Drugs in pregnancy and lactation By Mariam Talal Yusor Jaffar Sherin Raad

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Drugs in pregnancy and lactation
By
Mariam Talal
Yusor Jaffar
Sherin Raad

By
Mariam Talal
Yusor Jafar
Sherin Raad

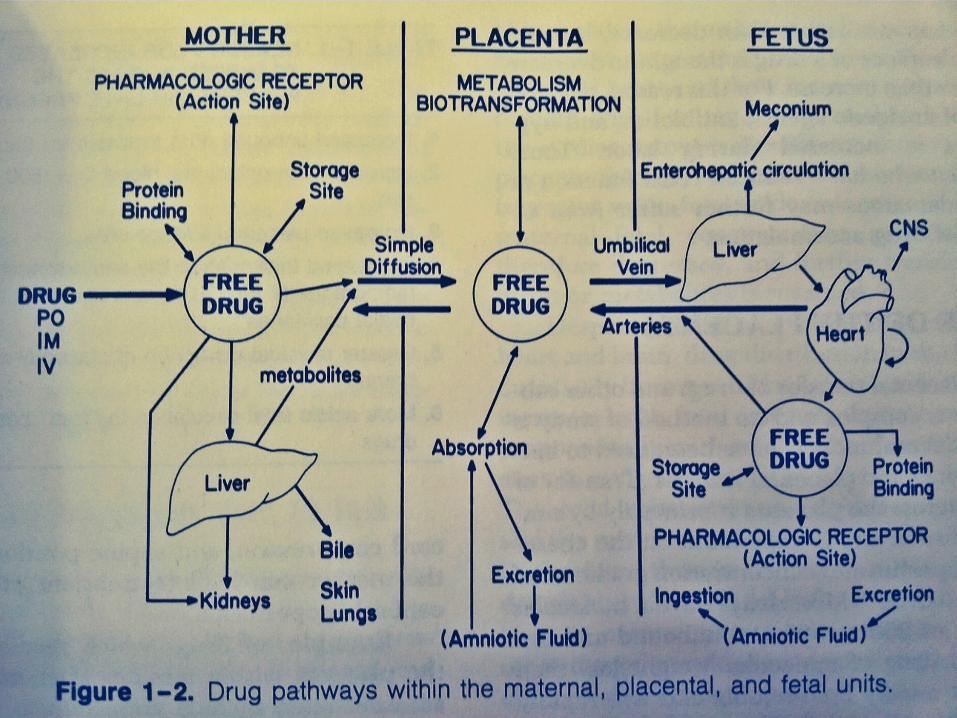
Pharmacokinetics in pregnancy• Absorption• Albumin and albumin binding capacity• Metabolism • Excretion• Most drugs are expected to have shorter
half life during late pregnancy• During labor, the drug concentration may
increase rather than decrease
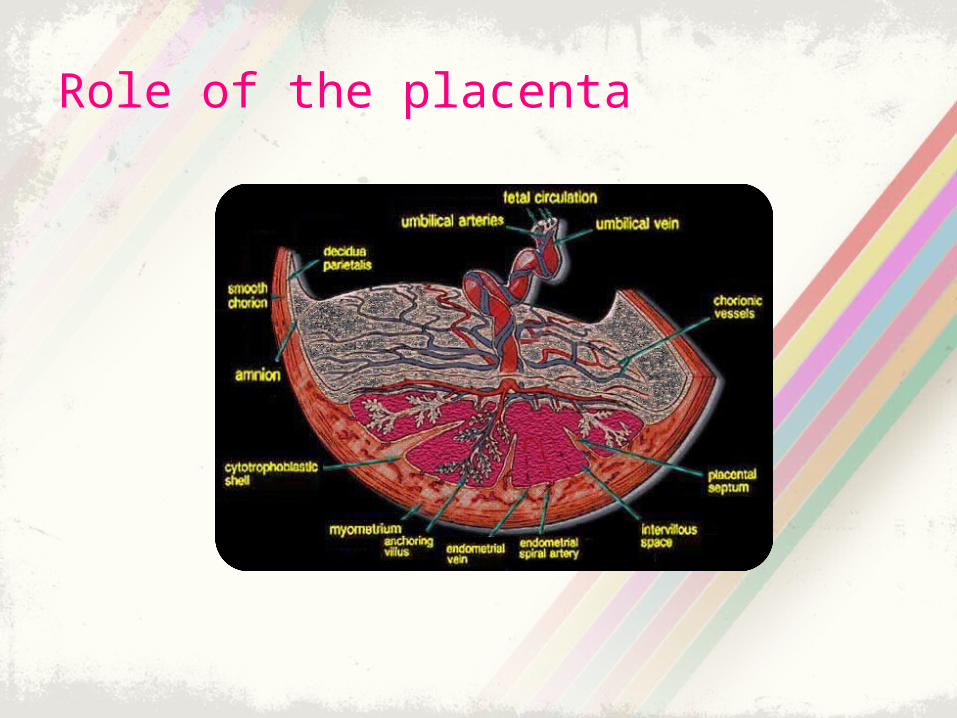
Role of the placenta
• Drug transfer is greater during late gestation because
• Pathological processes can affect uteroplacental blood flow
• Certain drugs can also induce or inhibit placental enzymes

Drug effects on the fetus• Chronic drug exposure rather than single-
dose therapy may influence fetal cell growth
• Drug may act as teratogenic agent in many ways
• Cardiac output is greater in fetus than adult
• Blood-brain permeability is greater in the fetus

• Mitochondrial number increase in in the fetal brain and heart
• Total body water and plasma protein• Autonomic receptors• Human fetal liver microsomes• Excretion of most drug is slower in fetus

Fetal drug therapy
• Specific fetal tissues may be more selective in drug uptake
• Drug administration can occur by:
I. Passive transplacental route
II. Direct intra-amniotic intramuscular injection


Drug effects on the fetusThe effect of a teratogen is depend on:
I. The dose reaching the developing embryo or fetus
II. Gestational age
III. Duration of exposure
IV. The genotype of the mother and the fetus
V. Effect of other agents
VI. Difficulty to prove a drug effect
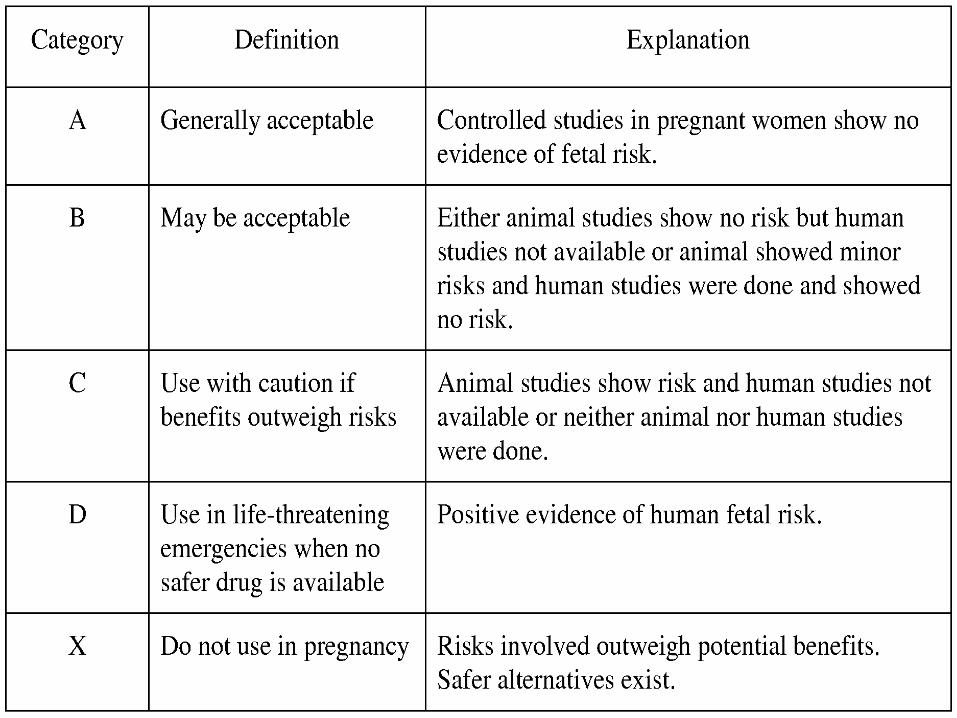


Drugs Commonly Prescribed in Pregnancy and Breast-feeding
Antianxiety drugdiazepam … FDA = D

Antibiotics

Anticoagulants

Anticonvulsants

Antihypertensives

Chemotherapy drugsFDA=D,X
Mood-stabilizing drug

Nonsteroidal anti-inflammatory drugs (NSAIDs)

Oral antihyperglycemic drugs

Sex hormones

Skin treatments

Thyroid drugs

Vaccines (live virus)

Others


Related Documents











