Dr Sherif Tawfeek Consultant Gynaecologist Christchurch Gynaecology Associates Christchurch 8:30 - 9:25 WS #142: Interpreting Gynae Ultrasounds 9:35 - 10:30 WS #152: Interpreting Gynae Ultrasounds (Repeated) Dr Rachel Belsham Consultant Radiologist Christchurch Women's Hospital Christchurch

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Dr Sherif TawfeekConsultant Gynaecologist
Christchurch Gynaecology Associates
Christchurch
8:30 - 9:25 WS #142: Interpreting Gynae Ultrasounds
9:35 - 10:30 WS #152: Interpreting Gynae Ultrasounds (Repeated)
Dr Rachel BelshamConsultant Radiologist
Christchurch Women's Hospital
Christchurch

Interpreting Gynaecology Ultrasounds
Rachel BelshamFRANZCR
Women’s Radiologist, Christchurch Hospital
Sherif TawfeekFRANZCOG, FRCOG, FICS, MSc, Dip-Endoscopy
Consultant in Obstetrics and GynaecologySenior lecturer at University of Otago

Objective
• 4 x Cases with different diagnosis• Sharing the common Gynae presenting complaints
and examination findings Sudden onset of abdominal pain +/- PV bleedingNausea, +/-vomitingO/E: Abdo tenderness, mild guarding but no rebound
• Radiology report complement a tentative diagnosisby giving a degree of certainty

Case 130yr, G4P2+1Abdominal pain, with PV spottingNausea, but no vomitingInitial USS ? Molar pregnancyERPOC 12th July -histology: Decidua onlyRepeat β-HCG:
Follow up scan:
2nd July 8th July 15th July
1670 2660 2490

Image Findings:
- “empty uterus” + pseudo-sac
- Right adnexal mass
- complex free fluid
DIAGNOSIS = ruptured RIGHT tubal ectopic
Empty Uterus + pseudo-sac Right adnexal mass
Complex free fluid

ECTOPIC PREGNANCY
Diagnosis becoming more complicated
- atypical symptoms >50%
- rare types ectopic increasing (IVF, LSCS)
Cornual
Ovarian
Abdominal
Cervical
**Scar
Heterotopic
Intramural
Chronic

Ovarian Ectopic
Cornual Ectopic
Heterotopic Scar Ectopic
Abdominal Ectopic

ECTOPIC PREGNANCY
Differential Diagnosis:
1. Exo-phytic corpus luteum of pregnancy
2. Pedunculated fibroid
3. PUL – pregnancy of unknown location

CORPUS LUTEUM Usually within ovary
Can be on margin “Exophytic”
>>> Can be mistaken for tubal ectopic
>>> Corpus luteum can rupture
Solution: clips with probe pressure ….. Ectopic separates from ovary
Normal CL within ovary Exophytic CL Tubal Ectopic
Large HaemoperitoneumRuptured CL at surgery

OTHER ADNEXAL MASSES
Fibroids
pedunculated, subserosal
“Claw” sign
Endometrioma
Ovarian Mass
HELPFUL TIP:
? seen on previous scan
Follow-up scan
Right subserosal fibroid + “claw” sign
Endometrioma + adhesions + LOV cyst
E LOVA

PREGNANCY OF UNKNOWN LOCATION
DEFINITION:
- no visible pregnancy within the uterus or elsewhere in the pelvis
PITFALL:
- often mistaken for complete miscarriage!
(History bleeding)
DIFFERENTIAL:
1. Early IUP not yet visible
2. Early ectopic not yet visible (20%)
3. Complete miscarriage
HELPFUL TIP: Follow-up serum BHCG +/- FU scan
PUL
EctopicOn FU scan

ECTOPIC PREGNANCY IMAGING TIPS
Don’t put off an Ultrasound scan
- symptoms often atypical (>50%)!
Include history of IVF, Caesarean on request form
- Rare types ectopic increasing
Serum BHCG very helpful
- any ectopic
- after scan showing Pregnancy of Unknown Location

MISCARRIAGE
Many Types:
- threatened, incomplete, complete, missed
Management:
- conservative, medical (Misoprostol), surgical (ERPOC)
Many Imaging Appearances:
- retained tissue, retained pregnancy structures
- early pregnancy failure

Retained tissue “RPOC”Large empty sac“Blighted ovum” Retained fetus
Incomplete miscarriage …sac has moved down Retained placenta

EARLY PREGNANCY FAILURE
Complicated diagnosis
Previously overcalled (Doubilet et al 2013)
New diagnostic criteria
1. CRL >= 7 mm + no heartbeat
2. No heartbeat present on a FU scan when it was seen on a previous scan
If criteria not met ….
Follow-up scan often recommended by Radiologist!

CRL = 9 mm. No heartbeat.EARLY PREGNANCY FAILURE.
CRL = 3 mm + no heartbeat.DOES NOT MEET CRITERIA. Needs FU scan!
HELPFUL TIPS:
Radiologist will often advise FU scan if criteria not met History is unreliable (sure dates cannot diagnose EPF) Poor prognostic features cannot diagnose EPF
- sub chorionic hg, distorted low sac, bradycardia Serial serum BHCG is helpful (reducing BHCG suggests failure)

Key notes1. At what β-HCG level is TV-USS able to identify intrauterine pregnancy?
1500 IU/L
2. What is recurrence rate of ectopic pregnancy 15-20%
3. What is the management options are available and which management would be preferred in this particular case?
4. What is the risk factors for ectopic pregnancy

Risk factors for ectopic pregnancy
➢ Smoking➢ Previous ectopic➢ History of Infertility / infertility treatment e.g.
IVF➢ Previous tubal surgery➢ Previous ectopic pregnancy➢ Contraception e.g. IUCD / progesterone only pill

Case 2
16yr, P0RIF pain Nausea & vomiting,Tender on right sideBlood=N, CRP <3
USS:

Image Findings:
- enlarged heterogeneous avascular ovary
- dilated thick-walled fallopian tube + internal haemorrhage
- free fluid
DIAGNOSIS: Torsion right ovary and right fallopian tube
Enlarged avascular ovary Fallopian tube with haemorrhage
ROV

OVARIAN TORSION
Classic Torsion: - normal ovaries ( increased mobility ) - pre-pubertal girls, pregnancy- highly sensitive - uncommon
Non-classic Torsion:- abnormal ovaries ( pre-existing cyst/mass )- older women- low sensitivity- common

BEWARE!
Vascularity does not exclude Torsion!
- Dual blood supply
- Varying twisting
- Intermittent/partial Torsion
Classic Torsion – 16 yr Non-classic Torsion – 35 yrOvarian cyst
Classic Torsion 13 weeks pregnant
Torsion – 13 weeks pregnant

OVARIAN TORTION
Differential diagnosis ( RIF pain ) :
Haemorrhagic cyst/follicle
Ovarian dermoid
Appendicitis
Mesenteric adenitis
Crohn’s (terminal ileum)
Renal
No cause seen
LOV haemorrhagic cyst - 13 yr girl
Appendicitis 16 yr

OVARIAN TORTION
IMAGING TIPS:
• Sudden onset severe pain suggestive
• At risk: pre-pubertal girls, pregnancy
pre-existing ovarian lesions
• Pelvic USS first investigation
• Classic >>>>> highly sensitive!
• Most cases Non-classic >>>>> USS cannot confirm Torsion
Final management should be based on clinical grounds.

Question
1. What is the incidence of ovarian torsion? A. 5% B. 10% C. 15%
1. What is the risk factor(s) for ovarian torsion?A. Ovarian cystB. SterilisationC. IVF treatment cycleE. Hysterectomy with conservation of ovaries

Key notes
➢Torsion of the ovary is a common diagnostic challenge in the emergency setting
➢Diagnosis can be difficult and is mainly based on clinical symptoms (non-specific) and imaging (A normal ultrasound scan does not exclude adnexal torsion)
➢Treatment is traditionally surgical removal of the ovary, however, there is increasing evidence for conservative surgery, such as de-torsion and oophoropexy, particularly in younger women.

Key notes
Symptoms of ovarian torsion (non-specific)
General
Pelvic or abdominal pain,
fluctuating, radiating to loin or thigh
Nausea
Vomiting
Signs
GeneralPyrexia
Tachycardia
Abdominal examination Generalised abdominal tenderness, localised guarding, rebound
Vaginal examination Cervical excitation, adnexal tenderness, adnexal mass

Case 333yr, P2 NVDSudden onset of RIFNausea & vomitingSmokerMirena in situO/E: Abdo tenderness, no guarding or rebound
USS:

Image Findings:
- “Lace like” septations
- Echogenic foci
- Complex free fluid (haemorrhage)
DIAGNOSIS: haemorrhagic cyst with rupture
Hg cystFree fluid

Haemorrhagic Ovarian Cyst.
Ovarian Cyst complications:- rupture- haemorrhage- ovarian Torsion
Ultrasound Features:- classic features >>>>> diagnostic
Differential Diagnosis: 1. endometrioma2. dermoid3. abscess4. neoplasia

Classic Ultrasound Features:
- “lace-like” internal architecture
- “asymmetric” internal material
- mobile internal blood products
“Lace-like” architecture Asymmetric materialClot retraction
Mobile layering blood products

Physiological follicleSmall < 30 mm
Dermoid: Fat, fluid, hair, calcification.
Tubo ovarian abscess. Thick walled cyst, dilated tube, fever, WCC
Tooth

ENDOMETRIOSIS
Superficial lesions not visible on imaging >>>>> laparoscopy
Deep Infiltrating Endometriosis:
1. Ultrasound - endometriomas retroverted uterusuterus surface plaques, bowel lesionsureter lesionsorgan mobility (adhesions ) >>>> reduced “sliding”
2. MRI - endometriomas plaques (peritoneum, serosa, POD, Uterosacral ligaments)tethering (adhesions)

Large bilateral endometriomas Rectal wall deposit
“Kissing ovaries” in POD Posterior uterus plaque + rectal tethering

Normal Sliding Uterus

Abnormal Sliding Grade 4 Endometriosis

OVARIAN NEOPLASIAHaemorrhagic cyst Ovarian Neoplasia
Solid nodules, projections Rarely Often present
Thick irregular septations Absent Often present
Internal vascularity Absent Often present
Tumour markers Negative Often high (endos, TOA also high)

HAEMORRHAGIC OVARIAN CYST
IMAGING TIPS:
1. Classic Features are diagnostic
2. Otherwise need to exclude other differentials
3. ? Follow-up ultrasound
- classic dermoid ………… refer to Gynaecology
- likely neoplasia ………… refer to Gynaecology
? Haemorrhagic cyst vs ? Endometrioma ……… Follow up scan in 8 weeks
1. haemorrhagic cyst resolves
2. endometrioma persists/progresses

Risk factors for Ovarian cancer➢Age: most common in women 50 to 60 years.
➢ Inherited gene mutation. BRCA1, BRCA2, Lynch syndrome
➢Family history
➢Obesity
➢Estrogen hormone replacement therapy
➢Age when menstruation started and ended.
➢Nulliparity
➢Fertility treatment

Case 4
32 year old, P0Pelvic painSevere dysmenorrhoeamenorrhagia
USS:

Imaging Findings: Diagnosis:
- central uterus mass Submucosal fibroid
- mild vascularity
- poorly seen endometrium

FIBROIDS “LEIOMYOMA”
Types: submucosal intramural subserosal pedunculated
Complications:Calcificationcystic degenerationprolapse Torsion (pedunculated) renal obstructionmiscarriageunstable lie
FIBROIDS
Differential Diagnosis:
1. Polyp
2. Thickened endometrium : hyperplasia, Tamoxifen, carcinoma
3. Focal adenomyoma
4. Ovarian fibroma (pedunculated)

Huge fibroid uterus 25 cm
Pedunculated fibroid
Fibroids MRI
Fibroids
Fibroids CT
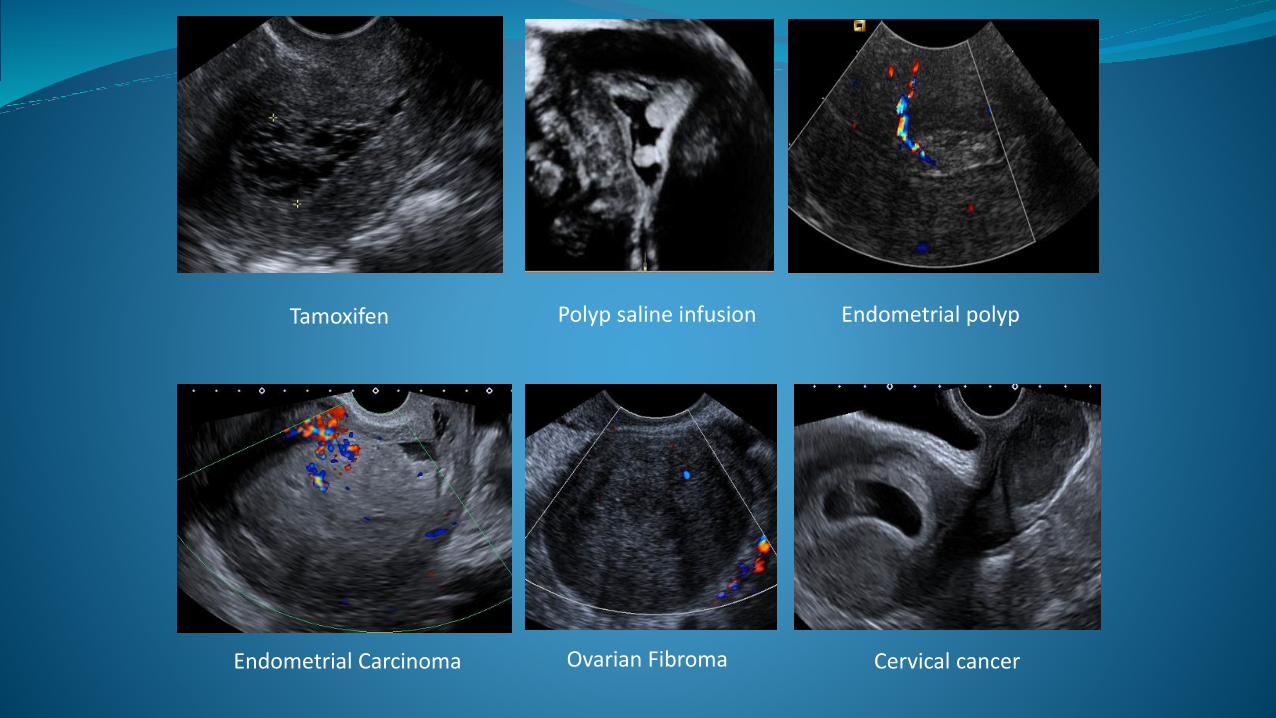
Tamoxifen Endometrial polyp
Ovarian FibromaEndometrial Carcinoma Cervical cancer
Polyp saline infusion

ADENOMYOSIS
Endometrial glands within the myometrium
Diffuse + focal
Bulky uterus, myometrial cysts, “venetian blind”
coarsened heterogeneous myometrium
Sub endometrial cysts Bulky “venetian blind” MRI

FIBROIDS
IMAGING TIPS:
First investigation Pelvic Ultrasound
MRI for pre op planning (myomectomy)
Saline infusion USS ? Polyp ? submucosal fibroid extent into endometrial cavity
Treatment – Mirena, medical, surgical, embolisation
If Treatment not working consider alternative diagnosis
i.e.. Focal adenomyosis
Necrosis post emb

Question
Q. What treatment options are approved for uterine fibroid?
A. Uterine artery embolisationB. Gonadotropin-releasing hormone analogues (Zoladex)D. Hysteroscopic myomectomyE. Laparoscopic myomectomyF. HysterectomyG. Levonorgestrel intrauterine system (Mirena)H. All of the above

Key notes
➢ Fibroids are the most common uterine growth - 20-30%
➢ Management options are affected by the woman's symptoms, age, desire to conceive and local resources.
➢ Pharmacological agents are effective in alleviating symptoms and may improve women’s quality of life.
➢ Interventional radiology procedures may prevent the need for hysterectomy.
➢ Conventional surgical procedures and minimal access surgery are important in management of fibroids.

TEST 1
35 year old woman, positive pregnancy test, vague lower abdominal discomfort and PV bleeding, history of previous miscarriages, she is SURE she has passed products …….
Early Pregnancy USS shows empty uterus and no ectopic
(Pregnancy of Unknown Location).
What do you do?
A tell her it must be a complete miscarriage and discharge her
B perform a FU BHCG just to be sure

TEST 1
A week later BHCG has slightly risen and she says she is still spotting and now feels a bit lightheaded
What is the diagnosis?
A miscarriage
B ruptured left ectopic pregnancy
Empty uterus L adnexal mass and complex free fluid
mass
ff
ff
LOV

TEST 2
30 year woman sure dates 8 weeks,
PV spotting, BHCG 15,000.
Ultrasound CRL = 3 mm (6 weeks) but no heartbeat and small sub chorionic haemorrhage
What do you do?
A tell her she has had a miscarriage and arrange ERPOC
B arrange a follow up USS in 10-14 days +/-
follow up BHCG
CRL 3 mm no FHB small SCH
GSacSCHg

TEST 2
What is the USS diagnosis?
A failed early pregnancy
B single live intrauterine pregnancy
Initial scan at 8 weeks gestation by datesCRL = 3 mm no heartbeat (app 6 week size)
Follow up scan in 10 days CRL = 5 mmWith Heartbeat present = 125 bpm

TEST 3
Which of these COULD be Torsion?
A B C All None
If Ultrasound is indeterminate, but patient has severe pain typical for Torsion what next?
- assume hg cyst give pain relief and send home when settled
- cannot exclude Torsion based on clinical so theatre arranged
A B
C
ROV
Ut
Enlarged ROV with haemorrhage 16 yr
Large ROV Cyst25 yr
Large AvascularLOV 19 yr

TEST 4
Which one is the haemorrhagic cyst?
A or B
If cyst could be an endometrioma but not certain what is recommended further management?
A tell the patient she has cancer
B refer straight to a Gynaecologist
C order a follow up USS in 8 weeks and then review
A B

TEST 5
Which one is the fibroid? A or B
If treatment not working most common alternative diagnosis:
- polyp
- tumour
- adenomyosis/adenomyoma
A B

TEST 6
Spot the abnormality
Related Documents











