Dynamic Evaluation of Sutureless Vitrectomy Wounds: An Optical Coherence Tomography and Histopathology Study Mehran Taban, MD, Alexandre A. C. M. Ventura, MD, Sumit Sharma, BS, Peter K. Kaiser, MD Purpose: To investigate the in vitro dynamic wound morphology of fresh 25- and 23-gauge sutureless sclerotomy wounds. Design: Experimental study; laboratory investigation. Participants: Sixteen eyes of New Zealand white rabbits. Methods: Eight cadaver heads were obtained, and the eyes were enucleated with their conjunctiva intact to simulate an intact globe. Four eyes were analyzed using 4 different wound types and cannula sizes: 25-gauge straight incision (group a); 25-gauge angled incision (group b); 23-gauge straight incision (group c); and 23-gauge angled incision (group d). Three incisions were created in each eye using either a 25- or 23-gauge trocar/cannula system. Intraocular pressure (IOP) was controlled with intraocular balanced salt solution infused through the infusion cannula. The incisions were imaged with a prototype, anterior segment spectral domain optical coherence tomography device under variable IOP to simulate successive blinks or rubbing of the eye and to evaluate the wounds in a dynamic state. Finally, India ink was applied to the surface of the eye under variable IOP to evaluate for wound leakage and potential ink ingress. The eyes were then analyzed by frozen section. Main Outcome Measures: Wound gaping as evaluated with optical coherence tomography (OCT) and presence of India ink particles in incisions evaluated by histology. Results: Gross examination revealed obvious leakage of intraocular fluid in groups A and C (straight incisions) under variable IOP, with some even developing conjunctival blebs. Groups B and D (angled incisions) demonstrated minimal to no clinical leakage. Spectral domain optical coherence tomography demonstrated open wounds in straight incisions under all IOP conditions, with a slightly larger open wound under high IOP. Angled incisions demonstrated less wound gap overall and better wound apposition under high IOP versus low IOP. Histologic examination revealed India ink particles in all straight incisions with penetration across the whole incision in some wounds, whereas no ink particles were observed in angled incisions. Conclusions: Angled incisions have been proposed for sutureless vitrectomy to prevent wound leakage, hypotony, and the secondary risk of endophthalmitis. This study demonstrates that angled incisions provide better wound apposition under dynamic IOP conditions immediately after formation that simulate real-world situations: blinking, squeezing, or even rubbing of the eye. Financial Disclosure(s): Proprietary or commercial disclosure may be found after the references. Ophthalmology 2008;115:2221–2228 © 2008 by the American Academy of Ophthalmology. During the last few years, advancements in microsurgical instrumentation have led to increased adoption of “suture- less vitrectomy” using 23- or 25-gauge instrumentation. 1–3 The 2007 Practice and Trends survey of the American Society of Retina Specialists revealed that 47% of respon- dents use 23- or 25-gauge systems in the majority of their cases and that at least 75% use it in some of their cases (https://www.retinaspecialists.org/services/pat_survey/). In this small incision surgery, sclerotomies are performed through the conjunctiva; thus, no conjunctival suturing is required at the completion of surgery. Furthermore, the sclerotomies are not sutured because of their small size and presumed self-sealing characteristics. Using small incision surgery has reportedly led to reduced operating times, in- creased patient comfort, and faster healing times. 1,4 –7 How- ever, there have been questions raised in regard to the true self-sealing properties of some of these sutureless scleroto- mies. There are reports of increased hypotony and endoph- thalmitis rates with sutureless vitrectomies. 2,8 –14 Some in- vestigators have promoted the creation of angled (beveled) sclerotomy incisions as opposed to straight incisions to prevent leakage through these sutureless wounds. 15–17 How- ever, because of the lack of studies comparing various wound architectures (i.e., 23- vs. 25-gauge, straight vs. beveled, suture vs. sutureless), the debate still continues with respect to the best wound architecture for small inci- sion surgery. Ultrasound biomicroscopy (UBM) has been a valuable imaging tool to examine sclerotomy sites after pars plana vitrectomy, as in cases of proliferative diabetic retinopathy, anterior hyaloidal fibrovascular proliferation, and vitreous incarceration. 18 –20 There have been some studies using UBM to evaluate the wound architecture after microincision surgery; however, they have been limited for several rea- 2221 © 2008 by the American Academy of Ophthalmology ISSN 0161-6420/08/$–see front matter Published by Elsevier Inc. doi:10.1016/j.ophtha.2008.08.027

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Dynamic Evaluation of SuturelessVitrectomy Wounds: An Optical CoherenceTomography and Histopathology Study
Mehran Taban, MD, Alexandre A. C. M. Ventura, MD, Sumit Sharma, BS, Peter K. Kaiser, MD
Purpose: To investigate the in vitro dynamic wound morphology of fresh 25- and 23-gauge suturelesssclerotomy wounds.
Design: Experimental study; laboratory investigation.Participants: Sixteen eyes of New Zealand white rabbits.Methods: Eight cadaver heads were obtained, and the eyes were enucleated with their conjunctiva intact to
simulate an intact globe. Four eyes were analyzed using 4 different wound types and cannula sizes: 25-gaugestraight incision (group a); 25-gauge angled incision (group b); 23-gauge straight incision (group c); and 23-gaugeangled incision (group d). Three incisions were created in each eye using either a 25- or 23-gauge trocar/cannulasystem. Intraocular pressure (IOP) was controlled with intraocular balanced salt solution infused through theinfusion cannula. The incisions were imaged with a prototype, anterior segment spectral domain opticalcoherence tomography device under variable IOP to simulate successive blinks or rubbing of the eye and toevaluate the wounds in a dynamic state. Finally, India ink was applied to the surface of the eye under variable IOPto evaluate for wound leakage and potential ink ingress. The eyes were then analyzed by frozen section.
Main Outcome Measures: Wound gaping as evaluated with optical coherence tomography (OCT) andpresence of India ink particles in incisions evaluated by histology.
Results: Gross examination revealed obvious leakage of intraocular fluid in groups A and C (straightincisions) under variable IOP, with some even developing conjunctival blebs. Groups B and D (angled incisions)demonstrated minimal to no clinical leakage. Spectral domain optical coherence tomography demonstratedopen wounds in straight incisions under all IOP conditions, with a slightly larger open wound under high IOP.Angled incisions demonstrated less wound gap overall and better wound apposition under high IOP versus lowIOP. Histologic examination revealed India ink particles in all straight incisions with penetration across the wholeincision in some wounds, whereas no ink particles were observed in angled incisions.
Conclusions: Angled incisions have been proposed for sutureless vitrectomy to prevent wound leakage,hypotony, and the secondary risk of endophthalmitis. This study demonstrates that angled incisions providebetter wound apposition under dynamic IOP conditions immediately after formation that simulate real-worldsituations: blinking, squeezing, or even rubbing of the eye.
Financial Disclosure(s): Proprietary or commercial disclosure may be found after the references.
Ophthalmology 2008;115:2221–2228 © 2008 by the American Academy of Ophthalmology.During the last few years, advancements in microsurgicalinstrumentation have led to increased adoption of “suture-less vitrectomy” using 23- or 25-gauge instrumentation.1–3
The 2007 Practice and Trends survey of the AmericanSociety of Retina Specialists revealed that 47% of respon-dents use 23- or 25-gauge systems in the majority of theircases and that at least 75% use it in some of their cases(https://www.retinaspecialists.org/services/pat_survey/). Inthis small incision surgery, sclerotomies are performedthrough the conjunctiva; thus, no conjunctival suturing isrequired at the completion of surgery. Furthermore, thesclerotomies are not sutured because of their small size andpresumed self-sealing characteristics. Using small incisionsurgery has reportedly led to reduced operating times, in-creased patient comfort, and faster healing times.1,4–7 How-ever, there have been questions raised in regard to the true
self-sealing properties of some of these sutureless scleroto-© 2008 by the American Academy of OphthalmologyPublished by Elsevier Inc.
mies. There are reports of increased hypotony and endoph-thalmitis rates with sutureless vitrectomies.2,8–14 Some in-vestigators have promoted the creation of angled (beveled)sclerotomy incisions as opposed to straight incisions toprevent leakage through these sutureless wounds.15–17 How-ever, because of the lack of studies comparing variouswound architectures (i.e., 23- vs. 25-gauge, straight vs.beveled, suture vs. sutureless), the debate still continueswith respect to the best wound architecture for small inci-sion surgery.
Ultrasound biomicroscopy (UBM) has been a valuableimaging tool to examine sclerotomy sites after pars planavitrectomy, as in cases of proliferative diabetic retinopathy,anterior hyaloidal fibrovascular proliferation, and vitreousincarceration.18–20 There have been some studies usingUBM to evaluate the wound architecture after microincision
surgery; however, they have been limited for several rea-2221ISSN 0161-6420/08/$–see front matterdoi:10.1016/j.ophtha.2008.08.027

Ophthalmology Volume 115, Number 12, December 2008
sons, including the fact that the resolution of UBM is poorfor imaging small areas such as these sclerotomy sites.20–25
Histologic studies have been performed but were also lim-ited because they do not provide information on the dy-namic state of the wound under varying intraocular condi-tions.16 Optical coherence tomography (OCT) is a noncontact,noninvasive, high-speed, high-resolution imaging modalitythat has been used to image the retina, optic nerve, andanterior segment structures, such as the angle and cor-nea.26–35 However, we are unaware of previous studiesusing spectral domain optical coherence tomography (SD-OCT) to image sclerotomy wounds and provide details ofthe anatomic structure. Furthermore, there are no dynamicreal-time studies of wound behavior as in the immediatepostoperative period when the wounds are still not healedafter microincision surgery. Finally, although leakage ofintraocular fluid and gas (outflow) has clearly been observedand reported after microincision surgery,16 to our knowl-edge, there have been no studies evaluating the potentialingress of extraocular/surface material (e.g., bacteria) throughthe wounds and into the globe (inflow), which is the pur-ported mechanism for development of endophthalmitis.
The purpose of this study is to investigate the in vitrodynamic (i.e., under intraocular pressure [IOP] variation)real-time characteristics of various sutureless sclerotomyincisions using anterior segment SD-OCT and to evaluatethe potential for ingress of extraocular fluid through thesewounds using India ink. India ink has been established as a
Figure 1. Schematic of how incisions were created. A, B, For angled(tunnel, bevel) incisions, the eye was penetrated as tangentially as possibleparallel to the limbus with the bevel up; once past the trocar sleeve, theangle was changed to 90 degrees (perpendicular to surface). C, For straightincisions, the eye was penetrated perpendicular to the globe.
valuable tool to assess inflow through sutureless corneal
2222
incisions, because the ink particles can be easily visible ifpresent.27,36–38 Furthermore, these particles can simulatebacteria because the size of some particles can be simi-lar.27,36
Materials and Methods
Tissue Preparation and Surgical Procedure
Eight fresh cadaver heads of New Zealand white rabbit wereobtained from a local abattoir. The globes were enucleated withtheir conjunctiva intact to simulate an intact globe and placed in aglobe holder. Three incisions were created in each eye, includingthe infusion cannula using either a 25- or 23-gauge trocar andcannula system depending on the group assignment of the eye.Incisions were placed 2.5 mm posterior to the limbus. Four eyeswere analyzed using 4 different wound types and cannula sizes:25-gauge straight incision (group a); 25-gauge angled incision(group b); 23-gauge straight incision (group c); and 23-gauge angledincision (group d). For angled (tunnel, bevel) incisions, the eye waspenetrated as tangentially as possible parallel to the limbus with thebevel up. Once past the trocar sleeve, the angle was changed to 90degrees (perpendicular to surface) (Fig 1A, B). For straight incisions,the eye was penetrated perpendicular to the globe (Fig 1C). Intraoc-ular pressure was controlled with a 25- or 23-gauge infusioncannula (depending on the group assignment) connected to a bottleof balanced salt solution with intravenous tubing. At the end of theprocedure, the cannulas were removed by slowly pulling them outfollowing the angled or straight entry path. An experienced vit-reoretinal surgeon performed all surgical incisions.
Optical Coherence Tomography
The principle of OCT has been described.39 The sclerotomywounds were imaged with a prototype anterior segment spectraldomain OCT (Bioptigen, Research Triangle Park, NC) with anaxial resolution of 6 �m, a lateral resolution of 20 �m, and animaging depth of 2 mm. The OCT device was used to scan across
Figure 2. The setup of our experiment showing anterior segment OCT
and a rabbit globe.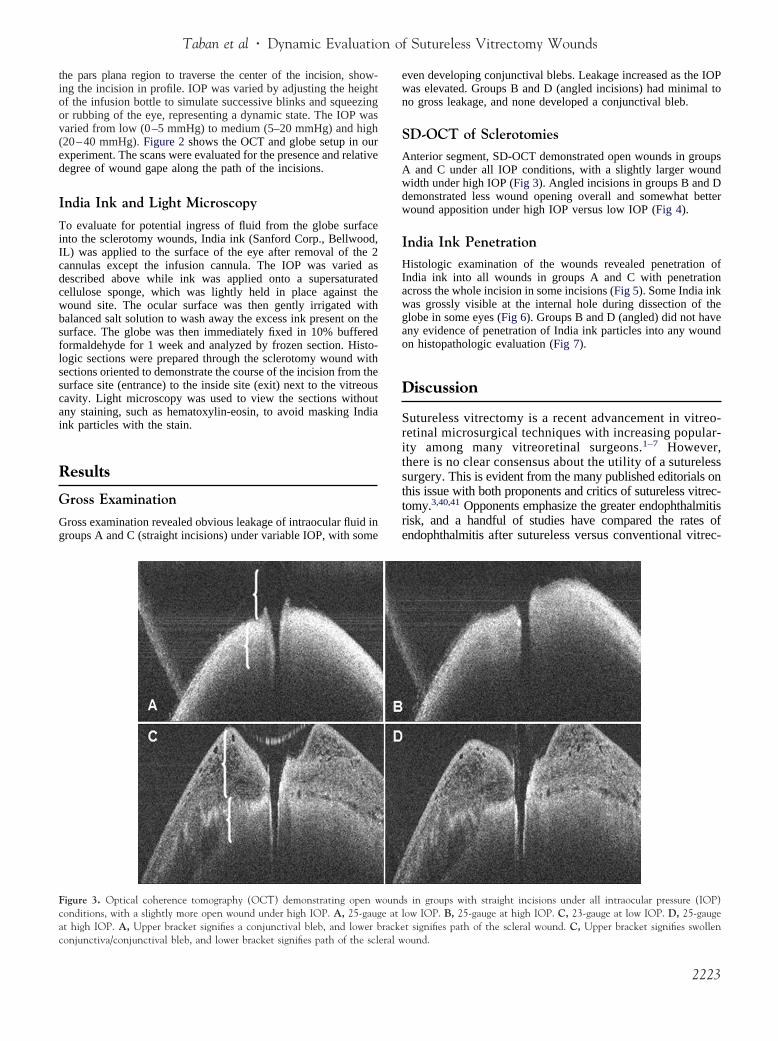
Taban et al � Dynamic Evaluation of Sutureless Vitrectomy Wounds
the pars plana region to traverse the center of the incision, show-ing the incision in profile. IOP was varied by adjusting the heightof the infusion bottle to simulate successive blinks and squeezingor rubbing of the eye, representing a dynamic state. The IOP wasvaried from low (0–5 mmHg) to medium (5–20 mmHg) and high(20–40 mmHg). Figure 2 shows the OCT and globe setup in ourexperiment. The scans were evaluated for the presence and relativedegree of wound gape along the path of the incisions.
India Ink and Light Microscopy
To evaluate for potential ingress of fluid from the globe surfaceinto the sclerotomy wounds, India ink (Sanford Corp., Bellwood,IL) was applied to the surface of the eye after removal of the 2cannulas except the infusion cannula. The IOP was varied asdescribed above while ink was applied onto a supersaturatedcellulose sponge, which was lightly held in place against thewound site. The ocular surface was then gently irrigated withbalanced salt solution to wash away the excess ink present on thesurface. The globe was then immediately fixed in 10% bufferedformaldehyde for 1 week and analyzed by frozen section. Histo-logic sections were prepared through the sclerotomy wound withsections oriented to demonstrate the course of the incision from thesurface site (entrance) to the inside site (exit) next to the vitreouscavity. Light microscopy was used to view the sections withoutany staining, such as hematoxylin-eosin, to avoid masking Indiaink particles with the stain.
Results
Gross Examination
Gross examination revealed obvious leakage of intraocular fluid ingroups A and C (straight incisions) under variable IOP, with some
Figure 3. Optical coherence tomography (OCT) demonstrating open wconditions, with a slightly more open wound under high IOP. A, 25-gaugat high IOP. A, Upper bracket signifies a conjunctival bleb, and lower b
conjunctiva/conjunctival bleb, and lower bracket signifies path of the scleral weven developing conjunctival blebs. Leakage increased as the IOPwas elevated. Groups B and D (angled incisions) had minimal tono gross leakage, and none developed a conjunctival bleb.
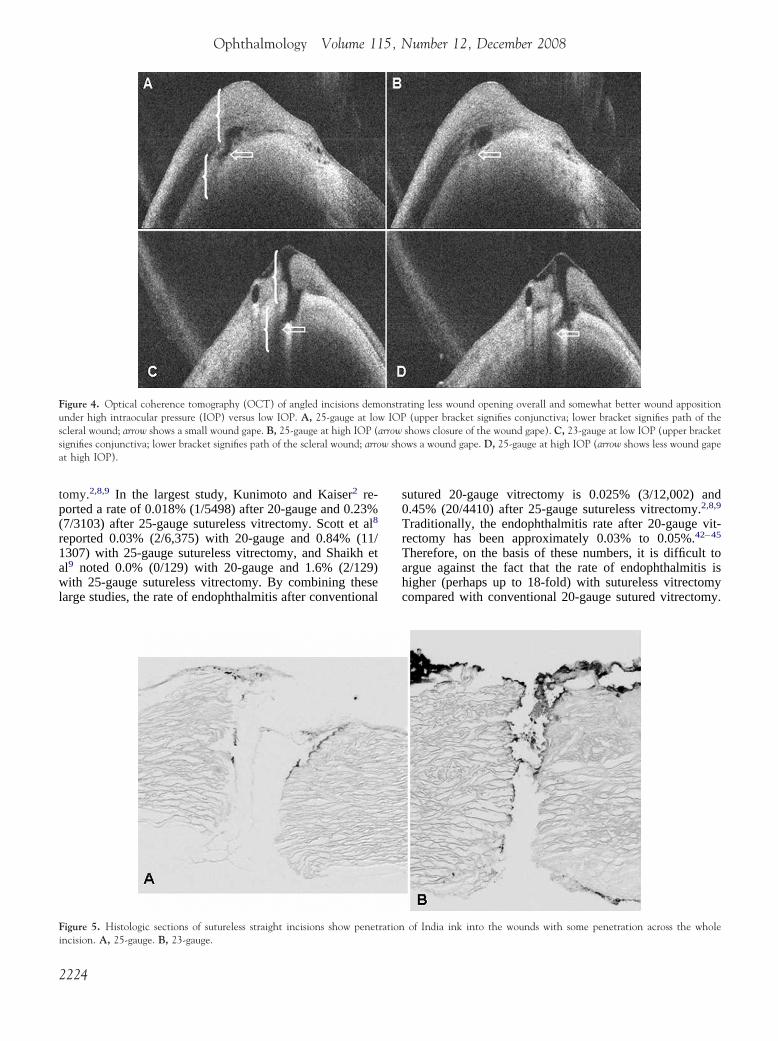
SD-OCT of SclerotomiesAnterior segment, SD-OCT demonstrated open wounds in groupsA and C under all IOP conditions, with a slightly larger woundwidth under high IOP (Fig 3). Angled incisions in groups B and Ddemonstrated less wound opening overall and somewhat betterwound apposition under high IOP versus low IOP (Fig 4).
India Ink PenetrationHistologic examination of the wounds revealed penetration ofIndia ink into all wounds in groups A and C with penetrationacross the whole incision in some incisions (Fig 5). Some India inkwas grossly visible at the internal hole during dissection of theglobe in some eyes (Fig 6). Groups B and D (angled) did not haveany evidence of penetration of India ink particles into any woundon histopathologic evaluation (Fig 7).
Discussion
Sutureless vitrectomy is a recent advancement in vitreo-retinal microsurgical techniques with increasing popular-ity among many vitreoretinal surgeons.1–7 However,there is no clear consensus about the utility of a suturelesssurgery. This is evident from the many published editorials onthis issue with both proponents and critics of sutureless vitrec-tomy.3,40,41 Opponents emphasize the greater endophthalmitisrisk, and a handful of studies have compared the rates ofendophthalmitis after sutureless versus conventional vitrec-
s in groups with straight incisions under all intraocular pressure (IOP)ow IOP. B, 25-gauge at high IOP. C, 23-gauge at low IOP. D, 25-gauget signifies path of the scleral wound. C, Upper bracket signifies swollen
ounde at lracke
ound.
2223
Ophthalmology Volume 115, Number 12, December 2008
tomy.2,8,9 In the largest study, Kunimoto and Kaiser2 re-ported a rate of 0.018% (1/5498) after 20-gauge and 0.23%(7/3103) after 25-gauge sutureless vitrectomy. Scott et al8
reported 0.03% (2/6,375) with 20-gauge and 0.84% (11/1307) with 25-gauge sutureless vitrectomy, and Shaikh etal9 noted 0.0% (0/129) with 20-gauge and 1.6% (2/129)with 25-gauge sutureless vitrectomy. By combining theselarge studies, the rate of endophthalmitis after conventional
Figure 4. Optical coherence tomography (OCT) of angled incisions demunder high intraocular pressure (IOP) versus low IOP. A, 25-gauge at loscleral wound; arrow shows a small wound gape. B, 25-gauge at high IOP (signifies conjunctiva; lower bracket signifies path of the scleral wound; arroat high IOP).
Figure 5. Histologic sections of sutureless straight incisions show penet
incision. A, 25-gauge. B, 23-gauge.2224
sutured 20-gauge vitrectomy is 0.025% (3/12,002) and0.45% (20/4410) after 25-gauge sutureless vitrectomy.2,8,9
Traditionally, the endophthalmitis rate after 20-gauge vit-rectomy has been approximately 0.03% to 0.05%.42–45
Therefore, on the basis of these numbers, it is difficult toargue against the fact that the rate of endophthalmitis ishigher (perhaps up to 18-fold) with sutureless vitrectomycompared with conventional 20-gauge sutured vitrectomy.
ating less wound opening overall and somewhat better wound apposition(upper bracket signifies conjunctiva; lower bracket signifies path of the
shows closure of the wound gape). C, 23-gauge at low IOP (upper bracketws a wound gape. D, 25-gauge at high IOP (arrow shows less wound gape
of India ink into the wounds with some penetration across the whole
onstrw IOParroww sho
ration

Taban et al � Dynamic Evaluation of Sutureless Vitrectomy Wounds
The question is why? The answer may lie in wound con-struction. Kunimoto and Kaiser2 stated that no beveling ofthe wound was performed in their series, whereas 73% ofthe endophthalmitis cases in Scott et al’s8 series were from
Figure 6. Ink grossly visible at the internal hole (arrow) of sclera (next tothe vitreous cavity) for some sutureless straight incisions, as was the casewith this 23-gauge wound.
Figure 7. Histologic sections of angled (beveled) incisions do not have an
B, 23-gauge.straight incision. According to many investigators, angledincision can help prevent wound leakage by having theinternal lip press against the outer lip through IOP, therebyclosing the wound.15–17 Our study found that angled inci-sions decrease or prevent wound gap immediately aftercannula removal and, more important, prevent secondarywound leakage and potential inflow of pathogens. However,some incisions may not be created as truly beveled. Fur-thermore, significant manipulation of the sclerotomies viamoving of instruments in awkward and extreme directions/positions during vitrectomy and membrane peeling canchange the wound architecture from its original constructionand deem the wound relatively unstable and unpredictable.Other possible explanations for the disparity in endoph-thalmitis rates could be the larger skirt of vitreous leftbehind with sutureless vitrectomy or vitreous wick syn-drome.2,8,46
The in situ OCT evaluation performed in this studyshowed that not all sutureless sclerotomies result in a stablewound morphology immediately after they are created.Straight incisions appear to gape considerably more thanbeveled incisions. OCT demonstrated open wounds in thosegroups with straight incisions under all IOP conditions, witha slightly larger wound width under high IOP conditions.Angled incisions, however, demonstrated less wound open-ing overall and somewhat better wound apposition underhigh IOP versus low IOP. These findings are similar to thoseobserved in sutureless clear corneal incisions.26,27
Histologic analysis of the wounds showed penetration ofIndia ink along the entire length of all straight incisions,with some India ink even visible grossly at the internal holeduring dissection of the globe. In contrast, no India inkparticles were observed along the length of angled incisions.
dence of penetration of India ink particles into the wounds. A, 25-gauge.
y evi2225

Ophthalmology Volume 115, Number 12, December 2008
This indicates the potential for surface fluid inflow throughstraight incisions before the occurrence of any wound heal-ing or closure. The drawing of ocular surface fluid into thewound as demonstrated by the India ink particles, followedby a transient gaping of the internal aspect of the incision,would allow bacteria to reach inside the globe withoutnecessarily having a continuous gaping along the full lengthof the sclerotomy incision. A “suction pump” mechanismmay explain how the surface fluid enters the eye.36,47 Thisis induced by the substantial pressure variation applied tothe globe by the squeezing of the lids or even normalunconscious blinking. The presence of this force has beenrecognized for decades. Blinking can result in pressureincreases of up to 10 mmHg, whereas squeezing can pro-duce prompt elevations up to 110 mmHg (or a 90 mmHgincrease), followed by an 8 mmHg undershoot after lidopening relative to baseline IOP.48,49 These findings con-firm the clinically apparent fact that blinking or squeezingof the lids can exert tremendous forces on the globe thatmay be important after microincision vitrectomy surgery.
On preparation of this article, Singh et al50 published astudy demonstrating ingress of ocular surface fluid (Indiaink) into sutureless straight incisions after 25-gauge vitrec-tomy in cadaver human globes, without any inflow intosutured wounds. This study corroborates our investigationshowing the potential of ocular surface fluid ingress intosutureless straight sclerotomies. However, Singh et al50 didnot evaluate 23-gauge incisions or oblique sclerotomies.Furthermore, there was no dynamic real-time evaluation ofwound morphology using OCT as performed in currentinvestigation.
There are potential limitations to this ex vivo experiment,such as lack of a complete anatomy, including adnexalcomponents. Second, no vitrectomy was performed in theseeyes, although vitreous presence would have theoreticallyplugged the sclerotomies and decreased the chance of fluidpassage. Furthermore, intraocular air or gas was not used,which could have a possible tamponade effect on the woundinternally, decreasing passage of material across the inci-sion. Finally, there might be a difference in the scleralrigidity of rabbit eyes relative to humans. However, thesefindings still indicate the importance of paying careful at-tention to the angle of the sclerotomy incision irrespectiveof whether 23- or 25-gauge cannulas are used. We areplanning future in vivo studies to confirm these findings andevaluate the role of vitreous removal and presence of in-traocular gas or air on wound dynamics.
The suggestion of an increased risk of acute endoph-thalmitis after sutureless vitrectomy raises the question ofwhether it might be possible for surface bacteria to trans-verse these incisions during the early postoperative periodwhen the wounds are still unhealed. The current set ofexperiments suggest that straight incisions pose a higherrisk of wound unapposition and fluid inflow compared withbeveled incisions and therefore have several implications.First, the clinician should pay attention when creating thesclerotomy incisions. Second, one should carefully evaluatethe state of the wound at the completion of surgery andevaluate for signs of leakage and gaping. If there is any
question in regard to the self-sealing characteristic of the2226
wound after surgery (e.g., continued leakage), surgeonsshould not hesitate to place a suture even if they thoughtthey created a self-sealing beveled incision initially. This iseither because the incision may not have been truly beveledto begin with or significant manipulation of the sclerotomiesvia moving of instruments in awkward and extreme direc-tions/positions changed the wound architecture and thusmade it relatively unstable and unpredictable. Furthermore,straight incisions (23- or 25-gauge) should not be left un-sutured. Finally, it might be safer to keep the globe slightlyon the higher side of IOP (for beveled sclerotomies) toincrease the apposition of the wound, although one shouldalways consider the complete picture (i.e., presence of gas,history of glaucoma). The effect of fluid-filled eye versusair/gas-filled eye will have to be further investigated.
The findings of the present study demonstrate that angled(beveled) incisions provide better wound apposition underdynamic IOP conditions that simulate real-world situations(e.g., blinking, squeezing, or even rubbing of the eye) andtherefore help against inflow through the sclerotomies.There are important variables that contribute to the dynamicmorphology of sclerotomies in the early postoperative pe-riod, namely, the incision angle and IOP act together todetermine the wound structure and thus its accessibility topotentially pathogenic organisms. This is similar to whathas been shown with sutureless clear corneal incisions.26,27
Vitreoretinal surgeons should be aware of these factorswhen constructing and evaluating their wounds postopera-tively to minimize the risk of wound gaping, leakage, andendophthalmitis.
Furthermore, the value of OCT as a tool for ophthalmicimaging is further supported by this investigation. Origi-nally used for retinal and optic nerve imaging33–35 in recentyears, the applications of OCT have expanded to visual-ization of anterior segment components (cornea, LASIKflaps, angle).26 –32 The noncontact, noninvasive, and high-resolution characteristics of OCT make it extremely attr-active for the study of surgical wounds and the healing proc-ess during the immediate postoperative period.26,27 Futurehigher-resolution OCT may provide even better assessmentof surgical wounds.
References
1. Lakhanpal RR, Humayun MS, de Juan E Jr, et al. Outcomesof 140 consecutive cases of 25-gauge transconjunctival sur-gery for posterior segment disease. Ophthalmology 2005;112:817–24.
2. Kunimoto DY, Kaiser RS, Wills Eye Retina Service. Inci-dence of endophthalmitis after 20- and 25-gauge vitrectomy.Ophthalmology 2007;114:2133–7.
3. Lewis H. Sutureless microincision vitrectomy surgery: unclearbenefit, uncertain safety. Am J Ophthalmol 2007;144:613–5.
4. Fujii GY, De Juan E Jr, Humayun MS, et al. Initial experienceusing the transconjunctival sutureless vitrectomy system forvitreoretinal surgery. Ophthalmology 2002;109:1814–20.
5. Fujii GY, De Juan E Jr, Humayun MS, et al. A new 25-gaugeinstrument system for transconjunctival sutureless vitrectomy
surgery. Ophthalmology 2002;109:1807–12.
Taban et al � Dynamic Evaluation of Sutureless Vitrectomy Wounds
6. Chen E. 25-gauge transconjunctival sutureless vitrectomy.Curr Opin Ophthalmol 2007;18:188–93.
7. Fine HF, Iranmanesh R, Iturralde D, Spaide RF. Outcomes of77 consecutive cases of 23-gauge transconjunctival vitrectomysurgery for posterior segment disease. Ophthalmology 2007;114:1197–200.
8. Scott IU, Flynn HW Jr, Dev S, et al. Endophthalmitis after25-gauge and 20-gauge pars plana vitrectomy: incidence andoutcomes. Retina 2008;28:138–42.
9. Shaikh S, Ho S, Richmond PP, et al. Untoward outcomes in25-gauge versus 20-gauge vitreoretinal surgery. Retina 2007;27:1048–53.
10. Gupta OP, Weichel ED, Regillo CD, et al. Postoperativecomplications associated with 25-gauge pars plana vitrec-tomy. Ophthalmic Surg Lasers Imaging 2007;38:270–5.
11. Byeon SH, Chu YK, Lee SC, et al. Problems associated withthe 25-gauge transconjunctival sutureless vitrectomy systemduring and after surgery. Ophthalmologica 2006;220:259–65.
12. Taban M, Ufret-Vincenty RL, Sears JE. Endophthalmitis after25-gauge transconjunctival sutureless vitrectomy. Retina 2006;26:830–1.
13. Taylor SR, Aylward GW. Endophthalmitis following 25-gauge vitrectomy [letter]. Eye 2005;19:1228–9.
14. Acar N, Unver YB, Altan T, Kapran Z. Acute endophthalmitisafter 25-gauge sutureless vitrectomy. Int Ophthalmol 2007;27:361–3.
15. Eckardt C. Transconjunctival sutureless 23-gauge vitrectomy.Retina 2005;25:208–11.
16. Singh RP, Bando H, Brasil OF, et al. Evaluation of woundclosure using different incision techniques with 23-gauge and25-gauge microincision vitrectomy systems. Retina 2008;28:242–8.
17. Shimada H, Nakashizuka H, Mori R, et al. 25-gauge scleraltunnel transconjunctival vitrectomy. Am J Ophthalmol 2006;142:871–3.
18. Boker T, Spitznas M. Ultrasound biomicroscopy for exami-nation of the sclerotomy site after pars plana vitrectomy. Am JOphthalmol 1994;118:813–5.
19. Bhende M, Agraharam SG, Gopal L, et al. Ultrasoundbiomicroscopy of sclerotomy sites after pars plana vitrectomyfor diabetic vitreous hemorrhage. Ophthalmology 2000;107:1729–36.
20. Keshavamurthy R, Venkatesh P, Garg S. Ultrasound biomi-croscopy findings of 25 G transconjunctival sutureless (TSV)and conventional (20G) pars plana sclerotomy in the samepatient. BMC Ophthalmol [serial online] 2006;6:7. Availableat: http://www.biomedcentral.com/1471-2415/6/7. AccessedAugust 1, 2008.
21. López-Guajardo L, Vleming-Pinilla E, Pareja-Esteban J,Teus-Guezala MA. Ultrasound biomicroscopy study of directand oblique 25-gauge vitrectomy sclerotomies. Am J Ophthal-mol 2007;143:881–3.
22. Zhengyu S, Fang W, Ying F, Qinghua Q. The experimentalresearch of rabbit’s sclerotomy sites undergoing transcon-junctival sutureless vitrectomy. Curr Eye Res 2007;32:647–52.
23. Rizzo S, Genovesi-Ebert F, Vento A, et al. Modified incisionin 25-gauge vitrectomy in the creation of a tunneled airtightsclerotomy: an ultrabiomicroscopic study. Graefes Arch ClinExp Ophthalmol 2007;245:1281–8.
24. Kwok AK, Tham CC, Loo AV, et al. Ultrasound biomicros-copy of conventional and sutureless pars plana sclerotomies: acomparative and longitudinal study. Am J Ophthalmol 2001;132:172–7.
25. Theelen T, Verbeek AM, Tilanus MA, van den Biesen PR.
A novel technique for self-sealing, wedge-shaped parsplana sclerotomies and its features in ultrasound bio-microscopy and clinical outcome. Am J Ophthalmol 2003;136:1085–92.
26. Taban M, Rao B, Reznik J, et al. Dynamic morphology ofsutureless cataract wounds–effect of incision angle and loca-tion. Surv Ophthalmol 2004;49(suppl):S62–72.
27. McDonnell PJ, Taban M, Sarayba M, et al. Dynamic mor-phology of clear corneal cataract incisions. Ophthalmology2003;110:2342–8.
28. Ustundag C, Bahcecioglu H, Ozdamar A, et al. Optical coher-ence tomography for evaluation of anatomical changes in thecornea after laser in situ keratomileusis. J Cataract RefractSurg 2000;26:1458–62.
29. Thompson RW Jr, Choi DM, Price MO, et al. Noncontactoptical coherence tomography for measurement of corneal flapand residual stromal bed thickness after laser in situ kerato-mileusis. J Refract Surg 2003;19:507–15.
30. Radhakrishnan S, See J, Smith SD, et al. Reproducibility ofanterior chamber angle measurements obtained with anteriorsegment optical coherence tomography. Invest OphthalmolVis Sci 2007;48:3683–8.
31. Singh M, Chew PT, Friedman DS, et al. Imaging of trabecu-lectomy blebs using anterior segment optical coherence to-mography. Ophthalmology 2007;114:47–53.
32. Radhakrishnan S, Huang D, Smith SD. Optical coherencetomography imaging of the anterior chamber angle. Ophthal-mol Clin North Am 2005;18:375–81, vi.
33. Puliafito CA, Hee MR, Lin CP, et al. Imaging of maculardiseases with optical coherence tomography. Ophthalmology1995;102:217–29.
34. Hee MR, Izatt JA, Swanson EA, et al. Optical coherencetomography of the human retina. Arch Ophthalmol 1995;113:325–32.
35. Schuman JS, Hee MR, Arya AV, et al. Optical coherencetomography: a new tool for glaucoma diagnosis. Curr OpinOphthalmol 1995;6:89–95.
36. Taban M, Sarayba MA, Ignacio TS, et al. Ingress of India inkinto the anterior chamber through sutureless clear cornealcataract wounds. Arch Ophthalmol 2005;123:643–8.
37. Berdahl JP, DeStafeno JJ, Kim T. Corneal wound architectureand integrity after phacoemulsification evaluation of coaxial,microincision coaxial, and microincision bimanual tech-niques. J Cataract Refract Surg 2007;33:510–5.
38. Hovanesian JA, Karageozian VH. Watertight cataract incisionclosure using fibrin tissue adhesive. J Cataract Refract Surg2007;33:1461–3.
39. Huang D, Swanson EA, Lin CP, et al. Optical coherencetomography. Science 1991;254:1178–81.
40. Martidis A, Chang TS. Sutureless 25-gauge vitrectomy: riskyor rewarding? Ophthalmology 2007;114:2131–2.
41. Williams GA. 25-, 23-, or 20-gauge instrumentation for vit-reous surgery? Eye 2008;22:1263–6.
42. Mollan SP, Mollan AJ, Konstantinos C, et al. Incidence ofendophthalmitis following vitreoretinal surgery. Int Ophthal-mol 2008 Mar 1. [Epub ahead of print].
43. Eifrig CW, Flynn HW Jr, Scott IU, Newton J. Acute-onsetpostoperative endophthalmitis: review of incidence and visualoutcomes (1995–2001). Ophthalmic Surg Lasers 2002;33:373–8.
44. Eifrig CW, Scott IU, Flynn HW Jr, et al. Endophthalmitisafter pars plana vitrectomy: incidence, causative organisms,and visual acuity outcomes. Am J Ophthalmol 2004;138:799 – 802.
45. Aaberg TM Jr, Flynn HW Jr, Schiffman J, Newton J. Noso-
comial acute-onset postoperative endophthalmitis survey: a2227

Ophthalmology Volume 115, Number 12, December 2008
10-year review of incidence and outcomes. Ophthalmology1998;105:1004–10.
46. Venkatesh P, Verma L, Tewari H. Posterior vitreous wicksyndrome: a potential cause of endophthalmitis followingvitreo-retinal surgery. Med Hypotheses 2002;58:513–5.
47. McGowan BL. Mechanism for development of endophthalmi-
tis [letter]. J Cataract Refract Surg 1994;20:111.from Alcon on his behalf. PKK serves on the scientific retinal advisory
2228
48. Miller D. Pressure of the lid on the eye. Arch Ophthalmol1967;78:328–30.
49. Coleman DJ, Trokel S. Direct-recorded intraocular pressure vari-ations in a human subject. Arch Ophthalmol 1969;82:637–40.
50. Singh A, Chen JA, Stewart JM. Ocular surface fluid contam-ination of sutureless 25-gauge vitrectomy incisions. Retina
2008;28:553–7.Footnotes and Financial Disclosures
Originally received: April 15, 2008.Final revision: August 8, 2008.Accepted: August 8, 2008. Manuscript no. 2008-474.
Cole Eye Institute, Cleveland Clinic, Cleveland, Ohio.
Financial Disclosure(s):The Cole Eye Institute, the employer of PKK, has received a research grant
board of Alcon. The authors have no proprietary or conflicting interests inany material discussed in this report.Paper presented at: The 41st Annual Meeting of The Retina Society, Septem-ber 25–28, 2008, Scottsdale, Arizona.
Correspondence:Peter K. Kaiser, MD, Cleveland Clinic, 9500 Euclid Ave, Desk i3, Cleve-
land, OH 44195. E-mail: [email protected].
Related Documents











