Drugs for Dyslipidemia Gam/IVE(CW) 1 1 Drugs for Drugs for Dyslipidemia Dyslipidemia Vivien Vivien Gam Gam, , Pharm.D Pharm.D. 2 Dyslipidemia Dyslipidemia Imbalances in lipid components Imbalances in lipid components – High total cholesterol High total cholesterol – High LDL cholesterol High LDL cholesterol – Low HDL cholesterol Low HDL cholesterol – High triglycerides High triglycerides Significant risk factor for cardiovascular diseases Significant risk factor for cardiovascular diseases Heart disease Heart disease – 1 st st leading cause of death in US* leading cause of death in US* Stroke Stroke – 3 rd rd leading cause of death in US* leading cause of death in US* * 2005 statistics, Am Heart Association * 2005 statistics, Am Heart Association

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Drugs for Dyslipidemia
Gam/IVE(CW) 1
11
Drugs for Drugs for DyslipidemiaDyslipidemiaVivien Vivien GamGam, , Pharm.DPharm.D..
22
DyslipidemiaDyslipidemia
Imbalances in lipid componentsImbalances in lipid components–– High total cholesterolHigh total cholesterol–– High LDL cholesterolHigh LDL cholesterol–– Low HDL cholesterolLow HDL cholesterol–– High triglyceridesHigh triglycerides
Significant risk factor for cardiovascular diseasesSignificant risk factor for cardiovascular diseasesHeart disease Heart disease –– 11stst leading cause of death in US*leading cause of death in US*Stroke Stroke –– 33rdrd leading cause of death in US*leading cause of death in US*
* 2005 statistics, Am Heart Association* 2005 statistics, Am Heart Association

Drugs for Dyslipidemia
Gam/IVE(CW) 2
33
DyslipidemiaDyslipidemia
Other risk factors of CV diseasesOther risk factors of CV diseases–– High blood pressureHigh blood pressure–– Tobacco useTobacco use–– DiabetesDiabetes–– Physical inactivityPhysical inactivity–– Poor nutritionPoor nutrition
44
LipidsLipids
Molecules mainly of hydrogen and carbon Molecules mainly of hydrogen and carbon atomsatomsLinked by neutral covalent bondsLinked by neutral covalent bondsNonpolarNonpolar, insoluble in water, insoluble in water4 subclasses4 subclasses
Drugs for Dyslipidemia
Gam/IVE(CW) 3
55
LipidsLipidsFatty acidsFatty acids–– Saturated, monounsaturated, polyunsaturatedSaturated, monounsaturated, polyunsaturated
TriacylglycerolsTriacylglycerols–– Also known as triglycerides (fat)Also known as triglycerides (fat)–– Majority lipids in this formMajority lipids in this form
PhospholipidsPhospholipids–– Similar to Similar to triacyglycerolstriacyglycerols except one hydroxyl group of except one hydroxyl group of
glycerol is attached to a phosphate groupglycerol is attached to a phosphate groupCholesterolCholesterol–– A steroidA steroid–– 4 interconnected rings forming the background4 interconnected rings forming the background
66
CholesterolCholesterol
Present in cell membranesPresent in cell membranesA precursor of bile acids and steroid A precursor of bile acids and steroid hormoneshormonesTravels in the blood in distinct particles Travels in the blood in distinct particles containing both lipid and proteins containing both lipid and proteins (lipoproteins)(lipoproteins)

Drugs for Dyslipidemia
Gam/IVE(CW) 4
77
Lipid transportLipid transportLipids are insoluble in waterLipids are insoluble in water–– Transported in plasma as complexes of lipid and proteins known Transported in plasma as complexes of lipid and proteins known
as lipoproteinsas lipoproteinsLipoproteinsLipoproteins–– Spherical shape with lipid coreSpherical shape with lipid core–– CenterCenter
hydrophobic lipid (triglycerides, cholesterol esters)hydrophobic lipid (triglycerides, cholesterol esters)–– SurfaceSurface
hydrophilic coat of cholesterol and hydrophilic coat of cholesterol and phospholipidphospholipidapolipoproteinsapolipoproteins embedded on the surfaceembedded on the surface
ApolipoproteinsApolipoproteins act as recognition sites for interaction of act as recognition sites for interaction of lipoproteins with tissueslipoproteins with tissues–– Several classes of Several classes of apolipoproteinsapolipoproteins–– A,B,C,D,E,H, and JA,B,C,D,E,H, and J
88
Lipoproteins classificationLipoproteins classification
3 major classes based on density3 major classes based on densityLarger particle, more lipid content, lower Larger particle, more lipid content, lower densitydensityVLDL (Very Low Density Lipoprotein) VLDL (Very Low Density Lipoprotein) LDL (Low Density Lipoprotein)LDL (Low Density Lipoprotein)HDL (High density Lipoprotein)HDL (High density Lipoprotein)IDL (intermediate density) is measured as IDL (intermediate density) is measured as LDL in clinical practiceLDL in clinical practice

Drugs for Dyslipidemia
Gam/IVE(CW) 5
99
VLDLVLDLTriglyceride rich lipoproteinsTriglyceride rich lipoproteinsContain some cholesterol, 10Contain some cholesterol, 10--15% of the total 15% of the total serum cholesterolserum cholesterolProduced by liver and precursors of LDLProduced by liver and precursors of LDLMajor Major apolipoproteinsapolipoproteins are are apoapo B 100, B 100, apoapo Cs Cs and and apoapo EEAppear to promote atherosclerosisAppear to promote atherosclerosisMajor form of transport for endogenously Major form of transport for endogenously synthesized triglyceridessynthesized triglyceridesTriglycerides degraded by lipoprotein lipase to Triglycerides degraded by lipoprotein lipase to free fatty acids for storage and oxidationfree fatty acids for storage and oxidation
1010
LDLLDLAS more triglycerides are removed from VLDL AS more triglycerides are removed from VLDL →→ cholesterol rich LDLcholesterol rich LDLMajor reservoir of cholesterol, typically makes up Major reservoir of cholesterol, typically makes up 6060--70% of the total serum cholesterol70% of the total serum cholesterolContains a single Contains a single apolipoproteinapolipoprotein ((apoapo B 100)B 100)Enhance deposition of cholesterol in arterial Enhance deposition of cholesterol in arterial wallswallsMajor Major atherogenicatherogenic lipoprotein lipoprotein -- ““badbad”” lipoproteinlipoproteinRisk of CAD is directly related to Risk of CAD is directly related to ↑↑ LDLLDLPrimary target of cholesterolPrimary target of cholesterol--lowering therapylowering therapy

Drugs for Dyslipidemia
Gam/IVE(CW) 6
1111
HDLHDL
Normally makes up 20Normally makes up 20--30% of the total serum 30% of the total serum cholesterolcholesterolMajor Major apolipoproteinsapolipoproteins are are apoapo AsAsTransport cholesterol from tissues to the liver for Transport cholesterol from tissues to the liver for secretion into the bilesecretion into the bileLevels are inversely correlated with risk for CHDLevels are inversely correlated with risk for CHDA low HDL level often reflects the presence of A low HDL level often reflects the presence of other other atherogenicatherogenic factorsfactors““goodgood”” cholesterolcholesterol
1212
ChylomicronsChylomicrons
Formed in the intestine form dietary fatFormed in the intestine form dietary fatAppear in the blood after a fat containing Appear in the blood after a fat containing mealmealTriglycerideTriglyceride--rich lipoproteinsrich lipoproteins

Drugs for Dyslipidemia
Gam/IVE(CW) 7
1313
LDL receptorsLDL receptors
Located in a wide range of tissues, react Located in a wide range of tissues, react with circulating LDLwith circulating LDLLiver contains the greatest number of LDL Liver contains the greatest number of LDL receptorsreceptorsLDL entering cells by receptor mediated LDL entering cells by receptor mediated endocytosisendocytosisCholesterol utilized for synthesis of plasma Cholesterol utilized for synthesis of plasma membranes, bile acids, steroid hormonesmembranes, bile acids, steroid hormones
1414
LDL receptorsLDL receptors
Reduced number of LDL receptors can Reduced number of LDL receptors can elevate plasma LDLelevate plasma LDLLDL receptors suppress cholesterol LDL receptors suppress cholesterol synthesis in the liversynthesis in the liver∴∴ LDL receptor controlsLDL receptor controls–– Uptake of cholesterolUptake of cholesterol–– Synthesis of cholesterolSynthesis of cholesterol↑↑ risk of atherosclerosis associated with a risk of atherosclerosis associated with a deficit of LDL receptorsdeficit of LDL receptors
Drugs for Dyslipidemia
Gam/IVE(CW) 8
1515
PathophysiologyPathophysiology
The deposition and retention of cholesterol The deposition and retention of cholesterol in the arterial walls are the central features in the arterial walls are the central features of the pathogenesis in atherosclerosisof the pathogenesis in atherosclerosisRisk factorsRisk factors–– Oxidized LDLOxidized LDL–– GlycosylatedGlycosylated proteinsproteins–– High levels of High levels of homocysteinehomocysteine–– Changes in the endothelium (mechanical, Changes in the endothelium (mechanical,
immunological, infectionimmunological, infection--induced)induced)
1616
PathophysiologyPathophysiology
LDL is modified (mildly oxidized) in the LDL is modified (mildly oxidized) in the subendothelialsubendothelial layer layer LDL modification is enhanced inLDL modification is enhanced in–– DiabetesDiabetes–– Cigarette smokingCigarette smoking–– HypertriglyceridemicHypertriglyceridemic low HDLlow HDL

Drugs for Dyslipidemia
Gam/IVE(CW) 9
1717
PathophysiologyPathophysiology
Mildly oxidized LDL attracts Mildly oxidized LDL attracts monocytesmonocytesinto the artery wallinto the artery wallMonocytesMonocytes transform into macrophages transform into macrophages that accelerate LDL oxidationthat accelerate LDL oxidationOxidized LDL provokes an inflammatory Oxidized LDL provokes an inflammatory response (response (proinflammatoryproinflammatory cytokines, T cytokines, T lympohcyteslympohcytes and growth factors)and growth factors)
1818
PathophysiologyPathophysiology
Macrophages soak up lipids and become Macrophages soak up lipids and become foam cells causing more injury and lumen foam cells causing more injury and lumen more restrictedmore restrictedRepeated injury and repair within an Repeated injury and repair within an atherosclerotic plaque leads to formation atherosclerotic plaque leads to formation of a fibrous capof a fibrous capMaintenance of the fibrous plaque is Maintenance of the fibrous plaque is critical to prevent plaque rupture and critical to prevent plaque rupture and subsequent coronary thrombosissubsequent coronary thrombosis

Drugs for Dyslipidemia
Gam/IVE(CW) 10
1919
PathophysiologyPathophysiology
Early stageEarly stage–– coronary remodeling (outgrowth of vessel wall) coronary remodeling (outgrowth of vessel wall)
to preserve coronary lumento preserve coronary lumenAdvanced stageAdvanced stage–– plaque ruptureplaque rupture
2020
Detection and EvaluationDetection and Evaluation
NCEP ATP III guidelines, 2001, NIHNCEP ATP III guidelines, 2001, NIH(National Cholesterol Education Program Adult Treatment Panel)(National Cholesterol Education Program Adult Treatment Panel)
Fasting lipoprotein profile (total cholesterol, Fasting lipoprotein profile (total cholesterol, LDL cholesterol, HDL cholesterol, LDL cholesterol, HDL cholesterol, triglycerides) and risk factor assessment at triglycerides) and risk factor assessment at least once q5yr in adults age least once q5yr in adults age ≥≥ 2020

Drugs for Dyslipidemia
Gam/IVE(CW) 11
2121
Detection and EvaluationDetection and Evaluation
Patients are categorized into different risk Patients are categorized into different risk groups based on the overall risk of a CHD groups based on the overall risk of a CHD event over 10 yearsevent over 10 yearsThe intensity of LDLThe intensity of LDL--lowering therapy is lowering therapy is adjusted to the individualadjusted to the individual’’s degree of risk s degree of risk for CHDfor CHD
2222
NonNon--pharmacological Therapy pharmacological Therapy Therapeutic Lifestyle Changes (Therapeutic Lifestyle Changes (TLCsTLCs))
Dietary therapyDietary therapy–– Low consumption of saturated fat and cholesterol Low consumption of saturated fat and cholesterol –– Use monounsaturated (olive oil) or polyunsaturated Use monounsaturated (olive oil) or polyunsaturated
fat (canola oil, fish oils rich in omegafat (canola oil, fish oils rich in omega--3 fatty acids) 3 fatty acids) –– Avoid transAvoid trans--fatty acids (partially hydrogenated fats fatty acids (partially hydrogenated fats
such as margarine)such as margarine)–– Increase fiber, complex carbohydrates (whole grains Increase fiber, complex carbohydrates (whole grains
and beans, brown rice, whole wheat bread and cereal, and beans, brown rice, whole wheat bread and cereal, fruit and vegetable)fruit and vegetable)
–– If diet alone is inadequate, dietary supplements of If diet alone is inadequate, dietary supplements of soluble fiber and plant sterols/soluble fiber and plant sterols/stanolsstanols ((↓↓ LDLLDL--C)C)fish oil (fish oil (↓↓ triglycerides, but not LDLtriglycerides, but not LDL--C)C)

Drugs for Dyslipidemia
Gam/IVE(CW) 12
2323
NonNon--pharmacological Therapy pharmacological Therapy Therapeutic Lifestyle Changes (Therapeutic Lifestyle Changes (TLCsTLCs))
Physical activity Physical activity –– Aerobic exercise 30 min/day for most days of Aerobic exercise 30 min/day for most days of
the weekthe weekWeight reduction if overweightWeight reduction if overweightStop smoking Stop smoking
2424
Drug therapyDrug therapy
HMGHMG--CoACoA reductasereductase inhibitors (inhibitors (StatinsStatins) ) FibratesFibratesBile acid binding resinsBile acid binding resinsNicotinic acidNicotinic acidEzetimibeEzetimibeOmegaOmega--3 fatty acids3 fatty acids
Drugs for Dyslipidemia
Gam/IVE(CW) 13
2525
HMGHMG--CoACoA reductasereductase inhibitorsinhibitors
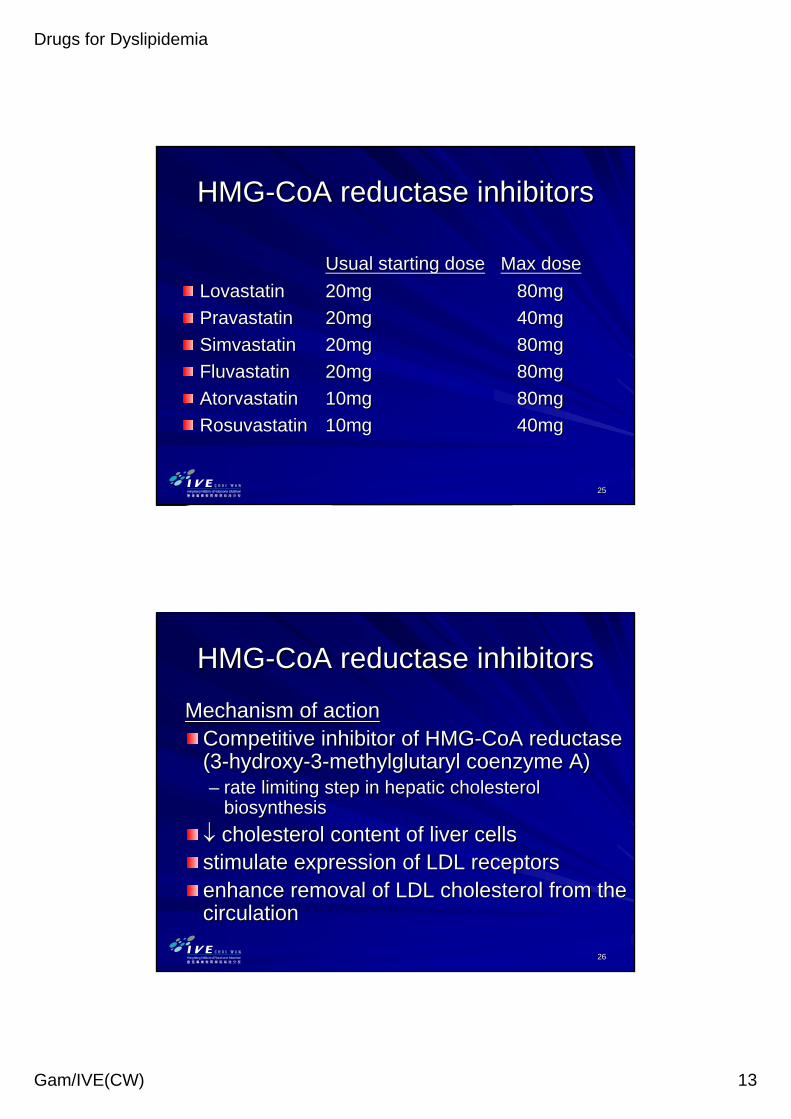
Usual starting doseUsual starting dose Max doseMax doseLovastatinLovastatin 20mg20mg 80mg80mgPravastatinPravastatin 20mg20mg 40mg40mgSimvastatinSimvastatin 20mg20mg 80mg80mgFluvastatinFluvastatin 20mg20mg 80mg80mgAtorvastatinAtorvastatin 10mg10mg 80mg80mgRosuvastatinRosuvastatin 10mg10mg 40mg40mg
2626
HMGHMG--CoACoA reductasereductase inhibitorsinhibitors
Mechanism of actionMechanism of actionCompetitive inhibitor of HMGCompetitive inhibitor of HMG--CoACoA reductasereductase(3(3--hydroxyhydroxy--33--methylglutaryl coenzyme A)methylglutaryl coenzyme A)–– rate limiting step in hepatic cholesterol rate limiting step in hepatic cholesterol
biosynthesisbiosynthesis↓↓ cholesterol content of liver cellscholesterol content of liver cellsstimulate expression of LDL receptorsstimulate expression of LDL receptorsenhance removal of LDL cholesterol from the enhance removal of LDL cholesterol from the circulationcirculation

Drugs for Dyslipidemia
Gam/IVE(CW) 14
2727
HMGHMG--CoACoA reductasereductase inhibitorsinhibitors
Very effective for lowering LDLVery effective for lowering LDL--C levelsC levelsModest effective in reducing triglyceride Modest effective in reducing triglyceride and increasing HDLand increasing HDL--C levelsC levelsGreater LDLGreater LDL--C lowering effects at their C lowering effects at their highest doses compared with other highest doses compared with other statinsstatins–– simvastatinsimvastatin, , atorvastatinatorvastatin, , rosuvastatinrosuvastatinConsidered as 1Considered as 1stst--line choice for reducing line choice for reducing LDLLDL--CCGenerally safe therapyGenerally safe therapy
2828
HMGHMG--CoACoA reductasereductase inhibitorsinhibitors
Use as Use as monotherapymonotherapy or combination or combination therapytherapyCombination therapyCombination therapy–– bile acid resinbile acid resin–– ezetimibeezetimibe

Drugs for Dyslipidemia
Gam/IVE(CW) 15
2929
HMGHMG--CoACoA reductasereductase inhibitorsinhibitorsAdministrationAdministration
Once dailyOnce dailyTake with evening meal or with food at Take with evening meal or with food at bedtimebedtime–– Cholesterol biosynthesis highest at nighttimeCholesterol biosynthesis highest at nighttimeAtorvastatinAtorvastatin can be taken anytime during can be taken anytime during the day (long halfthe day (long half--life), morning life), morning administration is equally effectiveadministration is equally effectiveMost Most statinsstatins have a short half lifehave a short half life
3030
HMGHMG--CoACoA reductasereductase inhibitorsinhibitorsSide/ Adverse effectsSide/ Adverse effects
GI disturbance, constipationGI disturbance, constipationIncrease liver Increase liver transaminasestransaminases–– Occurrence ~ 0.5 Occurrence ~ 0.5 –– 2%2%–– True True hepatotoxicityhepatotoxicity ????–– DoseDose--dependentdependent–– Usually return to normal upon DC of drug, dose Usually return to normal upon DC of drug, dose
reduction, or even with continued dosereduction, or even with continued dose–– Baseline + evaluate liver function periodicallyBaseline + evaluate liver function periodically–– If If ↑↑, m, monitor with 2onitor with 2ndnd liver function evaluationliver function evaluation–– Risk of Risk of hepatoxicityhepatoxicity increase when coincrease when co--administered administered
with niacin with niacin

Drugs for Dyslipidemia
Gam/IVE(CW) 16
3131
HMGHMG--CoACoA reductasereductase inhibitorsinhibitorsSide/ Adverse effectsSide/ Adverse effects
MyopathyMyopathy (1(1--5%)5%)–– ↑↑ creatinecreatine kinasekinase–– Muscle ache, soreness, weaknessMuscle ache, soreness, weakness–– Failure to recognize Failure to recognize myopathymyopathy and DC drug can lead and DC drug can lead
to to rhabdomyolysisrhabdomyolysisRhabdomyolysisRhabdomyolysis–– Rare but severeRare but severe–– Breakdown of skeletal muscleBreakdown of skeletal muscle–– Accumulation of the muscle breakdown products Accumulation of the muscle breakdown products
leading to leading to myoglobinuriamyoglobinuria (urine dark color) and renal (urine dark color) and renal failurefailure
3232
HMGHMG--CoACoA reductasereductase inhibitorsinhibitorsSide/ Adverse effectsSide/ Adverse effects
MyopathyMyopathy more likely to occur:more likely to occur:--–– Older patientsOlder patients–– Patients with complex medical problems on multiple Patients with complex medical problems on multiple
medicationsmedications–– ↑↑ risk risk when concomitantly used with potent inhibitors when concomitantly used with potent inhibitors
of CYP3A4of CYP3A4–– cyclosporine, cyclosporine, macrolidemacrolide antibiotics, certain antiantibiotics, certain anti--fungal fungal
drugs (drugs (ketoconazoleketoconazole, , itraconazoleitraconazole), HIV protease ), HIV protease inhibitors, inhibitors, amiodaroneamiodarone, , verapamilverapamil, , fibratesfibrates, niacin, , niacin, grapefruit juicegrapefruit juice

Drugs for Dyslipidemia
Gam/IVE(CW) 17
3333
HMGHMG--CoACoA reductasereductase inhibitorsinhibitors
Incidence of Incidence of myopathymyopathy and and rhabdomyolysisrhabdomyolysis with with statinsstatins is lowis lowUp to 1/3 of prescriptions of Up to 1/3 of prescriptions of statinsstatins were in were in combination with drugs that potentially can combination with drugs that potentially can interact, side effects occurred in 3% of interact, side effects occurred in 3% of these patients*these patients*
*Safety of *Safety of statinsstatins. Circulation, Jun 15, 2004. Circulation, Jun 15, 2004
3434
HMGHMG--CoACoA reductasereductase inhibitorsinhibitors
MyopathyMyopathy–– Immediately report muscle pain, weakness, or Immediately report muscle pain, weakness, or
brown urinebrown urine–– CreatineCreatine kinasekinase measurementmeasurement–– Routine laboratory monitoring of Routine laboratory monitoring of creatinecreatine
kinasekinase is of little value in the absence of is of little value in the absence of clinical signs or symptomsclinical signs or symptoms
Drugs for Dyslipidemia
Gam/IVE(CW) 18
3535
HMGHMG--CoACoA reductasereductase inhibitorsinhibitors
FluvastatinFluvastatin and and PravastatinPravastatin not not metabolized by P450 3A4 systemmetabolized by P450 3A4 system–– Less likely to have drugLess likely to have drug--drug interactions at drug interactions at
the level of the liver the level of the liver
3636
HMGHMG--CoACoA reductasereductase inhibitorsinhibitors
Absolute contraindicationsAbsolute contraindications–– Active or chronic liver diseaseActive or chronic liver diseaseRelative contraindicationsRelative contraindications–– Concomitant use ofConcomitant use of–– CyclosporineCyclosporine–– MacrolideMacrolide antibioticsantibiotics–– Various antiVarious anti--fungal drugsfungal drugs–– CytochromeCytochrome P450 inhibitors P450 inhibitors –– FibratesFibrates and niacin (use with caution)and niacin (use with caution)

Drugs for Dyslipidemia
Gam/IVE(CW) 19
3737
FibratesFibratesGemfibrozilGemfibrozil–– 600mg bid600mg bid–– Max 1500 mgMax 1500 mg–– 900mg ER as a single evening dose900mg ER as a single evening dose
FenofibrateFenofibrate–– 100mg 100mg tdstds–– Max 400mg dailyMax 400mg daily–– MicronizedMicronized: 200mg once daily: 200mg once daily–– ER: 250ER: 250--300 mg once daily300 mg once daily–– Supra form: 160mg once dailySupra form: 160mg once daily
ClofibrateClofibrate–– 2 g daily in divided doses2 g daily in divided doses
3838
FibratesFibrates
Most effective in lowering triglyceride Most effective in lowering triglyceride levelslevelsEffective for increase HDLEffective for increase HDL--CCModerate for reducing LDLModerate for reducing LDL--CC

Drugs for Dyslipidemia
Gam/IVE(CW) 20
3939
FibratesFibrates
MechanismMechanism–– ComplexComplex–– Agonist for the nuclear receptors Agonist for the nuclear receptors --peroxisomeperoxisome
proliferatorproliferator--activated receptorsactivated receptors--alpha (PPARalpha (PPAR--αα))
Stimulate lipoprotein lipase activityStimulate lipoprotein lipase activity↑↑ hhydrolysis of ydrolysis of triacylglycerolstriacylglycerols in VLDLin VLDLHasten removal of VLDL from plasmaHasten removal of VLDL from plasmaReduce TGReduce TG--rich lipoproteins from plasmarich lipoproteins from plasma
4040
FibratesFibrates
Adverse effectsAdverse effects–– GI disturbances (most common)GI disturbances (most common)–– Increase risk for Increase risk for hepatotoxicityhepatotoxicity and skeletal and skeletal
muscle toxicity of muscle toxicity of statinsstatins–– FenofibrateFenofibrate appears to have a lower risk of appears to have a lower risk of
interfering with interfering with statinstatin metabolism (preferred metabolism (preferred fibratefibrate for combination therapy)for combination therapy)
–– Increase risk of gallstones (Increase risk of gallstones (clofibrateclofibrate))

Drugs for Dyslipidemia
Gam/IVE(CW) 21
4141
Bile acid binding resinsBile acid binding resinsColestyramineColestyramine–– 44--24g 24g pwdpwd/day (/day (tdstds--qdsqds))ColestipolColestipol–– 55--30g 30g pwdpwd /day (once or in divided doses)/day (once or in divided doses)–– 22--16 g tab /day (once or in divided doses)16 g tab /day (once or in divided doses)ColesevelamColesevelam–– 3.75 g/day (once or in 2 divided doses)3.75 g/day (once or in 2 divided doses)–– 2.52.5--3.75 g/day when used with a 3.75 g/day when used with a statinstatin–– minimal GI effectsminimal GI effects
4242
Bile acid binding resinsBile acid binding resins
↓↓↓↓ LDLLDL--C (a modest reduction)C (a modest reduction)Mild increase of HDLMild increase of HDLIncrease hepatic VLDL production, Increase hepatic VLDL production, ∴∴ can can raise serum triglyceride level in some raise serum triglyceride level in some personspersons

Drugs for Dyslipidemia
Gam/IVE(CW) 22
4343
Bile acid binding resinsBile acid binding resins
MechanismMechanism–– Anion exchange resin that bind bile acids in the Anion exchange resin that bind bile acids in the
intestinal lumen in exchange for chloride ionintestinal lumen in exchange for chloride ion–– Resin is not absorbedResin is not absorbed–– Promotes fecal excretion of bile acidsPromotes fecal excretion of bile acids–– ↓↓ enterohepaticenterohepatic recirculation of bile acidsrecirculation of bile acids–– Liver increase bile acid synthesis from cholesterolLiver increase bile acid synthesis from cholesterol–– Enhance LDL receptor expressionEnhance LDL receptor expression–– ↓↓ LDLLDL--CC
4444
Bile acid binding resinsBile acid binding resins
PharmacokineticsPharmacokineticsInsoluble in water, large molecular weightInsoluble in water, large molecular weightNeither absorbed nor metabolized in Neither absorbed nor metabolized in intestineintestineExcreted in fecesExcreted in feces

Drugs for Dyslipidemia
Gam/IVE(CW) 23
4545
Bile acid binding resinsBile acid binding resins
AdministrationAdministrationOnce or twice daily with mealsOnce or twice daily with mealsIf once daily, take with largest meal of the If once daily, take with largest meal of the daydayMix with water or juice, hydrate for a few Mix with water or juice, hydrate for a few min to minimize the gritty texturemin to minimize the gritty texture
4646
Bile acid binding resinsBile acid binding resins
Useful in combination therapyUseful in combination therapyDoubling the dose of a Doubling the dose of a statinstatin produces a 6% produces a 6% further reduction in LDLfurther reduction in LDL--C, adding a moderate C, adding a moderate dose of a bile acid binding resin further lower dose of a bile acid binding resin further lower LDLLDL--C by 12C by 12--16%16%Contraindicated as Contraindicated as monotherapymonotherapy in persons with in persons with high triglycerides (high triglycerides (>>400 mg/400 mg/dLdL))MonotherapyMonotherapy only in patients with triglyceride only in patients with triglyceride <<200mg/dL200mg/dL

Drugs for Dyslipidemia
Gam/IVE(CW) 24
4747
Bile acid binding resinsBile acid binding resins
Adverse effectsAdverse effects–– Bothersome GI side effectsBothersome GI side effects–– Constipation, abdominal pain, bloating, Constipation, abdominal pain, bloating,
fullness, nausea and flatulencefullness, nausea and flatulence–– Interfere with absorption of fat soluble Interfere with absorption of fat soluble
vitamins and some drugsvitamins and some drugs–– Take drugs 1 hour before or 4 hours after Take drugs 1 hour before or 4 hours after
administration of resinadministration of resin
4848
Nicotinic acid (Niacin)Nicotinic acid (Niacin)
Extended release nicotinic acidExtended release nicotinic acid–– 11--2 g once daily 2 g once daily
Effective on all major lipid fractions Effective on all major lipid fractions ↑↑ HDLHDL--CC↓↓↓↓ triglyceridestriglycerides↓↓ LDLLDL--CC

Drugs for Dyslipidemia
Gam/IVE(CW) 25
4949
Nicotinic acid (Niacin)Nicotinic acid (Niacin)
MechanismMechanism–– Inhibit Inhibit lipolysislipolysis in adipose tissue (primary in adipose tissue (primary
producer of circulating FFA)producer of circulating FFA)–– Liver uses the circulating FFA to synthesize Liver uses the circulating FFA to synthesize
triglyceridestriglycerides↓↓ liver triglyceride synthesisliver triglyceride synthesis↓↓ VLDL productionVLDL production↓↓ LDLLDL
5050
Nicotinic acid (Niacin)Nicotinic acid (Niacin)
Side/ Adverse effectsSide/ Adverse effects–– Intense Intense cutaneouscutaneous flushing flushing
Take ASA or ibuprofen 30 minutes prior to niacin, or take on Take ASA or ibuprofen 30 minutes prior to niacin, or take on full stomach can reduce severity of flushing)full stomach can reduce severity of flushing)Tolerance after prolonged useTolerance after prolonged useLess with prolonged release dosage formLess with prolonged release dosage form
–– GI disturbancesGI disturbances–– liver dysfunctionliver dysfunction–– decreased glucose tolerancedecreased glucose tolerance–– hyperuricemiahyperuricemia

Drugs for Dyslipidemia
Gam/IVE(CW) 26
5151
Nicotinic acid (Niacin)Nicotinic acid (Niacin)
AdministrationAdministration–– ER dosage form ER dosage form –– single dose at single dose at hshs–– ER form ER form –– reduced incidence of flushing and reduced incidence of flushing and
hepatotoxicityhepatotoxicity–– Can be used as combination therapyCan be used as combination therapy
5252
Nicotinic acid (Niacin)Nicotinic acid (Niacin)
ContraindicationsContraindications–– Chronic liver diseaseChronic liver disease–– Severe goutSevere goutRelative contraindicationsRelative contraindications–– HyperuricemiaHyperuricemia–– High doses in Type 2 diabetesHigh doses in Type 2 diabetes
Drugs for Dyslipidemia
Gam/IVE(CW) 27
5353
EzetimibeEzetimibe
Selective inhibitor of intestinal cholesterol Selective inhibitor of intestinal cholesterol absorptionabsorption–– Block the transfer of dietary and Block the transfer of dietary and biliarybiliary
cholesterol from intestinal micelles to brush cholesterol from intestinal micelles to brush border membrane border membrane enterocytesenterocytes
↓↓↓↓ LDLLDL--CC↓↓ total cholesterol, total cholesterol, ↑↑HDLHDL--C and C and ↓↓TG TG levelslevels
5454
EzetimibeEzetimibe
10 mg daily10 mg dailyMajor role in combination with a Major role in combination with a statinstatinVytorinVytorin = = ezetimibeezetimibe + + simvastatinsimvastatin–– 10/10mg; 10/20mg; 10/40mg; 10/80mg10/10mg; 10/20mg; 10/40mg; 10/80mg–– Inhibits absorption of cholesterol in small Inhibits absorption of cholesterol in small
intestineintestine–– Reduce cholesterol synthesis in liverReduce cholesterol synthesis in liver

Drugs for Dyslipidemia
Gam/IVE(CW) 28
5555
Fish Oil SupplementationFish Oil SupplementationNCEP ATP III guidelinesNCEP ATP III guidelines
–– OmegaOmega--3 fatty acids should be considered as an 3 fatty acids should be considered as an adjunct to therapy in patients with very high TG adjunct to therapy in patients with very high TG levelslevels
Complications of fish oil supplementation Complications of fish oil supplementation includeinclude
–– ThrombocytopeniaThrombocytopenia–– Bleeding disordersBleeding disordersDiets high in omegaDiets high in omega--3 3 PUFAsPUFAs (EPA) reduce (EPA) reduce cholesterol, triglycerides, LDL and VLDL, may cholesterol, triglycerides, LDL and VLDL, may elevate HDLelevate HDL--CC
5656
α-Linolenic Acid 18:3n-3 (green leafy veg, flaxseed
oil, canola oil, nuts)
EPA 20:5n-3 (fish oils)
DHA 22:6n-3 (fish oils)
Production pathway of ω-3 series of FA’s
The Omega-3 series
DDesaturaseesaturase
EElongaselongase
Omega-3-derived eicosanoids
3-series prostanoidsTXA3, PGE3, PGI3
5-series leukotrienesLTB5, C5, E5
Anti-inflammatory
Antithrombotic

Drugs for Dyslipidemia
Gam/IVE(CW) 29
5757
Combination TherapyCombination TherapyConsider combination therapy after adequate Consider combination therapy after adequate trials of trials of monotherapymonotherapyStatinsStatins may combine with bile acid resin, niacin, may combine with bile acid resin, niacin, fibratefibrate and omegaand omega--3 fatty acid3 fatty acidInclude Include gemfibrozilgemfibrozil or niacin to or niacin to ↑↑ HDLHDL--CCAddition of Addition of ezetimibeezetimibe to a to a statinstatin provides an provides an additional 14% to 17% reduction in LDLadditional 14% to 17% reduction in LDL--CCMonitor carefully for evidence of side effects Monitor carefully for evidence of side effects especially muscle related symptoms and especially muscle related symptoms and hepatotoxicityhepatotoxicity
Related Documents











