Overview of current KCNQ2-related epilepsy research at BCM Kristen Park, MD Colorado Children’s Univ. of Colorado Univ. John Millichap, MD Lurie Children’s Northwestern Univ. Ed Cooper, MD, PhD Associate Professor Neurology, Neuroscience, Molecular & Human Genetics BCM, Houston TX NINDS, AES CURE, Jack Pribaz GSK

Dr. ed cooper kcnq2 summit professional track learn more at kcnq2summit.org
Jul 15, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Overview of current KCNQ2-related
epilepsy research at BCM
Kristen Park, MD
Colorado Children’s
Univ. of Colorado Univ.
John Millichap, MD
Lurie Children’s
Northwestern Univ.
Ed Cooper, MD, PhD
Associate Professor
Neurology, Neuroscience,
Molecular & Human Genetics
BCM, Houston TX
NINDS,
AES
CURE,
Jack Pribaz
GSK

KCNQ2-related epilepsy: paradigm for
translating a well-established mechanism into
effective personalized epilepsy care
I. “Fill in” mechanistic understanding
II. “Reach out” across disciplines
III. “Fit in” to broader questions and medical
needs

“Filling in” mechanistic understanding
1. What are KCNQ2 (and KCNQ3)?
2. What do KCNQ2 mutations do?
3. Are there mechanism-based approaches to
therapy?
Li Li Mingxuan
Xu
Baouyen
TranZhigang Ji
Maarten Kole
What are KCNQ2 and KCNQ3?
1. Two of ~100 genes encoding potassium (K+)
channel subunits
2. The KCNQ2 and 3 names are used both for the
gene and the protein product, but Kv7.2 (3) are
alternative names for the protein products
3. KCNQ1 mutations cause the largest subset of
cases of inherited long QT. KCNQ4 mutations
causes a form of inherited childhood onset
deafness. KCNQ5 (no diseases known).
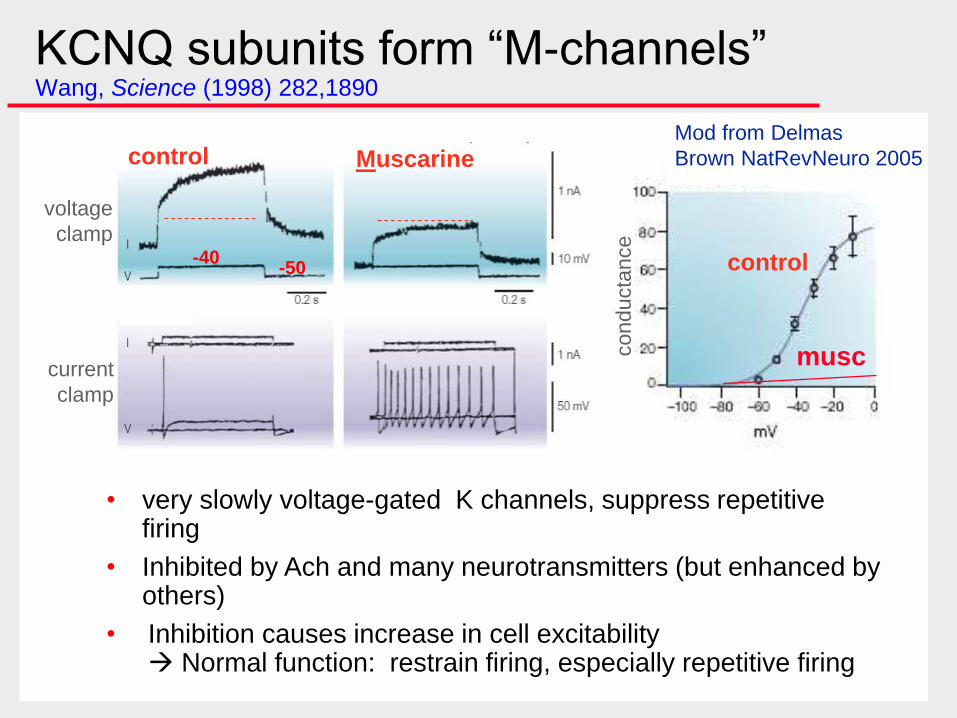
KCNQ subunits form “M-channels” Wang, Science (1998) 282,1890
• very slowly voltage-gated K channels, suppress repetitive firing
• Inhibited by Ach and many neurotransmitters (but enhanced by others)
• Inhibition causes increase in cell excitability Normal function: restrain firing, especially repetitive firing
musc
control
control Muscarine
current
clamp
voltage
clamp
conducta
nce
-40-50
Mod from Delmas
Brown NatRevNeuro 2005
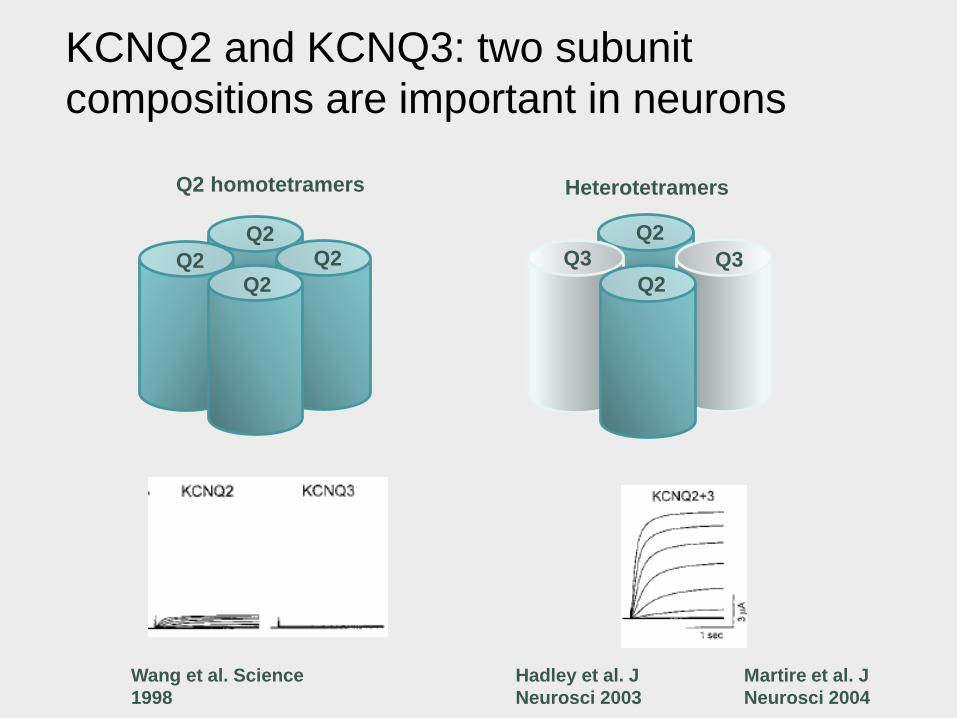
KCNQ2 and KCNQ3: two subunit
compositions are important in neurons
Q2 homotetramers
Q2Q2
Q2Q2
Heterotetramers
Q3
Q2
Q2
Q3
Wang et al. Science
1998
Hadley et al. J
Neurosci 2003
Martire et al. J
Neurosci 2004
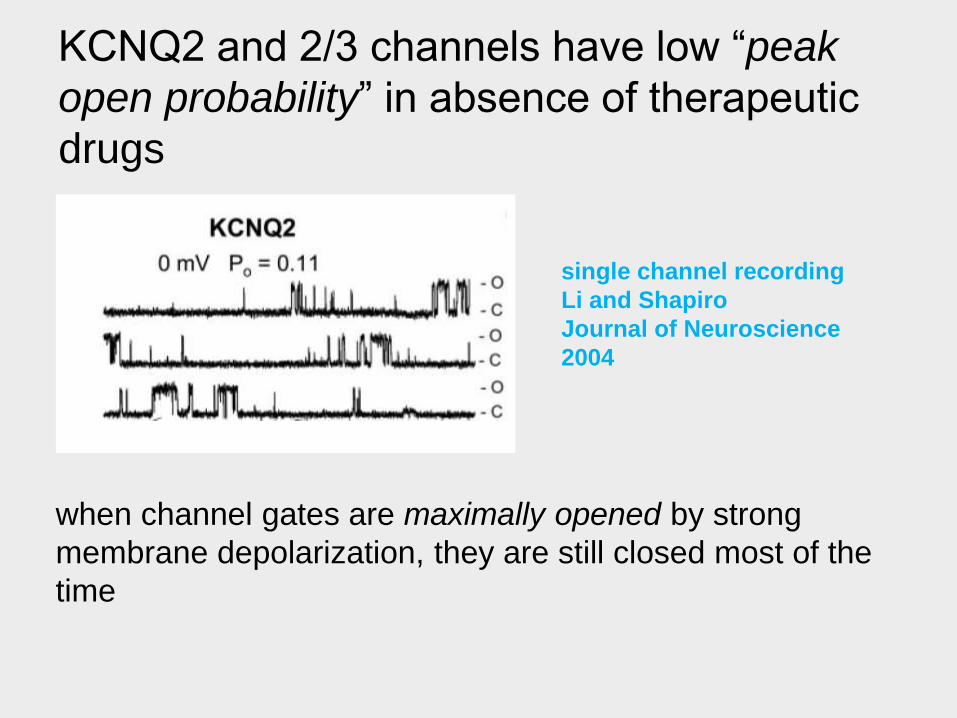
KCNQ2 and 2/3 channels have low “peak
open probability” in absence of therapeutic
drugs
when channel gates are maximally opened by strong
membrane depolarization, they are still closed most of the
time
single channel recording
Li and Shapiro
Journal of Neuroscience
2004
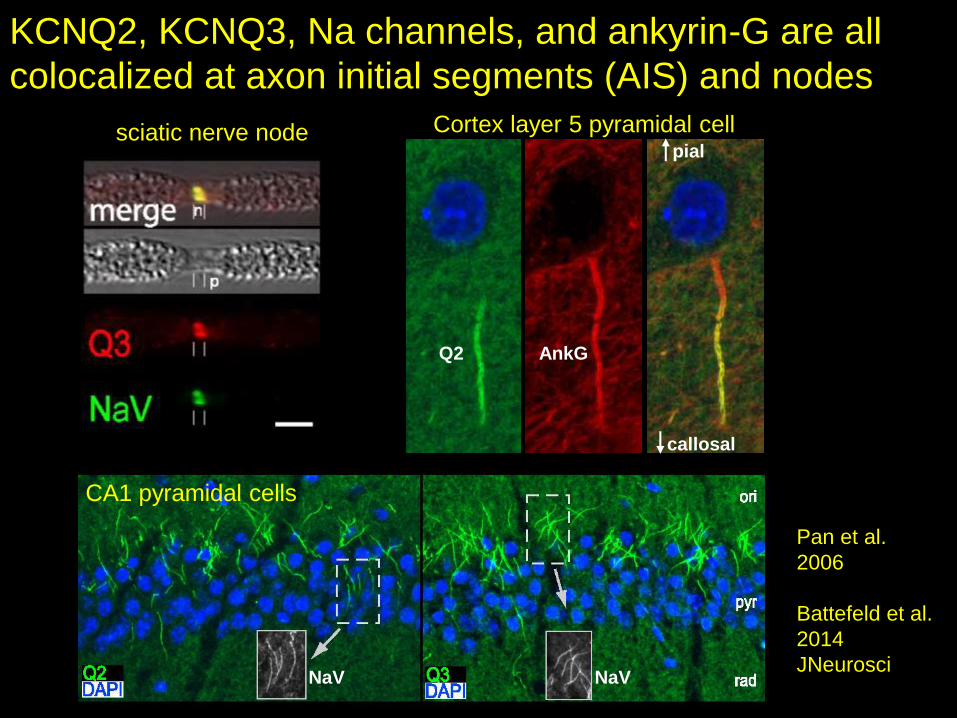
KCNQ2, KCNQ3, Na channels, and ankyrin-G are all
colocalized at axon initial segments (AIS) and nodes
Cortex layer 5 pyramidal cell
Q2 AnkG
pial
callosal
CA1 pyramidal cells
NaV NaV
sciatic nerve node
Pan et al.
2006
Battefeld et al.
2014
JNeurosci

KCNQ2/KCNQ3 at AISs are functional M-channels
Battefeld et al. 2014 JNeurosci
Bao
Tran
Houston
Maarten
Kole
Amsterdam
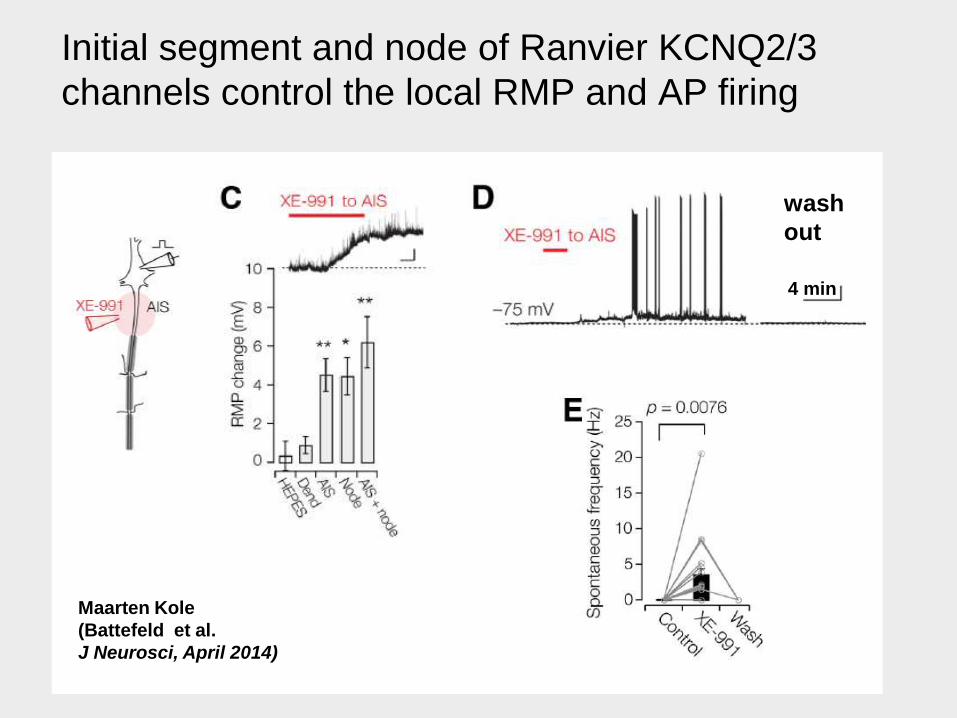
Initial segment and node of Ranvier KCNQ2/3
channels control the local RMP and AP firing
Maarten Kole
(Battefeld et al.
J Neurosci, April 2014)
wash
out
4 min
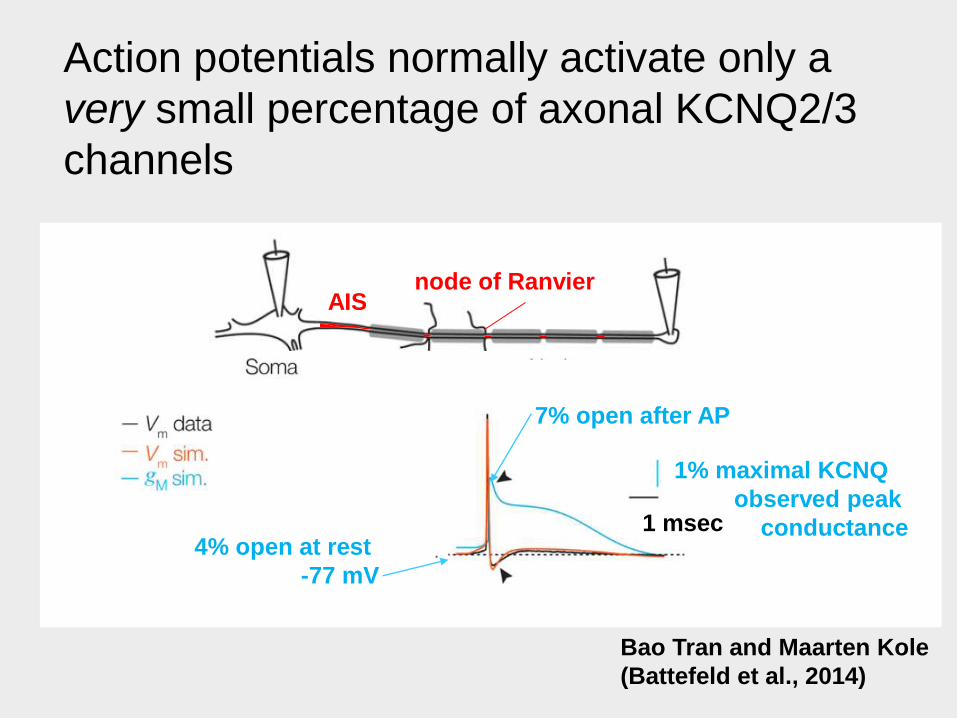
Action potentials normally activate only a
very small percentage of axonal KCNQ2/3
channels
1% maximal KCNQ
observed peak
conductance1 msec
Bao Tran and Maarten Kole
(Battefeld et al., 2014)
4% open at rest
-77 mV
AISnode of Ranvier
7% open after AP

Why do some KCNQ2 mutations cause mild,
but others cause severe disease?
Severe mutations are heterozygous and
missense–substitution of one aa in one of 2
KCNQ2 genes
to understand these, must think about how
channel primary sequence is assembled into a
3 dimensional structure (4 subunits x 872
aa/subunit)

“Macro”anatomy of a voltage-gated ion
channel
outside
inside
sensor
+
Resting potential: closed
gate
--
+
open
-70 mV -30 mV-
- -
++
- -
+
K+
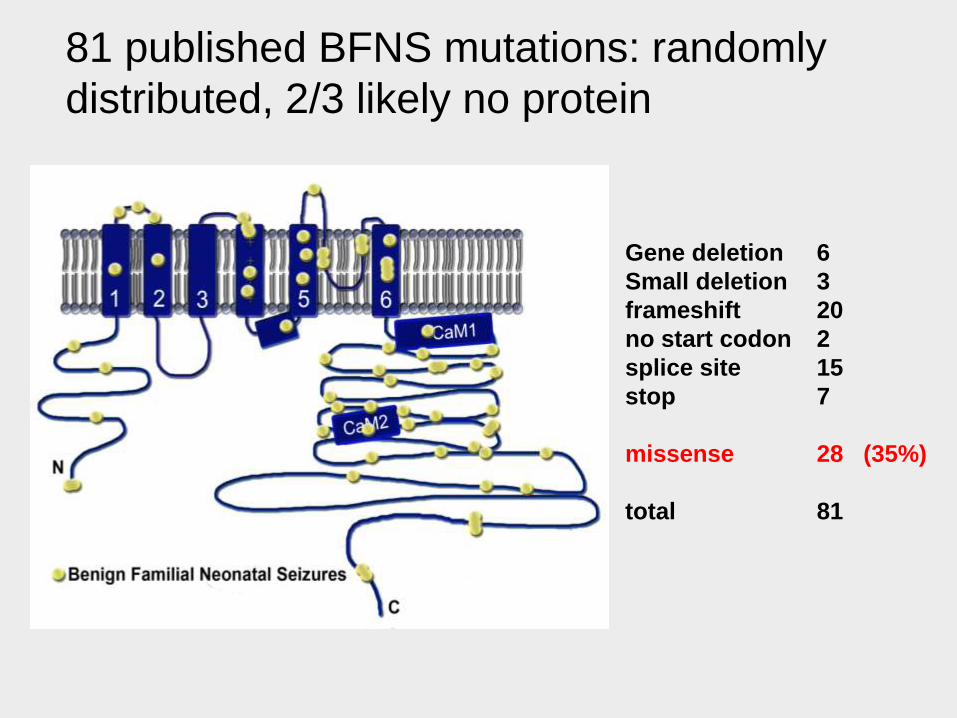
81 published BFNS mutations: randomly
distributed, 2/3 likely no protein
Gene deletion 6
Small deletion 3
frameshift 20
no start codon 2
splice site 15
stop 7
missense 28 (35%)
total 81

The first few encephalopathy mutations suggested
a mechanism: 3 functional “Achilles’ heels”
Weckhuysen... Berkovic , Scheffer, de Jonghe, 2012; Millichap and Cooper, 2012
T274M

The first few encephalopathy mutations suggested
a mechanism: 3 functional “Achilles’ heels”
Millichap and Cooper 2012
ER
golgi
plasma
membrane
calmodulin
X
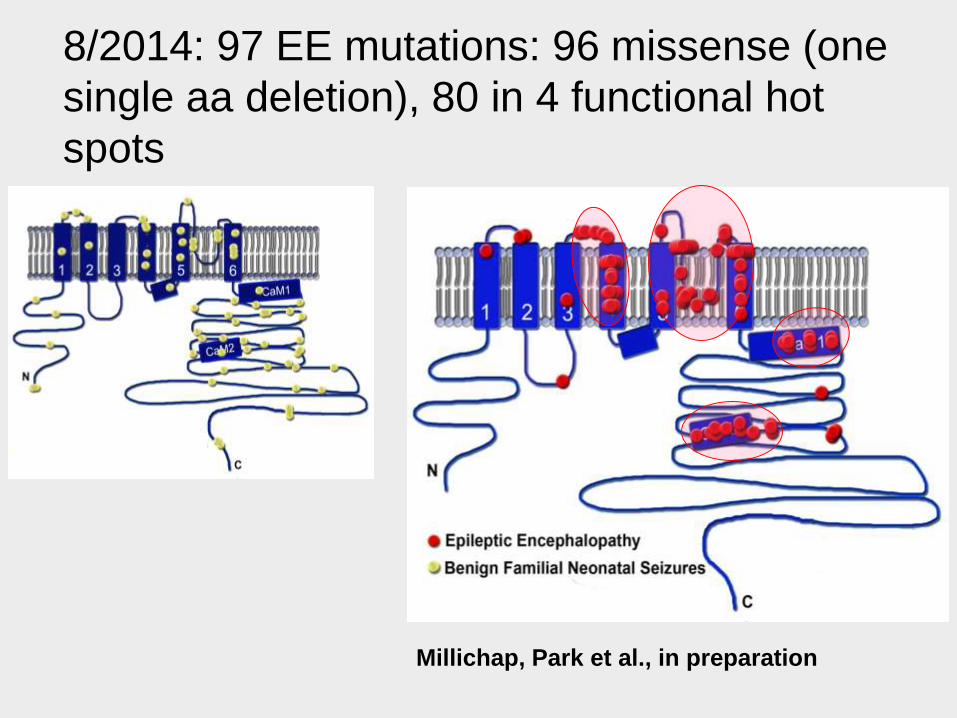
8/2014: 97 EE mutations: 96 missense (one
single aa deletion), 80 in 4 functional hot
spots
Millichap, Park et al., in preparation
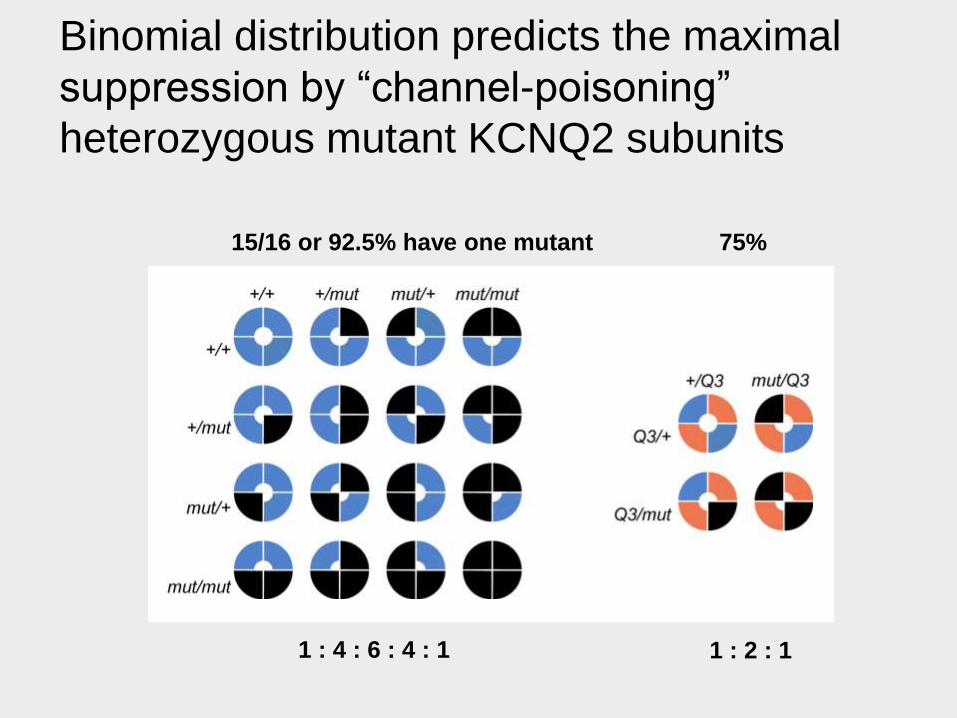
Binomial distribution predicts the maximal
suppression by “channel-poisoning”
heterozygous mutant KCNQ2 subunits
15/16 or 92.5% have one mutant 75%
1 : 4 : 6 : 4 : 1 1 : 2 : 1

T274M introduces a bulkier side-chain near the pore
Threonine (T) medium sizeMethionine (M) Slightly bigger
T274M
Rationale for drug treatment (summary)
1. Due to low peak open probability and slow voltage-
dependent gating, neurons use only small fraction of
.3 to 3% of KCNQ2 and KCNQ2/3 maximal capacity
2. With a efficacious enough drug, should be able to
increase activity considerably, even if only 1/16 of the
channels are capable of responding
3. 8-fold difference between worst predicted mutant
suppression and BFNS, a mild transient condition.

Retigabine/ezogabine and ICA-069673
promote channel opening through effects at
distinct sites
ICA binding site
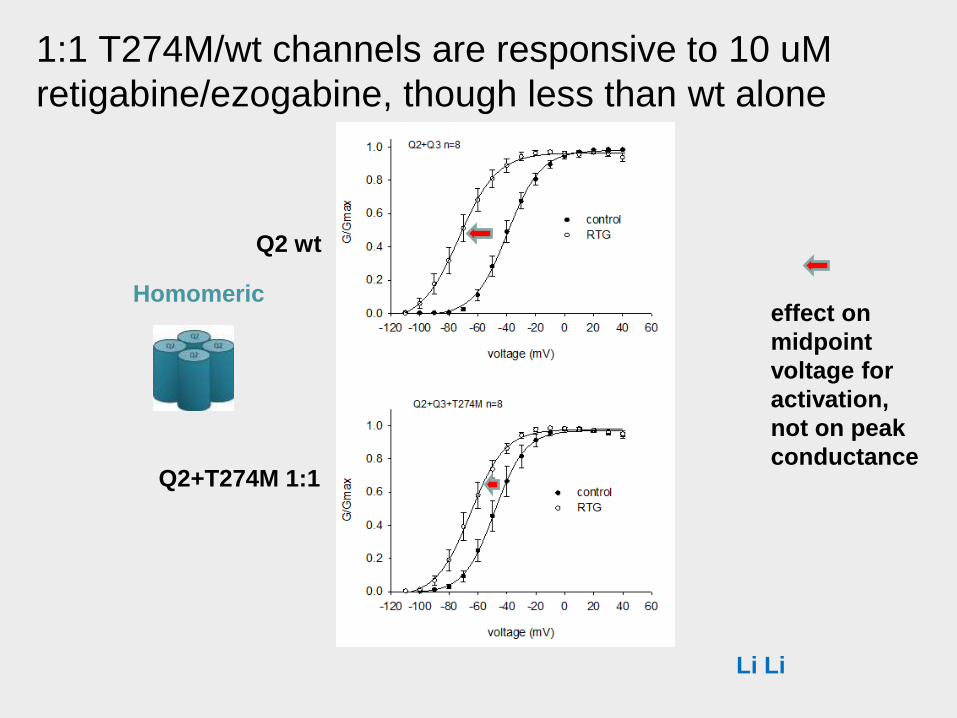
1:1 T274M/wt channels are responsive to 10 uM
retigabine/ezogabine, though less than wt alone
Li Li
Homomericeffect on
midpoint
voltage for
activation,
not on peak
conductance
Q2 wt
Q2+T274M 1:1

Bringing lab insights back to the clinic
1. What are KCNQ2 (and KCNQ3)?“natural anti-seizure function”
very slightly activated under physiological conditions
2. What do KCNQ2 mutations do?strongly suppress currents
some residual WT channels remain
3. Are there mechanism based approaches to
therapy?2 drugs potently and synergistically enhance currents
many other drugs in preclinical stages
no good data: pediatric safety, dosing, efficacy
The RIKEE project:
1. -Rational Intervention for KCNQ2 Epileptic
Encephalopathy: our efforts are focused on
developing and testing therapies
2. Completed: retrospective physician survey-
based study (23 patients/11 centers)
3. Just launched: IRB approved program of
prospective research including a patient
registry and website
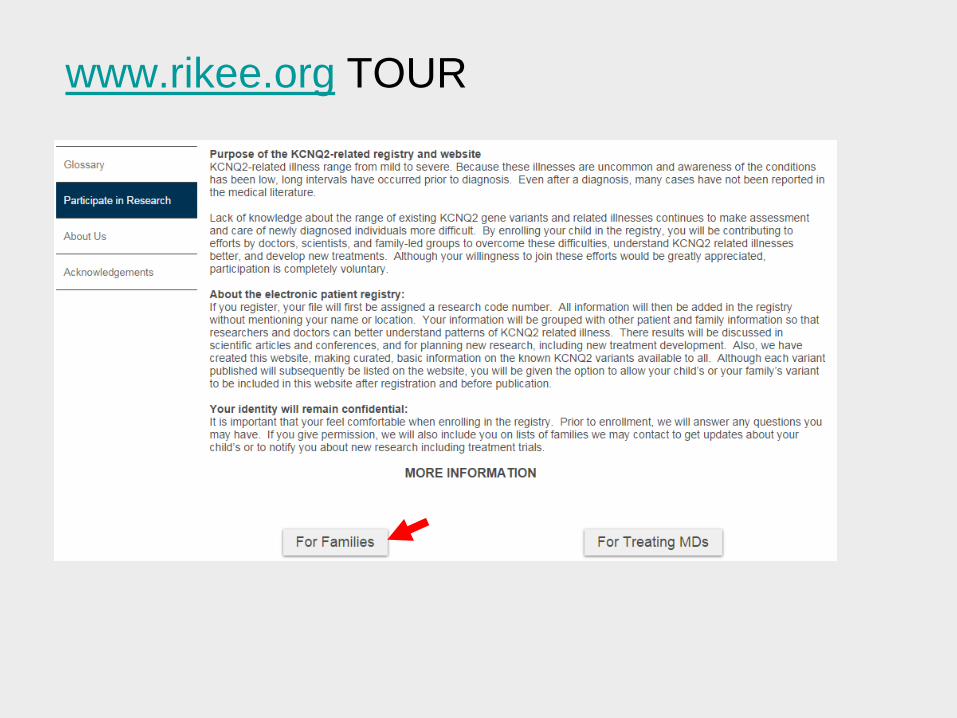
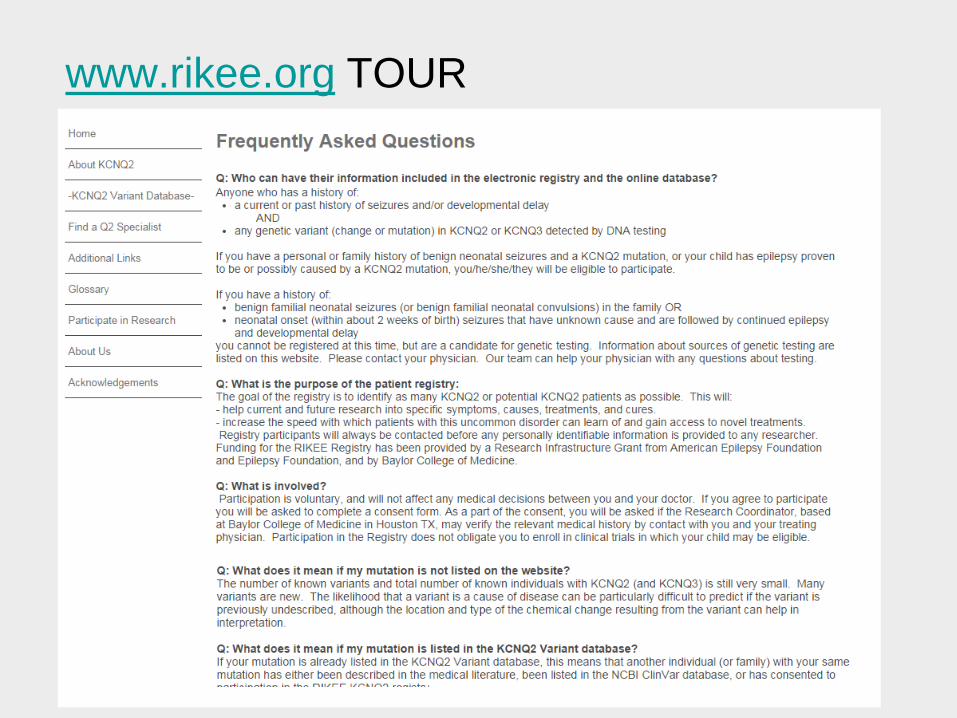
Why a website, why a registry, and how are
the two different?
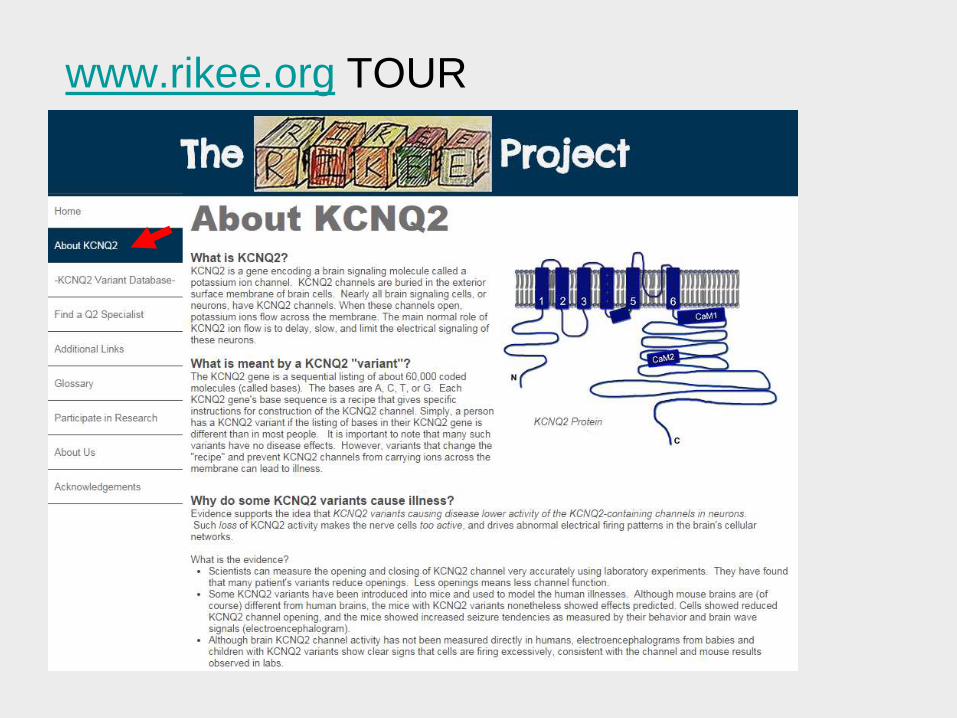
RIKEE Website
1. Information on all known
KCNQ2 and KCNQ3
variants
2. No personally
identifiable information
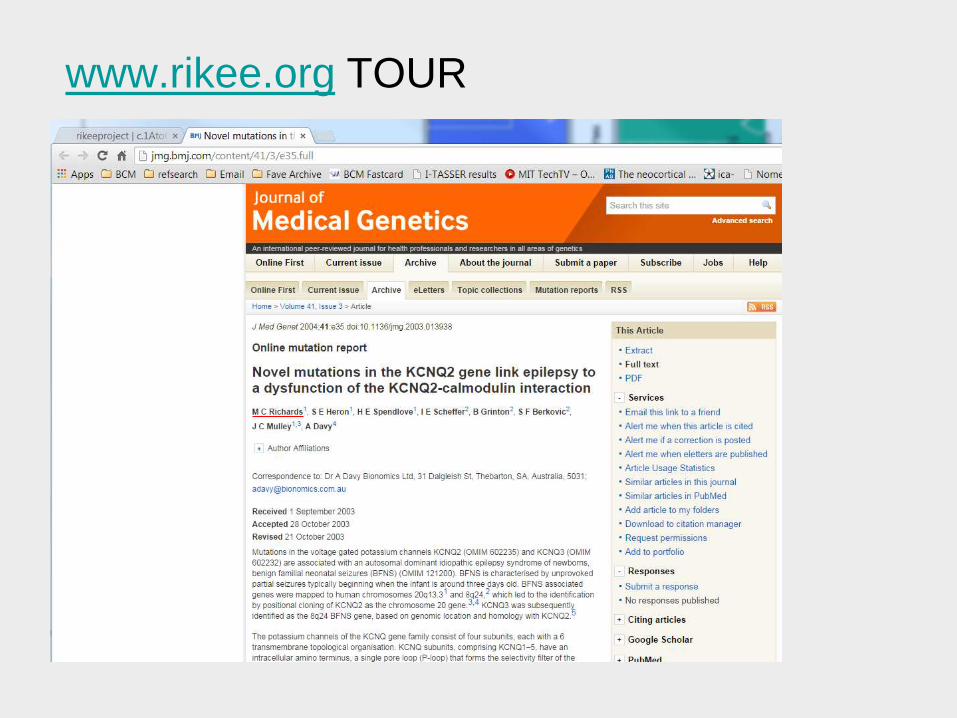
3. Extensive links to
scientific literature and
other resources
4. Curated by expert team
for use by all
5. “Complementary” model
KCNQ2 Registry
1. Information on patients
registered after informed
consent
2. At entry, permission to
recontact may be given
3. Clinical information
coded so can be
accessed for IRB
approved research but
personal information not
generally available
Building the registry and website: many
steps
1. Many documents require review and approval: protocol
summary, letters to MDs and patients, data entry forms,
advertisements, webpages...
2. In every case, family must initiate contact (MDs can
recommend to pt, not to us)
3. Informed consent requires direct conversation with our
team before enrollment
4. Procedures for receipt of information, encryption,
computer hardware/software
All designed to preserve patient autonomy, privacy
RIKEE clinical registry/website team
1. Cooper Lab
• Nishtha Joshi, MPH – coordinator
• Mia Cooper, BA – project intern
2. ICTR staff
• Alicia Brown, MPH, CCRP - regulatory
• Uma Ramamurthy, PhD - database
• Wren Pratt, BA, CCRC - coordination



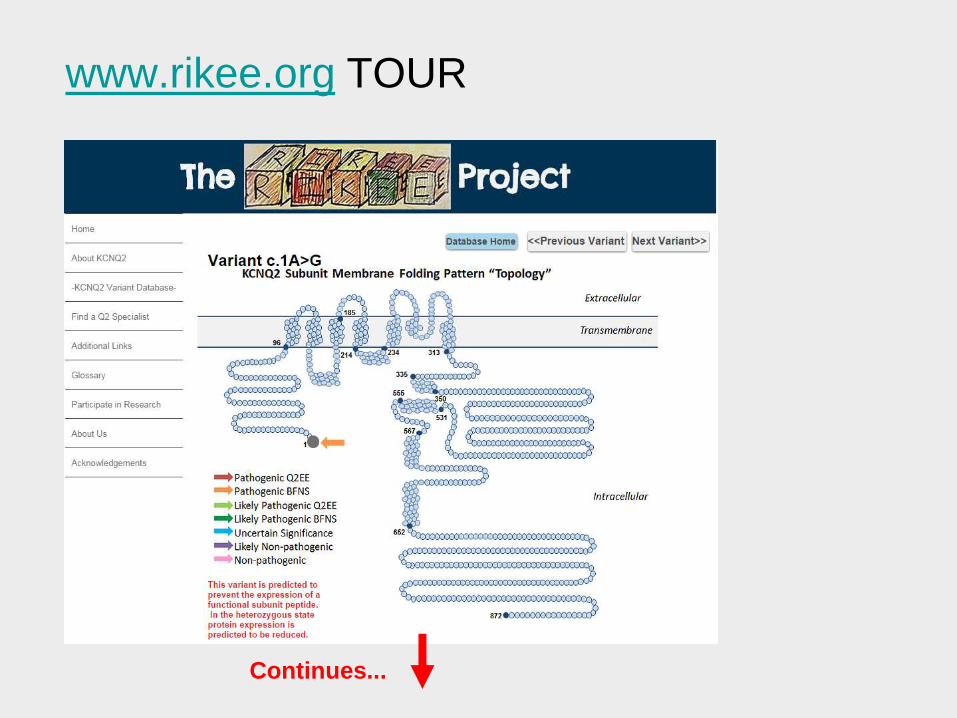
www.rikee.org TOURAll published variants
Unpublished variants
if permission granted
Reaching out: across disciplines & beyond
1. Clinical pediatric epileptologists neonatal
neurologists, neonatologists, others
2. Clinical Geneticists have a distinctive important
role
• Need for validated classification criteria
(ClinGen/NCBI ClinVar), rapid sequencing
test
3. Parents: network has rapidly globalized
4. Industry
5. Media
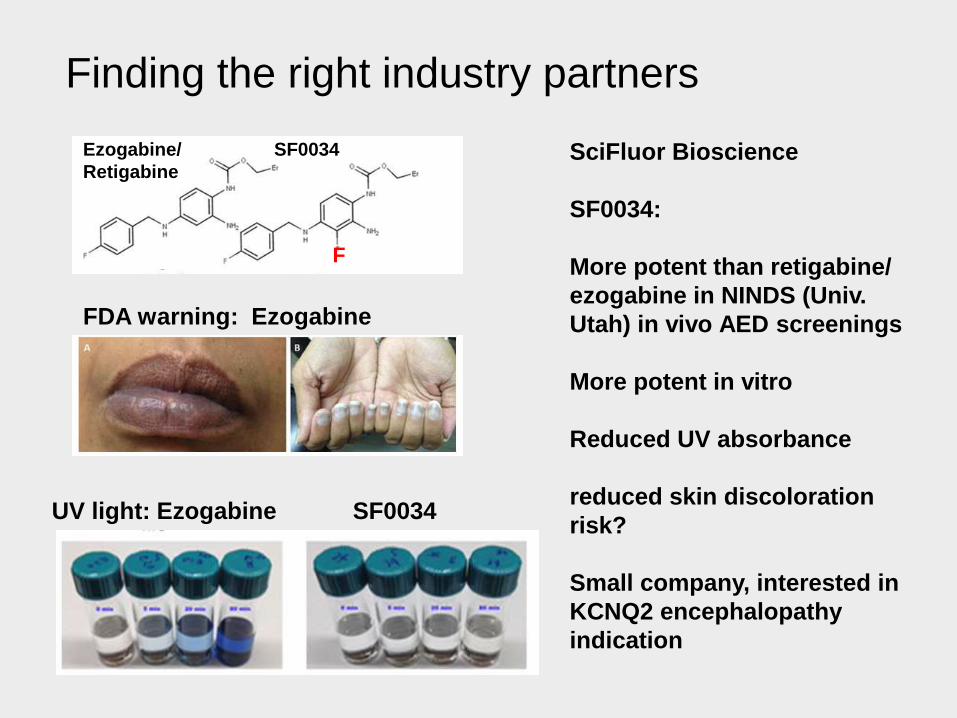
Finding the right industry partners
UV light: Ezogabine SF0034
SciFluor Bioscience
SF0034:
More potent than retigabine/
ezogabine in NINDS (Univ.
Utah) in vivo AED screenings
More potent in vitro
Reduced UV absorbance
reduced skin discoloration
risk?
Small company, interested in
KCNQ2 encephalopathy
indication
F
Ezogabine/
Retigabine
SF0034
FDA warning: Ezogabine

Linking up/Fitting in
KCNQ2-related
Epilepsy
Symptomatic
neonatal seizures
(Yogendra Raol,
Col Children’s)
Other “Severe Early
Life Epilepsies”--
Ohtahara, EMEGeneralized epilepsy
(Jackie French NYU,
Atul Maheshwari,
BCM)
Adult partial
epilepsy
Non-neonatal
syndromes w/
distinctive biologies

Summary
1. KCNQ2 encephalopathy is a new subtype of
neonatal-onset epilepsy with moderate to
profound global delay: de novo, missense
variants
2. First handful of mutations: dominant-negative
fitting mathematical/structural model
3. In vitro, drugs seem to work. In vivo, no
controlled studies but some promise
4. Infrastructure for longitudinal observational
studies and trials being built
5. Case number is still low for trials, requires
improved ascertainment

AcknowledgementsKCNQ2 families and supporters
BCM
Mingxuan Xu, Bao Tran, Li Li, Zhigang Ji
RIKEE Network
Lionel Carment, Universite de Montreal Marc Patterson, Mayo
Eric Marsh, Xilma Ortiz-Gonzalez, Emily Robbins Children’s Hospital of Philadelphia Bruria Ben Ze’ev Tel Aviv Molly Tracy Hasbro Children’s, Brown Univ.
Tammy Tsuchida, Phil Pearl (now BCH), Children’s National (DC)
John Millichap, Lurie Children’s (Northwestern U.)
Kristen Park, Paul Levisohn, Colorado Children’s (Aurora, CO)
Brenda Porter, Packard Children’s (Stanford)
Other Collaborations
UPENN
Zongming Pan Steve Scherer Amy Brooks-Kayal
Tingching Kao Steve Cranstoun Yogi Raol
Van Bennett (Duke) Jurgen Schwarz (Hamburg) Hugh Bostock (UCL) Ryuji Kaji(Tokushima) Yasushi Okamura, Atsuo Nishino (NIPS) Maarten Kole (Amsterdam, NIN) David Brown (UCL), Mala Shah (UCL)
Funding: NINDS, Miles Family Fund, AES/EF, Jack Pribaz Foundation, CURE, GSK
Related Documents











