Platinum Priority – Prostate Cancer Editorial by Manfred P. Wirth and Michael Froehner on pp. 953–954 of this issue Early Complication Rates in a Single-Surgeon Series of 2500 Robotic-Assisted Radical Prostatectomies: Report Applying a Standardized Grading System Rafael F. Coelho a,b,c , Kenneth J. Palmer a,b , Bernardo Rocco a,b,d , Ravendra R. Moniz e , Sanket Chauhan a,b , Marcelo A. Orvieto a,b , Geoff Coughlin a,b , Vipul R. Patel a,b, * a Global Robotics Institute, Florida Hospital Celebration Health, Celebration, Florida, USA b University of Central Florida School of Medicine, Orlando, Florida, USA c Hospital das Clinicas da Faculdade de Medicina da Universidade de Sa˜o Paulo, Divisa˜o de Urologia, Sa˜o Paulo, Brazil d Divisione di Urologia, Istituto Europeo di Oncologia, Milan, Italy e Division of Urology, Faculty of Medical Sciences Santa Casa, Sa˜o Paulo, Brazil EUROPEAN UROLOGY 57 (2010) 945–952 available at www.sciencedirect.com journal homepage: www.europeanurology.com Article info Article history: Received 12 December 2009 Accepted February 3, 2010 Published online ahead of print on February 13, 2010 Keywords: Prostatectomy Complications Robotics Prostatic neoplasm Abstract Background: Perioperative complications following robotic-assisted radical prostatectomy (RARP) have been previously reported in recent series. Few studies, however, have used standardized systems to classify surgical complications, and that inconsistency has hampered accurate comparisons between different series or surgical approaches. Objective: To assess trends in the incidence and to classify perioperative surgical complications following RARP in 2500 consecutive patients. Design, setting, and participants: We analyzed 2500 patients who underwent RARP for treat- ment of clinically localized prostate cancer (PCa) from August 2002 to February 2009. Data were prospectively collected in a customized database and retrospectively analyzed. Intervention: All patients underwent RARP performed by a single surgeon. Measurements: The data were collected prospectively in a customized database. Complica- tions were classified using the Clavien grading system. To evaluate trends regarding complica- tions and radiologic anastomotic leaks, we compared eight groups of 300 patients each, categorized according the surgeon’s experience (number of cases). Results and limitations: Our median operative time was 90 min (interquartile range [IQR]: 75– 100 min). The median estimated blood loss was 100 ml (IQR:100–150 ml). Our conversion rate was 0.08%, comprising two procedures converted to standard laparoscopy due to robot malfunc- tion. One hundred and forty complications were observed in 127 patients (5.08%). The following percentages of patients presented graded complications: grade 1, 2.24%; grade 2, 1.8%; grade 3a, 0.08%; grade 3b, 0.48%; grade 4a, 0.40%. There were no cases of multiple organ dysfunction or death (grades 4b and 5). There were significant decreases in the overall complication rates ( p = 0.0034) and in the number of anastomotic leaks ( p < 0.001) as the surgeon’s experience increased. Conclusions: RARP is a safe option for treatment of clinically localized PCa, presenting low complication rates in experienced hands. Although the robotic system provides the surgeon with enhanced vision and dexterity, proficiency is only accomplished with consistent surgical volume; complication rates demonstrated a tendency to decrease as the surgeon’s experience increased. # 2010 European Association of Urology. Published by Elsevier B.V. All rights reserved. * Corresponding author. Global Robotics Institute, 410 Celebration Place, Celebration, FL 34747 USA. Tel. +1 407 303 46 73; Fax: +1 407 303 46 32. E-mail address: vipul.patel.md@flhosp.org (V.R. Patel). 0302-2838/$ – see back matter # 2010 European Association of Urology. Published by Elsevier B.V. All rights reserved. doi:10.1016/j.eururo.2010.02.001

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Platinum Priority – Prostate CancerEditorial by Manfred P. Wirth and Michael Froehner on pp. 953–954 of this issue
Early Complication Rates in a Single-Surgeon Series of 2500
Robotic-Assisted Radical Prostatectomies: Report Applying a
Standardized Grading System
Rafael F. Coelho a,b,c, Kenneth J. Palmer a,b, Bernardo Rocco a,b,d, Ravendra R. Moniz e,Sanket Chauhan a,b, Marcelo A. Orvieto a,b, Geoff Coughlin a,b, Vipul R. Patel a,b,*
a Global Robotics Institute, Florida Hospital Celebration Health, Celebration, Florida, USAb University of Central Florida School of Medicine, Orlando, Florida, USAc Hospital das Clinicas da Faculdade de Medicina da Universidade de Sao Paulo, Divisao de Urologia, Sao Paulo, Brazild Divisione di Urologia, Istituto Europeo di Oncologia, Milan, Italye Division of Urology, Faculty of Medical Sciences Santa Casa, Sao Paulo, Brazil
E U R O P E A N U R O L O G Y 5 7 ( 2 0 1 0 ) 9 4 5 – 9 5 2
ava i lable at www.sciencedirect .com
journal homepage: www.europeanurology.com
Article info
Article history:
Received 12 December 2009Accepted February 3, 2010Published online ahead ofprint on February 13, 2010
Keywords:
Prostatectomy
Complications
Robotics
Prostatic neoplasm
Abstract
Background: Perioperative complications following robotic-assisted radical prostatectomy(RARP) have been previously reported in recent series. Few studies, however, have usedstandardized systems to classify surgical complications, and that inconsistency has hampered
accurate comparisons between different series or surgical approaches.Objective: To assess trends in the incidence and to classify perioperative surgical complicationsfollowing RARP in 2500 consecutive patients.Design, setting, and participants: We analyzed 2500 patients who underwent RARP for treat-ment of clinically localized prostate cancer (PCa) from August 2002 to February 2009. Data wereprospectively collected in a customized database and retrospectively analyzed.Intervention: All patients underwent RARP performed by a single surgeon.Measurements: The data were collected prospectively in a customized database. Complica-
tions were classified using the Clavien grading system. To evaluate trends regarding complica-tions and radiologic anastomotic leaks, we compared eight groups of 300 patients each,categorized according the surgeon’s experience (number of cases).Results and limitations: Our median operative time was 90 min (interquartile range [IQR]: 75–100 min). The median estimated blood loss was 100 ml (IQR:100–150 ml). Our conversion ratewas 0.08%, comprising two procedures converted to standard laparoscopy due to robot malfunc-
tion. One hundred and forty complications were observed in 127 patients (5.08%). The followingpercentages of patients presented graded complications: grade 1, 2.24%; grade 2, 1.8%; grade 3a,0.08%; grade 3b, 0.48%; grade 4a, 0.40%. There were no cases of multiple organ dysfunction ordeath (grades 4b and 5). There were significant decreases in the overall complication rates( p = 0.0034) and in the number of anastomotic leaks ( p < 0.001) as the surgeon’s experience
increased.Conclusions: RARP is a safe option for treatment of clinically localized PCa, presenting lowcomplication rates in experienced hands. Although the robotic system provides the surgeon
andrat
with enhanced visionvolume; complication
increased.# 2010 European Assoc
* Corresponding author. GloTel. +1 407 303 46 73; FaxE-mail address: vipul.patel.
0302-2838/$ – see back matter # 2010 European Association of Urology. Publis
dexterity, proficiency is only accomplished with consistent surgicales demonstrated a tendency to decrease as the surgeon’s experience
iation of Urology. Published by Elsevier B.V. All rights reserved.
bal Robotics Institute, 410 Celebration Place, Celebration, FL 34747 USA.: +1 407 303 46 [email protected] (V.R. Patel).
hed by Elsevier B.V. All rights reserved. doi:10.1016/j.eururo.2010.02.001

E U R O P E A N U R O L O G Y 5 7 ( 2 0 1 0 ) 9 4 5 – 9 5 2946
1. Introduction
Data from the Surveillance, Epidemiology and End Results
registry indicate that the incidence of prostate cancer (PCa)
in men under 50 has risen steadily over the past 10 yr, with
an annual percent increase of 9.5% [1]. In addition, with the
widespread diffusion of prostate-specific antigen (PSA)
testing, PCa is frequently diagnosed in younger and
healthier men with organ-confined disease. Consequently,
patients desire to undergo definitive treatment with short
recovery time and low complication rates while maintain-
ing their baseline quality of life.
Since Reiner and Walsh [2] first introduced the anatomic
nerve-sparing technique for radical retropubic prostatecto-
my (RRP), this procedure has become the gold standard and
the most widespread treatment for clinically localized PCa,
providing excellent cancer control in most patients with
clinically localized disease [3]. However, although several
modifications have been added to the original technique
and most urologic surgeons are now familiar with the
procedure, RRP still has an inherent morbidity.
In an effort to further decrease the morbidity of RRP, a
laparoscopic minimally invasivesurgicalapproachtotreating
PCa was first described by Schuessler and colleagues [4] in
1997. Although cancer cure with laparoscopic radical
prostatectomy (LRP) was deemed comparable to open
surgery, the technical demands of the surgery and the
protracted learning curve has prevented the widespread
adoption of LRP by most urologic surgeons. The da Vinci
Surgical System (Intuitive Surgical, Inc., Sunnyvale, CA) has
been introduced to the field of urologic surgery and, with
the advantages of three-dimensional vision, 7 degrees of
freedom, and magnification,hasraised newhopes ofreducing
both the morbidity and the learning curve of minimally
invasive prostatectomy [5]. But as expected, the introduction
of any innovative technology or surgical procedure is
associated with an initial learning curve and with the
potential of eliciting new risks and surgical complications [6].
Perioperative complications following robotic-assisted
radical prostatectomy (RARP) have been previously
reported in some recent series. Few studies, however, have
used standardized systems to classify surgical complica-
tions, and that inconsistency has hampered accurate
comparisons between different series or surgical
Table 1 – Classification of surgical complications: Clavien grading syst
Grade*
1 Any deviation from the normal postoperative course with
Allowed therapeutic regimens are drugs as antiemetics, a
also includes wound infections opened at the bedside.
2 Requiring pharmacologic treatment with drugs other tha
Blood transfusions and total parenteral nutrition are also
3 Complications requiring surgical, endoscopic, or radiolog
4 Any life-threatening complication requiring intermediate
multiple-organ dysfunction).
5 Death of a patient.
* If the patient suffers from a complication at the time of discharge, the suffix ‘‘d
indicates the need for follow-up to fully evaluate the complication.
approaches. Based on these limitations, Clavien and
colleagues proposed a grading system for surgical compli-
cations in 1992 and modified it in 2004 [7]. The Clavien
grading system is a simple, objective, and reproducible
approach for comprehensive surgical outcomes assessment
and has been applied more frequently in recent publications
reporting complications after RRP, LRP, and RARP.
In this study we analyzed early surgical complications in
a single-surgeon series of 2500 consecutive RARPs. Com-
plications were classified according to the modified Clavien
grading system, and trends in the incidence of morbidities
according to the surgeon’s experience were analyzed.
2. Materials and methods
We analyzed 2500 consecutive patients who underwent RARP for
treatment of clinically localized PCa. All of the procedures were
performed by a single surgeon (VRP) from August 2002 to February
2009. After institutional review board approval, data were prospectively
collected in a customized database and retrospectively analyzed.
Complications were classified in our database according to the modified
Clavien grading system (Table 1) [7].
2.1. Operative technique
All patients underwent a six-port transperitoneal technique, as described
previously by the authors [8]. An anterior approach was adopted by
dissecting the retzius space and ligating the dorsal venous complex (DVC).
Recently, we have adopted a periurethral suspension stitch [9] after the
ligation of the DVC. This step was followed by bladder neck dissection and
athermal mobilization of the seminal vesicles. The nerve sparing was
modified and performed athermally with an early retrograde release of the
neurovascular bundle. Bilateral pelvic lymph node dissection (PLND) was
performed in patients classified as intermediate or high risk, according to
the D’Amico classification [10]. A modified posterior reconstruction of the
rhabdosphincter [11] was then performed prior to vesicourethral
anastomosis in the last 1500 patients of our series. The anastomosis
was performed using a continuous running suture with two 3-0 monocryl
sutures tied together. A 18-Fr Foley catheter was inserted. The specimen
was then removed through the primary trocar incision, and a Jackson-Pratt
(JP) drain was positioned in the pelvic gutter.
2.2. Perioperative management
A single intravenous dose of a first-generation cephalosporin and 5000 U
of low-molecular-weight heparin (5000 IU subcutaneously 2 h prior to
em [6]
Description
no specific treatment required.
ntipyretics, analgetics, diuretics, electrolytes, and physiotherapy. This grade
n such allowed for grade 1 complications.
included.
ic intervention (grade 3b if under general anesthesia and grade 3a if not).
or intensive care (grade 4a for single-organ dysfunction and grade 4b for
’’ (for disability) is added to the respective grade of complication. This label

Table 2 – Preoperative patient characteristics
Patient characteristics
Age, yr, median (IQR) 61 (55–66)
BMI, kg/m2, median (IQR) 28 (26–31)
PSA level, ng/ml, median (IQR) 4.9 (3.8–6.7)
Prostate weight, g, median (IQR) 48 (40–59)
AUA-SS, median (IQR) 7 (3–12)
Biopsy Gleason score, %
�6 64
7 28.5
�8 7.5
Pathologic stage, %
pT2 75
pT3 24.3
pT4 0.7
Positive surgical margin rates, %
Overall 10.6
pT2 5
pT3 27.5
Pathologic Gleason score, %
�6 42
7 51.8
�8 6.2
AA-SS = American Urological Association symptom score; BMI = body mass
index; IQR = interquartile range; PSA = prostate-specific antigen.
E U R O P E A N U R O L O G Y 5 7 ( 2 0 1 0 ) 9 4 5 – 9 5 2 947
surgery and then every 12 h until hospital discharge) were administered
preoperatively.
Patients were allowed to drink and eat liberally in the postoperative
period and were discharged on postoperative day 1 once they were able
to ambulate and tolerate diet with minimal discomfort. Cystograms
were performed routinely prior to catheter removal, and in the event of
identifying a leak, the catheter was left in place for an additional 7 d.
Urinary retention was managed similarly with prolonged catheter
drainage until the patient was able to completely empty the bladder.
2.3. Data collection
Complications occurring during the surgical procedure or within 30 d
after surgery were analyzed (early complications). We examined 79%
(1975 of 2500) of our patients at our office 6 wk postoperatively;
complications that developed during the first postoperative month were
assessed and recorded. The 525 patients who were not evaluated at our
office were contacted via phone interview (32%), mail (3%), or e-mail
(65%). Initially, standardized questionnaires evaluating possible un-
scheduled visits to the primary urologist’s office or hospital admissions
were delivered by e-mail at 6–8 wk after surgery. Those patients who did
not reply were then contact by phone or by mail, applying the same
questionnaires. The phone calls were performed by a third party not
involved in direct patient care.
2.4. Definitions of complications
Perioperative blood transfusion was usually indicated for symptomatic
patients and/or hemoglobin levels �7 g/l. For intermediate hemoglobin
concentrations (ie, 7–10 g/dl), blood transfusion was indicated in case of
potential or actual ongoing bleeding or in the presence of risk factors for
complications secondary to inadequate oxygenation (ie, cardiac ische-
mic disease).
Ileus was defined as postoperative nausea, vomiting, and/or
abdominal distension requiring hospitalization time>2 d in the absence
of mechanical bowel obstruction.
Symptomatic lymphocele was defined as a pelvic fluid collection
(especially along the iliac vessels) in patients who underwent PLND and
associated with pelvic pain or pressure, unilateral leg edema and/or pain,
hydronephrosis, deep vein thrombosis (DVT), or infection/sepsis.
2.5. Statistical analysis
Continuous parametric variables were reported as the mean value plus
or minus standard deviation. Continuous nonparametric variables were
presented as the median values and interquartile range (IQR).
To evaluate trends regarding complications and anastomotic leaks,
we compared eight groups of 300 patients each, classified according the
surgeon’s experience (number of cases). The groups were compared
using the x2 test for linear trend. All statistical analyses were performed
using StatsDirect v.2.7.2 statistical software (StatsDirect Ltd., Cheshire,
UK). Statistical significance was defined as p < 0.05.
3. Results
3.1. Early surgical outcomes
Patient characteristics are presented in Table 2.
The median follow-up of our cohort was of 25 mo
(IQR:10–35 mo). Median operative time was 90 min (IQR:
75–100 min), and the median estimated blood loss was
100 ml (IQR:100–150 ml). Bilateral PLND was performed in
44.5% of our patients. Our conversion rate was 0.08%,
comprising two procedures converted to standard laparos-
copy due to robot malfunction. No cases were converted to
open surgery. In our series, 95% of patients were discharged
home on postoperative day 1, and only 0.6% of the patients
were hospitalized for >3 d. The median duration of in-
hospital stay was 1 d. Finally, the median catheterization
time was 5 d (IQR: 4–6 d).
3.2. Description of complications
We observed 140 complications in 127 patients (5.08%).
Intraoperative complications included two rectal injuries,
which occurred in the 8th and 15th patients. Both injuries
were recognized intraoperatively and closed primarily
using a two-layer technique. These patients had a full
mechanical bowel preparation and antibiotic prophylaxis
prior to surgery. Both patients were discharged from the
hospital on postoperative day 2. After surgery, neither
patient had adverse effects from the injuries.
Classification of the complications according the Clavien
grading system is shown in Table 3. There was no case of
multiple-organ dysfunction or death (grades 4b and 5).
Minor complications (grades 1 and 2) constituted 80.8% of
all complications. The incidence of severe complications
(grade �3) was <1% (0.96%; Table 4).
The two most common grade 1 complications were
anastomotic leaks (1.4%), detected on cystogram, and
urinary retention (0.52%). The third most common grade
1 complication was symptomatic lymphocele (0.36%).
Clinical manifestations of lymphocele included pelvic
pressure in four cases, abdominal distension in three cases,
leg pain or weakness in one case, and costovertebral
tenderness in one case. Of these patients, only one required
computed tomography (CT)–guided drainage for treatment
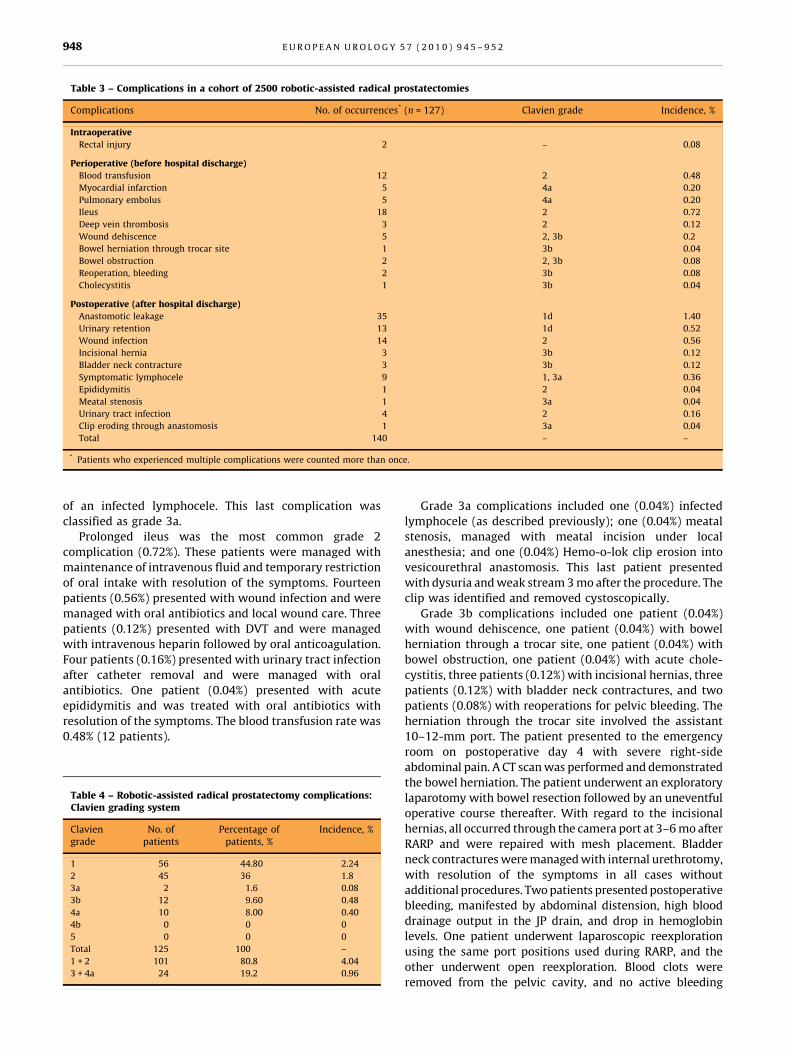
Table 3 – Complications in a cohort of 2500 robotic-assisted radical prostatectomies
Complications No. of occurrences* (n = 127) Clavien grade Incidence, %
Intraoperative
Rectal injury 2 – 0.08
Perioperative (before hospital discharge)
Blood transfusion 12 2 0.48
Myocardial infarction 5 4a 0.20
Pulmonary embolus 5 4a 0.20
Ileus 18 2 0.72
Deep vein thrombosis 3 2 0.12
Wound dehiscence 5 2, 3b 0.2
Bowel herniation through trocar site 1 3b 0.04
Bowel obstruction 2 2, 3b 0.08
Reoperation, bleeding 2 3b 0.08
Cholecystitis 1 3b 0.04
Postoperative (after hospital discharge)
Anastomotic leakage 35 1d 1.40
Urinary retention 13 1d 0.52
Wound infection 14 2 0.56
Incisional hernia 3 3b 0.12
Bladder neck contracture 3 3b 0.12
Symptomatic lymphocele 9 1, 3a 0.36
Epididymitis 1 2 0.04
Meatal stenosis 1 3a 0.04
Urinary tract infection 4 2 0.16
Clip eroding through anastomosis 1 3a 0.04
Total 140 – –
* Patients who experienced multiple complications were counted more than once.
E U R O P E A N U R O L O G Y 5 7 ( 2 0 1 0 ) 9 4 5 – 9 5 2948
of an infected lymphocele. This last complication was
classified as grade 3a.
Prolonged ileus was the most common grade 2
complication (0.72%). These patients were managed with
maintenance of intravenous fluid and temporary restriction
of oral intake with resolution of the symptoms. Fourteen
patients (0.56%) presented with wound infection and were
managed with oral antibiotics and local wound care. Three
patients (0.12%) presented with DVT and were managed
with intravenous heparin followed by oral anticoagulation.
Four patients (0.16%) presented with urinary tract infection
after catheter removal and were managed with oral
antibiotics. One patient (0.04%) presented with acute
epididymitis and was treated with oral antibiotics with
resolution of the symptoms. The blood transfusion rate was
0.48% (12 patients).
Table 4 – Robotic-assisted radical prostatectomy complications:Clavien grading system
Claviengrade
No. ofpatients
Percentage ofpatients, %
Incidence, %
1 56 44.80 2.24
2 45 36 1.8
3a 2 1.6 0.08
3b 12 9.60 0.48
4a 10 8.00 0.40
4b 0 0 0
5 0 0 0
Total 125 100 –
1 + 2 101 80.8 4.04
3 + 4a 24 19.2 0.96
Grade 3a complications included one (0.04%) infected
lymphocele (as described previously); one (0.04%) meatal
stenosis, managed with meatal incision under local
anesthesia; and one (0.04%) Hemo-o-lok clip erosion into
vesicourethral anastomosis. This last patient presented
with dysuria and weak stream 3 mo after the procedure. The
clip was identified and removed cystoscopically.
Grade 3b complications included one patient (0.04%)
with wound dehiscence, one patient (0.04%) with bowel
herniation through a trocar site, one patient (0.04%) with
bowel obstruction, one patient (0.04%) with acute chole-
cystitis, three patients (0.12%) with incisional hernias, three
patients (0.12%) with bladder neck contractures, and two
patients (0.08%) with reoperations for pelvic bleeding. The
herniation through the trocar site involved the assistant
10–12-mm port. The patient presented to the emergency
room on postoperative day 4 with severe right-side
abdominal pain. A CT scan was performed and demonstrated
the bowel herniation. The patient underwent an exploratory
laparotomy with bowel resection followed by an uneventful
operative course thereafter. With regard to the incisional
hernias, all occurred through the camera port at 3–6 mo after
RARP and were repaired with mesh placement. Bladder
neck contractures were managed with internal urethrotomy,
with resolution of the symptoms in all cases without
additional procedures. Two patients presented postoperative
bleeding, manifested by abdominal distension, high blood
drainage output in the JP drain, and drop in hemoglobin
levels. One patient underwent laparoscopic reexploration
using the same port positions used during RARP, and the
other underwent open reexploration. Blood clots were
removed from the pelvic cavity, and no active bleeding
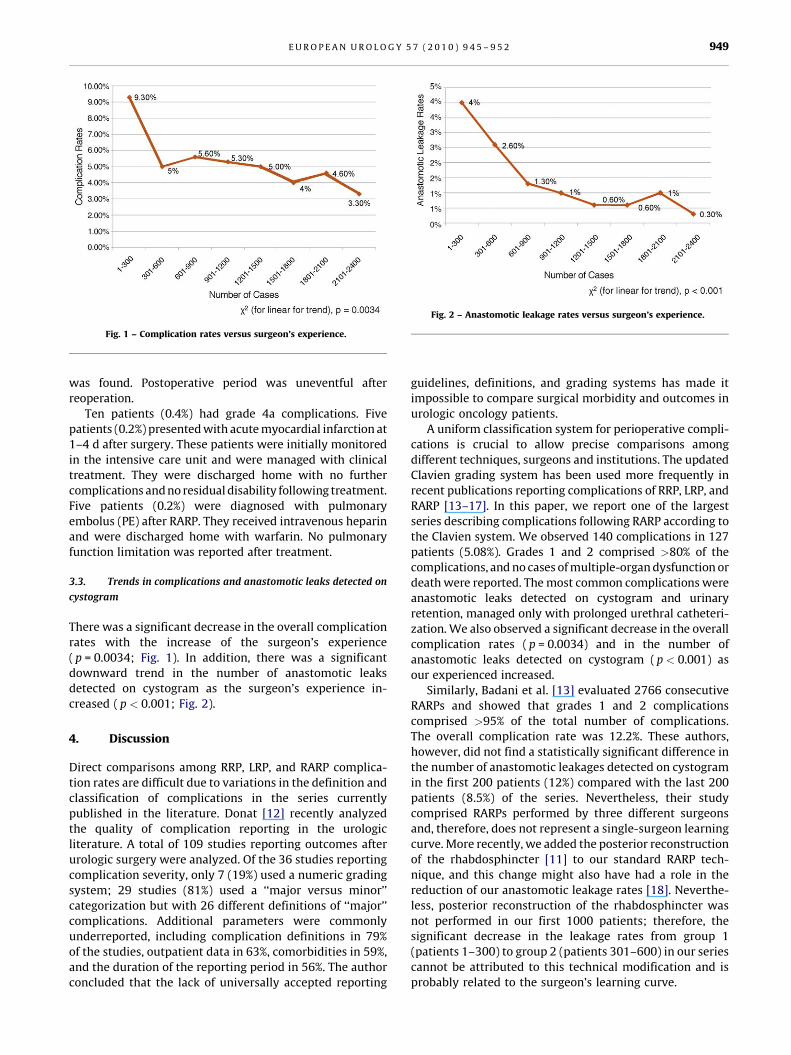
Fig. 1 – Complication rates versus surgeon’s experience.
Fig. 2 – Anastomotic leakage rates versus surgeon’s experience.
E U R O P E A N U R O L O G Y 5 7 ( 2 0 1 0 ) 9 4 5 – 9 5 2 949
was found. Postoperative period was uneventful after
reoperation.
Ten patients (0.4%) had grade 4a complications. Five
patients (0.2%) presented with acute myocardial infarction at
1–4 d after surgery. These patients were initially monitored
in the intensive care unit and were managed with clinical
treatment. They were discharged home with no further
complications and no residual disability following treatment.
Five patients (0.2%) were diagnosed with pulmonary
embolus (PE) after RARP. They received intravenous heparin
and were discharged home with warfarin. No pulmonary
function limitation was reported after treatment.
3.3. Trends in complications and anastomotic leaks detected on
cystogram
There was a significant decrease in the overall complication
rates with the increase of the surgeon’s experience
( p = 0.0034; Fig. 1). In addition, there was a significant
downward trend in the number of anastomotic leaks
detected on cystogram as the surgeon’s experience in-
creased ( p < 0.001; Fig. 2).
4. Discussion
Direct comparisons among RRP, LRP, and RARP complica-
tion rates are difficult due to variations in the definition and
classification of complications in the series currently
published in the literature. Donat [12] recently analyzed
the quality of complication reporting in the urologic
literature. A total of 109 studies reporting outcomes after
urologic surgery were analyzed. Of the 36 studies reporting
complication severity, only 7 (19%) used a numeric grading
system; 29 studies (81%) used a ‘‘major versus minor’’
categorization but with 26 different definitions of ‘‘major’’
complications. Additional parameters were commonly
underreported, including complication definitions in 79%
of the studies, outpatient data in 63%, comorbidities in 59%,
and the duration of the reporting period in 56%. The author
concluded that the lack of universally accepted reporting
guidelines, definitions, and grading systems has made it
impossible to compare surgical morbidity and outcomes in
urologic oncology patients.
A uniform classification system for perioperative compli-
cations is crucial to allow precise comparisons among
different techniques, surgeons and institutions. The updated
Clavien grading system has been used more frequently in
recent publications reporting complications of RRP, LRP, and
RARP [13–17]. In this paper, we report one of the largest
series describing complications following RARP according to
the Clavien system. We observed 140 complications in 127
patients (5.08%). Grades 1 and 2 comprised >80% of the
complications, and no cases of multiple-organ dysfunction or
death were reported. The most common complications were
anastomotic leaks detected on cystogram and urinary
retention, managed only with prolonged urethral catheteri-
zation. We also observed a significant decrease in the overall
complication rates ( p = 0.0034) and in the number of
anastomotic leaks detected on cystogram ( p < 0.001) as
our experienced increased.
Similarly, Badani et al. [13] evaluated 2766 consecutive
RARPs and showed that grades 1 and 2 complications
comprised >95% of the total number of complications.
The overall complication rate was 12.2%. These authors,
however, did not find a statistically significant difference in
the number of anastomotic leakages detected on cystogram
in the first 200 patients (12%) compared with the last 200
patients (8.5%) of the series. Nevertheless, their study
comprised RARPs performed by three different surgeons
and, therefore, does not represent a single-surgeon learning
curve. More recently, we added the posterior reconstruction
of the rhabdosphincter [11] to our standard RARP tech-
nique, and this change might also have had a role in the
reduction of our anastomotic leakage rates [18]. Neverthe-
less, posterior reconstruction of the rhabdosphincter was
not performed in our first 1000 patients; therefore, the
significant decrease in the leakage rates from group 1
(patients 1–300) to group 2 (patients 301–600) in our series
cannot be attributed to this technical modification and is
probably related to the surgeon’s learning curve.
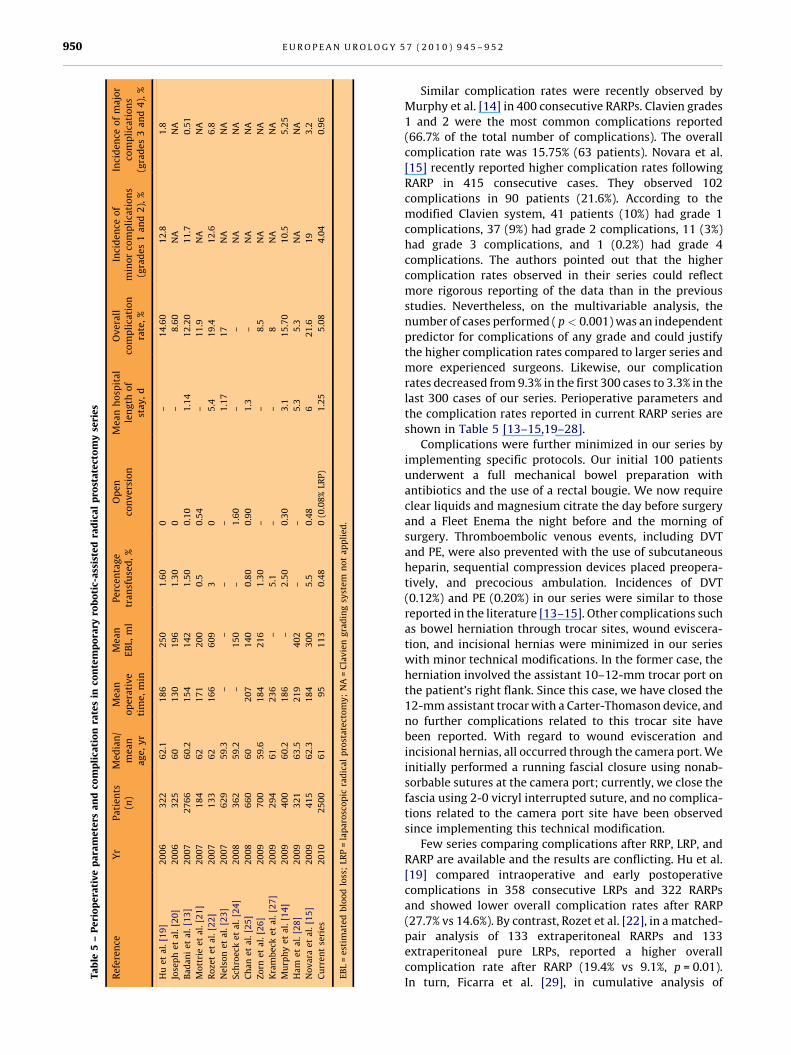
Ta
ble
5–
Pe
rio
pe
rati
ve
pa
ram
ete
rsa
nd
com
pli
cati
on
rate
sin
con
tem
po
rary
rob
oti
c-a
ssis
ted
rad
ica
lp
rost
ate
cto
my
seri
es
Re
fere
nce
Yr
Pa
tie
nts
(n)
Me
dia
n/
me
an
ag
e,
yr
Me
an
op
era
tiv
eti
me
,m
in
Me
an
EB
L,m
lP
erc
en
tag
etr
an
sfu
sed
,%
Op
en
con
ve
rsio
nM
ea
nh
osp
ita
lle
ng
tho
fst
ay
,d
Ov
era
llco
mp
lica
tio
nra
te,
%
Inci
de
nce
of
min
or
com
pli
cati
on
s(g
rad
es
1a
nd
2),
%
Inci
de
nce
of
ma
jor
com
pli
cati
on
s(g
rad
es
3a
nd
4),
%
Hu
et
al.
[19
]2
00
63
22
62
.11
86
25
01
.60
0–
14
.60
12
.81
.8
Jose
ph
et
al.
[20
]2
00
63
25
60
13
01
96
1.3
00
–8
.60
NA
NA
Ba
da
ni
et
al.
[13
]2
00
72
76
66
0.2
15
41
42
1.5
00
.10
1.1
41
2.2
01
1.7
0.5
1
Mo
ttri
ee
ta
l.[2
1]
20
07
18
46
21
71
20
00
.50
.54
–1
1.9
NA
NA
Ro
zet
et
al.
[22
]2
00
71
33
62
16
66
09
30
5.4
19
.41
2.6
6.8
Ne
lso
ne
ta
l.[2
3]
20
07
62
95
9.3
––
––
1.1
71
7N
AN
A
Sch
roe
cke
ta
l.[2
4]
20
08
36
25
9.2
–1
50
–1
.60
––
NA
NA
Ch
an
et
al.
[25
]2
00
86
60
60
20
71
40
0.8
00
.90
1.3
–N
AN
A
Zo
rne
ta
l.[2
6]
20
09
70
05
9.6
18
42
16
1.3
0–
–8
.5N
AN
A
Kra
mb
eck
et
al.
[27
]2
00
92
94
61
23
6–
5.1
––
8N
AN
A
Mu
rph
ye
ta
l.[1
4]
20
09
40
06
0.2
18
6–
2.5
00
.30
3.1
15
.70
10
.55
.25
Ha
me
ta
l.[2
8]
20
09
32
16
3.5
21
94
02
––
5.3
5.3
NA
NA
No
va
rae
ta
l.[1
5]
20
09
41
56
2.3
18
43
00
5.5
0.4
86
21
.61
93
.2
Cu
rre
nt
seri
es
20
10
25
00
61
95
11
30
.48
0(0
.08
%LR
P)
1.2
55
.08
4.0
40
.96
EB
L=
est
ima
ted
blo
od
loss
;LR
P=
lap
aro
sco
pic
rad
ica
lp
rost
ate
cto
my
;N
A=
Cla
vie
ng
rad
ing
syst
em
no
ta
pp
lie
d.
E U R O P E A N U R O L O G Y 5 7 ( 2 0 1 0 ) 9 4 5 – 9 5 2950
Similar complication rates were recently observed by
Murphy et al. [14] in 400 consecutive RARPs. Clavien grades
1 and 2 were the most common complications reported
(66.7% of the total number of complications). The overall
complication rate was 15.75% (63 patients). Novara et al.
[15] recently reported higher complication rates following
RARP in 415 consecutive cases. They observed 102
complications in 90 patients (21.6%). According to the
modified Clavien system, 41 patients (10%) had grade 1
complications, 37 (9%) had grade 2 complications, 11 (3%)
had grade 3 complications, and 1 (0.2%) had grade 4
complications. The authors pointed out that the higher
complication rates observed in their series could reflect
more rigorous reporting of the data than in the previous
studies. Nevertheless, on the multivariable analysis, the
number of cases performed ( p < 0.001) was an independent
predictor for complications of any grade and could justify
the higher complication rates compared to larger series and
more experienced surgeons. Likewise, our complication
rates decreased from 9.3% in the first 300 cases to 3.3% in the
last 300 cases of our series. Perioperative parameters and
the complication rates reported in current RARP series are
shown in Table 5 [13–15,19–28].
Complications were further minimized in our series by
implementing specific protocols. Our initial 100 patients
underwent a full mechanical bowel preparation with
antibiotics and the use of a rectal bougie. We now require
clear liquids and magnesium citrate the day before surgery
and a Fleet Enema the night before and the morning of
surgery. Thromboembolic venous events, including DVT
and PE, were also prevented with the use of subcutaneous
heparin, sequential compression devices placed preopera-
tively, and precocious ambulation. Incidences of DVT
(0.12%) and PE (0.20%) in our series were similar to those
reported in the literature [13–15]. Other complications such
as bowel herniation through trocar sites, wound eviscera-
tion, and incisional hernias were minimized in our series
with minor technical modifications. In the former case, the
herniation involved the assistant 10–12-mm trocar port on
the patient’s right flank. Since this case, we have closed the
12-mm assistant trocar with a Carter-Thomason device, and
no further complications related to this trocar site have
been reported. With regard to wound evisceration and
incisional hernias, all occurred through the camera port. We
initially performed a running fascial closure using nonab-
sorbable sutures at the camera port; currently, we close the
fascia using 2-0 vicryl interrupted suture, and no complica-
tions related to the camera port site have been observed
since implementing this technical modification.
Few series comparing complications after RRP, LRP, and
RARP are available and the results are conflicting. Hu et al.
[19] compared intraoperative and early postoperative
complications in 358 consecutive LRPs and 322 RARPs
and showed lower overall complication rates after RARP
(27.7% vs 14.6%). By contrast, Rozet et al. [22], in a matched-
pair analysis of 133 extraperitoneal RARPs and 133
extraperitoneal pure LRPs, reported a higher overall
complication rate after RARP (19.4% vs 9.1%, p = 0.01).
In turn, Ficarra et al. [29], in cumulative analysis of

E U R O P E A N U R O L O G Y 5 7 ( 2 0 1 0 ) 9 4 5 – 9 5 2 951
comparative studies, showed similar complication rates
after RARP and LRP (risk ratio [RR]: 1.83; 95% confidence
interval [CI], 0.78–4.31; p = 0.16). With regard to the
comparison between RRP and RARP, similar complication
rates were reported in most of the available publications.
Krambeck et al. [27] recently reported comparable periop-
erative overall complication rates between RARP and RRP
(8.0% vs 4.8%, p = 0.064). Similarly, Nelson et al. [23] showed
equivalent rates of unscheduled visits (RRP 10% vs RARP
10%, p = 0.95) and readmissions (RRP 5% vs RARP 7%,
p = 0.12) due to complications for these two surgical
approaches. Finally, the cumulative analysis of comparative
studies performed by Ficarra et al. [29] showed only a
nonstatistically significant trend in favor of RARP (RR: 1.33;
95% CI, 0.64–2.74; p = 0.44).
The strengths of our study are the large number of
patients, the single-surgeon experience, the application of a
standardized classification system, and the evaluation of
the complication rates stratified by the number of previous
procedures. We believe our study provides a valuable
contribution for future comparisons among different RP
series and surgical approaches. Nevertheless, our study has
some limitations. Despite our strict follow-up, our compli-
cation rate is subject to underreporting due to the short
duration of in-hospital stay and to the ‘‘retrospective’’
evaluation of complications at the 6-wk follow-up visit.
Additionally, although patients who were not evaluated at
our office were followed via phone interview or e-mail, the
patients’ primary urologists were not contacted in all cases;
therefore, some minor complications might have been
underreported by the patients. Moreover, we analyzed early
complications after RARP performed by a single surgeon
with large surgical experience; hence, our results might not
be applicable to low-volume RARP centers. Finally, Martin
et al. [30] recently proposed a standardized method for
reporting surgical complications based on 10 strict criteria
(eg, methods of data collection, duration of follow-up,
presence of outpatient information, definitions of compli-
cations, mortality and morbidity rates, procedure-specific
complication, grading system, length of in-hospital stay,
analysis of risk factors). Our study does not fulfill all of the
Martin criteria because some of the potential predictive
factors for complications (Charlson Index, comorbidities,
Eastern Cooperative Oncology Group performance status)
are not consistently available in our database and an
accurate multivariate analysis of risk factors for complica-
tions was not possible.
5. Conclusions
RARP is a safe option for treatment of clinically localized
PCa, presenting low complication rates in experienced
hands. Although the robotic system provides the surgeon
with enhanced vision and dexterity, proficiency is only
accomplished with consistent surgical volume; complica-
tion rates demonstrated a tendency to decrease as the
surgeon’s experience increased. The use of standardized
classification systems to analyze surgical complications will
allow proper comparisons among different surgical tech-
niques, surgeons, and institutions.
Author contributions: Vipul R. Patel had full access to all the data in the
study and takes responsibility for the integrity of the data and the
accuracy of the data analysis.
Study concept and design: Coelho, Palmer, Rocco, Patel.
Acquisition of data: Palmer, Coelho, Moniz, Chauhan.
Analysis and interpretation of data: Coelho, Moniz.
Drafting of the manuscript: Coelho, Moniz.
Critical revision of the manuscript for important intellectual content: Patel,
Rocco.
Statistical analysis: Coelho.
Obtaining funding: None.
Administrative, technical, or material support: None.
Supervision: Patel.
Other (specify): None.
Financial disclosures: I certify that all conflicts of interest, including
specific financial interests and relationships and affiliations relevant to
the subject matter or materials discussed in the manuscript (eg,
employment/affiliation, grants or funding, consultancies, honoraria,
stock ownership or options, expert testimony, royalties, or patents filed,
received, or pending), are the following: None.
Funding/Support and role of the sponsor: None.
References
[1] Hayat HJ, Howlander N, Reichman ME, Edwards BK. Cancer statistics,
trends and multiple primary cancer analyses from the Surveillance,
Epidemiology and End Results (SEER) program. Oncologist 2007;
12:20–37.
[2] Reiner WB, Walsh PC. An anatomical approach to the surgical
management of the dorsal vein and Santorini’s plexus during radi-
cal retropubic surgery. J Urol 1979;121:198–200.
[3] Bill-Axelson A, Holmberg L, Ruutu M, et al. Scandinavian Prostate
Cancer Group Study, 4. Radical prostatectomy versus watchful
waiting in early prostate cancer. N Engl J Med 2005;12:1977–84.
[4] Schuessler WW, Schulam PG, Clayman RV, Kavoussi LR. Laparoscopic
radical prostatectomy: initial short-term experience. Urology 1997;
50:854–7.
[5] Binder J, Kramer W. Robotically-assisted laparoscopic radical pros-
tatectomy. BJU Int 2001;87:408–10.
[6] Vickers AJ, Savage CJ, Hruza M, et al. The surgical learning curve for
laparoscopic radical prostatectomy: a retrospective cohort study.
Lancet Oncol 2009;10:475–80.
[7] Dindo D, Demartines N, Clavien PA. Classification of surgical com-
plications: a new proposal with evaluation in a cohort of 6336
patients and results of a survey. Ann Surg 2004;240:205–13.
[8] Patel VR, Thaly R, Shah K. Robotic radical prostatectomy: outcomes
of 500 cases. BJU Int 2007;99:1109–12.
[9] Patel VR, Coelho RF, Palmer KJ, Rocco B. Periurethral suspension
stitch during robotic-assisted laparoscopic radical prostatectomy:
description of the technique and continence outcomes. Eur Urol
2009;56:472–8.
[10] D’Amico AV, Whittington R, Malkowicz SB, et al. Biochemical
outcome after radical prostatectomy, external beam radiation ther-
apy, or interstitial radiation therapy for clinically localized prostate
cancer. JAMA 1998;280:969–74.
[11] Coughlin G, Dangle PP, Patil NN, et al. Surgery illustrated—focus on
details. Modified posterior reconstruction of the rhabdosphincter:
application to robotic-assisted laparoscopic prostatectomy. BJU Int
2008;102:1482–5.
E U R O P E A N U R O L O G Y 5 7 ( 2 0 1 0 ) 9 4 5 – 9 5 2952
[12] Donat SM. Standards for surgical complication reporting in urologic
oncology: time for a change. Urology 2007;69:221–5.
[13] Badani KK, Kaul S, Menon M. Evolution of robotic radical prostatec-
tomy: assessment after 2766 procedures. Cancer 2007;110:1951–8.
[14] Murphy DG, Kerger M, Crowe H, Peters JS, Costello AJ. Operative
details and oncological and functional outcome of robotic-assisted
laparoscopic radical prostatectomy: 400 cases with a minimum of
12 months follow-up. Eur Urol 2009;55:1358–67.
[15] Novara G, Ficarra V, D’Elia C, Secco S, Cavalleri S, Artibani W.
Prospective evaluation with standardised criteria for postoperative
complications after robotic-assisted laparoscopic radical prostatec-
tomy. Eur Urol 2010;57:363–70.
[16] Gonzalgo ML, Pavlovich CP, Trock BJ, et al. Classification and trends
of perioperative morbidities following laparoscopic radical prosta-
tectomy. J Urol 2005;174:135–9.
[17] Constantinides CA, Tyritzis SI, Skolarikos A, Liatsikos E, Zervas A,
Deliveliotis C. Short- and long-term complications of open radical
prostatectomy according to the Clavien classification system. BJU
Int 2009;103:336–40.
[18] Menon M, Muhletaler F, Campos M, Peabody JO. Assessment of early
continence after reconstruction of the periprostatic tissues in
patients undergoing computer assisted (robotic) prostatectomy:
results of a 2 group parallel randomized controlled trial. J Urol
2008;180:1018–23.
[19] Hu JC, Nelson RA, Wilson TG, et al. Perioperative complications of
laparoscopic and robotic assisted laparoscopic radical prostatecto-
my. J Urol 2006;175:541–6.
[20] Joseph JV, Rosenbaum R, Madeb R, Erturk E, Patel HR. Robotic
extraperitoneal radical prostatectomy: an alternative approach. J
Urol 2006;175:945–50.
[21] Mottrie A, Van Migem P, De Naeyer G, Schatteman P, Carpentier P,
Fonteyne E. Robot-assisted laparoscopic radical prostatectomy:
oncologic and functional results of 184 cases. Eur Urol 2007;52:
746–51.
[22] Rozet F, Jaffe J, Braud G, et al. A direct comparison of robotic assisted
versus pure laparoscopic radical prostatectomy: a single institution
experience. J Urol 2007;178:478–82.
[23] Nelson B, Kaufman M, Broughton G, et al. Comparison of length of
hospital stay between radical retropubic prostatectomy and robotic
assisted laparoscopic prostatectomy. J Urol 2007;177:929–31.
[24] Schroeck FR, Sun L, Freedland SJ, et al. Comparison of prostate-
specific antigen recurrence-free survival in a contemporary cohort
of patients undergoing either radical retropubic or robot-assisted
laparoscopic radical prostatectomy. BJU Int 2008;102:28–32.
[25] Chan RC, Barocas DA, Chang SS, et al. Effect of a large prostate gland
on open and robotically assisted laparoscopic radical prostatecto-
my. BJU Int 2008;101:1140–4.
[26] Zorn KC, Wille MA, Thong AE, et al. Continued improvement of
perioperative, pathological and continence outcomes during 700
robot-assisted radical prostatectomies. Can J Urol 2009;16:4742–9.
[27] Krambeck AE, DiMarco DS, Rangel LJ, et al. Radical prostatectomy
for prostatic adenocarcinoma: a matched comparison of open
retropubic and robot-assisted techniques. BJU Int 2008;103:
448–53.
[28] Ham WS, Park SY, Rha KH, Kim WT, Choi YD. Robotic radical
prostatectomy for patients with locally advanced prostate cancer
is feasible. Results of a single-institution study. J Laparoendosc Adv
Surg Tech A 2009;19:329–32.
[29] Ficarra V, Novara G, Artibani W, et al. Retropubic, laparoscopic, and
robot-assisted radical prostatectomy: a systematic review and
cumulative analysis of comparative studies. Eur Urol 2009;55:
1037–63.
[30] Martin RC, Brennan MF, Jaques DP. Quality of complication report-
ing in the surgical literature. Ann Surg 2002;235:803–13.
Related Documents











