A small thyroid papillary cancer The role of Shear Wave Elastography Antonio Pio Masciotra Campobasso – Molise – Italy Website www.masciotra.net YouTube Channel https ://www.youtube.com/channel/UCgCj21nKGAhR997Ia3-QegQ 51 years old asymptomatic woman at her first thyroid US exam. Two small nodules were found in her left lobe, one in the lower pole, the other near the isthmus.

Dr. masciotra sonoelastography and us in the diagnosis of small thyroid papillary cancers
Jul 26, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

A small thyroid papillary cancerThe role of Shear Wave Elastography
Antonio Pio MasciotraCampobasso – Molise – Italy
Website www.masciotra.net
YouTube Channel https://www.youtube.com/channel/UCgCj21nKGAhR997Ia3-QegQ
51 years old asymptomatic woman at her first thyroid US exam.Two small nodules were found in her left lobe, one in the lower pole, the other near the isthmus.

This is the lower pole nodule, slightlyhypoechoic wth a few intranodularvessels at powerdoppler.At Shear Wave Elastography it shows astiffness substantially not different fromthe one of surrounding normalparenchyma.

This is the second nodule (8 mm in diameter and 0,2 ml in volume).It is inhomogenehously hypoechoic, with undefined borders, taller than wide,
with small calcification and many intranodular vessels.
10-2 Mhz Linear probe 15-4 MHz Linear probe 16-5 MHz Linear Probe

This is the 3D US studyalso in elastography

10-2 Mhz probe 15-4 MHz probe 16-5 MHz probe
Left lobe paraisthmicnodule (kPa)
10-2 MHz 15-4 MHz 16-5 MHz
Mean stiffness 72-104 58-72 51-71
Maximum stiffness 95-133 76-111 87-91
Minimum stiffness 71-89 26-41 1-49
Standard Deviation 9-13 9-20 11-23
Ratio 1,4-3,4 2,4-4,3 1,8-3,8

Lower pole nodule Paraisthmic nodule
15-4 MHZ Probe SWE Features (kPa)
Lower pole nodule
Paraisthmicnodule
Mean stiffness 31-33 58-72
Maximum stiffness 36-43 76-111
Minimum stiffness 25-31 26-41
Standard Deviation 1-3 9-20
Ratio 1,0-1,4 2,4-4,3

This is the FNA cytology of the left lobe’sparaisthmic nodule classified TIR 5* (correspondingto Thy VI in the Bethesda Classification), diagnosticfor PTC.At surgery this nodule was confirmed PTC, while thelower pole nodule was benign (simply hyperplastic).
* ITALIAN CONSENSUS GROUP FOR THE CLASSIFICATION AND REPORTING OF THYROID CYTOLOGYFrancesco Nardi, Fulvio Basolo, Anna Crescenzi, Guido Fadda, Andrea Frasoldati, Fabio Orlandi, Lucio Palombini, Enrico Papini, Alfredo Pontecorvi, Paolo Vitti (2013)
TIR1: Not diagnostic.
TIR1C: Not diagnostic - Cyst.
TIR2: Not neoplastic.
TIR3A: Low risk follicular lesion.
TIR3B: High risk follicular lesion.
TIR4: Suspicious for malignancy.
TIR5: Diagnostic of malignancy.

Two more small thyroid papillary cancersThe role of Sonoelastography
Antonio Pio MasciotraCampobasso – Molise – Italy
Website www.masciotra.net
YouTube Channel https://www.youtube.com/channel/UCgCj21nKGAhR997Ia3-QegQ
37 years old asymptomatic woman at her first thyroid US exam.Two small nodules were found, one in the right lobe near the isthmus, the other in the lower pole of the left lobe.

This is the right lobe’s paraisthmicnodule, slightly hypoechoic withintranodular vessels at powerdoppler.At Shear Wave Elastography it showsstiffness features substantially notdifferent from the ones showed by theright lobe’s paraisthmic nodule.

This is the lower pole nodule, slightlyhypoechoic with a few intranodularvessels at powerdoppler.At Shear Wave Elastography it showsstiffness features substantially notdifferent from the ones showed by theright lobe’s paraisthmic nodule.

Right lobe paraisthmicnodule (kPa)
10-2 MHz 15-4 MHz 16-5 MHz
Mean stiffness 42-45 42-71 15-36
Maximum stiffness 47-59 68-77 20-47
Minimum stiffness 19-42 15-63 8-13
Standard Deviation 1,4-7,7 4,0-11,2 2,8-9,3
Ratio 1,4-2,1 2,9-5,2 1,0-2,6
Left lobe nodule(kPa)
10-2 MHz 15-4 MHz 16-5 MHz
Mean stiffness 19-30 28-66 15-16
Maximum stiffness 21-41 32-69 20-23
Minimum stiffness 16-17 11-63 1-8
Standard Deviation 0,8-7,8 1,2-9,7 2,8-7,1
Ratio 1,0-2,9 1,2-3,8 1,0-1,6
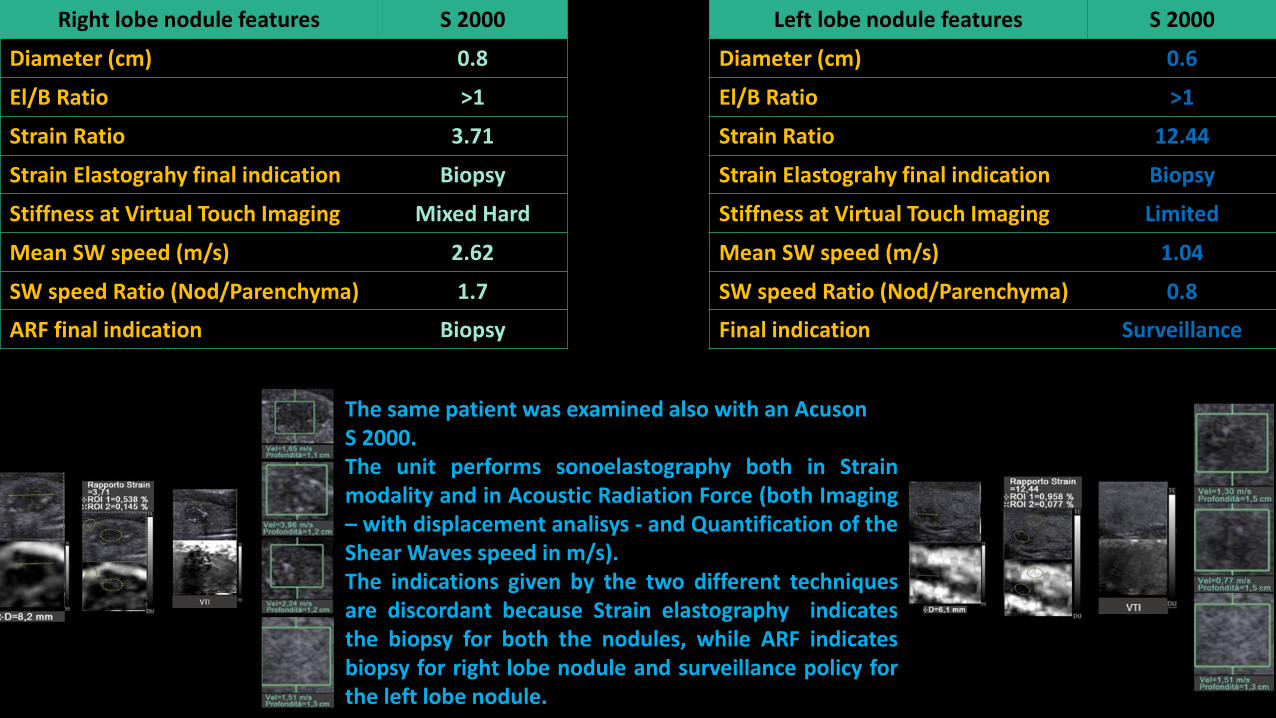
Left lobe nodule features S 2000
Diameter (cm) 0.6
El/B Ratio >1
Strain Ratio 12.44
Strain Elastograhy final indication Biopsy
Stiffness at Virtual Touch Imaging Limited
Mean SW speed (m/s) 1.04
SW speed Ratio (Nod/Parenchyma) 0.8
Final indication Surveillance
Right lobe nodule features S 2000
Diameter (cm) 0.8
El/B Ratio >1
Strain Ratio 3.71
Strain Elastograhy final indication Biopsy
Stiffness at Virtual Touch Imaging Mixed Hard
Mean SW speed (m/s) 2.62
SW speed Ratio (Nod/Parenchyma) 1.7
ARF final indication Biopsy
The same patient was examined also with an AcusonS 2000.The unit performs sonoelastography both in Strainmodality and in Acoustic Radiation Force (both Imaging– with displacement analisys - and Quantification of theShear Waves speed in m/s).The indications given by the two different techniquesare discordant because Strain elastography indicatesthe biopsy for both the nodules, while ARF indicatesbiopsy for right lobe nodule and surveillance policy forthe left lobe nodule.

This is the FN cytology of the right lobe’sparaisthmic nodule classified TIR 4* (correspondingto Thy V in the Bethesda Classification), suspiciousfor PTC.At surgery both nodules were PTC.
* ITALIAN CONSENSUS GROUP FOR THE CLASSIFICATION AND REPORTING OF THYROID CYTOLOGYFrancesco Nardi, Fulvio Basolo, Anna Crescenzi, Guido Fadda, Andrea Frasoldati, Fabio Orlandi, Lucio Palombini, Enrico Papini, Alfredo Pontecorvi, Paolo Vitti (2013)
TIR1: Not diagnostic.
TIR1C: Not diagnostic - Cyst.
TIR2: Not neoplastic.
TIR3A: Low risk follicular lesion.
TIR3B: High risk follicular lesion.
TIR4: Suspicious for malignancy.
TIR5: Diagnostic of malignancy.

Case n.2
SSI SWE Features (15-4 MHz Probe) Right lobe nodule Left lobe nodule
Mean stiffness (kPa) 42-71 28-66
Maximum stiffness (kPa) 68-77 32-69
Minimum stiffness (kPa) 15-63 11-63
Standard Deviation (kPa) 4-11 1-9
Ratio 2,9-5,2 1,2-3,8
Acuson S 2000 Features (9-4 MHz Probe) Right lobe nodule Left lobe nodule
Elasto/B image Ratio >1 >1
Strain Ratio 3,71 12,44
Stiffness at Virtual Touch Imaging Mixed Hard Almost Isostiff
Mean SW speed (m/s) 2,62 1,04
SW speed Ratio (Nodule/Parenchyma) 1,7 0,8
Acuson S 2000 Final Indication Biopsy Biopsy (Strain)Surveillance (ARF)
SSI SWE Final Indication Biopsy Biopsy
FNA Citology TIR 4 (Thy V) Not performed
Pathological diagnosis Malignant (PTC) Malignant (PTC)
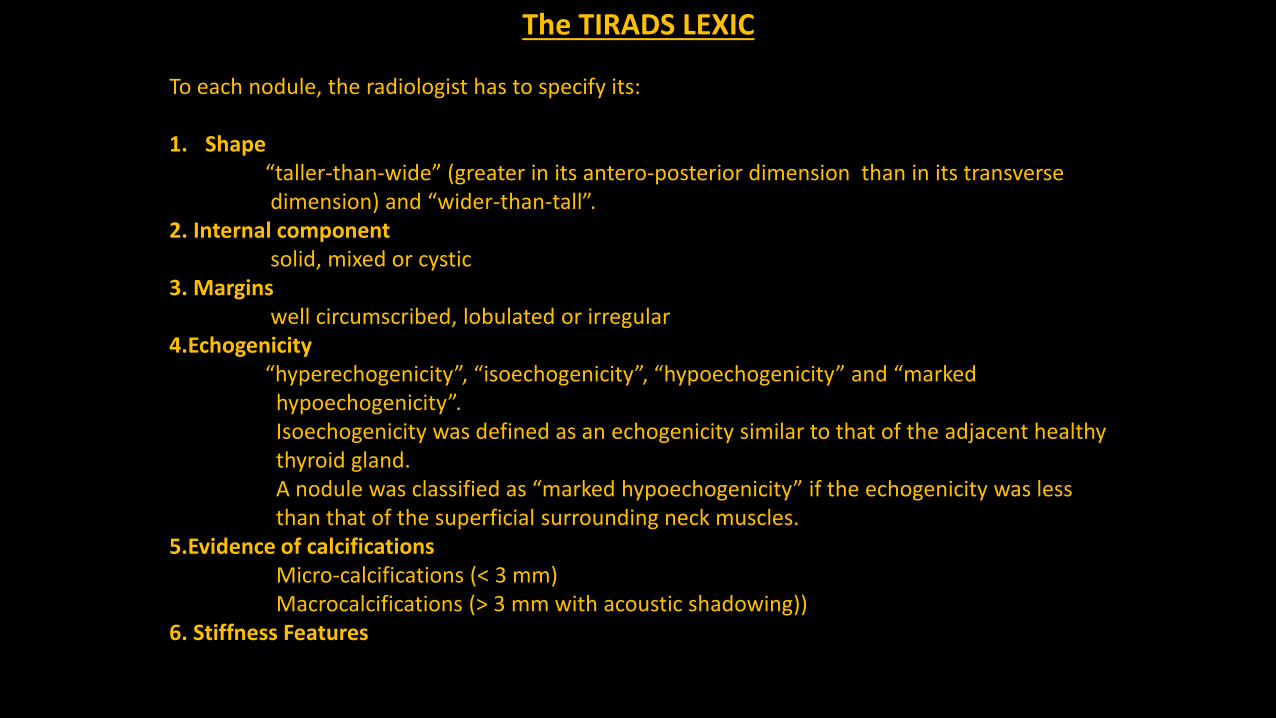
The TIRADS LEXIC
To each nodule, the radiologist has to specify its:
1. Shape“taller-than-wide” (greater in its antero-posterior dimension than in its transverse dimension) and “wider-than-tall”.
2. Internal componentsolid, mixed or cystic
3. Marginswell circumscribed, lobulated or irregular
4.Echogenicity“hyperechogenicity”, “isoechogenicity”, “hypoechogenicity” and “marked
hypoechogenicity”.Isoechogenicity was defined as an echogenicity similar to that of the adjacent healthy thyroid gland. A nodule was classified as “marked hypoechogenicity” if the echogenicity was less than that of the superficial surrounding neck muscles.
5.Evidence of calcificationsMicro-calcifications (< 3 mm) Macrocalcifications (> 3 mm with acoustic shadowing))
6. Stiffness Features

TIRADS classification(modified Russ classification)
TIRADS 1 - Normal thyroidTIRADS 2 - Benign aspects (0% chance of malignancy)
Simple cystSpongiform nodule‘White Knight’ aspectIsolated macrocalcificationTypical sub acute thyroiditis
TIRADS 3 - Probably benign aspects (<5% chance of malignancy)
None of the highly suspicious aspectsIsoechogenicHyperechogenic
TIRADS 4A - Low suspicious aspects (5-10% chance of malignancy)
None of the highly suspicious aspectsModerately hypoechogenic
TIRADS 4B / 5: High suspicious aspectsTaller than wide shapeIrregular or microlobulated marginsMicrocalcificationsMarked hypoéchogenicityHigh stiffness index with elastography (if available ) * 4B: 1 or 2 signs and no adenopathy (10-80% chance of malignancy)
* 5: 3 or more signs and/or adenopathy (>80% chance of malignancy)
TIRADS 6 – Biopsy proven malignant nodules
All studies show that most cancers were found in the TIRADS 3, 4 and 5 categories.
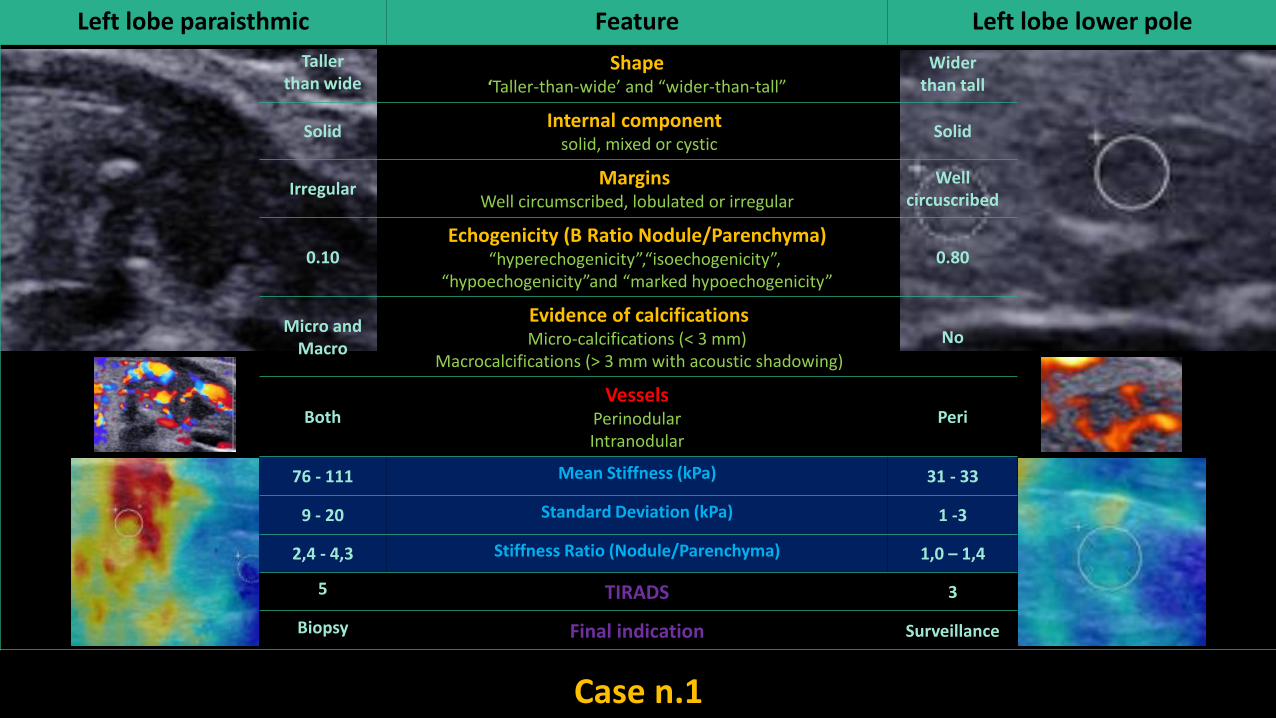
Left lobe paraisthmic Feature Left lobe lower pole
Tallerthan wide
Shape‘Taller-than-wide’ and “wider-than-tall”
Widerthan tall
SolidInternal component
solid, mixed or cysticSolid
IrregularMargins
Well circumscribed, lobulated or irregular
Wellcircuscribed
0.10Echogenicity (B Ratio Nodule/Parenchyma)
“hyperechogenicity”,“isoechogenicity”,“hypoechogenicity”and “marked hypoechogenicity”
0.80
Micro and Macro
Evidence of calcificationsMicro-calcifications (< 3 mm)
Macrocalcifications (> 3 mm with acoustic shadowing)
No
BothVessels
PerinodularIntranodular
Peri
76 - 111 Mean Stiffness (kPa) 31 - 33
9 - 20 Standard Deviation (kPa) 1 -3
2,4 - 4,3 Stiffness Ratio (Nodule/Parenchyma) 1,0 – 1,4
5 TIRADS 3
Biopsy Final indication Surveillance
Case n.1

Right lobe Feature Left lobe
Widerthan tall
Shape‘Taller-than-wide’ and “wider-than-tall”
Widerthan tall
SolidInternal component
solid, mixed or cysticSolid
LobulatedMargins
Well circumscribed, lobulated or irregular Lobulated
0.45Echogenicity (B Ratio Nodule/Parenchyma)
“hyperechogenicity”,“isoechogenicity”,“hypoechogenicity”and “marked hypoechogenicity”
0.59
Micro and Macro
Evidence of calcificationsMicro-calcifications (< 3 mm)
Macrocalcifications (> 3 mm with acoustic shadowing)
Micro
BothVessels
PerinodularIntranodular
Both
42 -71 Mean Stiffness (kPa) 28 - 66
4,0 - 11,2 Standard Deviation (kPa) 1,2 - 9,7
2,9 – 5,2 Stiffness Ratio (Nodule/Parenchyma) 1,2 – 3,8
5 TIRADS 4B
Biopsy Final indication Biopsy
Case n.2

SSI 15-4 MHz Probe Case n.1 Case n.2
SWE Features Paraisthmic nodule Lower pole nodule Right lobe nodule Left lobe nodule
Mean stiffness (kPa) 58-72 31-33 42-71 28-66
Maximum stiffness (kPa) 76-111 36-43 68-77 32-69
Minimum stiffness (kPa) 26-41 25-31 15-63 11-63
Standard Deviation (kPa) 9-20 1-3 4-11 1-9
Ratio 2,4-4,3 1,0-1,4 2,9-5,2 1,2-3,8
TIRADS 5 3 5 4B
Final indication Biopsy Surveillance Biopsy Biopsy
FNA TIR 5 (Thy VI) Not performed TIR 4 (Thy V) Not performed
Pathological diagnosis Malignant (PTC) Benign Malignant (PTC) Malignant (PTC)
Keypoints of the cases and ‘take home messages’
Shear wave elastography one more time shows its reliability in identifying stiff thyroid nodules alsowith small volume (< 1 cm) and in the guidance of the FNAC, like in this cases of three small PTCs.
It correctly characterize as ‘soft’ the only one benign nodule (one on four).

Keypoints of the cases and ‘take home messages’
While Papillary cancers are usually stiff, Follicular cancers can be soft.
This cases show one more time that small nodules can be cancer, while large nodules can be benign.
Uptodate my impression is that we cannot rely on absolute number because they change dependingon too many variables (frequency of the probe, speed of sound selected, grade of compression youdo with your hand, depth of the lesion and surrounding environment, and so on) and , sure, becausewe well know that cancers can be 'soft' and benign lesions can be stiff.
My actual belief is that large more reliable in addressing our impression are two other parameters (or features) : 1) Standard Deviation (higher in malignant lesions cause of their almost constant inhomogeneity)
2) Elasticity Ratio Vs a standard reference tissues.
Well, while the kPa's numbers (E-mean, min and max) can be very variable, SD and Ratio remain unmodified, unconditioned by the above mentioned factors.
I think that international guidelines on the indications to thyroid biopsy should be rediscussed(at least regarding the dimensions) and that, on the other side, we should analyze the real risk of overdiagnosis and overtreatment in these situations.
In conclusion nowadays advanced ultrasonography offers so many tools that it would be unsafe to rely the diagnostic workup only on one of the US modes (B-mode, Doppler and sonoelastography).
Uptodate TIRADS is based on all these informations that make ultrasonography to deserve in full the definition of ‘Multiparametric Diagnostic Modality’.

Ultrasonography of thyroid focal diseases : a true Multiparametric Diagnostic Modality
Mode Features Informations
B Mode
Shape‘Taller-than-wide’ and “wider-than-tall”
Morphologyand
Structure
Internal componentsolid, mixed or cystic
MarginsWell circumscribed, lobulated or irregular
Echogenicity (B Ratio Nodule/Parenchyma)“hyperechogenicity”,“isoechogenicity”,
“hypoechogenicity”and “marked hypoechogenicity”
Evidence of calcificationsMicro-calcifications (< 3 mm)
Macrocalcifications (> 3 mm with acoustic shadowing)
Doppler ModeCDI, PDI , dPDI Number, density and distribution of the vessels Vascular
Pulsed Wave Blood flow characterisation and quantification Blood Flow – Functional (?)
SonoelastographyStrain Relative Stiffness
Mechanical propertiesShear Wave Relative stiffness and Stiffnes quantification

Antonio Pio MasciotraCampobasso – Molise – Italy
Website www.masciotra.net
YouTube Channel https://www.youtube.com/channel/UCgCj21nKGAhR997Ia3-QegQ
Thanks for your attention
Related Documents











