Dynamics of Cytomegalovirus (CMV) Plasma DNAemia in Initial and Recurrent Episodes of Active CMV Infection in the Allogeneic Stem Cell Transplantation Setting: Implications for Designing Preemptive Antiviral Therapy Strategies Beatriz Mu~ noz-Cobo, 1 Carlos Solano, 2,3 Elisa Costa, 1 Dayana Bravo, 1 Mar ıa Angeles Clari, 1 Isabel Benet, 2,3 Mar ıa Jos e Remigia, 2 Juan Montoro, 2 David Navarro 1,4 Preemptive antiviral therapy strategies for active cytomegalovirus (CMV) infection occurring in allogeneic stem cell transplant recipients should be optimized to avoid overtreatment. The current study was aimed at determining whether the analysis of the kinetics of CMV DNA load in plasma may provide useful informa- tion for the therapeutic management of active CMV infection in this setting. A total of 59 consecutive patients were included in the study, of which 40 (67.8%) developed 1 (n 5 21) or more (n 5 19) episodes of CMV DNAemia. The need for antiviral therapy for initial or secondary episodes of CMV DNAemia could not be predicted on the basis of the CMV DNA load value in the first plasma testing positive by polymerase chain reaction (PCR). In contrast, in the absence of antiviral therapy, an increase of $3-fold between the baseline CMV DNA load and that measured a median of 6 days later discriminated between initial episodes eventually requiring antiviral treatment and those resolving spontaneously (sensitivity, 76.4%; specificity, 89.4%; positive predictive value, 86.6%; negative predictive value, 80.9%). This criterion was not useful for identifying recurrent episodes of CMV DNAemia that required antiviral therapy. The CMV doubling time and CMV DNA loads at the time of the first positive PCR and at initiation of preemptive therapy did not differ significantly between episodes that responded immediately to antiviral therapy from those showing a delayed response. The analysis of the dynamics of CMV DNA load in plasma in the absence of antiviral therapy allowed early recognition of episodes of CMV DNAemia that eventually needed to be treated, but did not permit prediction of the kinetics of CMV DNA clearance in response to antiviral therapy. Biol Blood Marrow Transplant 17: 1602-1611 (2011) Ó 2011 American Society for Blood and Marrow Transplantation KEY WORDS: Cytomegalovirus (CMV), CMV DNA load in plasma, Self-resolving episodes of active CMV infection, CMV doubling time, Kinetics of CMV DNA load decline, Preemptive antiviral therapy INTRODUCTION Cytomegalovirus (CMV) infection is a major cause of morbidity and mortality following allogeneic stem cell transplantation (allo-SCT) [1]. Preemptive anti- viral therapy, consisting of the administration of anti- virals upon detection of CMV replication in the blood compartment, has been adopted by most transplant centers as the first-choice strategy for the prevention of CMV end-organ disease [2]. In recent years, most laboratories have switched from the pp65 antigenemia assay to quantitative real-time polymerase chain reaction (PCR) methods for the surveillance of active CMV infection and guidance of preemptive antiviral therapy. In this setting, antiviral treatment is usually initiated when the CMV DNAemia level reaches a certain predetermined threshold (ranging from 1000 to 10,000 copies/mL in whole blood, or from 100 to 10,000 copies/mL of plasma) [2,3]. At some centers, the CMV DNA load cutoff triggering the initiation of antiviral therapy is stratified according to the individual risk of patients for developing From the 1 Microbiology Service Hospital Cl ınico Universitario, Valencia, Spain; 2 Hematology and Medical Oncology Service, Hospital Cl ınico Universitario, Valencia, Spain; 3 Department of Medicine, School of Medicine, University of Valencia, Valen- cia, Spain; and 4 Department of Microbiology, School of Medi- cine, University of Valencia, Valencia, Spain. Financial disclosure: See Acknowledgments on page 1610. Correspondence and reprint requests: David Navarro, MD, PhD, Microbiology Service, Hospital Cl ınico Universitario, and Department of Microbiology, School of Medicine, Av. Blasco Ib a~ nez 17, 46010 Valencia, Spain (e-mail: [email protected]). Received June 27, 2011; accepted August 15, 2011 Ó 2011 American Society for Blood and Marrow Transplantation 1083-8791/$36.00 doi:10.1016/j.bbmt.2011.08.014 1602

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
From theValenHospofMecia Spcine
Financial dCorrespon
MicroDepaIba~ne
Received J 2011 Am1083-8791doi10101
1602
Dynamics of Cytomegalovirus (CMV) Plasma DNAemiain Initial and Recurrent Episodes of Active CMV
Infection in the Allogeneic Stem Cell TransplantationSetting Implications for Designing Preemptive
Antiviral Therapy Strategies
Beatriz Mu~noz-Cobo1 Carlos Solano23 Elisa Costa1 Dayana Bravo1 Marıa Angeles Clari1
Isabel Benet23 Marıa Jose Remigia2 Juan Montoro2 David Navarro14
Preemptive antiviral therapy strategies for active cytomegalovirus (CMV) infection occurring in allogeneicstem cell transplant recipients should be optimized to avoid overtreatment The current study was aimedat determining whether the analysis of the kinetics of CMV DNA load in plasma may provide useful informa-tion for the therapeutic management of active CMV infection in this setting A total of 59 consecutive patientswere included in the study of which 40 (678) developed 1 (n 5 21) or more (n 5 19) episodes ofCMV DNAemia The need for antiviral therapy for initial or secondary episodes of CMV DNAemia couldnot be predicted on the basis of the CMV DNA load value in the first plasma testing positive by polymerasechain reaction (PCR) In contrast in the absence of antiviral therapy an increase of $3-fold between thebaseline CMV DNA load and that measured a median of 6 days later discriminated between initial episodeseventually requiring antiviral treatment and those resolving spontaneously (sensitivity 764 specificity894 positive predictive value 866 negative predictive value 809) This criterion was not useful foridentifying recurrent episodes of CMV DNAemia that required antiviral therapy The CMV doubling timeand CMVDNA loads at the time of the first positive PCR and at initiation of preemptive therapy did not differsignificantly between episodes that responded immediately to antiviral therapy from those showing a delayedresponse The analysis of the dynamics of CMV DNA load in plasma in the absence of antiviral therapyallowed early recognition of episodes of CMV DNAemia that eventually needed to be treated but didnot permit prediction of the kinetics of CMV DNA clearance in response to antiviral therapy
Biol Blood Marrow Transplant 17 1602-1611 (2011) 2011 American Society for Blood and Marrow Transplantation
KEY WORDS Cytomegalovirus (CMV) CMV DNA load in plasma Self-resolving episodes of active CMVinfection CMV doubling time Kinetics of CMV DNA load decline Preemptive antiviral therapy
INTRODUCTION
Cytomegalovirus (CMV) infection is a major causeof morbidity and mortality following allogeneic stem
1Microbiology Service Hospital Clınico Universitariocia Spain 2Hematology and Medical Oncology Serviceital Clınico Universitario Valencia Spain 3Departmentdicine School ofMedicine University of Valencia Valen-ain and 4Department of Microbiology School of Medi-
University of Valencia Valencia Spainisclosure See Acknowledgments on page 1610dence and reprint requests David Navarro MD PhDbiology Service Hospital Clınico Universitario andrtment of Microbiology School of Medicine Av Blascoz 17 46010 Valencia Spain (e-mail davidnavarrouves)une 27 2011 accepted August 15 2011erican Society for Blood and Marrow Transplantation$36006jbbmt201108014
cell transplantation (allo-SCT) [1] Preemptive anti-viral therapy consisting of the administration of anti-virals upon detection of CMV replication in the bloodcompartment has been adopted by most transplantcenters as the first-choice strategy for the preventionof CMV end-organ disease [2] In recent years mostlaboratories have switched from the pp65 antigenemiaassay to quantitative real-time polymerase chainreaction (PCR) methods for the surveillance of activeCMV infection and guidance of preemptive antiviraltherapy In this setting antiviral treatment is usuallyinitiated when the CMV DNAemia level reachesa certain predetermined threshold (ranging from1000 to 10000 copiesmL in whole blood or from100 to 10000 copiesmL of plasma) [23] At somecenters the CMV DNA load cutoff triggering theinitiation of antiviral therapy is stratified accordingto the individual risk of patients for developing
Table 1 Demographic and Clinical Data of the Patients
Parameter No of Patients ()
Patients 59Median age years (range) 49 (16-71)Sex no male patientsno female patients 3920Underlying diseaseAcute myeloid leukemia 24 (406)Non-Hodgkinrsquos lymphoma 16 (271)Acute lymphocytic leukaemia 6 (101)Chronic lymphocytic leukaemia 4 (67)Multiple myeloma 2 (33)Myelodysplastic syndrome 2 (33)Hodgkinrsquos lymphoma 2 (33)Myeloproliferative syndrome 1 (16)Chronic myeloid leukaemia 1 (16)Plasma cell disorders 1 (16)
CMV-serostatusD+R+ 28 (474)D2R+ 22 (372)D+R2 5 (85)D2R2 4 (67)
Donor typeHLA-identical sibling 28 (474)Matched unrelated 20 (339)Mismatched related 2 (34)Mismatched unrelated 9 (153)
Conditioning regimenNonmyeloablative 35 (593)
MelphalanFludarabine 23 (389)BusulfanFludarabine 7 (118)MelphalanFludarabineRituximab 5 (84)
Myeloablative 24 (407)BusulfanCyclophosphamide 11 (186)
Biol Blood Marrow Transplant 171602-1611 2011 1603Kinetics of CMV Plasma DNAemia in Allo-SCT
CMV disease and the time at which CMV DNAemiaoccurs [3] Alternatively preemptive therapy may beinitiated upon a documented increase in CMVDNAe-mia between 2 consecutive determinations [3-5]Although preemptive antiviral therapy regimens havebeen shown to effectively prevent the occurrence ofCMV end-organ disease they probably result in over-treatment [67]
The analysis of the dynamics of CMV replicationduring active CMV infection in allo-SCT recipientshas been shown to be useful for predicting the risk ofCMV end-organ disease and nonrelapse mortality[8-11] the likelihood of the occurrence of recurrentepisodes of active CMV infection and the kinetics ofresponse to antiviral therapy [1213] Neverthelessno practical therapeutic intervention measures havebeen derived from these studies The current studywas aimed at determining whether knowledgeregarding the kinetics of CMV DNA load in plasmamay provide useful information for the therapeuticmanagement of active CMV infection in allo-SCTrecipients In addition the effects of pretransplantand clinical factors on the kinetic pattern of CMVplasmaDNAemia clearance in initial episodes of activeCMV infection and on the incidence of recurrentepisodes in this clinical setting were investigated
BusulfanFludarabineThiotepaAntytimoglobulin 10 (169)BusulfanCyclophosphamideAntytimoglobulin 2 (32)FludarabineBusulfanAntytimoglobulin 1 (16)
Stem cell sourcePeripheral blood 50 (847)Umbilical cord blood 9 (153)
GVHD prophylaxisCyclosporin AMethotrexate 33 (559)Cyclosporin Amycophenolatemofetil 9 (153)Rapamycin + Tacrolimus 10 (169)Cyclosporine APrednisone 3 (51)Others 4 (67)
Acute GVHDGrades 0-I 36 (611)Grades II-IV 23 (389)
D indicates donor R recipient + CMV seropositive2 CMV seroneg-
PATIENTS AND METHODS
Patients
A total of 59 consecutive patients undergoing non-manipulated T cell replete allo-SCT between January2009 and March 2011 at the Hospital Clınico Univer-sitario of Valencia were included in the study Relevantclinical and demographic data of the patients are sum-marized in Table 1 The study was approved by theEthics Committee and all patients gave their informedconsent to participate in the study
ativeAge is given as median (range)
Management of Active CMV Infection
Virologic monitoring of CMV infection was per-formed using the Abbott CMV PCR Kit (producedby Qiagen GmbH Hilde Germany for Abbott Diag-nostics Des Plaines IL) [4] on the m2000RT system(Abbott Molecular Des Plaines IL) In our experi-ence this assay is able to reliably quantify CMVDNA loads 10 copiesmL [14] Nucleic acid extrac-tion was performed with the Abbott mSample prepara-tion system DNA Kit on the m24 SP instrument(Abbott Diagnostics) using 500 mL of plasma Viro-logic monitoring was performed weekly within the first120 days following transplantation and at each sched-uled patient visit thereafter During episodes of activeCMV infection virologic monitoring was scheduled to
be performed twice a week although this was not donefor all patients
Patients with active CMV infection were preemp-tively treated with oral valganciclovir (900 mg12 h)iv ganciclovir (5 mgkg12 h) or foscarnet (iv60 mgkg12 h) upon detection of 500 CMV DNAcopiesmL in the plasma Antiviral therapy was discon-tinued after 2 consecutive negative PCR resultsobtained 3 to 7 days apart All patients with antibodiesagainst herpes simplex virus received acyclovir prophy-laxis as follows recipients of unrelated graftswere treated with iv acyclovir (750 mg8 h) wheneither the patient the donor or both were
1604 Biol Blood Marrow Transplant 171602-1611 2011B Mu~noz-Cobo et al
CMV-seropositive recipients of related grafts andCMV-seronegative patients receiving an unrelatedgraft from a CMV-seronegative donor were treatedwith oral acyclovir (800 mg12 h) Acyclovir was ad-ministered until stable hematopoietic cell engraftmentwas achieved usually around day 130
Definitions
Active CMV infection was diagnosed upon detec-tion of CMV DNA (any level) in 1 or more plasmaspecimens Episodes of active CMV infection withonly 1 specimen testing positive by PCR were consid-ered true episodes if a different aliquot of plasma alsotested positive For data analysis the commencementand end of a given episode of active viral infectionwere defined by the first positive (any level of plasmaviral load) and first negative results respectivelyOnly increases in CMVDNA loads$3 times the base-line levels were considered true increases as these wereabove the intraassay variability of the PCR test(approximately 02 log10 for low CMV DNA values)[3] Recurrent episodes of active CMV infection werethose that occurred at least 15 days after clearance (firstnegative PCR) of the preceding episode CMV end-organ disease was diagnosed and treated as previouslyreported [15]
Analyses of the Kinetics of CMV PlasmaDNAemia
To determine the rate of virus replication the viraldoubling time (dt) of CMV was estimated consideringfor analysis the first 2 PCR positive results in theabsence of antiviral treatment [16] The dt was givenby dt 5 (t2 2 t1) log(2)log(q2q1) with q1 and t1being the CMV DNA load (copiesmL) at the time ofthe first positive PCR (in days) respectively and q2and t2 the CMV DNA load at the time of the secondpositive PCR respectively This formula assumesa constant growth rate which occurs in the early phaseof virus replication CMV dt calculations were per-formed only for episodes in which the increase inCMVDNA load between the first and the second pos-itive PCR determinations was$3-fold The kinetics ofCMV DNA load clearance followed a logarithmicdecay curve in most treated episodes but only in a fewself-resolving episodes (see below) expressed by theequation yt 5 y0e
2kt where y0 is the initial CMVDNA load t is time from initiation of antiviral therapy(for self-resolving episodes t is the duration of theepisode) and k is the decay constant [121718] Anominal value of 9 copiesmL was arbitrarily ascribedfor plasma specimens with undetectable CMV DNAload on the basis of the actual limit of detection ofthe assay CMVDNA load half-life was then calculatedusing the equation ln2k
Statistical Analysis
The data were analyzed with the aid of the statisti-cal package SPSS version 170 (SPSS North ChicagoIL)Comparisonswere carried out using the chi-squaretest for categoric variables and the nonparametricMann-Whitney U-test or the Wilcoxon signed-ranktest for unpaired or paired continuous data respec-tively Two-sided exact P values are reported AP value05 was considered statistically significant
RESULTS
Incidence of CMV Plasma DNAemia during theStudy Period
Forty of 59 patients (678) developed 1 (n 5 21)or more (n 5 19) episodes of CMV DNAemia duringthe study period Three of the latter 19 patients expe-rienced more than 2 episodes (in all 63 episodes weredetected) The patients were followed up for a medianof 220 days (range 10-375 days)
Virologic Features of Initial Episodes of CMVPlasma DNAemia
Initial episodes of CMV plasma DNAemia weredetected at a median of 30 days (range 1-90 days) aftertransplantation Twenty-three out of the 40 episodes(57) resolved spontaneously Of these 19 had 1specimen testing positive by PCR Twelve of theremaining 17 episodes cleared following instaurationof antiviral therapy The median time to the firstCMVDNA positive result was not significantly differ-ent for self-resolving or for treated episodes (P5 930)The CMV DNA load in plasma rapidly declined afterimplementation of antiviral therapy in 5 episodes(type A episodes) whereas in 12 episodes CMVDNA load increased within the next 2 to 3 weeksfollowing the instauration of antiviral therapy andthen progressively declined (type B episodes) Fivetreated episodes (type B) were still active at the timeof the patientrsquos death As shown in Table 2 the dura-tion of CMV DNAemia was significantly shorter forself-resolving episodes than for treated episodes(P 5 001) irrespective of whether the latter weretype A (P 5 022) or type B (P 5 001) episodes Theduration of type B episodes was longer than that oftype A episodes although the difference did not reachstatistical significance (P 5 432)
In most of self-resolving episodes (15 of 19 epi-sodes with 1 positive PCR result) either fluctuatingor rather stable levels of CMV DNA loads (mean dif-ference between samples02 log10 copiesmL) wereobserved until resolution In the remaining 4 episodesCMV DNA load decline did follow an exponentialfunction (Figure 1) The CMV DNA load decay rate(k) in these episodes was lower than for treated
Table 2 Virologic Features of Initial Episodes of Cytomegalovirus (CMV) Plasma DNAemia
Type of Episode(No of Episodes)
Initial VL(CopiesmL)
VL at Treatment(CopiesmL)
Peak VL(CopiesmL)
Duration(Days)
Virus DoublingTime (Days) KdeclineDay21 Half-Life (Days)
Self-resolving (23) 28 (20-135) NA 40 (25-308) 16 (3-48) NA 013 (009-027) 557 (252-743)Treated (17) 70 (25-216) 1216 (523-15244) 3872 (676-66329) 405 (18-130) 218 (104-876) 035 (006-065) 190 (106-1150)Treated Type A (5) 63 (25-133) 1455 (676-1739) 1455 (676-1739) 40 (21-68) 445 (120-876) 037 (018-037) 187 (183-385)Treated Type Bdagger (12) 79 (28-216) 939 (523-15244) 9907 (918-66329) 44 (18-130) 201 (104-310) 014 (006-065) 477 (106-1150)
VL indicates CMV DNA load NA not applicableFigures are given as median numbers (range)Immediate response to antiviral therapydaggerDelayed response to antiviral therapy
Biol Blood Marrow Transplant 171602-1611 2011 1605Kinetics of CMV Plasma DNAemia in Allo-SCT
episodes though statistical significance was notreached (P 5 297) Accordingly the median half-lifeof CMV DNA load was shorter in treated episodesthan in self-resolving episodes (P5 304) The medianvalue of k was higher for type A than for typeB episodes (P 5 422) Thus the median half-life ofCMV DNA load was shorter in type A than in typeB episodes (P 5 287)
Analysis of Early Kinetics of CMV DNAemia forPredicting the Virologic Outcome of InitialEpisodes of Active CMV Infection
The median initial CMV DNA load (first positivePCR) was significantly lower (P 5 001) in self-resolving episodes than in those that were eventuallytreated Type A and type B episodes had comparableinitial CMV DNA viral loads (P 5 62) Despite the
Days0 2 4 6 8 10
Lmseipoc
aimeA
NDVMCgoL
08
10
12
14
16
18
20
Lmseipoc
aimeA
NDVMCgoL
Days
0 2 4 6 8 10 12 14
Lmseipoc
aimeA
NDVMCgoL
08
10
12
14
16
18
20
Figure 1 Initial episodes of active CMV infection that resolved spontaneouexponential decay function Black circles are data points The line of best fit is
above findings a cutoff value for the initial CMVDNA load reliably predicting the subsequent kineticsof CMV DNAemia could not be established becauseof a high degree of overlap
We next sought to determine whether the compar-ison of CMV DNA loads measured at baseline (initialviral load) and shortly thereafter (second positivePCR) a median of 6 days (range 4-8 days) after thefirst positive PCR would allow for discriminatingbetween episodes eventually requiring antiviral treat-ment from those that would resolve without theneed of antiviral therapy No significant variation(3-fold) in the CMV DNA load between measure-ments was observed in 17 of 19 self-resolving episodes(see Figure 2A and B) A significant increase ($3-fold)in CMVDNA load was found in 3 of 5 type A episodesand in 10 of 12 type B episodes (Figure 2C) Thus thesensitivity specificity positive predictive value and
Days0 5 10 15 20 25 30
08
10
12
14
16
18
20
22
24
Days
0 5 10 15 20
Lmseipoc
aimeA
NDVMCgoL
09
10
11
12
13
14
15
16
17
sly in which the kinetics of CMV plasma DNA clearance followed anshown Day 0 represents the day of the first positive PCR result
Days0 10 20 30 40 50
Lmseipoc
aimeA
NDVMCgoL
08
10
12
14
16
18
20
22
24
26
Days0 5 10 15 20 25 30
Lmseipoc
aimeA
NDVMCgoL
08
10
12
14
16
18
20
22
24
Days0 10 20 30 40
Lmseipoc
aimeA
NDVMCgoL
10
15
20
25
30
35
40
45
Figure 2 (A) Kinetics of CMV plasma DNAemia in initial episodes of active CMV infection that resolved spontaneously A $3-fold increase ofCMVDNA load between the values in the first and second PCR positive specimens was documented in only 2 episodes (B) Early kinetics of CMV plasmaDNAemia in initial episodes of active CMV infection that were eventually treated preemptively with antivirals (n5 17) before initiation of therapy (C) In5 of these episodes (white triangles) CMV DNA load rapidly decreased following instauration of antiviral therapy in 5 episodes in the remaining12 episodes a delayed response to therapy was observed (black diamonds) Day 0 represents the day of the first positive PCR result
1606 Biol Blood Marrow Transplant 171602-1611 2011B Mu~noz-Cobo et al
negative predictive value for this criterion to identifyepisodes that required therapeutic intervention were764 894 866 and 809 respectively
As shown in Table 2 the doubling times for CMVin the 2 self-resolving episodes inwhich a significant in-crease in CMV DNA load was documented (277 and318) were slightly lower than for treated episodes (me-dian 218 range 104-876) The CMV doubling timewas higher for typeA than for typeB episodes althoughthe difference did not reach statistical significance (P5160) In addition the median CMV DNA load at thetime of initiation of preemptive therapy was not signif-icantly different between type A and type B episodes(P 5 743)
Effects of Pretransplant and Clinical Factors onthe Kinetic Pattern of First Episodes of CMVDNAemia
As shown in Table 3 nonsignificant tendencies toexperience more frequent episodes of CMVDNAemiarequiring antiviral therapy were observed in patientsreceiving cord blood orHLA-mismatched grafts in pa-tients who had undergone myeloablative conditioningor in those who were treated with MMF or prednisoneas a part of the graft-vs-host disease (GVHD) prophy-laxis regimen CMV D1R1 allo-SCT recipientsdeveloped more frequently self-resolving episodesthan D2R1 or D1R2 patients although the differ-
ence did not reach statistical significance Likewisea trend toward a higher incidence of episodes requiringantiviral therapy was observed in patients with a priordiagnosis of acute grade II-IV GVHD Interestinglyepisodes requiring antiviral therapy for resolutionappeared to occur at a lower frequency in patientstreated with rapamycin as a part of theGVHDprophy-laxis regimen than in those treated with other combi-nations of immunosuppressive drugs
Virologic Features of Recurrent Episodes ofCMV DNAemia
Twelve of 23 patients (521) experiencing an ini-tial self-resolving episode of active CMV infectiondeveloped a recurrent episode of CMV DNAemiawithin the first year after transplantation All of these12 episodes resolved without therapeutic intervention(9 had 1 positive PCR result) The incidence ofrecurrent episodes of CMV DNAemia in patientswho had experienced a treated episode (7 of 17 pa-tients 42) was comparable to the incidence inpatients with prior self-resolving episodes (P 5 905)Nevertheless 3 of these 7 secondary episodes requiredantiviral treatment (2 were type B and 1 was type Aepisodes) In addition recurrent episodes of CMVDNAemia occurred with equal frequencies followingtype A and type B episodes (P 5 10) The virologicfeatures of recurrent episodes of CMV DNAemia are
Table 4 Virologic Features of Recurrent Episodes of CMVPlasma DNAemia
Virologic Parameter
Type of Episode
P ValueSelf-Resolving Treated
Initial VL (copiesmL) 25 (20-63) 35 (28-161) 054Peak VL (copiesmL) 43 (22-477) 1012 (5674-1395) 002Duration (days) 19 (6-67) 34 (26-35) 295Day of first + PCR 96 (54-260) 160 (96-180) 421
VL indicates CMV DNA loadFigures are given as median numbers (range)As determined by the Mann-Whitney U-test A P value 05 was con-sidered statistically significant
Table 3 Effects of Pretransplant and Clinical Factors on theOccurrence of Self-Resolving or Treated Initial Episodes ofCytomegalovirus (CMV) DNAemia
Factor
No of Patients with ActiveCMV Infection ()
P ValueTotal Self-Resolving Treated
CMV-serostatusD+R+ 21 13 (619) 8 (381)D2R+ 16 9 (562) 7 (438)D+R2 3 1 (250) 2 (750) 623
Type of donorand HLA match
Relatedmatched 17 10 (588) 7 (412)Relatedmismatched 2 0 (00) 2 (1000)Unrelatedmatched 13 9 (692) 4 (308)Unrelatedmismatched 8 4 (500) 4 (500) 388
Stem cells sourcePeripheral blood 32 19 (593) 13 (407)Cord blood 8 4 (500) 4 (500) 702
ConditioningMyeloablative 19 10 (526) 9 (474)Nonmyeloablative 21 13 (619) 8 (391) 750
GVHD prophylaxisCSA + MTX 20 14 (650) 6 (350)CSA + MMF 9 4 (444) 5 (556)RapamycinTacrolimus 7 5 (714) 2 (296)CSA + PDN 2 0 (00) 2 (1000) 123
Acute GVHDdaggerGrades 0-I 25 14 (560) 11 (440)Grades II-IV 10 5 (500) 5 (500) 10
D indicates donor R recipient CSA cyclosporine A MTX methotrex-ate MMF mycophenolate mofetil PDN prednisoneFrequency comparisons were carried out using the chi-square test(Fisherrsquos exact test) A P value05was considered statistically significantdaggerOnly those cases in which acute GVHD occurred before detection ofCMV DNAemia were considered for analysis
Biol Blood Marrow Transplant 171602-1611 2011 1607Kinetics of CMV Plasma DNAemia in Allo-SCT
summarized in Table 4 The duration of treatedepisodes was longer than that of self-resolvingepisodes although statistical significance was notreached As for first episodes the initial CMV DNAload in recurrent episodes was significantly higher inself-resolving episodes than in treated episodesalthough again a high degree of overlap was observedNevertheless in contrast to what was observed ininitial episodes variation in CMV DNA load betweenbaseline levels and those measured in the second pos-itive PCR did not allow for discrimination between
Days0 20 40 60
Lmseipoc
aimeA
NDVMCgoL
08
10
12
14
16
18
20
22
24
26
28
Lmseipoc
aimeA
NDVMCgoL
1
1
1
1
2
2
2
2
2
3
3
3
Figure 3 (A) Kinetics of CMV plasma DNAemia in recurrent episodes of aplasma DNAemia in initial episodes of active CMV infection that required preethe day of the first positive PCR result
episodes resolving spontaneously (Figure 3A) andthose requiring antiviral therapy (Figure 3B) In factsignificant variations between measurements wereobserved in none out of 9 self-resolving episodeswith more than 1 positive PCR result and in 1 of 3 ep-isodes eventually treated (Figure 3B) The CMVDNAload decay rate in these episodes was a median of024 day21 (range 016-059 day21) which corre-sponded to a median half-life of 285 days (range117-410 days) The kinetics of CMV DNAemiaclearance for secondary episodes that resolved sponta-neously did not follow an exponential decay function(not shown)
Effects of Pretransplant and Clinical Factorson the Incidence of Recurrent Episodes of CMVDNAemia
A trend toward a more frequent occurrence ofrecurrent episodes of CMV DNAemia was observedin CMV D2R1 patients and in the setting of unre-latedmismatched and umbilical cord blood allo-SCTThe differences however did not reach statisticalsignificance (Table 5)
Kinetics of CMV Plasma DNAemia in Patientswith CMV End-Organ Disease
Two patients developed CMV end-organ disease(enteritis) within the first 100 days after transplantationBoth received unrelatedHLA-matched peripheral
Days0 5 10 15 20
2
4
6
8
0
2
4
6
8
0
2
4
ctive CMV infection that resolved spontaneously (B) Kinetics of CMVmptive antiviral therapy before initiation of treatment Day 0 represents
Table 5 Effects of Pretransplant and Clinical Factors on theIncidence of Recurrent Episodes of Cytomegalovirus (CMV)DNAemia within the Study Period
Factor
Recurrent Episode of CMVDNAemia No of Patients ()
P ValueYes No
CMV-serostatusD+R+ 9 (428) 12 (572)D2R+ 10 (625) 6 (375)D+R2 0 (0) 3 (100) 111
Type of donorand HLA match
Relatedmatched 8 (470) 9 (530)Relatedmismatched 0 (0) 2 (100)Unrelatedmatched 6 (461) 7 (539)Unrelatedmismatched 5 (625) 3 (375) 655
Stem cells sourcePeripheral blood 14 (437) 18 (563)Cord blood 5 (625) 3 (375) 442
ConditioningMyeloablative 10 (526) 9 (474)Nonmyeloablative 9 (428) 12 (572) 752
GVHD prophylaxisCSA + MTX 10 (500) 10 (500)CSA + MMF 5 (555) 4 (455)RapamycinTacrolimus 4 (571) 3 (429)CSA + PDN 0 (0) 2 (100) 123
Acute GVHDdaggerGrades 0-I 14 (560) 11 (440)Grades II-IV 7 (466) 8 (534) 504
D indicates donor R recipient CSA cyclosporine A MTX Methotrex-ate MMF mycophenolate mofetil PDN prednisoneFrequency comparisons were carried out using the chi-square test(Fisherrsquos exact test) A P value05 was considered statistically significantdaggerOnly those cases in which acute GVHD occurred before detection ofCMV DNAemia were considered for analysis
1608 Biol Blood Marrow Transplant 171602-1611 2011B Mu~noz-Cobo et al
blood stemcell graftswere conditionedwith anonmye-loablative regimen (fludarabine plus melphalan) andwere treated with cyclosporine A and methotrexate forprophylaxis of GVHD CMV-serostatus of donorsand recipients were D1R1 in 1 case and D2R1 inthe other Neither of these patients developed acuteGVHD (aGVHD) Both patients had low initialCMVDNAemia levels (91 and 28 copiesmL) A signif-icant increase in CMV DNA load before initiation ofantiviral therapy was observed in 1 of these episodes(dt 5 25 days) Both episodes (type B) were treatedwith iv ganciclovir and had a duration of 102 and87 days respectively The peak of CMV DNAemiawas reached at days 121 (66329 copiesmL) and130 (35431 copiesmL) respectively after the firstpositivePCRresultBothpatientsdevelopedarecurrentepisode of CMV DNAemia
DISCUSSION
In the current study we took advantage of a highlysensitive real-time PCR and a relatively conservativestrategy for initiation of preemptive antiviral therapy(500CMVDNA copiesmL in plasma) to investigate
whether the analysis of the kinetics of CMVDNAemiamay yield useful information for the therapeutic man-agement of active CMV infection in the allo-SCTsetting In our cohort the overall rate of CMV DNA-emia was exceedingly high (almost 70) which wasmost likely related not only to the sensitivity of thePCR assay employed for the surveillance of CMVinfection but also to the high-risk profile of the studygroup In effect almost 50 of patients received anunrelated andor HLA-mismatched graft and 44of CMV-seropositive patients received a graft froma CMV-seronegative donor These pretransplant con-ditions have been consistently associated with a highincidence of active CMV infection in the allo-SCTsetting [2] More than half of the initial episodes ofCMV DNAemia resolved spontaneously The dura-tion of self-resolving episodes of CMV DNAemiawas significantly shorter than that for episodes thatwere eventually treated Yet these episodes lasted fora median of 16 days This finding should encouragestudies aimed at determining the impact of low-levelCMV replication which is permitted when initiationof antiviral treatment is delayed until a certain CMVDNAemia threshold is reached (usually between 500to 1000 CMV DNA copiesmL) on the incidenceand severity of indirect effects linked to CMV [12]
For most self-resolving episodes the kinetics ofCMVplasmaDNA clearance did not follow a logarith-mic decay curve in fact either fluctuating or ratherstable levels of CMV DNA loads were observed untilresolution In agreement with data recently publishedby Buyck et al [12] the Kdecline for CMVDNA load inepisodes that resolved without antiviral therapy waslower than that observed in episodes that requiredantiviral treatment for resolution Accordingly thehalf-life of CMV DNA load was shorter in the formerepisodes Notably whole-blood samples were ana-lyzed in the study by Buyck et al [12] whereas plasmaspecimens were used in the current study
First we asked whether the initial CMV plasmaDNA load value (first positive PCR result) may allowfor discrimination between episodes eventually requir-ing antiviral therapy from those resolving without theneed of antiviral treatment If this were the case theinitiation of preemptive therapy could be anticipatedperhaps leading to a more rapid resolution of theepisode and thereby minimizing the potential deleteri-ous effects of continuous CMV replication Eventhough the median initial CMV DNA load was signif-icantly lower for self-resolving episodes than for thosethat required antiviral therapy for clearance we founda high degree of overlap among values measured inboth groups It is known that the coefficient of varia-tion of PCR assays for CMV DNA loads close to thelimit of detection as were most of the initial valuesin our patients may be as high as 30 [19] In lightof the above observations the data suggested that
Biol Blood Marrow Transplant 171602-1611 2011 1609Kinetics of CMV Plasma DNAemia in Allo-SCT
a threshold value for the initial CMV DNA load reli-ably predicting the subsequent kinetics of CMVDNAemia is unlikely to be established at least whenusing highly sensitive real-time PCR assays such asthe method employed in the current study for moni-toring of active CMV infection In this sense it mustbe noted that initial CMV DNA loads measured inthis study were below the limit of detection of mostcommercially available real-time PCRs [2]
We next sought to determine whether the compar-ison between CMV DNA loads measured at baseline(initial viral load) and shortly thereafter (second posi-tive PCRmdasha median of 6 days after the first positivePCR result)mdashwould allow for identification ofepisodes eventually requiring antiviral treatment Wefound significant increases of CMV DNA load($3-fold) in 76 of episodes eventually requiringantiviral treatment but in 10 of self-resolvingepisodes The use of the above criterion would haveidentified the episodes that eventually required anti-viral treatment with a high sensitivity specificity andpositive and negative predictive values In our cohortthis strategy would have allowed for the anticipationof the initiation of antiviral treatment in only 2 epi-sodes (3 and 7 days) because the second CMV DNA-emia value measured was above the established cutofffor initiation of antiviral therapy nevertheless a largernumber of patients (6 of 13) would have benefited fromthis strategy had a higher CMV DNAemia level(1000 copiesmL) been set as the threshold for the ini-tiation of antiviral therapy as in other transplant cen-ters In light of these findings studies designed todetermine whether anticipation of preemptive therapybased on the above criterion would lead to a reductionin the cumulative dose of antivirals administered or toany clinically significant benefit are warranted Priorstudies have proposed CMV plasma DNA levelincreases of 174 copiesmLday [5] or 266 copies be-tween 2 consecutive determinations drawn a medianof 7 days apart [4] to discriminate between episodesthat required preemptive treatment and those thatdid not These estimations nevertheless were madein the setting of a preemptive strategy consisting ofthe initiation of antiviral therapy upon detection ofany level of pp65 antigenemia In addition Boeckhand Ljungman [3] proposed an increase of $5-foldfor initiation of preemptive therapy in low-riskallo-SCT recipients To our knowledge no data onthe clinical efficacy and safety of such strategies havebeen published
Preemptive antiviral therapy results in most casesin a rapid decline of CMV DNA load (type A episodesin the current study) nevertheless increasing levels ofCMV DNAemia early after the initiation of antiviraltherapy (type B episodes in this study) are occasionallydocumented [20-23] This paradoxical phenomenonhas been related to a lack of prompt expansion of
functional CMV-specific T cells in response to viralreplication [23] The occurrence of episodes witha delayed response to antiviral therapy is associatedwith an increased risk of CMV end-organ disease[12] Thus early recognition of this type of episodewould allow for rapid therapeutic interventionperhaps including the use of adoptive immunotherapyin order to reduce the risk of CMV-related morbidityIn this context Buyck et al [12] found a significantlyhigher mean growth rate and higher baseline viralload at the initiation of therapy in episodes witha delayed response to therapy with respect to thosewith an immediate response to therapy whereas theinitial CMV DNA load appeared to be comparablefor both type of episodes Our data partly agree withthose of Buyck et al [12] In effect the CMV doublingtime was lower in type B than in type A episodesalthough statistical significance was not reached andthe initial CMV DNA load did not differ significantlybetween both types of episodes Nevertheless in con-trast to the data reported in the above study baselineCMV DNA loads at the time of initiation of preemp-tive therapy did not differ significantly between bothtypes of episodes Thus in our experience the analysisof the early kinetics ofCMVDNAemia did not allowusto consistently identify the episodes of active CMVinfection with a delayed response to antiviral therapyDiscrepancies between our data and those of Buycket al [12] may be related to several factors includingthe use of different specimens for CMV DNA quanti-fication the use of distinct CMV DNA thresholds fortriggering the initiation of preemptive therapy andthe extensive use of Campath-1H in their study
Recurrent episodes of active CMV infectionoccurred with a comparable frequency among patientswho had an initial self-resolving episode and those whodeveloped an initial preemptively treated episodeNevertheless the likelihood of experiencing a second-ary episode that required antiviral therapy was higherin patients who had developed a treated episode thanin those who had experienced a self-resolving episodeIn agreement with a previous study [12] the risk ofrecurrence was not associated with the rate of CMVDNA decline in primary treated episodes followinginitiation of therapy As for initial episodes the base-line CMV DNA load in secondary episodes did notallow for a prediction of the subsequent kinetics ofCMV DNAemia Nevertheless in contrast to initialepisodes variation in CMV DNA load between base-line levels and those measured in the second positivePCR did not allow for discrimination between epi-sodes resolving spontaneously and those requiringantiviral therapy As ultimate control of CMV replica-tion depends upon adequate expansion of functionalCMV-specific T cells [2324] the above findinglikely reflected a more efficient and prompt T cellresponse in secondary episodes
1610 Biol Blood Marrow Transplant 171602-1611 2011B Mu~noz-Cobo et al
We were interested in assessing the impact ofseveral pretransplant and posttransplant clinical factorson the kinetics ofCMVDNAemia during first episodesof activeCMV infection and the incidence of recurrentepisodes Although we found no significant associa-tions a trend toward a higher frequency of episodesthat required antiviral therapy was observed in CMVD2R1 recipients in patients who received umbilicalcord blood or HLA-mismatched grafts in those whoreceived mycophenolate mofetil or prednisone(1 mgkgday) as a part of the GVHD prophylaxisregimen and in patients who were treated with highdoses of corticosteroids (1 mgkgday) for grades IIto IV GVHD These findings were not unexpected asall the above conditions have been shown to be associ-ated with delayed CMV-specific immune recovery[25-30] In this context it has previously been shownthat the magnitude and promptness of the expansionof functional CMV-specific CD81 and CD41 T cellsin response to CMV replication critically determinethe kinetics of CMV DNAemia clearance [23] Inter-estingly the use of rapamycin for the prevention ofGVHD was clearly associated with a relatively lowincidence of episodes that required antiviral treatmentThe scarce number of patients treated with this drug inour cohort did not allow to draw definitive conclusionson this issue nevertheless this effect has been previ-ously documented in the solid organ transplantationsetting [31] and is likely because of a direct inhibitoryeffect of rapamycin on viral replication [32]
Delayed recovery of CMV-specific T immunityhas been shown to be a significant risk factor for thedevelopment of recurrent episodes of active CMVinfection in allo-SCT recipients [3033] In supportof this view we found that CMV D2R1 recipientsand patients who underwent unrelatedmismatchedor umbilical cord blood allo-SCT tended to experi-ence recurrent episodes of active CMV infectionwith higher frequencies As mentioned above all thesepretransplant and clinical conditions have been previ-ously documented to be associated with an impairmentof CMV-specific T cell recovery
The incidence of CMV end-organ disease in ourcohort was 33 (2 patients) which is in accordanceto data previously published by our group [4] Unfor-tunately neither the analysis of the early kinetics ofCMV plasma DNAemia in the absence of antiviraltherapy nor the assessment of the dynamics of CMVplasma DNA load following the instauration of anti-viral treatment in these 2 episodes allowed for the an-ticipation of the development of CMV end-organdisease Obviously no definitive conclusions can bedrawn from these data given the limited number ofcases subjected to analysis
This study has 2 main limitations First thenumber of patients included in the cohort may havebeen insufficient to assess precisely the impact of
pretransplant and clinical factors on the kinetics ofCMVDNAemia Second there might be certain inac-curacies in the CMV DNAemia kinetics calculationsbecause of insufficient frequency of sampling In thisrespect there is no consensus as to what should bethe frequency of CMV DNA load monitoring duringepisodes of active CMV infection in the allo-SCT set-ting our data seemed to support the idea that theschedule of once-a-week monitoring is probably safeas long as a highly sensitive PCR is used for the surveil-lance of CMV infection Nevertheless it may also bereasonable to implement the twice-a-week schedulefor high-risk patients such as those receiving an unre-lated or HLA-mismatched graft (including recipientsof umbilical cord blood transplants) in whom the dou-bling time of CMV during the episodes of viral repli-cation is clearly faster
In summary in the current study we further char-acterized the dynamics of CMV DNAemia duringinitial and recurrent episodes of active CMV infectionin the allo-SCT setting The data reported hereinshould be taken into consideration for the design ofpreemptive antiviral therapy strategies based on viro-logic monitoring
ACKNOWLEDGMENTS
We thank Julia Garcıa and Monica Reig for theirtechnical assistance
Financial disclosureThis research was supported bya grant (091117) from FIS (Fondo de InvestigacionesSanitarias Ministerio de Sanidad y Consumo Spain)
AUTHORrsquoS CONTRIBUTIONS
BM-C ECMAC andDB did PCR analysesand assisted in the analysis of the data CS IBMJR and JM analyzed the data and attended thepatients DN designed the study analyzed the dataand wrote the paper
REFERENCES
1 Ljungman P CMV infections after hematopoietic stem celltransplantation Bone Marrow Transplant 200842S70-S72
2 Solano C Navarro D Clinical virology of cytomegalovirusinfection following hematopoietic transplantation Future Virol20105111-124
3 Boeckh M Ljungman P How we treat cytomegalovirus inhematopoietic cell transplant recipients Blood 20091135711-5719
4 Gimeno C Solano C Latorre JC et al Quantification of DNAin plasma by an automated real-time PCR assay (cytomegalovi-rus PCR kit) for surveillance of active cytomegalovirus infectionand guidance of preemptive therapy for allogeneic hematopoi-etic stem cell transplant recipients J Clin Microbiol 2008463311-3318
5 Halfon P Berger P Khiri H et al Algorithm based on CMVkinetics DNA viral load for preemptive therapy initiation after
Biol Blood Marrow Transplant 171602-1611 2011 1611Kinetics of CMV Plasma DNAemia in Allo-SCT
hematopoietic cell transplantation J Med Virol 201183490-495
6 Ljungman PWouldmonitoring CMV immune responses allowimproved control of CMV in stem cell transplant patients J ClinVirol 200635493-495
7 Avetisyan G Aschan J Heuroagglund H Ringden O Ljungman PEvaluation of intervention strategy based on CMV-specificimmune responses after allogeneic SCT Bone Marrow Trans-plant 200740865-869
8 GorD Sabin C PrenticeHG et al Longitudinal fluctuations incytomegalovirus load in bone marrow transplant patients rela-tionship between peak virus load donorrecipient serostatusacute GVHD and CMV disease Bone Marrow Transplant199821597-605
9 Emery VC Sabin CA Cope AV Gor D Hassan-Walker AFGriffiths PD Application of viral-load kinetics to identifypatients who develop cytomegalovirus disease after transplanta-tion Lancet 20003552032-2036
10 Avetisyan G Larsson K Aschan J Nilsson C Hassan MLjungman P Impact on the cytomegalovirus (CMV) viral load byCMV-specific T-cell immunity in recipients of allogeneic stemcell transplantation Bone Marrow Transplant 200638687-692
11 Stachel D Kirby K Corey L Boeckh M Viral load as predictorfor transplant-related mortality in the era of pre-emptive ther-apy Bone Marrow Transplant 200841S46
12 Buyck HC Griffiths PD Emery VC Human cytomegalovirus(HCMV) replication kinetics in stem cell transplant recipientsfollowing anti-HCMV therapy J Clin Virol 20104932-36
13 Torre-Cisneros J Caston-Osorio JJ Martın C et al Impact ofinitial cytomegalovirus viral load on efficacy of preemptive ther-apy with ganciclovir in allogeneic stem cell transplant recipientsEnferm Infecc Microbiol Clin 2010286-12
14 Chilet M Aguilar G Benet I et al Virological and immunolog-ical features of active cytomegalovirus infection in nonimmuno-suppressed patients in a surgical and trauma intensive care unitJ Med Virol 2010821384-1391
15 Ljungman P Griffiths P Paya C Definitions of HCMV infec-tion and disease in transplant recipients Clin Infect Dis 2002341094-1097
16 TormoN Solano C de la Camara R et al An assessment of theeffect of human herpesvirus-6 replication on active cytomegalo-virus infection after allogeneic stem cell transplantation BiolBlood Marrow Transplant 201016653-661
17 Emery VC Cope AV Bowen EF Gor D Griffiths PD The dy-namics of human cytomegalovirus replication in vivo J ExpMed1999190177-182
18 Humar A Kumar D Boivin G Caliendo AM Cytomegalovirus(CMV) virus load kinetics to predict recurrent disease in solid-organ transplant patients with CMV disease J Infect Dis 2002186829-833
19 BoeckhMHuangM Ferrenberg J et al Optimization of quan-titative detection of cytomegalovirus DNA in plasma by real-time PCR J Clin Microbiol 2004421142-1148
20 BoeckhM Gooley TA MyersonD CunninghamT Schoch GBowden RA Cytomegalovirus pp65 antigenemia-guided earlytreatment with ganciclovir versus ganciclovir at engraftment af-ter allogeneic marrow transplantation a randomized double-blind study Blood 1996884063-4071
21 Nichols WG Corey L Gooley T et al Rising pp65 antigene-mia during preemptive anticytomegalovirus therapy afterallogeneic hematopoietic stem cell transplantation risk factorscorrelation with DNA load and outcomes Blood 200197867-874
22 Gerna G Lilleri D Zecca M et al Rising antigenemia levelsmay be misleading in pre-emptive therapy of human cytomega-lovirus infection in allogeneic hematopoietic stem cell transplantrecipients Haematologica 200590526-533
23 TormoN Solano C Benet I et al Lack of prompt expansion ofcytomegalovirus pp65 and IE-1-specific IFNgamma CD81 andCD41 T cells is associated with rising levels of pp65 antigene-mia and DNAemia during pre-emptive therapy in allogeneichematopoietic stem cell transplant recipients Bone MarrowTransplant 201045543-549
24 Tormo N Solano C Benet I et al Kinetics of cytomegalovirus(CMV) pp65 and IE-1-specific IFNgamma CD81 and CD41T cells during episodes of viral DNAemia in allogeneic stemcell transplant recipients potential implications for the manage-ment of active CMV infection J Med Virol 2010821208-1215
25 FosterAEGottliebDJ SartorMHertzbergMS BradstockKFCytomegalovirus-specific CD41 and CD81 T-cells followa similar reconstitution pattern after allogeneic stem cell trans-plantation Biol Blood Marrow Transplant 20028501-511
26 Hakki M Riddell SR Storek J et al Immune reconstitution tocytomegalovirus after allogeneic stem cell transplantationimpact of host factors drug therapy and subclinical reactivationBlood 20031023060-3067
27 Lilleri D Fornara C Chiesa A Caldera D Alessandrino EPGerna G Human cytomegalovirus-specific CD41 and CD81T-cell reconstitution in adult allogeneic hematopoietic stemcell transplant recipients and immune control of viral infectionHaematologica 200893248-256
28 Pourgheysari B Piper KP McLarnon A et al Early reconstitu-tion of effector memory CD41 CMV-specific T cells protectsagainst CMV reactivation following allogeneic SCT BoneMarrow Transplant 200943853-861
29 Zhou W Longmate J Lacey SF et al Impact of donor CMVstatus on viral infection and reconstitution of multifunctionCMV-specific T cells in CMV-positive transplant recipientsBlood 20091136465-6476
30 TormoN SolanoC Benet I et al Reconstitution of CMVpp65and IE-1-specific IFN-gCD8(1) and CD4(1) T-cell responsesaffording protection fromCMVDNAemia following allogeneichematopoietic SCT Bone Marrow Transplant 2011 Jan 17[Epub ahead of print]
31 San Juan R Aguado JM Lumbreras C et al Impact of currenttransplantation management on the development of cytomega-lovirus disease after renal transplantation Clin Infect Dis 200847875-882
32 Moorman NJ Shenk T Rapamycin-resistant mTORC1 kinaseactivity is required for herpesvirus replication J Virol 2010845260-5269
33 Gratama JW Boeckh M Nakamura R et al Immune monitor-ing with iTAg MHC Tetramers for prediction of recurrent orpersistent cytomegalovirus infection or disease in allogeneichematopoietic stem cell transplant recipients a prospectivemulticenter study Blood 20101161655-1662
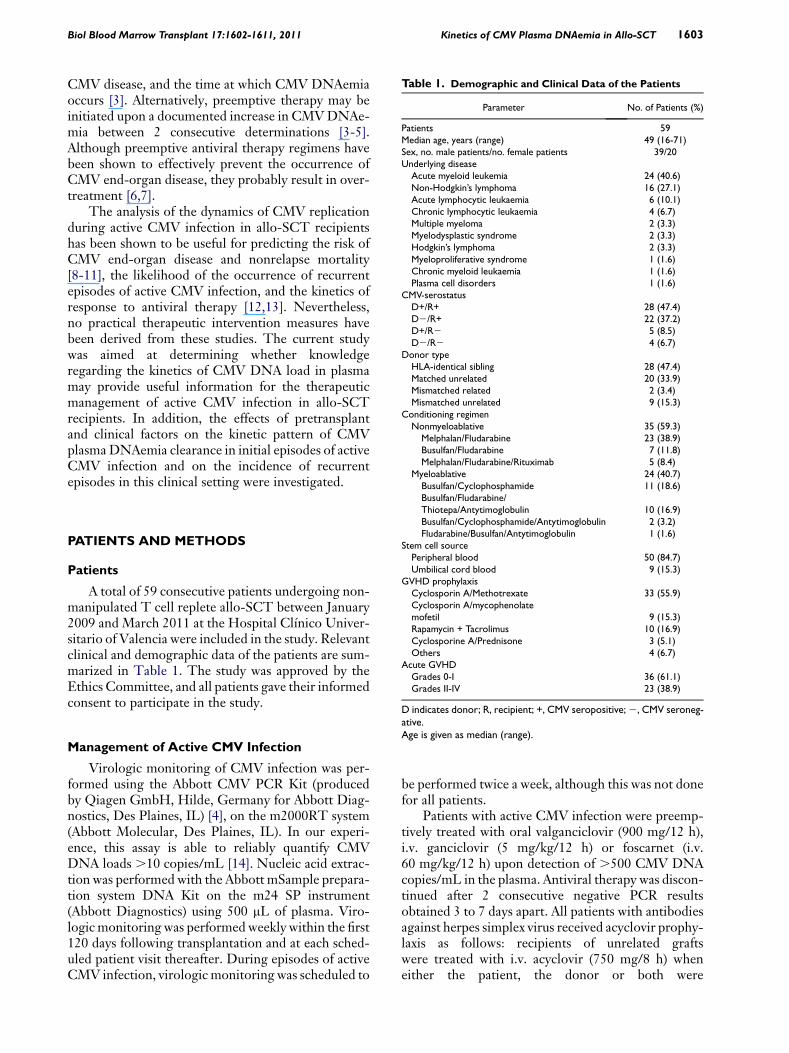
Table 1 Demographic and Clinical Data of the Patients
Parameter No of Patients ()
Patients 59Median age years (range) 49 (16-71)Sex no male patientsno female patients 3920Underlying diseaseAcute myeloid leukemia 24 (406)Non-Hodgkinrsquos lymphoma 16 (271)Acute lymphocytic leukaemia 6 (101)Chronic lymphocytic leukaemia 4 (67)Multiple myeloma 2 (33)Myelodysplastic syndrome 2 (33)Hodgkinrsquos lymphoma 2 (33)Myeloproliferative syndrome 1 (16)Chronic myeloid leukaemia 1 (16)Plasma cell disorders 1 (16)
CMV-serostatusD+R+ 28 (474)D2R+ 22 (372)D+R2 5 (85)D2R2 4 (67)
Donor typeHLA-identical sibling 28 (474)Matched unrelated 20 (339)Mismatched related 2 (34)Mismatched unrelated 9 (153)
Conditioning regimenNonmyeloablative 35 (593)
MelphalanFludarabine 23 (389)BusulfanFludarabine 7 (118)MelphalanFludarabineRituximab 5 (84)
Myeloablative 24 (407)BusulfanCyclophosphamide 11 (186)
Biol Blood Marrow Transplant 171602-1611 2011 1603Kinetics of CMV Plasma DNAemia in Allo-SCT
CMV disease and the time at which CMV DNAemiaoccurs [3] Alternatively preemptive therapy may beinitiated upon a documented increase in CMVDNAe-mia between 2 consecutive determinations [3-5]Although preemptive antiviral therapy regimens havebeen shown to effectively prevent the occurrence ofCMV end-organ disease they probably result in over-treatment [67]
The analysis of the dynamics of CMV replicationduring active CMV infection in allo-SCT recipientshas been shown to be useful for predicting the risk ofCMV end-organ disease and nonrelapse mortality[8-11] the likelihood of the occurrence of recurrentepisodes of active CMV infection and the kinetics ofresponse to antiviral therapy [1213] Neverthelessno practical therapeutic intervention measures havebeen derived from these studies The current studywas aimed at determining whether knowledgeregarding the kinetics of CMV DNA load in plasmamay provide useful information for the therapeuticmanagement of active CMV infection in allo-SCTrecipients In addition the effects of pretransplantand clinical factors on the kinetic pattern of CMVplasmaDNAemia clearance in initial episodes of activeCMV infection and on the incidence of recurrentepisodes in this clinical setting were investigated
BusulfanFludarabineThiotepaAntytimoglobulin 10 (169)BusulfanCyclophosphamideAntytimoglobulin 2 (32)FludarabineBusulfanAntytimoglobulin 1 (16)
Stem cell sourcePeripheral blood 50 (847)Umbilical cord blood 9 (153)
GVHD prophylaxisCyclosporin AMethotrexate 33 (559)Cyclosporin Amycophenolatemofetil 9 (153)Rapamycin + Tacrolimus 10 (169)Cyclosporine APrednisone 3 (51)Others 4 (67)
Acute GVHDGrades 0-I 36 (611)Grades II-IV 23 (389)
D indicates donor R recipient + CMV seropositive2 CMV seroneg-
PATIENTS AND METHODS
Patients
A total of 59 consecutive patients undergoing non-manipulated T cell replete allo-SCT between January2009 and March 2011 at the Hospital Clınico Univer-sitario of Valencia were included in the study Relevantclinical and demographic data of the patients are sum-marized in Table 1 The study was approved by theEthics Committee and all patients gave their informedconsent to participate in the study
ativeAge is given as median (range)
Management of Active CMV Infection
Virologic monitoring of CMV infection was per-formed using the Abbott CMV PCR Kit (producedby Qiagen GmbH Hilde Germany for Abbott Diag-nostics Des Plaines IL) [4] on the m2000RT system(Abbott Molecular Des Plaines IL) In our experi-ence this assay is able to reliably quantify CMVDNA loads 10 copiesmL [14] Nucleic acid extrac-tion was performed with the Abbott mSample prepara-tion system DNA Kit on the m24 SP instrument(Abbott Diagnostics) using 500 mL of plasma Viro-logic monitoring was performed weekly within the first120 days following transplantation and at each sched-uled patient visit thereafter During episodes of activeCMV infection virologic monitoring was scheduled to
be performed twice a week although this was not donefor all patients
Patients with active CMV infection were preemp-tively treated with oral valganciclovir (900 mg12 h)iv ganciclovir (5 mgkg12 h) or foscarnet (iv60 mgkg12 h) upon detection of 500 CMV DNAcopiesmL in the plasma Antiviral therapy was discon-tinued after 2 consecutive negative PCR resultsobtained 3 to 7 days apart All patients with antibodiesagainst herpes simplex virus received acyclovir prophy-laxis as follows recipients of unrelated graftswere treated with iv acyclovir (750 mg8 h) wheneither the patient the donor or both were
1604 Biol Blood Marrow Transplant 171602-1611 2011B Mu~noz-Cobo et al
CMV-seropositive recipients of related grafts andCMV-seronegative patients receiving an unrelatedgraft from a CMV-seronegative donor were treatedwith oral acyclovir (800 mg12 h) Acyclovir was ad-ministered until stable hematopoietic cell engraftmentwas achieved usually around day 130
Definitions
Active CMV infection was diagnosed upon detec-tion of CMV DNA (any level) in 1 or more plasmaspecimens Episodes of active CMV infection withonly 1 specimen testing positive by PCR were consid-ered true episodes if a different aliquot of plasma alsotested positive For data analysis the commencementand end of a given episode of active viral infectionwere defined by the first positive (any level of plasmaviral load) and first negative results respectivelyOnly increases in CMVDNA loads$3 times the base-line levels were considered true increases as these wereabove the intraassay variability of the PCR test(approximately 02 log10 for low CMV DNA values)[3] Recurrent episodes of active CMV infection werethose that occurred at least 15 days after clearance (firstnegative PCR) of the preceding episode CMV end-organ disease was diagnosed and treated as previouslyreported [15]
Analyses of the Kinetics of CMV PlasmaDNAemia
To determine the rate of virus replication the viraldoubling time (dt) of CMV was estimated consideringfor analysis the first 2 PCR positive results in theabsence of antiviral treatment [16] The dt was givenby dt 5 (t2 2 t1) log(2)log(q2q1) with q1 and t1being the CMV DNA load (copiesmL) at the time ofthe first positive PCR (in days) respectively and q2and t2 the CMV DNA load at the time of the secondpositive PCR respectively This formula assumesa constant growth rate which occurs in the early phaseof virus replication CMV dt calculations were per-formed only for episodes in which the increase inCMVDNA load between the first and the second pos-itive PCR determinations was$3-fold The kinetics ofCMV DNA load clearance followed a logarithmicdecay curve in most treated episodes but only in a fewself-resolving episodes (see below) expressed by theequation yt 5 y0e
2kt where y0 is the initial CMVDNA load t is time from initiation of antiviral therapy(for self-resolving episodes t is the duration of theepisode) and k is the decay constant [121718] Anominal value of 9 copiesmL was arbitrarily ascribedfor plasma specimens with undetectable CMV DNAload on the basis of the actual limit of detection ofthe assay CMVDNA load half-life was then calculatedusing the equation ln2k
Statistical Analysis
The data were analyzed with the aid of the statisti-cal package SPSS version 170 (SPSS North ChicagoIL)Comparisonswere carried out using the chi-squaretest for categoric variables and the nonparametricMann-Whitney U-test or the Wilcoxon signed-ranktest for unpaired or paired continuous data respec-tively Two-sided exact P values are reported AP value05 was considered statistically significant
RESULTS
Incidence of CMV Plasma DNAemia during theStudy Period
Forty of 59 patients (678) developed 1 (n 5 21)or more (n 5 19) episodes of CMV DNAemia duringthe study period Three of the latter 19 patients expe-rienced more than 2 episodes (in all 63 episodes weredetected) The patients were followed up for a medianof 220 days (range 10-375 days)
Virologic Features of Initial Episodes of CMVPlasma DNAemia
Initial episodes of CMV plasma DNAemia weredetected at a median of 30 days (range 1-90 days) aftertransplantation Twenty-three out of the 40 episodes(57) resolved spontaneously Of these 19 had 1specimen testing positive by PCR Twelve of theremaining 17 episodes cleared following instaurationof antiviral therapy The median time to the firstCMVDNA positive result was not significantly differ-ent for self-resolving or for treated episodes (P5 930)The CMV DNA load in plasma rapidly declined afterimplementation of antiviral therapy in 5 episodes(type A episodes) whereas in 12 episodes CMVDNA load increased within the next 2 to 3 weeksfollowing the instauration of antiviral therapy andthen progressively declined (type B episodes) Fivetreated episodes (type B) were still active at the timeof the patientrsquos death As shown in Table 2 the dura-tion of CMV DNAemia was significantly shorter forself-resolving episodes than for treated episodes(P 5 001) irrespective of whether the latter weretype A (P 5 022) or type B (P 5 001) episodes Theduration of type B episodes was longer than that oftype A episodes although the difference did not reachstatistical significance (P 5 432)
In most of self-resolving episodes (15 of 19 epi-sodes with 1 positive PCR result) either fluctuatingor rather stable levels of CMV DNA loads (mean dif-ference between samples02 log10 copiesmL) wereobserved until resolution In the remaining 4 episodesCMV DNA load decline did follow an exponentialfunction (Figure 1) The CMV DNA load decay rate(k) in these episodes was lower than for treated
Table 2 Virologic Features of Initial Episodes of Cytomegalovirus (CMV) Plasma DNAemia
Type of Episode(No of Episodes)
Initial VL(CopiesmL)
VL at Treatment(CopiesmL)
Peak VL(CopiesmL)
Duration(Days)
Virus DoublingTime (Days) KdeclineDay21 Half-Life (Days)
Self-resolving (23) 28 (20-135) NA 40 (25-308) 16 (3-48) NA 013 (009-027) 557 (252-743)Treated (17) 70 (25-216) 1216 (523-15244) 3872 (676-66329) 405 (18-130) 218 (104-876) 035 (006-065) 190 (106-1150)Treated Type A (5) 63 (25-133) 1455 (676-1739) 1455 (676-1739) 40 (21-68) 445 (120-876) 037 (018-037) 187 (183-385)Treated Type Bdagger (12) 79 (28-216) 939 (523-15244) 9907 (918-66329) 44 (18-130) 201 (104-310) 014 (006-065) 477 (106-1150)
VL indicates CMV DNA load NA not applicableFigures are given as median numbers (range)Immediate response to antiviral therapydaggerDelayed response to antiviral therapy
Biol Blood Marrow Transplant 171602-1611 2011 1605Kinetics of CMV Plasma DNAemia in Allo-SCT
episodes though statistical significance was notreached (P 5 297) Accordingly the median half-lifeof CMV DNA load was shorter in treated episodesthan in self-resolving episodes (P5 304) The medianvalue of k was higher for type A than for typeB episodes (P 5 422) Thus the median half-life ofCMV DNA load was shorter in type A than in typeB episodes (P 5 287)
Analysis of Early Kinetics of CMV DNAemia forPredicting the Virologic Outcome of InitialEpisodes of Active CMV Infection
The median initial CMV DNA load (first positivePCR) was significantly lower (P 5 001) in self-resolving episodes than in those that were eventuallytreated Type A and type B episodes had comparableinitial CMV DNA viral loads (P 5 62) Despite the
Days0 2 4 6 8 10
Lmseipoc
aimeA
NDVMCgoL
08
10
12
14
16
18
20
Lmseipoc
aimeA
NDVMCgoL
Days
0 2 4 6 8 10 12 14
Lmseipoc
aimeA
NDVMCgoL
08
10
12
14
16
18
20
Figure 1 Initial episodes of active CMV infection that resolved spontaneouexponential decay function Black circles are data points The line of best fit is
above findings a cutoff value for the initial CMVDNA load reliably predicting the subsequent kineticsof CMV DNAemia could not be established becauseof a high degree of overlap
We next sought to determine whether the compar-ison of CMV DNA loads measured at baseline (initialviral load) and shortly thereafter (second positivePCR) a median of 6 days (range 4-8 days) after thefirst positive PCR would allow for discriminatingbetween episodes eventually requiring antiviral treat-ment from those that would resolve without theneed of antiviral therapy No significant variation(3-fold) in the CMV DNA load between measure-ments was observed in 17 of 19 self-resolving episodes(see Figure 2A and B) A significant increase ($3-fold)in CMVDNA load was found in 3 of 5 type A episodesand in 10 of 12 type B episodes (Figure 2C) Thus thesensitivity specificity positive predictive value and
Days0 5 10 15 20 25 30
08
10
12
14
16
18
20
22
24
Days
0 5 10 15 20
Lmseipoc
aimeA
NDVMCgoL
09
10
11
12
13
14
15
16
17
sly in which the kinetics of CMV plasma DNA clearance followed anshown Day 0 represents the day of the first positive PCR result
Days0 10 20 30 40 50
Lmseipoc
aimeA
NDVMCgoL
08
10
12
14
16
18
20
22
24
26
Days0 5 10 15 20 25 30
Lmseipoc
aimeA
NDVMCgoL
08
10
12
14
16
18
20
22
24
Days0 10 20 30 40
Lmseipoc
aimeA
NDVMCgoL
10
15
20
25
30
35
40
45
Figure 2 (A) Kinetics of CMV plasma DNAemia in initial episodes of active CMV infection that resolved spontaneously A $3-fold increase ofCMVDNA load between the values in the first and second PCR positive specimens was documented in only 2 episodes (B) Early kinetics of CMV plasmaDNAemia in initial episodes of active CMV infection that were eventually treated preemptively with antivirals (n5 17) before initiation of therapy (C) In5 of these episodes (white triangles) CMV DNA load rapidly decreased following instauration of antiviral therapy in 5 episodes in the remaining12 episodes a delayed response to therapy was observed (black diamonds) Day 0 represents the day of the first positive PCR result
1606 Biol Blood Marrow Transplant 171602-1611 2011B Mu~noz-Cobo et al
negative predictive value for this criterion to identifyepisodes that required therapeutic intervention were764 894 866 and 809 respectively
As shown in Table 2 the doubling times for CMVin the 2 self-resolving episodes inwhich a significant in-crease in CMV DNA load was documented (277 and318) were slightly lower than for treated episodes (me-dian 218 range 104-876) The CMV doubling timewas higher for typeA than for typeB episodes althoughthe difference did not reach statistical significance (P5160) In addition the median CMV DNA load at thetime of initiation of preemptive therapy was not signif-icantly different between type A and type B episodes(P 5 743)
Effects of Pretransplant and Clinical Factors onthe Kinetic Pattern of First Episodes of CMVDNAemia
As shown in Table 3 nonsignificant tendencies toexperience more frequent episodes of CMVDNAemiarequiring antiviral therapy were observed in patientsreceiving cord blood orHLA-mismatched grafts in pa-tients who had undergone myeloablative conditioningor in those who were treated with MMF or prednisoneas a part of the graft-vs-host disease (GVHD) prophy-laxis regimen CMV D1R1 allo-SCT recipientsdeveloped more frequently self-resolving episodesthan D2R1 or D1R2 patients although the differ-
ence did not reach statistical significance Likewisea trend toward a higher incidence of episodes requiringantiviral therapy was observed in patients with a priordiagnosis of acute grade II-IV GVHD Interestinglyepisodes requiring antiviral therapy for resolutionappeared to occur at a lower frequency in patientstreated with rapamycin as a part of theGVHDprophy-laxis regimen than in those treated with other combi-nations of immunosuppressive drugs
Virologic Features of Recurrent Episodes ofCMV DNAemia
Twelve of 23 patients (521) experiencing an ini-tial self-resolving episode of active CMV infectiondeveloped a recurrent episode of CMV DNAemiawithin the first year after transplantation All of these12 episodes resolved without therapeutic intervention(9 had 1 positive PCR result) The incidence ofrecurrent episodes of CMV DNAemia in patientswho had experienced a treated episode (7 of 17 pa-tients 42) was comparable to the incidence inpatients with prior self-resolving episodes (P 5 905)Nevertheless 3 of these 7 secondary episodes requiredantiviral treatment (2 were type B and 1 was type Aepisodes) In addition recurrent episodes of CMVDNAemia occurred with equal frequencies followingtype A and type B episodes (P 5 10) The virologicfeatures of recurrent episodes of CMV DNAemia are
Table 4 Virologic Features of Recurrent Episodes of CMVPlasma DNAemia
Virologic Parameter
Type of Episode
P ValueSelf-Resolving Treated
Initial VL (copiesmL) 25 (20-63) 35 (28-161) 054Peak VL (copiesmL) 43 (22-477) 1012 (5674-1395) 002Duration (days) 19 (6-67) 34 (26-35) 295Day of first + PCR 96 (54-260) 160 (96-180) 421
VL indicates CMV DNA loadFigures are given as median numbers (range)As determined by the Mann-Whitney U-test A P value 05 was con-sidered statistically significant
Table 3 Effects of Pretransplant and Clinical Factors on theOccurrence of Self-Resolving or Treated Initial Episodes ofCytomegalovirus (CMV) DNAemia
Factor
No of Patients with ActiveCMV Infection ()
P ValueTotal Self-Resolving Treated
CMV-serostatusD+R+ 21 13 (619) 8 (381)D2R+ 16 9 (562) 7 (438)D+R2 3 1 (250) 2 (750) 623
Type of donorand HLA match
Relatedmatched 17 10 (588) 7 (412)Relatedmismatched 2 0 (00) 2 (1000)Unrelatedmatched 13 9 (692) 4 (308)Unrelatedmismatched 8 4 (500) 4 (500) 388
Stem cells sourcePeripheral blood 32 19 (593) 13 (407)Cord blood 8 4 (500) 4 (500) 702
ConditioningMyeloablative 19 10 (526) 9 (474)Nonmyeloablative 21 13 (619) 8 (391) 750
GVHD prophylaxisCSA + MTX 20 14 (650) 6 (350)CSA + MMF 9 4 (444) 5 (556)RapamycinTacrolimus 7 5 (714) 2 (296)CSA + PDN 2 0 (00) 2 (1000) 123
Acute GVHDdaggerGrades 0-I 25 14 (560) 11 (440)Grades II-IV 10 5 (500) 5 (500) 10
D indicates donor R recipient CSA cyclosporine A MTX methotrex-ate MMF mycophenolate mofetil PDN prednisoneFrequency comparisons were carried out using the chi-square test(Fisherrsquos exact test) A P value05was considered statistically significantdaggerOnly those cases in which acute GVHD occurred before detection ofCMV DNAemia were considered for analysis
Biol Blood Marrow Transplant 171602-1611 2011 1607Kinetics of CMV Plasma DNAemia in Allo-SCT
summarized in Table 4 The duration of treatedepisodes was longer than that of self-resolvingepisodes although statistical significance was notreached As for first episodes the initial CMV DNAload in recurrent episodes was significantly higher inself-resolving episodes than in treated episodesalthough again a high degree of overlap was observedNevertheless in contrast to what was observed ininitial episodes variation in CMV DNA load betweenbaseline levels and those measured in the second pos-itive PCR did not allow for discrimination between
Days0 20 40 60
Lmseipoc
aimeA
NDVMCgoL
08
10
12
14
16
18
20
22
24
26
28
Lmseipoc
aimeA
NDVMCgoL
1
1
1
1
2
2
2
2
2
3
3
3
Figure 3 (A) Kinetics of CMV plasma DNAemia in recurrent episodes of aplasma DNAemia in initial episodes of active CMV infection that required preethe day of the first positive PCR result
episodes resolving spontaneously (Figure 3A) andthose requiring antiviral therapy (Figure 3B) In factsignificant variations between measurements wereobserved in none out of 9 self-resolving episodeswith more than 1 positive PCR result and in 1 of 3 ep-isodes eventually treated (Figure 3B) The CMVDNAload decay rate in these episodes was a median of024 day21 (range 016-059 day21) which corre-sponded to a median half-life of 285 days (range117-410 days) The kinetics of CMV DNAemiaclearance for secondary episodes that resolved sponta-neously did not follow an exponential decay function(not shown)
Effects of Pretransplant and Clinical Factorson the Incidence of Recurrent Episodes of CMVDNAemia
A trend toward a more frequent occurrence ofrecurrent episodes of CMV DNAemia was observedin CMV D2R1 patients and in the setting of unre-latedmismatched and umbilical cord blood allo-SCTThe differences however did not reach statisticalsignificance (Table 5)
Kinetics of CMV Plasma DNAemia in Patientswith CMV End-Organ Disease
Two patients developed CMV end-organ disease(enteritis) within the first 100 days after transplantationBoth received unrelatedHLA-matched peripheral
Days0 5 10 15 20
2
4
6
8
0
2
4
6
8
0
2
4
ctive CMV infection that resolved spontaneously (B) Kinetics of CMVmptive antiviral therapy before initiation of treatment Day 0 represents
Table 5 Effects of Pretransplant and Clinical Factors on theIncidence of Recurrent Episodes of Cytomegalovirus (CMV)DNAemia within the Study Period
Factor
Recurrent Episode of CMVDNAemia No of Patients ()
P ValueYes No
CMV-serostatusD+R+ 9 (428) 12 (572)D2R+ 10 (625) 6 (375)D+R2 0 (0) 3 (100) 111
Type of donorand HLA match
Relatedmatched 8 (470) 9 (530)Relatedmismatched 0 (0) 2 (100)Unrelatedmatched 6 (461) 7 (539)Unrelatedmismatched 5 (625) 3 (375) 655
Stem cells sourcePeripheral blood 14 (437) 18 (563)Cord blood 5 (625) 3 (375) 442
ConditioningMyeloablative 10 (526) 9 (474)Nonmyeloablative 9 (428) 12 (572) 752
GVHD prophylaxisCSA + MTX 10 (500) 10 (500)CSA + MMF 5 (555) 4 (455)RapamycinTacrolimus 4 (571) 3 (429)CSA + PDN 0 (0) 2 (100) 123
Acute GVHDdaggerGrades 0-I 14 (560) 11 (440)Grades II-IV 7 (466) 8 (534) 504
D indicates donor R recipient CSA cyclosporine A MTX Methotrex-ate MMF mycophenolate mofetil PDN prednisoneFrequency comparisons were carried out using the chi-square test(Fisherrsquos exact test) A P value05 was considered statistically significantdaggerOnly those cases in which acute GVHD occurred before detection ofCMV DNAemia were considered for analysis
1608 Biol Blood Marrow Transplant 171602-1611 2011B Mu~noz-Cobo et al
blood stemcell graftswere conditionedwith anonmye-loablative regimen (fludarabine plus melphalan) andwere treated with cyclosporine A and methotrexate forprophylaxis of GVHD CMV-serostatus of donorsand recipients were D1R1 in 1 case and D2R1 inthe other Neither of these patients developed acuteGVHD (aGVHD) Both patients had low initialCMVDNAemia levels (91 and 28 copiesmL) A signif-icant increase in CMV DNA load before initiation ofantiviral therapy was observed in 1 of these episodes(dt 5 25 days) Both episodes (type B) were treatedwith iv ganciclovir and had a duration of 102 and87 days respectively The peak of CMV DNAemiawas reached at days 121 (66329 copiesmL) and130 (35431 copiesmL) respectively after the firstpositivePCRresultBothpatientsdevelopedarecurrentepisode of CMV DNAemia
DISCUSSION
In the current study we took advantage of a highlysensitive real-time PCR and a relatively conservativestrategy for initiation of preemptive antiviral therapy(500CMVDNA copiesmL in plasma) to investigate
whether the analysis of the kinetics of CMVDNAemiamay yield useful information for the therapeutic man-agement of active CMV infection in the allo-SCTsetting In our cohort the overall rate of CMV DNA-emia was exceedingly high (almost 70) which wasmost likely related not only to the sensitivity of thePCR assay employed for the surveillance of CMVinfection but also to the high-risk profile of the studygroup In effect almost 50 of patients received anunrelated andor HLA-mismatched graft and 44of CMV-seropositive patients received a graft froma CMV-seronegative donor These pretransplant con-ditions have been consistently associated with a highincidence of active CMV infection in the allo-SCTsetting [2] More than half of the initial episodes ofCMV DNAemia resolved spontaneously The dura-tion of self-resolving episodes of CMV DNAemiawas significantly shorter than that for episodes thatwere eventually treated Yet these episodes lasted fora median of 16 days This finding should encouragestudies aimed at determining the impact of low-levelCMV replication which is permitted when initiationof antiviral treatment is delayed until a certain CMVDNAemia threshold is reached (usually between 500to 1000 CMV DNA copiesmL) on the incidenceand severity of indirect effects linked to CMV [12]
For most self-resolving episodes the kinetics ofCMVplasmaDNA clearance did not follow a logarith-mic decay curve in fact either fluctuating or ratherstable levels of CMV DNA loads were observed untilresolution In agreement with data recently publishedby Buyck et al [12] the Kdecline for CMVDNA load inepisodes that resolved without antiviral therapy waslower than that observed in episodes that requiredantiviral treatment for resolution Accordingly thehalf-life of CMV DNA load was shorter in the formerepisodes Notably whole-blood samples were ana-lyzed in the study by Buyck et al [12] whereas plasmaspecimens were used in the current study
First we asked whether the initial CMV plasmaDNA load value (first positive PCR result) may allowfor discrimination between episodes eventually requir-ing antiviral therapy from those resolving without theneed of antiviral treatment If this were the case theinitiation of preemptive therapy could be anticipatedperhaps leading to a more rapid resolution of theepisode and thereby minimizing the potential deleteri-ous effects of continuous CMV replication Eventhough the median initial CMV DNA load was signif-icantly lower for self-resolving episodes than for thosethat required antiviral therapy for clearance we founda high degree of overlap among values measured inboth groups It is known that the coefficient of varia-tion of PCR assays for CMV DNA loads close to thelimit of detection as were most of the initial valuesin our patients may be as high as 30 [19] In lightof the above observations the data suggested that
Biol Blood Marrow Transplant 171602-1611 2011 1609Kinetics of CMV Plasma DNAemia in Allo-SCT
a threshold value for the initial CMV DNA load reli-ably predicting the subsequent kinetics of CMVDNAemia is unlikely to be established at least whenusing highly sensitive real-time PCR assays such asthe method employed in the current study for moni-toring of active CMV infection In this sense it mustbe noted that initial CMV DNA loads measured inthis study were below the limit of detection of mostcommercially available real-time PCRs [2]
We next sought to determine whether the compar-ison between CMV DNA loads measured at baseline(initial viral load) and shortly thereafter (second posi-tive PCRmdasha median of 6 days after the first positivePCR result)mdashwould allow for identification ofepisodes eventually requiring antiviral treatment Wefound significant increases of CMV DNA load($3-fold) in 76 of episodes eventually requiringantiviral treatment but in 10 of self-resolvingepisodes The use of the above criterion would haveidentified the episodes that eventually required anti-viral treatment with a high sensitivity specificity andpositive and negative predictive values In our cohortthis strategy would have allowed for the anticipationof the initiation of antiviral treatment in only 2 epi-sodes (3 and 7 days) because the second CMV DNA-emia value measured was above the established cutofffor initiation of antiviral therapy nevertheless a largernumber of patients (6 of 13) would have benefited fromthis strategy had a higher CMV DNAemia level(1000 copiesmL) been set as the threshold for the ini-tiation of antiviral therapy as in other transplant cen-ters In light of these findings studies designed todetermine whether anticipation of preemptive therapybased on the above criterion would lead to a reductionin the cumulative dose of antivirals administered or toany clinically significant benefit are warranted Priorstudies have proposed CMV plasma DNA levelincreases of 174 copiesmLday [5] or 266 copies be-tween 2 consecutive determinations drawn a medianof 7 days apart [4] to discriminate between episodesthat required preemptive treatment and those thatdid not These estimations nevertheless were madein the setting of a preemptive strategy consisting ofthe initiation of antiviral therapy upon detection ofany level of pp65 antigenemia In addition Boeckhand Ljungman [3] proposed an increase of $5-foldfor initiation of preemptive therapy in low-riskallo-SCT recipients To our knowledge no data onthe clinical efficacy and safety of such strategies havebeen published
Preemptive antiviral therapy results in most casesin a rapid decline of CMV DNA load (type A episodesin the current study) nevertheless increasing levels ofCMV DNAemia early after the initiation of antiviraltherapy (type B episodes in this study) are occasionallydocumented [20-23] This paradoxical phenomenonhas been related to a lack of prompt expansion of
functional CMV-specific T cells in response to viralreplication [23] The occurrence of episodes witha delayed response to antiviral therapy is associatedwith an increased risk of CMV end-organ disease[12] Thus early recognition of this type of episodewould allow for rapid therapeutic interventionperhaps including the use of adoptive immunotherapyin order to reduce the risk of CMV-related morbidityIn this context Buyck et al [12] found a significantlyhigher mean growth rate and higher baseline viralload at the initiation of therapy in episodes witha delayed response to therapy with respect to thosewith an immediate response to therapy whereas theinitial CMV DNA load appeared to be comparablefor both type of episodes Our data partly agree withthose of Buyck et al [12] In effect the CMV doublingtime was lower in type B than in type A episodesalthough statistical significance was not reached andthe initial CMV DNA load did not differ significantlybetween both types of episodes Nevertheless in con-trast to the data reported in the above study baselineCMV DNA loads at the time of initiation of preemp-tive therapy did not differ significantly between bothtypes of episodes Thus in our experience the analysisof the early kinetics ofCMVDNAemia did not allowusto consistently identify the episodes of active CMVinfection with a delayed response to antiviral therapyDiscrepancies between our data and those of Buycket al [12] may be related to several factors includingthe use of different specimens for CMV DNA quanti-fication the use of distinct CMV DNA thresholds fortriggering the initiation of preemptive therapy andthe extensive use of Campath-1H in their study
Recurrent episodes of active CMV infectionoccurred with a comparable frequency among patientswho had an initial self-resolving episode and those whodeveloped an initial preemptively treated episodeNevertheless the likelihood of experiencing a second-ary episode that required antiviral therapy was higherin patients who had developed a treated episode thanin those who had experienced a self-resolving episodeIn agreement with a previous study [12] the risk ofrecurrence was not associated with the rate of CMVDNA decline in primary treated episodes followinginitiation of therapy As for initial episodes the base-line CMV DNA load in secondary episodes did notallow for a prediction of the subsequent kinetics ofCMV DNAemia Nevertheless in contrast to initialepisodes variation in CMV DNA load between base-line levels and those measured in the second positivePCR did not allow for discrimination between epi-sodes resolving spontaneously and those requiringantiviral therapy As ultimate control of CMV replica-tion depends upon adequate expansion of functionalCMV-specific T cells [2324] the above findinglikely reflected a more efficient and prompt T cellresponse in secondary episodes
1610 Biol Blood Marrow Transplant 171602-1611 2011B Mu~noz-Cobo et al
We were interested in assessing the impact ofseveral pretransplant and posttransplant clinical factorson the kinetics ofCMVDNAemia during first episodesof activeCMV infection and the incidence of recurrentepisodes Although we found no significant associa-tions a trend toward a higher frequency of episodesthat required antiviral therapy was observed in CMVD2R1 recipients in patients who received umbilicalcord blood or HLA-mismatched grafts in those whoreceived mycophenolate mofetil or prednisone(1 mgkgday) as a part of the GVHD prophylaxisregimen and in patients who were treated with highdoses of corticosteroids (1 mgkgday) for grades IIto IV GVHD These findings were not unexpected asall the above conditions have been shown to be associ-ated with delayed CMV-specific immune recovery[25-30] In this context it has previously been shownthat the magnitude and promptness of the expansionof functional CMV-specific CD81 and CD41 T cellsin response to CMV replication critically determinethe kinetics of CMV DNAemia clearance [23] Inter-estingly the use of rapamycin for the prevention ofGVHD was clearly associated with a relatively lowincidence of episodes that required antiviral treatmentThe scarce number of patients treated with this drug inour cohort did not allow to draw definitive conclusionson this issue nevertheless this effect has been previ-ously documented in the solid organ transplantationsetting [31] and is likely because of a direct inhibitoryeffect of rapamycin on viral replication [32]
Delayed recovery of CMV-specific T immunityhas been shown to be a significant risk factor for thedevelopment of recurrent episodes of active CMVinfection in allo-SCT recipients [3033] In supportof this view we found that CMV D2R1 recipientsand patients who underwent unrelatedmismatchedor umbilical cord blood allo-SCT tended to experi-ence recurrent episodes of active CMV infectionwith higher frequencies As mentioned above all thesepretransplant and clinical conditions have been previ-ously documented to be associated with an impairmentof CMV-specific T cell recovery
The incidence of CMV end-organ disease in ourcohort was 33 (2 patients) which is in accordanceto data previously published by our group [4] Unfor-tunately neither the analysis of the early kinetics ofCMV plasma DNAemia in the absence of antiviraltherapy nor the assessment of the dynamics of CMVplasma DNA load following the instauration of anti-viral treatment in these 2 episodes allowed for the an-ticipation of the development of CMV end-organdisease Obviously no definitive conclusions can bedrawn from these data given the limited number ofcases subjected to analysis
This study has 2 main limitations First thenumber of patients included in the cohort may havebeen insufficient to assess precisely the impact of
pretransplant and clinical factors on the kinetics ofCMVDNAemia Second there might be certain inac-curacies in the CMV DNAemia kinetics calculationsbecause of insufficient frequency of sampling In thisrespect there is no consensus as to what should bethe frequency of CMV DNA load monitoring duringepisodes of active CMV infection in the allo-SCT set-ting our data seemed to support the idea that theschedule of once-a-week monitoring is probably safeas long as a highly sensitive PCR is used for the surveil-lance of CMV infection Nevertheless it may also bereasonable to implement the twice-a-week schedulefor high-risk patients such as those receiving an unre-lated or HLA-mismatched graft (including recipientsof umbilical cord blood transplants) in whom the dou-bling time of CMV during the episodes of viral repli-cation is clearly faster
In summary in the current study we further char-acterized the dynamics of CMV DNAemia duringinitial and recurrent episodes of active CMV infectionin the allo-SCT setting The data reported hereinshould be taken into consideration for the design ofpreemptive antiviral therapy strategies based on viro-logic monitoring
ACKNOWLEDGMENTS
We thank Julia Garcıa and Monica Reig for theirtechnical assistance
Financial disclosureThis research was supported bya grant (091117) from FIS (Fondo de InvestigacionesSanitarias Ministerio de Sanidad y Consumo Spain)
AUTHORrsquoS CONTRIBUTIONS
BM-C ECMAC andDB did PCR analysesand assisted in the analysis of the data CS IBMJR and JM analyzed the data and attended thepatients DN designed the study analyzed the dataand wrote the paper
REFERENCES
1 Ljungman P CMV infections after hematopoietic stem celltransplantation Bone Marrow Transplant 200842S70-S72
2 Solano C Navarro D Clinical virology of cytomegalovirusinfection following hematopoietic transplantation Future Virol20105111-124
3 Boeckh M Ljungman P How we treat cytomegalovirus inhematopoietic cell transplant recipients Blood 20091135711-5719
4 Gimeno C Solano C Latorre JC et al Quantification of DNAin plasma by an automated real-time PCR assay (cytomegalovi-rus PCR kit) for surveillance of active cytomegalovirus infectionand guidance of preemptive therapy for allogeneic hematopoi-etic stem cell transplant recipients J Clin Microbiol 2008463311-3318
5 Halfon P Berger P Khiri H et al Algorithm based on CMVkinetics DNA viral load for preemptive therapy initiation after
Biol Blood Marrow Transplant 171602-1611 2011 1611Kinetics of CMV Plasma DNAemia in Allo-SCT
hematopoietic cell transplantation J Med Virol 201183490-495
6 Ljungman PWouldmonitoring CMV immune responses allowimproved control of CMV in stem cell transplant patients J ClinVirol 200635493-495
7 Avetisyan G Aschan J Heuroagglund H Ringden O Ljungman PEvaluation of intervention strategy based on CMV-specificimmune responses after allogeneic SCT Bone Marrow Trans-plant 200740865-869
8 GorD Sabin C PrenticeHG et al Longitudinal fluctuations incytomegalovirus load in bone marrow transplant patients rela-tionship between peak virus load donorrecipient serostatusacute GVHD and CMV disease Bone Marrow Transplant199821597-605
9 Emery VC Sabin CA Cope AV Gor D Hassan-Walker AFGriffiths PD Application of viral-load kinetics to identifypatients who develop cytomegalovirus disease after transplanta-tion Lancet 20003552032-2036
10 Avetisyan G Larsson K Aschan J Nilsson C Hassan MLjungman P Impact on the cytomegalovirus (CMV) viral load byCMV-specific T-cell immunity in recipients of allogeneic stemcell transplantation Bone Marrow Transplant 200638687-692
11 Stachel D Kirby K Corey L Boeckh M Viral load as predictorfor transplant-related mortality in the era of pre-emptive ther-apy Bone Marrow Transplant 200841S46
12 Buyck HC Griffiths PD Emery VC Human cytomegalovirus(HCMV) replication kinetics in stem cell transplant recipientsfollowing anti-HCMV therapy J Clin Virol 20104932-36
13 Torre-Cisneros J Caston-Osorio JJ Martın C et al Impact ofinitial cytomegalovirus viral load on efficacy of preemptive ther-apy with ganciclovir in allogeneic stem cell transplant recipientsEnferm Infecc Microbiol Clin 2010286-12
14 Chilet M Aguilar G Benet I et al Virological and immunolog-ical features of active cytomegalovirus infection in nonimmuno-suppressed patients in a surgical and trauma intensive care unitJ Med Virol 2010821384-1391
15 Ljungman P Griffiths P Paya C Definitions of HCMV infec-tion and disease in transplant recipients Clin Infect Dis 2002341094-1097
16 TormoN Solano C de la Camara R et al An assessment of theeffect of human herpesvirus-6 replication on active cytomegalo-virus infection after allogeneic stem cell transplantation BiolBlood Marrow Transplant 201016653-661
17 Emery VC Cope AV Bowen EF Gor D Griffiths PD The dy-namics of human cytomegalovirus replication in vivo J ExpMed1999190177-182
18 Humar A Kumar D Boivin G Caliendo AM Cytomegalovirus(CMV) virus load kinetics to predict recurrent disease in solid-organ transplant patients with CMV disease J Infect Dis 2002186829-833
19 BoeckhMHuangM Ferrenberg J et al Optimization of quan-titative detection of cytomegalovirus DNA in plasma by real-time PCR J Clin Microbiol 2004421142-1148
20 BoeckhM Gooley TA MyersonD CunninghamT Schoch GBowden RA Cytomegalovirus pp65 antigenemia-guided earlytreatment with ganciclovir versus ganciclovir at engraftment af-ter allogeneic marrow transplantation a randomized double-blind study Blood 1996884063-4071
21 Nichols WG Corey L Gooley T et al Rising pp65 antigene-mia during preemptive anticytomegalovirus therapy afterallogeneic hematopoietic stem cell transplantation risk factorscorrelation with DNA load and outcomes Blood 200197867-874
22 Gerna G Lilleri D Zecca M et al Rising antigenemia levelsmay be misleading in pre-emptive therapy of human cytomega-lovirus infection in allogeneic hematopoietic stem cell transplantrecipients Haematologica 200590526-533
23 TormoN Solano C Benet I et al Lack of prompt expansion ofcytomegalovirus pp65 and IE-1-specific IFNgamma CD81 andCD41 T cells is associated with rising levels of pp65 antigene-mia and DNAemia during pre-emptive therapy in allogeneichematopoietic stem cell transplant recipients Bone MarrowTransplant 201045543-549
24 Tormo N Solano C Benet I et al Kinetics of cytomegalovirus(CMV) pp65 and IE-1-specific IFNgamma CD81 and CD41T cells during episodes of viral DNAemia in allogeneic stemcell transplant recipients potential implications for the manage-ment of active CMV infection J Med Virol 2010821208-1215
25 FosterAEGottliebDJ SartorMHertzbergMS BradstockKFCytomegalovirus-specific CD41 and CD81 T-cells followa similar reconstitution pattern after allogeneic stem cell trans-plantation Biol Blood Marrow Transplant 20028501-511
26 Hakki M Riddell SR Storek J et al Immune reconstitution tocytomegalovirus after allogeneic stem cell transplantationimpact of host factors drug therapy and subclinical reactivationBlood 20031023060-3067
27 Lilleri D Fornara C Chiesa A Caldera D Alessandrino EPGerna G Human cytomegalovirus-specific CD41 and CD81T-cell reconstitution in adult allogeneic hematopoietic stemcell transplant recipients and immune control of viral infectionHaematologica 200893248-256
28 Pourgheysari B Piper KP McLarnon A et al Early reconstitu-tion of effector memory CD41 CMV-specific T cells protectsagainst CMV reactivation following allogeneic SCT BoneMarrow Transplant 200943853-861
29 Zhou W Longmate J Lacey SF et al Impact of donor CMVstatus on viral infection and reconstitution of multifunctionCMV-specific T cells in CMV-positive transplant recipientsBlood 20091136465-6476
30 TormoN SolanoC Benet I et al Reconstitution of CMVpp65and IE-1-specific IFN-gCD8(1) and CD4(1) T-cell responsesaffording protection fromCMVDNAemia following allogeneichematopoietic SCT Bone Marrow Transplant 2011 Jan 17[Epub ahead of print]
31 San Juan R Aguado JM Lumbreras C et al Impact of currenttransplantation management on the development of cytomega-lovirus disease after renal transplantation Clin Infect Dis 200847875-882
32 Moorman NJ Shenk T Rapamycin-resistant mTORC1 kinaseactivity is required for herpesvirus replication J Virol 2010845260-5269
33 Gratama JW Boeckh M Nakamura R et al Immune monitor-ing with iTAg MHC Tetramers for prediction of recurrent orpersistent cytomegalovirus infection or disease in allogeneichematopoietic stem cell transplant recipients a prospectivemulticenter study Blood 20101161655-1662

1604 Biol Blood Marrow Transplant 171602-1611 2011B Mu~noz-Cobo et al
CMV-seropositive recipients of related grafts andCMV-seronegative patients receiving an unrelatedgraft from a CMV-seronegative donor were treatedwith oral acyclovir (800 mg12 h) Acyclovir was ad-ministered until stable hematopoietic cell engraftmentwas achieved usually around day 130
Definitions
Active CMV infection was diagnosed upon detec-tion of CMV DNA (any level) in 1 or more plasmaspecimens Episodes of active CMV infection withonly 1 specimen testing positive by PCR were consid-ered true episodes if a different aliquot of plasma alsotested positive For data analysis the commencementand end of a given episode of active viral infectionwere defined by the first positive (any level of plasmaviral load) and first negative results respectivelyOnly increases in CMVDNA loads$3 times the base-line levels were considered true increases as these wereabove the intraassay variability of the PCR test(approximately 02 log10 for low CMV DNA values)[3] Recurrent episodes of active CMV infection werethose that occurred at least 15 days after clearance (firstnegative PCR) of the preceding episode CMV end-organ disease was diagnosed and treated as previouslyreported [15]
Analyses of the Kinetics of CMV PlasmaDNAemia
To determine the rate of virus replication the viraldoubling time (dt) of CMV was estimated consideringfor analysis the first 2 PCR positive results in theabsence of antiviral treatment [16] The dt was givenby dt 5 (t2 2 t1) log(2)log(q2q1) with q1 and t1being the CMV DNA load (copiesmL) at the time ofthe first positive PCR (in days) respectively and q2and t2 the CMV DNA load at the time of the secondpositive PCR respectively This formula assumesa constant growth rate which occurs in the early phaseof virus replication CMV dt calculations were per-formed only for episodes in which the increase inCMVDNA load between the first and the second pos-itive PCR determinations was$3-fold The kinetics ofCMV DNA load clearance followed a logarithmicdecay curve in most treated episodes but only in a fewself-resolving episodes (see below) expressed by theequation yt 5 y0e
2kt where y0 is the initial CMVDNA load t is time from initiation of antiviral therapy(for self-resolving episodes t is the duration of theepisode) and k is the decay constant [121718] Anominal value of 9 copiesmL was arbitrarily ascribedfor plasma specimens with undetectable CMV DNAload on the basis of the actual limit of detection ofthe assay CMVDNA load half-life was then calculatedusing the equation ln2k
Statistical Analysis
The data were analyzed with the aid of the statisti-cal package SPSS version 170 (SPSS North ChicagoIL)Comparisonswere carried out using the chi-squaretest for categoric variables and the nonparametricMann-Whitney U-test or the Wilcoxon signed-ranktest for unpaired or paired continuous data respec-tively Two-sided exact P values are reported AP value05 was considered statistically significant
RESULTS
Incidence of CMV Plasma DNAemia during theStudy Period
Forty of 59 patients (678) developed 1 (n 5 21)or more (n 5 19) episodes of CMV DNAemia duringthe study period Three of the latter 19 patients expe-rienced more than 2 episodes (in all 63 episodes weredetected) The patients were followed up for a medianof 220 days (range 10-375 days)
Virologic Features of Initial Episodes of CMVPlasma DNAemia
Initial episodes of CMV plasma DNAemia weredetected at a median of 30 days (range 1-90 days) aftertransplantation Twenty-three out of the 40 episodes(57) resolved spontaneously Of these 19 had 1specimen testing positive by PCR Twelve of theremaining 17 episodes cleared following instaurationof antiviral therapy The median time to the firstCMVDNA positive result was not significantly differ-ent for self-resolving or for treated episodes (P5 930)The CMV DNA load in plasma rapidly declined afterimplementation of antiviral therapy in 5 episodes(type A episodes) whereas in 12 episodes CMVDNA load increased within the next 2 to 3 weeksfollowing the instauration of antiviral therapy andthen progressively declined (type B episodes) Fivetreated episodes (type B) were still active at the timeof the patientrsquos death As shown in Table 2 the dura-tion of CMV DNAemia was significantly shorter forself-resolving episodes than for treated episodes(P 5 001) irrespective of whether the latter weretype A (P 5 022) or type B (P 5 001) episodes Theduration of type B episodes was longer than that oftype A episodes although the difference did not reachstatistical significance (P 5 432)
In most of self-resolving episodes (15 of 19 epi-sodes with 1 positive PCR result) either fluctuatingor rather stable levels of CMV DNA loads (mean dif-ference between samples02 log10 copiesmL) wereobserved until resolution In the remaining 4 episodesCMV DNA load decline did follow an exponentialfunction (Figure 1) The CMV DNA load decay rate(k) in these episodes was lower than for treated
Table 2 Virologic Features of Initial Episodes of Cytomegalovirus (CMV) Plasma DNAemia
Type of Episode(No of Episodes)
Initial VL(CopiesmL)
VL at Treatment(CopiesmL)
Peak VL(CopiesmL)
Duration(Days)
Virus DoublingTime (Days) KdeclineDay21 Half-Life (Days)
Self-resolving (23) 28 (20-135) NA 40 (25-308) 16 (3-48) NA 013 (009-027) 557 (252-743)Treated (17) 70 (25-216) 1216 (523-15244) 3872 (676-66329) 405 (18-130) 218 (104-876) 035 (006-065) 190 (106-1150)Treated Type A (5) 63 (25-133) 1455 (676-1739) 1455 (676-1739) 40 (21-68) 445 (120-876) 037 (018-037) 187 (183-385)Treated Type Bdagger (12) 79 (28-216) 939 (523-15244) 9907 (918-66329) 44 (18-130) 201 (104-310) 014 (006-065) 477 (106-1150)
VL indicates CMV DNA load NA not applicableFigures are given as median numbers (range)Immediate response to antiviral therapydaggerDelayed response to antiviral therapy
Biol Blood Marrow Transplant 171602-1611 2011 1605Kinetics of CMV Plasma DNAemia in Allo-SCT
episodes though statistical significance was notreached (P 5 297) Accordingly the median half-lifeof CMV DNA load was shorter in treated episodesthan in self-resolving episodes (P5 304) The medianvalue of k was higher for type A than for typeB episodes (P 5 422) Thus the median half-life ofCMV DNA load was shorter in type A than in typeB episodes (P 5 287)
Analysis of Early Kinetics of CMV DNAemia forPredicting the Virologic Outcome of InitialEpisodes of Active CMV Infection
The median initial CMV DNA load (first positivePCR) was significantly lower (P 5 001) in self-resolving episodes than in those that were eventuallytreated Type A and type B episodes had comparableinitial CMV DNA viral loads (P 5 62) Despite the
Days0 2 4 6 8 10
Lmseipoc
aimeA
NDVMCgoL
08
10
12
14
16
18
20
Lmseipoc
aimeA
NDVMCgoL
Days
0 2 4 6 8 10 12 14
Lmseipoc
aimeA
NDVMCgoL
08
10
12
14
16
18
20
Figure 1 Initial episodes of active CMV infection that resolved spontaneouexponential decay function Black circles are data points The line of best fit is
above findings a cutoff value for the initial CMVDNA load reliably predicting the subsequent kineticsof CMV DNAemia could not be established becauseof a high degree of overlap
We next sought to determine whether the compar-ison of CMV DNA loads measured at baseline (initialviral load) and shortly thereafter (second positivePCR) a median of 6 days (range 4-8 days) after thefirst positive PCR would allow for discriminatingbetween episodes eventually requiring antiviral treat-ment from those that would resolve without theneed of antiviral therapy No significant variation(3-fold) in the CMV DNA load between measure-ments was observed in 17 of 19 self-resolving episodes(see Figure 2A and B) A significant increase ($3-fold)in CMVDNA load was found in 3 of 5 type A episodesand in 10 of 12 type B episodes (Figure 2C) Thus thesensitivity specificity positive predictive value and
Days0 5 10 15 20 25 30
08
10
12
14
16
18
20
22
24
Days
0 5 10 15 20
Lmseipoc
aimeA
NDVMCgoL
09
10
11
12
13
14
15
16
17
sly in which the kinetics of CMV plasma DNA clearance followed anshown Day 0 represents the day of the first positive PCR result
Days0 10 20 30 40 50
Lmseipoc
aimeA
NDVMCgoL
08
10
12
14
16
18
20
22
24
26
Days0 5 10 15 20 25 30
Lmseipoc
aimeA
NDVMCgoL
08
10
12
14
16
18
20
22
24
Days0 10 20 30 40
Lmseipoc
aimeA
NDVMCgoL
10
15
20
25
30
35
40
45
Figure 2 (A) Kinetics of CMV plasma DNAemia in initial episodes of active CMV infection that resolved spontaneously A $3-fold increase ofCMVDNA load between the values in the first and second PCR positive specimens was documented in only 2 episodes (B) Early kinetics of CMV plasmaDNAemia in initial episodes of active CMV infection that were eventually treated preemptively with antivirals (n5 17) before initiation of therapy (C) In5 of these episodes (white triangles) CMV DNA load rapidly decreased following instauration of antiviral therapy in 5 episodes in the remaining12 episodes a delayed response to therapy was observed (black diamonds) Day 0 represents the day of the first positive PCR result
1606 Biol Blood Marrow Transplant 171602-1611 2011B Mu~noz-Cobo et al
negative predictive value for this criterion to identifyepisodes that required therapeutic intervention were764 894 866 and 809 respectively
As shown in Table 2 the doubling times for CMVin the 2 self-resolving episodes inwhich a significant in-crease in CMV DNA load was documented (277 and318) were slightly lower than for treated episodes (me-dian 218 range 104-876) The CMV doubling timewas higher for typeA than for typeB episodes althoughthe difference did not reach statistical significance (P5160) In addition the median CMV DNA load at thetime of initiation of preemptive therapy was not signif-icantly different between type A and type B episodes(P 5 743)
Effects of Pretransplant and Clinical Factors onthe Kinetic Pattern of First Episodes of CMVDNAemia
As shown in Table 3 nonsignificant tendencies toexperience more frequent episodes of CMVDNAemiarequiring antiviral therapy were observed in patientsreceiving cord blood orHLA-mismatched grafts in pa-tients who had undergone myeloablative conditioningor in those who were treated with MMF or prednisoneas a part of the graft-vs-host disease (GVHD) prophy-laxis regimen CMV D1R1 allo-SCT recipientsdeveloped more frequently self-resolving episodesthan D2R1 or D1R2 patients although the differ-
ence did not reach statistical significance Likewisea trend toward a higher incidence of episodes requiringantiviral therapy was observed in patients with a priordiagnosis of acute grade II-IV GVHD Interestinglyepisodes requiring antiviral therapy for resolutionappeared to occur at a lower frequency in patientstreated with rapamycin as a part of theGVHDprophy-laxis regimen than in those treated with other combi-nations of immunosuppressive drugs
Virologic Features of Recurrent Episodes ofCMV DNAemia
Twelve of 23 patients (521) experiencing an ini-tial self-resolving episode of active CMV infectiondeveloped a recurrent episode of CMV DNAemiawithin the first year after transplantation All of these12 episodes resolved without therapeutic intervention(9 had 1 positive PCR result) The incidence ofrecurrent episodes of CMV DNAemia in patientswho had experienced a treated episode (7 of 17 pa-tients 42) was comparable to the incidence inpatients with prior self-resolving episodes (P 5 905)Nevertheless 3 of these 7 secondary episodes requiredantiviral treatment (2 were type B and 1 was type Aepisodes) In addition recurrent episodes of CMVDNAemia occurred with equal frequencies followingtype A and type B episodes (P 5 10) The virologicfeatures of recurrent episodes of CMV DNAemia are
Table 4 Virologic Features of Recurrent Episodes of CMVPlasma DNAemia
Virologic Parameter
Type of Episode
P ValueSelf-Resolving Treated
Initial VL (copiesmL) 25 (20-63) 35 (28-161) 054Peak VL (copiesmL) 43 (22-477) 1012 (5674-1395) 002Duration (days) 19 (6-67) 34 (26-35) 295Day of first + PCR 96 (54-260) 160 (96-180) 421
VL indicates CMV DNA loadFigures are given as median numbers (range)As determined by the Mann-Whitney U-test A P value 05 was con-sidered statistically significant
Table 3 Effects of Pretransplant and Clinical Factors on theOccurrence of Self-Resolving or Treated Initial Episodes ofCytomegalovirus (CMV) DNAemia
Factor
No of Patients with ActiveCMV Infection ()
P ValueTotal Self-Resolving Treated
CMV-serostatusD+R+ 21 13 (619) 8 (381)D2R+ 16 9 (562) 7 (438)D+R2 3 1 (250) 2 (750) 623
Type of donorand HLA match
Relatedmatched 17 10 (588) 7 (412)Relatedmismatched 2 0 (00) 2 (1000)Unrelatedmatched 13 9 (692) 4 (308)Unrelatedmismatched 8 4 (500) 4 (500) 388
Stem cells sourcePeripheral blood 32 19 (593) 13 (407)Cord blood 8 4 (500) 4 (500) 702
ConditioningMyeloablative 19 10 (526) 9 (474)Nonmyeloablative 21 13 (619) 8 (391) 750
GVHD prophylaxisCSA + MTX 20 14 (650) 6 (350)CSA + MMF 9 4 (444) 5 (556)RapamycinTacrolimus 7 5 (714) 2 (296)CSA + PDN 2 0 (00) 2 (1000) 123
Acute GVHDdaggerGrades 0-I 25 14 (560) 11 (440)Grades II-IV 10 5 (500) 5 (500) 10
D indicates donor R recipient CSA cyclosporine A MTX methotrex-ate MMF mycophenolate mofetil PDN prednisoneFrequency comparisons were carried out using the chi-square test(Fisherrsquos exact test) A P value05was considered statistically significantdaggerOnly those cases in which acute GVHD occurred before detection ofCMV DNAemia were considered for analysis
Biol Blood Marrow Transplant 171602-1611 2011 1607Kinetics of CMV Plasma DNAemia in Allo-SCT
summarized in Table 4 The duration of treatedepisodes was longer than that of self-resolvingepisodes although statistical significance was notreached As for first episodes the initial CMV DNAload in recurrent episodes was significantly higher inself-resolving episodes than in treated episodesalthough again a high degree of overlap was observedNevertheless in contrast to what was observed ininitial episodes variation in CMV DNA load betweenbaseline levels and those measured in the second pos-itive PCR did not allow for discrimination between
Days0 20 40 60
Lmseipoc
aimeA
NDVMCgoL
08
10
12
14
16
18
20
22
24
26
28
Lmseipoc
aimeA
NDVMCgoL
1
1
1
1
2
2
2
2
2
3
3
3
Figure 3 (A) Kinetics of CMV plasma DNAemia in recurrent episodes of aplasma DNAemia in initial episodes of active CMV infection that required preethe day of the first positive PCR result
episodes resolving spontaneously (Figure 3A) andthose requiring antiviral therapy (Figure 3B) In factsignificant variations between measurements wereobserved in none out of 9 self-resolving episodeswith more than 1 positive PCR result and in 1 of 3 ep-isodes eventually treated (Figure 3B) The CMVDNAload decay rate in these episodes was a median of024 day21 (range 016-059 day21) which corre-sponded to a median half-life of 285 days (range117-410 days) The kinetics of CMV DNAemiaclearance for secondary episodes that resolved sponta-neously did not follow an exponential decay function(not shown)
Effects of Pretransplant and Clinical Factorson the Incidence of Recurrent Episodes of CMVDNAemia
A trend toward a more frequent occurrence ofrecurrent episodes of CMV DNAemia was observedin CMV D2R1 patients and in the setting of unre-latedmismatched and umbilical cord blood allo-SCTThe differences however did not reach statisticalsignificance (Table 5)
Kinetics of CMV Plasma DNAemia in Patientswith CMV End-Organ Disease
Two patients developed CMV end-organ disease(enteritis) within the first 100 days after transplantationBoth received unrelatedHLA-matched peripheral
Days0 5 10 15 20
2
4
6
8
0
2
4
6
8
0
2
4
ctive CMV infection that resolved spontaneously (B) Kinetics of CMVmptive antiviral therapy before initiation of treatment Day 0 represents
Table 5 Effects of Pretransplant and Clinical Factors on theIncidence of Recurrent Episodes of Cytomegalovirus (CMV)DNAemia within the Study Period
Factor
Recurrent Episode of CMVDNAemia No of Patients ()
P ValueYes No
CMV-serostatusD+R+ 9 (428) 12 (572)D2R+ 10 (625) 6 (375)D+R2 0 (0) 3 (100) 111
Type of donorand HLA match
Relatedmatched 8 (470) 9 (530)Relatedmismatched 0 (0) 2 (100)Unrelatedmatched 6 (461) 7 (539)Unrelatedmismatched 5 (625) 3 (375) 655
Stem cells sourcePeripheral blood 14 (437) 18 (563)Cord blood 5 (625) 3 (375) 442
ConditioningMyeloablative 10 (526) 9 (474)Nonmyeloablative 9 (428) 12 (572) 752
GVHD prophylaxisCSA + MTX 10 (500) 10 (500)CSA + MMF 5 (555) 4 (455)RapamycinTacrolimus 4 (571) 3 (429)CSA + PDN 0 (0) 2 (100) 123
Acute GVHDdaggerGrades 0-I 14 (560) 11 (440)Grades II-IV 7 (466) 8 (534) 504
D indicates donor R recipient CSA cyclosporine A MTX Methotrex-ate MMF mycophenolate mofetil PDN prednisoneFrequency comparisons were carried out using the chi-square test(Fisherrsquos exact test) A P value05 was considered statistically significantdaggerOnly those cases in which acute GVHD occurred before detection ofCMV DNAemia were considered for analysis
1608 Biol Blood Marrow Transplant 171602-1611 2011B Mu~noz-Cobo et al
blood stemcell graftswere conditionedwith anonmye-loablative regimen (fludarabine plus melphalan) andwere treated with cyclosporine A and methotrexate forprophylaxis of GVHD CMV-serostatus of donorsand recipients were D1R1 in 1 case and D2R1 inthe other Neither of these patients developed acuteGVHD (aGVHD) Both patients had low initialCMVDNAemia levels (91 and 28 copiesmL) A signif-icant increase in CMV DNA load before initiation ofantiviral therapy was observed in 1 of these episodes(dt 5 25 days) Both episodes (type B) were treatedwith iv ganciclovir and had a duration of 102 and87 days respectively The peak of CMV DNAemiawas reached at days 121 (66329 copiesmL) and130 (35431 copiesmL) respectively after the firstpositivePCRresultBothpatientsdevelopedarecurrentepisode of CMV DNAemia
DISCUSSION
In the current study we took advantage of a highlysensitive real-time PCR and a relatively conservativestrategy for initiation of preemptive antiviral therapy(500CMVDNA copiesmL in plasma) to investigate
whether the analysis of the kinetics of CMVDNAemiamay yield useful information for the therapeutic man-agement of active CMV infection in the allo-SCTsetting In our cohort the overall rate of CMV DNA-emia was exceedingly high (almost 70) which wasmost likely related not only to the sensitivity of thePCR assay employed for the surveillance of CMVinfection but also to the high-risk profile of the studygroup In effect almost 50 of patients received anunrelated andor HLA-mismatched graft and 44of CMV-seropositive patients received a graft froma CMV-seronegative donor These pretransplant con-ditions have been consistently associated with a highincidence of active CMV infection in the allo-SCTsetting [2] More than half of the initial episodes ofCMV DNAemia resolved spontaneously The dura-tion of self-resolving episodes of CMV DNAemiawas significantly shorter than that for episodes thatwere eventually treated Yet these episodes lasted fora median of 16 days This finding should encouragestudies aimed at determining the impact of low-levelCMV replication which is permitted when initiationof antiviral treatment is delayed until a certain CMVDNAemia threshold is reached (usually between 500to 1000 CMV DNA copiesmL) on the incidenceand severity of indirect effects linked to CMV [12]
For most self-resolving episodes the kinetics ofCMVplasmaDNA clearance did not follow a logarith-mic decay curve in fact either fluctuating or ratherstable levels of CMV DNA loads were observed untilresolution In agreement with data recently publishedby Buyck et al [12] the Kdecline for CMVDNA load inepisodes that resolved without antiviral therapy waslower than that observed in episodes that requiredantiviral treatment for resolution Accordingly thehalf-life of CMV DNA load was shorter in the formerepisodes Notably whole-blood samples were ana-lyzed in the study by Buyck et al [12] whereas plasmaspecimens were used in the current study
First we asked whether the initial CMV plasmaDNA load value (first positive PCR result) may allowfor discrimination between episodes eventually requir-ing antiviral therapy from those resolving without theneed of antiviral treatment If this were the case theinitiation of preemptive therapy could be anticipatedperhaps leading to a more rapid resolution of theepisode and thereby minimizing the potential deleteri-ous effects of continuous CMV replication Eventhough the median initial CMV DNA load was signif-icantly lower for self-resolving episodes than for thosethat required antiviral therapy for clearance we founda high degree of overlap among values measured inboth groups It is known that the coefficient of varia-tion of PCR assays for CMV DNA loads close to thelimit of detection as were most of the initial valuesin our patients may be as high as 30 [19] In lightof the above observations the data suggested that
Biol Blood Marrow Transplant 171602-1611 2011 1609Kinetics of CMV Plasma DNAemia in Allo-SCT
a threshold value for the initial CMV DNA load reli-ably predicting the subsequent kinetics of CMVDNAemia is unlikely to be established at least whenusing highly sensitive real-time PCR assays such asthe method employed in the current study for moni-toring of active CMV infection In this sense it mustbe noted that initial CMV DNA loads measured inthis study were below the limit of detection of mostcommercially available real-time PCRs [2]
We next sought to determine whether the compar-ison between CMV DNA loads measured at baseline(initial viral load) and shortly thereafter (second posi-tive PCRmdasha median of 6 days after the first positivePCR result)mdashwould allow for identification ofepisodes eventually requiring antiviral treatment Wefound significant increases of CMV DNA load($3-fold) in 76 of episodes eventually requiringantiviral treatment but in 10 of self-resolvingepisodes The use of the above criterion would haveidentified the episodes that eventually required anti-viral treatment with a high sensitivity specificity andpositive and negative predictive values In our cohortthis strategy would have allowed for the anticipationof the initiation of antiviral treatment in only 2 epi-sodes (3 and 7 days) because the second CMV DNA-emia value measured was above the established cutofffor initiation of antiviral therapy nevertheless a largernumber of patients (6 of 13) would have benefited fromthis strategy had a higher CMV DNAemia level(1000 copiesmL) been set as the threshold for the ini-tiation of antiviral therapy as in other transplant cen-ters In light of these findings studies designed todetermine whether anticipation of preemptive therapybased on the above criterion would lead to a reductionin the cumulative dose of antivirals administered or toany clinically significant benefit are warranted Priorstudies have proposed CMV plasma DNA levelincreases of 174 copiesmLday [5] or 266 copies be-tween 2 consecutive determinations drawn a medianof 7 days apart [4] to discriminate between episodesthat required preemptive treatment and those thatdid not These estimations nevertheless were madein the setting of a preemptive strategy consisting ofthe initiation of antiviral therapy upon detection ofany level of pp65 antigenemia In addition Boeckhand Ljungman [3] proposed an increase of $5-foldfor initiation of preemptive therapy in low-riskallo-SCT recipients To our knowledge no data onthe clinical efficacy and safety of such strategies havebeen published
Preemptive antiviral therapy results in most casesin a rapid decline of CMV DNA load (type A episodesin the current study) nevertheless increasing levels ofCMV DNAemia early after the initiation of antiviraltherapy (type B episodes in this study) are occasionallydocumented [20-23] This paradoxical phenomenonhas been related to a lack of prompt expansion of
functional CMV-specific T cells in response to viralreplication [23] The occurrence of episodes witha delayed response to antiviral therapy is associatedwith an increased risk of CMV end-organ disease[12] Thus early recognition of this type of episodewould allow for rapid therapeutic interventionperhaps including the use of adoptive immunotherapyin order to reduce the risk of CMV-related morbidityIn this context Buyck et al [12] found a significantlyhigher mean growth rate and higher baseline viralload at the initiation of therapy in episodes witha delayed response to therapy with respect to thosewith an immediate response to therapy whereas theinitial CMV DNA load appeared to be comparablefor both type of episodes Our data partly agree withthose of Buyck et al [12] In effect the CMV doublingtime was lower in type B than in type A episodesalthough statistical significance was not reached andthe initial CMV DNA load did not differ significantlybetween both types of episodes Nevertheless in con-trast to the data reported in the above study baselineCMV DNA loads at the time of initiation of preemp-tive therapy did not differ significantly between bothtypes of episodes Thus in our experience the analysisof the early kinetics ofCMVDNAemia did not allowusto consistently identify the episodes of active CMVinfection with a delayed response to antiviral therapyDiscrepancies between our data and those of Buycket al [12] may be related to several factors includingthe use of different specimens for CMV DNA quanti-fication the use of distinct CMV DNA thresholds fortriggering the initiation of preemptive therapy andthe extensive use of Campath-1H in their study
Recurrent episodes of active CMV infectionoccurred with a comparable frequency among patientswho had an initial self-resolving episode and those whodeveloped an initial preemptively treated episodeNevertheless the likelihood of experiencing a second-ary episode that required antiviral therapy was higherin patients who had developed a treated episode thanin those who had experienced a self-resolving episodeIn agreement with a previous study [12] the risk ofrecurrence was not associated with the rate of CMVDNA decline in primary treated episodes followinginitiation of therapy As for initial episodes the base-line CMV DNA load in secondary episodes did notallow for a prediction of the subsequent kinetics ofCMV DNAemia Nevertheless in contrast to initialepisodes variation in CMV DNA load between base-line levels and those measured in the second positivePCR did not allow for discrimination between epi-sodes resolving spontaneously and those requiringantiviral therapy As ultimate control of CMV replica-tion depends upon adequate expansion of functionalCMV-specific T cells [2324] the above findinglikely reflected a more efficient and prompt T cellresponse in secondary episodes
1610 Biol Blood Marrow Transplant 171602-1611 2011B Mu~noz-Cobo et al
We were interested in assessing the impact ofseveral pretransplant and posttransplant clinical factorson the kinetics ofCMVDNAemia during first episodesof activeCMV infection and the incidence of recurrentepisodes Although we found no significant associa-tions a trend toward a higher frequency of episodesthat required antiviral therapy was observed in CMVD2R1 recipients in patients who received umbilicalcord blood or HLA-mismatched grafts in those whoreceived mycophenolate mofetil or prednisone(1 mgkgday) as a part of the GVHD prophylaxisregimen and in patients who were treated with highdoses of corticosteroids (1 mgkgday) for grades IIto IV GVHD These findings were not unexpected asall the above conditions have been shown to be associ-ated with delayed CMV-specific immune recovery[25-30] In this context it has previously been shownthat the magnitude and promptness of the expansionof functional CMV-specific CD81 and CD41 T cellsin response to CMV replication critically determinethe kinetics of CMV DNAemia clearance [23] Inter-estingly the use of rapamycin for the prevention ofGVHD was clearly associated with a relatively lowincidence of episodes that required antiviral treatmentThe scarce number of patients treated with this drug inour cohort did not allow to draw definitive conclusionson this issue nevertheless this effect has been previ-ously documented in the solid organ transplantationsetting [31] and is likely because of a direct inhibitoryeffect of rapamycin on viral replication [32]
Delayed recovery of CMV-specific T immunityhas been shown to be a significant risk factor for thedevelopment of recurrent episodes of active CMVinfection in allo-SCT recipients [3033] In supportof this view we found that CMV D2R1 recipientsand patients who underwent unrelatedmismatchedor umbilical cord blood allo-SCT tended to experi-ence recurrent episodes of active CMV infectionwith higher frequencies As mentioned above all thesepretransplant and clinical conditions have been previ-ously documented to be associated with an impairmentof CMV-specific T cell recovery
The incidence of CMV end-organ disease in ourcohort was 33 (2 patients) which is in accordanceto data previously published by our group [4] Unfor-tunately neither the analysis of the early kinetics ofCMV plasma DNAemia in the absence of antiviraltherapy nor the assessment of the dynamics of CMVplasma DNA load following the instauration of anti-viral treatment in these 2 episodes allowed for the an-ticipation of the development of CMV end-organdisease Obviously no definitive conclusions can bedrawn from these data given the limited number ofcases subjected to analysis
This study has 2 main limitations First thenumber of patients included in the cohort may havebeen insufficient to assess precisely the impact of
pretransplant and clinical factors on the kinetics ofCMVDNAemia Second there might be certain inac-curacies in the CMV DNAemia kinetics calculationsbecause of insufficient frequency of sampling In thisrespect there is no consensus as to what should bethe frequency of CMV DNA load monitoring duringepisodes of active CMV infection in the allo-SCT set-ting our data seemed to support the idea that theschedule of once-a-week monitoring is probably safeas long as a highly sensitive PCR is used for the surveil-lance of CMV infection Nevertheless it may also bereasonable to implement the twice-a-week schedulefor high-risk patients such as those receiving an unre-lated or HLA-mismatched graft (including recipientsof umbilical cord blood transplants) in whom the dou-bling time of CMV during the episodes of viral repli-cation is clearly faster
In summary in the current study we further char-acterized the dynamics of CMV DNAemia duringinitial and recurrent episodes of active CMV infectionin the allo-SCT setting The data reported hereinshould be taken into consideration for the design ofpreemptive antiviral therapy strategies based on viro-logic monitoring
ACKNOWLEDGMENTS
We thank Julia Garcıa and Monica Reig for theirtechnical assistance
Financial disclosureThis research was supported bya grant (091117) from FIS (Fondo de InvestigacionesSanitarias Ministerio de Sanidad y Consumo Spain)
AUTHORrsquoS CONTRIBUTIONS
BM-C ECMAC andDB did PCR analysesand assisted in the analysis of the data CS IBMJR and JM analyzed the data and attended thepatients DN designed the study analyzed the dataand wrote the paper
REFERENCES
1 Ljungman P CMV infections after hematopoietic stem celltransplantation Bone Marrow Transplant 200842S70-S72
2 Solano C Navarro D Clinical virology of cytomegalovirusinfection following hematopoietic transplantation Future Virol20105111-124
3 Boeckh M Ljungman P How we treat cytomegalovirus inhematopoietic cell transplant recipients Blood 20091135711-5719
4 Gimeno C Solano C Latorre JC et al Quantification of DNAin plasma by an automated real-time PCR assay (cytomegalovi-rus PCR kit) for surveillance of active cytomegalovirus infectionand guidance of preemptive therapy for allogeneic hematopoi-etic stem cell transplant recipients J Clin Microbiol 2008463311-3318
5 Halfon P Berger P Khiri H et al Algorithm based on CMVkinetics DNA viral load for preemptive therapy initiation after
Biol Blood Marrow Transplant 171602-1611 2011 1611Kinetics of CMV Plasma DNAemia in Allo-SCT
hematopoietic cell transplantation J Med Virol 201183490-495
6 Ljungman PWouldmonitoring CMV immune responses allowimproved control of CMV in stem cell transplant patients J ClinVirol 200635493-495
7 Avetisyan G Aschan J Heuroagglund H Ringden O Ljungman PEvaluation of intervention strategy based on CMV-specificimmune responses after allogeneic SCT Bone Marrow Trans-plant 200740865-869
8 GorD Sabin C PrenticeHG et al Longitudinal fluctuations incytomegalovirus load in bone marrow transplant patients rela-tionship between peak virus load donorrecipient serostatusacute GVHD and CMV disease Bone Marrow Transplant199821597-605
9 Emery VC Sabin CA Cope AV Gor D Hassan-Walker AFGriffiths PD Application of viral-load kinetics to identifypatients who develop cytomegalovirus disease after transplanta-tion Lancet 20003552032-2036
10 Avetisyan G Larsson K Aschan J Nilsson C Hassan MLjungman P Impact on the cytomegalovirus (CMV) viral load byCMV-specific T-cell immunity in recipients of allogeneic stemcell transplantation Bone Marrow Transplant 200638687-692
11 Stachel D Kirby K Corey L Boeckh M Viral load as predictorfor transplant-related mortality in the era of pre-emptive ther-apy Bone Marrow Transplant 200841S46
12 Buyck HC Griffiths PD Emery VC Human cytomegalovirus(HCMV) replication kinetics in stem cell transplant recipientsfollowing anti-HCMV therapy J Clin Virol 20104932-36
13 Torre-Cisneros J Caston-Osorio JJ Martın C et al Impact ofinitial cytomegalovirus viral load on efficacy of preemptive ther-apy with ganciclovir in allogeneic stem cell transplant recipientsEnferm Infecc Microbiol Clin 2010286-12
14 Chilet M Aguilar G Benet I et al Virological and immunolog-ical features of active cytomegalovirus infection in nonimmuno-suppressed patients in a surgical and trauma intensive care unitJ Med Virol 2010821384-1391
15 Ljungman P Griffiths P Paya C Definitions of HCMV infec-tion and disease in transplant recipients Clin Infect Dis 2002341094-1097
16 TormoN Solano C de la Camara R et al An assessment of theeffect of human herpesvirus-6 replication on active cytomegalo-virus infection after allogeneic stem cell transplantation BiolBlood Marrow Transplant 201016653-661
17 Emery VC Cope AV Bowen EF Gor D Griffiths PD The dy-namics of human cytomegalovirus replication in vivo J ExpMed1999190177-182
18 Humar A Kumar D Boivin G Caliendo AM Cytomegalovirus(CMV) virus load kinetics to predict recurrent disease in solid-organ transplant patients with CMV disease J Infect Dis 2002186829-833
19 BoeckhMHuangM Ferrenberg J et al Optimization of quan-titative detection of cytomegalovirus DNA in plasma by real-time PCR J Clin Microbiol 2004421142-1148
20 BoeckhM Gooley TA MyersonD CunninghamT Schoch GBowden RA Cytomegalovirus pp65 antigenemia-guided earlytreatment with ganciclovir versus ganciclovir at engraftment af-ter allogeneic marrow transplantation a randomized double-blind study Blood 1996884063-4071
21 Nichols WG Corey L Gooley T et al Rising pp65 antigene-mia during preemptive anticytomegalovirus therapy afterallogeneic hematopoietic stem cell transplantation risk factorscorrelation with DNA load and outcomes Blood 200197867-874
22 Gerna G Lilleri D Zecca M et al Rising antigenemia levelsmay be misleading in pre-emptive therapy of human cytomega-lovirus infection in allogeneic hematopoietic stem cell transplantrecipients Haematologica 200590526-533
23 TormoN Solano C Benet I et al Lack of prompt expansion ofcytomegalovirus pp65 and IE-1-specific IFNgamma CD81 andCD41 T cells is associated with rising levels of pp65 antigene-mia and DNAemia during pre-emptive therapy in allogeneichematopoietic stem cell transplant recipients Bone MarrowTransplant 201045543-549
24 Tormo N Solano C Benet I et al Kinetics of cytomegalovirus(CMV) pp65 and IE-1-specific IFNgamma CD81 and CD41T cells during episodes of viral DNAemia in allogeneic stemcell transplant recipients potential implications for the manage-ment of active CMV infection J Med Virol 2010821208-1215
25 FosterAEGottliebDJ SartorMHertzbergMS BradstockKFCytomegalovirus-specific CD41 and CD81 T-cells followa similar reconstitution pattern after allogeneic stem cell trans-plantation Biol Blood Marrow Transplant 20028501-511
26 Hakki M Riddell SR Storek J et al Immune reconstitution tocytomegalovirus after allogeneic stem cell transplantationimpact of host factors drug therapy and subclinical reactivationBlood 20031023060-3067
27 Lilleri D Fornara C Chiesa A Caldera D Alessandrino EPGerna G Human cytomegalovirus-specific CD41 and CD81T-cell reconstitution in adult allogeneic hematopoietic stemcell transplant recipients and immune control of viral infectionHaematologica 200893248-256
28 Pourgheysari B Piper KP McLarnon A et al Early reconstitu-tion of effector memory CD41 CMV-specific T cells protectsagainst CMV reactivation following allogeneic SCT BoneMarrow Transplant 200943853-861
29 Zhou W Longmate J Lacey SF et al Impact of donor CMVstatus on viral infection and reconstitution of multifunctionCMV-specific T cells in CMV-positive transplant recipientsBlood 20091136465-6476
30 TormoN SolanoC Benet I et al Reconstitution of CMVpp65and IE-1-specific IFN-gCD8(1) and CD4(1) T-cell responsesaffording protection fromCMVDNAemia following allogeneichematopoietic SCT Bone Marrow Transplant 2011 Jan 17[Epub ahead of print]
31 San Juan R Aguado JM Lumbreras C et al Impact of currenttransplantation management on the development of cytomega-lovirus disease after renal transplantation Clin Infect Dis 200847875-882
32 Moorman NJ Shenk T Rapamycin-resistant mTORC1 kinaseactivity is required for herpesvirus replication J Virol 2010845260-5269
33 Gratama JW Boeckh M Nakamura R et al Immune monitor-ing with iTAg MHC Tetramers for prediction of recurrent orpersistent cytomegalovirus infection or disease in allogeneichematopoietic stem cell transplant recipients a prospectivemulticenter study Blood 20101161655-1662
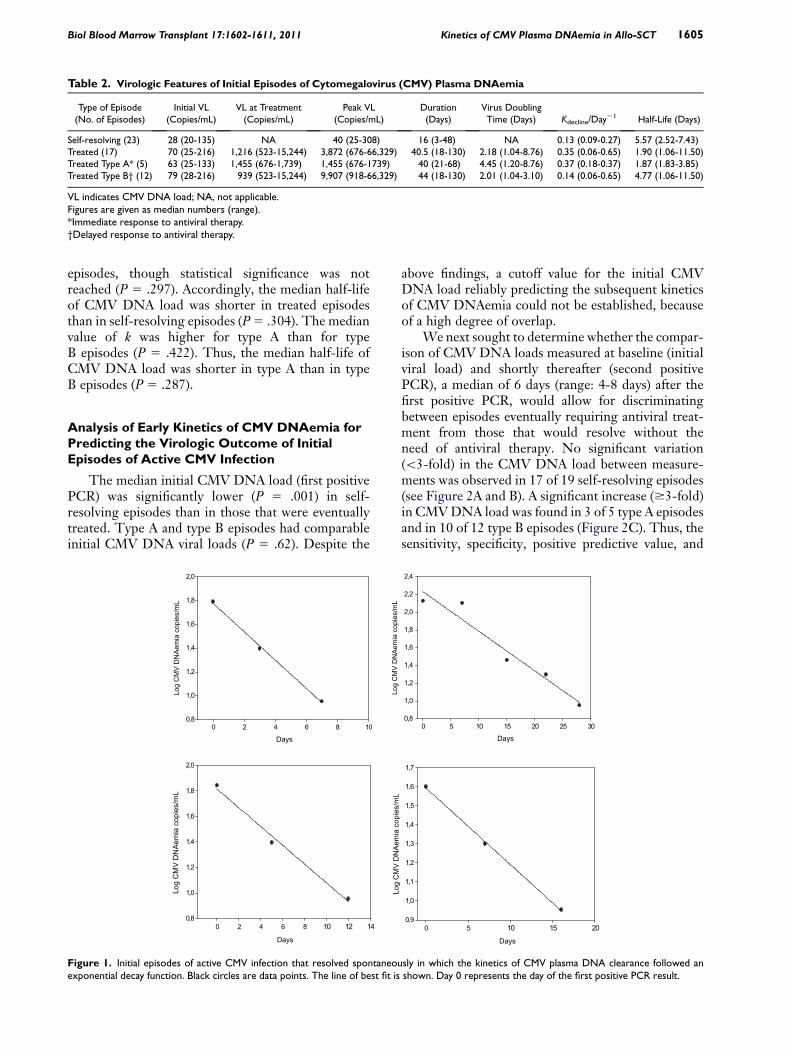
Table 2 Virologic Features of Initial Episodes of Cytomegalovirus (CMV) Plasma DNAemia
Type of Episode(No of Episodes)
Initial VL(CopiesmL)
VL at Treatment(CopiesmL)
Peak VL(CopiesmL)
Duration(Days)
Virus DoublingTime (Days) KdeclineDay21 Half-Life (Days)
Self-resolving (23) 28 (20-135) NA 40 (25-308) 16 (3-48) NA 013 (009-027) 557 (252-743)Treated (17) 70 (25-216) 1216 (523-15244) 3872 (676-66329) 405 (18-130) 218 (104-876) 035 (006-065) 190 (106-1150)Treated Type A (5) 63 (25-133) 1455 (676-1739) 1455 (676-1739) 40 (21-68) 445 (120-876) 037 (018-037) 187 (183-385)Treated Type Bdagger (12) 79 (28-216) 939 (523-15244) 9907 (918-66329) 44 (18-130) 201 (104-310) 014 (006-065) 477 (106-1150)
VL indicates CMV DNA load NA not applicableFigures are given as median numbers (range)Immediate response to antiviral therapydaggerDelayed response to antiviral therapy
Biol Blood Marrow Transplant 171602-1611 2011 1605Kinetics of CMV Plasma DNAemia in Allo-SCT
episodes though statistical significance was notreached (P 5 297) Accordingly the median half-lifeof CMV DNA load was shorter in treated episodesthan in self-resolving episodes (P5 304) The medianvalue of k was higher for type A than for typeB episodes (P 5 422) Thus the median half-life ofCMV DNA load was shorter in type A than in typeB episodes (P 5 287)
Analysis of Early Kinetics of CMV DNAemia forPredicting the Virologic Outcome of InitialEpisodes of Active CMV Infection
The median initial CMV DNA load (first positivePCR) was significantly lower (P 5 001) in self-resolving episodes than in those that were eventuallytreated Type A and type B episodes had comparableinitial CMV DNA viral loads (P 5 62) Despite the
Days0 2 4 6 8 10
Lmseipoc
aimeA
NDVMCgoL
08
10
12
14
16
18
20
Lmseipoc
aimeA
NDVMCgoL
Days
0 2 4 6 8 10 12 14
Lmseipoc
aimeA
NDVMCgoL
08
10
12
14
16
18
20
Figure 1 Initial episodes of active CMV infection that resolved spontaneouexponential decay function Black circles are data points The line of best fit is
above findings a cutoff value for the initial CMVDNA load reliably predicting the subsequent kineticsof CMV DNAemia could not be established becauseof a high degree of overlap
We next sought to determine whether the compar-ison of CMV DNA loads measured at baseline (initialviral load) and shortly thereafter (second positivePCR) a median of 6 days (range 4-8 days) after thefirst positive PCR would allow for discriminatingbetween episodes eventually requiring antiviral treat-ment from those that would resolve without theneed of antiviral therapy No significant variation(3-fold) in the CMV DNA load between measure-ments was observed in 17 of 19 self-resolving episodes(see Figure 2A and B) A significant increase ($3-fold)in CMVDNA load was found in 3 of 5 type A episodesand in 10 of 12 type B episodes (Figure 2C) Thus thesensitivity specificity positive predictive value and
Days0 5 10 15 20 25 30
08
10
12
14
16
18
20
22
24
Days
0 5 10 15 20
Lmseipoc
aimeA
NDVMCgoL
09
10
11
12
13
14
15
16
17
sly in which the kinetics of CMV plasma DNA clearance followed anshown Day 0 represents the day of the first positive PCR result
Days0 10 20 30 40 50
Lmseipoc
aimeA
NDVMCgoL
08
10
12
14
16
18
20
22
24
26
Days0 5 10 15 20 25 30
Lmseipoc
aimeA
NDVMCgoL
08
10
12
14
16
18
20
22
24
Days0 10 20 30 40
Lmseipoc
aimeA
NDVMCgoL
10
15
20
25
30
35
40
45
Figure 2 (A) Kinetics of CMV plasma DNAemia in initial episodes of active CMV infection that resolved spontaneously A $3-fold increase ofCMVDNA load between the values in the first and second PCR positive specimens was documented in only 2 episodes (B) Early kinetics of CMV plasmaDNAemia in initial episodes of active CMV infection that were eventually treated preemptively with antivirals (n5 17) before initiation of therapy (C) In5 of these episodes (white triangles) CMV DNA load rapidly decreased following instauration of antiviral therapy in 5 episodes in the remaining12 episodes a delayed response to therapy was observed (black diamonds) Day 0 represents the day of the first positive PCR result
1606 Biol Blood Marrow Transplant 171602-1611 2011B Mu~noz-Cobo et al
negative predictive value for this criterion to identifyepisodes that required therapeutic intervention were764 894 866 and 809 respectively
As shown in Table 2 the doubling times for CMVin the 2 self-resolving episodes inwhich a significant in-crease in CMV DNA load was documented (277 and318) were slightly lower than for treated episodes (me-dian 218 range 104-876) The CMV doubling timewas higher for typeA than for typeB episodes althoughthe difference did not reach statistical significance (P5160) In addition the median CMV DNA load at thetime of initiation of preemptive therapy was not signif-icantly different between type A and type B episodes(P 5 743)
Effects of Pretransplant and Clinical Factors onthe Kinetic Pattern of First Episodes of CMVDNAemia
As shown in Table 3 nonsignificant tendencies toexperience more frequent episodes of CMVDNAemiarequiring antiviral therapy were observed in patientsreceiving cord blood orHLA-mismatched grafts in pa-tients who had undergone myeloablative conditioningor in those who were treated with MMF or prednisoneas a part of the graft-vs-host disease (GVHD) prophy-laxis regimen CMV D1R1 allo-SCT recipientsdeveloped more frequently self-resolving episodesthan D2R1 or D1R2 patients although the differ-
ence did not reach statistical significance Likewisea trend toward a higher incidence of episodes requiringantiviral therapy was observed in patients with a priordiagnosis of acute grade II-IV GVHD Interestinglyepisodes requiring antiviral therapy for resolutionappeared to occur at a lower frequency in patientstreated with rapamycin as a part of theGVHDprophy-laxis regimen than in those treated with other combi-nations of immunosuppressive drugs
Virologic Features of Recurrent Episodes ofCMV DNAemia
Twelve of 23 patients (521) experiencing an ini-tial self-resolving episode of active CMV infectiondeveloped a recurrent episode of CMV DNAemiawithin the first year after transplantation All of these12 episodes resolved without therapeutic intervention(9 had 1 positive PCR result) The incidence ofrecurrent episodes of CMV DNAemia in patientswho had experienced a treated episode (7 of 17 pa-tients 42) was comparable to the incidence inpatients with prior self-resolving episodes (P 5 905)Nevertheless 3 of these 7 secondary episodes requiredantiviral treatment (2 were type B and 1 was type Aepisodes) In addition recurrent episodes of CMVDNAemia occurred with equal frequencies followingtype A and type B episodes (P 5 10) The virologicfeatures of recurrent episodes of CMV DNAemia are
Table 4 Virologic Features of Recurrent Episodes of CMVPlasma DNAemia
Virologic Parameter
Type of Episode
P ValueSelf-Resolving Treated
Initial VL (copiesmL) 25 (20-63) 35 (28-161) 054Peak VL (copiesmL) 43 (22-477) 1012 (5674-1395) 002Duration (days) 19 (6-67) 34 (26-35) 295Day of first + PCR 96 (54-260) 160 (96-180) 421
VL indicates CMV DNA loadFigures are given as median numbers (range)As determined by the Mann-Whitney U-test A P value 05 was con-sidered statistically significant
Table 3 Effects of Pretransplant and Clinical Factors on theOccurrence of Self-Resolving or Treated Initial Episodes ofCytomegalovirus (CMV) DNAemia
Factor
No of Patients with ActiveCMV Infection ()
P ValueTotal Self-Resolving Treated
CMV-serostatusD+R+ 21 13 (619) 8 (381)D2R+ 16 9 (562) 7 (438)D+R2 3 1 (250) 2 (750) 623
Type of donorand HLA match
Relatedmatched 17 10 (588) 7 (412)Relatedmismatched 2 0 (00) 2 (1000)Unrelatedmatched 13 9 (692) 4 (308)Unrelatedmismatched 8 4 (500) 4 (500) 388
Stem cells sourcePeripheral blood 32 19 (593) 13 (407)Cord blood 8 4 (500) 4 (500) 702
ConditioningMyeloablative 19 10 (526) 9 (474)Nonmyeloablative 21 13 (619) 8 (391) 750
GVHD prophylaxisCSA + MTX 20 14 (650) 6 (350)CSA + MMF 9 4 (444) 5 (556)RapamycinTacrolimus 7 5 (714) 2 (296)CSA + PDN 2 0 (00) 2 (1000) 123
Acute GVHDdaggerGrades 0-I 25 14 (560) 11 (440)Grades II-IV 10 5 (500) 5 (500) 10
D indicates donor R recipient CSA cyclosporine A MTX methotrex-ate MMF mycophenolate mofetil PDN prednisoneFrequency comparisons were carried out using the chi-square test(Fisherrsquos exact test) A P value05was considered statistically significantdaggerOnly those cases in which acute GVHD occurred before detection ofCMV DNAemia were considered for analysis
Biol Blood Marrow Transplant 171602-1611 2011 1607Kinetics of CMV Plasma DNAemia in Allo-SCT
summarized in Table 4 The duration of treatedepisodes was longer than that of self-resolvingepisodes although statistical significance was notreached As for first episodes the initial CMV DNAload in recurrent episodes was significantly higher inself-resolving episodes than in treated episodesalthough again a high degree of overlap was observedNevertheless in contrast to what was observed ininitial episodes variation in CMV DNA load betweenbaseline levels and those measured in the second pos-itive PCR did not allow for discrimination between
Days0 20 40 60
Lmseipoc
aimeA
NDVMCgoL
08
10
12
14
16
18
20
22
24
26
28
Lmseipoc
aimeA
NDVMCgoL
1
1
1
1
2
2
2
2
2
3
3
3
Figure 3 (A) Kinetics of CMV plasma DNAemia in recurrent episodes of aplasma DNAemia in initial episodes of active CMV infection that required preethe day of the first positive PCR result
episodes resolving spontaneously (Figure 3A) andthose requiring antiviral therapy (Figure 3B) In factsignificant variations between measurements wereobserved in none out of 9 self-resolving episodeswith more than 1 positive PCR result and in 1 of 3 ep-isodes eventually treated (Figure 3B) The CMVDNAload decay rate in these episodes was a median of024 day21 (range 016-059 day21) which corre-sponded to a median half-life of 285 days (range117-410 days) The kinetics of CMV DNAemiaclearance for secondary episodes that resolved sponta-neously did not follow an exponential decay function(not shown)
Effects of Pretransplant and Clinical Factorson the Incidence of Recurrent Episodes of CMVDNAemia
A trend toward a more frequent occurrence ofrecurrent episodes of CMV DNAemia was observedin CMV D2R1 patients and in the setting of unre-latedmismatched and umbilical cord blood allo-SCTThe differences however did not reach statisticalsignificance (Table 5)
Kinetics of CMV Plasma DNAemia in Patientswith CMV End-Organ Disease
Two patients developed CMV end-organ disease(enteritis) within the first 100 days after transplantationBoth received unrelatedHLA-matched peripheral
Days0 5 10 15 20
2
4
6
8
0
2
4
6
8
0
2
4
ctive CMV infection that resolved spontaneously (B) Kinetics of CMVmptive antiviral therapy before initiation of treatment Day 0 represents
Table 5 Effects of Pretransplant and Clinical Factors on theIncidence of Recurrent Episodes of Cytomegalovirus (CMV)DNAemia within the Study Period
Factor
Recurrent Episode of CMVDNAemia No of Patients ()
P ValueYes No
CMV-serostatusD+R+ 9 (428) 12 (572)D2R+ 10 (625) 6 (375)D+R2 0 (0) 3 (100) 111
Type of donorand HLA match
Relatedmatched 8 (470) 9 (530)Relatedmismatched 0 (0) 2 (100)Unrelatedmatched 6 (461) 7 (539)Unrelatedmismatched 5 (625) 3 (375) 655
Stem cells sourcePeripheral blood 14 (437) 18 (563)Cord blood 5 (625) 3 (375) 442
ConditioningMyeloablative 10 (526) 9 (474)Nonmyeloablative 9 (428) 12 (572) 752
GVHD prophylaxisCSA + MTX 10 (500) 10 (500)CSA + MMF 5 (555) 4 (455)RapamycinTacrolimus 4 (571) 3 (429)CSA + PDN 0 (0) 2 (100) 123
Acute GVHDdaggerGrades 0-I 14 (560) 11 (440)Grades II-IV 7 (466) 8 (534) 504
D indicates donor R recipient CSA cyclosporine A MTX Methotrex-ate MMF mycophenolate mofetil PDN prednisoneFrequency comparisons were carried out using the chi-square test(Fisherrsquos exact test) A P value05 was considered statistically significantdaggerOnly those cases in which acute GVHD occurred before detection ofCMV DNAemia were considered for analysis
1608 Biol Blood Marrow Transplant 171602-1611 2011B Mu~noz-Cobo et al
blood stemcell graftswere conditionedwith anonmye-loablative regimen (fludarabine plus melphalan) andwere treated with cyclosporine A and methotrexate forprophylaxis of GVHD CMV-serostatus of donorsand recipients were D1R1 in 1 case and D2R1 inthe other Neither of these patients developed acuteGVHD (aGVHD) Both patients had low initialCMVDNAemia levels (91 and 28 copiesmL) A signif-icant increase in CMV DNA load before initiation ofantiviral therapy was observed in 1 of these episodes(dt 5 25 days) Both episodes (type B) were treatedwith iv ganciclovir and had a duration of 102 and87 days respectively The peak of CMV DNAemiawas reached at days 121 (66329 copiesmL) and130 (35431 copiesmL) respectively after the firstpositivePCRresultBothpatientsdevelopedarecurrentepisode of CMV DNAemia
DISCUSSION
In the current study we took advantage of a highlysensitive real-time PCR and a relatively conservativestrategy for initiation of preemptive antiviral therapy(500CMVDNA copiesmL in plasma) to investigate
whether the analysis of the kinetics of CMVDNAemiamay yield useful information for the therapeutic man-agement of active CMV infection in the allo-SCTsetting In our cohort the overall rate of CMV DNA-emia was exceedingly high (almost 70) which wasmost likely related not only to the sensitivity of thePCR assay employed for the surveillance of CMVinfection but also to the high-risk profile of the studygroup In effect almost 50 of patients received anunrelated andor HLA-mismatched graft and 44of CMV-seropositive patients received a graft froma CMV-seronegative donor These pretransplant con-ditions have been consistently associated with a highincidence of active CMV infection in the allo-SCTsetting [2] More than half of the initial episodes ofCMV DNAemia resolved spontaneously The dura-tion of self-resolving episodes of CMV DNAemiawas significantly shorter than that for episodes thatwere eventually treated Yet these episodes lasted fora median of 16 days This finding should encouragestudies aimed at determining the impact of low-levelCMV replication which is permitted when initiationof antiviral treatment is delayed until a certain CMVDNAemia threshold is reached (usually between 500to 1000 CMV DNA copiesmL) on the incidenceand severity of indirect effects linked to CMV [12]
For most self-resolving episodes the kinetics ofCMVplasmaDNA clearance did not follow a logarith-mic decay curve in fact either fluctuating or ratherstable levels of CMV DNA loads were observed untilresolution In agreement with data recently publishedby Buyck et al [12] the Kdecline for CMVDNA load inepisodes that resolved without antiviral therapy waslower than that observed in episodes that requiredantiviral treatment for resolution Accordingly thehalf-life of CMV DNA load was shorter in the formerepisodes Notably whole-blood samples were ana-lyzed in the study by Buyck et al [12] whereas plasmaspecimens were used in the current study
First we asked whether the initial CMV plasmaDNA load value (first positive PCR result) may allowfor discrimination between episodes eventually requir-ing antiviral therapy from those resolving without theneed of antiviral treatment If this were the case theinitiation of preemptive therapy could be anticipatedperhaps leading to a more rapid resolution of theepisode and thereby minimizing the potential deleteri-ous effects of continuous CMV replication Eventhough the median initial CMV DNA load was signif-icantly lower for self-resolving episodes than for thosethat required antiviral therapy for clearance we founda high degree of overlap among values measured inboth groups It is known that the coefficient of varia-tion of PCR assays for CMV DNA loads close to thelimit of detection as were most of the initial valuesin our patients may be as high as 30 [19] In lightof the above observations the data suggested that
Biol Blood Marrow Transplant 171602-1611 2011 1609Kinetics of CMV Plasma DNAemia in Allo-SCT
a threshold value for the initial CMV DNA load reli-ably predicting the subsequent kinetics of CMVDNAemia is unlikely to be established at least whenusing highly sensitive real-time PCR assays such asthe method employed in the current study for moni-toring of active CMV infection In this sense it mustbe noted that initial CMV DNA loads measured inthis study were below the limit of detection of mostcommercially available real-time PCRs [2]
We next sought to determine whether the compar-ison between CMV DNA loads measured at baseline(initial viral load) and shortly thereafter (second posi-tive PCRmdasha median of 6 days after the first positivePCR result)mdashwould allow for identification ofepisodes eventually requiring antiviral treatment Wefound significant increases of CMV DNA load($3-fold) in 76 of episodes eventually requiringantiviral treatment but in 10 of self-resolvingepisodes The use of the above criterion would haveidentified the episodes that eventually required anti-viral treatment with a high sensitivity specificity andpositive and negative predictive values In our cohortthis strategy would have allowed for the anticipationof the initiation of antiviral treatment in only 2 epi-sodes (3 and 7 days) because the second CMV DNA-emia value measured was above the established cutofffor initiation of antiviral therapy nevertheless a largernumber of patients (6 of 13) would have benefited fromthis strategy had a higher CMV DNAemia level(1000 copiesmL) been set as the threshold for the ini-tiation of antiviral therapy as in other transplant cen-ters In light of these findings studies designed todetermine whether anticipation of preemptive therapybased on the above criterion would lead to a reductionin the cumulative dose of antivirals administered or toany clinically significant benefit are warranted Priorstudies have proposed CMV plasma DNA levelincreases of 174 copiesmLday [5] or 266 copies be-tween 2 consecutive determinations drawn a medianof 7 days apart [4] to discriminate between episodesthat required preemptive treatment and those thatdid not These estimations nevertheless were madein the setting of a preemptive strategy consisting ofthe initiation of antiviral therapy upon detection ofany level of pp65 antigenemia In addition Boeckhand Ljungman [3] proposed an increase of $5-foldfor initiation of preemptive therapy in low-riskallo-SCT recipients To our knowledge no data onthe clinical efficacy and safety of such strategies havebeen published
Preemptive antiviral therapy results in most casesin a rapid decline of CMV DNA load (type A episodesin the current study) nevertheless increasing levels ofCMV DNAemia early after the initiation of antiviraltherapy (type B episodes in this study) are occasionallydocumented [20-23] This paradoxical phenomenonhas been related to a lack of prompt expansion of
functional CMV-specific T cells in response to viralreplication [23] The occurrence of episodes witha delayed response to antiviral therapy is associatedwith an increased risk of CMV end-organ disease[12] Thus early recognition of this type of episodewould allow for rapid therapeutic interventionperhaps including the use of adoptive immunotherapyin order to reduce the risk of CMV-related morbidityIn this context Buyck et al [12] found a significantlyhigher mean growth rate and higher baseline viralload at the initiation of therapy in episodes witha delayed response to therapy with respect to thosewith an immediate response to therapy whereas theinitial CMV DNA load appeared to be comparablefor both type of episodes Our data partly agree withthose of Buyck et al [12] In effect the CMV doublingtime was lower in type B than in type A episodesalthough statistical significance was not reached andthe initial CMV DNA load did not differ significantlybetween both types of episodes Nevertheless in con-trast to the data reported in the above study baselineCMV DNA loads at the time of initiation of preemp-tive therapy did not differ significantly between bothtypes of episodes Thus in our experience the analysisof the early kinetics ofCMVDNAemia did not allowusto consistently identify the episodes of active CMVinfection with a delayed response to antiviral therapyDiscrepancies between our data and those of Buycket al [12] may be related to several factors includingthe use of different specimens for CMV DNA quanti-fication the use of distinct CMV DNA thresholds fortriggering the initiation of preemptive therapy andthe extensive use of Campath-1H in their study
Recurrent episodes of active CMV infectionoccurred with a comparable frequency among patientswho had an initial self-resolving episode and those whodeveloped an initial preemptively treated episodeNevertheless the likelihood of experiencing a second-ary episode that required antiviral therapy was higherin patients who had developed a treated episode thanin those who had experienced a self-resolving episodeIn agreement with a previous study [12] the risk ofrecurrence was not associated with the rate of CMVDNA decline in primary treated episodes followinginitiation of therapy As for initial episodes the base-line CMV DNA load in secondary episodes did notallow for a prediction of the subsequent kinetics ofCMV DNAemia Nevertheless in contrast to initialepisodes variation in CMV DNA load between base-line levels and those measured in the second positivePCR did not allow for discrimination between epi-sodes resolving spontaneously and those requiringantiviral therapy As ultimate control of CMV replica-tion depends upon adequate expansion of functionalCMV-specific T cells [2324] the above findinglikely reflected a more efficient and prompt T cellresponse in secondary episodes
1610 Biol Blood Marrow Transplant 171602-1611 2011B Mu~noz-Cobo et al
We were interested in assessing the impact ofseveral pretransplant and posttransplant clinical factorson the kinetics ofCMVDNAemia during first episodesof activeCMV infection and the incidence of recurrentepisodes Although we found no significant associa-tions a trend toward a higher frequency of episodesthat required antiviral therapy was observed in CMVD2R1 recipients in patients who received umbilicalcord blood or HLA-mismatched grafts in those whoreceived mycophenolate mofetil or prednisone(1 mgkgday) as a part of the GVHD prophylaxisregimen and in patients who were treated with highdoses of corticosteroids (1 mgkgday) for grades IIto IV GVHD These findings were not unexpected asall the above conditions have been shown to be associ-ated with delayed CMV-specific immune recovery[25-30] In this context it has previously been shownthat the magnitude and promptness of the expansionof functional CMV-specific CD81 and CD41 T cellsin response to CMV replication critically determinethe kinetics of CMV DNAemia clearance [23] Inter-estingly the use of rapamycin for the prevention ofGVHD was clearly associated with a relatively lowincidence of episodes that required antiviral treatmentThe scarce number of patients treated with this drug inour cohort did not allow to draw definitive conclusionson this issue nevertheless this effect has been previ-ously documented in the solid organ transplantationsetting [31] and is likely because of a direct inhibitoryeffect of rapamycin on viral replication [32]
Delayed recovery of CMV-specific T immunityhas been shown to be a significant risk factor for thedevelopment of recurrent episodes of active CMVinfection in allo-SCT recipients [3033] In supportof this view we found that CMV D2R1 recipientsand patients who underwent unrelatedmismatchedor umbilical cord blood allo-SCT tended to experi-ence recurrent episodes of active CMV infectionwith higher frequencies As mentioned above all thesepretransplant and clinical conditions have been previ-ously documented to be associated with an impairmentof CMV-specific T cell recovery
The incidence of CMV end-organ disease in ourcohort was 33 (2 patients) which is in accordanceto data previously published by our group [4] Unfor-tunately neither the analysis of the early kinetics ofCMV plasma DNAemia in the absence of antiviraltherapy nor the assessment of the dynamics of CMVplasma DNA load following the instauration of anti-viral treatment in these 2 episodes allowed for the an-ticipation of the development of CMV end-organdisease Obviously no definitive conclusions can bedrawn from these data given the limited number ofcases subjected to analysis
This study has 2 main limitations First thenumber of patients included in the cohort may havebeen insufficient to assess precisely the impact of
pretransplant and clinical factors on the kinetics ofCMVDNAemia Second there might be certain inac-curacies in the CMV DNAemia kinetics calculationsbecause of insufficient frequency of sampling In thisrespect there is no consensus as to what should bethe frequency of CMV DNA load monitoring duringepisodes of active CMV infection in the allo-SCT set-ting our data seemed to support the idea that theschedule of once-a-week monitoring is probably safeas long as a highly sensitive PCR is used for the surveil-lance of CMV infection Nevertheless it may also bereasonable to implement the twice-a-week schedulefor high-risk patients such as those receiving an unre-lated or HLA-mismatched graft (including recipientsof umbilical cord blood transplants) in whom the dou-bling time of CMV during the episodes of viral repli-cation is clearly faster
In summary in the current study we further char-acterized the dynamics of CMV DNAemia duringinitial and recurrent episodes of active CMV infectionin the allo-SCT setting The data reported hereinshould be taken into consideration for the design ofpreemptive antiviral therapy strategies based on viro-logic monitoring
ACKNOWLEDGMENTS
We thank Julia Garcıa and Monica Reig for theirtechnical assistance
Financial disclosureThis research was supported bya grant (091117) from FIS (Fondo de InvestigacionesSanitarias Ministerio de Sanidad y Consumo Spain)
AUTHORrsquoS CONTRIBUTIONS
BM-C ECMAC andDB did PCR analysesand assisted in the analysis of the data CS IBMJR and JM analyzed the data and attended thepatients DN designed the study analyzed the dataand wrote the paper
REFERENCES
1 Ljungman P CMV infections after hematopoietic stem celltransplantation Bone Marrow Transplant 200842S70-S72
2 Solano C Navarro D Clinical virology of cytomegalovirusinfection following hematopoietic transplantation Future Virol20105111-124
3 Boeckh M Ljungman P How we treat cytomegalovirus inhematopoietic cell transplant recipients Blood 20091135711-5719
4 Gimeno C Solano C Latorre JC et al Quantification of DNAin plasma by an automated real-time PCR assay (cytomegalovi-rus PCR kit) for surveillance of active cytomegalovirus infectionand guidance of preemptive therapy for allogeneic hematopoi-etic stem cell transplant recipients J Clin Microbiol 2008463311-3318
5 Halfon P Berger P Khiri H et al Algorithm based on CMVkinetics DNA viral load for preemptive therapy initiation after
Biol Blood Marrow Transplant 171602-1611 2011 1611Kinetics of CMV Plasma DNAemia in Allo-SCT
hematopoietic cell transplantation J Med Virol 201183490-495
6 Ljungman PWouldmonitoring CMV immune responses allowimproved control of CMV in stem cell transplant patients J ClinVirol 200635493-495
7 Avetisyan G Aschan J Heuroagglund H Ringden O Ljungman PEvaluation of intervention strategy based on CMV-specificimmune responses after allogeneic SCT Bone Marrow Trans-plant 200740865-869
8 GorD Sabin C PrenticeHG et al Longitudinal fluctuations incytomegalovirus load in bone marrow transplant patients rela-tionship between peak virus load donorrecipient serostatusacute GVHD and CMV disease Bone Marrow Transplant199821597-605
9 Emery VC Sabin CA Cope AV Gor D Hassan-Walker AFGriffiths PD Application of viral-load kinetics to identifypatients who develop cytomegalovirus disease after transplanta-tion Lancet 20003552032-2036
10 Avetisyan G Larsson K Aschan J Nilsson C Hassan MLjungman P Impact on the cytomegalovirus (CMV) viral load byCMV-specific T-cell immunity in recipients of allogeneic stemcell transplantation Bone Marrow Transplant 200638687-692
11 Stachel D Kirby K Corey L Boeckh M Viral load as predictorfor transplant-related mortality in the era of pre-emptive ther-apy Bone Marrow Transplant 200841S46
12 Buyck HC Griffiths PD Emery VC Human cytomegalovirus(HCMV) replication kinetics in stem cell transplant recipientsfollowing anti-HCMV therapy J Clin Virol 20104932-36
13 Torre-Cisneros J Caston-Osorio JJ Martın C et al Impact ofinitial cytomegalovirus viral load on efficacy of preemptive ther-apy with ganciclovir in allogeneic stem cell transplant recipientsEnferm Infecc Microbiol Clin 2010286-12
14 Chilet M Aguilar G Benet I et al Virological and immunolog-ical features of active cytomegalovirus infection in nonimmuno-suppressed patients in a surgical and trauma intensive care unitJ Med Virol 2010821384-1391
15 Ljungman P Griffiths P Paya C Definitions of HCMV infec-tion and disease in transplant recipients Clin Infect Dis 2002341094-1097
16 TormoN Solano C de la Camara R et al An assessment of theeffect of human herpesvirus-6 replication on active cytomegalo-virus infection after allogeneic stem cell transplantation BiolBlood Marrow Transplant 201016653-661
17 Emery VC Cope AV Bowen EF Gor D Griffiths PD The dy-namics of human cytomegalovirus replication in vivo J ExpMed1999190177-182
18 Humar A Kumar D Boivin G Caliendo AM Cytomegalovirus(CMV) virus load kinetics to predict recurrent disease in solid-organ transplant patients with CMV disease J Infect Dis 2002186829-833
19 BoeckhMHuangM Ferrenberg J et al Optimization of quan-titative detection of cytomegalovirus DNA in plasma by real-time PCR J Clin Microbiol 2004421142-1148
20 BoeckhM Gooley TA MyersonD CunninghamT Schoch GBowden RA Cytomegalovirus pp65 antigenemia-guided earlytreatment with ganciclovir versus ganciclovir at engraftment af-ter allogeneic marrow transplantation a randomized double-blind study Blood 1996884063-4071
21 Nichols WG Corey L Gooley T et al Rising pp65 antigene-mia during preemptive anticytomegalovirus therapy afterallogeneic hematopoietic stem cell transplantation risk factorscorrelation with DNA load and outcomes Blood 200197867-874
22 Gerna G Lilleri D Zecca M et al Rising antigenemia levelsmay be misleading in pre-emptive therapy of human cytomega-lovirus infection in allogeneic hematopoietic stem cell transplantrecipients Haematologica 200590526-533
23 TormoN Solano C Benet I et al Lack of prompt expansion ofcytomegalovirus pp65 and IE-1-specific IFNgamma CD81 andCD41 T cells is associated with rising levels of pp65 antigene-mia and DNAemia during pre-emptive therapy in allogeneichematopoietic stem cell transplant recipients Bone MarrowTransplant 201045543-549
24 Tormo N Solano C Benet I et al Kinetics of cytomegalovirus(CMV) pp65 and IE-1-specific IFNgamma CD81 and CD41T cells during episodes of viral DNAemia in allogeneic stemcell transplant recipients potential implications for the manage-ment of active CMV infection J Med Virol 2010821208-1215
25 FosterAEGottliebDJ SartorMHertzbergMS BradstockKFCytomegalovirus-specific CD41 and CD81 T-cells followa similar reconstitution pattern after allogeneic stem cell trans-plantation Biol Blood Marrow Transplant 20028501-511
26 Hakki M Riddell SR Storek J et al Immune reconstitution tocytomegalovirus after allogeneic stem cell transplantationimpact of host factors drug therapy and subclinical reactivationBlood 20031023060-3067
27 Lilleri D Fornara C Chiesa A Caldera D Alessandrino EPGerna G Human cytomegalovirus-specific CD41 and CD81T-cell reconstitution in adult allogeneic hematopoietic stemcell transplant recipients and immune control of viral infectionHaematologica 200893248-256
28 Pourgheysari B Piper KP McLarnon A et al Early reconstitu-tion of effector memory CD41 CMV-specific T cells protectsagainst CMV reactivation following allogeneic SCT BoneMarrow Transplant 200943853-861
29 Zhou W Longmate J Lacey SF et al Impact of donor CMVstatus on viral infection and reconstitution of multifunctionCMV-specific T cells in CMV-positive transplant recipientsBlood 20091136465-6476
30 TormoN SolanoC Benet I et al Reconstitution of CMVpp65and IE-1-specific IFN-gCD8(1) and CD4(1) T-cell responsesaffording protection fromCMVDNAemia following allogeneichematopoietic SCT Bone Marrow Transplant 2011 Jan 17[Epub ahead of print]
31 San Juan R Aguado JM Lumbreras C et al Impact of currenttransplantation management on the development of cytomega-lovirus disease after renal transplantation Clin Infect Dis 200847875-882
32 Moorman NJ Shenk T Rapamycin-resistant mTORC1 kinaseactivity is required for herpesvirus replication J Virol 2010845260-5269
33 Gratama JW Boeckh M Nakamura R et al Immune monitor-ing with iTAg MHC Tetramers for prediction of recurrent orpersistent cytomegalovirus infection or disease in allogeneichematopoietic stem cell transplant recipients a prospectivemulticenter study Blood 20101161655-1662
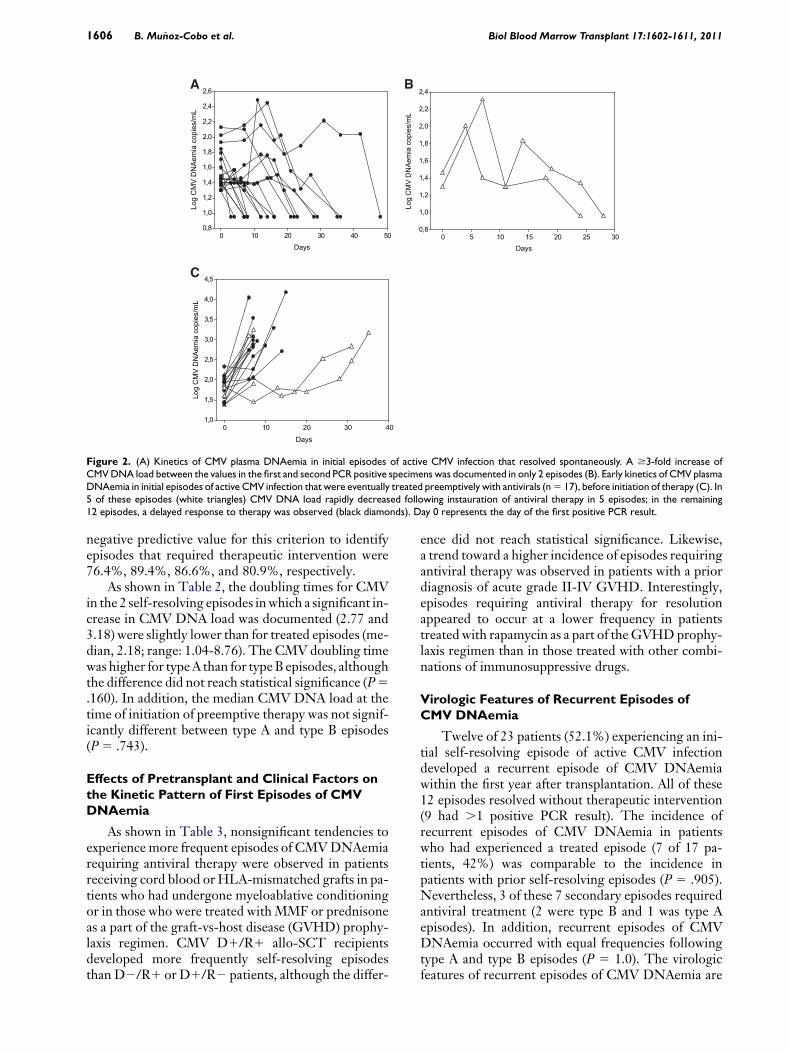
Days0 10 20 30 40 50
Lmseipoc
aimeA
NDVMCgoL
08
10
12
14
16
18
20
22
24
26
Days0 5 10 15 20 25 30
Lmseipoc
aimeA
NDVMCgoL
08
10
12
14
16
18
20
22
24
Days0 10 20 30 40
Lmseipoc
aimeA
NDVMCgoL
10
15
20
25
30
35
40
45
Figure 2 (A) Kinetics of CMV plasma DNAemia in initial episodes of active CMV infection that resolved spontaneously A $3-fold increase ofCMVDNA load between the values in the first and second PCR positive specimens was documented in only 2 episodes (B) Early kinetics of CMV plasmaDNAemia in initial episodes of active CMV infection that were eventually treated preemptively with antivirals (n5 17) before initiation of therapy (C) In5 of these episodes (white triangles) CMV DNA load rapidly decreased following instauration of antiviral therapy in 5 episodes in the remaining12 episodes a delayed response to therapy was observed (black diamonds) Day 0 represents the day of the first positive PCR result
1606 Biol Blood Marrow Transplant 171602-1611 2011B Mu~noz-Cobo et al
negative predictive value for this criterion to identifyepisodes that required therapeutic intervention were764 894 866 and 809 respectively
As shown in Table 2 the doubling times for CMVin the 2 self-resolving episodes inwhich a significant in-crease in CMV DNA load was documented (277 and318) were slightly lower than for treated episodes (me-dian 218 range 104-876) The CMV doubling timewas higher for typeA than for typeB episodes althoughthe difference did not reach statistical significance (P5160) In addition the median CMV DNA load at thetime of initiation of preemptive therapy was not signif-icantly different between type A and type B episodes(P 5 743)
Effects of Pretransplant and Clinical Factors onthe Kinetic Pattern of First Episodes of CMVDNAemia
As shown in Table 3 nonsignificant tendencies toexperience more frequent episodes of CMVDNAemiarequiring antiviral therapy were observed in patientsreceiving cord blood orHLA-mismatched grafts in pa-tients who had undergone myeloablative conditioningor in those who were treated with MMF or prednisoneas a part of the graft-vs-host disease (GVHD) prophy-laxis regimen CMV D1R1 allo-SCT recipientsdeveloped more frequently self-resolving episodesthan D2R1 or D1R2 patients although the differ-
ence did not reach statistical significance Likewisea trend toward a higher incidence of episodes requiringantiviral therapy was observed in patients with a priordiagnosis of acute grade II-IV GVHD Interestinglyepisodes requiring antiviral therapy for resolutionappeared to occur at a lower frequency in patientstreated with rapamycin as a part of theGVHDprophy-laxis regimen than in those treated with other combi-nations of immunosuppressive drugs
Virologic Features of Recurrent Episodes ofCMV DNAemia
Twelve of 23 patients (521) experiencing an ini-tial self-resolving episode of active CMV infectiondeveloped a recurrent episode of CMV DNAemiawithin the first year after transplantation All of these12 episodes resolved without therapeutic intervention(9 had 1 positive PCR result) The incidence ofrecurrent episodes of CMV DNAemia in patientswho had experienced a treated episode (7 of 17 pa-tients 42) was comparable to the incidence inpatients with prior self-resolving episodes (P 5 905)Nevertheless 3 of these 7 secondary episodes requiredantiviral treatment (2 were type B and 1 was type Aepisodes) In addition recurrent episodes of CMVDNAemia occurred with equal frequencies followingtype A and type B episodes (P 5 10) The virologicfeatures of recurrent episodes of CMV DNAemia are
Table 4 Virologic Features of Recurrent Episodes of CMVPlasma DNAemia
Virologic Parameter
Type of Episode
P ValueSelf-Resolving Treated
Initial VL (copiesmL) 25 (20-63) 35 (28-161) 054Peak VL (copiesmL) 43 (22-477) 1012 (5674-1395) 002Duration (days) 19 (6-67) 34 (26-35) 295Day of first + PCR 96 (54-260) 160 (96-180) 421
VL indicates CMV DNA loadFigures are given as median numbers (range)As determined by the Mann-Whitney U-test A P value 05 was con-sidered statistically significant
Table 3 Effects of Pretransplant and Clinical Factors on theOccurrence of Self-Resolving or Treated Initial Episodes ofCytomegalovirus (CMV) DNAemia
Factor
No of Patients with ActiveCMV Infection ()
P ValueTotal Self-Resolving Treated
CMV-serostatusD+R+ 21 13 (619) 8 (381)D2R+ 16 9 (562) 7 (438)D+R2 3 1 (250) 2 (750) 623
Type of donorand HLA match
Relatedmatched 17 10 (588) 7 (412)Relatedmismatched 2 0 (00) 2 (1000)Unrelatedmatched 13 9 (692) 4 (308)Unrelatedmismatched 8 4 (500) 4 (500) 388
Stem cells sourcePeripheral blood 32 19 (593) 13 (407)Cord blood 8 4 (500) 4 (500) 702
ConditioningMyeloablative 19 10 (526) 9 (474)Nonmyeloablative 21 13 (619) 8 (391) 750
GVHD prophylaxisCSA + MTX 20 14 (650) 6 (350)CSA + MMF 9 4 (444) 5 (556)RapamycinTacrolimus 7 5 (714) 2 (296)CSA + PDN 2 0 (00) 2 (1000) 123
Acute GVHDdaggerGrades 0-I 25 14 (560) 11 (440)Grades II-IV 10 5 (500) 5 (500) 10
D indicates donor R recipient CSA cyclosporine A MTX methotrex-ate MMF mycophenolate mofetil PDN prednisoneFrequency comparisons were carried out using the chi-square test(Fisherrsquos exact test) A P value05was considered statistically significantdaggerOnly those cases in which acute GVHD occurred before detection ofCMV DNAemia were considered for analysis
Biol Blood Marrow Transplant 171602-1611 2011 1607Kinetics of CMV Plasma DNAemia in Allo-SCT
summarized in Table 4 The duration of treatedepisodes was longer than that of self-resolvingepisodes although statistical significance was notreached As for first episodes the initial CMV DNAload in recurrent episodes was significantly higher inself-resolving episodes than in treated episodesalthough again a high degree of overlap was observedNevertheless in contrast to what was observed ininitial episodes variation in CMV DNA load betweenbaseline levels and those measured in the second pos-itive PCR did not allow for discrimination between
Days0 20 40 60
Lmseipoc
aimeA
NDVMCgoL
08
10
12
14
16
18
20
22
24
26
28
Lmseipoc
aimeA
NDVMCgoL
1
1
1
1
2
2
2
2
2
3
3
3
Figure 3 (A) Kinetics of CMV plasma DNAemia in recurrent episodes of aplasma DNAemia in initial episodes of active CMV infection that required preethe day of the first positive PCR result
episodes resolving spontaneously (Figure 3A) andthose requiring antiviral therapy (Figure 3B) In factsignificant variations between measurements wereobserved in none out of 9 self-resolving episodeswith more than 1 positive PCR result and in 1 of 3 ep-isodes eventually treated (Figure 3B) The CMVDNAload decay rate in these episodes was a median of024 day21 (range 016-059 day21) which corre-sponded to a median half-life of 285 days (range117-410 days) The kinetics of CMV DNAemiaclearance for secondary episodes that resolved sponta-neously did not follow an exponential decay function(not shown)
Effects of Pretransplant and Clinical Factorson the Incidence of Recurrent Episodes of CMVDNAemia
A trend toward a more frequent occurrence ofrecurrent episodes of CMV DNAemia was observedin CMV D2R1 patients and in the setting of unre-latedmismatched and umbilical cord blood allo-SCTThe differences however did not reach statisticalsignificance (Table 5)
Kinetics of CMV Plasma DNAemia in Patientswith CMV End-Organ Disease
Two patients developed CMV end-organ disease(enteritis) within the first 100 days after transplantationBoth received unrelatedHLA-matched peripheral
Days0 5 10 15 20
2
4
6
8
0
2
4
6
8
0
2
4
ctive CMV infection that resolved spontaneously (B) Kinetics of CMVmptive antiviral therapy before initiation of treatment Day 0 represents
Table 5 Effects of Pretransplant and Clinical Factors on theIncidence of Recurrent Episodes of Cytomegalovirus (CMV)DNAemia within the Study Period
Factor
Recurrent Episode of CMVDNAemia No of Patients ()
P ValueYes No
CMV-serostatusD+R+ 9 (428) 12 (572)D2R+ 10 (625) 6 (375)D+R2 0 (0) 3 (100) 111
Type of donorand HLA match
Relatedmatched 8 (470) 9 (530)Relatedmismatched 0 (0) 2 (100)Unrelatedmatched 6 (461) 7 (539)Unrelatedmismatched 5 (625) 3 (375) 655
Stem cells sourcePeripheral blood 14 (437) 18 (563)Cord blood 5 (625) 3 (375) 442
ConditioningMyeloablative 10 (526) 9 (474)Nonmyeloablative 9 (428) 12 (572) 752
GVHD prophylaxisCSA + MTX 10 (500) 10 (500)CSA + MMF 5 (555) 4 (455)RapamycinTacrolimus 4 (571) 3 (429)CSA + PDN 0 (0) 2 (100) 123
Acute GVHDdaggerGrades 0-I 14 (560) 11 (440)Grades II-IV 7 (466) 8 (534) 504
D indicates donor R recipient CSA cyclosporine A MTX Methotrex-ate MMF mycophenolate mofetil PDN prednisoneFrequency comparisons were carried out using the chi-square test(Fisherrsquos exact test) A P value05 was considered statistically significantdaggerOnly those cases in which acute GVHD occurred before detection ofCMV DNAemia were considered for analysis
1608 Biol Blood Marrow Transplant 171602-1611 2011B Mu~noz-Cobo et al
blood stemcell graftswere conditionedwith anonmye-loablative regimen (fludarabine plus melphalan) andwere treated with cyclosporine A and methotrexate forprophylaxis of GVHD CMV-serostatus of donorsand recipients were D1R1 in 1 case and D2R1 inthe other Neither of these patients developed acuteGVHD (aGVHD) Both patients had low initialCMVDNAemia levels (91 and 28 copiesmL) A signif-icant increase in CMV DNA load before initiation ofantiviral therapy was observed in 1 of these episodes(dt 5 25 days) Both episodes (type B) were treatedwith iv ganciclovir and had a duration of 102 and87 days respectively The peak of CMV DNAemiawas reached at days 121 (66329 copiesmL) and130 (35431 copiesmL) respectively after the firstpositivePCRresultBothpatientsdevelopedarecurrentepisode of CMV DNAemia
DISCUSSION
In the current study we took advantage of a highlysensitive real-time PCR and a relatively conservativestrategy for initiation of preemptive antiviral therapy(500CMVDNA copiesmL in plasma) to investigate
whether the analysis of the kinetics of CMVDNAemiamay yield useful information for the therapeutic man-agement of active CMV infection in the allo-SCTsetting In our cohort the overall rate of CMV DNA-emia was exceedingly high (almost 70) which wasmost likely related not only to the sensitivity of thePCR assay employed for the surveillance of CMVinfection but also to the high-risk profile of the studygroup In effect almost 50 of patients received anunrelated andor HLA-mismatched graft and 44of CMV-seropositive patients received a graft froma CMV-seronegative donor These pretransplant con-ditions have been consistently associated with a highincidence of active CMV infection in the allo-SCTsetting [2] More than half of the initial episodes ofCMV DNAemia resolved spontaneously The dura-tion of self-resolving episodes of CMV DNAemiawas significantly shorter than that for episodes thatwere eventually treated Yet these episodes lasted fora median of 16 days This finding should encouragestudies aimed at determining the impact of low-levelCMV replication which is permitted when initiationof antiviral treatment is delayed until a certain CMVDNAemia threshold is reached (usually between 500to 1000 CMV DNA copiesmL) on the incidenceand severity of indirect effects linked to CMV [12]
For most self-resolving episodes the kinetics ofCMVplasmaDNA clearance did not follow a logarith-mic decay curve in fact either fluctuating or ratherstable levels of CMV DNA loads were observed untilresolution In agreement with data recently publishedby Buyck et al [12] the Kdecline for CMVDNA load inepisodes that resolved without antiviral therapy waslower than that observed in episodes that requiredantiviral treatment for resolution Accordingly thehalf-life of CMV DNA load was shorter in the formerepisodes Notably whole-blood samples were ana-lyzed in the study by Buyck et al [12] whereas plasmaspecimens were used in the current study
First we asked whether the initial CMV plasmaDNA load value (first positive PCR result) may allowfor discrimination between episodes eventually requir-ing antiviral therapy from those resolving without theneed of antiviral treatment If this were the case theinitiation of preemptive therapy could be anticipatedperhaps leading to a more rapid resolution of theepisode and thereby minimizing the potential deleteri-ous effects of continuous CMV replication Eventhough the median initial CMV DNA load was signif-icantly lower for self-resolving episodes than for thosethat required antiviral therapy for clearance we founda high degree of overlap among values measured inboth groups It is known that the coefficient of varia-tion of PCR assays for CMV DNA loads close to thelimit of detection as were most of the initial valuesin our patients may be as high as 30 [19] In lightof the above observations the data suggested that
Biol Blood Marrow Transplant 171602-1611 2011 1609Kinetics of CMV Plasma DNAemia in Allo-SCT
a threshold value for the initial CMV DNA load reli-ably predicting the subsequent kinetics of CMVDNAemia is unlikely to be established at least whenusing highly sensitive real-time PCR assays such asthe method employed in the current study for moni-toring of active CMV infection In this sense it mustbe noted that initial CMV DNA loads measured inthis study were below the limit of detection of mostcommercially available real-time PCRs [2]
We next sought to determine whether the compar-ison between CMV DNA loads measured at baseline(initial viral load) and shortly thereafter (second posi-tive PCRmdasha median of 6 days after the first positivePCR result)mdashwould allow for identification ofepisodes eventually requiring antiviral treatment Wefound significant increases of CMV DNA load($3-fold) in 76 of episodes eventually requiringantiviral treatment but in 10 of self-resolvingepisodes The use of the above criterion would haveidentified the episodes that eventually required anti-viral treatment with a high sensitivity specificity andpositive and negative predictive values In our cohortthis strategy would have allowed for the anticipationof the initiation of antiviral treatment in only 2 epi-sodes (3 and 7 days) because the second CMV DNA-emia value measured was above the established cutofffor initiation of antiviral therapy nevertheless a largernumber of patients (6 of 13) would have benefited fromthis strategy had a higher CMV DNAemia level(1000 copiesmL) been set as the threshold for the ini-tiation of antiviral therapy as in other transplant cen-ters In light of these findings studies designed todetermine whether anticipation of preemptive therapybased on the above criterion would lead to a reductionin the cumulative dose of antivirals administered or toany clinically significant benefit are warranted Priorstudies have proposed CMV plasma DNA levelincreases of 174 copiesmLday [5] or 266 copies be-tween 2 consecutive determinations drawn a medianof 7 days apart [4] to discriminate between episodesthat required preemptive treatment and those thatdid not These estimations nevertheless were madein the setting of a preemptive strategy consisting ofthe initiation of antiviral therapy upon detection ofany level of pp65 antigenemia In addition Boeckhand Ljungman [3] proposed an increase of $5-foldfor initiation of preemptive therapy in low-riskallo-SCT recipients To our knowledge no data onthe clinical efficacy and safety of such strategies havebeen published
Preemptive antiviral therapy results in most casesin a rapid decline of CMV DNA load (type A episodesin the current study) nevertheless increasing levels ofCMV DNAemia early after the initiation of antiviraltherapy (type B episodes in this study) are occasionallydocumented [20-23] This paradoxical phenomenonhas been related to a lack of prompt expansion of
functional CMV-specific T cells in response to viralreplication [23] The occurrence of episodes witha delayed response to antiviral therapy is associatedwith an increased risk of CMV end-organ disease[12] Thus early recognition of this type of episodewould allow for rapid therapeutic interventionperhaps including the use of adoptive immunotherapyin order to reduce the risk of CMV-related morbidityIn this context Buyck et al [12] found a significantlyhigher mean growth rate and higher baseline viralload at the initiation of therapy in episodes witha delayed response to therapy with respect to thosewith an immediate response to therapy whereas theinitial CMV DNA load appeared to be comparablefor both type of episodes Our data partly agree withthose of Buyck et al [12] In effect the CMV doublingtime was lower in type B than in type A episodesalthough statistical significance was not reached andthe initial CMV DNA load did not differ significantlybetween both types of episodes Nevertheless in con-trast to the data reported in the above study baselineCMV DNA loads at the time of initiation of preemp-tive therapy did not differ significantly between bothtypes of episodes Thus in our experience the analysisof the early kinetics ofCMVDNAemia did not allowusto consistently identify the episodes of active CMVinfection with a delayed response to antiviral therapyDiscrepancies between our data and those of Buycket al [12] may be related to several factors includingthe use of different specimens for CMV DNA quanti-fication the use of distinct CMV DNA thresholds fortriggering the initiation of preemptive therapy andthe extensive use of Campath-1H in their study
Recurrent episodes of active CMV infectionoccurred with a comparable frequency among patientswho had an initial self-resolving episode and those whodeveloped an initial preemptively treated episodeNevertheless the likelihood of experiencing a second-ary episode that required antiviral therapy was higherin patients who had developed a treated episode thanin those who had experienced a self-resolving episodeIn agreement with a previous study [12] the risk ofrecurrence was not associated with the rate of CMVDNA decline in primary treated episodes followinginitiation of therapy As for initial episodes the base-line CMV DNA load in secondary episodes did notallow for a prediction of the subsequent kinetics ofCMV DNAemia Nevertheless in contrast to initialepisodes variation in CMV DNA load between base-line levels and those measured in the second positivePCR did not allow for discrimination between epi-sodes resolving spontaneously and those requiringantiviral therapy As ultimate control of CMV replica-tion depends upon adequate expansion of functionalCMV-specific T cells [2324] the above findinglikely reflected a more efficient and prompt T cellresponse in secondary episodes
1610 Biol Blood Marrow Transplant 171602-1611 2011B Mu~noz-Cobo et al
We were interested in assessing the impact ofseveral pretransplant and posttransplant clinical factorson the kinetics ofCMVDNAemia during first episodesof activeCMV infection and the incidence of recurrentepisodes Although we found no significant associa-tions a trend toward a higher frequency of episodesthat required antiviral therapy was observed in CMVD2R1 recipients in patients who received umbilicalcord blood or HLA-mismatched grafts in those whoreceived mycophenolate mofetil or prednisone(1 mgkgday) as a part of the GVHD prophylaxisregimen and in patients who were treated with highdoses of corticosteroids (1 mgkgday) for grades IIto IV GVHD These findings were not unexpected asall the above conditions have been shown to be associ-ated with delayed CMV-specific immune recovery[25-30] In this context it has previously been shownthat the magnitude and promptness of the expansionof functional CMV-specific CD81 and CD41 T cellsin response to CMV replication critically determinethe kinetics of CMV DNAemia clearance [23] Inter-estingly the use of rapamycin for the prevention ofGVHD was clearly associated with a relatively lowincidence of episodes that required antiviral treatmentThe scarce number of patients treated with this drug inour cohort did not allow to draw definitive conclusionson this issue nevertheless this effect has been previ-ously documented in the solid organ transplantationsetting [31] and is likely because of a direct inhibitoryeffect of rapamycin on viral replication [32]
Delayed recovery of CMV-specific T immunityhas been shown to be a significant risk factor for thedevelopment of recurrent episodes of active CMVinfection in allo-SCT recipients [3033] In supportof this view we found that CMV D2R1 recipientsand patients who underwent unrelatedmismatchedor umbilical cord blood allo-SCT tended to experi-ence recurrent episodes of active CMV infectionwith higher frequencies As mentioned above all thesepretransplant and clinical conditions have been previ-ously documented to be associated with an impairmentof CMV-specific T cell recovery
The incidence of CMV end-organ disease in ourcohort was 33 (2 patients) which is in accordanceto data previously published by our group [4] Unfor-tunately neither the analysis of the early kinetics ofCMV plasma DNAemia in the absence of antiviraltherapy nor the assessment of the dynamics of CMVplasma DNA load following the instauration of anti-viral treatment in these 2 episodes allowed for the an-ticipation of the development of CMV end-organdisease Obviously no definitive conclusions can bedrawn from these data given the limited number ofcases subjected to analysis
This study has 2 main limitations First thenumber of patients included in the cohort may havebeen insufficient to assess precisely the impact of
pretransplant and clinical factors on the kinetics ofCMVDNAemia Second there might be certain inac-curacies in the CMV DNAemia kinetics calculationsbecause of insufficient frequency of sampling In thisrespect there is no consensus as to what should bethe frequency of CMV DNA load monitoring duringepisodes of active CMV infection in the allo-SCT set-ting our data seemed to support the idea that theschedule of once-a-week monitoring is probably safeas long as a highly sensitive PCR is used for the surveil-lance of CMV infection Nevertheless it may also bereasonable to implement the twice-a-week schedulefor high-risk patients such as those receiving an unre-lated or HLA-mismatched graft (including recipientsof umbilical cord blood transplants) in whom the dou-bling time of CMV during the episodes of viral repli-cation is clearly faster
In summary in the current study we further char-acterized the dynamics of CMV DNAemia duringinitial and recurrent episodes of active CMV infectionin the allo-SCT setting The data reported hereinshould be taken into consideration for the design ofpreemptive antiviral therapy strategies based on viro-logic monitoring
ACKNOWLEDGMENTS
We thank Julia Garcıa and Monica Reig for theirtechnical assistance
Financial disclosureThis research was supported bya grant (091117) from FIS (Fondo de InvestigacionesSanitarias Ministerio de Sanidad y Consumo Spain)
AUTHORrsquoS CONTRIBUTIONS
BM-C ECMAC andDB did PCR analysesand assisted in the analysis of the data CS IBMJR and JM analyzed the data and attended thepatients DN designed the study analyzed the dataand wrote the paper
REFERENCES
1 Ljungman P CMV infections after hematopoietic stem celltransplantation Bone Marrow Transplant 200842S70-S72
2 Solano C Navarro D Clinical virology of cytomegalovirusinfection following hematopoietic transplantation Future Virol20105111-124
3 Boeckh M Ljungman P How we treat cytomegalovirus inhematopoietic cell transplant recipients Blood 20091135711-5719
4 Gimeno C Solano C Latorre JC et al Quantification of DNAin plasma by an automated real-time PCR assay (cytomegalovi-rus PCR kit) for surveillance of active cytomegalovirus infectionand guidance of preemptive therapy for allogeneic hematopoi-etic stem cell transplant recipients J Clin Microbiol 2008463311-3318
5 Halfon P Berger P Khiri H et al Algorithm based on CMVkinetics DNA viral load for preemptive therapy initiation after
Biol Blood Marrow Transplant 171602-1611 2011 1611Kinetics of CMV Plasma DNAemia in Allo-SCT
hematopoietic cell transplantation J Med Virol 201183490-495
6 Ljungman PWouldmonitoring CMV immune responses allowimproved control of CMV in stem cell transplant patients J ClinVirol 200635493-495
7 Avetisyan G Aschan J Heuroagglund H Ringden O Ljungman PEvaluation of intervention strategy based on CMV-specificimmune responses after allogeneic SCT Bone Marrow Trans-plant 200740865-869
8 GorD Sabin C PrenticeHG et al Longitudinal fluctuations incytomegalovirus load in bone marrow transplant patients rela-tionship between peak virus load donorrecipient serostatusacute GVHD and CMV disease Bone Marrow Transplant199821597-605
9 Emery VC Sabin CA Cope AV Gor D Hassan-Walker AFGriffiths PD Application of viral-load kinetics to identifypatients who develop cytomegalovirus disease after transplanta-tion Lancet 20003552032-2036
10 Avetisyan G Larsson K Aschan J Nilsson C Hassan MLjungman P Impact on the cytomegalovirus (CMV) viral load byCMV-specific T-cell immunity in recipients of allogeneic stemcell transplantation Bone Marrow Transplant 200638687-692
11 Stachel D Kirby K Corey L Boeckh M Viral load as predictorfor transplant-related mortality in the era of pre-emptive ther-apy Bone Marrow Transplant 200841S46
12 Buyck HC Griffiths PD Emery VC Human cytomegalovirus(HCMV) replication kinetics in stem cell transplant recipientsfollowing anti-HCMV therapy J Clin Virol 20104932-36
13 Torre-Cisneros J Caston-Osorio JJ Martın C et al Impact ofinitial cytomegalovirus viral load on efficacy of preemptive ther-apy with ganciclovir in allogeneic stem cell transplant recipientsEnferm Infecc Microbiol Clin 2010286-12
14 Chilet M Aguilar G Benet I et al Virological and immunolog-ical features of active cytomegalovirus infection in nonimmuno-suppressed patients in a surgical and trauma intensive care unitJ Med Virol 2010821384-1391
15 Ljungman P Griffiths P Paya C Definitions of HCMV infec-tion and disease in transplant recipients Clin Infect Dis 2002341094-1097
16 TormoN Solano C de la Camara R et al An assessment of theeffect of human herpesvirus-6 replication on active cytomegalo-virus infection after allogeneic stem cell transplantation BiolBlood Marrow Transplant 201016653-661
17 Emery VC Cope AV Bowen EF Gor D Griffiths PD The dy-namics of human cytomegalovirus replication in vivo J ExpMed1999190177-182
18 Humar A Kumar D Boivin G Caliendo AM Cytomegalovirus(CMV) virus load kinetics to predict recurrent disease in solid-organ transplant patients with CMV disease J Infect Dis 2002186829-833
19 BoeckhMHuangM Ferrenberg J et al Optimization of quan-titative detection of cytomegalovirus DNA in plasma by real-time PCR J Clin Microbiol 2004421142-1148
20 BoeckhM Gooley TA MyersonD CunninghamT Schoch GBowden RA Cytomegalovirus pp65 antigenemia-guided earlytreatment with ganciclovir versus ganciclovir at engraftment af-ter allogeneic marrow transplantation a randomized double-blind study Blood 1996884063-4071
21 Nichols WG Corey L Gooley T et al Rising pp65 antigene-mia during preemptive anticytomegalovirus therapy afterallogeneic hematopoietic stem cell transplantation risk factorscorrelation with DNA load and outcomes Blood 200197867-874
22 Gerna G Lilleri D Zecca M et al Rising antigenemia levelsmay be misleading in pre-emptive therapy of human cytomega-lovirus infection in allogeneic hematopoietic stem cell transplantrecipients Haematologica 200590526-533
23 TormoN Solano C Benet I et al Lack of prompt expansion ofcytomegalovirus pp65 and IE-1-specific IFNgamma CD81 andCD41 T cells is associated with rising levels of pp65 antigene-mia and DNAemia during pre-emptive therapy in allogeneichematopoietic stem cell transplant recipients Bone MarrowTransplant 201045543-549
24 Tormo N Solano C Benet I et al Kinetics of cytomegalovirus(CMV) pp65 and IE-1-specific IFNgamma CD81 and CD41T cells during episodes of viral DNAemia in allogeneic stemcell transplant recipients potential implications for the manage-ment of active CMV infection J Med Virol 2010821208-1215
25 FosterAEGottliebDJ SartorMHertzbergMS BradstockKFCytomegalovirus-specific CD41 and CD81 T-cells followa similar reconstitution pattern after allogeneic stem cell trans-plantation Biol Blood Marrow Transplant 20028501-511
26 Hakki M Riddell SR Storek J et al Immune reconstitution tocytomegalovirus after allogeneic stem cell transplantationimpact of host factors drug therapy and subclinical reactivationBlood 20031023060-3067
27 Lilleri D Fornara C Chiesa A Caldera D Alessandrino EPGerna G Human cytomegalovirus-specific CD41 and CD81T-cell reconstitution in adult allogeneic hematopoietic stemcell transplant recipients and immune control of viral infectionHaematologica 200893248-256
28 Pourgheysari B Piper KP McLarnon A et al Early reconstitu-tion of effector memory CD41 CMV-specific T cells protectsagainst CMV reactivation following allogeneic SCT BoneMarrow Transplant 200943853-861
29 Zhou W Longmate J Lacey SF et al Impact of donor CMVstatus on viral infection and reconstitution of multifunctionCMV-specific T cells in CMV-positive transplant recipientsBlood 20091136465-6476
30 TormoN SolanoC Benet I et al Reconstitution of CMVpp65and IE-1-specific IFN-gCD8(1) and CD4(1) T-cell responsesaffording protection fromCMVDNAemia following allogeneichematopoietic SCT Bone Marrow Transplant 2011 Jan 17[Epub ahead of print]
31 San Juan R Aguado JM Lumbreras C et al Impact of currenttransplantation management on the development of cytomega-lovirus disease after renal transplantation Clin Infect Dis 200847875-882
32 Moorman NJ Shenk T Rapamycin-resistant mTORC1 kinaseactivity is required for herpesvirus replication J Virol 2010845260-5269
33 Gratama JW Boeckh M Nakamura R et al Immune monitor-ing with iTAg MHC Tetramers for prediction of recurrent orpersistent cytomegalovirus infection or disease in allogeneichematopoietic stem cell transplant recipients a prospectivemulticenter study Blood 20101161655-1662
Table 4 Virologic Features of Recurrent Episodes of CMVPlasma DNAemia
Virologic Parameter
Type of Episode
P ValueSelf-Resolving Treated
Initial VL (copiesmL) 25 (20-63) 35 (28-161) 054Peak VL (copiesmL) 43 (22-477) 1012 (5674-1395) 002Duration (days) 19 (6-67) 34 (26-35) 295Day of first + PCR 96 (54-260) 160 (96-180) 421
VL indicates CMV DNA loadFigures are given as median numbers (range)As determined by the Mann-Whitney U-test A P value 05 was con-sidered statistically significant
Table 3 Effects of Pretransplant and Clinical Factors on theOccurrence of Self-Resolving or Treated Initial Episodes ofCytomegalovirus (CMV) DNAemia
Factor
No of Patients with ActiveCMV Infection ()
P ValueTotal Self-Resolving Treated
CMV-serostatusD+R+ 21 13 (619) 8 (381)D2R+ 16 9 (562) 7 (438)D+R2 3 1 (250) 2 (750) 623
Type of donorand HLA match
Relatedmatched 17 10 (588) 7 (412)Relatedmismatched 2 0 (00) 2 (1000)Unrelatedmatched 13 9 (692) 4 (308)Unrelatedmismatched 8 4 (500) 4 (500) 388
Stem cells sourcePeripheral blood 32 19 (593) 13 (407)Cord blood 8 4 (500) 4 (500) 702
ConditioningMyeloablative 19 10 (526) 9 (474)Nonmyeloablative 21 13 (619) 8 (391) 750
GVHD prophylaxisCSA + MTX 20 14 (650) 6 (350)CSA + MMF 9 4 (444) 5 (556)RapamycinTacrolimus 7 5 (714) 2 (296)CSA + PDN 2 0 (00) 2 (1000) 123
Acute GVHDdaggerGrades 0-I 25 14 (560) 11 (440)Grades II-IV 10 5 (500) 5 (500) 10
D indicates donor R recipient CSA cyclosporine A MTX methotrex-ate MMF mycophenolate mofetil PDN prednisoneFrequency comparisons were carried out using the chi-square test(Fisherrsquos exact test) A P value05was considered statistically significantdaggerOnly those cases in which acute GVHD occurred before detection ofCMV DNAemia were considered for analysis
Biol Blood Marrow Transplant 171602-1611 2011 1607Kinetics of CMV Plasma DNAemia in Allo-SCT
summarized in Table 4 The duration of treatedepisodes was longer than that of self-resolvingepisodes although statistical significance was notreached As for first episodes the initial CMV DNAload in recurrent episodes was significantly higher inself-resolving episodes than in treated episodesalthough again a high degree of overlap was observedNevertheless in contrast to what was observed ininitial episodes variation in CMV DNA load betweenbaseline levels and those measured in the second pos-itive PCR did not allow for discrimination between
Days0 20 40 60
Lmseipoc
aimeA
NDVMCgoL
08
10
12
14
16
18
20
22
24
26
28
Lmseipoc
aimeA
NDVMCgoL
1
1
1
1
2
2
2
2
2
3
3
3
Figure 3 (A) Kinetics of CMV plasma DNAemia in recurrent episodes of aplasma DNAemia in initial episodes of active CMV infection that required preethe day of the first positive PCR result
episodes resolving spontaneously (Figure 3A) andthose requiring antiviral therapy (Figure 3B) In factsignificant variations between measurements wereobserved in none out of 9 self-resolving episodeswith more than 1 positive PCR result and in 1 of 3 ep-isodes eventually treated (Figure 3B) The CMVDNAload decay rate in these episodes was a median of024 day21 (range 016-059 day21) which corre-sponded to a median half-life of 285 days (range117-410 days) The kinetics of CMV DNAemiaclearance for secondary episodes that resolved sponta-neously did not follow an exponential decay function(not shown)
Effects of Pretransplant and Clinical Factorson the Incidence of Recurrent Episodes of CMVDNAemia
A trend toward a more frequent occurrence ofrecurrent episodes of CMV DNAemia was observedin CMV D2R1 patients and in the setting of unre-latedmismatched and umbilical cord blood allo-SCTThe differences however did not reach statisticalsignificance (Table 5)
Kinetics of CMV Plasma DNAemia in Patientswith CMV End-Organ Disease
Two patients developed CMV end-organ disease(enteritis) within the first 100 days after transplantationBoth received unrelatedHLA-matched peripheral
Days0 5 10 15 20
2
4
6
8
0
2
4
6
8
0
2
4
ctive CMV infection that resolved spontaneously (B) Kinetics of CMVmptive antiviral therapy before initiation of treatment Day 0 represents
Table 5 Effects of Pretransplant and Clinical Factors on theIncidence of Recurrent Episodes of Cytomegalovirus (CMV)DNAemia within the Study Period
Factor
Recurrent Episode of CMVDNAemia No of Patients ()
P ValueYes No
CMV-serostatusD+R+ 9 (428) 12 (572)D2R+ 10 (625) 6 (375)D+R2 0 (0) 3 (100) 111
Type of donorand HLA match
Relatedmatched 8 (470) 9 (530)Relatedmismatched 0 (0) 2 (100)Unrelatedmatched 6 (461) 7 (539)Unrelatedmismatched 5 (625) 3 (375) 655
Stem cells sourcePeripheral blood 14 (437) 18 (563)Cord blood 5 (625) 3 (375) 442
ConditioningMyeloablative 10 (526) 9 (474)Nonmyeloablative 9 (428) 12 (572) 752
GVHD prophylaxisCSA + MTX 10 (500) 10 (500)CSA + MMF 5 (555) 4 (455)RapamycinTacrolimus 4 (571) 3 (429)CSA + PDN 0 (0) 2 (100) 123
Acute GVHDdaggerGrades 0-I 14 (560) 11 (440)Grades II-IV 7 (466) 8 (534) 504
D indicates donor R recipient CSA cyclosporine A MTX Methotrex-ate MMF mycophenolate mofetil PDN prednisoneFrequency comparisons were carried out using the chi-square test(Fisherrsquos exact test) A P value05 was considered statistically significantdaggerOnly those cases in which acute GVHD occurred before detection ofCMV DNAemia were considered for analysis
1608 Biol Blood Marrow Transplant 171602-1611 2011B Mu~noz-Cobo et al
blood stemcell graftswere conditionedwith anonmye-loablative regimen (fludarabine plus melphalan) andwere treated with cyclosporine A and methotrexate forprophylaxis of GVHD CMV-serostatus of donorsand recipients were D1R1 in 1 case and D2R1 inthe other Neither of these patients developed acuteGVHD (aGVHD) Both patients had low initialCMVDNAemia levels (91 and 28 copiesmL) A signif-icant increase in CMV DNA load before initiation ofantiviral therapy was observed in 1 of these episodes(dt 5 25 days) Both episodes (type B) were treatedwith iv ganciclovir and had a duration of 102 and87 days respectively The peak of CMV DNAemiawas reached at days 121 (66329 copiesmL) and130 (35431 copiesmL) respectively after the firstpositivePCRresultBothpatientsdevelopedarecurrentepisode of CMV DNAemia
DISCUSSION
In the current study we took advantage of a highlysensitive real-time PCR and a relatively conservativestrategy for initiation of preemptive antiviral therapy(500CMVDNA copiesmL in plasma) to investigate
whether the analysis of the kinetics of CMVDNAemiamay yield useful information for the therapeutic man-agement of active CMV infection in the allo-SCTsetting In our cohort the overall rate of CMV DNA-emia was exceedingly high (almost 70) which wasmost likely related not only to the sensitivity of thePCR assay employed for the surveillance of CMVinfection but also to the high-risk profile of the studygroup In effect almost 50 of patients received anunrelated andor HLA-mismatched graft and 44of CMV-seropositive patients received a graft froma CMV-seronegative donor These pretransplant con-ditions have been consistently associated with a highincidence of active CMV infection in the allo-SCTsetting [2] More than half of the initial episodes ofCMV DNAemia resolved spontaneously The dura-tion of self-resolving episodes of CMV DNAemiawas significantly shorter than that for episodes thatwere eventually treated Yet these episodes lasted fora median of 16 days This finding should encouragestudies aimed at determining the impact of low-levelCMV replication which is permitted when initiationof antiviral treatment is delayed until a certain CMVDNAemia threshold is reached (usually between 500to 1000 CMV DNA copiesmL) on the incidenceand severity of indirect effects linked to CMV [12]
For most self-resolving episodes the kinetics ofCMVplasmaDNA clearance did not follow a logarith-mic decay curve in fact either fluctuating or ratherstable levels of CMV DNA loads were observed untilresolution In agreement with data recently publishedby Buyck et al [12] the Kdecline for CMVDNA load inepisodes that resolved without antiviral therapy waslower than that observed in episodes that requiredantiviral treatment for resolution Accordingly thehalf-life of CMV DNA load was shorter in the formerepisodes Notably whole-blood samples were ana-lyzed in the study by Buyck et al [12] whereas plasmaspecimens were used in the current study
First we asked whether the initial CMV plasmaDNA load value (first positive PCR result) may allowfor discrimination between episodes eventually requir-ing antiviral therapy from those resolving without theneed of antiviral treatment If this were the case theinitiation of preemptive therapy could be anticipatedperhaps leading to a more rapid resolution of theepisode and thereby minimizing the potential deleteri-ous effects of continuous CMV replication Eventhough the median initial CMV DNA load was signif-icantly lower for self-resolving episodes than for thosethat required antiviral therapy for clearance we founda high degree of overlap among values measured inboth groups It is known that the coefficient of varia-tion of PCR assays for CMV DNA loads close to thelimit of detection as were most of the initial valuesin our patients may be as high as 30 [19] In lightof the above observations the data suggested that
Biol Blood Marrow Transplant 171602-1611 2011 1609Kinetics of CMV Plasma DNAemia in Allo-SCT
a threshold value for the initial CMV DNA load reli-ably predicting the subsequent kinetics of CMVDNAemia is unlikely to be established at least whenusing highly sensitive real-time PCR assays such asthe method employed in the current study for moni-toring of active CMV infection In this sense it mustbe noted that initial CMV DNA loads measured inthis study were below the limit of detection of mostcommercially available real-time PCRs [2]
We next sought to determine whether the compar-ison between CMV DNA loads measured at baseline(initial viral load) and shortly thereafter (second posi-tive PCRmdasha median of 6 days after the first positivePCR result)mdashwould allow for identification ofepisodes eventually requiring antiviral treatment Wefound significant increases of CMV DNA load($3-fold) in 76 of episodes eventually requiringantiviral treatment but in 10 of self-resolvingepisodes The use of the above criterion would haveidentified the episodes that eventually required anti-viral treatment with a high sensitivity specificity andpositive and negative predictive values In our cohortthis strategy would have allowed for the anticipationof the initiation of antiviral treatment in only 2 epi-sodes (3 and 7 days) because the second CMV DNA-emia value measured was above the established cutofffor initiation of antiviral therapy nevertheless a largernumber of patients (6 of 13) would have benefited fromthis strategy had a higher CMV DNAemia level(1000 copiesmL) been set as the threshold for the ini-tiation of antiviral therapy as in other transplant cen-ters In light of these findings studies designed todetermine whether anticipation of preemptive therapybased on the above criterion would lead to a reductionin the cumulative dose of antivirals administered or toany clinically significant benefit are warranted Priorstudies have proposed CMV plasma DNA levelincreases of 174 copiesmLday [5] or 266 copies be-tween 2 consecutive determinations drawn a medianof 7 days apart [4] to discriminate between episodesthat required preemptive treatment and those thatdid not These estimations nevertheless were madein the setting of a preemptive strategy consisting ofthe initiation of antiviral therapy upon detection ofany level of pp65 antigenemia In addition Boeckhand Ljungman [3] proposed an increase of $5-foldfor initiation of preemptive therapy in low-riskallo-SCT recipients To our knowledge no data onthe clinical efficacy and safety of such strategies havebeen published
Preemptive antiviral therapy results in most casesin a rapid decline of CMV DNA load (type A episodesin the current study) nevertheless increasing levels ofCMV DNAemia early after the initiation of antiviraltherapy (type B episodes in this study) are occasionallydocumented [20-23] This paradoxical phenomenonhas been related to a lack of prompt expansion of
functional CMV-specific T cells in response to viralreplication [23] The occurrence of episodes witha delayed response to antiviral therapy is associatedwith an increased risk of CMV end-organ disease[12] Thus early recognition of this type of episodewould allow for rapid therapeutic interventionperhaps including the use of adoptive immunotherapyin order to reduce the risk of CMV-related morbidityIn this context Buyck et al [12] found a significantlyhigher mean growth rate and higher baseline viralload at the initiation of therapy in episodes witha delayed response to therapy with respect to thosewith an immediate response to therapy whereas theinitial CMV DNA load appeared to be comparablefor both type of episodes Our data partly agree withthose of Buyck et al [12] In effect the CMV doublingtime was lower in type B than in type A episodesalthough statistical significance was not reached andthe initial CMV DNA load did not differ significantlybetween both types of episodes Nevertheless in con-trast to the data reported in the above study baselineCMV DNA loads at the time of initiation of preemp-tive therapy did not differ significantly between bothtypes of episodes Thus in our experience the analysisof the early kinetics ofCMVDNAemia did not allowusto consistently identify the episodes of active CMVinfection with a delayed response to antiviral therapyDiscrepancies between our data and those of Buycket al [12] may be related to several factors includingthe use of different specimens for CMV DNA quanti-fication the use of distinct CMV DNA thresholds fortriggering the initiation of preemptive therapy andthe extensive use of Campath-1H in their study
Recurrent episodes of active CMV infectionoccurred with a comparable frequency among patientswho had an initial self-resolving episode and those whodeveloped an initial preemptively treated episodeNevertheless the likelihood of experiencing a second-ary episode that required antiviral therapy was higherin patients who had developed a treated episode thanin those who had experienced a self-resolving episodeIn agreement with a previous study [12] the risk ofrecurrence was not associated with the rate of CMVDNA decline in primary treated episodes followinginitiation of therapy As for initial episodes the base-line CMV DNA load in secondary episodes did notallow for a prediction of the subsequent kinetics ofCMV DNAemia Nevertheless in contrast to initialepisodes variation in CMV DNA load between base-line levels and those measured in the second positivePCR did not allow for discrimination between epi-sodes resolving spontaneously and those requiringantiviral therapy As ultimate control of CMV replica-tion depends upon adequate expansion of functionalCMV-specific T cells [2324] the above findinglikely reflected a more efficient and prompt T cellresponse in secondary episodes
1610 Biol Blood Marrow Transplant 171602-1611 2011B Mu~noz-Cobo et al
We were interested in assessing the impact ofseveral pretransplant and posttransplant clinical factorson the kinetics ofCMVDNAemia during first episodesof activeCMV infection and the incidence of recurrentepisodes Although we found no significant associa-tions a trend toward a higher frequency of episodesthat required antiviral therapy was observed in CMVD2R1 recipients in patients who received umbilicalcord blood or HLA-mismatched grafts in those whoreceived mycophenolate mofetil or prednisone(1 mgkgday) as a part of the GVHD prophylaxisregimen and in patients who were treated with highdoses of corticosteroids (1 mgkgday) for grades IIto IV GVHD These findings were not unexpected asall the above conditions have been shown to be associ-ated with delayed CMV-specific immune recovery[25-30] In this context it has previously been shownthat the magnitude and promptness of the expansionof functional CMV-specific CD81 and CD41 T cellsin response to CMV replication critically determinethe kinetics of CMV DNAemia clearance [23] Inter-estingly the use of rapamycin for the prevention ofGVHD was clearly associated with a relatively lowincidence of episodes that required antiviral treatmentThe scarce number of patients treated with this drug inour cohort did not allow to draw definitive conclusionson this issue nevertheless this effect has been previ-ously documented in the solid organ transplantationsetting [31] and is likely because of a direct inhibitoryeffect of rapamycin on viral replication [32]
Delayed recovery of CMV-specific T immunityhas been shown to be a significant risk factor for thedevelopment of recurrent episodes of active CMVinfection in allo-SCT recipients [3033] In supportof this view we found that CMV D2R1 recipientsand patients who underwent unrelatedmismatchedor umbilical cord blood allo-SCT tended to experi-ence recurrent episodes of active CMV infectionwith higher frequencies As mentioned above all thesepretransplant and clinical conditions have been previ-ously documented to be associated with an impairmentof CMV-specific T cell recovery
The incidence of CMV end-organ disease in ourcohort was 33 (2 patients) which is in accordanceto data previously published by our group [4] Unfor-tunately neither the analysis of the early kinetics ofCMV plasma DNAemia in the absence of antiviraltherapy nor the assessment of the dynamics of CMVplasma DNA load following the instauration of anti-viral treatment in these 2 episodes allowed for the an-ticipation of the development of CMV end-organdisease Obviously no definitive conclusions can bedrawn from these data given the limited number ofcases subjected to analysis
This study has 2 main limitations First thenumber of patients included in the cohort may havebeen insufficient to assess precisely the impact of
pretransplant and clinical factors on the kinetics ofCMVDNAemia Second there might be certain inac-curacies in the CMV DNAemia kinetics calculationsbecause of insufficient frequency of sampling In thisrespect there is no consensus as to what should bethe frequency of CMV DNA load monitoring duringepisodes of active CMV infection in the allo-SCT set-ting our data seemed to support the idea that theschedule of once-a-week monitoring is probably safeas long as a highly sensitive PCR is used for the surveil-lance of CMV infection Nevertheless it may also bereasonable to implement the twice-a-week schedulefor high-risk patients such as those receiving an unre-lated or HLA-mismatched graft (including recipientsof umbilical cord blood transplants) in whom the dou-bling time of CMV during the episodes of viral repli-cation is clearly faster
In summary in the current study we further char-acterized the dynamics of CMV DNAemia duringinitial and recurrent episodes of active CMV infectionin the allo-SCT setting The data reported hereinshould be taken into consideration for the design ofpreemptive antiviral therapy strategies based on viro-logic monitoring
ACKNOWLEDGMENTS
We thank Julia Garcıa and Monica Reig for theirtechnical assistance
Financial disclosureThis research was supported bya grant (091117) from FIS (Fondo de InvestigacionesSanitarias Ministerio de Sanidad y Consumo Spain)
AUTHORrsquoS CONTRIBUTIONS
BM-C ECMAC andDB did PCR analysesand assisted in the analysis of the data CS IBMJR and JM analyzed the data and attended thepatients DN designed the study analyzed the dataand wrote the paper
REFERENCES
1 Ljungman P CMV infections after hematopoietic stem celltransplantation Bone Marrow Transplant 200842S70-S72
2 Solano C Navarro D Clinical virology of cytomegalovirusinfection following hematopoietic transplantation Future Virol20105111-124
3 Boeckh M Ljungman P How we treat cytomegalovirus inhematopoietic cell transplant recipients Blood 20091135711-5719
4 Gimeno C Solano C Latorre JC et al Quantification of DNAin plasma by an automated real-time PCR assay (cytomegalovi-rus PCR kit) for surveillance of active cytomegalovirus infectionand guidance of preemptive therapy for allogeneic hematopoi-etic stem cell transplant recipients J Clin Microbiol 2008463311-3318
5 Halfon P Berger P Khiri H et al Algorithm based on CMVkinetics DNA viral load for preemptive therapy initiation after
Biol Blood Marrow Transplant 171602-1611 2011 1611Kinetics of CMV Plasma DNAemia in Allo-SCT
hematopoietic cell transplantation J Med Virol 201183490-495
6 Ljungman PWouldmonitoring CMV immune responses allowimproved control of CMV in stem cell transplant patients J ClinVirol 200635493-495
7 Avetisyan G Aschan J Heuroagglund H Ringden O Ljungman PEvaluation of intervention strategy based on CMV-specificimmune responses after allogeneic SCT Bone Marrow Trans-plant 200740865-869
8 GorD Sabin C PrenticeHG et al Longitudinal fluctuations incytomegalovirus load in bone marrow transplant patients rela-tionship between peak virus load donorrecipient serostatusacute GVHD and CMV disease Bone Marrow Transplant199821597-605
9 Emery VC Sabin CA Cope AV Gor D Hassan-Walker AFGriffiths PD Application of viral-load kinetics to identifypatients who develop cytomegalovirus disease after transplanta-tion Lancet 20003552032-2036
10 Avetisyan G Larsson K Aschan J Nilsson C Hassan MLjungman P Impact on the cytomegalovirus (CMV) viral load byCMV-specific T-cell immunity in recipients of allogeneic stemcell transplantation Bone Marrow Transplant 200638687-692
11 Stachel D Kirby K Corey L Boeckh M Viral load as predictorfor transplant-related mortality in the era of pre-emptive ther-apy Bone Marrow Transplant 200841S46
12 Buyck HC Griffiths PD Emery VC Human cytomegalovirus(HCMV) replication kinetics in stem cell transplant recipientsfollowing anti-HCMV therapy J Clin Virol 20104932-36
13 Torre-Cisneros J Caston-Osorio JJ Martın C et al Impact ofinitial cytomegalovirus viral load on efficacy of preemptive ther-apy with ganciclovir in allogeneic stem cell transplant recipientsEnferm Infecc Microbiol Clin 2010286-12
14 Chilet M Aguilar G Benet I et al Virological and immunolog-ical features of active cytomegalovirus infection in nonimmuno-suppressed patients in a surgical and trauma intensive care unitJ Med Virol 2010821384-1391
15 Ljungman P Griffiths P Paya C Definitions of HCMV infec-tion and disease in transplant recipients Clin Infect Dis 2002341094-1097
16 TormoN Solano C de la Camara R et al An assessment of theeffect of human herpesvirus-6 replication on active cytomegalo-virus infection after allogeneic stem cell transplantation BiolBlood Marrow Transplant 201016653-661
17 Emery VC Cope AV Bowen EF Gor D Griffiths PD The dy-namics of human cytomegalovirus replication in vivo J ExpMed1999190177-182
18 Humar A Kumar D Boivin G Caliendo AM Cytomegalovirus(CMV) virus load kinetics to predict recurrent disease in solid-organ transplant patients with CMV disease J Infect Dis 2002186829-833
19 BoeckhMHuangM Ferrenberg J et al Optimization of quan-titative detection of cytomegalovirus DNA in plasma by real-time PCR J Clin Microbiol 2004421142-1148
20 BoeckhM Gooley TA MyersonD CunninghamT Schoch GBowden RA Cytomegalovirus pp65 antigenemia-guided earlytreatment with ganciclovir versus ganciclovir at engraftment af-ter allogeneic marrow transplantation a randomized double-blind study Blood 1996884063-4071
21 Nichols WG Corey L Gooley T et al Rising pp65 antigene-mia during preemptive anticytomegalovirus therapy afterallogeneic hematopoietic stem cell transplantation risk factorscorrelation with DNA load and outcomes Blood 200197867-874
22 Gerna G Lilleri D Zecca M et al Rising antigenemia levelsmay be misleading in pre-emptive therapy of human cytomega-lovirus infection in allogeneic hematopoietic stem cell transplantrecipients Haematologica 200590526-533
23 TormoN Solano C Benet I et al Lack of prompt expansion ofcytomegalovirus pp65 and IE-1-specific IFNgamma CD81 andCD41 T cells is associated with rising levels of pp65 antigene-mia and DNAemia during pre-emptive therapy in allogeneichematopoietic stem cell transplant recipients Bone MarrowTransplant 201045543-549
24 Tormo N Solano C Benet I et al Kinetics of cytomegalovirus(CMV) pp65 and IE-1-specific IFNgamma CD81 and CD41T cells during episodes of viral DNAemia in allogeneic stemcell transplant recipients potential implications for the manage-ment of active CMV infection J Med Virol 2010821208-1215
25 FosterAEGottliebDJ SartorMHertzbergMS BradstockKFCytomegalovirus-specific CD41 and CD81 T-cells followa similar reconstitution pattern after allogeneic stem cell trans-plantation Biol Blood Marrow Transplant 20028501-511
26 Hakki M Riddell SR Storek J et al Immune reconstitution tocytomegalovirus after allogeneic stem cell transplantationimpact of host factors drug therapy and subclinical reactivationBlood 20031023060-3067
27 Lilleri D Fornara C Chiesa A Caldera D Alessandrino EPGerna G Human cytomegalovirus-specific CD41 and CD81T-cell reconstitution in adult allogeneic hematopoietic stemcell transplant recipients and immune control of viral infectionHaematologica 200893248-256
28 Pourgheysari B Piper KP McLarnon A et al Early reconstitu-tion of effector memory CD41 CMV-specific T cells protectsagainst CMV reactivation following allogeneic SCT BoneMarrow Transplant 200943853-861
29 Zhou W Longmate J Lacey SF et al Impact of donor CMVstatus on viral infection and reconstitution of multifunctionCMV-specific T cells in CMV-positive transplant recipientsBlood 20091136465-6476
30 TormoN SolanoC Benet I et al Reconstitution of CMVpp65and IE-1-specific IFN-gCD8(1) and CD4(1) T-cell responsesaffording protection fromCMVDNAemia following allogeneichematopoietic SCT Bone Marrow Transplant 2011 Jan 17[Epub ahead of print]
31 San Juan R Aguado JM Lumbreras C et al Impact of currenttransplantation management on the development of cytomega-lovirus disease after renal transplantation Clin Infect Dis 200847875-882
32 Moorman NJ Shenk T Rapamycin-resistant mTORC1 kinaseactivity is required for herpesvirus replication J Virol 2010845260-5269
33 Gratama JW Boeckh M Nakamura R et al Immune monitor-ing with iTAg MHC Tetramers for prediction of recurrent orpersistent cytomegalovirus infection or disease in allogeneichematopoietic stem cell transplant recipients a prospectivemulticenter study Blood 20101161655-1662
Table 5 Effects of Pretransplant and Clinical Factors on theIncidence of Recurrent Episodes of Cytomegalovirus (CMV)DNAemia within the Study Period
Factor
Recurrent Episode of CMVDNAemia No of Patients ()
P ValueYes No
CMV-serostatusD+R+ 9 (428) 12 (572)D2R+ 10 (625) 6 (375)D+R2 0 (0) 3 (100) 111
Type of donorand HLA match
Relatedmatched 8 (470) 9 (530)Relatedmismatched 0 (0) 2 (100)Unrelatedmatched 6 (461) 7 (539)Unrelatedmismatched 5 (625) 3 (375) 655
Stem cells sourcePeripheral blood 14 (437) 18 (563)Cord blood 5 (625) 3 (375) 442
ConditioningMyeloablative 10 (526) 9 (474)Nonmyeloablative 9 (428) 12 (572) 752
GVHD prophylaxisCSA + MTX 10 (500) 10 (500)CSA + MMF 5 (555) 4 (455)RapamycinTacrolimus 4 (571) 3 (429)CSA + PDN 0 (0) 2 (100) 123
Acute GVHDdaggerGrades 0-I 14 (560) 11 (440)Grades II-IV 7 (466) 8 (534) 504
D indicates donor R recipient CSA cyclosporine A MTX Methotrex-ate MMF mycophenolate mofetil PDN prednisoneFrequency comparisons were carried out using the chi-square test(Fisherrsquos exact test) A P value05 was considered statistically significantdaggerOnly those cases in which acute GVHD occurred before detection ofCMV DNAemia were considered for analysis
1608 Biol Blood Marrow Transplant 171602-1611 2011B Mu~noz-Cobo et al
blood stemcell graftswere conditionedwith anonmye-loablative regimen (fludarabine plus melphalan) andwere treated with cyclosporine A and methotrexate forprophylaxis of GVHD CMV-serostatus of donorsand recipients were D1R1 in 1 case and D2R1 inthe other Neither of these patients developed acuteGVHD (aGVHD) Both patients had low initialCMVDNAemia levels (91 and 28 copiesmL) A signif-icant increase in CMV DNA load before initiation ofantiviral therapy was observed in 1 of these episodes(dt 5 25 days) Both episodes (type B) were treatedwith iv ganciclovir and had a duration of 102 and87 days respectively The peak of CMV DNAemiawas reached at days 121 (66329 copiesmL) and130 (35431 copiesmL) respectively after the firstpositivePCRresultBothpatientsdevelopedarecurrentepisode of CMV DNAemia
DISCUSSION
In the current study we took advantage of a highlysensitive real-time PCR and a relatively conservativestrategy for initiation of preemptive antiviral therapy(500CMVDNA copiesmL in plasma) to investigate
whether the analysis of the kinetics of CMVDNAemiamay yield useful information for the therapeutic man-agement of active CMV infection in the allo-SCTsetting In our cohort the overall rate of CMV DNA-emia was exceedingly high (almost 70) which wasmost likely related not only to the sensitivity of thePCR assay employed for the surveillance of CMVinfection but also to the high-risk profile of the studygroup In effect almost 50 of patients received anunrelated andor HLA-mismatched graft and 44of CMV-seropositive patients received a graft froma CMV-seronegative donor These pretransplant con-ditions have been consistently associated with a highincidence of active CMV infection in the allo-SCTsetting [2] More than half of the initial episodes ofCMV DNAemia resolved spontaneously The dura-tion of self-resolving episodes of CMV DNAemiawas significantly shorter than that for episodes thatwere eventually treated Yet these episodes lasted fora median of 16 days This finding should encouragestudies aimed at determining the impact of low-levelCMV replication which is permitted when initiationof antiviral treatment is delayed until a certain CMVDNAemia threshold is reached (usually between 500to 1000 CMV DNA copiesmL) on the incidenceand severity of indirect effects linked to CMV [12]
For most self-resolving episodes the kinetics ofCMVplasmaDNA clearance did not follow a logarith-mic decay curve in fact either fluctuating or ratherstable levels of CMV DNA loads were observed untilresolution In agreement with data recently publishedby Buyck et al [12] the Kdecline for CMVDNA load inepisodes that resolved without antiviral therapy waslower than that observed in episodes that requiredantiviral treatment for resolution Accordingly thehalf-life of CMV DNA load was shorter in the formerepisodes Notably whole-blood samples were ana-lyzed in the study by Buyck et al [12] whereas plasmaspecimens were used in the current study
First we asked whether the initial CMV plasmaDNA load value (first positive PCR result) may allowfor discrimination between episodes eventually requir-ing antiviral therapy from those resolving without theneed of antiviral treatment If this were the case theinitiation of preemptive therapy could be anticipatedperhaps leading to a more rapid resolution of theepisode and thereby minimizing the potential deleteri-ous effects of continuous CMV replication Eventhough the median initial CMV DNA load was signif-icantly lower for self-resolving episodes than for thosethat required antiviral therapy for clearance we founda high degree of overlap among values measured inboth groups It is known that the coefficient of varia-tion of PCR assays for CMV DNA loads close to thelimit of detection as were most of the initial valuesin our patients may be as high as 30 [19] In lightof the above observations the data suggested that
Biol Blood Marrow Transplant 171602-1611 2011 1609Kinetics of CMV Plasma DNAemia in Allo-SCT
a threshold value for the initial CMV DNA load reli-ably predicting the subsequent kinetics of CMVDNAemia is unlikely to be established at least whenusing highly sensitive real-time PCR assays such asthe method employed in the current study for moni-toring of active CMV infection In this sense it mustbe noted that initial CMV DNA loads measured inthis study were below the limit of detection of mostcommercially available real-time PCRs [2]
We next sought to determine whether the compar-ison between CMV DNA loads measured at baseline(initial viral load) and shortly thereafter (second posi-tive PCRmdasha median of 6 days after the first positivePCR result)mdashwould allow for identification ofepisodes eventually requiring antiviral treatment Wefound significant increases of CMV DNA load($3-fold) in 76 of episodes eventually requiringantiviral treatment but in 10 of self-resolvingepisodes The use of the above criterion would haveidentified the episodes that eventually required anti-viral treatment with a high sensitivity specificity andpositive and negative predictive values In our cohortthis strategy would have allowed for the anticipationof the initiation of antiviral treatment in only 2 epi-sodes (3 and 7 days) because the second CMV DNA-emia value measured was above the established cutofffor initiation of antiviral therapy nevertheless a largernumber of patients (6 of 13) would have benefited fromthis strategy had a higher CMV DNAemia level(1000 copiesmL) been set as the threshold for the ini-tiation of antiviral therapy as in other transplant cen-ters In light of these findings studies designed todetermine whether anticipation of preemptive therapybased on the above criterion would lead to a reductionin the cumulative dose of antivirals administered or toany clinically significant benefit are warranted Priorstudies have proposed CMV plasma DNA levelincreases of 174 copiesmLday [5] or 266 copies be-tween 2 consecutive determinations drawn a medianof 7 days apart [4] to discriminate between episodesthat required preemptive treatment and those thatdid not These estimations nevertheless were madein the setting of a preemptive strategy consisting ofthe initiation of antiviral therapy upon detection ofany level of pp65 antigenemia In addition Boeckhand Ljungman [3] proposed an increase of $5-foldfor initiation of preemptive therapy in low-riskallo-SCT recipients To our knowledge no data onthe clinical efficacy and safety of such strategies havebeen published
Preemptive antiviral therapy results in most casesin a rapid decline of CMV DNA load (type A episodesin the current study) nevertheless increasing levels ofCMV DNAemia early after the initiation of antiviraltherapy (type B episodes in this study) are occasionallydocumented [20-23] This paradoxical phenomenonhas been related to a lack of prompt expansion of
functional CMV-specific T cells in response to viralreplication [23] The occurrence of episodes witha delayed response to antiviral therapy is associatedwith an increased risk of CMV end-organ disease[12] Thus early recognition of this type of episodewould allow for rapid therapeutic interventionperhaps including the use of adoptive immunotherapyin order to reduce the risk of CMV-related morbidityIn this context Buyck et al [12] found a significantlyhigher mean growth rate and higher baseline viralload at the initiation of therapy in episodes witha delayed response to therapy with respect to thosewith an immediate response to therapy whereas theinitial CMV DNA load appeared to be comparablefor both type of episodes Our data partly agree withthose of Buyck et al [12] In effect the CMV doublingtime was lower in type B than in type A episodesalthough statistical significance was not reached andthe initial CMV DNA load did not differ significantlybetween both types of episodes Nevertheless in con-trast to the data reported in the above study baselineCMV DNA loads at the time of initiation of preemp-tive therapy did not differ significantly between bothtypes of episodes Thus in our experience the analysisof the early kinetics ofCMVDNAemia did not allowusto consistently identify the episodes of active CMVinfection with a delayed response to antiviral therapyDiscrepancies between our data and those of Buycket al [12] may be related to several factors includingthe use of different specimens for CMV DNA quanti-fication the use of distinct CMV DNA thresholds fortriggering the initiation of preemptive therapy andthe extensive use of Campath-1H in their study
Recurrent episodes of active CMV infectionoccurred with a comparable frequency among patientswho had an initial self-resolving episode and those whodeveloped an initial preemptively treated episodeNevertheless the likelihood of experiencing a second-ary episode that required antiviral therapy was higherin patients who had developed a treated episode thanin those who had experienced a self-resolving episodeIn agreement with a previous study [12] the risk ofrecurrence was not associated with the rate of CMVDNA decline in primary treated episodes followinginitiation of therapy As for initial episodes the base-line CMV DNA load in secondary episodes did notallow for a prediction of the subsequent kinetics ofCMV DNAemia Nevertheless in contrast to initialepisodes variation in CMV DNA load between base-line levels and those measured in the second positivePCR did not allow for discrimination between epi-sodes resolving spontaneously and those requiringantiviral therapy As ultimate control of CMV replica-tion depends upon adequate expansion of functionalCMV-specific T cells [2324] the above findinglikely reflected a more efficient and prompt T cellresponse in secondary episodes
1610 Biol Blood Marrow Transplant 171602-1611 2011B Mu~noz-Cobo et al
We were interested in assessing the impact ofseveral pretransplant and posttransplant clinical factorson the kinetics ofCMVDNAemia during first episodesof activeCMV infection and the incidence of recurrentepisodes Although we found no significant associa-tions a trend toward a higher frequency of episodesthat required antiviral therapy was observed in CMVD2R1 recipients in patients who received umbilicalcord blood or HLA-mismatched grafts in those whoreceived mycophenolate mofetil or prednisone(1 mgkgday) as a part of the GVHD prophylaxisregimen and in patients who were treated with highdoses of corticosteroids (1 mgkgday) for grades IIto IV GVHD These findings were not unexpected asall the above conditions have been shown to be associ-ated with delayed CMV-specific immune recovery[25-30] In this context it has previously been shownthat the magnitude and promptness of the expansionof functional CMV-specific CD81 and CD41 T cellsin response to CMV replication critically determinethe kinetics of CMV DNAemia clearance [23] Inter-estingly the use of rapamycin for the prevention ofGVHD was clearly associated with a relatively lowincidence of episodes that required antiviral treatmentThe scarce number of patients treated with this drug inour cohort did not allow to draw definitive conclusionson this issue nevertheless this effect has been previ-ously documented in the solid organ transplantationsetting [31] and is likely because of a direct inhibitoryeffect of rapamycin on viral replication [32]
Delayed recovery of CMV-specific T immunityhas been shown to be a significant risk factor for thedevelopment of recurrent episodes of active CMVinfection in allo-SCT recipients [3033] In supportof this view we found that CMV D2R1 recipientsand patients who underwent unrelatedmismatchedor umbilical cord blood allo-SCT tended to experi-ence recurrent episodes of active CMV infectionwith higher frequencies As mentioned above all thesepretransplant and clinical conditions have been previ-ously documented to be associated with an impairmentof CMV-specific T cell recovery
The incidence of CMV end-organ disease in ourcohort was 33 (2 patients) which is in accordanceto data previously published by our group [4] Unfor-tunately neither the analysis of the early kinetics ofCMV plasma DNAemia in the absence of antiviraltherapy nor the assessment of the dynamics of CMVplasma DNA load following the instauration of anti-viral treatment in these 2 episodes allowed for the an-ticipation of the development of CMV end-organdisease Obviously no definitive conclusions can bedrawn from these data given the limited number ofcases subjected to analysis
This study has 2 main limitations First thenumber of patients included in the cohort may havebeen insufficient to assess precisely the impact of
pretransplant and clinical factors on the kinetics ofCMVDNAemia Second there might be certain inac-curacies in the CMV DNAemia kinetics calculationsbecause of insufficient frequency of sampling In thisrespect there is no consensus as to what should bethe frequency of CMV DNA load monitoring duringepisodes of active CMV infection in the allo-SCT set-ting our data seemed to support the idea that theschedule of once-a-week monitoring is probably safeas long as a highly sensitive PCR is used for the surveil-lance of CMV infection Nevertheless it may also bereasonable to implement the twice-a-week schedulefor high-risk patients such as those receiving an unre-lated or HLA-mismatched graft (including recipientsof umbilical cord blood transplants) in whom the dou-bling time of CMV during the episodes of viral repli-cation is clearly faster
In summary in the current study we further char-acterized the dynamics of CMV DNAemia duringinitial and recurrent episodes of active CMV infectionin the allo-SCT setting The data reported hereinshould be taken into consideration for the design ofpreemptive antiviral therapy strategies based on viro-logic monitoring
ACKNOWLEDGMENTS
We thank Julia Garcıa and Monica Reig for theirtechnical assistance
Financial disclosureThis research was supported bya grant (091117) from FIS (Fondo de InvestigacionesSanitarias Ministerio de Sanidad y Consumo Spain)
AUTHORrsquoS CONTRIBUTIONS
BM-C ECMAC andDB did PCR analysesand assisted in the analysis of the data CS IBMJR and JM analyzed the data and attended thepatients DN designed the study analyzed the dataand wrote the paper
REFERENCES
1 Ljungman P CMV infections after hematopoietic stem celltransplantation Bone Marrow Transplant 200842S70-S72
2 Solano C Navarro D Clinical virology of cytomegalovirusinfection following hematopoietic transplantation Future Virol20105111-124
3 Boeckh M Ljungman P How we treat cytomegalovirus inhematopoietic cell transplant recipients Blood 20091135711-5719
4 Gimeno C Solano C Latorre JC et al Quantification of DNAin plasma by an automated real-time PCR assay (cytomegalovi-rus PCR kit) for surveillance of active cytomegalovirus infectionand guidance of preemptive therapy for allogeneic hematopoi-etic stem cell transplant recipients J Clin Microbiol 2008463311-3318
5 Halfon P Berger P Khiri H et al Algorithm based on CMVkinetics DNA viral load for preemptive therapy initiation after
Biol Blood Marrow Transplant 171602-1611 2011 1611Kinetics of CMV Plasma DNAemia in Allo-SCT
hematopoietic cell transplantation J Med Virol 201183490-495
6 Ljungman PWouldmonitoring CMV immune responses allowimproved control of CMV in stem cell transplant patients J ClinVirol 200635493-495
7 Avetisyan G Aschan J Heuroagglund H Ringden O Ljungman PEvaluation of intervention strategy based on CMV-specificimmune responses after allogeneic SCT Bone Marrow Trans-plant 200740865-869
8 GorD Sabin C PrenticeHG et al Longitudinal fluctuations incytomegalovirus load in bone marrow transplant patients rela-tionship between peak virus load donorrecipient serostatusacute GVHD and CMV disease Bone Marrow Transplant199821597-605
9 Emery VC Sabin CA Cope AV Gor D Hassan-Walker AFGriffiths PD Application of viral-load kinetics to identifypatients who develop cytomegalovirus disease after transplanta-tion Lancet 20003552032-2036
10 Avetisyan G Larsson K Aschan J Nilsson C Hassan MLjungman P Impact on the cytomegalovirus (CMV) viral load byCMV-specific T-cell immunity in recipients of allogeneic stemcell transplantation Bone Marrow Transplant 200638687-692
11 Stachel D Kirby K Corey L Boeckh M Viral load as predictorfor transplant-related mortality in the era of pre-emptive ther-apy Bone Marrow Transplant 200841S46
12 Buyck HC Griffiths PD Emery VC Human cytomegalovirus(HCMV) replication kinetics in stem cell transplant recipientsfollowing anti-HCMV therapy J Clin Virol 20104932-36
13 Torre-Cisneros J Caston-Osorio JJ Martın C et al Impact ofinitial cytomegalovirus viral load on efficacy of preemptive ther-apy with ganciclovir in allogeneic stem cell transplant recipientsEnferm Infecc Microbiol Clin 2010286-12
14 Chilet M Aguilar G Benet I et al Virological and immunolog-ical features of active cytomegalovirus infection in nonimmuno-suppressed patients in a surgical and trauma intensive care unitJ Med Virol 2010821384-1391
15 Ljungman P Griffiths P Paya C Definitions of HCMV infec-tion and disease in transplant recipients Clin Infect Dis 2002341094-1097
16 TormoN Solano C de la Camara R et al An assessment of theeffect of human herpesvirus-6 replication on active cytomegalo-virus infection after allogeneic stem cell transplantation BiolBlood Marrow Transplant 201016653-661
17 Emery VC Cope AV Bowen EF Gor D Griffiths PD The dy-namics of human cytomegalovirus replication in vivo J ExpMed1999190177-182
18 Humar A Kumar D Boivin G Caliendo AM Cytomegalovirus(CMV) virus load kinetics to predict recurrent disease in solid-organ transplant patients with CMV disease J Infect Dis 2002186829-833
19 BoeckhMHuangM Ferrenberg J et al Optimization of quan-titative detection of cytomegalovirus DNA in plasma by real-time PCR J Clin Microbiol 2004421142-1148
20 BoeckhM Gooley TA MyersonD CunninghamT Schoch GBowden RA Cytomegalovirus pp65 antigenemia-guided earlytreatment with ganciclovir versus ganciclovir at engraftment af-ter allogeneic marrow transplantation a randomized double-blind study Blood 1996884063-4071
21 Nichols WG Corey L Gooley T et al Rising pp65 antigene-mia during preemptive anticytomegalovirus therapy afterallogeneic hematopoietic stem cell transplantation risk factorscorrelation with DNA load and outcomes Blood 200197867-874
22 Gerna G Lilleri D Zecca M et al Rising antigenemia levelsmay be misleading in pre-emptive therapy of human cytomega-lovirus infection in allogeneic hematopoietic stem cell transplantrecipients Haematologica 200590526-533
23 TormoN Solano C Benet I et al Lack of prompt expansion ofcytomegalovirus pp65 and IE-1-specific IFNgamma CD81 andCD41 T cells is associated with rising levels of pp65 antigene-mia and DNAemia during pre-emptive therapy in allogeneichematopoietic stem cell transplant recipients Bone MarrowTransplant 201045543-549
24 Tormo N Solano C Benet I et al Kinetics of cytomegalovirus(CMV) pp65 and IE-1-specific IFNgamma CD81 and CD41T cells during episodes of viral DNAemia in allogeneic stemcell transplant recipients potential implications for the manage-ment of active CMV infection J Med Virol 2010821208-1215
25 FosterAEGottliebDJ SartorMHertzbergMS BradstockKFCytomegalovirus-specific CD41 and CD81 T-cells followa similar reconstitution pattern after allogeneic stem cell trans-plantation Biol Blood Marrow Transplant 20028501-511
26 Hakki M Riddell SR Storek J et al Immune reconstitution tocytomegalovirus after allogeneic stem cell transplantationimpact of host factors drug therapy and subclinical reactivationBlood 20031023060-3067
27 Lilleri D Fornara C Chiesa A Caldera D Alessandrino EPGerna G Human cytomegalovirus-specific CD41 and CD81T-cell reconstitution in adult allogeneic hematopoietic stemcell transplant recipients and immune control of viral infectionHaematologica 200893248-256
28 Pourgheysari B Piper KP McLarnon A et al Early reconstitu-tion of effector memory CD41 CMV-specific T cells protectsagainst CMV reactivation following allogeneic SCT BoneMarrow Transplant 200943853-861
29 Zhou W Longmate J Lacey SF et al Impact of donor CMVstatus on viral infection and reconstitution of multifunctionCMV-specific T cells in CMV-positive transplant recipientsBlood 20091136465-6476
30 TormoN SolanoC Benet I et al Reconstitution of CMVpp65and IE-1-specific IFN-gCD8(1) and CD4(1) T-cell responsesaffording protection fromCMVDNAemia following allogeneichematopoietic SCT Bone Marrow Transplant 2011 Jan 17[Epub ahead of print]
31 San Juan R Aguado JM Lumbreras C et al Impact of currenttransplantation management on the development of cytomega-lovirus disease after renal transplantation Clin Infect Dis 200847875-882
32 Moorman NJ Shenk T Rapamycin-resistant mTORC1 kinaseactivity is required for herpesvirus replication J Virol 2010845260-5269
33 Gratama JW Boeckh M Nakamura R et al Immune monitor-ing with iTAg MHC Tetramers for prediction of recurrent orpersistent cytomegalovirus infection or disease in allogeneichematopoietic stem cell transplant recipients a prospectivemulticenter study Blood 20101161655-1662

Biol Blood Marrow Transplant 171602-1611 2011 1609Kinetics of CMV Plasma DNAemia in Allo-SCT
a threshold value for the initial CMV DNA load reli-ably predicting the subsequent kinetics of CMVDNAemia is unlikely to be established at least whenusing highly sensitive real-time PCR assays such asthe method employed in the current study for moni-toring of active CMV infection In this sense it mustbe noted that initial CMV DNA loads measured inthis study were below the limit of detection of mostcommercially available real-time PCRs [2]
We next sought to determine whether the compar-ison between CMV DNA loads measured at baseline(initial viral load) and shortly thereafter (second posi-tive PCRmdasha median of 6 days after the first positivePCR result)mdashwould allow for identification ofepisodes eventually requiring antiviral treatment Wefound significant increases of CMV DNA load($3-fold) in 76 of episodes eventually requiringantiviral treatment but in 10 of self-resolvingepisodes The use of the above criterion would haveidentified the episodes that eventually required anti-viral treatment with a high sensitivity specificity andpositive and negative predictive values In our cohortthis strategy would have allowed for the anticipationof the initiation of antiviral treatment in only 2 epi-sodes (3 and 7 days) because the second CMV DNA-emia value measured was above the established cutofffor initiation of antiviral therapy nevertheless a largernumber of patients (6 of 13) would have benefited fromthis strategy had a higher CMV DNAemia level(1000 copiesmL) been set as the threshold for the ini-tiation of antiviral therapy as in other transplant cen-ters In light of these findings studies designed todetermine whether anticipation of preemptive therapybased on the above criterion would lead to a reductionin the cumulative dose of antivirals administered or toany clinically significant benefit are warranted Priorstudies have proposed CMV plasma DNA levelincreases of 174 copiesmLday [5] or 266 copies be-tween 2 consecutive determinations drawn a medianof 7 days apart [4] to discriminate between episodesthat required preemptive treatment and those thatdid not These estimations nevertheless were madein the setting of a preemptive strategy consisting ofthe initiation of antiviral therapy upon detection ofany level of pp65 antigenemia In addition Boeckhand Ljungman [3] proposed an increase of $5-foldfor initiation of preemptive therapy in low-riskallo-SCT recipients To our knowledge no data onthe clinical efficacy and safety of such strategies havebeen published
Preemptive antiviral therapy results in most casesin a rapid decline of CMV DNA load (type A episodesin the current study) nevertheless increasing levels ofCMV DNAemia early after the initiation of antiviraltherapy (type B episodes in this study) are occasionallydocumented [20-23] This paradoxical phenomenonhas been related to a lack of prompt expansion of
functional CMV-specific T cells in response to viralreplication [23] The occurrence of episodes witha delayed response to antiviral therapy is associatedwith an increased risk of CMV end-organ disease[12] Thus early recognition of this type of episodewould allow for rapid therapeutic interventionperhaps including the use of adoptive immunotherapyin order to reduce the risk of CMV-related morbidityIn this context Buyck et al [12] found a significantlyhigher mean growth rate and higher baseline viralload at the initiation of therapy in episodes witha delayed response to therapy with respect to thosewith an immediate response to therapy whereas theinitial CMV DNA load appeared to be comparablefor both type of episodes Our data partly agree withthose of Buyck et al [12] In effect the CMV doublingtime was lower in type B than in type A episodesalthough statistical significance was not reached andthe initial CMV DNA load did not differ significantlybetween both types of episodes Nevertheless in con-trast to the data reported in the above study baselineCMV DNA loads at the time of initiation of preemp-tive therapy did not differ significantly between bothtypes of episodes Thus in our experience the analysisof the early kinetics ofCMVDNAemia did not allowusto consistently identify the episodes of active CMVinfection with a delayed response to antiviral therapyDiscrepancies between our data and those of Buycket al [12] may be related to several factors includingthe use of different specimens for CMV DNA quanti-fication the use of distinct CMV DNA thresholds fortriggering the initiation of preemptive therapy andthe extensive use of Campath-1H in their study
Recurrent episodes of active CMV infectionoccurred with a comparable frequency among patientswho had an initial self-resolving episode and those whodeveloped an initial preemptively treated episodeNevertheless the likelihood of experiencing a second-ary episode that required antiviral therapy was higherin patients who had developed a treated episode thanin those who had experienced a self-resolving episodeIn agreement with a previous study [12] the risk ofrecurrence was not associated with the rate of CMVDNA decline in primary treated episodes followinginitiation of therapy As for initial episodes the base-line CMV DNA load in secondary episodes did notallow for a prediction of the subsequent kinetics ofCMV DNAemia Nevertheless in contrast to initialepisodes variation in CMV DNA load between base-line levels and those measured in the second positivePCR did not allow for discrimination between epi-sodes resolving spontaneously and those requiringantiviral therapy As ultimate control of CMV replica-tion depends upon adequate expansion of functionalCMV-specific T cells [2324] the above findinglikely reflected a more efficient and prompt T cellresponse in secondary episodes
1610 Biol Blood Marrow Transplant 171602-1611 2011B Mu~noz-Cobo et al
We were interested in assessing the impact ofseveral pretransplant and posttransplant clinical factorson the kinetics ofCMVDNAemia during first episodesof activeCMV infection and the incidence of recurrentepisodes Although we found no significant associa-tions a trend toward a higher frequency of episodesthat required antiviral therapy was observed in CMVD2R1 recipients in patients who received umbilicalcord blood or HLA-mismatched grafts in those whoreceived mycophenolate mofetil or prednisone(1 mgkgday) as a part of the GVHD prophylaxisregimen and in patients who were treated with highdoses of corticosteroids (1 mgkgday) for grades IIto IV GVHD These findings were not unexpected asall the above conditions have been shown to be associ-ated with delayed CMV-specific immune recovery[25-30] In this context it has previously been shownthat the magnitude and promptness of the expansionof functional CMV-specific CD81 and CD41 T cellsin response to CMV replication critically determinethe kinetics of CMV DNAemia clearance [23] Inter-estingly the use of rapamycin for the prevention ofGVHD was clearly associated with a relatively lowincidence of episodes that required antiviral treatmentThe scarce number of patients treated with this drug inour cohort did not allow to draw definitive conclusionson this issue nevertheless this effect has been previ-ously documented in the solid organ transplantationsetting [31] and is likely because of a direct inhibitoryeffect of rapamycin on viral replication [32]
Delayed recovery of CMV-specific T immunityhas been shown to be a significant risk factor for thedevelopment of recurrent episodes of active CMVinfection in allo-SCT recipients [3033] In supportof this view we found that CMV D2R1 recipientsand patients who underwent unrelatedmismatchedor umbilical cord blood allo-SCT tended to experi-ence recurrent episodes of active CMV infectionwith higher frequencies As mentioned above all thesepretransplant and clinical conditions have been previ-ously documented to be associated with an impairmentof CMV-specific T cell recovery
The incidence of CMV end-organ disease in ourcohort was 33 (2 patients) which is in accordanceto data previously published by our group [4] Unfor-tunately neither the analysis of the early kinetics ofCMV plasma DNAemia in the absence of antiviraltherapy nor the assessment of the dynamics of CMVplasma DNA load following the instauration of anti-viral treatment in these 2 episodes allowed for the an-ticipation of the development of CMV end-organdisease Obviously no definitive conclusions can bedrawn from these data given the limited number ofcases subjected to analysis
This study has 2 main limitations First thenumber of patients included in the cohort may havebeen insufficient to assess precisely the impact of
pretransplant and clinical factors on the kinetics ofCMVDNAemia Second there might be certain inac-curacies in the CMV DNAemia kinetics calculationsbecause of insufficient frequency of sampling In thisrespect there is no consensus as to what should bethe frequency of CMV DNA load monitoring duringepisodes of active CMV infection in the allo-SCT set-ting our data seemed to support the idea that theschedule of once-a-week monitoring is probably safeas long as a highly sensitive PCR is used for the surveil-lance of CMV infection Nevertheless it may also bereasonable to implement the twice-a-week schedulefor high-risk patients such as those receiving an unre-lated or HLA-mismatched graft (including recipientsof umbilical cord blood transplants) in whom the dou-bling time of CMV during the episodes of viral repli-cation is clearly faster
In summary in the current study we further char-acterized the dynamics of CMV DNAemia duringinitial and recurrent episodes of active CMV infectionin the allo-SCT setting The data reported hereinshould be taken into consideration for the design ofpreemptive antiviral therapy strategies based on viro-logic monitoring
ACKNOWLEDGMENTS
We thank Julia Garcıa and Monica Reig for theirtechnical assistance
Financial disclosureThis research was supported bya grant (091117) from FIS (Fondo de InvestigacionesSanitarias Ministerio de Sanidad y Consumo Spain)
AUTHORrsquoS CONTRIBUTIONS
BM-C ECMAC andDB did PCR analysesand assisted in the analysis of the data CS IBMJR and JM analyzed the data and attended thepatients DN designed the study analyzed the dataand wrote the paper
REFERENCES
1 Ljungman P CMV infections after hematopoietic stem celltransplantation Bone Marrow Transplant 200842S70-S72
2 Solano C Navarro D Clinical virology of cytomegalovirusinfection following hematopoietic transplantation Future Virol20105111-124
3 Boeckh M Ljungman P How we treat cytomegalovirus inhematopoietic cell transplant recipients Blood 20091135711-5719
4 Gimeno C Solano C Latorre JC et al Quantification of DNAin plasma by an automated real-time PCR assay (cytomegalovi-rus PCR kit) for surveillance of active cytomegalovirus infectionand guidance of preemptive therapy for allogeneic hematopoi-etic stem cell transplant recipients J Clin Microbiol 2008463311-3318
5 Halfon P Berger P Khiri H et al Algorithm based on CMVkinetics DNA viral load for preemptive therapy initiation after
Biol Blood Marrow Transplant 171602-1611 2011 1611Kinetics of CMV Plasma DNAemia in Allo-SCT
hematopoietic cell transplantation J Med Virol 201183490-495
6 Ljungman PWouldmonitoring CMV immune responses allowimproved control of CMV in stem cell transplant patients J ClinVirol 200635493-495
7 Avetisyan G Aschan J Heuroagglund H Ringden O Ljungman PEvaluation of intervention strategy based on CMV-specificimmune responses after allogeneic SCT Bone Marrow Trans-plant 200740865-869
8 GorD Sabin C PrenticeHG et al Longitudinal fluctuations incytomegalovirus load in bone marrow transplant patients rela-tionship between peak virus load donorrecipient serostatusacute GVHD and CMV disease Bone Marrow Transplant199821597-605
9 Emery VC Sabin CA Cope AV Gor D Hassan-Walker AFGriffiths PD Application of viral-load kinetics to identifypatients who develop cytomegalovirus disease after transplanta-tion Lancet 20003552032-2036
10 Avetisyan G Larsson K Aschan J Nilsson C Hassan MLjungman P Impact on the cytomegalovirus (CMV) viral load byCMV-specific T-cell immunity in recipients of allogeneic stemcell transplantation Bone Marrow Transplant 200638687-692
11 Stachel D Kirby K Corey L Boeckh M Viral load as predictorfor transplant-related mortality in the era of pre-emptive ther-apy Bone Marrow Transplant 200841S46
12 Buyck HC Griffiths PD Emery VC Human cytomegalovirus(HCMV) replication kinetics in stem cell transplant recipientsfollowing anti-HCMV therapy J Clin Virol 20104932-36
13 Torre-Cisneros J Caston-Osorio JJ Martın C et al Impact ofinitial cytomegalovirus viral load on efficacy of preemptive ther-apy with ganciclovir in allogeneic stem cell transplant recipientsEnferm Infecc Microbiol Clin 2010286-12
14 Chilet M Aguilar G Benet I et al Virological and immunolog-ical features of active cytomegalovirus infection in nonimmuno-suppressed patients in a surgical and trauma intensive care unitJ Med Virol 2010821384-1391
15 Ljungman P Griffiths P Paya C Definitions of HCMV infec-tion and disease in transplant recipients Clin Infect Dis 2002341094-1097
16 TormoN Solano C de la Camara R et al An assessment of theeffect of human herpesvirus-6 replication on active cytomegalo-virus infection after allogeneic stem cell transplantation BiolBlood Marrow Transplant 201016653-661
17 Emery VC Cope AV Bowen EF Gor D Griffiths PD The dy-namics of human cytomegalovirus replication in vivo J ExpMed1999190177-182
18 Humar A Kumar D Boivin G Caliendo AM Cytomegalovirus(CMV) virus load kinetics to predict recurrent disease in solid-organ transplant patients with CMV disease J Infect Dis 2002186829-833
19 BoeckhMHuangM Ferrenberg J et al Optimization of quan-titative detection of cytomegalovirus DNA in plasma by real-time PCR J Clin Microbiol 2004421142-1148
20 BoeckhM Gooley TA MyersonD CunninghamT Schoch GBowden RA Cytomegalovirus pp65 antigenemia-guided earlytreatment with ganciclovir versus ganciclovir at engraftment af-ter allogeneic marrow transplantation a randomized double-blind study Blood 1996884063-4071
21 Nichols WG Corey L Gooley T et al Rising pp65 antigene-mia during preemptive anticytomegalovirus therapy afterallogeneic hematopoietic stem cell transplantation risk factorscorrelation with DNA load and outcomes Blood 200197867-874
22 Gerna G Lilleri D Zecca M et al Rising antigenemia levelsmay be misleading in pre-emptive therapy of human cytomega-lovirus infection in allogeneic hematopoietic stem cell transplantrecipients Haematologica 200590526-533
23 TormoN Solano C Benet I et al Lack of prompt expansion ofcytomegalovirus pp65 and IE-1-specific IFNgamma CD81 andCD41 T cells is associated with rising levels of pp65 antigene-mia and DNAemia during pre-emptive therapy in allogeneichematopoietic stem cell transplant recipients Bone MarrowTransplant 201045543-549
24 Tormo N Solano C Benet I et al Kinetics of cytomegalovirus(CMV) pp65 and IE-1-specific IFNgamma CD81 and CD41T cells during episodes of viral DNAemia in allogeneic stemcell transplant recipients potential implications for the manage-ment of active CMV infection J Med Virol 2010821208-1215
25 FosterAEGottliebDJ SartorMHertzbergMS BradstockKFCytomegalovirus-specific CD41 and CD81 T-cells followa similar reconstitution pattern after allogeneic stem cell trans-plantation Biol Blood Marrow Transplant 20028501-511
26 Hakki M Riddell SR Storek J et al Immune reconstitution tocytomegalovirus after allogeneic stem cell transplantationimpact of host factors drug therapy and subclinical reactivationBlood 20031023060-3067
27 Lilleri D Fornara C Chiesa A Caldera D Alessandrino EPGerna G Human cytomegalovirus-specific CD41 and CD81T-cell reconstitution in adult allogeneic hematopoietic stemcell transplant recipients and immune control of viral infectionHaematologica 200893248-256
28 Pourgheysari B Piper KP McLarnon A et al Early reconstitu-tion of effector memory CD41 CMV-specific T cells protectsagainst CMV reactivation following allogeneic SCT BoneMarrow Transplant 200943853-861
29 Zhou W Longmate J Lacey SF et al Impact of donor CMVstatus on viral infection and reconstitution of multifunctionCMV-specific T cells in CMV-positive transplant recipientsBlood 20091136465-6476
30 TormoN SolanoC Benet I et al Reconstitution of CMVpp65and IE-1-specific IFN-gCD8(1) and CD4(1) T-cell responsesaffording protection fromCMVDNAemia following allogeneichematopoietic SCT Bone Marrow Transplant 2011 Jan 17[Epub ahead of print]
31 San Juan R Aguado JM Lumbreras C et al Impact of currenttransplantation management on the development of cytomega-lovirus disease after renal transplantation Clin Infect Dis 200847875-882
32 Moorman NJ Shenk T Rapamycin-resistant mTORC1 kinaseactivity is required for herpesvirus replication J Virol 2010845260-5269
33 Gratama JW Boeckh M Nakamura R et al Immune monitor-ing with iTAg MHC Tetramers for prediction of recurrent orpersistent cytomegalovirus infection or disease in allogeneichematopoietic stem cell transplant recipients a prospectivemulticenter study Blood 20101161655-1662

1610 Biol Blood Marrow Transplant 171602-1611 2011B Mu~noz-Cobo et al
We were interested in assessing the impact ofseveral pretransplant and posttransplant clinical factorson the kinetics ofCMVDNAemia during first episodesof activeCMV infection and the incidence of recurrentepisodes Although we found no significant associa-tions a trend toward a higher frequency of episodesthat required antiviral therapy was observed in CMVD2R1 recipients in patients who received umbilicalcord blood or HLA-mismatched grafts in those whoreceived mycophenolate mofetil or prednisone(1 mgkgday) as a part of the GVHD prophylaxisregimen and in patients who were treated with highdoses of corticosteroids (1 mgkgday) for grades IIto IV GVHD These findings were not unexpected asall the above conditions have been shown to be associ-ated with delayed CMV-specific immune recovery[25-30] In this context it has previously been shownthat the magnitude and promptness of the expansionof functional CMV-specific CD81 and CD41 T cellsin response to CMV replication critically determinethe kinetics of CMV DNAemia clearance [23] Inter-estingly the use of rapamycin for the prevention ofGVHD was clearly associated with a relatively lowincidence of episodes that required antiviral treatmentThe scarce number of patients treated with this drug inour cohort did not allow to draw definitive conclusionson this issue nevertheless this effect has been previ-ously documented in the solid organ transplantationsetting [31] and is likely because of a direct inhibitoryeffect of rapamycin on viral replication [32]
Delayed recovery of CMV-specific T immunityhas been shown to be a significant risk factor for thedevelopment of recurrent episodes of active CMVinfection in allo-SCT recipients [3033] In supportof this view we found that CMV D2R1 recipientsand patients who underwent unrelatedmismatchedor umbilical cord blood allo-SCT tended to experi-ence recurrent episodes of active CMV infectionwith higher frequencies As mentioned above all thesepretransplant and clinical conditions have been previ-ously documented to be associated with an impairmentof CMV-specific T cell recovery
The incidence of CMV end-organ disease in ourcohort was 33 (2 patients) which is in accordanceto data previously published by our group [4] Unfor-tunately neither the analysis of the early kinetics ofCMV plasma DNAemia in the absence of antiviraltherapy nor the assessment of the dynamics of CMVplasma DNA load following the instauration of anti-viral treatment in these 2 episodes allowed for the an-ticipation of the development of CMV end-organdisease Obviously no definitive conclusions can bedrawn from these data given the limited number ofcases subjected to analysis
This study has 2 main limitations First thenumber of patients included in the cohort may havebeen insufficient to assess precisely the impact of
pretransplant and clinical factors on the kinetics ofCMVDNAemia Second there might be certain inac-curacies in the CMV DNAemia kinetics calculationsbecause of insufficient frequency of sampling In thisrespect there is no consensus as to what should bethe frequency of CMV DNA load monitoring duringepisodes of active CMV infection in the allo-SCT set-ting our data seemed to support the idea that theschedule of once-a-week monitoring is probably safeas long as a highly sensitive PCR is used for the surveil-lance of CMV infection Nevertheless it may also bereasonable to implement the twice-a-week schedulefor high-risk patients such as those receiving an unre-lated or HLA-mismatched graft (including recipientsof umbilical cord blood transplants) in whom the dou-bling time of CMV during the episodes of viral repli-cation is clearly faster
In summary in the current study we further char-acterized the dynamics of CMV DNAemia duringinitial and recurrent episodes of active CMV infectionin the allo-SCT setting The data reported hereinshould be taken into consideration for the design ofpreemptive antiviral therapy strategies based on viro-logic monitoring
ACKNOWLEDGMENTS
We thank Julia Garcıa and Monica Reig for theirtechnical assistance
Financial disclosureThis research was supported bya grant (091117) from FIS (Fondo de InvestigacionesSanitarias Ministerio de Sanidad y Consumo Spain)
AUTHORrsquoS CONTRIBUTIONS
BM-C ECMAC andDB did PCR analysesand assisted in the analysis of the data CS IBMJR and JM analyzed the data and attended thepatients DN designed the study analyzed the dataand wrote the paper
REFERENCES
1 Ljungman P CMV infections after hematopoietic stem celltransplantation Bone Marrow Transplant 200842S70-S72
2 Solano C Navarro D Clinical virology of cytomegalovirusinfection following hematopoietic transplantation Future Virol20105111-124
3 Boeckh M Ljungman P How we treat cytomegalovirus inhematopoietic cell transplant recipients Blood 20091135711-5719
4 Gimeno C Solano C Latorre JC et al Quantification of DNAin plasma by an automated real-time PCR assay (cytomegalovi-rus PCR kit) for surveillance of active cytomegalovirus infectionand guidance of preemptive therapy for allogeneic hematopoi-etic stem cell transplant recipients J Clin Microbiol 2008463311-3318
5 Halfon P Berger P Khiri H et al Algorithm based on CMVkinetics DNA viral load for preemptive therapy initiation after
Biol Blood Marrow Transplant 171602-1611 2011 1611Kinetics of CMV Plasma DNAemia in Allo-SCT
hematopoietic cell transplantation J Med Virol 201183490-495
6 Ljungman PWouldmonitoring CMV immune responses allowimproved control of CMV in stem cell transplant patients J ClinVirol 200635493-495
7 Avetisyan G Aschan J Heuroagglund H Ringden O Ljungman PEvaluation of intervention strategy based on CMV-specificimmune responses after allogeneic SCT Bone Marrow Trans-plant 200740865-869
8 GorD Sabin C PrenticeHG et al Longitudinal fluctuations incytomegalovirus load in bone marrow transplant patients rela-tionship between peak virus load donorrecipient serostatusacute GVHD and CMV disease Bone Marrow Transplant199821597-605
9 Emery VC Sabin CA Cope AV Gor D Hassan-Walker AFGriffiths PD Application of viral-load kinetics to identifypatients who develop cytomegalovirus disease after transplanta-tion Lancet 20003552032-2036
10 Avetisyan G Larsson K Aschan J Nilsson C Hassan MLjungman P Impact on the cytomegalovirus (CMV) viral load byCMV-specific T-cell immunity in recipients of allogeneic stemcell transplantation Bone Marrow Transplant 200638687-692
11 Stachel D Kirby K Corey L Boeckh M Viral load as predictorfor transplant-related mortality in the era of pre-emptive ther-apy Bone Marrow Transplant 200841S46
12 Buyck HC Griffiths PD Emery VC Human cytomegalovirus(HCMV) replication kinetics in stem cell transplant recipientsfollowing anti-HCMV therapy J Clin Virol 20104932-36
13 Torre-Cisneros J Caston-Osorio JJ Martın C et al Impact ofinitial cytomegalovirus viral load on efficacy of preemptive ther-apy with ganciclovir in allogeneic stem cell transplant recipientsEnferm Infecc Microbiol Clin 2010286-12
14 Chilet M Aguilar G Benet I et al Virological and immunolog-ical features of active cytomegalovirus infection in nonimmuno-suppressed patients in a surgical and trauma intensive care unitJ Med Virol 2010821384-1391
15 Ljungman P Griffiths P Paya C Definitions of HCMV infec-tion and disease in transplant recipients Clin Infect Dis 2002341094-1097
16 TormoN Solano C de la Camara R et al An assessment of theeffect of human herpesvirus-6 replication on active cytomegalo-virus infection after allogeneic stem cell transplantation BiolBlood Marrow Transplant 201016653-661
17 Emery VC Cope AV Bowen EF Gor D Griffiths PD The dy-namics of human cytomegalovirus replication in vivo J ExpMed1999190177-182
18 Humar A Kumar D Boivin G Caliendo AM Cytomegalovirus(CMV) virus load kinetics to predict recurrent disease in solid-organ transplant patients with CMV disease J Infect Dis 2002186829-833
19 BoeckhMHuangM Ferrenberg J et al Optimization of quan-titative detection of cytomegalovirus DNA in plasma by real-time PCR J Clin Microbiol 2004421142-1148
20 BoeckhM Gooley TA MyersonD CunninghamT Schoch GBowden RA Cytomegalovirus pp65 antigenemia-guided earlytreatment with ganciclovir versus ganciclovir at engraftment af-ter allogeneic marrow transplantation a randomized double-blind study Blood 1996884063-4071
21 Nichols WG Corey L Gooley T et al Rising pp65 antigene-mia during preemptive anticytomegalovirus therapy afterallogeneic hematopoietic stem cell transplantation risk factorscorrelation with DNA load and outcomes Blood 200197867-874
22 Gerna G Lilleri D Zecca M et al Rising antigenemia levelsmay be misleading in pre-emptive therapy of human cytomega-lovirus infection in allogeneic hematopoietic stem cell transplantrecipients Haematologica 200590526-533
23 TormoN Solano C Benet I et al Lack of prompt expansion ofcytomegalovirus pp65 and IE-1-specific IFNgamma CD81 andCD41 T cells is associated with rising levels of pp65 antigene-mia and DNAemia during pre-emptive therapy in allogeneichematopoietic stem cell transplant recipients Bone MarrowTransplant 201045543-549
24 Tormo N Solano C Benet I et al Kinetics of cytomegalovirus(CMV) pp65 and IE-1-specific IFNgamma CD81 and CD41T cells during episodes of viral DNAemia in allogeneic stemcell transplant recipients potential implications for the manage-ment of active CMV infection J Med Virol 2010821208-1215
25 FosterAEGottliebDJ SartorMHertzbergMS BradstockKFCytomegalovirus-specific CD41 and CD81 T-cells followa similar reconstitution pattern after allogeneic stem cell trans-plantation Biol Blood Marrow Transplant 20028501-511
26 Hakki M Riddell SR Storek J et al Immune reconstitution tocytomegalovirus after allogeneic stem cell transplantationimpact of host factors drug therapy and subclinical reactivationBlood 20031023060-3067
27 Lilleri D Fornara C Chiesa A Caldera D Alessandrino EPGerna G Human cytomegalovirus-specific CD41 and CD81T-cell reconstitution in adult allogeneic hematopoietic stemcell transplant recipients and immune control of viral infectionHaematologica 200893248-256
28 Pourgheysari B Piper KP McLarnon A et al Early reconstitu-tion of effector memory CD41 CMV-specific T cells protectsagainst CMV reactivation following allogeneic SCT BoneMarrow Transplant 200943853-861
29 Zhou W Longmate J Lacey SF et al Impact of donor CMVstatus on viral infection and reconstitution of multifunctionCMV-specific T cells in CMV-positive transplant recipientsBlood 20091136465-6476
30 TormoN SolanoC Benet I et al Reconstitution of CMVpp65and IE-1-specific IFN-gCD8(1) and CD4(1) T-cell responsesaffording protection fromCMVDNAemia following allogeneichematopoietic SCT Bone Marrow Transplant 2011 Jan 17[Epub ahead of print]
31 San Juan R Aguado JM Lumbreras C et al Impact of currenttransplantation management on the development of cytomega-lovirus disease after renal transplantation Clin Infect Dis 200847875-882
32 Moorman NJ Shenk T Rapamycin-resistant mTORC1 kinaseactivity is required for herpesvirus replication J Virol 2010845260-5269
33 Gratama JW Boeckh M Nakamura R et al Immune monitor-ing with iTAg MHC Tetramers for prediction of recurrent orpersistent cytomegalovirus infection or disease in allogeneichematopoietic stem cell transplant recipients a prospectivemulticenter study Blood 20101161655-1662
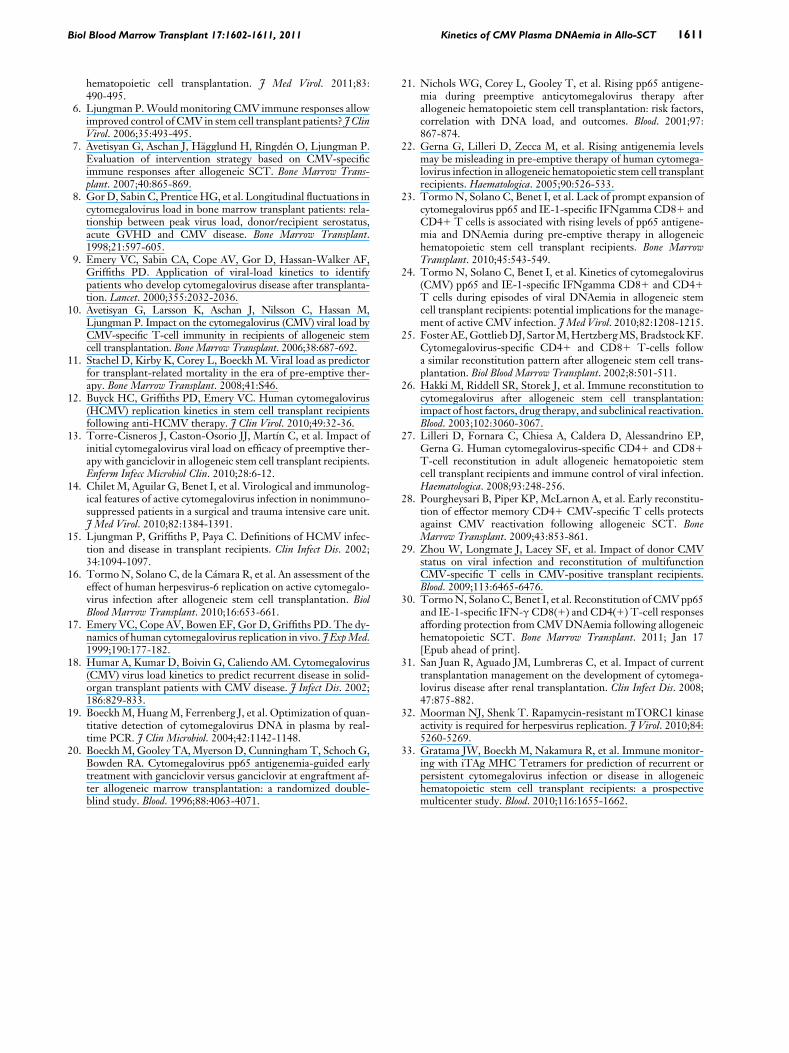
Biol Blood Marrow Transplant 171602-1611 2011 1611Kinetics of CMV Plasma DNAemia in Allo-SCT
hematopoietic cell transplantation J Med Virol 201183490-495
6 Ljungman PWouldmonitoring CMV immune responses allowimproved control of CMV in stem cell transplant patients J ClinVirol 200635493-495
7 Avetisyan G Aschan J Heuroagglund H Ringden O Ljungman PEvaluation of intervention strategy based on CMV-specificimmune responses after allogeneic SCT Bone Marrow Trans-plant 200740865-869
8 GorD Sabin C PrenticeHG et al Longitudinal fluctuations incytomegalovirus load in bone marrow transplant patients rela-tionship between peak virus load donorrecipient serostatusacute GVHD and CMV disease Bone Marrow Transplant199821597-605
9 Emery VC Sabin CA Cope AV Gor D Hassan-Walker AFGriffiths PD Application of viral-load kinetics to identifypatients who develop cytomegalovirus disease after transplanta-tion Lancet 20003552032-2036
10 Avetisyan G Larsson K Aschan J Nilsson C Hassan MLjungman P Impact on the cytomegalovirus (CMV) viral load byCMV-specific T-cell immunity in recipients of allogeneic stemcell transplantation Bone Marrow Transplant 200638687-692
11 Stachel D Kirby K Corey L Boeckh M Viral load as predictorfor transplant-related mortality in the era of pre-emptive ther-apy Bone Marrow Transplant 200841S46
12 Buyck HC Griffiths PD Emery VC Human cytomegalovirus(HCMV) replication kinetics in stem cell transplant recipientsfollowing anti-HCMV therapy J Clin Virol 20104932-36
13 Torre-Cisneros J Caston-Osorio JJ Martın C et al Impact ofinitial cytomegalovirus viral load on efficacy of preemptive ther-apy with ganciclovir in allogeneic stem cell transplant recipientsEnferm Infecc Microbiol Clin 2010286-12
14 Chilet M Aguilar G Benet I et al Virological and immunolog-ical features of active cytomegalovirus infection in nonimmuno-suppressed patients in a surgical and trauma intensive care unitJ Med Virol 2010821384-1391
15 Ljungman P Griffiths P Paya C Definitions of HCMV infec-tion and disease in transplant recipients Clin Infect Dis 2002341094-1097
16 TormoN Solano C de la Camara R et al An assessment of theeffect of human herpesvirus-6 replication on active cytomegalo-virus infection after allogeneic stem cell transplantation BiolBlood Marrow Transplant 201016653-661
17 Emery VC Cope AV Bowen EF Gor D Griffiths PD The dy-namics of human cytomegalovirus replication in vivo J ExpMed1999190177-182
18 Humar A Kumar D Boivin G Caliendo AM Cytomegalovirus(CMV) virus load kinetics to predict recurrent disease in solid-organ transplant patients with CMV disease J Infect Dis 2002186829-833
19 BoeckhMHuangM Ferrenberg J et al Optimization of quan-titative detection of cytomegalovirus DNA in plasma by real-time PCR J Clin Microbiol 2004421142-1148
20 BoeckhM Gooley TA MyersonD CunninghamT Schoch GBowden RA Cytomegalovirus pp65 antigenemia-guided earlytreatment with ganciclovir versus ganciclovir at engraftment af-ter allogeneic marrow transplantation a randomized double-blind study Blood 1996884063-4071
21 Nichols WG Corey L Gooley T et al Rising pp65 antigene-mia during preemptive anticytomegalovirus therapy afterallogeneic hematopoietic stem cell transplantation risk factorscorrelation with DNA load and outcomes Blood 200197867-874
22 Gerna G Lilleri D Zecca M et al Rising antigenemia levelsmay be misleading in pre-emptive therapy of human cytomega-lovirus infection in allogeneic hematopoietic stem cell transplantrecipients Haematologica 200590526-533
23 TormoN Solano C Benet I et al Lack of prompt expansion ofcytomegalovirus pp65 and IE-1-specific IFNgamma CD81 andCD41 T cells is associated with rising levels of pp65 antigene-mia and DNAemia during pre-emptive therapy in allogeneichematopoietic stem cell transplant recipients Bone MarrowTransplant 201045543-549
24 Tormo N Solano C Benet I et al Kinetics of cytomegalovirus(CMV) pp65 and IE-1-specific IFNgamma CD81 and CD41T cells during episodes of viral DNAemia in allogeneic stemcell transplant recipients potential implications for the manage-ment of active CMV infection J Med Virol 2010821208-1215
25 FosterAEGottliebDJ SartorMHertzbergMS BradstockKFCytomegalovirus-specific CD41 and CD81 T-cells followa similar reconstitution pattern after allogeneic stem cell trans-plantation Biol Blood Marrow Transplant 20028501-511
26 Hakki M Riddell SR Storek J et al Immune reconstitution tocytomegalovirus after allogeneic stem cell transplantationimpact of host factors drug therapy and subclinical reactivationBlood 20031023060-3067
27 Lilleri D Fornara C Chiesa A Caldera D Alessandrino EPGerna G Human cytomegalovirus-specific CD41 and CD81T-cell reconstitution in adult allogeneic hematopoietic stemcell transplant recipients and immune control of viral infectionHaematologica 200893248-256
28 Pourgheysari B Piper KP McLarnon A et al Early reconstitu-tion of effector memory CD41 CMV-specific T cells protectsagainst CMV reactivation following allogeneic SCT BoneMarrow Transplant 200943853-861
29 Zhou W Longmate J Lacey SF et al Impact of donor CMVstatus on viral infection and reconstitution of multifunctionCMV-specific T cells in CMV-positive transplant recipientsBlood 20091136465-6476
30 TormoN SolanoC Benet I et al Reconstitution of CMVpp65and IE-1-specific IFN-gCD8(1) and CD4(1) T-cell responsesaffording protection fromCMVDNAemia following allogeneichematopoietic SCT Bone Marrow Transplant 2011 Jan 17[Epub ahead of print]
31 San Juan R Aguado JM Lumbreras C et al Impact of currenttransplantation management on the development of cytomega-lovirus disease after renal transplantation Clin Infect Dis 200847875-882
32 Moorman NJ Shenk T Rapamycin-resistant mTORC1 kinaseactivity is required for herpesvirus replication J Virol 2010845260-5269
33 Gratama JW Boeckh M Nakamura R et al Immune monitor-ing with iTAg MHC Tetramers for prediction of recurrent orpersistent cytomegalovirus infection or disease in allogeneichematopoietic stem cell transplant recipients a prospectivemulticenter study Blood 20101161655-1662
Related Documents











