Dpt. Infection and Tropic al Medicine, Sheffield Te aching Hospitals Clinical Aspects of Clinical Aspects of Tuberculosis Tuberculosis Professor Mike McKendrick Lead Physician Department of Infection and Tropical Medicine Royal Hallamshire Hospital Sheffield Honorary Professor Division of Genomic Medicine University of Sheffield

Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals Clinical Aspects of Tuberculosis Professor Mike McKendrick Lead Physician Department.
Dec 22, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals
Clinical Aspects of Clinical Aspects of TuberculosisTuberculosis
Professor Mike McKendrick
Lead PhysicianDepartment of Infection and Tropical Medicine
Royal Hallamshire HospitalSheffield
Honorary ProfessorDivision of Genomic Medicine
University of Sheffield

Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals
Clinical aspects of TBClinical aspects of TB
PathogenisisClinical diagnosisTreatment and monitoring and controlNew issues

Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals
Clinical Aspects of Clinical Aspects of TuberculosisTuberculosis
Pathogenesis of tuberculosis– Infection versus disease
Host factors Pathogen factors

Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals
PathogenesisPathogenesis
Host factors include– Social e.g.
Poverty alcoholism
– Age e.g. Baby Teenage girl Old age
– Immunity e.g. HIV Gamma interferon SCID

Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals
PathogenesisPathogenesis
Organism factors e.g.– Virulence factors – [Drug resistance]

Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals
Pathogenesis Pathogenesis
MTB into lungs (or to cervical nodes or abdo. nodes) Replication of organisms Primary complex (lung and mediastinal lymph nodes)
Mycobacteraemia with potential for ‘seeding’
Consequence of tuberculous infection– Symptomatic illness – disease (minority) – immunological control (majority) with Ghon focus on Xray.
Infection is ‘contained’ by granuloma but not eliminated

Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals
PathogenesisPathogenesis
Tuberculous disease is a consequence of:– Primary infection e.g. in baby
– Reactivation ‘natural’ Associated with immunosupression
– Re infection

Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals
Clinical features Clinical features
Clinical illness– Pulmonary – Extrapulmonary

Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals
Clinical illnessClinical illness Chest
– Pulmonary – Pleural– Mediastinal nodes– pericardium
Extra pulmonary– skin and soft tissues (including lymph nodes)– Bone– Abdominal– Intra cranial– other

Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals
Clinical clues for TBClinical clues for TB Clinical symptoms – usually ‘chronic’ rather than acute
– Fever– Sweats – Weight loss– Focal symptoms
Epidemiology– History of TB, HIV– Country of origin, recent travel/work– Contact with TB
[England, Wales & NI 2004 7,176 notifications, 414 children 70% foreign born population groups]

Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals
TB – guidelines for the clinicianTB – guidelines for the clinician
Great mimickerLow index of suspicionPulmonary TB usually easy to considerNon pulmonary often requires ‘lateral
thinking’

Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals
Clinical TBClinical TB
Laboratory samples– In the current era every effort must be made to
obtain adequate samples likely to lead to a microbiological diagnosis before treatment is started (sometimes difficult with surgical specimens!)
Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals
What can the laboratory do to What can the laboratory do to help the clinician?help the clinician?
Awareness of TB e.g. in the patient with recurrent sputum samples for ‘chronic bronchitis’
‘Rapid’ diagnosis of infection and resistance– Culture and sensitivities – the clinician wants answers
immediately if possible– PCR – further opportunities for development– Gamma interferon based tests??– other

Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals
What samples? Depends on clinical What samples? Depends on clinical scenarioscenario
Chest– Sputum – if productive– Induced sputum– Bronchoscopic alveolar lavage (BAL)– Pleural biopsy– Pleural fluid
Other– E.g. Lymph node, aspiration of abscess, mesenteric
biopsy, stool, bone marrow etc.– What about EMSU? - should be done selectively
where it is likely to be helpful

Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals
Induced sputumInduced sputum
Hypertonic saline nebuliser in negative pressure room with HEPA filter and well trained physiotherapist– Study of 27 confirmed positive patients
13 +ve induced sputum only 1 +ve bronchoscopy only 13 +ve induced sputum and bronchoscopy
McWilliams T et al Thorax 2002: 57; 1010-1014

Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals
Audit of induced sputum in Audit of induced sputum in Department of Infection in SheffieldDepartment of Infection in Sheffield
– Criteria for procedure– Past history TB or contact with TB in last year– Respiratory symptoms of one or more of:
• Non-productive cough• Fever, Night sweats, weight loss• Haemoptysis
114 procedures, 12 positive for TB– Cohort followed up for 12 months, no cases
missed - Bell et al. J Infection 2003:
47; 317-321

Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals
Clinical casesClinical cases
Cases of – pulmonary infection– Non pulmonary infection– Examples of spectrum of disease produced by
TB

Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals
Pulmonary and non pulmonary Pulmonary and non pulmonary TB disease – Sheffield 2005TB disease – Sheffield 2005
Equal numbers of patients with pulmonary and non pulmonary tuberculosis

Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals
Clinical presentation 1Clinical presentation 1
35 year old African lady with fever and dry cough for 3 weeks.
Mildly unwellNight sweatsWeight loss 4 poundsNo history of contact with TBCXR

Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals
Case 1 – miliary tuberculosisCase 1 – miliary tuberculosis

Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals
Pulmonary TB typically affects Pulmonary TB typically affects the upper zones of the lungthe upper zones of the lung

Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals
Case 1Case 1
Investigation– FBC normal– ESR 53– U and E normal– LFT – albumen 31– CRP 40– Induced sputum – smear negative

Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals
Case 1Case 1Progress
– Clinical diagnosis of TB 4 drug treatment Clinical improvement
– TB culture positive at week 3 fully sensitive (week 5) Modified anti TB drug regime in light of lab results

Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals
Case 1Case 1
What about HIV testing? – who to test?– Strong association between HIV and TB– Universal testing or selective testing?
What about testing for vitamin D?– Vitamin D has role in activating macrophages to
destroy mycobacteria– Vitamin D deficiency in ethnic populations in UK often
low

Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals
Case 1Case 1
Cured after standard 6 months therapy

Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals
Clinical presentation 2Clinical presentation 2
28 year old African lady with backache for 6 weeks
Diagnosed initially as non specificDeveloped fever – no obvious causeID opinion soughtInvestigation with MRI scan

Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals
Clinical case 2Clinical case 2
Diagnosis– Vertebral osteomyelitis with soft tissue mass
impinging on the cord
Investigation Biopsy and culture
Treatment– 4 anti TB drugs and antibiotic therapy

Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals
Clinical case 2 Clinical case 2
What will happen if diagnosis or treatment for TB spinal osteomyelitis is delayed?

Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals
What will happen if treatment delayed? – gibbus What will happen if treatment delayed? – gibbus formation (acute angulation of spine with or formation (acute angulation of spine with or
without neurological damage)without neurological damage)

Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals
The physical appearance – Potts The physical appearance – Potts disease of spine - gibbusdisease of spine - gibbus

Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals
Clinical case 2Clinical case 2
Progress– Increasing back pain and neurological
symptoms – mild leg weakness– Repeat MRI – changes similar
Treatment– Continue therapy – consider surgical decompression

Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals
Clinical case 2Clinical case 2Further progress
Weakness of legs Neurosurgery and internal splinting
Other considerations - clinical Has she got HIV? Is her vitamin D level normal?
Other considerations - epidemiological From where has she got infection? To whom might she have given it?

Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals
TB may affect any tissue of the body
including:– Skin and soft tissue– Lymph nodes– Bones and joints– Intra abdominal structures including
peritoneum Kidneys Adrenal glands Lymph nodes
– Central nervous system Tuberculoma meningitis

Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals
Skin and soft tissue
Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals
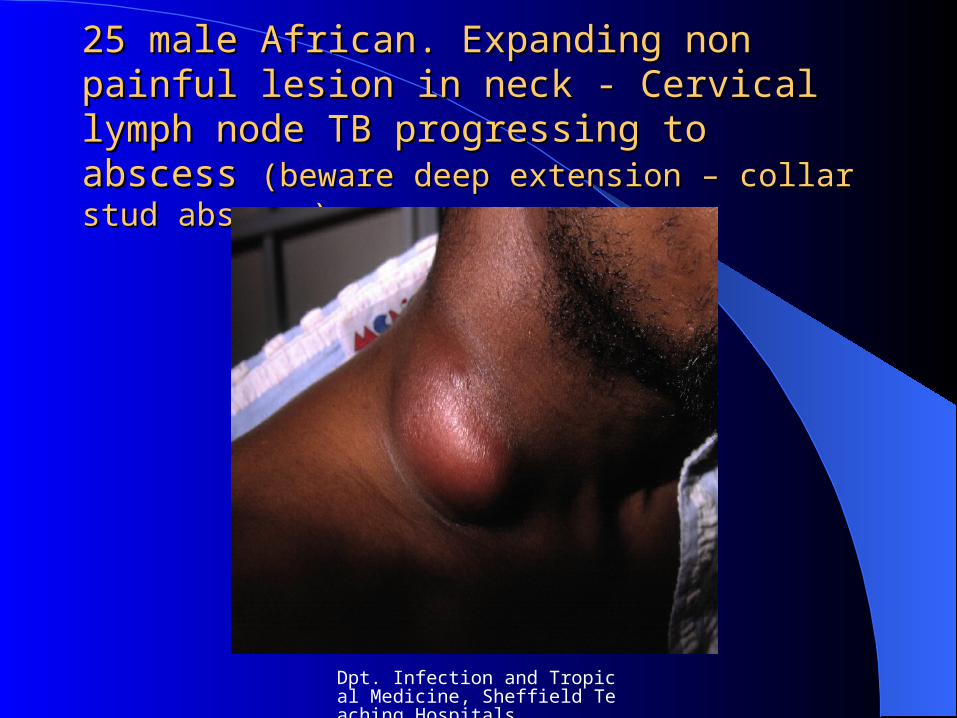
25 male African. Expanding non painful lesion 25 male African. Expanding non painful lesion in neck - Cervical lymph node TB progressing to in neck - Cervical lymph node TB progressing to abscess abscess (beware deep extension – collar stud (beware deep extension – collar stud abscess)abscess)

Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals
TB node in neck with deep TB node in neck with deep extensionextension

Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals
35 female African – systemically well - hand 35 female African – systemically well - hand and foot lesions present for 6 months – and foot lesions present for 6 months – MTB MTB
grown on biopsy by plastic surgeonsgrown on biopsy by plastic surgeons (HIV neg)(HIV neg)

Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals
Bony tuberculosis

Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals
Astute radiologist should enable the Astute radiologist should enable the appropriate further investigationappropriate further investigation

Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals
Often associated with delay in diagnosis – Often associated with delay in diagnosis – anyany chronic discharging lesion must be chronic discharging lesion must be
considered possibly TBconsidered possibly TB

Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals
Abdominal Tuberculosis

Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals
Renal tuberculosis Renal tuberculosis (may have few (may have few or no symptoms) leading to or no symptoms) leading to
autonephrectomyautonephrectomy

Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals
30 middle eastern asylum seeker - abdo pain, 30 middle eastern asylum seeker - abdo pain, fever, sweats – CT scan - peritoneal TB fever, sweats – CT scan - peritoneal TB
confirmed on biopsy – may mimic malignancy confirmed on biopsy – may mimic malignancy

Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals
Intracranial TB

Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals
miliary TB on MRI scanmiliary TB on MRI scantuberclomas on CT scantuberclomas on CT scan

Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals
meningitismeningitis – diagnosis usually made on – diagnosis usually made on clinical groundsclinical grounds
Clinical Acute or subacute Prognosis related to severity of disease at onset of treatment Commonly delay between presentation and diagnosis Common in children c100 cases per year in England
CSF– Cell count 50-500 (50% lymphs, 50% polys)– High protein ++– Low glucose– Micro often negative (PCR/culture important)

Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals
Treatment of TB

Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals
BTS guidelines – 1999 Thorax 2000: 55; 210-218
NICE guidelines – 2006
– Sensitive TB – 4 drugs for 2 months 2 drugs for 4 months
– Resistant TB - 6 drugs for 24 months (second line drugs are not so effective)
[Eng, Wales & NI 2004, 6.8% Isoniazid resistant, 1% MDR TB (R to Isoniazid and rifampicin)]

Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals
Problems of TB therapyProblems of TB therapy
Toxicity e.g. liverMultiple therapyProlonged treatmentDrug interactions e.g. anti HIV drugs

Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals
ComplianceCompliance
– Treatment will not work if not taken
– DOTS (Directly Observed Therapy) if: Likely poor compliance MDRTB

Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals
OutcomeOutcome WHO target (1991)
– detect 70% infectious cases of TB and cure at least 85% by 2005
Eng, Wales and NI– Probably detect 70% cases infectious TB– Cure rate uncertain
Among all TB patients with a known outcome the proportion of cases that have completed treatment
– 79% in 2003– 78% in 2002 – 79% in 2001 CDR 23 March 2006

Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals
Why failure?Why failure?
Patient non compliance– Deliberate– Failure to understand e.g. language, culture– Social e.g. alcohol
Patient movement e.g. ‘lost to follow up’Lack of medical/nursing supportothers

Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals
public health - public health - avoiding avoiding
transmissiontransmission TB is statutorily notifiable disease Multidisciplinary approach – medical, TB nurses,
CCDC etc. Identify and manage possible sources of infection and contacts
Considerations treat as OP where possible multi occupancy housing, social deprivation negative pressure rooms in hospitals (limited facility) beware transmission in OP setting e.g. waiting area

Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals
New challenges in TBNew challenges in TB

Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals
Challenges in TBChallenges in TB
Anti TNF therapy (Eg infliximab, etanercept)– May promote breakdown of granulomas and
reactivation of TB– How to screen
Clinical history CXR (? With induced sputum) Skin testing ?? Value of gamma interferon tests

Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals
Challenges in TBChallenges in TB
What will be the place of Quantiferon and Elispot type tests in clinical practice?

Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals
Clinical need for new and better anti TB drugs

Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals
Objective - to lead to more effective shorter course regimen– Better pharmacokinetics
longer half life better penetration to cavities
– Better activity kill TB in dormant phase Active against resistant strains
– Safer and easier Lack of interaction with anti HIV therapy Less toxic
– Low cost

Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals
Will there be new affordable Will there be new affordable therapy for TB?therapy for TB?
Global Alliance for TB Drug DevelopmentTB development drug discovery research
unit– Astra Zenica– Glaxo SmithKline– Novartis
WHO links with pharmaTB trials consortium (US CDC)

Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals
Will there be new affordable Will there be new affordable therapy for TB?therapy for TB?
MoxifloxacinTMC 207OPC-67683PA-824LL3858

Dpt. Infection and Tropical Medicine, Sheffield Teaching Hospitals
SummarySummary
TB is a challenging disease for the clinicianMust have microbiology before starting
treatment – more rapid lab tests?Need to encourage complianceNeed for multidisciplinary approach to
diagnosis and management and controlNeed shorter, better, cheap anti TB regimes
Related Documents





![BIFURCATION OF TIME PERIODIC SOLUTIONS OF THE McKENDRICK … · of the McKendrick equations is sometimes done in order to gain insight into the dynamics[l2]. The goal of this paper](https://static.cupdf.com/doc/110x72/5e82dd71a2f82c14010fe7f2/bifurcation-of-time-periodic-solutions-of-the-mckendrick-of-the-mckendrick-equations.jpg)





![ID training in Europe, 2004 Dr Mike McKendrick · Dr Mike McKendrick [President European Board of Infectious Diseases, UEMS 1998-2003] Consultant Physician Department of Infection](https://static.cupdf.com/doc/110x72/5e82dc71bf65702d964a7fbf/id-training-in-europe-2004-dr-mike-mckendrick-dr-mike-mckendrick-president-european.jpg)