Dr Annie NK Chiu United Christian Hospital Joint Hospital Surgical Grand Round 20 th Apr 2013

Dr Annie NK Chiu United Christian Hospital Joint Hospital Surgical Grand Round 20 th Apr 2013.
Dec 16, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Dr Annie NK ChiuUnited Christian Hospital
Joint Hospital Surgical Grand Round20th Apr 2013

IntroductionThyroid surgery is a common operation
1751 thyroid operations in 2011/12 in HA hospitalsPostoperative hypocalcemia is one of the most
common complications after total or completion thyroidectomy
Temporary: 1.6% - 50%Permanent (> 6 months): 0.5% - 2%
1. Surgical outcomes monitoring & improvement program (SOMIP) report. Vol 4 Jul 2011-Jun 20122. Reeve T, Thompson NW. Complications of thyroid surgery: how to avoid them, how to manage
them, and obsevations on their possible effect on the whole patient. World J Surg. 2000; 24(8): 971-975
Post-thyroidectomy HypocalcemiaMultifactorialHypoparathyroidism – most important cause
StunningDevascularizationInadvertent resection

Post-thyroidectomy HypocalcemiaIncreased risk of postoperative hypocalcemia
Malignant diseaseCentral neck dissectionDocumented resection of parathyroid gland at
operation (with or without autotransplantation)
Landry CS et al. Predictable criteria for selective, rather than routine, calcium supplementation following thyroidectomy. Arch Surg 2012; 147(4): 338-344

ManagementMonitoring clinical symptoms and signs of hypocalcemiaDaily monitoring serum calcium levelManifestation 24 – 48 hours after operation, may be
delayed up to several daysProlonged hospitalization

Does routine calcium supplement prevent post-thyroidectomy hypocalcemia?

Routine Supplements after ThyroidectomyThere are 2 small RCTsOral calcium +/- vitamin D supplementsSignificantly fewer patients developed hypocalcemiaMilder symptoms of hypocalcemiaAllows earlier discharge
1. Bellantone R et al. Is routine supplementation therapy (calcium and vitamin D) useful after total thyroidectomy? Surgery 132: 1109-1112; discussion 1112-1103
2. Roh JL et al. Routine oral calcium and vitamin D supplements for the prevention of hypocalcemia after total thyroidectomy. Am J Surg 192: 675-678

Pitfalls
Over treatMultiple doses per daySerial laboratory tests for monitoringAdverse effects of unnecessary calcium supplement:
Nausea, decreased appetite, constipationHypercalcemia – suppress parathyroid function


Parathyroid Hormone (PTH)Hypoparathyroidism – most important cause for
post-thyroidectomy hypocalcemia
PTH half-life: 2-5 minutes
Hypothesis – perioperative PTH level predicts post-thyroidectomy hypocalcemia


Questions to be answeredHow accurate
When to measureWhat cutoff value
How to apply

Early prediction of postthyroidectomy hypocalcemia by one single iPTH measurement.Lombardi CP et al. Surgery 2004; 136: 1236-1241
Prospective study53 patients underwent total or completion
thyroidectomyiPTH < 10 pg/mL (normal range 10-65 pg/mL) at 4
and 6 hours postop correctly predicted hypocalcemiaSensitivity 94%, specificity 100%, overall accuracy
98%

Parathyroid hormone early percent change: an individualized approach to predict postthyroidectomy hypocalcemiaChapman DB et al. Am J Otolaryngol 2012; 33: 216-220
Retrospective study52 patients underwent total or completion
thyroidectomy>44% decrease in PTH level at 6-hour postop
→Likely to develop hypocalcemia, sensitivity 100%Likewise, if <44% decrease in PTH level at 6-hour,
patients can be considered safe for early discharge

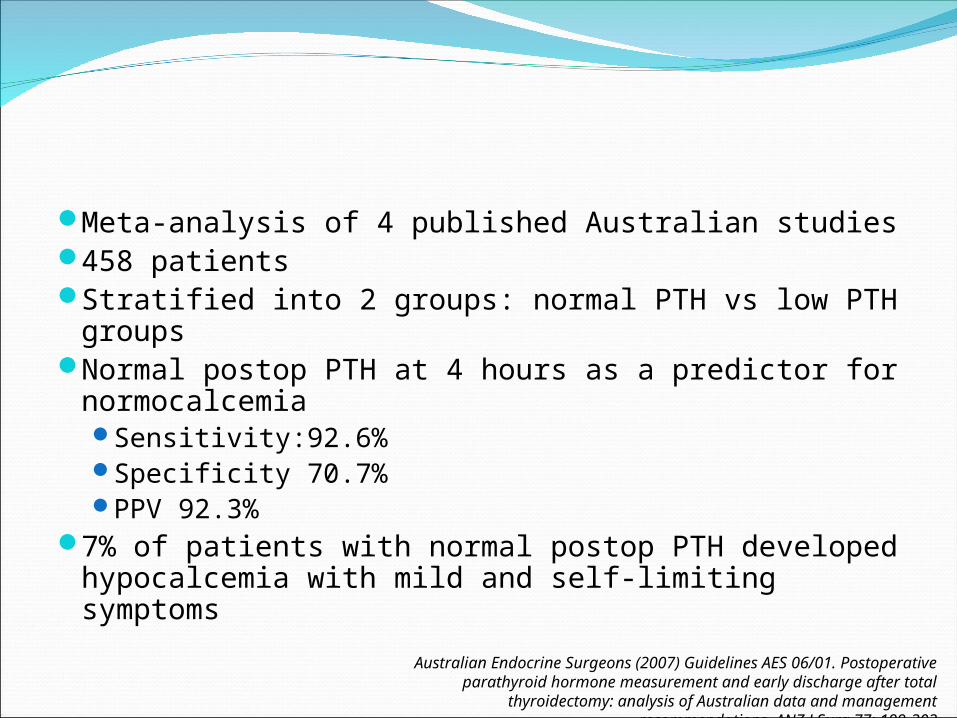
Meta-analysis of 4 published Australian studies458 patientsStratified into 2 groups: normal PTH vs low PTH groupsNormal postop PTH at 4 hours as a predictor for
normocalcemiaSensitivity:92.6%Specificity 70.7%PPV 92.3%
7% of patients with normal postop PTH developed hypocalcemia with mild and self-limiting symptoms
Australian Endocrine Surgeons (2007) Guidelines AES 06/01. Postoperative parathyroid hormone measurement and early discharge after total thyroidectomy: analysis of
Australian data and management recommendations. ANZ J Surg 77: 199-202

Evidence for the Role of Perioperative PTH Measurement after Total Thyroidectomy as a Predictor of HypocalcemiaGrodski S et al. World J Surg 2008; 32: 1367-1373
Systemic review, a Medline search of English language literature
Issues addressed:Accuracy of PTH in predicting hypocalcemiaOptimal timing for measuring PTH

Accuracy of PTH24 case series, 3 case-control trialsMajor differences in study designs and dataSome studies excluded patients with Graves’ disease or
thyroid cancer with central neck dissectionStrong correlation of postop PTH with hypocalcemia after
thyroidectomy
Grodski S et al. Evidence for the role of perioperative PTH measurement after total thyroidectomy as a predictor of hypocalcemia. World J Surg 2008; 32: 1367-1373

Accuracy of PTHRecommendations (Grade C):
Post-thyroidectomy PTH levels accurately predict hypocalcemia but lack 100% accuracy
Both absolute levels and percentage decline showed similar accuracy
Progressive and severe hypocalcemia is unlikely if normal postop PTH
Facilitates early supplementation therapyFacilitates early and safe discharge
Grodski S et al. Evidence for the role of perioperative PTH measurement after total thyroidectomy as a predictor of hypocalcemia. World J Surg 2008; 32: 1367-1373

Timing of PTH Sample4 case series10 minutes to 24 hours postopHalf-life of PTH: 2 – 5 minutesNo difference in PTH levels at early postoperative
period and days after operation
Grodski S et al. Evidence for the role of perioperative PTH measurement after total thyroidectomy as a predictor of hypocalcemia. World J Surg 2008; 32: 1367-1373

Timing of PTH SampleRecommendation (Grade C):
A single PTH measurement taken any time from 10 min postoperative to several hours later will provide equally accurate results for predicting post-thyroidectomy hypocalcemia.
Grodski S et al. Evidence for the role of perioperative PTH measurement after total thyroidectomy as a predictor of hypocalcemia. World J Surg 2008; 32: 1367-1373

How to apply it into clinical practice?

Use of postoperative PTH in patient management after total or completion thyroidectomy

Retrospective studyPatients underwent total or completion
thyroidectomyExclusion criteria: modified radical neck dissection,
parathyroidectomy, chronic renal disease, preop calcium/ vitamin D supplements
Jan 2010 to Mar 2013

Results107 patients: 100 total (93.5%); 7 completion (6.5%)Hypocalcemia – adjusted Ca 2+ <2.00 mmol/L at any
time pointTransient 47.7% (51/107)Persistent 5.6% (6/107)

107 Patients
54 PatientsGroup 1-traditional Mx
Since June 2011 – Use of postop D1 PTH
Before
53 PatientsGroup 2-PTH guided Mx
After

ResultsComparable in age, sex distribution, type of
operation, documented resection of parathyroid gland, paratracheal LN dissection and malignant pathology
No difference in rate of hypoparathyroidism, rate of hypocalcemia, need for oral calcium and vitamin D supplement
1 patient from PTH guided Mx group re-admitted due to hypocalcemia

Results

Results
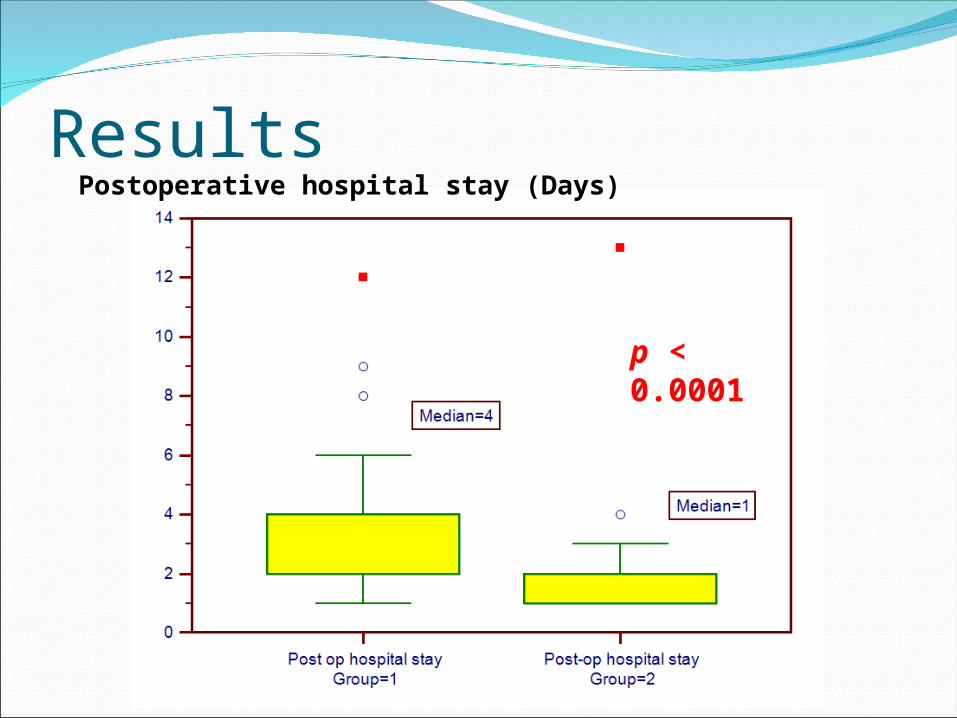
ResultsPostoperative hospital stay (Days)
p < 0.0001

ConclusionsHypocalcemia is a common complication after total
or completion thyroidectomy. Traditionally, patients have to stay in hospital for serial monitoring of serum calcium
A single PTH measurement at early postoperative period can accurately predict which patients are prone to hypocalcemia and facilitate early supplementation therapy.

ConclusionsAsymptomatic patients with normal PTH levels can
be safely discharged on the first postoperative day.
Patients with normal PTH levels may develop mild and self-limiting hypocalcemia. These patients may be discharged safely with calcium supplements and educations on hypocalcemic symptoms
Related Documents