Doug Hohbein Assistant State Fire Marshal Nebraska State Fire Marshal Agency [email protected] 402-471-2027

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Doug Hohbein
Assistant State Fire Marshal
Nebraska State Fire Marshal Agency
402-471-2027

Most often cited deficiencies
New code requirements
Q & A
NFPA 101 – 2012NFPA 99 – 2012NFPA 72 – 2010NFPA 13 – 2010 NFPA 96 – 2011NFPA 90A – 2012NFPA 80 – 2010NFPA 110 – 2010
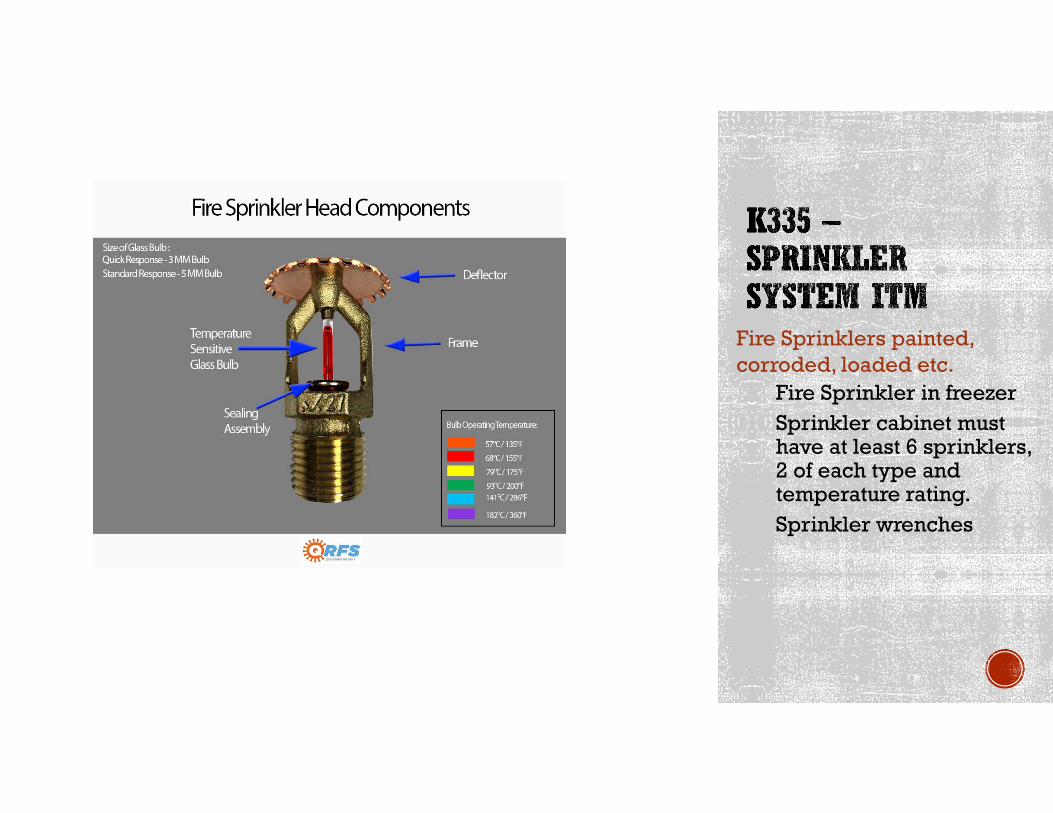
Fire Sprinklers painted, corroded, loaded etc.
Fire Sprinkler in freezerSprinkler cabinet must have at least 6 sprinklers, 2 of each type and temperature rating.Sprinkler wrenches
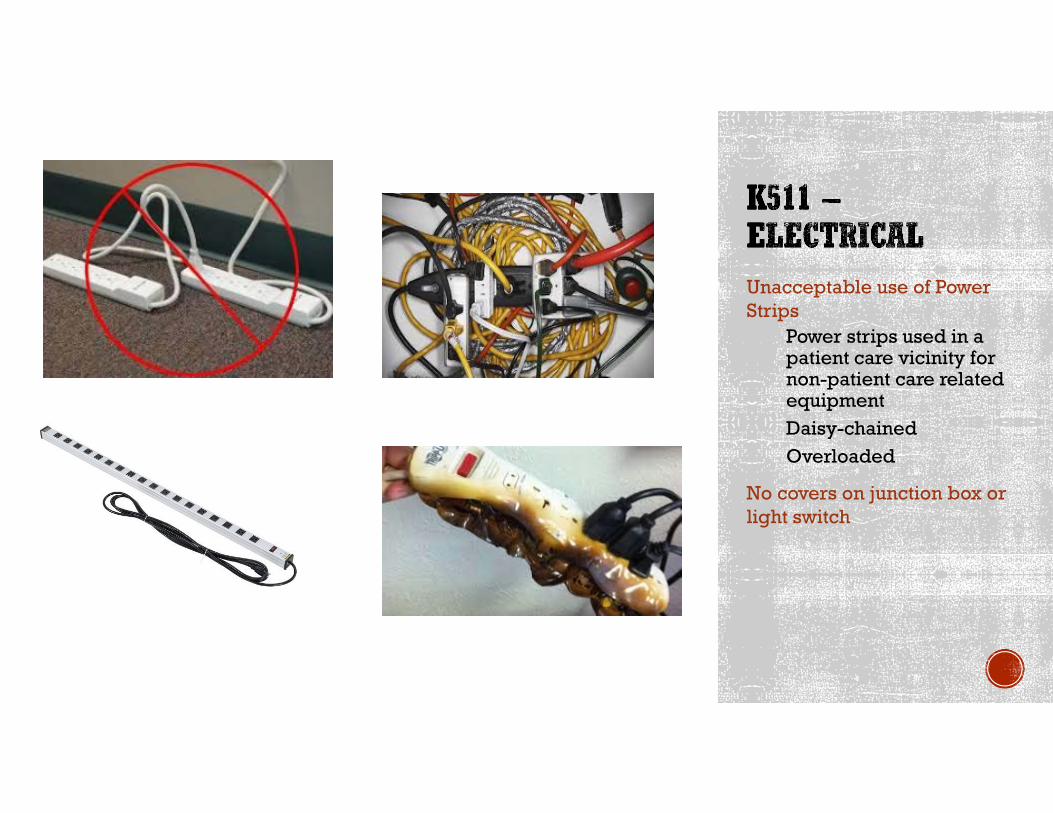
Unacceptable use of Power Strips
Power strips used in a patient care vicinity for non-patient care related equipmentDaisy-chainedOverloaded
No covers on junction box or light switch
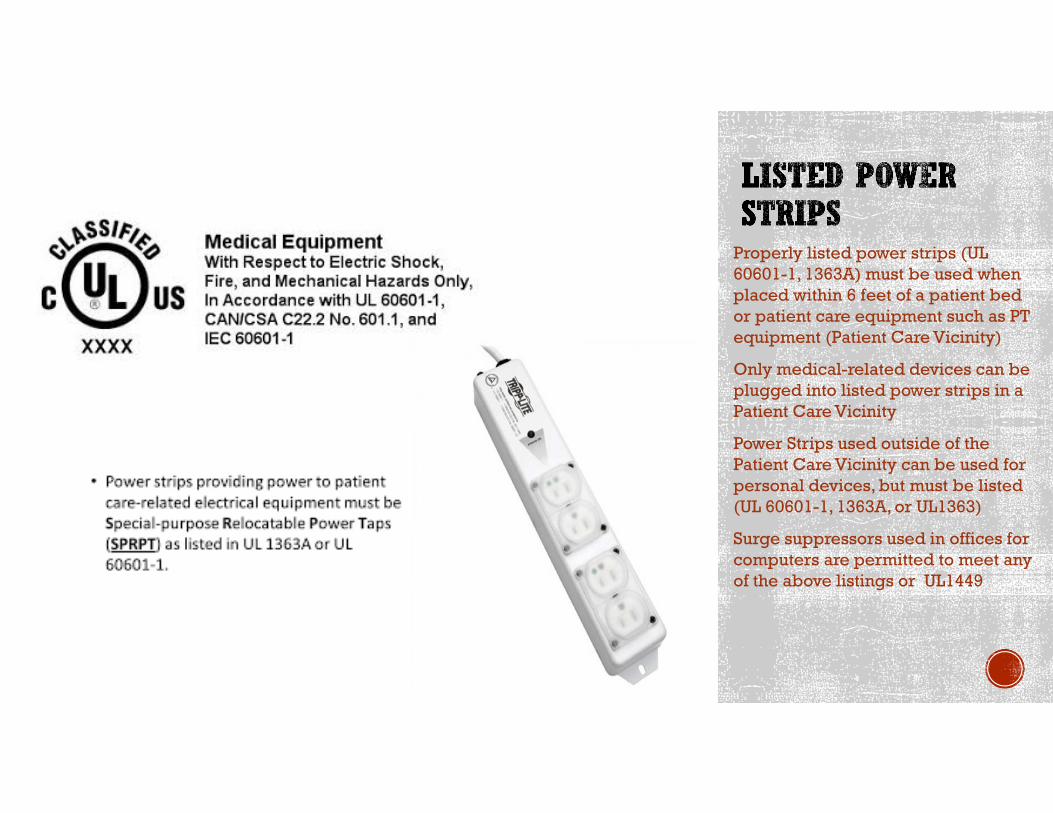
Properly listed power strips (UL 60601-1, 1363A) must be used when placed within 6 feet of a patient bed or patient care equipment such as PT equipment (Patient Care Vicinity)
Only medical-related devices can be plugged into listed power strips in a Patient Care Vicinity
Power Strips used outside of the Patient Care Vicinity can be used for personal devices, but must be listed (UL 60601-1, 1363A, or UL1363)
Surge suppressors used in offices for computers are permitted to meet any of the above listings or UL1449
Audit and Documentation
A written audit of all power strips shall be conducted by the facility annually. The audit shall list:
The specific location and listing identification of all power strips in the facility.
Changes to the number/location/listing from the previous audit.
Specific appliances/equipment connected to each power strip. No High-Draw appliances ( no motors/75% rule)
If the facility chooses not to conduct annual audits, documentation from the power strip manufacturer shall be provided that will confirm a different testing procedure/schedule.
Audit and Documentation
Non-PCREE used in a patient care vicinity that will come into contact with patients shall be visually inspected and documented annually. This includes personal items used and owned by the patient. Any appliances or equipment that appears not to be in proper working order or in a worn condition shall be removed from service. Note that these devices cannot be connected to a power strip.
Household appliances and equipment located in a patient care vicinity shall have a grounding conductor (three-prong plug) or the device must be double-insulated.
The facility shall establish written polices for the control of electrical appliances not provided by the facility (incoming inspection, periodic checks).
Potential questions to address with the policy:
Is the appliance patient-care related?
Is the appliance to be used by the facility staff on the patient?
Is the appliance to be used by the patient only?
Is the appliance properly listed?
Area 6 feet around a patient bed or treatment area and 7’6” above.
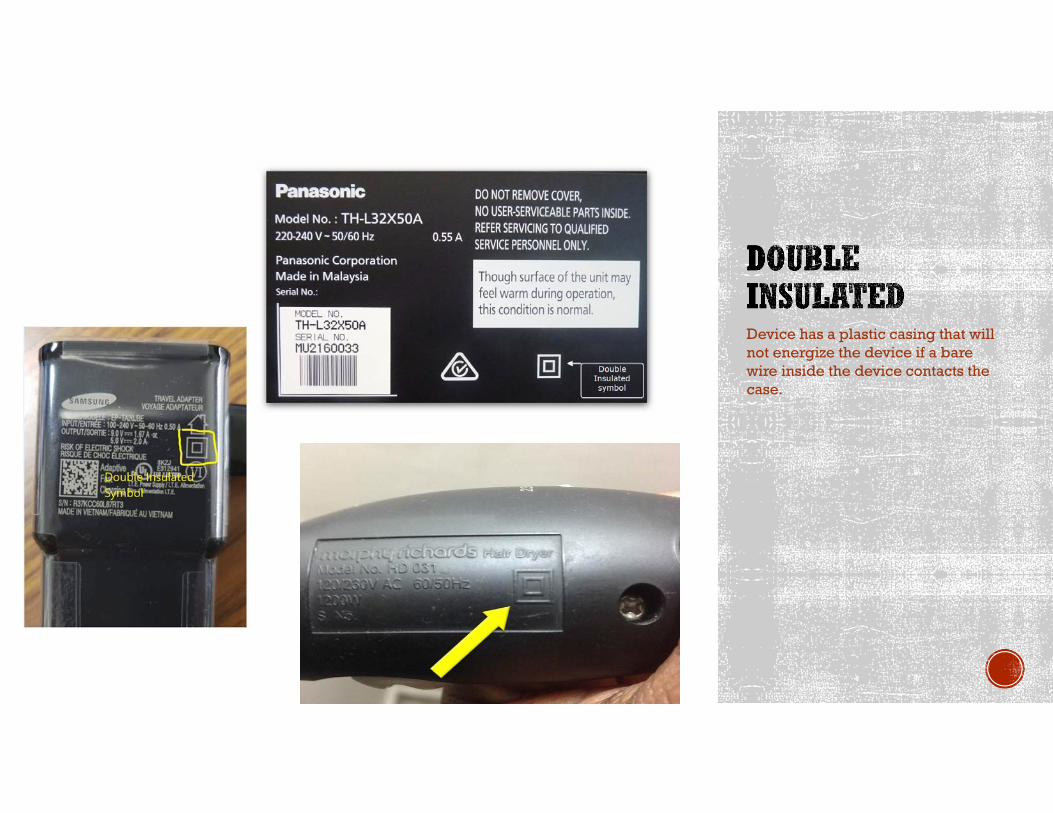
Device has a plastic casing that will not energize the device if a bare wire inside the device contacts the case.
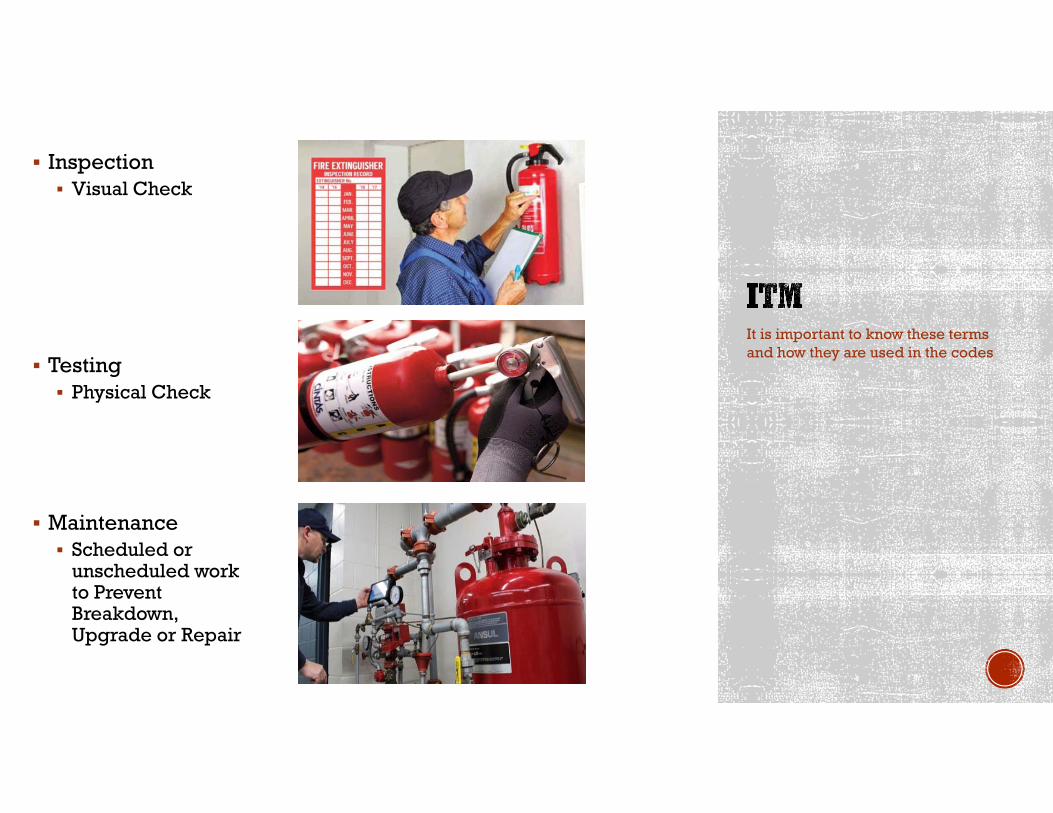
Inspection Visual Check
Testing Physical Check
Maintenance Scheduled or
unscheduled work to Prevent Breakdown, Upgrade or Repair
It is important to know these terms and how they are used in the codes
When is Certification Required?
Fire Extinguishers Maintenance or Recharging (not inspections) Manufacturer
NAFED (www.nafed.org)*
Must have manufacturers manuals
Kitchen Exhaust Hood/Ducts Inspection Testing and Maintenance IKECA (www.ikeca.org)
Kitchen Fire-Extinguishing Systems Inspection Testing and Maintenance Manufacturer
NAFED (www.nafed.org)*
*Must have manufacturer manuals
Fire Alarm and Fire Sprinkler Certified through State Fire Marshal’s Office
NFPA codes require persons conducting certain Inspections/Testing/Maintenance of safety equipment to be certified
Local jurisdictions may have specific licensing requirements
Hoods and ducts must be inspected twice a year Not required to be certified
If found contaminated, hood and ducts must be cleaned by a certified person
Cooking equipment that collects grease below and/or behind the cooking surface or in the flue gas exhaust must be inspected annually by a trained and qualified person Not required to be certified Typically griddles or charbroilers
Note that you are NOT required to CLEAN hoods and ducts, only to INSPECT them.
If found dirty, then cleaning is required.
Corrective Action – How was the deficiency corrected?
System Change – How will the facility ensure the deficiency doesn’t repeat in the future?
Monitoring Process – How does the facility make sure the System Change is effective?
Example: Sprinklers in Laundry covered in lint Corrective Action: Clean sprinklers in Laundry System Change: Implement a program to inspect 25% of
all sprinklers in the facility quarterly Monitoring Process: Give to QAPI Committee for them to
review follow through at monthly meetings
What is required to be included in a Plan of Correction?
Plans of Correction must include supporting documentation.
Required for all deficiencies
Can include: Copies of Receipts Invoices Verifiable Photos Auditing Tools Education Information Copy of signature sheet (inservice, fire drill etc.)
Revised or New Policies and Procedures ITM Schedules/Reports
Starting January 1, 2020 PoC’s without supporting documentation will not be approved!
Attach with ePOC or email with PoC sent to DHHS
OR email to:
Tests are required for all patient care-related equipment used in patient rooms. Nebulizers O2 Concentrators Monitors
10.5.2.1.1 The facility shall establish policies and protocols for
the type of test and intervals of testing for patient care–related
electrical equipment.
10.5.2.1.2 All patient care–related electrical equipment used in
patient care rooms shall be tested in accordance with 10.3.5.4 or
10.3.6 before being put into service for the first time and after any
repair or modification that might have compromised electrical
safety.
10.3.5.4 Touch Leakage Test Procedure.
10.3.6* Lead Leakage Current Tests and Limits — Portable
Equipment.
From NFPA 99, 10.5.2.1
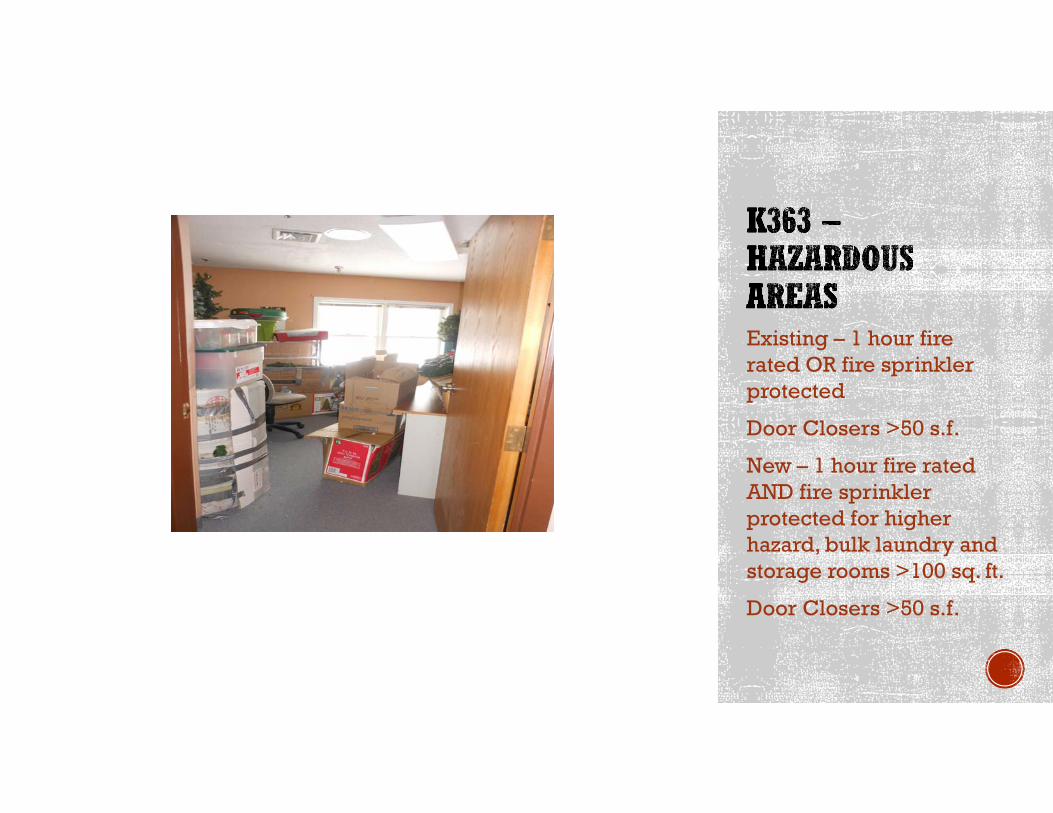
Existing – 1 hour fire rated OR fire sprinkler protected
Door Closers >50 s.f.
New – 1 hour fire rated AND fire sprinkler protected for higher hazard, bulk laundry and storage rooms >100 sq. ft.
Door Closers >50 s.f.
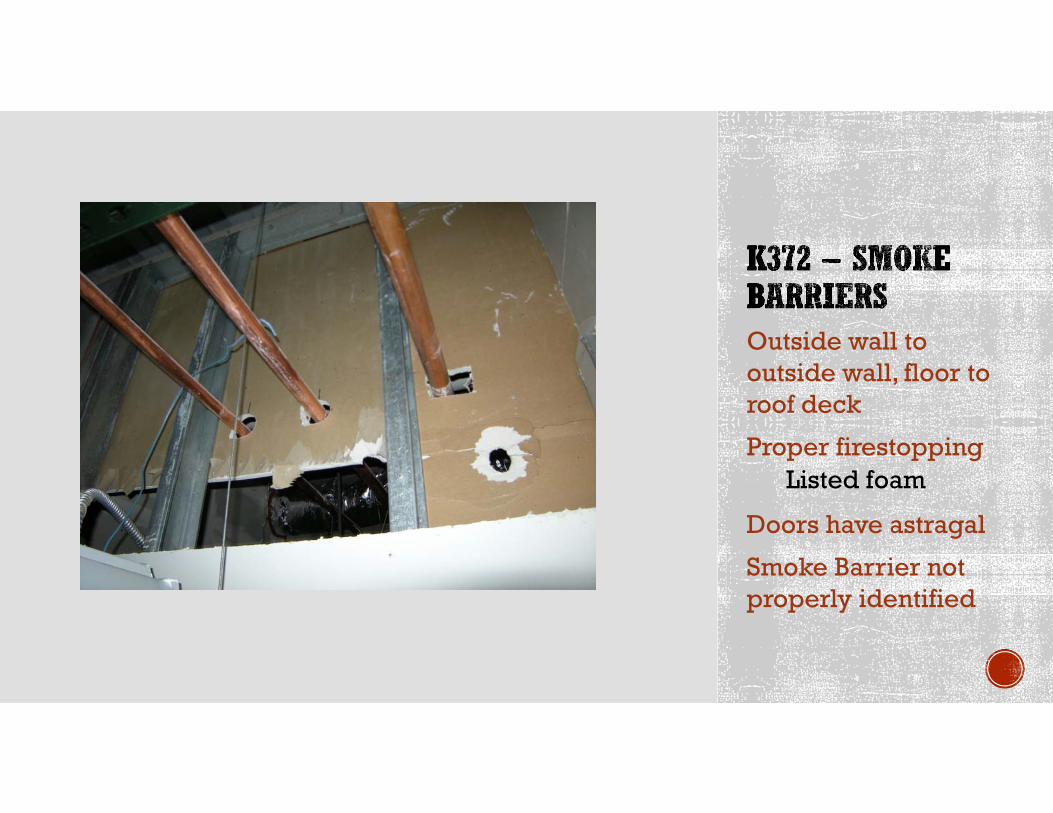
Outside wall to outside wall, floor to roof deck
Proper firestoppingListed foam
Doors have astragal
Smoke Barrier not properly identified
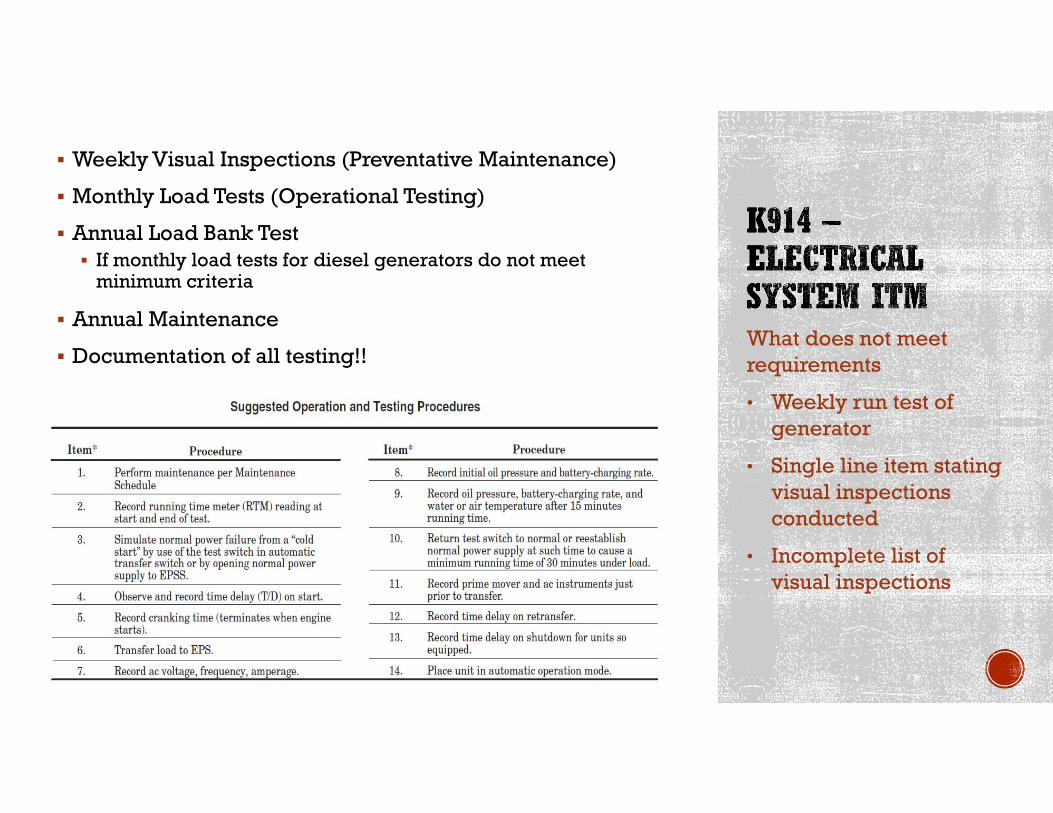
Weekly Visual Inspections (Preventative Maintenance)
Monthly Load Tests (Operational Testing)
Annual Load Bank Test If monthly load tests for diesel generators do not meet
minimum criteria
Annual Maintenance
Documentation of all testing!!What does not meet requirements
• Weekly run test of generator
• Single line item stating visual inspections conducted
• Incomplete list of visual inspections
NFPA 110, Figure A-8.4.1(a) contains ten components Fuel, Lubrication System, Cooling System, Exhaust
System, Battery System, Electrical System, Prime Mover, Generator
Each component has subcomponents At least one subcomponent of each component requires a
weekly visual inspection Examples: Fuel level, oil level, cooling system hoses, battery
electrolyte level, service room/housing housekeeping
Visual inspection only. No certification of licensing required.
8.4.2* Diesel generator sets in service shall be exercised at least once monthly, for a minimum of 30 minutes, using one of the following methods:
(1) Loading that maintains the minimum exhaust gas temperatures as recommended by the manufacturer(2) Under operating temperature conditions and at not less than 30 percent of the EPS nameplate kW rating
8.4.2.3 Diesel-powered EPS installations that do not meet the requirements of 8.4.2 shall be exercised monthly with the available EPSS load and shall be exercised annually with supplemental loads at not less than 50 percent of the EPS nameplate kW rating for 30 continuous minutes and at not less than 75 percent of the EPS nameplate kW rating for 1 continuous hour for a total test duration of not less than 1.5 continuous hours.
A minimum time delay of 5 minutes shall be provided for unloaded running of the EPS prior to shutdown to allow for engine cooldown. The time delay on the prime mover cooldown period
and shutdown shall be recorded.
Load Bank and cooldown time period
Q: I have two questions regarding spark-ignited emergency power generators:
1. What maintenance tests are required for natural gas or propane generators?
2. Are load bank tests required for natural gas or propane gas powered generators?
A:
1. Monthly tests are required, but since they are spark-ignited generators they do not have to meet a particular load. They just have to operate with the available EPSS load for a minimum of 30 minutes or until the water temperature and oil pressure have stabilized.
(See section 8.4.2.4 of NFPA 110-2010).
2. No, spark-ignited generators (natural gas) are not required to have an annual load bank test. An annual load bank test is required when dieselpowered generators cannot meet the minimum load of 30% of the nameplate rating (in kW) during each monthly load test. Spark-ignited generators are exempt from having to meet this requirement. (Diesel only per 8.4.2.3)
For Level 1 EPSS, (hospitals) a 3-year, 4-hour load test is required for all generators, including spark-ignited generators. But you are not permitted to use a load bank on spark-ignited generators. The 3-year, 4-hour load test must operate using the load from the ATS. For spark-ignited generators, the load is permitted to be the available load. (See section 8.4.9.5.3 of the NFPA 110-2010.) Load banks are not permitted for the 3-year 4-hour load test for spark-ignited generator.
An annual load bank test is not required.
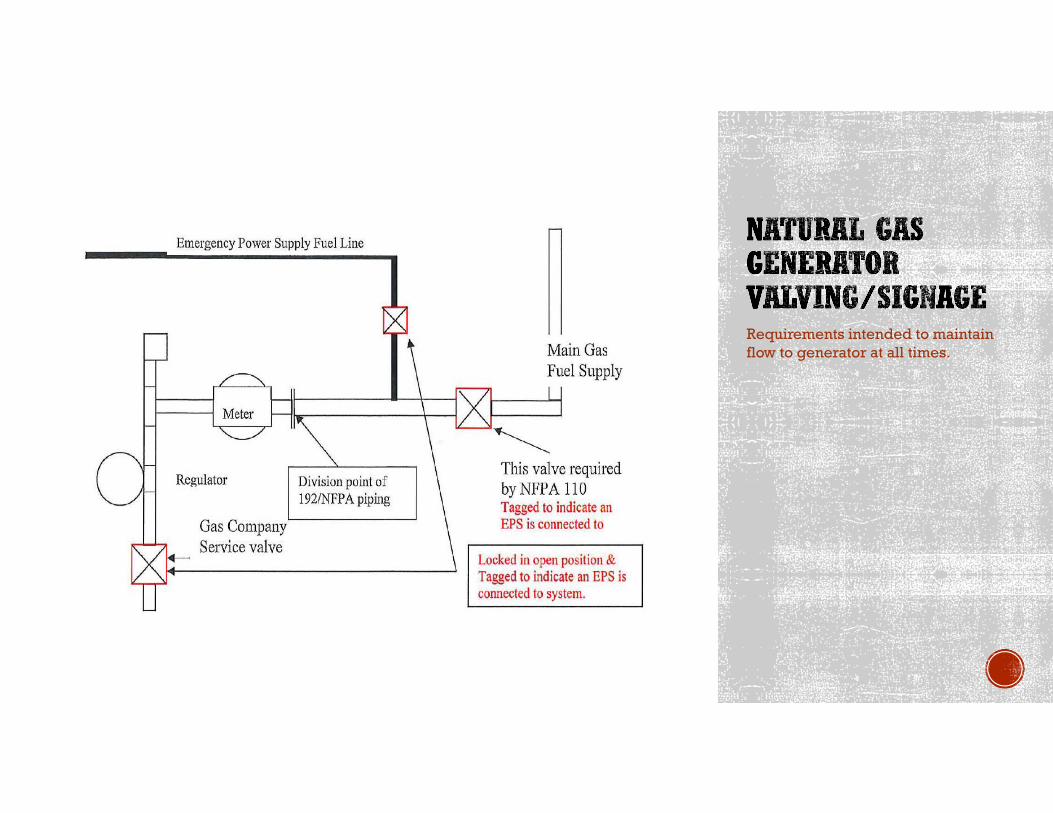
Requirements intended to maintain flow to generator at all times.
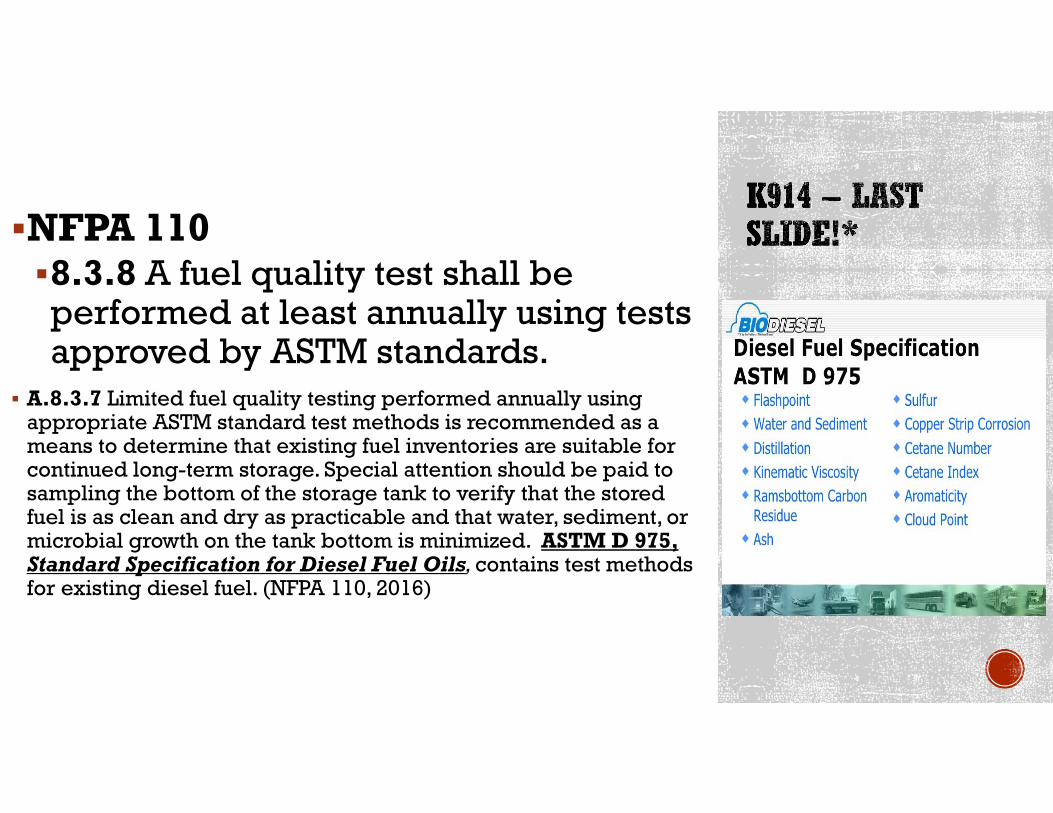
NFPA 1108.3.8 A fuel quality test shall be performed at least annually using tests approved by ASTM standards.
A.8.3.7 Limited fuel quality testing performed annually using appropriate ASTM standard test methods is recommended as a means to determine that existing fuel inventories are suitable for continued long-term storage. Special attention should be paid to sampling the bottom of the storage tank to verify that the stored fuel is as clean and dry as practicable and that water, sediment, or microbial growth on the tank bottom is minimized. ASTM D 975, Standard Specification for Diesel Fuel Oils, contains test methods for existing diesel fuel. (NFPA 110, 2016)
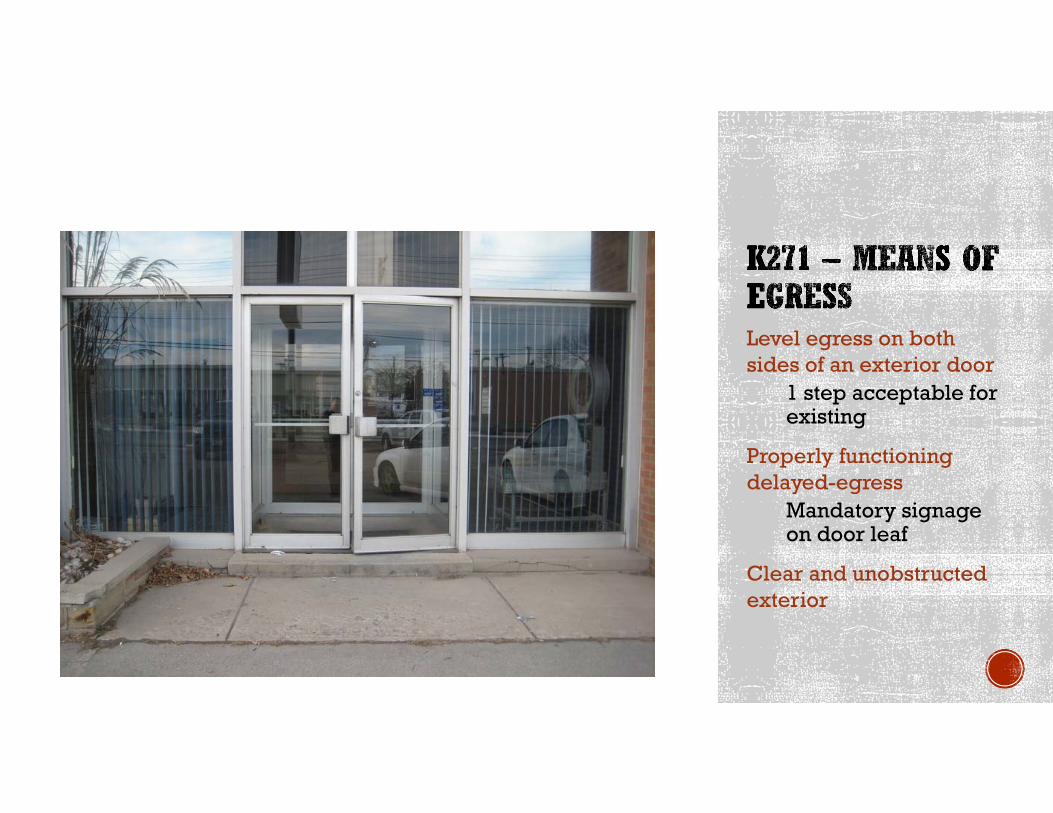
Level egress on both sides of an exterior door
1 step acceptable for existing
Properly functioning delayed-egress
Mandatory signage on door leaf
Clear and unobstructed exterior

1/shift/quarter
Conducted at varying times (1 hour between drills each quarter) Are these drills compliant?
1. January 12, 7:00am
2. April 2, 10:45am
3. August 20, 1:15pm
4. November 9, 7:45am
Documentation!!!
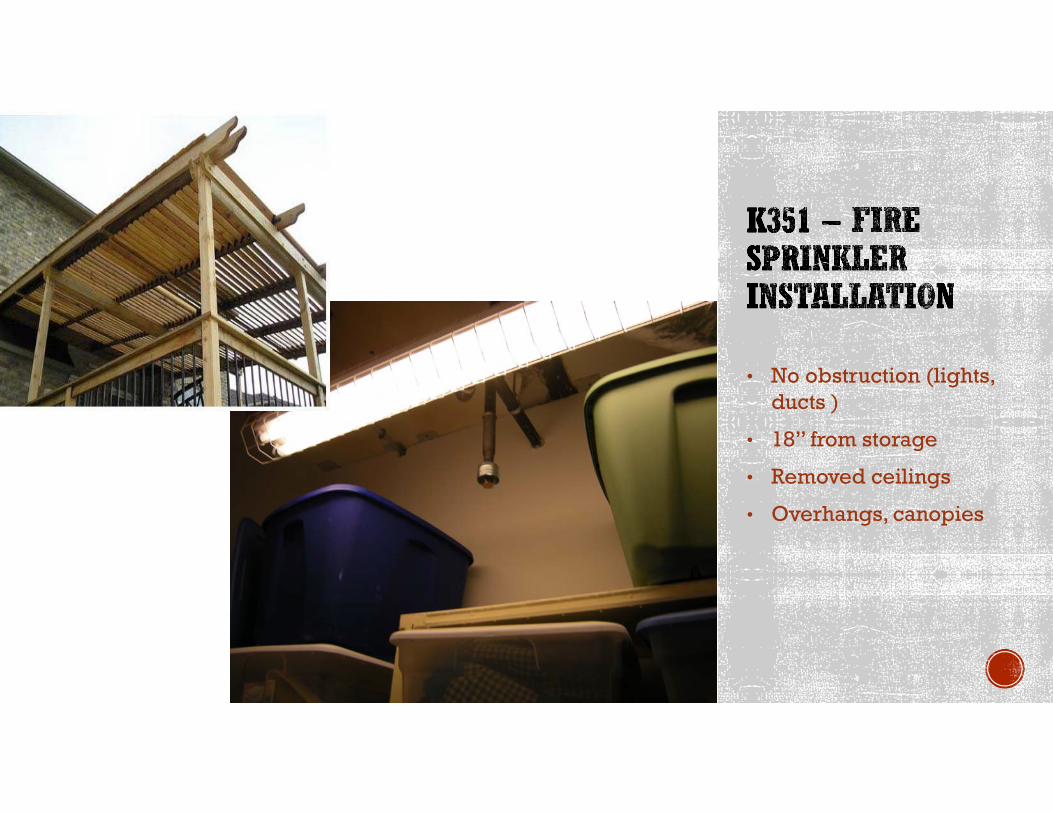
• No obstruction (lights, ducts )
• 18” from storage
• Removed ceilings
• Overhangs, canopies
(1) No open holes or breaks exist in surfaces of either the door or frame.
(2) Glazing, vision light frames, and glazing beads are intact and securely fastened in place, if so equipped.
(3) The door, frame, hinges, hardware, and noncombustible threshold are secured, aligned, and in working order with no visible signs of damage.
(4) No parts are missing or broken.
(5) Door clearances do not exceed clearances listed in 4.8.4 and 6.3.1.7.
(6) The self-closing device is operational; that is, the active door completely closes when operated from the full open position.
(7) If a coordinator is installed, the inactive leaf closes before the active leaf.
(8) Latching hardware operates and secures the door when it is in the closed position.
(9) Auxiliary hardware items that interfere or prohibit operation are not installed on the door or frame.
(10) No field modifications to the door assembly have been performed that void the label.
(11) Gasketing and edge seals, where required, are inspected to verify their presence and integrity.
Patient room doors and doors in Smoke Barriers must be inspected routinely
Not required to conduct the full 11 point inspections for fire rated doors
Simple inspection Confirm door operation (doesn’t drag on floor) Gaps between door and frame are not excessive Doors with latching hardware positively latch Does not take excessive force to open or close
Documentation!
Mandated by CMS S & C Memo 17-38-LSC
Which receptacles must be tested and how often? All new receptacles in patient care areas must be tested
prior to use.
Existing receptacles Hospital-grade receptacles: 6.3.4.1.1 Where hospital-grade receptacles are required at
patient bed locations and in locations where deep sedation or general anesthesia is administered, testing shall be performed after initial installation, replacement, or servicing of the device.
6.3.4.1.2 Additional testing of receptacles in patient care rooms shall be performed at intervals defined by documented performance data.
What is ‘Documented Performance Data’? Manufacturer’s recommendation Historical testing data from similar receptacles help
determine frequency of testing
Nonhospital-grade receptacles: 6.3.4.1.3 Receptacles not listed as hospital-grade, at
patient bed locations and in locations where deep sedation or general anesthesia is administered, shall be tested at intervals not exceeding 12 months.
What tests are required? (Hospital-grade and Nonhospital-grade) 6.3.3.2 Receptacle Testing in Patient Care Rooms. 6.3.3.2.1 The physical integrity of each receptacle shall be
confirmed by visual inspection. 6.3.3.2.2 The continuity of the grounding circuit in each electrical
receptacle shall be verified. 6.3.3.2.3 Correct polarity of the hot and neutral connections in
each electrical receptacle shall be confirmed. 6.3.3.2.4 The retention force of the grounding blade of each
electrical receptacle (except locking-type receptacles) shall be not less than 115 g (4 oz.).
Personnel applying, handling and maintaining medical gases shall be trained on the associated risks. Typically includes physicians, nurses, CNA’s, Respiratory
Therapists, Technicians, Maintenance etc.
Policies and Procedures Purchase specifications Cylinders Marking Connections
Training Piped systems Use and transport Verification of content/connection
Policies Storage and handling Evaluation of warning signals Capability to cope with complete gas system loss Documentation of testing/verification Bulk O2 location
NFPA 99, 11.5.2 and 11.6
Most of these requirements apply to piped systems in hospitals
Underlined apply to Nursing homes using oxygen cylinders/containers
Are treated the same as tobacco cigars/cigarettes for LSC enforcement. No Smoking/vaping where oxygen or
flammable/combustible liquids/gases are stored/used Proper ashtrays and self-closing containers for ashes. (!)
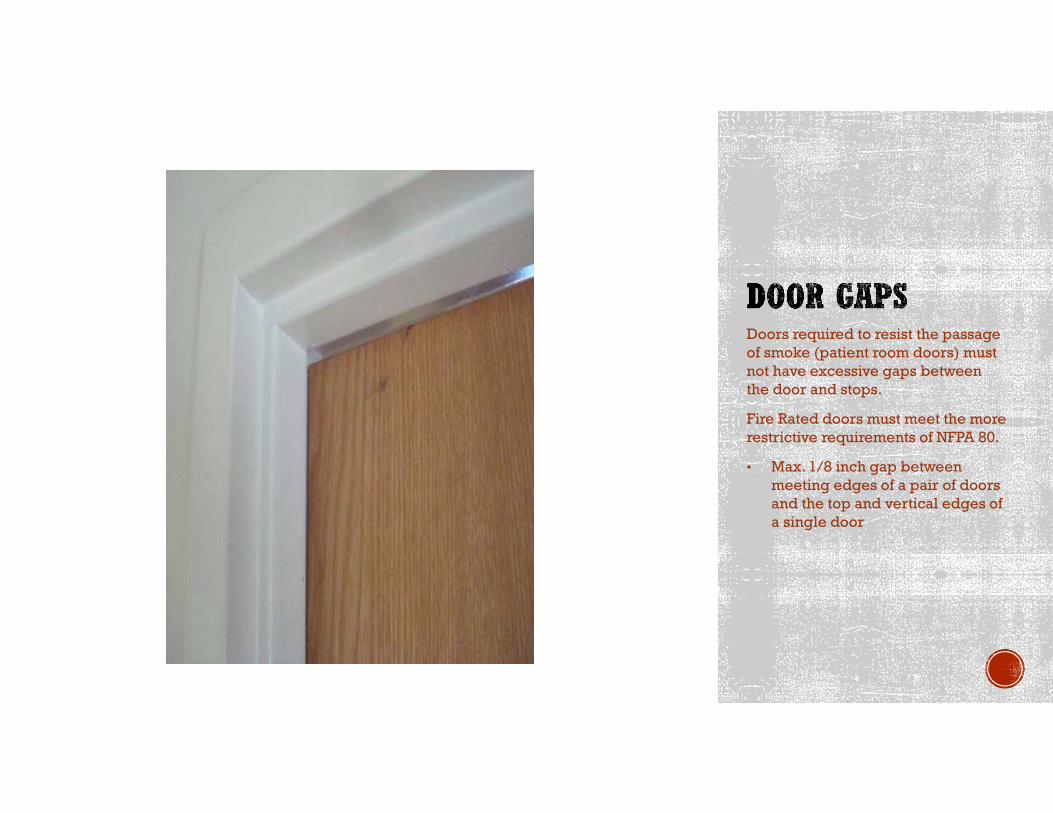
Doors required to resist the passage of smoke (patient room doors) must not have excessive gaps between the door and stops.
Fire Rated doors must meet the more restrictive requirements of NFPA 80.
• Max. 1/8 inch gap between meeting edges of a pair of doors and the top and vertical edges of a single door
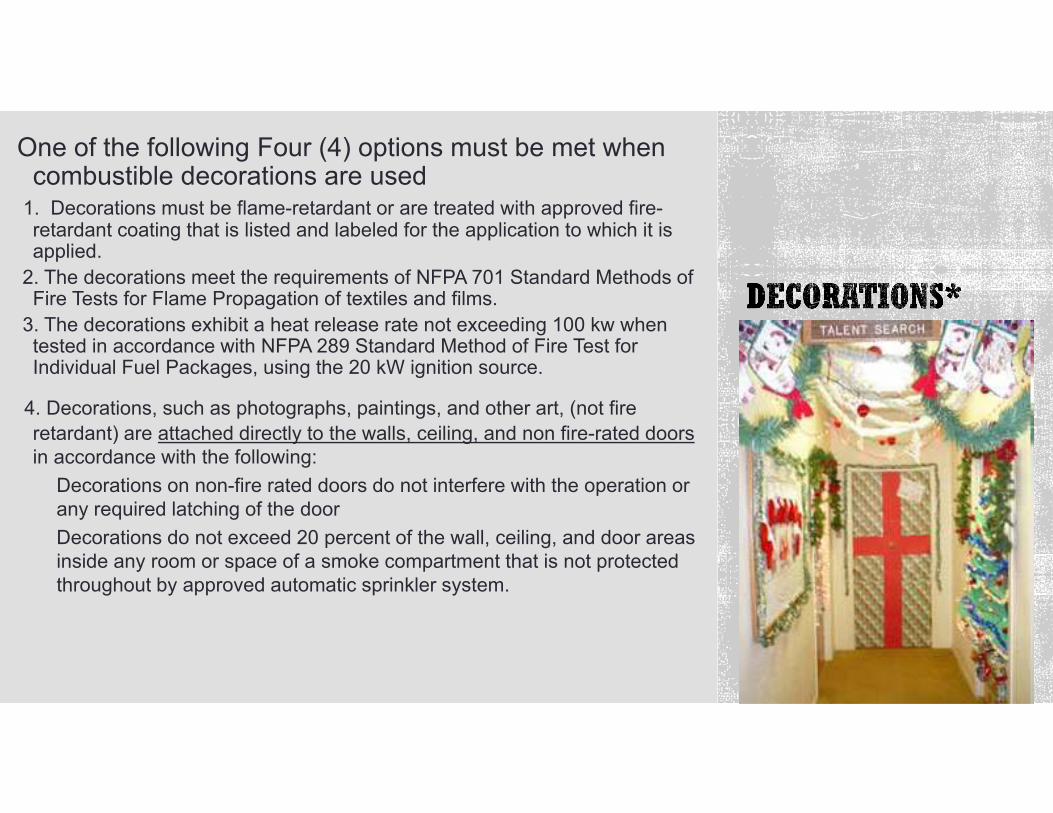
One of the following Four (4) options must be met when combustible decorations are used
1. Decorations must be flame-retardant or are treated with approved fire-retardant coating that is listed and labeled for the application to which it is applied.
2. The decorations meet the requirements of NFPA 701 Standard Methods of Fire Tests for Flame Propagation of textiles and films.
3. The decorations exhibit a heat release rate not exceeding 100 kw when tested in accordance with NFPA 289 Standard Method of Fire Test for Individual Fuel Packages, using the 20 kW ignition source.
4. Decorations, such as photographs, paintings, and other art, (not fire retardant) are attached directly to the walls, ceiling, and non fire-rated doors in accordance with the following:
Decorations on non-fire rated doors do not interfere with the operation or any required latching of the door Decorations do not exceed 20 percent of the wall, ceiling, and door areas inside any room or space of a smoke compartment that is not protected throughout by approved automatic sprinkler system.
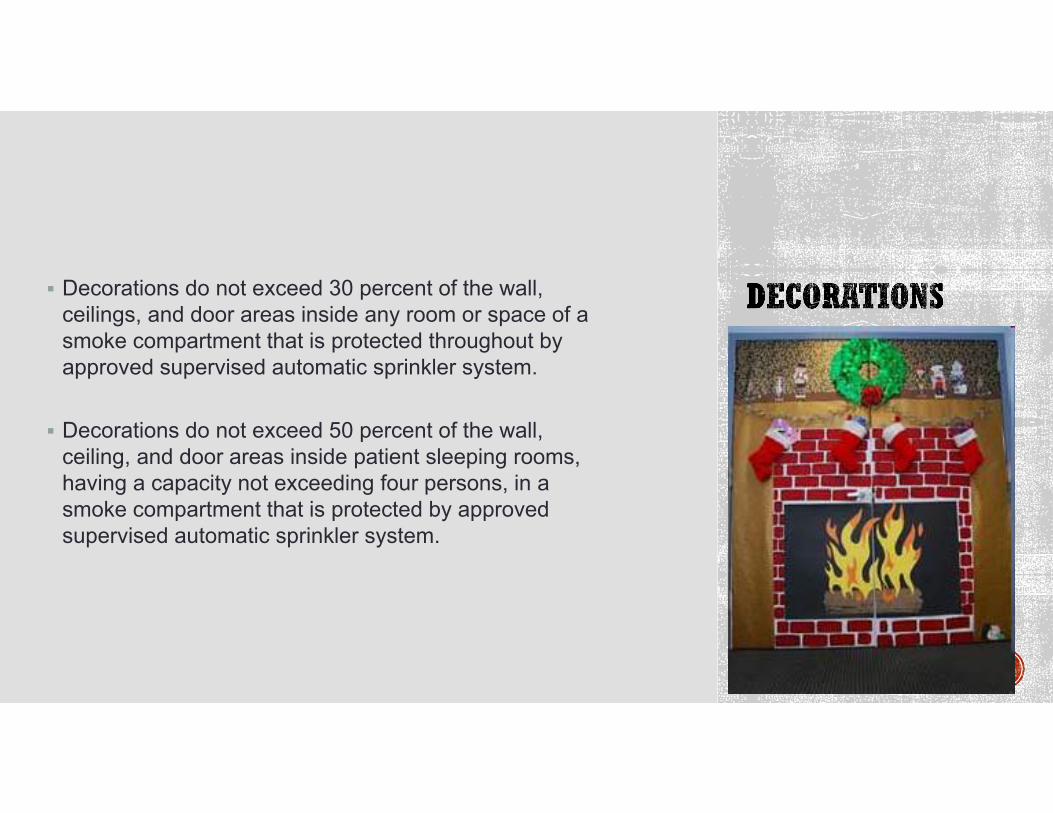
Decorations do not exceed 30 percent of the wall, ceilings, and door areas inside any room or space of a smoke compartment that is protected throughout by approved supervised automatic sprinkler system.
Decorations do not exceed 50 percent of the wall, ceiling, and door areas inside patient sleeping rooms, having a capacity not exceeding four persons, in a smoke compartment that is protected by approved supervised automatic sprinkler system.
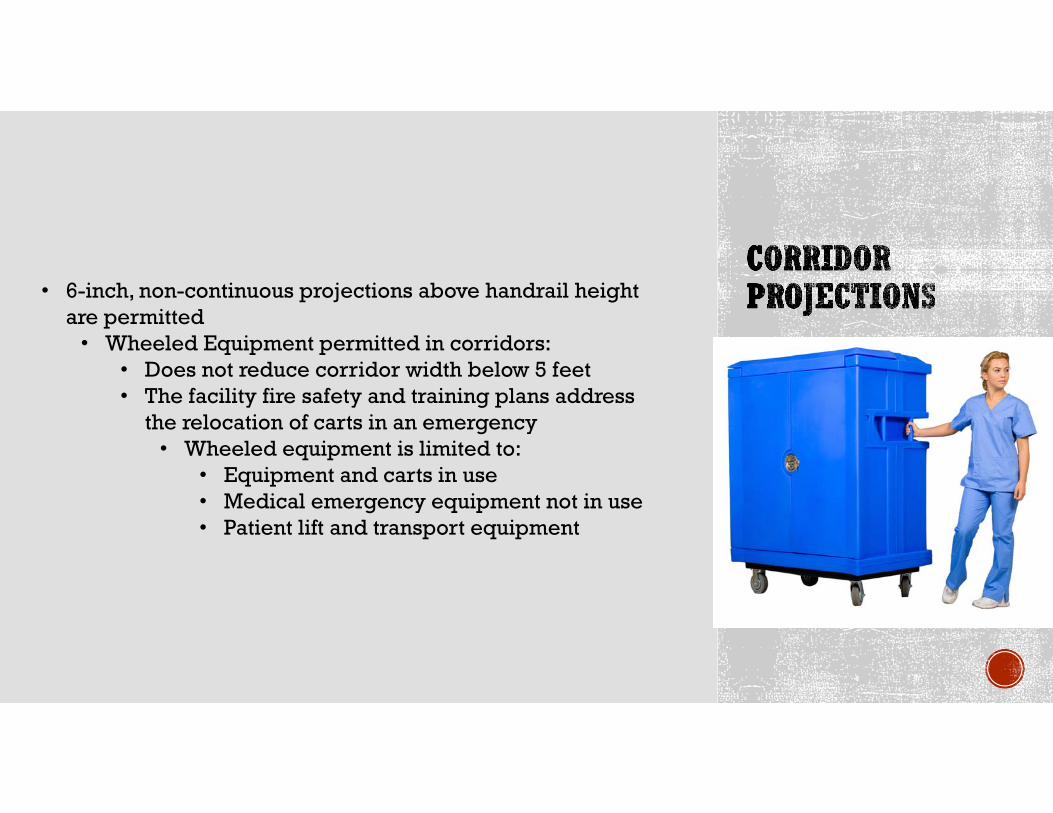
• 6-inch, non-continuous projections above handrail height are permitted
• Wheeled Equipment permitted in corridors:• Does not reduce corridor width below 5 feet• The facility fire safety and training plans address
the relocation of carts in an emergency• Wheeled equipment is limited to:
• Equipment and carts in use• Medical emergency equipment not in use• Patient lift and transport equipment
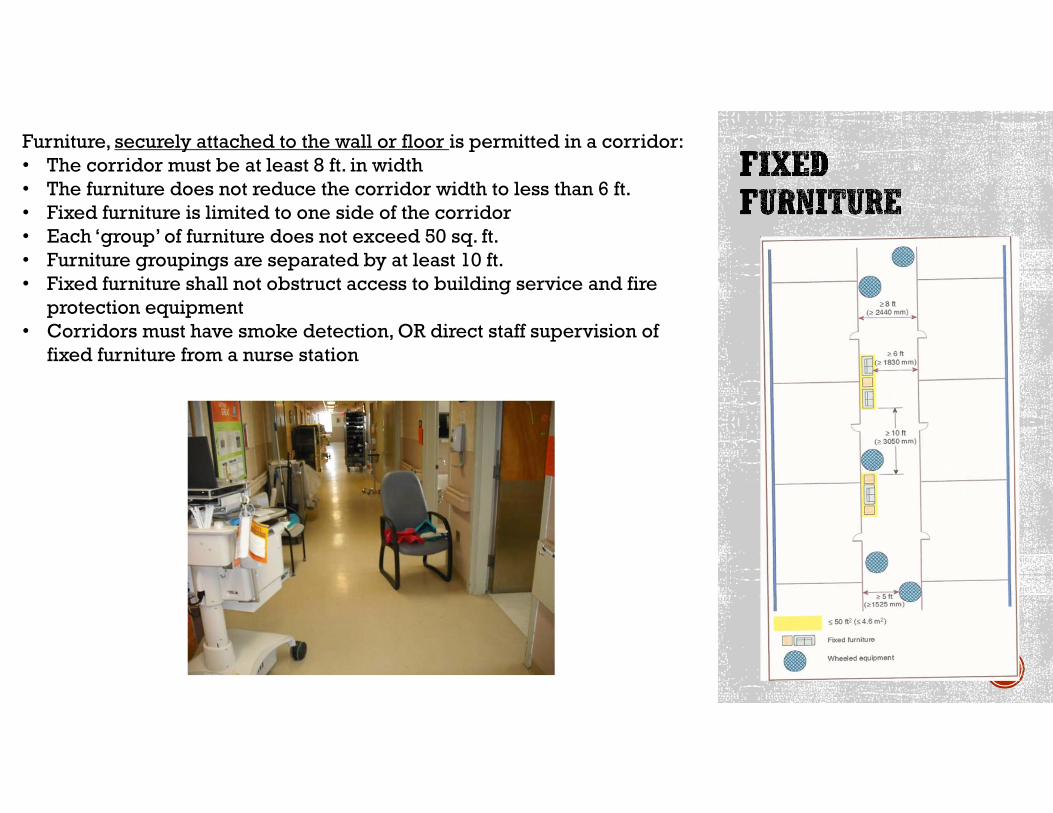
Furniture, securely attached to the wall or floor is permitted in a corridor:• The corridor must be at least 8 ft. in width• The furniture does not reduce the corridor width to less than 6 ft.• Fixed furniture is limited to one side of the corridor• Each ‘group’ of furniture does not exceed 50 sq. ft.• Furniture groupings are separated by at least 10 ft.• Fixed furniture shall not obstruct access to building service and fire
protection equipment• Corridors must have smoke detection, OR direct staff supervision of
fixed furniture from a nurse station
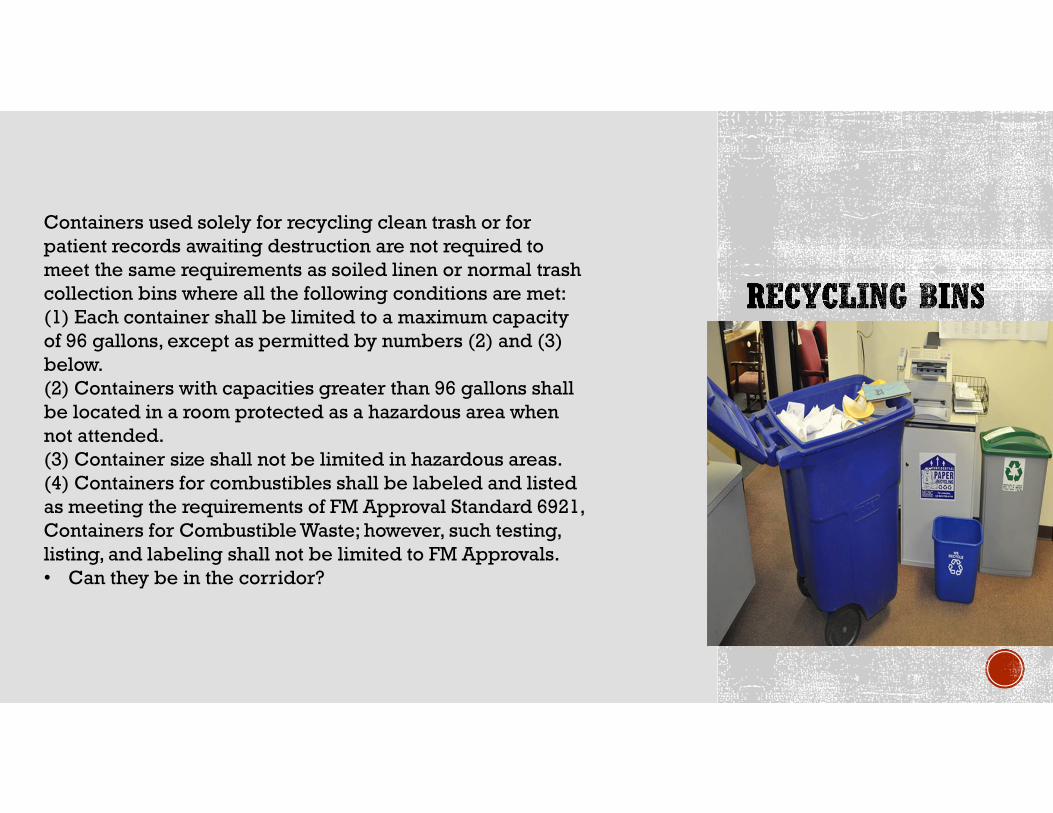
Containers used solely for recycling clean trash or for patient records awaiting destruction are not required to meet the same requirements as soiled linen or normal trash collection bins where all the following conditions are met:(1) Each container shall be limited to a maximum capacity of 96 gallons, except as permitted by numbers (2) and (3) below.(2) Containers with capacities greater than 96 gallons shall be located in a room protected as a hazardous area when not attended.(3) Container size shall not be limited in hazardous areas.(4) Containers for combustibles shall be labeled and listed as meeting the requirements of FM Approval Standard 6921, Containers for Combustible Waste; however, such testing, listing, and labeling shall not be limited to FM Approvals.• Can they be in the corridor?
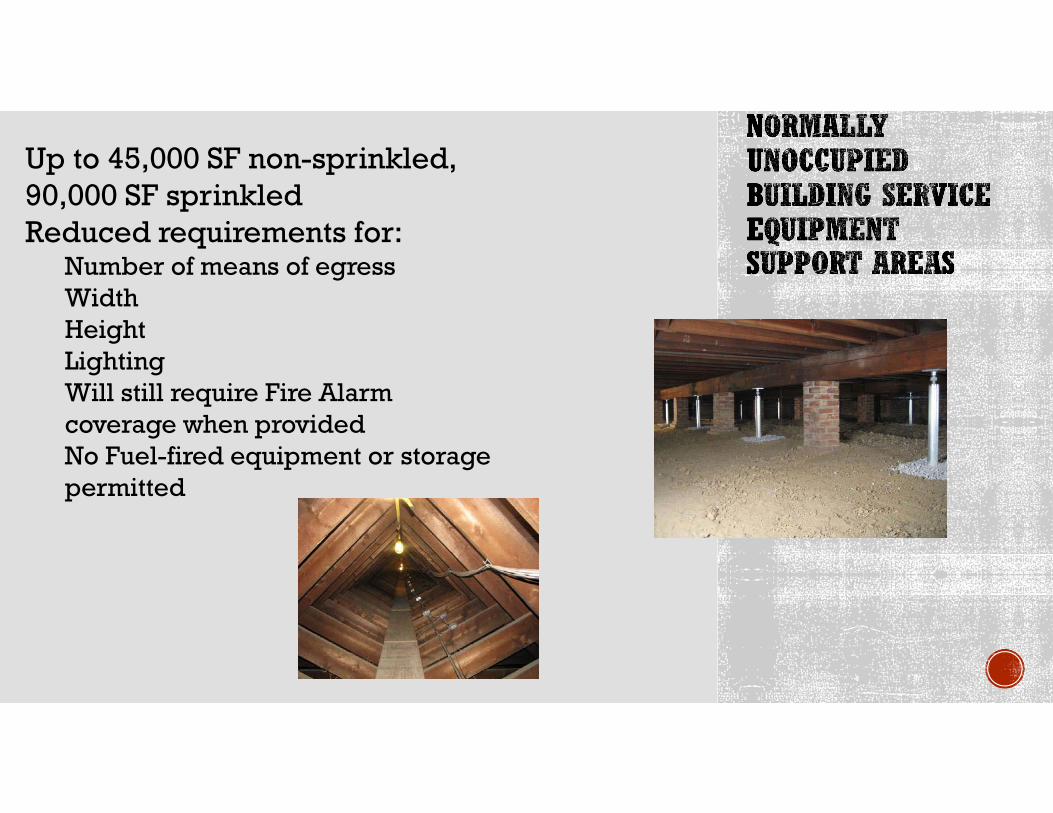
Up to 45,000 SF non-sprinkled, 90,000 SF sprinkledReduced requirements for:
Number of means of egress Width HeightLightingWill still require Fire Alarm coverage when providedNo Fuel-fired equipment or storage permitted
Related Documents











