Early Acute Kidney Injury Predicts Progressive Renal Dysfunction and Higher Mortality in Severely Burned Adults Michael J. Mosier, MD * , Tam N. Pham, MD * , Matthew B. Klein, MD * , Nicole S. Gibran, MD * , Brett D. Arnoldo, MD † , Richard L. Gamelli, MD ‡ , Ronald G. Tompkins, MD, ScD § , and David N. Herndon, MD ¶ * University of Washington Burn Center at Harborview Medical Center, Seattle † UT Southwestern Parkland Memorial Hospital, Dallas, Texas ‡ Loyola University Medical Center, Maywood, Illinois § Massachusetts General Hospital, Boston ¶ UT Medical Branch, Galveston, Texas Abstract The incidence and prognosis of acute kidney injury (AKI) developing during acute resuscitation have not been well characterized in burn patients. The recently developed Risk, Injury, Failure, Loss, and End-stage (RIFLE) classification provides a stringent stratification of AKI severity and can allow for the study of AKI after burn injury. We hypothesized that AKI frequently develops early during resuscitation and is associated with poor outcomes in severely burned patients. We conducted a retrospective review of patients enrolled in the prospective observational multicenter study “Inflammation and the Host Response to Injury.” A RIFLE score was calculated for all patients at 24 hours and throughout hospitalization. Univariate and multivariate analyses were performed to distinguish the impact of early AKI on progressive renal dysfunction, need for renal replacement therapy, and hospital mortality. A total of 221 adult burn patients were included, with a mean TBSA burn of 42%. Crystalloid resuscitation averaged 5.2 ml/kg/%TBSA, with urine output of 1.0 ± 0.6 ml/kg/hr at 24 hours. Sixty-two patients met criteria for AKI at 24 hours: 23 patients (10%) classified as risk, 32 patients (15%) as injury, and 7 (3%) as failure. After adjusting for age, TBSA, inhalation injury, and nonrenal Acute Physiology and Chronic Health Evaluation II ≥20, early AKI was associated with an adjusted odds ratio 2.9 for death (95% CI 1.1–7.5, P = . 03). In this cohort of severely burned patients, 28% of patients developed AKI during acute resuscitation. AKI was not always transient, with 29% developing progressive renal deterioration by RIFLE criteria. Early AKI was associated with early multiple organ dysfunction and higher mortality risk. Better understanding of how early AKI develops and which patients are at risk for progressive renal dysfunction may lead to improved outcomes. Acute renal failure with severe oliguria is an uncommon but ominous development during burn shock resuscitation. Transient oliguria and acute creatinine elevations, however, occur more commonly during the resuscitative phase but are of uncertain prognostic significance. Because of varying definitions, the incidence of acute renal dysfunction in burn intensive care units (ICUs) has varied widely from 15 to 40%, 1, 2 and few studies have evaluated the functional significance of transient renal dysfunction. Copyright © 2010 by the American Burn Association. Address correspondence to Michael J. Mosier, MD, University of Washington Burn Center, Harborview Medical Center, Box 359796, 325 Ninth Avenue, Seattle, Washington 98104. NIH Public Access Author Manuscript J Burn Care Res. Author manuscript; available in PMC 2011 February 27. Published in final edited form as: J Burn Care Res. 2010 ; 31(1): 83–92. doi:10.1097/BCR.0b013e3181cb8c87. NIH-PA Author Manuscript NIH-PA Author Manuscript NIH-PA Author Manuscript

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Early Acute Kidney Injury Predicts Progressive RenalDysfunction and Higher Mortality in Severely Burned Adults
Michael J. Mosier, MD*, Tam N. Pham, MD*, Matthew B. Klein, MD*, Nicole S. Gibran, MD*,Brett D. Arnoldo, MD†, Richard L. Gamelli, MD‡, Ronald G. Tompkins, MD, ScD§, and DavidN. Herndon, MD¶*University of Washington Burn Center at Harborview Medical Center, Seattle†UT Southwestern Parkland Memorial Hospital, Dallas, Texas‡Loyola University Medical Center, Maywood, Illinois§Massachusetts General Hospital, Boston¶UT Medical Branch, Galveston, Texas
AbstractThe incidence and prognosis of acute kidney injury (AKI) developing during acute resuscitationhave not been well characterized in burn patients. The recently developed Risk, Injury, Failure,Loss, and End-stage (RIFLE) classification provides a stringent stratification of AKI severity andcan allow for the study of AKI after burn injury. We hypothesized that AKI frequently developsearly during resuscitation and is associated with poor outcomes in severely burned patients. Weconducted a retrospective review of patients enrolled in the prospective observational multicenterstudy “Inflammation and the Host Response to Injury.” A RIFLE score was calculated for allpatients at 24 hours and throughout hospitalization. Univariate and multivariate analyses wereperformed to distinguish the impact of early AKI on progressive renal dysfunction, need for renalreplacement therapy, and hospital mortality. A total of 221 adult burn patients were included, witha mean TBSA burn of 42%. Crystalloid resuscitation averaged 5.2 ml/kg/%TBSA, with urineoutput of 1.0 ± 0.6 ml/kg/hr at 24 hours. Sixty-two patients met criteria for AKI at 24 hours: 23patients (10%) classified as risk, 32 patients (15%) as injury, and 7 (3%) as failure. After adjustingfor age, TBSA, inhalation injury, and nonrenal Acute Physiology and Chronic Health EvaluationII ≥20, early AKI was associated with an adjusted odds ratio 2.9 for death (95% CI 1.1–7.5, P = .03). In this cohort of severely burned patients, 28% of patients developed AKI during acuteresuscitation. AKI was not always transient, with 29% developing progressive renal deteriorationby RIFLE criteria. Early AKI was associated with early multiple organ dysfunction and highermortality risk. Better understanding of how early AKI develops and which patients are at risk forprogressive renal dysfunction may lead to improved outcomes.
Acute renal failure with severe oliguria is an uncommon but ominous development duringburn shock resuscitation. Transient oliguria and acute creatinine elevations, however, occurmore commonly during the resuscitative phase but are of uncertain prognostic significance.Because of varying definitions, the incidence of acute renal dysfunction in burn intensivecare units (ICUs) has varied widely from 15 to 40%,1,2 and few studies have evaluated thefunctional significance of transient renal dysfunction.
Copyright © 2010 by the American Burn Association.Address correspondence to Michael J. Mosier, MD, University of Washington Burn Center, Harborview Medical Center, Box 359796,325 Ninth Avenue, Seattle, Washington 98104.
NIH Public AccessAuthor ManuscriptJ Burn Care Res. Author manuscript; available in PMC 2011 February 27.
Published in final edited form as:J Burn Care Res. 2010 ; 31(1): 83–92. doi:10.1097/BCR.0b013e3181cb8c87.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

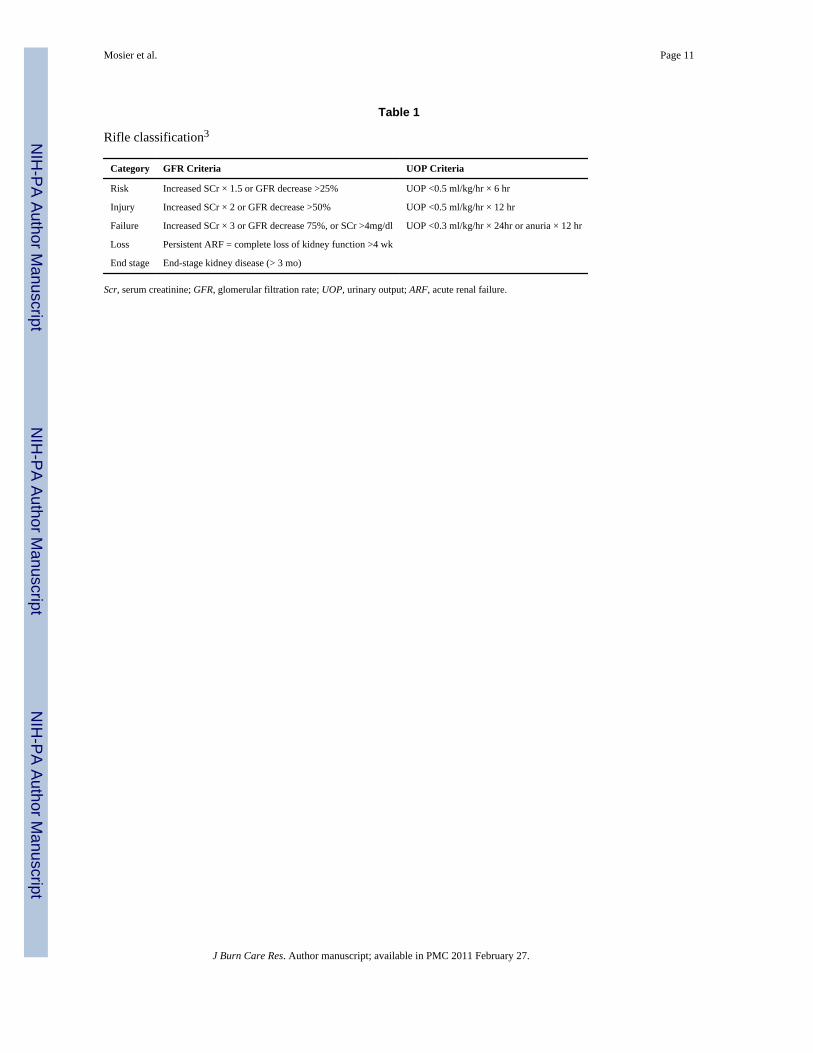
The Risk, Injury, Failure, Loss, and End-stage kidney (RIFLE) classification system (Table1)3 was recently developed to categorize severity of renal dysfunction and has enabledinvestigators to examine the impact of acute kidney dysfunction in critically ill patients.RIFLE defines three grades of increasing severity of acute kidney injury (AKI): risk, injury,and failure, based on changes in either serum creatinine or urine output, and two outcomecategories (loss and end-stage kidney disease). Several critical care studies have validatedthe use of RIFLE criteria in mixed ICU patient populations.4–6 Several recent reports inburn patients have correlated worst RIFLE score during hospitalization to outcomes andexamined the effect of continuous renal replacement therapy (RRT) on AKI compared withhistorical controls.7,8 However, the use of RIFLE as a tool to identify AKI during burnresuscitation has not yet been evaluated.
The “Inflammation and Host Response to Injury” is a collaborative program supported bythe National Institute of General Medical Sciences with primary intent to better define theproteomic and genomic response to trauma and burn injuries. As part of this study, a largeclinical database of patients with extensive burn injury has been maintained. In the contextof this prospective cohort study, we sought out to investigate the incidence of AKI duringburn resuscitation and its impact on hospitalization outcomes, including initiation of RRTand death.
METHODSStudy Design
We conducted a retrospective cohort study to evaluate the relationship between early AKIand outcome after thermal injury in the context of a prospective multicenter observationalstudy. The principal exposure of interest was development of AKI (defined as a RIFLEclassification of risk, injury, or failure) in the first 24 hours after burn injury, and mainoutcomes of interest were progression of AKI, administration of RRT, and inhospitalmortality.
Patients and Data CollectionEligible subjects included all adults with complete outcome data enrolled in the burncomponent of the Inflammation and Host Response to Injury (Glue Grant) program as ofAugust 15, 2008.9 There are five participating centers in the study: Loyola UniversityMedical Center, Massachusetts General Hospital, Parkland Memorial Hospital, Universityof Texas-Galveston, and the University of Washington. Criteria for adult patient enrollmentinto the multicenter study were age ≥18 years, burn size ≥20% TBSA, no other concomitanttrauma, and admission to the study center within 96 hours of injury. Patients who were notresuscitated and placed on comfort care were not eligible for enrollment. This study wasconducted after approval by the Glue Grant administrative core and by the University ofWashington Institutional Review Board.
Data CollectionClinical data were prospectively collected by trained nurse abstractors and entered into aweb-based data collection platform specifically adapted for this program. Data integrity wasevaluated centrally and by external review, as previously described.9 For this study, weabstracted data on all enrolled adult patients with complete hospitalization entries as ofAugust 15, 2008.
DefinitionsInitiation and methods of RRT were not part of standard operating procedures and were,thus, managed at the discretion of the burn surgeons at individual centers. AKI was
Mosier et al. Page 2
J Burn Care Res. Author manuscript; available in PMC 2011 February 27.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

identified by retrospectively calculating a RIFLE score at 24 hours on all patients followingthe method detailed in Table 1 and categorized as “early AKI.” Subjects with identifiedpreinjury chronic renal insufficiency were excluded from this analysis. Because baselinecreatinine levels were not available in injured patients, and the initial creatinine level athospital admission likely reflects the effects of the burn injury that occurred before hospitaladmission, or during the initial phase of care, baseline values were estimated by age, racialbackground, and sex according to the method of Bellomo et al3 in the second internationalconsensus conference of the Acute Dialysis Quality Initiative Group using the modificationof diet in renal disease equation. After reviewing each patient’s medical history, theircomorbidities (Table 2) were compared with the conditions listed in Table 3 to create aCharlson score. Any patient with a Charlson score of ≥1 was described as “comorbiditypresent.”
Data AnalysisWe compared baseline patient and clinical characteristics between patients with and withoutAKI including age, sex, ethnicity, %TBSA, burn mechanism, presence of inhalation injury,Acute Physiology and Chronic Health Evaluation (APACHE) II score, Denver multiorganfailure score9 at 24 hours and maximal Denver score, resuscitation volume, urine output,abdominal compartment syndrome, escharotomy, and decompression laparotomy. Totalfluid volume (including colloid and crystalloid) administered in the first 24 hours afterinjury was examined as a function of the volume predicted by the Parkland Formula (4 ml/kg/%TBSA). Acute respiratory distress syndrome (ARDS), progression of AKI defined byworsening RIFLE classification, initiation of RRT, and discharge status were recorded foreach patient. Given that APACHE II and Denver scores both include a renal dysfunctioncomponent, a modified APACHE II score and Nonrenal Organ Failure (NROF) score werecalculated by omitting the creatinine component from the total APACHE II and Denverscores, respectively. The NROF score assigns one point for each nonrenal organ system indysfunction (cardiac, pulmonary, or hepatic), as recently advocated by Barrantes et al.11Thus, a nonrenal Denver score of ≥4 from two or more organ systems (cardiac, pulmonary,or hepatic) was defined as NROF ≥2 organ systems and, thus, represent early nonrenalmultiple organ dysfunction syndrome (MODS).
Categorical variables, reported as proportions, were compared with χ2 tests. Continuousvariables are reported as mean ± SD. Means were compared using Student’s t-test if anormal distribution was detected. Nonparametric variables were compared with Wilcoxonrank-sum test where appropriate. Logistic regression analyses were performed to assess anodds ratio (OR) for death for each variable, including early AKI and AKI at any point duringthe hospitalization, as well as severity of illness variables such as NROF ≥2 and nonrenalAPACHE II ≥20.
To adjust for confounding variables and assess possible effect modification, multiple logisticregression analyses were performed. Variables were included in the regression analyses ifthey demonstrated significant association with the outcome of interest in the bivariateanalyses. Given the significant effect of early multiple organ failure, multivariate analyseswere performed with and without the variable “NROF ≥2” to test the level of associationbetween early AKI and hospital mortality. All statistical analyses were performed with theuse of STATA 10 (College Station, TX), a statistical software package. Actual P values arereported.
Mosier et al. Page 3
J Burn Care Res. Author manuscript; available in PMC 2011 February 27.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

RESULTSBaseline Patient and Injury Characteristics
At the time of our analysis on August 15, 2008, there were 437 patients enrolled with datarecorded. Children (n = 202) and adults with incomplete resuscitation data (n = 14) wereexcluded. Thus, the study population consisted of 221 adult subjects. Patients and theirfamilies were interviewed about their medical history and any history of preexisting renaldysfunction. When available, medical records before injury were also reviewed to learnabout medical illnesses including chronic renal dysfunction. Through this process, none ofthe 221 patients included in this study had a known history of chronic renal dysfunction. Ofthese 221 patients, 62 patients (28%) met AKI criteria at 24 hours (Table 4). Twenty-threepatients (10%) met risk criteria, 32 (15%) were categorized as injury, and 7 (3%) as failure.Those who developed early AKI were significantly older (50.8 vs 39.1 years, P < .01), had ahigher illness severity on admission (APACHE II: 23.6 vs 19.4, P < .01), and had a greaterpercentage with comorbidities (41.9 vs 20.8%, P < .01; Table 4). Mean burn size and full-thickness component were similar among patients with and without AKI.
Resuscitation Over the First 24 HoursTime from injury to admission to the burn unit was similar between groups (4.1 vs 4.4hours, P = 0.36), and in that time period, both groups received fluids at a volume greaterthan predicted by Parkland (Table 5). Total 24-hour resuscitation volume and amount ofcolloid were similar between those who developed early AKI and those who did not. Sevenpatients received plasmapheresis. Five of those patients did not have early AKI, and two hadearly AKI (one risk, one injury). No patients received high-dose vitamin C. A significantdifference between groups was the initial base deficit (BD) and the worst BD over the initial24 hours (−6.5 vs −4.9, P = 0.01 and −8.0 vs −6.1, P < .01, respectively). Both groupsaveraged a urine output within the recommended 0.5 to 1.0 ml/kg/hr or greater; however,those who developed early AKI had a significantly lower average urine output (0.6 vs 1.16ml/kg/hr, P < .01).
OutcomesEarly AKI—Eighteen (29%) of the 62 patients with early AKI had further deterioration inrenal function, such that 48% (11 of 23) of patients initially classified as risk progressed toinjury or failure and 22% (7 of 32) of patients initially classified as injury progressed tofailure (Figure 1). Twelve patients (19%) with early AKI eventually received RRT, and 9 ofthose 12 (75%) did not survive. Four of six patients (67%) with deteriorating renal functionwho did not receive RRT died. Two died within the first 8 days, and the other two died inthe second and third months of their hospitalization. In contrast, 35 of the 44 patients (80%)who had stabilization or improvement of their early AKI were discharged alive. Thus, allearly AKI patients with renal deterioration had a markedly higher mortality (72%) thanthose who stabilized or improved in their renal function (20%). Overall, early AKI patientshad higher mortality (36%) compared with those without AKI (13%), with multiple organfailure and sepsis as the most common causes of death.
Late-Onset AKI—Of those who did not develop early AKI, 47 patients (30%) developedAKI later in their hospitalization (Figure 2). The most common cause of late-onset AKI wasMODS (occurring in 22 patients, with 5 of the 22 also suffering from sepsis). The secondmost common etiology was sepsis (preceding multiple organ failure in two patients). Theremaining 23 patients who developed late-onset AKI did so due to unknown causes.Thirteen patients (28%) with late-onset AKI received RRT, and 7 of those 13 (54%) did notsurvive. All late-onset AKI patients who received RRT had concomitant multiple organfailure. Twenty-five of the 34 patients (74%) who did not receive RRT were discharged
Mosier et al. Page 4
J Burn Care Res. Author manuscript; available in PMC 2011 February 27.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

alive. Late-onset AKI patients had 54% mortality in those receiving RRT and 26% in thosewithout RRT. Interestingly, there was no significant difference in Baux scores on admissionin those who eventually received RRT and those who did not (94 vs 92). In contrast, of the112 patients who never developed AKI, 106 patients (95%) were discharged alive.
Renal Replacement Therapy—Twenty-five patients received RRT at a mean of 19 daysof hospitalization. Seven patients were started on RRT in the first week, and the remaining18 patients had RRT initiated by a mean of 25 days. Thirteen of those patients were initiallycategorized as no AKI, 6 patients as risk, and 6 patients as injury. Overall, RRT wasassociated with a 64% mortality (16 patients) and was higher for patients with early AKI(75% mortality) compared with late-onset AKI (54% mortality). The RRT method was notprotocolized among the participating centers. Thus, both continuous RRT and intermittenthemodialysis were used, and the RRT modality depended on the hemodynamic status andvolume status of patients over time.
Development of Early AKI—Bivariate analysis revealed that age, presence of acomorbidity, preadmission fluid ratio, NROF ≥2, initial BD, and worst BD in the initial 24hours were significantly associated with development of early AKI (Table 6). Therefore, amultivariate analysis was performed, which revealed age and preadmission fluid ratio to besignificantly associated with development of early AKI and worst BD in the initial 24 hoursto be nearly significant (Table 7).
Association Between Early AKI and Mortality—Mortality was higher among patientswith early AKI than those without (36 vs 13%, P < .01; Table 8). Early AKI was associatedwith an unadjusted OR of 3.61 for death (95% CI 1.81–7.23, P < .01; Table 9). Multivariatelogistic regression, adjusting for the effects of age, %TBSA, inhalation injury, nonrenalAPACHE II ≥20, and presence of a comorbidity, indicated that early AKI had an adjustedOR of 2.87 for death (95% CI 1.11–7.45, P = 0.03). However, a significant proportion ofpatients with early AKI also developed early-onset NROF ≥2 during the resuscitation timeframe. This factor was also associated with the mortality outcome by unadjusted analysis.When early-onset NROF ≥2 was factored into the regression analysis, early AKI had anadjusted OR of 2.32 for death (95% CI 0.85–6.36, P = .10), thus decreasing the strength ofthe association because of the greater effect of early MODS on mortality (Table 10).
DISCUSSIONResuscitation from burn shock remains one of the essential challenges of modern burn care.The severely burned patient has multiple risk factors for AKI during burn shockresuscitation. Intravascular hypovolemia, release of local and systemic cytokines, andcardiovascular dysfunction that accompany extensive tissue destruction in the acute injuryphase, all create significant potential for early AKI.12–15 RIFLE is a recently describedclassification that allows for a more precise examination of the impact of renal dysfunctionon outcome. The prognostic value of the RIFLE classification has been validated bycorrelating the patient’s worst RIFLE stage during hospitalization with mortality risk in amixed ICU population and in burn patients.5,6,8 We have attempted to separate out earlyAKI in this cohort study to focus on AKI as a complication of burn shock.
By using RIFLE, we identified AKI as a common complication (28%) during burnresuscitation, with older and sicker patients with more comorbidities to be more likely tosuffer from early AKI and found that patients with early AKI had a high incidence ofdeterioration of their renal function and increased mortality compared with patients withoutearly AKI. These data indicate that episodes of oliguria and creatinine elevation duringresuscitation that meet risk or injury criteria (Table 1) should be interpreted as complications
Mosier et al. Page 5
J Burn Care Res. Author manuscript; available in PMC 2011 February 27.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

of burn shock, predicting worse hospitalization outcomes. Early AKI, however, should berecognized and construed in the context of early multiple organ failure, which clearlyportends a higher mortality risk. Adjusting for the presence of early nonrenal multiple organfailure in the regression model inevitably weakens the association between early AKI andmortality.
Historically, renal failure resulting from under resuscitation was a focus in burn care;however, the majority of recent studies have focused on the risks of excess resuscitation,which is associated with complications, including pneumonia, ARDS, elevated compartmentsyndromes, and higher risk of death.9,16,17 Average resuscitation volume in the first 24hours in this cohort was 5.2 ml/kg/%TBSA and did not statistically differ between early AKIand nonearly AKI patients. Although higher than predicted Parkland formula-estimatedvolumes, this average is consistent with many other contemporary studies, which includesreported experiences of civilian and military burn centers.16,18 Given the lack of differencein resuscitation volumes between those who developed early AKI and those who did not, ourdata suggest that development of early AKI is multifactorial and not solely dependent on theamount of fluid received. In addition, the fact that the 24-hour average urine output forpatients who developed early AKI was within the recommended guideline of 0.5 to 1.0 ml/kg/hr (0.6 ml/kg/hr) suggests that a patient may still develop early AKI despite maintainingan average urine output within 0.5 to 1.0 ml/kg/hr. Interestingly, patients who developedearly AKI had a worse initial and worst BD in the first 24 hours, suggesting a greater degreeof shock with its associated malperfusion. Cartotto et al19 have shown that a 24-hour BD <−6 was associated with a greater degree of systemic inflammatory response syndrome,ARDS, and MODS. Similarly, Cochran et al20 have shown BD and lactate values in the first24 hours to be significantly worse in nonsurvivors. This is similar to other burn studies,which have shown elevated BDs to be associated with more extensive burns, inhalationinjuries, higher than anticipated fluid requirements, and an increased risk of death.21–23Thus, perhaps the greater degree of inflammation and malperfusion in these patients leads tothe development of early AKI, with its associated increased mortality. However, currentlyavailable methods of monitoring resuscitation, including preload monitoring, BD, and otherindices of shock, have not been proven superior to target mean arterial pressure and urinaryoutput,23–25 and it remains unknown whether an effort to actively correct these parameterswould lead to improved outcomes.
The high incidence of early AKI, coupled with the lack of difference in total resuscitationvolume in the two groups, may also suggest that adjunct therapies to counter burn-associatedsystemic inflammation should be considered to mitigate early complications. These mayinclude high-dose ascorbic acid, plasma exchange therapy, or early institution of RRT forAKI, as advocated by a recent report by the U.S. Army Institute of Surgical Research.26–28
Although each of these highly promising interventions is currently practiced at variouscenters, confirmation by well-conducted prospective randomized trials, such as theanticipated multicenter trials group investigation of early continuous RRT, is necessarybefore they are widely accepted by the burn community.
Our study has several limitations to consider. First, this cohort is limited to adults with burnsof ≥20% TBSA and, therefore, does not address children or patients who are less severelyburned, hence, may be less generalizable to children or those with smaller burns. Second,the retrospective nature of our cohort study hindered the completeness of data acquisition,such that although average urine output could be calculated, individual hourly urine output,periods of hypotension, and invasive measurements of intravascular volume status were notavailable. Third, baseline creatinine values before injury were not known and, thus, requiredestimation, given the outcome of interest of development of AKI at 24 hours. This is aninherent limitation to research in injured patients, because it is not possible to verify actual
Mosier et al. Page 6
J Burn Care Res. Author manuscript; available in PMC 2011 February 27.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

baseline (preinjury) creatinine. Although imperfect, we estimated baseline creatinine levelsusing reference values provided by the Acute Dialysis Quality Initiative Group, who usedthe modification of diet in renal disease equation, taking into account age, sex, and ethnicity.Finally, the outcomes we selected—progressive renal dysfunction, RRT, and hospitalmortality—may not capture all relevant consequences of AKI. Increased resource utilizationin and out of the burn ICU, subsequent development of chronic kidney disease, and need forfuture RRT because of successive acute, chronic, or acute and chronic injuries are allpotential additional outcomes of significance. Future analysis of RRT initiation may alsosuggest optimal timing and intensity of renal replacement for improved outcomes.
CONCLUSIONAKI after burn injury is a common occurrence, with a quarter of patients developing earlyAKI and nearly half developing AKI over the acute hospitalization. Early AKI can beprogressive and is more likely with larger TBSA burns. Patients with early AKI have asignificantly increased mortality. Better understanding of the pathophysiology of AKIduring burn shock, recognition of its significance, and improved treatment may improvefuture outcomes in severely burned patients.
AcknowledgmentsWe thank the contribution of the Inflammation and the Host Response to Injury Large-Scale Collaborative ProjectAward 2-U54-GM062119 from the National Institute of General Medical Sciences, KL2 (1KL2RR025015-01)from the National Center for Research Resources), and the David and Nancy Auth-Washington ResearchFoundation Endowment.
Supported by the National Institute of General Medical Sciences.
This manuscript was prepared using a dataset obtained from the Glue Grant program and does not necessarilyreflect the opinions or views of the Inflammation and the Host Response to Injury Investigators or the NIGMS.
REFERENCES1. Mustonen KM, Vuola J. Acute renal failure in intensive care burn patients. J Burn Car Res
2008;29:227–237.2. Holm C, Horbrand F, von Donnersmarck GH, Mühlbauer W. Acute renal failure in severely burned
patients. Burns 1999;25:171–178. [PubMed: 10208394]3. Bellomo R, Ronocco C, Kellum JA, Mehta RL, Palevsky P. Acute Dialysis Quality Initiative
Workgroup. Acute renal failure—definition, outcome measures, animal models, fluid therapy andinformation technology needs: the Second International Consensus Conference of the AcuteDialysis Quality Initiative (ADQI) Group. Crit Care 2004;8:R204–R212. [PubMed: 15312219]
4. Ricci Z, Cruz D, Ronco C. The RIFLE criteria and mortality in acute kidney injury: a systematicreview. Kidney Int 2008;73:538–546. [PubMed: 18160961]
5. Hoste EA, Clemont G, Kersten A, et al. RIFLE criteria for acute kidney injury are associated withhospital mortality in critically ill patients: a cohort analysis. Crit Care 2006;10:R73. [PubMed:16696865]
6. Bagshaw SM, George C, Dinu I, Bellomo R. A multi-centre evaluation of the RIFLE criteria forearly acute kidney injury in critically ill patients. Nephrol Dial Transplant 2008;23:1203–1210.[PubMed: 17962378]
7. Chung KK, Juncos LA, Wolf SE, et al. Continuous renal replacement therapy improves survival inseverely burned military casualties with acute kidney injury. J Trauma 2008;64:S179–S187.discussion S185–7. [PubMed: 18376163]
8. Coca SG, Bauling P, Schifftner T, Howard CS, Teitelbaum I, Parikh CR. Contribution of acutekidney injury toward morbidity and mortality in burns: a contemporary analysis. Am J Kidney Dis2007;49:517–523. [PubMed: 17386319]
Mosier et al. Page 7
J Burn Care Res. Author manuscript; available in PMC 2011 February 27.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
9. Klein MB, Hayden D, Elson C, et al. The association between fluid administration and outcomefollowing major burn: a multicenter study. Ann Surg 2007;245:622–628. [PubMed: 17414612]
10. Charlson M, Szatrowski TP, Peterson J, Gold J. Validation of a combined comorbidity index. JClin Epidemiol 1994;47:1245–1251. [PubMed: 7722560]
11. Barrantes F, Tian J, Vazquez R, Amoateng-Adjepong Y, Manthous CA. Acute kidney injurycriteria predict outcomes of critically ill patients. Crit Care Med 2008;36:1397–1403. [PubMed:18434915]
12. Davies MP, Evans J, McGonigle RJ. The dialysis debate: acute renal failure in burn patients. Burns1994;20:71–73. [PubMed: 8148082]
13. Schiavon M, Di Landro D, Baldo M, De Silvestro G, Chiarelli A. A study of renal damage inseverely burned patients. Burns 1988;14:107–114.
14. Aikawa N, Wakabayashi G, Ueda M, Shinozawa Y. Regulation of renal function in thermal injury.J Trauma 1990;30:S174–S178. [PubMed: 2147724]
15. Planas M, Wachtel T, Frank H, Henderson LW. Characterization of acute renal failure in theburned patient. Arch Intern Med 1982;142:2087–2091. [PubMed: 7138158]
16. Cancio LC, Chavez S, Alvarado-Ortega M, et al. Predicting increased fluid requirements duringthe resuscitation of thermally injured patients. J Trauma 2004;56:404–413. discussion 413–4.[PubMed: 14960986]
17. Pham TN, Cancio LC, Gibran NS. American Burn Association practice guidelines burn shockresuscitation. J Burn Care Res 2008;29:257–266. [PubMed: 18182930]
18. Ennis JL, Chung KK, Renz EM, et al. Joint Theater Trauma System implementation of burnresuscitation guidelines improves outcomes in severely burned military casualties. J Trauma2008;64:S146–S151. [PubMed: 18376158]
19. Cartotto R, Choi J, Gomez M, Cooper A. A prospective study on the implications of a base deficitduring fluid resuscitation. J Burn Car Rehabil 2003;24:75–84.
20. Cochran A, Edelman L, Saffle J, Morris SE. The relationship of serum lactate and base deficit inburn patients to mortality. J Burn Care Res 2007;28:231–240. [PubMed: 17351438]
21. Kaups KL, Davis J, Dominic WJ. Base deficit as an indicator of resuscitation needs in patientswith burn injuries. J Burn Car Rehabil 1998;19:346–348.
22. Wolf SE, Rose J, Desai MH, Mileski JP, Barrow RE, Herndon DN. Mortality determinants inmassive pediatric burns: an analysis of 103 children with > or = 80% TBSA burns (> or = 70%full-thickness). Ann Surg 1997;225:554–565. [PubMed: 9193183]
23. Jeng JC, Lee K, Jablonski K, et al. Serum lactate and base deficit suggest inadequate resuscitationof patients with burn injuries: application of a point of care laboratory instrument. J Burn CarRehabil 1997;18:402–405.
24. Cancio LC, Galvez E Jr, Turner CE, Jordan MH. Base deficit and alveolar-arterial gradient duringresuscitation contribute independently but modestly to the prediction of mortality after burn injury.J Burn Care Res 2006;27:289–296. discussion 296–7. [PubMed: 16679895]
25. Holm C, Mayr M, Tegeler J, et al. A clinical randomized study on the effects of invasivemonitoring on burn shock resuscitation. Burns 2004;30:798–807. [PubMed: 15555792]
26. Tanaka H, Matsuda T, Miyagantani Y, Yukioka T, Matsuda H, Shimazaki S. Reduction ofresuscitation fluid volumes in severely burned patients using ascorbic acid administration: arandomized, prospective study. Arch Surg 2000;135:326–331. [PubMed: 10722036]
27. Chung KK, Juncos L, Wolf SE, et al. Continuous renal replacement therapy improves survival inseverely burned military casualties with acute kidney injury. J Trauma 2008;64:S179–S185.[PubMed: 18376163]
28. Kravitz M, Warden G, Sullivan JJ, Saffle JR. A randomized trial of plasma exchange in thetreatment of burn shock. J Burn Car Rehabil 1989;10:17–26.
Mosier et al. Page 8
J Burn Care Res. Author manuscript; available in PMC 2011 February 27.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Figure 1.Early acute kidney injury was common (28%) and associated with higher mortality,especially if it was progressive: 13 patients with renal deterioration died (72%).
Mosier et al. Page 9
J Burn Care Res. Author manuscript; available in PMC 2011 February 27.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Figure 2.Late onset acute kidney injury was also common (29.6%) and was also associated withincreased mortality (34%).
Mosier et al. Page 10
J Burn Care Res. Author manuscript; available in PMC 2011 February 27.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Mosier et al. Page 11
Table 1
Rifle classification3
Category GFR Criteria UOP Criteria
Risk Increased SCr × 1.5 or GFR decrease >25% UOP <0.5 ml/kg/hr × 6 hr
Injury Increased SCr × 2 or GFR decrease >50% UOP <0.5 ml/kg/hr × 12 hr
Failure Increased SCr × 3 or GFR decrease 75%, or SCr >4mg/dl UOP <0.3 ml/kg/hr × 24hr or anuria × 12 hr
Loss Persistent ARF = complete loss of kidney function >4 wk
End stage End-stage kidney disease (> 3 mo)
Scr, serum creatinine; GFR, glomerular filtration rate; UOP, urinary output; ARF, acute renal failure.
J Burn Care Res. Author manuscript; available in PMC 2011 February 27.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Mosier et al. Page 12
Table 2
Patient comorbidities
ComorbidityTotal
Number (%)Early
AKI (%)No
AKI (%)
Smoking 95 (43) 24 (39) 71 (45)
Alcohol 40 (18) 13 (21) 27 (17)
Hypertension 39 (18) 21 (34) 18 (11)
Psychiatric illness 38 (17) 10 (16) 28 (18)
COPD/asthma 21 (10) 8 (13) 13 (8)
Diabetes 19 (9) 8 (13) 11 (7)
TBI/seizure disorder 15 (7) 5 (8) 10 (6)
Liver disease 10 (5) 5 (8) 5 (3)
MI 9 (4) 4 (6) 5 (3)
Cancer 8 (4) 4 (6) 4 (3)
Hypercholesterolemia 7 (3) 3 (5) 4 (3)
CAD 6 (3) 3 (5) 3 (2)
CHF/valvular disease 6 (3) 4 (6) 2 (1)
Rheumatologic disease 5 (2) 3 (5) 2 (1)
PVD/AAA 5 (2) 2 (3) 3 (2)
Dysrhythmia 4 (2) 2 (3) 2 (1)
Hypothyroidism 4 (2) 3 (5) 1 (1)
CVA 4 (2) 4 (6) 0 (0)
Dementia/Parkinson’s disease
2 (1) 0 (0) 2 (1)
PUD 2 (1) 1 (2) 1 (1)
Hyperthyroid 1 (<1) 0 (0) 1 (1)
Crohn disease 1 (<1) 0 (0) 1 (1)
HIV 1 (<1) 0 (0) 1 (1)
History of advanced cancer 1 (<1) 1 (2) 0 (0)
Pregnancy 1 (<1) 0 (0) 1 (1)
AKI, acute kidney injury; COPD, chronic obstructive pulmonary disease; TBI, traumatic brain injury; MI, myocardial infarction; CAD, coronaryartery disease; CHF, congestive heart failure; PVD, peripheral vascular disease; AAA, abdominal aortic aneurysm; CVA, cerebral vascular accident;PUD, peptic ulcer disease.
J Burn Care Res. Author manuscript; available in PMC 2011 February 27.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Mosier et al. Page 13
Table 3
Charlson score
Assigned Weightsfor Conditions* Conditions
1 Acute myocardial infarction
Congestive heart failure
Peripheral vascular disease
Cerebrovascular disease
Dementia
Chronic pulmonary disease
Connective tissue disorder
Peptic ulcer disease
Mild liver disease
Diabetes
2 Hemiplegia
Moderate or severe renal disease
Diabetes with end-organ damage
Any tumor
Leukemia
Lymphoma
3 Moderate or severe liver disease
6 Metastatic tumor
Acquired immunodeficiency syndrome (AIDS)
*Total equals comorbidity score.10
J Burn Care Res. Author manuscript; available in PMC 2011 February 27.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Mosier et al. Page 14
Table 4
Patient and injury characteristics by development of AKI
VariableAKI
(n = 62)No AKI(n = 159) P
Age 50.8 (18.3) 39.1 (14.0) <.01
% Male 69.4 74.2 .47
BMI 30.1 (8.8) 27.9 (11.7) .09
% TBSA 42.5 (17.6) 41.8 (19.4) .40
% Full-thickness 33.1 (21.0) 29.9 (19.1) .14
Burn mechanism
Flame/flash 87.1 91.8 .32
Scald 3.2 3.8
Other 9.7 4.4
Inhalation injury 45.2 36.7 .25
APACHE II 23.6 (9.0) 19.4 (9.0) <.01
Nonrenal APACHE II ≥20 (%) 59.7 50.9 .24
Comorbidity present (%) 41.9 20.8 <.01
Data are reported as means (±SD) or percentage, where appropriate.
AKI, acute kidney injury; BMI, body mass index; APACHE, Acute Physiology and Chronic Health Evaluation.
J Burn Care Res. Author manuscript; available in PMC 2011 February 27.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Mosier et al. Page 15
Table 5
First 24-hr resuscitation
VariableAKI
(n = 62)No AKI(n = 159) P
Injury to admission (hr) 4.1 (4.9) 4.4 (7.1) .36
Preadmission fluid (observed/expected)
1.5 (1.2) 2.5 (3.2) .08
Initial BD −6.5 (5.7) −4.9 (4.0) .01
Worst BD −8.0 (5.5) −6.1 (4.3) <.01
Albumin 318.1 (451.4) 330.6 (776.1) .45
Parkland score 1.24 (0.50) 1.32 (0.62) .82
Urine output (ml/kg/hr)
0.60 (0.35) 1.16 (0.67) <.01
Data are reported as means (±SD) or percentage, where appropriate.
AKI, acute kidney injury; BD, base deficit.
J Burn Care Res. Author manuscript; available in PMC 2011 February 27.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Mosier et al. Page 16
Table 6
Unadjusted logistic regression for development AKI
Variable Odds Ratio P 95% CI
Age 1.05 <.01 1.03–1.07
% TBSA 1.00 .81 0.99–1.02
Presence of a comorbidity 2.76 <.01 1.46–5.20
Nonrenal APACHE II >20 1.42 .24 0.79–2.58
NROF ≥2 4.07 <.01 1.55–10.68
Injury to admission (hr) 0.99 .72 0.94–1.04
Preadmission fluid ratio (observed/expected)
0.78 .02 0.64–0.96
Initial BD 0.93 .04 0.87–0.99
Worst BD first 24 hr 0.92 .02 0.86–0.98
AKI, acute kidney injury; APACHE, Acute Physiology and Chronic Health Evaluation; BD, base deficit; NROF, nonrenal organ failure.
J Burn Care Res. Author manuscript; available in PMC 2011 February 27.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Mosier et al. Page 17
Table 7
Multivariate logistic regression for development of early AKI
VariableOddsRatio P 95% CI
Age 1.06 <.01 1.03–1.09
Presence of a comorbidity 0.87 .76 0.34–2.18
Preadmission fluid ratio (observed/expected)
0.60 <.01 0.43–0.82
NROF ≥2 1.81 .36 0.51–6.33
Initial BD 1.06 .61 0.85–1.32
Worst BD first 24 hr 0.81 .07 0.65–1.02
AKI, acute kidney injury; BD, base deficit; NROF, nonrenal organ failure.
J Burn Care Res. Author manuscript; available in PMC 2011 February 27.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Mosier et al. Page 18
Table 8
Treatment and hospitalization outcomes, by development of Acute Kidney Injury (AKI)
Variable AKI (n = 62) No AKI (n = 159) P
24-hr resuscitation (Parkland score) 1.24 (0.50) 1.32 (0.62) .82
48-hr resuscitation (Parkland score) 0.52 (0.33) 0.45 (0.35) .09
24-hr urine output (ml/kg/hr) 0.60 (0.35) 1.16 (0.67) <.01
48-hr urine output (ml/kg/hr) 0.91 (0.47) 1.06 (0.54) .03
No. transfusions 8.6 (8.5) 9.3 (16.4) .63
Amount transfused (ml) 7181 (8019) 7172 (9601) .50
Abdominal compartment syndrome (%) 3.2 3.1 .97
Escharotomies (%) 30.7 33.3 .70
Total operations* 5.9 (4.9) 4.8 (4.4) .05
Length of stay (d)† 52.37 (28.75) 47.56 (41.89) .25
ICU length of stay (d)† 37.13 (29.22) 34.08 (41.11) .34
Ventilator days† 17.18 (15.25) 16.85 (25.03) .47
Early-onset NROF ≥2 (%) 17.7 5.0 <.01
ARDS (%) 37.1 32.1 .48
Pneumonia (%) 50.0 48.4 .83
Sepsis (%) 11.3 7.5 .37
Mortality (%) 35.5 13.2 <.01
Data are reported as means (±SD) or percentage, where appropriate.
*Calculated only in patients who underwent operations.
†Calculated in survivors only.
AKI, acute kidney injury; ICU, intensive care unit; NROF, nonrenal organ failure; ARDS, acute respiratory distress syndrome.
J Burn Care Res. Author manuscript; available in PMC 2011 February 27.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Mosier et al. Page 19
Table 9
Unadjusted logistic regression for mortality
VariableOddsRatio P 95% CI
Age 1.05 <.01 1.03–1.07
% TBSA 1.06 <.01 1.04–1.08
% Full thickness 1.05 <.01 1.03–1.07
Inhalation injury 2.34 .01 1.19–4.60
Male 1.11 .80 0.52–2.36
BMI 1.00 .97 0.97–1.03
Early AKI 3.61 <.01 1.81–7.23
AKI over hospitalization 9.08 <.01 3.64–22.62
Nonrenal APACHE II ≥20 2.70 .01 1.30–5.60
Early-onset NROF ≥2 9.46 <.01 3.45–25.90
Presence of a comorbidity 3.99 <.01 1.98–8.03
AKI, acute kidney injury; APACHE, Acute Physiology and Chronic Health Evaluation; NROF, nonrenal organ failure.
J Burn Care Res. Author manuscript; available in PMC 2011 February 27.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Mosier et al. Page 20
Table 10
Adjusted logistic regressions for mortality
VariableOddsRatio P 95% CI
Without early-onset NROF factor
Early AKI 2.87 .03 1.11–7.45
Age 1.07 <.01 1.04–1.11
% TBSA 1.09 <.01 1.06–1.12
Inhalation injury 1.07 .88 0.43–2.68
Nonrenal APACHE II ≥20 1.39 .51 0.52–3.70
Presence of a comorbidity 1.61 .37 0.57–4.31
With early-onset NROF factor
Early AKI 2.32 .10 0.85–6.36
Age 1.07 <.01 1.04–1.12
% TBSA 1.09 <.01 1.06–1.12
Inhalation injury 0.79 .64 0.29–2.13
Nonrenal APACHE II ≥20 1.11 .83 0.41–3.05
Presence of a comorbidity 1.44 .50 0.49–4.22
Early-onset NROF ≥2 4.52 .03 1.20–17.05
AKI, acute kidney injury; APACHE, Acute Physiology and Chronic Health Evaluation; NROF, nonrenal organ failure.
J Burn Care Res. Author manuscript; available in PMC 2011 February 27.
Related Documents











