Dr. R L Salmon, NPHS CDSC, Temple of Peace and Health, King Edward VII Avenue, Cathays Park, Cardiff, CF10 3AP. Telephone: 029 20402471 Further information on infectious diseases in Wales can be found on our web site at http://nww.nphs.wales.nhs.uk or http://www.nphs.wales.nhs.uk 18 th January 2007 INCIDENCE RATES 4 WEEKLY TRENDS 0 2 4 6 8 10 12 Chicken pox Influenza Measles Mumps Rubella Shingles Whooping cough Pneumonia Ra te per 1 00 ,0 00 popula tion 24-Dec-2006 31-Dec-2006 07-Jan-2007 14-Jan-2007 Influenza season update Influenza activity for Wales increased during week two of 2007. The clinical consultation rate for week two was 5.13 consultations per 100,000; this is still well within baseline levels (below 25 consultations per 100,000 practice population). Clinical consultation rate for influenza, from sentinel practices, was highest among 15 to 24 year olds and 45 to 64 year olds. Two influenza A positive samples have been detected through the GP sentinel enhanced virological surveillance during weeks one and two; both samples came from the Swansea area (figures for week two are provisional). Influenza activity in other UK countries also appears to have increased during the last two weeks. In England the clinical consultation rate increased from 17.2 to 20.7 consultations per 100,000 during week 2, but is still within baseline levels (baseline in England is set at 30 per 100,000). In Scotland the clinical consultation rate during week two was 158 consultations per 100,000 practice population; which exceeds baseline levels (baseline in Scotland is set at 50 per 100,000). Clinical consultation rate for influenza in Northern Ireland also increased sharply during week two to 136.4 consultations per 100,000. Elsewhere in Europe, influenza activity in most countries remains at low levels. CDSC Wales thanks its sentinel practices for contributing weekly data to both clinical and virological flu surveillance, and would like to remind practices that cases reported through the virological scheme should also be reported via the weekly clinical surveillance of infections scheme. 0 20 40 60 80 100 120 140 160 180 200 40 42 44 46 48 50 52 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38 Week Consultation rate per 100,000 1999 - 2000 2005 - 2006 2006 - 2007 Series4 Series5 Baseline activity Normal seasonal activity Higher than average seasonal acvtivity Further information on influenza surveillance in Wales can be found on: http://www2.nphs.wales.nhs.uk/icds/page.cfm?pid=507

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Dr. R L Salmon, NPHS CDSC, Temple of Peace and Health, King Edward VIIAvenue, Cathays Park, Cardiff, CF10 3AP. Telephone: 029 20402471
Further information on infectious diseases in Wales can be found on our web site athttp://nww.nphs.wales.nhs.uk or http://www.nphs.wales.nhs.uk
18th January 2007
INCIDENCE RATES4 WEEKLY TRENDS
0
2
4
6
8
10
12
Chicken pox Influenza Measles Mumps Rubella Shingles Whoopingcough
Pneumonia
Ra
tepe
r1
00,0
00po
pula
tion 24-Dec-2006 31-Dec-2006
07-Jan-2007 14-Jan-2007
Influenza season update
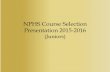
Influenza activity for Wales increased during week two of 2007. The clinical consultation rate forweek two was 5.13 consultations per 100,000; this is still well within baseline levels (below 25consultations per 100,000 practice population). Clinical consultation rate for influenza, from sentinelpractices, was highest among 15 to 24 year olds and 45 to 64 year olds. Two influenza A positivesamples have been detected through the GP sentinel enhanced virological surveillance duringweeks one and two; both samples came from the Swansea area (figures for week two areprovisional).Influenza activity in other UK countries also appears to have increased during the last two weeks. InEngland the clinical consultation rate increased from 17.2 to 20.7 consultations per 100,000 duringweek 2, but is still within baseline levels (baseline in England is set at 30 per 100,000). In Scotlandthe clinical consultation rate during week two was 158 consultations per 100,000 practice population;which exceeds baseline levels (baseline in Scotland is set at 50 per 100,000). Clinical consultationrate for influenza in Northern Ireland also increased sharply during week two to 136.4 consultationsper 100,000. Elsewhere in Europe, influenza activity in most countries remains at low levels.
CDSC Wales thanks its sentinel practices for contributing weekly data to both clinical and virologicalflu surveillance, and would like to remind practices that cases reported through the virologicalscheme should also be reported via the weekly clinical surveillance of infections scheme.
0
20
40
60
80
100
120
140
160
180
200
40 42 44 46 48 50 52 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38
Week
Co
nsu
lta
tio
nra
tep
er
100
,00
0
1999 - 2000 2005 - 2006 2006 - 2007Series4 Series5
Baseline activity
Normal seasonal activity
Higher than average seasonalacvtivity
Further information on influenza surveillance in Wales can be found on:http://www2.nphs.wales.nhs.uk/icds/page.cfm?pid=507
Dr. R L Salmon, NPHS CDSC, Temple of Peace and Health, King Edward VIIAvenue, Cathays Park, Cardiff, CF10 3AP. Telephone: 029 20402471
Further information on infectious diseases in Wales can be found on our web site athttp://nww.nphs.wales.nhs.uk or http://www.nphs.wales.nhs.uk
24th January 2007
INCIDENCE RATES4 WEEKLY TRENDS
0
2
4
6
8
10
12
Chicken pox Influenza Measles Mumps Rubella Shingles Whoopingcough
Pneumonia
Rat
epe
r100
,000
pop
ulat
ion 31-Dec-2006 07-Jan-2007
14-Jan-2007 21-Jan-2007
Advice to pregnant women during the lambing seasonInfection with certain organisms can cause abortion in pregnant sheep, and if a pregnantwoman becomes infected with these organisms they may harm her unborn child. Themost important organisms are Chlamydophila abortus [which causes enzootic abortion ofewes - EAE], Toxoplasma and Listeria.Although the number of reports of these infections and human miscarriages resultingfrom contact with sheep are extremely small it is important that pregnant women areaware of the potential risks. To avoid the possible risk of infection, pregnant women areadvised that they should:
Not help to lamb or milk ewes Avoid contact with aborted or new-born lambs Avoid contact with the afterbirth Avoid handling (including washing) clothing, boots, or any materials that have come
into contact with ewes, lambs or afterbirth. Should ensure that full hygiene precautions are followed by all household members Ensure partners attending lambing ewes observe full hygiene procedures Ensure that if they or their partners do come into contact, they should shower, bath
or wash thoroughly (including hair) as soon as practicable after handling a lambingewe
Scrub hands, and keep finger nails short and clean Wash clothes used in lambing separately, pregnant women should not handle dirty
clothes worn during the lambing season – if it is not possible to clean up thoroughlyduring the night, then sleep in separate bedrooms
Should not handle any vaccines, and should avoid contact with recently vaccinatedsheep.
Pregnant women should seek medical advice if they experience fever or influenza-likesymptoms, or if concerned that they could have acquired infection from a farmenvironment.
Comprehensive information on this topic is available from the HPA website at:http://www.hpa.org.uk/infections/topics_az/zoonoses/chlamydophila/default.htm
Dr. R L Salmon, NPHS CDSC, Temple of Peace and Health, King Edward VIIAvenue, Cathays Park, Cardiff, CF10 3AP. Telephone: 029 20402471
Further information on infectious diseases in Wales can be found on our web site athttp://nww.nphs.wales.nhs.uk or http://www.nphs.wales.nhs.uk
1st February 2007
INCIDENCE RATES4 WEEKLY TRENDS
0
2
4
6
8
10
12
Chicken pox Influenza Measles Mumps Rubella Shingles Whoopingcough
Pneumonia
Ra
tepe
r10
0,0
00po
pula
tion 07-Jan-2007 14-Jan-2007
21-Jan-2007 28-Jan-2007
Malaria treatment guidelines
New guidelines for the treatment of malaria have been publishedin the Journal of Infection, Volume 54 Issue 2, February 2007and for the HPA Advisory Committee on Malaria Prevention inUK Travellers.
The abstract and related links are also published in Pub Med at:http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=17215045&dopt=Abstract
Malaria is the tropical disease most commonly imported into the UK, with 1500-2000 cases reported each year, and 10-20 deaths. In Wales 10 cases of malariawere notified (through NOIDS) in 2005 and 7 cases in 2006 (NOIDS provisionalfigures).
Approximately three-quarters of reported malaria cases in the UK are caused byPlasmodium falciparum, which is capable of invading a high proportion of red bloodcells and rapidly leading to severe or life-threatening multi-organ disease.
Malaria should be considered in every ill patient who has recently returned from thetropics. For those with a fever returning from the tropics, the illness should beconsidered to be malaria until laboratory tests prove otherwise. Malaria in children(and sometimes in adults) may present with misleading symptoms such asgastrointestinal features, sore throat or lower respiratory complaints.
Malaria is a notifiable disease. All malaria cases should also be reported tothe Health Protection Agency Malaria Reference Laboratoryhttp://www.malaria-reference.co.uk.
Dr. R L Salmon, NPHS CDSC, Temple of Peace and Health, King Edward VIIAvenue, Cathays Park, Cardiff, CF10 3AP. Telephone: 029 20402471
Further information on infectious diseases in Wales can be found on our web site athttp://nww.nphs.wales.nhs.uk or http://www.nphs.wales.nhs.uk
7th February 2007
INCIDENCE RATES4 WEEKLY TRENDS
0
3
6
9
12
15
Chicken pox Influenza Measles Mumps Rubella Shingles Whoopingcough
Pneumonia
Ra
tep
er10
0,0
00
po
pula
tio
n 14-Jan-2007 21-Jan-2007
28-Jan-2007 04-Feb-2007
Immunisation against seasonal influenza in poultry workers
With the recent outbreak of H5N1 avian influenza in a turkey farm in East Anglia and theincreasing activity of seasonal influenza, Welsh Assembly requirements that local healthboards (LHBs) make arrangements to ensure that poultry workers are offered seasonalinfluenza vaccine seem prudent.
This immunisation programme results from a public health policy to reduce the risk of aninfluenza pandemic emerging in Wales. By protecting poultry workers against circulatinghuman influenza, the very slight risk that the worker could catch human and avian influenza atthe same time is reduced. If a poultry worker became infected with both human and bird fluviruses at the same time then there is a very slight risk that the two viruses could mix to createa new and potentially serious influenza virus. Seasonal flu vaccine protects against ordinaryhuman flu thus reducing the risk of a new virus emerging in this way.
From the 22nd January 2007 to 31st March 2007, each local health board in Wales is requiredto make arrangements to ensure as far as possible that poultry workers, as defined under thePrimary Medical Services (Influenza Immunisation Scheme for Poultry Workers) (Wales)Directions 2007, are offered seasonal influenza vaccine. Full details, including definitions of a‘poultry worker’ and how LHBs should identify and contact this occupational group, areavailable in a Welsh Health Circular (WHC (2007)001, see:http://howis.wales.nhs.uk/whcirculars.cfm).
Seasonal influenza activity, as measured by the Wales GP Surveillance Scheme, increasedthis week from 4.8 to 13.6 consultations per 100 000 practice population.
Dr. R L Salmon, NPHS CDSC, Temple of Peace and Health, King Edward VIIAvenue, Cathays Park, Cardiff, CF10 3AP. Telephone: 029 20402471
Further information on infectious diseases in Wales can be found on our web site athttp://nww.nphs.wales.nhs.uk or http://www.nphs.wales.nhs.uk
13th February 2007
INCIDENCE RATES4 WEEKLY TRENDS
0
3
6
9
12
15
Chicken pox Inf luenza Measles Mumps Rubella Shingles Whoopingcough
Pneumonia
Ra
tep
er
100
,00
0p
op
ula
tion
21-Jan-2007 28-Jan-2007
04-Feb-2007 11-Feb-2007
Use of antivirals now recommended for influenza-like illness in at-riskpatients
It has been officially announced that clinical and virological indicators suggest thatinfluenza viruses are now circulating in the community in significant numbers. Thismeans that oseltamivir and zanamivir are now licensed for use in line with NICEguidance. Note that oseltamivir (Tamiflu) is now licensed for treatment andprophylaxis in risk groups from 1 year of age. Algorithms and guidance can befound on the NPHS Vaccine Preventable Diseases Programme intranet page:http://nww.nphs.wales.nhs.uk/immunisation/page.cfm?pid=1323
4th Welsh Immunisation Conference
The fourth Welsh Immunisation Conference will take place at the Orangery,Margam Park, Port Talbot on 8th March 2007. The conference is aimed at all healthprofessionals involved in immunisation with a full and varied programme. Theconference fee is £25 and registration can be made through the National PublicHealth Service website:http://nww.nphs.wales.nhs.uk/immunisation/docopen.cfm?ID=2152.

Dr. R L Salmon, NPHS CDSC, Temple of Peace and Health, King Edward VIIAvenue, Cathays Park, Cardiff, CF10 3AP. Telephone: 029 20402471
Further information on infectious diseases in Wales can be found on our web site athttp://nww.nphs.wales.nhs.uk or http://www.nphs.wales.nhs.uk
22nd February 2007
INCIDENCE RATES4 WEEKLY TRENDS
0
5
10
15
20
Chicken pox Influenza Measles Mumps Rubella Shingles Whoopingcough
Pneumonia
Rat
epe
r10
0,0
00po
pula
tion 28-Jan-2007 04-Feb-2007
11-Feb-2007 18-Feb-2007
Houmous products recalled
The food manufacturer Bakkavor is recalling a number of houmous products which havebeen on sale in the UK and the Republic of Ireland. This action is being taken on aprecautionary basis after two Marks & Spencer products tested positive for Salmonella.Salmonella can cause food poisoning and should not be present in ready-to-eat foods.
The products, all manufactured by Bakkavor, which are being recalled are:
Co-op own-brand houmous and flavoured houmousAll date codes up to 28 February 2007
Marks & Spencer own-brand houmous, flavoured houmous and topped houmousAll date codes
Sainsbury’s own brand houmous, flavoured houmous and topped houmousAll date codes up to 28 February 2007
Somerfield own brand houmous and flavoured houmousAll date codes up to 28 February 2007
Tesco own brand houmous, flavoured houmous and topped houmousAll date codes up to 28 February 2007
Waitrose own brand houmous, flavoured houmous and topped houmousAll date codes up to 28 February 2007
According to the Food Standards Agency (see: http://www.foodstandards.gov.uk/news/newsarchive/2007/feb/bakkavor), all of these products have now been removed from sale.Bakkavor is advising customers who have bought these products not to eat them, but toreturn them to the store where they bought them for a refund. Further information about theproducts being recalled can be found on the Bakkavor Group website(http://www.bakkavor.com./media-centre/press-releases). Consumers who have anyqueries should contact the retailer direct or Bakkavor ' s Customer Careline on 0800 0232960 (for callers from within the UK ). Callers outside the UK should dial +44 207 266 6444.
Dr. R L Salmon, NPHS CDSC, Temple of Peace and Health, King Edward VIIAvenue, Cathays Park, Cardiff, CF10 3AP. Telephone: 029 20402471
Further information on infectious diseases in Wales can be found on our web site athttp://nww.nphs.wales.nhs.uk or http://www.nphs.wales.nhs.uk
1st March 2007
INCIDENCE RATES4 WEEKLY TRENDS
0
5
10
15
20
Chicken pox Influenza Measles Mumps Rubella Shingles Whoopingcough
Pneumonia
Ra
tep
er10
0,0
00po
pula
tion
04-Feb-2007 11-Feb-2007
18-Feb-2007 25-Feb-2007
Surveillance figures for Creutzfeldt-Jakob disease (CJD)
Table 1 shows the surveillance figures for definite and probable cases of Creutzfeldt-Jakob disease (CJD) in theUnited Kingdom up to 2 February 2007. In 2006, there were 109 referrals to the CJD surveillance unit with fiveconfirmed as vCJD. To date in 2007 there have been six referrals to the unit with none confirmed as vCJD.
While this version of the table does not show figures for years prior to 1995 (the first year for which there arevCJD confirmations), a more extended version can be accessed on the National CJD Surveillance Unit website(http://www.cjd.ed.ac.uk/figures.htm).
TABLE 1: Definite and probable CJD cases in the UK from 1995 to 2 February 2007
Referrals for DeathsYear investigation Sporadic Iatrogenic Familial GSS* vCJD
confirmed
vCJDProbable still
alive1995 87 35 4 2 3 3 -1996 133 40 4 2 4 10 -1997 162 60 6 4 1 10 -1998 154 63 3 3 2 18 -1999 170 62 6 2 0 15 -2000 178 50 1 2 1 28 -2001 179 58 4 3 2 20 -2002 163 72 0 4 1 17 -2003 162 79 5 4 2 18 -2004 114 51 2 4 1 9 -2005 123 65 3 7 6 5 -2006 109 55 1 6 3 5 -2007 6 1 1 0 0 0 7Total 158
* Gerstmann-Straussler-Scheinker syndrome
Bovine Spongiform Encephalopathy
Table 2 details the cases of Bovine Spongiform Encephalopathy confirmed in Great Britain since the peak of theoutbreak in 1992 to 23 February 2007.
TABLE 2: Confirmed cases of BSE to 23 February 2007
1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007
GB 36680 34370 23943 14301 8013 4310 3179 2556 1311 781 445 173 82 39 15 1

Dr. R L Salmon, NPHS CDSC, Temple of Peace and Health, King Edward VIIAvenue, Cathays Park, Cardiff, CF10 3AP. Telephone: 029 20402471
Further information on infectious diseases in Wales can be found on our web site athttp://nww.nphs.wales.nhs.uk or http://www.nphs.wales.nhs.uk
8th March 2007
INCIDENCE RATES4 WEEKLY TRENDS
0
5
10
15
20
Chicken pox Influenza Measles Mumps Rubella Shingles Whoopingcough
Pneumonia
Ra
tep
er10
0,0
00
po
pula
tion 11-Feb-2007 18-Feb-2007
25-Feb-2007 04-Mar-2007
Influenza activity in Wales
Influenza activity continues to remain at low levels. This week the consultation rate in Welsh sentinelpractices dropped to 9 consultations per 100, 000 population. Indeed the last significant seasonalactivity in Wales occurred in Winter 1999/2000, reaching 190 consultations per 100, 000 populationper week in January 2000.
So far this Winter, a total of 78 samples have been submitted by sentinel GPs in Wales for testing(Table). Twenty one of these samples have tested positive for influenza A. Six samples have testedpositive to date for RSV. None of the submitted samples have tested positive for influenza B. Thiscompares to last season, when influenza B predominated.
Table. Specimens submitted for testing by Welsh sentinel GPs (as of 01/03/07).
Week Specimens Specimenssubmitted tested Influenza A Influenza B RSV
40 - 01 29 28 2 0 42 6 6 1 0 13 2 2 0 0 04 8 8 2 0 15 9 9 3 0 06 6 6 2 0 07 13 13 8 0 08 5 3 3 0 0
Total 78 75 21 0 6
Positive identifications
Dr. R L Salmon, NPHS CDSC, Temple of Peace and Health, King Edward VIIAvenue, Cathays Park, Cardiff, CF10 3AP. Telephone: 029 20402471
Further information on infectious diseases in Wales can be found on our web site athttp://nww.nphs.wales.nhs.uk or http://www.nphs.wales.nhs.uk
15th March 2007
INCIDENCE RATES4 WEEKLY TRENDS
0
5
10
15
20
Chicken pox Influenza Measles Mumps Rubella Shingles Whoopingcough
Pneumonia
Rat
epe
r10
0,00
0po
pula
tion 18-Feb-2007 25-Feb-2007
04-Mar-2007 11-Mar-2007
Ongoing malaria outbreak in Goa
Since December 2006, a cluster of cases of Plasmodium falciparum malaria has beendetected in travellers who had visited northern Goa. As at 9th March, five cases of P.falciparum in travellers from the United Kingdom have been confirmed by the MalariaReference Laboratory (MRL). The four latest cases, confirmed by MRL between 4 Januaryand 15 February 2007, occurred in three female and one male traveller who visited Goaseparately, and who had stayed in a variety of accommodation. None of the travellers hadtaken malaria prevention tablets.
In recent years, the number of P. falciparum malaria cases reported from India has beenlow. In 2006 eleven cases of falciparum malaria were reported, and in 2005 nine caseswere reported. Many advisors, including the Health Protection Agency Advisory Committeefor Malaria Prevention (ACMP), had ceased recommending chemoprophylaxis for visitors tolow-risk regions including Goa.
Based on the additional cases of falciparum malaria reported form Goa, the ACMP nowadvises that health professionals who are advising travellers: highlight the risk of malaria,instruct on the use of mosquito bite avoidance measures and consider recommendingmalaria prevention tablets for travellers visiting Goa.
This advice for travellers to Goa to consider taking malaria prevention tablets is a change tocurrent ACMP guidelines for India and remains in effect until further notice.The recommended malaria prevention tablets for Goa are chloroquine plus proguanil.Alternatives are mefloquine, atovaquone/proguanil (Malarone®) or doxycycline.
Travellers should seek medical attention promptly if they become unwell and inform theirdoctor that they have been in a malarious area. Healthcare workers should considermalaria in every ill patient who has recently returned from the tropics.
Source: http://www.nathnac.org/pro/clinical_updates/malaria_Goa090307.htm

Dr. R L Salmon, NPHS CDSC, Temple of Peace and Health, King Edward VIIAvenue, Cathays Park, Cardiff, CF10 3AP. Telephone: 029 20402471
Further information on infectious diseases in Wales can be found on our web site athttp://nww.nphs.wales.nhs.uk or http://www.nphs.wales.nhs.uk
22nd March 2007
INCIDENCE RATES4 WEEKLY TRENDS
0
4
8
12
Chicken pox Influenza Measles Mumps Rubella Shingles Whoopingcough
Pneumonia
Rat
epe
r10
0,00
0po
pula
tion 25-Feb-2007 04-Mar-2007
11-Mar-2007 18-Mar-2007
World TB Day, Saturday March 24th – TB Anywhere is TB Everywhere
The theme of this year’s World TB Day is ‘TB anywhere is TB everywhere’ reminding us that,although TB is preventable and curable, it remains a global emergency. In 2005 there were 8.8million new cases and 1.6 million deaths worldwide caused by tuberculosis. The gradual yetsignificant year-on-year increases in TB notification in the UK since 1994 combined with thespectre of drug resistance make control of TB within Wales and the UK a public health priority.
TB rates have remained relatively stable over the last six years in Wales (Figure) at between150 and 200 cases per year. Whilst rates in Wales are lower than the UK average (6.5 forWales compared to 14.7 per 100,000 for the UK) patterns are similar, with higher rates in Asianand Black African ethnic populations, and rates higher in males and persons aged 25-34 andover 65 years.
Figure. Total Number of Cases and Rates of TB Infection in Wales1999-2005
5.7
6.2 6.3
5.3
5.9
6.5 6.5
0
50
100
150
200
250
1999 2000 2001 2002 2003 2004 2005
Year
Nu
mb
er
of
Ca
ses
0
1
2
3
4
5
6
7
8
9
10R
ate
pe
r1
00,0
00p
op
ula
tio
nNumber of Cases Rates
Source – Enhanced TB Surveillance Scheme
Dr. R L Salmon, NPHS CDSC, Temple of Peace and Health, King Edward VIIAvenue, Cathays Park, Cardiff, CF10 3AP. Telephone: 029 20402471
Further information on infectious diseases in Wales can be found on our web site athttp://nww.nphs.wales.nhs.uk or http://www.nphs.wales.nhs.uk
28th March 2007
INCIDENCE RATES4 WEEKLY TRENDS
0
4
8
12
Chicken pox Inf luenza Measles Mumps Rubella Shingles Whoopingcough
Pneumonia
Ra
tep
er
100
,00
0p
op
ula
tio
n 04-Mar-2007 11-Mar-2007
18-Mar-2007 25-Mar-2007
Uptake of childhood immunisations in Wales
Uptake of all three doses of the combined “5 in 1” DTaP/IPV/Hib vaccine, scheduled at 2, 3 and4 months of age, is 95.5%, just above the 95% target (Figure). Uptake of the first dose of MMR inchildren reaching 2 years of age is 88%, and follows a period of sustained recovery over the lastthree years. Uptake of the second dose of MMR in five year old children has increased butremains low at 77%. Marked regional differences remain in MMR uptake, with uptake of the firstdose by two years of age ranging from 81% to 92% by LHB and uptake of the second dose by fiveyears of age ranging from 70% to 85%.
Figure . Percentage uptake of childhood immunisations in Wales, quarter 4 1990 to quarter 4 2006.Data are for children reaching 1 year of age each quarter for diphtheria, pertussis and Hib, childrenreaching 2 years of age for MMR1 (first dose), and 5 years of age for MMR2 (second dose).
60
65
70
75
80
85
90
95
100
1990
- 419
91- 2
1991
- 41 9
92-2
1992
-419
9 3-2
1993
- 419
94- 2
1994
- 41 9
95- 2
1995
-419
9 6-2
1996
- 419
97- 2
1997
- 419
98- 2
1998
- 419
99- 2
199 9
-420
00-2
2000
- 420
01- 2
2001
- 420
02- 2
200 2
-420
03-2
2003
- 420
04- 2
2004
- 420
05- 2
2 005
- 420
06-2
2006
-4
Up
take
(%)
MMR1 (2yrs) Diphtheria Pertussis Hib Men C MMR2 (5yrs)
Dr. R L Salmon, NPHS CDSC, Temple of Peace and Health, King Edward VIIAvenue, Cathays Park, Cardiff, CF10 3AP. Telephone: 029 20402471
Further information on infectious diseases in Wales can be found on our web site athttp://nww.nphs.wales.nhs.uk or http://www.nphs.wales.nhs.uk
4th April 2007
INCIDENCE RATES4 WEEKLY TRENDS
0
4
8
12
Chicken pox Influenza Measles Mumps Rubella Shingles Whoopingcough
Pneumonia
Rat
epe
r10
0,00
0po
pula
tion 11-Mar-2007 18-Mar-2007
25-Mar-2007 01-Apr-2007
Influenza Immunisation Programme 2007/2008
A Welsh Health Circular has just been issued outlining the influenza immunisationcampaign for 2007/2008. As in previous years, the national policy is that flu vaccine shouldbe offered free to the following groups:
i. All those aged 65 years and over.
ii. All those aged over 6 months in a clinical risk group.
iii. Those living in long-stay residential care homes or other long-stay facilities whererapid spread is likely to follow introduction of infection and cause high morbidity andmortality ( this does not include prisons, young offenders institutions, university hallsof residence etc).
iv. Those who are in receipt of a carer’s allowance, or those who are the main carer foran elderly or disabled person who welfare may be at risk if the carer falls ill. Thisshould be given on an individual basis at the GP’s discretion in the context of otherclinical risk groups in the practice.
Following advice from the Joint Committee on Vaccination and Immunisation (JCVI) thefollowing new group has been added to the list of those clinical risk groups recommendedto be offered vaccination:
Individuals with the following neurological conditions: cerbrovascular disease(principally stroke and transient ischaemic attacks (TIAs)); multiple sclerosis andrelated conditions; and hereditary and degenerative disease of the central nervoussystem.
Source: WHC (2007) 037 (http://howis.wales.nhs.uk/whcirculars.cfm)
Dr. R L Salmon, NPHS CDSC, Temple of Peace and Health, King Edward VIIAvenue, Cathays Park, Cardiff, CF10 3AP. Telephone: 029 20402471
Further information on infectious diseases in Wales can be found on our web site athttp://nww.nphs.wales.nhs.uk or http://www.nphs.wales.nhs.uk
16th April 2007
INCIDENCE RATES4 WEEKLY TRENDS
0
2
4
6
8
10
Chicken pox Inf luenza Measles Mumps Rubella Shingles Whoopingcough
Pneumonia
Ra
tep
er
10
0,0
00
pop
ula
tion 18-Mar-2007 25-Mar-2007
01-Apr-2007 08-Apr-2007
Influenza vaccine composition for 2007/08
The World Health Organisation (WHO) recommends flu vaccine strains based oncareful mapping of flu viruses as they move around the world. This monitoring iscontinuous and allows experts to make predictions of which strains are most likelyto cause influenza outbreaks in the northern hemisphere in the coming winter.
The strains of influenza virus recommended by WHO to be used in the 2007/08season (northern hemisphere winter) are:
an A/Solomon Islands/3/2006 (H1N1)-like virus
an A/Wisconsin/67/2005 (H3N2)-like virus
a B/Malaysia/2506/2004-llike virus
Candidate viruses include:
an A/Wisconsin/67/2005(H3N2) and A/Hiroshima/52/2005
See http://www.who.int/csr/disease/influenza/20078anorthreport.pdf
Dr. R L Salmon, NPHS CDSC, Temple of Peace and Health, King Edward VIIAvenue, Cathays Park, Cardiff, CF10 3AP. Telephone: 029 20402471
Further information on infectious diseases in Wales can be found on our web site athttp://nww.nphs.wales.nhs.uk or http://www.nphs.wales.nhs.uk
19th April 2007
INCIDENCE RATES4 WEEKLY TRENDS
0
2
4
6
8
10
Chicken pox Influenza Measles Mumps Rubella Shingles Whoopingcough
Pneumonia
Ra
tepe
r10
0,00
0po
pul
atio
n 25-Mar-2007 01-Apr-2007
08-Apr-2007 15-Apr-2007
Influenza immunisation in unpaid carers
In 2005 the Welsh Assembly Government added ‘carers’ to the list of target groups thatshould be offered seasonal influenza immunisation by their doctor. In 2006 NPHS and thenational charity Crossroads Caring for Carers carried out a survey to assess awarenessand uptake of ‘flu immunisation in a sample of carers recruited from the community.
Key Findings are that:
Over half of the unpaid carers surveyed are not aware that they are eligible for freeinfluenza immunisation from their general practice
Carers not in another Welsh Assembly Government target group for influenzaimmunisation, that is: those younger than 65 years not in a chronic disease riskgroup, are least likely to be offered immunisation by their practice and least likely tobe immunised
Identifying people in this group and offering them immunisation provides thegreatest opportunity to increase uptake amongst carers
Young carers, that is: those younger than 18 years, appear to be a group currentlyneglected
A copy of the full report is available from the NPHS intranet site at:http://nww2.nphs.wales.nhs.uk/icds/docopen.cfm?ID=2199. Information on this Winter’s fluimmunization campaign is available in the Welsh Health Circular:http://new.wales.gov.uk/docrepos/40382/40382311111/comms/whc/1222709/37-07-influenza-e?lang=en
Dr. R L Salmon, NPHS CDSC, Temple of Peace and Health, King Edward VIIAvenue, Cathays Park, Cardiff, CF10 3AP. Telephone: 029 20402471
Further information on infectious diseases in Wales can be found on our web site athttp://nww.nphs.wales.nhs.uk or http://www.nphs.wales.nhs.uk
26th April 2007
INCIDENCE RATES4 WEEKLY TRENDS
0
2
4
6
8
10
12
14
Chicken pox Influenza Measles Mumps Rubella Shingles Whoopingcough
Pneumonia
Rat
epe
r10
0,00
0po
pula
tion 01-Apr-2007 08-Apr-2007
15-Apr-2007 22-Apr-2007
Health Protection 2007: Call for abstracts
This is the leading multi-disciplinary health protection conference in Europe,showcasing the latest scientific research and its application to practice. Theconference, taking place at Warwick University between 17th and 19 th September,will be attended by over 1000 participants working in health protection - from publichealth, laboratories, hospitals, emergency planning, infection control, environmentalhealth and academic institutions. The conference focuses on the latest scientificresearch and its practical application to key areas of health protection. Theconference programme will comprise a number of symposia running in parallel,covering topical issues across the breadth of health protection. Topics this yearinclude: ‘Prison Health’, ‘Health Care Associated Infection’, ‘Chronic effects ofenvironmental factors’ and ‘The Changing Landscape of Diagnostic Microbiology’.
Abstracts for presentation at Health Protection 2007 are now being invited forsubmission before the closing date of midnight on Thursday 10 May. Theconference is an opportunity to showcase the latest scientific research and practicein a wide range of key areas of health protection. Abstracts on new findings anddevelopments are welcomed. There will be a prize for the most innovative poster.
Further information, including the full programme, and an area for on-line booking and submission ofabstracts, can be found at: http://www.healthprotectionconference.org.uk/
Dr. R L Salmon, NPHS CDSC, Temple of Peace and Health, King Edward VIIAvenue, Cathays Park, Cardiff, CF10 3AP. Telephone: 029 20402471
Further information on infectious diseases in Wales can be found on our web site athttp://nww.nphs.wales.nhs.uk or http://www.nphs.wales.nhs.uk
2nd May 2007
INCIDENCE RATES4 WEEKLY TRENDS
0
2
4
6
8
10
12
14
Chicken pox Inf luenza Measles Mumps Rubella Shingles Whoopingcough
Pneumonia
Ra
tep
er
10
0,0
00
pop
ula
tio
n 08-Apr-2007 15-Apr-2007
22-Apr-2007 29-Apr-2007
Hepatitis B vaccine coverage in prisons in WalesThe Health Protection Agency Prison Infection Prevention Team co-ordinates thesurveillance of infectious diseases affecting the prison population of England and Wales.Data on the uptake of hepatitis B vaccination in Welsh prisons in 2006 are presented below:
Table. Hepatitis B vaccine coverage in prisons in Wales, 2006.
Establishment Category Average monthlythroughput
Average monthly vaccinecoverage
Cardiff Local 240 21.0Parc YOI 160 6.5Prescoed Training 54 13.9Swansea Local 210 3.1Usk Training 18 11.3
The May edition of Infection Inside: The Prison Infectious Disease Quarterly has justbeen published by the Health Protection Agency
Features this issue include: New Prison Health Key Performance Indicators National AIDS Trust Launches Best Practice Framework for Tackling Blood-Borne
Viruses in Prisons Women’s Health in Prisons Improving Hepatitis B Vaccination Coverage – Best Practice at HMPs Liverpool and
Reading
You can access both current and past copies of the newsletter at:http://www.hpa.org.uk/infections/topics_az/prisons/reports.htm. The ‘Health Protection2007’ conference will have 3 prisoner health sessions on Monday 17th September.Abstracts on good practice in prisons are being encouraged. To submit an abstract by May10th go to: www.healthprotectionconference.org.uk/
Dr. R L Salmon, NPHS CDSC, Temple of Peace and Health, King Edward VIIAvenue, Cathays Park, Cardiff, CF10 3AP. Telephone: 029 20402471
Further information on infectious diseases in Wales can be found on our web site athttp://nww.nphs.wales.nhs.uk or http://www.nphs.wales.nhs.uk
11th May 2007
INCIDENCE RATES4 WEEKLY TRENDS
0
2
4
6
8
10
12
14
Chicken pox Influenza Measles Mumps Rubella Shingles Whoopingcough
Pneumonia
Rat
epe
r10
0,00
0p
opul
atio
n 15-Apr-2007 22-Apr-2007
29-Apr-2007 06-May-2007
Surveillance figures for Creutzfeldt-Jakob disease (CJD)
Table 1 shows the surveillance figures for definite and probable cases of Creutzfeldt-Jakob disease (CJD) in theUnited Kingdom up to 4 May 2007. In 2006, there were 109 referrals to the CJD surveillance unit with fiveconfirmed as vCJD. To date in 2007 there have been 34 referrals to the unit with two confirmed as vCJD.
While this version of the table does not show figures for years prior to 1995 (the first year for which there arevCJD confirmations), a more extended version can be accessed on the National CJD Surveillance Unit website(http://www.cjd.ed.ac.uk/figures.htm).
TABLE 1: Definite and probable CJD cases in the UK from 1995 to 4 May 2007
Referrals for DeathsYear investigation Sporadic Iatrogenic Familial GSS* vCJD
confirmed
vCJDProbable still
alive1995 87 35 4 2 3 3 -1996 133 40 4 2 4 10 -1997 162 60 6 4 1 10 -1998 154 63 3 3 2 18 -1999 170 62 6 2 0 15 -2000 178 50 1 2 1 28 -2001 179 58 4 3 2 20 -2002 163 72 0 4 1 17 -2003 162 79 5 4 2 18 -2004 114 51 2 4 1 9 -2005 123 65 3 7 6 5 -2006 109 57 1 6 3 5 -2007 34 7 2 0 1 2 5Total 160
* Gerstmann-Straussler-Scheinker syndrome
Bovine Spongiform Encephalopathy
Table 2 details the cases of Bovine Spongiform Encephalopathy confirmed in Great Britain since the peak of theoutbreak in 1992 to 4 May 2007.
TABLE 2: Confirmed cases of BSE to 4 May 2007
1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007
GB 36680 34370 23943 14301 8013 4310 3179 2556 1311 781 445 173 82 39 15 3

Dr. R L Salmon, NPHS CDSC, Temple of Peace and Health, King Edward VIIAvenue, Cathays Park, Cardiff, CF10 3AP. Telephone: 029 20402471
Further information on infectious diseases in Wales can be found on our web site athttp://nww.nphs.wales.nhs.uk or http://www.nphs.wales.nhs.uk
18th May 2007
INCIDENCE RATES4 WEEKLY TRENDS
0
2
4
6
8
10
12
14
Chicken pox Inf luenza Measles Mumps Rubella Shingles Whoopingcough
Pneumonia
Rat
epe
r10
0,00
0po
pula
tion 22-Apr-2007 29-Apr-2007
06-May-2007 13-May-2007
Syphilis in WalesNPHS has been carrying out enhanced surveillance of infectious syphilis in Wales since2002. To the end of April 2007, there have been 249 reports of infectious syphilis fromGUM clinics in Wales: 27 in 2002, 57 in 2003, 49 in 2004, 48 in 2005, 57 in 2006 and 11 sofar in 2007. 46% of reports have been of primary syphilis, 26% secondary, and 23% earlylatent. Cases have been predominantly in white men and 72% of cases are in men whoreport having sex with men (MSM) - of which 32 reported being bisexual. So far there havebeen 69 cases in heterosexuals and it does appear that the proportion of cases acquiredheterosexually is increasing (see Figure). To date, 179 of cases were reported from clinicsin South East Wales, 33 from Mid and West Wales and 37 from North Wales. 60% of casesreported probably acquired their infection in Wales. One in five (21%) of MSM cases and7% of heterosexual cases were known to be HIV positive.
Cases of infectious syphilis in Wales: 3 month rolling average,February 2002 to January 2007
0
1
2
3
4
5
6
7
Feb
-02
May
-02
Aug
-02
Nov
-02
Feb
-03
May
-03
Aug
-03
Nov
-03
Feb
-04
May
-04
Aug
-04
Nov
-04
Feb
-05
May
-05
Aug
-05
Nov
-05
Feb
-06
May
-06
Aug
-06
Nov
-06
Hetero MSM

Dr. R L Salmon, NPHS CDSC, Temple of Peace and Health, King Edward VIIAvenue, Cathays Park, Cardiff, CF10 3AP. Telephone: 029 20402471
Further information on infectious diseases in Wales can be found on our web site athttp://nww.nphs.wales.nhs.uk or http://www.nphs.wales.nhs.uk
24th May 2007
INCIDENCE RATES4 WEEKLY TRENDS
0
2
4
6
8
10
Chicken pox Influenza Measles Mumps Rubella Shingles Whoopingcough
Pneumonia
Rat
ep
er10
0,00
0po
pula
tion 29-Apr-2007 06-May-2007
13-May-2007 20-May-2007
Tick bites and Lyme disease
The number of people being infected by ticks carrying Lyme borreliosis (Lyme disease) hasincreased from 292 reported cases in 2003, to 684 (provisionally) in 2006. Areas whereinfection has been acquired in the UK include Exmoor, the New Forest, the South Downs, partsof Wiltshire and Berkshire, Thetford Forest, the Lake District, the Yorkshire moors and theScottish Highlands. A significant number were acquired during activity holidays when walking,trekking and mountain-biking. The peak times for tick bites are late spring, early summer andautumn.
The most common symptom is a slowly expanding rash (which is not significantly painful oritchy) originating from the site of the bite, usually after 5-14 days. This may enlarge over manyweeks if not treated with antibiotics, but will eventually disappear without treatment. Otherpresenting symptoms may include tiredness, headaches and aches and pains in muscles andjoints. If left untreated the infection may spread in the bloodstream and to other parts of thebody, including the nervous system, joints and other organs, and some patients may developcomplications caused by tissue damage.
To minimise the risk of being bitten by an infected tick:
Wear appropriate clothing in tick-infested areas (i.e. light-coloured long sleeved shirtand long trousers tucked into socks).
Inspect skin (including skin folds, neck, head and scalp) and clothing for ticks frequentlyand at the end of the day and remove any attached ticks.
Consider using insect repellents, e.g. DEET-containing preparations.
Check that pets do not bring unfed ticks into the home on their fur.
To remove a tick, gently grip it as close to the skin as possible, preferably using fine-toothedtweezers or a similar implement, and pull steadily away from the skin. Some veterinarysurgeries and pet shops sell inexpensive tick removal devices. Covering the tick with creams orvolatile oils or using lighted cigarettes or matches are not recommended.
See: www.hpa.org.uk/infections/topics_az/zoonoses/lyme_borreliosis/default.htm
Dr. R L Salmon, NPHS CDSC, Temple of Peace and Health, King Edward VIIAvenue, Cathays Park, Cardiff, CF10 3AP. Telephone: 029 20402471
Further information on infectious diseases in Wales can be found on our web site athttp://nww.nphs.wales.nhs.uk or http://www.nphs.wales.nhs.uk
30th May 2007
INCIDENCE RATES4 WEEKLY TRENDS
0
2
4
6
8
10
Chicken pox Inf luenza Measles Mumps Rubella Shingles Whoopingcough
Pneumonia
Ra
tep
er
10
0,0
00p
op
ula
tio
n 06-May-2007 13-May-2007
20-May-2007 27-May-2007
Avian flu H7N2 outbreak in North Wales
On 24 May 2007 an outbreak of low pathogenic H7N2 avian influenza was confirmed in poultry on asmallholding near Corwen, Conwy, North Wales.
On 25 May, 4 people were confirmed to have been infected with the H7 virus-two from Wales andtwo from England. To date, 12 individuals who have a history of contact with either the infected birdsor another human case have been identified as having or have had symptoms of a flu like illness orconjunctivitis. No one is seriously ill and three individuals admitted to hospital have since beendischarged.
The NPHS are continuing to trace and follow-up all close contacts of the people who are cases.People identified as contacts are being offered antiviral medication as a precautionary measure. Thisincludes 12 pupils and 2 teachers at a local primary school and 148 patients and staff from twohospitals.
Preliminary investigations indicate that the occurrence of person-to-person spread cannot beexcluded as some people exhibiting signs of infection did not have close contact with infectedpoultry. Person to person spread would be very unusual but limited spread of this type has beenseen elsewhere in the past in some cases of bird flu.
Although the NPHS believe the risk to the health of the general public is low the public healthresponse to this outbreak is being actively managed as experience of this particular avian influenza(H7N2) is limited. Avian flu is primarily a disease of birds and infection with H7N2 is very mildcompared with infection with avian influenza subtype H5N1, currently circulating predominantly inAsia.
Over the last decade in the UK only a small number of H7 avian influenza infections have beenconfirmed in individuals who had close contact with either poultry or their housing.
In 1996 a female farmer acquired H7N7 avian influenza and suffered conjunctivitis after cleaning outa poultry house. More recently, in May 2006 one case of conjunctivitis was reported in a worker at apoultry farm in Norfolk following an outbreak of H7N3 avian influenza in the flock.
A daily update of the situation in North Wales including information leaflets produced by the NPHSfor the public is available from the main NPHS internet site: http://www.nphs.wales.nhs.uk/
The NPHS has also issued guidelines for health professionals with regard to this outbreak which areavailable to download from: http://nww2.nphs.wales.nhs.uk/page.cfm?pid=1655
Dr. R L Salmon, NPHS CDSC, Temple of Peace and Health, King Edward VIIAvenue, Cathays Park, Cardiff, CF10 3AP. Telephone: 029 20402471
Further information on infectious diseases in Wales can be found on our web site athttp://nww.nphs.wales.nhs.uk or http://www.nphs.wales.nhs.uk
7th June 2007
INCIDENCE RATES4 WEEKLY TRENDS
0
2
4
6
8
Chicken pox Influenza Measles Mumps Rubella Shingles Whoopingcough
Pneumonia
Rat
epe
r10
0,00
0po
pula
tion
13-May-2007 20-May-2007
27-May-2007 03-Jun-2007
Salmonella Senftenberg and fresh basil
Since the beginning of 2007, the HPA’s Laboratory of Enteric Pathogens has received45 isolates of Salmonella Senftenberg from cases not reporting foreign travel. Thiscompares to ten in the same time period in 2006. A total of 34 (76%) of these isolateshave been received since week 15 (8 April 2007). Cases have been reported fromacross England and Wales and most cases are between the ages of 15 and 64 years ofage
Since May 2007, NPHS has been involved in a collaborative UK study of themicrobiological quality of retail fresh herbs. To date, seven samples of pre-packed freshbasil, grown and packed in Israel, have tested positive for Salmonella spp. Results areavailable for four of the seven isolates which have been confirmed as S. Senftenberg.
Pulsed-field gel electrophoresis (PFGE) was carried out on two of the basil isolateswhich was given the PFGE profile SSFTXB.0014. Fourteen (50%) of the humanisolates tested so far and received after week 15 are also SSFTXB.0014.
Although a definite link between the rise in the number of human cases of SalmonellaSenftenberg and fresh basil has not been established, Salmonella Senftenberg is arelatively uncommon form of Salmonella in England and Wales. Further investigationsare ongoing.
The Food Standards Agency (FSA) issued a food alert on 25 May 2007 warningconsumers not to eat basil from the same batches that were found to be contaminatedat the time.
Source: Health Protection Report, 1 June 2007, Volume 1, No 22
Dr. R L Salmon, NPHS CDSC, Temple of Peace and Health, King Edward VIIAvenue, Cathays Park, Cardiff, CF10 3AP. Telephone: 029 20402471
Further information on infectious diseases in Wales can be found on our web site athttp://nww.nphs.wales.nhs.uk or http://www.nphs.wales.nhs.uk
14th June 2007
INCIDENCE RATES4 WEEKLY TRENDS
0
2
4
6
8
Chicken pox Influenza Measles Mumps Rubella Shingles Whoopingcough
Pneumonia
Rat
epe
r10
0,0
00po
pula
tion 20-May-2007 27-May-2007
03-Jun-2007 10-Jun-2007
Food Safety Week- ‘Bugs like it hot’
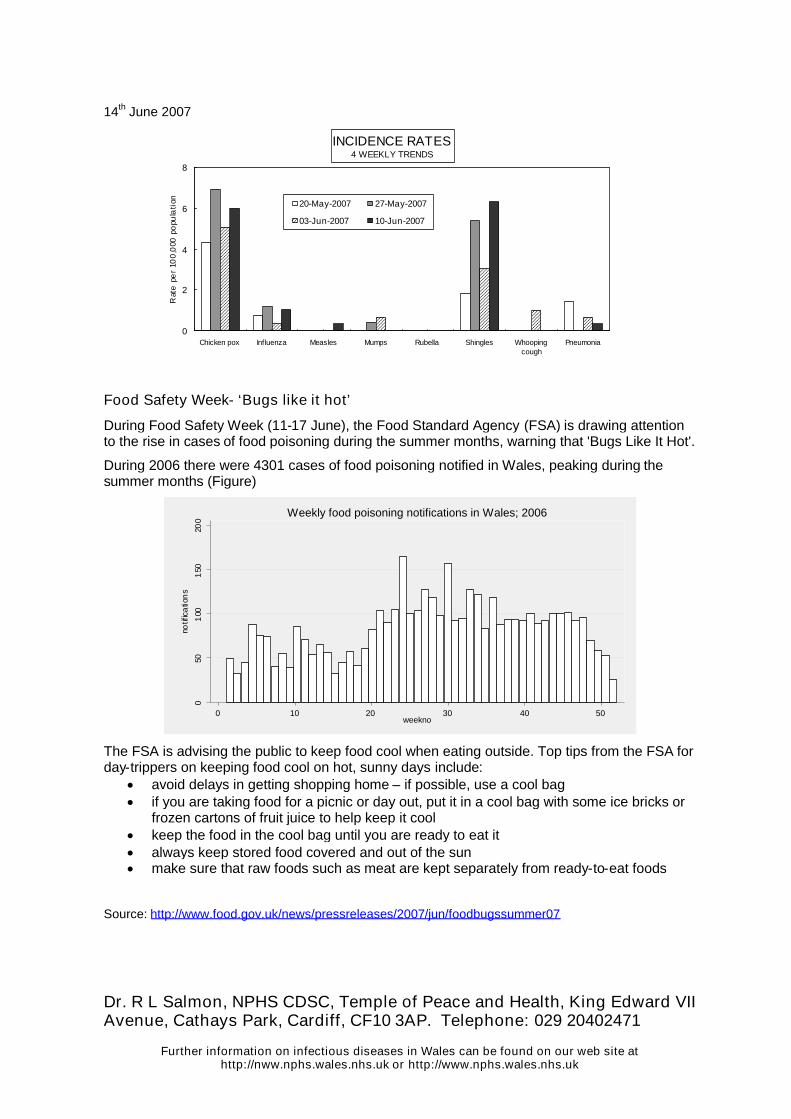
During Food Safety Week (11-17 June), the Food Standard Agency (FSA) is drawing attentionto the rise in cases of food poisoning during the summer months, warning that 'Bugs Like It Hot'.
During 2006 there were 4301 cases of food poisoning notified in Wales, peaking during thesummer months (Figure)
050
100
150
200
notif
ica
tion
s
0 10 20 30 40 50weekno
Weekly food poisoning notifications in Wales; 2006
The FSA is advising the public to keep food cool when eating outside. Top tips from the FSA forday-trippers on keeping food cool on hot, sunny days include:
avoid delays in getting shopping home – if possible, use a cool bag if you are taking food for a picnic or day out, put it in a cool bag with some ice bricks or
frozen cartons of fruit juice to help keep it cool keep the food in the cool bag until you are ready to eat it always keep stored food covered and out of the sun make sure that raw foods such as meat are kept separately from ready-to-eat foods
Source: http://www.food.gov.uk/news/pressreleases/2007/jun/foodbugssummer07
Dr. R L Salmon, NPHS CDSC, Temple of Peace and Health, King Edward VIIAvenue, Cathays Park, Cardiff, CF10 3AP. Telephone: 029 20402471
Further information on infectious diseases in Wales can be found on our web site athttp://nww.nphs.wales.nhs.uk or http://www.nphs.wales.nhs.uk
21 June 2007
INCIDENCE RATES4 WEEKLY TRENDS
0
2
4
6
8
Chicken pox Influenza Measles Mumps Rubella Shingles Whoopingcough
Pneumonia
Rat
epe
r1
00,
000
po
pula
tio
n 27-May-2007 03-Jun-2007
10-Jun-2007 17-Jun-2007
Tuberculosis in Wales
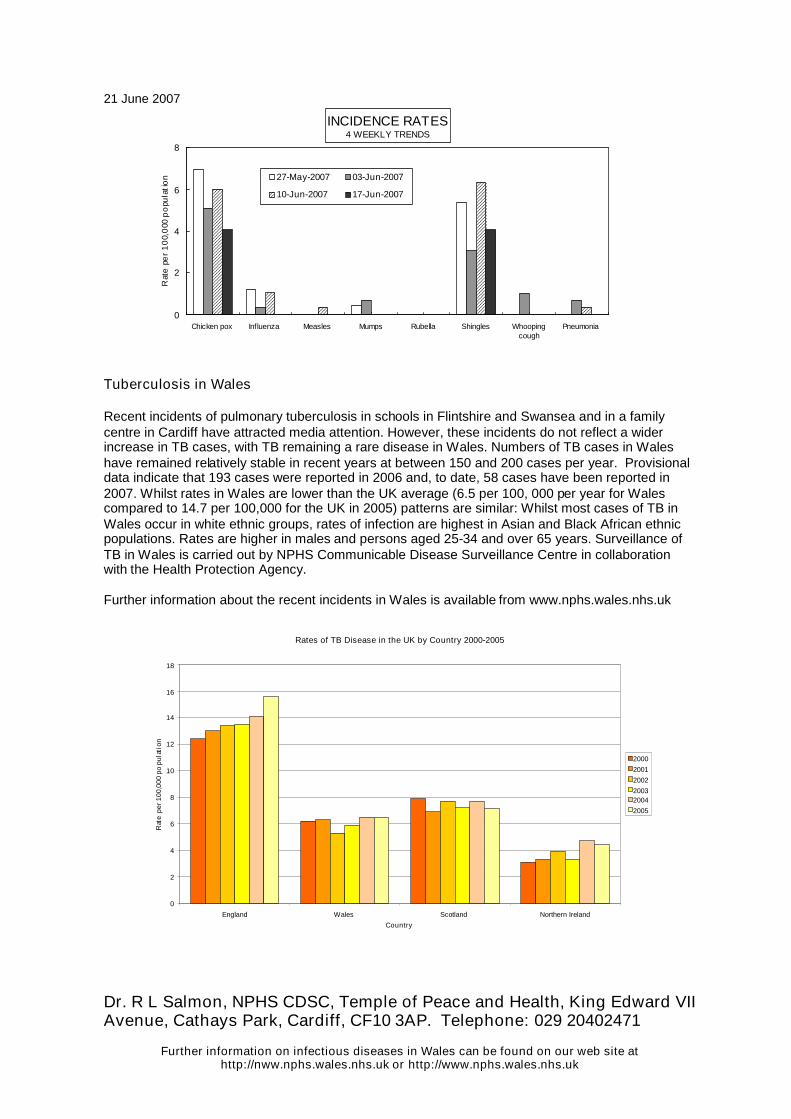
Recent incidents of pulmonary tuberculosis in schools in Flintshire and Swansea and in a familycentre in Cardiff have attracted media attention. However, these incidents do not reflect a widerincrease in TB cases, with TB remaining a rare disease in Wales. Numbers of TB cases in Waleshave remained relatively stable in recent years at between 150 and 200 cases per year. Provisionaldata indicate that 193 cases were reported in 2006 and, to date, 58 cases have been reported in2007. Whilst rates in Wales are lower than the UK average (6.5 per 100, 000 per year for Walescompared to 14.7 per 100,000 for the UK in 2005) patterns are similar: Whilst most cases of TB inWales occur in white ethnic groups, rates of infection are highest in Asian and Black African ethnicpopulations. Rates are higher in males and persons aged 25-34 and over 65 years. Surveillance ofTB in Wales is carried out by NPHS Communicable Disease Surveillance Centre in collaborationwith the Health Protection Agency.
Further information about the recent incidents in Wales is available from www.nphs.wales.nhs.uk
Rates of TB Disease in the UK by Country 2000-2005
0
2
4
6
8
10
12
14
16
18
England Wales Scotland Northern Ireland
Country
Rat
epe
r100
,000
popu
lati
on
2000
2001
2002
20032004
2005
Dr. R L Salmon, NPHS CDSC, Temple of Peace and Health, King Edward VIIAvenue, Cathays Park, Cardiff, CF10 3AP. Telephone: 029 20402471
Further information on infectious diseases in Wales can be found on our web site athttp://nww.nphs.wales.nhs.uk or http://www.nphs.wales.nhs.uk
28 June 2007
INCIDENCE RATES4 WEEKLY TRENDS
0
2
4
6
8
Chicken pox Inf luenza Measles Mumps Rubella Shingles Whoopingcough
Pneumonia
Ra
tep
er1
00
,00
0po
pu
latio
n 03-Jun-2007 10-Jun-2007
17-Jun-2007 24-Jun-2007
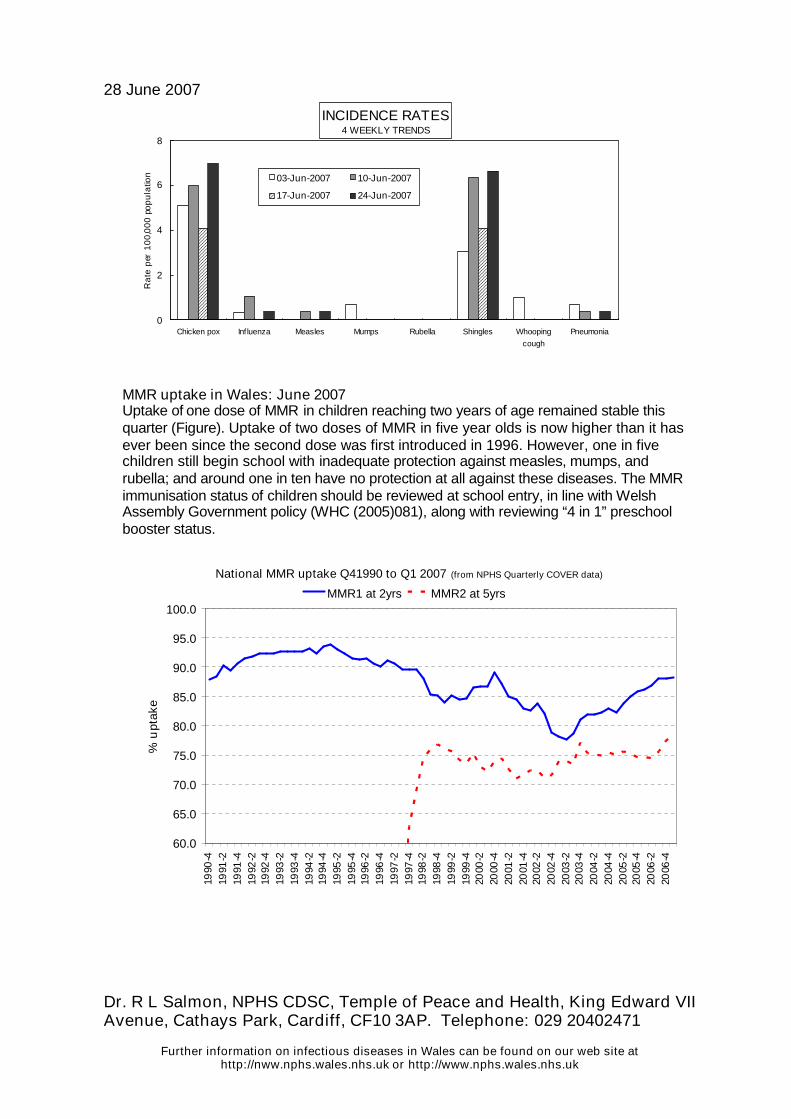
MMR uptake in Wales: June 2007Uptake of one dose of MMR in children reaching two years of age remained stable thisquarter (Figure). Uptake of two doses of MMR in five year olds is now higher than it hasever been since the second dose was first introduced in 1996. However, one in fivechildren still begin school with inadequate protection against measles, mumps, andrubella; and around one in ten have no protection at all against these diseases. The MMRimmunisation status of children should be reviewed at school entry, in line with WelshAssembly Government policy (WHC (2005)081), along with reviewing “4 in 1” preschoolbooster status.
National MMR uptake Q41990 to Q1 2007 (from NPHS Quarterly COVER data)
60.0
65.0
70.0
75.0
80.0
85.0
90.0
95.0
100.0
1990
-419
91-2
1991
-419
92-2
1992
-419
93-2
1993
-419
94-2
1994
-419
95-2
1995
-419
96-2
1996
-419
97-2
1997
-419
98-2
1998
-419
99-2
1999
-420
00-2
2000
-420
01-2
2001
-420
02-2
2002
-420
03-2
2003
-420
04-2
2004
-420
05-2
2005
-420
06-2
2006
-4
%u
ptak
e
MMR1 at 2yrs MMR2 at 5yrs
Dr. R L Salmon, NPHS CDSC, Temple of Peace and Health, King Edward VIIAvenue, Cathays Park, Cardiff, CF10 3AP. Telephone: 029 20402471
Further information on infectious diseases in Wales can be found on our web site athttp://nww.nphs.wales.nhs.uk or http://www.nphs.wales.nhs.uk
5 July 2007
INCIDENCE RATES4 WEEKLY TRENDS
0
2
4
6
8
Chicken pox Influenza Measles Mumps Rubella Shingles Whoopingcough
Pneumonia
Ra
tepe
r10
0,0
00
po
pula
tion 10-Jun-2007 17-Jun-2007
24-Jun-2007 01-Jul-2007
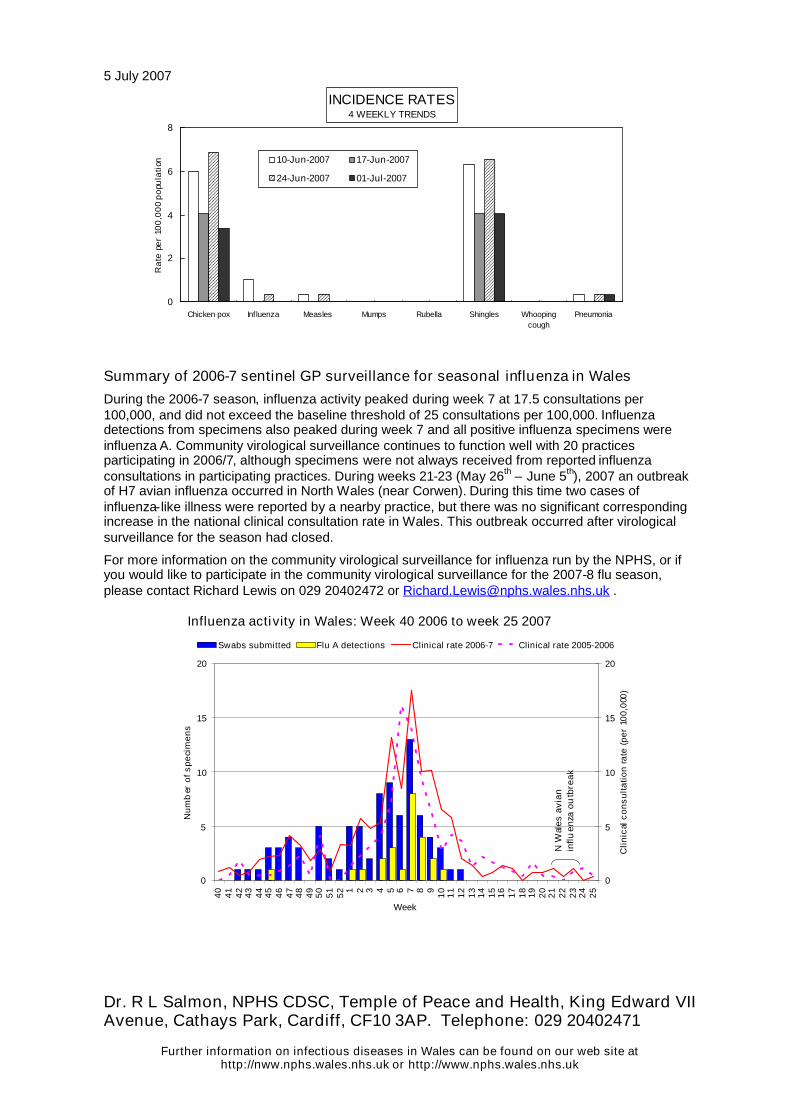
Summary of 2006-7 sentinel GP surveillance for seasonal influenza in Wales
During the 2006-7 season, influenza activity peaked during week 7 at 17.5 consultations per100,000, and did not exceed the baseline threshold of 25 consultations per 100,000. Influenzadetections from specimens also peaked during week 7 and all positive influenza specimens wereinfluenza A. Community virological surveillance continues to function well with 20 practicesparticipating in 2006/7, although specimens were not always received from reported influenzaconsultations in participating practices. During weeks 21-23 (May 26th – June 5th), 2007 an outbreakof H7 avian influenza occurred in North Wales (near Corwen). During this time two cases ofinfluenza-like illness were reported by a nearby practice, but there was no significant correspondingincrease in the national clinical consultation rate in Wales. This outbreak occurred after virologicalsurveillance for the season had closed.
For more information on the community virological surveillance for influenza run by the NPHS, or ifyou would like to participate in the community virological surveillance for the 2007-8 flu season,please contact Richard Lewis on 029 20402472 or [email protected] .
Influenza activity in Wales: Week 40 2006 to week 25 2007
0
5
10
15
20
40 41 42 43 44 45 46 47 48 49 50 51 52 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25
Week
Num
ber
ofsp
ecim
ens
0
5
10
15
20
Clin
ical
cons
ulta
tion
rate
(per
100,
000)
Swabs submitted Flu A detections Clinical rate 2006-7 Clinical rate 2005-2006
NW
ales
avia
nin
fluen
zaou
tbre
ak
Dr. R L Salmon, NPHS CDSC, Temple of Peace and Health, King Edward VIIAvenue, Cathays Park, Cardiff, CF10 3AP. Telephone: 029 20402471
Further information on infectious diseases in Wales can be found on our web site athttp://nww.nphs.wales.nhs.uk or http://www.nphs.wales.nhs.uk
12 July 2007
INCIDENCE RATES4 WEEKLY TRENDS
0
2
4
6
8
Chicken pox Influenza Measles Mumps Rubella Shingles Whoopingcough
Pneumonia
Rat
epe
r10
0,00
0po
pula
tion 17-Jun-2007 24-Jun-2007
01-Jul-2007 08-Jul-2007
Public health in US prime-time televisionThe US Centers for Disease Control is targeting prime time and daytime televisionprograms, such as ER, Grey's Anatomy and Girlfriends, to provide outlets for public healthinformation and influence behaviour. The CDC Entertainment Education Program works inpartnership with Hollywood, Health & Society (HH&S) based at the University of SouthernCalifornia, and provides expert consultation, education and resources for writers andproducers who develop scripts with health storylines and information. The EntertainmentEducation Program also serves as a resource providing accurate, timely health informationon a wide variety of important public health issues.
From January 2001 to September 2006, more than 700 inquiries from television writerswere received. Over 400 TV episodes contained public health information, including 82major storylines. Eleven shows ran some combination of informational public serviceannouncements, info spots, and free-phone numbers and more than 200 links wereprovided between TV series and public health web sites. Additionally, 28 storylines havebeen evaluated for effect on viewing audiences, and the health content of 109 showsevaluated.
A recent episode of Grey's Anatomy covered the topic of health disparities for threeminutes. The advertising rate during this show is more than $352,000 per 30 seconds. Anepisode has an average audience of 18.5 million viewers.
In March 2003, Girlfriends aired a show discussing HIV stigma that reached 3.63 millionviewers. An evaluation found that viewers were less likely to agree with the belief thatpeople who contracted AIDS through sex or drug use had ‘gotten what they deserve’. Theyalso had a lower level of HIV stigma within the year after the episode was aired, and higherintention to be tested for HIV, compared to before broadcast.
Source: http://www.cdc.gov/news/2007/07/pubhealth_tv.html

Dr. R L Salmon, NPHS CDSC, Temple of Peace and Health, King Edward VIIAvenue, Cathays Park, Cardiff, CF10 3AP. Telephone: 029 20402471
Further information on infectious diseases in Wales can be found on our web site athttp://nww.nphs.wales.nhs.uk or http://www.nphs.wales.nhs.uk
20th July 2007
INCIDENCE RATES4 WEEKLY TRENDS
0
2
4
6
8
Chicken pox Inf luenza Measles Mumps Rubella Shingles Whoopingcough
Pneumonia
Rat
ep
er10
0,00
0p
opul
atio
n 24-Jun-2007 01-Jul-2007
08-Jul-2007 15-Jul-2007
Q fever cluster in Cheltenham
Five cases of acute Q fever have been reported in residents of Cheltenham(Gloucestershire), population 109,800, with onset dates between the end of May and 14June 2007. There had been no cases reported in Gloucestershire since 2002. The casesreported in Cheltenham did not have any occupational risk factors. Although all five casesreported possible environmental risk factors, no common exposures have been identified sofar.
Q fever (Coxiella burnetti) is thought to account for approximately 1% of communityacquired pneumonia in the UK each year, and can result in serious complications such asendocarditis. The main reservoirs are sheep, goats and cattle. Transmission of Q feveroccurs primarily through inhalation of contaminated aerosols. The organism is robust andcan survive in dust and animal litter for many weeks, and in dried blood for at least sixmonths at room temperature. The most infectious animal materials are the fluids of birthand afterbirth, followed by blood, milk, urine and faeces. Such infectious materials can bederived from livestock as above, or from domestic animals, particularly parturient cats.
The local Health Protection Unit would be grateful for information on any cases of Q feverwho have visited Gloucestershire during the incubation period (two to three weeksdepending on the infective dose). Please contact the Consultant Regional Epidemiologist,Isabel Oliver email: [email protected]. A standard questionnaire for newly diagnosedcases of Q fever can be obtained from the Emerging Infections and Zoonoses section of theHPA Centre for Infections. Please contact Mandy Walsh on 020 8327 7483, email:[email protected].
Source: Health Protection Report, July 27th 2007 (http://www.hpa.org.uk/hpr/news/default.htm#qfever)
Dr. R L Salmon, NPHS CDSC, Temple of Peace and Health, King Edward VIIAvenue, Cathays Park, Cardiff, CF10 3AP. Telephone: 029 20402471
Further information on infectious diseases in Wales can be found on our web site athttp://nww.nphs.wales.nhs.uk or http://www.nphs.wales.nhs.uk
27th July 2007
INCIDENCE RATES4 WEEKLY TRENDS
0
2
4
6
8
Chicken pox Influenza Measles Mumps Rubella Shingles Whoopingcough
Pneumonia
Ra
tep
er
10
0,0
00p
op
ula
tio
n 01-Jul-2007 08-Jul-2007
15-Jul-2007 22-Jul-2007
Health effects of flooding
The risk of contracting an infectious disease following a flooding event in the UK isthought to be low. However, it is wise to follow simple precautions when coming intocontact with flood water, particularly if it is contaminated with sewage. Theseinclude: regular hand-washing with hot soapy water, particularly before touchingfood, and covering any open wounds with waterproof plaster. Where drinking watersupply is interrupted or contaminated special precautions must be taken in usingwater to make infant formula milk. Bowser or bottled water brought to a ‘rolling boil’should be used following formula milk manufacturers instructions. However, itshould be noted that not all bottled waters are suitable for making infant formula dueto high salt contents. Parents should check labeling on the bottle or test the waterfor a salty taste. Anyone who has come into contact with flood water who is unwellwith vomiting, diarrhoea, fever or abdominal pain within the following 10 daysshould seek medical advice.
The Health Protection Agency has posted a series of guidelines on their websitegiving advice on what measures should be taken to reduce health risks, includingthose during cleaning up after a flood. These are available at:http://www.hpa.org.uk/flooding/default.htm. Further advice and links are alsoavailable on the NPHS website(http://www.wales.nhs.uk/sites3/news.cfm?orgid=719&contentid=7137).

Dr. R L Salmon, NPHS CDSC, Temple of Peace and Health, King Edward VIIAvenue, Cathays Park, Cardiff, CF10 3AP. Telephone: 029 20402471
Further information on infectious diseases in Wales can be found on our web site athttp://nww.nphs.wales.nhs.uk or http://www.nphs.wales.nhs.uk
10th August 2007
INCIDENCE RATES4 WEEKLY TRENDS
0
2
4
6
8
Chicken pox Influenza Measles Mumps Rubella Shingles Whoopingcough
Pneumonia
Ra
tep
er
10
0,0
00
pop
ula
tion 15-Jul-2007 22-Jul-2007
29-Jul-2007 05-Aug-2007
Temporary enhancement to the childhood immunisation schedule
The Welsh Assembly Government have announced a temporary enhancement of thechildhood immunisation programme (explained in Welsh Health Circular 2007 057).
From 10 September 2007 until 3 March 2009 a Hib booster will to be offered to youngchildren who have not previously received one - children born between 13 March 2003 and3 September 2005 who will be aged between two years old and four years and five monthsold at the start of the campaign. These children were too young to have had a booster aspart of the 2003 Hib catch-up campaign, and too old to have received the new Hib/MenCbooster. Implementing this temporary enhancement will mean that this group of childrenwill then have received the same level of protection against Haemophilus influenzae balready offered to older and younger children.
For younger children the Hib booster will be offered as a pre-school booster by temporarilychanging the pre-school booster vaccine to one that contains an additional Hib component(Infanrix-IPV+Hib, or alternatively Pediacel). The older children in the cohort, who havealready received their pre-school booster, will be offered an additional appointment toreceive Hib/MenC vaccine (Menitorix).
During the course of this campaign, the age at which the pre-school immunisation is offeredwill also be reduced - in areas where this is not already the case - to 3 years 4 months ofage.
Further information on this temporary enhancement can be found in WHC 2007 057:http://new.wales.gov.uk/docrepos/40382/cmo/comms/whc/1222709/57-07-hib?lang=en
Dr. R L Salmon, NPHS CDSC, Temple of Peace and Health, King Edward VIIAvenue, Cathays Park, Cardiff, CF10 3AP. Telephone: 029 20402471
Further information on infectious diseases in Wales can be found on our web site athttp://nww.nphs.wales.nhs.uk or http://www.nphs.wales.nhs.uk
16th August 2007
INCIDENCE RATES4 WEEKLY TRENDS
0
2
4
6
Chicken pox Influenza Measles Mumps Rubella Shingles Whoopingcough
Pneumonia
Rat
ep
er
10
0,0
00
pop
ula
tio
n 22-Jul-2007 29-Jul-2007
05-Aug-2007 12-Aug-2007
Outbreak of E. coli O157 in Scotland
The Public Health Protection Unit at NHS Greater Glasgow and Clyde is investigating anoutbreak of E coli O157 in the Paisley area. Currently there are two family clusters and twoisolated cases. In the first family, a 66 year-old woman has died as a result of contractingthe infection. Her husband, 72, is seriously ill in hospital. In the second family, two womenaged 23 and 45 and a man aged 46 are all recovering well at home. One of the singlecases is a 71 year-old women who is unwell but stable in the Royal Alexandra Hospital inPaisley. The second single case is a woman aged 86 who is recovering at home.
The Public Health Protection Unit is working closely with Environmental Health colleaguesfrom Renfrewshire Council, the Food Standards Agency and Health Protection Scotland toidentify the source of this infection. Initial investigations have indicated that there may be alink to the consumption of some sliced cold meats bought locally from the delicatessencounters of two Morrisons supermarkets in Paisley, the Lonend store and the Falside Roadstore.
Further investigations are continuing, but, as a precaution, sliced cold meats have beenwithdrawn from these two stores and anyone who has bought sliced cold meat from thesedelicatessen counters is being advised not to consume them. There is no evidence tosuggest that pre-packed cooked meats purchased from the stores or other food purchasedfrom the delicatessen counters are implicated.
Source: NHS Greater Glasgow and Clyde website:http://www.nhsggc.org.uk/content/default.asp?page=s765_3&newsid=5635&back=home_news
24th August 2007

Dr. R L Salmon, NPHS CDSC, Temple of Peace and Health, King Edward VIIAvenue, Cathays Park, Cardiff, CF10 3AP. Telephone: 029 20402471
Further information on infectious diseases in Wales can be found on our web site athttp://nww.nphs.wales.nhs.uk or http://www.nphs.wales.nhs.uk
INCIDENCE RATES4 WEEKLY TRENDS
0
2
4
6
8
Chicken pox Influenza Measles Mumps Rubella Shingles Whoopingcough
Pneumonia
Ra
tep
er
100
,00
0p
op
ula
tion 29-Jul-2007 05-Aug-2007
12-Aug-2007 19-Aug-2007
Waitrose recalls two own-brand Scottish salmon products due to contamination withListeria monocytogenes
The supermarket Waitrose has recalled two of its own-brand Scottish salmon products dueto contamination with Listeria monocytogenes. Product recall notices appeared in thenational press on 21st August 2007 and point of sale notices are being displayed in allWaitrose stores. These notices will alert customers to the recall and advise them of whatactions to take if they have purchased the affected products.The Products recalled are:
Waitrose Scottish Smoked Salmon Parcels 115g Waitrose Scottish Poached Salmon Terrines 100g
All date codes up to and including 28 August 2007.No other Waitrose products are known to be affected.
Listeria is an unusual bacterium because it can grow at low temperatures, includingrefrigeration temperatures of below 5°C. It is, however, killed by cooking food thoroughlyand by pasteurisation. Foods most likely to be contaminated with listeria are unpasteurisedcheeses, cold cuts of meat, pâtés and smoked fish, or ready meals which have been pre-cooked and then chilled for some time before consumption.
Listeriosis is a rare disease. However, there is evidence to suggest it’s incidence has beenincreasing in the UK in recent years. In Wales, there have been 13 laboratory confirmedcases of infection so far in 2007 compared to 6 in 2006 and 10 in 2005. Cases have beenmainly in older adults. Infection can be life-threatening but in healthy adults is likely to beonly mild infection, causing flu-like symptoms or gastroenteritis. However, listeria infectioncan occasionally lead to severe blood poisoning (septicaemia) or meningitis. Pregnantwomen, the elderly and people with weakened immune systems are more susceptible tolisteria. It is particularly dangerous in pregnancy as although the illness is unlikely to beserious for the mother, it can cause miscarriage, premature delivery or severe illness in anewborn child.
A copy of the product recall notice issued by Waitrose Ltd. Can be obtained from:http://www.food.gov.uk/enforcement/alerts/2007/aug/waitrosesalmon. Further information on listeriais available from the HPA website: http://www.hpa.org.uk/infections/topics_az/listeria/menu.htm.
Dr. R L Salmon, NPHS CDSC, Temple of Peace and Health, King Edward VIIAvenue, Cathays Park, Cardiff, CF10 3AP. Telephone: 029 20402471
Further information on infectious diseases in Wales can be found on our web site athttp://nww.nphs.wales.nhs.uk or http://www.nphs.wales.nhs.uk
31st August 2007
INCIDENCE RATES4 WEEKLY TRENDS
0
2
4
6
8
Chicken pox Influenza Measles Mumps Rubella Shingles Whoopingcough
Pneumonia
Ra
tep
er1
00,
00
0p
op
ula
tio
n 05-Aug-2007 12-Aug-2007
19-Aug-2007 26-Aug-2007
MeaslesThere have been 480 confirmed cases of measles in the UK so far this year. This compareswith a provisional total of 756 cases during the whole of 2006. The number of cases in 2006was the highest number recorded since the current method of monitoring began in 1995and this year looks set to show a further increase. To 24th August, 10 confirmed cases ofmeasles were from Wales, 5 from Scotland and 465 from England.
The increase in cases this year has been particularly in communities where uptake ofmeasles-mumps-rubella (MMR) vaccine is lower, including in children on traveller sites, butcases are currently occurring in unvaccinated school age children. Over the course of theyear, there have also been small outbreaks in primary schools and cases in peoplereturning from other countries. An outbreak recently occurred in a primary school inNewport in South-East Wales.
Currently in Wales, 88% of five year-olds have received a single dose of MMR vaccine, andonly 78% have received two doses. It is important that children complete their full course(two doses) of MMR vaccine as after the first dose, between 5% and 10% of children arenot protected against measles.
It is never too late for children to get vaccinated and the Health Protection Agency iscurrently urging parents to protect their children against measles by getting themimmunised with two doses of MMR before they return to school this September.
More information about measles can be found on this website from the link:http://www.wales.nhs.uk/sites3/page.cfm?orgId=719&pid=23148
More information about immunisation and MMR can be found on this website from thelink: http://www.wales.nhs.uk/sites3/page.cfm?orgid=719&pid=22646 and at:www.mmrthefacts.nhs.uk
Dr. R L Salmon, NPHS CDSC, Temple of Peace and Health, King Edward VIIAvenue, Cathays Park, Cardiff, CF10 3AP. Telephone: 029 20402471
Further information on infectious diseases in Wales can be found on our web site athttp://nww.nphs.wales.nhs.uk or http://www.nphs.wales.nhs.uk
7th September 2007
INCIDENCE RATES4 WEEKLY TRENDS
0
2
4
6
8
Chicken pox Influenza Measles Mumps Rubella Shingles Whoopingcough
Pneumonia
Rat
epe
r100
,000
popu
latio
n 12-Aug-2007 19-Aug-2007
26-Aug-2007 02-Sep-2007
Proposals for national programme to control Salmonella in poultry
The Minister for Rural Affairs, Elin Jones, recently announced a Welsh AssemblyGovernment consultation on a programme to protect public health by updating andenhancing existing controls on salmonella in commercial egg-producing (laying) poultryflocks. The proposed Regulations will set a target for an annual reduction of at least 10% inthe number of salmonella-positive adult laying flocks, compared with the previous year. Thestarting baseline in Wales and for the rest of the UK, will be 8% prevalence of SalmonellaEnteritidis and Salmonella Typhimurium serotypes. This prevalence is based on the resultsof survey of commercial laying flocks carried out in 2004/2005 which showed that around8% of layer flock holdings in the UK were infected with Salmonella Enteritidis or SalmonellaTyphimurium.
Implementation of a National Control Programme (NCP) for the monitoring and control ofSalmonella in laying flocks will be enforced by the introduction of The Control of Salmonellain Poultry (Wales) Regulations 2007. It will be brought into force in 2008 to comply with therequirements of EU Regulations 2160/2003 and 1168/2006.
The NCP will require operators to collect samples for Salmonella testing, from day-old layerchicks coming onto the farm and then from pullets 2 weeks before transfer to the layerhouse. It also requires that laying flocks be sampled every 15 weeks during production. Thesamples have to be submitted to an approved laboratory for examination for Salmonella.For holdings with over 1,000 birds there is the additional requirement that one flock per yearshould be sampled and tested under the control of the Competent Authority to verify theachievement of the Salmonella reduction target.
Under the same legislation there will be a requirement, from 1 January 2009 that eggs forhuman consumption from flocks infected with Salmonella Enteritidis or SalmonellaTyphimurium undergo heat treatment to eliminate Salmonella; i.e., the sale of fresh shelleggs from these flocks will not be permitted. In addition from November 2007 thisrequirement will apply to flocks when the eggs from the flock are linked to a foodborneoutbreak of Salmonellosis in humans.
Source: http://new.wales.gov.uk/news/presreleasearchive/1652509/?lang=en
Dr. R L Salmon, NPHS CDSC, Temple of Peace and Health, King Edward VIIAvenue, Cathays Park, Cardiff, CF10 3AP. Telephone: 029 20402471
Further information on infectious diseases in Wales can be found on our web site athttp://nww.nphs.wales.nhs.uk or http://www.nphs.wales.nhs.uk
13th September 2007
INCIDENCE RATES4 WEEKLY TRENDS
0
2
4
6
8
Chicken pox Inf luenza Measles Mumps Rubella Shingles Whoopingcough
Pneumonia
Ra
tepe
r10
0,0
00
pop
ula
tion 19-Aug-2007 26-Aug-2007
02-Sep-2007 09-Sep-2007
E.coli O157 outbreak report published
The report by the Outbreak Control Team (OCT) of the outbreak of E.coli O157 in SouthWales in the autumn of 2005 has been published. The report was completed in June 2006but publication was delayed pending legal proceedings involving the local meat supplier atthe centre of the outbreak. Legal proceedings ended on Friday 7th September in Cardiff withthe supplier being jailed for a year for food safety offences after Cardiff Crown Court heardthat a vacuum-packing machine, "wrongly used" for both raw and cooked meats, was thesource of contaminated meat to schools.
The report makes nine recommendations, including a review of how Local Authorities buyfood for their schools and care homes, and the setting up of national minimum standards forensuring good hygiene within the school environment.
The report will now be passed to Professor Hugh Pennington, who is heading a publicinquiry into the outbreak.
In September 2005, the largest E. coli O157 outbreak ever seen in Wales occurred. Therewere 157 cases meeting the case definition of whom 118 were microbiologically confirmed.109 of these confirmed cases were of phage type 21/28 and of a strain unique to thisoutbreak. Primary cases were mostly amongst schoolchildren attending 44 schools inBridgend, Caerphilly, Merthyr Tydfil and Rhondda Cynon Taf.
Thirty-one cases were hospitalised, 11 of whom were transferred to tertiary hospitals, andone child died.
The full report is available to download from the following link:http://www.wales.nhs.uk/sites3/Documents/719/E%20coli%20O157%20OCT%20report.pdf
Related Documents