
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Cholesterol is lipid serves as precursor to steroid hormones , bile acid, and the main component of cell membrane.
Cholesterol in blood reflect 40-60% of endogenous cholesterol.
Cholesterol , triglyceride and lipid transport through lipoprotein.
Saturated ,unsaturated fats and cholesterol digested, reformulated and packaged into chylomicrons by cell of intestinal endothelium.
Source:clinical pharmacy &therapeutic 5th edition
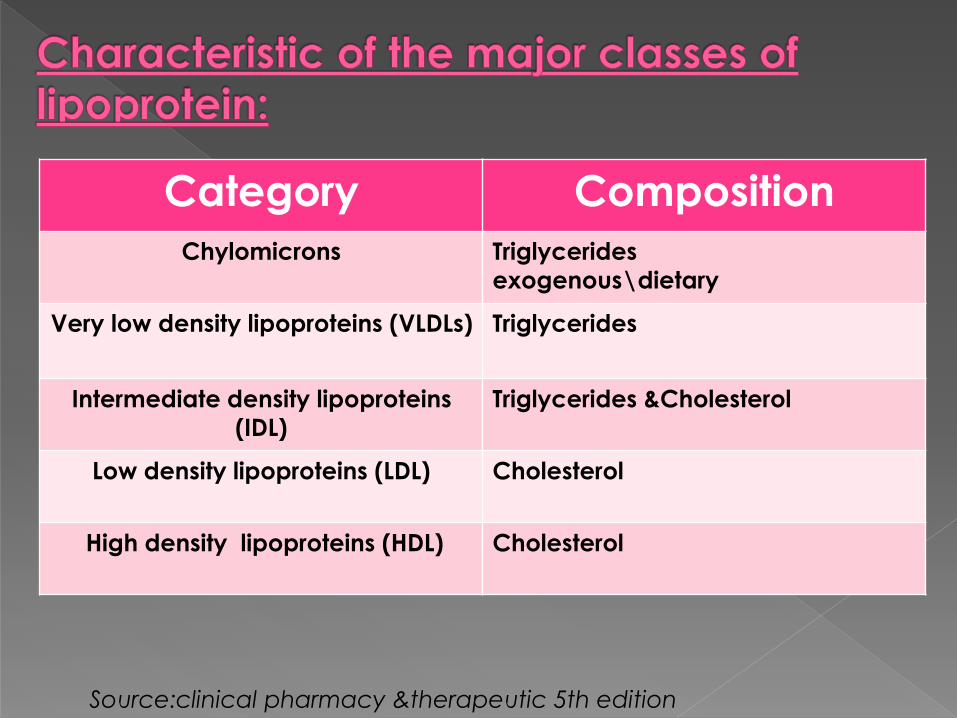
Category Composition
Chylomicrons Triglycerides
exogenous\dietary
Very low density lipoproteins (VLDLs) Triglycerides
Intermediate density lipoproteins
(IDL)
Triglycerides &Cholesterol
Low density lipoproteins (LDL) Cholesterol
High density lipoproteins (HDL) Cholesterol
Source:clinical pharmacy &therapeutic 5th edition
Chylomicrons enter the lymphatic system and travel through body until broken down by lipoprotein lipase in the capillary beds to chylomicron remnant (smaller , less dense and contain apolipoprotein B48,E and then cleared from circulation by LDL receptor in the liver
This is replenishing cholesterol pool in the liver which synthesize cholesterol also by endogenous pathway and transported by LDL,VLDL and HDL.
Triglyceride (TG) synthesis by the liver in the excess of carbohydrate and secreted as VLDL
Source:clinical pharmacy &therapeutic 5th edition

VLDL contain five times more TG than
cholesterol and contain apolipoprotein
C-II,B-100 ,E. Apolipoprotein B-100 and E
link with LDL cell receptor.
Apo lipoprotein C-II function as cofactor
for lipoprotein lipase.
Source:clinical pharmacy &therapeutic 5th edition
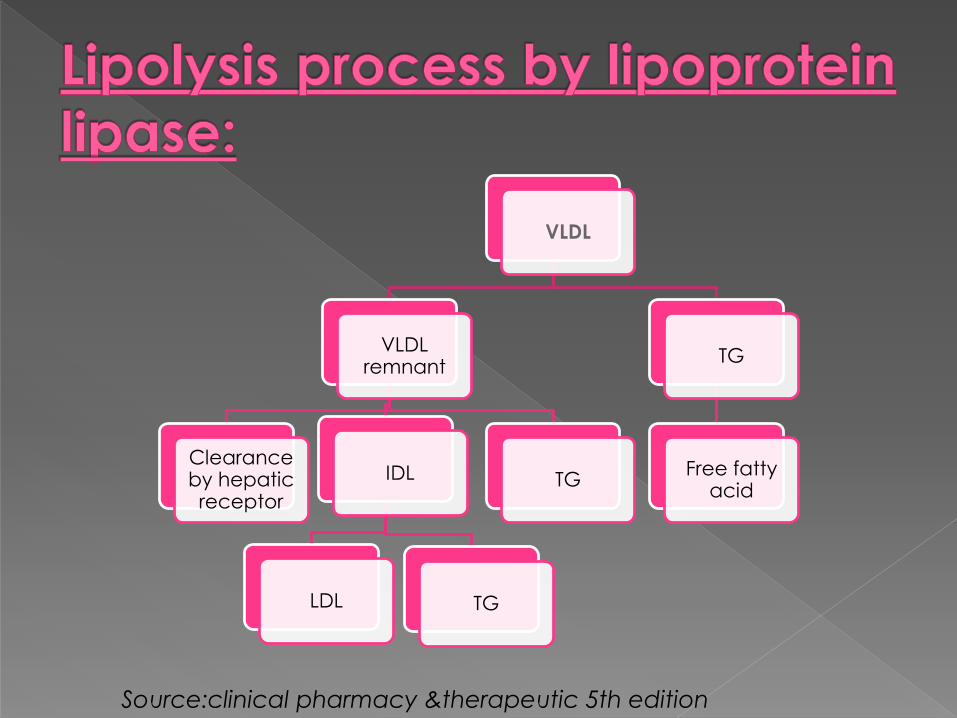
VLDL
VLDL remnant
Clearance by hepatic receptor
IDL
LDL TG
TG
TG
Free fatty acid
Source:clinical pharmacy &therapeutic 5th edition

LDL is primary atherogenic lipoprotein and
the smaller size of LDL particle of more able
to penetrate into sub endothelial tissue
where it contribute to the development of
atherosclerosis .
Two type of LDL been associated with CHD:
1\ Lipoprotein(a) LP(a) particle is LDL particle
surrounded by plasminogen –like protein
2\Atherogenic lipoprotein phenotype B found
in30%population associated with CHD risk.
Source:clinical pharmacy &therapeutic 5th edition
The atherosclerotic plaque formation initiated by entrance of LDL and LP(a)into sub endothelial space with their oxidative modified free radicals produced by cells which activated macrophage yielding lipid rich foam which continue to progress with same times of the cell proliferation and collagen synthesis.
HDL rich in cholesterol and very small ,However appears in reverse cholesterol transport resulting in anti atherogenic effect.
Source:clinical pharmacy &therapeutic 5th edition
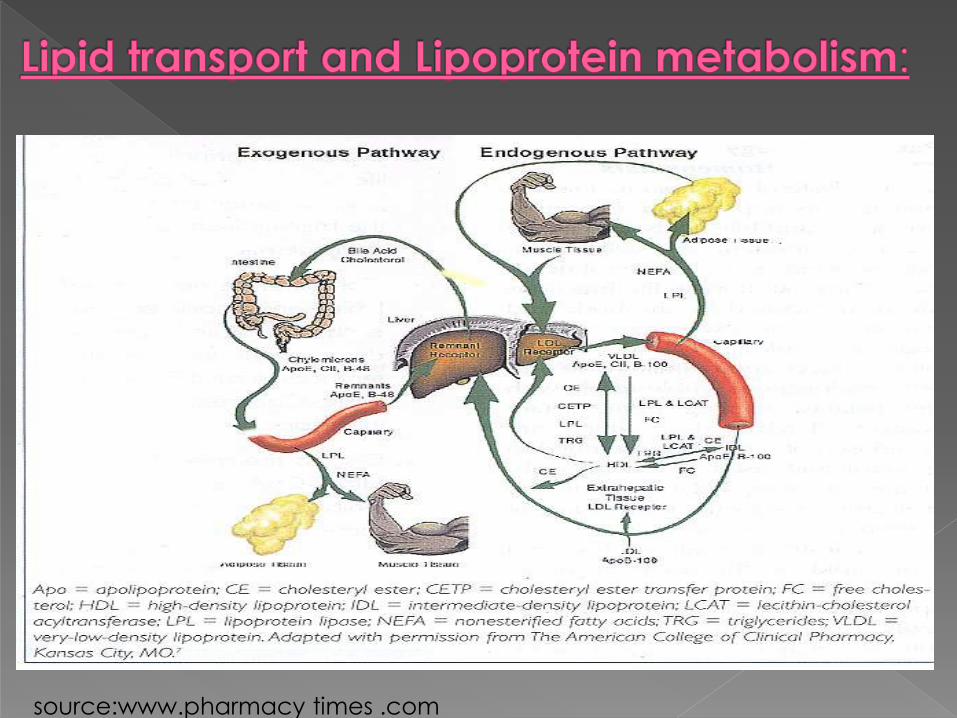
source:www.pharmacy times .com
HDL may prevent or remove cholesterol in the intimae by :
1\competitively inhibit uptake of LDL by endothelial cells
2\ prevent LDL oxidation.
3\ inhibit platelet activation by LDL and aggregation by increase prostacyclin production.
4\promote fibrolysis by stabilizing prostacyclin.
LDL serve as marker of metabolism of chylomicron and VLDL (increase TG, decrease HDL).
Source:clinical pharmacy &therapeutic 5th edition

1- Type I (high level of chylomicrons).
2-Type II a (high level of LDL)
3-Type II b (high level of LDL+VLDL)
4-Type III (high level of IDL )
5-Type IV (high level of VLDL)
6-Type V ( high level of VLDL
+chylomicrons)
Source:hand book of pharmacotherapy 8th edition
Dyslipidaemia defined as elevated of
total cholesterol ,LDL, TG, low HDL or
combination of these abnormalities.
According to etiology dyslipidaemia
classified to:
1- primary or genetic lipoprotein disorder.
2-secondary dyslipidaemia (drugs
&diseases).
Source:hand book of pharmacotherapy 8th edition
Secondary dyslipidaemia due to:
1. Diseases( liver disease ,chronic renal
failure ,nephrotic syndrome, obesity
,hypothyroidism ,diabetes ,alcohol )
2. Drugs (corticosteroids,thiazide diuretic
,cyclosporine ,oral contraceptive , HIV
protease inhibitors ,B-blockers)
Source:clinicl pharmacology 5th edition
In type I there are:
1-repeated attack of pancreatitis.
2-abdominal pain.
3-euraptive cutanous xanthomatosis.
4-hepatosplenomegaly beginning in childhood.
Note: symptoms severity increased with increased dietary fat intake. accelerated atherosclerosis not associated with this disease
Source:hand book of pharmacotherapy 8th edition
Type III the clinical feature appears after 20 years :
1- xanthoma
2- severe atherosclerosis
Type IV occur in adult and similar to secondary dyslipidaemia.
Type V :
-abdominal pain , pancreatitis ,xanthoma ,peripheral polyneuropathy and renal insufficient.
Note: atherosclerosis is increased with this disorder
Source:hand book of pharmacotherapy 8th edition
Angina.
Myocardial infraction (MI).
Arrhythmias.
Stroke.
Peripheral arterial disease.
Abdominal aortic aneurysm.
Sudden death.
Source:hand book of pharmacotherapy 8th edition

CVD is the leader amongst the causes of death worldwide.
Prevalence of CVD including CHD is increasing rapidly in Sudan.
Increasing burden of risk factors like:› Hypertension
› Smoking
› Obesity
› Diabetes
› Dyslipidemia
Source:clinical pharmacy &therapeutic 5th edition

CVD 30%
17.4 million
OTHERS
Total 58 million death worldwide
3.3 times than the total
no. of death due to HIV,
Malaria, and
Tuberculosis combined
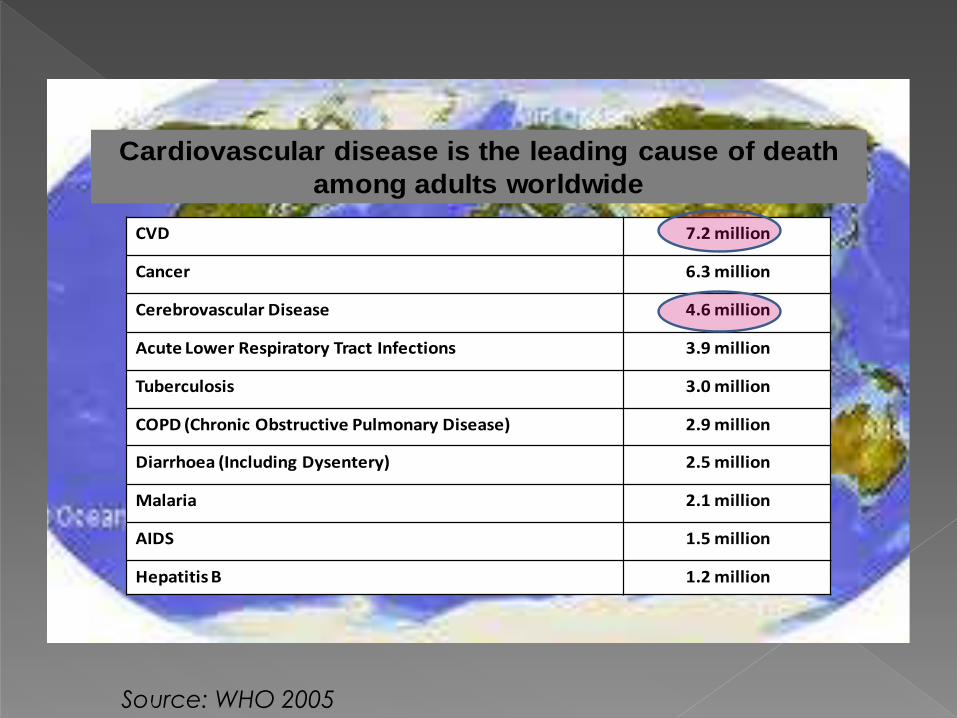
Cardiovascular disease is the leading cause of death
among adults worldwide
CVD 7.2 million
Cancer 6.3 million
Cerebrovascular Disease 4.6 million
Acute Lower Respiratory Tract Infections 3.9 million
Tuberculosis 3.0 million
COPD (Chronic Obstructive Pulmonary Disease) 2.9 million
Diarrhoea (Including Dysentery) 2.5 million
Malaria 2.1 million
AIDS 1.5 million
Hepatitis B 1.2 million
Source: WHO 2005
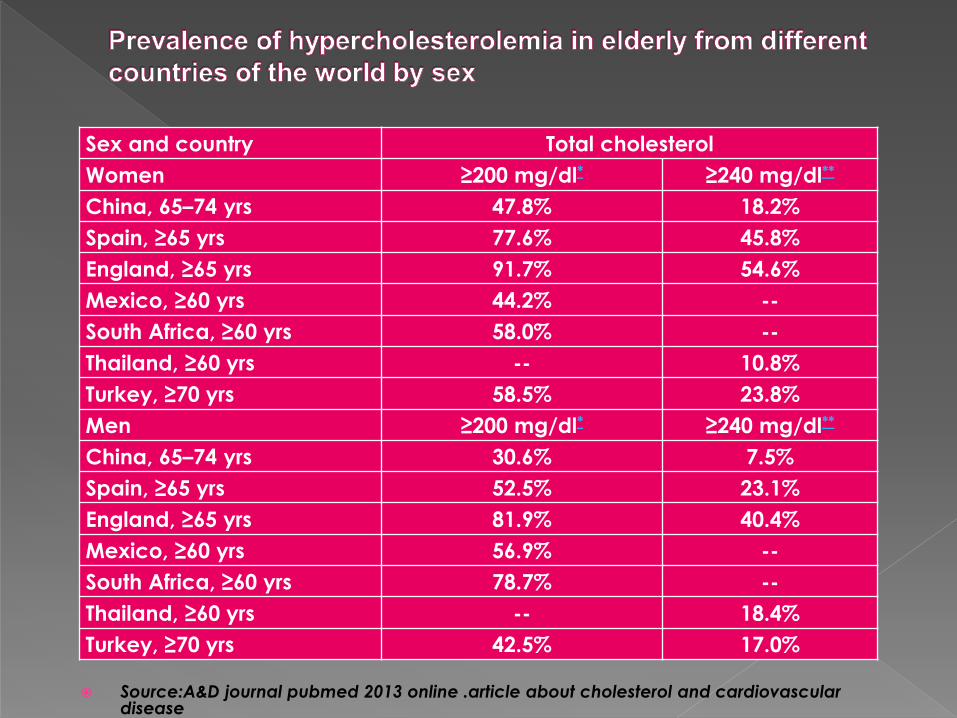
Source:A&D journal pubmed 2013 online .article about cholesterol and cardiovascular disease
Sex and country Total cholesterol
Women ≥200 mg/dl* ≥240 mg/dl**
China, 65–74 yrs 47.8% 18.2%
Spain, ≥65 yrs 77.6% 45.8%
England, ≥65 yrs 91.7% 54.6%
Mexico, ≥60 yrs 44.2% --
South Africa, ≥60 yrs 58.0% --
Thailand, ≥60 yrs -- 10.8%
Turkey, ≥70 yrs 58.5% 23.8%
Men ≥200 mg/dl* ≥240 mg/dl**
China, 65–74 yrs 30.6% 7.5%
Spain, ≥65 yrs 52.5% 23.1%
England, ≥65 yrs 81.9% 40.4%
Mexico, ≥60 yrs 56.9% --
South Africa, ≥60 yrs 78.7% --
Thailand, ≥60 yrs -- 18.4%
Turkey, ≥70 yrs 42.5% 17.0%
DM in Africa: Up to 13% or more adults in
urban communities.
Diabetes is present in 10% of all hospital
admission in Sudan.
Diabetes is responsible for 10% of
hospital mortality.
Source:Diabetes Int 2000; 10: 18-9.
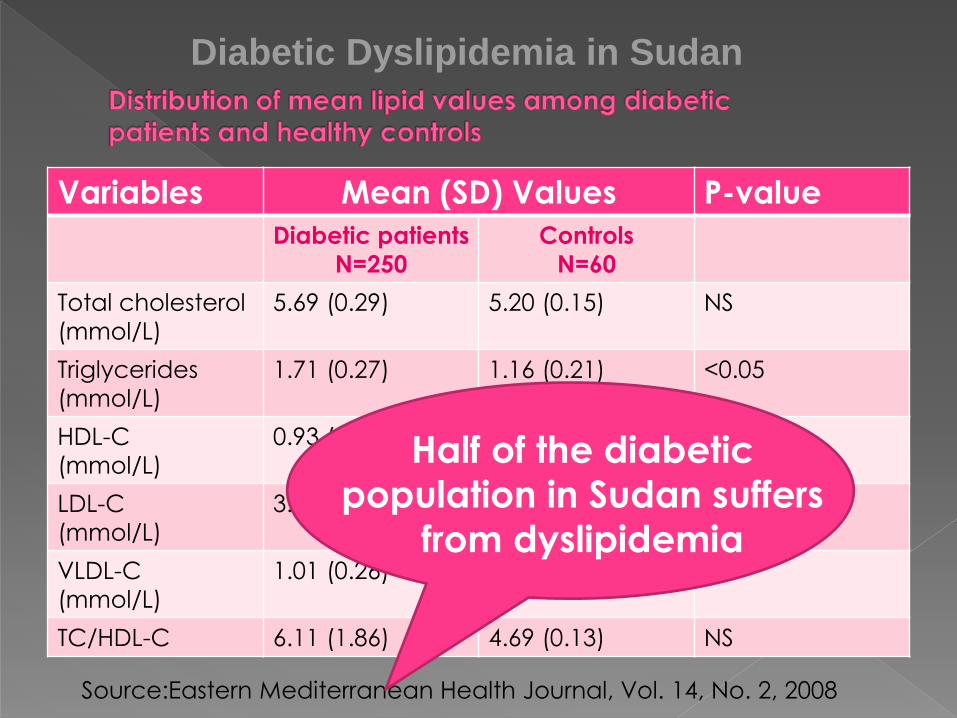
Variables Mean (SD) Values P-value
Diabetic patients
N=250
Controls
N=60
Total cholesterol
(mmol/L)
5.69 (0.29) 5.20 (0.15) NS
Triglycerides
(mmol/L)
1.71 (0.27) 1.16 (0.21) <0.05
HDL-C
(mmol/L)
0.93 (0.15) 1.11 (0.18) <0.05
LDL-C
(mmol/L)
3.68 (0.21) 3.45 (0.14) NS
VLDL-C
(mmol/L)
1.01 (0.26) 0.81 (0.11) NS
TC/HDL-C 6.11 (1.86) 4.69 (0.13) NS
Source:Eastern Mediterranean Health Journal, Vol. 14, No. 2, 2008
Half of the diabetic
population in Sudan suffers
from dyslipidemia
Diabetic Dyslipidemia in Sudan

What is being tested?
Cholesterol &Triglyceride in the blood sample.
Total cholesterol is determined from the
amount of cholesterol found in HDL, LDL and
VLDL.
LDL - if triglycerides < 400 then LDL is
calculated using Friewald formula:
((Calculated LDL=chol−HDL−TG/5)).
If triglycerides > 400 then LDL is measured
directly.
Non HDL= Total cholesterol – HDLc.Source: labtest online.org
How to ensure quality of the sample?
Fasting for 9-12 hrs before making the test
,only water is permitted.
When it is ordered ?
Adult:
Healthy adult with no risk factor for heart
disease once every 5 years.
Source: labtest online.org
Children &Adolescent :
AAP(American academy of pediatrics) recommended one test between 9 -11 yrs &again between 17- 21 yrs .
What does test results means?
LDL CholesterolOptimal: Less than 100 mg/dL (2.59 mmol/L) Near/above optimal: 100-129 mg/dL (2.59-3.34 mmol/L) Borderline high: 130-159 mg/dL (3.37-4.12 mmol/L) High: 160-189 mg/dL (4.15-4.90 mmol/L) Very high: Greater than 190 mg/dL (4.90 mmol/L)
Source: labtest online.org
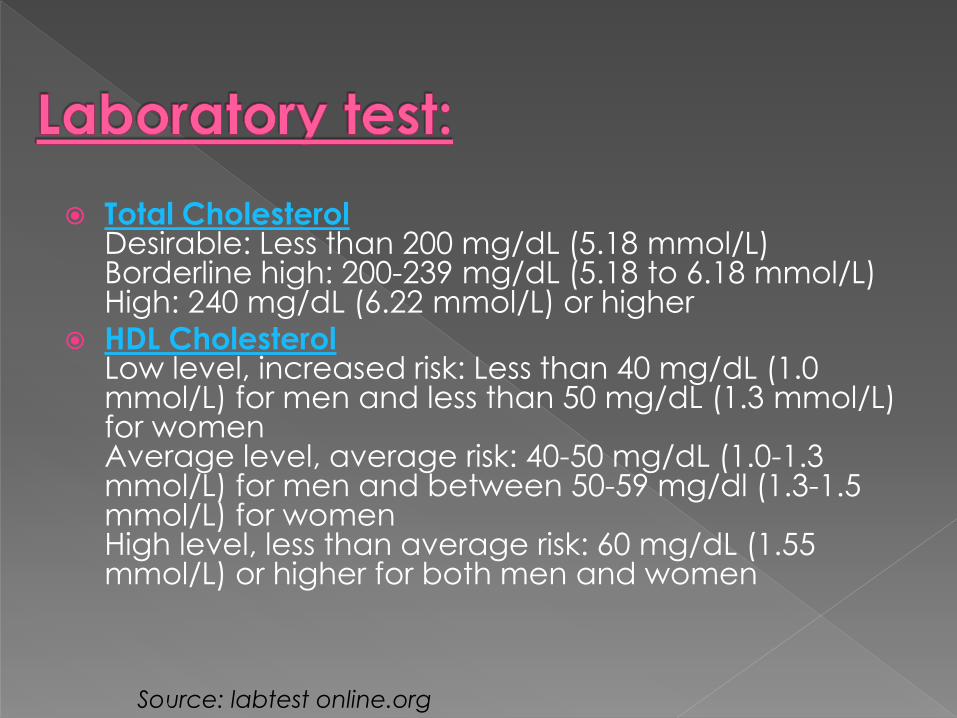
Total CholesterolDesirable: Less than 200 mg/dL (5.18 mmol/L) Borderline high: 200-239 mg/dL (5.18 to 6.18 mmol/L) High: 240 mg/dL (6.22 mmol/L) or higher
HDL CholesterolLow level, increased risk: Less than 40 mg/dL (1.0 mmol/L) for men and less than 50 mg/dL (1.3 mmol/L) for women Average level, average risk: 40-50 mg/dL (1.0-1.3 mmol/L) for men and between 50-59 mg/dl (1.3-1.5 mmol/L) for women High level, less than average risk: 60 mg/dL (1.55 mmol/L) or higher for both men and women
Source: labtest online.org
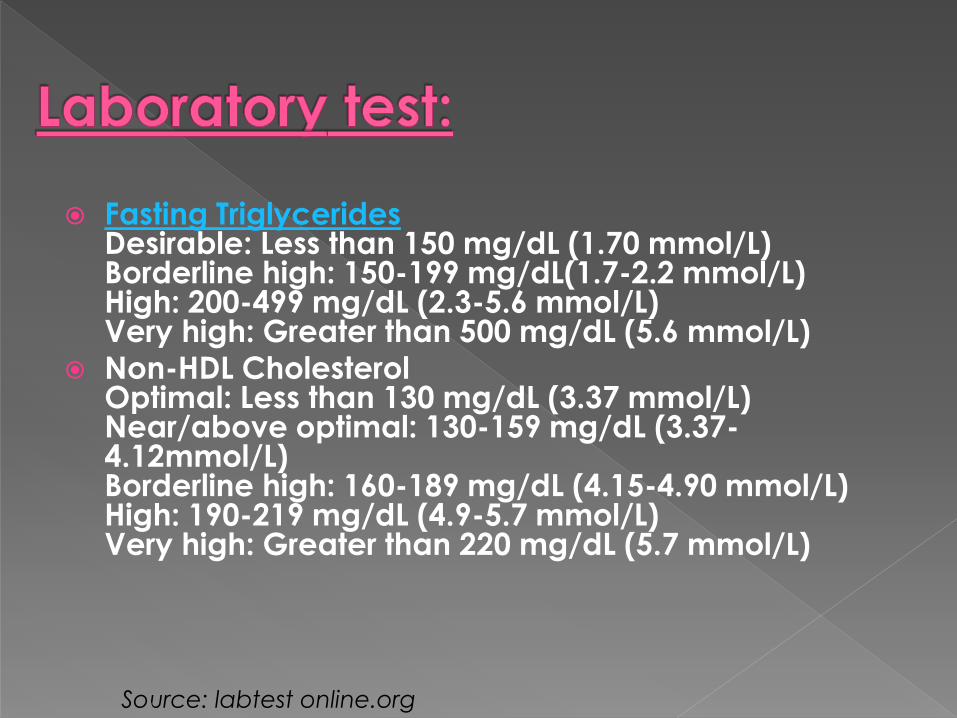
Fasting TriglyceridesDesirable: Less than 150 mg/dL (1.70 mmol/L)Borderline high: 150-199 mg/dL(1.7-2.2 mmol/L) High: 200-499 mg/dL (2.3-5.6 mmol/L) Very high: Greater than 500 mg/dL (5.6 mmol/L)
Non-HDL CholesterolOptimal: Less than 130 mg/dL (3.37 mmol/L) Near/above optimal: 130-159 mg/dL (3.37-4.12mmol/L) Borderline high: 160-189 mg/dL (4.15-4.90 mmol/L) High: 190-219 mg/dL (4.9-5.7 mmol/L) Very high: Greater than 220 mg/dL (5.7 mmol/L)
Source: labtest online.org
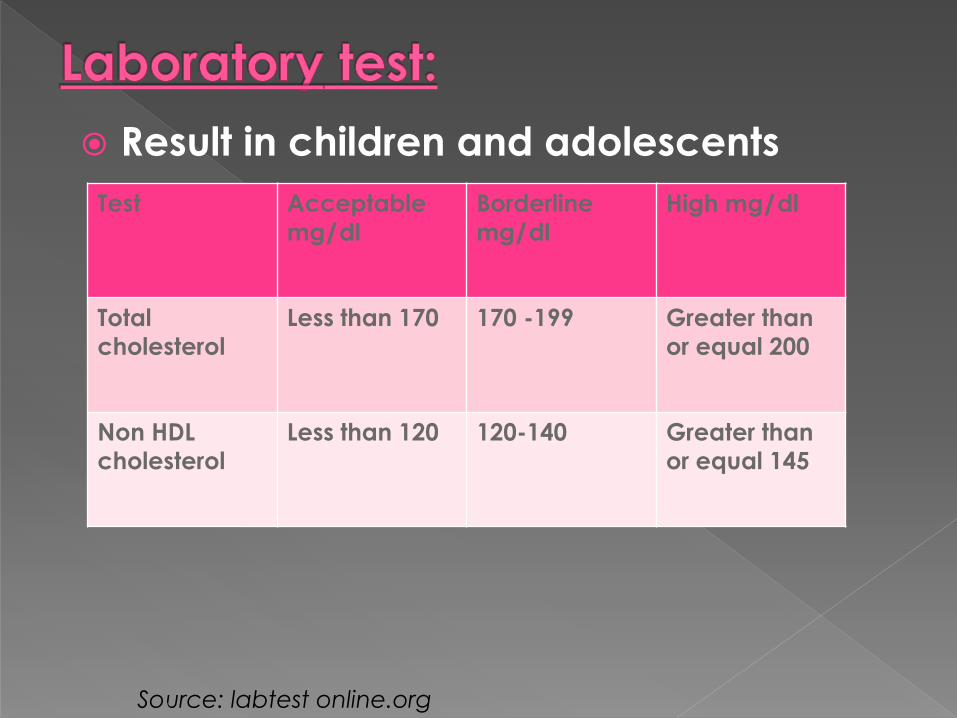
Result in children and adolescents
Test Acceptable
mg/dl
Borderline
mg/dl
High mg/dl
Total
cholesterol
Less than 170 170 -199 Greater than
or equal 200
Non HDL
cholesterol
Less than 120 120-140 Greater than
or equal 145
Source: labtest online.org

Therapeutic lifestyle change(TLC)should
be the first approach tried in all patient
this includes:
Dietary restriction of cholesterol and
saturated fatty acid.
Regular exercise.
Weight reduction.
Source:pharnacotherapy text book 7th edition

Inhibit cholesterol synthesis by inhibit
(HMG-Co A), increase LDL receptor and
enhance receptor mediated metabolism
and clearance of LDL from serum.
Beneficial effect on lipid parameters:
LDL c ↓ 18%-55%
HDL c ↑5-15%
TG ↓7%-30%
24%-40% reduction in coronary events.
source: medescape.org/ view article/561751
Potential adverse effects:
Myalgia ,Myopathy and increased liver enzymes
Contraindications:
Liver disease.
Precautions:
CYP3A4 enzyme inducer(phenytoin & barbiturate)
CYP3A4 enzyme inhibitors(ciclosporin & ketoconazole)
source: medescape.org/ view article/561751
Potential pleiotropic effects:
Improve endothelial function(up regulate eNOs, scavenge superoxide)
Antithrombotic effects(improve fibrinolytic balance ,inhibit platelet aggregation)
Anti-inflammatory effects(decrease activation of NF ,decrease macrophage infiltration)
Enhance plaque stability
Attenuate vascular smooth muscle cell proliferation
source: medescape.org/ view article/561751
Response to statin
Is there a role of ‘GENE’?
Genetic variation in HMGCR may
contribute to variation in the response
The CAP study, a 6-week simvastatin (40
mg/d) trial.
Designed to examine role of gene in
ethnic variability in statin response in
African/African Americans and
Caucasians.
Source :Circulation 2008;117;1537-1544

People carrying either H-2 or H-7 haplotypes:
African/African American: 64%
Caucasians: 11.6%
12 people carrying both, H-2 and H-7 haplotypes
11 were African/African American
1 was Caucasian
LDL-C reduction in carriers of both, H-2 and H-7 haplotypes vs. non-carriers -28% vs. -41.5%
Source:Circulation 2008;117;1537-1544
We need high dose of statins: Increasing prevalence of risk factors
Presence of multiple risk factors is also very high.
Studies have established that African respond lesser to statins compared to Caucasians.
Two (H-2 and H-7) SNP haplotypes are commonly associated with poor response to statins and these haplotypes are highly prevalent in African compared to Caucasians.
Statins: benefits are beyond LDL-C and are dose dependent.
Source :Circulation 2008;117;1537-1544
Early, intensive lipid-lowering treatment with statin, initiated during the acute phase of unstable angina or non–Q-wave MI, reduces early recurrent ischemic events
A benefit was observed in a population with low to normal baseline LDL-C levels.
Source:Schwartz et al JAMA 2001;285:1711-8
Increase peripheral lipolysis and decrease hepatic TG production(by binding to peroxysome proliferators activated receptors alpha in hepatocytes PPAR alpha)
Beneficial effects on lipid parameter:
TG ↓ 25%-50%
LDLc ↓ or remain the same or↑
LDL &HDL ↑ 10%-25% in hypertriglyceridemia
Adverse effects:
GIT up set, cholelithiasis , myositis .
Contraindication: hepatic or renal dysfunction ,gallbladder diseases.
Indication: hypertrigylceridemia(type IV&V)combined hyperlipidemia(type IIb) with low HDLc.
source: medescape.org/ view article/561751
Beneficial effect on lipid parameter:
LDLc ↓ 5%-25%
TG ↓20%-60%
HDL ↑15%-39%
Reduce coronary events
Adverse effect :
Flushing ,itching ,headache
Hepatotoxicity
Activation of peptic ulcer
Hyperglycemia/reduced insulin senetivity
Contraindications:
Active liver disease, peptic ulcer disease
NOTE: Tredaptive(nicotinic acid +laropriprant)2008
Laropriprant(selective antagonist of prostaglandin D2 receptor).
source: medescape.org/ view article/561751
Binding to bile acid and increase excretion of cholesterol
Beneficial effect on lipid parameter:
LDL c↓ 15%-30%
HDL c ↑3%-5%
TG may increase in patient with elevated TG
Reduced coronary events
Adverse effect:
GIT intolerance ,constipation, bloating ,abdominal pain, flatulence
Drug interaction:
Bind negatively to charged drugs, interfere with absorption of drugs/fat soluble vitamins(other drugs 1hr before or 4-6 hrs after)
source: medescape.org/ view article/561751

Reduce cholesterol absorption by
binding to intestinal cholesterol
transporter (inhibit delivery of cholesterol
to liver &increase hepatic LDL receptor)
Beneficial effect on lipid parameter:
LDL c ↓18%-20%(in monotherapy or
“add-on” to statin no change in TG&HDL.
source: medescape.org/ view article/561751
Fish oil:It is rich in omega3 fatty acid ,decrease VLDL
synthesis and little change in LDL and HDL level.
Omega 3 fatty acids protect against CHD mortality particularly sudden death.
Can be used as alternative to fibrate or in combination with statins.
Soluble fibers:Bind to bile acids in the gut and increase
conversion of cholesterol to bile acids in the liver.
source: medescape.org/ view article/561751
source: medescape.org/ view article/561751
CETP:
It transfers cholesterol from HDL to LDL&VLDL ,so it inhibition will result in increase of HDL level and reduce cardiovascular events.
Combination drug therapy:
First monotherapy is used ,then if there is alack of response combination is used.
In general Statins + bile acid sequestrants .
niacin+ bile acid sequesterant.
Both provide great reduction in total &LDL cholesterol.
To increase HDL level gemifebrozil or niacin is used.

drug Dosage forms Usual daily dose Maximum
daily dose
cholestyramine Bulk powder 4g
packet
8g TID 32g
Colestipol
hydrochlorid
Bulk powder 5g
packet
10g BID 30g
colesevelam 625 mg tablet 1,875mg BID 4,375mg
niacin 50,100,250,500mg
tab
125,250,500mg
cap
1,000-2,000 mg
once daily
6g
Extended release
niacin
500,750,1000mg
tab
1000-2000mg
once daily
2000mg
Fenofibrate 67.134,200mg cap
54,160,40,120mg
tab
54mg or 67mg 201mg
gemfibrizol 300mg cap 600mg BID 1.5g
ezetimibe 10mg tab 10mg 10mg
source:pharmacotherapy text book.7th edition

drug Dosage form Usual daily dose Maximum daily
dose
lovastatin 20,40mg tab 20-4-mg 80mg
pravastatin 10,20,40,80mg
tab
10-20mg 40mg
simvastatin 5,10,20,40,80mg
tab
10-20mg 80mg
atorvastatin 10,20,40,80mg
tab
10mg 80mg
rosuvastatin 5,10,20,40 mg
tab
5mg 40mg
pitavastatin 1,2,4mg 2mg 4mg
source:pharmacotherapy textbook. 7th edition
According to the NCEP(national cholesterol education programme &the national institute of health (USA):
The most important step in management of high cholesterol level in the blood is assessing person’s risk status. By 3 steps:
First: detecting fast lipoprotein profile (total cholesterol , LDL c, HDL c ,TG).
Second: identifying any risk determinants.
Third: estimation of 10 years CHD risk according to Framingham scoring.
Major risk determinants:
Cigarette smoking
Hypertension
Low HDL ≤ 40mg\dl
Family history of CHD
Age { men ≥45 yrs women≥55ys}
Note :there are other factors ,but only the major factors modify LDL c goals
Source: Ntional cholesterol education programme.National heart,lung&blood
institute NIH publication No .01-3670 May 2011
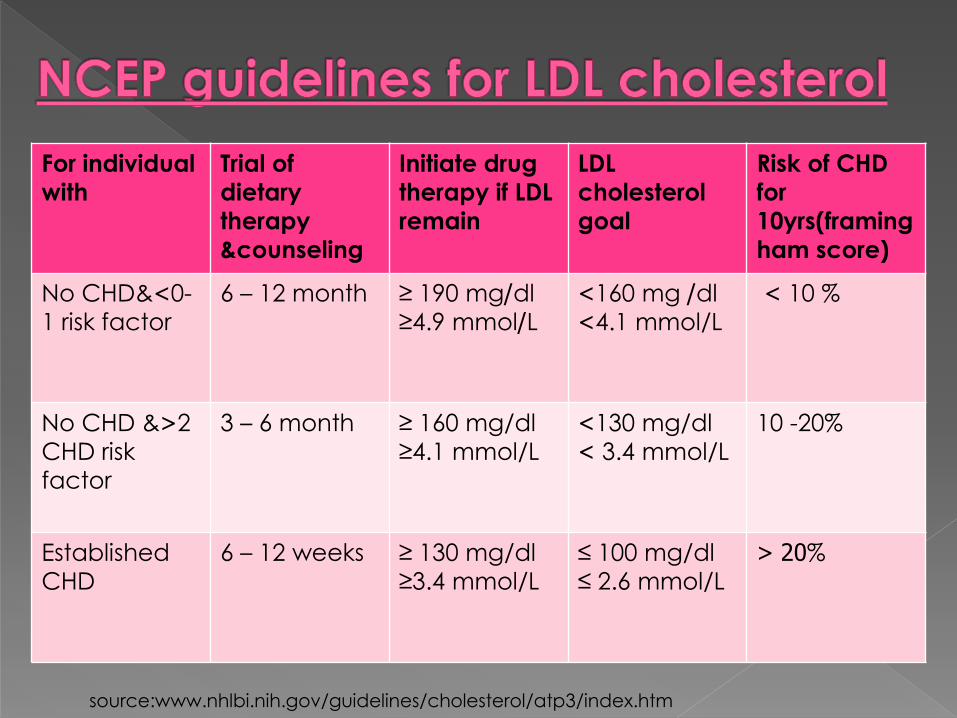
For individual
with
Trial of
dietary
therapy
&counseling
Initiate drug
therapy if LDL
remain
LDL
cholesterol
goal
Risk of CHD
for
10yrs(framing
ham score)
No CHD&>0-
1 risk factor
6 – 12 month ≥ 190 mg/dl
≥4.9 mmol/L>160 mg /dl
>4.1 mmol/L
> 10 %
No CHD &<2
CHD risk
factor
3 – 6 month ≥ 160 mg/dl
≥4.1 mmol/L
>130 mg/dl
> 3.4 mmol/L
10 -20%
Established
CHD
6 – 12 weeks ≥ 130 mg/dl
≥3.4 mmol/L
≤ 100 mg/dl
≤ 2.6 mmol/L
< 20%
source:www.nhlbi.nih.gov/guidelines/cholesterol/atp3/index.htm

source:www.cvtoolbox.com
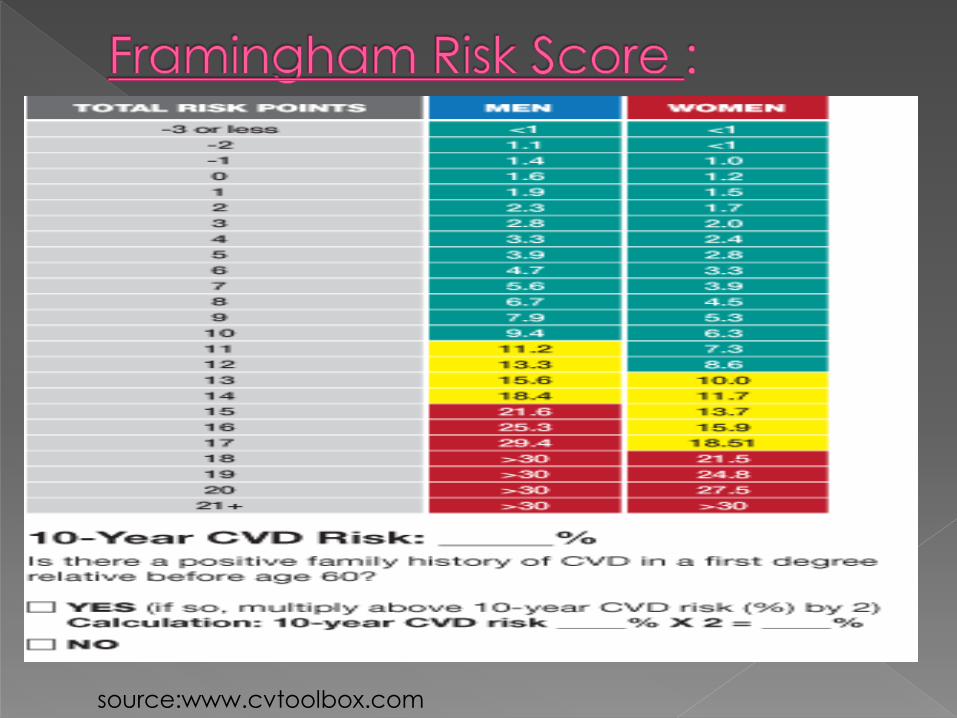
source:www.cvtoolbox.com
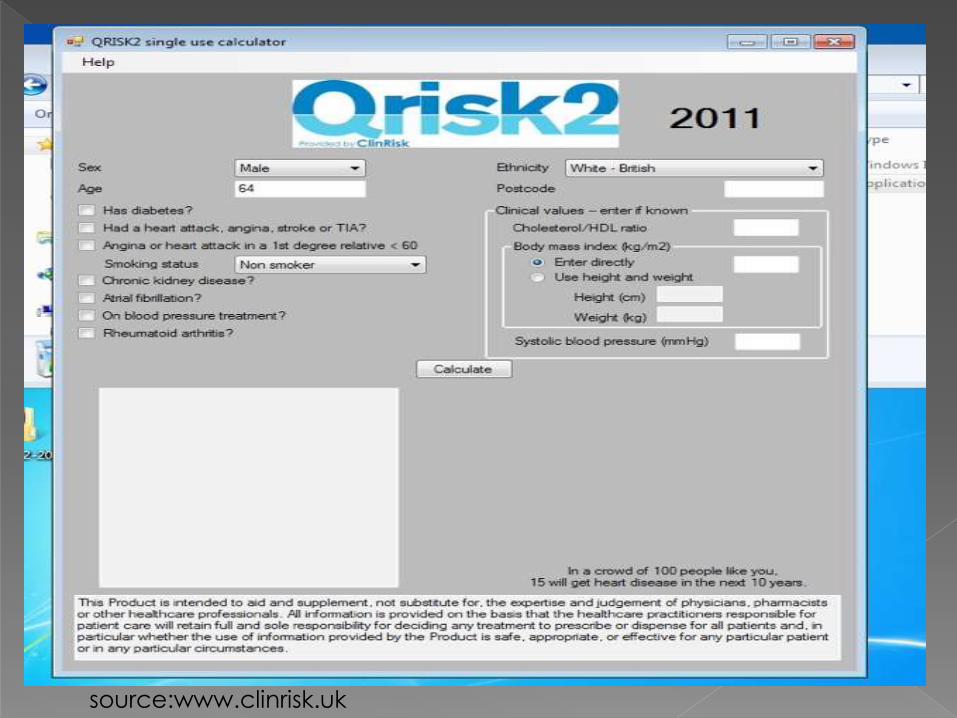
source:www.clinrisk.uk
It constitute due to , life habit risk factors
and emerging factors .
It characteristic by atherogenic
dyslipideamia, abdominal obesity, insulin
resistance and high blood pressure
(DROP syndrome)
Source: Ntional cholesterol education programme.National heart,lung&blood
institute NIH publication No .01-3670 May 2011
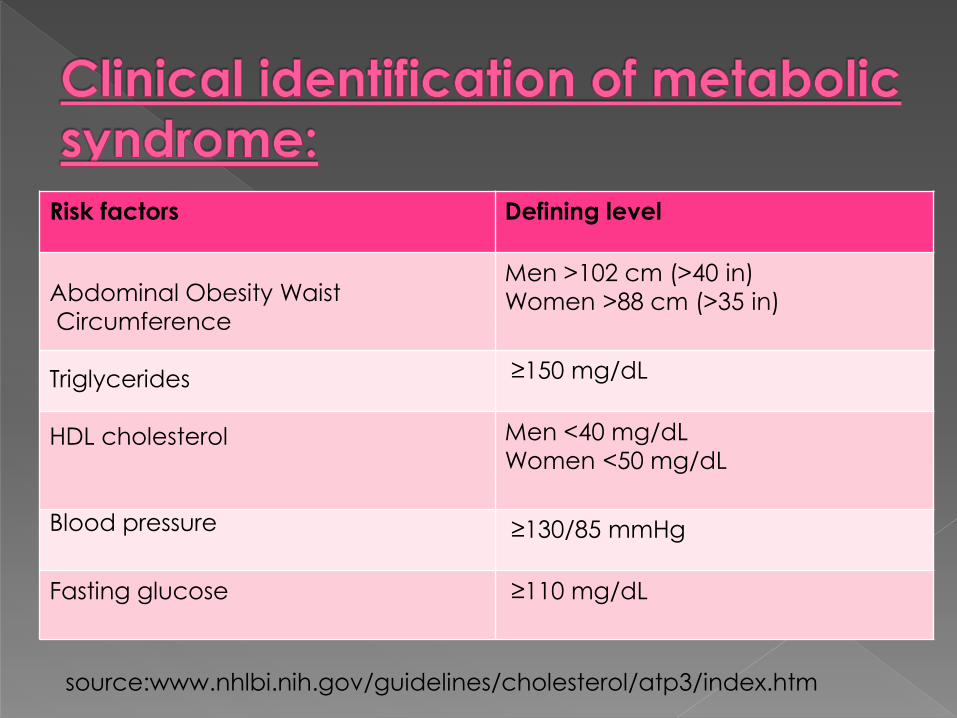
Risk factors Defining level
Men >102 cm (>40 in)
Women >88 cm (>35 in)
≥150 mg/dL
Men <40 mg/dL
Women <50 mg/dL
≥130/85 mmHg
Fasting glucose ≥110 mg/dL
Abdominal Obesity Waist
Circumference
Triglycerides
HDL cholesterol
Blood pressure
source:www.nhlbi.nih.gov/guidelines/cholesterol/atp3/index.htm
Target of therapy :
1\ primary target (LDL cholesterols)
2\ secondary target (metabolic syndrome)
Modalities of therapy:
1\Therapeutic lifestyle change(TLC)
2\Drug therapy
Source: Ntional cholesterol education programme.National heart,lung&blood
institute NIH publication No .01-3670 May 2011

Nutrient Recommended intake
Saturated fat Less than 7% of total
calories
Polyunsaturated fat Up to 10% of total calories
Monounsaturated fat Up to 20% of total calories
Total fat 25-35% of total calories
Carbohydrate 50-60% of total calories
Fiber 20-30 g/day
Protein Approximately 15% of total calories
Cholesterol Less than 200 mg/day
source:www.nhlbi.nih.gov/guidelines/cholesterol/atp3/index.htm
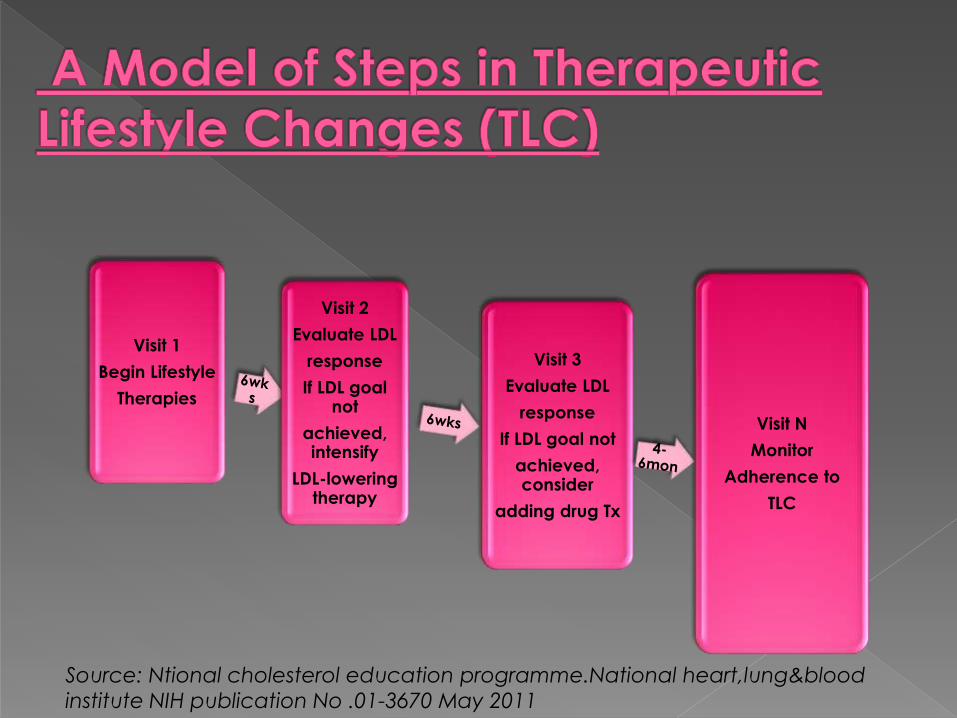
Visit 1
Begin Lifestyle
Therapies
Visit 2
Evaluate LDL
response
If LDL goal not
achieved, intensify
LDL-lowering therapy
Visit 3
Evaluate LDL
response
If LDL goal not
achieved, consider
adding drug Tx
Visit N
Monitor
Adherence to
TLC
Source: Ntional cholesterol education programme.National heart,lung&blood
institute NIH publication No .01-3670 May 2011
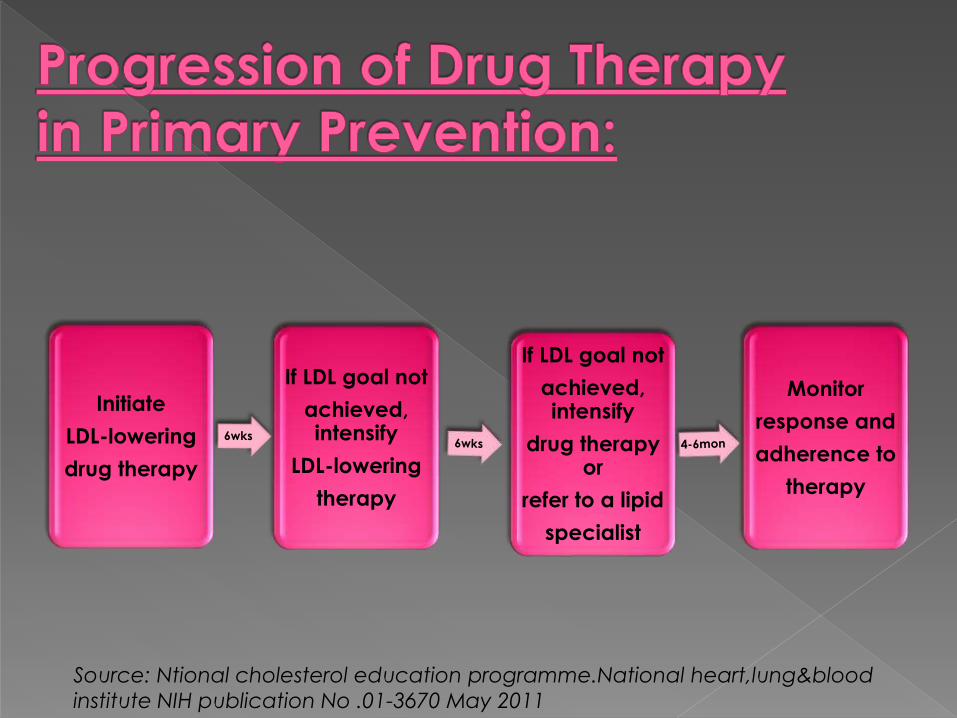
Initiate
LDL-lowering
drug therapy
If LDL goal not
achieved, intensify
LDL-lowering
therapy
If LDL goal not
achieved, intensify
drug therapy or
refer to a lipid
specialist
Monitor
response and
adherence to
therapy
Source: Ntional cholesterol education programme.National heart,lung&blood
institute NIH publication No .01-3670 May 2011

the clinical approach calls for TLC for
primary prevention of CHD .
For higher risk persons , clinical
approach intensifies prevention
strategies . aiming to reduce long tern
risk > 10 years.
Source: Ntional cholesterol education programme.National heart,lung&blood
institute NIH publication No .01-3670 May 2011
The recent clinical trials demonstrate that
LDL lowering therapy reduce (coronary
mortality, major coronary events,
procedures and strokes)
For persons with established CHD or CHD
equivalent ,ATPIII specifies an LDL c <
100 mg/dl as the goal of therapy for
secondary prevention.
Source: Ntional cholesterol education programme.National heart,lung&blood
institute NIH publication No .01-3670 May 2011
pharmacists should always counsel patients on the disease process, and reinforce lifestyle modifications, with added emphasis on the benefits of intervention and compliance.
The most important message pharmacists can relay to patients is that the management of dyslipidemia is not a short- term assignment with immediate, visible outcomes. Rather, it is a long-term process that should be integrated into one’s daily life.
Source: pharmacytimes.com
Implementing clinical pharmacy services in Jordan has improved the lipid profile of dyslipidemic patients, majority of pharmacist recommendation (90.4%) were followed by physician and the overall lipid lowering agent use was increased to (91.8%) in intervention group patient & (86.5%) in control group compared to (69.9%-78.8%) respectively at baseline.
Article: (The role of clinical pharmacist on lipid control in dyslipidemic patients in Jordan)
Source: Int J clin pharm 2011 Ap;33(2):229-236

Interdisciplinary medication team that include clinical pharmacists in lipid lowering management resulted in improved treatment success as measured by reduction in LDL level (5 %-22% per visit)
Article: (Assessment of clinical pharmacist management of lipid lowering therapy in primary care)
Source: J manage care pharm 2003May;9(3):269-273

66