Dynamic change of proximal conduction in demyelinating neuropathies: A cervical magnetic stimulation combined with maximum voluntary contraction Takefumi Hitomi a , Ryuji Kaji b , Nagako Murase a,b, * , Nobuo Kohara c , Takahiro Mezaki a , Hiroyuki Nodera b , Takashi Kawamura d , Akio Ikeda a , Hiroshi Shibasaki a,e a Department of Neurology, Kyoto University Hospital, Japan b Department of Neurology, Tokushima University Hospital, Japan c Department of Neurology, Kobe City General Hospital, Japan d Department of Medicine and Epidemiology, Kyoto University Health Service, Japan e Takeda General Hospital, Kyoto, Japan Accepted 18 November 2006 Abstract Objective: To evaluate conduction abnormalities in the nerves innervating the proximal muscles in demyelinating neuropathies (DN) using cervical magnetic stimulation. Methods: We applied cervical root magnetic stimulation in the biceps brachii muscles and examined its activity-dependent conduction changes produced by maximal voluntary contraction (MVC) in 12 DN patients (seven chronic inflammatory demyelinating polyradic- uloneuropathy and five multifocal motor neuropathy), six motor neuron disease (MND) patients, and 12 healthy volunteers. Results: Defining the upper normal limit of motor threshold (31%) and latency (6.7 ms) of the compound muscle action potential (CMAP) as mean + 2SD, most DN patients revealed an abnormality in motor threshold (10/12) and latency (11/12) in contrast to MND patients (motor threshold (1/6) and latency (0/6)). These parameters contribute to the differentiation of DN from MND (P < 0.01). Furthermore, the MVC maneuver transiently decreased the CMAP amplitude ratio (after MVC/before MVC · 100) in DN (83 ± 18 %) compared with MND (P < 0.01). Two of three DN patients who showed normal motor threshold or latency as in MND were successfully differentiated from MND by the MVC maneuver. Conclusions: In DN patients, conduction abnormality in the nerves innervating the proximal muscles was revealed by cervical magnetic stimulation combined with the MVC maneuver. Significance: Our results suggested that conduction abnormalities in the proximal nerves innervating the proximal muscles could be eval- uated by this method. Ó 2006 International Federation of Clinical Neurophysiology. Published by Elsevier Ireland Ltd. All rights reserved. Keywords: Cervical magnetic stimulation; Proximal muscle; Activity-dependent conduction block; CIDP; MMN; MND 1388-2457/$32.00 Ó 2006 International Federation of Clinical Neurophysiology. Published by Elsevier Ireland Ltd. All rights reserved. doi:10.1016/j.clinph.2006.11.013 Abbreviations: chronic inflammatory demyelinating polyradiculoneuropathy, CIDP; compound muscle action potential, CMAP; demyelinating neu- ropathy, DN; electromyogram, EMG; intravenous immunoglobulin, IVIg; maximum voluntary contraction, MVC; Medical Research Council, MRC; motor neuron disease, MND; multifocal motor neuropathy, MMN; nerve conduction study, NCS; analysis of variance, ANOVA. * Corresponding author. Department of Neurology, National Hospital Organization, Utano National Hospital, Ondoyama-cho 8, Narutaki, Ukyo-ku, Kyoto 616-8255, Japan. Tel.: +81 88 461 5121. E-mail address: [email protected] (N. Murase). www.elsevier.com/locate/clinph Clinical Neurophysiology 118 (2007) 741–750

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
www.elsevier.com/locate/clinph
Clinical Neurophysiology 118 (2007) 741–750
Dynamic change of proximal conduction in demyelinatingneuropathies: A cervical magnetic stimulation combined
with maximum voluntary contraction
Takefumi Hitomi a, Ryuji Kaji b, Nagako Murase a,b,*, Nobuo Kohara c,Takahiro Mezaki a, Hiroyuki Nodera b, Takashi Kawamura d,
Akio Ikeda a, Hiroshi Shibasaki a,e
a Department of Neurology, Kyoto University Hospital, Japanb Department of Neurology, Tokushima University Hospital, Japan
c Department of Neurology, Kobe City General Hospital, Japand Department of Medicine and Epidemiology, Kyoto University Health Service, Japan
e Takeda General Hospital, Kyoto, Japan
Accepted 18 November 2006
Abstract
Objective: To evaluate conduction abnormalities in the nerves innervating the proximal muscles in demyelinating neuropathies (DN)using cervical magnetic stimulation.Methods: We applied cervical root magnetic stimulation in the biceps brachii muscles and examined its activity-dependent conductionchanges produced by maximal voluntary contraction (MVC) in 12 DN patients (seven chronic inflammatory demyelinating polyradic-uloneuropathy and five multifocal motor neuropathy), six motor neuron disease (MND) patients, and 12 healthy volunteers.Results: Defining the upper normal limit of motor threshold (31%) and latency (6.7 ms) of the compound muscle action potential(CMAP) as mean + 2SD, most DN patients revealed an abnormality in motor threshold (10/12) and latency (11/12) in contrast toMND patients (motor threshold (1/6) and latency (0/6)). These parameters contribute to the differentiation of DN from MND(P < 0.01). Furthermore, the MVC maneuver transiently decreased the CMAP amplitude ratio (after MVC/before MVC · 100) inDN (83 ± 18 %) compared with MND (P < 0.01). Two of three DN patients who showed normal motor threshold or latency as inMND were successfully differentiated from MND by the MVC maneuver.Conclusions: In DN patients, conduction abnormality in the nerves innervating the proximal muscles was revealed by cervical magneticstimulation combined with the MVC maneuver.Significance: Our results suggested that conduction abnormalities in the proximal nerves innervating the proximal muscles could be eval-uated by this method.� 2006 International Federation of Clinical Neurophysiology. Published by Elsevier Ireland Ltd. All rights reserved.
Keywords: Cervical magnetic stimulation; Proximal muscle; Activity-dependent conduction block; CIDP; MMN; MND
1388-2457/$32.00 � 2006 International Federation of Clinical Neurophysiology. Published by Elsevier Ireland Ltd. All rights reserved.
doi:10.1016/j.clinph.2006.11.013
Abbreviations: chronic inflammatory demyelinating polyradiculoneuropathy, CIDP; compound muscle action potential, CMAP; demyelinating neu-ropathy, DN; electromyogram, EMG; intravenous immunoglobulin, IVIg; maximum voluntary contraction, MVC; Medical Research Council, MRC;motor neuron disease, MND; multifocal motor neuropathy, MMN; nerve conduction study, NCS; analysis of variance, ANOVA.
* Corresponding author. Department of Neurology, National Hospital Organization, Utano National Hospital, Ondoyama-cho 8, Narutaki, Ukyo-ku,Kyoto 616-8255, Japan. Tel.: +81 88 461 5121.
E-mail address: [email protected] (N. Murase).

742 T. Hitomi et al. / Clinical Neurophysiology 118 (2007) 741–750
1. Introduction
For the diagnosis of acquired demyelinating neuropa-thies (DN), such as chronic inflammatory demyelinatingpolyradiculoneuropathy (CIDP) and multifocal motor neu-ropathy (MMN), motor nerve conduction studies (NCSs)for the distal hand muscles are commonly used to detectthe site of conduction block or slowing. When the lesionsite is located in the proximal segment, cervical root stim-ulation with a magnetic coil is also used. It effectively acti-vates the deep structures with little discomfort(Chokroverty et al., 1991; Cros et al., 1990) and can beused to evaluate proximal motor conduction (Bischoffet al., 1993; Boyacıyan et al., 1996; Inaba et al., 2002; Mae-gaki et al., 1994; Takada and Ravnborg, 2000; Wohrleet al., 1995).
It would, however, be difficult to test conduction abnor-malities in DN patients with severely atrophied hand mus-cles due to secondary axonal degeneration, because of thelow amplitude of compound muscle action potentials(CMAPs). NCSs using less atrophied proximal muscleswould, then, be feasible rather than those of distal handmuscles (Cros et al., 1990; Epstein, 1993). NCSs of themusculocutaneous nerve have been investigated by electricstimulation applied at the axilla and Erb’s point (Troja-borg, 1976). However, this can cause severe discomfort insome subjects and will not detect lesion sites more proximalthan Erb’s point.
According to previous reports (Cappelen-Smith et al.,2000; Kaji et al., 2000), patients with MMN and CIDPshowed a peculiar fatigue phenomenon after sustainedmuscle contraction. The CMAPs of their distal hand mus-cles showed significant decreases of amplitude and increas-es of threshold after a maximum contraction for 60 s(Cappelen-Smith et al., 2000; Kaji et al., 2000). These stud-ies indicate that hyperpolarization of the axonal membraneinduced by activity causes a transient and activity-depen-dent conduction block, resulting in easy fatigability.
In this study, we examined conduction and also investi-gated the dynamic changes of CMAP parameters beforeand after sustained voluntary contraction in proximal mus-cles to detect occult demyelinating lesions in the nervesinnervating the proximal muscle. We also compared thefindings before and after intravenous immunoglobulin(IVIg) therapy.
2. Methods
2.1. Subjects
Seven CIDP patients (Four women and three men, age35.4 ± 13.2 years (mean ± SD), range 19–60 years) and 5MMN patients (one woman and four men, age 56.2 ± 7.8years, range 48–64 years) participated in this study. SixMND patients (one woman and five men, age 60.0 ± 12.8years, range 43–73 years) served as disease controls, and12 healthy volunteers (three women and nine men, age
48.5 ± 15.9 years, range 26–72 years) served as normal con-trols. All patients but one (Patient 12 in Table 1) wererecruited from Kyoto University Hospital, and Patient 12from Tokushima University Hospital. The demographicdata of the patients are summarized in Table 1. Accordingto the conventional NCSs and F-wave latencies of themedian, ulnar, and tibial nerves (Viking 2 and 4, Nicolet,Madison, USA) for DN and needle EMG studies forMND, all of the patients fulfilled the diagnostic criteriafor each disease (Ad hoc subcommittee of the AmericanAcademy of Neurology AIDS Task Force, 1991; Sumner,1997; Brooks, 1994). Three-hertz repetitive stimulationapplied to the affected hand muscles excluded abnormalneuromuscular transmission in all patients. The strengthof the biceps brachii muscle was assessed in each subjectusing the Medical Research Council (MRC) scores (0–5points including 4+). Two CIDP patients and one MMNpatient (Patients 4, 5, and 10) had normal muscle strengthon examination, but all of them used to have weakness inthe biceps brachii muscles when the disease was active.Their disabilities were assessed using the Hughes functionalgrading scale (grade 4 = bound to bed, grade 3 = able towalk 5 m with aid, grade 2 = ambulates independently,grade 1 = minimal signs and symptoms and able to run).All CIDP and MMN patients were categorized into grades1, 2, or 3. Two MMN patients (Patients 8 and 9) with ele-vated cerebrospinal fluid protein were included in thisstudy because it is sometimes (30%) detected in MMN(Nobile-Orazio et al., 2005). All subjects gave theirinformed written consent to participate in the study, whichwas approved by the Institutional Ethics Committees ofKyoto University Hospital and Tokushima UniversityHospital.
2.2. Cervical magnetic stimulation
CMAPs were recorded from the biceps brachii musclefollowing stimulation at the cervical level with a magneticstimulator (Magstim Model 200TM, Magstim, UK) anda circular coil with an outer diameter of 12 cm (2.0 T atthe coil surface when connected to the magnetic stimula-tor). The center of the coil was placed over the C7 spinousprocess where the maximum CMAP amplitude for thebiceps brachii muscle is elicited (Cros et al., 1990). The coilcurrent traveled clockwise for the nerves innervating theright biceps brachii muscle and vice versa (Cros et al.,1990). CMAPs of the biceps brachii muscle were recordedon the side of weaker muscle strength or on the right side ifmuscle strength was similar on both sides. The subjectswere seated in a comfortable chair with their head bentslightly forward and their forearms fixed on an armrest.Surface electrodes were placed over the motor point(active) and over the tendon (reference) of the biceps bra-chii muscle. The ground electrode was placed between thestimulus site and the recording site. The coil position andthe subject’s posture were kept fixed during theexamination.
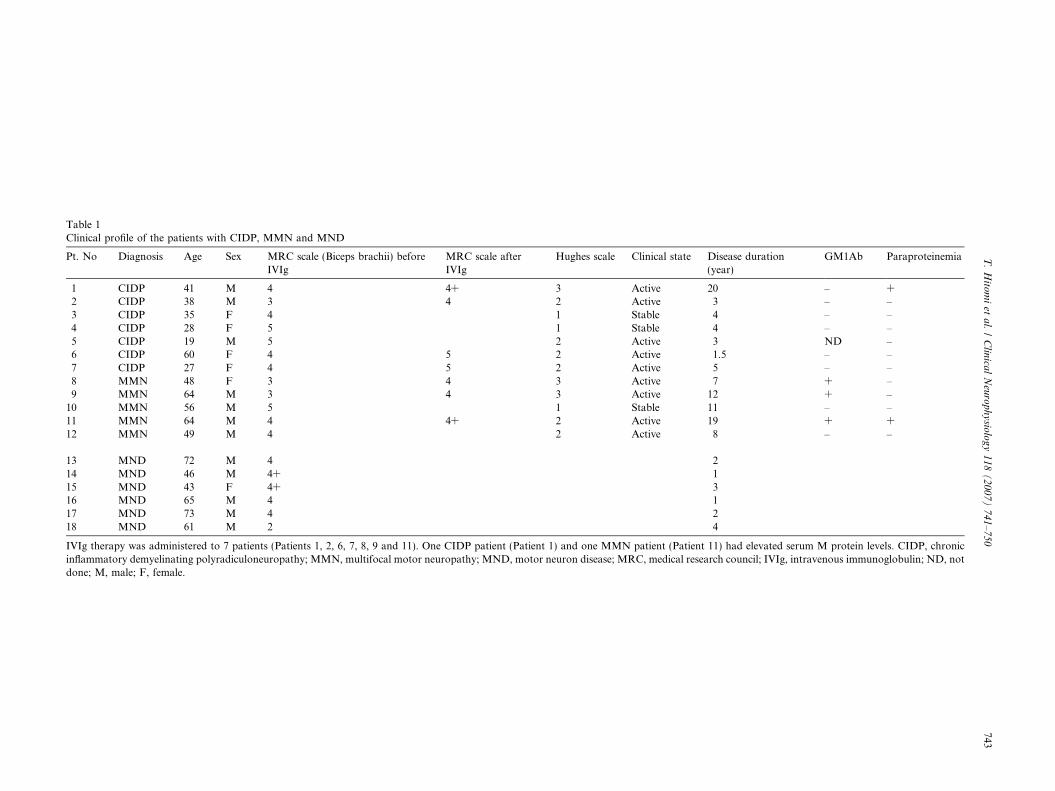
Table 1Clinical profile of the patients with CIDP, MMN and MND
Pt. No Diagnosis Age Sex MRC scale (Biceps brachii) beforeIVIg
MRC scale afterIVIg
Hughes scale Clinical state Disease duration(year)
GM1Ab Paraproteinemia
1 CIDP 41 M 4 4+ 3 Active 20 – +2 CIDP 38 M 3 4 2 Active 3 – –3 CIDP 35 F 4 1 Stable 4 – –4 CIDP 28 F 5 1 Stable 4 – –5 CIDP 19 M 5 2 Active 3 ND –6 CIDP 60 F 4 5 2 Active 1.5 – –7 CIDP 27 F 4 5 2 Active 5 – –8 MMN 48 F 3 4 3 Active 7 + –9 MMN 64 M 3 4 3 Active 12 + –
10 MMN 56 M 5 1 Stable 11 – –11 MMN 64 M 4 4+ 2 Active 19 + +12 MMN 49 M 4 2 Active 8 – –
13 MND 72 M 4 214 MND 46 M 4+ 115 MND 43 F 4+ 316 MND 65 M 4 117 MND 73 M 4 218 MND 61 M 2 4
IVIg therapy was administered to 7 patients (Patients 1, 2, 6, 7, 8, 9 and 11). One CIDP patient (Patient 1) and one MMN patient (Patient 11) had elevated serum M protein levels. CIDP, chronicinflammatory demyelinating polyradiculoneuropathy; MMN, multifocal motor neuropathy; MND, motor neuron disease; MRC, medical research council; IVIg, intravenous immunoglobulin; ND, notdone; M, male; F, female.
T.
Hito
mi
eta
l./
Clin
ical
Neu
rop
hy
siolo
gy
11
8(
20
07
)7
41
–7
50
743
744 T. Hitomi et al. / Clinical Neurophysiology 118 (2007) 741–750
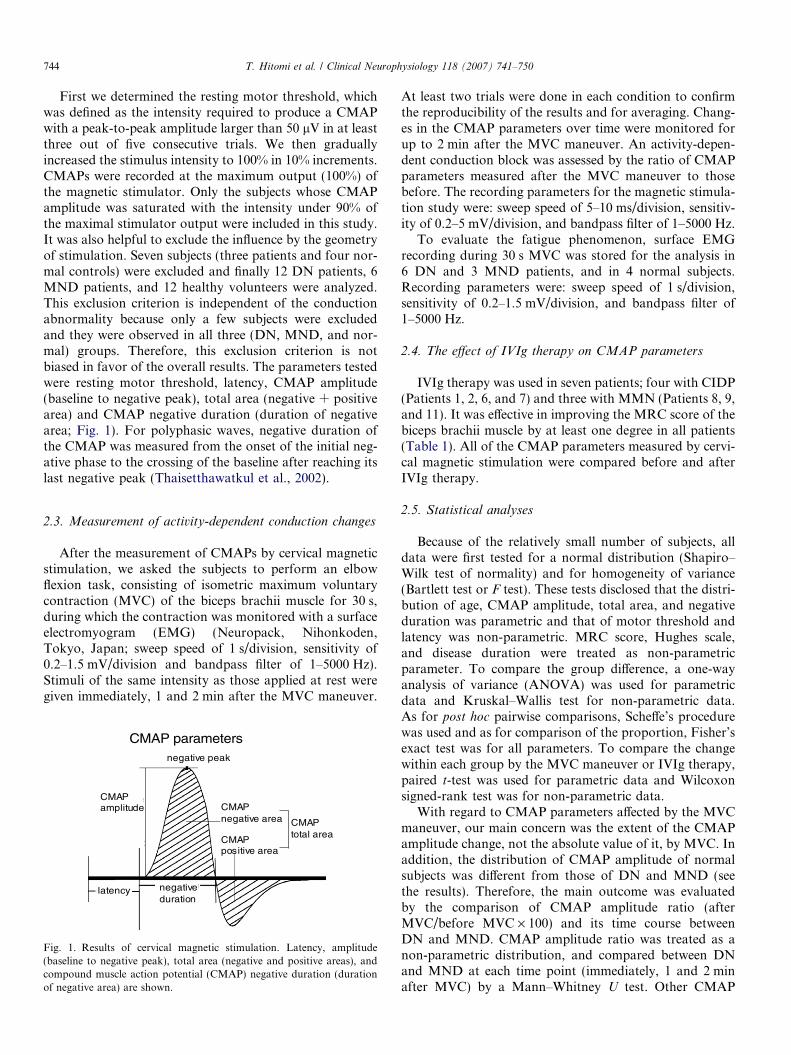
First we determined the resting motor threshold, whichwas defined as the intensity required to produce a CMAPwith a peak-to-peak amplitude larger than 50 lV in at leastthree out of five consecutive trials. We then graduallyincreased the stimulus intensity to 100% in 10% increments.CMAPs were recorded at the maximum output (100%) ofthe magnetic stimulator. Only the subjects whose CMAPamplitude was saturated with the intensity under 90% ofthe maximal stimulator output were included in this study.It was also helpful to exclude the influence by the geometryof stimulation. Seven subjects (three patients and four nor-mal controls) were excluded and finally 12 DN patients, 6MND patients, and 12 healthy volunteers were analyzed.This exclusion criterion is independent of the conductionabnormality because only a few subjects were excludedand they were observed in all three (DN, MND, and nor-mal) groups. Therefore, this exclusion criterion is notbiased in favor of the overall results. The parameters testedwere resting motor threshold, latency, CMAP amplitude(baseline to negative peak), total area (negative + positivearea) and CMAP negative duration (duration of negativearea; Fig. 1). For polyphasic waves, negative duration ofthe CMAP was measured from the onset of the initial neg-ative phase to the crossing of the baseline after reaching itslast negative peak (Thaisetthawatkul et al., 2002).
2.3. Measurement of activity-dependent conduction changes
After the measurement of CMAPs by cervical magneticstimulation, we asked the subjects to perform an elbowflexion task, consisting of isometric maximum voluntarycontraction (MVC) of the biceps brachii muscle for 30 s,during which the contraction was monitored with a surfaceelectromyogram (EMG) (Neuropack, Nihonkoden,Tokyo, Japan; sweep speed of 1 s/division, sensitivity of0.2–1.5 mV/division and bandpass filter of 1–5000 Hz).Stimuli of the same intensity as those applied at rest weregiven immediately, 1 and 2 min after the MVC maneuver.
CMAP parametersnegative peak
CMAPamplitude
latency negativeduration
CMAPtotal area
CMAPnegative area
CMAPpositive area
Fig. 1. Results of cervical magnetic stimulation. Latency, amplitude(baseline to negative peak), total area (negative and positive areas), andcompound muscle action potential (CMAP) negative duration (durationof negative area) are shown.
At least two trials were done in each condition to confirmthe reproducibility of the results and for averaging. Chang-es in the CMAP parameters over time were monitored forup to 2 min after the MVC maneuver. An activity-depen-dent conduction block was assessed by the ratio of CMAPparameters measured after the MVC maneuver to thosebefore. The recording parameters for the magnetic stimula-tion study were: sweep speed of 5–10 ms/division, sensitiv-ity of 0.2–5 mV/division, and bandpass filter of 1–5000 Hz.
To evaluate the fatigue phenomenon, surface EMGrecording during 30 s MVC was stored for the analysis in6 DN and 3 MND patients, and in 4 normal subjects.Recording parameters were: sweep speed of 1 s/division,sensitivity of 0.2–1.5 mV/division, and bandpass filter of1–5000 Hz.
2.4. The effect of IVIg therapy on CMAP parameters
IVIg therapy was used in seven patients; four with CIDP(Patients 1, 2, 6, and 7) and three with MMN (Patients 8, 9,and 11). It was effective in improving the MRC score of thebiceps brachii muscle by at least one degree in all patients(Table 1). All of the CMAP parameters measured by cervi-cal magnetic stimulation were compared before and afterIVIg therapy.
2.5. Statistical analyses
Because of the relatively small number of subjects, alldata were first tested for a normal distribution (Shapiro–Wilk test of normality) and for homogeneity of variance(Bartlett test or F test). These tests disclosed that the distri-bution of age, CMAP amplitude, total area, and negativeduration was parametric and that of motor threshold andlatency was non-parametric. MRC score, Hughes scale,and disease duration were treated as non-parametricparameter. To compare the group difference, a one-wayanalysis of variance (ANOVA) was used for parametricdata and Kruskal–Wallis test for non-parametric data.As for post hoc pairwise comparisons, Scheffe’s procedurewas used and as for comparison of the proportion, Fisher’sexact test was for all parameters. To compare the changewithin each group by the MVC maneuver or IVIg therapy,paired t-test was used for parametric data and Wilcoxonsigned-rank test was for non-parametric data.
With regard to CMAP parameters affected by the MVCmaneuver, our main concern was the extent of the CMAPamplitude change, not the absolute value of it, by MVC. Inaddition, the distribution of CMAP amplitude of normalsubjects was different from those of DN and MND (seethe results). Therefore, the main outcome was evaluatedby the comparison of CMAP amplitude ratio (afterMVC/before MVC · 100) and its time course betweenDN and MND. CMAP amplitude ratio was treated as anon-parametric distribution, and compared between DNand MND at each time point (immediately, 1 and 2 minafter MVC) by a Mann–Whitney U test. Other CMAP
Tab
le2
CM
AP
par
amet
ers
for
cerv
ical
mag
net
icst
imu
lati
on
Gro
up
Th
resh
old
(%)
Lat
ency
(ms)
CM
AP
amp
litu
de
(mV
)C
MA
Pto
tal
area
(mV
ms)
Neg
ativ
ed
ura
tio
n(m
s)
Dem
yeli
nat
ing
neu
rop
ath
y39
.7±
11.5
(P=
0.00
02)
9.4
±2.
9(P
=0.
0003
)2.
7±
2.7
(P<
0.00
01)
46.2
±45
.7(P
=0.
0003
)17
.6±
4.0
(P=
0.00
2)C
IDP
41.9
±11
.210
.4±
3.1
3.2
±2.
752
.1±
41.7
17.9
±4.
9M
MN
36.6
±12
.47.
9±
2.0
2.1
±2.
838
.0±
54.6
17.0
±2.
8M
ND
26.5
±10
.86.
3±
0.3
5.8
±2.
7(P
=0.
03)
73.7
±30
.7(P
=0.
04)
13.2
±2.
5N
orm
alsu
bje
cts
21.4
±4.
95.
7±
0.5
10.2
±3.
513
0.7
±47
.212
.7±
1.6
Lim
ito
fn
orm
alva
lue
(mea
ns
+2S
Da
or�
2SD
b)
31.2
a6.
7a4.
2b36
.3b
15.9
a
Val
ues
are
exp
ress
edas
mea
ns
±S
D.
Pva
lues
inp
aren
thes
esd
eno
teP
<0.
05(p
ost
ho
can
alys
is)
inC
MA
Pp
aram
eter
so
fd
emye
lin
atin
gn
euro
pat
hy
and
MN
Dw
hen
com
par
edw
ith
tho
seo
fn
orm
alsu
bje
cts.
CID
P,
chro
nic
infl
amm
ato
ryd
emye
lin
atin
gp
oly
rad
icu
lon
euro
pat
hy;
MM
N,
mu
ltif
oca
lm
oto
rn
euro
pat
hy;
MN
D,
mo
tor
neu
ron
dis
ease
.
T. Hitomi et al. / Clinical Neurophysiology 118 (2007) 741–750 745
parameters (total area, latency, and negative duration)were also analyzed by the same procedure.
Pearson’s correlation or Spearman rank correlationcoefficients were used to evaluate the relationship betweenthe patient characteristics (age, MRC scores, Hughesscales, and disease duration) and the CMAP parametersof biceps brachii muscle, or between the effect of IVIg ther-apy on the MRC scores and CMAP amplitude. The level ofstatistical significance was set at P < 0.05.
3. Results
There were no significant differences in any of theCMAP parameters obtained by conventional NCSs(data not shown) and cervical magnetic stimulation,between the patients with CIDP and those with MMN(Table 2). These two groups were thus regarded as a sin-gle DN group. The MND patients were significantly old-er than the CIDP patients (P = 0.01), but the mean ageof patients with DN (grouped CIDP and MMN patientstogether) (44.1 ± 15.2 years, range 19–64 years) was notsignificantly different from that of normal subjects (mean48.5 ± 15.9 years, range 26–72 years) or MND patients(mean 60.0 ± 12.8 years, range 43–73 years). Weaknessof biceps brachii muscles, as expressed by MRC scores,was similar among the three groups (DN and MND)(Table 1).
3.1. CMAP parameters on cervical magnetic stimulation
Motor threshold, latency, CMAP amplitude, CMAPtotal area, and CMAP negative duration were significantlydifferent among the three groups (DN, MND, and normal)(P = 0.005 for motor threshold; P < 0.0001 for latency;P < 0.0001 for CMAP amplitude; P = 0.0003 for CMAPtotal area; and P = 0.0009 for CMAP negative duration;Table 2).
The post hoc analysis showed that the DN patients had asignificantly higher motor threshold, longer latency, small-er CMAP amplitude, smaller CMAP total area, and longerCMAP negative duration than normal subjects (Table 2).When compared with MND patients, DN patients had asignificantly higher motor threshold (P = 0.03), longerlatency (P = 0.01), and longer CMAP negative duration(P = 0.02). CMAP amplitude and total area were similarbetween these two patient groups. The MND patientshad significantly lower CMAP amplitudes and total areasthan normal subjects (Table 2).
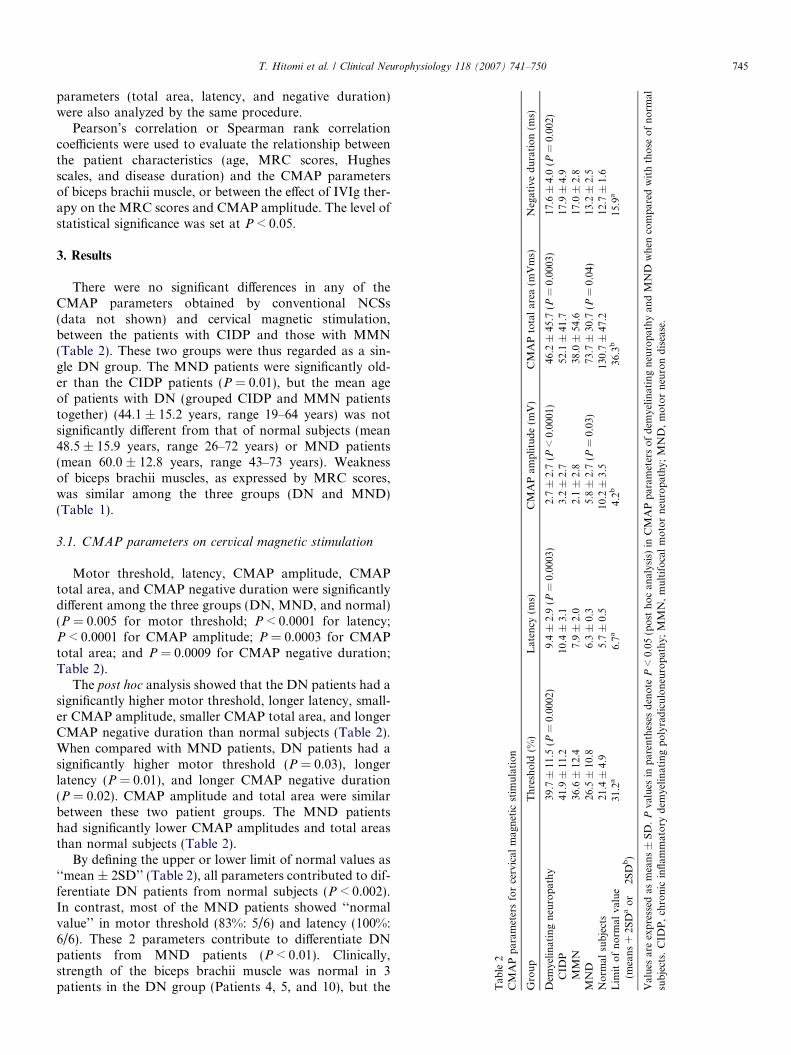
By defining the upper or lower limit of normal values as‘‘mean ± 2SD’’ (Table 2), all parameters contributed to dif-ferentiate DN patients from normal subjects (P < 0.002).In contrast, most of the MND patients showed ‘‘normalvalue’’ in motor threshold (83%: 5/6) and latency (100%:6/6). These 2 parameters contribute to differentiate DNpatients from MND patients (P < 0.01). Clinically,strength of the biceps brachii muscle was normal in 3patients in the DN group (Patients 4, 5, and 10), but the
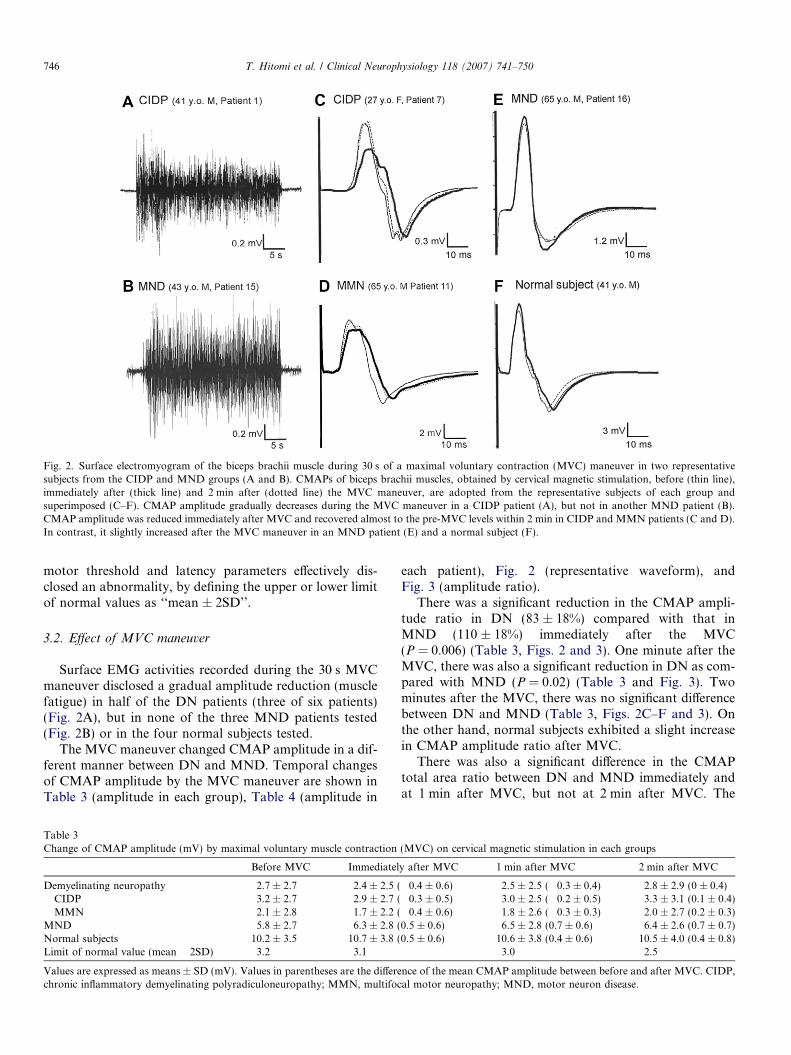
Fig. 2. Surface electromyogram of the biceps brachii muscle during 30 s of a maximal voluntary contraction (MVC) maneuver in two representativesubjects from the CIDP and MND groups (A and B). CMAPs of biceps brachii muscles, obtained by cervical magnetic stimulation, before (thin line),immediately after (thick line) and 2 min after (dotted line) the MVC maneuver, are adopted from the representative subjects of each group andsuperimposed (C–F). CMAP amplitude gradually decreases during the MVC maneuver in a CIDP patient (A), but not in another MND patient (B).CMAP amplitude was reduced immediately after MVC and recovered almost to the pre-MVC levels within 2 min in CIDP and MMN patients (C and D).In contrast, it slightly increased after the MVC maneuver in an MND patient (E) and a normal subject (F).
746 T. Hitomi et al. / Clinical Neurophysiology 118 (2007) 741–750
motor threshold and latency parameters effectively dis-closed an abnormality, by defining the upper or lower limitof normal values as ‘‘mean ± 2SD’’.
3.2. Effect of MVC maneuver
Surface EMG activities recorded during the 30 s MVCmaneuver disclosed a gradual amplitude reduction (musclefatigue) in half of the DN patients (three of six patients)(Fig. 2A), but in none of the three MND patients tested(Fig. 2B) or in the four normal subjects tested.
The MVC maneuver changed CMAP amplitude in a dif-ferent manner between DN and MND. Temporal changesof CMAP amplitude by the MVC maneuver are shown inTable 3 (amplitude in each group), Table 4 (amplitude in
Table 3Change of CMAP amplitude (mV) by maximal voluntary muscle contraction
Before MVC Immediatel
Demyelinating neuropathy 2.7 ± 2.7 2.4 ± 2.5 (CIDP 3.2 ± 2.7 2.9 ± 2.7 (MMN 2.1 ± 2.8 1.7 ± 2.2 (
MND 5.8 ± 2.7 6.3 ± 2.8 (Normal subjects 10.2 ± 3.5 10.7 ± 3.8 (Limit of normal value (mean � 2SD) 3.2 3.1
Values are expressed as means ± SD (mV). Values in parentheses are the differechronic inflammatory demyelinating polyradiculoneuropathy; MMN, multifoc
each patient), Fig. 2 (representative waveform), andFig. 3 (amplitude ratio).
There was a significant reduction in the CMAP ampli-tude ratio in DN (83 ± 18%) compared with that inMND (110 ± 18%) immediately after the MVC(P = 0.006) (Table 3, Figs. 2 and 3). One minute after theMVC, there was also a significant reduction in DN as com-pared with MND (P = 0.02) (Table 3 and Fig. 3). Twominutes after the MVC, there was no significant differencebetween DN and MND (Table 3, Figs. 2C–F and 3). Onthe other hand, normal subjects exhibited a slight increasein CMAP amplitude ratio after MVC.
There was also a significant difference in the CMAPtotal area ratio between DN and MND immediately andat 1 min after MVC, but not at 2 min after MVC. The
(MVC) on cervical magnetic stimulation in each groups
y after MVC 1 min after MVC 2 min after MVC
�0.4 ± 0.6) 2.5 ± 2.5 (�0.3 ± 0.4) 2.8 ± 2.9 (0 ± 0.4)�0.3 ± 0.5) 3.0 ± 2.5 (�0.2 ± 0.5) 3.3 ± 3.1 (0.1 ± 0.4)�0.4 ± 0.6) 1.8 ± 2.6 (�0.3 ± 0.3) 2.0 ± 2.7 (0.2 ± 0.3)0.5 ± 0.6) 6.5 ± 2.8 (0.7 ± 0.6) 6.4 ± 2.6 (0.7 ± 0.7)0.5 ± 0.6) 10.6 ± 3.8 (0.4 ± 0.6) 10.5 ± 4.0 (0.4 ± 0.8)
3.0 2.5
nce of the mean CMAP amplitude between before and after MVC. CIDP,al motor neuropathy; MND, motor neuron disease.

Table 4Change of CMAP amplitude (mV) by maximal voluntary musclecontraction (MVC) on cervical magnetic stimulation in each patients
Pt.No
Diagnosis BeforeMVC
Immediatelyafter MVC
1 min afterMVC
2 min afterMVC
1 CIDP 2.9 2.3 2.4 2.82 CIDP 0.8 0.7 0.9 1.03 CIDP 3.4 2.1 2.6 2.94 CIDP 4.5 5.1 4.9 5.05 CIDP 8.6 8.1 7.6 9.46 CIDP 0.9 0.9 0.9 0.77 CIDP 1.4 1.0 1.4 1.48 MMN 0.5 0.3 0.2 0.49 MMN 0.3 0.3 0.4 0.4
10 MMN 1.7 1.7 1.7 1.911 MMN 7.0 5.5 6.4 6.612 MMN 1.0 0.6 0.3 0.4
13 MND 2.7 3.4 4.1 4.414 MND 8.9 10.3 10.2 9.715 MND 5.5 5.8 6.3 6.316 MND 7.1 7.6 7.2 7.117 MND 7.9 7.7 8.7 8.818 MND 2.7 2.8 2.6 2.5
CIDP, chronic inflammatory demyelinating polyradiculoneuropathy;MMN, multifocal motor neuropathy; MND, motor neuron disease.
T. Hitomi et al. / Clinical Neurophysiology 118 (2007) 741–750 747
other parameters of latency and CMAP negative durationwere not significantly altered after the MVC between DNand MND.
Within DN patients, the CMAP amplitude ratio was notsignificantly correlated with any of the patient characteris-tics (age, MRC scores, Hughes scales, and disease dura-tion), but the CMAP total area ratio (immediately afterMVC/before MVC · 100) was significantly correlated with
Demyelinating Neuropathy (CIDP and MMN)
MND
20
40
60
80
100
120
140
Just afterMVC
Before MVC
MND
%160
A B
MMNCIDP
Just afterMVC
1 min afterMVC
2 min afterMVC
BeforeMVC
20
40
60
80
100
120
140
%160
Fig. 3. Time course of changes in CMAP amplitude ratio (immediately after Mand after the MVC maneuver in CIDP and MMN patients (A), in MND patienamplitude decreased immediately after the MVC maneuver in most of the CIDP2 min (A). In contrast, MND patients and normal subjects showed a slight increlimit of normal values of the CMAP amplitude ratio as ‘‘mean � 2SD of normaamplitude ratio in one CIDP and two MMN patients who exhibited normalsuccessfully differentiated from MND.
the strength of the biceps brachii muscle: the weaker themuscle power, the greater the reduction in CMAP totalarea immediately after the MVC maneuver (P = 0.009,q = 0.785).
3.3. Utility of MVC maneuver
When the lower limit of the normal value of the CMAPamplitude ratio (immediately after MVC/beforeMVC · 100) was defined ‘‘mean � 2SD’’ (i.e., about93%), only seven out of 12 DN patients showed abnormal-ity. However, this parameter was appropriate for differen-tiating between DN from MND because CMAPamplitude ratio was more than 93% in all of the 12 normalsubjects and six MND patients tested. Moreover, three outof 12 DN patients (Patients 5, 11, and 12) showed normalmotor threshold or latency, but the MVC maneuver suc-cessfully differentiated two DN patients (Patients 11 and12) from MND (Fig. 3A).
3.4. Effect of IVIg on CMAP parameters
All of the seven patients (four CIDP and three MMN)who were treated by IVIg showed a clinical improvementincluding the strength of their biceps brachii muscles asrevealed by MRC scores (Table 1), and a significantincrease in CMAP amplitude (before IVIg: 2.0 ± 2.4 mV,after IVIg: 2.7 ± 2.1 mV, P = 0.03). Other parametersincluding CMAP total area did not change. The ratio ofbase CMAP amplitude (‘after IVIg and before MVC’ to‘before IVIg and before MVC’) was significantly correlatedwith the difference of MRC scores (after–before IVIg)
1 min afterMVC
2 min afterMVC
Normal subjects
20
40
60
80
100
120
140
Just afterMVC
1 min afterMVC
2 min afterMVC
Before MVC
Normal subjects
%160
C
VC/before MVC · 100) assessed by cervical magnetic stimulation beforets (B), and in normal subjects (C). Each individual datum is plotted. CMAP
and MMN patients, but had almost recovered to pre-MVC values withinase after the MVC maneuver (B and C). Gray bold lines indicate the lower
l subjects’’ (i.e., 93 %). Crosses denote the time course of changes in CMAPmotor threshold or latency (A). Among these patients, two patients were
748 T. Hitomi et al. / Clinical Neurophysiology 118 (2007) 741–750
(P = 0.03, r = 0.794). Nevertheless IVIg therapy did notimprove the MVC-induced reduction of CMAP amplitudeor total area.
4. Discussion
The present study demonstrated that cervical root mag-netic stimulation combined with MVC maneuver could dif-ferentiate DN from MND and normal subjects. Motorthreshold was increased and CMAP latencies were pro-longed in most DN patients, and the MVC maneuverdecreased CMAP amplitude selectively only in DNpatients. Although the number of subjects was small andwe tested the already proven patients, our preliminary find-ings suggested that the dynamic change of CMAP afterMVC could predict demyelinating lesions amenable totreatment.
4.1. Cervical magnetic stimulation
Cervical magnetic stimulation is considered to stimulatethe proximal motor roots around the neural foramen, 2–6 cm from the spinal cord (Samii et al., 1998; Chokrovertyet al., 1991; Inaba et al., 2002), and it has been used toexamine the nerves innervating proximal muscles whenelectric stimulation to the proximal nerve segments is tech-nically difficult. Despite its clinical utility (Cros et al.,1990), the decreased CMAP amplitude and increased con-duction time measured in the biceps brachii muscles wererarely demonstrated in DN patients (Takada and Ravn-borg, 2000). Our findings of increased motor threshold,prolonged latencies, decreased CMAP amplitudes, andtotal areas were compatible with previous reports of thedistal muscles by conventional NCSs (Kimura, 2001) orcervical magnetic stimulation (Oge et al., 1997). In thisstudy, the cervical magnetic stimulation was also able todisclose the presence of demyelination in Patients 4, 5,and 10 who had full muscle power (MRC grade 5).
One problem of stimulating a nerve at depth by cervicalmagnetic stimulation was the difficulty in achieving supra-maximum stimulation. We used a round coil to stimulate abroad area, and asked the subjects to flex their neck ante-riorly to allow fixing the coil firmly. Despite these precau-tions, it was difficult to overcome the geometry effect. Thiswas important because the motor threshold was seriouslyinfluenced by this factor. Thus, we only recruited subjectswhose CMAP amplitude was saturated with an intensityat less than 90% of the maximal stimulator output and thenstimulated them with 100% stimulator output. We con-firmed that the CMAP waveform was actually reproducibleeven after MVC in the present study. Even so, DN patientsmay not be stimulated with supra-maximum intensity afterthe maneuver because DN patients showed an increasedthreshold after MVC (Cappelen-Smith et al., 2000; Kajiet al., 2000). This technical limitation exists in our method.We could not differentiate the activity-dependent hyperpo-larization, from the insufficient stimulation after MVC due
to elevated motor threshold, in some subjects. Neverthelessour results were meaningful because two phenomena arebased on the same mechanism of elevated threshold. Thusthis technical limitation did not deny our methodology.
4.2. Activity-dependent conduction block
Sustained muscle contraction can produce persistentaxonal hyperpolarization. When the motor axon con-ducts trains of impulses, Na+ ions accumulate insidethe motor axon. This altered distribution stimulates theNa+/K+ pump, resulting in axonal hyperpolarizationbecause the ion swap of this pump activity is not bal-anced (·3 Na+ out for ·2 K+ in). This hyperpolarizationdictates an elevated threshold of the axonal membranepotential (Burke et al., 2001; Vagg et al., 1998; Ingliset al., 1998; Morita et al., 1993; Bostock and Grafe,1985). Basically for the safety transmission of action cur-rent at the Node of Ranvier, the outward capacitativecurrent at the next node (the driving current) mustexceed the threshold current. The ratio of the drivingcurrent to the threshold current is called safety factorof transmission. It is normally >5, and if it falls below1 conduction will fail (Burke et al., 2001). When the safe-ty factor decreases, conduction failure due to hyperpolar-ization occurs while trains of impulses are beingconducted through the axon (Bostock and Grafe, 1985).This MVC-induced hyperpolarization block occurs inboth CIDP and MMN (Cappelen-Smith et al., 2000; Kajiet al., 2000). This conduction failure after the MVCmaneuver was consistent with our results. However, wecould not exactly examine the motor threshold afterMVC because it took at least 1–2 min to detect it andreduced CMAP amplitude recovered within 2 min afterMVC. We could only see the amplitude and area changewith the same intensity as those before MVC. Since theprevious studies demonstrated conduction block accom-panied with elevated motor threshold (Cappelen-Smithet al., 2000; Kaji et al., 2000), it is reasonable to considerthis CMAP change was activity-dependent conductionblock due to elevated motor threshold.
Another possibility is that the amplitude decrement afterMVC might be the effect of few motor unit potentials orphase cancellation, because baseline CMAP amplitudewas small in some DN patients. However, it is not plausiblebecause CMAP negative duration was not changed. Someindividual data did not support this possibility, either.Three out of 7 DN patients with preserved CMAP ampli-tude (>1.0 mV) showed a decreased CMAP amplituderatio. In contrast, 2 MND patients (Patients 13 and 18)with small amplitude (Patient 13: 2.8 mV, Patient 18:2.7 mV) did not show a decrement after MVC (CMAPamplitude ratio: Patient 13: 127%, Patient 18: 106%). Inaddition, a positive correlation between MRC scores andCMAP amplitude ratio could suggest high vulnerabilityof the axonal membrane in the nerves innervating moreseverely affected muscles in DN.

T. Hitomi et al. / Clinical Neurophysiology 118 (2007) 741–750 749
In the clinical situation, activity-dependent conductionblock may explain fatigability in patients with CIDP andMMN as well as in patients with multiple sclerosis (Petajanand White, 2000). Most of our patients complained thatthey were easily fatigued (all seven CIDP patients and fourof five MMN patients). As shown in their surface EMG(Fig. 2A), they felt fatigue when the muscle contractionwas sustained.
Fatigue phenomena are well documented in various dis-eases of neuromuscular transmission. Repetitive nervestimulation at three hertz shows significant decrease ofCMAP amplitudes at the 4th or 5th stimulus in myastheniagravis. We also tested three-hertz stimulation in all of ourpatients who showed activity-dependent conduction block,and found no decrement. Defects of neuromuscular trans-mission are therefore unlikely in our cases.
Easy fatigability was also seen in four MND patients,although they did not show a clear decrement of CMAPamplitudes during MVC. Some papers reported thedecreased amplitudes by exercise and the fatigabilityseemed to be the result of the impairment of neuromuscu-lar transmission, especially in a rapidly progressive form ofMND (Kimura, 2001; Killian et al., 1994). This discrepan-cy in our data compared with that of others may be due toa difference in clinical course (Kimura, 2001; Killian et al.,1994). Other studies assessed the fatigability in MNDpatients during intermittent contraction and they conclud-ed it as having a central (Kent-Braun and Miller, 2000) ormuscular origin (Sharma et al., 1995; Sharma and Miller,1996).
On the other hand, CMAP amplitude increased inMND after sustained muscle contraction in some otherstudies (Sharma et al., 1995; Sharma and Miller, 1996) asshown in our study. The increment of CMAP after MVCin some normal subjects and MND patients in our studyindicates some possibilities. One is, despite every effort touse a supra-maximal stimulation as described in the paper,the stimulus might have been slightly less than adequate inthese cases. Other possibilities would include ‘‘pseudofacil-itation’’, based on hypersynchronization after tetanic con-traction. Increased area itself is not a reliable reason ofdenying the pseudofacilitation, because this phenomenon,which primarily affects the amplitude, could also alter thearea under the waveform based on phase cancellation.Also, it is possible that posttetanic potentiation increasesindividual action potentials recorded from muscle fibers(which are hyperpolarized) (Thomas et al., 2006; Burkeet al., 2001). If so, CMAP, as sum of these increased unitdischarges, also become larger (Hicks et al., 1989; McCo-mas et al., 1994).
The exact mechanism is not clarified yet, but whateverthe underlying mechanism for the unexpected posttetanicincrease, this change goes opposite to the finding inpatients with DN, which is associated with decrease inthe size of CMAP. Thus, this will not in any way alterour primary conclusion seen in this group of patients com-pared to the controls and MND.
4.3. Effect of IVIg on CMAP parameters
IVIg therapy, which is effective for treating both CIDP(Mendell et al., 2001; Hughes et al., 2001) and MMN(Federico et al., 2000; Van den Berg-Vos et al., 2002),increased the CMAP amplitude in all of the patients treat-ed, but the decrease of CMAP amplitude after MVCmaneuver was not improved. The lack of effect for activi-ty-dependent conduction block was concordant with theonly partial effect of IVIg therapy on the fatigability. Itmight reflect the remaining instability of the axonal mem-brane, resulting in the relatively short duration (around 2months) of the clinical effect of IVIg.
5. Conclusion
The nerves innervating the proximal muscles revealedconduction failure immediately after the MVC maneuverin patients with DN. The techniques used in this studyare regarded as a dynamic conduction test in the timedomain rather than in the space or nerve length domain,and is a possible method for differentiating treatable condi-tions from MND. This technique might detect occultlesions in the proximal site, if present, even though distalmuscles are not available because of the severe atrophyby secondary axonal degeneration.
Acknowledgements
We thank Dr. Jun Kimura (University of Iowa, IowaCity, IA) for comments on CMAP change. We thank Dr.Nobuyuki Oka (South Kyoto Hospital, Japan) for assess-ing the antiganglioside antibody titers and sural nervebiopsy. We thank Drs. Akira Kuzuya and HirofumiYamashita for their help with some experiments.
References
Ad hoc subcommittee of the American Academy of Neurology AIDSTask Force. Research criteria for diagnosis of chronic inflamma-tory demyelinating polyneuropathy (CIDP). Neurology1991;41:617–618.
Bischoff C, Meyer BU, Machetanz J, Conrad B. The value of magneticstimulation in the diagnosis of radiculopathies. Muscle Nerve1993;16:154–61.
Bostock H, Grafe P. Activity-dependent excitability changes in normaland demyelinated rat spinal root axons. J Physiol 1985;365:239–57.
Boyacıyan A, Oge AE, Yazıcı J, Aslay I, Baslo A. Electrophysiologicalfindings in patients who received radiation therapy over the brachialplexus: a magnetic stimulation study. Electroencephalogr Clin Neuro-physiol 1996;101:483–90.
Brooks BR. El Escorial World Federation of Neurology criteria for thediagnosis of amyotrophic lateral sclerosis. J Neurol Sci1994;124(Supplement):96–107.
Burke D, Kiernan MC, Bostock H. Excitability of human axons. ClinNeurophysiol 2001;112:1575–85.
Cappelen-Smith C, Kuwabara S, Lin CS, Mogyoros I, Burke D.Activity-dependent hyperpolarization and conduction block inchronic inflammatory demyelinating polyneuropathy. Ann Neurol2000;48:826–32.

750 T. Hitomi et al. / Clinical Neurophysiology 118 (2007) 741–750
Chokroverty S, Picone MA, Chokroverty M. Percutaneous magnetic coilstimulation of human cervical vertebral column: site of stimulation andclinical application. Electroencephalogr Clin Neurophysiol1991;81:359–65.
Cros D, Chiappa KH, Gominak S, Fang J, Santamaria J, King PJ, et al.Cervical magnetic stimulation. Neurology 1990;40:1751–6.
Epstein CM. Magnetic mapping of human cervical nerve roots: variationin normal subjects. Electroencephalogr Clin Neurophysiol1993;89:145–53.
Federico P, Zochodne DW, Hahn AF, Brown WF, Feasby TE. Multifocalmotor neuropathy improved by IVIg: randomized, double-blind,placebo-controlled study. Neurology 2000;55:1256–62.
Hicks A, Fenton J, Garner S, McComas AJ. M wave potentiation duringand after muscle activity. J Appl Physiol 1989;66:2606–10.
Hughes R, Bensa S, Willison H, Van den Bergh P, Comi G, Illa I, et al.Inflammatory Neuropathy Cause and Treatment (INCAT) Group.Randomized controlled trial of intravenous immunoglobulin versusoral prednisolone in chronic inflammatory demyelinating polyradicu-loneuropathy. Ann Neurol 2001;50:195–201.
Inaba A, Yokota T, Otagiri A, Nishimura T, Saito Y, Ichikawa T, et al.Electrophysiological evaluation of conduction in the most proximalmotor root segment. Muscle Nerve 2002;25:608–11.
Inglis JT, Leeper JB, Wilson LR, Gandevia SC, Burke D. The develop-ment of conduction block in single human axons following a focalnerve injury. J Physiol 1998;513:127–33.
Kaji R, Bostock H, Kohara N, Murase N, Kimura J, Shibasaki H.Activity-dependent conduction block in multifocal motor neuropathy.Brain 2000;123:1602–11.
Kent-Braun JA, Miller RG. Central fatigue during isometricexercise in amyotrophic lateral sclerosis. Muscle Nerve2000;23:909–14.
Killian JM, Wilfong AA, Burnett L, Appel SH, Boland D. Decrementalmotor responses to repetitive nerve stimulation in ALS. Muscle Nerve1994;17:747–54.
Kimura J. Electrodiagnosis in diseases of nerve and muscle: principles andpractice. 3rd ed. Oxford: Oxford University Press; 2001.
Maegaki Y, Inagaki M, Takeshita K. Cervical magnetic stimulation inchildren and adolescents: normal values and evaluation of theproximal lesion of the peripheral motor nerve in cases with polyra-diculoneuropathy. Electroencephalogr Clin Neurophysiol1994;93:318–23.
Mendell JR, Barohn RJ, Freimer ML, Kissel JT, King W, Nagaraja HN,et al. Working Group on Peripheral Neuropathy. Randomizedcontrolled trial of IVIg in untreated chronic inflammatory demyelin-ating polyradiculoneuropathy. Neurology 2001;56:445–9.
McComas AJ, Galea V, Einhorn RW. Pseudofacilitation: a misleadingterm. Muscle Nerve 1994;17:599–607.
Morita K, David G, Barrett JN, Barrett EF. Posttetanic hyperpolarizationproduced by electrogenic Na+-K+ pump in lizard axons impaled neartheir motor terminals. J Neurophysiol 1993;70:1874–84.
Nobile-Orazio E, Cappellari A, Priori A. Multifocal motor neuropathy:current concepts and controversies. Muscle Nerve 2005;31:663–80.
Oge AE, Boyaciyan A, Gurvit H, Yazici J, Degirmenci M, Kantemir E.Magnetic nerve root stimulation in two types of brachial plexus injury:segmental demyelination and axonal degeneration. Muscle Nerve1997;20:823–32.
Petajan JH, White AT. Motor-evoked potentials in response to fatiguinggrip exercise in multiple sclerosis patients. Clin Neurophysiol2000;111:2188–95.
Samii A, Luciano CA, Dambrosia JM, Hallett M. Central motorconduction time: reproducibility and discomfort of different methods.Muscle Nerve 1998;21:1445–50.
Sharma KR, Miller RG. Electrical and mechanical properties of skeletalmuscle underlying increased fatigue in patients with amyotrophiclateral sclerosis. Muscle Nerve 1996;19:1391–400.
Sharma KR, Kent-Braun JA, Majumdar S, Huang Y, Mynhier M, WeinerMW, et al. Physiology of fatigue in amyotrophic lateral sclerosis.Neurology 1995;45:733–40.
Sumner A. Consensus criteria for the diagnosis of partial conductionblock and multifocal motor neuropathy. In: Kimura J, Kaji R, editors.Physiology of ALS and related diseases. Amsterdam: Elsevier; 1997.p. 221–7.
Thaisetthawatkul P, Logigian EL, Herrmann DN. Dispersion of the distalcompound muscle action potential as a diagnostic criterion for chronicinflammatory demyelinating polyneuropathy. Neurology2002;59:1526–32.
Takada H, Ravnborg M. Magnetically evoked motor potentials indemyelinating and axonal polyneuropathy: a comparative study. EurJ Neurol 2000;7:63–9.
Thomas CK, Johansson RS, Bigland-Ritchie B. EMG changes in humanthenar motor units with force potentiation and fatigue. J Neurophysiol2006;95:1518–26.
Trojaborg W. Motor and sensory conduction in the musculocutaneousnerve. J Neurol Neurosurg Psychiatry 1976;39:890–9.
Vagg R, Mogyoros I, Kiernan MC, Burke D. Activity-dependenthyperpolarization of human motor axons produced by natural activity.J Physiol 1998;507:919–25.
Van den Berg-Vos RM, Franssen H, Wokke JH, Van den Berg LH.Multifocal motor neuropathy: long-term clinical and electrophysio-logical assessment of intravenous immunoglobulin maintenance treat-ment. Brain 2002;125:1875–86.
Wohrle JC, Kammer T, Steinke W, Hennerici M. Motor evoked potentialsto magnetic stimulation in chronic and acute inflammatory demyelin-ating polyneuropathy. Muscle Nerve 1995;18:904–6.
Related Documents











