DYSPHAGIA DYSPHAGIA Drravikumar M.S(ENT) Drravikumar M.S(ENT)

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 1/92
DYSPHAGIADYSPHAGIA
Drravikumar M.S(ENT)Drravikumar M.S(ENT)

8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 2/92
Esophageal AnatomyEsophageal Anatomy
Muscular tube connecting theMuscular tube connecting thepharynx to the stomachpharynx to the stomach
Esophagus begins where theEsophagus begins where theinferior pharyngeal constrictor inferior pharyngeal constrictor merges with the cricopharyngeusmerges with the cricopharyngeus ± ± Upper esophageal sphincter Upper esophageal sphincter
(UES)(UES)
18 to 26 cm in length18 to 26 cm in length
Lower esophageal sphincter (LES)Lower esophageal sphincter (LES) ± ± Thickened circular smooth muscleThickened circular smooth muscle
± ± 40cm from incisors40cm from incisors
Extrinsic indentationsExtrinsic indentations ± ± Anterior body of C7 (worsen by Anterior body of C7 (worsen by
osteophytes)osteophytes)
± ± Arch of the aorta, the left Arch of the aorta, the leftmainstem bronchusmainstem bronchus
± ± Diaphragmatic hiatusDiaphragmatic hiatus
8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 3/92
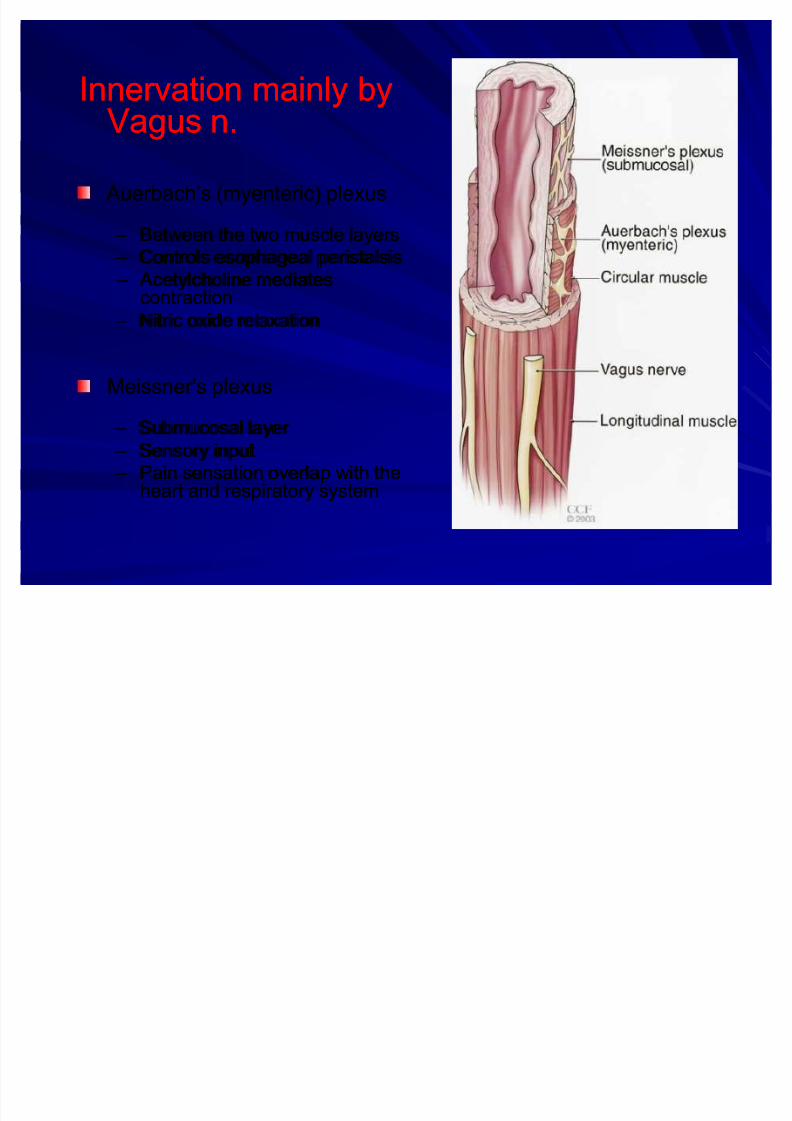
Innervation mainly byInnervation mainly by
Vagus n.Vagus n. Auerbach¶s (myenteric) plexus Auerbach¶s (myenteric) plexus
± ± Between the two muscle layersBetween the two muscle layers
± ± Controls esophageal peristalsisControls esophageal peristalsis
± ± Acetylcholine mediates Acetylcholine mediatescontractioncontraction
± ± Nitric oxide relaxationNitric oxide relaxation
Meissner's plexusMeissner's plexus
± ± Submucosal layer Submucosal layer
± ± Sensory inputSensory input
± ± Pain sensation overlap with thePain sensation overlap with theheart and respiratory systemheart and respiratory system

8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 4/92
Esophageal physiologyEsophageal physiology
1.1. swallowswallow (Esophageal Transport by(Esophageal Transport byGravity)Gravity)The oropharyngeal phaseThe oropharyngeal phase : Swallowing begins: Swallowing beginswhen a food bolus is propelled into the pharynxwhen a food bolus is propelled into the pharynxfrom the mouth. It isfrom the mouth. It is voluntaryvoluntary..
The esophageal phaseThe esophageal phase. It is. It is involuntary.involuntary.
It takes approximately 8 to 10 seconds fromIt takes approximately 8 to 10 seconds frominitiation of the swallow to entry into theinitiation of the swallow to entry into the
stomach .stomach . In rapid sequence and with precise coordination,In rapid sequence and with precise coordination,
the larynx is elevated and the epiglottis seals thethe larynx is elevated and the epiglottis seals theairway.airway.

8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 5/92
Esophageal physiologyEsophageal physiology
2.Secretion (submucosal mucous2.Secretion (submucosal mucous
glands)glands)
3.Protection : Gastroesophageal3.Protection : Gastroesophageal
reflux (machenic , secretion )reflux (machenic , secretion )
8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 6/92
DysphagiaDysphagiaGreekGreek dysdys (difficulty, disordered) and(difficulty, disordered) and phagia phagia (to(toeat)eat)
Sensation that food is hindered in its passageSensation that food is hindered in its passage
from the mouth to the stomachfrom the mouth to the stomach
Most patients complain that foodMost patients complain that food ± ± ³sticks,´ ³hangs up,´ ³stops,´ or ³just won't go down³sticks,´ ³hangs up,´ ³stops,´ or ³just won't go down
right´right´
8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 7/92
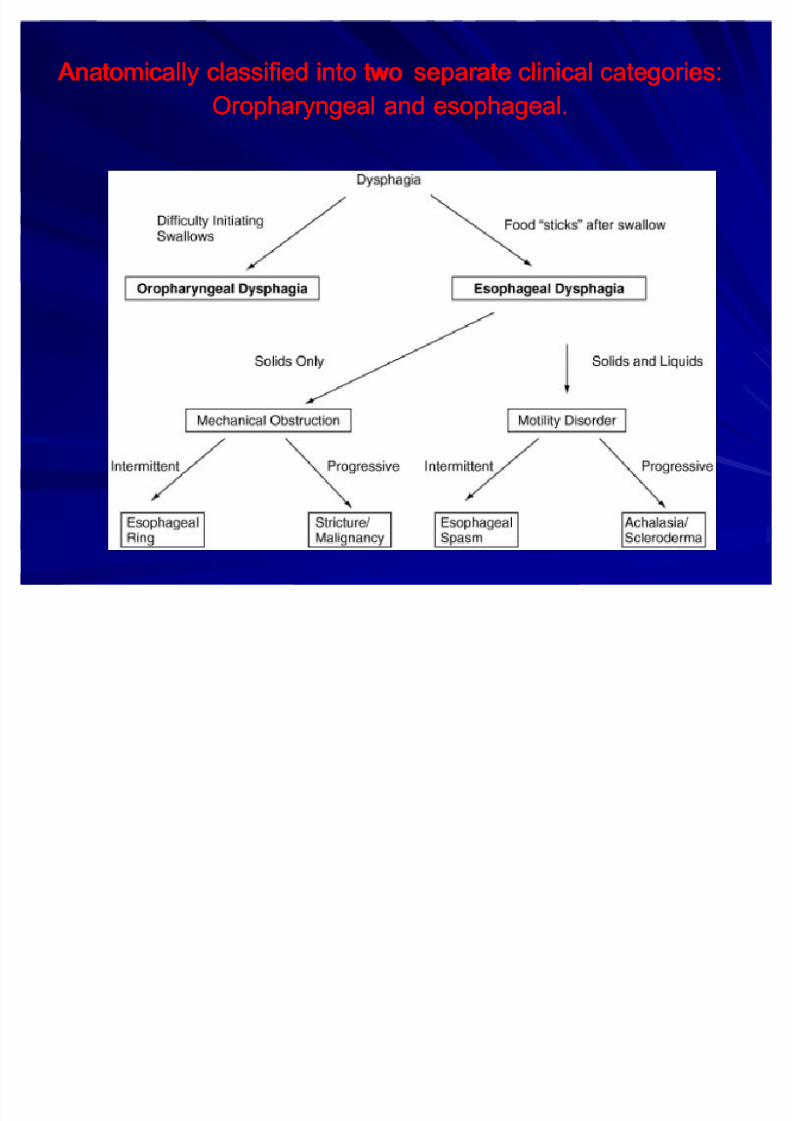
Anatomically classified into two Anatomically classified into two separate clinical categories:separate clinical categories:
Oropharyngeal and esophageal.Oropharyngeal and esophageal.
8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 8/92
HistoryHistory
Three questions are crucialThree questions are crucial::
(1) What type of food or liquid causes symptoms?(1) What type of food or liquid causes symptoms? ± ± Mechanical vs neuromuscular defectMechanical vs neuromuscular defect
± ± Primarily solidsPrimarily solidsStructural lesionStructural lesion-- peptic stricture, ring, or malignancypeptic stricture, ring, or malignancy
± ± Both solid and liquidBoth solid and liquida motility disorder like achalasia or sclerodermaa motility disorder like achalasia or scleroderma
(2) Is the dysphagia intermittent or progressive?(2) Is the dysphagia intermittent or progressive? ± ± Esophageal rings tend to cause intermittent solid food dysphagiaEsophageal rings tend to cause intermittent solid food dysphagia
± ± Strictures and cancer cause progressive dysphagiaStrictures and cancer cause progressive dysphagia
(3) Does the patient have heartburn?(3) Does the patient have heartburn? ± ± Complication of GERDComplication of GERD-- Esophagitis, stricture & Barrett¶sEsophagitis, stricture & Barrett¶s
8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 9/92
HistoryHistory
Location of dysphagiaLocation of dysphagia
± ± Limited value (Referred from any site)Limited value (Referred from any site)
Weight lossWeight loss
± ± Significance and duration of the diseaseSignificance and duration of the disease
Dietary changesDietary changes
± ± Nature and severity of disease.Nature and severity of disease.
Dysphagia must be distinguished fromDysphagia must be distinguished fromodynophagiaodynophagia
± ± Associated with an inflammatory condition Associated with an inflammatory condition
(esophagitis)(esophagitis)

8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 10/92
Physical ExaminationPhysical ExaminationComplete head and neck examComplete head and neck exam
Look for signs of chronic illness or recent weightLook for signs of chronic illness or recent weightlossloss
³wet´ voice³wet´ voice ± ± failure to clear the HP of retained secretionsfailure to clear the HP of retained secretions
Palpable crepitus or gurgling noises in the neckPalpable crepitus or gurgling noises in the neck ± ± Possible Zenker's diverticulum or other pouchPossible Zenker's diverticulum or other pouch
DroolingDrooling
8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 11/92
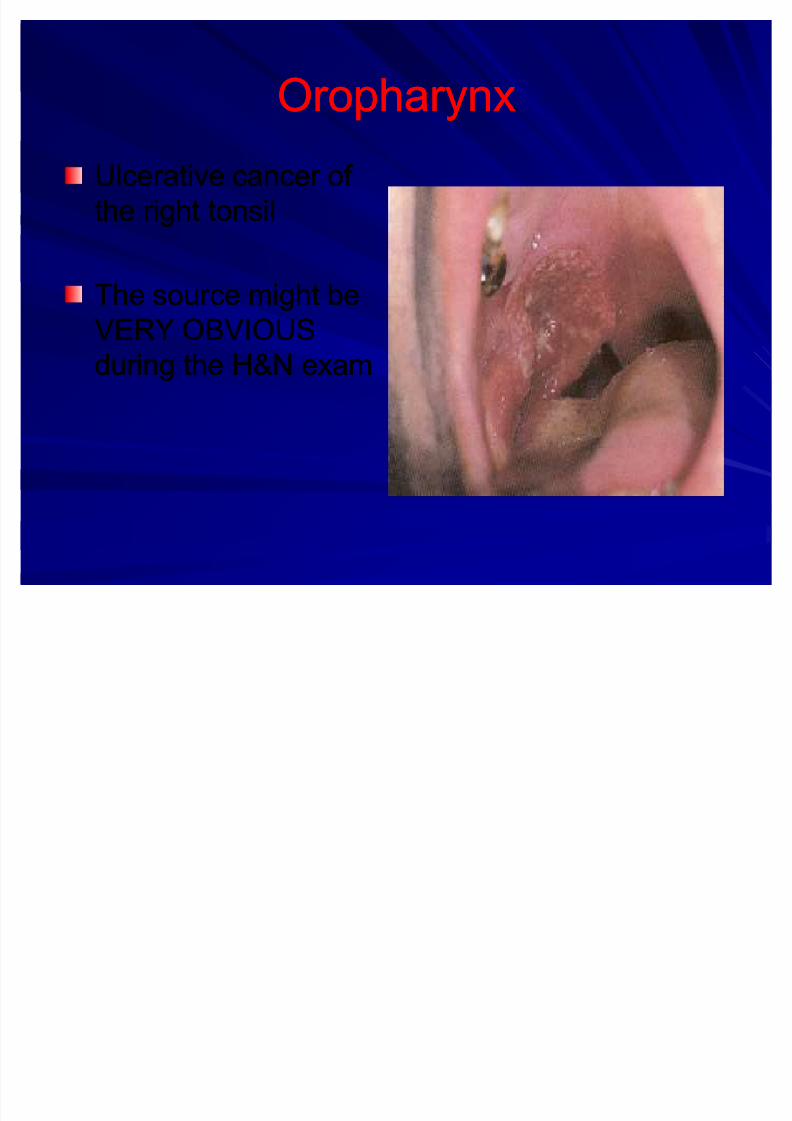
OropharynxOropharynx
Ulcerative cancer of Ulcerative cancer of
the right tonsilthe right tonsil
The source might beThe source might be
VERY OBVIOUSVERY OBVIOUS
during the H&N examduring the H&N exam

8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 12/92
ExamExam
Absence of an upward movement of larynx with Absence of an upward movement of larynx withdeglutitiondeglutition ± ± indicates fixation due to inflammation, tumor, or indicates fixation due to inflammation, tumor, or
paralysisparalysis
Neurologic examNeurologic exam ± ± Evaluate for other deficits or CN palsiesEvaluate for other deficits or CN palsies
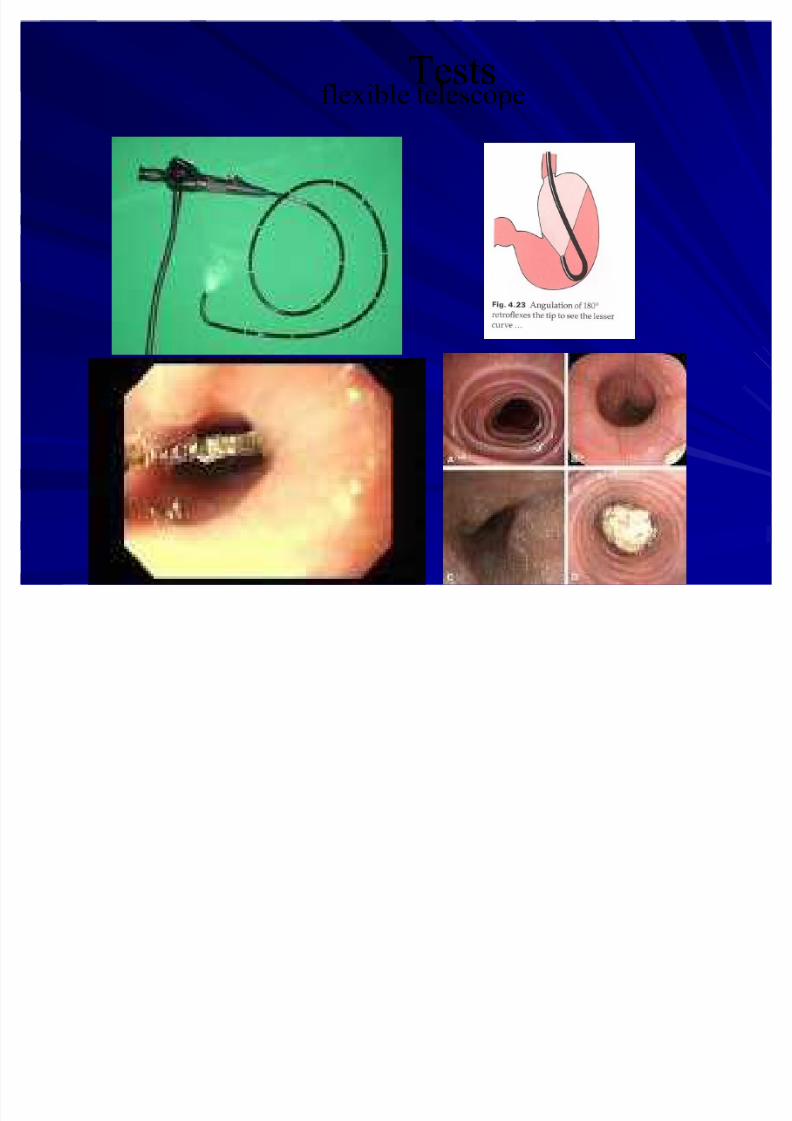
Flexible fiberoptic laryngoscopyFlexible fiberoptic laryngoscopy ± ± identify defects in the larynx/pharynx, pooling of identify defects in the larynx/pharynx, pooling of
secretions in the hypopharynx, or mass lesions thatsecretions in the hypopharynx, or mass lesions thatmay produce obstructionmay produce obstruction
8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 13/92
TestsTestsflexible telescope
8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 14/92
RadiographyRadiography
CXRCXR ± ± foreign bodyforeign body
± ± perforationperforation
± ± mediastinal anatomymediastinal anatomy
CTCT ± ± Only to evaluate mass lesions in the neckOnly to evaluate mass lesions in the neck
MRIMRI ± ± useful when neurologic disorders are suspecteduseful when neurologic disorders are suspected
± ± Delineate mass lesions in the brainDelineate mass lesions in the brain
± ± Evaluate degenerative processes in the brain and spinal cordEvaluate degenerative processes in the brain and spinal cord
8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 15/92
FluoroscopyFluoroscopy
Standard barium swallowStandard barium swallow uses thin barium, is auses thin barium, is aquick view, and is not satisfactory for mostquick view, and is not satisfactory for mostswallowing disordersswallowing disorders
MBSMBS is the definitive study for evaluation of theis the definitive study for evaluation of theswallowing mechanismswallowing mechanism
Uses both thick and thin barium consistenciesUses both thick and thin barium consistenciesand simulated foodsand simulated foods
Assess pharyngeal anatomy and motility Assess pharyngeal anatomy and motility

8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 16/92
FEESFEES(Fiberoptic endoscopic evaluation)(Fiberoptic endoscopic evaluation)
Directly viewing liquid or food bolus viaDirectly viewing liquid or food bolus viascopescope
Positioned high in oropharynxPositioned high in oropharynx
Observation of Observation of
± ± vocal and arytenoid movementsvocal and arytenoid movements
± ± Elevation of larynx and tongue baseElevation of larynx and tongue base
Pooling and aspiration can be notedPooling and aspiration can be noted
8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 17/92
EsophagoscopyEsophagoscopy
FlexibleFlexible (in office)(in office) vs. rigidvs. rigid ± ± Foreign body, biopsy of lesions, evaluation of Foreign body, biopsy of lesions, evaluation of
stenosisstenosis
Esophagus should be biopsied in all patientsEsophagus should be biopsied in all patientssuspected of having esophagitis, asuspected of having esophagitis, aneuromuscular disorder, or a collagen vascular neuromuscular disorder, or a collagen vascular
diseasedisease

8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 18/92
TestsTests
EndoscopyEndoscopy (Rigid & flexible telescope(Rigid & flexible telescope--under sedation)under sedation)
Rigid Endoscopy

8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 19/92
Special TestsSpecial Tests
pH probepH probe -- monitors over a 24 hour periodmonitors over a 24 hour period
Acid infusion tests Acid infusion tests ± ± infuses a dilute HCL solution into the esophagusinfuses a dilute HCL solution into the esophagus
± ± checks reproducibility of symptomschecks reproducibility of symptoms
ManometryManometry ± ± essential if dysfunction of theessential if dysfunction of thecricopharyngeus, esophagus or LES identifiedcricopharyngeus, esophagus or LES identified
on swallow studyon swallow study ± ± Quality laboratoryQuality laboratory
± ± Interpreted by an experienced gastroenterologistInterpreted by an experienced gastroenterologist
8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 20/92
Causes of dysphagiaCauses of dysphagia
OesophagealOesophagealIn the lumenIn the lumen
Foreign bodyForeign bodyLarge bolusLarge bolus
In the wallIn the wall
congentialcongential
TraumaticTraumatic
InflammationInflammation
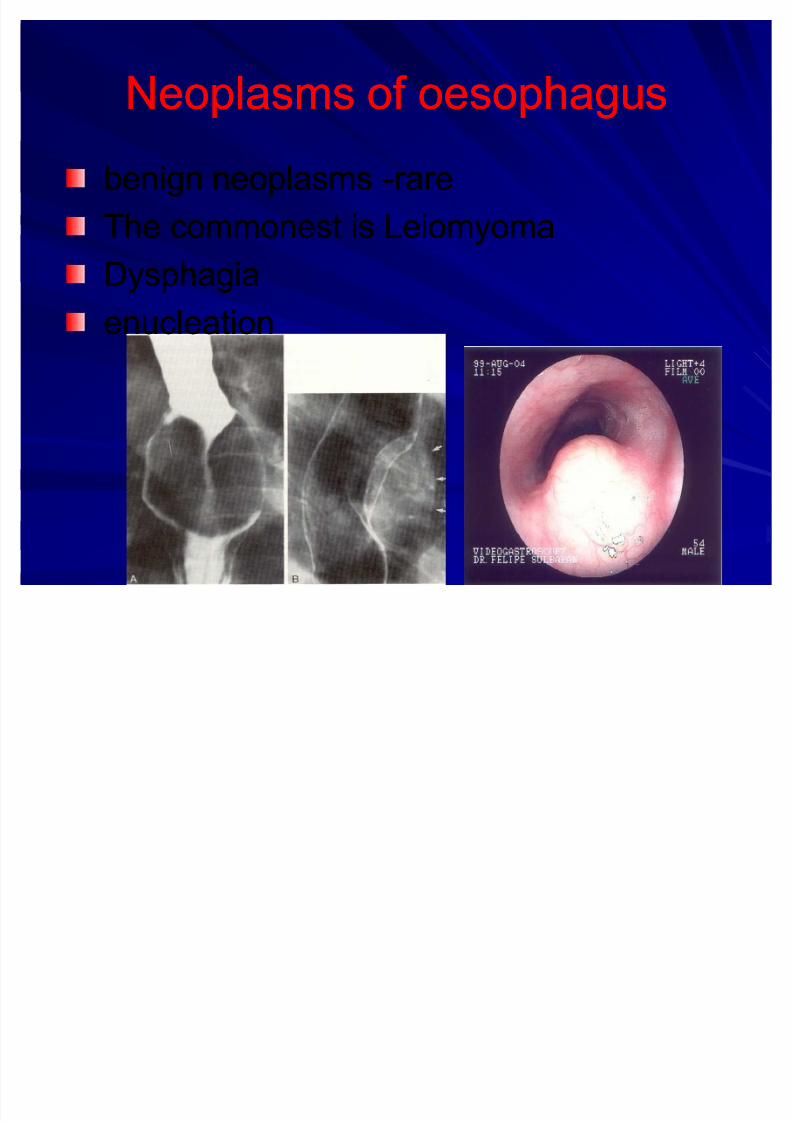
NeoplasmsNeoplasms
NeurologicalNeurological
MiscellaneousMiscellaneous
8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 21/92
Causes of dysphagiaCauses of dysphagia
Pressure on the oesophagusPressure on the oesophagus
CervicalCervical
ThroracicThroracicabdominalabdominal
8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 22/92
Causes of dysphagiaCauses of dysphagia
ExtraExtra--oesophageal causesoesophageal causes--
Oral cavityOral cavity
PharynxPharynxLarynxLarynx
FunctionalFunctional--Globus hystericusGlobus hystericus
8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 23/92
Definition
Primary esophageal motility disorder characterized by:
1) Absence of peristalsis,
2) Elevated pressure of the LES,
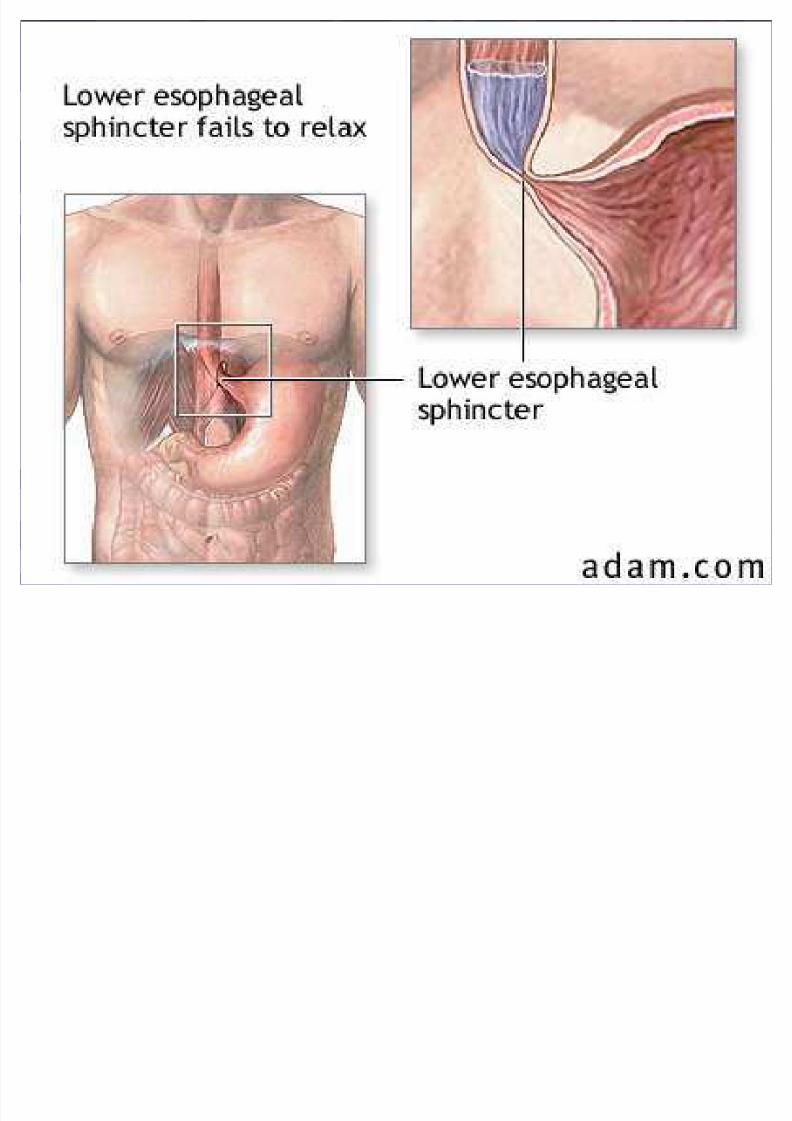
3) Failure of the LES to relax during swallowing,
Causing functional obstruction at the gastroesophageal junction.
Achalasia of the cardia Achalasia of the cardia
8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 24/92

8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 25/92
Achalasia Achalasia
Primary esophageal motilityPrimary esophageal motilitydisorder disorder ± ± Insufficient LES relaxationInsufficient LES relaxation
± ± Loss of esophageal peristalsisLoss of esophageal peristalsis
PrimaryPrimary ± ± idiopathic degeneration of the ganglion cells of idiopathic degeneration of the ganglion cells of
Auerbach¶s plexus Auerbach¶s plexus
SecondarySecondary -- caused by other conditionscaused by other conditions ± ± i.e. Distal esophageal carcinoma, Chagas¶i.e. Distal esophageal carcinoma, Chagas¶
disease, postvagotomy syndrome, CVA, DMdisease, postvagotomy syndrome, CVA, DM

8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 26/92
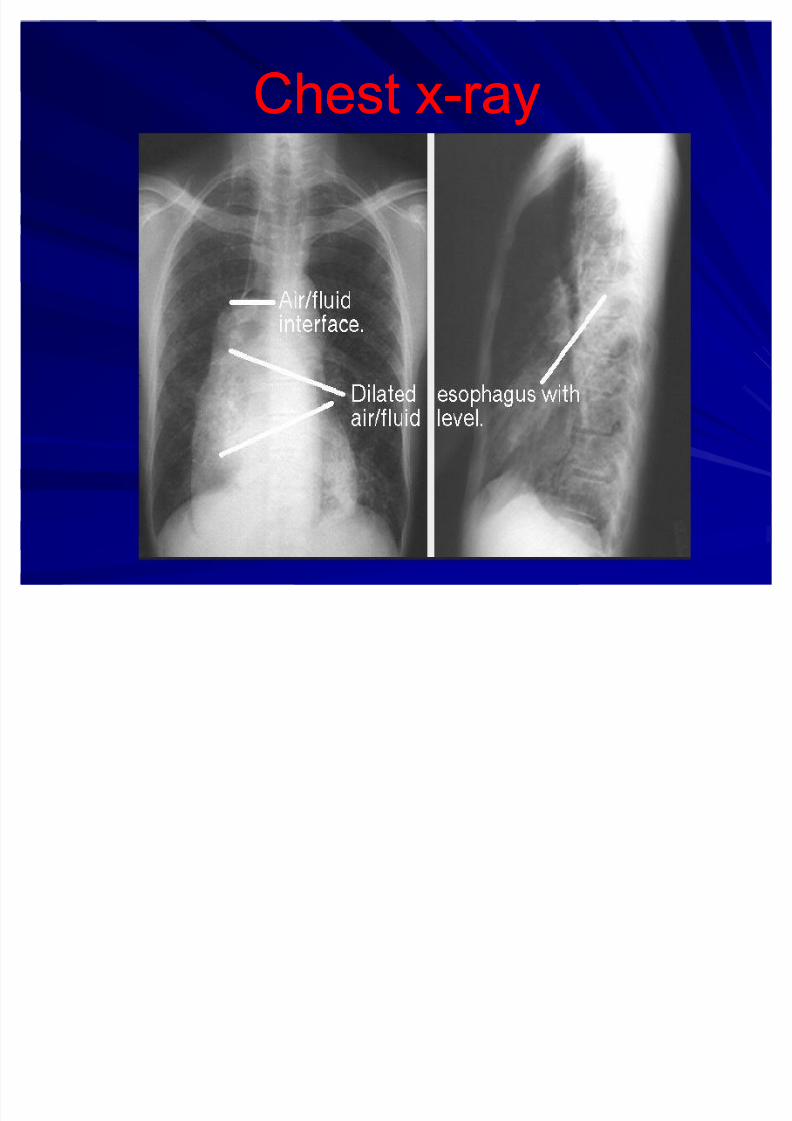
Clinical picture of AchalasiaClinical picture of AchalasiaHistoryHistory
Dysphagia (most common)Dysphagia (most common)RegurgitationRegurgitation
Chest painChest painHeartburnHeartburnWeight lossWeight loss
Physical:Physical:
Physical examination is noncontributory.Physical examination is noncontributory.
8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 27/92
8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 28/92
Chest xChest x--rayray
8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 29/92
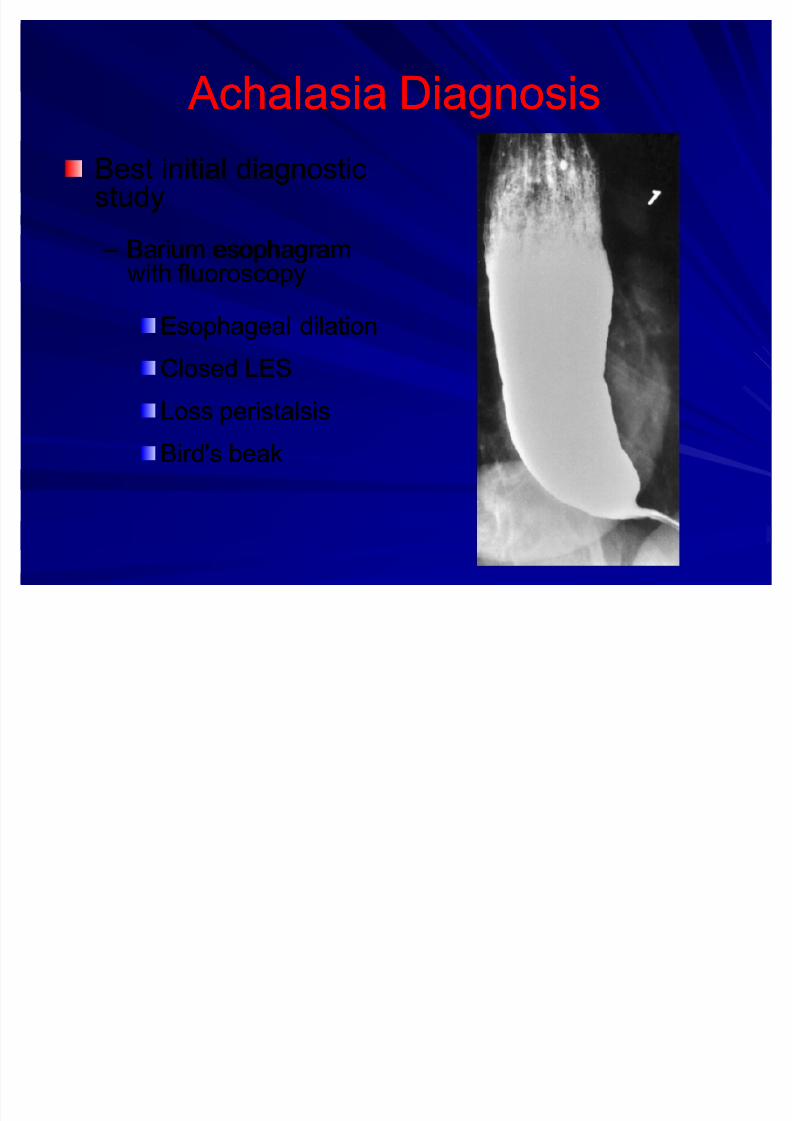
Achalasia Diagnosis Achalasia Diagnosis
Best initial diagnosticBest initial diagnosticstudystudy
± ± Barium esophagramBarium esophagram
with fluoroscopywith fluoroscopy
Esophageal dilationEsophageal dilation
Closed LESClosed LES
Loss peristalsisLoss peristalsisBird's beakBird's beak
8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 30/92
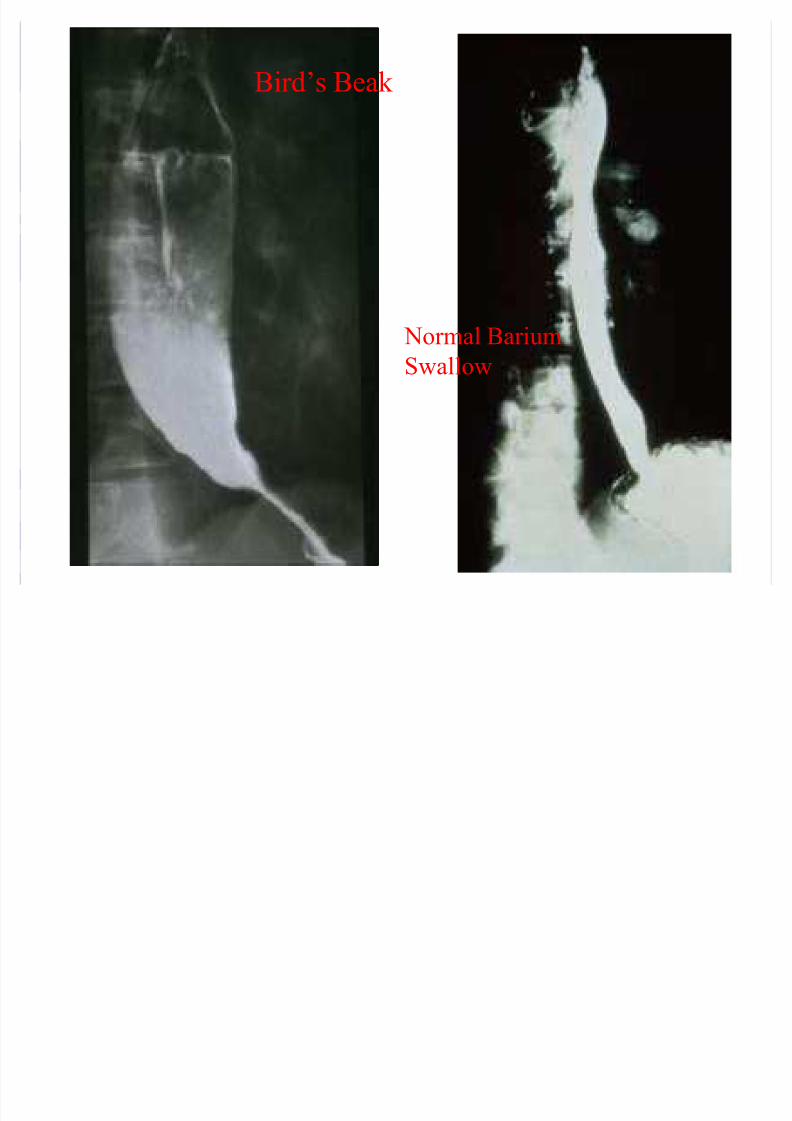
Normal Barium
Swallow
Birds beak xrayBird¶s Beak
8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 31/92
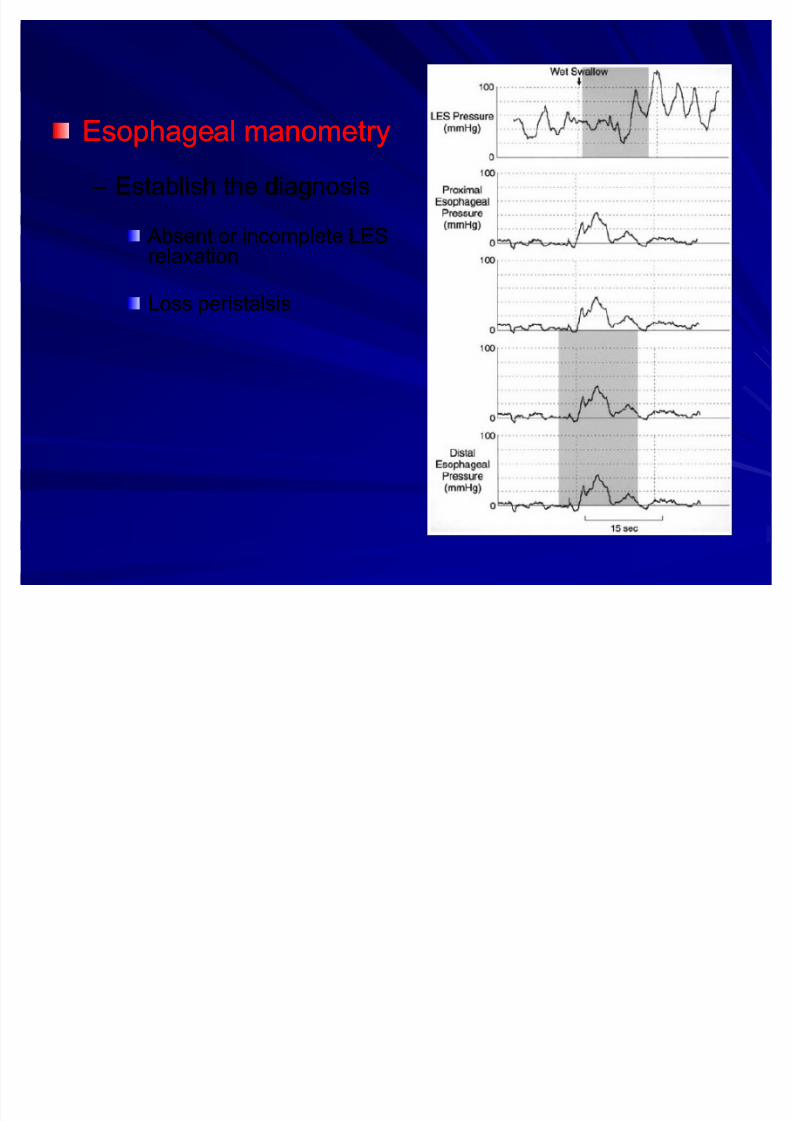
Esophageal manometryEsophageal manometry ± ± Establish the diagnosisEstablish the diagnosis
Absent or incomplete LES Absent or incomplete LESrelaxationrelaxation
Loss peristalsisLoss peristalsis
8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 32/92
The goal of therapy for achalasia is to relieveThe goal of therapy for achalasia is to relievesymptoms by eliminating the outflow resistancesymptoms by eliminating the outflow resistancecaused by the hypertensive and nonrelaxing LEScaused by the hypertensive and nonrelaxing LES..
1)1) Medical Management Medical Management 2)2) Surgical Management Surgical Management
How would you manage thisHow would you manage thispatient?patient?
8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 33/92
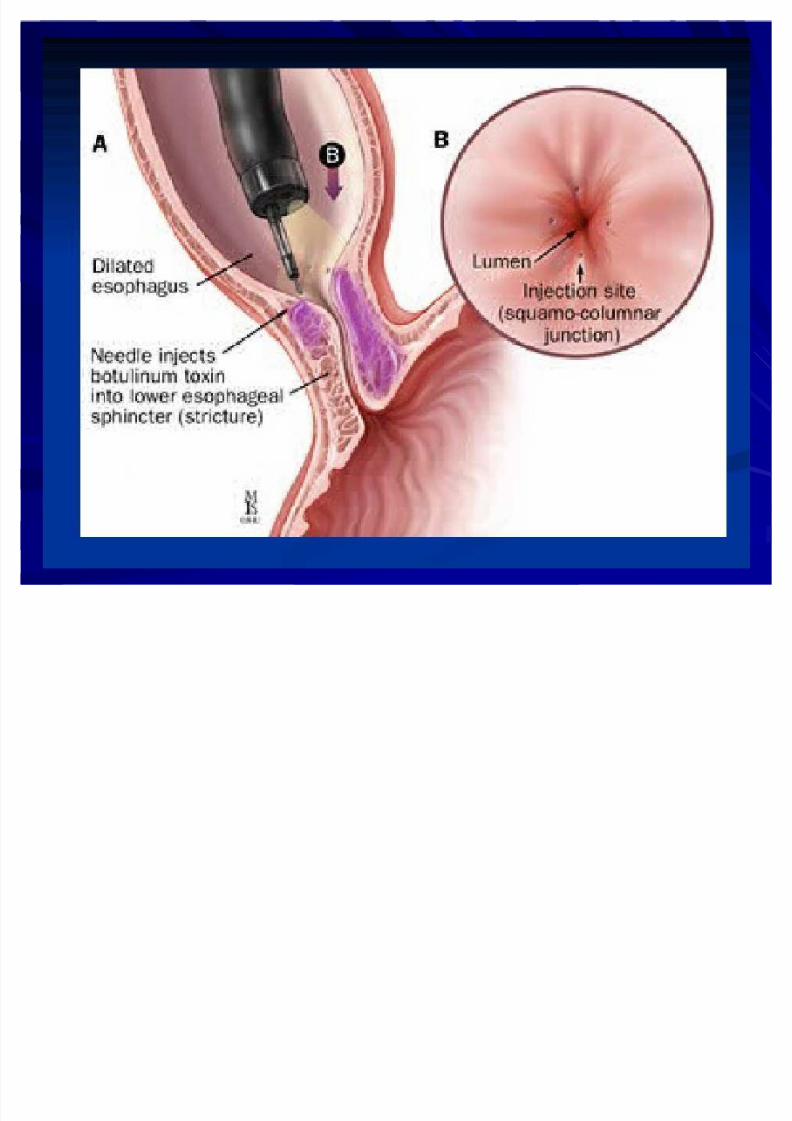
Medical Management Medical Management a)a) Botulinum toxinBotulinum toxin:: intrasphincteric injectionintrasphincteric injection
Only 30% of patient's treated endoscopically stillOnly 30% of patient's treated endoscopically stillhave relief of dysphagia 1 year after treatment.have relief of dysphagia 1 year after treatment.
bb)) Pharmacologic therapyPharmacologic therapy:: relax the smoothrelax the smooth
muscle of the LES.muscle of the LES.Calcium channel blockersCalcium channel blockers -- Nifedipine andNifedipine andverapamilverapamil
Anticholinergic agents Anticholinergic agents -- Cimetropium bromideCimetropium bromide
NitratesNitrates -- Isosorbide dinitrateIsosorbide dinitrate
8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 34/92
8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 35/92
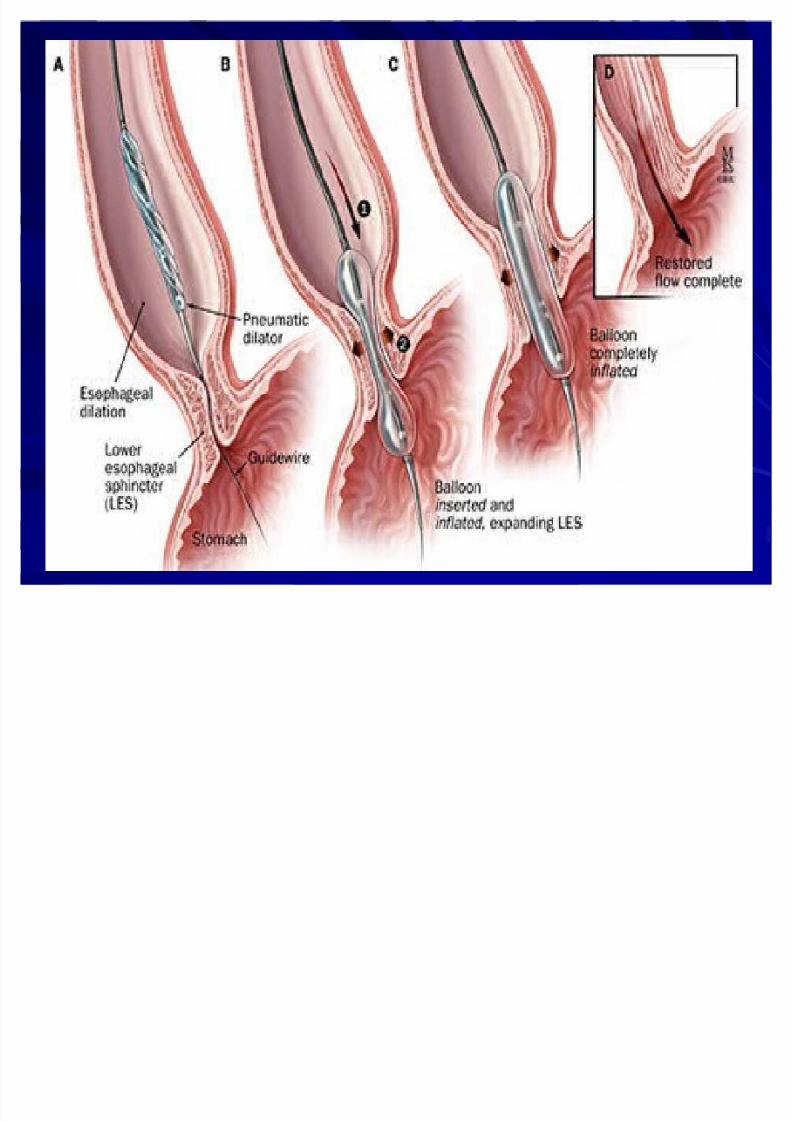
TreatmentTreatment
Pneumatic dilationPneumatic dilation
± ± Should be a surgical candidatesShould be a surgical candidates
2% to 5% risk of perforation2% to 5% risk of perforation
± ± After dilation need a gastrograffin study After dilation need a gastrograffin study
followed by barium swallow to excludefollowed by barium swallow to exclude
esophageal perforationesophageal perforation
± ± Good to excellent relief of symptoms in 50%Good to excellent relief of symptoms in 50%
to 93% of patientsto 93% of patients

8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 36/92
8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 37/92
8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 38/92
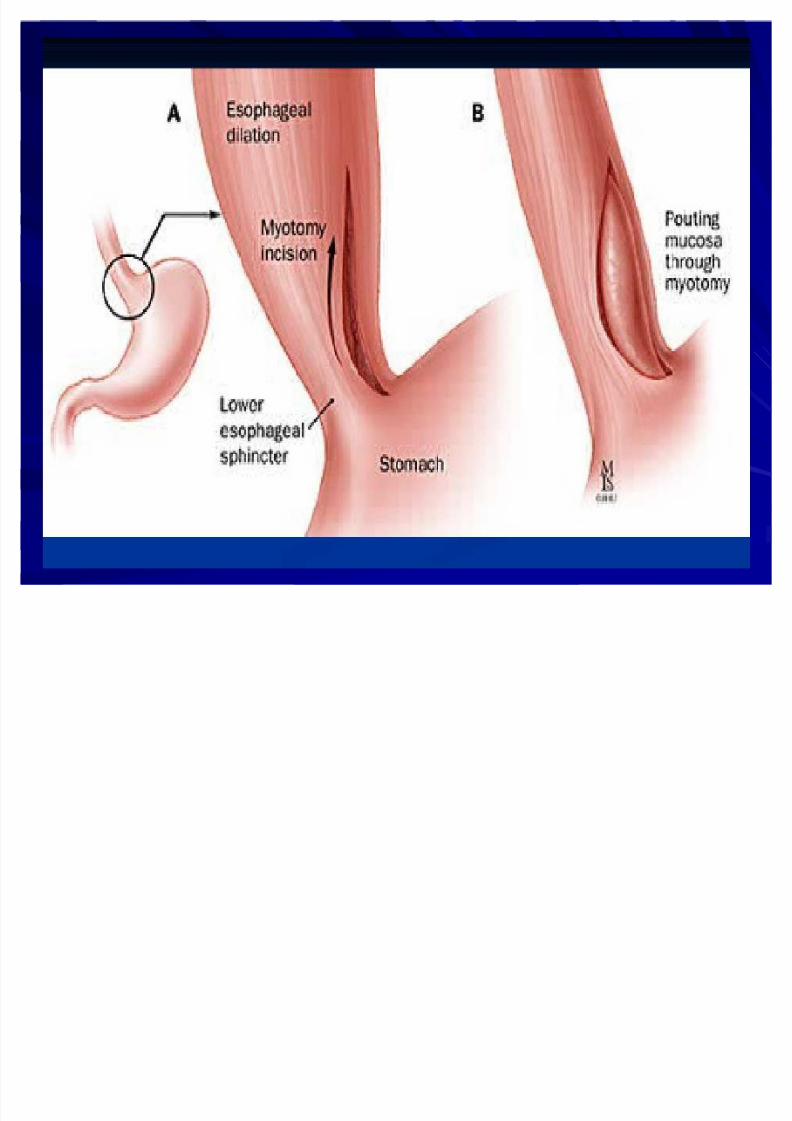
Surgical myotomySurgical myotomy
± ± Myotomy across the LESMyotomy across the LES
± ± Laparoscopy with a response rate of 80% toLaparoscopy with a response rate of 80% to
94%94%
± ± ComplicationComplication-- GERD in 10% to 20%GERD in 10% to 20%
8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 39/92
8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 40/92
NonNon--achalasia Motility Disordersachalasia Motility Disorders
Diffuse esophageal spasm (DES)Diffuse esophageal spasm (DES) ± ± Simultaneous and repetitive contractions inSimultaneous and repetitive contractions in
the esophageal bodythe esophageal body
± ± Normal LES relaxationNormal LES relaxation ± ± Dysphagia if the contraction amplitudes areDysphagia if the contraction amplitudes are
lowlow
± ± Chest pain if the contraction amplitudes areChest pain if the contraction amplitudes arehighhigh
8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 41/92

8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 42/92
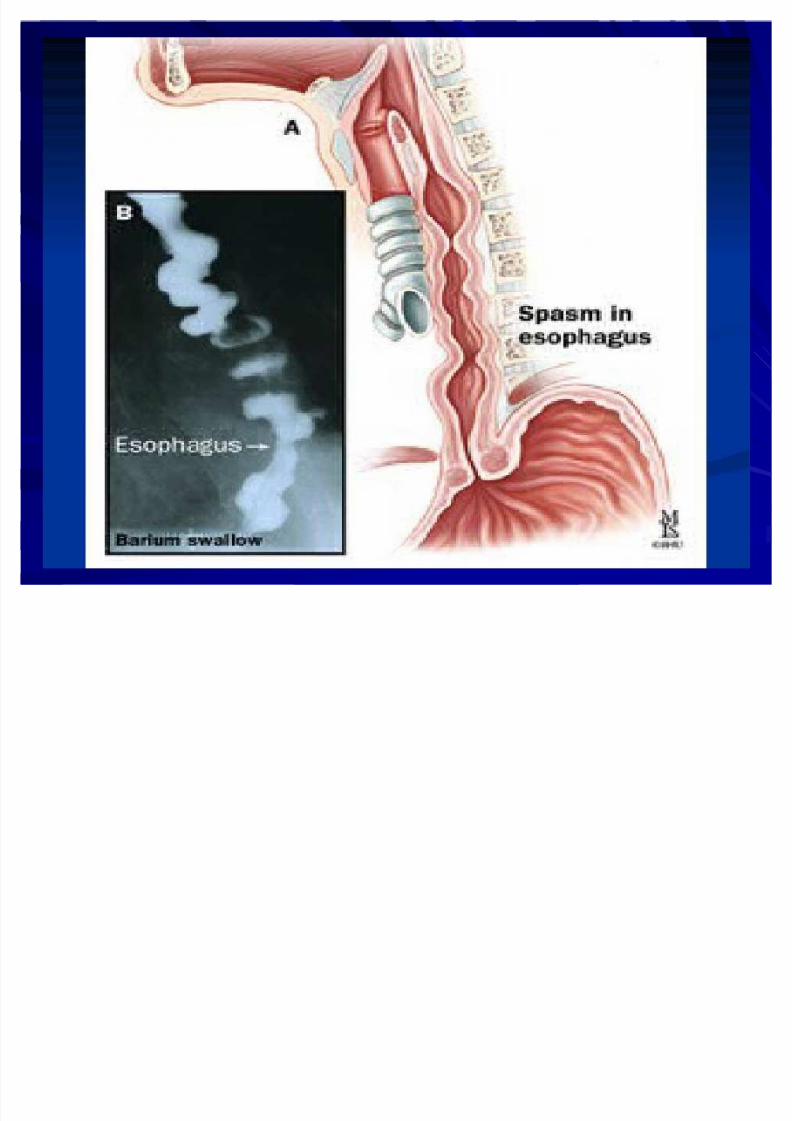
Diffuse esophageal spasmDiffuse esophageal spasm
DiagnosisDiagnosis ± ± EsophagogramEsophagogram
"corkscrew" esophagus"corkscrew" esophagus
± ± ManometryManometrySimultaneous andSimultaneous andrepetitive contractionsrepetitive contractionsin the esophageal bodyin the esophageal body
TreatmentTreatment ± ± Medications that relaxMedications that relax
the esophagusthe esophagusNitrates and calciumNitrates and calcium--channel blockerschannel blockers
8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 43/92
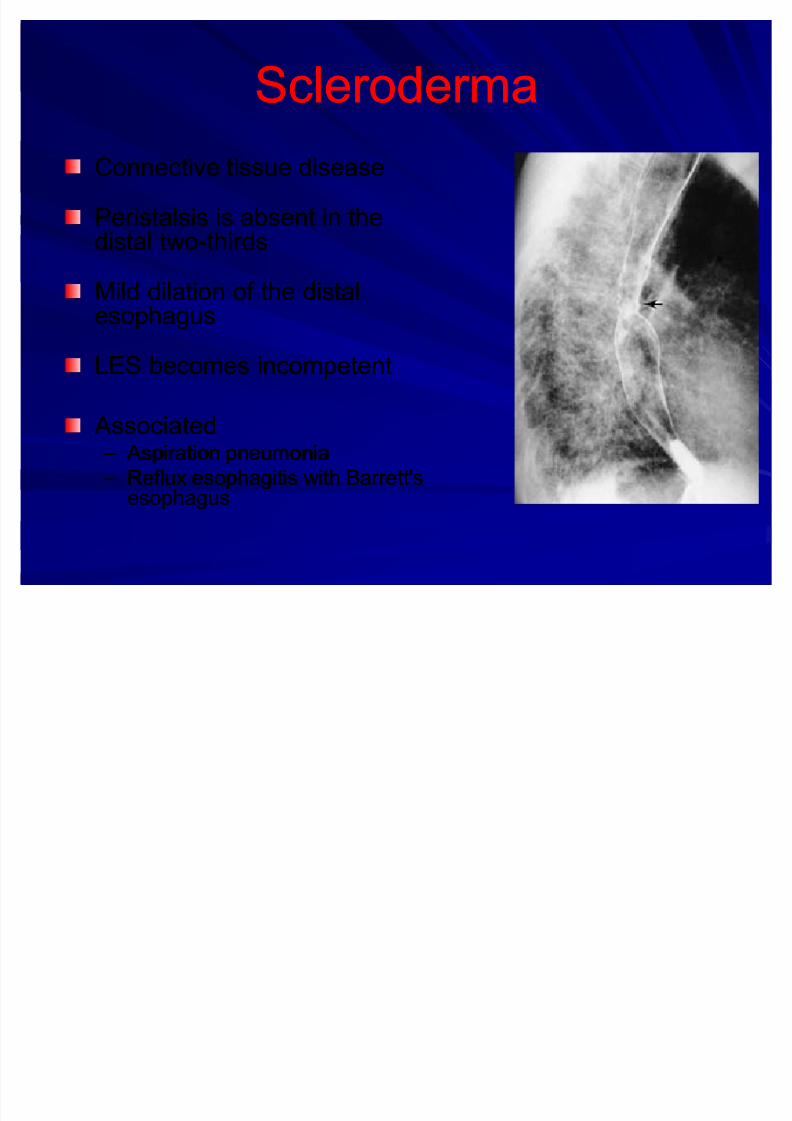
SclerodermaScleroderma
Connective tissue diseaseConnective tissue disease
Peristalsis is absent in thePeristalsis is absent in thedistal twodistal two--thirdsthirds
Mild dilation of the distalMild dilation of the distalesophagusesophagus
LES becomes incompetentLES becomes incompetent
Associated Associated ± ± Aspiration pneumonia Aspiration pneumonia
± ± Reflux esophagitis with Barrett'sReflux esophagitis with Barrett'sesophagusesophagus
8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 44/92
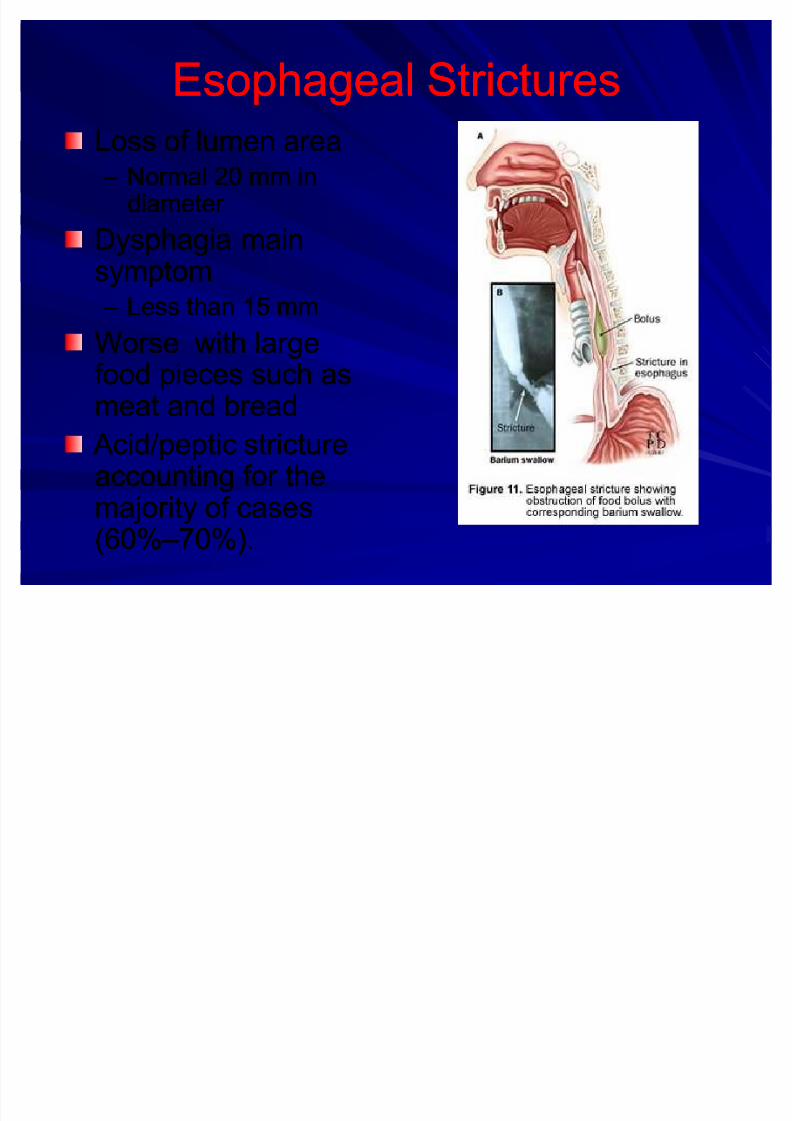
Esophageal StricturesEsophageal Strictures
Loss of lumen areaLoss of lumen area ± ± Normal 20 mm inNormal 20 mm in
diameter diameter
Dysphagia mainDysphagia main
symptomsymptom ± ± Less than 15 mmLess than 15 mm
Worse with largeWorse with largefood pieces such asfood pieces such as
meat and breadmeat and bread Acid/peptic stricture Acid/peptic strictureaccounting for theaccounting for themajority of casesmajority of cases(60%(60%± ±70%).70%).
8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 45/92
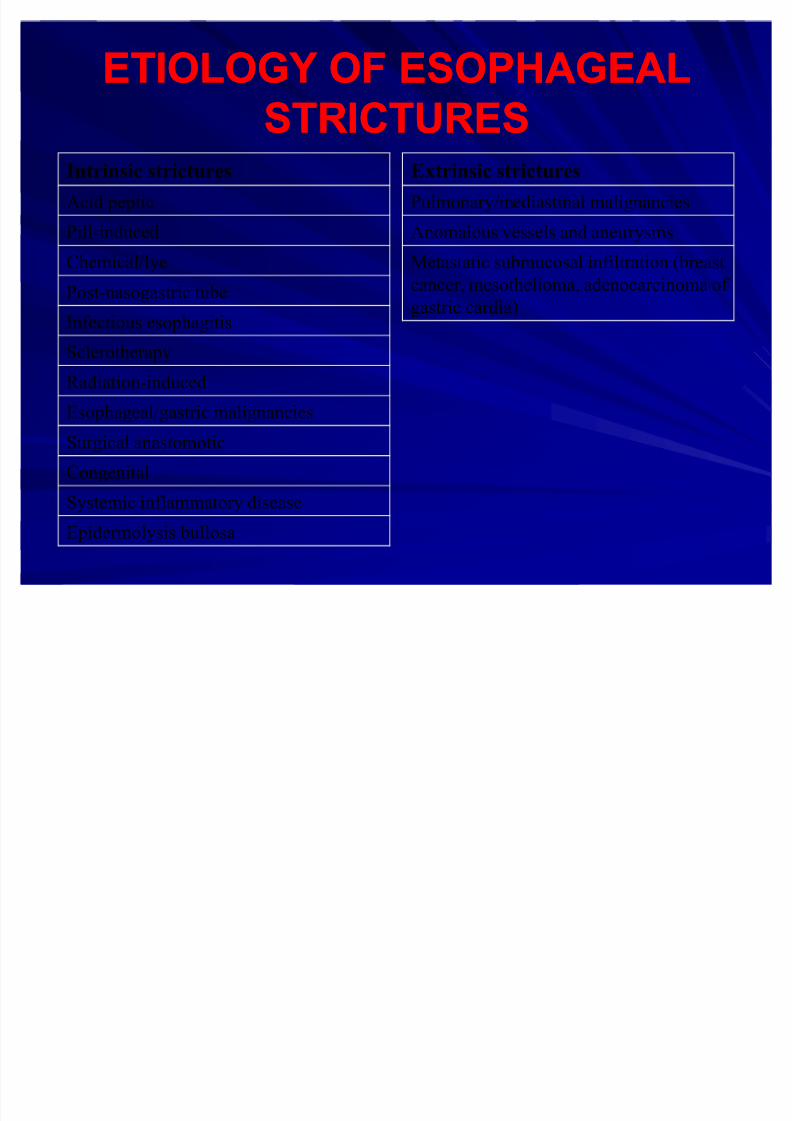
ETIOLOGY OF ESOPHAGEALETIOLOGY OF ESOPHAGEAL
STRICTURESSTRICTURESIntrinsic strictures
Acid peptic
Pill-induced
Chemical/lye
Post-nasogastric tube
Infectious esophagitis
Sclerotherapy
Radiation-induced
Esophageal/gastric malignanciesSurgical anastomotic
Congenital
Systemic inflammatory disease
Epidermolysis bullosa
Extrinsic strictures
Pulmonary/mediastinal malignancies
Anomalous vessels and aneurysms
Metastatic submucosal infiltration (breast
cancer, mesothelioma, adenocarcinoma of gastric cardia)

8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 46/92
DiagnosisDiagnosis
EsophagogramEsophagogram
± ± Initial diagnostic studyInitial diagnostic study
± ± Delineate the strictureDelineate the stricture
EndoscopyEndoscopy ± ± Evaluate the mucosaEvaluate the mucosa
Distal stricture Caustic ingestion
normal mucosa Barrett's metaplasia
8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 47/92
8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 48/92
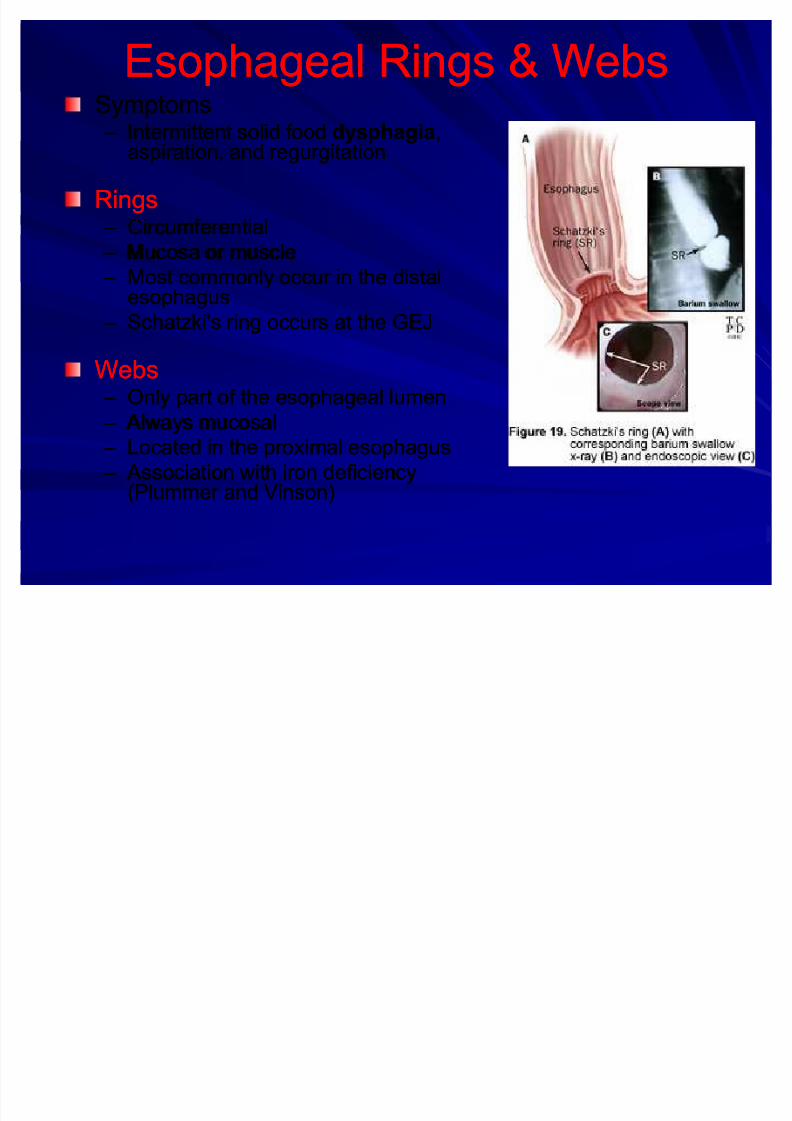
Esophageal Rings & WebsEsophageal Rings & WebsSymptomsSymptoms ± ± Intermittent solid foodIntermittent solid food dysphagiadysphagia,,
aspiration, and regurgitationaspiration, and regurgitation
RingsRings ± ± CircumferentialCircumferential
± ± Mucosa or muscleMucosa or muscle
± ± Most commonly occur in the distalMost commonly occur in the distalesophagusesophagus
± ± Schatzki's ring occurs at the GEJSchatzki's ring occurs at the GEJ
WebsWebs ± ± Only part of the esophageal lumenOnly part of the esophageal lumen
± ± Always mucosal Always mucosal ± ± Located in the proximal esophagusLocated in the proximal esophagus
± ± Association with iron deficiency Association with iron deficiency(Plummer and Vinson)(Plummer and Vinson)

8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 49/92
DiagnosisDiagnosis
Barium EsophagogramBarium Esophagogram ± ± Most sensitive testMost sensitive test
Endoscopic visualizationEndoscopic visualization ± ± NormalNormal--appearing mucosalappearing mucosal
± ± Cervical webs are associatedCervical webs are associatedwith carcinomawith carcinoma
TreatmentTreatment ± ± Endoscopic dilationEndoscopic dilation
± ± Large bougie or balloon (15 toLarge bougie or balloon (15 to20 mm) so as to fracture the20 mm) so as to fracture the
ringring ± ± Refractory ringsRefractory rings
Pneumatic dilation (largePneumatic dilation (largeballoon)balloon)
Electrosurgical incisionElectrosurgical incision
Surgical resectionSurgical resection
Treat GERDTreat GERD

8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 50/92
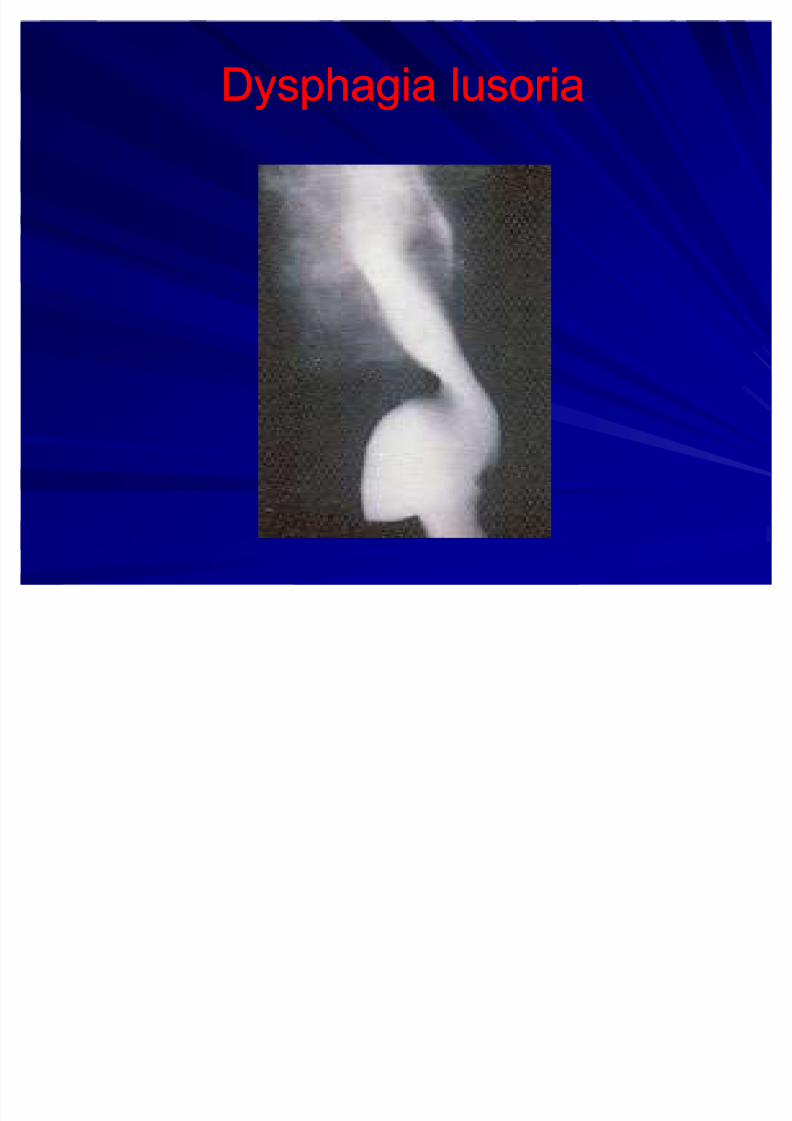
Dysphagia lusoriaDysphagia lusoria
Aberrant right subclavian artery Aberrant right subclavian artery ± ± Arises from the left side of the aortic arch Arises from the left side of the aortic arch
± ± Compress the posterior esophagusCompress the posterior esophagus
± ± 20% of cases anterior 20% of cases anterior Barium esophagogramBarium esophagogram
± ± Indentation at the level of the third and fourthIndentation at the level of the third and fourth
thoracic vertebraethoracic vertebrae
ConfirmationConfirmation
± ± CT, MRI, arteriography, or EUSCT, MRI, arteriography, or EUS
8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 51/92
Dysphagia lusoriaDysphagia lusoria
EndoscopyEndoscopy ± ± Right radial pulse may diminish with compression of Right radial pulse may diminish with compression of
the right subclavian arterythe right subclavian artery
Esophageal manometryEsophageal manometry ± ± HighHigh--pressure zone at the location of the aberrantpressure zone at the location of the aberrantarteryartery
Symptoms usually respond to changes in diet toSymptoms usually respond to changes in diet tosoft consistency and small sizesoft consistency and small size
When necessary, surgery relieves theWhen necessary, surgery relieves theobstruction by reanastomosing the aberrantobstruction by reanastomosing the aberrantartery to the ascending aortaartery to the ascending aorta
8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 52/92
8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 53/92
Globus hystericusGlobus hystericus
Pressure, fullness, or a lump in the throat,Pressure, fullness, or a lump in the throat,
not related to mealsnot related to meals
overweight, depressed, obsessive,overweight, depressed, obsessive,menopausal femalesmenopausal females
Pt may have fear of cancer in the throatPt may have fear of cancer in the throat
Actually often associated with GERD Actually often associated with GERDClinical examClinical exam--normalnormal
TreatmentTreatment--reassurancereassurance
8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 54/92
Gastroesophageal RefluxGastroesophageal Reflux
DiseaseDisease
GERD is recognized in about 10GERD is recognized in about 10--15% of the15% of thepopulationpopulation
Ref lux esophagitisRef lux esophagitis ± ± Changes in the esophageal mucosaChanges in the esophageal mucosa
± ± Present in 30% to 40%Present in 30% to 40%
Barrett's esophagusBarrett's esophagus ± ± 10% to 20%10% to 20%
Defects in the esophagogastric barrier such asDefects in the esophagogastric barrier such as ± ± LES incompetenceLES incompetence
± ± Transient relaxation of LESTransient relaxation of LES
± ± Hiatal herniaHiatal hernia

8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 55/92
55

8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 56/92
8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 57/92
8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 58/92
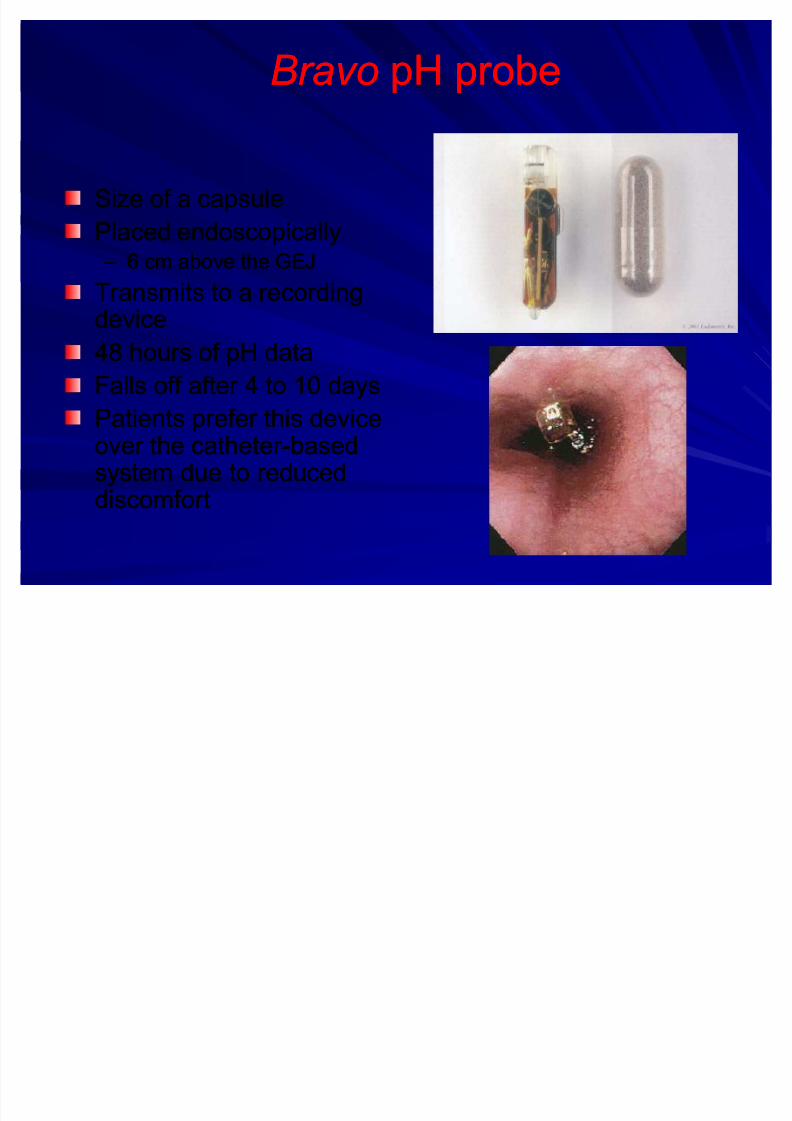
BravoBravo pH probepH probe
Size of a capsuleSize of a capsule
Placed endoscopicallyPlaced endoscopically ± ± 6 cm above the GEJ6 cm above the GEJ
Transmits to a recordingTransmits to a recordingdevicedevice
48 hours of pH data48 hours of pH data
Falls off after 4 to 10 daysFalls off after 4 to 10 days
Patients prefer this devicePatients prefer this deviceover the catheter over the catheter--basedbasedsystem due to reducedsystem due to reduceddiscomfortdiscomfort

8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 59/92
EndoscopyEndoscopy
± ± Reflux esophagitisReflux esophagitis
Erosions or ulcerationsErosions or ulcerations
± ± pH probe results arepH probe results arenormal in 25% of normal in 25% of
patients with erosivepatients with erosive
esophagitisesophagitis
8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 60/92

8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 61/92
8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 62/92
62

8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 63/92
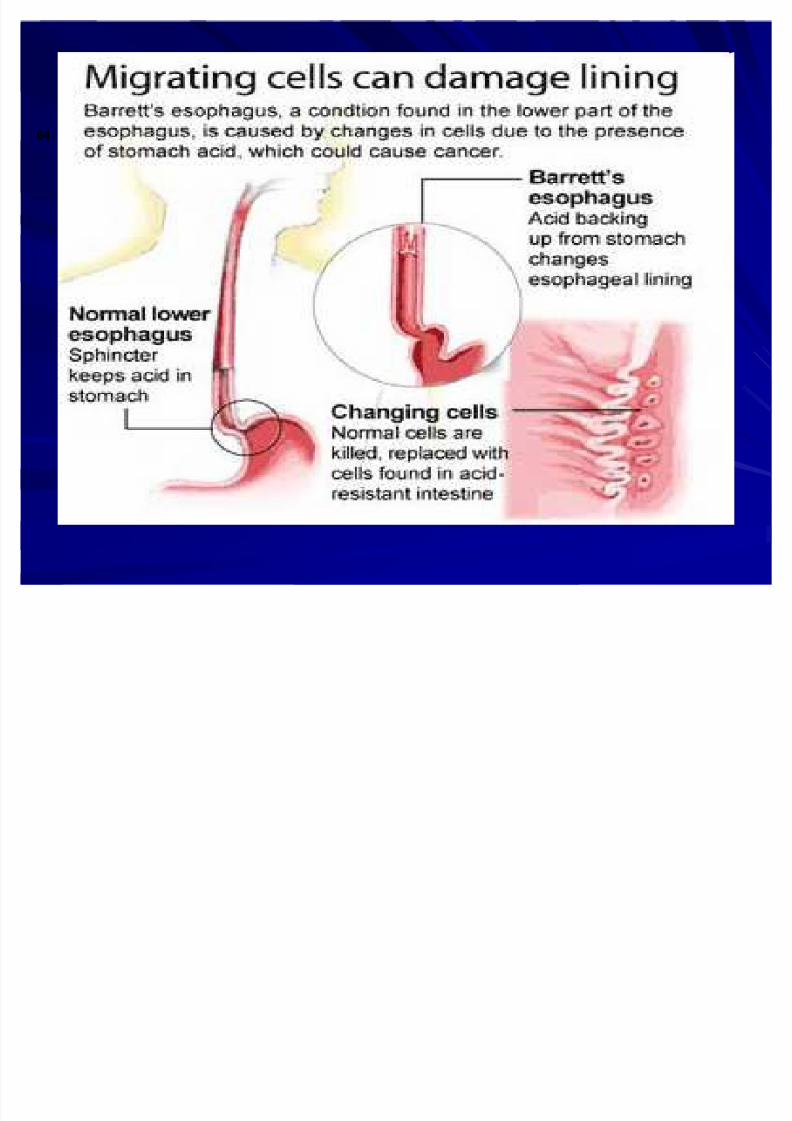
Barrett's esophagusBarrett's esophagus
Potentially serious complication of longPotentially serious complication of long--standing GERDstanding GERD
Stratified squamous epithelium of theStratified squamous epithelium of the
distal esophagus is replaced by intestinaldistal esophagus is replaced by intestinalcolumnar metaplasiacolumnar metaplasia
It is the most significant outcome of It is the most significant outcome of
chronic GERD and predisposes patients tochronic GERD and predisposes patients tothe development of esophagealthe development of esophagealadenocarcinoma.adenocarcinoma.
8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 64/92
8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 65/92

8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 66/92
Zenker¶s DiverticulumZenker¶s Diverticulum
Esophageal diverticula areEsophageal diverticula areclassified based on:classified based on: ± ± Anatomic location Anatomic location
± ± Mechanism of origin (pulsion or Mechanism of origin (pulsion or traction).traction).
Zenker's diverticulum (ZD)Zenker's diverticulum (ZD) ± ± Pulsion type diverticulumPulsion type diverticulum
Herniation of esophageal mucosa andHerniation of esophageal mucosa and
submucosa through an area of weakenedsubmucosa through an area of weakenedesophageal musculatureesophageal musculature
± ± Males predominance (2 to 3 times)Males predominance (2 to 3 times)
8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 67/92
Risk factorsRisk factors
Older ageOlder age
Male gender Male gender
Hiatal herniaHiatal herniaGastroesophageal refluxGastroesophageal reflux
NOTES:
Up to 94% of patients with pharyngeal pouches are found to have GERD
and/or hiatal hernias.
8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 68/92
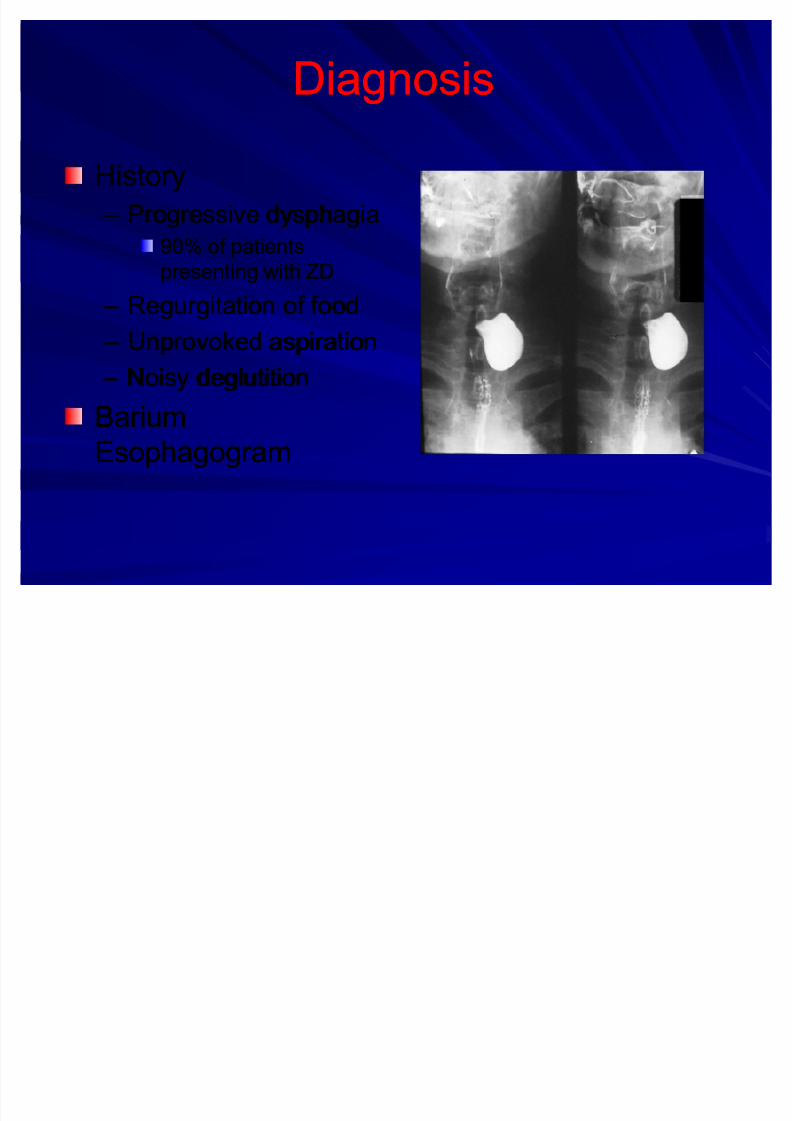
DiagnosisDiagnosis
HistoryHistory
± ± Progressive dysphagiaProgressive dysphagia
90% of patients90% of patients
presenting with ZDpresenting with ZD
± ± Regurgitation of foodRegurgitation of food
± ± Unprovoked aspirationUnprovoked aspiration
± ± Noisy deglutitionNoisy deglutition
BariumBariumEsophagogramEsophagogram

8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 69/92
TreatmentTreatment
ExternalExternal ± ± cricopharyngealcricopharyngeal
myotomymyotomy
± ± Diverticulum isDiverticulum isexcised and theexcised and thedefect closeddefect closed
Endoscopic techniquesEndoscopic techniques::endoscopic stapleendoscopic staplediverticulostomy, CO2diverticulostomy, CO2laser, electrocauterylaser, electrocautery

8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 70/92
8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 71/92
8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 72/92
InvestigationsInvestigations
Full blood count:Full blood count: hypochromic microcytichypochromic microcytic
anemia, low serum ferritin levelsanemia, low serum ferritin levels
Barium swallow:Barium swallow: narrowing of the upper narrowing of the upper
esophagus with a web in the anterior wallesophagus with a web in the anterior wall
Endoscopy:Endoscopy: friable web can be seenfriable web can be seen
across the lumen of the esophagusacross the lumen of the esophagus
72

8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 73/92

8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 74/92
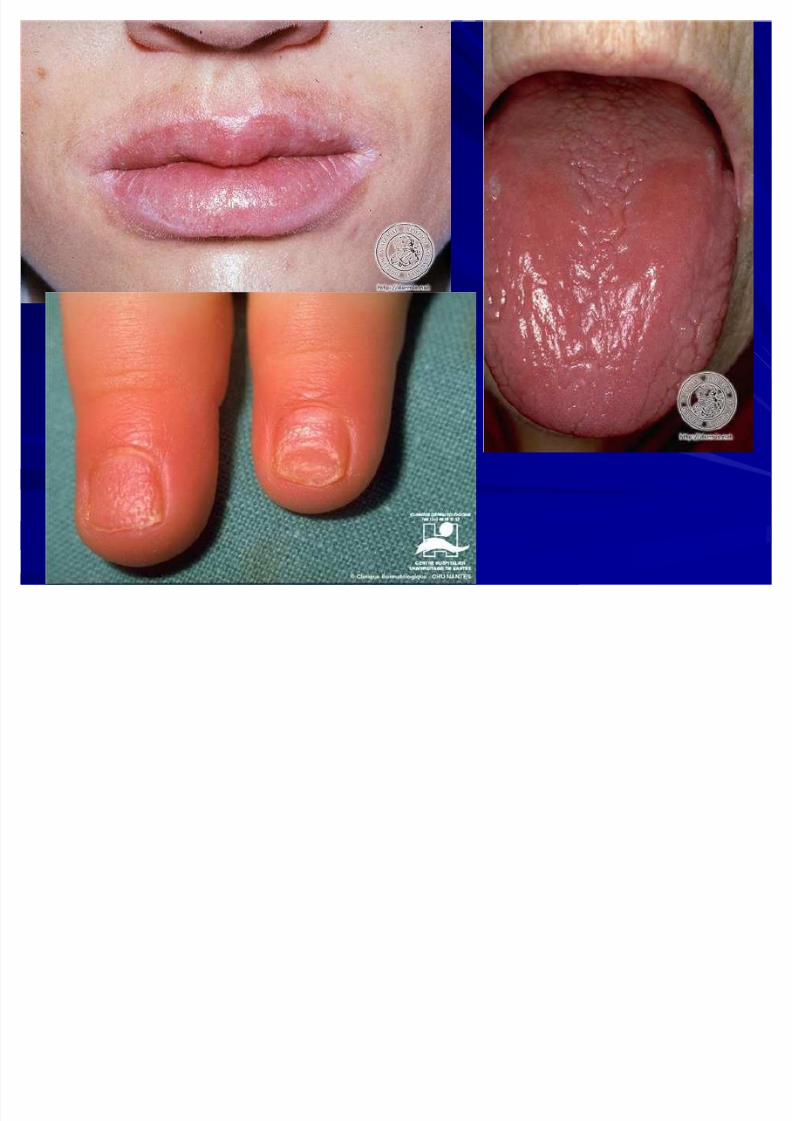
Plummer Plummer--Vinson SyndromeVinson Syndrome
Rx: iron replacement alone may reverse someRx: iron replacement alone may reverse some
of the pathologic changesof the pathologic changes
dilation of webdilation of web
Increased incidence of postcricoid CAIncreased incidence of postcricoid CA
8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 75/92
8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 76/92
Esophageal CarcinomaEsophageal Carcinoma
Oesophageal carcinoma is becoming more common,Oesophageal carcinoma is becoming more common,unlike the trend observed in gastric carcinoma.unlike the trend observed in gastric carcinoma.
Squamous carcinomaSquamous carcinoma typically arises in the upper typically arises in the upper 2/3 of the oesophagus2/3 of the oesophagus
AdenocarcinomaAdenocarcinoma usually arises in a region of usually arises in a region of
specialised columnar epithelium (SCE) metaplasia inspecialised columnar epithelium (SCE) metaplasia inthe lower 1/3 of the oesophagusthe lower 1/3 of the oesophagus -- Barrett'sBarrett'soesophagus.oesophagus.
Risk Factors for Oesophageal CaRisk Factors for Oesophageal Ca
8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 77/92
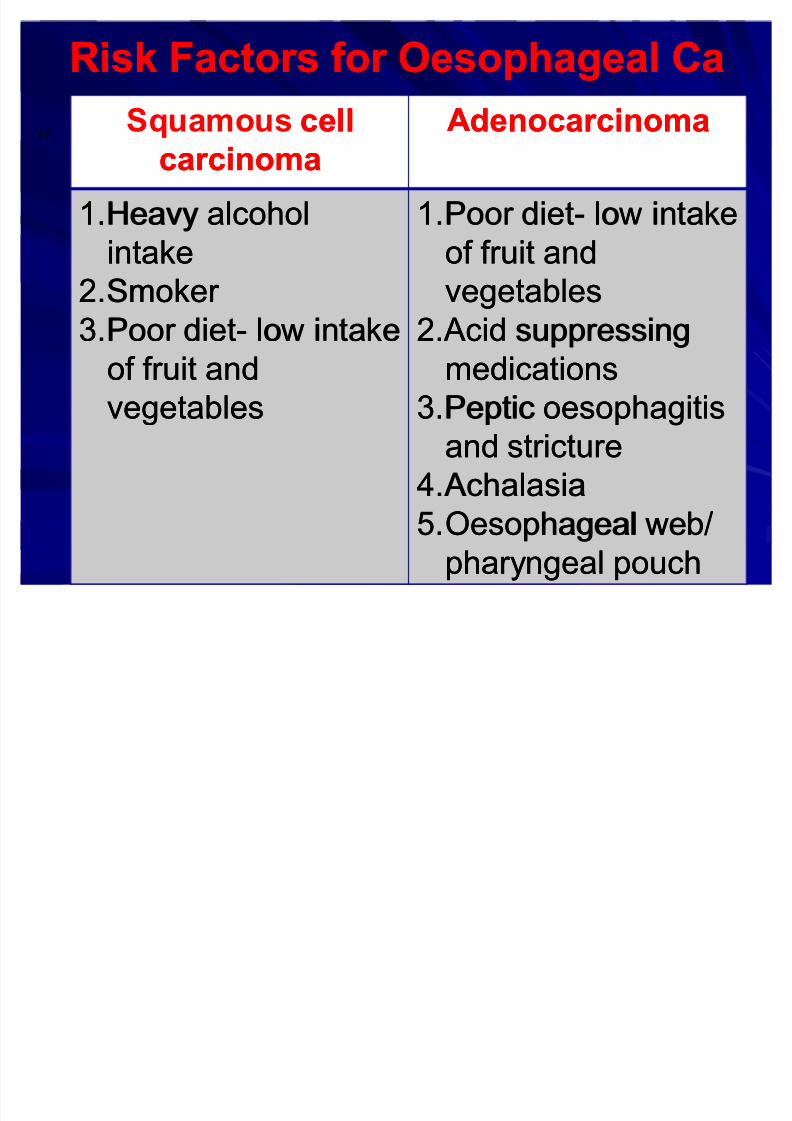
Risk Factors for Oesophageal CaRisk Factors for Oesophageal Ca
Squamous cellcell
carcinomacarcinoma
AdenocarcinomaAdenocarcinoma
1.1.Heavy alcoholHeavy alcohol
intakeintake
2.2.Smoker Smoker 3.3.Poor dietPoor diet-- low intakelow intake
of fruit andof fruit and
vegetablesvegetables
1.1.Poor dietPoor diet-- low intakelow intake
of fruit andof fruit and
vegetablesvegetables2.2.Acid suppressing Acid suppressing
medicationsmedications
3.3.Peptic oesophagitisPeptic oesophagitis
and strictureand stricture
4.4.Achalasia Achalasia
5.5.Oesophageal web/Oesophageal web/
pharyngeal pouchpharyngeal pouch
77
8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 78/92
Clinical FeaturesClinical Features
Dysphagia is the most frequently presentedDysphagia is the most frequently presented
feature of oesophageal carcinoma :feature of oesophageal carcinoma :
± ± patient may recount a short history of progressivepatient may recount a short history of progressive
dysphagia, initially affecting solids only, butdysphagia, initially affecting solids only, but
gradually affecting the swallowing of fluids.gradually affecting the swallowing of fluids.
± ± interruption of the passage of food may causeinterruption of the passage of food may cause
the individual to slowly alter the diet from solid tothe individual to slowly alter the diet from solid to
liquid nutrition.liquid nutrition.
8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 79/92
Clinical FeaturesClinical Features
± ± the level at which difficulty in swallowing isthe level at which difficulty in swallowing is
encountered may be identifiable by theencountered may be identifiable by thepatient.patient.
± ± Short history of Short history of dysphagiadysphagia in anin an elderlyelderly
male is almostmale is almost certainlycertainly carcinomacarcinoma of theof the
oesophagus or the cardia of the stomach.oesophagus or the cardia of the stomach.

8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 80/92
Clinical FeaturesClinical Features
Other local features may include :Other local features may include :
± ± regurgitation of food or bloodregurgitation of food or blood--stained vomitstained vomit
± ± aspiration pneumoniaaspiration pneumonia
± ± pain :pain :
classically, retrosternally and in the interscapular classically, retrosternally and in the interscapular
regionregion
it may radiate to the jaws and armsit may radiate to the jaws and arms
8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 81/92
8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 82/92
DiagnosisDiagnosis
The diagnosis of oesophageal carcinoma isThe diagnosis of oesophageal carcinoma is
made on :made on :
± ± History and examinationHistory and examination
± ± Barium swallowBarium swallow
± ± Endoscopy and biopsyEndoscopy and biopsy
± ± CytologyCytology
± ± CT scanCT scan ± ± BronchoscopyBronchoscopy
± ± UltrasoundUltrasound
8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 83/92
InvestigationsInvestigations
Barium swallowBarium swallow ::
± ± the firstthe first--line investigation after the history of line investigation after the history of
dysphagiadysphagia
± ± characteristic image of an irregular stricturecharacteristic image of an irregular stricturewith shouldered margins, 4with shouldered margins, 4--10 cm long and10 cm long and
often tortuousoften tortuous
± ± a tracheoa tracheo--oesophageal fistula may also beoesophageal fistula may also be
demonstrateddemonstrated
E h l CE h l C

8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 84/92
Esophageal Cancer Esophageal Cancer
Barium SwallowBarium Swallow EndoscopyEndoscopy
8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 85/92
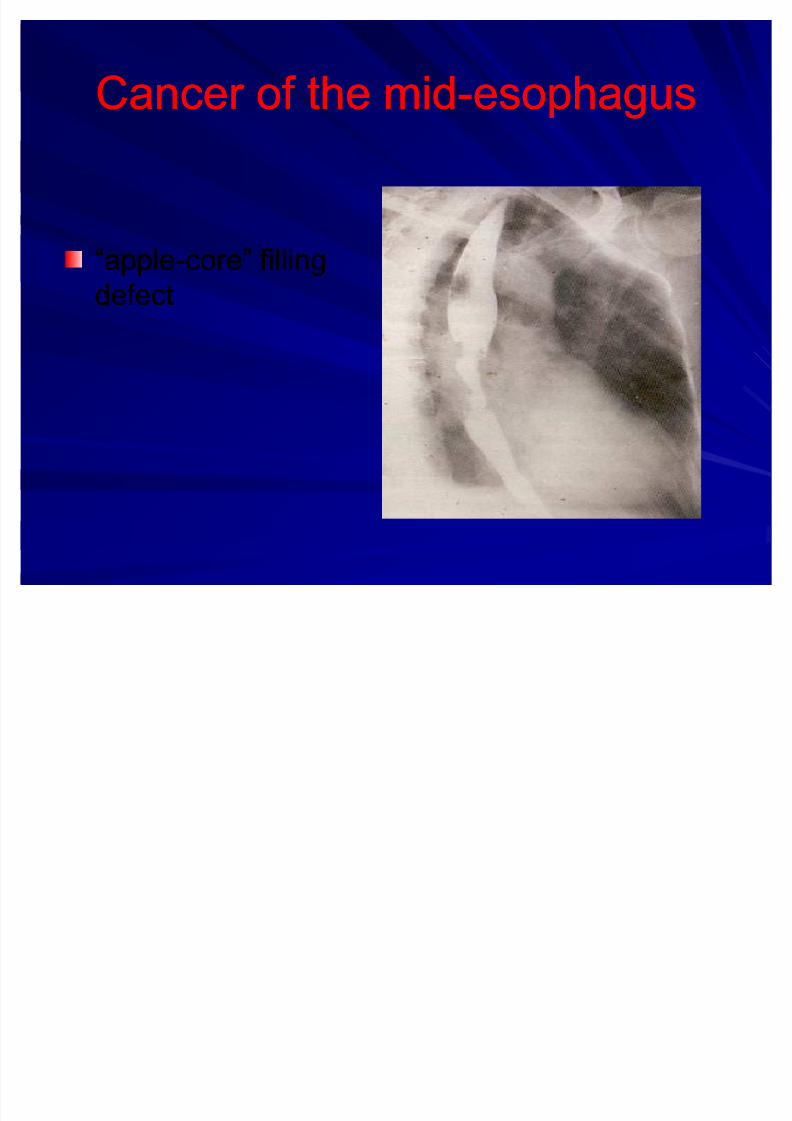
Cancer of the midCancer of the mid--esophagusesophagus
³apple³apple--core´ fillingcore´ filling
defectdefect

8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 86/92
InvestigationsInvestigations
Endoscopy and BiopsyEndoscopy and Biopsy ::
± ± establishes histology and limits of lesionestablishes histology and limits of lesion
± ± can be used therapeutically to dilate, socan be used therapeutically to dilate, so
improving nutrition before a definitiveimproving nutrition before a definitiveoperative interventionoperative intervention
I ti tiI ti ti
8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 87/92
InvestigationsInvestigationscytologycytology by washing / abrasion techniqueby washing / abrasion technique
CT scanningCT scanning helps to determine mediastinalhelps to determine mediastinal
involvement and whether metastasis hasinvolvement and whether metastasis has
occurred to the liver occurred to the liver
bronchoscopybronchoscopy may be needed to excludemay be needed to exclude
bronchial involvement in upper and middlebronchial involvement in upper and middle--thirdthird
lesionslesions
ultrasoundultrasound may be used to identify secondarymay be used to identify secondary
liver depositsliver deposits
8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 88/92
ManagementManagement
Management of oesophageal carcinomaManagement of oesophageal carcinoma
is dependent on the level of the lesion andis dependent on the level of the lesion and
the stage of the disease.the stage of the disease.
± ± Upper third lesionUpper third lesion
± ± Middle third lesionMiddle third lesion
± ± Lower third lesionLower third lesion
M tM t
8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 89/92
ManagementManagement
Upper third lesionUpper third lesion::high dose radiotherapy is indicatedhigh dose radiotherapy is indicated
Middle third lesionMiddle third lesion ::
Early tumours are resectable. Again,Early tumours are resectable. Again,radical radiotherapy may be indicated if theradical radiotherapy may be indicated if the
lesion is up to 5 cm long .lesion is up to 5 cm long .
Lower third lesionLower third lesion ::
most accessible surgically;most accessible surgically;adenocarcinomas areadenocarcinomas are radioresistantradioresistant
8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 90/92
ManagementManagement
Extensive disease requiresExtensive disease requires palliation of palliation of
dysphagiadysphagia::
± ± endoscopic laser surgery for lesions less than 8endoscopic laser surgery for lesions less than 8
cm longcm long
± ± oesophageal stentingoesophageal stenting
e.g. with a Celestin tubee.g. with a Celestin tube -- if longer than 8 cmif longer than 8 cm
± ± alternatives include:alternatives include:oesophagooesophago--gastrostomy or oesophagogastrostomy or oesophago--jejunostomy jejunostomy
short course radiotherapyshort course radiotherapy

8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 91/92

8/8/2019 dysphagia new1
http://slidepdf.com/reader/full/dysphagia-new1 92/92
Thank
you
Related Documents











