Dr.Toba kazemi Associate Professor of Cardiology BUMS-BCRC 17 Esfand 1390

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Dr.Toba kazemiAssociate Professor of Cardiology
BUMS-BCRC17 Esfand 1390

تعريف :تعريف :
منجر که سرم چربیهای سطح اختالل منجر به که سرم چربیهای سطح اختالل بهقلبی بیماریهای ریسک افزایش قلبی به بیماریهای ریسک افزایش به
که شود می گفته شود، می که عروقی شود می گفته شود، می عروقی هیپرتریهیپرتری، ، هیپرکلسترولمیهیپرکلسترولمیشامل شامل
و LDLLDL، ، گلیسریدمیگلیسریدمی و باال می HDLHDLباال می پايين پايين باشد.باشد.

ليپيدمي ديس ليپيدمي اهميت ديس اهميتاحتمال بيماري قلبي
عروقيچربي خونتغيير در ميزان چربي
احتم;ال بيم;اري % 1اف;زايش در زنان ومردان
ازاي mg/dlبه افزايش1
LDL
احتم;ال بيم;اري % 1اف;زايش در زنان ومردان
mg/dlبه ازاي فزايشا1
Non-HDL
% احتمال 37افزايش % 14وبيماري در زنان
درمردان
mg/dlبه ازاي افزايش89
TG
در ميزان مرگ % 3كاهش ومير بيماري قلبي در زنان
درمردان%2و
mg/dlبه ازاي افزايش1
HDL

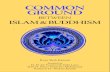
Log-linear Relationship Between LDL-C Levels and Log-linear Relationship Between LDL-C Levels and Relative Risk for CHDRelative Risk for CHD
• This relationship is consistent with a large body of epidemiological data and with data available from clinical trials of LDL-lowering therapy
• These data suggest that for every 30-mg/dL change in LDL-C, the relative risk for CHD is changed in proportion by about 30%. The relative risk is set at 1.0 for LDL-C 40 mg/dL.
Grundy S, et al. Circulation. 2004;110:227-239
RelativeRiskfor
CoronaryHeart
Disease(Log Scale)
LDL-Cholesterol, mg/dL
40 70 100 130 160 190
1.0
1.3
1.7
2.2
2.9
3.7

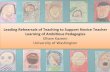
Risk of CHD by TG LevelRisk of CHD by TG LevelThe Framingham Heart Study )30-Year Follow-Up(The Framingham Heart Study )30-Year Follow-Up(
Reprinted from Castelli WP. Am J Cardiol. 1992;70:3H-9H, with permission from Elsevier.
Rel
ativ
e C
HD
Ris
k
TG Level, mg/dL
0
0.5
1
1.5
2
2.5
3
50 100 150 200 250 300 350 400
N = 5127 patients with no history of CHD
Men
Women
Univariate analysis of data from the Framingham Heart Study, including 5127 patients aged 30to 60 years without CHD, to determine the relationship between TGs and CHD.

بندي بندي تقسيم تقسيم


ايجادايجاد عللعلل
اوليهاوليه) (ژنتيك) ژنتيك)ثانويهثانويه)..... / و ) بيماريها زندگي شيوه .....(تغييرات / و ) بيماريها زندگي شيوه تغييرات

(اوليهاوليه (ژنتيك) ژنتيك)
Primary causes : single or multiple Primary causes : single or multiple genegene mutations that result in either mutations that result in either overproductionoverproduction or or defective clearance defective clearance of TG and LDL cholesterol, or of TG and LDL cholesterol, or in underproduction or excessive clearance of HDLin underproduction or excessive clearance of HDL
Primary disorders, Primary disorders, the most common cause the most common cause of of dyslipidemia in dyslipidemia in childrenchildren, do not cause a large , do not cause a large percentage of cases in adults.percentage of cases in adults.


Secondary causesSecondary causes
Secondary causes contribute to Secondary causes contribute to mostmost cases of cases of dyslipidemia in dyslipidemia in adultsadults..
The The mostmost important secondary cause in developed important secondary cause in developed countries is a countries is a sedentary lifestyle sedentary lifestyle with excessive dietary with excessive dietary intakeintake of saturated fat, cholesterol, and trans fats. of saturated fat, cholesterol, and trans fats.
Other :DM, alcohol overuse, chronic kidney disease, Other :DM, alcohol overuse, chronic kidney disease, hypothyroidism, primary biliary cirrhosis and liver hypothyroidism, primary biliary cirrhosis and liver diseasesdiseases
DrugsDrugs: Thiazides, β-blockers, retinoids, highly active : Thiazides, β-blockers, retinoids, highly active antiretroviral agents, estrogen , progestins, antiretroviral agents, estrogen , progestins,

فاميليال فاميليال هيپركلسترولمي ((FHFH))هيپركلسترولمي FH is an FH is an ADAD disorder characterized : disorder characterized : elevated LDL-C + normal TG , tendon xanthomas, elevated LDL-C + normal TG , tendon xanthomas, prematurepremature
CADCAD FH is caused by a large number )>1000( mutationsFH is caused by a large number )>1000( mutations
in the LDL receptor gene.in the LDL receptor gene. The elevated levels of LDL-C in FH are due to an increase in The elevated levels of LDL-C in FH are due to an increase in
the production of LDL from IDL )since a portion of IDL is the production of LDL from IDL )since a portion of IDL is normally cleared by LDL receptor-mediated endocytosis( and normally cleared by LDL receptor-mediated endocytosis( and a delayed removal of LDL from the blood.a delayed removal of LDL from the blood.
FH homozygotesFH homozygotes: : 22 mutated LDL receptor mutated LDL receptor FH heterozygotesFH heterozygotes: : 11 mutant allele mutant allele Individuals with FH homozygotes haveIndividuals with FH homozygotes have
higher LDL-C levels than those FH heterozygoteshigher LDL-C levels than those FH heterozygotes

LDL receptorLDL receptor
A mutated LDL receptorA normal LDL receptor

HomozygousHomozygous FHFH
1 in 1 million persons worldwide.1 in 1 million persons worldwide. The disease has The disease has >90% penetrance >90% penetrance so both parents of FH so both parents of FH
homozygotes usually have hypercholesterolemia.homozygotes usually have hypercholesterolemia.
Clinical manifestation:Clinical manifestation: cutaneous xanthomas on the hands, wrists, elbows, knees, heels, or cutaneous xanthomas on the hands, wrists, elbows, knees, heels, or
buttocks present in childhood buttocks present in childhood CHOL are usually >500 mg/dL and can be higher than 1000 CHOL are usually >500 mg/dL and can be higher than 1000 mglmgldL.dL. Important complication of is Important complication of is accelerated atherosclerosisaccelerated atherosclerosis, which can result in , which can result in
disability and death in childhood.disability and death in childhood. Atherosclerosis often develops first in the aortic root, where it can cause Atherosclerosis often develops first in the aortic root, where it can cause
aortic valvular or supravalvular stenosis, and typically extends into the aortic valvular or supravalvular stenosis, and typically extends into the coronary ostia, which become stenotic.coronary ostia, which become stenotic.

HomozygousHomozygous FHFH
Exams and Tests:Exams and Tests: A physical examination may reveal A physical examination may reveal xanthomas and corneal arcus. and corneal arcus. A strong A strong familyfamily historyhistory of familial hypercholesterolemia or early heart of familial hypercholesterolemia or early heart
attacksattacks High levels High levels of LDL of LDL in either or both in either or both parentsparents.. Individuals from families with a strong history of early heart attacks should Individuals from families with a strong history of early heart attacks should
have blood tests done to determine lipid levels.have blood tests done to determine lipid levels.

DysbetalipoproteinemiaDysbetalipoproteinemia
Dysbetalipoproteinemia,, is a rare lipid disorder characterized by high levels Dysbetalipoproteinemia,, is a rare lipid disorder characterized by high levels of blood of blood cholesterol & & TG.TG.
CHOLCHOL range from range from 300-600300-600 mg/dL. mg/dL. TGTG are usually are usually >400 >400 mg/dL and may mg/dL and may exceed 1000 mg/dL. exceed 1000 mg/dL.
Moderately elevated total cholesterol and triglyceride levels accompanied by Moderately elevated total cholesterol and triglyceride levels accompanied by the presence of the presence of palmar crease xanthomas palmar crease xanthomas confirm the diagnosis confirm the diagnosis dysbetalipoproteinemiadysbetalipoproteinemia

ClinicalClinical findingsfindings
Patients may have no physical findings or may have skin lesions called Patients may have no physical findings or may have skin lesions called xanthomasxanthomas, particularly in more severe presentations. , particularly in more severe presentations.
Xanthoma striata palmarisXanthoma striata palmaris Tuberoeruptive and tuberous xanthomasTuberoeruptive and tuberous xanthomas Corneal arcus ,Corneal arcus , Xanthelasmas Obesity or signs of Obesity or signs of hypothyroidism may be noted. may be noted.


باليني باليني عاليم عاليم
فندارد ليپيدمي ديس به مربوط مشخصا كه فندارد عالمتي ليپيدمي ديس به مربوط مشخصا كه عالمتي محيطي عروق يا كرونر بيماري مثل عاليم با فرد محيطي ممكنست عروق يا كرونر بيماري مثل عاليم با فرد ممكنستHigh levels of TGs )> 1000 mg/dL( can cause High levels of TGs )> 1000 mg/dL( can cause acute acute
pancreatitispancreatitis . . زودرس خطر خطر كرونر زودرس بيماري كرونر بيماري شدن شدن طبيعي پيشرفت طبيعي يا ايجاد مانع پيشرفت ليپيد يا ايجاد مانع ليپيد
..((pancreatitispancreatitis//premature CADpremature CAD))عوارضعوارض

باليني هاي باليني يافته هاي يافته High levels of High levels of LDLLDL :eyelid :eyelid xanthelasmasxanthelasmas; ; arcusarcus corneae; corneae;
tendinoustendinous xanthomas . xanthomas . familial hypercholesterolemia :the above findings plus planar familial hypercholesterolemia :the above findings plus planar
or cutaneous xanthomasor cutaneous xanthomas severe elevations of severe elevations of TGsTGs can have can have eruptiveeruptive xanthomas xanthomas Patients with Patients with dysbetalipoproteinemiadysbetalipoproteinemia can have can have palmarpalmar and and
tuberous xanthomastuberous xanthomas Severe Severe hypertriglyceridemiahypertriglyceridemia )> 2000 mg/dL( can give retinal )> 2000 mg/dL( can give retinal
arteries and veins a creamy white appearance )arteries and veins a creamy white appearance )lipemia lipemia retinalis(.retinalis(.
Extremely high lipid levels also give a lactescent )milky( Extremely high lipid levels also give a lactescent )milky( appearance to blood plasma.appearance to blood plasma.



DiagnosisDiagnosis Lipid profile measurementLipid profile measurement Testing should be postponed until after Testing should be postponed until after resolution of acute resolution of acute
illnessillness, because TGs increase and cholesterol levels , because TGs increase and cholesterol levels decrease in inflammatory states. Lipid profiles can vary for decrease in inflammatory states. Lipid profiles can vary for about 30 days after an about 30 days after an acute MIacute MI; however, results obtained ; however, results obtained within 24 h after MI are usually reliable enough to guide within 24 h after MI are usually reliable enough to guide initial lipid-lowering therapy.initial lipid-lowering therapy.
TC, TGs, and HDL cholesterol are measured directly.TC, TGs, and HDL cholesterol are measured directly. LDL cholesterol = TC − [HDL cholesterol + )TGs ÷ 5(] LDL cholesterol = TC − [HDL cholesterol + )TGs ÷ 5(]
))Friedewald formula(.Friedewald formula(. This calculation is valid only when This calculation is valid only when TGs are < 400 TGs are < 400 mg/dL mg/dL
and patients are and patients are fastingfasting

ScreeningScreening: : A fasting TC, TGs, HDL cholesterol, and A fasting TC, TGs, HDL cholesterol, and calculated LDL cholesterol should be obtained in all calculated LDL cholesterol should be obtained in all adults adults ≥ 20 yr ≥ 20 yr and should be repeated and should be repeated every 5 yrevery 5 yr..
screeningscreening patients patients < 20 yr< 20 yr: atherosclerotic : atherosclerotic risk factorsrisk factors, , such as diabetes, hypertension, cigarette smoking, and such as diabetes, hypertension, cigarette smoking, and obesity; obesity; premature CAD premature CAD in a parent, grandparent, or in a parent, grandparent, or sibling; or a sibling; or a cholesterol level > 240 mg/dL or known cholesterol level > 240 mg/dL or known dyslipidemia in a parent.dyslipidemia in a parent.
12 hours fasting12 hours fasting

Other testsOther tests 1- Lp)a( measurement 1- Lp)a( measurement :: Patients with premature atherosclerotic cardiovascular Patients with premature atherosclerotic cardiovascular
diseasedisease cardiovascular disease with normal or near-normal lipid cardiovascular disease with normal or near-normal lipid
levelslevels high LDL levels refractory to drughigh LDL levels refractory to drug Patients with an extensive family history of heart diseasePatients with an extensive family history of heart disease 2-C-reactive protein and homocysteine 2-C-reactive protein and homocysteine measurement may measurement may
be considered in the same populations.be considered in the same populations. 3-Tests for secondary causes3-Tests for secondary causes

3-Tests for secondary causes 3-Tests for secondary causes :: FBS, FBS, liver enzymes,liver enzymes, CreatininCreatinin TSHTSH urinary proteinurinary protein For who? )newly diagnosed dyslipidemia , when a For who? )newly diagnosed dyslipidemia , when a
component of the lipid profile has changed for the worse.component of the lipid profile has changed for the worse. A definite age after which no require screeningA definite age after which no require screening ?? ?? into their into their 80s80s, especially in the presence of , especially in the presence of
atherosclerotic cardiovascular disease.atherosclerotic cardiovascular disease.

US Hypertriglyceridemia )HTG( PrevalenceUS Hypertriglyceridemia )HTG( Prevalence
US Adult PopulationTotal = 217 millionTG ≥500 mg/dLTG ≥500 mg/dL
~~2.5%2.5%5-65-6 M patientsM patients
TG ≥500 mg/dLTG ≥500 mg/dL ~~2.5%2.5%
5-65-6 M patientsM patients
TG 200-499 mg/dLTG 200-499 mg/dL**~~13%13%
~~2828 M patientsM patients
TG 200-499 mg/dLTG 200-499 mg/dL**~~13%13%
~~2828 M patientsM patients

HIGH TGHIGH TG
INDEPENDENT RISK FACTOR FOR HEART INDEPENDENT RISK FACTOR FOR HEART ATTACKATTACK
INDEPENDENT RISK FACTOR FORINDEPENDENT RISK FACTOR FOR STROKESTROKE ASSOCIATED WITH LOW HDLASSOCIATED WITH LOW HDL ASSOCIATED WITH INCREASED CLOTTING ASSOCIATED WITH INCREASED CLOTTING
VIA HIGH PLASMINOGEN ACTIVATOR VIA HIGH PLASMINOGEN ACTIVATOR INHIBITOR ACTIVITY, HYPOFIBRINOLYSIS INHIBITOR ACTIVITY, HYPOFIBRINOLYSIS (CAN’T CHOP UP BLOOD CLOTS EASILY)(CAN’T CHOP UP BLOOD CLOTS EASILY)
A FUNDAMENTAL PART OF METABOLIC A FUNDAMENTAL PART OF METABOLIC SYNDROME, HIGH CHD RISKSYNDROME, HIGH CHD RISK

ديگر عوامل به ثانويه ديگر اغلب عوامل به ثانويه اغلباگزوژن اگزوژن استروژنهاي OCPOCP,,استروژنهاي
زياد زياد الكل الكلنشده كنترل خوب نشده ديابت كنترل خوب ديابت
سيستميك كورتن سيستميك مصرف كورتن مصرفكليه كليه نارسايي نارسايي

Familial hypertriglyceridemiaFamilial hypertriglyceridemia
Familial hypertriglyceridemia is a common disorder passed Familial hypertriglyceridemia is a common disorder passed down through families in which down through families in which the level of TG the level of TG are higher than are higher than normal.normal.
The condition is The condition is notnot associated with a significant increase in associated with a significant increase in cholesterolcholesterol levels. levels.
An An autosomal dominant fashion fashion Familial hypertriglyceridemia does Familial hypertriglyceridemia does notnot usually become usually become
noticeable noticeable until puberty or early adulthooduntil puberty or early adulthood. . Obesity, hyperglycemia )high blood glucose levels(, and high Obesity, hyperglycemia )high blood glucose levels(, and high
levels of insulin are often also present and may cause even levels of insulin are often also present and may cause even higher triglyceride levels.higher triglyceride levels.
about 1 in 500 individuals in the United States. about 1 in 500 individuals in the United States. Risk factors are a Risk factors are a family history of hypertriglyceridemia or a family history of hypertriglyceridemia or a
family history of family history of heart disease before the age of before the age of 5050..

FamilialFamilial hypertriglyceridemiahypertriglyceridemia--
Exams and TestsExams and Tests People with a family history of this condition should have blood tests to People with a family history of this condition should have blood tests to
check check very low density lipoprotein ) )VLDL( and ( and triglyceride levels. Blood tests levels. Blood tests usually show a mild to moderate increase in triglycerides usually show a mild to moderate increase in triglycerides )about 200 to 500 )about 200 to 500 mg/dL(mg/dL(

باال تريگليسريد تشخيصي باال رويكرد تريگليسريد تشخيصي رويكرد
علل علل رد ثانويهثانويهرد ميزان ميزان بررسي تريگليسريدتريگليسريدبررسي از از بيش تري 500500بيش اساس بر تري درمان اساس بر درمان
گليسريدگليسريد بین خون گلیسرید تری که صورتی بین در خون گلیسرید تری که صورتی dLdL//mgmgدر
باید 200- 200500- 500 ابتدا باید باشد ابتدا باشدChOLChOL––HDLHDL- - NonNon سپس و کنیم محاسبه سپس را و کنیم محاسبه را
بگیریم بگیریم تصمیم تصمیم). ). Non-HDL chol=Total Chol-HDLNon-HDL chol=Total Chol-HDL(( Target Non-HDL =LDL+30Target Non-HDL =LDL+30((((

LOW HDLLOW HDL
علل:علل: ( است انسولين به مقاومت با همراه است ) اغلب انسولين به مقاومت با همراه اغلب
. ، وزن اضافه چاقي ، باال گليسريد . تري ، وزن اضافه چاقي ، باال گليسريد تريتيپ ديابت ، كم فيزيكي تيپ فعاليت ديابت ، كم فيزيكي ( (22فعاليت
سيگارسيگار زياد خيلي هيدرات كربو با زياد رژيم خيلي هيدرات كربو با رژيم ( ، آنابوليك استروئيدهاي ، بتابلوكرها ) داروها ، آنابوليك استروئيدهاي ، بتابلوكرها داروها
ها ( ها (پروژستين پروژستين

LOW HDLLOW HDL درماندرمان
انجام LDLدرمان بر اساس
شود
HDL همراه پايين
n باال LDLبا
گليسريد تريدرمان بر اساس
باال
HDLهمراه با پايين
گليسريد تري
رژيم فعاليت بدني ، كاهش وزن
CAD يا CAD اگر بيمار
equivalent درمان با فيبرات يا :
نياسين
Isolated LOW HDL

Ddiagnostic approach-summaryDdiagnostic approach-summary
1-Measure fasting lipoproteins
3 -Identify CAD or CAD equivalents & CAD risk factors Slide 32
4 -If ≥ 2 major risk factors without CAD or CAD equivalent, assess 10-yr risk of MI or CAD death
using Framingham risk tables
5-refer to NCEP ATP III Guidelines for Treatment of Hyperlipidemia
2-primary/secondary

افراد در سرمی چربیهای افراد سطح در سرمی چربیهای سطح ))mg/dlmg/dlبالغ (بالغ (
خیلی باال
(very-high)
باال(high)
باالی
طبیعی
(high-
normal)
طبیعی
(normal)
--240≤ 239-200200< توتال
کلسترول
190≥ 189-160159-130130 <LDL
500≥ 499-200199-150150 <تری
گلیسرید
در زنها> 50 در مردها و > 40غیر طبیعی :
≤حد خيلي خوب وپيشگيري كننده از بيماريهاي قلبي 60
عروقي محسوب ميشود.
HDL

Rule out secondary causes)FBS,U/A,CR,TSH,LFT(Rule out secondary causes)FBS,U/A,CR,TSH,LFT( SedentarySedentary lifestyle, lifestyle, obesityobesity, and , and smokingsmoking are all associated with are all associated with
low HDL-C levels, and patients should be counseled about low HDL-C levels, and patients should be counseled about these issues.these issues.
Patients with hyperlipidemia, especially hypertriglyceridemia, Patients with hyperlipidemia, especially hypertriglyceridemia, who drink who drink alcoholalcohol should be encouraged to decrease their should be encouraged to decrease their intake.intake.
DrugsDrugs Attempts should be made to diagnose the Attempts should be made to diagnose the primaryprimary lipid disorder lipid disorder

CAD equivalentsCAD equivalents:: Peripheral arterial diseasePeripheral arterial disease Abdominal aortic aneurysmAbdominal aortic aneurysm Symptomatic carotid artery diseaseSymptomatic carotid artery disease Diabetes mellitusDiabetes mellitus
Major CAD risk factors in dyslipidemia:Major CAD risk factors in dyslipidemia: Cigarette smokingCigarette smoking Hypertension (BP ≥ 140/90 or on antihypertensive drug)Hypertension (BP ≥ 140/90 or on antihypertensive drug) Low HDL (≤ 40 mg/dL [1.03 mmol/L])Low HDL (≤ 40 mg/dL [1.03 mmol/L]) Family history of premature CAD (CAD in a male 1st-degree relative < Family history of premature CAD (CAD in a male 1st-degree relative <
55 or in a female 1st-degree relative < 65)55 or in a female 1st-degree relative < 65) Age (men ≥ 45, women ≥ 55)Age (men ≥ 45, women ≥ 55)

Framingham Framingham TenTen Year Risk Year Risk
Men Women

Framingham Ten Year RiskFramingham Ten Year Risk
0

Framingham Ten Year RiskFramingham Ten Year Risk
0
3 Non-Smoker
0

Framingham Ten Year RiskFramingham Ten Year Risk
0
3
0HDL = 43
1

Framingham Ten Year RiskFramingham Ten Year Risk
0
3
0
1SBP = 119, untreated
0
4

Framingham Ten Year RiskFramingham Ten Year Risk
0
3
0
1
0
4

ال ايده ال سطح ايده افراد Non HDLNon HDLووLDLLDLسطح افراد در درمختلفمختلف
میزان ریسکوضعیت بیمارLDL هدف
)mg/dl(شروع رژیم
غذایی و فعالیت
شروع دارو
HDL non-
هدف) mg/dl)
وبيماري عروق كرونر ديابت يا چند ريسك
فاكتور قلبي
Very High كمتراز 70
كمتر از ≥70 ≥70 100
بيماري عروق معادالت ياكرونر
آن
High كمتر از100
كمتر از ≥ 100 ≥ 100 130
ريسك فاكتور قلبي 2 ≥و احتمال بيماري كرونر
سال آینده 10در %10-20بين
Moderately High
كمتر از 100
كمتر از ≥ 130 ≥ 130 130
ريسك فاكتور 2 ≤قلبي و احتمال
بيماري كرونر در سال آینده کمتر 10
%10از
Moderate كمتر از130
كمتر از ≥ 160 ≥ 130 160
190كمتر از ≥ 190 ≥ 160 160كمتر از lowيك ريسك فاكتور ويا كمتر

TREATMENTTREATMENT

Ddiagnostic approach-summaryDdiagnostic approach-summary
1-Measure fasting lipoproteins
3 -Identify CAD or CAD equivalents & CAD risk factors
4 -If ≥ 2 major risk factors without CAD or CAD equivalent, assess 10-yr risk of MI or CAD death
using Framingham risk
5-refer to NCEP ATP III Guidelines for Treatment of Hyperlipidemia
2-primary/secondary

شماره بیمار شماره معرفی بیمار ::11معرفی
بیماریهای 5454خانم خانم از پیشگیری کلینیک به ای بیماریهای ساله از پیشگیری کلینیک به ای سالهمراجعه خود سالمت وضعیت بررسی جهت مراجعه غیرواگیر خود سالمت وضعیت بررسی جهت غیرواگیر
. k کامال تاکنون و ندارد عالمتی هیچگونه وي کند k . می کامال تاکنون و ندارد عالمتی هیچگونه وي کند می . و هیپرتانسیون دیابت، سابقه است بوده . سالم و هیپرتانسیون دیابت، سابقه است بوده سالم
. در کند نمی ذکر خانواده در را عروقی قلبی . بیماری در کند نمی ذکر خانواده در را عروقی قلبی بیماری . نشد مشاهده غیرطبیعی نکته . معاینه نشد مشاهده غیرطبیعی نکته معاینه
از بعد بیمار خون از آزمایشات بعد بیمار خون به 1212آزمایشات ناشتایی به ساعت ناشتایی ساعت: است زیر :شرح است زیر شرح
FBS=85 Chol = 220 TG= 332 HDL=42 FBS=85 Chol = 220 TG= 332 HDL=42 LDL=111 LDL=111

خانم خانم بیمار فاکتور 5454بیمار ریسک باال سن جز به که است ای فاکتور ساله ریسک باال سن جز به که است ای ساله . حد در بیمار خون قند و فشارخون ندارد عروقي . دیگرقلبي حد در بیمار خون قند و فشارخون ندارد عروقي دیگرقلبي
. توتال، کلسترول است . طبیعی توتال، کلسترول است قابل HDLHDLو و LDLLDLطبیعی حد در kقابل تقریبا حد در kتقریباباالست بیمار گلیسرید تری اما است، باالست قبولي بیمار گلیسرید تری اما است، قبولي
Non HDL- ChOL = 220-42=178Non HDL- ChOL = 220-42=178

باتشكر از همه شركت كنندگانwww.bums.ac.ir/heartwww.bums.ac.ir/heart
Related Documents