G ~-N AC* O & !~ /K/I_J A. ~' 1938 o p Journal of the American Academy of DERMATOLOGY VOLUME 35 NUMBER 6 DECEMBER 1996 CONTINUING MEDICAL EDUCATION Drug photosensitivity, and sunscreens idiopathic photodermatoses, Emesto Gonzgdez, MD, and Salvador Gonzgdez, MD, PhD Boston, Massachusetts Photosensitization may be defined as a process in which a reaction to normally innocuous radiation is induced by the introduction of a specific radiation-absorbing substance (the pho- tosensitizer) that causes another component (the substrate) to be changed by the radiation. This review focuses on photosensitization produced by exogenous chemicals. Idiopathic photo- dermatoses, including polymorphous light eruption and its variants, solar urticaria and chronic actinic dermatitis, are also discussed. Clinical recognition patterns of the photodermatoses are stressed as well as several diagnostic procedures available for confitanation of the condition. Finally, descriptions, therapeutic uses, mad adverse reactions of stmscreens are provided. (J Am Acad Dermatol 1996;35:871-85.) Learning objective: At the conclusion of this learning activity, participants should have an overview of the exogenous chemicals, both topical and systemic, that produce photosensi- tization as well as a more complete knowledge of idiopathic photodermatoses and sunscreens. An understanding of the photodermatoses should enable the clinician to choose appropriate procedures to aid in diagnosis. Photosensitization may be defined as a process in which a reaction to normally innocuous radiation is induced by the introduction of a specific radiation- absorbing substance (the photosensitizer) that causes another component (the substrate) to be changed by radiation.1 We confine our discussion to photosen- sitization produced by exogenous chemicals, either to chemicals applied directly on the skin (topical photosensitizers) or to those reaching the skin via the general circulation (systemic photosensitizers). The second section deals with idiopathic photoderma- toses including polymorphous light eruption and its variants, solar urticaria and chronic actinic dermati- tis. For each of the photodermatoses clinical recog- ORTHO The CME articles are made possible through an educational grant from the Dermatological Division, Ortho Pharma- ceutical Corporation. From the Department of Dermatology, Massachusetts General Hospi- tal, and Harvard Medical School. Reprint requests: Ernesto Gonzglez, MD, Department of Dermatology, Massachusetts General Hospital, Boston, MA 02114. Copyright © 1996 by the American Academy of Dermatology, Inc. 0190-9622/96 $5.00 + 0 16/2/77078 ninon patterns will be stressed, including some diagnostic procedures available for confirmation. A third section reviews sunscreens, their use in the treatment of idiopathic photodermatoses and drag- induced photosensitivity as well as their adverse re- actions, including paradoxical phototoxic and pho- toallergic reactions. DRUG PHOTOSENSITIVITY The incidence of drug photosensitivity is 16% to 25% for chlorpromazine,2' 3 25% for demethylchlor- tetracycline, 4 and 0.025% to 15% for fluoroquino- lones. 5 These variations probably reflect the interac- tive relation between the three elements essential for a photochemical reaction: the person (substrate), the chemical (drug), and the radiant energy. Radiant energy Although the electromagnetic spectrum emitted by sunlight extends from ionizing radiation to radio waves, the portion producing photosensitization is limited to UV radiation and visible light. This form of energy is absorbed by molecules in the skin 871

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

G ~-N AC*
O & ! ~ / K / I _ J A.
~' 1938 o
p
Journal of the American Academy of
DERMATOLOGY VOLUME 35 NUMBER 6 DECEMBER 1996
CONTINUING MEDICAL EDUCATION
Drug photosensitivity, and sunscreens
idiopathic photodermatoses,
Emesto Gonzgdez, MD, and Salvador Gonzgdez, MD, PhD Boston, Massachusetts
Photosensitization may be defined as a process in which a reaction to normally innocuous radiation is induced by the introduction of a specific radiation-absorbing substance (the pho- tosensitizer) that causes another component (the substrate) to be changed by the radiation. This review focuses on photosensitization produced by exogenous chemicals. Idiopathic photo- dermatoses, including polymorphous light eruption and its variants, solar urticaria and chronic actinic dermatitis, are also discussed. Clinical recognition patterns of the photodermatoses are stressed as well as several diagnostic procedures available for confitanation of the condition. Finally, descriptions, therapeutic uses, mad adverse reactions of stmscreens are provided. (J Am Acad Dermatol 1996;35:871-85.)
Learning objective: At the conclusion of this learning activity, participants should have an overview of the exogenous chemicals, both topical and systemic, that produce photosensi- tization as well as a more complete knowledge of idiopathic photodermatoses and sunscreens. An understanding of the photodermatoses should enable the clinician to choose appropriate procedures to aid in diagnosis.
Photosensitization may be defined as a process in which a reaction to normally innocuous radiation is induced by the introduction of a specific radiation- absorbing substance (the photosensitizer) that causes another component (the substrate) to be changed by radiation.1 We confine our discussion to photosen- sitization produced by exogenous chemicals, either to chemicals applied directly on the skin (topical photosensitizers) or to those reaching the skin via the general circulation (systemic photosensitizers). The second section deals with idiopathic photoderma- toses including polymorphous light eruption and its variants, solar urticaria and chronic actinic dermati- tis. For each of the photodermatoses clinical recog-
ORTHO The CME articles are made possible through an educational grant from the Dermatological Division, Ortho Pharma- ceutical Corporation.
From the Department of Dermatology, Massachusetts General Hospi- tal, and Harvard Medical School.
Reprint requests: Ernesto Gonzglez, MD, Department of Dermatology, Massachusetts General Hospital, Boston, MA 02114.
Copyright © 1996 by the American Academy of Dermatology, Inc.
0190-9622/96 $5.00 + 0 16/2/77078
ninon patterns will be stressed, including some diagnostic procedures available for confirmation. A third section reviews sunscreens, their use in the treatment of idiopathic photodermatoses and drag- induced photosensitivity as well as their adverse re- actions, including paradoxical phototoxic and pho- toallergic reactions.
DRUG PHOTOSENSITIVITY
The incidence of drug photosensitivity is 16% to 25% for chlorpromazine, 2' 3 25% for demethylchlor- tetracycline, 4 and 0.025% to 15% for fluoroquino- lones. 5 These variations probably reflect the interac- tive relation between the three elements essential for a photochemical reaction: the person (substrate), the chemical (drug), and the radiant energy.
Radiant energy
Although the electromagnetic spectrum emitted by sunlight extends from ionizing radiation to radio waves, the portion producing photosensitization is limited to UV radiation and visible light. This form of energy is absorbed by molecules in the skin
871
872 Gonzdlez and Gonzdlez Journal of the American Academy of Dermatology
December 1996
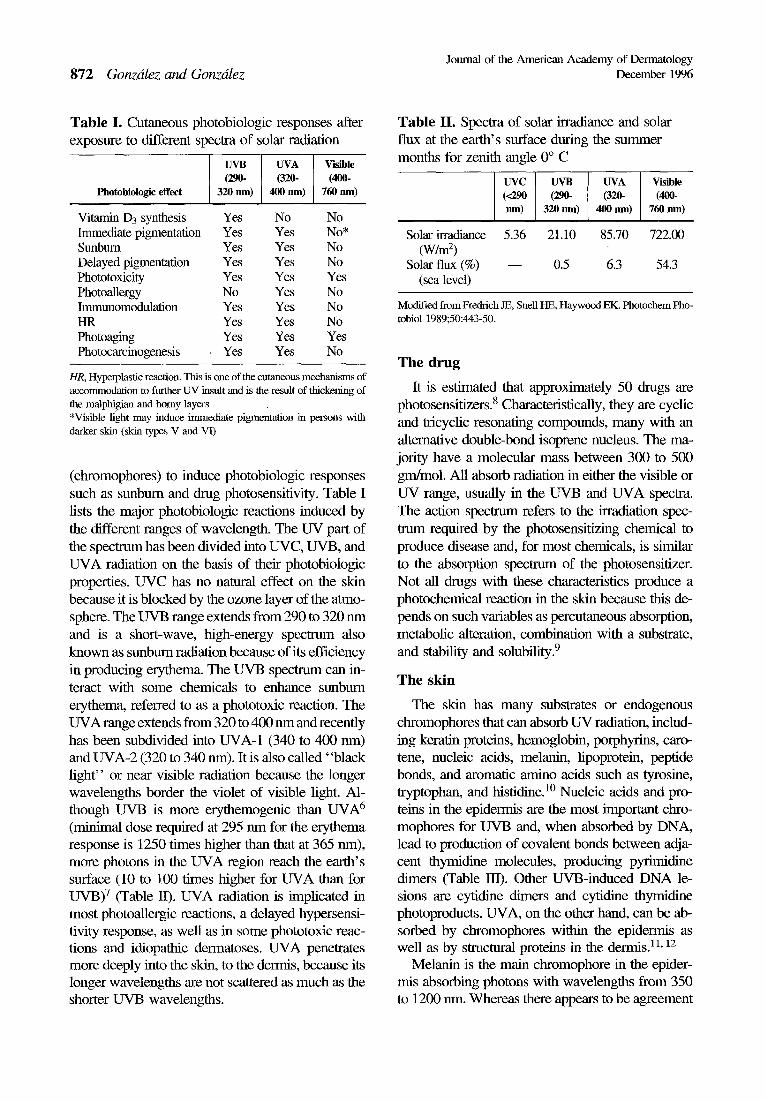
Table I. Cutaneous photobiologic responses after exposure to different spectra of solar radiation
UVB UVA Visible (290- (320- (400-
Photobiologie effect 320 nm) 400 nm) 760 rim)
Vitamin D3 synthesis Yes No No Immediate pigmentation Yes Yes No* Sunburn Yes Yes No Delayed pigmentation Yes Yes No Phototoxicity Yes Yes Yes PhotoaUergy No Yes No Immunomodulation Yes Yes No HR Yes Yes No Photoaging Yes Yes Yes Photocarcinogenesis Yes Yes No
HR, Hyperplastic reaction. This is one of the cutaneous mechanisms of accommodation to further UV insult and is the result of thickening of the malphigian and horny layers *Visible light may induce immediate pigmentation in persons with darker skin (skin types V and VI)
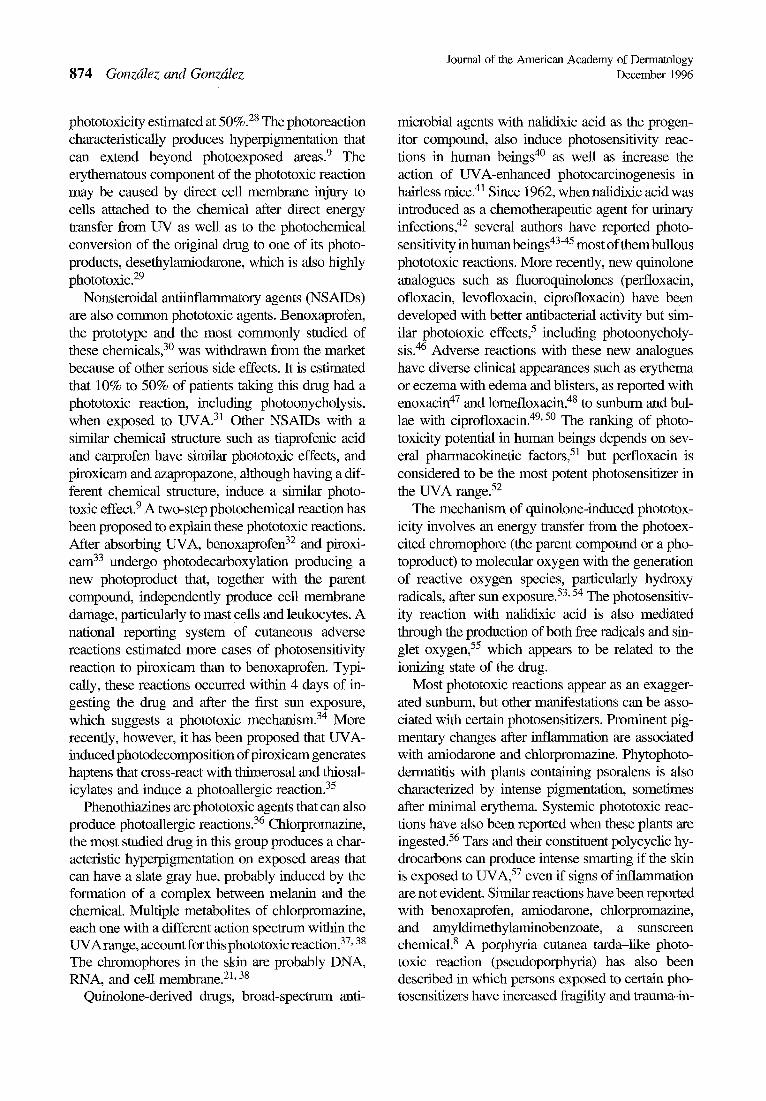
(chromophores) to induce photobiologic responses such as sunburn and drag photosensitivity. Table I lists the major photobiologic reactions induced by the different ranges of wavelength. The UV part of the spectrum has been divided into UVC, UVB, and UVA radiation on the basis of their photobiologic properties. UVC has no natural effect on the skin because it is blocked by the ozone layer of the atmo- sphere. The UVB range extends from 290 to 320 nm and is a short-wave, high-energy spectnLm also known as sunburn radiation because of its efficiency in producing erythema. The UVB specmma can in- teract with some chemicals to enhance sunburn erythema, referred to as a phototoxic reaction. The UVA range extends from 320 to 400 nm and recently has been subdivided into UVA-1 (340 to 400 nm) and UVA-2 (320 to 340 nm). It is also called "black light" or near visible radiation because the longer wavelengths border the violet of visible light. Al- though UVB is more erythemogenic than UVA 6 (minimal dose required at 295 nm for the erythema response is 1250 times higher than that at 365 nm), more photons in the UVA region reach the earth's surface (10 to 100 times higher for UVA than for UVB) 7 (Table I/). UVA radiation is implicated in most photoa_llergic reactions, a delayed hypersensi- tivity response, as well as in some phototoxic reac- tions and idiopathic dermatoses. UVA penetrates more deeply into the skin, to the dermis, because its longer wavelengths are not scattered as much as the shorter UVB wavelengths.
Table II. Spectra of solar irradiance and solar flux at the earth's surface during the summer months for zenith angle 0 ° C
Solar irradiance ( W / m 2)
Solar flux (%) (sea level)
UVC UVB UVA Visible (<290 (2~ (3~- ( ~ l nm) 320 nm) 400 nm) 760 run)
5.36 21 .10 85 .70 722.00
- - 0.5 6.3 54.3
Modified from Fredfich JE, Snell HE, Haywood EK. Photochem Pho- tobiol 1989;50:443-50.
The drug
It is estimated that approximately 50 drags are photosensitizers. 8 Characteristically, they are cyclic and tricyclic resonating compounds, many with an alternative double-bond isoprene nucleus. The ma- jority have a molecular mass between 300 to 500 grn/mol. All absorb radiation in either the visible or UV range, usually in the UVB and UVA spectra. The action specmma refers to the irradiation spec- mma required by the photosensitizing chemical to produce disease and, for most chemicals, is similar to the absorption spectrum of the photosensitizer. Not all drugs with these characteristics produce a photochemical reaction in the skin because this de- pends on such variables as percutaneous absorption, metabolic alteration, combination with a substrate, and stability and solubility. 9
The skin
The skin has many substrates or endogenous chromophores that can absorb UV radiation, includ- ing keratin proteins, hemoglobin, porphyrins, caro- tene, nucleic acids, melanin, fipoprotein, peptide bonds, and aromatic amino acids such as tyrosine, tryptophan, and histidine. 1° Nucleic acids and pro- teins in the epidermis are the most important chro- mophores for UVB and, when absorbed by DNA, lead to production of covalent bonds between adja- cent thymidine molecules, producing pyrirnidine dimers (Table m). Other UVB-induced DNA le- sions are cyfidine dimers and cytidine thymidine photoproducts. UVA, on the other hand, can be ab- sorbed by chromophores within the epidermis as well as by structural proteins in the dermis. TM 12
Melanin is the main chromophore in the epider- mis absorbing photons with wavelengths from 350 to 1200 nm. Whereas there appears to be agreement

Journal of the American Academy of Dermatology Volume 35, Number 6 Gonzdlez and Gonzdlez 873
on the protective effect that melanin absorption of visible light has on human skin, protection against LWB radiation does not seem to be as complete. In studies on vifiliginous skin, for example, it has been shown that the protection conferred by melanin against photobiologic reactions in the UVB range is only partial, a3 In addition, darkly complected pa- tients with HIV infection frequently have photosen- sitivity reactions. 14, ~5
Mechanisms of interaction
All photosensitizers must absorb energy in the form of specific photons. The absorbed photons from the electromagnetic spectrum are converted into chemical energy that is stored by the molecule in an electronically excited state until the energy is utilized for chemical reactions that can transform the original chemical into a metabolite (a photoproduct), transfer the energy to a biologic molecule such as protein, or shed the energy as either light or heat) 6 Most photosensitized reactions are oxygen-depen- dent and represent photodynamic action. In most phototoxic reactions, after excitation, the photosen- sitizer is converted to a short-lived, highly energized singlet state compound, which in turn is converted into a longer-lived, slightly less energetic compound that has a higher probability of participating in pho- tobiologic reactions. This can occur through two major pathways identified as type I and type 1I reac- tions. The type I reaction can result in hydrogen atom abstraction, producing radicals, or it can involve transfer of an electron from the triplet state of the photosensitizer to another compound to produce free radicals. Subsequently, a variety of oxidation-reduc- tion reactions occur and hydroperoxides are formed)2, 16 The type II reaction is a direct energy transfer reaction between the triplet state of the ex- cited photosensitizer and the ground-state oxygen prodncing a highly energetic singlet oxygen that re- acts with and oxidizes a wide variety of biologic compounds including lipid peroxides. 17
Photosensitivity reactions can be oxygen inde- pendent. The most important one is the UVA- induced covalent binding of psoralens to DNA to produce a phototoxic reaction. This can occur natu- rally during exposure to plants containing psoralens (limes, celery) and to UVA from sunlight to produce a phytophotodermatitis. The clinical application of this photochemical reaction is the combination of topical or oral psoralens and UVA from sunlight or a~Jficial sources to exert an effect on specific chro-
Table IlL UV-induced DNA damage
UV SPECTRUM DNA damage
UVC Pyrimidine dimers (<290 r im) Pyrimidine photoadducts
Strand breaks UVB Pyrimidine dimers
(290-320 nm) Photodynamic actions (ROS production)
UVA Photodynamic actions (320-400 nm) Photosensitization reactions (protein
and DNA cross-finks, DNA-photosensitizer photoadducts)
ROS, Reactive oxygen species.
mophores of the skin for therapeutic value such as induction of pigmentation in vitiligo] 8 suppression of DNA synthesis of epidermal cells in psoriasis, 19 and immunomodulation in lichen planus. 2°
Phototoxicity
Phototoxicity refers to an immediate or delayed inflammatory reaction reflecting direct cellular dam- age produced by the photochemical reaction be- tween a chemical photosensitizer and the appropri- ate radiation on the skin. The reaction will occur during the first exposure in may person of the same skin type as long as the threshold for the concentra- tion of the chemical and radiation has been attained. The most common manifestation of this photochem- ical reaction is an exaggerated sunburn in exposed areas. The action spectrum of these photochemical and photobiologic reactions expands from the UVB to the UVA range (Table I). Although presumably not immunologically mediated, recent evidence sug- gests a role for complement in this reaction. 21 Other mediators implicated in phototoxic reactions include histamine, 22 proteases, and prostaglandins. 23
One of the most common causes of phototoxic reactions are the tetracyclines. Demethylchlortetra- cycline 4, 24 and doxycycline 25 have the highest index of phototoxicity, whereas tetracycline, the parent compound, has a lower index. Phototoxic reactions to minocycline, a synthetic tetracycline, are rare. Human and in vitro studies have identified the action specmun to be in the UVA range. 25 The precise mechanism is unclear, but in vitro studies have shown that they are dependent on oxygen and com- plement, 2~ and the chromophores in the skin are the cell membranes and DNA. 26,27 Amiodarone, an- other common photosensitizer, has an incidence of
874 Gonzdlez and Gonzdlez Journal of the American Academy of Dermatology
December 1996
phototoxicity estimated at 50%. 2s The photoreaction characteristically produces hyperpigmentation that can extend beyond photoexposed areas. 9 The erythematous component of the phototoxic reaction may be caused by direct cell membrane injury to cells attached to the chemical after direct energy transfer from UV as well as to the photochemical conversion of the original drug to one of its photo- products, desethylamiodarone, which is also highly phototoxic. 29
Nonsteroidal antiinflammatory agents (NSAIDs) are also common phototoxic agents. Benoxaprofen, the prototype and the most commonly studied of these chemicals, 3° was withdrawn from the market because of other serious side effects. It is estimated that 10% to 50% of patients taking this drug had a phototoxic reaction, including photoonycholysis, when exposed to UVA. 31 Other NSAIDs with a similar chemical structure such as tiaprofenic acid and carprofen have similar phototoxic effects, and piroxicam and azapropazone, although having a dif- ferent chemical stxucmre, induce a similar photo- toxic effect. 9 A two-step photochemical reaction has been proposed to explain these phototoxic reactions. After absorbing UVA, benoxaprofen 32 and piroxi- cam 33 undergo photodecarboxylation producing a new photoproduct that, together with the parent compound, independently produce cell membrane damage, particularly to mast cells and leukocytes. A national reporting system of cutaneous adverse reactions estimated more cases of photosensitivity reaction to piroxicam than to benoxaprofen. Typi- cally, these reactions occurred within 4 days of in- gesting the drag and after the first sun exposure, which suggests a phototoxic mechanism. 34 More recently, however, it has been proposed that UVA- induced photodecomposition of piroxicam generates haptens that cross-react with thimerosal and thiosal- icylates and induce a photoallergic reaction. 35
Phenothiazines are phototoxic agents that can also produce photoallergic reactions. 36 Chlorpromazine, the most studied drug in this group produces a char- acteristic hyperpigmentation on exposed areas that can have a slate gray hue, probably induced by the formation of a complex between melanin and the chemical. Multiple metabolites of chlorpromazine, each one with a different action spectrum within the
37 38 UVArange, account for this phototoxic reaction. , The chromophores in the skin are probably DNA, RNA, and cell membrane. 21'38
Quinolone-derived drugs, broad-specmun anti-
microbial agents with nalidixic acid as the progen- itor compound, also induce photosensitivity reac- tions in human beings 4° as well as increase the action of UVA-enhanced photocarcinogenesis in hairless mice. 41 Since 1962, when nalidixic acid was introduced as a chemotherapeutic agent for urinary infections, 42 several authors have reported photo- sensitivity in human beings 4345 most of them bullous phototoxic reactions. More recently, new quinolone analogues such as fluoroquinolones (perfloxacin, ofloxacin, levofloxacin, ciprofloxacin) have been developed with better antibacterial activity but sim- ilar phototoxic effects, 5 including photoonycholy- sis. 46 Adverse reactions with these new analogues have diverse clinical appearances such as erythema or eczema with edema and blisters, as reported with enoxacin 47 and lomefloxacin, 48 to sunburn and bul- lae with ciprofloxacin. 49, 5o The ranking of photo- toxicity potential in human beings depends on sev- eral pharmacokinetic factors, 51 but perfloxacin is considered to be the most potent photosensitizer in the UVA range. 52
The mechanism of quinolone-induced phototox- icity involves an energy transfer from the photoex- cited chromophore (the parent compound or a pho- toproduct) to molecular oxygen with the generation of reactive oxygen species, particularly hydroxy radicals, after sun exposure. 53, 54 The photosensitiv- ity reaction with nalidixic acid is also mediated through the production of both free radicals and sin- glet oxygen, 55 which appears to be related to the ionizing state of the drug.
Most phototoxic reactions appear as an exagger- ated sunburn, but other manifestations can be asso- ciated with certain photosensitizers. Prominent pig- mentary changes after inflammation are associated with amiodarone and chlorpromazine. Phytophoto- dermatitis with plants containing psoralens is also characterized by intense pigmentation, sometimes after minimal erythema. Systemic phototoxic reac- tions have also been reported when these plants are ingested. 56 Tars and their constituent polycyclic hy- drocarbons can produce intense smarting if the skin is exposed to UVA, 57 even if signs of inflammation are not evident. Similar reactions have been reported with benoxaprofen, amiodarone, chlorpromazine, and amyldimethylaminobenzoate, a sunscreen chemical, s A porphyria cutanea tarda-like photo- toxic reaction (pseudoporphyria) has also been described in which persons exposed to certain pho- tosensitizers have increased fragility and trauma-in-

Journal of the American Academy of Dermatology Volume 35, Number 6 Gonzdlez and Gonzdlez 875
duced blisters on exposed areas instead of the more common acute phototoxic manifestations. Nalidixic acid, furosemide, naproxen, amiodarone, 28 and high- dose tetracycline 58 have been implicated.
Histopathologic changes in most phototoxic reac- tions include variable edema, vasodilation, and a mononuclear infiltrate in the dermis as well as intra- cellular and intercellular edema of keratinocytes (spongiosis) with basal cell degeneration. Phototoxic reactions produced by topical photosensitizers are usually more severe than with systemic drags. 8
Confn'matory tests for phototoxicity are many, 59 but the clinical application of any individual test is still controversial because of the lack of sensitivity. An in vitro test that uses photolysis of Candida al- bicans 6° has been utilized, which, when combined with testing on animal models such as the "mouse tail" test 6~ and the guinea pig model, appears to correlate with the potential phototoxic effect in hu- man beings. Photopatch testing and intradermal testing in human beings are not reliable to diagnose phototoxic reactions.
Photoallergy
A photoallergic reaction is mediated by lympho- cytes and is characterized as a delayed hypersensi- tivity reaction. The coexistence of immediate and delayed hypersensitivity in patients with a photo- allergic reaction has been described. 62 The clinical, histologic, and pathophysiologic features are similar to those of allergic contact dermatitis except that ra- diation is essential in the formation of a complete antigen. 63 Unlike phototoxic reactions, photoa_llergic reactions require an induction and elicitation phase, affect fewer persons, and are not as dependent on the concentration of the photoagent or the duration of the exposure. The action spectrum of these reactions is in the UVA range (Table I).
The events in the photochemical reaction in- volved in the formation of a complete antigen are not well understood. It has been postulated that the ab- sorbed radiation can convert the drug into an immu- nologically active compound, or the drug itself can absorb the photons, to interact photochemically with the carrier protein to become a complete anti- gen.63, 64 Conversely, a stable dimer may form from the interaction of photons and the drug to become a hapten, 65 as has been shown with 6-methylcou- matin, a photosensitizer in fragrance removed from the market because of its frequent photoallergic re- actions. Once a complete photoantigen is formed, it
will be presented to lymphocytes by Langerhans cells to initiate the induction phase of a delayed hy- persensitivity response. On subsequent exposure a cascade of events (elicitation phase) mediated by cytokines produces an inflammatory response iden- tical to allergic contact dermatitis.
Most photoallergic reactions are mediated by topical agents and the most common early offenders were biocides added to soaps, such as the haloge- nated phenolic compounds, 66 as well as ingredients in fragrance such as 6-methylcoumarin and musk ambrette.67, 68 These ingredients are rarely found in topical products since they have been removed from the market. Systemic photoallergens such as phe- nothiazines, chlorpromazine, and sulfa-derived products, 69 as well as NSAIDs, 35 can produce pho- toallergic reactions, although most of their photo- sensitive reactions are phototoxic.
The histopathologic changes of photoallergic re- actions are identical to allergic contact dermatitis with spongiosis in the epidermis and an intense perivascular infiltrate composed primarily of lym- phocytes in the dermis.
The confirmatory test for photoallergy is the pho- topatch test based on the principle that a photosen- sitized person will react with an eczematous derma- titis if exposed to the incriminated photoantigen and the appropriate radiation. Two identical panels of common photosensitizers are applied under occlu- sion to the back for 24 hours. One of the panels is exposed to a measured amount of radiation below the level of energy that will normally produce erythema, whereas the other panel, serving as the control, is protected from radiation. Reactions are interpreted at 72 to 96 hours. A positive reaction ob- served in the panel exposed to radiation is diagnos- tic. ff both panels showed similar reactions, a con- tact allergic dermatitis should be suspected. The ra- diation s p e c ~ r n used in photopatch testing is in the UVA range because this is the radiation absorbed by photoallergens. The energy used is usually 10 J/cm 2, which is below the threshold of erythema (minimal erythema dose [MED]) for normal persons. Because some patients with a photodermatosis may have ab- normal reactions to radiation, we recommend per- forming phototesting to determine the MED in each patient before the photopatch test is done. 7° This procedure requires incremental exposures of radia- tion on normal skin through templated windows to determine the minimal energy that will produce a well-defined erythema. 71

Journal of the American Academy of Dermatology 876 Gonzdlez and Gonzdlez December 1996
Lichenoid photosensitivity reactions
Lichenoid reactions to photosensitizers appear as violaceous or brown, papulosquamous lesions on exposed areas that morphologically resemble idio- pathic lichen planus. 72 Unlike the latter, the lesions are confined to sun-exposed areas, oral lesions are absent, and histologic examination reveals an intense and deep dermal lymphocytic infiltrate. Hydrochlo- rothiazide 73 is a frequent inducer of this reaction, but other common photosensitizers, including NSAIDs and qninidine-defived drugs, 72, 74, 75 have been in- criminated. These reactions are delayed in onset and suggest a hypersensitivity response to the photosen- sitizer.
Persistent light reaction
Persistent light reaction is a subset of photoaller- gic dermatitis in which the patient continues to have an eczematous dermatitis when exposed to specific radiation even after the photochemical offender has been removed from the environment. The original cases were associated with exposure to the haloge- nated salicylanilides present in soaps in England 76 and, later on, were reported in the United States as- sociated with exposure to bithionol in topical anti- septics. 77 In addition to their expected abnormal photopatch test reactivity, these patients have an ab- normal MED to UVB and the histologic features are consistent with an eczematous dermatitis. 78 The majority of cases of persistent light reactions have been associated with topical photosensitizers, such as the halogenated salicylanilides, bithionol, phe- nothiazines, musk ambrette, and 6-methylcoumarin, although systemic photosensitizers such as chlor- promazine have also been implicated. 9
Treatment
Photosensitivity reactions are more complex than other drug hypersensitivities because both the drag and the spectrum of absorbed radiation have to be identified for successful therapy. Removal of the drag will be effective in most patients with the ex- ception of persistent fight reactors, for whom it is essential to avoid the offending UV specmma. Pho- totoxic reactions wiU subside within a week, similar to a sunburn, whereas photoallergic reactions will behave like contact allergic eczematous dermatitis and last up to 3 weeks. Persistent fight reactions can be serf-perpetuating and can last for decades.
An acute phototoxic reaction can be managed
with wet cool compresses. Topical or oral corticos- teroids have not been shown to be of consistent value. For acute or chronic photoallergic reactions, topical or systemic corticosteroids are indicated and are important in persistent light reactions because of its chronicity. The combination of photochemother- apy (PUVA) and oral corticosteroids has been beneficial in producing temporary remissions. 79 Preventive therapy is dependent on the use of sun- protecting agents such as headcovers, clothing, and topical sunscreens, either chemical or physical. It is important to know the UV absorption or action spectra of the chemical photosensifizers because preventive measures may need to be tailored to them. For example, a patient exposed to a photosensifizer with an action spectrum in the UVA range would not be protected by windshield or window glass, which only blocks UVB radiation, and will need to rely on clothing, sunblockers, or sunscreens that are effec- tive in that range. Unfortunately, premarketing tox- icity evaluations for chemicals do not require photo- testing, and therefore information on the absorption and action spectrum of most chemicals is lacking. Photoprotection encompassing the entire UV spec- trtma is therefore recommended for patients exposed to these photochemicals. Topical sunscreens and their protective characteristics are discussed later.
IDIOPATHIC PHOTODERMATOSES
Idiopathic photodermatoses represent a group of diseases in which unidentified endogenous chemi- cal(s) interact with a specific spectrum of UV radi- ation and visible fight to produce a well-character- ized clinicopathologic entity. Their importance stems from their frequent and widespread occurrence and their overlapping clinical features with other diseases such as lupus erythematosus, urticarial and eczem- atous dermatoses, as well as cutaneous T-cell lym- phoma. By far, the most common of these disorders is polymorphous light eruption (PMLE) and its sub- sets, which account for about one third of all idiopathic photodermatoses. Solar urticaria is the least prevalent; chronic actinic dermatitis has been described more frequently in European countries than in the United States. A recent report, however, evaluated 51 patients with chronic actinic dermato- sis seen in three centers in the United States (42 pa- tients) and one in Japan (nine patients) and suggested that the disease is more common than previously suspected. It should be noted that the criteria for the diagnosis of chronic actinic dermatosis (see "Chron-
Journal of the American Academy of Dermatology Volume 35, Number 6 Gonzdlez and Gonzdlez 877
ic Actinic Dermatitis") in this study was modified to include patients with less than 1 year of a persistent eczematous eruption and an abnormal MED to UVB was not required. Furthermore, 63% of the 35 patients in one institution were sldn types V and VI. so
P M L E
Although the true prevalence of PMLE is not known, a survey of 271 apparently healthy persons demonstrated that 10% had a history consistent with this entity. 81 Because the symptomatic expression of the disease is variable, it is likely that many milder cases go unreported. The colloquial terms for this condition are sun poisoning or sun allergy. Charac- teristically, PMLE is a disease of young, fair-skinned women, particularly those younger than 30 years of age. However, the eruption can affect persons of different races and color 82 and can occur during childhood, primarily in boys 5 to 12 years of age; it is referred to as ' 'juvenile spring eruption." 83 PMLE is considered to be inherited as an autosomal dom- inant disease with reduced penetrance in 3% to 56% of patients. 84, 85 Environmental or geographic factors may also play a role because fair-skinned natives from geographic locations with high UV flux rarely have the disease. 86 It is not known whether this phe- nomenon is due to a hardening effect on the skin by continuous exposure, to some immunologic sup- pression, or to a natural selection process.
The diagnosis of PMLE is based mainly on his- tory and physical examination because laboratory findings are nonspecific. Histopathologic findings are not characteristic and there are no serologic or immunologic confirmatory tests. The typical history is the development of a pruritic eruption on exposed areas of the body, particularly the mid upper chest and extensor aspect of the arms, which appears be- tween 2 hours and 5 days after exposure to relatively intense UV radiation, either as the first exposure during early spring in temperate zones or as occa- sional exposure to sunlight in a high flux area such as the tropics. The eruption subsides spontaneously in 1 to 6 days if there is no further exposure to sun- light. With gradual, incremental exposure to UV ra- diation the condition clears; and it is typical for pa- tients to describe increased tolerance to sunlight as they continue to expose during the summer months. The fact that the face is frequently spared is proba- bly an expression of this hardening effect because the face is continuously exposed to some UV radiation,
even during winter months in colder environments. The term PMLE reflects the pleomorphic nature
of the eruption with the appearance of papules, plaques, vesicles, erythema mul~brme-like, and eczematous lesions in different patients. However, most patients will have a monomorphic manifesta- tion, primarily papular, of the disease. Eczematous lesions may be secondary to scratching or friction 87 because they are not reproduced by diagnostic chal- lenge with UV radiation. Lesions usually healed with no scarring.
The histopathologic changes of PMLE are not characteristic, consisting of parakeratosis and spon- giosis in the epidermis and a lymphocytic perivas- cular infiltrate in the papillary and reticular dermis with variable edema. Serologic tests such as those to detect antinuclear and Ro/La antibodies, as well as direct and indirect immunofluorescence, are nega- tive, and they can help differentiate PMLE from conditions such as lupus erythematosus.
The results of conventional phototesting to deter- mine MED are frequently normal. Provocative pho- totesting with daily consecutive UV radiation, par- ticularly to UVA, until the original eruption is reproduced has been advocated, but standardization is lacking and results are variable. A common method is to expose nonlesional skin to a measurable amount of subthreshold erythema levels of UVA or UVB radiation for 4 to 8 consecutive days. Fifty-six percent of patients have their action spectrum in the UVA range, and 26% will react to both UVA and UVB radiation, s8 Other investigators have reported the reproduction of PMLE lesions primarily with UVB.S9 A crude but practical method is to challenge and observe the patient after 1 hour of sun exposure at peak hours. Photopatch tests are usually negative.
The pathogenesis of PMLE is not fully under- stood, although it has been postulated to be a man- gestation of a delayed hypersensitivity reaction be- cause it resembles immunologic responses mediated by CD4 + lymphocytes and these activated cells pre- dominate in the skin infiltrate. 9°
The disease is usually recurrent with a mean du- ration ranging from 6.8 to 13.9 years; 57% of patients still report some manifestations 7 years lat- er. 9l
Controversy still abounds concerning other idio- pathic photodermatoses that share some clinical fea- tures with PMLE. Hydroa aestivale, considered at one time to be an entity sui generis, is now consid- ered to be a PMLE variant in children, whereas other

878 Gonzdlez and Gonz6lez Journal of the American Academy of Dermatology
December 1996
cases may have been undiagnosed erythropoietic protoporphyria. Hydroa vacciniforme is a rare pho- tosensitive dermatosis affecting primarily boys in the farst decade of life, with a family history of photo- sensitivity and a strong personal history of atopic dermatitis in at least 25% of them. 88 Characteristi- cally, a vesicular eruption develops in these children in crops on the face, ears, and chest, associated at times with fever and malaise at its onset. Lesions become necrotic and leave prominent scarring like smallpox, hence the term vacciniforme. In contrast with PMLE, the eruption can occur all year, although it is more symptomatic in the summer months. The condition clears or abates spontaneously during adulthood. 92
Some observers consider actinic prurigo a variant of PMLE, and others believe it is a different disor- der. 93 This entity has features that overlap the man- ifestations of hydroa vacciniforme such as onset before 10 years of age in 80% of patients, family history of photosensitivity, and personal history of atopy; the eruption can involve nonexposed areas and occur throughout the year. Distinguishing fea- tures from PMLE and hydroa vacciniforme include prominent centrofacial involvement, primarily the nose, and the presence of cheilitis. 92 American Indi- ans from Canada to South America seem to have a familial tendency for this photodermatosis, which at one time was called hereditary PMLE94; the cases reported from Europe are more sporadic. Histologic findings and routine phototesting can not differenti- ate these entities from PMLE.
Therapy for PMLE and these other diseases is similar and consists of protection from the specific UV spectrum with physical exogenous barriers such as clothing and sunscreens as well as with systemic treatments including antimalarial drugs, 95 carotene, 96 phototherapy, 97 and, in more severe and recalcitrant cases, thalidomide 98 and azathioprine. 99
Solar urticaria
Solar urticaria is a rare idiopathic photodermato- sis that represents an IgE-mediated hypersensitivity reaction, analogous to acute urticaria, which appears on UV-exposed areas within 30 minutes of expo- sure. Individual lesions can clear within 24 hours. Solar urticaria has a predilection for young women. In severe cases, constitutional symptoms associated with release of histamine and other mediators of in- flammation can be severe enough to require emer- gency intervention. 1°° The action spectrum is across
the range of UV radiation and, less commonly, vis- ible fight. Phototesting with the specific energy will produce an urticarial response within 1 hour. Histo- pathologic changes are those of an urticarial reaction with dermal edema, vasodilation and a variable perivascular infiltrate consisting of lymphocytes and eosinophils.
Therapy with antihistamines, either histamine1 (H1) blockers or H1 and H2 blockers combined, has sometimes been successful in controlling the erup- tion. 1°1 Avoidance of the specific UV radiation or visible fight with external physical agents is para- mount or, conversely, the use of photochemotherapy with or without systemic steroids has been effective to induce tolerance, as with other photoderma- toses. 1°2 Clearing has also been reported after re- peated exposures to fluorescent lamps or sunlightJ °3
Chronic actinic dermatitis
The term chronic actinic dermatitis encompasses previously described individual photodermatoses that appear to have common features, especially an
104 abnormal MED to UVB. Photosensitive eczema, chronic photosensitivity dermatitis, persistent fight reaction, and actinic reticuloid 1°5 are now considered part of this spectrum that primarily affects white men older than 50 years of age, although it has also been described in Japanese and black persons. 1°6 The condition is characterized by a persistent (at least a year), prudtic, eczematous dermatitis with promi- nent fichenification, mainly involving sun-exposed areas, although erythroderma develops in a large percentage of patients. The eruption extends into the winter months and therefore can be disabling through the entire year. The histologic features can vary from typical eczematous changes to a lymphoma-like ap- pearance with atypical ceils infiltrating the dennis and epidermis as originally reported in the cases of actinic reticuloid. 1°5' 107 Severe cases of actinic reticuloid have been shown to have circulating S6zary ceils and, rarely, have evolved into a true lymphoma, l°s Another report, however, found that the incidence of lymphoma in 231 patients with chronic actinic dermatosis was no different than that expected in the general population. 1°9 Furthermore, another study comparing 11 patients with chronic actinic dermatosis with three patients who had erythrodermic cutaneous T-ceil lymphoma demon- strated that the infiltrate of the former was immuno- histochemically different from the latter. The pa- tients in this study, however, deviated from the

Journal of the American Academy of Dermatology Volume 35, Number 6 Gonzdlez and Gonzdlez 879
Table IV. Topical sunscreens
Topical sunscreens
Chemical photoprotective agents
Physical photoprotective agents
Subtypes Examples
UV-absorbing
UV antioxidants UV scattering
UVB (PABA and its esters, cinnamates, salicylates, homosalate, anthranilates, triolaeate, PL*)
UVA (acrylates, anthranilates, benzophenones, dibenzoylmethanes)
Vitamin C, [3-carotene, PL* melanin, ZnO, FeC13 UV reflecting ZnO, TiO2t
FeCI3, Ferric chloride; PABA, p-aminobenzoic acid; PL, Polypodium leucotomos extract; Ti02, titanium dioxide; ZnO, zinc oxide. *Pathak MA, Gonz51ez S, Fitzpatrick TB. Polypodium leucotomos extract as photoprotectant. U.S. Patent Serial No. 08/388,261. See also Gonzfilez S, Pathak MA. Inhibition of ultraviolet-induced formation of reactive oxygen species, lipid peroxidation, erythema and skin photosensitization by Polypodium leucotomos. Photodermatol Photoimmunol Photomed 1996; 12:45-56 +Recent evidence shows that ZO and TiO2 can also absorb the impinging photons of certain wavelengths. 118
typical patients with chronic actinic dennatosis be- cause 73% were black and some had normal MED to UVB. Furthermore, no phototesting was per- formed on the patients diagnosed with lymphoma and one Caucasian subject diagnosed with chronic actinic dermatitis had a normal MED to UVB, UVA, and visible light as well as photoallergy to musk ambrette, which cast some doubts on these observations. 11°
Phototesting results are w~-iable with some pa- tients having an abnormal MED to UVB with or without an abnormal MED to UVA and visible light. Patients with the actinic reticuloid stage of chronic actinic dermatosis are particularly sensitive to UVA and visible light. Photopatch tests can be positive in some patients with chronic actinic dermatosis, par- ticularly the ones with persistent light reaction. Pos- itive patch tests to plant antigens, pm~cnlarly from the Compositae family, have been frequently de- scribed in patients originally diagnosed as having actinic reticuloid, tll
It has been postulated that during photoallergic reactions in patients with chronic actinic dermatosis alterations and transformation of a skin chromophore develop into an endogenous antigen that can perpet- ually react with a specific photon to induce a chronic inflammatory process.112
Therapy for chronic actinic dermatosis, as with the other photodermatoses, is primarily dependent on protection from natural or artificial sources of the specific radiation. Tolerance has been induced with both UVB and PUVA, 113'114 whereas systemic drugs such as azathioprine, 1°s danazol, 115 and cy- closporineJ16, 117 have been used in more severe cases.
SUNSCREENS
Sunscreens can be divided into two broad catego- ries: chemical sunscreens and physical sunscreens or sunblockers (Table IV). Chemical sunscreens are agents that absorb specific photons of UV radiation and therefore are considered photosensitizers. Phys- ical sunscreens until recently were considered to play a passive role in these reactions, serving primarily as physical barriers that will reflect or scatter radiation and light, similar to clothing. Recent studies, how- ever, have demonstrated that some of these chemi- cals, such as titanium dioxide and zinc oxide, have a strong absorption band in the UV specmnn, and, as it pertains to UV radiation, they can be considered chemical sunscreens. 118 Presumably, chemical sun- screens absorb radiation energy at a level in the skin where no viable cells are present (stratum comeum), hence, their photoprotective properties. The fact that some of these sunscreens can produce phototoxic and photoallergic reactions suggests that at times a photochemical reaction can occur with endogenous chromophores present in viable skin.
Chemical sunscreens are wavelength-selective with a specific absorption specmma. Therefore they are divided into UVB and UVA sunscreens. The UVB sunscreens are effective in absorbing the entire UVB spectrum. UVA sunscreens, on the other hand, have a limited absorption spectrum, primarily ab- sorbing shorter wavelengths of UVA (320 to 360 nm). Therefore sunscreens are effective for UVB photoprotection, but because the action spectrum of many photodermatoses is in the UVA spectrum, the preventive therapeutic benefit of these sunscreens is limited. Furthermore, some concern has been raised about the possible adverse effects of prolonged UVA
880 Gonzdlez and Gonzdlez Journal of the American Academy of Dermatology
December 1996
exposure in persons using UVB sunscreens that will protect them from UVB-induced sunburn. UVA ra- diation is less erythemogenic than UVB; therefore persons can be exposed to excessive doses of UVA radiation without manifesting erythema. Because UVA radiation penetrates more deeply into the der- mis than UVB radiation, more chromophores in the skin can absorb UVA radiation with possible onco- genic and immunogenic consequences. UVA radia- tion produces dermal connective tissue alterations,119 induces release of vasoactive mediators, 12°' 121 and alters epidermal DNA synthesis 121 (Tables I and HI). Furthermore, UVA radiation can additively or syn- ergistically enhance UVB-induced erythema, UVB- induced carcinogenesis, and elastosisJ 22'123 An editorial presents an opposing view to this concern and provides evidence, based on biophysics calcula- tions, to dismiss the notion that higher potency sun- screens enhance exposure to dangerous amounts of UVA. 124
U V B s u n s c r e e n s
The UVB sunscreens are based on para-ami- nobenzoic acid (PABA) and its esters (padimate A and O) as well as on cinnamates and salicylates. 125 They effectively block approximately 90% of UVB radiation across its entire spectrum (290 to 320 nm) and therefore offer complete protection against UVB-indueed sunburn. Because of the concern for frequent adverse reactions reported with PABA and some of its esters (e.g., padimate A), many products are now labeled PABA-ffee. Cinnamates have be- come the most common ingredients in LWB sun- screens.
A standard test referred to as sun protection fac- tor (SPF) has been developed to establish the pho- toprotective value of these sunscreens and is part of the labeling required by the Food and Drug Admin- istration (FDA) in the United States. This SPF determination compares UVB-induced ery~ema, measured in MED, before and after use of the sun- screen in a controlled environment and under opti- mal conditions. A UVB sunscreen with an SPF of 4, therefore, will protect a person four times longer than if the unprotected skin was exposed to the same amount of UVB.
U V A s u n s c r e e n s
The UVA sunscreens, which provide limited pro- tection, contain benzophenones, anthralinates, and
126 dibenzoylmethanes. Benzophenones and anthrali-
nates have an absorption spectrum limited to 300 to 350 nm, whereas butyl methoxy dibenzoylmethane (Parsol 1789) absorbs maximally at 340 to 350 nm. Unfortunately, safety concerns for the latter, prima- rily contact allergy and its instability, have precluded its wider use. 127 Because these chemicals are par- tially absorbed in the UVB specmun, they are com- bined with sunscreens that offer a more complete protection in the UVB range.
Presently, there is no standard test to determine the photoprotective qualities of UVA sunscreens be- cause determining UVA-induced erythema requires impractical, prolonged exposures. Tests of other features of UVA photoprotection by these sun- screens are being evaluated by several investigators, but up to now the FDA has not recommended any method326, 127
P h y s i c a l s u n s c r e e n s
Physical sunscreens, also called sunblockers, have been defined as opaque formulations, the effective- ness of which depends on the diameter or size of its particles and the thickness of the fdm to reflect or scatter UV radiation and visible lightJ 2s On the basis of more recent data, 118 however, they can be cate- gorized according to their optical properties into chemicals that scatter visible light and UV radiation equally well, scatter visible light and absorb UV radiation, or scatter and absorb visible light and UV radiation to different extents. Titanium dioxide and zinc oxide, the two most common chemicals, can absorb UVA wavelengths up to 400 nm as well as scatter and reflect visible light and UV radiationJ 18
The previous belief that compliance and cosmetic acceptance were poor because sunblockers had to be applied as thick films and their effectiveness was limited by environmental factors, such as sweat and swimming, is being reconsidered. The recent data suggest that thin invisible films that are cosmetically acceptable are effective and they can be photopro- tective despite adverse environmental factors. Re- cently, titanium dioxide has been micronized to pro- vide a more cosmetically acceptable product 129 without sacrificing photoprotection. An additional advantage of these two chemicals is that they are not antigenic.
C o m b i n a t i o n s u n s c r e e n s
Most available sunscreens are a combination of UVB and UVA chemical sunscreens, frequently

Journal of the American Academy of Dermatology
Volume 35, Number 6 Gonzdlez and Gonzdlez 881
Table V. Adverse reactions to sunscreens
Chemical agent Contact I (optical density range) 133 hypersensitivity PhotoaUergy [ Phototoxicity Examples*
Benzophenone-3134-136 (270-350 nm) No Yes No PreSun-15, Ultrashade,
2-Ethyl-hexyl-p-dimethylaminobenzoate (290-315 nm)
PABA 135'136 (260-313 nm) Homomenthyl saficylate 137 (290-315 rim) Butylmethoxydibenzoylmethane136,13s, 139 4-Isopropyldibenzoylmethane 139 2-Ethoxy-ethyl-hexyl-p-methoxy-
cinnamate (270-328 rim)
Sundown-15, Coppertone Supershade- 15, Coppertone Sport 30
No Yes No Ultrashade, Sundown, Suprashade, Coppertone, Photoplex?
Yes Yes Yes Sunbrella, Pabanol Yes No No Aztec, Coppertone oil and lotion Yes Yes No Photoplex No Yes No
Digalloyl Irioleate (270-320 nm) Methyl anthranilate (290-320 nm)
No Yes No Yes No No
Shade-15, Sundown, Solbar, Coppertone, Almay FuUer Filter Sun Creme
Sun Protectol, Sun Swept Cream Maxafil, A-Fil
Benzophenone-3 = oxybenzone; 2-ethyl-hexyl-p-dimethylaminobenzoate = padimate-O; butylmethoxydibenzoylmethane = Parsol 1789; 4-isopro- pyldibenzoyl methane = Eusolex 8020; 2-ethoxy-ethyl-hexyl-p-methoxy-cinnamate = Cinnoxate. ~Withdrawn from the U.S. market. *Registered trademark.
with the addition of a physical surlscreen. These combinations confer more effective photoprotection for persons with fair skin (skin types I and II), those who undergo prolonged sun exposure, and persons with abnormal responses to UV radiation and visi- ble light. The American Academy of Dermatology Consensus Statement on Photoaging/Photodamage as a Public Health Concern recommends that a maximally protective sunscreen (SPF 15 or higher) be applied under most conditions.*
Vehicle and substantivity
The vehicle of the chemical stmscreen is signifi- cant in its photoprotective properties because it de- termines whether a sunscreen remains effective un- der general use conditions, such as sweating, swim- ruing, and prolonged sunbathing. The adherent property of the sunscreen to the skin or substantivity varies considerably among commercially available formulations. Sunscreen preparations with a poly- acrylamide base, for example, are highly substantive to the skin and tend to resist washing off or removal after sweating or swimming. 12s, 130
Sunscreens are classified in terms of their resis- tance to water or waterproof qualifies. A water-
*American Academy of Dermatology. Consensus Conference on Photoaging/Photodamage as a Public Health Concern. Boston, Mass., 1988,
resistant sunscreen should retain its substantivity, determined by comparing SPF factors before and after 40 minutes of immersion in water while the user is swimming in a controlled environment, whereas a waterproof sunscreen should show the same prop- erty after 80 minutes of water immersion during swimming, 127
Adverse reactions to sunscreens
Adverse reactions to chemical sunscreen formu- lations include contact dermatitis, both irritant and allergic, as well as phototoxic and photoallergic re- actions. 131-139 Contact allergic dermatitis can be produced by chemical sunscreens, the most common being PABA, benzophenones, cilmamates, and methoxydibenzoylmethane, as well as by excipients in the formulation of which fragrance and the preservatives are the most common. Table V fists examples of adverse reactions. Phototoxic and pho- toallergic reactions axe primarily produced by the chemical snnscreen, although in some situations ex- cipients such as fragrance can also produce photo- allergic responses. 131, 132, 136
Zinc oxide and titanium dioxide used in physical sunscreen formulations do not produce contact sen- sitization, phototoxicity, or photoallergy. The excip- ients in the physical sunscreen should be suspected if such reactions occur.
Journal of the American Academy of Dermatology 8 8 2 Gonzdlez and Gonzdlez December 1996
REFERENCES
1. Spikes JD. Photosensitization. In: Smith KC, editor. The science of photobiology. New York: Plenum, 1977:87- 110.
2. Ayd JF Jr. The dermatologic and systemic manifestations of chlorpromazine hypersensitivity: their clinical signif- icance and management. J Nerv Mental Dis 1956;124: 84-7.
3. Calnan CD, Frain Bell W, Cuthbert JW. Occupational dermatitis from chiorpromazine. Trans St John's Hosp Derm Soc 1962;48:49-74.
4. Orentreich A, Harber LC, Tromovitch TA. Photosensi- tivity and photoonycholysis due to demethylchlortetracy- cline. Arch Dermatol 1961;83:730-7.
5. Halkin H. Adverse effects of the fluoroquinolones. Rev Infect Dis 1988;10(suppl):S258-61.
6. Parfish JA, Jaenicke KF, Anderson RR. Erythema and melanogenesis action spectra of normal human skin. Phntochem Photobiol 1982;36:187-91.
7. Fredrich JE, Snell HE, Haywood EK. Solar ultraviolet ra- diation at the earth's surface. Photochem Phntobiol 1989;50:443-50.
8. Johnson BE, Ferguson J. Drug and chemical photosensi- tivity. In: Maibach HI, editor. Seminars in dermatology. Philadelphia, WB Saunders, 1990:39-46.
9. Harber LC. Abnormal responses to ultraviolet radiation: drug-induced photosensitivity. In: Fitzpatrick TB, Eisen AZ, Wolff K, et al, editors. Dermatology in general med- icine. New York: McGraw-Hill, 1993:1677-89.
10. Ledo E. Photodermatosis. Part 1: Photobiology, photo- immunology, and idiopathic photodermatoses. Int J Der- matol 1993;12:387-96.
11. Peak MJ, Peak JG, Churchill ME. Cellular and molecular effects of UVA radiation and visible light in mammalian cells. In: Urbach F, editor. Biological response to ultravi- olet A radiation. Overland Park, KS: Valdenmer Publish- ing, 1992:39-46.
12. Goldstein BD, Harber LC. Erythropoietic porphyria: lipid peroxidation and red cell membrane damage associated with photochemolysis. J Invest Dermatol 1972;51:892- 902.
13. Kollias N, Baqer AH. The role of human melanin in providing photoprotection from solar mid-ultraviolet ra- diation (280-320 nm). J Soc Cosmet Chem 1988;39:347- 54.
14. Berger TG, Dhar A. Lichenoid photoemptions in human immunodeficiency virus infection. Arch Dermatol 1994; 130:609-13.
15. Pappert A, Grossman M, DeLeo V. Photosensitivity as the presenting illness in four patients with human immuno- deficiency viral infection. Arch Dermatol 1994; 130:618- 23.
16. Spikes JD. Photodynamic reactions ha photomedicine. In: Regan J, Parrish JA, editors. The science of photomedi- cine. New York: Plenum Press, 1982:113-44.
17. Bissett DL, Chatterjee R, Haunon DP. Photoprotective effect of superoxide scavenging antioxidants against ultraviolet radiation-induced chronic skin damage in the hairless mouse. Photodermatol Photoimmunol Phntomed 1990;7:56-62.
18. Parrish JA, Fitzpatrick TB, Shea C, et al. Photochemo- therapy of vifiligo: use of orally administered psoralens and a high-intensity long-wave ultraviolet light system. Arch Dermatol 1976;112:1531-4.
19. Gonzalez E. PUVA for psoriasis. Dermatol Clin 1995; 13:851-66.
20. Gonzalez E, Momtaz T K, Freedman S. Bilateral com- parison of generalized lichen planus treated with psor- alens and ultraviolet A. J Am Acad Dermatol 1984;10: 958-61.
21. Lim HW, Novotny H, Gigli I. Role of complement and polymorphonuclear cells in demethylchlortetracycline- induced phototoxicity in guinea pigs. J Clin Invest 1983; 71:1326-35.
22. Lam SK, Tomlinson DR. Chlorpromazine-induced histamine release from guinea pig skin in vitro: a photo- sensitivity reaction. Arch Dermatol Res 1976;255:219- 23.
23. Falk MS. Light sensitivity to demethylchiortetracycline: report of four cases. JAMA 1960;172:156-8.
24. Bjellemp M, Ljunggren B. Double blind cross-over studies on phototoxicity to three tetracycline derivatives in human volunteers. Photodermatology 1987;4:281-7.
25. Bjellerup M. Tetracycline phototoxicity: an experimental and clinical study. Phi) thesis. Lurid, Sweden, 1986.
26. Kochevar IE. Mechanisms of drug photosensitization. Photochem Photobiol 1987;45:891-5.
27. Piette J, Decuyper J, Van De Vorst A. DNA alterations photosensitized by tetracycline and some of its deriva- tives. J Invest Dermatol 1986;86:653-8.
28. Chalmers R J, Muston HL, Srinivas V, et al. High incidence of amiodarone-induced photosensitivity in No~hwest England. Br Med J 1982;285:341-2.
29. Hasan T, Kochevar IE, Abdulah D. Amiodarone photo- toxicity to human erythrocytes and lymphocytes. Photo- chem Photobiol 1984;40:715-9.
30. Ljunggren B, Bjeilemp M, Moiler H. Experimental studies on the mechanism of benoxaprofen photoreac- tions. Arch Dermatol Res 1983;275:318-23.
31. Ljnnggren B, Bjellemp M. Systemic drug photosensitiv- ity. Photodermatology 1986;3:26-35.
32. Kochevar IE, Hoover KW, Gawienowski M. Benoxapro- fen photosensitization of ceil membrane disruption. J In- vest Dermatol 1984;82:214-8.
33. Kochevar IE, Morison WL, Lamm JL, et al. Possible mechanisms of piroxicam-induced photosensitivity. Arch Dermatol 1986;12:1283-7.
34. Stern R. Phototoxic reactions to piroxicam and other nonsteroidal anti-inflammatory agents. N Engl J Med 1983 ;309:186-7.
35. Ikezawa Z, Kitamura K, Osawa J, et al. Photosensitivity to piroxicam is inttuced by sensitization to thirnerosal and thiosalicylate. J Invest Dermatol 1992;98:918-22.
36. Epstein S. Chlorpromazine photosensitivity: phototoxic and photoallergic reactions. Arch Dermatol 1968;98: 354-63.
37. Ljunggren B, M611er H. Phenothiazine phototoxicity: an experimental study in chlorpromazine and its metabolites. J Invest Dermatol 1977;68:313-7.
38. Ljunggren B. Phenothiazine phototoxicity: toxic chlor- promazine photoproducts. J Invest Dermatol 1977;69: 383-6.
39. Hunter JAA, Bhutani LK, Magnus IA. Chlorpromazine photosensitivity in the mouse: its action specmun and the effect of anti-inflammatory agents. Br J Dermatol 1970; 82:157-68.
40. Takayama S, Hirohashi M, Kato M, et al. Toxicity of quinolone anfimicrobial agents. J Toxicol Environ Health 1995 ;45:1-45.
41. Baes H. Photosensitivity caused by nalidixic acid. Der- matologica 1968;136:61-4.
42. Lesher GY, Froelich EJ, Gmett MD, et al. 1,8-Naphtyr-
Journal of the American Academy of Dermatology Volume 35, Number 6 Gonzdlez and Gonzdlez 883
idine derivatives: a new class of chemotherapeutic agents. J Med Pharm Chem 1962;5:1063-8.
43. Birkett DA, Gawets M, Stevenson CJ. Phototoxic bullous eruptions due to nalidixic acid. Br J Dermatol 1969; 81:342-4.
44. Ramsay CA, Obreshkova E. Photosensitivity from nalid- ixic acid. Br J Dermatol 1974;91:523-8.
45. Brauner GJ. Bullous photoreaction to nalidixic acid. Am J Med 1975;58:576-80.
46. Baran R, Brun P. Photoonycholysis induced by fluoro- qninolones perfloxacine and ofloxacine. Dermatologica 1986; 173:185-8.
47. Izu R, Gardeazabal J, Gonz~lez M, et al. Enoxacin- induced photosensitivity: study of two cases. Photoder- matol Photoimmunol Photomed 1992;9:86-8.
48. Kummaji Y, Shono M. Scarified photopatch testing in lomefloxacin photosensitivity. Contact Dermatitis 1992; 26:5-10.
49. Nedorost ST, Dijkstra JWE. Drag-induced photosensi- tivity reaction. Arch Dermatol 1989;125:433-4.
50. Granowitz EV. Photosensitivity rash in a patient being treated with ciprofloxacin. J Infect Dis 1989; 160:910-1.
51. Fujita H, Matsuo I. In vitro phototoxic activities of new quinolone antibacterial agents: lipid peroxidative poten- tials. Photodermatol Photoimmunol Photomed 1994;10: 202-5.
52. Christ W, Lehnert T. Toxicity of the quinolones. In: Si- porin C, Heifetz CL, Domagala JIM, editors. The new generation of qninolones. New York: Marcel Dekker. 1990:165-86.
53. Wagai N, Tawara K. Possible direct role of reactive ox- ygens in the cause of cutaneous phototoxicity induced by five quinolones in mice. Arch Toxicol 1992;66:392-7.
54. Wagai N, Tawara K. Possible reasons for difference in phototoxicity of 5 qninolone antibacterial agents: gener- ation of toxic oxygen. Free Radic Res Comm 1992;17: 387-98.
55. Dayhaw-Barker P, Tmscott TG. Direct detection of sin- glet oxygen sensitized by nalidixic acid: the effect of pH and melanin. Photochem Photobiol 1988;47:765-7.
56. Ljunggren B. Severe phototoxic bum following celery ingestion. Arch Dennatol 1990; 126:1134-6.
57. Crow KD, Alexander E, Buck WHL, et al. Photosensi- tivity due to pitch. Br J Dermatol 1961;73:220-2.
58. Epstein JI-I, Tuffanelll DL, Seibert JS, et al. Porphyria-like cutaneous changes induced by tetracycline hydrochloride photosensitization. Arch Dermatol 1976;112:661-6.
59. Johnson BE, Walker EM, Hetherington AM. In vitro models for cutaneous phototoxicity. In: Marks R, Plewig G, editors. Skin models to study function and disease of skin. New York: Springer-Verlag, 1986:264-81.
60. Ison AE, Davis CM. Phototoxicity of qninoline methanols and other drugs in mice and yeast. J Invest Dermatol 1969 ;52:193-8.
61. Ljunggren B. The mouse tail phototoxicity test. Photo- dermatology 1984;1:96-100.
62. HoriT. Chlorpromazinephotoallergy: coexistence ofim- mediate and delayed type. Arch Dermatol 1975;111: 1469-71.
63. Harber LC, Harris H, Baer RL. Photoallergic contact der- matitis due to halogenated salicylanilides and related compounds. Arch Dermatol 1966;94:255-62.
64. Harber LC, Targovnik SE, Baer RL. Contact photosensi- tivity patterns to halogenated salicylanifides, in man and guinea pigs. Arch Dermatol 1967;96:646-56.
65. Kato S, Seki T, Katsumura Y, et al. Mechanism for 6-m-
ethylcoumarin photoallergenicity. Toxicol Appl Pharma- col 1985;18:295-301.
66. Smith SZ, Epstein JH. Photocontact dermatitis to haloge- nated salicylanilides and related compounds. Arch Der- matol 1977;113:1372-4.
67. Raugi GJ, Storrs J, Larsen WG. Photoallergic contact dermatitis to men's perfumes. Contact Dermatitis 1979;5: 251-60.
68. Wojnarowska F, Calnan CD. Contact and photocontact allergy to musk ambrette. Br J Dermatol 1986;114: 667-75.
69. Magnire HC, Kaidbey K. Studies in experimental photo- allergy. In: Parrish JA, editor. The effect of ultraviolet ra- diation on the immune system. Skillman, NJ: Johnson & Johnson, 1983:181-92.
70. Granstein RD, Gonzfilez E. Photoallergic contact derma- titis. In: Provost TT, Farmer ER, editor. Current therapy in dermatology: 2. Toronto: BC Decker, 1988:168-71.
71. Bilsland D, Diffey BL, Farr PM, et al. Diagnostic photo- testing in the United Kingdom. Br J Dermatol 1992;127: 297-9.
72. Frain-Bell WC. Drug-induced photosensitivity, ha: Frain- Bell WC, editor. Cutaneous photobiology. Oxford: Ox- ford University Press 1985:125-52.
73. Harber LC, Lashinsky AM, Baer RL. Skin manifestations of photosensitivity due to chlorothiazide and hydrochlo- rothiazide. J Invest Dermatol 1959;33:83-4.
74. Wolf R, Doffman B, Krakowski A. Quinidine-induced lichenoid and eczematous photodermatitis. Dermatolog- ica 1987;174:285-9.
75. Tan SV, Barth-Jones J, Bums DA. Lichen planus and photo-onycholysis induced by quinine [letter]. Chn Exp Dermatol 1989;21:1304-5.
76. Wilkinson DS. Photodermatitis due to tetrachlorosalicy- lanilide. Br J Dermatol 1961;73:213-9.
77. Jillson OF, Baughnaan RD. Contact photoderrnatitis from bithionol. Arch Dermatol 1963;88:409-18.
78. Kaidbey KH, Messenger JL. The clinical spec~m of the persistent light reactor. Arch Dermatol 1984; 120:1441-8.
79. Mofison WL. Other photodermatoses. In: Parrish JA, Kripke MI, Morison WL, editors. Photoimmunology. New York: Plenum Press, 1983:267-71.
80. Lhn HW, Mofison WL, Kamide R, et al. Chronic actinic dermatitis: an analysis of 51 patients evaluated in the United States and Japan. ArchDermato11994; 130:1284-9.
81. Morison WL, Stern RS. Polymorphous fight eruption: a common reaction uncommonly recognized. Acta Derm Venereol (Stockh) 1982;62:237-40.
82. Epstein JH. Polymorphous light eruption. J Am Acad Dermatol 1980;3:329-43.
83. Van Praag MCG, Boom BW, Vermeer JB. Diagnosis and treatment of polymorphous light eruption. Int J Dermatol 1994;33:233-9.
84. Jansen CT. Heredity of chronic polymorphous fight erup- tions. Arch Dermatol 1978;114:188-90.
85. Holzle E, Plewig G, von Kries R, et al. Polymorphous light eruption. J Invest Dermatol 1987;88(suppl):32s-8s.
86. Harber LC, Bickers DR. Polymorphous light eruption. In: Photosensitivity diseases: principles of diagnosis and treatment. 2nd ed. Toronto: BC Decker, 1989:219-34.
87. Hawk J, Cheong WK. Eczematous photodermatoses. In: Marks R, editor. Eczema. London: Martin Dtmitz, 1992: 149-56.
88. Ortel B, Tanew A, Wolff K, et al. Polymorphous light eruption: action spectrum and photoprotection. J Am Acad Dermatol 1986;14:748-53.
884 Gonzdlez and Gonzdlez Journal of the American Academy of Dermatology
December 1996
89. Epstein JH. Polymorphous light eruption. Dermatol Clin 1986;4:243-51.
90. Sckenins A, Fischer T, Forsum U. Phenotypic character- ization in situ of iifflammatory cells in allergic and irritant contact dermatitis in men. Clln Exp Immunol 1984;55: 81-90.
91. Jansen CT, Karvonen J. Polymorphous light eruption: a seven-year follow-up evaluation of 114 patients. Arch Dermatol 1984;120:862-5.
92. Magnus IA. Hydroa vacciniforme. In: Dermatological photobiology. Oxford: Blackwell 1976:189-90.
93. Addo HA, Frain-Bell W. Actinic pmrigo: A specific der- matosis? Photodermatology 1984;1:119-28.
94. Birt AR, Davis RA. Hereditary polymorphous light eruption of American Indians. Int J Dermatol 1975;14: 105-11.
95. Murphy GM, Hawk JLM, Magnus IA. Hydroxychloro- quine ha polymorphous light eruption: a controlled trial with drug and visual sensitivity monitoring. Br J Derma- tol 1987;116:379-86.
96. Parrish JA, Levine MJ, Morison WL, et al. Comparison of PUVA and beta-carotene in the treatment of polymor- phous light eruption. Br J Dermatol 1979;110:193-7.
97. Murphy GM, Logan RA, Lowell CR. Prophylactic PUVA and UVB therapy in polymorphous fight eruption: a controlled trial. Br J Dermatol 1986;116:531-8.
98. Saul A, Flores O, Novales J. Polymorphous light eruption: treatment with thalidomide. Australas J Dermatol 1976; 17:17-21.
99. Norris PG, Hawk JLM. Successful treatment of severe polymorphous fight eruption with azathiopfine. Arch Dermatol 1989;125:1377-9.
100. Lawrence N, Ray MC, Gattely LE HI. Photoimmunology: solar urticaria. In: Ray MC, editor. Applied immunoder- matology. New York: Igaku-Shoin, 1992:72-4.
101. Monfrecola G, Nappa P, Pini D. Solar urticaria in the vis- ible spectrum successfully treated with astemizole. Der- matologica 1990;180:154-6.
102. Morison WL. Solar urticaria. In: Parrish JA, Kripke MI, Morison WL, editor. Photoimmunology. New York: Ple- num Press, 1983:215-26.
103. Ramsay CA. Solar urticaria treatment by inducing toler- ance to artificial radiation and natural light. Arch Derma- tol 1977;113:1222-5.
104. Ramsay CA, Black A. Photosensitive eczema. Trans St Johns' Hosp Dermatol Soc 1973;59:152-8.
105. Ive FA, Magnus IA, Warin RP. Actinic reticuloid: a chronic photodermatosis associated with severe photo- sensitivity and histological resemblance to lymphoma. Br J Dermatol 1969;81:469-85.
106. Kingston TP, Lowe NJ, Sofen HL, et al. Actinic reticu- loid in a black man: successful therapy with azathioprine. J Am Acad Dermatol 1987;16:1079-83.
107. Toonstra J, Henquet CJM, van Weelden H. Actinic retic- uloid. J Am Acad Dermatol 1989;21:205-14.
108. Leigh IM, Hawk JLM. Treatment of chronic actinic dermatitis with azathioprine. Br J Dermatol 1984;110: 691-5.
109. Bilsland D, Crombie IK, Ferguson J. The photosensitiv- ity dermatitis and actinic reticuloid syndrome: no associ- ation with lymphoreticular malignancy. Br J Dermatol 1994;131:209-14.
110. Heller P, Wieczorek R, Waldo E, et al. Chronic actinic dermatitis, an immunohistochemical study of its T-cell antigenic profile, with comparison to cutaneous T-cell lymphoma. Am J Derm Pathol 1994;16:510-6.
111. Frain-Bell W, Hetherington A, Johnson BE. Contact al- lergic sensitivity to chrysanthemum and the photosensi- tivity dermatitis and actinic reticuloid syndrome. Br J Dermatot 1979;101:491-501.
112. Norris PG, Hawk JLM. Chronic actinic dermatitis. Arch Dermatol 1990;126:376-8.
113. Hindson C, Spiro J, Downey A. PLWA therapy of chronic actinic dermatitis. Br J Dermatol 1985;113:157-60.
114. Morison WL, White HAD, Gonzgdez E, et al. Oral methoxalen photochemotherapy of uncommon photo- dermatoses. Acta DermVenereol (Stockh) 1979;59: 366-8.
115. Humbert P, Drobacheff C, Vigan M. Chronic actinic der- matitis responding to danazol. Br J Dermatol 1991;124: 195-7.
116. Biren CA, Barr RJ Dermatologic applications of cyclo- sporine A. Arch Dermatol 1986;122:1028-32.
117. Norris PG, Camp RDR, Hawk JLM. Actinic reticuloid: response to cyclosporine A. J Am Acad Dermatol 1989; 21:307-9.
118. Sayre RM, Kollias N, Roberts RL, et al. Physical sunscreens. J Soc Cosmet Chem 1990;41:109-9.
119. Gilchrest BA, Soter NA, Hawk JL M, et al. Histologic changes associated with ultraviolet A-induced ery- thema in normal human skin. J Am Acad Dermatol 1983;3:213-9.
120. Hawk JL, Black AK, Jaenicke KF, et al. Increased concentration of arachidonic acid, prostaglandin E2, D2, and 6-oxo-Fl~, and histamine in human skin following UVA irradiation. J Invest Dermatol 1983;80: 496-9.
121. Matsni MS, DeLeo VA. Induction of protein kinase C activity by ultraviolet radiation. Carcinogenesis 1990; 11: 229-34.
122. Chew S, DeLeo VA, Harber LC. Long-wave ultraviolet radiation (UVA)-induced alteration of epidermal DNA synthesis. Photochem Photobiol 1988;47:383-9.
123. Paul BS, Parrish JA. The interaction of UVA and UVB in the production of threshold erythema. J Invest Derma- tol 1982;78:371-4.
124. Urbach F. Ultraviolet A transmission by modem sun- screens: Is there a real risk? Photodermatol Photoimmu- nol Photomed 1992/1993;9:237-41.
125. Lowe NJ. Photoprotection. Semin Dermatol 1990;9: 78-83.
126. Menter JM. Recent developments in UVA photoprotec- tion. Int J Dermatol 1990;29:389-401.
127. Ramsay CA: Ultraviolet A protective sunscreens. Clin Dermatol 1989;7:163-166.
128. Pathak MA, Fitzpatrick TB. Preventive treatment of sun- bum, dermatoheliosis, and skin cancer with sun-protective agents. In: Fitzpatrick TB, Eisen AZ, Wolff K, et al, ed- itor. Dermatology and general medicine. New York: McGraw-Hill, 1993:1689-717.
129. Klein K. Encyclopedia of UV absorbers for sunscreen products. Cosmet Toiletries 1992;107:45-62.
130. Stiller MJ, Davis IC, Shnpack JL. A concise guide to top- ical sunscreens: state of the art. Int J Dermatol 1992;31: 540-3.
131. Dromgoole SH, Maibach HI. Contact sensitization and photocontact sensitization of sunscreening agents. In: Lowe NJ, Shaath NA, editors. Sunscreens: development, evaluation, and regulatory aspects. Cosmetic Science and Technology Series; vol 10. New York: Marcel Dekker, 1990:313-40.
132. Foley F, Nickson R, Marks R, et al. The frequency of re- actions to sunscreens: results of a longitudinal population-
Journal of the American Academy of Dermatology Volume 35, Number 6 Gonzdlez and Gonzdlez 885
based study on the regular use of sunscreens in Australia. Br J Dermatol 1993;128:512-8.
133. Pathak MA. Sunscreens: topical and systemic protection against solar radiation for human skin. Photochem Pho- tophys 1987;4(suppl):447-61.
134. Collins P, Ferguson J. Photoallergic contact dermatitis to oxybenzone. Br J Dermatol 1994;131:124-9.
135. Szczurko C, Dompmartin A, Michel M, et al. Photo- contact allergy to oxybenzone: ten years of experience. Photodermatol Photoimmunol Photomed 1994;10:144-7.
136. DeLeo VA, Suarez SM, Maso MJ. Photoallergic contact
dermatitis: results of photopatch testing in New York, 1985 to 1990. Arch Dermatol 1992;128:1513-8.
137. Rietschel RL, Lewis CW. Contact dermatitis to homo- menthyl salicylate. Arch Dermatol 1978;114:442-3.
138. De Groot AC, Weyland JW. Contact allergy to butyl methoxydibenzoylmethane. Contact Dermatitis 1987; 16:278.
139. Motley RJ, Reynolds AJ. Photocontact dermatitis due to isopropyl and butyl methoxy dibenzoylmethanes (Euso- lex 8020 and Parsol 1789). Contact Dermatitis 1989; 21:109-10.
Related Documents











