INTERNATIONAL JOURNAL OF IMMUNOPATHOLOGY AND PHARMACOLOGY 0394-6320 (2011) Copyright © by BIOLIFE, s.a.s. This publication and/or article is for individual use only and may not be further reproduced without written permission from the copyright holder. Unauthorized reproduction may result in financial and other penalties 95 (S) Oral Squamous Cell Carcinoma (OSCC) is the sixth most common cancer and accounts for approximately 5% of all malignant tumors worldwide and a subgroup of OSCC have been demonstrated to contain anogenital HPV infection. The high risk HPV type 16 tends to be the most predominant type detected in oral cancer (1). DOUBLE DEMONSTRATION OF ONCOGENIC HIGH RISK HUMAN PAPILLOMA VIRUS DNA AND HPV-E7 PROTEIN IN ORAL CANCERS G. PANNONE* 1 , A. SANTORO 1 *, F. CARINCI 2 , P. BUFO 1,3 , S. M. PAPAGERAKIS 4 , C. RUBINI 5 , G. CAMPISI 6 , L. GIOVANNELLI 6 , M. CONTALDO 7 , R. SERPICO 7 , M. MAZZOTTA 8 , L. LO MUZIO 3,8 1 Department of Surgical Sciences, Section of Anatomic Pathology and Cytopathology, University of Foggia, Foggia, Italy 2 Department of D.M.C.C.C., Section of Maxillofacial and Plastic Surgery, University of Ferrara, Ferrara, Italy 3 IRCCS CROB, Centro di Riferimento Oncologico di Basilicata, Rionero in Vulture, Potenza, Italy 4 Department of Otolaryngology, Head and Neck Surgery and Oncology, Medical School, University of Michigan Ann Arbor, Ann Arbor, MI, USA 5 Section of Anatomic Pathology, Università Politecnica delle Marche, Ancona, Italy 6 Department of Oral Pathology, Oral Medicine Section, Palermo, Italy 7 Department of Oral Pathology Orthodontics and Oral Surgery, Institute of Biochemistry, Second University of Napoli, Napoli, Italy 8 Department of Surgical Sciences, Section of Oral Pathology, University of Foggia, Foggia, Italy *These authors have contributed to the work in the same way. Oncogenic HPVs are necessarily involved in cervical cancer but their role in oral carcinogenesis is debated. To detect HPV in oral cancer, 38 cases of formalin fixed-paraffin embedded OSCC were studied by both DNA genotyping (MY09/11 L1 consensus primers in combination with GP5-GP6 primer pair followed by sequencing) and immunohistochemistry (monoclonal Abs against capsid protein and HPV-E7 protein, K1H8 DAKO and clone 8C9 INVITROGEN, respectively). HPV-16 tonsil cancer was used as positive control. The overall prevalence of HPV infection in OSCCs was 10.5%. Amplification of DNA samples showed single HPV DNA infection in 3 cases (HPV16; HPV53; HPV70) and double infection in one case of cheek cancer (HPV31/HPV44). The overall HR- HPV prevalence was 7.5%. E-7 antigen was immunohistochemically detected in all HPV-positive cases. HPV+ OSCC cases showed an overall better outcome than HPV negative oral cancers, as evaluated by Kaplan-Meier curves. HPVs exert their oncogenic role after DNA integration, gene expression of E5, E6 and E7 loci and p53/pRb host proteins suppression. This study showed that HPV-E7 protein inactivating pRb is expressed in oral cancer cells infected by oncogenic HPV other than classical HR-HPV-16/18. Interestingly HPV-70, considered a low risk virus with no definite collocation in oncogenic type category, gives rise to the expression of HPV-E7 protein and inactivate pRb in oral cancer. HPV-70, as proved in current literature, is able to inactivates also p53 protein, promoting cell immortalization. HPV-53, classified as a possible high risk virus, expresses E7 protein in OSCC, contributing to oral carcinogenesis. We have identified among OSCCs, a subgroup characterized by HPV infection (10.5%). Finally, we have proved the oncogenic potential of some HPV virus types, not well known in literature. Key words: HPV, OSCC, oral carcinogenesis, oncogenic proteins, E-7 Corresponding author: Prof. Francesco Carinci, M.D Department of D.M.C.C.C. Section of Maxillofacial and Plastic Surgery University of Ferrara Corso Giovecca 203 44100 Ferrara ITALY E-mail: [email protected] Web: www.carinci.org Phone: +39.0532.455874; Fax: +39.0532.455582 Vol. 24, no. 2 (S), 95-101 (2011)

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

INTERNATIONAL JOURNAL OF IMMUNOPATHOLOGY AND PHARMACOLOGY
0394-6320 (2011)Copyright © by BIOLIFE, s.a.s.
This publication and/or article is for individual use only and may not be furtherreproduced without written permission from the copyright holder.
Unauthorized reproduction may result in financial and other penalties95 (S)
Oral Squamous Cell Carcinoma (OSCC) is the sixth most common cancer and accounts for approximately 5% of all malignant tumors worldwide and a subgroup of
OSCC have been demonstrated to contain anogenital HPV infection. The high risk HPV type 16 tends to be the most predominant type detected in oral cancer (1).
DOUBLE DEMONSTRATION OF ONCOGENIC HIGH RISK HUMAN PAPILLOMA VIRUS DNA AND HPV-E7 PROTEIN IN ORAL CANCERS
G. PANNONE* 1, A. SANTORO1*, F. CARINCI2, P. BUFO 1,3,S. M. PAPAGERAKIS4, C. RUBINI5, G. CAMPISI 6, L. GIOVANNELLI6,
M. CONTALDO7, R. SERPICO 7, M. MAZZOTTA8, L. LO MUZIO3,8
1Department of Surgical Sciences, Section of Anatomic Pathology and Cytopathology,University of Foggia, Foggia, Italy
2Department of D.M.C.C.C., Section of Maxillofacial and Plastic Surgery, University of Ferrara, Ferrara, Italy3IRCCS CROB, Centro di Riferimento Oncologico di Basilicata, Rionero in Vulture, Potenza, Italy
4Department of Otolaryngology, Head and Neck Surgery and Oncology, Medical School, University of Michigan Ann Arbor, Ann Arbor, MI, USA
5Section of Anatomic Pathology, Università Politecnica delle Marche, Ancona, Italy6Department of Oral Pathology, Oral Medicine Section, Palermo, Italy
7Department of Oral Pathology Orthodontics and Oral Surgery, Institute of Biochemistry,Second University of Napoli, Napoli, Italy
8Department of Surgical Sciences, Section of Oral Pathology, University of Foggia, Foggia, Italy
*These authors have contributed to the work in the same way.
Oncogenic HPVs are necessarily involved in cervical cancer but their role in oral carcinogenesis is debated. To detect HPV in oral cancer, 38 cases of formalin fixed-paraffin embedded OSCC were studied by both DNA genotyping (MY09/11 L1 consensus primers in combination with GP5-GP6 primer pair followed by sequencing) and immunohistochemistry (monoclonal Abs against capsid protein and HPV-E7 protein, K1H8 DAKO and clone 8C9 INVITROGEN, respectively). HPV-16 tonsil cancer was used as positive control. The overall prevalence of HPV infection in OSCCs was 10.5%. Amplification of DNA samples showed single HPV DNA infection in 3 cases (HPV16; HPV53; HPV70) and double infection in one case of cheek cancer (HPV31/HPV44). The overall HR-HPV prevalence was 7.5%. E-7 antigen was immunohistochemically detected in all HPV-positive cases. HPV+ OSCC cases showed an overall better outcome than HPV negative oral cancers, as evaluated by Kaplan-Meier curves. HPVs exert their oncogenic role after DNA integration, gene expression of E5, E6 and E7 loci and p53/pRb host proteins suppression. This study showed that HPV-E7 protein inactivating pRb is expressed in oral cancer cells infected by oncogenic HPV other than classical HR-HPV-16/18. Interestingly HPV-70, considered a low risk virus with no definite collocation in oncogenic type category, gives rise to the expression of HPV-E7 protein and inactivate pRb in oral cancer. HPV-70, as proved in current literature, is able to inactivates also p53 protein, promoting cell immortalization. HPV-53, classified as a possible high risk virus, expresses E7 protein in OSCC, contributing to oral carcinogenesis. We have identified among OSCCs, a subgroup characterized by HPV infection (10.5%). Finally, we have proved the oncogenic potential of some HPV virus types, not well known in literature.
Key words: HPV, OSCC, oral carcinogenesis, oncogenic proteins, E-7
Corresponding author: Prof. Francesco Carinci, M.DDepartment of D.M.C.C.C. Section of Maxillofacial and Plastic SurgeryUniversity of Ferrara Corso Giovecca 20344100 Ferrara ITALYE-mail: [email protected]: www.carinci.orgPhone: +39.0532.455874; Fax: +39.0532.455582
Vol. 24, no. 2 (S), 95-101 (2011)

96 (S) 97 (S)Int. J. Immunopathol. Pharmacol.
Registry of Tumors at the Ospedale Torrette - Ancona from 1997 to 2005.
All samples were routinely fixed in 10% neutral buffered formalin and embedded in paraffin blocks. Selection of paraffin blocks was based on examination of one haematoxylin and eosin-stained slide to estimate the malignant area of tissue. Paraffin blocks with corresponding normal epithelium distant from tumor were also selected. Surgical dissection of tumor was performed on selected paraffin blocks. Five 10 µM sections were cut from each formalin-fixed, paraffin-embedded tumor sample and transferred into microcentrifuge tubes.
Dna extractionThe paraffin samples were dissolved using xylene followed
by two washes with 100% ethanol and one wash with phosphate-buffered saline. The samples were then incubated in lysis solution (proteinase K - Qiagen, 20mg/ml, 50 micro-L; 1 M Tris HCl solution, 10 micro-L; 0,5M EDTA, 2 micro-L; 10% SDS 0.7 M) and incubating at 65°C for 4 h. DNA was recovered using the Wizard DNA clean-up kit (Promega, Madison, WI) according to the manufacturer’s protocols. To test the integrity of isolated DNA the wide beta-globin gene was amplified by PCR and visualized by gel electrophoresis for both control and pathological samples. The beta-globin gene primers used were: forward, 5’-GAA GAG CCA AGG ACA GGT AC-3’, and reverse, 5’- GGA AAA TAG ACC AAT AGG CAG 3’.
PCR analysisHPV DNA presence was researched by nested PCR (MY/
GP primers), and HPV genotype was determined by direct sequencing of PCR fragments. Three types of control were included in each reaction series: blank control, HPV-negative Wi cells as negative control and HPV-18 DNA-positive HeLa cells, in dilutions from 20,000–50,000 down to 2–5 HPV DNA copies, as positive control. HPV DNA was amplified by PCR assay (MY09–MY11 primer pair in combination with GP5–GP6 primer pair) as previously described (10) and amplifications were performed in a DNA thermal cycler (Mastercycler gradient; Eppendorf, Hamburg, Germany); amplification products were analyzed in 8% polyacrylamide gel.
Sequencing analysisHPV genotyping was based on direct sequencing of MY or
MY/GP PCR fragments. Amplification products were purified by Microcon YM-100 (Amicon-Millipore, Billerica, MA); the sequence of both DNA strands was determined by the BigDye Ready Reaction Kit in the automatic sequencer ABI Prism 310 Analyzer (both from Perkin-Elmer Applied Biosystems, Foster City, CA). Alignments were obtained from the GenBank on-line BLAST server and HPV sequences downloaded from the HPV database (http://hpv-web.lanl.gov).
Immunohistochemical analysisImmunohistochemistry was performed on the sections
mounted on poly-L-lysine-coated glass slides, by standard LSAB-HRP technique, as previously described (11, 12) using specific monoclonal antibodies against HPV-E7 (anti HPV16-E7, mouse monoclonal, Zymed Laboratories, clone 8C9; anti HPV-E7, mouse monoclonal, DAKO, clone K1H8). This type
HPVs are a group of host specific DNA virus with a remarkable epithelial cell specificity. More than 120 different HPV genotypes have been identified and almost 45 subtypes, isolated from the low genital tract, have been grouped into high- and low- risk HPV types, considering their potential risk to induce an invasive cervical cancer (2). Up to now, data about HPV prevalence in oral infection, risk factors, genetic pathway, molecular pathogenesis, and its potential oncogenic role in oral carcinogenesis are very scanty (3).
The involvement of a virus in carcinogenesis is demonstrated after its integration in host DNA with consequent expression of oncogenic proteins. (4, 5).
Therefore, the new interesting approach to the study of the oral cancer should be based on the understanding of its molecular viral background and on the detection of over-expressed viral oncoproteins. These proteins may be target of therapeutic vaccines against cancer. Indeed the L1 region of HPV DNA could not be expressed in cancer cells while HPV E-6 and E7 are necessarily involved in cancer cell blocking host tumor suppressor genes (6, 7).
Aims of this work are to detect HPV in oral cancer, to perform genotyping and demonstrate the oncogenic protein E7 in oral cancer.
The investigation of oncogenic gene expression in HPV-related OSCC and the study of its potential value as predictor of neoplastic progression and clinical outcome could allow characterization of a possible evolutive morphologycal profile of oral cancer and its precancerous lesions.
The employment of biomarkers improves the current diagnostic tools but also can contribute indirectly to therapeutics as predictor of choice for the correct clinical management.
MATERIALS AND METHODS
Study populationThe study group was composed of 38 patients with OSCC,
coming from north and middle of Italy, undergone oral maxillo-facial surgery at the ‘Ospedale Regionale Torrette - Ancona; mean age was 63.06 years (range 44–84). Informed consent was obtained from all participants or from their relatives. The histopathological diagnosis of OSCC was consecutively made at the Section of Anatomic Pathology - Università Politecnica delle Marche - Ancona, and, then, confirmed at the Section of Anatomic Pathology of the University of Foggia - Foggia. Microscopic evaluation was performed by two oral pathologists, determining the entity of inflammatory infiltrate (WADA), the degree of differentiation according to WHO grading system (8), and establishing tumor extent according to the TNM system (9).
TissuesArchival formalin-fixed, paraffin-embedded human tonsil
cancer and 38 OSCCs of oral sites were obtained from Surgery
G. PANNONE ET AL.
96 (S) 97 (S)Int. J. Immunopathol. Pharmacol.
of antibody must be used in high concentration because of the low E7 protein levels in infected cells. Only HPV DNA positive cases with strong E7 immunostaining in all cells have been considered E7 positive OSCCs.
Human HPV16+ tonsil SCC tissue was used as a positive control, and a negative control was performed by omitting incubation with primary antibody replaced by mouse IgG (DakoCytomation) diluted at the same concentration. Negative control slides without primary antibody were included for each staining.
Finally, 38 cases of formalin fixed-paraffin embedded OSCC were studied by both DNA genotyping (MY09/11 L1 consensus primers in combination with GP5-GP6 primer pair followed by sequencing) and immunohistochemistry (specific monoclonal Abs against capsid protein and HPV-E7 protein, K1H8 DAKO and clone 8C9 INVITROGEN, respectively).
RESULTS
Clinicopathological characteristics of patients and
HPV status have been shown in Table 1.The overall prevalence of HPV infection in OSCCs
was 10.5%. Amplification of DNA samples showed single HPV DNA infection in 3 cases (HPV16; HPV53; HPV70) and double infection in one case of cheek cancer (HPV31/HPV44).
The overall HR-HPV prevalence was 7.8%. E-7 antigen was immunohistochemically detected in all HPV-positive cases (Figure 1). Interestingly, the majority of HPV positive OSCCs were moderately poorly differentiated. About oral sub-site location, we founded two HR-HPV positive cases (HPV16; HPV53) and one LR-HPV (HPV70) in Waldayer’s ring area. Outside Waldayer’s area we founded just one mixed LR-HPV and HR HPV infection (HPV31-44).
Furthermore, tumor histological characteristics of HPV-positive patients differed from those of HPV-negative patients (Figure 2). HPV-positive OSCCs were
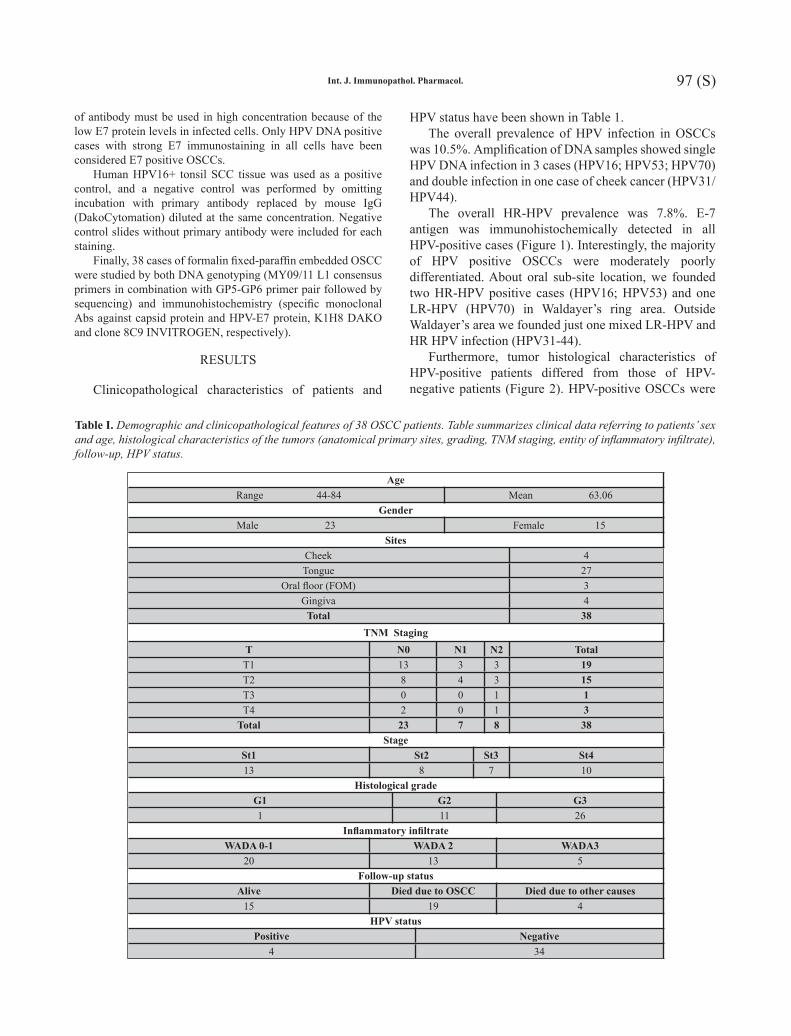
Table I. Demographic and clinicopathological features of 38 OSCC patients. Table summarizes clinical data referring to patients’ sex and age, histological characteristics of the tumors (anatomical primary sites, grading, TNM staging, entity of inflammatory infiltrate), follow-up, HPV status.
Age Range 44-84 Mean 63.06
GenderMale 23 Female 15
SitesCheek 4Tongue 27
Oral floor (FOM) 3Gingiva 4
Total 38TNM Staging
T N0 N1 N2 TotalT1 13 3 3 19T2 8 4 3 15T3 0 0 1 1T4 2 0 1 3
Total 23 7 8 38Stage
St1 St2 St3 St413 8 7 10
Histological gradeG1 G2 G31 11 26
Inflammatory infiltrateWADA 0-1 WADA 2 WADA3
20 13 5Follow-up status
Alive Died due to OSCC Died due to other causes15 19 4
HPV statusPositive Negative
4 34

98 (S) 99 (S)Int. J. Immunopathol. Pharmacol.
more likely than HPV-negative tumors to be moderately differentiated, to show areas of comedo-like necrosis and to arise prevalently from tongue-base. Since this is a mucosal associated lymphoid tissue (MALT) area HPV positive tumors show intense infiltration of resident lymphocytes, plasma cells and multinucleated giant cells.
Particularly, the HPV16 positive cancer exhibited also basaloid features, with a lobular and solid pattern of growth, peripheral palisading cell and prominent nuclear basophilia, due to high nuclear to cytoplasmic ratio, not
seen in HPV-negative squamous cell carcinomas. The morphologic hallmark of HPV infection, also known as koilocytic atypia, characterized by a sharply outlined perinuclear vacuolation, dense peripheral cytoplasm, one or multiple enlarged nucleus with undulating nuclear membrane and a rope-like chromatin pattern, was typically not plain in the major part of HPV positive tumors. Only the double infected carcinoma (HPV31/44) has shown evident sign of koilocytosis close to comedo-like necrosis areas.
All these histological findings provide further evidence that HPV-positive OSCCs are a unique morphological entity distinct from HPV-negative tumors.
HPV+ OSCC cases showed an overall better outcome than HPV-negative oral cancers, as evaluated by Kaplan-Meier curves. Following stratification by Stage we demonstrated in each group (II, III, IV; stage I excluded) a worse prognosis for HPV-negative cancer (Figure 3). Furthermore, we showed a better prognosis in HPV positive cases characterized by high chronic inflammatory infiltrate (WADA 2-3), also constituted by giant multinucleated cells and by histological areas of comedo-like necrosis, if compared to HPV negative carcinomas with low inflammatory score (WADA 0-1)(P<0.05)(Figure 3).
According to site and perineural infiltration, we have noted for each group (tongue cancers and OSCCs from other sites; with and without perineural infiltration) a worse outcome for HPV-negative carcinomas.
DISCUSSION
Several factors are involved in oral carcinogenesis, such as age, gender, ethnicity, lifestyle, genetic background, status of health and exposure to one or more oncogenic factors. In several epidemiologic studies, tobacco smoking and alcohol consumption have been well documented as major risk factors for oral cancer, with attributable fractions of approximately 90%. However, 15–20% of head-and-neck squamous cell carcinomas have no known tobacco or alcohol exposure (13). Thus, other agents, such as viruses, are being investigated. In particular, with regard to viral involvement, it is still highly controversial whether HR-HPV, widely reported as one of the prominent mechanism behind the development of squamous cell carcinoma, can also be considered an aetiological or a malignant risk factor in oral carcinogenesis (14).
Links between HPV and oral cavity cancer have been suggested, though the association is less well established. Some research groups (10) have identified HR-HPV antigens and viral DNA in potentially malignant and pre-malignant oral lesions, and others have defined HR-HPV
Fig. 1. E-7 immunostaining in all HPV-positive oral cancersNote (a) the HPV-E7 positive immunostaining in HPV-16 infected posterior tongue mucosa overlying lymphocytes in follicular aggregates with germinative centres (LSAB-HRP, nuclear counterstaining with haematoxylin, original magnification x4). The same case (b) has shown diffuse cytoplasmic staining for E-7 HPV protein in poorly differentiated neoplastic areas (LSAB-HRP, nuclear counterstaining with haematoxylin, original magnification x4. HPV-70, considered a low risk virus with no definite collocation in oncogenic type category, gives rise to the expression of HPV-E7 protein and in turn may inactivate pRb in this sample of HPV-70 positive oral cancer (c) (LSAB-HRP, nuclear counterstaining with haematoxylin, original magnification x10). An HPV-31/44 positive OSCC (d) E-7 protein is largely expressed (LSAB-HRP, nuclear counterstaining with haematoxylin, original magnification x20). An HPV-53 positive OSCC, E-7 strong citoplasmatic positivity has been observed. In the same case (f) note the massive presence of giant cells and lymphocytic infiltration (LSAB-HRP, nuclear counterstaining with haematoxylin, original magnification x40).
G. PANNONE ET AL.

98 (S) 99 (S)Int. J. Immunopathol. Pharmacol.
Fig. 2. Morphological findings of HPV infected oral cancerSome representative histological findings provided evidence that HPV-positive OSCCs are a unique morphological entity distinct from HPV-negative tumors. HPV-16 positive squamous tongue cancer exhibited diffuse basaloid features, with a lobular and solid pattern of growth, peripheral palisading cell and prominent nuclear basophilia, due to high nuclear to cytoplasmic ratio (a, H&E, original magnification x4). These tumors have shown areas of comedo-like necrosis (a; b, H&E, original magnification x10) and inflammatory infiltration of giant multinucleated cells (d, H&E, original magnification x40). The morphologic hallmark of HPV infection, also known as koilocytic atypia (c, H&E, original magnification x40), characterized by a sharply outlined perinuclear vacuolation, dense peripheral cytoplasm, one or multiple enlarged nucleus with undulating nuclear membrane and a rope-like chromatin pattern, was plain only in the double infected OSCC (HPV31/44).
Fig. 3. Disease free survival according to flogosis and tumoral stageNote the better prognosis in HPV positive cases characterized by high chronic inflammatory infiltrate (WADA 2-3), also constituted by giant multinucleated cells (a) and by histological areas of comedo-like necrosis, if compared to HPV negative carcinomas with low inflammatory score (WADA 0-1)(P<0.05). Following stratification by Stage (b) we demonstrated in each group (II, III, IV; stage I excluded) a worse prognosis for HPV-negative cancer (p<0.05).

100 (S) 101 (S)Int. J. Immunopathol. Pharmacol.
as playing an important role in OSCC, especially in the absence of common oral habits.
Consistent with the existing literature (15), our data highlighted the evidence that HPV positive oral squamous cell carcinomas are different type of cancer, with a distinct clinical history and with characteristic histological findings.
A very wide range of HPV (0-100%) prevalence in oral cancer (16) has been reported in literature and this widespread variability can only be in part due to the cancer site, geographic location and study sample size. Up to now, the exact proportion of oral cancer attributable to viral infection is unclear. The International Agency on Treatment of Cancer (IARC) Multicenter Study estimated that 18% of oro-pharynx cancers worldwide are HPV associated (17-18).
The higher percentage value of viral prevalence, reported and discussed in literature, derives from methodological bias (19), because of the HPV prevalence has been often estimated on different type of squamous cancer arisen from different sites in the head and neck district: oral cavity, Waldeyer’s area and oro-pharynx (20).
We have identified, in the oral cavity, among OSCCs, a subgroup characterized by HPV infection (10.5%), with overall HR-HPV frequency of 7.8% (2.6% respectively for HPV16, HPV31 and HPV 53), percentage values not at all unconspicuous. Furthermore, we have proved the oncogenic potential of some HPV virus types, not well known in literature. Particularly, outside Waldeyer’s ring area we have frequently detected LR-HPV (HPV44), also in association with a HR-HPV (HPV31). Interestingly, HPV-70, considered a low risk virus with no definite collocation in oncogenic type category, gives rise to the expression of HPV-E7 protein and inactivate pRb in a Waldeyer’s ring cancer. HPV-70, as proved in current literature, is able to inactivate also p53 protein, promoting cell immortalization. This study showed that HPV-E7 protein inactivating pRb is expressed in oral cancer cells infected by oncogenic LR-HPV other than classical HR-HPV16/18.
Our data underline the pathogenetic role of HPVs in oral carcinogenesis different from the classical oncogenic viruses detected in cervical squamous cell carcinomas. We have proved that LR-HPVs and potential high risk viruses with a not well known oncogenic potential may take part in oral carcinogenesis, by inhibiting p53 and by strengthening the oncogenic activity of HR-HPVs.
In our study, HPV DNA was detected by both PCR analyses, DNA genotyping followed by sequencing and by immunohistochemical valuation of E7 oncoprotein.
In this study, we have observed a subgroup of oral cancer characterized by HPV infection, we have proved the existence of an oncogenic potential for viruses, known for their low risk oncogenicity or for their no definite
collocation in a risk category. We also retain that only standardized technical procedures could assist clinicians to provide innovative and effective treatment and more efficient screening systems for OSCC patients. A specific panel of different HPV types, possibly including LR and HR-viruses, should be defined in order to prepare adequate vaccine reducing the risk of HPV positive oropharyngeal cancers in male and female population.
ACKNOWLEDGEMENTS
First of all, we thank all our patients or their relatives for their voluntary participation in this study. Then, a particular thanks to Maria Carmela Pedicillo and Simona Cagiano, for their fundamental technical contribution. This work was partly supported by Fondazione Cassa di Risparmio di Puglia (Progetto integrato per la salvaguardia della salute dell’uomo), and by MURST-PRIN (Italian Ministry of University Science and Technology, 2007 - prot. 2007YMS5NS-001.
REFERENCES
1. Fakhry C, Westra WH, Li S, Cmelak A, Ridge JA, Pinto H, Forastiere A,Gillison ML. Improved survival of patients with human papillomavirus-positive head and neck squamous cell carcinoma in a prospective clinical trial. J Natl Cancer Inst 2008; 100:261-9.
2. Campisi G,Giovannelli L. Controversies surrounding human papilloma virus infection, head & neck vs oral cancer, implications for prophylaxis and treatment. Head Neck Oncol 2009; 1:8.
3. Szarka K, Tar I, Feher E, Gall T, Kis A, Toth ED, Boda R, Marton I,Gergely L. Progressive increase of human papillomavirus carriage rates in potentially malignant and malignant oral disorders with increasing malignant potential. Oral Microbiol Immunol 2009; 24:314-8.
4. Martin CM, Astbury K, McEvoy L, O’Toole S, Sheils O,O’Leary JJ. Gene expression profiling in cervical cancer: identification of novel markers for disease diagnosis and therapy. Methods Mol Biol 2009; 511:333-59.
5. Rampias T, Sasaki C, Weinberger P,Psyrri A. E6 and e7 gene silencing and transformed phenotype of human papillomavirus 16-positive oropharyngeal cancer cells. J Natl Cancer Inst 2009; 101:412-23.
6. Preville X, Ladant D, Timmerman B,Leclerc C. Eradication of established tumors by vaccination with recombinant Bordetella pertussis adenylate cyclase carrying the human papillomavirus 16 E7 oncoprotein. Cancer Res 2005; 65:641-9.
7. Shillitoe EJ. The role of viruses in squamous cell carcinoma
G. PANNONE ET AL.

100 (S) 101 (S)Int. J. Immunopathol. Pharmacol.
of the oropharyngeal mucosa. Oral Oncol 2009; 45:351-5.8. Poh CF, Ng S, Berean KW, Williams PM, Rosin
MP,Zhang L. Biopsy and histopathologic diagnosis of oral premalignant and malignant lesions. J Can Dent Assoc 2008; 74:283-8.
9. de Araujo RF, Jr., Barboza CA, Clebis NK, de Moura SA,Lopes Costa Ade L. Prognostic significance of the anatomical location and TNM clinical classification in oral squamous cell carcinoma. Med Oral Patol Oral Cir Bucal 2008; 13:E344-7.
10. Campisi G, Di Fede O, Giovannelli L, Capra G, Greco I, Calvino F, Maria Florena A,Lo Muzio L. Use of fuzzy neural networks in modeling relationships of HPV infection with apoptotic and proliferation markers in potentially malignant oral lesions. Oral Oncol 2005; 41:994-1004.
11. Morshed K, Korobowicz E, Szymanski M, Skomra D, Golabek W. Immunohistochemical demonstration of multiple HPV types in laryngeal squamous cell carcinoma. Eur Arch Otorhinolaryngol 2005; 262:917-20.
12. Handa K, Yugawa T, Narisawa-Saito M, Ohno S, Fujita M,Kiyono T. E6AP-dependent degradation of DLG4/PSD95 by high-risk human papillomavirus type 18 E6 protein. J Virol 2007; 81:1379-89.
13. Jo S, Juhasz A, Zhang K, Ruel C, Loera S, Wilczynski SP, Yen Y, Liu X, Ellenhorn J, Lim D, Paz B, Somlo G, Vora N,Shibata S. Human papillomavirus infection as a prognostic factor in oropharyngeal squamous cell carcinomas treated in a prospective phase II clinical trial.
Anticancer Res 2009; 29:1467-74.14. Chaudhary AK, Singh M, Sundaram S,Mehrotra R. Role
of human papillomavirus and its detection in potentially malignant and malignant head and neck lesions: updated review. Head Neck Oncol 2009; 1:22.
15. Kadaja M, Isok-Paas H, Laos T, Ustav E,Ustav M. Mechanism of genomic instability in cells infected with the high-risk human papillomaviruses. PLoS Pathog 2009; 5:e1000397.
16. Hennessey PT, Westra WH,Califano JA. Human papillomavirus and head and neck squamous cell carcinoma: recent evidence and clinical implications. J Dent Res 2009; 88:300-6.
17. Tachezy R, Klozar J, Rubenstein L, Smith E, Salakova M, Smahelova J, Ludvikova V, Rotnaglova E, Kodet R,Hamsikova E. Demographic and risk factors in patients with head and neck tumors. J Med Virol 2009; 81:878-87.
18. Petersen PE. Oral cancer prevention and control--the approach of the World Health Organization. Oral Oncol 2009; 45:454-60.
19. Kreimer AR, Clifford GM, Boyle P, Franceschi S. Human papillomavirus types in head and neck squamous cell carcinomas worldwide: a systematic review. Cancer Epidemiol Biomarkers Prev 2005; 14:467-75.
20. Scapoli L, Palmieri A, Rubini C, Martinelli M, Spinelli G, Ionna F, Carinci F. Low prevalence of human papillomavirus in squamous-cell carcinoma limited to oral cavity proper. Mod Pathol 2009; 22:366-72.
Related Documents











