Dr. Steve Hinder Consultant Psychiatrist April 23rd 2008

Dr. Steve Hinder Consultant Psychiatrist April 23rd 2008.
Dec 17, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Dr. Steve Hinder
Consultant Psychiatrist
April 23rd 2008
Sulphate and Autism
10 years ago, very few biological markers
↑ platelet serotonin in 30%
Proxy for reduced serotonin brain function
Borne out by success of SSRI’s and Risperidone
Rosemary Waring found low sulphate as a marker in autistic children
Pursued links with Allergy Induced Autism group, finding migraine in mothers
Foods that worsen behaviour contain PHENOLS
Phenols are metabolized by Sulphation, catalyzed by Sulphotransferase enzyme (PST)
PST is low in migraine

RESULTS INAUTISTIC CHILDREN
Very low Sulphate levels (10% of normal)
High Cysteine levels PST very low in individuals with food reactions
PST normal in other children
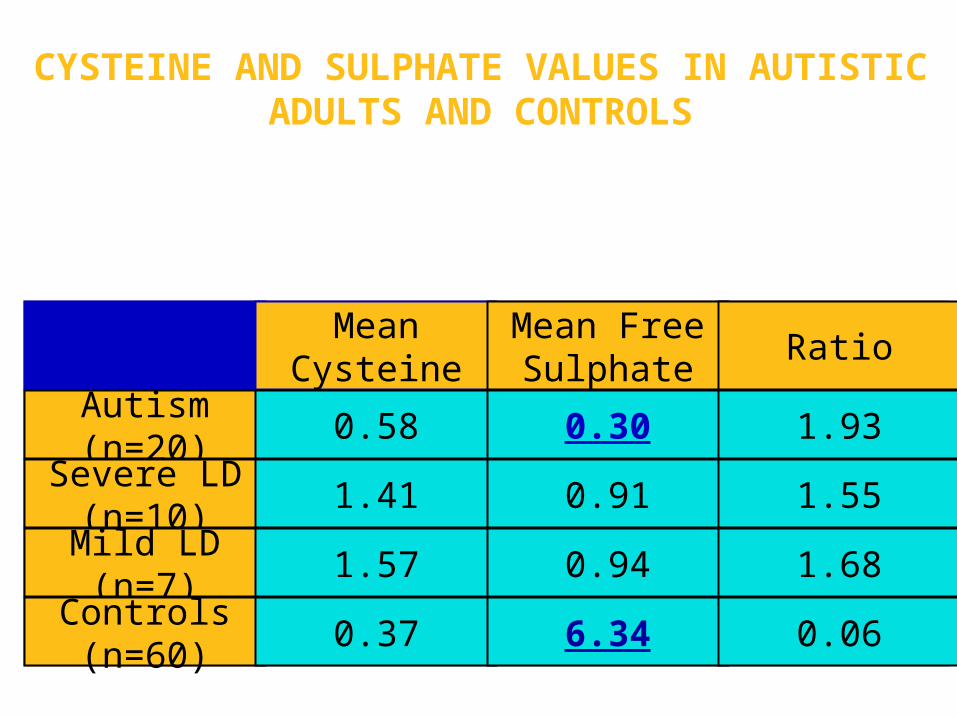
CYSTEINE AND SULPHATE VALUES IN AUTISTIC ADULTS AND CONTROLS
Mean
CysteineMean FreeSulphate
Ratio
Autism(n=20)
0.58 0.30 1.93Severe LD
(n=10)1.41 0.91 1.55
Mild LD(n=7)
1.57 0.94 1.68Controls(n=60)
0.37 6.34 0.06
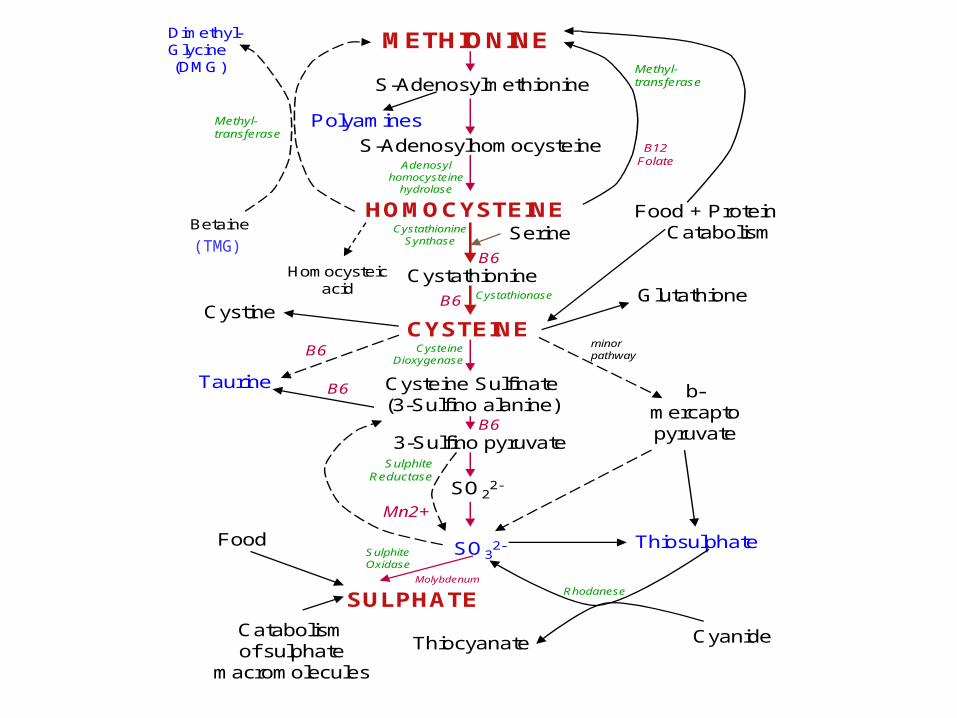
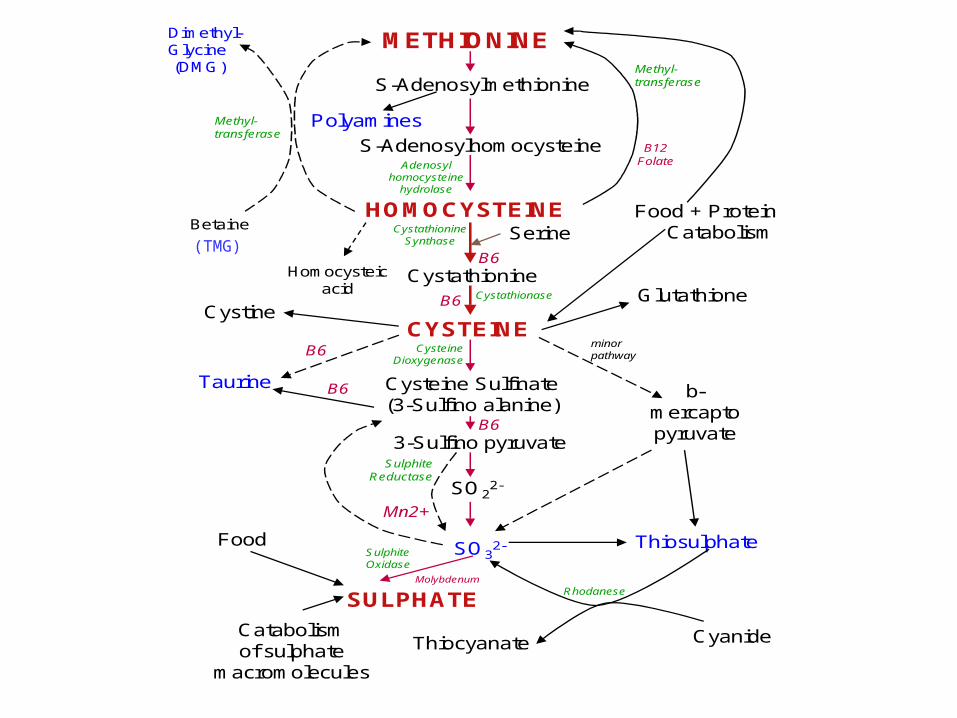
METHIONINE
S-Adenosylmethionine
S-Adenosylhomocysteine
HOMOCYSTEINE
Cystathionine
Serine
CYSTEINE
Cysteine Sulfinate(3-Sulfino alanine)
3-Sulfino pyruvate
SO22-
SO32-
SULPHATE
Food + Protein Catabolism
Cystine
Taurine b-mercaptopyruvate
ThiosulphateFood
Catabolismof sulphate
macromolecules
Thiocyanate Cyanide
minorpathway
Rhodanese
CysteineDioxygenase
SulphiteOxidase
Glutathione
Adenosylhomocysteine
hydrolase
Cystathionase
CystathionineSynthase
B6
B6
B6
B6
B6
Molybdenum
SulphiteReductase
Mn2+
B12Folate
Methyl-transferase
Betaine
Dimethyl-Glycine (DMG)
Methyl-transferase
Polyamines
Homocysteicacid
(TMG)
Gaining New Knowledge
Autism Research Unit
Durham conferences
Allergy Induced Autism
Hyperactive Childrens Support Group
Informal networking
Andrew Wakefield
Developmental histories
Taking parents more seriously
Dietary history
Immunity
Vaccines
Eventually brave enough to give advice !
People Practice
OPIATE EXCESS THEORY OF AUTISM
Reduced crying when isolated Decreased pain sensitivity Insistence on sameness Increased stereotypical behaviour Fearlessness Abnormal social play Unusual body postures Changes in eating patterns Increase in seizures Social withdrawal Hyperactivity Lack of response to sensory stimuli
All signs ofopiate addiction
or withdrawal
EXOGENOUS OPIOIDS
Intact peptides can cross mucosa (Gardner, 1983)
Gluten and Casomorphin fragments have opioid activity
Peptide peaks in urine of autistic patients have opioid activity (Shattock, Reichelt)
Abnormal intestinal permeability in autism (D'Eufemia et al, 1996)
Effect of gluten and casein-free diets?

CAUSES OF LEAKY GUTSTrauma CytokinesImmunodeficiency/AllergyGut flora imbalance or CandidaAnkylosing Spondylitis or ArthritisLow GlycosaminoglycansMeasles/MMR ?? Learning disability?

GLYCOSAMINOGLYCANS (GAG's) + CANDIDA
GAG's required for gut wall integrity Normally sulphated - produces negative
charge Lack of sulphate interrupts normal
production Candida no longer repelled Candida very common in autism Known to deplete sulphate Positive feedback ?
Recent Trends
- Increased incidence, was 1 in 2000 now 1 in 100- majority feel due to better diagnosis and wider definitions, but significant minority feel genuinely increasing- “Active but odd” group now more prominent ?- Less LD than you would expect (20% rather than 80%)- Children with autism seem to be making extraordinary progress

If autism is increasing, what might the cause be ?
- “Leaky Gut syndrome”- MMR/other vaccines- Overuse of antibiotics Candida or clostridium- Pesticides or organophosphates- Food additives (Eg. MSG, Aspartame)- Lowered immunity/increased autoimmune disease - Mercury toxicity- Unusual viruses or other infections- Opiate use during delivery- Chemicals in environment
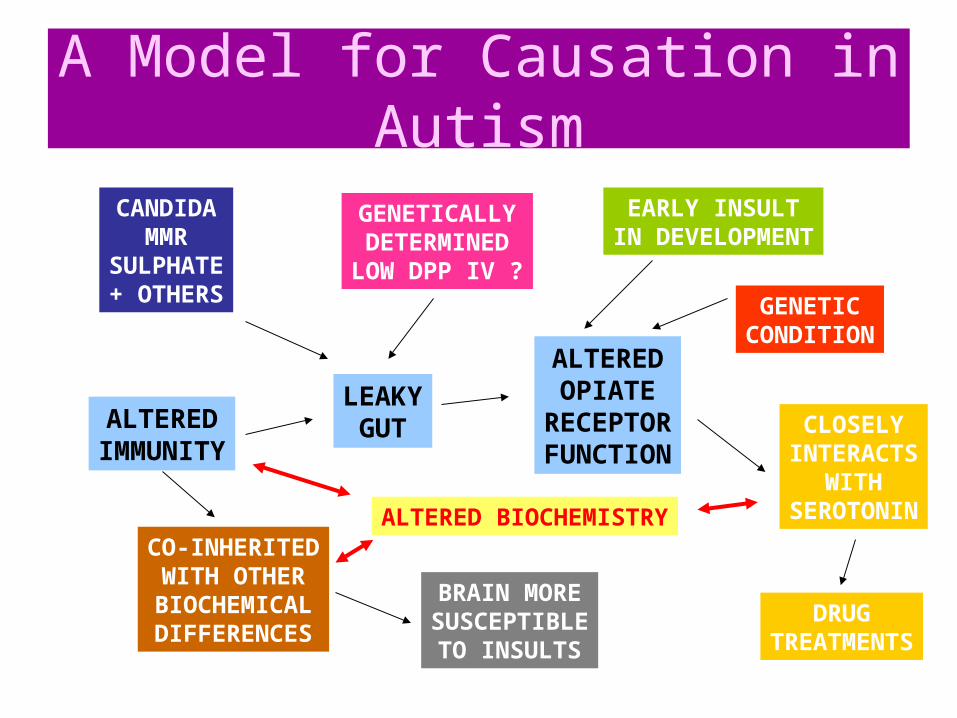
A Model for Causation in Autism
LEAKYGUT
ALTEREDOPIATE
RECEPTORFUNCTION
EARLY INSULTIN DEVELOPMENT
GENETICCONDITION
CLOSELYINTERACTS
WITHSEROTONIN
GENETICALLYDETERMINEDLOW DPP IV ?
CANDIDAMMR
SULPHATE+ OTHERS
ALTEREDIMMUNITY
CO-INHERITEDWITH OTHER
BIOCHEMICALDIFFERENCES
BRAIN MORESUSCEPTIBLETO INSULTS
DRUGTREATMENTS
ALTERED BIOCHEMISTRY
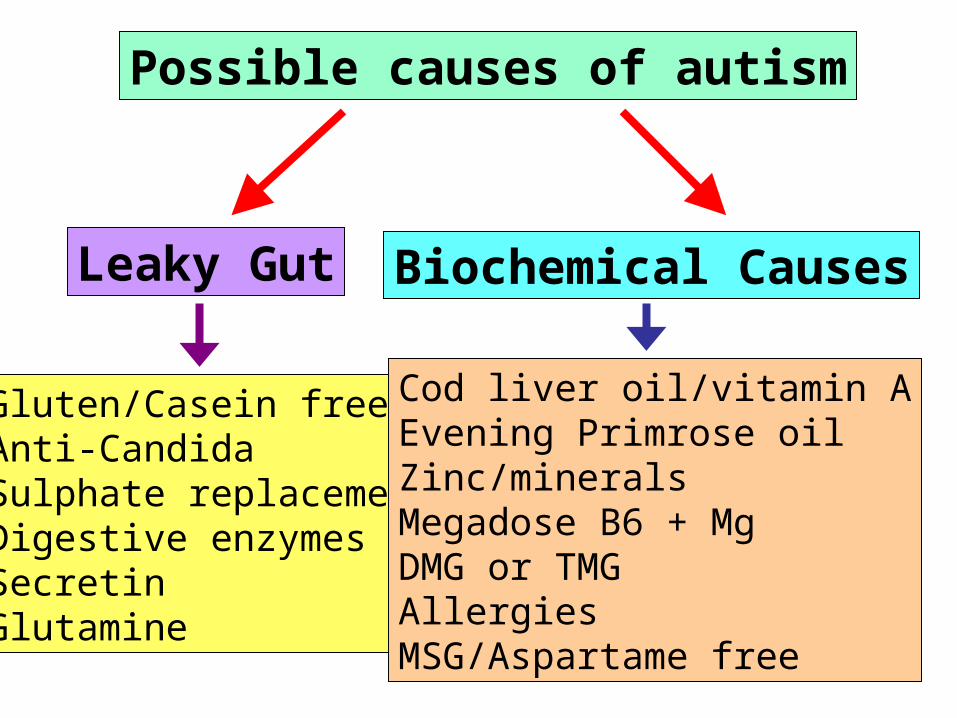
Possible causes of autism
Leaky Gut Biochemical Causes
Gluten/Casein freeAnti-CandidaSulphate replacementDigestive enzymesSecretinGlutamine
Cod liver oil/vitamin AEvening Primrose oilZinc/mineralsMegadose B6 + MgDMG or TMGAllergiesMSG/Aspartame free
Gluten/Casein-free Combination of both works best May be easiest to start with casein, but often not enough Persevere with casein for at least 2 months ? Persevere with gluten for at least 6 months ? May get “cold turkey”, esp. with casein Constipation/MMR history suggests gluten May previously have craved these substances, or avoided Sunderland urine test can be non-specific May work better in younger children May be less effective if clear genetic cause Improvement in 40% on combined diet ? NEED TOTAL ELIMINATION (in most, but not all) Re-exposure can cause severe behaviours
Sulphate
• No blood test available• May be low in 90% of children• Causes diarrhoea if taken orally• Can try slowly increasing epsom
salt baths• Glucosamine sulphate• Cranberry juice• Cut out citrus fruit, apples,
vinegar, tomatoes• Avoid paracetamol• Overlap with Feingold diet for
hyperactivityEpsomSalts
Treating Candida
• Suggested by early antibiotic use• Difficult to test (we all have it)• NYSTATIN oral drops• Low sugar• Capryllic acid + other natural products• Probiotics (acidophilus, Lactobacillus, Bifidus)• Possibly low yeast diet• Can get massive die-off reaction
Essential fatty acids
• Cod liver oil, may be vitamin A, omega 3• Evening Primrose oil, omega 6 (GLA)• Flaxseed (Linseed) oil• Zinc may aid absorption• Good for hyperactivity/concentration• May improve eye contact• Caution with EPO in epilepsy
Other supplements
• Good evidence for high dose B6, Magnesium• May tie in with sulphate pathways• DMG/TMG may have additive effect
METHIONINE
S-Adenosylmethionine
S-Adenosylhomocysteine
HOMOCYSTEINE
Cystathionine
Serine
CYSTEINE
Cysteine Sulfinate(3-Sulfino alanine)
3-Sulfino pyruvate
SO22-
SO32-
SULPHATE
Food + Protein Catabolism
Cystine
Taurine b-mercaptopyruvate
ThiosulphateFood
Catabolismof sulphate
macromolecules
Thiocyanate Cyanide
minorpathway
Rhodanese
CysteineDioxygenase
SulphiteOxidase
Glutathione
Adenosylhomocysteine
hydrolase
Cystathionase
CystathionineSynthase
B6
B6
B6
B6
B6
Molybdenum
SulphiteReductase
Mn2+
B12Folate
Methyl-transferase
Betaine
Dimethyl-Glycine (DMG)
Methyl-transferase
Polyamines
Homocysteicacid
(TMG)
Other supplements
• Good evidence for high dose B6, Magnesium• May tie in with sulphate pathways• DMG/TMG may have additive effect• Can all improve core social symptoms• Digestive enzymes promising (CCK connection,
DPP IV)• Secretin not yet safe• Other vitamins/minerals may help• Glutamine can heal leaky gut?• Monosodium glutamate/Aspartame important• MANY OTHER THINGS BEING TRIED (Methyl B12,
Glutathione)
Things to consider
• Early treatment probably best• Interventions can also help ADHD/LD• Is mercury important?• Are UK and USA children different? – cysteine
levels seem paradoxical• DAN protocol – Is it humanly possible?• Dilemma re single versus many treatments, as
may be synergistic• Do not take lightly (do have biological action),
but give dietary interventions a try• Therapeutic alliance with parents

Related Documents











