changes in kidney function moreover its concentration does not differentiate between structural kidney damage and functional hemodynamic triggers and it could be affected by many factors
bull Especially in intensive care unit patients creatinine-based definitions of AKI can be influenced by baseline creatinine estimation fluid overload malnourishment and muscle wasting
Cystatin-C
bull Cystatin-C is produced at a constant rate by nucleated cells filtered by the glomerular cells almost completely reabsorbed and catabolized (but not secreted) in the proximal tubule It is a polypeptide chain with 120 amino acid residues
bull In this way some of the limitations of serum creatinine effect of muscle mass diet gender and tubular secretion may not be a problem with cystatin C and appear to rise one to two days earlier than serum creatinine
bull Cystatin C is better marker of GFR than serum creatinine as demonstrated in several studies
bull Over the past decade Cystatin C (CyC) a serum measure of renal function is a stronger predictor of the risk of death and cardiovascular events in elderly persons than is creatinine
bull Koyner et al demonstrated that urinary CyC was superior to SCr and plasma CyC in the early diagnosis of acute kidney injury following adult cardiac surgery
bull Roos et al performed a systematic review comparing the diagnostic accuracy of plasma and urine CyC with SCr in patients undergoing cardiac surgery They concluded that the diagnostic accuracy for impaired renal function favors urine CyC
bull However while Cys-C levels are a more precise indicator of kidney function than SCr concentration they seem to be influenced by old age large doses of corticosteroids hyperthyroidism inflammation neoplasia smoking and alcohol consumption
bull Currently it is unclear whether the value of Cys-C is generalizable to all forms of AKI or specific to particular populations
Damage biomarkers
Neutrophil Gelatinase-Associated Lipocalin(NGAL)
bull Human NGAL is a 25 kDa protein firstly identified bound to gelatinase in specific granules of the neutrophil NGAL is a critical component of innate immunity to bacterial infection and is expressed by immune cells hepatocytes and renal tubular cells in various disease states
bull Its resistance to proteolysis further enhanced potential suitability as a clinical biomarker
bull In healthy kidneys it is barel detectable in either plasma or urine
bull However in the setting of acute tubular injury NGAL undergoes rapid and profound upregulation with large increases in both urine and plasma
bull Distinct from traditional markers of function such as creatinine this rapid response enables NGAL to potentially identify injured kidney much earlier than was previously possible The endogenous role of NGAL remains unclear It seems to be involved with iron transportation to and from the proximal tubular epithelial cells and animal studies demonstrate a renoprotective effect of exogenously administered NGAL in the setting of acute ischemic injury
bull NGAL was also detected in the urine of mice in the early stage of cisplatin-induced nephrotoxicity
bull These animal studies demonstrated that NGAL may represent an early sensitive and noninvasive urinary biomarker for ischemic and nephrotoxic kidney injury
bull NGAL is markedly upregulated and abundantly expressed in the kidney after renal ischemia
bull In this setting NGAL may function to dampen toxicity by reducing apoptosis and increasing the normal proliferation of kidney tubule cells
bull following ischemia reperfusion as evidenced by a rise in creatinine the kidneys illuminate indicating NGAL production at the site of injury
bull Interestingly following maneuvers that lead to significant prerenal disease there was no NGAL illumination indicating that prerenal disease does not induce NGAL expression
bull Thus NGAL may potentially be useful in differentiating prerenal disease from ATN
bull In these studies the average sensitivity and specificity of NGAL measured one to three days prior to AKI diagnosis was 76 and 77 percent respectively for cardiac surgery patients and 73 and 80 percent respectively for patients admitted to the intensive care unit (ICU)
bull NGAL may also represent early sensitive biomarker of AKI after contrast administrations for coronary angiography
bull NGAL was measured in the serum and urine before and at 2 4 12 24 and 48 h after contrast administration they found a significant rise in serum NGAL 2 and 4 h after PCI and a rise in urinary NGAL 4 and 12 h after PCI
bull A similar study of 25 patients with normal serum creatinine undergoing PCI due to unstable angina There was a significant rise in serum NGAL after 2 and 4 hours Urinary NGAL and urinary L-FABP followed the same pattern Both markers increased significantly after 4 hours and remained elevated up to 48 hours after PCI
bull Urine and plasma NGAL levels also represent early biomarkers of AKI in ICU
bull A multicenter study of serum NGAL was performed in 143 critically ill children with systemic inflammatory response syndrome (SIRS) or septic shock during the first 24 h of admission to the ICU there was a significant difference in serum NGAL between healthy children ill children with SIRS and septic shock the study was concluded that serum NGAL is a highly sensitive but nonspecific predictor of acute kidney injury in critically ill children with septic shock
bull A 2010 study evaluated 88 ICU patient and found that an NGAL level of ge150 nmolL predicted AKI with 82 sensitivity and 97 specificity
bull A recent study had 98 patients who were divided in two groups depending on the presence of sepsis Fifty-six patients had sepsis while forty-two patients were nonseptic Among septic patients subjects who developed AKI showed signi1048853 cant higher levels of NGAL
bull A more study of 65 patients with septic shock were found that urine NGAL levels 12 hours before AKI diagnosis were a good predictor of AKI
Kidney Injury Molecule-1 (KIM-1)
bull KIM-1 mRNA and protein are expressed at a low level in normal kidney but are increased dramatically in postischemic kidney
bull KIM-1 has been identified as the first nonmyeloidphosphatidylserine receptor that confers a phagocytic phenotype on injured epithelial cells both in vivo and in vitro
bull Urinary KIM-1 has been found to be an early indicator of AKI that compares favorably to a number of conventional biomarkers and tubular enzymes
bull KIM-1 is also a tissue and urinary biomarker for nephrotoxicant-induced kidney injury
bull Tissue and urinary expressions were measured with different nephrotoxic doses of cisplatin folic acide cadmium gentamycin mercury
bull As early as 1 day after cisplatin treatment positive KIM- 1 immunostaining observed in the outer medulla of the kidney and changes in urinary clusterin indicated the onset of proximal tubular injury in the absence of functional effects
bull Tissue KIM-1 was the most sensitive biomarker for detection of cisplatin-induced kidney damage
bull KIM-1 is a biomarker of AKI in humans bull Urine samples were collected from 32 patients with various
acute and chronic kidney diseases as well as from eight normal controls there was extensive expression of KIM-1 in proximal tubule cells in kidney biopsies from six patients with biopsy confirmed acute tubular necrosis (ATN)
bull Urinary KIM-1 levels were significantly higher in patients with ischemic ATN compared to levels in patients with other forms of acute renal failure or chronic renal disease
bull Adjusted for age gender and length of time delay between the initial insult and sampling of the urine a one-unit increase in normalized KIM-1 was associated with a greater than 12-fold risk for the presence of ATN
bull In hospital patients with AKI urinary levels of KIM-1 that higher levels correlated with a higher odds ratio for dialysis requirement or hospital death
bull this study demonstrated that urinary biomarker of AKI such as KIM-1 can predict adverse clinical outcomes in patients with AKI
bull Both renal and urinary KIM-1 correlate with kidney damage and negatively with renal function but not with proteinuria
bull A recent study has explored urinary KIM-1correlated with kidney function in kidney allograft recipients Kidney transplant recipients showed significantly higher KIM-1 values than the healthy volunteers this study concluded that even a successful kidney transplantation is associated with kidney injury as reflected by elevated urinary KIM-1
bull A rapid direct 15-minute assay for the detection of urinary human KIM-1 has been developed Using this assay more urinary KIM-1 was detected in the urine of patients with AKI than in the urine from healthy volunteers
Urinary interleukin-18
bull Interleukin18 (IL-18) is a 22 kDa pro-inflammatory cytokine that increases in the kidney after ischemia-reperfusion injury in a caspase- 1-dependent manner
bull Patients with ATN had significantly greater urinary IL-18 concentrations than those with other conditions (healthy controls patients with pre-renal azotemia urinary tract infection CKD and nephrotic syndrome)
bull urinary IL-18 concentrations measured in the first 24 h after kidney transplantation were higher in patients who received a cadaveric kidney that developed delayed graft function compared to patients who received a cadaveric kidney with prompt graft function and patients who received a kidney with prompt graft function from a living donor
bull However the performance of urinary IL-18 measured 1 day before AKI was modest
bull Its predictive utility for AKI following cardiac surgery could not be demonstrated in one prospective observational study of 100 adult patients
bull In addition in a large study population of 1439 critically ill patients IL-18 had a poor-to-moderate ability to predict AKI renal replacement therapy (RRT) or 90-day mortality
Liver-Type Fatty Acid Binding Protein(L-FABP)
bull Liver-type fatty acid-binding protein (L-FABP) is a 14 kDa protein from the large super- family of lipidbinding proteins
bull The 14-kD L-FABP protein can be localized predominantly in the proximal tubule
bull Noiri et al demonstrated that increase of urinary L-FABP was observed at 1 h after ischemia even in the 5-min IRI group and urinary L-FABP was superior to BUN and urinary NAG for early and accurate detection of acute tubular necrosis in different models of animal AKI
bull urinary L-FABP may be a promising biomarker for early detection of AKI and prediction of dialysis requirement and in-hospital mortality
bull Urinary excretion of urinary liver-type fatty acid-binding protein (L-FABP) reflects stress of proximal tubular epithelial cells and correlates with severity of ischemic tubular injury
bull A meta-analysis of 15 prospective cohort studies demonstrated that in hospitalndashbased cohorts of patients at risk of AKI L-FABP can discriminate for the diagnosis of AKI and predict the need for dialysis and in-hospital mortality
bull It was correlated with the degree of tubulointerstitial damage in a folic acid induced nephropathy
bull In ischemic and cisplatin-induced AKI L-FABP was increased in the urine before the increase in BUN
bull In cisplatin-induced AKI urinary L-FABP levels increased exponentially even in the lowest dose group as early as 2 hours whereas BUN levels increased at 48 hours
bull L-FABP was measured in 80 critically ill patients Urinary L-FABP levels in patients with septic shock were significantly higher than severe sepsis without shock Serum L-FABP levels did not have significant differences between patients with septic shock severe sepsis and healthy
bull Another study was evaluated 145 septic shock patients complicated with established AKI Urinary L-FABP measured at admission was significantly higher in the nonsurvivors of septic shock with established acute kidney injury than in the survivors
Failure of the TRIBE-AKI study
bull The Translational Research Investigating Biomarker Endpoints in AKI (TRIBE-AKI) study evaluated the performance of urinary c-glutamyltranspeptidase ( c-GTP) alkaline phosphatase NGAL Cys-C KIM-1 and IL-18 in AKI diagnosis
bull The results of four novel urine biomarkers and one plasma biomarker (urine NGAL IL-18 KIM-1 and L-FABP and plasma NGAL) were provided Of all the novel biomarkers only urine IL-18 and plasma NGAL in adults were helpful in predicting progression of AKI when measured on the day of clinical AKI diagnosis
bull Combinations of three biomarkers in adults from two different time points and combinations of two biomarkers in children from two time points were found to be able to increase the ROC for AKI up to 078
bull In summary the clinical use of single damage biomarkers in AKI prediction remains unclear because large prospective multicenter trials such as the TRIBE-AKI study (nfrac141530) have failed to demonstrate troponin-like diagnostic performance
Various clinical scenarios of AKI based onfunction damage and stress
bull Over the last decade a number of novel damage biomarkers have been evaluated for their capacity to detect kidney damage and predict the development of AKI However the relationship between decreasing function and increasing damage is not as straightforward as might be assumed
bull The characteristic pattern whereby damage precedes loss of function (panel A) may be seen in some cases of AKI and affords an opportunity to detect ldquosubclinicalrdquo AKI before function start to fall Unfortunately other patterns might also occur For example functional decline may start to occur alongside damage (panel B) and in some cases function may start to decline even before damage (panel C)
bull This makes damage markers difficult to use for predicting AKI However other markers might actually measure the ldquostressrdquo occurring at the cellular level before damage or loss of function
Paradigm shift to pre-injury phase biomarkers
bull Katz et al proposed that the pre-injury phase that leads to AKI can be described as ldquoacute kidney stressrdquo (AKS) after the report of the identification of cell cycle arrest biomarkers that signal the potential development of AKI is part of an evolution in the molecular diagnosis and understanding of AKI
bull These biomarkers are released by kidney cells along a path which may lead to AKI during a pre-injury phase
bull AKS is defined as the increased-risk phase (pre-injury phase) that leads to AKI
bull This ldquoAKSrdquo may or may not lead to damage and functional declinebull But it is the earliest possible the process of AKI can be detected
Pre-injury phase biomarkers
Stress biomarkersbull In 2013 Kashani et al reported the results of a prospective international
observational investigation (the Sapphire study) of tissue inhibitor of metalloproteinases- 2 (TIMP-2) and insulin-like growth factor-binding protein 7 (IGFBP7) in a heterogeneous group of critically ill patients [TIMP-2][IGFBP7] was significantly superior to all previously described markers of AKI (plt0002)
bull Next the Opal and Topaz study showed the cut-off value and risk assessment using the urinary[TIMP-2] [IGFBP7]
bull The urine [IGFBP7][TIMP2] biomarker is already FDA approved and commercially available in the United States
bull Falsepositive results are common and they will be magnified if the test is used inappropriately in low-risk patients In addition this biomarker should not be used in ambulatory practices and it is not beneficial in patients with established AKI
microRNAsbull microRNAs (miRNAs) are endogenous single-stranded non-coding
mRNAs of about 19-23 nucleotides bull In the past years researchers have begun to investigate the
relevance of miRNAs to AKI with many miRNAs being implicated bull Some of them contribute to pathogenesis by regulating apoptosis
and inflammation amplifying or reducing acute injury responses while others regulate fibrosis and angiogenesis participating in renal recovery or progression to fibrosis
bull Certain miRNAs have been investigated for their potential as novel biomarkers for the early detection or prognostication of AKI
Hemojuvelinbull Hemojuvelin (HJV) a glycophosphatidylinositol (GPI)- linked
membrane protein is highly expressed in liver and skeletal musclesbull The molecular weight of HJV is 42 kDa for the soluble form (sHJV)
and can be passed through glomerular filtration and reabsorbed by the renal tubules Increased iron content in the kidney and urine is observed in human and animal models of AKI and increased iron load can induce renal tubular cell injury
bull There is evidence that the increased expression of the hemojuvelin-hepcidin ferroportin pathway is an intrinsic response to iron overload conditions during AKI
bull Therefore urine HJV (uHJV) has the potential to be an early AKI biomarker in response to iron homeostasis during AKI
Combination of functional and damage biomarkers
bull While new biomarkers are being validated functional biomarkers (serum creatinine serum urea and urine output) continue to be utilized in the diagnosis and staging of AKI In the future existing or newer damage biomarkers will likely be combined with the use of functional biomarkers to enhance the ability of RIFLE AKIN
bull A study of 345 children after cardiopulmonary bypass surgery demonstrated that the composite of functional biomarker such as plasma cystatin C and urinary NGAL was superior to changes in serum creatinine to predict AKI
PROGNOSTIC BIOMARKERS
bull Most of the biomarkers described above allow early detection of acute kidney injury but do not predict severe AKI
Urinary renin and angiotensinogen
bull Urinary renin angiotensinogen and plasma NGAL may predict the development of severe AKI
bull Among 99 consecutively enrolled patients who developed AKI the ratio of urinary angiotensinogen to urinary creatinine (uAnCR expressed as ng per mg creatinine)calculated Patients with the highest uAnCR had a higher risk of worsening AKI compared with patients with the lowest uAnCR An elevated uAnCR predicted a longer hospital stay
bull Among 204 patients who developed Acute Kidney Injury Network (AKIN) stage 1 following cardiac surgery the urinary renin-to-creatinine ratio and the angiotensinogen-to-creatinine ratio predicted a composite outcome of death or AKIN stage 3 or death
Plasma NGAL
bull In a prospective cohort study in which 616 patients admitted from the emergency department were classified by clinical criteria as AKI transient azotemia stable CKD or normal kidney function plasma NGAL discriminated AKI from normal function and from transient azotemia
bull Higher concentrations of NGAL were associated with more severe AKI
Thanks for your attention

Urinary indices
bull Diagnostic urinary indices of AKI are the fractional excretion of sodium (FENa) urea (FEurea) uric acid urine sodium and urine osmolality
bull Reduced effective circulating volume stimulates anti-diuretic hormone (ADH) release which results in increased distal water and urea reabsorption Thus low FEurea (lt35) is more sensitive and specific than FENa in differentiating between prerenal and renal causes of AKI especially when diuretics have been administered
bull FEurea and FENa have low diagnostic sensitivity in distinguishing azotemia associated with renal vasoconstriction and intact tubular function from established AKI with tubular dysfunction
Urinary tubular enzymes
bull Traditional urinary biomarkers including low- and high-molecular-weight proteins (a1-microglobulin b2- microglobulin retinol-binding proteins) brush border antigens (NaH exchanger isoform-3) urinary enzymes (a-glutathione S-transferase c-glutamyl transpeptidase N-acetyl-b-D-glucosaminidase) and Tamm-Horsfallprotein
bull have not entered clinical routine for AKI patients due to the lack of sufficient validation lack of standardized assays
Urinary tubular enzymes
bull Urinary tubular enzymes consist of proximal renal tubular epithelial antigen (HRTE-1) alpha-glutathione S-transferase (alpha-GST) glutamyltranspeptidase(gamma-GT) alanine aminopeptidase (AAP) lactate dehydrogenase (LDH) N-acetyl-beta-glucosaminidase(NAG) and alkaline phosphatase (ALP)
bull Most of these are released from proximal tubular epithelial cells within 12 hours and four days earlier than a detectable rise in serum creatinine
bull No validated cut-off points currently exist to help distinguish prerenal disease from ATN
Urinary low-molecular-weight proteins
bull Alpha1-microglobulin (alpha1-m) beta2-microglobulin (beta2-m) retinol-binding protein (RBP) adenosine deaminase-binding protein (ABP) and urinary cystatin C are urinary lowmolecular- weight proteins
bull They are produced at different sites filtered at the glomerulus and reabsorbed at the proximal tubule with no secretion
bull Although promising prognostically and to help distinguish prerenal disease from ATN increased levels may be observed after reversible and mild dysfunction and may not necessarily be associated with persistent or irreversible damage
Functional biomarkersSerum creatinine
bull Currently the standard diagnostic tools for AKI detection are SCrconcentration and UO both of which are markers of renal function but not kidney injury
bull SCr is an integrator of various intra- and extra-renal functions and its concentration indicates the balance between creatinine generation and excretion
bull Unfortunately due to the non-linear relationship between GFR and sCr the increase of creatinine may be within the reference range in early phase of AKI and may overlooked
bull SCr does not indicate the severity of the injury until a steady state has been reached in AKI Therefore SCr is a delayed and insensitive biomarker of changes in kidney function moreover its concentration does not differentiate between structural kidney damage and functional hemodynamic triggers and it could be affected by many factors
bull Especially in intensive care unit patients creatinine-based definitions of AKI can be influenced by baseline creatinine estimation fluid overload malnourishment and muscle wasting
Cystatin-C
bull Cystatin-C is produced at a constant rate by nucleated cells filtered by the glomerular cells almost completely reabsorbed and catabolized (but not secreted) in the proximal tubule It is a polypeptide chain with 120 amino acid residues
bull In this way some of the limitations of serum creatinine effect of muscle mass diet gender and tubular secretion may not be a problem with cystatin C and appear to rise one to two days earlier than serum creatinine
bull Cystatin C is better marker of GFR than serum creatinine as demonstrated in several studies
bull Over the past decade Cystatin C (CyC) a serum measure of renal function is a stronger predictor of the risk of death and cardiovascular events in elderly persons than is creatinine
bull Koyner et al demonstrated that urinary CyC was superior to SCr and plasma CyC in the early diagnosis of acute kidney injury following adult cardiac surgery
bull Roos et al performed a systematic review comparing the diagnostic accuracy of plasma and urine CyC with SCr in patients undergoing cardiac surgery They concluded that the diagnostic accuracy for impaired renal function favors urine CyC
bull However while Cys-C levels are a more precise indicator of kidney function than SCr concentration they seem to be influenced by old age large doses of corticosteroids hyperthyroidism inflammation neoplasia smoking and alcohol consumption
bull Currently it is unclear whether the value of Cys-C is generalizable to all forms of AKI or specific to particular populations
Damage biomarkers
Neutrophil Gelatinase-Associated Lipocalin(NGAL)
bull Human NGAL is a 25 kDa protein firstly identified bound to gelatinase in specific granules of the neutrophil NGAL is a critical component of innate immunity to bacterial infection and is expressed by immune cells hepatocytes and renal tubular cells in various disease states
bull Its resistance to proteolysis further enhanced potential suitability as a clinical biomarker
bull In healthy kidneys it is barel detectable in either plasma or urine
bull However in the setting of acute tubular injury NGAL undergoes rapid and profound upregulation with large increases in both urine and plasma
bull Distinct from traditional markers of function such as creatinine this rapid response enables NGAL to potentially identify injured kidney much earlier than was previously possible The endogenous role of NGAL remains unclear It seems to be involved with iron transportation to and from the proximal tubular epithelial cells and animal studies demonstrate a renoprotective effect of exogenously administered NGAL in the setting of acute ischemic injury
bull NGAL was also detected in the urine of mice in the early stage of cisplatin-induced nephrotoxicity
bull These animal studies demonstrated that NGAL may represent an early sensitive and noninvasive urinary biomarker for ischemic and nephrotoxic kidney injury
bull NGAL is markedly upregulated and abundantly expressed in the kidney after renal ischemia
bull In this setting NGAL may function to dampen toxicity by reducing apoptosis and increasing the normal proliferation of kidney tubule cells
bull following ischemia reperfusion as evidenced by a rise in creatinine the kidneys illuminate indicating NGAL production at the site of injury
bull Interestingly following maneuvers that lead to significant prerenal disease there was no NGAL illumination indicating that prerenal disease does not induce NGAL expression
bull Thus NGAL may potentially be useful in differentiating prerenal disease from ATN
bull In these studies the average sensitivity and specificity of NGAL measured one to three days prior to AKI diagnosis was 76 and 77 percent respectively for cardiac surgery patients and 73 and 80 percent respectively for patients admitted to the intensive care unit (ICU)
bull NGAL may also represent early sensitive biomarker of AKI after contrast administrations for coronary angiography
bull NGAL was measured in the serum and urine before and at 2 4 12 24 and 48 h after contrast administration they found a significant rise in serum NGAL 2 and 4 h after PCI and a rise in urinary NGAL 4 and 12 h after PCI
bull A similar study of 25 patients with normal serum creatinine undergoing PCI due to unstable angina There was a significant rise in serum NGAL after 2 and 4 hours Urinary NGAL and urinary L-FABP followed the same pattern Both markers increased significantly after 4 hours and remained elevated up to 48 hours after PCI
bull Urine and plasma NGAL levels also represent early biomarkers of AKI in ICU
bull A multicenter study of serum NGAL was performed in 143 critically ill children with systemic inflammatory response syndrome (SIRS) or septic shock during the first 24 h of admission to the ICU there was a significant difference in serum NGAL between healthy children ill children with SIRS and septic shock the study was concluded that serum NGAL is a highly sensitive but nonspecific predictor of acute kidney injury in critically ill children with septic shock
bull A 2010 study evaluated 88 ICU patient and found that an NGAL level of ge150 nmolL predicted AKI with 82 sensitivity and 97 specificity
bull A recent study had 98 patients who were divided in two groups depending on the presence of sepsis Fifty-six patients had sepsis while forty-two patients were nonseptic Among septic patients subjects who developed AKI showed signi1048853 cant higher levels of NGAL
bull A more study of 65 patients with septic shock were found that urine NGAL levels 12 hours before AKI diagnosis were a good predictor of AKI
Kidney Injury Molecule-1 (KIM-1)
bull KIM-1 mRNA and protein are expressed at a low level in normal kidney but are increased dramatically in postischemic kidney
bull KIM-1 has been identified as the first nonmyeloidphosphatidylserine receptor that confers a phagocytic phenotype on injured epithelial cells both in vivo and in vitro
bull Urinary KIM-1 has been found to be an early indicator of AKI that compares favorably to a number of conventional biomarkers and tubular enzymes
bull KIM-1 is also a tissue and urinary biomarker for nephrotoxicant-induced kidney injury
bull Tissue and urinary expressions were measured with different nephrotoxic doses of cisplatin folic acide cadmium gentamycin mercury
bull As early as 1 day after cisplatin treatment positive KIM- 1 immunostaining observed in the outer medulla of the kidney and changes in urinary clusterin indicated the onset of proximal tubular injury in the absence of functional effects
bull Tissue KIM-1 was the most sensitive biomarker for detection of cisplatin-induced kidney damage
bull KIM-1 is a biomarker of AKI in humans bull Urine samples were collected from 32 patients with various
acute and chronic kidney diseases as well as from eight normal controls there was extensive expression of KIM-1 in proximal tubule cells in kidney biopsies from six patients with biopsy confirmed acute tubular necrosis (ATN)
bull Urinary KIM-1 levels were significantly higher in patients with ischemic ATN compared to levels in patients with other forms of acute renal failure or chronic renal disease
bull Adjusted for age gender and length of time delay between the initial insult and sampling of the urine a one-unit increase in normalized KIM-1 was associated with a greater than 12-fold risk for the presence of ATN
bull In hospital patients with AKI urinary levels of KIM-1 that higher levels correlated with a higher odds ratio for dialysis requirement or hospital death
bull this study demonstrated that urinary biomarker of AKI such as KIM-1 can predict adverse clinical outcomes in patients with AKI
bull Both renal and urinary KIM-1 correlate with kidney damage and negatively with renal function but not with proteinuria
bull A recent study has explored urinary KIM-1correlated with kidney function in kidney allograft recipients Kidney transplant recipients showed significantly higher KIM-1 values than the healthy volunteers this study concluded that even a successful kidney transplantation is associated with kidney injury as reflected by elevated urinary KIM-1
bull A rapid direct 15-minute assay for the detection of urinary human KIM-1 has been developed Using this assay more urinary KIM-1 was detected in the urine of patients with AKI than in the urine from healthy volunteers
Urinary interleukin-18
bull Interleukin18 (IL-18) is a 22 kDa pro-inflammatory cytokine that increases in the kidney after ischemia-reperfusion injury in a caspase- 1-dependent manner
bull Patients with ATN had significantly greater urinary IL-18 concentrations than those with other conditions (healthy controls patients with pre-renal azotemia urinary tract infection CKD and nephrotic syndrome)
bull urinary IL-18 concentrations measured in the first 24 h after kidney transplantation were higher in patients who received a cadaveric kidney that developed delayed graft function compared to patients who received a cadaveric kidney with prompt graft function and patients who received a kidney with prompt graft function from a living donor
bull However the performance of urinary IL-18 measured 1 day before AKI was modest
bull Its predictive utility for AKI following cardiac surgery could not be demonstrated in one prospective observational study of 100 adult patients
bull In addition in a large study population of 1439 critically ill patients IL-18 had a poor-to-moderate ability to predict AKI renal replacement therapy (RRT) or 90-day mortality
Liver-Type Fatty Acid Binding Protein(L-FABP)
bull Liver-type fatty acid-binding protein (L-FABP) is a 14 kDa protein from the large super- family of lipidbinding proteins
bull The 14-kD L-FABP protein can be localized predominantly in the proximal tubule
bull Noiri et al demonstrated that increase of urinary L-FABP was observed at 1 h after ischemia even in the 5-min IRI group and urinary L-FABP was superior to BUN and urinary NAG for early and accurate detection of acute tubular necrosis in different models of animal AKI
bull urinary L-FABP may be a promising biomarker for early detection of AKI and prediction of dialysis requirement and in-hospital mortality
bull Urinary excretion of urinary liver-type fatty acid-binding protein (L-FABP) reflects stress of proximal tubular epithelial cells and correlates with severity of ischemic tubular injury
bull A meta-analysis of 15 prospective cohort studies demonstrated that in hospitalndashbased cohorts of patients at risk of AKI L-FABP can discriminate for the diagnosis of AKI and predict the need for dialysis and in-hospital mortality
bull It was correlated with the degree of tubulointerstitial damage in a folic acid induced nephropathy
bull In ischemic and cisplatin-induced AKI L-FABP was increased in the urine before the increase in BUN
bull In cisplatin-induced AKI urinary L-FABP levels increased exponentially even in the lowest dose group as early as 2 hours whereas BUN levels increased at 48 hours
bull L-FABP was measured in 80 critically ill patients Urinary L-FABP levels in patients with septic shock were significantly higher than severe sepsis without shock Serum L-FABP levels did not have significant differences between patients with septic shock severe sepsis and healthy
bull Another study was evaluated 145 septic shock patients complicated with established AKI Urinary L-FABP measured at admission was significantly higher in the nonsurvivors of septic shock with established acute kidney injury than in the survivors
Failure of the TRIBE-AKI study
bull The Translational Research Investigating Biomarker Endpoints in AKI (TRIBE-AKI) study evaluated the performance of urinary c-glutamyltranspeptidase ( c-GTP) alkaline phosphatase NGAL Cys-C KIM-1 and IL-18 in AKI diagnosis
bull The results of four novel urine biomarkers and one plasma biomarker (urine NGAL IL-18 KIM-1 and L-FABP and plasma NGAL) were provided Of all the novel biomarkers only urine IL-18 and plasma NGAL in adults were helpful in predicting progression of AKI when measured on the day of clinical AKI diagnosis
bull Combinations of three biomarkers in adults from two different time points and combinations of two biomarkers in children from two time points were found to be able to increase the ROC for AKI up to 078
bull In summary the clinical use of single damage biomarkers in AKI prediction remains unclear because large prospective multicenter trials such as the TRIBE-AKI study (nfrac141530) have failed to demonstrate troponin-like diagnostic performance
Various clinical scenarios of AKI based onfunction damage and stress
bull Over the last decade a number of novel damage biomarkers have been evaluated for their capacity to detect kidney damage and predict the development of AKI However the relationship between decreasing function and increasing damage is not as straightforward as might be assumed
bull The characteristic pattern whereby damage precedes loss of function (panel A) may be seen in some cases of AKI and affords an opportunity to detect ldquosubclinicalrdquo AKI before function start to fall Unfortunately other patterns might also occur For example functional decline may start to occur alongside damage (panel B) and in some cases function may start to decline even before damage (panel C)
bull This makes damage markers difficult to use for predicting AKI However other markers might actually measure the ldquostressrdquo occurring at the cellular level before damage or loss of function
Paradigm shift to pre-injury phase biomarkers
bull Katz et al proposed that the pre-injury phase that leads to AKI can be described as ldquoacute kidney stressrdquo (AKS) after the report of the identification of cell cycle arrest biomarkers that signal the potential development of AKI is part of an evolution in the molecular diagnosis and understanding of AKI
bull These biomarkers are released by kidney cells along a path which may lead to AKI during a pre-injury phase
bull AKS is defined as the increased-risk phase (pre-injury phase) that leads to AKI
bull This ldquoAKSrdquo may or may not lead to damage and functional declinebull But it is the earliest possible the process of AKI can be detected
Pre-injury phase biomarkers
Stress biomarkersbull In 2013 Kashani et al reported the results of a prospective international
observational investigation (the Sapphire study) of tissue inhibitor of metalloproteinases- 2 (TIMP-2) and insulin-like growth factor-binding protein 7 (IGFBP7) in a heterogeneous group of critically ill patients [TIMP-2][IGFBP7] was significantly superior to all previously described markers of AKI (plt0002)
bull Next the Opal and Topaz study showed the cut-off value and risk assessment using the urinary[TIMP-2] [IGFBP7]
bull The urine [IGFBP7][TIMP2] biomarker is already FDA approved and commercially available in the United States
bull Falsepositive results are common and they will be magnified if the test is used inappropriately in low-risk patients In addition this biomarker should not be used in ambulatory practices and it is not beneficial in patients with established AKI
microRNAsbull microRNAs (miRNAs) are endogenous single-stranded non-coding
mRNAs of about 19-23 nucleotides bull In the past years researchers have begun to investigate the
relevance of miRNAs to AKI with many miRNAs being implicated bull Some of them contribute to pathogenesis by regulating apoptosis
and inflammation amplifying or reducing acute injury responses while others regulate fibrosis and angiogenesis participating in renal recovery or progression to fibrosis
bull Certain miRNAs have been investigated for their potential as novel biomarkers for the early detection or prognostication of AKI
Hemojuvelinbull Hemojuvelin (HJV) a glycophosphatidylinositol (GPI)- linked
membrane protein is highly expressed in liver and skeletal musclesbull The molecular weight of HJV is 42 kDa for the soluble form (sHJV)
and can be passed through glomerular filtration and reabsorbed by the renal tubules Increased iron content in the kidney and urine is observed in human and animal models of AKI and increased iron load can induce renal tubular cell injury
bull There is evidence that the increased expression of the hemojuvelin-hepcidin ferroportin pathway is an intrinsic response to iron overload conditions during AKI
bull Therefore urine HJV (uHJV) has the potential to be an early AKI biomarker in response to iron homeostasis during AKI
Combination of functional and damage biomarkers
bull While new biomarkers are being validated functional biomarkers (serum creatinine serum urea and urine output) continue to be utilized in the diagnosis and staging of AKI In the future existing or newer damage biomarkers will likely be combined with the use of functional biomarkers to enhance the ability of RIFLE AKIN
bull A study of 345 children after cardiopulmonary bypass surgery demonstrated that the composite of functional biomarker such as plasma cystatin C and urinary NGAL was superior to changes in serum creatinine to predict AKI
PROGNOSTIC BIOMARKERS
bull Most of the biomarkers described above allow early detection of acute kidney injury but do not predict severe AKI
Urinary renin and angiotensinogen
bull Urinary renin angiotensinogen and plasma NGAL may predict the development of severe AKI
bull Among 99 consecutively enrolled patients who developed AKI the ratio of urinary angiotensinogen to urinary creatinine (uAnCR expressed as ng per mg creatinine)calculated Patients with the highest uAnCR had a higher risk of worsening AKI compared with patients with the lowest uAnCR An elevated uAnCR predicted a longer hospital stay
bull Among 204 patients who developed Acute Kidney Injury Network (AKIN) stage 1 following cardiac surgery the urinary renin-to-creatinine ratio and the angiotensinogen-to-creatinine ratio predicted a composite outcome of death or AKIN stage 3 or death
Plasma NGAL
bull In a prospective cohort study in which 616 patients admitted from the emergency department were classified by clinical criteria as AKI transient azotemia stable CKD or normal kidney function plasma NGAL discriminated AKI from normal function and from transient azotemia
bull Higher concentrations of NGAL were associated with more severe AKI
Thanks for your attention

Urinary tubular enzymes
bull Traditional urinary biomarkers including low- and high-molecular-weight proteins (a1-microglobulin b2- microglobulin retinol-binding proteins) brush border antigens (NaH exchanger isoform-3) urinary enzymes (a-glutathione S-transferase c-glutamyl transpeptidase N-acetyl-b-D-glucosaminidase) and Tamm-Horsfallprotein
bull have not entered clinical routine for AKI patients due to the lack of sufficient validation lack of standardized assays
Urinary tubular enzymes
bull Urinary tubular enzymes consist of proximal renal tubular epithelial antigen (HRTE-1) alpha-glutathione S-transferase (alpha-GST) glutamyltranspeptidase(gamma-GT) alanine aminopeptidase (AAP) lactate dehydrogenase (LDH) N-acetyl-beta-glucosaminidase(NAG) and alkaline phosphatase (ALP)
bull Most of these are released from proximal tubular epithelial cells within 12 hours and four days earlier than a detectable rise in serum creatinine
bull No validated cut-off points currently exist to help distinguish prerenal disease from ATN
Urinary low-molecular-weight proteins
bull Alpha1-microglobulin (alpha1-m) beta2-microglobulin (beta2-m) retinol-binding protein (RBP) adenosine deaminase-binding protein (ABP) and urinary cystatin C are urinary lowmolecular- weight proteins
bull They are produced at different sites filtered at the glomerulus and reabsorbed at the proximal tubule with no secretion
bull Although promising prognostically and to help distinguish prerenal disease from ATN increased levels may be observed after reversible and mild dysfunction and may not necessarily be associated with persistent or irreversible damage
Functional biomarkersSerum creatinine
bull Currently the standard diagnostic tools for AKI detection are SCrconcentration and UO both of which are markers of renal function but not kidney injury
bull SCr is an integrator of various intra- and extra-renal functions and its concentration indicates the balance between creatinine generation and excretion
bull Unfortunately due to the non-linear relationship between GFR and sCr the increase of creatinine may be within the reference range in early phase of AKI and may overlooked
bull SCr does not indicate the severity of the injury until a steady state has been reached in AKI Therefore SCr is a delayed and insensitive biomarker of changes in kidney function moreover its concentration does not differentiate between structural kidney damage and functional hemodynamic triggers and it could be affected by many factors
bull Especially in intensive care unit patients creatinine-based definitions of AKI can be influenced by baseline creatinine estimation fluid overload malnourishment and muscle wasting
Cystatin-C
bull Cystatin-C is produced at a constant rate by nucleated cells filtered by the glomerular cells almost completely reabsorbed and catabolized (but not secreted) in the proximal tubule It is a polypeptide chain with 120 amino acid residues
bull In this way some of the limitations of serum creatinine effect of muscle mass diet gender and tubular secretion may not be a problem with cystatin C and appear to rise one to two days earlier than serum creatinine
bull Cystatin C is better marker of GFR than serum creatinine as demonstrated in several studies
bull Over the past decade Cystatin C (CyC) a serum measure of renal function is a stronger predictor of the risk of death and cardiovascular events in elderly persons than is creatinine
bull Koyner et al demonstrated that urinary CyC was superior to SCr and plasma CyC in the early diagnosis of acute kidney injury following adult cardiac surgery
bull Roos et al performed a systematic review comparing the diagnostic accuracy of plasma and urine CyC with SCr in patients undergoing cardiac surgery They concluded that the diagnostic accuracy for impaired renal function favors urine CyC
bull However while Cys-C levels are a more precise indicator of kidney function than SCr concentration they seem to be influenced by old age large doses of corticosteroids hyperthyroidism inflammation neoplasia smoking and alcohol consumption
bull Currently it is unclear whether the value of Cys-C is generalizable to all forms of AKI or specific to particular populations
Damage biomarkers
Neutrophil Gelatinase-Associated Lipocalin(NGAL)
bull Human NGAL is a 25 kDa protein firstly identified bound to gelatinase in specific granules of the neutrophil NGAL is a critical component of innate immunity to bacterial infection and is expressed by immune cells hepatocytes and renal tubular cells in various disease states
bull Its resistance to proteolysis further enhanced potential suitability as a clinical biomarker
bull In healthy kidneys it is barel detectable in either plasma or urine
bull However in the setting of acute tubular injury NGAL undergoes rapid and profound upregulation with large increases in both urine and plasma
bull Distinct from traditional markers of function such as creatinine this rapid response enables NGAL to potentially identify injured kidney much earlier than was previously possible The endogenous role of NGAL remains unclear It seems to be involved with iron transportation to and from the proximal tubular epithelial cells and animal studies demonstrate a renoprotective effect of exogenously administered NGAL in the setting of acute ischemic injury
bull NGAL was also detected in the urine of mice in the early stage of cisplatin-induced nephrotoxicity
bull These animal studies demonstrated that NGAL may represent an early sensitive and noninvasive urinary biomarker for ischemic and nephrotoxic kidney injury
bull NGAL is markedly upregulated and abundantly expressed in the kidney after renal ischemia
bull In this setting NGAL may function to dampen toxicity by reducing apoptosis and increasing the normal proliferation of kidney tubule cells
bull following ischemia reperfusion as evidenced by a rise in creatinine the kidneys illuminate indicating NGAL production at the site of injury
bull Interestingly following maneuvers that lead to significant prerenal disease there was no NGAL illumination indicating that prerenal disease does not induce NGAL expression
bull Thus NGAL may potentially be useful in differentiating prerenal disease from ATN
bull In these studies the average sensitivity and specificity of NGAL measured one to three days prior to AKI diagnosis was 76 and 77 percent respectively for cardiac surgery patients and 73 and 80 percent respectively for patients admitted to the intensive care unit (ICU)
bull NGAL may also represent early sensitive biomarker of AKI after contrast administrations for coronary angiography
bull NGAL was measured in the serum and urine before and at 2 4 12 24 and 48 h after contrast administration they found a significant rise in serum NGAL 2 and 4 h after PCI and a rise in urinary NGAL 4 and 12 h after PCI
bull A similar study of 25 patients with normal serum creatinine undergoing PCI due to unstable angina There was a significant rise in serum NGAL after 2 and 4 hours Urinary NGAL and urinary L-FABP followed the same pattern Both markers increased significantly after 4 hours and remained elevated up to 48 hours after PCI
bull Urine and plasma NGAL levels also represent early biomarkers of AKI in ICU
bull A multicenter study of serum NGAL was performed in 143 critically ill children with systemic inflammatory response syndrome (SIRS) or septic shock during the first 24 h of admission to the ICU there was a significant difference in serum NGAL between healthy children ill children with SIRS and septic shock the study was concluded that serum NGAL is a highly sensitive but nonspecific predictor of acute kidney injury in critically ill children with septic shock
bull A 2010 study evaluated 88 ICU patient and found that an NGAL level of ge150 nmolL predicted AKI with 82 sensitivity and 97 specificity
bull A recent study had 98 patients who were divided in two groups depending on the presence of sepsis Fifty-six patients had sepsis while forty-two patients were nonseptic Among septic patients subjects who developed AKI showed signi1048853 cant higher levels of NGAL
bull A more study of 65 patients with septic shock were found that urine NGAL levels 12 hours before AKI diagnosis were a good predictor of AKI
Kidney Injury Molecule-1 (KIM-1)
bull KIM-1 mRNA and protein are expressed at a low level in normal kidney but are increased dramatically in postischemic kidney
bull KIM-1 has been identified as the first nonmyeloidphosphatidylserine receptor that confers a phagocytic phenotype on injured epithelial cells both in vivo and in vitro
bull Urinary KIM-1 has been found to be an early indicator of AKI that compares favorably to a number of conventional biomarkers and tubular enzymes
bull KIM-1 is also a tissue and urinary biomarker for nephrotoxicant-induced kidney injury
bull Tissue and urinary expressions were measured with different nephrotoxic doses of cisplatin folic acide cadmium gentamycin mercury
bull As early as 1 day after cisplatin treatment positive KIM- 1 immunostaining observed in the outer medulla of the kidney and changes in urinary clusterin indicated the onset of proximal tubular injury in the absence of functional effects
bull Tissue KIM-1 was the most sensitive biomarker for detection of cisplatin-induced kidney damage
bull KIM-1 is a biomarker of AKI in humans bull Urine samples were collected from 32 patients with various
acute and chronic kidney diseases as well as from eight normal controls there was extensive expression of KIM-1 in proximal tubule cells in kidney biopsies from six patients with biopsy confirmed acute tubular necrosis (ATN)
bull Urinary KIM-1 levels were significantly higher in patients with ischemic ATN compared to levels in patients with other forms of acute renal failure or chronic renal disease
bull Adjusted for age gender and length of time delay between the initial insult and sampling of the urine a one-unit increase in normalized KIM-1 was associated with a greater than 12-fold risk for the presence of ATN
bull In hospital patients with AKI urinary levels of KIM-1 that higher levels correlated with a higher odds ratio for dialysis requirement or hospital death
bull this study demonstrated that urinary biomarker of AKI such as KIM-1 can predict adverse clinical outcomes in patients with AKI
bull Both renal and urinary KIM-1 correlate with kidney damage and negatively with renal function but not with proteinuria
bull A recent study has explored urinary KIM-1correlated with kidney function in kidney allograft recipients Kidney transplant recipients showed significantly higher KIM-1 values than the healthy volunteers this study concluded that even a successful kidney transplantation is associated with kidney injury as reflected by elevated urinary KIM-1
bull A rapid direct 15-minute assay for the detection of urinary human KIM-1 has been developed Using this assay more urinary KIM-1 was detected in the urine of patients with AKI than in the urine from healthy volunteers
Urinary interleukin-18
bull Interleukin18 (IL-18) is a 22 kDa pro-inflammatory cytokine that increases in the kidney after ischemia-reperfusion injury in a caspase- 1-dependent manner
bull Patients with ATN had significantly greater urinary IL-18 concentrations than those with other conditions (healthy controls patients with pre-renal azotemia urinary tract infection CKD and nephrotic syndrome)
bull urinary IL-18 concentrations measured in the first 24 h after kidney transplantation were higher in patients who received a cadaveric kidney that developed delayed graft function compared to patients who received a cadaveric kidney with prompt graft function and patients who received a kidney with prompt graft function from a living donor
bull However the performance of urinary IL-18 measured 1 day before AKI was modest
bull Its predictive utility for AKI following cardiac surgery could not be demonstrated in one prospective observational study of 100 adult patients
bull In addition in a large study population of 1439 critically ill patients IL-18 had a poor-to-moderate ability to predict AKI renal replacement therapy (RRT) or 90-day mortality
Liver-Type Fatty Acid Binding Protein(L-FABP)
bull Liver-type fatty acid-binding protein (L-FABP) is a 14 kDa protein from the large super- family of lipidbinding proteins
bull The 14-kD L-FABP protein can be localized predominantly in the proximal tubule
bull Noiri et al demonstrated that increase of urinary L-FABP was observed at 1 h after ischemia even in the 5-min IRI group and urinary L-FABP was superior to BUN and urinary NAG for early and accurate detection of acute tubular necrosis in different models of animal AKI
bull urinary L-FABP may be a promising biomarker for early detection of AKI and prediction of dialysis requirement and in-hospital mortality
bull Urinary excretion of urinary liver-type fatty acid-binding protein (L-FABP) reflects stress of proximal tubular epithelial cells and correlates with severity of ischemic tubular injury
bull A meta-analysis of 15 prospective cohort studies demonstrated that in hospitalndashbased cohorts of patients at risk of AKI L-FABP can discriminate for the diagnosis of AKI and predict the need for dialysis and in-hospital mortality
bull It was correlated with the degree of tubulointerstitial damage in a folic acid induced nephropathy
bull In ischemic and cisplatin-induced AKI L-FABP was increased in the urine before the increase in BUN
bull In cisplatin-induced AKI urinary L-FABP levels increased exponentially even in the lowest dose group as early as 2 hours whereas BUN levels increased at 48 hours
bull L-FABP was measured in 80 critically ill patients Urinary L-FABP levels in patients with septic shock were significantly higher than severe sepsis without shock Serum L-FABP levels did not have significant differences between patients with septic shock severe sepsis and healthy
bull Another study was evaluated 145 septic shock patients complicated with established AKI Urinary L-FABP measured at admission was significantly higher in the nonsurvivors of septic shock with established acute kidney injury than in the survivors
Failure of the TRIBE-AKI study
bull The Translational Research Investigating Biomarker Endpoints in AKI (TRIBE-AKI) study evaluated the performance of urinary c-glutamyltranspeptidase ( c-GTP) alkaline phosphatase NGAL Cys-C KIM-1 and IL-18 in AKI diagnosis
bull The results of four novel urine biomarkers and one plasma biomarker (urine NGAL IL-18 KIM-1 and L-FABP and plasma NGAL) were provided Of all the novel biomarkers only urine IL-18 and plasma NGAL in adults were helpful in predicting progression of AKI when measured on the day of clinical AKI diagnosis
bull Combinations of three biomarkers in adults from two different time points and combinations of two biomarkers in children from two time points were found to be able to increase the ROC for AKI up to 078
bull In summary the clinical use of single damage biomarkers in AKI prediction remains unclear because large prospective multicenter trials such as the TRIBE-AKI study (nfrac141530) have failed to demonstrate troponin-like diagnostic performance
Various clinical scenarios of AKI based onfunction damage and stress
bull Over the last decade a number of novel damage biomarkers have been evaluated for their capacity to detect kidney damage and predict the development of AKI However the relationship between decreasing function and increasing damage is not as straightforward as might be assumed
bull The characteristic pattern whereby damage precedes loss of function (panel A) may be seen in some cases of AKI and affords an opportunity to detect ldquosubclinicalrdquo AKI before function start to fall Unfortunately other patterns might also occur For example functional decline may start to occur alongside damage (panel B) and in some cases function may start to decline even before damage (panel C)
bull This makes damage markers difficult to use for predicting AKI However other markers might actually measure the ldquostressrdquo occurring at the cellular level before damage or loss of function
Paradigm shift to pre-injury phase biomarkers
bull Katz et al proposed that the pre-injury phase that leads to AKI can be described as ldquoacute kidney stressrdquo (AKS) after the report of the identification of cell cycle arrest biomarkers that signal the potential development of AKI is part of an evolution in the molecular diagnosis and understanding of AKI
bull These biomarkers are released by kidney cells along a path which may lead to AKI during a pre-injury phase
bull AKS is defined as the increased-risk phase (pre-injury phase) that leads to AKI
bull This ldquoAKSrdquo may or may not lead to damage and functional declinebull But it is the earliest possible the process of AKI can be detected
Pre-injury phase biomarkers
Stress biomarkersbull In 2013 Kashani et al reported the results of a prospective international
observational investigation (the Sapphire study) of tissue inhibitor of metalloproteinases- 2 (TIMP-2) and insulin-like growth factor-binding protein 7 (IGFBP7) in a heterogeneous group of critically ill patients [TIMP-2][IGFBP7] was significantly superior to all previously described markers of AKI (plt0002)
bull Next the Opal and Topaz study showed the cut-off value and risk assessment using the urinary[TIMP-2] [IGFBP7]
bull The urine [IGFBP7][TIMP2] biomarker is already FDA approved and commercially available in the United States
bull Falsepositive results are common and they will be magnified if the test is used inappropriately in low-risk patients In addition this biomarker should not be used in ambulatory practices and it is not beneficial in patients with established AKI
microRNAsbull microRNAs (miRNAs) are endogenous single-stranded non-coding
mRNAs of about 19-23 nucleotides bull In the past years researchers have begun to investigate the
relevance of miRNAs to AKI with many miRNAs being implicated bull Some of them contribute to pathogenesis by regulating apoptosis
and inflammation amplifying or reducing acute injury responses while others regulate fibrosis and angiogenesis participating in renal recovery or progression to fibrosis
bull Certain miRNAs have been investigated for their potential as novel biomarkers for the early detection or prognostication of AKI
Hemojuvelinbull Hemojuvelin (HJV) a glycophosphatidylinositol (GPI)- linked
membrane protein is highly expressed in liver and skeletal musclesbull The molecular weight of HJV is 42 kDa for the soluble form (sHJV)
and can be passed through glomerular filtration and reabsorbed by the renal tubules Increased iron content in the kidney and urine is observed in human and animal models of AKI and increased iron load can induce renal tubular cell injury
bull There is evidence that the increased expression of the hemojuvelin-hepcidin ferroportin pathway is an intrinsic response to iron overload conditions during AKI
bull Therefore urine HJV (uHJV) has the potential to be an early AKI biomarker in response to iron homeostasis during AKI
Combination of functional and damage biomarkers
bull While new biomarkers are being validated functional biomarkers (serum creatinine serum urea and urine output) continue to be utilized in the diagnosis and staging of AKI In the future existing or newer damage biomarkers will likely be combined with the use of functional biomarkers to enhance the ability of RIFLE AKIN
bull A study of 345 children after cardiopulmonary bypass surgery demonstrated that the composite of functional biomarker such as plasma cystatin C and urinary NGAL was superior to changes in serum creatinine to predict AKI
PROGNOSTIC BIOMARKERS
bull Most of the biomarkers described above allow early detection of acute kidney injury but do not predict severe AKI
Urinary renin and angiotensinogen
bull Urinary renin angiotensinogen and plasma NGAL may predict the development of severe AKI
bull Among 99 consecutively enrolled patients who developed AKI the ratio of urinary angiotensinogen to urinary creatinine (uAnCR expressed as ng per mg creatinine)calculated Patients with the highest uAnCR had a higher risk of worsening AKI compared with patients with the lowest uAnCR An elevated uAnCR predicted a longer hospital stay
bull Among 204 patients who developed Acute Kidney Injury Network (AKIN) stage 1 following cardiac surgery the urinary renin-to-creatinine ratio and the angiotensinogen-to-creatinine ratio predicted a composite outcome of death or AKIN stage 3 or death
Plasma NGAL
bull In a prospective cohort study in which 616 patients admitted from the emergency department were classified by clinical criteria as AKI transient azotemia stable CKD or normal kidney function plasma NGAL discriminated AKI from normal function and from transient azotemia
bull Higher concentrations of NGAL were associated with more severe AKI
Thanks for your attention

Urinary tubular enzymes
bull Urinary tubular enzymes consist of proximal renal tubular epithelial antigen (HRTE-1) alpha-glutathione S-transferase (alpha-GST) glutamyltranspeptidase(gamma-GT) alanine aminopeptidase (AAP) lactate dehydrogenase (LDH) N-acetyl-beta-glucosaminidase(NAG) and alkaline phosphatase (ALP)
bull Most of these are released from proximal tubular epithelial cells within 12 hours and four days earlier than a detectable rise in serum creatinine
bull No validated cut-off points currently exist to help distinguish prerenal disease from ATN
Urinary low-molecular-weight proteins
bull Alpha1-microglobulin (alpha1-m) beta2-microglobulin (beta2-m) retinol-binding protein (RBP) adenosine deaminase-binding protein (ABP) and urinary cystatin C are urinary lowmolecular- weight proteins
bull They are produced at different sites filtered at the glomerulus and reabsorbed at the proximal tubule with no secretion
bull Although promising prognostically and to help distinguish prerenal disease from ATN increased levels may be observed after reversible and mild dysfunction and may not necessarily be associated with persistent or irreversible damage
Functional biomarkersSerum creatinine
bull Currently the standard diagnostic tools for AKI detection are SCrconcentration and UO both of which are markers of renal function but not kidney injury
bull SCr is an integrator of various intra- and extra-renal functions and its concentration indicates the balance between creatinine generation and excretion
bull Unfortunately due to the non-linear relationship between GFR and sCr the increase of creatinine may be within the reference range in early phase of AKI and may overlooked
bull SCr does not indicate the severity of the injury until a steady state has been reached in AKI Therefore SCr is a delayed and insensitive biomarker of changes in kidney function moreover its concentration does not differentiate between structural kidney damage and functional hemodynamic triggers and it could be affected by many factors
bull Especially in intensive care unit patients creatinine-based definitions of AKI can be influenced by baseline creatinine estimation fluid overload malnourishment and muscle wasting
Cystatin-C
bull Cystatin-C is produced at a constant rate by nucleated cells filtered by the glomerular cells almost completely reabsorbed and catabolized (but not secreted) in the proximal tubule It is a polypeptide chain with 120 amino acid residues
bull In this way some of the limitations of serum creatinine effect of muscle mass diet gender and tubular secretion may not be a problem with cystatin C and appear to rise one to two days earlier than serum creatinine
bull Cystatin C is better marker of GFR than serum creatinine as demonstrated in several studies
bull Over the past decade Cystatin C (CyC) a serum measure of renal function is a stronger predictor of the risk of death and cardiovascular events in elderly persons than is creatinine
bull Koyner et al demonstrated that urinary CyC was superior to SCr and plasma CyC in the early diagnosis of acute kidney injury following adult cardiac surgery
bull Roos et al performed a systematic review comparing the diagnostic accuracy of plasma and urine CyC with SCr in patients undergoing cardiac surgery They concluded that the diagnostic accuracy for impaired renal function favors urine CyC
bull However while Cys-C levels are a more precise indicator of kidney function than SCr concentration they seem to be influenced by old age large doses of corticosteroids hyperthyroidism inflammation neoplasia smoking and alcohol consumption
bull Currently it is unclear whether the value of Cys-C is generalizable to all forms of AKI or specific to particular populations
Damage biomarkers
Neutrophil Gelatinase-Associated Lipocalin(NGAL)
bull Human NGAL is a 25 kDa protein firstly identified bound to gelatinase in specific granules of the neutrophil NGAL is a critical component of innate immunity to bacterial infection and is expressed by immune cells hepatocytes and renal tubular cells in various disease states
bull Its resistance to proteolysis further enhanced potential suitability as a clinical biomarker
bull In healthy kidneys it is barel detectable in either plasma or urine
bull However in the setting of acute tubular injury NGAL undergoes rapid and profound upregulation with large increases in both urine and plasma
bull Distinct from traditional markers of function such as creatinine this rapid response enables NGAL to potentially identify injured kidney much earlier than was previously possible The endogenous role of NGAL remains unclear It seems to be involved with iron transportation to and from the proximal tubular epithelial cells and animal studies demonstrate a renoprotective effect of exogenously administered NGAL in the setting of acute ischemic injury
bull NGAL was also detected in the urine of mice in the early stage of cisplatin-induced nephrotoxicity
bull These animal studies demonstrated that NGAL may represent an early sensitive and noninvasive urinary biomarker for ischemic and nephrotoxic kidney injury
bull NGAL is markedly upregulated and abundantly expressed in the kidney after renal ischemia
bull In this setting NGAL may function to dampen toxicity by reducing apoptosis and increasing the normal proliferation of kidney tubule cells
bull following ischemia reperfusion as evidenced by a rise in creatinine the kidneys illuminate indicating NGAL production at the site of injury
bull Interestingly following maneuvers that lead to significant prerenal disease there was no NGAL illumination indicating that prerenal disease does not induce NGAL expression
bull Thus NGAL may potentially be useful in differentiating prerenal disease from ATN
bull In these studies the average sensitivity and specificity of NGAL measured one to three days prior to AKI diagnosis was 76 and 77 percent respectively for cardiac surgery patients and 73 and 80 percent respectively for patients admitted to the intensive care unit (ICU)
bull NGAL may also represent early sensitive biomarker of AKI after contrast administrations for coronary angiography
bull NGAL was measured in the serum and urine before and at 2 4 12 24 and 48 h after contrast administration they found a significant rise in serum NGAL 2 and 4 h after PCI and a rise in urinary NGAL 4 and 12 h after PCI
bull A similar study of 25 patients with normal serum creatinine undergoing PCI due to unstable angina There was a significant rise in serum NGAL after 2 and 4 hours Urinary NGAL and urinary L-FABP followed the same pattern Both markers increased significantly after 4 hours and remained elevated up to 48 hours after PCI
bull Urine and plasma NGAL levels also represent early biomarkers of AKI in ICU
bull A multicenter study of serum NGAL was performed in 143 critically ill children with systemic inflammatory response syndrome (SIRS) or septic shock during the first 24 h of admission to the ICU there was a significant difference in serum NGAL between healthy children ill children with SIRS and septic shock the study was concluded that serum NGAL is a highly sensitive but nonspecific predictor of acute kidney injury in critically ill children with septic shock
bull A 2010 study evaluated 88 ICU patient and found that an NGAL level of ge150 nmolL predicted AKI with 82 sensitivity and 97 specificity
bull A recent study had 98 patients who were divided in two groups depending on the presence of sepsis Fifty-six patients had sepsis while forty-two patients were nonseptic Among septic patients subjects who developed AKI showed signi1048853 cant higher levels of NGAL
bull A more study of 65 patients with septic shock were found that urine NGAL levels 12 hours before AKI diagnosis were a good predictor of AKI
Kidney Injury Molecule-1 (KIM-1)
bull KIM-1 mRNA and protein are expressed at a low level in normal kidney but are increased dramatically in postischemic kidney
bull KIM-1 has been identified as the first nonmyeloidphosphatidylserine receptor that confers a phagocytic phenotype on injured epithelial cells both in vivo and in vitro
bull Urinary KIM-1 has been found to be an early indicator of AKI that compares favorably to a number of conventional biomarkers and tubular enzymes
bull KIM-1 is also a tissue and urinary biomarker for nephrotoxicant-induced kidney injury
bull Tissue and urinary expressions were measured with different nephrotoxic doses of cisplatin folic acide cadmium gentamycin mercury
bull As early as 1 day after cisplatin treatment positive KIM- 1 immunostaining observed in the outer medulla of the kidney and changes in urinary clusterin indicated the onset of proximal tubular injury in the absence of functional effects
bull Tissue KIM-1 was the most sensitive biomarker for detection of cisplatin-induced kidney damage
bull KIM-1 is a biomarker of AKI in humans bull Urine samples were collected from 32 patients with various
acute and chronic kidney diseases as well as from eight normal controls there was extensive expression of KIM-1 in proximal tubule cells in kidney biopsies from six patients with biopsy confirmed acute tubular necrosis (ATN)
bull Urinary KIM-1 levels were significantly higher in patients with ischemic ATN compared to levels in patients with other forms of acute renal failure or chronic renal disease
bull Adjusted for age gender and length of time delay between the initial insult and sampling of the urine a one-unit increase in normalized KIM-1 was associated with a greater than 12-fold risk for the presence of ATN
bull In hospital patients with AKI urinary levels of KIM-1 that higher levels correlated with a higher odds ratio for dialysis requirement or hospital death
bull this study demonstrated that urinary biomarker of AKI such as KIM-1 can predict adverse clinical outcomes in patients with AKI
bull Both renal and urinary KIM-1 correlate with kidney damage and negatively with renal function but not with proteinuria
bull A recent study has explored urinary KIM-1correlated with kidney function in kidney allograft recipients Kidney transplant recipients showed significantly higher KIM-1 values than the healthy volunteers this study concluded that even a successful kidney transplantation is associated with kidney injury as reflected by elevated urinary KIM-1
bull A rapid direct 15-minute assay for the detection of urinary human KIM-1 has been developed Using this assay more urinary KIM-1 was detected in the urine of patients with AKI than in the urine from healthy volunteers
Urinary interleukin-18
bull Interleukin18 (IL-18) is a 22 kDa pro-inflammatory cytokine that increases in the kidney after ischemia-reperfusion injury in a caspase- 1-dependent manner
bull Patients with ATN had significantly greater urinary IL-18 concentrations than those with other conditions (healthy controls patients with pre-renal azotemia urinary tract infection CKD and nephrotic syndrome)
bull urinary IL-18 concentrations measured in the first 24 h after kidney transplantation were higher in patients who received a cadaveric kidney that developed delayed graft function compared to patients who received a cadaveric kidney with prompt graft function and patients who received a kidney with prompt graft function from a living donor
bull However the performance of urinary IL-18 measured 1 day before AKI was modest
bull Its predictive utility for AKI following cardiac surgery could not be demonstrated in one prospective observational study of 100 adult patients
bull In addition in a large study population of 1439 critically ill patients IL-18 had a poor-to-moderate ability to predict AKI renal replacement therapy (RRT) or 90-day mortality
Liver-Type Fatty Acid Binding Protein(L-FABP)
bull Liver-type fatty acid-binding protein (L-FABP) is a 14 kDa protein from the large super- family of lipidbinding proteins
bull The 14-kD L-FABP protein can be localized predominantly in the proximal tubule
bull Noiri et al demonstrated that increase of urinary L-FABP was observed at 1 h after ischemia even in the 5-min IRI group and urinary L-FABP was superior to BUN and urinary NAG for early and accurate detection of acute tubular necrosis in different models of animal AKI
bull urinary L-FABP may be a promising biomarker for early detection of AKI and prediction of dialysis requirement and in-hospital mortality
bull Urinary excretion of urinary liver-type fatty acid-binding protein (L-FABP) reflects stress of proximal tubular epithelial cells and correlates with severity of ischemic tubular injury
bull A meta-analysis of 15 prospective cohort studies demonstrated that in hospitalndashbased cohorts of patients at risk of AKI L-FABP can discriminate for the diagnosis of AKI and predict the need for dialysis and in-hospital mortality
bull It was correlated with the degree of tubulointerstitial damage in a folic acid induced nephropathy
bull In ischemic and cisplatin-induced AKI L-FABP was increased in the urine before the increase in BUN
bull In cisplatin-induced AKI urinary L-FABP levels increased exponentially even in the lowest dose group as early as 2 hours whereas BUN levels increased at 48 hours
bull L-FABP was measured in 80 critically ill patients Urinary L-FABP levels in patients with septic shock were significantly higher than severe sepsis without shock Serum L-FABP levels did not have significant differences between patients with septic shock severe sepsis and healthy
bull Another study was evaluated 145 septic shock patients complicated with established AKI Urinary L-FABP measured at admission was significantly higher in the nonsurvivors of septic shock with established acute kidney injury than in the survivors
Failure of the TRIBE-AKI study
bull The Translational Research Investigating Biomarker Endpoints in AKI (TRIBE-AKI) study evaluated the performance of urinary c-glutamyltranspeptidase ( c-GTP) alkaline phosphatase NGAL Cys-C KIM-1 and IL-18 in AKI diagnosis
bull The results of four novel urine biomarkers and one plasma biomarker (urine NGAL IL-18 KIM-1 and L-FABP and plasma NGAL) were provided Of all the novel biomarkers only urine IL-18 and plasma NGAL in adults were helpful in predicting progression of AKI when measured on the day of clinical AKI diagnosis
bull Combinations of three biomarkers in adults from two different time points and combinations of two biomarkers in children from two time points were found to be able to increase the ROC for AKI up to 078
bull In summary the clinical use of single damage biomarkers in AKI prediction remains unclear because large prospective multicenter trials such as the TRIBE-AKI study (nfrac141530) have failed to demonstrate troponin-like diagnostic performance
Various clinical scenarios of AKI based onfunction damage and stress
bull Over the last decade a number of novel damage biomarkers have been evaluated for their capacity to detect kidney damage and predict the development of AKI However the relationship between decreasing function and increasing damage is not as straightforward as might be assumed
bull The characteristic pattern whereby damage precedes loss of function (panel A) may be seen in some cases of AKI and affords an opportunity to detect ldquosubclinicalrdquo AKI before function start to fall Unfortunately other patterns might also occur For example functional decline may start to occur alongside damage (panel B) and in some cases function may start to decline even before damage (panel C)
bull This makes damage markers difficult to use for predicting AKI However other markers might actually measure the ldquostressrdquo occurring at the cellular level before damage or loss of function
Paradigm shift to pre-injury phase biomarkers
bull Katz et al proposed that the pre-injury phase that leads to AKI can be described as ldquoacute kidney stressrdquo (AKS) after the report of the identification of cell cycle arrest biomarkers that signal the potential development of AKI is part of an evolution in the molecular diagnosis and understanding of AKI
bull These biomarkers are released by kidney cells along a path which may lead to AKI during a pre-injury phase
bull AKS is defined as the increased-risk phase (pre-injury phase) that leads to AKI
bull This ldquoAKSrdquo may or may not lead to damage and functional declinebull But it is the earliest possible the process of AKI can be detected
Pre-injury phase biomarkers
Stress biomarkersbull In 2013 Kashani et al reported the results of a prospective international
observational investigation (the Sapphire study) of tissue inhibitor of metalloproteinases- 2 (TIMP-2) and insulin-like growth factor-binding protein 7 (IGFBP7) in a heterogeneous group of critically ill patients [TIMP-2][IGFBP7] was significantly superior to all previously described markers of AKI (plt0002)
bull Next the Opal and Topaz study showed the cut-off value and risk assessment using the urinary[TIMP-2] [IGFBP7]
bull The urine [IGFBP7][TIMP2] biomarker is already FDA approved and commercially available in the United States
bull Falsepositive results are common and they will be magnified if the test is used inappropriately in low-risk patients In addition this biomarker should not be used in ambulatory practices and it is not beneficial in patients with established AKI
microRNAsbull microRNAs (miRNAs) are endogenous single-stranded non-coding
mRNAs of about 19-23 nucleotides bull In the past years researchers have begun to investigate the
relevance of miRNAs to AKI with many miRNAs being implicated bull Some of them contribute to pathogenesis by regulating apoptosis
and inflammation amplifying or reducing acute injury responses while others regulate fibrosis and angiogenesis participating in renal recovery or progression to fibrosis
bull Certain miRNAs have been investigated for their potential as novel biomarkers for the early detection or prognostication of AKI
Hemojuvelinbull Hemojuvelin (HJV) a glycophosphatidylinositol (GPI)- linked
membrane protein is highly expressed in liver and skeletal musclesbull The molecular weight of HJV is 42 kDa for the soluble form (sHJV)
and can be passed through glomerular filtration and reabsorbed by the renal tubules Increased iron content in the kidney and urine is observed in human and animal models of AKI and increased iron load can induce renal tubular cell injury
bull There is evidence that the increased expression of the hemojuvelin-hepcidin ferroportin pathway is an intrinsic response to iron overload conditions during AKI
bull Therefore urine HJV (uHJV) has the potential to be an early AKI biomarker in response to iron homeostasis during AKI
Combination of functional and damage biomarkers
bull While new biomarkers are being validated functional biomarkers (serum creatinine serum urea and urine output) continue to be utilized in the diagnosis and staging of AKI In the future existing or newer damage biomarkers will likely be combined with the use of functional biomarkers to enhance the ability of RIFLE AKIN
bull A study of 345 children after cardiopulmonary bypass surgery demonstrated that the composite of functional biomarker such as plasma cystatin C and urinary NGAL was superior to changes in serum creatinine to predict AKI
PROGNOSTIC BIOMARKERS
bull Most of the biomarkers described above allow early detection of acute kidney injury but do not predict severe AKI
Urinary renin and angiotensinogen
bull Urinary renin angiotensinogen and plasma NGAL may predict the development of severe AKI
bull Among 99 consecutively enrolled patients who developed AKI the ratio of urinary angiotensinogen to urinary creatinine (uAnCR expressed as ng per mg creatinine)calculated Patients with the highest uAnCR had a higher risk of worsening AKI compared with patients with the lowest uAnCR An elevated uAnCR predicted a longer hospital stay
bull Among 204 patients who developed Acute Kidney Injury Network (AKIN) stage 1 following cardiac surgery the urinary renin-to-creatinine ratio and the angiotensinogen-to-creatinine ratio predicted a composite outcome of death or AKIN stage 3 or death
Plasma NGAL
bull In a prospective cohort study in which 616 patients admitted from the emergency department were classified by clinical criteria as AKI transient azotemia stable CKD or normal kidney function plasma NGAL discriminated AKI from normal function and from transient azotemia
bull Higher concentrations of NGAL were associated with more severe AKI
Thanks for your attention

Urinary low-molecular-weight proteins
bull Alpha1-microglobulin (alpha1-m) beta2-microglobulin (beta2-m) retinol-binding protein (RBP) adenosine deaminase-binding protein (ABP) and urinary cystatin C are urinary lowmolecular- weight proteins
bull They are produced at different sites filtered at the glomerulus and reabsorbed at the proximal tubule with no secretion
bull Although promising prognostically and to help distinguish prerenal disease from ATN increased levels may be observed after reversible and mild dysfunction and may not necessarily be associated with persistent or irreversible damage
Functional biomarkersSerum creatinine
bull Currently the standard diagnostic tools for AKI detection are SCrconcentration and UO both of which are markers of renal function but not kidney injury
bull SCr is an integrator of various intra- and extra-renal functions and its concentration indicates the balance between creatinine generation and excretion
bull Unfortunately due to the non-linear relationship between GFR and sCr the increase of creatinine may be within the reference range in early phase of AKI and may overlooked
bull SCr does not indicate the severity of the injury until a steady state has been reached in AKI Therefore SCr is a delayed and insensitive biomarker of changes in kidney function moreover its concentration does not differentiate between structural kidney damage and functional hemodynamic triggers and it could be affected by many factors
bull Especially in intensive care unit patients creatinine-based definitions of AKI can be influenced by baseline creatinine estimation fluid overload malnourishment and muscle wasting
Cystatin-C
bull Cystatin-C is produced at a constant rate by nucleated cells filtered by the glomerular cells almost completely reabsorbed and catabolized (but not secreted) in the proximal tubule It is a polypeptide chain with 120 amino acid residues
bull In this way some of the limitations of serum creatinine effect of muscle mass diet gender and tubular secretion may not be a problem with cystatin C and appear to rise one to two days earlier than serum creatinine
bull Cystatin C is better marker of GFR than serum creatinine as demonstrated in several studies
bull Over the past decade Cystatin C (CyC) a serum measure of renal function is a stronger predictor of the risk of death and cardiovascular events in elderly persons than is creatinine
bull Koyner et al demonstrated that urinary CyC was superior to SCr and plasma CyC in the early diagnosis of acute kidney injury following adult cardiac surgery
bull Roos et al performed a systematic review comparing the diagnostic accuracy of plasma and urine CyC with SCr in patients undergoing cardiac surgery They concluded that the diagnostic accuracy for impaired renal function favors urine CyC
bull However while Cys-C levels are a more precise indicator of kidney function than SCr concentration they seem to be influenced by old age large doses of corticosteroids hyperthyroidism inflammation neoplasia smoking and alcohol consumption
bull Currently it is unclear whether the value of Cys-C is generalizable to all forms of AKI or specific to particular populations
Damage biomarkers
Neutrophil Gelatinase-Associated Lipocalin(NGAL)
bull Human NGAL is a 25 kDa protein firstly identified bound to gelatinase in specific granules of the neutrophil NGAL is a critical component of innate immunity to bacterial infection and is expressed by immune cells hepatocytes and renal tubular cells in various disease states
bull Its resistance to proteolysis further enhanced potential suitability as a clinical biomarker
bull In healthy kidneys it is barel detectable in either plasma or urine
bull However in the setting of acute tubular injury NGAL undergoes rapid and profound upregulation with large increases in both urine and plasma
bull Distinct from traditional markers of function such as creatinine this rapid response enables NGAL to potentially identify injured kidney much earlier than was previously possible The endogenous role of NGAL remains unclear It seems to be involved with iron transportation to and from the proximal tubular epithelial cells and animal studies demonstrate a renoprotective effect of exogenously administered NGAL in the setting of acute ischemic injury
bull NGAL was also detected in the urine of mice in the early stage of cisplatin-induced nephrotoxicity
bull These animal studies demonstrated that NGAL may represent an early sensitive and noninvasive urinary biomarker for ischemic and nephrotoxic kidney injury
bull NGAL is markedly upregulated and abundantly expressed in the kidney after renal ischemia
bull In this setting NGAL may function to dampen toxicity by reducing apoptosis and increasing the normal proliferation of kidney tubule cells
bull following ischemia reperfusion as evidenced by a rise in creatinine the kidneys illuminate indicating NGAL production at the site of injury
bull Interestingly following maneuvers that lead to significant prerenal disease there was no NGAL illumination indicating that prerenal disease does not induce NGAL expression
bull Thus NGAL may potentially be useful in differentiating prerenal disease from ATN
bull In these studies the average sensitivity and specificity of NGAL measured one to three days prior to AKI diagnosis was 76 and 77 percent respectively for cardiac surgery patients and 73 and 80 percent respectively for patients admitted to the intensive care unit (ICU)
bull NGAL may also represent early sensitive biomarker of AKI after contrast administrations for coronary angiography
bull NGAL was measured in the serum and urine before and at 2 4 12 24 and 48 h after contrast administration they found a significant rise in serum NGAL 2 and 4 h after PCI and a rise in urinary NGAL 4 and 12 h after PCI
bull A similar study of 25 patients with normal serum creatinine undergoing PCI due to unstable angina There was a significant rise in serum NGAL after 2 and 4 hours Urinary NGAL and urinary L-FABP followed the same pattern Both markers increased significantly after 4 hours and remained elevated up to 48 hours after PCI
bull Urine and plasma NGAL levels also represent early biomarkers of AKI in ICU
bull A multicenter study of serum NGAL was performed in 143 critically ill children with systemic inflammatory response syndrome (SIRS) or septic shock during the first 24 h of admission to the ICU there was a significant difference in serum NGAL between healthy children ill children with SIRS and septic shock the study was concluded that serum NGAL is a highly sensitive but nonspecific predictor of acute kidney injury in critically ill children with septic shock
bull A 2010 study evaluated 88 ICU patient and found that an NGAL level of ge150 nmolL predicted AKI with 82 sensitivity and 97 specificity
bull A recent study had 98 patients who were divided in two groups depending on the presence of sepsis Fifty-six patients had sepsis while forty-two patients were nonseptic Among septic patients subjects who developed AKI showed signi1048853 cant higher levels of NGAL
bull A more study of 65 patients with septic shock were found that urine NGAL levels 12 hours before AKI diagnosis were a good predictor of AKI
Kidney Injury Molecule-1 (KIM-1)
bull KIM-1 mRNA and protein are expressed at a low level in normal kidney but are increased dramatically in postischemic kidney
bull KIM-1 has been identified as the first nonmyeloidphosphatidylserine receptor that confers a phagocytic phenotype on injured epithelial cells both in vivo and in vitro
bull Urinary KIM-1 has been found to be an early indicator of AKI that compares favorably to a number of conventional biomarkers and tubular enzymes
bull KIM-1 is also a tissue and urinary biomarker for nephrotoxicant-induced kidney injury
bull Tissue and urinary expressions were measured with different nephrotoxic doses of cisplatin folic acide cadmium gentamycin mercury
bull As early as 1 day after cisplatin treatment positive KIM- 1 immunostaining observed in the outer medulla of the kidney and changes in urinary clusterin indicated the onset of proximal tubular injury in the absence of functional effects
bull Tissue KIM-1 was the most sensitive biomarker for detection of cisplatin-induced kidney damage
bull KIM-1 is a biomarker of AKI in humans bull Urine samples were collected from 32 patients with various
acute and chronic kidney diseases as well as from eight normal controls there was extensive expression of KIM-1 in proximal tubule cells in kidney biopsies from six patients with biopsy confirmed acute tubular necrosis (ATN)
bull Urinary KIM-1 levels were significantly higher in patients with ischemic ATN compared to levels in patients with other forms of acute renal failure or chronic renal disease
bull Adjusted for age gender and length of time delay between the initial insult and sampling of the urine a one-unit increase in normalized KIM-1 was associated with a greater than 12-fold risk for the presence of ATN
bull In hospital patients with AKI urinary levels of KIM-1 that higher levels correlated with a higher odds ratio for dialysis requirement or hospital death
bull this study demonstrated that urinary biomarker of AKI such as KIM-1 can predict adverse clinical outcomes in patients with AKI
bull Both renal and urinary KIM-1 correlate with kidney damage and negatively with renal function but not with proteinuria
bull A recent study has explored urinary KIM-1correlated with kidney function in kidney allograft recipients Kidney transplant recipients showed significantly higher KIM-1 values than the healthy volunteers this study concluded that even a successful kidney transplantation is associated with kidney injury as reflected by elevated urinary KIM-1
bull A rapid direct 15-minute assay for the detection of urinary human KIM-1 has been developed Using this assay more urinary KIM-1 was detected in the urine of patients with AKI than in the urine from healthy volunteers
Urinary interleukin-18
bull Interleukin18 (IL-18) is a 22 kDa pro-inflammatory cytokine that increases in the kidney after ischemia-reperfusion injury in a caspase- 1-dependent manner
bull Patients with ATN had significantly greater urinary IL-18 concentrations than those with other conditions (healthy controls patients with pre-renal azotemia urinary tract infection CKD and nephrotic syndrome)
bull urinary IL-18 concentrations measured in the first 24 h after kidney transplantation were higher in patients who received a cadaveric kidney that developed delayed graft function compared to patients who received a cadaveric kidney with prompt graft function and patients who received a kidney with prompt graft function from a living donor
bull However the performance of urinary IL-18 measured 1 day before AKI was modest
bull Its predictive utility for AKI following cardiac surgery could not be demonstrated in one prospective observational study of 100 adult patients
bull In addition in a large study population of 1439 critically ill patients IL-18 had a poor-to-moderate ability to predict AKI renal replacement therapy (RRT) or 90-day mortality
Liver-Type Fatty Acid Binding Protein(L-FABP)
bull Liver-type fatty acid-binding protein (L-FABP) is a 14 kDa protein from the large super- family of lipidbinding proteins
bull The 14-kD L-FABP protein can be localized predominantly in the proximal tubule
bull Noiri et al demonstrated that increase of urinary L-FABP was observed at 1 h after ischemia even in the 5-min IRI group and urinary L-FABP was superior to BUN and urinary NAG for early and accurate detection of acute tubular necrosis in different models of animal AKI
bull urinary L-FABP may be a promising biomarker for early detection of AKI and prediction of dialysis requirement and in-hospital mortality
bull Urinary excretion of urinary liver-type fatty acid-binding protein (L-FABP) reflects stress of proximal tubular epithelial cells and correlates with severity of ischemic tubular injury
bull A meta-analysis of 15 prospective cohort studies demonstrated that in hospitalndashbased cohorts of patients at risk of AKI L-FABP can discriminate for the diagnosis of AKI and predict the need for dialysis and in-hospital mortality
bull It was correlated with the degree of tubulointerstitial damage in a folic acid induced nephropathy
bull In ischemic and cisplatin-induced AKI L-FABP was increased in the urine before the increase in BUN
bull In cisplatin-induced AKI urinary L-FABP levels increased exponentially even in the lowest dose group as early as 2 hours whereas BUN levels increased at 48 hours
bull L-FABP was measured in 80 critically ill patients Urinary L-FABP levels in patients with septic shock were significantly higher than severe sepsis without shock Serum L-FABP levels did not have significant differences between patients with septic shock severe sepsis and healthy
bull Another study was evaluated 145 septic shock patients complicated with established AKI Urinary L-FABP measured at admission was significantly higher in the nonsurvivors of septic shock with established acute kidney injury than in the survivors
Failure of the TRIBE-AKI study
bull The Translational Research Investigating Biomarker Endpoints in AKI (TRIBE-AKI) study evaluated the performance of urinary c-glutamyltranspeptidase ( c-GTP) alkaline phosphatase NGAL Cys-C KIM-1 and IL-18 in AKI diagnosis
bull The results of four novel urine biomarkers and one plasma biomarker (urine NGAL IL-18 KIM-1 and L-FABP and plasma NGAL) were provided Of all the novel biomarkers only urine IL-18 and plasma NGAL in adults were helpful in predicting progression of AKI when measured on the day of clinical AKI diagnosis
bull Combinations of three biomarkers in adults from two different time points and combinations of two biomarkers in children from two time points were found to be able to increase the ROC for AKI up to 078
bull In summary the clinical use of single damage biomarkers in AKI prediction remains unclear because large prospective multicenter trials such as the TRIBE-AKI study (nfrac141530) have failed to demonstrate troponin-like diagnostic performance
Various clinical scenarios of AKI based onfunction damage and stress
bull Over the last decade a number of novel damage biomarkers have been evaluated for their capacity to detect kidney damage and predict the development of AKI However the relationship between decreasing function and increasing damage is not as straightforward as might be assumed
bull The characteristic pattern whereby damage precedes loss of function (panel A) may be seen in some cases of AKI and affords an opportunity to detect ldquosubclinicalrdquo AKI before function start to fall Unfortunately other patterns might also occur For example functional decline may start to occur alongside damage (panel B) and in some cases function may start to decline even before damage (panel C)
bull This makes damage markers difficult to use for predicting AKI However other markers might actually measure the ldquostressrdquo occurring at the cellular level before damage or loss of function
Paradigm shift to pre-injury phase biomarkers
bull Katz et al proposed that the pre-injury phase that leads to AKI can be described as ldquoacute kidney stressrdquo (AKS) after the report of the identification of cell cycle arrest biomarkers that signal the potential development of AKI is part of an evolution in the molecular diagnosis and understanding of AKI
bull These biomarkers are released by kidney cells along a path which may lead to AKI during a pre-injury phase
bull AKS is defined as the increased-risk phase (pre-injury phase) that leads to AKI
bull This ldquoAKSrdquo may or may not lead to damage and functional declinebull But it is the earliest possible the process of AKI can be detected
Pre-injury phase biomarkers
Stress biomarkersbull In 2013 Kashani et al reported the results of a prospective international
observational investigation (the Sapphire study) of tissue inhibitor of metalloproteinases- 2 (TIMP-2) and insulin-like growth factor-binding protein 7 (IGFBP7) in a heterogeneous group of critically ill patients [TIMP-2][IGFBP7] was significantly superior to all previously described markers of AKI (plt0002)
bull Next the Opal and Topaz study showed the cut-off value and risk assessment using the urinary[TIMP-2] [IGFBP7]
bull The urine [IGFBP7][TIMP2] biomarker is already FDA approved and commercially available in the United States
bull Falsepositive results are common and they will be magnified if the test is used inappropriately in low-risk patients In addition this biomarker should not be used in ambulatory practices and it is not beneficial in patients with established AKI
microRNAsbull microRNAs (miRNAs) are endogenous single-stranded non-coding
mRNAs of about 19-23 nucleotides bull In the past years researchers have begun to investigate the
relevance of miRNAs to AKI with many miRNAs being implicated bull Some of them contribute to pathogenesis by regulating apoptosis
and inflammation amplifying or reducing acute injury responses while others regulate fibrosis and angiogenesis participating in renal recovery or progression to fibrosis
bull Certain miRNAs have been investigated for their potential as novel biomarkers for the early detection or prognostication of AKI
Hemojuvelinbull Hemojuvelin (HJV) a glycophosphatidylinositol (GPI)- linked
membrane protein is highly expressed in liver and skeletal musclesbull The molecular weight of HJV is 42 kDa for the soluble form (sHJV)
and can be passed through glomerular filtration and reabsorbed by the renal tubules Increased iron content in the kidney and urine is observed in human and animal models of AKI and increased iron load can induce renal tubular cell injury
bull There is evidence that the increased expression of the hemojuvelin-hepcidin ferroportin pathway is an intrinsic response to iron overload conditions during AKI
bull Therefore urine HJV (uHJV) has the potential to be an early AKI biomarker in response to iron homeostasis during AKI
Combination of functional and damage biomarkers
bull While new biomarkers are being validated functional biomarkers (serum creatinine serum urea and urine output) continue to be utilized in the diagnosis and staging of AKI In the future existing or newer damage biomarkers will likely be combined with the use of functional biomarkers to enhance the ability of RIFLE AKIN
bull A study of 345 children after cardiopulmonary bypass surgery demonstrated that the composite of functional biomarker such as plasma cystatin C and urinary NGAL was superior to changes in serum creatinine to predict AKI
PROGNOSTIC BIOMARKERS
bull Most of the biomarkers described above allow early detection of acute kidney injury but do not predict severe AKI
Urinary renin and angiotensinogen
bull Urinary renin angiotensinogen and plasma NGAL may predict the development of severe AKI
bull Among 99 consecutively enrolled patients who developed AKI the ratio of urinary angiotensinogen to urinary creatinine (uAnCR expressed as ng per mg creatinine)calculated Patients with the highest uAnCR had a higher risk of worsening AKI compared with patients with the lowest uAnCR An elevated uAnCR predicted a longer hospital stay
bull Among 204 patients who developed Acute Kidney Injury Network (AKIN) stage 1 following cardiac surgery the urinary renin-to-creatinine ratio and the angiotensinogen-to-creatinine ratio predicted a composite outcome of death or AKIN stage 3 or death
Plasma NGAL
bull In a prospective cohort study in which 616 patients admitted from the emergency department were classified by clinical criteria as AKI transient azotemia stable CKD or normal kidney function plasma NGAL discriminated AKI from normal function and from transient azotemia
bull Higher concentrations of NGAL were associated with more severe AKI
Thanks for your attention

Functional biomarkersSerum creatinine
bull Currently the standard diagnostic tools for AKI detection are SCrconcentration and UO both of which are markers of renal function but not kidney injury
bull SCr is an integrator of various intra- and extra-renal functions and its concentration indicates the balance between creatinine generation and excretion
bull Unfortunately due to the non-linear relationship between GFR and sCr the increase of creatinine may be within the reference range in early phase of AKI and may overlooked
bull SCr does not indicate the severity of the injury until a steady state has been reached in AKI Therefore SCr is a delayed and insensitive biomarker of changes in kidney function moreover its concentration does not differentiate between structural kidney damage and functional hemodynamic triggers and it could be affected by many factors
bull Especially in intensive care unit patients creatinine-based definitions of AKI can be influenced by baseline creatinine estimation fluid overload malnourishment and muscle wasting
Cystatin-C
bull Cystatin-C is produced at a constant rate by nucleated cells filtered by the glomerular cells almost completely reabsorbed and catabolized (but not secreted) in the proximal tubule It is a polypeptide chain with 120 amino acid residues
bull In this way some of the limitations of serum creatinine effect of muscle mass diet gender and tubular secretion may not be a problem with cystatin C and appear to rise one to two days earlier than serum creatinine
bull Cystatin C is better marker of GFR than serum creatinine as demonstrated in several studies
bull Over the past decade Cystatin C (CyC) a serum measure of renal function is a stronger predictor of the risk of death and cardiovascular events in elderly persons than is creatinine
bull Koyner et al demonstrated that urinary CyC was superior to SCr and plasma CyC in the early diagnosis of acute kidney injury following adult cardiac surgery
bull Roos et al performed a systematic review comparing the diagnostic accuracy of plasma and urine CyC with SCr in patients undergoing cardiac surgery They concluded that the diagnostic accuracy for impaired renal function favors urine CyC
bull However while Cys-C levels are a more precise indicator of kidney function than SCr concentration they seem to be influenced by old age large doses of corticosteroids hyperthyroidism inflammation neoplasia smoking and alcohol consumption
bull Currently it is unclear whether the value of Cys-C is generalizable to all forms of AKI or specific to particular populations
Damage biomarkers
Neutrophil Gelatinase-Associated Lipocalin(NGAL)
bull Human NGAL is a 25 kDa protein firstly identified bound to gelatinase in specific granules of the neutrophil NGAL is a critical component of innate immunity to bacterial infection and is expressed by immune cells hepatocytes and renal tubular cells in various disease states
bull Its resistance to proteolysis further enhanced potential suitability as a clinical biomarker
bull In healthy kidneys it is barel detectable in either plasma or urine
bull However in the setting of acute tubular injury NGAL undergoes rapid and profound upregulation with large increases in both urine and plasma
bull Distinct from traditional markers of function such as creatinine this rapid response enables NGAL to potentially identify injured kidney much earlier than was previously possible The endogenous role of NGAL remains unclear It seems to be involved with iron transportation to and from the proximal tubular epithelial cells and animal studies demonstrate a renoprotective effect of exogenously administered NGAL in the setting of acute ischemic injury
bull NGAL was also detected in the urine of mice in the early stage of cisplatin-induced nephrotoxicity
bull These animal studies demonstrated that NGAL may represent an early sensitive and noninvasive urinary biomarker for ischemic and nephrotoxic kidney injury
bull NGAL is markedly upregulated and abundantly expressed in the kidney after renal ischemia
bull In this setting NGAL may function to dampen toxicity by reducing apoptosis and increasing the normal proliferation of kidney tubule cells
bull following ischemia reperfusion as evidenced by a rise in creatinine the kidneys illuminate indicating NGAL production at the site of injury
bull Interestingly following maneuvers that lead to significant prerenal disease there was no NGAL illumination indicating that prerenal disease does not induce NGAL expression
bull Thus NGAL may potentially be useful in differentiating prerenal disease from ATN
bull In these studies the average sensitivity and specificity of NGAL measured one to three days prior to AKI diagnosis was 76 and 77 percent respectively for cardiac surgery patients and 73 and 80 percent respectively for patients admitted to the intensive care unit (ICU)
bull NGAL may also represent early sensitive biomarker of AKI after contrast administrations for coronary angiography
bull NGAL was measured in the serum and urine before and at 2 4 12 24 and 48 h after contrast administration they found a significant rise in serum NGAL 2 and 4 h after PCI and a rise in urinary NGAL 4 and 12 h after PCI
bull A similar study of 25 patients with normal serum creatinine undergoing PCI due to unstable angina There was a significant rise in serum NGAL after 2 and 4 hours Urinary NGAL and urinary L-FABP followed the same pattern Both markers increased significantly after 4 hours and remained elevated up to 48 hours after PCI
bull Urine and plasma NGAL levels also represent early biomarkers of AKI in ICU
bull A multicenter study of serum NGAL was performed in 143 critically ill children with systemic inflammatory response syndrome (SIRS) or septic shock during the first 24 h of admission to the ICU there was a significant difference in serum NGAL between healthy children ill children with SIRS and septic shock the study was concluded that serum NGAL is a highly sensitive but nonspecific predictor of acute kidney injury in critically ill children with septic shock
bull A 2010 study evaluated 88 ICU patient and found that an NGAL level of ge150 nmolL predicted AKI with 82 sensitivity and 97 specificity
bull A recent study had 98 patients who were divided in two groups depending on the presence of sepsis Fifty-six patients had sepsis while forty-two patients were nonseptic Among septic patients subjects who developed AKI showed signi1048853 cant higher levels of NGAL
bull A more study of 65 patients with septic shock were found that urine NGAL levels 12 hours before AKI diagnosis were a good predictor of AKI
Kidney Injury Molecule-1 (KIM-1)
bull KIM-1 mRNA and protein are expressed at a low level in normal kidney but are increased dramatically in postischemic kidney
bull KIM-1 has been identified as the first nonmyeloidphosphatidylserine receptor that confers a phagocytic phenotype on injured epithelial cells both in vivo and in vitro
bull Urinary KIM-1 has been found to be an early indicator of AKI that compares favorably to a number of conventional biomarkers and tubular enzymes
bull KIM-1 is also a tissue and urinary biomarker for nephrotoxicant-induced kidney injury
bull Tissue and urinary expressions were measured with different nephrotoxic doses of cisplatin folic acide cadmium gentamycin mercury
bull As early as 1 day after cisplatin treatment positive KIM- 1 immunostaining observed in the outer medulla of the kidney and changes in urinary clusterin indicated the onset of proximal tubular injury in the absence of functional effects
bull Tissue KIM-1 was the most sensitive biomarker for detection of cisplatin-induced kidney damage
bull KIM-1 is a biomarker of AKI in humans bull Urine samples were collected from 32 patients with various
acute and chronic kidney diseases as well as from eight normal controls there was extensive expression of KIM-1 in proximal tubule cells in kidney biopsies from six patients with biopsy confirmed acute tubular necrosis (ATN)
bull Urinary KIM-1 levels were significantly higher in patients with ischemic ATN compared to levels in patients with other forms of acute renal failure or chronic renal disease
bull Adjusted for age gender and length of time delay between the initial insult and sampling of the urine a one-unit increase in normalized KIM-1 was associated with a greater than 12-fold risk for the presence of ATN
bull In hospital patients with AKI urinary levels of KIM-1 that higher levels correlated with a higher odds ratio for dialysis requirement or hospital death
bull this study demonstrated that urinary biomarker of AKI such as KIM-1 can predict adverse clinical outcomes in patients with AKI
bull Both renal and urinary KIM-1 correlate with kidney damage and negatively with renal function but not with proteinuria
bull A recent study has explored urinary KIM-1correlated with kidney function in kidney allograft recipients Kidney transplant recipients showed significantly higher KIM-1 values than the healthy volunteers this study concluded that even a successful kidney transplantation is associated with kidney injury as reflected by elevated urinary KIM-1
bull A rapid direct 15-minute assay for the detection of urinary human KIM-1 has been developed Using this assay more urinary KIM-1 was detected in the urine of patients with AKI than in the urine from healthy volunteers
Urinary interleukin-18
bull Interleukin18 (IL-18) is a 22 kDa pro-inflammatory cytokine that increases in the kidney after ischemia-reperfusion injury in a caspase- 1-dependent manner
bull Patients with ATN had significantly greater urinary IL-18 concentrations than those with other conditions (healthy controls patients with pre-renal azotemia urinary tract infection CKD and nephrotic syndrome)
bull urinary IL-18 concentrations measured in the first 24 h after kidney transplantation were higher in patients who received a cadaveric kidney that developed delayed graft function compared to patients who received a cadaveric kidney with prompt graft function and patients who received a kidney with prompt graft function from a living donor
bull However the performance of urinary IL-18 measured 1 day before AKI was modest
bull Its predictive utility for AKI following cardiac surgery could not be demonstrated in one prospective observational study of 100 adult patients
bull In addition in a large study population of 1439 critically ill patients IL-18 had a poor-to-moderate ability to predict AKI renal replacement therapy (RRT) or 90-day mortality
Liver-Type Fatty Acid Binding Protein(L-FABP)
bull Liver-type fatty acid-binding protein (L-FABP) is a 14 kDa protein from the large super- family of lipidbinding proteins
bull The 14-kD L-FABP protein can be localized predominantly in the proximal tubule
bull Noiri et al demonstrated that increase of urinary L-FABP was observed at 1 h after ischemia even in the 5-min IRI group and urinary L-FABP was superior to BUN and urinary NAG for early and accurate detection of acute tubular necrosis in different models of animal AKI
bull urinary L-FABP may be a promising biomarker for early detection of AKI and prediction of dialysis requirement and in-hospital mortality
bull Urinary excretion of urinary liver-type fatty acid-binding protein (L-FABP) reflects stress of proximal tubular epithelial cells and correlates with severity of ischemic tubular injury
bull A meta-analysis of 15 prospective cohort studies demonstrated that in hospitalndashbased cohorts of patients at risk of AKI L-FABP can discriminate for the diagnosis of AKI and predict the need for dialysis and in-hospital mortality
bull It was correlated with the degree of tubulointerstitial damage in a folic acid induced nephropathy
bull In ischemic and cisplatin-induced AKI L-FABP was increased in the urine before the increase in BUN
bull In cisplatin-induced AKI urinary L-FABP levels increased exponentially even in the lowest dose group as early as 2 hours whereas BUN levels increased at 48 hours
bull L-FABP was measured in 80 critically ill patients Urinary L-FABP levels in patients with septic shock were significantly higher than severe sepsis without shock Serum L-FABP levels did not have significant differences between patients with septic shock severe sepsis and healthy
bull Another study was evaluated 145 septic shock patients complicated with established AKI Urinary L-FABP measured at admission was significantly higher in the nonsurvivors of septic shock with established acute kidney injury than in the survivors
Failure of the TRIBE-AKI study
bull The Translational Research Investigating Biomarker Endpoints in AKI (TRIBE-AKI) study evaluated the performance of urinary c-glutamyltranspeptidase ( c-GTP) alkaline phosphatase NGAL Cys-C KIM-1 and IL-18 in AKI diagnosis
bull The results of four novel urine biomarkers and one plasma biomarker (urine NGAL IL-18 KIM-1 and L-FABP and plasma NGAL) were provided Of all the novel biomarkers only urine IL-18 and plasma NGAL in adults were helpful in predicting progression of AKI when measured on the day of clinical AKI diagnosis
bull Combinations of three biomarkers in adults from two different time points and combinations of two biomarkers in children from two time points were found to be able to increase the ROC for AKI up to 078
bull In summary the clinical use of single damage biomarkers in AKI prediction remains unclear because large prospective multicenter trials such as the TRIBE-AKI study (nfrac141530) have failed to demonstrate troponin-like diagnostic performance
Various clinical scenarios of AKI based onfunction damage and stress
bull Over the last decade a number of novel damage biomarkers have been evaluated for their capacity to detect kidney damage and predict the development of AKI However the relationship between decreasing function and increasing damage is not as straightforward as might be assumed
bull The characteristic pattern whereby damage precedes loss of function (panel A) may be seen in some cases of AKI and affords an opportunity to detect ldquosubclinicalrdquo AKI before function start to fall Unfortunately other patterns might also occur For example functional decline may start to occur alongside damage (panel B) and in some cases function may start to decline even before damage (panel C)
bull This makes damage markers difficult to use for predicting AKI However other markers might actually measure the ldquostressrdquo occurring at the cellular level before damage or loss of function
Paradigm shift to pre-injury phase biomarkers
bull Katz et al proposed that the pre-injury phase that leads to AKI can be described as ldquoacute kidney stressrdquo (AKS) after the report of the identification of cell cycle arrest biomarkers that signal the potential development of AKI is part of an evolution in the molecular diagnosis and understanding of AKI
bull These biomarkers are released by kidney cells along a path which may lead to AKI during a pre-injury phase
bull AKS is defined as the increased-risk phase (pre-injury phase) that leads to AKI
bull This ldquoAKSrdquo may or may not lead to damage and functional declinebull But it is the earliest possible the process of AKI can be detected
Pre-injury phase biomarkers
Stress biomarkersbull In 2013 Kashani et al reported the results of a prospective international
observational investigation (the Sapphire study) of tissue inhibitor of metalloproteinases- 2 (TIMP-2) and insulin-like growth factor-binding protein 7 (IGFBP7) in a heterogeneous group of critically ill patients [TIMP-2][IGFBP7] was significantly superior to all previously described markers of AKI (plt0002)
bull Next the Opal and Topaz study showed the cut-off value and risk assessment using the urinary[TIMP-2] [IGFBP7]
bull The urine [IGFBP7][TIMP2] biomarker is already FDA approved and commercially available in the United States
bull Falsepositive results are common and they will be magnified if the test is used inappropriately in low-risk patients In addition this biomarker should not be used in ambulatory practices and it is not beneficial in patients with established AKI
microRNAsbull microRNAs (miRNAs) are endogenous single-stranded non-coding
mRNAs of about 19-23 nucleotides bull In the past years researchers have begun to investigate the
relevance of miRNAs to AKI with many miRNAs being implicated bull Some of them contribute to pathogenesis by regulating apoptosis
and inflammation amplifying or reducing acute injury responses while others regulate fibrosis and angiogenesis participating in renal recovery or progression to fibrosis
bull Certain miRNAs have been investigated for their potential as novel biomarkers for the early detection or prognostication of AKI
Hemojuvelinbull Hemojuvelin (HJV) a glycophosphatidylinositol (GPI)- linked
membrane protein is highly expressed in liver and skeletal musclesbull The molecular weight of HJV is 42 kDa for the soluble form (sHJV)
and can be passed through glomerular filtration and reabsorbed by the renal tubules Increased iron content in the kidney and urine is observed in human and animal models of AKI and increased iron load can induce renal tubular cell injury
bull There is evidence that the increased expression of the hemojuvelin-hepcidin ferroportin pathway is an intrinsic response to iron overload conditions during AKI
bull Therefore urine HJV (uHJV) has the potential to be an early AKI biomarker in response to iron homeostasis during AKI
Combination of functional and damage biomarkers
bull While new biomarkers are being validated functional biomarkers (serum creatinine serum urea and urine output) continue to be utilized in the diagnosis and staging of AKI In the future existing or newer damage biomarkers will likely be combined with the use of functional biomarkers to enhance the ability of RIFLE AKIN
bull A study of 345 children after cardiopulmonary bypass surgery demonstrated that the composite of functional biomarker such as plasma cystatin C and urinary NGAL was superior to changes in serum creatinine to predict AKI
PROGNOSTIC BIOMARKERS
bull Most of the biomarkers described above allow early detection of acute kidney injury but do not predict severe AKI
Urinary renin and angiotensinogen
bull Urinary renin angiotensinogen and plasma NGAL may predict the development of severe AKI
bull Among 99 consecutively enrolled patients who developed AKI the ratio of urinary angiotensinogen to urinary creatinine (uAnCR expressed as ng per mg creatinine)calculated Patients with the highest uAnCR had a higher risk of worsening AKI compared with patients with the lowest uAnCR An elevated uAnCR predicted a longer hospital stay
bull Among 204 patients who developed Acute Kidney Injury Network (AKIN) stage 1 following cardiac surgery the urinary renin-to-creatinine ratio and the angiotensinogen-to-creatinine ratio predicted a composite outcome of death or AKIN stage 3 or death
Plasma NGAL
bull In a prospective cohort study in which 616 patients admitted from the emergency department were classified by clinical criteria as AKI transient azotemia stable CKD or normal kidney function plasma NGAL discriminated AKI from normal function and from transient azotemia
bull Higher concentrations of NGAL were associated with more severe AKI
Thanks for your attention

Cystatin-C
bull Cystatin-C is produced at a constant rate by nucleated cells filtered by the glomerular cells almost completely reabsorbed and catabolized (but not secreted) in the proximal tubule It is a polypeptide chain with 120 amino acid residues
bull In this way some of the limitations of serum creatinine effect of muscle mass diet gender and tubular secretion may not be a problem with cystatin C and appear to rise one to two days earlier than serum creatinine
bull Cystatin C is better marker of GFR than serum creatinine as demonstrated in several studies
bull Over the past decade Cystatin C (CyC) a serum measure of renal function is a stronger predictor of the risk of death and cardiovascular events in elderly persons than is creatinine
bull Koyner et al demonstrated that urinary CyC was superior to SCr and plasma CyC in the early diagnosis of acute kidney injury following adult cardiac surgery
bull Roos et al performed a systematic review comparing the diagnostic accuracy of plasma and urine CyC with SCr in patients undergoing cardiac surgery They concluded that the diagnostic accuracy for impaired renal function favors urine CyC
bull However while Cys-C levels are a more precise indicator of kidney function than SCr concentration they seem to be influenced by old age large doses of corticosteroids hyperthyroidism inflammation neoplasia smoking and alcohol consumption
bull Currently it is unclear whether the value of Cys-C is generalizable to all forms of AKI or specific to particular populations
Damage biomarkers
Neutrophil Gelatinase-Associated Lipocalin(NGAL)
bull Human NGAL is a 25 kDa protein firstly identified bound to gelatinase in specific granules of the neutrophil NGAL is a critical component of innate immunity to bacterial infection and is expressed by immune cells hepatocytes and renal tubular cells in various disease states
bull Its resistance to proteolysis further enhanced potential suitability as a clinical biomarker
bull In healthy kidneys it is barel detectable in either plasma or urine
bull However in the setting of acute tubular injury NGAL undergoes rapid and profound upregulation with large increases in both urine and plasma
bull Distinct from traditional markers of function such as creatinine this rapid response enables NGAL to potentially identify injured kidney much earlier than was previously possible The endogenous role of NGAL remains unclear It seems to be involved with iron transportation to and from the proximal tubular epithelial cells and animal studies demonstrate a renoprotective effect of exogenously administered NGAL in the setting of acute ischemic injury
bull NGAL was also detected in the urine of mice in the early stage of cisplatin-induced nephrotoxicity
bull These animal studies demonstrated that NGAL may represent an early sensitive and noninvasive urinary biomarker for ischemic and nephrotoxic kidney injury
bull NGAL is markedly upregulated and abundantly expressed in the kidney after renal ischemia
bull In this setting NGAL may function to dampen toxicity by reducing apoptosis and increasing the normal proliferation of kidney tubule cells
bull following ischemia reperfusion as evidenced by a rise in creatinine the kidneys illuminate indicating NGAL production at the site of injury
bull Interestingly following maneuvers that lead to significant prerenal disease there was no NGAL illumination indicating that prerenal disease does not induce NGAL expression
bull Thus NGAL may potentially be useful in differentiating prerenal disease from ATN
bull In these studies the average sensitivity and specificity of NGAL measured one to three days prior to AKI diagnosis was 76 and 77 percent respectively for cardiac surgery patients and 73 and 80 percent respectively for patients admitted to the intensive care unit (ICU)
bull NGAL may also represent early sensitive biomarker of AKI after contrast administrations for coronary angiography
bull NGAL was measured in the serum and urine before and at 2 4 12 24 and 48 h after contrast administration they found a significant rise in serum NGAL 2 and 4 h after PCI and a rise in urinary NGAL 4 and 12 h after PCI
bull A similar study of 25 patients with normal serum creatinine undergoing PCI due to unstable angina There was a significant rise in serum NGAL after 2 and 4 hours Urinary NGAL and urinary L-FABP followed the same pattern Both markers increased significantly after 4 hours and remained elevated up to 48 hours after PCI
bull Urine and plasma NGAL levels also represent early biomarkers of AKI in ICU
bull A multicenter study of serum NGAL was performed in 143 critically ill children with systemic inflammatory response syndrome (SIRS) or septic shock during the first 24 h of admission to the ICU there was a significant difference in serum NGAL between healthy children ill children with SIRS and septic shock the study was concluded that serum NGAL is a highly sensitive but nonspecific predictor of acute kidney injury in critically ill children with septic shock
bull A 2010 study evaluated 88 ICU patient and found that an NGAL level of ge150 nmolL predicted AKI with 82 sensitivity and 97 specificity
bull A recent study had 98 patients who were divided in two groups depending on the presence of sepsis Fifty-six patients had sepsis while forty-two patients were nonseptic Among septic patients subjects who developed AKI showed signi1048853 cant higher levels of NGAL
bull A more study of 65 patients with septic shock were found that urine NGAL levels 12 hours before AKI diagnosis were a good predictor of AKI
Kidney Injury Molecule-1 (KIM-1)
bull KIM-1 mRNA and protein are expressed at a low level in normal kidney but are increased dramatically in postischemic kidney
bull KIM-1 has been identified as the first nonmyeloidphosphatidylserine receptor that confers a phagocytic phenotype on injured epithelial cells both in vivo and in vitro
bull Urinary KIM-1 has been found to be an early indicator of AKI that compares favorably to a number of conventional biomarkers and tubular enzymes
bull KIM-1 is also a tissue and urinary biomarker for nephrotoxicant-induced kidney injury
bull Tissue and urinary expressions were measured with different nephrotoxic doses of cisplatin folic acide cadmium gentamycin mercury
bull As early as 1 day after cisplatin treatment positive KIM- 1 immunostaining observed in the outer medulla of the kidney and changes in urinary clusterin indicated the onset of proximal tubular injury in the absence of functional effects
bull Tissue KIM-1 was the most sensitive biomarker for detection of cisplatin-induced kidney damage
bull KIM-1 is a biomarker of AKI in humans bull Urine samples were collected from 32 patients with various
acute and chronic kidney diseases as well as from eight normal controls there was extensive expression of KIM-1 in proximal tubule cells in kidney biopsies from six patients with biopsy confirmed acute tubular necrosis (ATN)
bull Urinary KIM-1 levels were significantly higher in patients with ischemic ATN compared to levels in patients with other forms of acute renal failure or chronic renal disease
bull Adjusted for age gender and length of time delay between the initial insult and sampling of the urine a one-unit increase in normalized KIM-1 was associated with a greater than 12-fold risk for the presence of ATN
bull In hospital patients with AKI urinary levels of KIM-1 that higher levels correlated with a higher odds ratio for dialysis requirement or hospital death
bull this study demonstrated that urinary biomarker of AKI such as KIM-1 can predict adverse clinical outcomes in patients with AKI
bull Both renal and urinary KIM-1 correlate with kidney damage and negatively with renal function but not with proteinuria
bull A recent study has explored urinary KIM-1correlated with kidney function in kidney allograft recipients Kidney transplant recipients showed significantly higher KIM-1 values than the healthy volunteers this study concluded that even a successful kidney transplantation is associated with kidney injury as reflected by elevated urinary KIM-1
bull A rapid direct 15-minute assay for the detection of urinary human KIM-1 has been developed Using this assay more urinary KIM-1 was detected in the urine of patients with AKI than in the urine from healthy volunteers
Urinary interleukin-18
bull Interleukin18 (IL-18) is a 22 kDa pro-inflammatory cytokine that increases in the kidney after ischemia-reperfusion injury in a caspase- 1-dependent manner
bull Patients with ATN had significantly greater urinary IL-18 concentrations than those with other conditions (healthy controls patients with pre-renal azotemia urinary tract infection CKD and nephrotic syndrome)
bull urinary IL-18 concentrations measured in the first 24 h after kidney transplantation were higher in patients who received a cadaveric kidney that developed delayed graft function compared to patients who received a cadaveric kidney with prompt graft function and patients who received a kidney with prompt graft function from a living donor
bull However the performance of urinary IL-18 measured 1 day before AKI was modest
bull Its predictive utility for AKI following cardiac surgery could not be demonstrated in one prospective observational study of 100 adult patients
bull In addition in a large study population of 1439 critically ill patients IL-18 had a poor-to-moderate ability to predict AKI renal replacement therapy (RRT) or 90-day mortality
Liver-Type Fatty Acid Binding Protein(L-FABP)
bull Liver-type fatty acid-binding protein (L-FABP) is a 14 kDa protein from the large super- family of lipidbinding proteins
bull The 14-kD L-FABP protein can be localized predominantly in the proximal tubule
bull Noiri et al demonstrated that increase of urinary L-FABP was observed at 1 h after ischemia even in the 5-min IRI group and urinary L-FABP was superior to BUN and urinary NAG for early and accurate detection of acute tubular necrosis in different models of animal AKI
bull urinary L-FABP may be a promising biomarker for early detection of AKI and prediction of dialysis requirement and in-hospital mortality
bull Urinary excretion of urinary liver-type fatty acid-binding protein (L-FABP) reflects stress of proximal tubular epithelial cells and correlates with severity of ischemic tubular injury
bull A meta-analysis of 15 prospective cohort studies demonstrated that in hospitalndashbased cohorts of patients at risk of AKI L-FABP can discriminate for the diagnosis of AKI and predict the need for dialysis and in-hospital mortality
bull It was correlated with the degree of tubulointerstitial damage in a folic acid induced nephropathy
bull In ischemic and cisplatin-induced AKI L-FABP was increased in the urine before the increase in BUN
bull In cisplatin-induced AKI urinary L-FABP levels increased exponentially even in the lowest dose group as early as 2 hours whereas BUN levels increased at 48 hours
bull L-FABP was measured in 80 critically ill patients Urinary L-FABP levels in patients with septic shock were significantly higher than severe sepsis without shock Serum L-FABP levels did not have significant differences between patients with septic shock severe sepsis and healthy
bull Another study was evaluated 145 septic shock patients complicated with established AKI Urinary L-FABP measured at admission was significantly higher in the nonsurvivors of septic shock with established acute kidney injury than in the survivors
Failure of the TRIBE-AKI study
bull The Translational Research Investigating Biomarker Endpoints in AKI (TRIBE-AKI) study evaluated the performance of urinary c-glutamyltranspeptidase ( c-GTP) alkaline phosphatase NGAL Cys-C KIM-1 and IL-18 in AKI diagnosis
bull The results of four novel urine biomarkers and one plasma biomarker (urine NGAL IL-18 KIM-1 and L-FABP and plasma NGAL) were provided Of all the novel biomarkers only urine IL-18 and plasma NGAL in adults were helpful in predicting progression of AKI when measured on the day of clinical AKI diagnosis
bull Combinations of three biomarkers in adults from two different time points and combinations of two biomarkers in children from two time points were found to be able to increase the ROC for AKI up to 078
bull In summary the clinical use of single damage biomarkers in AKI prediction remains unclear because large prospective multicenter trials such as the TRIBE-AKI study (nfrac141530) have failed to demonstrate troponin-like diagnostic performance
Various clinical scenarios of AKI based onfunction damage and stress
bull Over the last decade a number of novel damage biomarkers have been evaluated for their capacity to detect kidney damage and predict the development of AKI However the relationship between decreasing function and increasing damage is not as straightforward as might be assumed
bull The characteristic pattern whereby damage precedes loss of function (panel A) may be seen in some cases of AKI and affords an opportunity to detect ldquosubclinicalrdquo AKI before function start to fall Unfortunately other patterns might also occur For example functional decline may start to occur alongside damage (panel B) and in some cases function may start to decline even before damage (panel C)
bull This makes damage markers difficult to use for predicting AKI However other markers might actually measure the ldquostressrdquo occurring at the cellular level before damage or loss of function
Paradigm shift to pre-injury phase biomarkers
bull Katz et al proposed that the pre-injury phase that leads to AKI can be described as ldquoacute kidney stressrdquo (AKS) after the report of the identification of cell cycle arrest biomarkers that signal the potential development of AKI is part of an evolution in the molecular diagnosis and understanding of AKI
bull These biomarkers are released by kidney cells along a path which may lead to AKI during a pre-injury phase
bull AKS is defined as the increased-risk phase (pre-injury phase) that leads to AKI
bull This ldquoAKSrdquo may or may not lead to damage and functional declinebull But it is the earliest possible the process of AKI can be detected
Pre-injury phase biomarkers
Stress biomarkersbull In 2013 Kashani et al reported the results of a prospective international
observational investigation (the Sapphire study) of tissue inhibitor of metalloproteinases- 2 (TIMP-2) and insulin-like growth factor-binding protein 7 (IGFBP7) in a heterogeneous group of critically ill patients [TIMP-2][IGFBP7] was significantly superior to all previously described markers of AKI (plt0002)
bull Next the Opal and Topaz study showed the cut-off value and risk assessment using the urinary[TIMP-2] [IGFBP7]
bull The urine [IGFBP7][TIMP2] biomarker is already FDA approved and commercially available in the United States
bull Falsepositive results are common and they will be magnified if the test is used inappropriately in low-risk patients In addition this biomarker should not be used in ambulatory practices and it is not beneficial in patients with established AKI
microRNAsbull microRNAs (miRNAs) are endogenous single-stranded non-coding
mRNAs of about 19-23 nucleotides bull In the past years researchers have begun to investigate the
relevance of miRNAs to AKI with many miRNAs being implicated bull Some of them contribute to pathogenesis by regulating apoptosis
and inflammation amplifying or reducing acute injury responses while others regulate fibrosis and angiogenesis participating in renal recovery or progression to fibrosis
bull Certain miRNAs have been investigated for their potential as novel biomarkers for the early detection or prognostication of AKI
Hemojuvelinbull Hemojuvelin (HJV) a glycophosphatidylinositol (GPI)- linked
membrane protein is highly expressed in liver and skeletal musclesbull The molecular weight of HJV is 42 kDa for the soluble form (sHJV)
and can be passed through glomerular filtration and reabsorbed by the renal tubules Increased iron content in the kidney and urine is observed in human and animal models of AKI and increased iron load can induce renal tubular cell injury
bull There is evidence that the increased expression of the hemojuvelin-hepcidin ferroportin pathway is an intrinsic response to iron overload conditions during AKI
bull Therefore urine HJV (uHJV) has the potential to be an early AKI biomarker in response to iron homeostasis during AKI
Combination of functional and damage biomarkers
bull While new biomarkers are being validated functional biomarkers (serum creatinine serum urea and urine output) continue to be utilized in the diagnosis and staging of AKI In the future existing or newer damage biomarkers will likely be combined with the use of functional biomarkers to enhance the ability of RIFLE AKIN
bull A study of 345 children after cardiopulmonary bypass surgery demonstrated that the composite of functional biomarker such as plasma cystatin C and urinary NGAL was superior to changes in serum creatinine to predict AKI
PROGNOSTIC BIOMARKERS
bull Most of the biomarkers described above allow early detection of acute kidney injury but do not predict severe AKI
Urinary renin and angiotensinogen
bull Urinary renin angiotensinogen and plasma NGAL may predict the development of severe AKI
bull Among 99 consecutively enrolled patients who developed AKI the ratio of urinary angiotensinogen to urinary creatinine (uAnCR expressed as ng per mg creatinine)calculated Patients with the highest uAnCR had a higher risk of worsening AKI compared with patients with the lowest uAnCR An elevated uAnCR predicted a longer hospital stay
bull Among 204 patients who developed Acute Kidney Injury Network (AKIN) stage 1 following cardiac surgery the urinary renin-to-creatinine ratio and the angiotensinogen-to-creatinine ratio predicted a composite outcome of death or AKIN stage 3 or death
Plasma NGAL
bull In a prospective cohort study in which 616 patients admitted from the emergency department were classified by clinical criteria as AKI transient azotemia stable CKD or normal kidney function plasma NGAL discriminated AKI from normal function and from transient azotemia
bull Higher concentrations of NGAL were associated with more severe AKI
Thanks for your attention

bull Over the past decade Cystatin C (CyC) a serum measure of renal function is a stronger predictor of the risk of death and cardiovascular events in elderly persons than is creatinine
bull Koyner et al demonstrated that urinary CyC was superior to SCr and plasma CyC in the early diagnosis of acute kidney injury following adult cardiac surgery
bull Roos et al performed a systematic review comparing the diagnostic accuracy of plasma and urine CyC with SCr in patients undergoing cardiac surgery They concluded that the diagnostic accuracy for impaired renal function favors urine CyC
bull However while Cys-C levels are a more precise indicator of kidney function than SCr concentration they seem to be influenced by old age large doses of corticosteroids hyperthyroidism inflammation neoplasia smoking and alcohol consumption
bull Currently it is unclear whether the value of Cys-C is generalizable to all forms of AKI or specific to particular populations
Damage biomarkers
Neutrophil Gelatinase-Associated Lipocalin(NGAL)
bull Human NGAL is a 25 kDa protein firstly identified bound to gelatinase in specific granules of the neutrophil NGAL is a critical component of innate immunity to bacterial infection and is expressed by immune cells hepatocytes and renal tubular cells in various disease states
bull Its resistance to proteolysis further enhanced potential suitability as a clinical biomarker
bull In healthy kidneys it is barel detectable in either plasma or urine
bull However in the setting of acute tubular injury NGAL undergoes rapid and profound upregulation with large increases in both urine and plasma
bull Distinct from traditional markers of function such as creatinine this rapid response enables NGAL to potentially identify injured kidney much earlier than was previously possible The endogenous role of NGAL remains unclear It seems to be involved with iron transportation to and from the proximal tubular epithelial cells and animal studies demonstrate a renoprotective effect of exogenously administered NGAL in the setting of acute ischemic injury
bull NGAL was also detected in the urine of mice in the early stage of cisplatin-induced nephrotoxicity
bull These animal studies demonstrated that NGAL may represent an early sensitive and noninvasive urinary biomarker for ischemic and nephrotoxic kidney injury
bull NGAL is markedly upregulated and abundantly expressed in the kidney after renal ischemia
bull In this setting NGAL may function to dampen toxicity by reducing apoptosis and increasing the normal proliferation of kidney tubule cells
bull following ischemia reperfusion as evidenced by a rise in creatinine the kidneys illuminate indicating NGAL production at the site of injury
bull Interestingly following maneuvers that lead to significant prerenal disease there was no NGAL illumination indicating that prerenal disease does not induce NGAL expression
bull Thus NGAL may potentially be useful in differentiating prerenal disease from ATN
bull In these studies the average sensitivity and specificity of NGAL measured one to three days prior to AKI diagnosis was 76 and 77 percent respectively for cardiac surgery patients and 73 and 80 percent respectively for patients admitted to the intensive care unit (ICU)
bull NGAL may also represent early sensitive biomarker of AKI after contrast administrations for coronary angiography
bull NGAL was measured in the serum and urine before and at 2 4 12 24 and 48 h after contrast administration they found a significant rise in serum NGAL 2 and 4 h after PCI and a rise in urinary NGAL 4 and 12 h after PCI
bull A similar study of 25 patients with normal serum creatinine undergoing PCI due to unstable angina There was a significant rise in serum NGAL after 2 and 4 hours Urinary NGAL and urinary L-FABP followed the same pattern Both markers increased significantly after 4 hours and remained elevated up to 48 hours after PCI
bull Urine and plasma NGAL levels also represent early biomarkers of AKI in ICU
bull A multicenter study of serum NGAL was performed in 143 critically ill children with systemic inflammatory response syndrome (SIRS) or septic shock during the first 24 h of admission to the ICU there was a significant difference in serum NGAL between healthy children ill children with SIRS and septic shock the study was concluded that serum NGAL is a highly sensitive but nonspecific predictor of acute kidney injury in critically ill children with septic shock
bull A 2010 study evaluated 88 ICU patient and found that an NGAL level of ge150 nmolL predicted AKI with 82 sensitivity and 97 specificity
bull A recent study had 98 patients who were divided in two groups depending on the presence of sepsis Fifty-six patients had sepsis while forty-two patients were nonseptic Among septic patients subjects who developed AKI showed signi1048853 cant higher levels of NGAL
bull A more study of 65 patients with septic shock were found that urine NGAL levels 12 hours before AKI diagnosis were a good predictor of AKI
Kidney Injury Molecule-1 (KIM-1)
bull KIM-1 mRNA and protein are expressed at a low level in normal kidney but are increased dramatically in postischemic kidney
bull KIM-1 has been identified as the first nonmyeloidphosphatidylserine receptor that confers a phagocytic phenotype on injured epithelial cells both in vivo and in vitro
bull Urinary KIM-1 has been found to be an early indicator of AKI that compares favorably to a number of conventional biomarkers and tubular enzymes
bull KIM-1 is also a tissue and urinary biomarker for nephrotoxicant-induced kidney injury
bull Tissue and urinary expressions were measured with different nephrotoxic doses of cisplatin folic acide cadmium gentamycin mercury
bull As early as 1 day after cisplatin treatment positive KIM- 1 immunostaining observed in the outer medulla of the kidney and changes in urinary clusterin indicated the onset of proximal tubular injury in the absence of functional effects
bull Tissue KIM-1 was the most sensitive biomarker for detection of cisplatin-induced kidney damage
bull KIM-1 is a biomarker of AKI in humans bull Urine samples were collected from 32 patients with various
acute and chronic kidney diseases as well as from eight normal controls there was extensive expression of KIM-1 in proximal tubule cells in kidney biopsies from six patients with biopsy confirmed acute tubular necrosis (ATN)
bull Urinary KIM-1 levels were significantly higher in patients with ischemic ATN compared to levels in patients with other forms of acute renal failure or chronic renal disease
bull Adjusted for age gender and length of time delay between the initial insult and sampling of the urine a one-unit increase in normalized KIM-1 was associated with a greater than 12-fold risk for the presence of ATN
bull In hospital patients with AKI urinary levels of KIM-1 that higher levels correlated with a higher odds ratio for dialysis requirement or hospital death
bull this study demonstrated that urinary biomarker of AKI such as KIM-1 can predict adverse clinical outcomes in patients with AKI
bull Both renal and urinary KIM-1 correlate with kidney damage and negatively with renal function but not with proteinuria
bull A recent study has explored urinary KIM-1correlated with kidney function in kidney allograft recipients Kidney transplant recipients showed significantly higher KIM-1 values than the healthy volunteers this study concluded that even a successful kidney transplantation is associated with kidney injury as reflected by elevated urinary KIM-1
bull A rapid direct 15-minute assay for the detection of urinary human KIM-1 has been developed Using this assay more urinary KIM-1 was detected in the urine of patients with AKI than in the urine from healthy volunteers
Urinary interleukin-18
bull Interleukin18 (IL-18) is a 22 kDa pro-inflammatory cytokine that increases in the kidney after ischemia-reperfusion injury in a caspase- 1-dependent manner
bull Patients with ATN had significantly greater urinary IL-18 concentrations than those with other conditions (healthy controls patients with pre-renal azotemia urinary tract infection CKD and nephrotic syndrome)
bull urinary IL-18 concentrations measured in the first 24 h after kidney transplantation were higher in patients who received a cadaveric kidney that developed delayed graft function compared to patients who received a cadaveric kidney with prompt graft function and patients who received a kidney with prompt graft function from a living donor
bull However the performance of urinary IL-18 measured 1 day before AKI was modest
bull Its predictive utility for AKI following cardiac surgery could not be demonstrated in one prospective observational study of 100 adult patients
bull In addition in a large study population of 1439 critically ill patients IL-18 had a poor-to-moderate ability to predict AKI renal replacement therapy (RRT) or 90-day mortality
Liver-Type Fatty Acid Binding Protein(L-FABP)
bull Liver-type fatty acid-binding protein (L-FABP) is a 14 kDa protein from the large super- family of lipidbinding proteins
bull The 14-kD L-FABP protein can be localized predominantly in the proximal tubule
bull Noiri et al demonstrated that increase of urinary L-FABP was observed at 1 h after ischemia even in the 5-min IRI group and urinary L-FABP was superior to BUN and urinary NAG for early and accurate detection of acute tubular necrosis in different models of animal AKI
bull urinary L-FABP may be a promising biomarker for early detection of AKI and prediction of dialysis requirement and in-hospital mortality
bull Urinary excretion of urinary liver-type fatty acid-binding protein (L-FABP) reflects stress of proximal tubular epithelial cells and correlates with severity of ischemic tubular injury
bull A meta-analysis of 15 prospective cohort studies demonstrated that in hospitalndashbased cohorts of patients at risk of AKI L-FABP can discriminate for the diagnosis of AKI and predict the need for dialysis and in-hospital mortality
bull It was correlated with the degree of tubulointerstitial damage in a folic acid induced nephropathy
bull In ischemic and cisplatin-induced AKI L-FABP was increased in the urine before the increase in BUN
bull In cisplatin-induced AKI urinary L-FABP levels increased exponentially even in the lowest dose group as early as 2 hours whereas BUN levels increased at 48 hours
bull L-FABP was measured in 80 critically ill patients Urinary L-FABP levels in patients with septic shock were significantly higher than severe sepsis without shock Serum L-FABP levels did not have significant differences between patients with septic shock severe sepsis and healthy
bull Another study was evaluated 145 septic shock patients complicated with established AKI Urinary L-FABP measured at admission was significantly higher in the nonsurvivors of septic shock with established acute kidney injury than in the survivors
Failure of the TRIBE-AKI study
bull The Translational Research Investigating Biomarker Endpoints in AKI (TRIBE-AKI) study evaluated the performance of urinary c-glutamyltranspeptidase ( c-GTP) alkaline phosphatase NGAL Cys-C KIM-1 and IL-18 in AKI diagnosis
bull The results of four novel urine biomarkers and one plasma biomarker (urine NGAL IL-18 KIM-1 and L-FABP and plasma NGAL) were provided Of all the novel biomarkers only urine IL-18 and plasma NGAL in adults were helpful in predicting progression of AKI when measured on the day of clinical AKI diagnosis
bull Combinations of three biomarkers in adults from two different time points and combinations of two biomarkers in children from two time points were found to be able to increase the ROC for AKI up to 078
bull In summary the clinical use of single damage biomarkers in AKI prediction remains unclear because large prospective multicenter trials such as the TRIBE-AKI study (nfrac141530) have failed to demonstrate troponin-like diagnostic performance
Various clinical scenarios of AKI based onfunction damage and stress
bull Over the last decade a number of novel damage biomarkers have been evaluated for their capacity to detect kidney damage and predict the development of AKI However the relationship between decreasing function and increasing damage is not as straightforward as might be assumed
bull The characteristic pattern whereby damage precedes loss of function (panel A) may be seen in some cases of AKI and affords an opportunity to detect ldquosubclinicalrdquo AKI before function start to fall Unfortunately other patterns might also occur For example functional decline may start to occur alongside damage (panel B) and in some cases function may start to decline even before damage (panel C)
bull This makes damage markers difficult to use for predicting AKI However other markers might actually measure the ldquostressrdquo occurring at the cellular level before damage or loss of function
Paradigm shift to pre-injury phase biomarkers
bull Katz et al proposed that the pre-injury phase that leads to AKI can be described as ldquoacute kidney stressrdquo (AKS) after the report of the identification of cell cycle arrest biomarkers that signal the potential development of AKI is part of an evolution in the molecular diagnosis and understanding of AKI
bull These biomarkers are released by kidney cells along a path which may lead to AKI during a pre-injury phase
bull AKS is defined as the increased-risk phase (pre-injury phase) that leads to AKI
bull This ldquoAKSrdquo may or may not lead to damage and functional declinebull But it is the earliest possible the process of AKI can be detected
Pre-injury phase biomarkers
Stress biomarkersbull In 2013 Kashani et al reported the results of a prospective international
observational investigation (the Sapphire study) of tissue inhibitor of metalloproteinases- 2 (TIMP-2) and insulin-like growth factor-binding protein 7 (IGFBP7) in a heterogeneous group of critically ill patients [TIMP-2][IGFBP7] was significantly superior to all previously described markers of AKI (plt0002)
bull Next the Opal and Topaz study showed the cut-off value and risk assessment using the urinary[TIMP-2] [IGFBP7]
bull The urine [IGFBP7][TIMP2] biomarker is already FDA approved and commercially available in the United States
bull Falsepositive results are common and they will be magnified if the test is used inappropriately in low-risk patients In addition this biomarker should not be used in ambulatory practices and it is not beneficial in patients with established AKI
microRNAsbull microRNAs (miRNAs) are endogenous single-stranded non-coding
mRNAs of about 19-23 nucleotides bull In the past years researchers have begun to investigate the
relevance of miRNAs to AKI with many miRNAs being implicated bull Some of them contribute to pathogenesis by regulating apoptosis
and inflammation amplifying or reducing acute injury responses while others regulate fibrosis and angiogenesis participating in renal recovery or progression to fibrosis
bull Certain miRNAs have been investigated for their potential as novel biomarkers for the early detection or prognostication of AKI
Hemojuvelinbull Hemojuvelin (HJV) a glycophosphatidylinositol (GPI)- linked
membrane protein is highly expressed in liver and skeletal musclesbull The molecular weight of HJV is 42 kDa for the soluble form (sHJV)
and can be passed through glomerular filtration and reabsorbed by the renal tubules Increased iron content in the kidney and urine is observed in human and animal models of AKI and increased iron load can induce renal tubular cell injury
bull There is evidence that the increased expression of the hemojuvelin-hepcidin ferroportin pathway is an intrinsic response to iron overload conditions during AKI
bull Therefore urine HJV (uHJV) has the potential to be an early AKI biomarker in response to iron homeostasis during AKI
Combination of functional and damage biomarkers
bull While new biomarkers are being validated functional biomarkers (serum creatinine serum urea and urine output) continue to be utilized in the diagnosis and staging of AKI In the future existing or newer damage biomarkers will likely be combined with the use of functional biomarkers to enhance the ability of RIFLE AKIN
bull A study of 345 children after cardiopulmonary bypass surgery demonstrated that the composite of functional biomarker such as plasma cystatin C and urinary NGAL was superior to changes in serum creatinine to predict AKI
PROGNOSTIC BIOMARKERS
bull Most of the biomarkers described above allow early detection of acute kidney injury but do not predict severe AKI
Urinary renin and angiotensinogen
bull Urinary renin angiotensinogen and plasma NGAL may predict the development of severe AKI
bull Among 99 consecutively enrolled patients who developed AKI the ratio of urinary angiotensinogen to urinary creatinine (uAnCR expressed as ng per mg creatinine)calculated Patients with the highest uAnCR had a higher risk of worsening AKI compared with patients with the lowest uAnCR An elevated uAnCR predicted a longer hospital stay
bull Among 204 patients who developed Acute Kidney Injury Network (AKIN) stage 1 following cardiac surgery the urinary renin-to-creatinine ratio and the angiotensinogen-to-creatinine ratio predicted a composite outcome of death or AKIN stage 3 or death
Plasma NGAL
bull In a prospective cohort study in which 616 patients admitted from the emergency department were classified by clinical criteria as AKI transient azotemia stable CKD or normal kidney function plasma NGAL discriminated AKI from normal function and from transient azotemia
bull Higher concentrations of NGAL were associated with more severe AKI
Thanks for your attention

Damage biomarkers
Neutrophil Gelatinase-Associated Lipocalin(NGAL)
bull Human NGAL is a 25 kDa protein firstly identified bound to gelatinase in specific granules of the neutrophil NGAL is a critical component of innate immunity to bacterial infection and is expressed by immune cells hepatocytes and renal tubular cells in various disease states
bull Its resistance to proteolysis further enhanced potential suitability as a clinical biomarker
bull In healthy kidneys it is barel detectable in either plasma or urine
bull However in the setting of acute tubular injury NGAL undergoes rapid and profound upregulation with large increases in both urine and plasma
bull Distinct from traditional markers of function such as creatinine this rapid response enables NGAL to potentially identify injured kidney much earlier than was previously possible The endogenous role of NGAL remains unclear It seems to be involved with iron transportation to and from the proximal tubular epithelial cells and animal studies demonstrate a renoprotective effect of exogenously administered NGAL in the setting of acute ischemic injury
bull NGAL was also detected in the urine of mice in the early stage of cisplatin-induced nephrotoxicity
bull These animal studies demonstrated that NGAL may represent an early sensitive and noninvasive urinary biomarker for ischemic and nephrotoxic kidney injury
bull NGAL is markedly upregulated and abundantly expressed in the kidney after renal ischemia
bull In this setting NGAL may function to dampen toxicity by reducing apoptosis and increasing the normal proliferation of kidney tubule cells
bull following ischemia reperfusion as evidenced by a rise in creatinine the kidneys illuminate indicating NGAL production at the site of injury
bull Interestingly following maneuvers that lead to significant prerenal disease there was no NGAL illumination indicating that prerenal disease does not induce NGAL expression
bull Thus NGAL may potentially be useful in differentiating prerenal disease from ATN
bull In these studies the average sensitivity and specificity of NGAL measured one to three days prior to AKI diagnosis was 76 and 77 percent respectively for cardiac surgery patients and 73 and 80 percent respectively for patients admitted to the intensive care unit (ICU)
bull NGAL may also represent early sensitive biomarker of AKI after contrast administrations for coronary angiography
bull NGAL was measured in the serum and urine before and at 2 4 12 24 and 48 h after contrast administration they found a significant rise in serum NGAL 2 and 4 h after PCI and a rise in urinary NGAL 4 and 12 h after PCI
bull A similar study of 25 patients with normal serum creatinine undergoing PCI due to unstable angina There was a significant rise in serum NGAL after 2 and 4 hours Urinary NGAL and urinary L-FABP followed the same pattern Both markers increased significantly after 4 hours and remained elevated up to 48 hours after PCI
bull Urine and plasma NGAL levels also represent early biomarkers of AKI in ICU
bull A multicenter study of serum NGAL was performed in 143 critically ill children with systemic inflammatory response syndrome (SIRS) or septic shock during the first 24 h of admission to the ICU there was a significant difference in serum NGAL between healthy children ill children with SIRS and septic shock the study was concluded that serum NGAL is a highly sensitive but nonspecific predictor of acute kidney injury in critically ill children with septic shock
bull A 2010 study evaluated 88 ICU patient and found that an NGAL level of ge150 nmolL predicted AKI with 82 sensitivity and 97 specificity
bull A recent study had 98 patients who were divided in two groups depending on the presence of sepsis Fifty-six patients had sepsis while forty-two patients were nonseptic Among septic patients subjects who developed AKI showed signi1048853 cant higher levels of NGAL
bull A more study of 65 patients with septic shock were found that urine NGAL levels 12 hours before AKI diagnosis were a good predictor of AKI
Kidney Injury Molecule-1 (KIM-1)
bull KIM-1 mRNA and protein are expressed at a low level in normal kidney but are increased dramatically in postischemic kidney
bull KIM-1 has been identified as the first nonmyeloidphosphatidylserine receptor that confers a phagocytic phenotype on injured epithelial cells both in vivo and in vitro
bull Urinary KIM-1 has been found to be an early indicator of AKI that compares favorably to a number of conventional biomarkers and tubular enzymes
bull KIM-1 is also a tissue and urinary biomarker for nephrotoxicant-induced kidney injury
bull Tissue and urinary expressions were measured with different nephrotoxic doses of cisplatin folic acide cadmium gentamycin mercury
bull As early as 1 day after cisplatin treatment positive KIM- 1 immunostaining observed in the outer medulla of the kidney and changes in urinary clusterin indicated the onset of proximal tubular injury in the absence of functional effects
bull Tissue KIM-1 was the most sensitive biomarker for detection of cisplatin-induced kidney damage
bull KIM-1 is a biomarker of AKI in humans bull Urine samples were collected from 32 patients with various
acute and chronic kidney diseases as well as from eight normal controls there was extensive expression of KIM-1 in proximal tubule cells in kidney biopsies from six patients with biopsy confirmed acute tubular necrosis (ATN)
bull Urinary KIM-1 levels were significantly higher in patients with ischemic ATN compared to levels in patients with other forms of acute renal failure or chronic renal disease
bull Adjusted for age gender and length of time delay between the initial insult and sampling of the urine a one-unit increase in normalized KIM-1 was associated with a greater than 12-fold risk for the presence of ATN
bull In hospital patients with AKI urinary levels of KIM-1 that higher levels correlated with a higher odds ratio for dialysis requirement or hospital death
bull this study demonstrated that urinary biomarker of AKI such as KIM-1 can predict adverse clinical outcomes in patients with AKI
bull Both renal and urinary KIM-1 correlate with kidney damage and negatively with renal function but not with proteinuria
bull A recent study has explored urinary KIM-1correlated with kidney function in kidney allograft recipients Kidney transplant recipients showed significantly higher KIM-1 values than the healthy volunteers this study concluded that even a successful kidney transplantation is associated with kidney injury as reflected by elevated urinary KIM-1
bull A rapid direct 15-minute assay for the detection of urinary human KIM-1 has been developed Using this assay more urinary KIM-1 was detected in the urine of patients with AKI than in the urine from healthy volunteers
Urinary interleukin-18
bull Interleukin18 (IL-18) is a 22 kDa pro-inflammatory cytokine that increases in the kidney after ischemia-reperfusion injury in a caspase- 1-dependent manner
bull Patients with ATN had significantly greater urinary IL-18 concentrations than those with other conditions (healthy controls patients with pre-renal azotemia urinary tract infection CKD and nephrotic syndrome)
bull urinary IL-18 concentrations measured in the first 24 h after kidney transplantation were higher in patients who received a cadaveric kidney that developed delayed graft function compared to patients who received a cadaveric kidney with prompt graft function and patients who received a kidney with prompt graft function from a living donor
bull However the performance of urinary IL-18 measured 1 day before AKI was modest
bull Its predictive utility for AKI following cardiac surgery could not be demonstrated in one prospective observational study of 100 adult patients
bull In addition in a large study population of 1439 critically ill patients IL-18 had a poor-to-moderate ability to predict AKI renal replacement therapy (RRT) or 90-day mortality
Liver-Type Fatty Acid Binding Protein(L-FABP)
bull Liver-type fatty acid-binding protein (L-FABP) is a 14 kDa protein from the large super- family of lipidbinding proteins
bull The 14-kD L-FABP protein can be localized predominantly in the proximal tubule
bull Noiri et al demonstrated that increase of urinary L-FABP was observed at 1 h after ischemia even in the 5-min IRI group and urinary L-FABP was superior to BUN and urinary NAG for early and accurate detection of acute tubular necrosis in different models of animal AKI
bull urinary L-FABP may be a promising biomarker for early detection of AKI and prediction of dialysis requirement and in-hospital mortality
bull Urinary excretion of urinary liver-type fatty acid-binding protein (L-FABP) reflects stress of proximal tubular epithelial cells and correlates with severity of ischemic tubular injury
bull A meta-analysis of 15 prospective cohort studies demonstrated that in hospitalndashbased cohorts of patients at risk of AKI L-FABP can discriminate for the diagnosis of AKI and predict the need for dialysis and in-hospital mortality
bull It was correlated with the degree of tubulointerstitial damage in a folic acid induced nephropathy
bull In ischemic and cisplatin-induced AKI L-FABP was increased in the urine before the increase in BUN
bull In cisplatin-induced AKI urinary L-FABP levels increased exponentially even in the lowest dose group as early as 2 hours whereas BUN levels increased at 48 hours
bull L-FABP was measured in 80 critically ill patients Urinary L-FABP levels in patients with septic shock were significantly higher than severe sepsis without shock Serum L-FABP levels did not have significant differences between patients with septic shock severe sepsis and healthy
bull Another study was evaluated 145 septic shock patients complicated with established AKI Urinary L-FABP measured at admission was significantly higher in the nonsurvivors of septic shock with established acute kidney injury than in the survivors
Failure of the TRIBE-AKI study
bull The Translational Research Investigating Biomarker Endpoints in AKI (TRIBE-AKI) study evaluated the performance of urinary c-glutamyltranspeptidase ( c-GTP) alkaline phosphatase NGAL Cys-C KIM-1 and IL-18 in AKI diagnosis
bull The results of four novel urine biomarkers and one plasma biomarker (urine NGAL IL-18 KIM-1 and L-FABP and plasma NGAL) were provided Of all the novel biomarkers only urine IL-18 and plasma NGAL in adults were helpful in predicting progression of AKI when measured on the day of clinical AKI diagnosis
bull Combinations of three biomarkers in adults from two different time points and combinations of two biomarkers in children from two time points were found to be able to increase the ROC for AKI up to 078
bull In summary the clinical use of single damage biomarkers in AKI prediction remains unclear because large prospective multicenter trials such as the TRIBE-AKI study (nfrac141530) have failed to demonstrate troponin-like diagnostic performance
Various clinical scenarios of AKI based onfunction damage and stress
bull Over the last decade a number of novel damage biomarkers have been evaluated for their capacity to detect kidney damage and predict the development of AKI However the relationship between decreasing function and increasing damage is not as straightforward as might be assumed
bull The characteristic pattern whereby damage precedes loss of function (panel A) may be seen in some cases of AKI and affords an opportunity to detect ldquosubclinicalrdquo AKI before function start to fall Unfortunately other patterns might also occur For example functional decline may start to occur alongside damage (panel B) and in some cases function may start to decline even before damage (panel C)
bull This makes damage markers difficult to use for predicting AKI However other markers might actually measure the ldquostressrdquo occurring at the cellular level before damage or loss of function
Paradigm shift to pre-injury phase biomarkers
bull Katz et al proposed that the pre-injury phase that leads to AKI can be described as ldquoacute kidney stressrdquo (AKS) after the report of the identification of cell cycle arrest biomarkers that signal the potential development of AKI is part of an evolution in the molecular diagnosis and understanding of AKI
bull These biomarkers are released by kidney cells along a path which may lead to AKI during a pre-injury phase
bull AKS is defined as the increased-risk phase (pre-injury phase) that leads to AKI
bull This ldquoAKSrdquo may or may not lead to damage and functional declinebull But it is the earliest possible the process of AKI can be detected
Pre-injury phase biomarkers
Stress biomarkersbull In 2013 Kashani et al reported the results of a prospective international
observational investigation (the Sapphire study) of tissue inhibitor of metalloproteinases- 2 (TIMP-2) and insulin-like growth factor-binding protein 7 (IGFBP7) in a heterogeneous group of critically ill patients [TIMP-2][IGFBP7] was significantly superior to all previously described markers of AKI (plt0002)
bull Next the Opal and Topaz study showed the cut-off value and risk assessment using the urinary[TIMP-2] [IGFBP7]
bull The urine [IGFBP7][TIMP2] biomarker is already FDA approved and commercially available in the United States
bull Falsepositive results are common and they will be magnified if the test is used inappropriately in low-risk patients In addition this biomarker should not be used in ambulatory practices and it is not beneficial in patients with established AKI
microRNAsbull microRNAs (miRNAs) are endogenous single-stranded non-coding
mRNAs of about 19-23 nucleotides bull In the past years researchers have begun to investigate the
relevance of miRNAs to AKI with many miRNAs being implicated bull Some of them contribute to pathogenesis by regulating apoptosis
and inflammation amplifying or reducing acute injury responses while others regulate fibrosis and angiogenesis participating in renal recovery or progression to fibrosis
bull Certain miRNAs have been investigated for their potential as novel biomarkers for the early detection or prognostication of AKI
Hemojuvelinbull Hemojuvelin (HJV) a glycophosphatidylinositol (GPI)- linked
membrane protein is highly expressed in liver and skeletal musclesbull The molecular weight of HJV is 42 kDa for the soluble form (sHJV)
and can be passed through glomerular filtration and reabsorbed by the renal tubules Increased iron content in the kidney and urine is observed in human and animal models of AKI and increased iron load can induce renal tubular cell injury
bull There is evidence that the increased expression of the hemojuvelin-hepcidin ferroportin pathway is an intrinsic response to iron overload conditions during AKI
bull Therefore urine HJV (uHJV) has the potential to be an early AKI biomarker in response to iron homeostasis during AKI
Combination of functional and damage biomarkers
bull While new biomarkers are being validated functional biomarkers (serum creatinine serum urea and urine output) continue to be utilized in the diagnosis and staging of AKI In the future existing or newer damage biomarkers will likely be combined with the use of functional biomarkers to enhance the ability of RIFLE AKIN
bull A study of 345 children after cardiopulmonary bypass surgery demonstrated that the composite of functional biomarker such as plasma cystatin C and urinary NGAL was superior to changes in serum creatinine to predict AKI
PROGNOSTIC BIOMARKERS
bull Most of the biomarkers described above allow early detection of acute kidney injury but do not predict severe AKI
Urinary renin and angiotensinogen
bull Urinary renin angiotensinogen and plasma NGAL may predict the development of severe AKI
bull Among 99 consecutively enrolled patients who developed AKI the ratio of urinary angiotensinogen to urinary creatinine (uAnCR expressed as ng per mg creatinine)calculated Patients with the highest uAnCR had a higher risk of worsening AKI compared with patients with the lowest uAnCR An elevated uAnCR predicted a longer hospital stay
bull Among 204 patients who developed Acute Kidney Injury Network (AKIN) stage 1 following cardiac surgery the urinary renin-to-creatinine ratio and the angiotensinogen-to-creatinine ratio predicted a composite outcome of death or AKIN stage 3 or death
Plasma NGAL
bull In a prospective cohort study in which 616 patients admitted from the emergency department were classified by clinical criteria as AKI transient azotemia stable CKD or normal kidney function plasma NGAL discriminated AKI from normal function and from transient azotemia
bull Higher concentrations of NGAL were associated with more severe AKI
Thanks for your attention

Neutrophil Gelatinase-Associated Lipocalin(NGAL)
bull Human NGAL is a 25 kDa protein firstly identified bound to gelatinase in specific granules of the neutrophil NGAL is a critical component of innate immunity to bacterial infection and is expressed by immune cells hepatocytes and renal tubular cells in various disease states
bull Its resistance to proteolysis further enhanced potential suitability as a clinical biomarker
bull In healthy kidneys it is barel detectable in either plasma or urine
bull However in the setting of acute tubular injury NGAL undergoes rapid and profound upregulation with large increases in both urine and plasma
bull Distinct from traditional markers of function such as creatinine this rapid response enables NGAL to potentially identify injured kidney much earlier than was previously possible The endogenous role of NGAL remains unclear It seems to be involved with iron transportation to and from the proximal tubular epithelial cells and animal studies demonstrate a renoprotective effect of exogenously administered NGAL in the setting of acute ischemic injury
bull NGAL was also detected in the urine of mice in the early stage of cisplatin-induced nephrotoxicity
bull These animal studies demonstrated that NGAL may represent an early sensitive and noninvasive urinary biomarker for ischemic and nephrotoxic kidney injury
bull NGAL is markedly upregulated and abundantly expressed in the kidney after renal ischemia
bull In this setting NGAL may function to dampen toxicity by reducing apoptosis and increasing the normal proliferation of kidney tubule cells
bull following ischemia reperfusion as evidenced by a rise in creatinine the kidneys illuminate indicating NGAL production at the site of injury
bull Interestingly following maneuvers that lead to significant prerenal disease there was no NGAL illumination indicating that prerenal disease does not induce NGAL expression
bull Thus NGAL may potentially be useful in differentiating prerenal disease from ATN
bull In these studies the average sensitivity and specificity of NGAL measured one to three days prior to AKI diagnosis was 76 and 77 percent respectively for cardiac surgery patients and 73 and 80 percent respectively for patients admitted to the intensive care unit (ICU)
bull NGAL may also represent early sensitive biomarker of AKI after contrast administrations for coronary angiography
bull NGAL was measured in the serum and urine before and at 2 4 12 24 and 48 h after contrast administration they found a significant rise in serum NGAL 2 and 4 h after PCI and a rise in urinary NGAL 4 and 12 h after PCI
bull A similar study of 25 patients with normal serum creatinine undergoing PCI due to unstable angina There was a significant rise in serum NGAL after 2 and 4 hours Urinary NGAL and urinary L-FABP followed the same pattern Both markers increased significantly after 4 hours and remained elevated up to 48 hours after PCI
bull Urine and plasma NGAL levels also represent early biomarkers of AKI in ICU
bull A multicenter study of serum NGAL was performed in 143 critically ill children with systemic inflammatory response syndrome (SIRS) or septic shock during the first 24 h of admission to the ICU there was a significant difference in serum NGAL between healthy children ill children with SIRS and septic shock the study was concluded that serum NGAL is a highly sensitive but nonspecific predictor of acute kidney injury in critically ill children with septic shock
bull A 2010 study evaluated 88 ICU patient and found that an NGAL level of ge150 nmolL predicted AKI with 82 sensitivity and 97 specificity
bull A recent study had 98 patients who were divided in two groups depending on the presence of sepsis Fifty-six patients had sepsis while forty-two patients were nonseptic Among septic patients subjects who developed AKI showed signi1048853 cant higher levels of NGAL
bull A more study of 65 patients with septic shock were found that urine NGAL levels 12 hours before AKI diagnosis were a good predictor of AKI
Kidney Injury Molecule-1 (KIM-1)
bull KIM-1 mRNA and protein are expressed at a low level in normal kidney but are increased dramatically in postischemic kidney
bull KIM-1 has been identified as the first nonmyeloidphosphatidylserine receptor that confers a phagocytic phenotype on injured epithelial cells both in vivo and in vitro
bull Urinary KIM-1 has been found to be an early indicator of AKI that compares favorably to a number of conventional biomarkers and tubular enzymes
bull KIM-1 is also a tissue and urinary biomarker for nephrotoxicant-induced kidney injury
bull Tissue and urinary expressions were measured with different nephrotoxic doses of cisplatin folic acide cadmium gentamycin mercury
bull As early as 1 day after cisplatin treatment positive KIM- 1 immunostaining observed in the outer medulla of the kidney and changes in urinary clusterin indicated the onset of proximal tubular injury in the absence of functional effects
bull Tissue KIM-1 was the most sensitive biomarker for detection of cisplatin-induced kidney damage
bull KIM-1 is a biomarker of AKI in humans bull Urine samples were collected from 32 patients with various
acute and chronic kidney diseases as well as from eight normal controls there was extensive expression of KIM-1 in proximal tubule cells in kidney biopsies from six patients with biopsy confirmed acute tubular necrosis (ATN)
bull Urinary KIM-1 levels were significantly higher in patients with ischemic ATN compared to levels in patients with other forms of acute renal failure or chronic renal disease
bull Adjusted for age gender and length of time delay between the initial insult and sampling of the urine a one-unit increase in normalized KIM-1 was associated with a greater than 12-fold risk for the presence of ATN
bull In hospital patients with AKI urinary levels of KIM-1 that higher levels correlated with a higher odds ratio for dialysis requirement or hospital death
bull this study demonstrated that urinary biomarker of AKI such as KIM-1 can predict adverse clinical outcomes in patients with AKI
bull Both renal and urinary KIM-1 correlate with kidney damage and negatively with renal function but not with proteinuria
bull A recent study has explored urinary KIM-1correlated with kidney function in kidney allograft recipients Kidney transplant recipients showed significantly higher KIM-1 values than the healthy volunteers this study concluded that even a successful kidney transplantation is associated with kidney injury as reflected by elevated urinary KIM-1
bull A rapid direct 15-minute assay for the detection of urinary human KIM-1 has been developed Using this assay more urinary KIM-1 was detected in the urine of patients with AKI than in the urine from healthy volunteers
Urinary interleukin-18
bull Interleukin18 (IL-18) is a 22 kDa pro-inflammatory cytokine that increases in the kidney after ischemia-reperfusion injury in a caspase- 1-dependent manner
bull Patients with ATN had significantly greater urinary IL-18 concentrations than those with other conditions (healthy controls patients with pre-renal azotemia urinary tract infection CKD and nephrotic syndrome)
bull urinary IL-18 concentrations measured in the first 24 h after kidney transplantation were higher in patients who received a cadaveric kidney that developed delayed graft function compared to patients who received a cadaveric kidney with prompt graft function and patients who received a kidney with prompt graft function from a living donor
bull However the performance of urinary IL-18 measured 1 day before AKI was modest
bull Its predictive utility for AKI following cardiac surgery could not be demonstrated in one prospective observational study of 100 adult patients
bull In addition in a large study population of 1439 critically ill patients IL-18 had a poor-to-moderate ability to predict AKI renal replacement therapy (RRT) or 90-day mortality
Liver-Type Fatty Acid Binding Protein(L-FABP)
bull Liver-type fatty acid-binding protein (L-FABP) is a 14 kDa protein from the large super- family of lipidbinding proteins
bull The 14-kD L-FABP protein can be localized predominantly in the proximal tubule
bull Noiri et al demonstrated that increase of urinary L-FABP was observed at 1 h after ischemia even in the 5-min IRI group and urinary L-FABP was superior to BUN and urinary NAG for early and accurate detection of acute tubular necrosis in different models of animal AKI
bull urinary L-FABP may be a promising biomarker for early detection of AKI and prediction of dialysis requirement and in-hospital mortality
bull Urinary excretion of urinary liver-type fatty acid-binding protein (L-FABP) reflects stress of proximal tubular epithelial cells and correlates with severity of ischemic tubular injury
bull A meta-analysis of 15 prospective cohort studies demonstrated that in hospitalndashbased cohorts of patients at risk of AKI L-FABP can discriminate for the diagnosis of AKI and predict the need for dialysis and in-hospital mortality
bull It was correlated with the degree of tubulointerstitial damage in a folic acid induced nephropathy
bull In ischemic and cisplatin-induced AKI L-FABP was increased in the urine before the increase in BUN
bull In cisplatin-induced AKI urinary L-FABP levels increased exponentially even in the lowest dose group as early as 2 hours whereas BUN levels increased at 48 hours
bull L-FABP was measured in 80 critically ill patients Urinary L-FABP levels in patients with septic shock were significantly higher than severe sepsis without shock Serum L-FABP levels did not have significant differences between patients with septic shock severe sepsis and healthy
bull Another study was evaluated 145 septic shock patients complicated with established AKI Urinary L-FABP measured at admission was significantly higher in the nonsurvivors of septic shock with established acute kidney injury than in the survivors
Failure of the TRIBE-AKI study
bull The Translational Research Investigating Biomarker Endpoints in AKI (TRIBE-AKI) study evaluated the performance of urinary c-glutamyltranspeptidase ( c-GTP) alkaline phosphatase NGAL Cys-C KIM-1 and IL-18 in AKI diagnosis
bull The results of four novel urine biomarkers and one plasma biomarker (urine NGAL IL-18 KIM-1 and L-FABP and plasma NGAL) were provided Of all the novel biomarkers only urine IL-18 and plasma NGAL in adults were helpful in predicting progression of AKI when measured on the day of clinical AKI diagnosis
bull Combinations of three biomarkers in adults from two different time points and combinations of two biomarkers in children from two time points were found to be able to increase the ROC for AKI up to 078
bull In summary the clinical use of single damage biomarkers in AKI prediction remains unclear because large prospective multicenter trials such as the TRIBE-AKI study (nfrac141530) have failed to demonstrate troponin-like diagnostic performance
Various clinical scenarios of AKI based onfunction damage and stress
bull Over the last decade a number of novel damage biomarkers have been evaluated for their capacity to detect kidney damage and predict the development of AKI However the relationship between decreasing function and increasing damage is not as straightforward as might be assumed
bull The characteristic pattern whereby damage precedes loss of function (panel A) may be seen in some cases of AKI and affords an opportunity to detect ldquosubclinicalrdquo AKI before function start to fall Unfortunately other patterns might also occur For example functional decline may start to occur alongside damage (panel B) and in some cases function may start to decline even before damage (panel C)
bull This makes damage markers difficult to use for predicting AKI However other markers might actually measure the ldquostressrdquo occurring at the cellular level before damage or loss of function
Paradigm shift to pre-injury phase biomarkers
bull Katz et al proposed that the pre-injury phase that leads to AKI can be described as ldquoacute kidney stressrdquo (AKS) after the report of the identification of cell cycle arrest biomarkers that signal the potential development of AKI is part of an evolution in the molecular diagnosis and understanding of AKI
bull These biomarkers are released by kidney cells along a path which may lead to AKI during a pre-injury phase
bull AKS is defined as the increased-risk phase (pre-injury phase) that leads to AKI
bull This ldquoAKSrdquo may or may not lead to damage and functional declinebull But it is the earliest possible the process of AKI can be detected
Pre-injury phase biomarkers
Stress biomarkersbull In 2013 Kashani et al reported the results of a prospective international
observational investigation (the Sapphire study) of tissue inhibitor of metalloproteinases- 2 (TIMP-2) and insulin-like growth factor-binding protein 7 (IGFBP7) in a heterogeneous group of critically ill patients [TIMP-2][IGFBP7] was significantly superior to all previously described markers of AKI (plt0002)
bull Next the Opal and Topaz study showed the cut-off value and risk assessment using the urinary[TIMP-2] [IGFBP7]
bull The urine [IGFBP7][TIMP2] biomarker is already FDA approved and commercially available in the United States
bull Falsepositive results are common and they will be magnified if the test is used inappropriately in low-risk patients In addition this biomarker should not be used in ambulatory practices and it is not beneficial in patients with established AKI
microRNAsbull microRNAs (miRNAs) are endogenous single-stranded non-coding
mRNAs of about 19-23 nucleotides bull In the past years researchers have begun to investigate the
relevance of miRNAs to AKI with many miRNAs being implicated bull Some of them contribute to pathogenesis by regulating apoptosis
and inflammation amplifying or reducing acute injury responses while others regulate fibrosis and angiogenesis participating in renal recovery or progression to fibrosis
bull Certain miRNAs have been investigated for their potential as novel biomarkers for the early detection or prognostication of AKI
Hemojuvelinbull Hemojuvelin (HJV) a glycophosphatidylinositol (GPI)- linked
membrane protein is highly expressed in liver and skeletal musclesbull The molecular weight of HJV is 42 kDa for the soluble form (sHJV)
and can be passed through glomerular filtration and reabsorbed by the renal tubules Increased iron content in the kidney and urine is observed in human and animal models of AKI and increased iron load can induce renal tubular cell injury
bull There is evidence that the increased expression of the hemojuvelin-hepcidin ferroportin pathway is an intrinsic response to iron overload conditions during AKI
bull Therefore urine HJV (uHJV) has the potential to be an early AKI biomarker in response to iron homeostasis during AKI
Combination of functional and damage biomarkers
bull While new biomarkers are being validated functional biomarkers (serum creatinine serum urea and urine output) continue to be utilized in the diagnosis and staging of AKI In the future existing or newer damage biomarkers will likely be combined with the use of functional biomarkers to enhance the ability of RIFLE AKIN
bull A study of 345 children after cardiopulmonary bypass surgery demonstrated that the composite of functional biomarker such as plasma cystatin C and urinary NGAL was superior to changes in serum creatinine to predict AKI
PROGNOSTIC BIOMARKERS
bull Most of the biomarkers described above allow early detection of acute kidney injury but do not predict severe AKI
Urinary renin and angiotensinogen
bull Urinary renin angiotensinogen and plasma NGAL may predict the development of severe AKI
bull Among 99 consecutively enrolled patients who developed AKI the ratio of urinary angiotensinogen to urinary creatinine (uAnCR expressed as ng per mg creatinine)calculated Patients with the highest uAnCR had a higher risk of worsening AKI compared with patients with the lowest uAnCR An elevated uAnCR predicted a longer hospital stay
bull Among 204 patients who developed Acute Kidney Injury Network (AKIN) stage 1 following cardiac surgery the urinary renin-to-creatinine ratio and the angiotensinogen-to-creatinine ratio predicted a composite outcome of death or AKIN stage 3 or death
Plasma NGAL
bull In a prospective cohort study in which 616 patients admitted from the emergency department were classified by clinical criteria as AKI transient azotemia stable CKD or normal kidney function plasma NGAL discriminated AKI from normal function and from transient azotemia
bull Higher concentrations of NGAL were associated with more severe AKI
Thanks for your attention
bull NGAL is markedly upregulated and abundantly expressed in the kidney after renal ischemia
bull In this setting NGAL may function to dampen toxicity by reducing apoptosis and increasing the normal proliferation of kidney tubule cells
bull following ischemia reperfusion as evidenced by a rise in creatinine the kidneys illuminate indicating NGAL production at the site of injury
bull Interestingly following maneuvers that lead to significant prerenal disease there was no NGAL illumination indicating that prerenal disease does not induce NGAL expression
bull Thus NGAL may potentially be useful in differentiating prerenal disease from ATN
bull In these studies the average sensitivity and specificity of NGAL measured one to three days prior to AKI diagnosis was 76 and 77 percent respectively for cardiac surgery patients and 73 and 80 percent respectively for patients admitted to the intensive care unit (ICU)
bull NGAL may also represent early sensitive biomarker of AKI after contrast administrations for coronary angiography
bull NGAL was measured in the serum and urine before and at 2 4 12 24 and 48 h after contrast administration they found a significant rise in serum NGAL 2 and 4 h after PCI and a rise in urinary NGAL 4 and 12 h after PCI
bull A similar study of 25 patients with normal serum creatinine undergoing PCI due to unstable angina There was a significant rise in serum NGAL after 2 and 4 hours Urinary NGAL and urinary L-FABP followed the same pattern Both markers increased significantly after 4 hours and remained elevated up to 48 hours after PCI
bull Urine and plasma NGAL levels also represent early biomarkers of AKI in ICU
bull A multicenter study of serum NGAL was performed in 143 critically ill children with systemic inflammatory response syndrome (SIRS) or septic shock during the first 24 h of admission to the ICU there was a significant difference in serum NGAL between healthy children ill children with SIRS and septic shock the study was concluded that serum NGAL is a highly sensitive but nonspecific predictor of acute kidney injury in critically ill children with septic shock
bull A 2010 study evaluated 88 ICU patient and found that an NGAL level of ge150 nmolL predicted AKI with 82 sensitivity and 97 specificity
bull A recent study had 98 patients who were divided in two groups depending on the presence of sepsis Fifty-six patients had sepsis while forty-two patients were nonseptic Among septic patients subjects who developed AKI showed signi1048853 cant higher levels of NGAL
bull A more study of 65 patients with septic shock were found that urine NGAL levels 12 hours before AKI diagnosis were a good predictor of AKI
Kidney Injury Molecule-1 (KIM-1)
bull KIM-1 mRNA and protein are expressed at a low level in normal kidney but are increased dramatically in postischemic kidney
bull KIM-1 has been identified as the first nonmyeloidphosphatidylserine receptor that confers a phagocytic phenotype on injured epithelial cells both in vivo and in vitro
bull Urinary KIM-1 has been found to be an early indicator of AKI that compares favorably to a number of conventional biomarkers and tubular enzymes
bull KIM-1 is also a tissue and urinary biomarker for nephrotoxicant-induced kidney injury
bull Tissue and urinary expressions were measured with different nephrotoxic doses of cisplatin folic acide cadmium gentamycin mercury
bull As early as 1 day after cisplatin treatment positive KIM- 1 immunostaining observed in the outer medulla of the kidney and changes in urinary clusterin indicated the onset of proximal tubular injury in the absence of functional effects
bull Tissue KIM-1 was the most sensitive biomarker for detection of cisplatin-induced kidney damage
bull KIM-1 is a biomarker of AKI in humans bull Urine samples were collected from 32 patients with various
acute and chronic kidney diseases as well as from eight normal controls there was extensive expression of KIM-1 in proximal tubule cells in kidney biopsies from six patients with biopsy confirmed acute tubular necrosis (ATN)
bull Urinary KIM-1 levels were significantly higher in patients with ischemic ATN compared to levels in patients with other forms of acute renal failure or chronic renal disease
bull Adjusted for age gender and length of time delay between the initial insult and sampling of the urine a one-unit increase in normalized KIM-1 was associated with a greater than 12-fold risk for the presence of ATN
bull In hospital patients with AKI urinary levels of KIM-1 that higher levels correlated with a higher odds ratio for dialysis requirement or hospital death
bull this study demonstrated that urinary biomarker of AKI such as KIM-1 can predict adverse clinical outcomes in patients with AKI
bull Both renal and urinary KIM-1 correlate with kidney damage and negatively with renal function but not with proteinuria
bull A recent study has explored urinary KIM-1correlated with kidney function in kidney allograft recipients Kidney transplant recipients showed significantly higher KIM-1 values than the healthy volunteers this study concluded that even a successful kidney transplantation is associated with kidney injury as reflected by elevated urinary KIM-1
bull A rapid direct 15-minute assay for the detection of urinary human KIM-1 has been developed Using this assay more urinary KIM-1 was detected in the urine of patients with AKI than in the urine from healthy volunteers
Urinary interleukin-18
bull Interleukin18 (IL-18) is a 22 kDa pro-inflammatory cytokine that increases in the kidney after ischemia-reperfusion injury in a caspase- 1-dependent manner
bull Patients with ATN had significantly greater urinary IL-18 concentrations than those with other conditions (healthy controls patients with pre-renal azotemia urinary tract infection CKD and nephrotic syndrome)
bull urinary IL-18 concentrations measured in the first 24 h after kidney transplantation were higher in patients who received a cadaveric kidney that developed delayed graft function compared to patients who received a cadaveric kidney with prompt graft function and patients who received a kidney with prompt graft function from a living donor
bull However the performance of urinary IL-18 measured 1 day before AKI was modest
bull Its predictive utility for AKI following cardiac surgery could not be demonstrated in one prospective observational study of 100 adult patients
bull In addition in a large study population of 1439 critically ill patients IL-18 had a poor-to-moderate ability to predict AKI renal replacement therapy (RRT) or 90-day mortality
Liver-Type Fatty Acid Binding Protein(L-FABP)
bull Liver-type fatty acid-binding protein (L-FABP) is a 14 kDa protein from the large super- family of lipidbinding proteins
bull The 14-kD L-FABP protein can be localized predominantly in the proximal tubule
bull Noiri et al demonstrated that increase of urinary L-FABP was observed at 1 h after ischemia even in the 5-min IRI group and urinary L-FABP was superior to BUN and urinary NAG for early and accurate detection of acute tubular necrosis in different models of animal AKI
bull urinary L-FABP may be a promising biomarker for early detection of AKI and prediction of dialysis requirement and in-hospital mortality
bull Urinary excretion of urinary liver-type fatty acid-binding protein (L-FABP) reflects stress of proximal tubular epithelial cells and correlates with severity of ischemic tubular injury
bull A meta-analysis of 15 prospective cohort studies demonstrated that in hospitalndashbased cohorts of patients at risk of AKI L-FABP can discriminate for the diagnosis of AKI and predict the need for dialysis and in-hospital mortality
bull It was correlated with the degree of tubulointerstitial damage in a folic acid induced nephropathy
bull In ischemic and cisplatin-induced AKI L-FABP was increased in the urine before the increase in BUN
bull In cisplatin-induced AKI urinary L-FABP levels increased exponentially even in the lowest dose group as early as 2 hours whereas BUN levels increased at 48 hours
bull L-FABP was measured in 80 critically ill patients Urinary L-FABP levels in patients with septic shock were significantly higher than severe sepsis without shock Serum L-FABP levels did not have significant differences between patients with septic shock severe sepsis and healthy
bull Another study was evaluated 145 septic shock patients complicated with established AKI Urinary L-FABP measured at admission was significantly higher in the nonsurvivors of septic shock with established acute kidney injury than in the survivors
Failure of the TRIBE-AKI study
bull The Translational Research Investigating Biomarker Endpoints in AKI (TRIBE-AKI) study evaluated the performance of urinary c-glutamyltranspeptidase ( c-GTP) alkaline phosphatase NGAL Cys-C KIM-1 and IL-18 in AKI diagnosis
bull The results of four novel urine biomarkers and one plasma biomarker (urine NGAL IL-18 KIM-1 and L-FABP and plasma NGAL) were provided Of all the novel biomarkers only urine IL-18 and plasma NGAL in adults were helpful in predicting progression of AKI when measured on the day of clinical AKI diagnosis
bull Combinations of three biomarkers in adults from two different time points and combinations of two biomarkers in children from two time points were found to be able to increase the ROC for AKI up to 078
bull In summary the clinical use of single damage biomarkers in AKI prediction remains unclear because large prospective multicenter trials such as the TRIBE-AKI study (nfrac141530) have failed to demonstrate troponin-like diagnostic performance
Various clinical scenarios of AKI based onfunction damage and stress
bull Over the last decade a number of novel damage biomarkers have been evaluated for their capacity to detect kidney damage and predict the development of AKI However the relationship between decreasing function and increasing damage is not as straightforward as might be assumed
bull The characteristic pattern whereby damage precedes loss of function (panel A) may be seen in some cases of AKI and affords an opportunity to detect ldquosubclinicalrdquo AKI before function start to fall Unfortunately other patterns might also occur For example functional decline may start to occur alongside damage (panel B) and in some cases function may start to decline even before damage (panel C)
bull This makes damage markers difficult to use for predicting AKI However other markers might actually measure the ldquostressrdquo occurring at the cellular level before damage or loss of function
Paradigm shift to pre-injury phase biomarkers
bull Katz et al proposed that the pre-injury phase that leads to AKI can be described as ldquoacute kidney stressrdquo (AKS) after the report of the identification of cell cycle arrest biomarkers that signal the potential development of AKI is part of an evolution in the molecular diagnosis and understanding of AKI
bull These biomarkers are released by kidney cells along a path which may lead to AKI during a pre-injury phase
bull AKS is defined as the increased-risk phase (pre-injury phase) that leads to AKI
bull This ldquoAKSrdquo may or may not lead to damage and functional declinebull But it is the earliest possible the process of AKI can be detected
Pre-injury phase biomarkers
Stress biomarkersbull In 2013 Kashani et al reported the results of a prospective international
observational investigation (the Sapphire study) of tissue inhibitor of metalloproteinases- 2 (TIMP-2) and insulin-like growth factor-binding protein 7 (IGFBP7) in a heterogeneous group of critically ill patients [TIMP-2][IGFBP7] was significantly superior to all previously described markers of AKI (plt0002)
bull Next the Opal and Topaz study showed the cut-off value and risk assessment using the urinary[TIMP-2] [IGFBP7]
bull The urine [IGFBP7][TIMP2] biomarker is already FDA approved and commercially available in the United States
bull Falsepositive results are common and they will be magnified if the test is used inappropriately in low-risk patients In addition this biomarker should not be used in ambulatory practices and it is not beneficial in patients with established AKI
microRNAsbull microRNAs (miRNAs) are endogenous single-stranded non-coding
mRNAs of about 19-23 nucleotides bull In the past years researchers have begun to investigate the
relevance of miRNAs to AKI with many miRNAs being implicated bull Some of them contribute to pathogenesis by regulating apoptosis
and inflammation amplifying or reducing acute injury responses while others regulate fibrosis and angiogenesis participating in renal recovery or progression to fibrosis
bull Certain miRNAs have been investigated for their potential as novel biomarkers for the early detection or prognostication of AKI
Hemojuvelinbull Hemojuvelin (HJV) a glycophosphatidylinositol (GPI)- linked
membrane protein is highly expressed in liver and skeletal musclesbull The molecular weight of HJV is 42 kDa for the soluble form (sHJV)
and can be passed through glomerular filtration and reabsorbed by the renal tubules Increased iron content in the kidney and urine is observed in human and animal models of AKI and increased iron load can induce renal tubular cell injury
bull There is evidence that the increased expression of the hemojuvelin-hepcidin ferroportin pathway is an intrinsic response to iron overload conditions during AKI
bull Therefore urine HJV (uHJV) has the potential to be an early AKI biomarker in response to iron homeostasis during AKI
Combination of functional and damage biomarkers
bull While new biomarkers are being validated functional biomarkers (serum creatinine serum urea and urine output) continue to be utilized in the diagnosis and staging of AKI In the future existing or newer damage biomarkers will likely be combined with the use of functional biomarkers to enhance the ability of RIFLE AKIN
bull A study of 345 children after cardiopulmonary bypass surgery demonstrated that the composite of functional biomarker such as plasma cystatin C and urinary NGAL was superior to changes in serum creatinine to predict AKI
PROGNOSTIC BIOMARKERS
bull Most of the biomarkers described above allow early detection of acute kidney injury but do not predict severe AKI
Urinary renin and angiotensinogen
bull Urinary renin angiotensinogen and plasma NGAL may predict the development of severe AKI
bull Among 99 consecutively enrolled patients who developed AKI the ratio of urinary angiotensinogen to urinary creatinine (uAnCR expressed as ng per mg creatinine)calculated Patients with the highest uAnCR had a higher risk of worsening AKI compared with patients with the lowest uAnCR An elevated uAnCR predicted a longer hospital stay
bull Among 204 patients who developed Acute Kidney Injury Network (AKIN) stage 1 following cardiac surgery the urinary renin-to-creatinine ratio and the angiotensinogen-to-creatinine ratio predicted a composite outcome of death or AKIN stage 3 or death
Plasma NGAL
bull In a prospective cohort study in which 616 patients admitted from the emergency department were classified by clinical criteria as AKI transient azotemia stable CKD or normal kidney function plasma NGAL discriminated AKI from normal function and from transient azotemia
bull Higher concentrations of NGAL were associated with more severe AKI
Thanks for your attention
bull NGAL may also represent early sensitive biomarker of AKI after contrast administrations for coronary angiography
bull NGAL was measured in the serum and urine before and at 2 4 12 24 and 48 h after contrast administration they found a significant rise in serum NGAL 2 and 4 h after PCI and a rise in urinary NGAL 4 and 12 h after PCI
bull A similar study of 25 patients with normal serum creatinine undergoing PCI due to unstable angina There was a significant rise in serum NGAL after 2 and 4 hours Urinary NGAL and urinary L-FABP followed the same pattern Both markers increased significantly after 4 hours and remained elevated up to 48 hours after PCI
bull Urine and plasma NGAL levels also represent early biomarkers of AKI in ICU
bull A multicenter study of serum NGAL was performed in 143 critically ill children with systemic inflammatory response syndrome (SIRS) or septic shock during the first 24 h of admission to the ICU there was a significant difference in serum NGAL between healthy children ill children with SIRS and septic shock the study was concluded that serum NGAL is a highly sensitive but nonspecific predictor of acute kidney injury in critically ill children with septic shock
bull A 2010 study evaluated 88 ICU patient and found that an NGAL level of ge150 nmolL predicted AKI with 82 sensitivity and 97 specificity
bull A recent study had 98 patients who were divided in two groups depending on the presence of sepsis Fifty-six patients had sepsis while forty-two patients were nonseptic Among septic patients subjects who developed AKI showed signi1048853 cant higher levels of NGAL
bull A more study of 65 patients with septic shock were found that urine NGAL levels 12 hours before AKI diagnosis were a good predictor of AKI
Kidney Injury Molecule-1 (KIM-1)
bull KIM-1 mRNA and protein are expressed at a low level in normal kidney but are increased dramatically in postischemic kidney
bull KIM-1 has been identified as the first nonmyeloidphosphatidylserine receptor that confers a phagocytic phenotype on injured epithelial cells both in vivo and in vitro
bull Urinary KIM-1 has been found to be an early indicator of AKI that compares favorably to a number of conventional biomarkers and tubular enzymes
bull KIM-1 is also a tissue and urinary biomarker for nephrotoxicant-induced kidney injury
bull Tissue and urinary expressions were measured with different nephrotoxic doses of cisplatin folic acide cadmium gentamycin mercury
bull As early as 1 day after cisplatin treatment positive KIM- 1 immunostaining observed in the outer medulla of the kidney and changes in urinary clusterin indicated the onset of proximal tubular injury in the absence of functional effects
bull Tissue KIM-1 was the most sensitive biomarker for detection of cisplatin-induced kidney damage
bull KIM-1 is a biomarker of AKI in humans bull Urine samples were collected from 32 patients with various
acute and chronic kidney diseases as well as from eight normal controls there was extensive expression of KIM-1 in proximal tubule cells in kidney biopsies from six patients with biopsy confirmed acute tubular necrosis (ATN)
bull Urinary KIM-1 levels were significantly higher in patients with ischemic ATN compared to levels in patients with other forms of acute renal failure or chronic renal disease
bull Adjusted for age gender and length of time delay between the initial insult and sampling of the urine a one-unit increase in normalized KIM-1 was associated with a greater than 12-fold risk for the presence of ATN
bull In hospital patients with AKI urinary levels of KIM-1 that higher levels correlated with a higher odds ratio for dialysis requirement or hospital death
bull this study demonstrated that urinary biomarker of AKI such as KIM-1 can predict adverse clinical outcomes in patients with AKI
bull Both renal and urinary KIM-1 correlate with kidney damage and negatively with renal function but not with proteinuria
bull A recent study has explored urinary KIM-1correlated with kidney function in kidney allograft recipients Kidney transplant recipients showed significantly higher KIM-1 values than the healthy volunteers this study concluded that even a successful kidney transplantation is associated with kidney injury as reflected by elevated urinary KIM-1
bull A rapid direct 15-minute assay for the detection of urinary human KIM-1 has been developed Using this assay more urinary KIM-1 was detected in the urine of patients with AKI than in the urine from healthy volunteers
Urinary interleukin-18
bull Interleukin18 (IL-18) is a 22 kDa pro-inflammatory cytokine that increases in the kidney after ischemia-reperfusion injury in a caspase- 1-dependent manner
bull Patients with ATN had significantly greater urinary IL-18 concentrations than those with other conditions (healthy controls patients with pre-renal azotemia urinary tract infection CKD and nephrotic syndrome)
bull urinary IL-18 concentrations measured in the first 24 h after kidney transplantation were higher in patients who received a cadaveric kidney that developed delayed graft function compared to patients who received a cadaveric kidney with prompt graft function and patients who received a kidney with prompt graft function from a living donor
bull However the performance of urinary IL-18 measured 1 day before AKI was modest
bull Its predictive utility for AKI following cardiac surgery could not be demonstrated in one prospective observational study of 100 adult patients
bull In addition in a large study population of 1439 critically ill patients IL-18 had a poor-to-moderate ability to predict AKI renal replacement therapy (RRT) or 90-day mortality
Liver-Type Fatty Acid Binding Protein(L-FABP)
bull Liver-type fatty acid-binding protein (L-FABP) is a 14 kDa protein from the large super- family of lipidbinding proteins
bull The 14-kD L-FABP protein can be localized predominantly in the proximal tubule
bull Noiri et al demonstrated that increase of urinary L-FABP was observed at 1 h after ischemia even in the 5-min IRI group and urinary L-FABP was superior to BUN and urinary NAG for early and accurate detection of acute tubular necrosis in different models of animal AKI
bull urinary L-FABP may be a promising biomarker for early detection of AKI and prediction of dialysis requirement and in-hospital mortality
bull Urinary excretion of urinary liver-type fatty acid-binding protein (L-FABP) reflects stress of proximal tubular epithelial cells and correlates with severity of ischemic tubular injury
bull A meta-analysis of 15 prospective cohort studies demonstrated that in hospitalndashbased cohorts of patients at risk of AKI L-FABP can discriminate for the diagnosis of AKI and predict the need for dialysis and in-hospital mortality
bull It was correlated with the degree of tubulointerstitial damage in a folic acid induced nephropathy
bull In ischemic and cisplatin-induced AKI L-FABP was increased in the urine before the increase in BUN
bull In cisplatin-induced AKI urinary L-FABP levels increased exponentially even in the lowest dose group as early as 2 hours whereas BUN levels increased at 48 hours
bull L-FABP was measured in 80 critically ill patients Urinary L-FABP levels in patients with septic shock were significantly higher than severe sepsis without shock Serum L-FABP levels did not have significant differences between patients with septic shock severe sepsis and healthy
bull Another study was evaluated 145 septic shock patients complicated with established AKI Urinary L-FABP measured at admission was significantly higher in the nonsurvivors of septic shock with established acute kidney injury than in the survivors
Failure of the TRIBE-AKI study
bull The Translational Research Investigating Biomarker Endpoints in AKI (TRIBE-AKI) study evaluated the performance of urinary c-glutamyltranspeptidase ( c-GTP) alkaline phosphatase NGAL Cys-C KIM-1 and IL-18 in AKI diagnosis
bull The results of four novel urine biomarkers and one plasma biomarker (urine NGAL IL-18 KIM-1 and L-FABP and plasma NGAL) were provided Of all the novel biomarkers only urine IL-18 and plasma NGAL in adults were helpful in predicting progression of AKI when measured on the day of clinical AKI diagnosis
bull Combinations of three biomarkers in adults from two different time points and combinations of two biomarkers in children from two time points were found to be able to increase the ROC for AKI up to 078
bull In summary the clinical use of single damage biomarkers in AKI prediction remains unclear because large prospective multicenter trials such as the TRIBE-AKI study (nfrac141530) have failed to demonstrate troponin-like diagnostic performance
Various clinical scenarios of AKI based onfunction damage and stress
bull Over the last decade a number of novel damage biomarkers have been evaluated for their capacity to detect kidney damage and predict the development of AKI However the relationship between decreasing function and increasing damage is not as straightforward as might be assumed
bull The characteristic pattern whereby damage precedes loss of function (panel A) may be seen in some cases of AKI and affords an opportunity to detect ldquosubclinicalrdquo AKI before function start to fall Unfortunately other patterns might also occur For example functional decline may start to occur alongside damage (panel B) and in some cases function may start to decline even before damage (panel C)
bull This makes damage markers difficult to use for predicting AKI However other markers might actually measure the ldquostressrdquo occurring at the cellular level before damage or loss of function
Paradigm shift to pre-injury phase biomarkers
bull Katz et al proposed that the pre-injury phase that leads to AKI can be described as ldquoacute kidney stressrdquo (AKS) after the report of the identification of cell cycle arrest biomarkers that signal the potential development of AKI is part of an evolution in the molecular diagnosis and understanding of AKI
bull These biomarkers are released by kidney cells along a path which may lead to AKI during a pre-injury phase
bull AKS is defined as the increased-risk phase (pre-injury phase) that leads to AKI
bull This ldquoAKSrdquo may or may not lead to damage and functional declinebull But it is the earliest possible the process of AKI can be detected
Pre-injury phase biomarkers
Stress biomarkersbull In 2013 Kashani et al reported the results of a prospective international
observational investigation (the Sapphire study) of tissue inhibitor of metalloproteinases- 2 (TIMP-2) and insulin-like growth factor-binding protein 7 (IGFBP7) in a heterogeneous group of critically ill patients [TIMP-2][IGFBP7] was significantly superior to all previously described markers of AKI (plt0002)
bull Next the Opal and Topaz study showed the cut-off value and risk assessment using the urinary[TIMP-2] [IGFBP7]
bull The urine [IGFBP7][TIMP2] biomarker is already FDA approved and commercially available in the United States
bull Falsepositive results are common and they will be magnified if the test is used inappropriately in low-risk patients In addition this biomarker should not be used in ambulatory practices and it is not beneficial in patients with established AKI
microRNAsbull microRNAs (miRNAs) are endogenous single-stranded non-coding
mRNAs of about 19-23 nucleotides bull In the past years researchers have begun to investigate the
relevance of miRNAs to AKI with many miRNAs being implicated bull Some of them contribute to pathogenesis by regulating apoptosis
and inflammation amplifying or reducing acute injury responses while others regulate fibrosis and angiogenesis participating in renal recovery or progression to fibrosis
bull Certain miRNAs have been investigated for their potential as novel biomarkers for the early detection or prognostication of AKI
Hemojuvelinbull Hemojuvelin (HJV) a glycophosphatidylinositol (GPI)- linked
membrane protein is highly expressed in liver and skeletal musclesbull The molecular weight of HJV is 42 kDa for the soluble form (sHJV)
and can be passed through glomerular filtration and reabsorbed by the renal tubules Increased iron content in the kidney and urine is observed in human and animal models of AKI and increased iron load can induce renal tubular cell injury
bull There is evidence that the increased expression of the hemojuvelin-hepcidin ferroportin pathway is an intrinsic response to iron overload conditions during AKI
bull Therefore urine HJV (uHJV) has the potential to be an early AKI biomarker in response to iron homeostasis during AKI
Combination of functional and damage biomarkers
bull While new biomarkers are being validated functional biomarkers (serum creatinine serum urea and urine output) continue to be utilized in the diagnosis and staging of AKI In the future existing or newer damage biomarkers will likely be combined with the use of functional biomarkers to enhance the ability of RIFLE AKIN
bull A study of 345 children after cardiopulmonary bypass surgery demonstrated that the composite of functional biomarker such as plasma cystatin C and urinary NGAL was superior to changes in serum creatinine to predict AKI
PROGNOSTIC BIOMARKERS
bull Most of the biomarkers described above allow early detection of acute kidney injury but do not predict severe AKI
Urinary renin and angiotensinogen
bull Urinary renin angiotensinogen and plasma NGAL may predict the development of severe AKI
bull Among 99 consecutively enrolled patients who developed AKI the ratio of urinary angiotensinogen to urinary creatinine (uAnCR expressed as ng per mg creatinine)calculated Patients with the highest uAnCR had a higher risk of worsening AKI compared with patients with the lowest uAnCR An elevated uAnCR predicted a longer hospital stay
bull Among 204 patients who developed Acute Kidney Injury Network (AKIN) stage 1 following cardiac surgery the urinary renin-to-creatinine ratio and the angiotensinogen-to-creatinine ratio predicted a composite outcome of death or AKIN stage 3 or death
Plasma NGAL
bull In a prospective cohort study in which 616 patients admitted from the emergency department were classified by clinical criteria as AKI transient azotemia stable CKD or normal kidney function plasma NGAL discriminated AKI from normal function and from transient azotemia
bull Higher concentrations of NGAL were associated with more severe AKI
Thanks for your attention

bull Urine and plasma NGAL levels also represent early biomarkers of AKI in ICU
bull A multicenter study of serum NGAL was performed in 143 critically ill children with systemic inflammatory response syndrome (SIRS) or septic shock during the first 24 h of admission to the ICU there was a significant difference in serum NGAL between healthy children ill children with SIRS and septic shock the study was concluded that serum NGAL is a highly sensitive but nonspecific predictor of acute kidney injury in critically ill children with septic shock
bull A 2010 study evaluated 88 ICU patient and found that an NGAL level of ge150 nmolL predicted AKI with 82 sensitivity and 97 specificity
bull A recent study had 98 patients who were divided in two groups depending on the presence of sepsis Fifty-six patients had sepsis while forty-two patients were nonseptic Among septic patients subjects who developed AKI showed signi1048853 cant higher levels of NGAL
bull A more study of 65 patients with septic shock were found that urine NGAL levels 12 hours before AKI diagnosis were a good predictor of AKI
Kidney Injury Molecule-1 (KIM-1)
bull KIM-1 mRNA and protein are expressed at a low level in normal kidney but are increased dramatically in postischemic kidney
bull KIM-1 has been identified as the first nonmyeloidphosphatidylserine receptor that confers a phagocytic phenotype on injured epithelial cells both in vivo and in vitro
bull Urinary KIM-1 has been found to be an early indicator of AKI that compares favorably to a number of conventional biomarkers and tubular enzymes
bull KIM-1 is also a tissue and urinary biomarker for nephrotoxicant-induced kidney injury
bull Tissue and urinary expressions were measured with different nephrotoxic doses of cisplatin folic acide cadmium gentamycin mercury
bull As early as 1 day after cisplatin treatment positive KIM- 1 immunostaining observed in the outer medulla of the kidney and changes in urinary clusterin indicated the onset of proximal tubular injury in the absence of functional effects
bull Tissue KIM-1 was the most sensitive biomarker for detection of cisplatin-induced kidney damage
bull KIM-1 is a biomarker of AKI in humans bull Urine samples were collected from 32 patients with various
acute and chronic kidney diseases as well as from eight normal controls there was extensive expression of KIM-1 in proximal tubule cells in kidney biopsies from six patients with biopsy confirmed acute tubular necrosis (ATN)
bull Urinary KIM-1 levels were significantly higher in patients with ischemic ATN compared to levels in patients with other forms of acute renal failure or chronic renal disease
bull Adjusted for age gender and length of time delay between the initial insult and sampling of the urine a one-unit increase in normalized KIM-1 was associated with a greater than 12-fold risk for the presence of ATN
bull In hospital patients with AKI urinary levels of KIM-1 that higher levels correlated with a higher odds ratio for dialysis requirement or hospital death
bull this study demonstrated that urinary biomarker of AKI such as KIM-1 can predict adverse clinical outcomes in patients with AKI
bull Both renal and urinary KIM-1 correlate with kidney damage and negatively with renal function but not with proteinuria
bull A recent study has explored urinary KIM-1correlated with kidney function in kidney allograft recipients Kidney transplant recipients showed significantly higher KIM-1 values than the healthy volunteers this study concluded that even a successful kidney transplantation is associated with kidney injury as reflected by elevated urinary KIM-1
bull A rapid direct 15-minute assay for the detection of urinary human KIM-1 has been developed Using this assay more urinary KIM-1 was detected in the urine of patients with AKI than in the urine from healthy volunteers
Urinary interleukin-18
bull Interleukin18 (IL-18) is a 22 kDa pro-inflammatory cytokine that increases in the kidney after ischemia-reperfusion injury in a caspase- 1-dependent manner
bull Patients with ATN had significantly greater urinary IL-18 concentrations than those with other conditions (healthy controls patients with pre-renal azotemia urinary tract infection CKD and nephrotic syndrome)
bull urinary IL-18 concentrations measured in the first 24 h after kidney transplantation were higher in patients who received a cadaveric kidney that developed delayed graft function compared to patients who received a cadaveric kidney with prompt graft function and patients who received a kidney with prompt graft function from a living donor
bull However the performance of urinary IL-18 measured 1 day before AKI was modest
bull Its predictive utility for AKI following cardiac surgery could not be demonstrated in one prospective observational study of 100 adult patients
bull In addition in a large study population of 1439 critically ill patients IL-18 had a poor-to-moderate ability to predict AKI renal replacement therapy (RRT) or 90-day mortality
Liver-Type Fatty Acid Binding Protein(L-FABP)
bull Liver-type fatty acid-binding protein (L-FABP) is a 14 kDa protein from the large super- family of lipidbinding proteins
bull The 14-kD L-FABP protein can be localized predominantly in the proximal tubule
bull Noiri et al demonstrated that increase of urinary L-FABP was observed at 1 h after ischemia even in the 5-min IRI group and urinary L-FABP was superior to BUN and urinary NAG for early and accurate detection of acute tubular necrosis in different models of animal AKI
bull urinary L-FABP may be a promising biomarker for early detection of AKI and prediction of dialysis requirement and in-hospital mortality
bull Urinary excretion of urinary liver-type fatty acid-binding protein (L-FABP) reflects stress of proximal tubular epithelial cells and correlates with severity of ischemic tubular injury
bull A meta-analysis of 15 prospective cohort studies demonstrated that in hospitalndashbased cohorts of patients at risk of AKI L-FABP can discriminate for the diagnosis of AKI and predict the need for dialysis and in-hospital mortality
bull It was correlated with the degree of tubulointerstitial damage in a folic acid induced nephropathy
bull In ischemic and cisplatin-induced AKI L-FABP was increased in the urine before the increase in BUN
bull In cisplatin-induced AKI urinary L-FABP levels increased exponentially even in the lowest dose group as early as 2 hours whereas BUN levels increased at 48 hours
bull L-FABP was measured in 80 critically ill patients Urinary L-FABP levels in patients with septic shock were significantly higher than severe sepsis without shock Serum L-FABP levels did not have significant differences between patients with septic shock severe sepsis and healthy
bull Another study was evaluated 145 septic shock patients complicated with established AKI Urinary L-FABP measured at admission was significantly higher in the nonsurvivors of septic shock with established acute kidney injury than in the survivors
Failure of the TRIBE-AKI study
bull The Translational Research Investigating Biomarker Endpoints in AKI (TRIBE-AKI) study evaluated the performance of urinary c-glutamyltranspeptidase ( c-GTP) alkaline phosphatase NGAL Cys-C KIM-1 and IL-18 in AKI diagnosis
bull The results of four novel urine biomarkers and one plasma biomarker (urine NGAL IL-18 KIM-1 and L-FABP and plasma NGAL) were provided Of all the novel biomarkers only urine IL-18 and plasma NGAL in adults were helpful in predicting progression of AKI when measured on the day of clinical AKI diagnosis
bull Combinations of three biomarkers in adults from two different time points and combinations of two biomarkers in children from two time points were found to be able to increase the ROC for AKI up to 078
bull In summary the clinical use of single damage biomarkers in AKI prediction remains unclear because large prospective multicenter trials such as the TRIBE-AKI study (nfrac141530) have failed to demonstrate troponin-like diagnostic performance
Various clinical scenarios of AKI based onfunction damage and stress
bull Over the last decade a number of novel damage biomarkers have been evaluated for their capacity to detect kidney damage and predict the development of AKI However the relationship between decreasing function and increasing damage is not as straightforward as might be assumed
bull The characteristic pattern whereby damage precedes loss of function (panel A) may be seen in some cases of AKI and affords an opportunity to detect ldquosubclinicalrdquo AKI before function start to fall Unfortunately other patterns might also occur For example functional decline may start to occur alongside damage (panel B) and in some cases function may start to decline even before damage (panel C)
bull This makes damage markers difficult to use for predicting AKI However other markers might actually measure the ldquostressrdquo occurring at the cellular level before damage or loss of function
Paradigm shift to pre-injury phase biomarkers
bull Katz et al proposed that the pre-injury phase that leads to AKI can be described as ldquoacute kidney stressrdquo (AKS) after the report of the identification of cell cycle arrest biomarkers that signal the potential development of AKI is part of an evolution in the molecular diagnosis and understanding of AKI
bull These biomarkers are released by kidney cells along a path which may lead to AKI during a pre-injury phase
bull AKS is defined as the increased-risk phase (pre-injury phase) that leads to AKI
bull This ldquoAKSrdquo may or may not lead to damage and functional declinebull But it is the earliest possible the process of AKI can be detected
Pre-injury phase biomarkers
Stress biomarkersbull In 2013 Kashani et al reported the results of a prospective international
observational investigation (the Sapphire study) of tissue inhibitor of metalloproteinases- 2 (TIMP-2) and insulin-like growth factor-binding protein 7 (IGFBP7) in a heterogeneous group of critically ill patients [TIMP-2][IGFBP7] was significantly superior to all previously described markers of AKI (plt0002)
bull Next the Opal and Topaz study showed the cut-off value and risk assessment using the urinary[TIMP-2] [IGFBP7]
bull The urine [IGFBP7][TIMP2] biomarker is already FDA approved and commercially available in the United States
bull Falsepositive results are common and they will be magnified if the test is used inappropriately in low-risk patients In addition this biomarker should not be used in ambulatory practices and it is not beneficial in patients with established AKI
microRNAsbull microRNAs (miRNAs) are endogenous single-stranded non-coding
mRNAs of about 19-23 nucleotides bull In the past years researchers have begun to investigate the
relevance of miRNAs to AKI with many miRNAs being implicated bull Some of them contribute to pathogenesis by regulating apoptosis
and inflammation amplifying or reducing acute injury responses while others regulate fibrosis and angiogenesis participating in renal recovery or progression to fibrosis
bull Certain miRNAs have been investigated for their potential as novel biomarkers for the early detection or prognostication of AKI
Hemojuvelinbull Hemojuvelin (HJV) a glycophosphatidylinositol (GPI)- linked
membrane protein is highly expressed in liver and skeletal musclesbull The molecular weight of HJV is 42 kDa for the soluble form (sHJV)
and can be passed through glomerular filtration and reabsorbed by the renal tubules Increased iron content in the kidney and urine is observed in human and animal models of AKI and increased iron load can induce renal tubular cell injury
bull There is evidence that the increased expression of the hemojuvelin-hepcidin ferroportin pathway is an intrinsic response to iron overload conditions during AKI
bull Therefore urine HJV (uHJV) has the potential to be an early AKI biomarker in response to iron homeostasis during AKI
Combination of functional and damage biomarkers
bull While new biomarkers are being validated functional biomarkers (serum creatinine serum urea and urine output) continue to be utilized in the diagnosis and staging of AKI In the future existing or newer damage biomarkers will likely be combined with the use of functional biomarkers to enhance the ability of RIFLE AKIN
bull A study of 345 children after cardiopulmonary bypass surgery demonstrated that the composite of functional biomarker such as plasma cystatin C and urinary NGAL was superior to changes in serum creatinine to predict AKI
PROGNOSTIC BIOMARKERS
bull Most of the biomarkers described above allow early detection of acute kidney injury but do not predict severe AKI
Urinary renin and angiotensinogen
bull Urinary renin angiotensinogen and plasma NGAL may predict the development of severe AKI
bull Among 99 consecutively enrolled patients who developed AKI the ratio of urinary angiotensinogen to urinary creatinine (uAnCR expressed as ng per mg creatinine)calculated Patients with the highest uAnCR had a higher risk of worsening AKI compared with patients with the lowest uAnCR An elevated uAnCR predicted a longer hospital stay
bull Among 204 patients who developed Acute Kidney Injury Network (AKIN) stage 1 following cardiac surgery the urinary renin-to-creatinine ratio and the angiotensinogen-to-creatinine ratio predicted a composite outcome of death or AKIN stage 3 or death
Plasma NGAL
bull In a prospective cohort study in which 616 patients admitted from the emergency department were classified by clinical criteria as AKI transient azotemia stable CKD or normal kidney function plasma NGAL discriminated AKI from normal function and from transient azotemia
bull Higher concentrations of NGAL were associated with more severe AKI
Thanks for your attention

Kidney Injury Molecule-1 (KIM-1)
bull KIM-1 mRNA and protein are expressed at a low level in normal kidney but are increased dramatically in postischemic kidney
bull KIM-1 has been identified as the first nonmyeloidphosphatidylserine receptor that confers a phagocytic phenotype on injured epithelial cells both in vivo and in vitro
bull Urinary KIM-1 has been found to be an early indicator of AKI that compares favorably to a number of conventional biomarkers and tubular enzymes
bull KIM-1 is also a tissue and urinary biomarker for nephrotoxicant-induced kidney injury
bull Tissue and urinary expressions were measured with different nephrotoxic doses of cisplatin folic acide cadmium gentamycin mercury
bull As early as 1 day after cisplatin treatment positive KIM- 1 immunostaining observed in the outer medulla of the kidney and changes in urinary clusterin indicated the onset of proximal tubular injury in the absence of functional effects
bull Tissue KIM-1 was the most sensitive biomarker for detection of cisplatin-induced kidney damage
bull KIM-1 is a biomarker of AKI in humans bull Urine samples were collected from 32 patients with various
acute and chronic kidney diseases as well as from eight normal controls there was extensive expression of KIM-1 in proximal tubule cells in kidney biopsies from six patients with biopsy confirmed acute tubular necrosis (ATN)
bull Urinary KIM-1 levels were significantly higher in patients with ischemic ATN compared to levels in patients with other forms of acute renal failure or chronic renal disease
bull Adjusted for age gender and length of time delay between the initial insult and sampling of the urine a one-unit increase in normalized KIM-1 was associated with a greater than 12-fold risk for the presence of ATN
bull In hospital patients with AKI urinary levels of KIM-1 that higher levels correlated with a higher odds ratio for dialysis requirement or hospital death
bull this study demonstrated that urinary biomarker of AKI such as KIM-1 can predict adverse clinical outcomes in patients with AKI
bull Both renal and urinary KIM-1 correlate with kidney damage and negatively with renal function but not with proteinuria
bull A recent study has explored urinary KIM-1correlated with kidney function in kidney allograft recipients Kidney transplant recipients showed significantly higher KIM-1 values than the healthy volunteers this study concluded that even a successful kidney transplantation is associated with kidney injury as reflected by elevated urinary KIM-1
bull A rapid direct 15-minute assay for the detection of urinary human KIM-1 has been developed Using this assay more urinary KIM-1 was detected in the urine of patients with AKI than in the urine from healthy volunteers
Urinary interleukin-18
bull Interleukin18 (IL-18) is a 22 kDa pro-inflammatory cytokine that increases in the kidney after ischemia-reperfusion injury in a caspase- 1-dependent manner
bull Patients with ATN had significantly greater urinary IL-18 concentrations than those with other conditions (healthy controls patients with pre-renal azotemia urinary tract infection CKD and nephrotic syndrome)
bull urinary IL-18 concentrations measured in the first 24 h after kidney transplantation were higher in patients who received a cadaveric kidney that developed delayed graft function compared to patients who received a cadaveric kidney with prompt graft function and patients who received a kidney with prompt graft function from a living donor
bull However the performance of urinary IL-18 measured 1 day before AKI was modest
bull Its predictive utility for AKI following cardiac surgery could not be demonstrated in one prospective observational study of 100 adult patients
bull In addition in a large study population of 1439 critically ill patients IL-18 had a poor-to-moderate ability to predict AKI renal replacement therapy (RRT) or 90-day mortality
Liver-Type Fatty Acid Binding Protein(L-FABP)
bull Liver-type fatty acid-binding protein (L-FABP) is a 14 kDa protein from the large super- family of lipidbinding proteins
bull The 14-kD L-FABP protein can be localized predominantly in the proximal tubule
bull Noiri et al demonstrated that increase of urinary L-FABP was observed at 1 h after ischemia even in the 5-min IRI group and urinary L-FABP was superior to BUN and urinary NAG for early and accurate detection of acute tubular necrosis in different models of animal AKI
bull urinary L-FABP may be a promising biomarker for early detection of AKI and prediction of dialysis requirement and in-hospital mortality
bull Urinary excretion of urinary liver-type fatty acid-binding protein (L-FABP) reflects stress of proximal tubular epithelial cells and correlates with severity of ischemic tubular injury
bull A meta-analysis of 15 prospective cohort studies demonstrated that in hospitalndashbased cohorts of patients at risk of AKI L-FABP can discriminate for the diagnosis of AKI and predict the need for dialysis and in-hospital mortality
bull It was correlated with the degree of tubulointerstitial damage in a folic acid induced nephropathy
bull In ischemic and cisplatin-induced AKI L-FABP was increased in the urine before the increase in BUN
bull In cisplatin-induced AKI urinary L-FABP levels increased exponentially even in the lowest dose group as early as 2 hours whereas BUN levels increased at 48 hours
bull L-FABP was measured in 80 critically ill patients Urinary L-FABP levels in patients with septic shock were significantly higher than severe sepsis without shock Serum L-FABP levels did not have significant differences between patients with septic shock severe sepsis and healthy
bull Another study was evaluated 145 septic shock patients complicated with established AKI Urinary L-FABP measured at admission was significantly higher in the nonsurvivors of septic shock with established acute kidney injury than in the survivors
Failure of the TRIBE-AKI study
bull The Translational Research Investigating Biomarker Endpoints in AKI (TRIBE-AKI) study evaluated the performance of urinary c-glutamyltranspeptidase ( c-GTP) alkaline phosphatase NGAL Cys-C KIM-1 and IL-18 in AKI diagnosis
bull The results of four novel urine biomarkers and one plasma biomarker (urine NGAL IL-18 KIM-1 and L-FABP and plasma NGAL) were provided Of all the novel biomarkers only urine IL-18 and plasma NGAL in adults were helpful in predicting progression of AKI when measured on the day of clinical AKI diagnosis
bull Combinations of three biomarkers in adults from two different time points and combinations of two biomarkers in children from two time points were found to be able to increase the ROC for AKI up to 078
bull In summary the clinical use of single damage biomarkers in AKI prediction remains unclear because large prospective multicenter trials such as the TRIBE-AKI study (nfrac141530) have failed to demonstrate troponin-like diagnostic performance
Various clinical scenarios of AKI based onfunction damage and stress
bull Over the last decade a number of novel damage biomarkers have been evaluated for their capacity to detect kidney damage and predict the development of AKI However the relationship between decreasing function and increasing damage is not as straightforward as might be assumed
bull The characteristic pattern whereby damage precedes loss of function (panel A) may be seen in some cases of AKI and affords an opportunity to detect ldquosubclinicalrdquo AKI before function start to fall Unfortunately other patterns might also occur For example functional decline may start to occur alongside damage (panel B) and in some cases function may start to decline even before damage (panel C)
bull This makes damage markers difficult to use for predicting AKI However other markers might actually measure the ldquostressrdquo occurring at the cellular level before damage or loss of function
Paradigm shift to pre-injury phase biomarkers
bull Katz et al proposed that the pre-injury phase that leads to AKI can be described as ldquoacute kidney stressrdquo (AKS) after the report of the identification of cell cycle arrest biomarkers that signal the potential development of AKI is part of an evolution in the molecular diagnosis and understanding of AKI
bull These biomarkers are released by kidney cells along a path which may lead to AKI during a pre-injury phase
bull AKS is defined as the increased-risk phase (pre-injury phase) that leads to AKI
bull This ldquoAKSrdquo may or may not lead to damage and functional declinebull But it is the earliest possible the process of AKI can be detected
Pre-injury phase biomarkers
Stress biomarkersbull In 2013 Kashani et al reported the results of a prospective international
observational investigation (the Sapphire study) of tissue inhibitor of metalloproteinases- 2 (TIMP-2) and insulin-like growth factor-binding protein 7 (IGFBP7) in a heterogeneous group of critically ill patients [TIMP-2][IGFBP7] was significantly superior to all previously described markers of AKI (plt0002)
bull Next the Opal and Topaz study showed the cut-off value and risk assessment using the urinary[TIMP-2] [IGFBP7]
bull The urine [IGFBP7][TIMP2] biomarker is already FDA approved and commercially available in the United States
bull Falsepositive results are common and they will be magnified if the test is used inappropriately in low-risk patients In addition this biomarker should not be used in ambulatory practices and it is not beneficial in patients with established AKI
microRNAsbull microRNAs (miRNAs) are endogenous single-stranded non-coding
mRNAs of about 19-23 nucleotides bull In the past years researchers have begun to investigate the
relevance of miRNAs to AKI with many miRNAs being implicated bull Some of them contribute to pathogenesis by regulating apoptosis
and inflammation amplifying or reducing acute injury responses while others regulate fibrosis and angiogenesis participating in renal recovery or progression to fibrosis
bull Certain miRNAs have been investigated for their potential as novel biomarkers for the early detection or prognostication of AKI
Hemojuvelinbull Hemojuvelin (HJV) a glycophosphatidylinositol (GPI)- linked
membrane protein is highly expressed in liver and skeletal musclesbull The molecular weight of HJV is 42 kDa for the soluble form (sHJV)
and can be passed through glomerular filtration and reabsorbed by the renal tubules Increased iron content in the kidney and urine is observed in human and animal models of AKI and increased iron load can induce renal tubular cell injury
bull There is evidence that the increased expression of the hemojuvelin-hepcidin ferroportin pathway is an intrinsic response to iron overload conditions during AKI
bull Therefore urine HJV (uHJV) has the potential to be an early AKI biomarker in response to iron homeostasis during AKI
Combination of functional and damage biomarkers
bull While new biomarkers are being validated functional biomarkers (serum creatinine serum urea and urine output) continue to be utilized in the diagnosis and staging of AKI In the future existing or newer damage biomarkers will likely be combined with the use of functional biomarkers to enhance the ability of RIFLE AKIN
bull A study of 345 children after cardiopulmonary bypass surgery demonstrated that the composite of functional biomarker such as plasma cystatin C and urinary NGAL was superior to changes in serum creatinine to predict AKI
PROGNOSTIC BIOMARKERS
bull Most of the biomarkers described above allow early detection of acute kidney injury but do not predict severe AKI
Urinary renin and angiotensinogen
bull Urinary renin angiotensinogen and plasma NGAL may predict the development of severe AKI
bull Among 99 consecutively enrolled patients who developed AKI the ratio of urinary angiotensinogen to urinary creatinine (uAnCR expressed as ng per mg creatinine)calculated Patients with the highest uAnCR had a higher risk of worsening AKI compared with patients with the lowest uAnCR An elevated uAnCR predicted a longer hospital stay
bull Among 204 patients who developed Acute Kidney Injury Network (AKIN) stage 1 following cardiac surgery the urinary renin-to-creatinine ratio and the angiotensinogen-to-creatinine ratio predicted a composite outcome of death or AKIN stage 3 or death
Plasma NGAL
bull In a prospective cohort study in which 616 patients admitted from the emergency department were classified by clinical criteria as AKI transient azotemia stable CKD or normal kidney function plasma NGAL discriminated AKI from normal function and from transient azotemia
bull Higher concentrations of NGAL were associated with more severe AKI
Thanks for your attention

bull KIM-1 is also a tissue and urinary biomarker for nephrotoxicant-induced kidney injury
bull Tissue and urinary expressions were measured with different nephrotoxic doses of cisplatin folic acide cadmium gentamycin mercury
bull As early as 1 day after cisplatin treatment positive KIM- 1 immunostaining observed in the outer medulla of the kidney and changes in urinary clusterin indicated the onset of proximal tubular injury in the absence of functional effects
bull Tissue KIM-1 was the most sensitive biomarker for detection of cisplatin-induced kidney damage
bull KIM-1 is a biomarker of AKI in humans bull Urine samples were collected from 32 patients with various
acute and chronic kidney diseases as well as from eight normal controls there was extensive expression of KIM-1 in proximal tubule cells in kidney biopsies from six patients with biopsy confirmed acute tubular necrosis (ATN)
bull Urinary KIM-1 levels were significantly higher in patients with ischemic ATN compared to levels in patients with other forms of acute renal failure or chronic renal disease
bull Adjusted for age gender and length of time delay between the initial insult and sampling of the urine a one-unit increase in normalized KIM-1 was associated with a greater than 12-fold risk for the presence of ATN
bull In hospital patients with AKI urinary levels of KIM-1 that higher levels correlated with a higher odds ratio for dialysis requirement or hospital death
bull this study demonstrated that urinary biomarker of AKI such as KIM-1 can predict adverse clinical outcomes in patients with AKI
bull Both renal and urinary KIM-1 correlate with kidney damage and negatively with renal function but not with proteinuria
bull A recent study has explored urinary KIM-1correlated with kidney function in kidney allograft recipients Kidney transplant recipients showed significantly higher KIM-1 values than the healthy volunteers this study concluded that even a successful kidney transplantation is associated with kidney injury as reflected by elevated urinary KIM-1
bull A rapid direct 15-minute assay for the detection of urinary human KIM-1 has been developed Using this assay more urinary KIM-1 was detected in the urine of patients with AKI than in the urine from healthy volunteers
Urinary interleukin-18
bull Interleukin18 (IL-18) is a 22 kDa pro-inflammatory cytokine that increases in the kidney after ischemia-reperfusion injury in a caspase- 1-dependent manner
bull Patients with ATN had significantly greater urinary IL-18 concentrations than those with other conditions (healthy controls patients with pre-renal azotemia urinary tract infection CKD and nephrotic syndrome)
bull urinary IL-18 concentrations measured in the first 24 h after kidney transplantation were higher in patients who received a cadaveric kidney that developed delayed graft function compared to patients who received a cadaveric kidney with prompt graft function and patients who received a kidney with prompt graft function from a living donor
bull However the performance of urinary IL-18 measured 1 day before AKI was modest
bull Its predictive utility for AKI following cardiac surgery could not be demonstrated in one prospective observational study of 100 adult patients
bull In addition in a large study population of 1439 critically ill patients IL-18 had a poor-to-moderate ability to predict AKI renal replacement therapy (RRT) or 90-day mortality
Liver-Type Fatty Acid Binding Protein(L-FABP)
bull Liver-type fatty acid-binding protein (L-FABP) is a 14 kDa protein from the large super- family of lipidbinding proteins
bull The 14-kD L-FABP protein can be localized predominantly in the proximal tubule
bull Noiri et al demonstrated that increase of urinary L-FABP was observed at 1 h after ischemia even in the 5-min IRI group and urinary L-FABP was superior to BUN and urinary NAG for early and accurate detection of acute tubular necrosis in different models of animal AKI
bull urinary L-FABP may be a promising biomarker for early detection of AKI and prediction of dialysis requirement and in-hospital mortality
bull Urinary excretion of urinary liver-type fatty acid-binding protein (L-FABP) reflects stress of proximal tubular epithelial cells and correlates with severity of ischemic tubular injury
bull A meta-analysis of 15 prospective cohort studies demonstrated that in hospitalndashbased cohorts of patients at risk of AKI L-FABP can discriminate for the diagnosis of AKI and predict the need for dialysis and in-hospital mortality
bull It was correlated with the degree of tubulointerstitial damage in a folic acid induced nephropathy
bull In ischemic and cisplatin-induced AKI L-FABP was increased in the urine before the increase in BUN
bull In cisplatin-induced AKI urinary L-FABP levels increased exponentially even in the lowest dose group as early as 2 hours whereas BUN levels increased at 48 hours
bull L-FABP was measured in 80 critically ill patients Urinary L-FABP levels in patients with septic shock were significantly higher than severe sepsis without shock Serum L-FABP levels did not have significant differences between patients with septic shock severe sepsis and healthy
bull Another study was evaluated 145 septic shock patients complicated with established AKI Urinary L-FABP measured at admission was significantly higher in the nonsurvivors of septic shock with established acute kidney injury than in the survivors
Failure of the TRIBE-AKI study
bull The Translational Research Investigating Biomarker Endpoints in AKI (TRIBE-AKI) study evaluated the performance of urinary c-glutamyltranspeptidase ( c-GTP) alkaline phosphatase NGAL Cys-C KIM-1 and IL-18 in AKI diagnosis
bull The results of four novel urine biomarkers and one plasma biomarker (urine NGAL IL-18 KIM-1 and L-FABP and plasma NGAL) were provided Of all the novel biomarkers only urine IL-18 and plasma NGAL in adults were helpful in predicting progression of AKI when measured on the day of clinical AKI diagnosis
bull Combinations of three biomarkers in adults from two different time points and combinations of two biomarkers in children from two time points were found to be able to increase the ROC for AKI up to 078
bull In summary the clinical use of single damage biomarkers in AKI prediction remains unclear because large prospective multicenter trials such as the TRIBE-AKI study (nfrac141530) have failed to demonstrate troponin-like diagnostic performance
Various clinical scenarios of AKI based onfunction damage and stress
bull Over the last decade a number of novel damage biomarkers have been evaluated for their capacity to detect kidney damage and predict the development of AKI However the relationship between decreasing function and increasing damage is not as straightforward as might be assumed
bull The characteristic pattern whereby damage precedes loss of function (panel A) may be seen in some cases of AKI and affords an opportunity to detect ldquosubclinicalrdquo AKI before function start to fall Unfortunately other patterns might also occur For example functional decline may start to occur alongside damage (panel B) and in some cases function may start to decline even before damage (panel C)
bull This makes damage markers difficult to use for predicting AKI However other markers might actually measure the ldquostressrdquo occurring at the cellular level before damage or loss of function
Paradigm shift to pre-injury phase biomarkers
bull Katz et al proposed that the pre-injury phase that leads to AKI can be described as ldquoacute kidney stressrdquo (AKS) after the report of the identification of cell cycle arrest biomarkers that signal the potential development of AKI is part of an evolution in the molecular diagnosis and understanding of AKI
bull These biomarkers are released by kidney cells along a path which may lead to AKI during a pre-injury phase
bull AKS is defined as the increased-risk phase (pre-injury phase) that leads to AKI
bull This ldquoAKSrdquo may or may not lead to damage and functional declinebull But it is the earliest possible the process of AKI can be detected
Pre-injury phase biomarkers
Stress biomarkersbull In 2013 Kashani et al reported the results of a prospective international
observational investigation (the Sapphire study) of tissue inhibitor of metalloproteinases- 2 (TIMP-2) and insulin-like growth factor-binding protein 7 (IGFBP7) in a heterogeneous group of critically ill patients [TIMP-2][IGFBP7] was significantly superior to all previously described markers of AKI (plt0002)
bull Next the Opal and Topaz study showed the cut-off value and risk assessment using the urinary[TIMP-2] [IGFBP7]
bull The urine [IGFBP7][TIMP2] biomarker is already FDA approved and commercially available in the United States
bull Falsepositive results are common and they will be magnified if the test is used inappropriately in low-risk patients In addition this biomarker should not be used in ambulatory practices and it is not beneficial in patients with established AKI
microRNAsbull microRNAs (miRNAs) are endogenous single-stranded non-coding
mRNAs of about 19-23 nucleotides bull In the past years researchers have begun to investigate the
relevance of miRNAs to AKI with many miRNAs being implicated bull Some of them contribute to pathogenesis by regulating apoptosis
and inflammation amplifying or reducing acute injury responses while others regulate fibrosis and angiogenesis participating in renal recovery or progression to fibrosis
bull Certain miRNAs have been investigated for their potential as novel biomarkers for the early detection or prognostication of AKI
Hemojuvelinbull Hemojuvelin (HJV) a glycophosphatidylinositol (GPI)- linked
membrane protein is highly expressed in liver and skeletal musclesbull The molecular weight of HJV is 42 kDa for the soluble form (sHJV)
and can be passed through glomerular filtration and reabsorbed by the renal tubules Increased iron content in the kidney and urine is observed in human and animal models of AKI and increased iron load can induce renal tubular cell injury
bull There is evidence that the increased expression of the hemojuvelin-hepcidin ferroportin pathway is an intrinsic response to iron overload conditions during AKI
bull Therefore urine HJV (uHJV) has the potential to be an early AKI biomarker in response to iron homeostasis during AKI
Combination of functional and damage biomarkers
bull While new biomarkers are being validated functional biomarkers (serum creatinine serum urea and urine output) continue to be utilized in the diagnosis and staging of AKI In the future existing or newer damage biomarkers will likely be combined with the use of functional biomarkers to enhance the ability of RIFLE AKIN
bull A study of 345 children after cardiopulmonary bypass surgery demonstrated that the composite of functional biomarker such as plasma cystatin C and urinary NGAL was superior to changes in serum creatinine to predict AKI
PROGNOSTIC BIOMARKERS
bull Most of the biomarkers described above allow early detection of acute kidney injury but do not predict severe AKI
Urinary renin and angiotensinogen
bull Urinary renin angiotensinogen and plasma NGAL may predict the development of severe AKI
bull Among 99 consecutively enrolled patients who developed AKI the ratio of urinary angiotensinogen to urinary creatinine (uAnCR expressed as ng per mg creatinine)calculated Patients with the highest uAnCR had a higher risk of worsening AKI compared with patients with the lowest uAnCR An elevated uAnCR predicted a longer hospital stay
bull Among 204 patients who developed Acute Kidney Injury Network (AKIN) stage 1 following cardiac surgery the urinary renin-to-creatinine ratio and the angiotensinogen-to-creatinine ratio predicted a composite outcome of death or AKIN stage 3 or death
Plasma NGAL
bull In a prospective cohort study in which 616 patients admitted from the emergency department were classified by clinical criteria as AKI transient azotemia stable CKD or normal kidney function plasma NGAL discriminated AKI from normal function and from transient azotemia
bull Higher concentrations of NGAL were associated with more severe AKI
Thanks for your attention

bull KIM-1 is a biomarker of AKI in humans bull Urine samples were collected from 32 patients with various
acute and chronic kidney diseases as well as from eight normal controls there was extensive expression of KIM-1 in proximal tubule cells in kidney biopsies from six patients with biopsy confirmed acute tubular necrosis (ATN)
bull Urinary KIM-1 levels were significantly higher in patients with ischemic ATN compared to levels in patients with other forms of acute renal failure or chronic renal disease
bull Adjusted for age gender and length of time delay between the initial insult and sampling of the urine a one-unit increase in normalized KIM-1 was associated with a greater than 12-fold risk for the presence of ATN
bull In hospital patients with AKI urinary levels of KIM-1 that higher levels correlated with a higher odds ratio for dialysis requirement or hospital death
bull this study demonstrated that urinary biomarker of AKI such as KIM-1 can predict adverse clinical outcomes in patients with AKI
bull Both renal and urinary KIM-1 correlate with kidney damage and negatively with renal function but not with proteinuria
bull A recent study has explored urinary KIM-1correlated with kidney function in kidney allograft recipients Kidney transplant recipients showed significantly higher KIM-1 values than the healthy volunteers this study concluded that even a successful kidney transplantation is associated with kidney injury as reflected by elevated urinary KIM-1
bull A rapid direct 15-minute assay for the detection of urinary human KIM-1 has been developed Using this assay more urinary KIM-1 was detected in the urine of patients with AKI than in the urine from healthy volunteers
Urinary interleukin-18
bull Interleukin18 (IL-18) is a 22 kDa pro-inflammatory cytokine that increases in the kidney after ischemia-reperfusion injury in a caspase- 1-dependent manner
bull Patients with ATN had significantly greater urinary IL-18 concentrations than those with other conditions (healthy controls patients with pre-renal azotemia urinary tract infection CKD and nephrotic syndrome)
bull urinary IL-18 concentrations measured in the first 24 h after kidney transplantation were higher in patients who received a cadaveric kidney that developed delayed graft function compared to patients who received a cadaveric kidney with prompt graft function and patients who received a kidney with prompt graft function from a living donor
bull However the performance of urinary IL-18 measured 1 day before AKI was modest
bull Its predictive utility for AKI following cardiac surgery could not be demonstrated in one prospective observational study of 100 adult patients
bull In addition in a large study population of 1439 critically ill patients IL-18 had a poor-to-moderate ability to predict AKI renal replacement therapy (RRT) or 90-day mortality
Liver-Type Fatty Acid Binding Protein(L-FABP)
bull Liver-type fatty acid-binding protein (L-FABP) is a 14 kDa protein from the large super- family of lipidbinding proteins
bull The 14-kD L-FABP protein can be localized predominantly in the proximal tubule
bull Noiri et al demonstrated that increase of urinary L-FABP was observed at 1 h after ischemia even in the 5-min IRI group and urinary L-FABP was superior to BUN and urinary NAG for early and accurate detection of acute tubular necrosis in different models of animal AKI
bull urinary L-FABP may be a promising biomarker for early detection of AKI and prediction of dialysis requirement and in-hospital mortality
bull Urinary excretion of urinary liver-type fatty acid-binding protein (L-FABP) reflects stress of proximal tubular epithelial cells and correlates with severity of ischemic tubular injury
bull A meta-analysis of 15 prospective cohort studies demonstrated that in hospitalndashbased cohorts of patients at risk of AKI L-FABP can discriminate for the diagnosis of AKI and predict the need for dialysis and in-hospital mortality
bull It was correlated with the degree of tubulointerstitial damage in a folic acid induced nephropathy
bull In ischemic and cisplatin-induced AKI L-FABP was increased in the urine before the increase in BUN
bull In cisplatin-induced AKI urinary L-FABP levels increased exponentially even in the lowest dose group as early as 2 hours whereas BUN levels increased at 48 hours
bull L-FABP was measured in 80 critically ill patients Urinary L-FABP levels in patients with septic shock were significantly higher than severe sepsis without shock Serum L-FABP levels did not have significant differences between patients with septic shock severe sepsis and healthy
bull Another study was evaluated 145 septic shock patients complicated with established AKI Urinary L-FABP measured at admission was significantly higher in the nonsurvivors of septic shock with established acute kidney injury than in the survivors
Failure of the TRIBE-AKI study
bull The Translational Research Investigating Biomarker Endpoints in AKI (TRIBE-AKI) study evaluated the performance of urinary c-glutamyltranspeptidase ( c-GTP) alkaline phosphatase NGAL Cys-C KIM-1 and IL-18 in AKI diagnosis
bull The results of four novel urine biomarkers and one plasma biomarker (urine NGAL IL-18 KIM-1 and L-FABP and plasma NGAL) were provided Of all the novel biomarkers only urine IL-18 and plasma NGAL in adults were helpful in predicting progression of AKI when measured on the day of clinical AKI diagnosis
bull Combinations of three biomarkers in adults from two different time points and combinations of two biomarkers in children from two time points were found to be able to increase the ROC for AKI up to 078
bull In summary the clinical use of single damage biomarkers in AKI prediction remains unclear because large prospective multicenter trials such as the TRIBE-AKI study (nfrac141530) have failed to demonstrate troponin-like diagnostic performance
Various clinical scenarios of AKI based onfunction damage and stress
bull Over the last decade a number of novel damage biomarkers have been evaluated for their capacity to detect kidney damage and predict the development of AKI However the relationship between decreasing function and increasing damage is not as straightforward as might be assumed
bull The characteristic pattern whereby damage precedes loss of function (panel A) may be seen in some cases of AKI and affords an opportunity to detect ldquosubclinicalrdquo AKI before function start to fall Unfortunately other patterns might also occur For example functional decline may start to occur alongside damage (panel B) and in some cases function may start to decline even before damage (panel C)
bull This makes damage markers difficult to use for predicting AKI However other markers might actually measure the ldquostressrdquo occurring at the cellular level before damage or loss of function
Paradigm shift to pre-injury phase biomarkers
bull Katz et al proposed that the pre-injury phase that leads to AKI can be described as ldquoacute kidney stressrdquo (AKS) after the report of the identification of cell cycle arrest biomarkers that signal the potential development of AKI is part of an evolution in the molecular diagnosis and understanding of AKI
bull These biomarkers are released by kidney cells along a path which may lead to AKI during a pre-injury phase
bull AKS is defined as the increased-risk phase (pre-injury phase) that leads to AKI
bull This ldquoAKSrdquo may or may not lead to damage and functional declinebull But it is the earliest possible the process of AKI can be detected
Pre-injury phase biomarkers
Stress biomarkersbull In 2013 Kashani et al reported the results of a prospective international
observational investigation (the Sapphire study) of tissue inhibitor of metalloproteinases- 2 (TIMP-2) and insulin-like growth factor-binding protein 7 (IGFBP7) in a heterogeneous group of critically ill patients [TIMP-2][IGFBP7] was significantly superior to all previously described markers of AKI (plt0002)
bull Next the Opal and Topaz study showed the cut-off value and risk assessment using the urinary[TIMP-2] [IGFBP7]
bull The urine [IGFBP7][TIMP2] biomarker is already FDA approved and commercially available in the United States
bull Falsepositive results are common and they will be magnified if the test is used inappropriately in low-risk patients In addition this biomarker should not be used in ambulatory practices and it is not beneficial in patients with established AKI
microRNAsbull microRNAs (miRNAs) are endogenous single-stranded non-coding
mRNAs of about 19-23 nucleotides bull In the past years researchers have begun to investigate the
relevance of miRNAs to AKI with many miRNAs being implicated bull Some of them contribute to pathogenesis by regulating apoptosis
and inflammation amplifying or reducing acute injury responses while others regulate fibrosis and angiogenesis participating in renal recovery or progression to fibrosis
bull Certain miRNAs have been investigated for their potential as novel biomarkers for the early detection or prognostication of AKI
Hemojuvelinbull Hemojuvelin (HJV) a glycophosphatidylinositol (GPI)- linked
membrane protein is highly expressed in liver and skeletal musclesbull The molecular weight of HJV is 42 kDa for the soluble form (sHJV)
and can be passed through glomerular filtration and reabsorbed by the renal tubules Increased iron content in the kidney and urine is observed in human and animal models of AKI and increased iron load can induce renal tubular cell injury
bull There is evidence that the increased expression of the hemojuvelin-hepcidin ferroportin pathway is an intrinsic response to iron overload conditions during AKI
bull Therefore urine HJV (uHJV) has the potential to be an early AKI biomarker in response to iron homeostasis during AKI
Combination of functional and damage biomarkers
bull While new biomarkers are being validated functional biomarkers (serum creatinine serum urea and urine output) continue to be utilized in the diagnosis and staging of AKI In the future existing or newer damage biomarkers will likely be combined with the use of functional biomarkers to enhance the ability of RIFLE AKIN
bull A study of 345 children after cardiopulmonary bypass surgery demonstrated that the composite of functional biomarker such as plasma cystatin C and urinary NGAL was superior to changes in serum creatinine to predict AKI
PROGNOSTIC BIOMARKERS
bull Most of the biomarkers described above allow early detection of acute kidney injury but do not predict severe AKI
Urinary renin and angiotensinogen
bull Urinary renin angiotensinogen and plasma NGAL may predict the development of severe AKI
bull Among 99 consecutively enrolled patients who developed AKI the ratio of urinary angiotensinogen to urinary creatinine (uAnCR expressed as ng per mg creatinine)calculated Patients with the highest uAnCR had a higher risk of worsening AKI compared with patients with the lowest uAnCR An elevated uAnCR predicted a longer hospital stay
bull Among 204 patients who developed Acute Kidney Injury Network (AKIN) stage 1 following cardiac surgery the urinary renin-to-creatinine ratio and the angiotensinogen-to-creatinine ratio predicted a composite outcome of death or AKIN stage 3 or death
Plasma NGAL
bull In a prospective cohort study in which 616 patients admitted from the emergency department were classified by clinical criteria as AKI transient azotemia stable CKD or normal kidney function plasma NGAL discriminated AKI from normal function and from transient azotemia
bull Higher concentrations of NGAL were associated with more severe AKI
Thanks for your attention
bull In hospital patients with AKI urinary levels of KIM-1 that higher levels correlated with a higher odds ratio for dialysis requirement or hospital death
bull this study demonstrated that urinary biomarker of AKI such as KIM-1 can predict adverse clinical outcomes in patients with AKI
bull Both renal and urinary KIM-1 correlate with kidney damage and negatively with renal function but not with proteinuria
bull A recent study has explored urinary KIM-1correlated with kidney function in kidney allograft recipients Kidney transplant recipients showed significantly higher KIM-1 values than the healthy volunteers this study concluded that even a successful kidney transplantation is associated with kidney injury as reflected by elevated urinary KIM-1
bull A rapid direct 15-minute assay for the detection of urinary human KIM-1 has been developed Using this assay more urinary KIM-1 was detected in the urine of patients with AKI than in the urine from healthy volunteers
Urinary interleukin-18
bull Interleukin18 (IL-18) is a 22 kDa pro-inflammatory cytokine that increases in the kidney after ischemia-reperfusion injury in a caspase- 1-dependent manner
bull Patients with ATN had significantly greater urinary IL-18 concentrations than those with other conditions (healthy controls patients with pre-renal azotemia urinary tract infection CKD and nephrotic syndrome)
bull urinary IL-18 concentrations measured in the first 24 h after kidney transplantation were higher in patients who received a cadaveric kidney that developed delayed graft function compared to patients who received a cadaveric kidney with prompt graft function and patients who received a kidney with prompt graft function from a living donor
bull However the performance of urinary IL-18 measured 1 day before AKI was modest
bull Its predictive utility for AKI following cardiac surgery could not be demonstrated in one prospective observational study of 100 adult patients
bull In addition in a large study population of 1439 critically ill patients IL-18 had a poor-to-moderate ability to predict AKI renal replacement therapy (RRT) or 90-day mortality
Liver-Type Fatty Acid Binding Protein(L-FABP)
bull Liver-type fatty acid-binding protein (L-FABP) is a 14 kDa protein from the large super- family of lipidbinding proteins
bull The 14-kD L-FABP protein can be localized predominantly in the proximal tubule
bull Noiri et al demonstrated that increase of urinary L-FABP was observed at 1 h after ischemia even in the 5-min IRI group and urinary L-FABP was superior to BUN and urinary NAG for early and accurate detection of acute tubular necrosis in different models of animal AKI
bull urinary L-FABP may be a promising biomarker for early detection of AKI and prediction of dialysis requirement and in-hospital mortality
bull Urinary excretion of urinary liver-type fatty acid-binding protein (L-FABP) reflects stress of proximal tubular epithelial cells and correlates with severity of ischemic tubular injury
bull A meta-analysis of 15 prospective cohort studies demonstrated that in hospitalndashbased cohorts of patients at risk of AKI L-FABP can discriminate for the diagnosis of AKI and predict the need for dialysis and in-hospital mortality
bull It was correlated with the degree of tubulointerstitial damage in a folic acid induced nephropathy
bull In ischemic and cisplatin-induced AKI L-FABP was increased in the urine before the increase in BUN
bull In cisplatin-induced AKI urinary L-FABP levels increased exponentially even in the lowest dose group as early as 2 hours whereas BUN levels increased at 48 hours
bull L-FABP was measured in 80 critically ill patients Urinary L-FABP levels in patients with septic shock were significantly higher than severe sepsis without shock Serum L-FABP levels did not have significant differences between patients with septic shock severe sepsis and healthy
bull Another study was evaluated 145 septic shock patients complicated with established AKI Urinary L-FABP measured at admission was significantly higher in the nonsurvivors of septic shock with established acute kidney injury than in the survivors
Failure of the TRIBE-AKI study
bull The Translational Research Investigating Biomarker Endpoints in AKI (TRIBE-AKI) study evaluated the performance of urinary c-glutamyltranspeptidase ( c-GTP) alkaline phosphatase NGAL Cys-C KIM-1 and IL-18 in AKI diagnosis
bull The results of four novel urine biomarkers and one plasma biomarker (urine NGAL IL-18 KIM-1 and L-FABP and plasma NGAL) were provided Of all the novel biomarkers only urine IL-18 and plasma NGAL in adults were helpful in predicting progression of AKI when measured on the day of clinical AKI diagnosis
bull Combinations of three biomarkers in adults from two different time points and combinations of two biomarkers in children from two time points were found to be able to increase the ROC for AKI up to 078
bull In summary the clinical use of single damage biomarkers in AKI prediction remains unclear because large prospective multicenter trials such as the TRIBE-AKI study (nfrac141530) have failed to demonstrate troponin-like diagnostic performance
Various clinical scenarios of AKI based onfunction damage and stress
bull Over the last decade a number of novel damage biomarkers have been evaluated for their capacity to detect kidney damage and predict the development of AKI However the relationship between decreasing function and increasing damage is not as straightforward as might be assumed
bull The characteristic pattern whereby damage precedes loss of function (panel A) may be seen in some cases of AKI and affords an opportunity to detect ldquosubclinicalrdquo AKI before function start to fall Unfortunately other patterns might also occur For example functional decline may start to occur alongside damage (panel B) and in some cases function may start to decline even before damage (panel C)
bull This makes damage markers difficult to use for predicting AKI However other markers might actually measure the ldquostressrdquo occurring at the cellular level before damage or loss of function
Paradigm shift to pre-injury phase biomarkers
bull Katz et al proposed that the pre-injury phase that leads to AKI can be described as ldquoacute kidney stressrdquo (AKS) after the report of the identification of cell cycle arrest biomarkers that signal the potential development of AKI is part of an evolution in the molecular diagnosis and understanding of AKI
bull These biomarkers are released by kidney cells along a path which may lead to AKI during a pre-injury phase
bull AKS is defined as the increased-risk phase (pre-injury phase) that leads to AKI
bull This ldquoAKSrdquo may or may not lead to damage and functional declinebull But it is the earliest possible the process of AKI can be detected
Pre-injury phase biomarkers
Stress biomarkersbull In 2013 Kashani et al reported the results of a prospective international
observational investigation (the Sapphire study) of tissue inhibitor of metalloproteinases- 2 (TIMP-2) and insulin-like growth factor-binding protein 7 (IGFBP7) in a heterogeneous group of critically ill patients [TIMP-2][IGFBP7] was significantly superior to all previously described markers of AKI (plt0002)
bull Next the Opal and Topaz study showed the cut-off value and risk assessment using the urinary[TIMP-2] [IGFBP7]
bull The urine [IGFBP7][TIMP2] biomarker is already FDA approved and commercially available in the United States
bull Falsepositive results are common and they will be magnified if the test is used inappropriately in low-risk patients In addition this biomarker should not be used in ambulatory practices and it is not beneficial in patients with established AKI
microRNAsbull microRNAs (miRNAs) are endogenous single-stranded non-coding
mRNAs of about 19-23 nucleotides bull In the past years researchers have begun to investigate the
relevance of miRNAs to AKI with many miRNAs being implicated bull Some of them contribute to pathogenesis by regulating apoptosis
and inflammation amplifying or reducing acute injury responses while others regulate fibrosis and angiogenesis participating in renal recovery or progression to fibrosis
bull Certain miRNAs have been investigated for their potential as novel biomarkers for the early detection or prognostication of AKI
Hemojuvelinbull Hemojuvelin (HJV) a glycophosphatidylinositol (GPI)- linked
membrane protein is highly expressed in liver and skeletal musclesbull The molecular weight of HJV is 42 kDa for the soluble form (sHJV)
and can be passed through glomerular filtration and reabsorbed by the renal tubules Increased iron content in the kidney and urine is observed in human and animal models of AKI and increased iron load can induce renal tubular cell injury
bull There is evidence that the increased expression of the hemojuvelin-hepcidin ferroportin pathway is an intrinsic response to iron overload conditions during AKI
bull Therefore urine HJV (uHJV) has the potential to be an early AKI biomarker in response to iron homeostasis during AKI
Combination of functional and damage biomarkers
bull While new biomarkers are being validated functional biomarkers (serum creatinine serum urea and urine output) continue to be utilized in the diagnosis and staging of AKI In the future existing or newer damage biomarkers will likely be combined with the use of functional biomarkers to enhance the ability of RIFLE AKIN
bull A study of 345 children after cardiopulmonary bypass surgery demonstrated that the composite of functional biomarker such as plasma cystatin C and urinary NGAL was superior to changes in serum creatinine to predict AKI
PROGNOSTIC BIOMARKERS
bull Most of the biomarkers described above allow early detection of acute kidney injury but do not predict severe AKI
Urinary renin and angiotensinogen
bull Urinary renin angiotensinogen and plasma NGAL may predict the development of severe AKI
bull Among 99 consecutively enrolled patients who developed AKI the ratio of urinary angiotensinogen to urinary creatinine (uAnCR expressed as ng per mg creatinine)calculated Patients with the highest uAnCR had a higher risk of worsening AKI compared with patients with the lowest uAnCR An elevated uAnCR predicted a longer hospital stay
bull Among 204 patients who developed Acute Kidney Injury Network (AKIN) stage 1 following cardiac surgery the urinary renin-to-creatinine ratio and the angiotensinogen-to-creatinine ratio predicted a composite outcome of death or AKIN stage 3 or death
Plasma NGAL
bull In a prospective cohort study in which 616 patients admitted from the emergency department were classified by clinical criteria as AKI transient azotemia stable CKD or normal kidney function plasma NGAL discriminated AKI from normal function and from transient azotemia
bull Higher concentrations of NGAL were associated with more severe AKI
Thanks for your attention

Urinary interleukin-18
bull Interleukin18 (IL-18) is a 22 kDa pro-inflammatory cytokine that increases in the kidney after ischemia-reperfusion injury in a caspase- 1-dependent manner
bull Patients with ATN had significantly greater urinary IL-18 concentrations than those with other conditions (healthy controls patients with pre-renal azotemia urinary tract infection CKD and nephrotic syndrome)
bull urinary IL-18 concentrations measured in the first 24 h after kidney transplantation were higher in patients who received a cadaveric kidney that developed delayed graft function compared to patients who received a cadaveric kidney with prompt graft function and patients who received a kidney with prompt graft function from a living donor
bull However the performance of urinary IL-18 measured 1 day before AKI was modest
bull Its predictive utility for AKI following cardiac surgery could not be demonstrated in one prospective observational study of 100 adult patients
bull In addition in a large study population of 1439 critically ill patients IL-18 had a poor-to-moderate ability to predict AKI renal replacement therapy (RRT) or 90-day mortality
Liver-Type Fatty Acid Binding Protein(L-FABP)
bull Liver-type fatty acid-binding protein (L-FABP) is a 14 kDa protein from the large super- family of lipidbinding proteins
bull The 14-kD L-FABP protein can be localized predominantly in the proximal tubule
bull Noiri et al demonstrated that increase of urinary L-FABP was observed at 1 h after ischemia even in the 5-min IRI group and urinary L-FABP was superior to BUN and urinary NAG for early and accurate detection of acute tubular necrosis in different models of animal AKI
bull urinary L-FABP may be a promising biomarker for early detection of AKI and prediction of dialysis requirement and in-hospital mortality
bull Urinary excretion of urinary liver-type fatty acid-binding protein (L-FABP) reflects stress of proximal tubular epithelial cells and correlates with severity of ischemic tubular injury
bull A meta-analysis of 15 prospective cohort studies demonstrated that in hospitalndashbased cohorts of patients at risk of AKI L-FABP can discriminate for the diagnosis of AKI and predict the need for dialysis and in-hospital mortality
bull It was correlated with the degree of tubulointerstitial damage in a folic acid induced nephropathy
bull In ischemic and cisplatin-induced AKI L-FABP was increased in the urine before the increase in BUN
bull In cisplatin-induced AKI urinary L-FABP levels increased exponentially even in the lowest dose group as early as 2 hours whereas BUN levels increased at 48 hours
bull L-FABP was measured in 80 critically ill patients Urinary L-FABP levels in patients with septic shock were significantly higher than severe sepsis without shock Serum L-FABP levels did not have significant differences between patients with septic shock severe sepsis and healthy
bull Another study was evaluated 145 septic shock patients complicated with established AKI Urinary L-FABP measured at admission was significantly higher in the nonsurvivors of septic shock with established acute kidney injury than in the survivors
Failure of the TRIBE-AKI study
bull The Translational Research Investigating Biomarker Endpoints in AKI (TRIBE-AKI) study evaluated the performance of urinary c-glutamyltranspeptidase ( c-GTP) alkaline phosphatase NGAL Cys-C KIM-1 and IL-18 in AKI diagnosis
bull The results of four novel urine biomarkers and one plasma biomarker (urine NGAL IL-18 KIM-1 and L-FABP and plasma NGAL) were provided Of all the novel biomarkers only urine IL-18 and plasma NGAL in adults were helpful in predicting progression of AKI when measured on the day of clinical AKI diagnosis
bull Combinations of three biomarkers in adults from two different time points and combinations of two biomarkers in children from two time points were found to be able to increase the ROC for AKI up to 078
bull In summary the clinical use of single damage biomarkers in AKI prediction remains unclear because large prospective multicenter trials such as the TRIBE-AKI study (nfrac141530) have failed to demonstrate troponin-like diagnostic performance
Various clinical scenarios of AKI based onfunction damage and stress
bull Over the last decade a number of novel damage biomarkers have been evaluated for their capacity to detect kidney damage and predict the development of AKI However the relationship between decreasing function and increasing damage is not as straightforward as might be assumed
bull The characteristic pattern whereby damage precedes loss of function (panel A) may be seen in some cases of AKI and affords an opportunity to detect ldquosubclinicalrdquo AKI before function start to fall Unfortunately other patterns might also occur For example functional decline may start to occur alongside damage (panel B) and in some cases function may start to decline even before damage (panel C)
bull This makes damage markers difficult to use for predicting AKI However other markers might actually measure the ldquostressrdquo occurring at the cellular level before damage or loss of function
Paradigm shift to pre-injury phase biomarkers
bull Katz et al proposed that the pre-injury phase that leads to AKI can be described as ldquoacute kidney stressrdquo (AKS) after the report of the identification of cell cycle arrest biomarkers that signal the potential development of AKI is part of an evolution in the molecular diagnosis and understanding of AKI
bull These biomarkers are released by kidney cells along a path which may lead to AKI during a pre-injury phase
bull AKS is defined as the increased-risk phase (pre-injury phase) that leads to AKI
bull This ldquoAKSrdquo may or may not lead to damage and functional declinebull But it is the earliest possible the process of AKI can be detected
Pre-injury phase biomarkers
Stress biomarkersbull In 2013 Kashani et al reported the results of a prospective international
observational investigation (the Sapphire study) of tissue inhibitor of metalloproteinases- 2 (TIMP-2) and insulin-like growth factor-binding protein 7 (IGFBP7) in a heterogeneous group of critically ill patients [TIMP-2][IGFBP7] was significantly superior to all previously described markers of AKI (plt0002)
bull Next the Opal and Topaz study showed the cut-off value and risk assessment using the urinary[TIMP-2] [IGFBP7]
bull The urine [IGFBP7][TIMP2] biomarker is already FDA approved and commercially available in the United States
bull Falsepositive results are common and they will be magnified if the test is used inappropriately in low-risk patients In addition this biomarker should not be used in ambulatory practices and it is not beneficial in patients with established AKI
microRNAsbull microRNAs (miRNAs) are endogenous single-stranded non-coding
mRNAs of about 19-23 nucleotides bull In the past years researchers have begun to investigate the
relevance of miRNAs to AKI with many miRNAs being implicated bull Some of them contribute to pathogenesis by regulating apoptosis
and inflammation amplifying or reducing acute injury responses while others regulate fibrosis and angiogenesis participating in renal recovery or progression to fibrosis
bull Certain miRNAs have been investigated for their potential as novel biomarkers for the early detection or prognostication of AKI
Hemojuvelinbull Hemojuvelin (HJV) a glycophosphatidylinositol (GPI)- linked
membrane protein is highly expressed in liver and skeletal musclesbull The molecular weight of HJV is 42 kDa for the soluble form (sHJV)
and can be passed through glomerular filtration and reabsorbed by the renal tubules Increased iron content in the kidney and urine is observed in human and animal models of AKI and increased iron load can induce renal tubular cell injury
bull There is evidence that the increased expression of the hemojuvelin-hepcidin ferroportin pathway is an intrinsic response to iron overload conditions during AKI
bull Therefore urine HJV (uHJV) has the potential to be an early AKI biomarker in response to iron homeostasis during AKI
Combination of functional and damage biomarkers
bull While new biomarkers are being validated functional biomarkers (serum creatinine serum urea and urine output) continue to be utilized in the diagnosis and staging of AKI In the future existing or newer damage biomarkers will likely be combined with the use of functional biomarkers to enhance the ability of RIFLE AKIN
bull A study of 345 children after cardiopulmonary bypass surgery demonstrated that the composite of functional biomarker such as plasma cystatin C and urinary NGAL was superior to changes in serum creatinine to predict AKI
PROGNOSTIC BIOMARKERS
bull Most of the biomarkers described above allow early detection of acute kidney injury but do not predict severe AKI
Urinary renin and angiotensinogen
bull Urinary renin angiotensinogen and plasma NGAL may predict the development of severe AKI
bull Among 99 consecutively enrolled patients who developed AKI the ratio of urinary angiotensinogen to urinary creatinine (uAnCR expressed as ng per mg creatinine)calculated Patients with the highest uAnCR had a higher risk of worsening AKI compared with patients with the lowest uAnCR An elevated uAnCR predicted a longer hospital stay
bull Among 204 patients who developed Acute Kidney Injury Network (AKIN) stage 1 following cardiac surgery the urinary renin-to-creatinine ratio and the angiotensinogen-to-creatinine ratio predicted a composite outcome of death or AKIN stage 3 or death
Plasma NGAL
bull In a prospective cohort study in which 616 patients admitted from the emergency department were classified by clinical criteria as AKI transient azotemia stable CKD or normal kidney function plasma NGAL discriminated AKI from normal function and from transient azotemia
bull Higher concentrations of NGAL were associated with more severe AKI
Thanks for your attention
bull urinary IL-18 concentrations measured in the first 24 h after kidney transplantation were higher in patients who received a cadaveric kidney that developed delayed graft function compared to patients who received a cadaveric kidney with prompt graft function and patients who received a kidney with prompt graft function from a living donor
bull However the performance of urinary IL-18 measured 1 day before AKI was modest
bull Its predictive utility for AKI following cardiac surgery could not be demonstrated in one prospective observational study of 100 adult patients
bull In addition in a large study population of 1439 critically ill patients IL-18 had a poor-to-moderate ability to predict AKI renal replacement therapy (RRT) or 90-day mortality
Liver-Type Fatty Acid Binding Protein(L-FABP)
bull Liver-type fatty acid-binding protein (L-FABP) is a 14 kDa protein from the large super- family of lipidbinding proteins
bull The 14-kD L-FABP protein can be localized predominantly in the proximal tubule
bull Noiri et al demonstrated that increase of urinary L-FABP was observed at 1 h after ischemia even in the 5-min IRI group and urinary L-FABP was superior to BUN and urinary NAG for early and accurate detection of acute tubular necrosis in different models of animal AKI
bull urinary L-FABP may be a promising biomarker for early detection of AKI and prediction of dialysis requirement and in-hospital mortality
bull Urinary excretion of urinary liver-type fatty acid-binding protein (L-FABP) reflects stress of proximal tubular epithelial cells and correlates with severity of ischemic tubular injury
bull A meta-analysis of 15 prospective cohort studies demonstrated that in hospitalndashbased cohorts of patients at risk of AKI L-FABP can discriminate for the diagnosis of AKI and predict the need for dialysis and in-hospital mortality
bull It was correlated with the degree of tubulointerstitial damage in a folic acid induced nephropathy
bull In ischemic and cisplatin-induced AKI L-FABP was increased in the urine before the increase in BUN
bull In cisplatin-induced AKI urinary L-FABP levels increased exponentially even in the lowest dose group as early as 2 hours whereas BUN levels increased at 48 hours
bull L-FABP was measured in 80 critically ill patients Urinary L-FABP levels in patients with septic shock were significantly higher than severe sepsis without shock Serum L-FABP levels did not have significant differences between patients with septic shock severe sepsis and healthy
bull Another study was evaluated 145 septic shock patients complicated with established AKI Urinary L-FABP measured at admission was significantly higher in the nonsurvivors of septic shock with established acute kidney injury than in the survivors
Failure of the TRIBE-AKI study
bull The Translational Research Investigating Biomarker Endpoints in AKI (TRIBE-AKI) study evaluated the performance of urinary c-glutamyltranspeptidase ( c-GTP) alkaline phosphatase NGAL Cys-C KIM-1 and IL-18 in AKI diagnosis
bull The results of four novel urine biomarkers and one plasma biomarker (urine NGAL IL-18 KIM-1 and L-FABP and plasma NGAL) were provided Of all the novel biomarkers only urine IL-18 and plasma NGAL in adults were helpful in predicting progression of AKI when measured on the day of clinical AKI diagnosis
bull Combinations of three biomarkers in adults from two different time points and combinations of two biomarkers in children from two time points were found to be able to increase the ROC for AKI up to 078
bull In summary the clinical use of single damage biomarkers in AKI prediction remains unclear because large prospective multicenter trials such as the TRIBE-AKI study (nfrac141530) have failed to demonstrate troponin-like diagnostic performance
Various clinical scenarios of AKI based onfunction damage and stress
bull Over the last decade a number of novel damage biomarkers have been evaluated for their capacity to detect kidney damage and predict the development of AKI However the relationship between decreasing function and increasing damage is not as straightforward as might be assumed
bull The characteristic pattern whereby damage precedes loss of function (panel A) may be seen in some cases of AKI and affords an opportunity to detect ldquosubclinicalrdquo AKI before function start to fall Unfortunately other patterns might also occur For example functional decline may start to occur alongside damage (panel B) and in some cases function may start to decline even before damage (panel C)
bull This makes damage markers difficult to use for predicting AKI However other markers might actually measure the ldquostressrdquo occurring at the cellular level before damage or loss of function
Paradigm shift to pre-injury phase biomarkers
bull Katz et al proposed that the pre-injury phase that leads to AKI can be described as ldquoacute kidney stressrdquo (AKS) after the report of the identification of cell cycle arrest biomarkers that signal the potential development of AKI is part of an evolution in the molecular diagnosis and understanding of AKI
bull These biomarkers are released by kidney cells along a path which may lead to AKI during a pre-injury phase
bull AKS is defined as the increased-risk phase (pre-injury phase) that leads to AKI
bull This ldquoAKSrdquo may or may not lead to damage and functional declinebull But it is the earliest possible the process of AKI can be detected
Pre-injury phase biomarkers
Stress biomarkersbull In 2013 Kashani et al reported the results of a prospective international
observational investigation (the Sapphire study) of tissue inhibitor of metalloproteinases- 2 (TIMP-2) and insulin-like growth factor-binding protein 7 (IGFBP7) in a heterogeneous group of critically ill patients [TIMP-2][IGFBP7] was significantly superior to all previously described markers of AKI (plt0002)
bull Next the Opal and Topaz study showed the cut-off value and risk assessment using the urinary[TIMP-2] [IGFBP7]
bull The urine [IGFBP7][TIMP2] biomarker is already FDA approved and commercially available in the United States
bull Falsepositive results are common and they will be magnified if the test is used inappropriately in low-risk patients In addition this biomarker should not be used in ambulatory practices and it is not beneficial in patients with established AKI
microRNAsbull microRNAs (miRNAs) are endogenous single-stranded non-coding
mRNAs of about 19-23 nucleotides bull In the past years researchers have begun to investigate the
relevance of miRNAs to AKI with many miRNAs being implicated bull Some of them contribute to pathogenesis by regulating apoptosis
and inflammation amplifying or reducing acute injury responses while others regulate fibrosis and angiogenesis participating in renal recovery or progression to fibrosis
bull Certain miRNAs have been investigated for their potential as novel biomarkers for the early detection or prognostication of AKI
Hemojuvelinbull Hemojuvelin (HJV) a glycophosphatidylinositol (GPI)- linked
membrane protein is highly expressed in liver and skeletal musclesbull The molecular weight of HJV is 42 kDa for the soluble form (sHJV)
and can be passed through glomerular filtration and reabsorbed by the renal tubules Increased iron content in the kidney and urine is observed in human and animal models of AKI and increased iron load can induce renal tubular cell injury
bull There is evidence that the increased expression of the hemojuvelin-hepcidin ferroportin pathway is an intrinsic response to iron overload conditions during AKI
bull Therefore urine HJV (uHJV) has the potential to be an early AKI biomarker in response to iron homeostasis during AKI
Combination of functional and damage biomarkers
bull While new biomarkers are being validated functional biomarkers (serum creatinine serum urea and urine output) continue to be utilized in the diagnosis and staging of AKI In the future existing or newer damage biomarkers will likely be combined with the use of functional biomarkers to enhance the ability of RIFLE AKIN
bull A study of 345 children after cardiopulmonary bypass surgery demonstrated that the composite of functional biomarker such as plasma cystatin C and urinary NGAL was superior to changes in serum creatinine to predict AKI
PROGNOSTIC BIOMARKERS
bull Most of the biomarkers described above allow early detection of acute kidney injury but do not predict severe AKI
Urinary renin and angiotensinogen
bull Urinary renin angiotensinogen and plasma NGAL may predict the development of severe AKI
bull Among 99 consecutively enrolled patients who developed AKI the ratio of urinary angiotensinogen to urinary creatinine (uAnCR expressed as ng per mg creatinine)calculated Patients with the highest uAnCR had a higher risk of worsening AKI compared with patients with the lowest uAnCR An elevated uAnCR predicted a longer hospital stay
bull Among 204 patients who developed Acute Kidney Injury Network (AKIN) stage 1 following cardiac surgery the urinary renin-to-creatinine ratio and the angiotensinogen-to-creatinine ratio predicted a composite outcome of death or AKIN stage 3 or death
Plasma NGAL
bull In a prospective cohort study in which 616 patients admitted from the emergency department were classified by clinical criteria as AKI transient azotemia stable CKD or normal kidney function plasma NGAL discriminated AKI from normal function and from transient azotemia
bull Higher concentrations of NGAL were associated with more severe AKI
Thanks for your attention

Liver-Type Fatty Acid Binding Protein(L-FABP)
bull Liver-type fatty acid-binding protein (L-FABP) is a 14 kDa protein from the large super- family of lipidbinding proteins
bull The 14-kD L-FABP protein can be localized predominantly in the proximal tubule
bull Noiri et al demonstrated that increase of urinary L-FABP was observed at 1 h after ischemia even in the 5-min IRI group and urinary L-FABP was superior to BUN and urinary NAG for early and accurate detection of acute tubular necrosis in different models of animal AKI
bull urinary L-FABP may be a promising biomarker for early detection of AKI and prediction of dialysis requirement and in-hospital mortality
bull Urinary excretion of urinary liver-type fatty acid-binding protein (L-FABP) reflects stress of proximal tubular epithelial cells and correlates with severity of ischemic tubular injury
bull A meta-analysis of 15 prospective cohort studies demonstrated that in hospitalndashbased cohorts of patients at risk of AKI L-FABP can discriminate for the diagnosis of AKI and predict the need for dialysis and in-hospital mortality
bull It was correlated with the degree of tubulointerstitial damage in a folic acid induced nephropathy
bull In ischemic and cisplatin-induced AKI L-FABP was increased in the urine before the increase in BUN
bull In cisplatin-induced AKI urinary L-FABP levels increased exponentially even in the lowest dose group as early as 2 hours whereas BUN levels increased at 48 hours
bull L-FABP was measured in 80 critically ill patients Urinary L-FABP levels in patients with septic shock were significantly higher than severe sepsis without shock Serum L-FABP levels did not have significant differences between patients with septic shock severe sepsis and healthy
bull Another study was evaluated 145 septic shock patients complicated with established AKI Urinary L-FABP measured at admission was significantly higher in the nonsurvivors of septic shock with established acute kidney injury than in the survivors
Failure of the TRIBE-AKI study
bull The Translational Research Investigating Biomarker Endpoints in AKI (TRIBE-AKI) study evaluated the performance of urinary c-glutamyltranspeptidase ( c-GTP) alkaline phosphatase NGAL Cys-C KIM-1 and IL-18 in AKI diagnosis
bull The results of four novel urine biomarkers and one plasma biomarker (urine NGAL IL-18 KIM-1 and L-FABP and plasma NGAL) were provided Of all the novel biomarkers only urine IL-18 and plasma NGAL in adults were helpful in predicting progression of AKI when measured on the day of clinical AKI diagnosis
bull Combinations of three biomarkers in adults from two different time points and combinations of two biomarkers in children from two time points were found to be able to increase the ROC for AKI up to 078
bull In summary the clinical use of single damage biomarkers in AKI prediction remains unclear because large prospective multicenter trials such as the TRIBE-AKI study (nfrac141530) have failed to demonstrate troponin-like diagnostic performance
Various clinical scenarios of AKI based onfunction damage and stress
bull Over the last decade a number of novel damage biomarkers have been evaluated for their capacity to detect kidney damage and predict the development of AKI However the relationship between decreasing function and increasing damage is not as straightforward as might be assumed
bull The characteristic pattern whereby damage precedes loss of function (panel A) may be seen in some cases of AKI and affords an opportunity to detect ldquosubclinicalrdquo AKI before function start to fall Unfortunately other patterns might also occur For example functional decline may start to occur alongside damage (panel B) and in some cases function may start to decline even before damage (panel C)
bull This makes damage markers difficult to use for predicting AKI However other markers might actually measure the ldquostressrdquo occurring at the cellular level before damage or loss of function
Paradigm shift to pre-injury phase biomarkers
bull Katz et al proposed that the pre-injury phase that leads to AKI can be described as ldquoacute kidney stressrdquo (AKS) after the report of the identification of cell cycle arrest biomarkers that signal the potential development of AKI is part of an evolution in the molecular diagnosis and understanding of AKI
bull These biomarkers are released by kidney cells along a path which may lead to AKI during a pre-injury phase
bull AKS is defined as the increased-risk phase (pre-injury phase) that leads to AKI
bull This ldquoAKSrdquo may or may not lead to damage and functional declinebull But it is the earliest possible the process of AKI can be detected
Pre-injury phase biomarkers
Stress biomarkersbull In 2013 Kashani et al reported the results of a prospective international
observational investigation (the Sapphire study) of tissue inhibitor of metalloproteinases- 2 (TIMP-2) and insulin-like growth factor-binding protein 7 (IGFBP7) in a heterogeneous group of critically ill patients [TIMP-2][IGFBP7] was significantly superior to all previously described markers of AKI (plt0002)
bull Next the Opal and Topaz study showed the cut-off value and risk assessment using the urinary[TIMP-2] [IGFBP7]
bull The urine [IGFBP7][TIMP2] biomarker is already FDA approved and commercially available in the United States
bull Falsepositive results are common and they will be magnified if the test is used inappropriately in low-risk patients In addition this biomarker should not be used in ambulatory practices and it is not beneficial in patients with established AKI
microRNAsbull microRNAs (miRNAs) are endogenous single-stranded non-coding
mRNAs of about 19-23 nucleotides bull In the past years researchers have begun to investigate the
relevance of miRNAs to AKI with many miRNAs being implicated bull Some of them contribute to pathogenesis by regulating apoptosis
and inflammation amplifying or reducing acute injury responses while others regulate fibrosis and angiogenesis participating in renal recovery or progression to fibrosis
bull Certain miRNAs have been investigated for their potential as novel biomarkers for the early detection or prognostication of AKI
Hemojuvelinbull Hemojuvelin (HJV) a glycophosphatidylinositol (GPI)- linked
membrane protein is highly expressed in liver and skeletal musclesbull The molecular weight of HJV is 42 kDa for the soluble form (sHJV)
and can be passed through glomerular filtration and reabsorbed by the renal tubules Increased iron content in the kidney and urine is observed in human and animal models of AKI and increased iron load can induce renal tubular cell injury
bull There is evidence that the increased expression of the hemojuvelin-hepcidin ferroportin pathway is an intrinsic response to iron overload conditions during AKI
bull Therefore urine HJV (uHJV) has the potential to be an early AKI biomarker in response to iron homeostasis during AKI
Combination of functional and damage biomarkers
bull While new biomarkers are being validated functional biomarkers (serum creatinine serum urea and urine output) continue to be utilized in the diagnosis and staging of AKI In the future existing or newer damage biomarkers will likely be combined with the use of functional biomarkers to enhance the ability of RIFLE AKIN
bull A study of 345 children after cardiopulmonary bypass surgery demonstrated that the composite of functional biomarker such as plasma cystatin C and urinary NGAL was superior to changes in serum creatinine to predict AKI
PROGNOSTIC BIOMARKERS
bull Most of the biomarkers described above allow early detection of acute kidney injury but do not predict severe AKI
Urinary renin and angiotensinogen
bull Urinary renin angiotensinogen and plasma NGAL may predict the development of severe AKI
bull Among 99 consecutively enrolled patients who developed AKI the ratio of urinary angiotensinogen to urinary creatinine (uAnCR expressed as ng per mg creatinine)calculated Patients with the highest uAnCR had a higher risk of worsening AKI compared with patients with the lowest uAnCR An elevated uAnCR predicted a longer hospital stay
bull Among 204 patients who developed Acute Kidney Injury Network (AKIN) stage 1 following cardiac surgery the urinary renin-to-creatinine ratio and the angiotensinogen-to-creatinine ratio predicted a composite outcome of death or AKIN stage 3 or death
Plasma NGAL
bull In a prospective cohort study in which 616 patients admitted from the emergency department were classified by clinical criteria as AKI transient azotemia stable CKD or normal kidney function plasma NGAL discriminated AKI from normal function and from transient azotemia
bull Higher concentrations of NGAL were associated with more severe AKI
Thanks for your attention

bull Urinary excretion of urinary liver-type fatty acid-binding protein (L-FABP) reflects stress of proximal tubular epithelial cells and correlates with severity of ischemic tubular injury
bull A meta-analysis of 15 prospective cohort studies demonstrated that in hospitalndashbased cohorts of patients at risk of AKI L-FABP can discriminate for the diagnosis of AKI and predict the need for dialysis and in-hospital mortality
bull It was correlated with the degree of tubulointerstitial damage in a folic acid induced nephropathy
bull In ischemic and cisplatin-induced AKI L-FABP was increased in the urine before the increase in BUN
bull In cisplatin-induced AKI urinary L-FABP levels increased exponentially even in the lowest dose group as early as 2 hours whereas BUN levels increased at 48 hours
bull L-FABP was measured in 80 critically ill patients Urinary L-FABP levels in patients with septic shock were significantly higher than severe sepsis without shock Serum L-FABP levels did not have significant differences between patients with septic shock severe sepsis and healthy
bull Another study was evaluated 145 septic shock patients complicated with established AKI Urinary L-FABP measured at admission was significantly higher in the nonsurvivors of septic shock with established acute kidney injury than in the survivors
Failure of the TRIBE-AKI study
bull The Translational Research Investigating Biomarker Endpoints in AKI (TRIBE-AKI) study evaluated the performance of urinary c-glutamyltranspeptidase ( c-GTP) alkaline phosphatase NGAL Cys-C KIM-1 and IL-18 in AKI diagnosis
bull The results of four novel urine biomarkers and one plasma biomarker (urine NGAL IL-18 KIM-1 and L-FABP and plasma NGAL) were provided Of all the novel biomarkers only urine IL-18 and plasma NGAL in adults were helpful in predicting progression of AKI when measured on the day of clinical AKI diagnosis
bull Combinations of three biomarkers in adults from two different time points and combinations of two biomarkers in children from two time points were found to be able to increase the ROC for AKI up to 078
bull In summary the clinical use of single damage biomarkers in AKI prediction remains unclear because large prospective multicenter trials such as the TRIBE-AKI study (nfrac141530) have failed to demonstrate troponin-like diagnostic performance
Various clinical scenarios of AKI based onfunction damage and stress
bull Over the last decade a number of novel damage biomarkers have been evaluated for their capacity to detect kidney damage and predict the development of AKI However the relationship between decreasing function and increasing damage is not as straightforward as might be assumed
bull The characteristic pattern whereby damage precedes loss of function (panel A) may be seen in some cases of AKI and affords an opportunity to detect ldquosubclinicalrdquo AKI before function start to fall Unfortunately other patterns might also occur For example functional decline may start to occur alongside damage (panel B) and in some cases function may start to decline even before damage (panel C)
bull This makes damage markers difficult to use for predicting AKI However other markers might actually measure the ldquostressrdquo occurring at the cellular level before damage or loss of function
Paradigm shift to pre-injury phase biomarkers
bull Katz et al proposed that the pre-injury phase that leads to AKI can be described as ldquoacute kidney stressrdquo (AKS) after the report of the identification of cell cycle arrest biomarkers that signal the potential development of AKI is part of an evolution in the molecular diagnosis and understanding of AKI
bull These biomarkers are released by kidney cells along a path which may lead to AKI during a pre-injury phase
bull AKS is defined as the increased-risk phase (pre-injury phase) that leads to AKI
bull This ldquoAKSrdquo may or may not lead to damage and functional declinebull But it is the earliest possible the process of AKI can be detected
Pre-injury phase biomarkers
Stress biomarkersbull In 2013 Kashani et al reported the results of a prospective international
observational investigation (the Sapphire study) of tissue inhibitor of metalloproteinases- 2 (TIMP-2) and insulin-like growth factor-binding protein 7 (IGFBP7) in a heterogeneous group of critically ill patients [TIMP-2][IGFBP7] was significantly superior to all previously described markers of AKI (plt0002)
bull Next the Opal and Topaz study showed the cut-off value and risk assessment using the urinary[TIMP-2] [IGFBP7]
bull The urine [IGFBP7][TIMP2] biomarker is already FDA approved and commercially available in the United States
bull Falsepositive results are common and they will be magnified if the test is used inappropriately in low-risk patients In addition this biomarker should not be used in ambulatory practices and it is not beneficial in patients with established AKI
microRNAsbull microRNAs (miRNAs) are endogenous single-stranded non-coding
mRNAs of about 19-23 nucleotides bull In the past years researchers have begun to investigate the
relevance of miRNAs to AKI with many miRNAs being implicated bull Some of them contribute to pathogenesis by regulating apoptosis
and inflammation amplifying or reducing acute injury responses while others regulate fibrosis and angiogenesis participating in renal recovery or progression to fibrosis
bull Certain miRNAs have been investigated for their potential as novel biomarkers for the early detection or prognostication of AKI
Hemojuvelinbull Hemojuvelin (HJV) a glycophosphatidylinositol (GPI)- linked
membrane protein is highly expressed in liver and skeletal musclesbull The molecular weight of HJV is 42 kDa for the soluble form (sHJV)
and can be passed through glomerular filtration and reabsorbed by the renal tubules Increased iron content in the kidney and urine is observed in human and animal models of AKI and increased iron load can induce renal tubular cell injury
bull There is evidence that the increased expression of the hemojuvelin-hepcidin ferroportin pathway is an intrinsic response to iron overload conditions during AKI
bull Therefore urine HJV (uHJV) has the potential to be an early AKI biomarker in response to iron homeostasis during AKI
Combination of functional and damage biomarkers
bull While new biomarkers are being validated functional biomarkers (serum creatinine serum urea and urine output) continue to be utilized in the diagnosis and staging of AKI In the future existing or newer damage biomarkers will likely be combined with the use of functional biomarkers to enhance the ability of RIFLE AKIN
bull A study of 345 children after cardiopulmonary bypass surgery demonstrated that the composite of functional biomarker such as plasma cystatin C and urinary NGAL was superior to changes in serum creatinine to predict AKI
PROGNOSTIC BIOMARKERS
bull Most of the biomarkers described above allow early detection of acute kidney injury but do not predict severe AKI
Urinary renin and angiotensinogen
bull Urinary renin angiotensinogen and plasma NGAL may predict the development of severe AKI
bull Among 99 consecutively enrolled patients who developed AKI the ratio of urinary angiotensinogen to urinary creatinine (uAnCR expressed as ng per mg creatinine)calculated Patients with the highest uAnCR had a higher risk of worsening AKI compared with patients with the lowest uAnCR An elevated uAnCR predicted a longer hospital stay
bull Among 204 patients who developed Acute Kidney Injury Network (AKIN) stage 1 following cardiac surgery the urinary renin-to-creatinine ratio and the angiotensinogen-to-creatinine ratio predicted a composite outcome of death or AKIN stage 3 or death
Plasma NGAL
bull In a prospective cohort study in which 616 patients admitted from the emergency department were classified by clinical criteria as AKI transient azotemia stable CKD or normal kidney function plasma NGAL discriminated AKI from normal function and from transient azotemia
bull Higher concentrations of NGAL were associated with more severe AKI
Thanks for your attention

bull It was correlated with the degree of tubulointerstitial damage in a folic acid induced nephropathy
bull In ischemic and cisplatin-induced AKI L-FABP was increased in the urine before the increase in BUN
bull In cisplatin-induced AKI urinary L-FABP levels increased exponentially even in the lowest dose group as early as 2 hours whereas BUN levels increased at 48 hours
bull L-FABP was measured in 80 critically ill patients Urinary L-FABP levels in patients with septic shock were significantly higher than severe sepsis without shock Serum L-FABP levels did not have significant differences between patients with septic shock severe sepsis and healthy
bull Another study was evaluated 145 septic shock patients complicated with established AKI Urinary L-FABP measured at admission was significantly higher in the nonsurvivors of septic shock with established acute kidney injury than in the survivors
Failure of the TRIBE-AKI study
bull The Translational Research Investigating Biomarker Endpoints in AKI (TRIBE-AKI) study evaluated the performance of urinary c-glutamyltranspeptidase ( c-GTP) alkaline phosphatase NGAL Cys-C KIM-1 and IL-18 in AKI diagnosis
bull The results of four novel urine biomarkers and one plasma biomarker (urine NGAL IL-18 KIM-1 and L-FABP and plasma NGAL) were provided Of all the novel biomarkers only urine IL-18 and plasma NGAL in adults were helpful in predicting progression of AKI when measured on the day of clinical AKI diagnosis
bull Combinations of three biomarkers in adults from two different time points and combinations of two biomarkers in children from two time points were found to be able to increase the ROC for AKI up to 078
bull In summary the clinical use of single damage biomarkers in AKI prediction remains unclear because large prospective multicenter trials such as the TRIBE-AKI study (nfrac141530) have failed to demonstrate troponin-like diagnostic performance
Various clinical scenarios of AKI based onfunction damage and stress
bull Over the last decade a number of novel damage biomarkers have been evaluated for their capacity to detect kidney damage and predict the development of AKI However the relationship between decreasing function and increasing damage is not as straightforward as might be assumed
bull The characteristic pattern whereby damage precedes loss of function (panel A) may be seen in some cases of AKI and affords an opportunity to detect ldquosubclinicalrdquo AKI before function start to fall Unfortunately other patterns might also occur For example functional decline may start to occur alongside damage (panel B) and in some cases function may start to decline even before damage (panel C)
bull This makes damage markers difficult to use for predicting AKI However other markers might actually measure the ldquostressrdquo occurring at the cellular level before damage or loss of function
Paradigm shift to pre-injury phase biomarkers
bull Katz et al proposed that the pre-injury phase that leads to AKI can be described as ldquoacute kidney stressrdquo (AKS) after the report of the identification of cell cycle arrest biomarkers that signal the potential development of AKI is part of an evolution in the molecular diagnosis and understanding of AKI
bull These biomarkers are released by kidney cells along a path which may lead to AKI during a pre-injury phase
bull AKS is defined as the increased-risk phase (pre-injury phase) that leads to AKI
bull This ldquoAKSrdquo may or may not lead to damage and functional declinebull But it is the earliest possible the process of AKI can be detected
Pre-injury phase biomarkers
Stress biomarkersbull In 2013 Kashani et al reported the results of a prospective international
observational investigation (the Sapphire study) of tissue inhibitor of metalloproteinases- 2 (TIMP-2) and insulin-like growth factor-binding protein 7 (IGFBP7) in a heterogeneous group of critically ill patients [TIMP-2][IGFBP7] was significantly superior to all previously described markers of AKI (plt0002)
bull Next the Opal and Topaz study showed the cut-off value and risk assessment using the urinary[TIMP-2] [IGFBP7]
bull The urine [IGFBP7][TIMP2] biomarker is already FDA approved and commercially available in the United States
bull Falsepositive results are common and they will be magnified if the test is used inappropriately in low-risk patients In addition this biomarker should not be used in ambulatory practices and it is not beneficial in patients with established AKI
microRNAsbull microRNAs (miRNAs) are endogenous single-stranded non-coding
mRNAs of about 19-23 nucleotides bull In the past years researchers have begun to investigate the
relevance of miRNAs to AKI with many miRNAs being implicated bull Some of them contribute to pathogenesis by regulating apoptosis
and inflammation amplifying or reducing acute injury responses while others regulate fibrosis and angiogenesis participating in renal recovery or progression to fibrosis
bull Certain miRNAs have been investigated for their potential as novel biomarkers for the early detection or prognostication of AKI
Hemojuvelinbull Hemojuvelin (HJV) a glycophosphatidylinositol (GPI)- linked
membrane protein is highly expressed in liver and skeletal musclesbull The molecular weight of HJV is 42 kDa for the soluble form (sHJV)
and can be passed through glomerular filtration and reabsorbed by the renal tubules Increased iron content in the kidney and urine is observed in human and animal models of AKI and increased iron load can induce renal tubular cell injury
bull There is evidence that the increased expression of the hemojuvelin-hepcidin ferroportin pathway is an intrinsic response to iron overload conditions during AKI
bull Therefore urine HJV (uHJV) has the potential to be an early AKI biomarker in response to iron homeostasis during AKI
Combination of functional and damage biomarkers
bull While new biomarkers are being validated functional biomarkers (serum creatinine serum urea and urine output) continue to be utilized in the diagnosis and staging of AKI In the future existing or newer damage biomarkers will likely be combined with the use of functional biomarkers to enhance the ability of RIFLE AKIN
bull A study of 345 children after cardiopulmonary bypass surgery demonstrated that the composite of functional biomarker such as plasma cystatin C and urinary NGAL was superior to changes in serum creatinine to predict AKI
PROGNOSTIC BIOMARKERS
bull Most of the biomarkers described above allow early detection of acute kidney injury but do not predict severe AKI
Urinary renin and angiotensinogen
bull Urinary renin angiotensinogen and plasma NGAL may predict the development of severe AKI
bull Among 99 consecutively enrolled patients who developed AKI the ratio of urinary angiotensinogen to urinary creatinine (uAnCR expressed as ng per mg creatinine)calculated Patients with the highest uAnCR had a higher risk of worsening AKI compared with patients with the lowest uAnCR An elevated uAnCR predicted a longer hospital stay
bull Among 204 patients who developed Acute Kidney Injury Network (AKIN) stage 1 following cardiac surgery the urinary renin-to-creatinine ratio and the angiotensinogen-to-creatinine ratio predicted a composite outcome of death or AKIN stage 3 or death
Plasma NGAL
bull In a prospective cohort study in which 616 patients admitted from the emergency department were classified by clinical criteria as AKI transient azotemia stable CKD or normal kidney function plasma NGAL discriminated AKI from normal function and from transient azotemia
bull Higher concentrations of NGAL were associated with more severe AKI
Thanks for your attention

bull L-FABP was measured in 80 critically ill patients Urinary L-FABP levels in patients with septic shock were significantly higher than severe sepsis without shock Serum L-FABP levels did not have significant differences between patients with septic shock severe sepsis and healthy
bull Another study was evaluated 145 septic shock patients complicated with established AKI Urinary L-FABP measured at admission was significantly higher in the nonsurvivors of septic shock with established acute kidney injury than in the survivors
Failure of the TRIBE-AKI study
bull The Translational Research Investigating Biomarker Endpoints in AKI (TRIBE-AKI) study evaluated the performance of urinary c-glutamyltranspeptidase ( c-GTP) alkaline phosphatase NGAL Cys-C KIM-1 and IL-18 in AKI diagnosis
bull The results of four novel urine biomarkers and one plasma biomarker (urine NGAL IL-18 KIM-1 and L-FABP and plasma NGAL) were provided Of all the novel biomarkers only urine IL-18 and plasma NGAL in adults were helpful in predicting progression of AKI when measured on the day of clinical AKI diagnosis
bull Combinations of three biomarkers in adults from two different time points and combinations of two biomarkers in children from two time points were found to be able to increase the ROC for AKI up to 078
bull In summary the clinical use of single damage biomarkers in AKI prediction remains unclear because large prospective multicenter trials such as the TRIBE-AKI study (nfrac141530) have failed to demonstrate troponin-like diagnostic performance
Various clinical scenarios of AKI based onfunction damage and stress
bull Over the last decade a number of novel damage biomarkers have been evaluated for their capacity to detect kidney damage and predict the development of AKI However the relationship between decreasing function and increasing damage is not as straightforward as might be assumed
bull The characteristic pattern whereby damage precedes loss of function (panel A) may be seen in some cases of AKI and affords an opportunity to detect ldquosubclinicalrdquo AKI before function start to fall Unfortunately other patterns might also occur For example functional decline may start to occur alongside damage (panel B) and in some cases function may start to decline even before damage (panel C)
bull This makes damage markers difficult to use for predicting AKI However other markers might actually measure the ldquostressrdquo occurring at the cellular level before damage or loss of function
Paradigm shift to pre-injury phase biomarkers
bull Katz et al proposed that the pre-injury phase that leads to AKI can be described as ldquoacute kidney stressrdquo (AKS) after the report of the identification of cell cycle arrest biomarkers that signal the potential development of AKI is part of an evolution in the molecular diagnosis and understanding of AKI
bull These biomarkers are released by kidney cells along a path which may lead to AKI during a pre-injury phase
bull AKS is defined as the increased-risk phase (pre-injury phase) that leads to AKI
bull This ldquoAKSrdquo may or may not lead to damage and functional declinebull But it is the earliest possible the process of AKI can be detected
Pre-injury phase biomarkers
Stress biomarkersbull In 2013 Kashani et al reported the results of a prospective international
observational investigation (the Sapphire study) of tissue inhibitor of metalloproteinases- 2 (TIMP-2) and insulin-like growth factor-binding protein 7 (IGFBP7) in a heterogeneous group of critically ill patients [TIMP-2][IGFBP7] was significantly superior to all previously described markers of AKI (plt0002)
bull Next the Opal and Topaz study showed the cut-off value and risk assessment using the urinary[TIMP-2] [IGFBP7]
bull The urine [IGFBP7][TIMP2] biomarker is already FDA approved and commercially available in the United States
bull Falsepositive results are common and they will be magnified if the test is used inappropriately in low-risk patients In addition this biomarker should not be used in ambulatory practices and it is not beneficial in patients with established AKI
microRNAsbull microRNAs (miRNAs) are endogenous single-stranded non-coding
mRNAs of about 19-23 nucleotides bull In the past years researchers have begun to investigate the
relevance of miRNAs to AKI with many miRNAs being implicated bull Some of them contribute to pathogenesis by regulating apoptosis
and inflammation amplifying or reducing acute injury responses while others regulate fibrosis and angiogenesis participating in renal recovery or progression to fibrosis
bull Certain miRNAs have been investigated for their potential as novel biomarkers for the early detection or prognostication of AKI
Hemojuvelinbull Hemojuvelin (HJV) a glycophosphatidylinositol (GPI)- linked
membrane protein is highly expressed in liver and skeletal musclesbull The molecular weight of HJV is 42 kDa for the soluble form (sHJV)
and can be passed through glomerular filtration and reabsorbed by the renal tubules Increased iron content in the kidney and urine is observed in human and animal models of AKI and increased iron load can induce renal tubular cell injury
bull There is evidence that the increased expression of the hemojuvelin-hepcidin ferroportin pathway is an intrinsic response to iron overload conditions during AKI
bull Therefore urine HJV (uHJV) has the potential to be an early AKI biomarker in response to iron homeostasis during AKI
Combination of functional and damage biomarkers
bull While new biomarkers are being validated functional biomarkers (serum creatinine serum urea and urine output) continue to be utilized in the diagnosis and staging of AKI In the future existing or newer damage biomarkers will likely be combined with the use of functional biomarkers to enhance the ability of RIFLE AKIN
bull A study of 345 children after cardiopulmonary bypass surgery demonstrated that the composite of functional biomarker such as plasma cystatin C and urinary NGAL was superior to changes in serum creatinine to predict AKI
PROGNOSTIC BIOMARKERS
bull Most of the biomarkers described above allow early detection of acute kidney injury but do not predict severe AKI
Urinary renin and angiotensinogen
bull Urinary renin angiotensinogen and plasma NGAL may predict the development of severe AKI
bull Among 99 consecutively enrolled patients who developed AKI the ratio of urinary angiotensinogen to urinary creatinine (uAnCR expressed as ng per mg creatinine)calculated Patients with the highest uAnCR had a higher risk of worsening AKI compared with patients with the lowest uAnCR An elevated uAnCR predicted a longer hospital stay
bull Among 204 patients who developed Acute Kidney Injury Network (AKIN) stage 1 following cardiac surgery the urinary renin-to-creatinine ratio and the angiotensinogen-to-creatinine ratio predicted a composite outcome of death or AKIN stage 3 or death
Plasma NGAL
bull In a prospective cohort study in which 616 patients admitted from the emergency department were classified by clinical criteria as AKI transient azotemia stable CKD or normal kidney function plasma NGAL discriminated AKI from normal function and from transient azotemia
bull Higher concentrations of NGAL were associated with more severe AKI
Thanks for your attention

Failure of the TRIBE-AKI study
bull The Translational Research Investigating Biomarker Endpoints in AKI (TRIBE-AKI) study evaluated the performance of urinary c-glutamyltranspeptidase ( c-GTP) alkaline phosphatase NGAL Cys-C KIM-1 and IL-18 in AKI diagnosis
bull The results of four novel urine biomarkers and one plasma biomarker (urine NGAL IL-18 KIM-1 and L-FABP and plasma NGAL) were provided Of all the novel biomarkers only urine IL-18 and plasma NGAL in adults were helpful in predicting progression of AKI when measured on the day of clinical AKI diagnosis
bull Combinations of three biomarkers in adults from two different time points and combinations of two biomarkers in children from two time points were found to be able to increase the ROC for AKI up to 078
bull In summary the clinical use of single damage biomarkers in AKI prediction remains unclear because large prospective multicenter trials such as the TRIBE-AKI study (nfrac141530) have failed to demonstrate troponin-like diagnostic performance
Various clinical scenarios of AKI based onfunction damage and stress
bull Over the last decade a number of novel damage biomarkers have been evaluated for their capacity to detect kidney damage and predict the development of AKI However the relationship between decreasing function and increasing damage is not as straightforward as might be assumed
bull The characteristic pattern whereby damage precedes loss of function (panel A) may be seen in some cases of AKI and affords an opportunity to detect ldquosubclinicalrdquo AKI before function start to fall Unfortunately other patterns might also occur For example functional decline may start to occur alongside damage (panel B) and in some cases function may start to decline even before damage (panel C)
bull This makes damage markers difficult to use for predicting AKI However other markers might actually measure the ldquostressrdquo occurring at the cellular level before damage or loss of function
Paradigm shift to pre-injury phase biomarkers
bull Katz et al proposed that the pre-injury phase that leads to AKI can be described as ldquoacute kidney stressrdquo (AKS) after the report of the identification of cell cycle arrest biomarkers that signal the potential development of AKI is part of an evolution in the molecular diagnosis and understanding of AKI
bull These biomarkers are released by kidney cells along a path which may lead to AKI during a pre-injury phase
bull AKS is defined as the increased-risk phase (pre-injury phase) that leads to AKI
bull This ldquoAKSrdquo may or may not lead to damage and functional declinebull But it is the earliest possible the process of AKI can be detected
Pre-injury phase biomarkers
Stress biomarkersbull In 2013 Kashani et al reported the results of a prospective international
observational investigation (the Sapphire study) of tissue inhibitor of metalloproteinases- 2 (TIMP-2) and insulin-like growth factor-binding protein 7 (IGFBP7) in a heterogeneous group of critically ill patients [TIMP-2][IGFBP7] was significantly superior to all previously described markers of AKI (plt0002)
bull Next the Opal and Topaz study showed the cut-off value and risk assessment using the urinary[TIMP-2] [IGFBP7]
bull The urine [IGFBP7][TIMP2] biomarker is already FDA approved and commercially available in the United States
bull Falsepositive results are common and they will be magnified if the test is used inappropriately in low-risk patients In addition this biomarker should not be used in ambulatory practices and it is not beneficial in patients with established AKI
microRNAsbull microRNAs (miRNAs) are endogenous single-stranded non-coding
mRNAs of about 19-23 nucleotides bull In the past years researchers have begun to investigate the
relevance of miRNAs to AKI with many miRNAs being implicated bull Some of them contribute to pathogenesis by regulating apoptosis
and inflammation amplifying or reducing acute injury responses while others regulate fibrosis and angiogenesis participating in renal recovery or progression to fibrosis
bull Certain miRNAs have been investigated for their potential as novel biomarkers for the early detection or prognostication of AKI
Hemojuvelinbull Hemojuvelin (HJV) a glycophosphatidylinositol (GPI)- linked
membrane protein is highly expressed in liver and skeletal musclesbull The molecular weight of HJV is 42 kDa for the soluble form (sHJV)
and can be passed through glomerular filtration and reabsorbed by the renal tubules Increased iron content in the kidney and urine is observed in human and animal models of AKI and increased iron load can induce renal tubular cell injury
bull There is evidence that the increased expression of the hemojuvelin-hepcidin ferroportin pathway is an intrinsic response to iron overload conditions during AKI
bull Therefore urine HJV (uHJV) has the potential to be an early AKI biomarker in response to iron homeostasis during AKI
Combination of functional and damage biomarkers
bull While new biomarkers are being validated functional biomarkers (serum creatinine serum urea and urine output) continue to be utilized in the diagnosis and staging of AKI In the future existing or newer damage biomarkers will likely be combined with the use of functional biomarkers to enhance the ability of RIFLE AKIN
bull A study of 345 children after cardiopulmonary bypass surgery demonstrated that the composite of functional biomarker such as plasma cystatin C and urinary NGAL was superior to changes in serum creatinine to predict AKI
PROGNOSTIC BIOMARKERS
bull Most of the biomarkers described above allow early detection of acute kidney injury but do not predict severe AKI
Urinary renin and angiotensinogen
bull Urinary renin angiotensinogen and plasma NGAL may predict the development of severe AKI
bull Among 99 consecutively enrolled patients who developed AKI the ratio of urinary angiotensinogen to urinary creatinine (uAnCR expressed as ng per mg creatinine)calculated Patients with the highest uAnCR had a higher risk of worsening AKI compared with patients with the lowest uAnCR An elevated uAnCR predicted a longer hospital stay
bull Among 204 patients who developed Acute Kidney Injury Network (AKIN) stage 1 following cardiac surgery the urinary renin-to-creatinine ratio and the angiotensinogen-to-creatinine ratio predicted a composite outcome of death or AKIN stage 3 or death
Plasma NGAL
bull In a prospective cohort study in which 616 patients admitted from the emergency department were classified by clinical criteria as AKI transient azotemia stable CKD or normal kidney function plasma NGAL discriminated AKI from normal function and from transient azotemia
bull Higher concentrations of NGAL were associated with more severe AKI
Thanks for your attention

Various clinical scenarios of AKI based onfunction damage and stress
bull Over the last decade a number of novel damage biomarkers have been evaluated for their capacity to detect kidney damage and predict the development of AKI However the relationship between decreasing function and increasing damage is not as straightforward as might be assumed
bull The characteristic pattern whereby damage precedes loss of function (panel A) may be seen in some cases of AKI and affords an opportunity to detect ldquosubclinicalrdquo AKI before function start to fall Unfortunately other patterns might also occur For example functional decline may start to occur alongside damage (panel B) and in some cases function may start to decline even before damage (panel C)
bull This makes damage markers difficult to use for predicting AKI However other markers might actually measure the ldquostressrdquo occurring at the cellular level before damage or loss of function
Paradigm shift to pre-injury phase biomarkers
bull Katz et al proposed that the pre-injury phase that leads to AKI can be described as ldquoacute kidney stressrdquo (AKS) after the report of the identification of cell cycle arrest biomarkers that signal the potential development of AKI is part of an evolution in the molecular diagnosis and understanding of AKI
bull These biomarkers are released by kidney cells along a path which may lead to AKI during a pre-injury phase
bull AKS is defined as the increased-risk phase (pre-injury phase) that leads to AKI
bull This ldquoAKSrdquo may or may not lead to damage and functional declinebull But it is the earliest possible the process of AKI can be detected
Pre-injury phase biomarkers
Stress biomarkersbull In 2013 Kashani et al reported the results of a prospective international
observational investigation (the Sapphire study) of tissue inhibitor of metalloproteinases- 2 (TIMP-2) and insulin-like growth factor-binding protein 7 (IGFBP7) in a heterogeneous group of critically ill patients [TIMP-2][IGFBP7] was significantly superior to all previously described markers of AKI (plt0002)
bull Next the Opal and Topaz study showed the cut-off value and risk assessment using the urinary[TIMP-2] [IGFBP7]
bull The urine [IGFBP7][TIMP2] biomarker is already FDA approved and commercially available in the United States
bull Falsepositive results are common and they will be magnified if the test is used inappropriately in low-risk patients In addition this biomarker should not be used in ambulatory practices and it is not beneficial in patients with established AKI
microRNAsbull microRNAs (miRNAs) are endogenous single-stranded non-coding
mRNAs of about 19-23 nucleotides bull In the past years researchers have begun to investigate the
relevance of miRNAs to AKI with many miRNAs being implicated bull Some of them contribute to pathogenesis by regulating apoptosis
and inflammation amplifying or reducing acute injury responses while others regulate fibrosis and angiogenesis participating in renal recovery or progression to fibrosis
bull Certain miRNAs have been investigated for their potential as novel biomarkers for the early detection or prognostication of AKI
Hemojuvelinbull Hemojuvelin (HJV) a glycophosphatidylinositol (GPI)- linked
membrane protein is highly expressed in liver and skeletal musclesbull The molecular weight of HJV is 42 kDa for the soluble form (sHJV)
and can be passed through glomerular filtration and reabsorbed by the renal tubules Increased iron content in the kidney and urine is observed in human and animal models of AKI and increased iron load can induce renal tubular cell injury
bull There is evidence that the increased expression of the hemojuvelin-hepcidin ferroportin pathway is an intrinsic response to iron overload conditions during AKI
bull Therefore urine HJV (uHJV) has the potential to be an early AKI biomarker in response to iron homeostasis during AKI
Combination of functional and damage biomarkers
bull While new biomarkers are being validated functional biomarkers (serum creatinine serum urea and urine output) continue to be utilized in the diagnosis and staging of AKI In the future existing or newer damage biomarkers will likely be combined with the use of functional biomarkers to enhance the ability of RIFLE AKIN
bull A study of 345 children after cardiopulmonary bypass surgery demonstrated that the composite of functional biomarker such as plasma cystatin C and urinary NGAL was superior to changes in serum creatinine to predict AKI
PROGNOSTIC BIOMARKERS
bull Most of the biomarkers described above allow early detection of acute kidney injury but do not predict severe AKI
Urinary renin and angiotensinogen
bull Urinary renin angiotensinogen and plasma NGAL may predict the development of severe AKI
bull Among 99 consecutively enrolled patients who developed AKI the ratio of urinary angiotensinogen to urinary creatinine (uAnCR expressed as ng per mg creatinine)calculated Patients with the highest uAnCR had a higher risk of worsening AKI compared with patients with the lowest uAnCR An elevated uAnCR predicted a longer hospital stay
bull Among 204 patients who developed Acute Kidney Injury Network (AKIN) stage 1 following cardiac surgery the urinary renin-to-creatinine ratio and the angiotensinogen-to-creatinine ratio predicted a composite outcome of death or AKIN stage 3 or death
Plasma NGAL
bull In a prospective cohort study in which 616 patients admitted from the emergency department were classified by clinical criteria as AKI transient azotemia stable CKD or normal kidney function plasma NGAL discriminated AKI from normal function and from transient azotemia
bull Higher concentrations of NGAL were associated with more severe AKI
Thanks for your attention

Paradigm shift to pre-injury phase biomarkers
bull Katz et al proposed that the pre-injury phase that leads to AKI can be described as ldquoacute kidney stressrdquo (AKS) after the report of the identification of cell cycle arrest biomarkers that signal the potential development of AKI is part of an evolution in the molecular diagnosis and understanding of AKI
bull These biomarkers are released by kidney cells along a path which may lead to AKI during a pre-injury phase
bull AKS is defined as the increased-risk phase (pre-injury phase) that leads to AKI
bull This ldquoAKSrdquo may or may not lead to damage and functional declinebull But it is the earliest possible the process of AKI can be detected
Pre-injury phase biomarkers
Stress biomarkersbull In 2013 Kashani et al reported the results of a prospective international
observational investigation (the Sapphire study) of tissue inhibitor of metalloproteinases- 2 (TIMP-2) and insulin-like growth factor-binding protein 7 (IGFBP7) in a heterogeneous group of critically ill patients [TIMP-2][IGFBP7] was significantly superior to all previously described markers of AKI (plt0002)
bull Next the Opal and Topaz study showed the cut-off value and risk assessment using the urinary[TIMP-2] [IGFBP7]
bull The urine [IGFBP7][TIMP2] biomarker is already FDA approved and commercially available in the United States
bull Falsepositive results are common and they will be magnified if the test is used inappropriately in low-risk patients In addition this biomarker should not be used in ambulatory practices and it is not beneficial in patients with established AKI
microRNAsbull microRNAs (miRNAs) are endogenous single-stranded non-coding
mRNAs of about 19-23 nucleotides bull In the past years researchers have begun to investigate the
relevance of miRNAs to AKI with many miRNAs being implicated bull Some of them contribute to pathogenesis by regulating apoptosis
and inflammation amplifying or reducing acute injury responses while others regulate fibrosis and angiogenesis participating in renal recovery or progression to fibrosis
bull Certain miRNAs have been investigated for their potential as novel biomarkers for the early detection or prognostication of AKI
Hemojuvelinbull Hemojuvelin (HJV) a glycophosphatidylinositol (GPI)- linked
membrane protein is highly expressed in liver and skeletal musclesbull The molecular weight of HJV is 42 kDa for the soluble form (sHJV)
and can be passed through glomerular filtration and reabsorbed by the renal tubules Increased iron content in the kidney and urine is observed in human and animal models of AKI and increased iron load can induce renal tubular cell injury
bull There is evidence that the increased expression of the hemojuvelin-hepcidin ferroportin pathway is an intrinsic response to iron overload conditions during AKI
bull Therefore urine HJV (uHJV) has the potential to be an early AKI biomarker in response to iron homeostasis during AKI
Combination of functional and damage biomarkers
bull While new biomarkers are being validated functional biomarkers (serum creatinine serum urea and urine output) continue to be utilized in the diagnosis and staging of AKI In the future existing or newer damage biomarkers will likely be combined with the use of functional biomarkers to enhance the ability of RIFLE AKIN
bull A study of 345 children after cardiopulmonary bypass surgery demonstrated that the composite of functional biomarker such as plasma cystatin C and urinary NGAL was superior to changes in serum creatinine to predict AKI
PROGNOSTIC BIOMARKERS
bull Most of the biomarkers described above allow early detection of acute kidney injury but do not predict severe AKI
Urinary renin and angiotensinogen
bull Urinary renin angiotensinogen and plasma NGAL may predict the development of severe AKI
bull Among 99 consecutively enrolled patients who developed AKI the ratio of urinary angiotensinogen to urinary creatinine (uAnCR expressed as ng per mg creatinine)calculated Patients with the highest uAnCR had a higher risk of worsening AKI compared with patients with the lowest uAnCR An elevated uAnCR predicted a longer hospital stay
bull Among 204 patients who developed Acute Kidney Injury Network (AKIN) stage 1 following cardiac surgery the urinary renin-to-creatinine ratio and the angiotensinogen-to-creatinine ratio predicted a composite outcome of death or AKIN stage 3 or death
Plasma NGAL
bull In a prospective cohort study in which 616 patients admitted from the emergency department were classified by clinical criteria as AKI transient azotemia stable CKD or normal kidney function plasma NGAL discriminated AKI from normal function and from transient azotemia
bull Higher concentrations of NGAL were associated with more severe AKI
Thanks for your attention
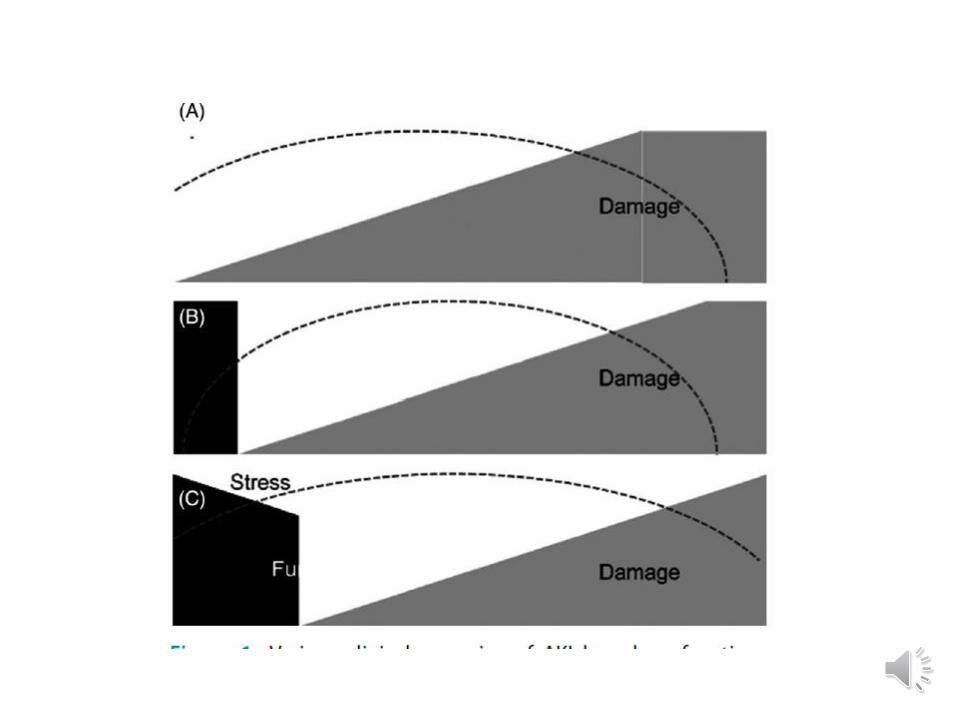
Pre-injury phase biomarkers
Stress biomarkersbull In 2013 Kashani et al reported the results of a prospective international
observational investigation (the Sapphire study) of tissue inhibitor of metalloproteinases- 2 (TIMP-2) and insulin-like growth factor-binding protein 7 (IGFBP7) in a heterogeneous group of critically ill patients [TIMP-2][IGFBP7] was significantly superior to all previously described markers of AKI (plt0002)
bull Next the Opal and Topaz study showed the cut-off value and risk assessment using the urinary[TIMP-2] [IGFBP7]
bull The urine [IGFBP7][TIMP2] biomarker is already FDA approved and commercially available in the United States
bull Falsepositive results are common and they will be magnified if the test is used inappropriately in low-risk patients In addition this biomarker should not be used in ambulatory practices and it is not beneficial in patients with established AKI
microRNAsbull microRNAs (miRNAs) are endogenous single-stranded non-coding
mRNAs of about 19-23 nucleotides bull In the past years researchers have begun to investigate the
relevance of miRNAs to AKI with many miRNAs being implicated bull Some of them contribute to pathogenesis by regulating apoptosis
and inflammation amplifying or reducing acute injury responses while others regulate fibrosis and angiogenesis participating in renal recovery or progression to fibrosis
bull Certain miRNAs have been investigated for their potential as novel biomarkers for the early detection or prognostication of AKI
Hemojuvelinbull Hemojuvelin (HJV) a glycophosphatidylinositol (GPI)- linked
membrane protein is highly expressed in liver and skeletal musclesbull The molecular weight of HJV is 42 kDa for the soluble form (sHJV)
and can be passed through glomerular filtration and reabsorbed by the renal tubules Increased iron content in the kidney and urine is observed in human and animal models of AKI and increased iron load can induce renal tubular cell injury
bull There is evidence that the increased expression of the hemojuvelin-hepcidin ferroportin pathway is an intrinsic response to iron overload conditions during AKI
bull Therefore urine HJV (uHJV) has the potential to be an early AKI biomarker in response to iron homeostasis during AKI
Combination of functional and damage biomarkers
bull While new biomarkers are being validated functional biomarkers (serum creatinine serum urea and urine output) continue to be utilized in the diagnosis and staging of AKI In the future existing or newer damage biomarkers will likely be combined with the use of functional biomarkers to enhance the ability of RIFLE AKIN
bull A study of 345 children after cardiopulmonary bypass surgery demonstrated that the composite of functional biomarker such as plasma cystatin C and urinary NGAL was superior to changes in serum creatinine to predict AKI
PROGNOSTIC BIOMARKERS
bull Most of the biomarkers described above allow early detection of acute kidney injury but do not predict severe AKI
Urinary renin and angiotensinogen
bull Urinary renin angiotensinogen and plasma NGAL may predict the development of severe AKI
bull Among 99 consecutively enrolled patients who developed AKI the ratio of urinary angiotensinogen to urinary creatinine (uAnCR expressed as ng per mg creatinine)calculated Patients with the highest uAnCR had a higher risk of worsening AKI compared with patients with the lowest uAnCR An elevated uAnCR predicted a longer hospital stay
bull Among 204 patients who developed Acute Kidney Injury Network (AKIN) stage 1 following cardiac surgery the urinary renin-to-creatinine ratio and the angiotensinogen-to-creatinine ratio predicted a composite outcome of death or AKIN stage 3 or death
Plasma NGAL
bull In a prospective cohort study in which 616 patients admitted from the emergency department were classified by clinical criteria as AKI transient azotemia stable CKD or normal kidney function plasma NGAL discriminated AKI from normal function and from transient azotemia
bull Higher concentrations of NGAL were associated with more severe AKI
Thanks for your attention
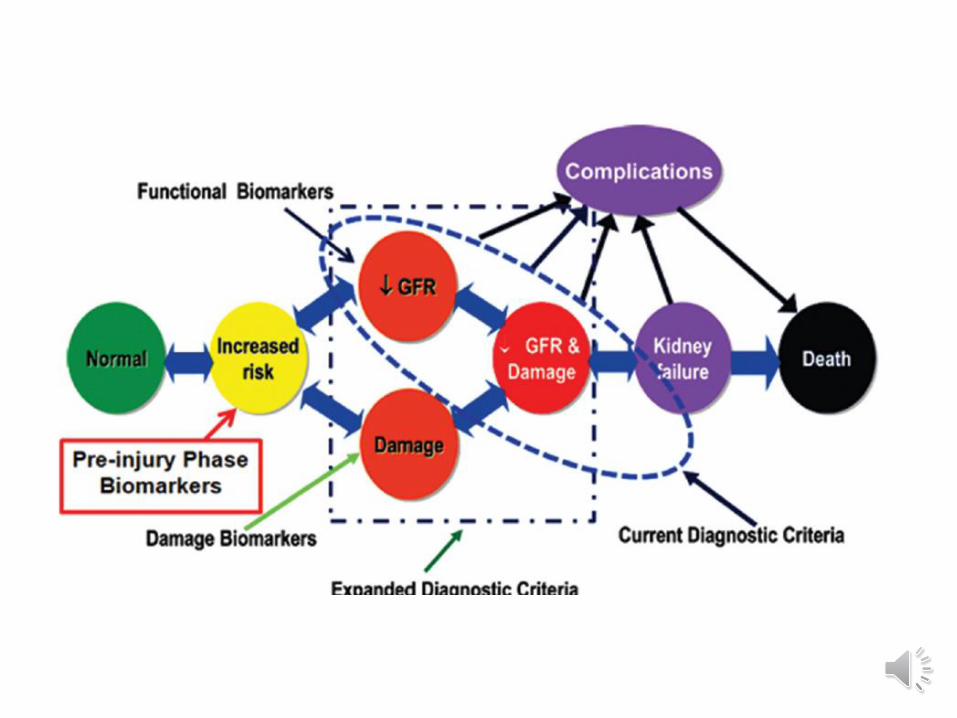
microRNAsbull microRNAs (miRNAs) are endogenous single-stranded non-coding
mRNAs of about 19-23 nucleotides bull In the past years researchers have begun to investigate the
relevance of miRNAs to AKI with many miRNAs being implicated bull Some of them contribute to pathogenesis by regulating apoptosis
and inflammation amplifying or reducing acute injury responses while others regulate fibrosis and angiogenesis participating in renal recovery or progression to fibrosis
bull Certain miRNAs have been investigated for their potential as novel biomarkers for the early detection or prognostication of AKI
Hemojuvelinbull Hemojuvelin (HJV) a glycophosphatidylinositol (GPI)- linked
membrane protein is highly expressed in liver and skeletal musclesbull The molecular weight of HJV is 42 kDa for the soluble form (sHJV)
and can be passed through glomerular filtration and reabsorbed by the renal tubules Increased iron content in the kidney and urine is observed in human and animal models of AKI and increased iron load can induce renal tubular cell injury
bull There is evidence that the increased expression of the hemojuvelin-hepcidin ferroportin pathway is an intrinsic response to iron overload conditions during AKI
bull Therefore urine HJV (uHJV) has the potential to be an early AKI biomarker in response to iron homeostasis during AKI
Combination of functional and damage biomarkers
bull While new biomarkers are being validated functional biomarkers (serum creatinine serum urea and urine output) continue to be utilized in the diagnosis and staging of AKI In the future existing or newer damage biomarkers will likely be combined with the use of functional biomarkers to enhance the ability of RIFLE AKIN
bull A study of 345 children after cardiopulmonary bypass surgery demonstrated that the composite of functional biomarker such as plasma cystatin C and urinary NGAL was superior to changes in serum creatinine to predict AKI
PROGNOSTIC BIOMARKERS
bull Most of the biomarkers described above allow early detection of acute kidney injury but do not predict severe AKI
Urinary renin and angiotensinogen
bull Urinary renin angiotensinogen and plasma NGAL may predict the development of severe AKI
bull Among 99 consecutively enrolled patients who developed AKI the ratio of urinary angiotensinogen to urinary creatinine (uAnCR expressed as ng per mg creatinine)calculated Patients with the highest uAnCR had a higher risk of worsening AKI compared with patients with the lowest uAnCR An elevated uAnCR predicted a longer hospital stay
bull Among 204 patients who developed Acute Kidney Injury Network (AKIN) stage 1 following cardiac surgery the urinary renin-to-creatinine ratio and the angiotensinogen-to-creatinine ratio predicted a composite outcome of death or AKIN stage 3 or death
Plasma NGAL
bull In a prospective cohort study in which 616 patients admitted from the emergency department were classified by clinical criteria as AKI transient azotemia stable CKD or normal kidney function plasma NGAL discriminated AKI from normal function and from transient azotemia
bull Higher concentrations of NGAL were associated with more severe AKI
Thanks for your attention

Hemojuvelinbull Hemojuvelin (HJV) a glycophosphatidylinositol (GPI)- linked
membrane protein is highly expressed in liver and skeletal musclesbull The molecular weight of HJV is 42 kDa for the soluble form (sHJV)
and can be passed through glomerular filtration and reabsorbed by the renal tubules Increased iron content in the kidney and urine is observed in human and animal models of AKI and increased iron load can induce renal tubular cell injury
bull There is evidence that the increased expression of the hemojuvelin-hepcidin ferroportin pathway is an intrinsic response to iron overload conditions during AKI
bull Therefore urine HJV (uHJV) has the potential to be an early AKI biomarker in response to iron homeostasis during AKI
Combination of functional and damage biomarkers
bull While new biomarkers are being validated functional biomarkers (serum creatinine serum urea and urine output) continue to be utilized in the diagnosis and staging of AKI In the future existing or newer damage biomarkers will likely be combined with the use of functional biomarkers to enhance the ability of RIFLE AKIN
bull A study of 345 children after cardiopulmonary bypass surgery demonstrated that the composite of functional biomarker such as plasma cystatin C and urinary NGAL was superior to changes in serum creatinine to predict AKI
PROGNOSTIC BIOMARKERS
bull Most of the biomarkers described above allow early detection of acute kidney injury but do not predict severe AKI
Urinary renin and angiotensinogen
bull Urinary renin angiotensinogen and plasma NGAL may predict the development of severe AKI
bull Among 99 consecutively enrolled patients who developed AKI the ratio of urinary angiotensinogen to urinary creatinine (uAnCR expressed as ng per mg creatinine)calculated Patients with the highest uAnCR had a higher risk of worsening AKI compared with patients with the lowest uAnCR An elevated uAnCR predicted a longer hospital stay
bull Among 204 patients who developed Acute Kidney Injury Network (AKIN) stage 1 following cardiac surgery the urinary renin-to-creatinine ratio and the angiotensinogen-to-creatinine ratio predicted a composite outcome of death or AKIN stage 3 or death
Plasma NGAL
bull In a prospective cohort study in which 616 patients admitted from the emergency department were classified by clinical criteria as AKI transient azotemia stable CKD or normal kidney function plasma NGAL discriminated AKI from normal function and from transient azotemia
bull Higher concentrations of NGAL were associated with more severe AKI
Thanks for your attention
Combination of functional and damage biomarkers
bull While new biomarkers are being validated functional biomarkers (serum creatinine serum urea and urine output) continue to be utilized in the diagnosis and staging of AKI In the future existing or newer damage biomarkers will likely be combined with the use of functional biomarkers to enhance the ability of RIFLE AKIN
bull A study of 345 children after cardiopulmonary bypass surgery demonstrated that the composite of functional biomarker such as plasma cystatin C and urinary NGAL was superior to changes in serum creatinine to predict AKI
PROGNOSTIC BIOMARKERS
bull Most of the biomarkers described above allow early detection of acute kidney injury but do not predict severe AKI
Urinary renin and angiotensinogen
bull Urinary renin angiotensinogen and plasma NGAL may predict the development of severe AKI
bull Among 99 consecutively enrolled patients who developed AKI the ratio of urinary angiotensinogen to urinary creatinine (uAnCR expressed as ng per mg creatinine)calculated Patients with the highest uAnCR had a higher risk of worsening AKI compared with patients with the lowest uAnCR An elevated uAnCR predicted a longer hospital stay
bull Among 204 patients who developed Acute Kidney Injury Network (AKIN) stage 1 following cardiac surgery the urinary renin-to-creatinine ratio and the angiotensinogen-to-creatinine ratio predicted a composite outcome of death or AKIN stage 3 or death
Plasma NGAL
bull In a prospective cohort study in which 616 patients admitted from the emergency department were classified by clinical criteria as AKI transient azotemia stable CKD or normal kidney function plasma NGAL discriminated AKI from normal function and from transient azotemia
bull Higher concentrations of NGAL were associated with more severe AKI
Thanks for your attention

PROGNOSTIC BIOMARKERS
bull Most of the biomarkers described above allow early detection of acute kidney injury but do not predict severe AKI
Urinary renin and angiotensinogen
bull Urinary renin angiotensinogen and plasma NGAL may predict the development of severe AKI
bull Among 99 consecutively enrolled patients who developed AKI the ratio of urinary angiotensinogen to urinary creatinine (uAnCR expressed as ng per mg creatinine)calculated Patients with the highest uAnCR had a higher risk of worsening AKI compared with patients with the lowest uAnCR An elevated uAnCR predicted a longer hospital stay
bull Among 204 patients who developed Acute Kidney Injury Network (AKIN) stage 1 following cardiac surgery the urinary renin-to-creatinine ratio and the angiotensinogen-to-creatinine ratio predicted a composite outcome of death or AKIN stage 3 or death
Plasma NGAL
bull In a prospective cohort study in which 616 patients admitted from the emergency department were classified by clinical criteria as AKI transient azotemia stable CKD or normal kidney function plasma NGAL discriminated AKI from normal function and from transient azotemia
bull Higher concentrations of NGAL were associated with more severe AKI
Thanks for your attention

Urinary renin and angiotensinogen
bull Urinary renin angiotensinogen and plasma NGAL may predict the development of severe AKI
bull Among 99 consecutively enrolled patients who developed AKI the ratio of urinary angiotensinogen to urinary creatinine (uAnCR expressed as ng per mg creatinine)calculated Patients with the highest uAnCR had a higher risk of worsening AKI compared with patients with the lowest uAnCR An elevated uAnCR predicted a longer hospital stay
bull Among 204 patients who developed Acute Kidney Injury Network (AKIN) stage 1 following cardiac surgery the urinary renin-to-creatinine ratio and the angiotensinogen-to-creatinine ratio predicted a composite outcome of death or AKIN stage 3 or death
Plasma NGAL
bull In a prospective cohort study in which 616 patients admitted from the emergency department were classified by clinical criteria as AKI transient azotemia stable CKD or normal kidney function plasma NGAL discriminated AKI from normal function and from transient azotemia
bull Higher concentrations of NGAL were associated with more severe AKI
Thanks for your attention

Plasma NGAL
bull In a prospective cohort study in which 616 patients admitted from the emergency department were classified by clinical criteria as AKI transient azotemia stable CKD or normal kidney function plasma NGAL discriminated AKI from normal function and from transient azotemia
bull Higher concentrations of NGAL were associated with more severe AKI
Thanks for your attention

Thanks for your attention
Related Documents