-
8/8/2019 Dystocia 2003 Comp
1/106
PREPARED BY;
MARJORIE GALICIA ROMANO
Clinical Instructor
-
8/8/2019 Dystocia 2003 Comp
2/106
PROBLEMS WITH THE PASSANGER
A. Fetal malposition: the ideal fetal position is flexed
with occiput in the right or left anterior quadrant of thematernal pelvis
1. Types of malpositions
a. Occiput posterior (OP) position
1) Right or left OP position occurs in about 25% ofall term pregnancies but usually rotates toocciput anterior (OA) as labor progresses
2) Failure to rotate is termed persistent occiputposterior
3) Maternal risk include prolonged labor, potential foroperative delivery, extension of the episiotomy, 3rd-
or 4th- degree of laceration of the perineum
-
8/8/2019 Dystocia 2003 Comp
3/106
4) Maternal syptoms include intense back pain inlabor, dysfunctional labor pattern, prolonged
active phase, secondary arrest of dilation, and/orarrest of descent
Possible Problem
yProlonged active phaseyArrested descent
Risk Factors
yAndroid pelvis
yAntrhopid pelvis
yContracted pelvis
-
8/8/2019 Dystocia 2003 Comp
4/106
b. Occiput tranverse (OT) position
1) Incomplete rotation of OP position to OA
results in the fetal head being in a horizontal ortranverse position (OT)
2) Persistent occiput tranverse position occurs as
a result of ineffective contractions or a flattenedbony pelvis
3) In the absence of abnormal pelvic structure,vaginal delivery can be accomplished bystimulating contractions with oxytocin (Pitocin)and application of forceps for delivery
-
8/8/2019 Dystocia 2003 Comp
5/106
2. Nursing care
a. Encourage the mother to lie on her side opposite from thefetal back, which may help with rotation
b. Knee-chest position may facilitate rotation
c. Pelvic rocking may help with rotation
d. Apply sacral counter-pressure with heel of the hand to
relieve back paine. Continue support and ecouragement
1) Keep client and family informed of progress
2) Encourage relaxation with contractions
3) Praise clients efforts to maintain controlf. Anticipate forceps/manual rotation and forceps- assistedbirth
-
8/8/2019 Dystocia 2003 Comp
6/106
MEDICAL MANAGEMENTa. Forceps: metal instruments applied to the fetal head to
facilitate delivery1) Provides traction or means of rotating the fetalhead
2) Risk are fetal ecchymosis or edema of the face,
transient facial paralysis, maternallacerations, or episiotomy extensions
b. Vacuum extraction: a suction cup applied to the fetal headto facilitate delivery
1) Provides traction to shorten the second stage oflabor
2) Risk are newborn cephalhematoma, retinalhemorrhage, and intracranial hemorrhage
-
8/8/2019 Dystocia 2003 Comp
7/106
FETAL MALPRESENTATION
1. Vertex malpresentations are caused by failure of the fetus to
assume a flexed attitudea. Brow presentation
1) Fetal forehead is the presenting part
2) 50% convert to vertex or face presentation
b. Face presentation1) Increased risk of prolonged labor and operative
delivery
2) Anticipate vaginal delivery if pelvis is adequate
and the chin (mentum) is in the anterior
position
3) Anticipate cesarean delivery if mentum is
posterior or signs of fetal distress occur
-
8/8/2019 Dystocia 2003 Comp
8/106
4) Fetal monitor electrode should not be placed
on the presenting part (infants face); requiresexternal fetal heart rate monitoring.
5) Edema and bruising of the face, eyes, and lips
are common occurrences clients should beprepared for this possibility before seeing the
infant for the first time
-
8/8/2019 Dystocia 2003 Comp
9/106
-
8/8/2019 Dystocia 2003 Comp
10/106
Caput succedaneum
-
8/8/2019 Dystocia 2003 Comp
11/106
A--Complete flexion. B-- Moderate flexion. C--Poor flexion. D--Hyperextension
-
8/8/2019 Dystocia 2003 Comp
12/106
TYPES OF ATTITUDE
-
8/8/2019 Dystocia 2003 Comp
13/106
y (a) Complete flexion. This is normal attitude in cephalicpresentation. With cephalic, there is complete flexion atthe head when the fetus "chin is on his chest." This
allows the smallest cephalic diameter to enter the pelvis,which gives the fewest mechanical problems withdescent and delivery.
y (b) Moderate flexion or military attitude. In cephalicpresentation, the fetus head is only partially flexed ornot flexed. It gives the appearance of a military person atattention. A larger diameter of the head would be
coming through the passageway.
-
8/8/2019 Dystocia 2003 Comp
14/106
y (c) Poor flexion or marked extension. In reference to thefetus head, it is extended or bent backwards. This would
be called a brow presentation. It is difficult to deliverbecause the widest diameter of the head enters the pelvisfirst. This type of cephalic presentation may require aC/Section if the attitude cannot be changed.
y (d) Hyperextended. In reference to the cephalic position,the fetus head is extended all the way back. This allows aface or chin to present first in the pelvis. If there isadequate room in the pelvis, the fetus may be delivered
vaginally.
-
8/8/2019 Dystocia 2003 Comp
15/106
Sincipital presentation (Military Attitude)
1) Larger diameter of the fetal head is presented
2) Labor progress is slowed with slower descent of the fetalhead
Breech Presentation
There are three types of breech presentation1. Complete breech: sacrum is the presenting part, knees
flexed
2. Frank breech: sacrum is the presenting part, legs are
extended3. Incomplete: (footling) one or both feet are presenting,
increasing the risk of umbilical cord prolapse
-
8/8/2019 Dystocia 2003 Comp
16/106
What causes a breech presentation?
The causes of breech presentations are not fullyknown. However, a breech birth is morecommon :
y In subsequent pregnancies
y In pregnancies of multiplesyWhen there is history of premature delivery
yWhen the uterus has too much or too little amnioticfluid
y In an abnormal shaped uterus or a uterus withabnormal growths, such as fibroids.
y For women with placenta previa
-
8/8/2019 Dystocia 2003 Comp
17/106
-
8/8/2019 Dystocia 2003 Comp
18/106
-
8/8/2019 Dystocia 2003 Comp
19/106
Maternal Risk
1) Prolonged labor due to decreasepressure exerted by breech on thecervix
2) Cesarean or forceps delivery
3) Trauma to birth canal during deliveryfrom manipulation and forceps to free
fetal head4) Intra partum or postpartumhemorrhage
-
8/8/2019 Dystocia 2003 Comp
20/106
Delivery of Breech Presentation by Forceps
-
8/8/2019 Dystocia 2003 Comp
21/106
Vaginal delivery versus cesarean for breech
birth?
Most health care providers do not believe a vaginal deliveryis possible for a breech birth, although some will wait tomake that decision until a woman is in labor. However,
the following are often necessary in order for a vaginalbirth to be attempted:
y The baby is full-term and in the frank breechpresentation
y The baby does not show signs of distress while its heartrate is closely monitored
y The process of labor is smooth and steady; the cervix iswidening and the baby is moving down
-
8/8/2019 Dystocia 2003 Comp
22/106
y The health care provider estimates that the baby is not
too big or the mother's pelvis too narrow for the babyto pass safely through the birth canal
y Anesthesia is available and a cesarean delivery can beperformed on short notice
-
8/8/2019 Dystocia 2003 Comp
23/106
Piper forceps - applied to the after comingfetal head
-
8/8/2019 Dystocia 2003 Comp
24/106
EXTERNAL CEPHALIC VERSIONManipulation of the fetus through the abdominal wall from
a breech or shoulder presentation to a vertexpresentation:
y May be done as early as 34 to 35 wks or usual time is 37 to38 wks
y
Client is placed on external fetal monitor and possiblyUTZ are recorded continuously
y IV fluids are started
y Terbutaline is administered via piggybacked IV line torelax the uterine muscle
y FHR is closely monitored during version attempt
yVersion is discontinued if undue maternal or fetal distressis noted
-
8/8/2019 Dystocia 2003 Comp
25/106
VERSION
y
The breech and vertex of the fetus are graspedtransabdominally by the examiners hands onthe womans abdomen.
yGentle pressure is then exerted to rotate thefetus in a forward direction to a cephalic lie.
yThe use of external version can decrease thenumber of cesarean section from breech
presentation.
-
8/8/2019 Dystocia 2003 Comp
26/106
Contraindication
y Multiple gestation
y Severe oligohydramnios
y Contraindications to vaginal births - The mother hasa condition (such as a heart problem) that prevents
her from receiving certain tocolytic medicines toprevent uterine contractions.
y Cord coil
y Unexplained third trimester bleeding (placenta
previa )
-
8/8/2019 Dystocia 2003 Comp
27/106
y The bag of waters (amniotic sac) has ruptured.
yA cesarean delivery is needed, such as when theplacenta partially or completely covers the cervix(placenta previa) or has separated from the wall ofthe uterus (placenta abruptio).
y Fetal monitoring shows that the fetus may not be
doing well.y The fetus has a hyperextended head. This means
that the neck is straight, rather than bending thehead forward with the chin tucked into the chest.
y The fetus is known or suspected to have a birthdefect.
y The mother's uterus does not have a normal shape.
-
8/8/2019 Dystocia 2003 Comp
28/106
External cephalic version has an average success rateof 58%. Version is most likely to succeed when:
y The mother has already had at least one pregnancyand childbirth.
y The fetus, or a foot or leg, has not dropped down intothe pelvis (has not engaged).
y The fetus is surrounded by a normal amount ofamniotic fluid.
y The procedure is performed near term (34 or more
completed weeks of pregnancy), before labor starts.
-
8/8/2019 Dystocia 2003 Comp
29/106
Version is least likely to succeed when:
y The fetus is engaged down in the mother's pelvis.
y The doctor cannot grasp the fetal head.
y The uterus is hard or tense to the touch.
yAbout 4% of fetuses return to a breech position after asuccessful version.
Compared to the first attempt, repeat version attemptsare less likely to be successful.
-
8/8/2019 Dystocia 2003 Comp
30/106
Risksy With frequent monitoring, the risks of external cephalic version
to the mother and fetus are low.
y Potential risks of version, for which the fetus and mother areclosely monitored, include:
y Twisting or squeezing of the umbilical cord, reducing blood flowand oxygen to the fetus.
y The beginning of labor, which can be caused by rupture of theamniotic sac around the fetus (premature rupture of themembranes, or PROM).
y Placenta abruptio, rupture of the uterus, or damage to theumbilical cord. The potential exists for such complications, but
they are very rare.On the rare occasion that labor begins or the fetus or mother
develops a serious problem during version, an emergencycesarean section (C-section) may be done to deliver the fetus.
-
8/8/2019 Dystocia 2003 Comp
31/106
Shoulder PresentationTranverse lie acromium process is the presenting part
a. Vaginal delivery is not considered possible in terminfant
b. CS is preferred method of delivery
Causes
y Prematurity
y Placenta Previa
yAbnormal uterus
y Contracted pelvis or relaxed abdominal wally Polyhydramnios
-
8/8/2019 Dystocia 2003 Comp
32/106
Shoulder presentation
-
8/8/2019 Dystocia 2003 Comp
33/106
SHOULDER PRESENTATION WITH PROLAPSED ARM
-
8/8/2019 Dystocia 2003 Comp
34/106
FETAL DISTRESS
- Insufficient oxygen supply to meet the demands of the
fetus
Causes
a. Compression of the umbilical cord
b. Uteroplacental insufficiency caused by placentalabnormalities or maternal condition
Signs and Sypmtoms
a. Meconium-stained amniotic fluid (excludingbreech presentation
-
8/8/2019 Dystocia 2003 Comp
35/106
b. Changes in fetal heart rate baseline
1) Tachycardia (above 160): early sign of distress
2) Bradycardia (below 110): late sign of distressc. Decreased or absence of variability of heart rate
1) Heart rate varies less than 2 to 5 beats per
minute causing a f lattened appearance to theheart rate
2) Indicates depression of the autonomic
nervous system that controls heart rate
3) Fetal sleep, sedation, and hypoxia may affect
variability
-
8/8/2019 Dystocia 2003 Comp
36/106
Late deceleration
1. Fetal heart rate slows following the peak of a contractionand slowly returns to baseline rate during the restingphase
2. Indicates fetal response to hypoxia from uteroplacentalinsufficiency
3. Considered an omnious pattern regardless of the depthof the deceleration of the FHR and requires immediateintervention
-
8/8/2019 Dystocia 2003 Comp
37/106
Nursing management
(uteroplacental insufficiency)
yReposition the mother on her left side
yAdminister oxygen via face-mask at 8-10
lpmyIncrease IV fluids
yDiscontinue oxytocin infusion, if labor is
being inducedyNotify the doctor
-
8/8/2019 Dystocia 2003 Comp
38/106
-
8/8/2019 Dystocia 2003 Comp
39/106
-
8/8/2019 Dystocia 2003 Comp
40/106
-
8/8/2019 Dystocia 2003 Comp
41/106
Severe variable deceleration
1. Fetal heart rate repeatedly deceleratesbelow 90 beats/min. for over 60 secs.before returning to baseline
2.Indicates interference of fetal blood flowfrom cord compression
3. Leads to fetal hypoxia and low APGAR
scores unless steps are taken to correct it
-
8/8/2019 Dystocia 2003 Comp
42/106
Nursing management
(cord compression)yReposition the mother on her side
y If not corrected, reposition to opposite side
y
Administer oxygen by face-mask at 8-10 lpmyTrendelenburg or knee-chest position, if not
corrected
y
Perform vaginal examination and applyupward digital pressure on the presenting partto relieve pressure on the cord.
-
8/8/2019 Dystocia 2003 Comp
43/106
AMNIOINFUSION
Amniotic fluid may be replacedwith warmed saline through anintrauterine catheter when signs
of cord compression are presentduring labor after PROM.
Infusion is continued until signsof cord compression disappear.
-
8/8/2019 Dystocia 2003 Comp
44/106
SEVERE VARIABLE DECELERATION
-
8/8/2019 Dystocia 2003 Comp
45/106
-
8/8/2019 Dystocia 2003 Comp
46/106
The two most common applications of transcervical
amnioinfusion are treatment of severe variable
decelerations and dilution of thick meconium fluidduring labor.
The greatest attractions of amnioinfusion have been
that it is easy to perform, inexpensive and safe.
After an initial bolus of 250 mL, normal saline is
infused at a rate of 10 to 20 mL per hour.
-
8/8/2019 Dystocia 2003 Comp
47/106
AMNIOINFUSION PROCEDURE
-
8/8/2019 Dystocia 2003 Comp
48/106
TECHNIQUE
y Amnioinfusion can per performed via a transcervical or
transabdominal route. The transcervical route is preferredbecause it is does not require ultrasound guidance and easily
allows for repeated fluid instillation.
y Transcervical approach A lactated Ringers or normal saline
(without dextrose) solution is infused into the amniotic cavitythrough an intrauterine pressure catheter. Normal saline
solution may cause derangement of neonatal electrolytes, thus
lactated ringers is preferable. Most protocols call for a bolus
infusion of 250 to 1,000 mL of fluid at a rate of 10 to 15mL/minute, followed by a continuous infusion of 100 to 200
mL/hour via pump infusion or gravity. Alternatively, repeat
boluses may be administered, as needed.
-
8/8/2019 Dystocia 2003 Comp
49/106
yThere is no evidence that the fluid needs to bewarmed above ambient room temperature
prior to administration. A blood warmer
should be used if warming to body
temperature is desired. In cases of prolongedamnioinfusion, sonographic assessment of the
amniotic fluid volume is suggested to avoid
iatrogenic polyhydramnios.
-
8/8/2019 Dystocia 2003 Comp
50/106
INTRAUTERINE RESUCITATION
Administration of terbutaline(tocolytics), to stop uterinecontractions and provide an
opportunity for uteroplacentalcirculation to improve when
fetal distress is present duringthe first stage of labor.
-
8/8/2019 Dystocia 2003 Comp
51/106
PREVENTION OF MECONIUM ASPIRATION
1. If meconium is present during labor (green-tinged amniotic fluid), steps to prevent
aspiration at the time of delivery should be
taken
2. The nasopharynx of the infant is suctioned prior
to delivery of the chest and abdomen
3. Visualization of the larynx and vocal cords with
deep suction is performed immediately after
delivery and before the first breath is taken
-
8/8/2019 Dystocia 2003 Comp
52/106
PROLAPSED UMBILICAL CORD
yCause: fetus is not firmly engaged, allowing room
for the cord to move beyond (overt prolased) oralongside the presenting part (occult prolapse)
yContributing factors
a. rupture of membranes before engagement of thepresenting part
b. small fetus
c. Breech presentation
d. multifetal pregnancy
e. Tranverse lie
-
8/8/2019 Dystocia 2003 Comp
53/106
-
8/8/2019 Dystocia 2003 Comp
54/106
Overt prolapse, which is the most common, refers to
protrusion of the cord in advance of the fetal
presenting part, often through the cervical os and intoor beyond the vagina. The fetal membranes are
invariably ruptured in these cases and the cord is
visible or palpable on examination.
Occult prolapse occurs when the cord descendsalongside, but not past, the presenting part. It can
occur with intact or ruptured membranes. The
diagnosis should be considered in the setting of a
sudden, prolonged fetal heart rate deceleration. Anoccult prolapse often cannot be diagnosed with
certainty, but is suggested by clinical features (eg, fetal
bradycardia) and findings at cesarean delivery.
-
8/8/2019 Dystocia 2003 Comp
55/106
-
8/8/2019 Dystocia 2003 Comp
56/106
-
8/8/2019 Dystocia 2003 Comp
57/106
Managing UCP
-
8/8/2019 Dystocia 2003 Comp
58/106
Managing UCP
Goal of care: actions to relieve pressure on the cord and
restore fetal oxygenation
a. Place the mothers hip higher than her head
y Knee-chest position
yTrendelenburg position
b. Perform sterile vaginal exam pushing fetal
presenting part upward with fingers to relieve
pressure on the cord
c. Administer oxygen by face mask at 8-10 lpm
d. Maintain continuous electronic fetal monitoring
-
8/8/2019 Dystocia 2003 Comp
59/106
Managing UCP
e. Prepare for rapid delivery eithervaginally or cesarean section
f. If cord protrudes through the vagina,
determine that pulsation is present and
apply sterile saline soaked dressing toprevent drying
-
8/8/2019 Dystocia 2003 Comp
60/106
-
8/8/2019 Dystocia 2003 Comp
61/106
Abnormal size or shape of pelvisContracted pelvic inlet: anterior-posterior diameter less than
11 cm; transverse dm less than 12 cm.1. Caused by rickets in early life or inherited small pelvis
2. Makes engagement difficult
3. Influences fetal position and presentation
4. Risk of UCP
Contracted mid-pelvic plane: interspinous dm less than 9.5 cm
1. Hampers internal rotation of the fetal head
2. Secondary arrest of dilation or arrest of fetal head occursContracted pelvic outlet: interschial tuberous diameter
less than 11 cm
TRIAL OF LABOR
-
8/8/2019 Dystocia 2003 Comp
62/106
TRIAL OF LABOR
y The physician may allow labor to continue or
even stimulate labor with oxytocin when pelvicmeasurements are borderline to see if the fetal
head will descend making vaginal delivery
possible; if progressive changes in dilation andstation do not occur, a cesarean delivery is
performed
yUrge woman to void every 2 hours
yAssess UCP after membranes ruptured
yEmphasize advantage of vaginal delivery
-
8/8/2019 Dystocia 2003 Comp
63/106
Cephalopelvic disproportion (CPD)
1. Fetal head is too large to pass through thebony pelvis
2. Signs & symptoms: fetal head does not
descend even though there are strongcontractions
3. Maternal risks include prolonged labor,
exhaustion, hemorrhage, and infection4. Fetal risks include hypoxia and birth trauma
5. Cesarean birth is necessary
-
8/8/2019 Dystocia 2003 Comp
64/106
-
8/8/2019 Dystocia 2003 Comp
65/106
Fetal macrosomia
yNeonatal Risk (Vaginal delivery)
1. Cervical nerve palsy
2. Diaphragmatic nerve injury
3. Fracture clavicle
h ld
-
8/8/2019 Dystocia 2003 Comp
66/106
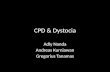
Shoulder Dystocia
y An obstetric emergency resulting from
difficulty or inability to deliver the shoulders.
Shoulder is too broad to enter and be born
through the pelvic outlet.
yFetal macrosomia increases the risk ofshoulder dystocia. Occurs at the second stage
of labor.
yMaternal Risk:1. Lacerations and tears of birth canal (vaginal
& cervical tears)
2. Postpartum hemorrhage
-
8/8/2019 Dystocia 2003 Comp
67/106
Shoulder Entrapment
-
8/8/2019 Dystocia 2003 Comp
68/106
y Neonatal Risks
1. Hypoxia
2. Fractures of clavicle or brachial plexus3. Injury to neck and head
y Risk Factors
1. Obesity
2. Increased fundal height
3. History of macrosomia
4. Maternal diabetes or gestational diabetes
5. Prolonged second-stage labor/descent arrest6. Post date pregnancy
7. Multiparity
-
8/8/2019 Dystocia 2003 Comp
69/106
-
8/8/2019 Dystocia 2003 Comp
70/106
-
8/8/2019 Dystocia 2003 Comp
71/106
-
8/8/2019 Dystocia 2003 Comp
72/106
McRoberts Maneuver
-
8/8/2019 Dystocia 2003 Comp
73/106
-
8/8/2019 Dystocia 2003 Comp
74/106
Rescue Maneuvers
y It is very rare that the baby cannot be delivered
by the maneuvers discussed so far. If theshoulder dystocia persists, however, other rescue
maneuvers include:
y Zavanelli Maneuve
r
.The baby's head and body are
pushed back into the uterus and cesarean
delivery is performed. Although there are some
risks to the mother and baby with this
procedure, there are many reports of itsuccessfully relieving severe shoulder dystocia.
This maneuver would be considered heroic and is
not practiced routinely.y .
-
8/8/2019 Dystocia 2003 Comp
75/106
-
8/8/2019 Dystocia 2003 Comp
76/106
Proctoepisiotomy.y
In this maneuver, the normal midlineepisiotomy is extended intentionally intothe rectum. Though this requires a
complex repair that can lead to futurerectal dysfunction, it can also serve towiden the birth canal posteriorly and
allow for disimpaction of the anteriorshoulder.
-
8/8/2019 Dystocia 2003 Comp
77/106
-
8/8/2019 Dystocia 2003 Comp
78/106
y Corkscrew. The shoulders of the baby are twisted
around and pushed out of the anterior-posterior (frontto back) plane. This may allow the front shoulder tocome out from behind the pubic bone and bedelivered.
y Delive
r
y of the fur
ther
ar
m. The obstetricianreaches back into the birth canal alongside the baby tograsp the baby's further hand or forearm and pull itout by sweeping it across the baby's chest. Once thearm is out, the rest of the baby's body is usually
delivered easily. The upper bone of the baby's arm,called the humerus, may be broken during thismaneuver, but it heals up quite easily.
-
8/8/2019 Dystocia 2003 Comp
79/106
Problems with Powers
-
8/8/2019 Dystocia 2003 Comp
80/106
Problems with Powers
A. Induction of labor: pharmacologic
and nonpharmacologic measures toinitiate contractions and cervicalchange
y Labor is started artificially
1. Methods of induction
a. Cervical Ripening1)Prostaglandins (PGE2) gel
2)Laminaria (hydrophilic agent)
D U d f I d ti f L b
-
8/8/2019 Dystocia 2003 Comp
81/106
Drugs Used for Induction of Labor
Drug Route/Action Side Effects & Potential
Complications
Prostaglandins(Cervidil;
Prepidil)
Intravaginally close tocervix;Causes softening &effacement or cervicalripening
Abdominal cramping, nausea,vomiting, diarrhea
Misoprostol(Cytotec)
Synthetic prostaglandinadministered orally orintravaginally to produce
contractions
Sudden onset of hypertoniccontractions & elevated restingtone of the uterus w/c may lead
to fetal distressOxytocin(Pitocin)
Synthetic oxytocinadministered IV in smallamts. & titrated toproduce contraction that
mimic normal labor
Uterine tetany & fetal distressare major concerns; can lead to
water intoxication,hyponatremia &
hypochloremia
Amniotomy
-
8/8/2019 Dystocia 2003 Comp
82/106
Amniotomyy Artificial rupture of membranes (AROM)
1) Auscultate FHR prior to and immediately afterAROM to detect prolapse of the umbilical cord or fetaldistress
2) Take maternal temperature q 1 to 2 hrs followingAROM to detect signs of infection
y Misoprostol (Cytotec) administration
1) administered orally/vaginally at doses of 25 to 50
mg2) Continuous monitoring of the FHR, uterineactivity, & maternal v/s is essential
y Oxytocin administration
-
8/8/2019 Dystocia 2003 Comp
83/106
y Oxytocin administration
1) Bishop score may be used to asses maternal
readiness for induction2) Prior to induction, begin external fetal monitoring
3) Assess & record maternal v/s, I&O, & contractionfrequency & intensity
4) Begin primary intravenous infusion
5) Mix oxytocin in 500 to 1000cc of IV balanced-saline fluids such as lactated Ringers & piggyback
into primary IV at a site as close to the client aspossible
6) Control & titrate the oxytocin solution using IVpump
-
8/8/2019 Dystocia 2003 Comp
84/106
-
8/8/2019 Dystocia 2003 Comp
85/106
Precipitate labor & birth
-
8/8/2019 Dystocia 2003 Comp
86/106
Precipitate labor & birth
y Rapid labor ( 3 hours) resulting in precipitous birth
y Maternal Risk
a. Cervical, vaginal, or rectal lacerations
b. Hemorrhage due to rapid passage through the birth
canalc. Injury at birth
y Interventionsa. Tocolytics
b. Do not leave the client; send someone or call for help
c. Don sterile gloves, if time allows
d. Instruct the client to pant or blow to decrease urge to push
d S t th i / t il t l i
-
8/8/2019 Dystocia 2003 Comp
87/106
d. Support the perineum w/ sterile towel as crowningoccurs
e. Apply gentle pressure on the fetal head to preventrapid delivery
1) lacerations of perineum can occur
2) Subdural or dural tears may occur w/ sudden
expulsion of the infants head
f. After delivery of the head, suction the infantsmouth then nose with bulb syringe
g. Check around the infants neck for possible tightumbilical cord; if present, cord must be clamped &cut before delivery
h Place hands on each side of the infants head &
-
8/8/2019 Dystocia 2003 Comp
88/106
h. Place hands on each side of the infant s head &instruct client to push
i. Gentle down ward pressure facilitates birth of theanterior shoulder
j. Gentle upward traction facilitates birth of theanterior shoulder
k. Support the infants body w/ a towel as it is expelledfrom the birth canal
l. suction & dry the infant
m. Place infant on mothers abdomen asapn. Clamp & cut U.C
o. Observe for placental separation
G tl ll th d hil i
-
8/8/2019 Dystocia 2003 Comp
89/106
p. Gently pull the cord while massagingthe fundus to deliver the placenta
q. Continue to massage the fundus toprevent hemorrhage or put the infant tobreast
r. Inspect the perineum for lacerations ortears
Uterine prolapse
-
8/8/2019 Dystocia 2003 Comp
90/106
Uterine prolapsey 1. Vigorous massage of the fundus and pulling on the
umbilical cord to speed placental separation may causeprolapse of the cervix and lower uterine segment through theintroitus.
y 2.Uterine inversion: turning inside out of the uterusy a. Complete inversion.
y 1.) Inverted uterus is visible outside the introitus.
y 2.) Life-threatening because of severe hemorrhage and
shock .y 3.) Uterus must be immediately replaced manually to
stop blood loss.
b. Partial inversion
) bl b b l d
-
8/8/2019 Dystocia 2003 Comp
91/106
1.) Is not visible but can be palpated.
2.)Uterine fundus is partially inverted hampering contraction
and control of hemerrhage.Nursing Management:
-Maintain IV line-optimal flow to restore fluid vol.
-Anticipate blood transfusion
-O2 by facemask
-Asses v/s and hypovolemic shock
-Anticipate CPR
-Woman will be placed on gen. anesthesia, tocolytics given to relaxuterus
-Oxytocin is administered after manual replacement for uterus tocontract and remain in place
-Future pregnancy will be delivered via CS
-Antibiotic therapy endometrium was exposed
3.) Corrected by the physician using a bimanual technique
Uterine rupture: tearing open or
-
8/8/2019 Dystocia 2003 Comp
92/106
Uterine rupture: tearing open or
separation of uterine wall
1.Rare but serious complication, occuring in 1 in 1,500 to2,000 births.
2.Most common causes
a. Separation of scar from previous classical cesarean
b. Uterine trauma
c. Intense uterine contractions
d. Overstimulation of labor with oxytocin
e. Difficult forceps-assisted birth
f. External cephalic or internal version
g. Prolonged labor
k f f
-
8/8/2019 Dystocia 2003 Comp
93/106
3. Risk factors for uterine rupture
a. Multiparity
b. Overdistension of the uterus (multifetal pregnancy)c. Malpresentation
d. Previous uterine surgery
4. Types
a. Complete extends through the uterine wall into theperitoneal cavity
b. Incomplete extends into the peritoneum but not into theperitoneal cavity
1.) Partial separation of cesarean scar2.) May go unnoticed until repeat cesarean is performed
y Medical management depends on t pe of rupture
-
8/8/2019 Dystocia 2003 Comp
94/106
y 5. Medical management depends on type of rupture
y a. Complete rupture requires management of shock,
replacement of blood, and hysterectomyy b. Incomplete rupture may require laparotomy, repair, and
blood transfusion
y 6. Nursing assessment: signs and symptoms may be silent
or dramatic.y a. Sudden, sharp, lower abdominal pain
y b. Tearing sensation
y c. Signs of shock
y
d. Cessation of contractionsy e. FHR ceases
y f. Blood loss is often concealed
y g. Fetal parts may be easily palpated through abdominal
wall
7 Priority nursing diagnosis; Risk for injury; Impaired gas
-
8/8/2019 Dystocia 2003 Comp
95/106
7. Priority nursing diagnosis; Risk for injury; Impaired gasexchange; Deficient fluid volume
8. Planning and implementationa. Prevention is best
1.) Identify clients at risk
2.) Avoid hyperstimulation of the uterus during induction
Amniotic Fluid Embolism
- amniotic fluid is forced into an open maternal uterineblood sinus due to membrane defects or after partial
premature separation of the placenta- anaphylactoid response
- lung embolism previously thought
Risk factors:
-
8/8/2019 Dystocia 2003 Comp
96/106
Risk factors:
-oxytocin administration
-abruptio placentae-hydramnios
S/Sx- in strong contraction of labor the woman sudden sits
up and grasps her chest because of sharp pain andinability to breath
- becomes pale then cyanotic
- admin oxygen by mask
- anticipate CPR death may occur
-
8/8/2019 Dystocia 2003 Comp
97/106
Problems with the Psyche
-
8/8/2019 Dystocia 2003 Comp
98/106
Problems with the Psyche
A. Factors influencing the psyche of the client inlabor
1. Fear and anxiety
2. Perception of the problem
3. Self-image4. Preparation for childbirth
5. Support systems
6. Coping ability
B. The effect of fear and anxiety on laborprogress
-
8/8/2019 Dystocia 2003 Comp
99/106
1. Epinephrine secretion in response to stress
2. Vascular changes divert blood from the uterus to skeletal
muscles3. Decrease in oxygen and glucose supply with accumulationof lactic acid in uterine muscle
4. Higher perception of pain
5. Decrease in available energy supply to support effectivecontractions
6. Labor progress is slowed
C. Nursing assessment
1. Determine clients past experience with, preparation for, andexpectations of labor and birth
2. Determine clients current coping behaviors and theireffectiveness with the current situation
-
8/8/2019 Dystocia 2003 Comp
100/106
E. Planning and implementation
1. Establish a trusting relationship with the client and
family2. Reamain at the bedside with the client and familyduring labor
3. Encourage relaxation
4. Keep the client and family informed about progressand procedures
5. Encourage positive coping behaviors and discouragenegative behaviors
6. Promote self-image by praising efforts
-
8/8/2019 Dystocia 2003 Comp
101/106
Cesarean Section
-
8/8/2019 Dystocia 2003 Comp
102/106
Cesarean SectionA. Delivery of the infant by an abdominal incision:
purpose is to facilitate delivery to preserve the health of themother and fetus
1. Number of cesarean births has increased dramaticallybeginning in the late 1970s and 1980s
2. National goal of Healthy People 2010 is to reduce theincidence from the current rate of 25% to 30% to 15% of alldeliveries
B. Major indications for cesarean delivery
1. Dystocia or CPD2. Fetal distress
3. Breech presentation
4. Previous cesarean birth
-
8/8/2019 Dystocia 2003 Comp
103/106
E Surgical techniques
-
8/8/2019 Dystocia 2003 Comp
104/106
E. Surgical techniques
1. Skin incisions
a. Verticalb. Pfannenstiels (transverse lower abdominal incision)
2. Uterine incisions
a. Classical: through the upper uterine segment
b. Low cervical transverse: lower uterine segmentc. Lower uterine segment vertical
F. Nursing assessment
1. Determine the reason for the cesarean delivery
2. Determine the clients understanding of the indication,procedure, and implications for recovery from abdominaldelivery
H. Planning and implementation
1 Discuss cesarean birth in childbirth preparation classes
-
8/8/2019 Dystocia 2003 Comp
105/106
1. Discuss cesarean birth in childbirth preparation classes
a. Clients and families cope better if they have time to learn aboutcesarean birth
b. Emergency cesarean birth increases anxiety and alters the couplesexpectations about childbirth
2. Preoperative care
a. Assess NPO status (mother should have nothing by mouth, if possibleto prevent aspiration)
b. Explain procedure so that client and family will know what to expect
c. Obtain client signature on consent form
d. Perform abdominal prep
e. Insert Folley catheter to prevent bladder trauma during surgery
f. Start intravenous fluids using a large bore catheterg. Administer an antacid either IV or PO to decrease risk of lung damage
from aspirating acidic gastric contents during surgery
h. Administer antibiotics, as ordered
i. Assist with positioning and administration of regional anesthesia, if
used
3. Intraoperative carea Provide heated crib and supplies to receive the newborn
-
8/8/2019 Dystocia 2003 Comp
106/106
a. Provide heated crib and supplies to receive the newborn
b. Provide immediate care to the newborn or assist nursery personnel asneeded
c. Provide assistance to surgical team and immediate care for the mother
4. Postoperative carea. Begin postanesthesia (recovery room) monitoring of vital signs, pulse
oximetry, and cardiac monitoring; monitor vital signs q 15 mins. for
first hour and until stableb. Assess fundus for firmness and location (if boggy, massage until
firm)
c. Assess vaginal bleeding
d. Assess abdominal dressinge. Assess catheter and urine output
f. Turn, cough, and deep breathe hourly
g Administer medications for pain as needed