
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

OPIATESDr. ZolfaghariAssistant Professor of Emergency Medicine
Dr. Farahmand RadAssistant Professor of Emergency Medicine

OPIUM
شیره گیاهی است که از تیغ زدن گیاه اوپیوم پاپاورسومینیفرم بدست می آید و حاوی تعدادی
.از آلکالوئیدها است
: به سه دسته تقسیم می شونداوپیوئیدهاطبیعی، نیمه صناعی، صناعی
به مشتقات طبیعی اوپیوم اطالق می اوپیات ها «شود مانند
هرویین, کدئین، مورفین

OPIOIDS
مشتقات نیمه صناعی: بوپرنورفین، هیدروکدون و اکسی کدون، هیدرومورفین و اکسی مورفین
:مشتقات صناعی اپیومپتدین, متادون, پنتازوسین, پروپوکسی فن,
دیفنوکسیالت, فنتانیل, ترامادول
سه گیرنده عمده برای مواد مخدر در بدن وجود دارد:
Mukappadelta
PATOPHYSIOLOGY

جدول اثرات بالینی گیرنده ها
Mu : analgesia, euphoria, sedation, prolactin secretion, analgesia, respiratory depression, bradycardia, itching, GI dysmotility, dependency
K: analgesia, myosis, diuresis
dysphoria, analgesia
Delta: analgesia, inhibition of dopamine secretion
CLINICAL PERESENTATION
Pin point myosis, respiratory depression, loss of consciousness
Cardiovascular: hypotension, bradycardia, cyanosis, cardiac dysrhythmia
Respiratory: respiratory depression, pulmonary edema, hypoxia, bronchospasm
GI: constipation, Ileus, GI movement dysfunction Renal: retention, ATN, GN, proteinuria,
myoglubinuria
Musculoskeletal: rhabdomyolysis Nervous system: loss of consciousness, coma,
seizure, tremor Others: hypo or hyperthermia, nausea & vomiting
CLINICAL PERESENTATION

Myosis there is not in all opium toxic patient. Mydriasis is present with intoxication with some
opioids such as” diphenoxylate, meperidine, morphine, pentazocine, propoxyphene”
CLINICAL PERESENTATION
OPIATE AGONISTS
Heroin Morphine Methadone Diphenoxylate & atropine Meperidine Propoxyphene Codeine, Hydrocodone, & Dihydrocodeine Pentazocine & oxycodone Butorphanol & nalbuphine

Paregoric Hyromorphone Tramadol
OPIATE AGONISTS
OPIATE AGONIST-ANTAGONISTS
Buprenorphine(B2) Pentazocine Butorphanol Nalbuphine
OPIATE ANTAGONISTS
Naloxone Naltrexone Nalmefene

DIAGNOSIS
Pin point myosis Respiratory depression (RR<12) loss of consciousness
OR Pin point myosis Respiratory depression (RR<12) Circumstantial evidence of opioid use

DD
Intoxication with: Clonidine Organophosphate Carbamate Phenothiazine Atypical antipsychotic medications Sedative-Hypnotic medications Carbon monoxide
MANAGEMENT
Respiratory depression is the major morbidity and the cause of essentially all the mortality from opioid intoxication.
Airway protection and ventilatory management are the most important treatment for opioid-intoxicated individuals.

Adequate oxygenation Naloxone or endotracheal intubation Single-dose activated charcoal Delayed and multiple doses of activated charcoal• Diphenoxylate hydrochloride • Atropine sulfate overdoses • Large ingestions of sustained-release preparations
MANAGEMENT

Naloxone is a pure competitive antagonist at all opioid receptors
Naloxone fully reverses all the effects of opioids,
Naloxone antagonizes opioid-induced seizures, except those induced by meperidine and tramadol
MANAGEMENT
ROUTE OF ADMINISTRATION
IV, SC, or IM or deposited on mucosa (intratracheally or intranasally, but not SL)
onset of action after IV administration : 1 to 2 minutes
duration of action: 20 to 90 minutes.
Intranasal administered naloxone can used by EMS personnel and in bystander naloxone administration programs

Naloxone effects are largely dependent on the
dose administered and the amount of opioid
that needs to be reversed.
ROUTE OF ADMINISTRATION
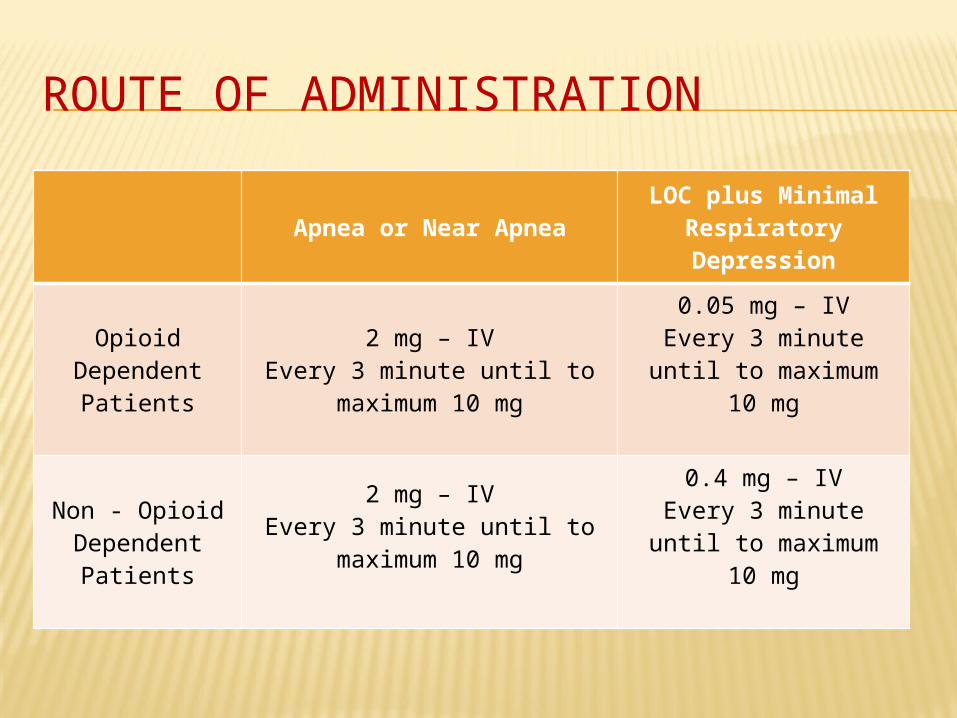
Apnea or Near ApneaLOC plus Minimal
Respiratory Depression
Opioid Dependent
Patients
2 mg – IVEvery 3 minute until to
maximum 10 mg
0.05 mg – IVEvery 3 minute until to maximum 10 mg
Non - Opioid Dependent
Patients
2 mg – IVEvery 3 minute until to
maximum 10 mg
0.4 mg – IVEvery 3 minute until to maximum 10 mg
ROUTE OF ADMINISTRATION
Recent literature recommends the same dose ranges in pediatric patients.
In neonatal patients naloxone, 0.01 milligram/kg IV, is recommended to treat mental and respiratory depression.
ROUTE OF ADMINISTRATION
Exposures to synthetic opioids, such as propoxyphene, fentanyl, pentazocine, or dextromethorphan, and to sustained-release preparations may require these larger-than-ordinary doses
Toxicity from leaking opioid-containing packets in the intestinal tract (i.e., in "body packers") can be extremely severe, and such patients require large and sustained naloxone doses until the drug-containing packets are expelled or removed.
ROUTE OF ADMINISTRATION

NALOXONE INFUSION
A continuous infusion should be considered only if the patient responded to the naloxone bolus and required repeat administration to support respiration
For long-acting opioids: buprenorphine, methadone, and propoxyphene.
for exposures to sustained-release preparations. Ingestions of dermal patches.
To calculate the naloxone continuous infusion dose, determine the "wakeup dose" and administer two thirds of that dose per hour by IV infusion.
It is recommended that patients maintained on naloxone infusions be admitted to a monitored unit.
NALOXONE INFUSION
NALOXONE ADVERSE EFFECTS
serious complications are rare
Common adverse effects are: anxiety, nausea, vomiting, diarrhea, abdominal cramps, piloerection, yawning
Careful dosing of naloxone can prevent the precipitation of opioid withdrawal symptoms
ENDOTRACHEAL INTUBATION
1) Severe respiratory depression unresponsive or poorly responsive to naloxone
2) In cases in which acute lung injury is suspected.
Rapid-sequence intubation, omitting anesthetic-sedative agents, is the preferred technique
ADVANTAGES
1. protection of the airway.
2. easy access for suctioning.
3. provision of an alternate route of administration for some medications.
4. total airway control.


HYPOGLYCEMIA
Definition:
Plasma Glucose less than 50 mg/dl in adult patients.
Hypoglycemia is defined as a plasma glucose level of <45 mg/dL in any symptomatic patient or <35 mg/dL in an asymptomatic neonate.
DEFINITION
Serum glucose level is affected when there is an imbalance between insulin (hypoglycemic
hormone) and its counterregulatory hormones cortisol, growth hormone, glucagon, and
epinephrine (hyperglycemic hormones)
ETIOLOGY
1. Inadequate intake of food
2. Inaccurate administration of insulin
3. Infection
4. Renal failure
5. Acute coronary syndrome
6. Unusual physical or mental stress
7. Metabolic Disorder
SIGNS & SYMPTOMS
Neuroglycopenic symptoms:
drowsiness, confusion, dizziness, tiredness,
inability to concentrate, and difficulty
speaking. Adrenergic symptoms: tremor, sweating, anxiety, nausea,
palpitations, feelings of warmth, and shivering, tachycardia, tachypnea.
Other symptoms such as hunger, weakness, and blurred vision.

SIGNS & SYMPTOMS IN NEONATES AND INFANTS
Alterations in mental status, coma or seizures.
Nonspecific symptoms: poor feeding, an abnormal or high-pitched cry, cyanosis, and hypothermia and varying degrees of irritability and jitteriness or lethargy.
symptoms of vomiting, diarrhea, abnormal urine output, jaundice, and temperature instability.

SIGNS & SYMPTOMS IN NEONATES AND INFANTS
Neonates and infants may not manifest these
signs, and lethargy, apnea, or seizures may be the prominent finding

DIAGNOSIS
rapid bedside screen for serum glucose level is the most important diagnostic test.
Confirm abnormal results with a venous sample sent to the laboratory.
A gray-topped sample tube should be filled and placed on ice for additional studies
TREATMENT
Treat hypoglycemia promptly while awaiting diagnostic results.
IV dextrose is the primary treatment (PO, NGT,PR, IV or IO).
The dose of dextrose is 0.5 to 1.0 gram/kg regardless of the route of administration.
TREATMENT
In alert patients with mild symptoms, oral consumption of sugar containing foods or beverages is often adequate.
In other patients, after blood is drawn for glucose determination, one to three ampules of 50% dextrose in water (D W) is administered intravenously while The patient’s airway, breathing, and circulation are assessed and maintained
DOSE OF DEXTROSE
Newborns: 5 mL/kg of 10% dextrose
infants and children : 2 mL/kg of 25% dextrose
Adult: 0.5 to 1.0 gram/kg of 50% dextrose
repeated if hypoglycemia persists after 15 minutes.
Glucagon, 0.3 milligram/kg IM or SQ (1 mg has an effect similar to that of one ampule of DW)
Maintenance dextrose at a rate of 6 to 8 milligrams/kg/min with D10
TREATMENT
Refractory hypoglycemia: more than 6 to 8
mg/kg/min
Frequent reevaluation and titration of infused dextrose is necessary in this situation.
TREATMENT
Administration of an ampule of DW 50% may range from less than 40 mg/dL to more than 350 mg/dL.
All patients with severe hypoglycemic reactions require aspiration and seizure precautions.

ADRENAL INSUFFICIENCY
hydrocortisone: • 25 grams IV or IM for neonates and infants
• 50 grams for toddlers and school-aged children
• 100 grams for adolescents

Thanks
For Your
Attentio
n
Related Documents











