ACUTE LIVER FAILURE Dr. LEONARDO DAIRY, SpPD – KGEH

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

ACUTE LIVER FAILURE
ACUTE LIVER FAILURE
Dr. LEONARDO DAIRY, SpPD – KGEH

DEFINITIONSDEFINITIONSDEFINITIONSDEFINITIONS
This is a general term applied to the rapid development of hepatic synthetic dysfunction associated with significant coagulopathy, usually defined by a prothrombin time or factor V level less than 50% of normal. The designation severe acute liver failure is applied when hepatic encephalopathy develops.

KLASSIFICATIONKLASSIFICATIONKLASSIFICATIONKLASSIFICATIONACUTE LIVER FAILURE,acute liver disease
with clinically jaundice to encephalopathy progresive rapidly
FULMINANT HEPATIC FAILURE, acute liver failure with hepatic encephalopathy,develoving less than 2 weeks or 8 weeks after onset jaundice
SUBFULMINANT HEPATIC FAILURE, acute liver disease with hepatic encepalopathy,develoving from 2/8 weeks to 3/6 month onset jaundice

KLASSIFICATIONKLASSIFICATIONO ”GRADY dkk : Based liver failure, onset of jaundice,
encepalopathyHYPERACUTE LIVER FAILURE interval less than 7 daysACUTE LIVER FAILURE interval 8 and 28 days SUBACUTE LIVER FAILURE interval between 5 and 12 weeks
EPIDEMIOLOGYEPIDEMIOLOGYEPIDEMIOLOGYEPIDEMIOLOGYThere are few reliable data on the incidence of acute
liver failure or FHF because there is no standard ICD-9 code specific for FHF
Using data from deaths, hospitalizations with death certificates, and discharge diagnoses, the number of deaths from FHF is estimated to be 3.5 permillion, with a hospitalization rate of 31.2 per million
Based on the Centers for Disease Control and Prevention Viral Hepatitis Surveillance Program and Sentinel Counties Study data, the total number of annual deaths due to acute viral hepatitis in the USA is approximately 2000

ETIOLOGY ETIOLOGY (FHF)(FHF)ETIOLOGY ETIOLOGY (FHF)(FHF)
Cause Frequency(%)
Acetaminophen overdose 39Other drug or toxin 13Indeterminate cause 17Hepatitis B 7Hepatitis A 4Various other identified causes 20
ETIOLOGY ETIOLOGY (AHF)(AHF)ETIOLOGY ETIOLOGY (AHF)(AHF)Viral hepatitis Hepatitis A,B,C,D,E Hepatitis due to other viruses, Herpes viruses 1,2
6 Adenovirus,Epstein Barr virus, CytomegalovirusDILI, Acetaminophen overdose Idiosyncratic drug
reactionsToxins ,Amanita phalloides Organicsolvents,Phosp.
Metabolic, Acute fatty liver of pregnancy, Reye’s syndrome
Vascular events,Acute circulatory failure Budd–Chiari syndrome Veno-occlusive disease,Heat stroke
Miscellaneous, Wilson disease AIH,Massive infiltration with tumor Liver transplantation with primary graft nonfunction
CLINICAL APPERANCECLINICAL APPERANCECLINICAL APPERANCECLINICAL APPERANCEICKTERUS PROGRESIF
BILIRUBIN > 20mg %
NAUSEA,MALAISE,VOMITING,FEVER.LIVER SIZE
SMALL.COMA MAY RAPIDLY
(FEWDAYS).TACHYCARDIA,HYPOTENSION,HYPE
RVENTILAT ION ,CEREBERAL OEDEME ARE
LATER FEATURES
PROLONG PROTROMBIN TIME,ALT/AST
INCREASE
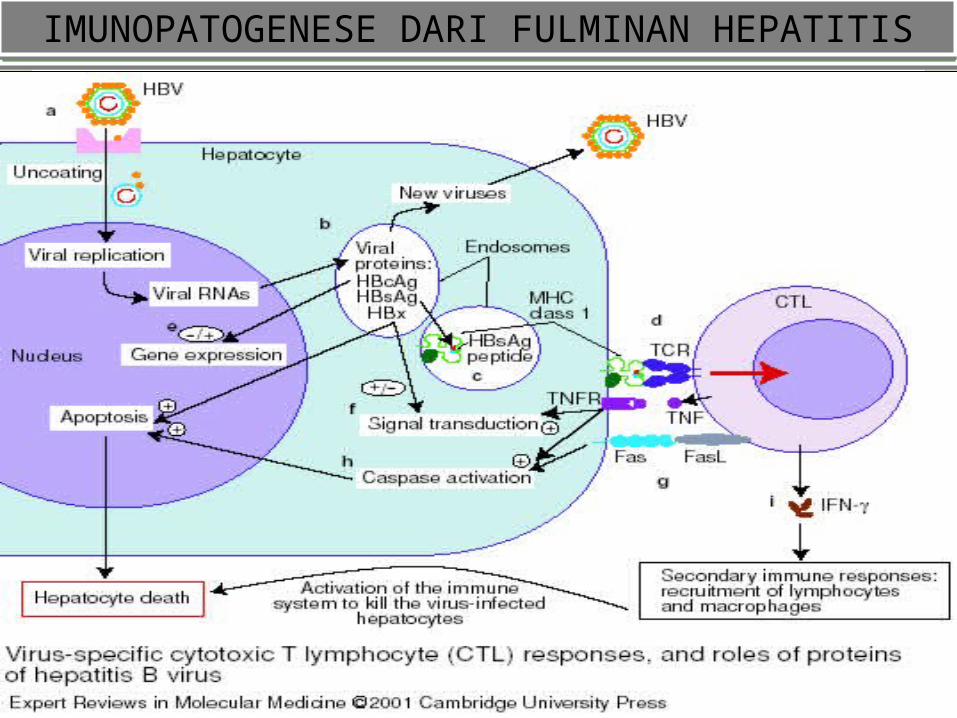
IMUNOPATOGENESE DARI FULMINAN HEPATITISIMUNOPATOGENESE DARI FULMINAN HEPATITISIMUNOPATOGENESE DARI FULMINAN HEPATITISIMUNOPATOGENESE DARI FULMINAN HEPATITIS
COMPLICATION COMPLICATION COMPLICATION COMPLICATION
The clinical syndrome of FHF is the result of hepatocellular injury and its effects on the physiology of multiple organs. Predictable effects include synthetic dysfunction (coagulation factors, albumin, glucose) and excretory failure (bilirubin, urea, drugs).
MANAGEMENTMANAGEMENTMANAGEMENTMANAGEMENTGeneral management of FHF Full hemodynamic monitoring(arterial line,pulm.artery catht) Endotracheal intubation and intracranial pressure monitoring Parenteral glucose (D10 or 20) to prevent hypoglycemia Correct electrolyte and acid-base disorders Parenteral PPIinfusion to reduce chance of GI bleeding Treat elevated intracranial pressure with mannitol Antibiotics broad-spectrum after cultures, antifungal therapy If acetaminophen poisoning is suspected, treat as follows: gastric lavage • N-acetylcysteine 140 mg/kg (An alternative
parenteral approach is to give 150 mg/kg i.v. in 200 mL D5W over 15 min, followed by 50 mg/kg in 500 mL D5W over 4 h and 100 mg/kg in 1000 mL D5W over 16 h (total 20 h therapy))
• if pills are present on lavage, give activated charcoal and parenteral N-acetylcysteine
THANK YOUTHANK YOU
Related Documents











