PAIN Managing Pain Dr TAREK NASRALLAH RHEUMATOLOGY AL AZHAR

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

PAINManaging Pain
Dr TAREK NASRALLAH
RHEUMATOLOGY
AL AZHAR
What is Pain?
• “An unpleasant sensory & emotional experience associated with actual or potential tissue damage, or described in terms of such damage” –
The International Association for the Study of Pain
• Subjective sensation• Pain Perceptions – based on expectations, past
experience, anxiety, suggestions– Affective – one’s emotional factors that can
affect pain experience– Behavioral – how one expresses or controls
pain– Cognitive – one’s beliefs (attitudes) about pain

What is Pain
• Physiological response produced by activation of specific types of nerve fibers
• Experienced because of nociceptors being sensitive to extreme mechanical, thermal, & chemical energy.
• Composed of a variety of discomforts • One of the body’s defense mechanism
(warns the brain that tissues may be in jeopardy)
• Acute vs. Chronic – – The total person must be considered. It
may be worse at night when the person is alone. They are more aware of the pain because of no external diversions.
Where Does Pain Come From?
• Cutaneous Pain – sharp, bright, burning; can have a fast or slow onset
• Deep Somatic Pain – stems from tendons, muscles, joints, periosteum, & b. vessels
• Visceral Pain – originates from internal organs; diffused @ 1st & later may be localized (i.e. appendicitis)
• Psychogenic Pain – individual feels pain but cause is emotional rather than physical

Pain Sources• Fast vs. Slow Pain –
– Fast – localized; carried through A-delta axons in skin
– Slow – aching, throbbing, burning; carried by C fibers
– Nociceptive neuron transmits pain information to spinal cord via unmyelinated C fibers & myelinated A-delta fibers.• The smaller C fibers carry impulses : rate 0.5
to 2.0 m/sec.• The larger A-delta fibers carry impulses : of 5
to 30 m/sec.

Acute pain: lasts less than 6 months, subsides
once the healing process is accomplished.
• Chronic pain:
• Complex processes & pathology. Usually altered anatomy & neural pathways.
• Constant & prolonged, > 6 months,
sometimes for life.
• “Lasting longer than expected time frame”

Altered Neuronal StructureChronic pain accompanied by
cortical reorganization Chronic back pain is accompanied
by brain atrophy

Most Common Chronic Pain Syndromes
• Low Back• Headaches• Neck• Facial• Arthritides• Fibromyalgia• Cancer
What is Referred Pain?• Occurs away from pain site
• Examples: McBurney’s point
• Types of referred pain:– Myofascial Pain – trigger points, small
hyperirritable areas within a m. in which n. impulses bombard CNS & are expressed at referred pain
– Sclerotomic & Dermatomic Pain – deep pain; may originate from sclerotomic, myotomic, or dermatomic n. irritation/injury• Sclerotome: area of bone/fascia that is supplied by
a single n. root• Myotome: m. supplied by a single n. rootDermatome: area of skin supplied by a single n. root

Terminology• Noxious – harmful, injurious
– Noxious stimuli – stimuli that activate nociceptors (pressure, cold/heat extremes, chemicals)
• Nociceptor – nerve receptors that transmits pain impulses
• Pain Threshold – level of noxious stimulus required to alert an individual of a potential threat to tissue
• Pain Tolerance – amount of pain a person is willing or able to tolerate
• Accommodation phenomenon – adaptation by the sensory receptors to various stimuli over an extended period of time (e.g. superficial hot & cold agents). Less sensitive to stimuli.
• Hyperesthesia – abnormal acuteness of sensitivity to touch, pain, or other sensory stimuli
• Paresthesia – abnormal sensation, such as burning, pricking, tingling
• Inhibition – depression or arrest of a function– Inhibitor – an agent that
restrains/retards physiologic, chemical, or enzymatic action
• Analgesic – a neurologic or pharmacologic state in which painful stimuli are no longer painful

• Dysesthesia – An unpleasant abnormal sensation, whether spontaneous or evoked.
• Allodynia – Pain due to a stimulus which does not normally provoke pain, such as pain caused by light touch to the skin
• Hyperalgesia – An increased response to a stimulus which is normally painful
• Hyperesthesia - Increased sensitivity to stimulation, excluding the special senses. Hyperesthesia includes both allodynia and hyperalgesia, but the more specific terms should be used wherever they are applicable.

Nerve Endings• “A nerve ending is the termination of a nerve
fiber in a peripheral structure.” (Prentice, p. 37)
• Nerve endings may be sensory (receptor) or motor (effector).
• Nerve endings may be: – Respond to phasic activity - produce an impulse
when the stimulus is or , but not during sustained stimulus; adapt to a constant stimulus (Meissner’s corpuscles & Pacinian corpuscles)
– Respond to tonic receptors produce impulses as long as the stimulus is present. (muscle spindles, free n. endings, Krause’s end bulbs)
– Superficial – Merkel’s corpuscles/disks, Meissner’s corpuscles
– Deep – Pacinian corpuscles,

Nerve Endings• Merkel’s
corpuscles/disks - – Sensitive to touch &
vibration– Slow adapting– Superficial location – Most sensitive
• Meissner’s corpuscles – – Sensitive to light touch &
vibrations– Rapid adapting– Superficial location
• Pacinian corpuscles -– Sensitive to deep pressure
& vibrations– Rapid adapting– Deep subcutaneous tissue
location
• Krause’s end bulbs – – Thermoreceptor
• Ruffini corpuscles/endings– Thermoreceptor– Sensitive to touch &
tension– Slow adapting
• Free nerve endings -– Afferent – Detects pain, touch,
temperature, mechanical stimuli

Types of Nerves
• Afferent (Ascending) – transmit impulses from the periphery to the brain– First Order neuron– Second Order neuron– Third Order neuron
• Efferent (Descending) – transmit impulses from the brain to the periphery

Peripheral and Central Pathways for Pain
Ascending TractsAscending Tracts Descending TractsDescending Tracts
Cortex
Midbrain
Medulla
Spinal Cord
Thalamus
Pons
First Order Neurons• Stimulated by sensory receptors• End in the dorsal horn of the spinal cord• Types
– A-alpha – non-pain impulses– A-beta – non-pain impulses
• Large, myelinated• Low threshold mechanoreceptor; respond to light touch &
low-intensity mechanical info– A-delta – pain impulses due to mechanical pressure
• Large diameter, thinly myelinated• Short duration, sharp, fast, bright, localized sensation
(prickling, stinging, burning)– C – pain impulses due to chemicals or mechanical
• Small diameter, unmyelinated• Delayed onset, diffuse nagging sensation (aching,
throbbing)
Second Order Neurons• Receive impulses from the FON in the dorsal horn
– Lamina II, Substantia Gelatinosa (SG) - determines the input sent to T cells from peripheral nerve• T Cells (transmission cells): transmission cell that connects
sensory n. to CNS; neurons that organize stimulus input & transmit stimulus to the brain
– Travel along the spinothalmic tract – Pass through Reticular Formation
• Types– Wide range specific
• Receive impulses from A-beta, A-delta, & C
– Nociceptive specific• Receive impulses from A-delta & C
• Ends in thalamus

Third Order Neurons• Begins in thalamus• Ends in specific brain centers
(cerebral cortex)– Perceive location, quality,
intensity– Allows to feel pain, integrate past
experiences & emotions and determine reaction to stimulus
Descending Neurons• Descending Pain Modulation (Descending Pain
Control Mechanism)• Transmit impulses from the brain (corticospinal
tract in the cortex) to the spinal cord (lamina)– Periaquaductal Gray Area (PGA) – release
enkephalins– Nucleus Raphe Magnus (NRM) – release serotonin– The release of these neurotransmitters inhibit
ascending neurons• Stimulation of the PGA in the midbrain & NRM
in the pons & medulla causes analgesia.• Endogenous opioid peptides - endorphins &
enkephalins

Pain Process
The neural mechanisms by which pain is perceived involves a process that has four major steps:
–Transduction
–Transmission
–Modulation
–Perception


Facilitating Transduction
• Biochemical mediators: “Chemical Soup”
ProstaglandinsBradykininsSerotonin
HistaminesCytokines
LeukotrienesSubstance P
Norepinephrine

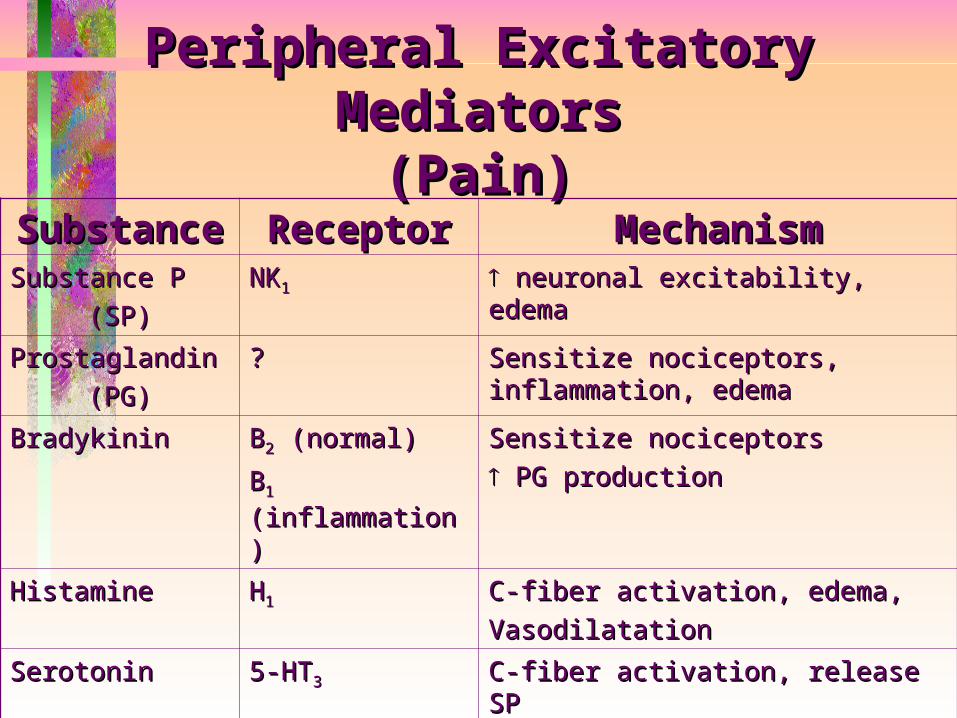
Peripheral Excitatory MediatorsPeripheral Excitatory Mediators(Pain)(Pain)
SubstancSubstancee
ReceptorReceptor MechanismMechanism
Substance PSubstance P
(SP)(SP)NKNK11 neuronal excitability, edemaneuronal excitability, edema
ProstaglandinProstaglandin
(PG)(PG)?? Sensitize nociceptors, Sensitize nociceptors,
inflammation, edemainflammation, edema
BradykininBradykinin BB22 (normal) (normal)
BB11 (inflammation)(inflammation)
Sensitize nociceptorsSensitize nociceptors
PG productionPG production
HistamineHistamine HH11 C-fiber activation, edema,C-fiber activation, edema,
VasodilatationVasodilatation
SerotoninSerotonin 5-HT5-HT33 C-fiber activation, release SPC-fiber activation, release SP
NorepinephrineNorepinephrine
(NE)(NE)11 Sensitize nociceptorsSensitize nociceptors
Activate nociceptorsActivate nociceptors

• NSAIDs ( local & systemic )• Antihistaminic drugs

Acetaminophen (paramol)
• Analgesic, antipyretic
• Inhibits prostaglandin synthetase in the CNS, weak peripheral anti-inflammatory activity
• Serotonergic effect at descending pathway
• Used to treat osteoarthritis

Acetaminophen (Tylenol)
• American Pain Society: Maximum dose 4,000 mg/day,
• American Liver Foundation: 3,000 mg/day
• Risk of hepatotoxicity with higher doses
• Antidote – acetylcysteine (Mucomyst, Acetadote)
Major Categories of Pain
Classified by inferred pathophysiology:
1. Nociceptive pain (stimuli from somatic and visceral structures)
2. Neuropathic pain (stimuli abnormally processed by the nervous system)
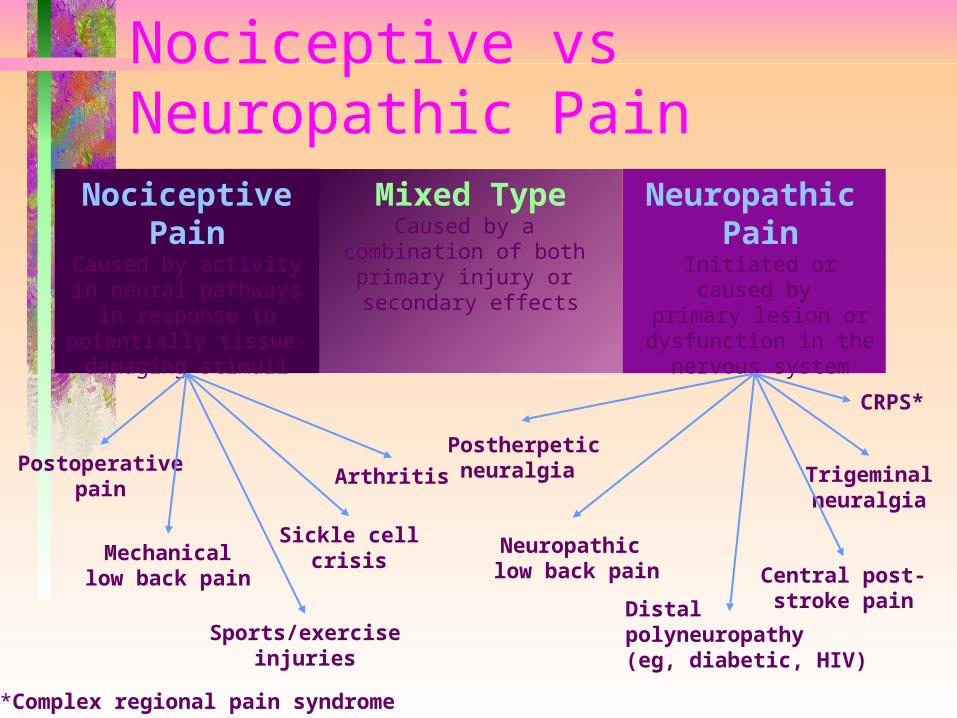
Mixed TypeCaused by a
combination of both primary injury or secondary effects
Nociceptive vs Neuropathic Pain
NociceptivePain
Caused by activity in neural pathways in
response to potentially tissue-damaging stimuli
Neuropathic Pain
Initiated or caused by primary lesion or dysfunction in the nervous system
Postoperativepain
Mechanicallow back pain
Sickle cellcrisis
Arthritis
Postherpeticneuralgia
Neuropathic low back pain
CRPS*
Sports/exerciseinjuries
*Complex regional pain syndrome
Central post-stroke pain
Trigeminalneuralgia
Distalpolyneuropathy (eg, diabetic, HIV)
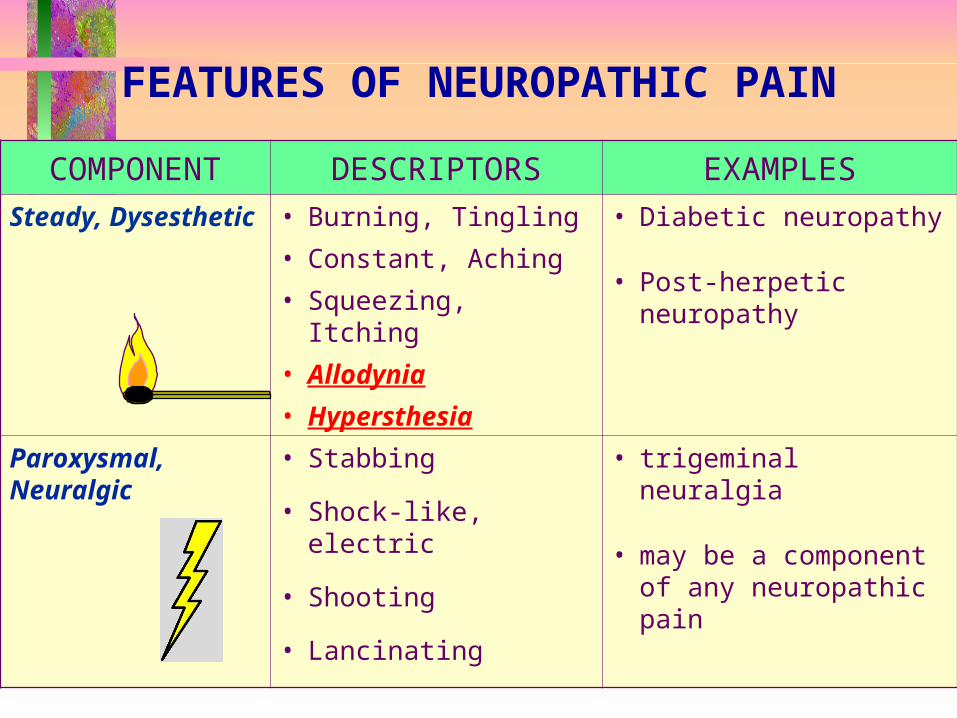
COMPONENT DESCRIPTORS EXAMPLESSteady, Dysesthetic
• Burning, Tingling
• Constant, Aching
• Squeezing, Itching
• Allodynia
• Hypersthesia
• Diabetic neuropathy
• Post-herpetic neuropathy
Paroxysmal, Neuralgic
• Stabbing
• Shock-like, electric
• Shooting
• Lancinating
• trigeminal neuralgia
• may be a component of any neuropathic pain
FEATURES OF NEUROPATHIC PAIN
Local Anesthetic Agents
•Patch (topical)•Eml gel: Lidocaine (topical)•Oint. 4% lidocaine (topical)

Local Anesthetics
Blocks conduction of nerve impulses by decreasing or preventing an increase in the permeability of excitable membranes to Na+.
Inhibits depolarization of nerve
Blocks neuronal firing
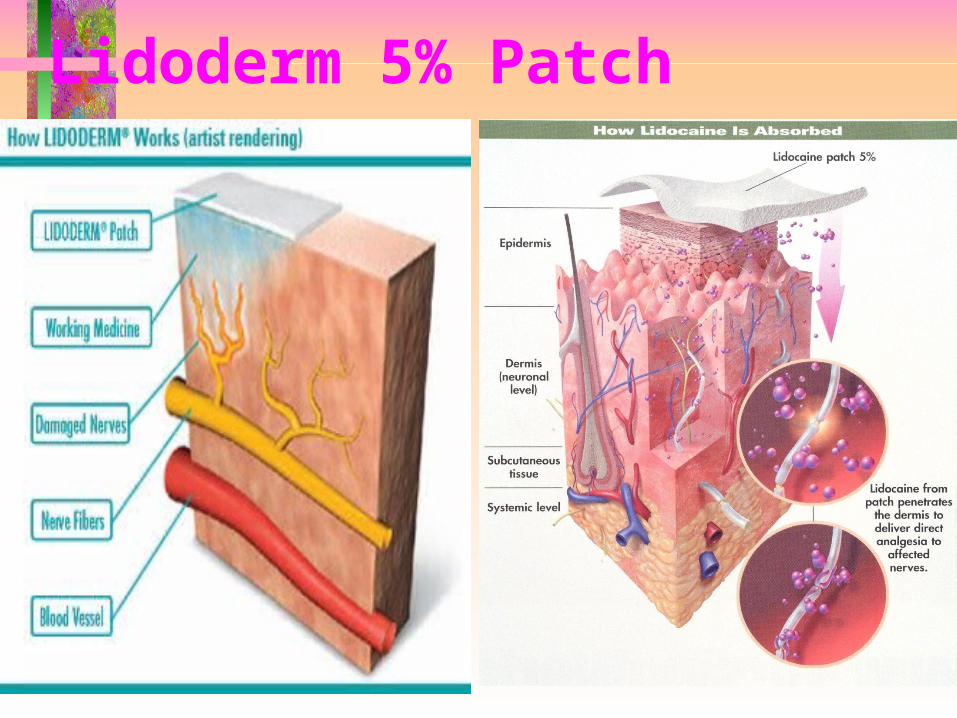
Lidoderm 5% Patch



Mentholatum
Menthol generates analgesic
activity through:• Ca2+ channel blocking
activity• Binding to kappa opioid
receptors
Methyl Salicylate Toxicity
• Salicylic acid derivative
• Lipid solubility increases toxicity
–More toxic than aspirin
–1 teaspoon (5ml) wintergreen oil contains 4,000 mg salicylate
–30ml wintergreen oil is a fatal dose in adults
• Risk of toxicity reduced with use for acute pain, limited to a small area of dermal application

Anticonvulsants
1)Inhibit sustained high-frequency neuronal firing by blocking Na+ channels after an action potential, reducing excitability in sensitized C-nociceptors.
2)Blockade of Na+ channels and increase in synthesis and activity of GABA, in inhibitory neurotransmitter, in the brain.
3)Modulates Ca+ channel current and increases synthesis of GABA.

Antiepileptic Agents• Broad clinical
actions in the CNS:– Reduce seizures– Neuropathic pain– Bipolar disorder– Anxiety– Schizophrenia– Agitation
• Impulse dyscontrol
• Dementia• Delirium
• Three proposed mechanisms of action:
– Blockade of voltage gated sodium channels ( glutamate release)
– Blockade of voltage gated calcium channels – alpha 2 delta subunits (reduces excessive neurotransmitter release)
– Enhancement of GABA actions

Lyrica PregabalinSchedule V

Transmission of pain
Defined as: Projection of pain into the
Central Nervous System

Transmission
A synapse contains three elements:
the presynaptic terminal
the synaptic cleft
the receptive membrane


Transmission
• The presynaptic terminal is the axon terminal of the presynaptic neuron
• Here that the presynaptic neuron releases neurotransmitters which are found in vesicles



Neurotransmitters
Chemical substances that allow nerve impulses to move from one neuron to another Found in synapses– Substance P - thought to be responsible for the
transmission of pain-producing impulses– Acetylcholine – responsible for transmitting motor
nerve impulses– Enkephalins – reduces pain perception by bonding
to pain receptor sites– Norepinephrine – causes vasoconstriction– Endorphins - morphine-like neurohormone; thought
to pain threshold by binding to receptor sites – Serotonin - substance that causes local
vasodilation & permeability of capillaries

Capsaicin• Hot peppers• May deplete & prevent
re-accumulation of substance P in primary afferent neurons responsible for transmitting painful impulses from peripheral sites to the CNS.
• Absorption, distribution, metabolism & excretion, half life – unknown
• May produce transient burning with application, usually disappears in 2-4 days, but may persist for several weeks.

Transmission• The synaptic cleft is the narrow
intercellular space between neurons. • Neurotransmitters cross the synaptic
cleft and bind to specific receptors on the postsynaptic neurons
• This will excite or inhibit the postsynaptic neurons.


Questions to Ask about Pain
• P-Q-R-S-T format• Provocation – How the injury occurred & what
activities the pain• Quality - characteristics of pain – Aching
(impingement), Burning (n. irritation), Sharp (acute injury), Radiating within dermatome (pressure on n.)?
• Referral/Radiation – – Referred – site distant to damaged tissue that
does not follow the course of a peripheral n.– Radiating – follows peripheral n.; diffuse
• Severity – How bad is it? Pain scale• Timing – When does it occur? p.m., a.m., before,
during, after activity, all the time
Pattern: onset & durationArea: locationIntensity: levelNature: description
Pain Assessment Scales
• McGill pain questionnaire– Evaluate sensory,
evaluative, & affective components of pain
– 20 subcategories, 78 words

Assessment of Pain Intensity
No Mild Moderate Severe Very Worstpain pain pain pain severe possible
pain pain
Verbal Pain Intensity Scale
No
pain
Visual Analog Scale
Faces Scale
0 1 2 3 4 5
0–10 Numeric Pain Intensity Scale
No Moderate Worstpain pain possible pain
0 1 2 3 4 5 6 7 8 9 10
Worstpossible
pain
21

Smiling Faces
Patients seldom remember how good a clinician your are. But they do remember how much they hurt when you were treating them.

• Questions
Related Documents











