This content has been downloaded from IOPscience. Please scroll down to see the full text. Download details: IP Address: 221.130.17.57 This content was downloaded on 11/10/2013 at 09:32 Please note that terms and conditions apply. Dosimetric parameters for small field sizes using Fricke xylenol gel, thermoluminescent and film dosimeters, and an ionization chamber View the table of contents for this issue, or go to the journal homepage for more 2007 Phys. Med. Biol. 52 1431 (http://iopscience.iop.org/0031-9155/52/5/014) Home Search Collections Journals About Contact us My IOPscience

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
This content has been downloaded from IOPscience. Please scroll down to see the full text.
Download details:
IP Address: 221.130.17.57
This content was downloaded on 11/10/2013 at 09:32
Please note that terms and conditions apply.
Dosimetric parameters for small field sizes using Fricke xylenol gel, thermoluminescent and
film dosimeters, and an ionization chamber
View the table of contents for this issue, or go to the journal homepage for more
2007 Phys. Med. Biol. 52 1431
(http://iopscience.iop.org/0031-9155/52/5/014)
Home Search Collections Journals About Contact us My IOPscience

IOP PUBLISHING PHYSICS IN MEDICINE AND BIOLOGY
Phys. Med. Biol. 52 (2007) 1431–1439 doi:10.1088/0031-9155/52/5/014
Dosimetric parameters for small field sizes usingFricke xylenol gel, thermoluminescent and filmdosimeters, and an ionization chamber
Carmen S Guzman Calcina1,2, Lucas N de Oliveira1,Carlos E de Almeida2 and Adelaide de Almeida1
1 Departamento de Fısica e Matematica, Faculdade de Filosofia, Ciencias e Letras de RibeiraoPreto, Universidade do Sao Paulo, Ribeirao Preto, Brazil2 Laboratorio de Ciencias Radiologicas, Universidade do Estado de Rio de Janeiro,Rio de Janeiro, Brazil
E-mail: [email protected]
Received 27 June 2006, in final form 3 January 2007Published 9 February 2007Online at stacks.iop.org/PMB/52/1431
AbstractDosimetric measurements in small therapeutic x-ray beam field sizes, suchas those used in radiosurgery, that have dimensions comparable to or smallerthan the build-up depth, require special care to avoid incorrect interpretationof measurements in regions of high gradients and electronic disequilibrium.These regions occur at the edges of any collimated field, and can extendto the centre of small fields. An inappropriate dosimeter can result in anunderestimation, which would lead to an overdose to the patient. We haveperformed a study of square and circular small field sizes of 6 MV photonsusing a thermoluminescent dosimeter (TLD), Fricke xylenol gel (FXG) andfilm dosimeters. PMMA phantoms were employed to measure lateral beamprofiles (1 × 1, 3 × 3 and 5 × 5 cm2 for square fields and 1, 2 and 4 cmdiameter circular fields), the percentage depth dose, the tissue maximum ratioand the output factor. An ionization chamber (IC) was used for calibrationand comparison. Our results demonstrate that high resolution FXG, TLD andfilm dosimeters agree with each other, and that an ionization chamber, withlow lateral resolution, underestimates the absorbed dose. Our results showthat, when planning small field radiotherapy, dosimeters with adequate lateralspatial resolution and tissue equivalence are required to provide an accuratebasic beam data set to correctly calculate the absorbed dose in regions ofelectronic disequilibrium.
Introduction
Clinical applications of radiation require precise planning and dosimetric measurements.Radiotherapeutic applications of ionizing radiation are expected to deliver to the patient an
0031-9155/07/051431+09$30.00 © 2007 IOP Publishing Ltd Printed in the UK 1431
1432 C S G Calcina et al
absorbed dose within 5% of that prescribed by the physician (ICRU 1976). For a number ofreasons, the dosimetric planning of small radiation fields is more critical than that for largefields. A field is considered large when its dimensions at the entrance to the patient are largecompared with the distance for the lateral decrease of absorbed dose inside the patient nearthe geometrical limits imposed by the collimators. This definition is applied here.
The absorbed dose at the edge of any size radiation field at the patient departs from thatdefined by the source/collimator geometry owing to scattering of the primary radiation, andowing to the fact that secondary radiation, electrons in this paper, is projected in all directions.The latter effect produces a lateral electronic disequilibrium (DEL) at the edge of the field inthe patient. For the same reason that electronic equilibrium is not established near the patiententry surface, it is lost at the edge of the field inside the patient. Moreover, the dimensionsof the profile at the field edge are comparable to the distance required to establish electronicequilibrium at the surface, the build-up distance. Both effects result in energy being absorbedoutside the defined field and less energy absorbed inside the field, even at the centre of thefield (Laub and Wong 2003, Serago et al 1992, Perucha et al 2003, Mack et al 2002).
When small radiation fields are used, the lateral profile of absorbed dose becomes aconcern for the physicist. If the dosimetric measurements across a small field are made withpoor spatial resolution, the result will be a lower dose than the true value due to volumeaveraging. This is a potentially serious error leading to overdosing the patient. Planningsmall field photon therapy requires that dosimeters, in addition of being tissue equivalentsuch that electronic disequilibrium at the field boundary is not perturbed, have small lateralspatial resolution compared with the build-up depth for those photons. Dosimeters should beindependent of the energy and direction of the secondary electrons (Mack et al 2002, Bjarngardet al 1990, Westermark et al 2000, Sanchez-Doblado et al 2003).
The literature has presented several types of photon detectors suitable for small fieldsize dosimetry, such as those required in radiosurgery. For radiosurgery, several researchershave investigated sensors with high resolution and compositions equivalent to soft tissue.Small field size dosimetry has been accomplished with diodes, films, thermoluminescentsand ionization chambers. With adequate characteristics, each has been shown to be usefulfor photon beam parameter measurements such as tissue maximum ratio (TMR), percentagedepth dose (PDD), output factor (OF) and beam profile (BF). Film sensors (McLaughlin andSoares 1994, Robar and Clark 1999), diamond sensors (De Vlamynck et al 1999, Heydarianet al 1996) and reviews involving comparisons between several types of sensors (Heydarianet al 1996, Duggan and Coffey 1998) have been reported in the literature.
In this work we study the beam parameters related to a 6 MV x-ray beam for smallfield sizes using TLD, film, an ionization chamber and our chemical FXG dosimeter. Wedemonstrate that a properly designed (Costa 2001, Felipe 2003, Caldeira Filho 2004) FXGdosimeter is adequate for small field size photon dosimetry. This dosimeter is derived fromthe standard Fricke solution, plus swine skin gelatin and orange xylenol. Its composition hasFe+2, that once irradiated is oxidized to Fe+3, that forms a complex with the orange xylenol.Optical absorbance measurements give a linear dependence on the absorbed dose. The FXGdosimeter is a true 3D dosimeter and the lateral and depth resolutions depend critically on thedirection and collimation of the optical beam used for absorbance measurements.
We report experimental procedures for correct dosimetry in homogeneous phantoms usingfour different dosimeters with millimetric spatial resolution. Lateral profiles and central fielddepth profiles of the absorbed dose were measured for incident x-rays produced by a 6 MVLINAC. The ratio of the central field dose for small fields with that for larger fields, the relativeoutput factor, was measured with each detector for each radiation condition. The experimentalconditions are described in the next section.
Dosimetric parameters for small field sizes using Fricke xylenol gel, TLD and IC 1433
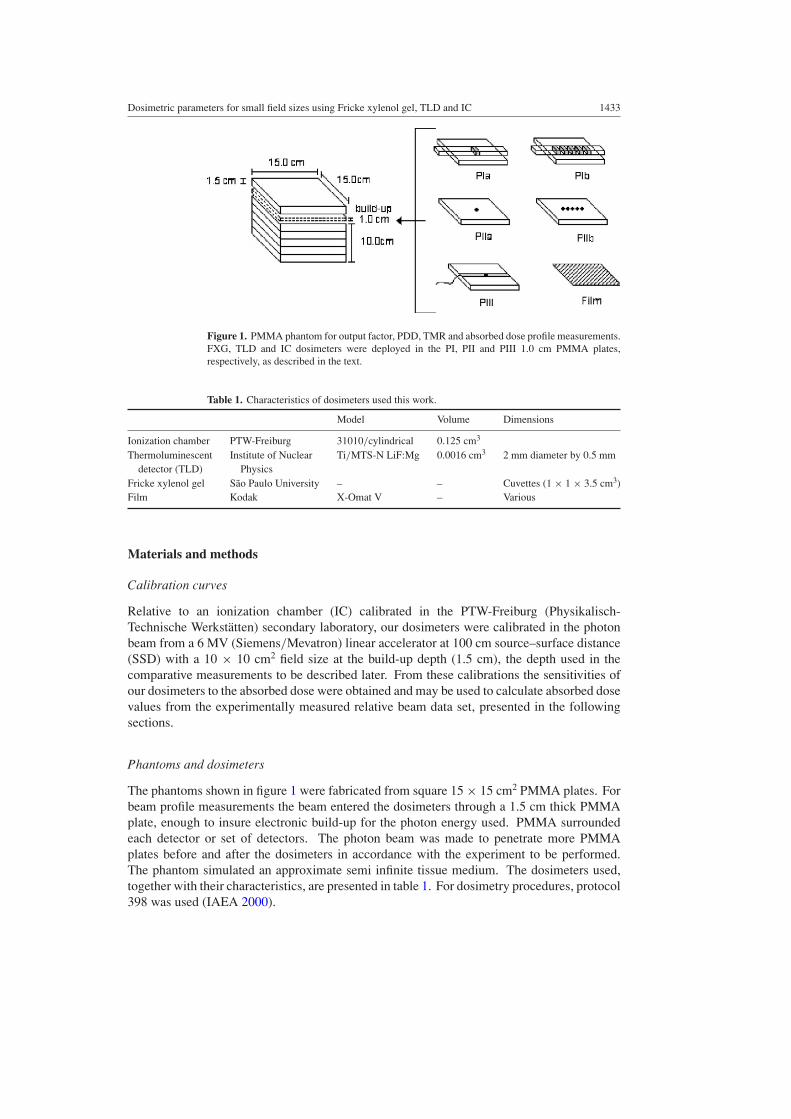
Figure 1. PMMA phantom for output factor, PDD, TMR and absorbed dose profile measurements.FXG, TLD and IC dosimeters were deployed in the PI, PII and PIII 1.0 cm PMMA plates,respectively, as described in the text.
Table 1. Characteristics of dosimeters used this work.
Model Volume Dimensions
Ionization chamber PTW-Freiburg 31010/cylindrical 0.125 cm3
Thermoluminescent Institute of Nuclear Ti/MTS-N LiF:Mg 0.0016 cm3 2 mm diameter by 0.5 mmdetector (TLD) Physics
Fricke xylenol gel Sao Paulo University – – Cuvettes (1 × 1 × 3.5 cm3)Film Kodak X-Omat V – Various
Materials and methods
Calibration curves
Relative to an ionization chamber (IC) calibrated in the PTW-Freiburg (Physikalisch-Technische Werkstatten) secondary laboratory, our dosimeters were calibrated in the photonbeam from a 6 MV (Siemens/Mevatron) linear accelerator at 100 cm source–surface distance(SSD) with a 10 × 10 cm2 field size at the build-up depth (1.5 cm), the depth used in thecomparative measurements to be described later. From these calibrations the sensitivities ofour dosimeters to the absorbed dose were obtained and may be used to calculate absorbed dosevalues from the experimentally measured relative beam data set, presented in the followingsections.
Phantoms and dosimeters
The phantoms shown in figure 1 were fabricated from square 15 × 15 cm2 PMMA plates. Forbeam profile measurements the beam entered the dosimeters through a 1.5 cm thick PMMAplate, enough to insure electronic build-up for the photon energy used. PMMA surroundedeach detector or set of detectors. The photon beam was made to penetrate more PMMAplates before and after the dosimeters in accordance with the experiment to be performed.The phantom simulated an approximate semi infinite tissue medium. The dosimeters used,together with their characteristics, are presented in table 1. For dosimetry procedures, protocol398 was used (IAEA 2000).
1434 C S G Calcina et al
The optical densities of the FXG and film dosimeters were determined with light beamsof diameters 2 and 1 mm, respectively. These diameters, and the 2 mm diameter of the TLDdosimeter, determine the lateral spatial resolution of the respective dosimeters.
The development and characteristics of our FXG and reading system are describedelsewhere (Bero et al 1999, Costa 2001, Felipe 2003, Caldeira Filho 2004). The FXGhas good sensitivity for low absorbed dose and can be used for radiotherapic dosimetry (Beroet al 1999, Costa 2001). It has linear dependence on the absorbed dose from 0.5 to 30 Gy forγ - and x-ray photons, atomic effective number of 7.75 and density of 1.139 g cm−3, near to7.64 and 1.040 g cm−3, respectively, for soft tissue.
For 6 MV photons (Compton region) the energy dependence of all sensors is less, sincesensitivity depends only on the electronic density of the target material. Attix has observedthat the Fricke energy dependence is almost non-existent for high energy photons (Attix andWillian 1996).
Output factor
The output factor is the ratio between the observed absorbed dose at the centre of a particularfield size and that from a large reference field size, both measurements made at the build-updepth in a phantom with all other irradiation conditions identical. We obtained the OF usingeach detector described, after 6 MV photons exposure incident on an appropriate phantom(figure 1) for a 100 cm SSD. Field sizes were varied from 0.5 × 0.5 to 10 × 10 cm2 square(Varian/Clinac 2100) and from 1.0 to 4.0 cm circular diameter (Siemens/Mevatron). Threemeasurements were made and averaged after an absorbed dose of 3 Gy for each field sizeand for each detector, except for film that received 1.1 Gy. The IC was irradiated in the PIIIphantom oriented perpendicular to the beam axis for square and circular fields. The FXGdosimeter in a PMMA cuvette was irradiated in the PIa phantom and the TLD was irradiatedin the phantom PIIa. All dosimeters were deployed under the 1.5 cm PMMA build-up plate.
The largest fields (10 × 10 cm2 square and 4 cm circular diameter) were used as referencesfor normalizing the measurements for smaller fields.
Percentage depth dose and tissue maximum ratio
The prescribed absorbed dose determines the time when the patient will be irradiated. Theirradiation time is calculated from the results of dosimetric measurements of the absorbed dosedistribution functions in the medium for each beam energy and geometry, tumour depth andthe radiation source absorbed dose rate. Two functions can be used for the calculations: thepercentage depth dose and the tissue maximum ratio. Both are measured with a dosimeter atthe centre of a radiation field by adding a tissue equivalent material between the photon sourceand the dosimeter. The PDD measurement is accomplished while maintaining the sourceto phantom surface distance (SSD) constant. The TMR is measured while maintaining thedosimeter at a constant distance from the photon source. The source to axis distance (SAD) isconstant such that the dose absorbed by the tumour is independent of the beam divergence anddepends only on the field size at that point and attenuation in the overlying tissue (Khan 1997).
The PDD and TMR functions depend on the collimator aperture, thickness of tissueequivalent material between source and dosimeter, on the beam quality and on the lateralspatial resolution of the dosimeter. They are commonly expressed as the absorbed dose at adepth of interest relative to the absorbed dose at the build-up depth.
Measurements were taken at the centre of each square and circular radiation field, thesame fields as those used for the OF measurements. For FXG, TLD and film dosimeters, three
Dosimetric parameters for small field sizes using Fricke xylenol gel, TLD and IC 1435
(a)
(b)
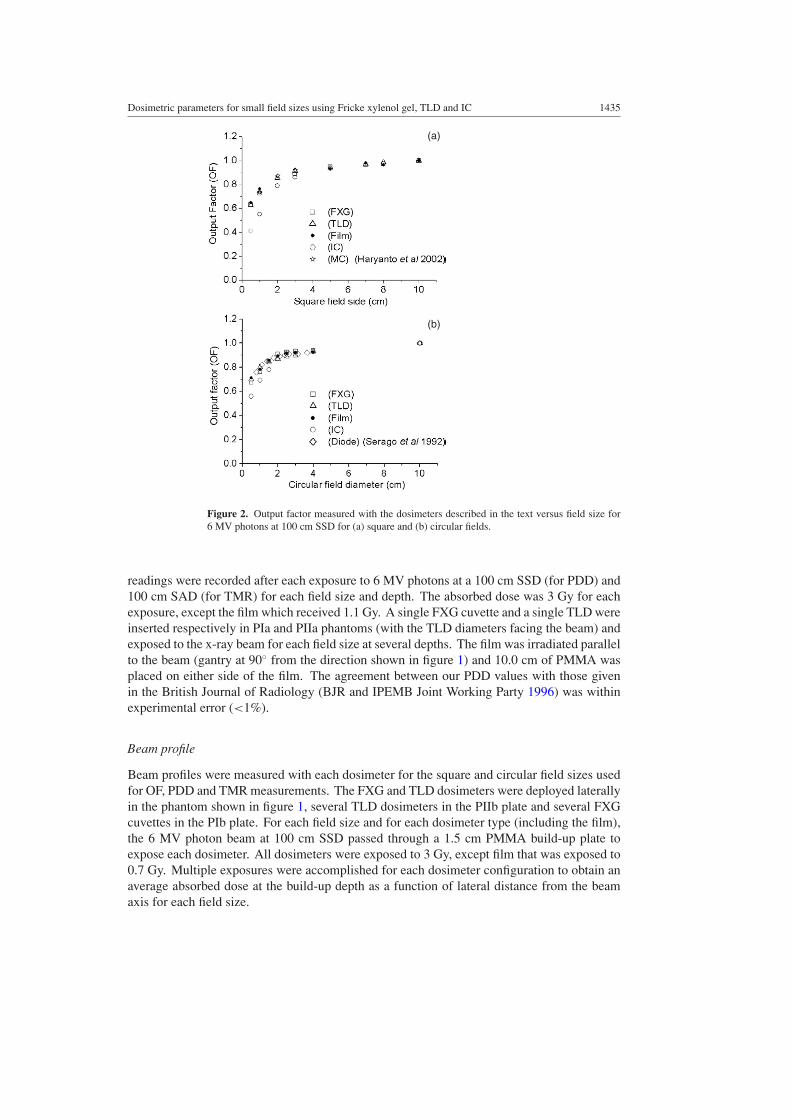
Figure 2. Output factor measured with the dosimeters described in the text versus field size for6 MV photons at 100 cm SSD for (a) square and (b) circular fields.
readings were recorded after each exposure to 6 MV photons at a 100 cm SSD (for PDD) and100 cm SAD (for TMR) for each field size and depth. The absorbed dose was 3 Gy for eachexposure, except the film which received 1.1 Gy. A single FXG cuvette and a single TLD wereinserted respectively in PIa and PIIa phantoms (with the TLD diameters facing the beam) andexposed to the x-ray beam for each field size at several depths. The film was irradiated parallelto the beam (gantry at 90◦ from the direction shown in figure 1) and 10.0 cm of PMMA wasplaced on either side of the film. The agreement between our PDD values with those givenin the British Journal of Radiology (BJR and IPEMB Joint Working Party 1996) was withinexperimental error (<1%).
Beam profile
Beam profiles were measured with each dosimeter for the square and circular field sizes usedfor OF, PDD and TMR measurements. The FXG and TLD dosimeters were deployed laterallyin the phantom shown in figure 1, several TLD dosimeters in the PIIb plate and several FXGcuvettes in the PIb plate. For each field size and for each dosimeter type (including the film),the 6 MV photon beam at 100 cm SSD passed through a 1.5 cm PMMA build-up plate toexpose each dosimeter. All dosimeters were exposed to 3 Gy, except film that was exposed to0.7 Gy. Multiple exposures were accomplished for each dosimeter configuration to obtain anaverage absorbed dose at the build-up depth as a function of lateral distance from the beamaxis for each field size.
1436 C S G Calcina et al
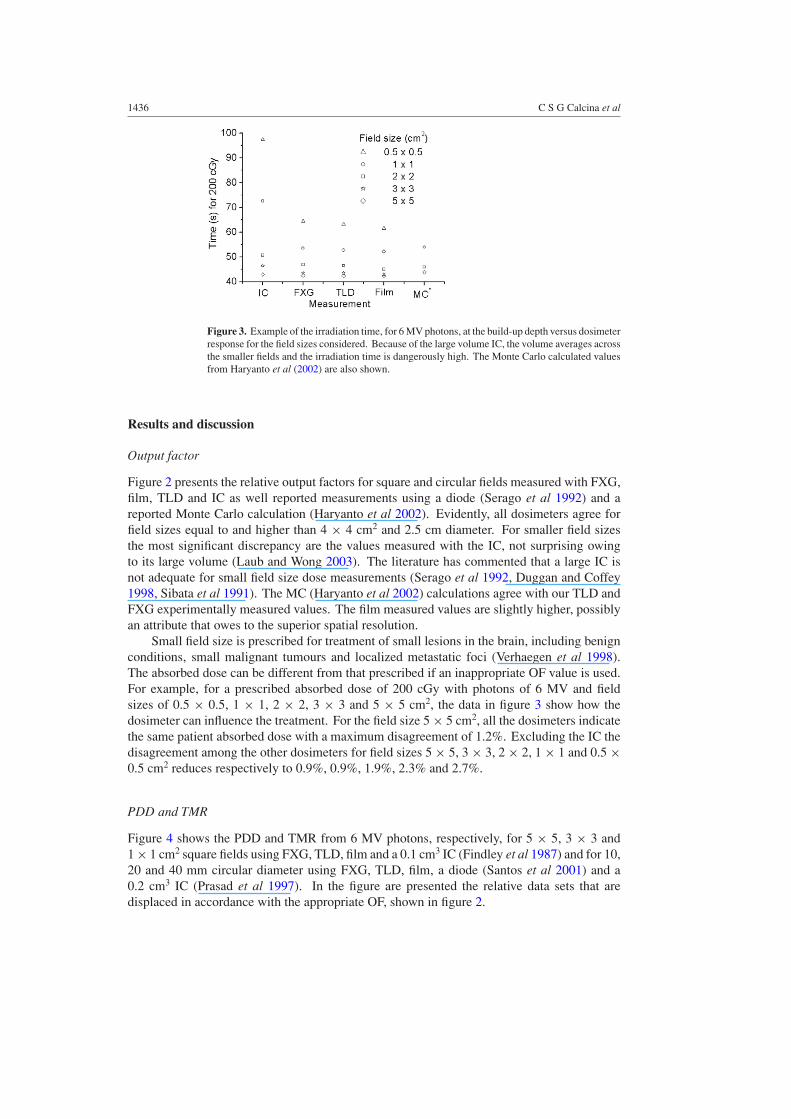
Figure 3. Example of the irradiation time, for 6 MV photons, at the build-up depth versus dosimeterresponse for the field sizes considered. Because of the large volume IC, the volume averages acrossthe smaller fields and the irradiation time is dangerously high. The Monte Carlo calculated valuesfrom Haryanto et al (2002) are also shown.
Results and discussion
Output factor
Figure 2 presents the relative output factors for square and circular fields measured with FXG,film, TLD and IC as well reported measurements using a diode (Serago et al 1992) and areported Monte Carlo calculation (Haryanto et al 2002). Evidently, all dosimeters agree forfield sizes equal to and higher than 4 × 4 cm2 and 2.5 cm diameter. For smaller field sizesthe most significant discrepancy are the values measured with the IC, not surprising owingto its large volume (Laub and Wong 2003). The literature has commented that a large IC isnot adequate for small field size dose measurements (Serago et al 1992, Duggan and Coffey1998, Sibata et al 1991). The MC (Haryanto et al 2002) calculations agree with our TLD andFXG experimentally measured values. The film measured values are slightly higher, possiblyan attribute that owes to the superior spatial resolution.
Small field size is prescribed for treatment of small lesions in the brain, including benignconditions, small malignant tumours and localized metastatic foci (Verhaegen et al 1998).The absorbed dose can be different from that prescribed if an inappropriate OF value is used.For example, for a prescribed absorbed dose of 200 cGy with photons of 6 MV and fieldsizes of 0.5 × 0.5, 1 × 1, 2 × 2, 3 × 3 and 5 × 5 cm2, the data in figure 3 show how thedosimeter can influence the treatment. For the field size 5 × 5 cm2, all the dosimeters indicatethe same patient absorbed dose with a maximum disagreement of 1.2%. Excluding the IC thedisagreement among the other dosimeters for field sizes 5 × 5, 3 × 3, 2 × 2, 1 × 1 and 0.5 ×0.5 cm2 reduces respectively to 0.9%, 0.9%, 1.9%, 2.3% and 2.7%.
PDD and TMR
Figure 4 shows the PDD and TMR from 6 MV photons, respectively, for 5 × 5, 3 × 3 and1 × 1 cm2 square fields using FXG, TLD, film and a 0.1 cm3 IC (Findley et al 1987) and for 10,20 and 40 mm circular diameter using FXG, TLD, film, a diode (Santos et al 2001) and a0.2 cm3 IC (Prasad et al 1997). In the figure are presented the relative data sets that aredisplaced in accordance with the appropriate OF, shown in figure 2.
Dosimetric parameters for small field sizes using Fricke xylenol gel, TLD and IC 1437
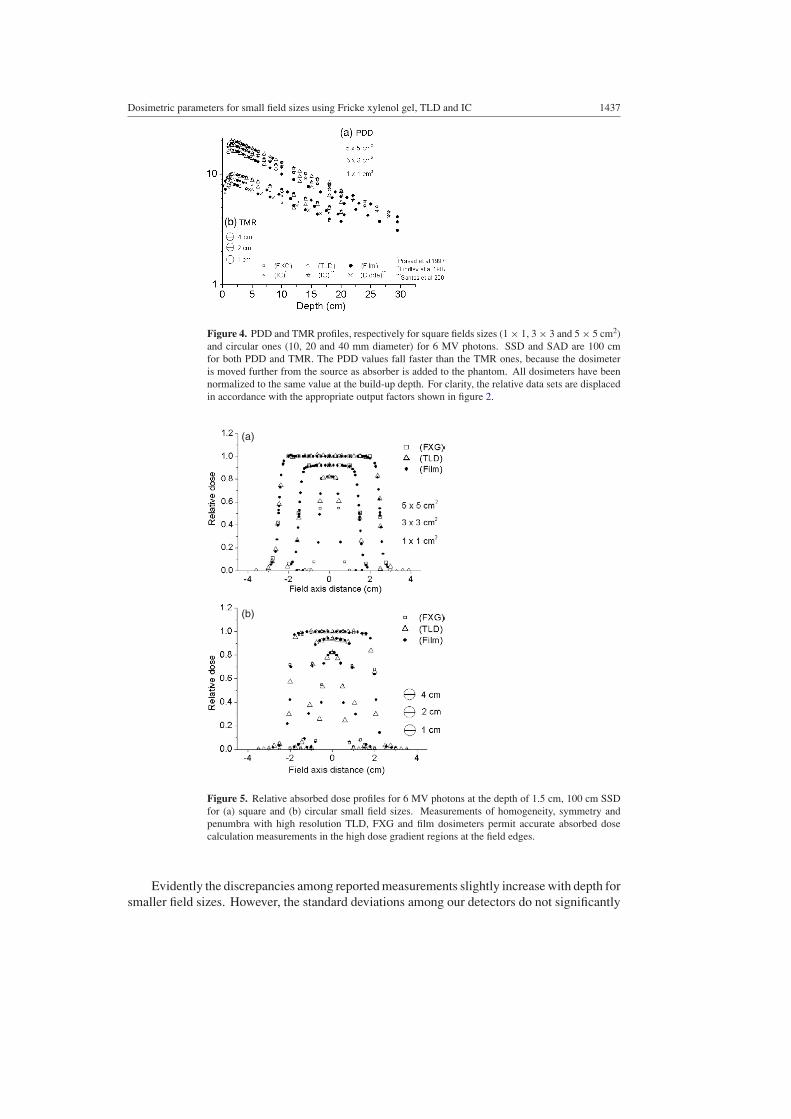
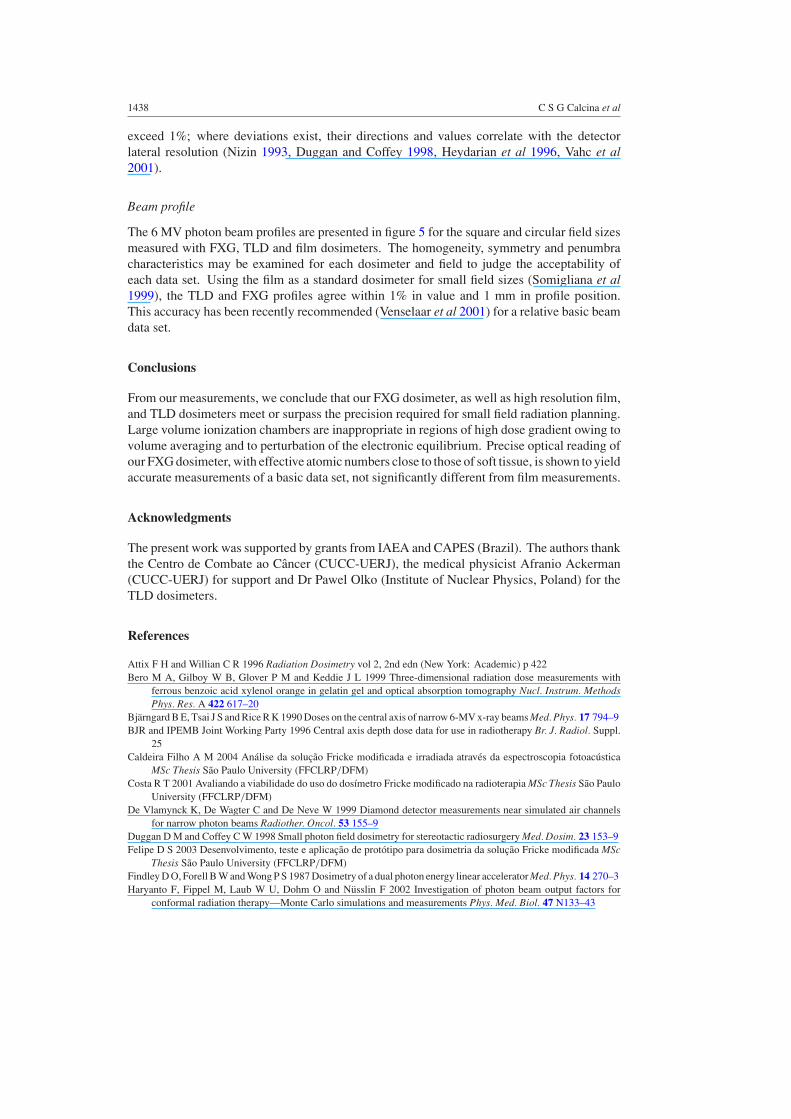
Figure 4. PDD and TMR profiles, respectively for square fields sizes (1 × 1, 3 × 3 and 5 × 5 cm2)and circular ones (10, 20 and 40 mm diameter) for 6 MV photons. SSD and SAD are 100 cmfor both PDD and TMR. The PDD values fall faster than the TMR ones, because the dosimeteris moved further from the source as absorber is added to the phantom. All dosimeters have beennormalized to the same value at the build-up depth. For clarity, the relative data sets are displacedin accordance with the appropriate output factors shown in figure 2.
(b)
(a)
Figure 5. Relative absorbed dose profiles for 6 MV photons at the depth of 1.5 cm, 100 cm SSDfor (a) square and (b) circular small field sizes. Measurements of homogeneity, symmetry andpenumbra with high resolution TLD, FXG and film dosimeters permit accurate absorbed dosecalculation measurements in the high dose gradient regions at the field edges.
Evidently the discrepancies among reported measurements slightly increase with depth forsmaller field sizes. However, the standard deviations among our detectors do not significantly
1438 C S G Calcina et al
exceed 1%; where deviations exist, their directions and values correlate with the detectorlateral resolution (Nizin 1993, Duggan and Coffey 1998, Heydarian et al 1996, Vahc et al2001).
Beam profile
The 6 MV photon beam profiles are presented in figure 5 for the square and circular field sizesmeasured with FXG, TLD and film dosimeters. The homogeneity, symmetry and penumbracharacteristics may be examined for each dosimeter and field to judge the acceptability ofeach data set. Using the film as a standard dosimeter for small field sizes (Somigliana et al1999), the TLD and FXG profiles agree within 1% in value and 1 mm in profile position.This accuracy has been recently recommended (Venselaar et al 2001) for a relative basic beamdata set.
Conclusions
From our measurements, we conclude that our FXG dosimeter, as well as high resolution film,and TLD dosimeters meet or surpass the precision required for small field radiation planning.Large volume ionization chambers are inappropriate in regions of high dose gradient owing tovolume averaging and to perturbation of the electronic equilibrium. Precise optical reading ofour FXG dosimeter, with effective atomic numbers close to those of soft tissue, is shown to yieldaccurate measurements of a basic data set, not significantly different from film measurements.
Acknowledgments
The present work was supported by grants from IAEA and CAPES (Brazil). The authors thankthe Centro de Combate ao Cancer (CUCC-UERJ), the medical physicist Afranio Ackerman(CUCC-UERJ) for support and Dr Pawel Olko (Institute of Nuclear Physics, Poland) for theTLD dosimeters.
References
Attix F H and Willian C R 1996 Radiation Dosimetry vol 2, 2nd edn (New York: Academic) p 422Bero M A, Gilboy W B, Glover P M and Keddie J L 1999 Three-dimensional radiation dose measurements with
ferrous benzoic acid xylenol orange in gelatin gel and optical absorption tomography Nucl. Instrum. MethodsPhys. Res. A 422 617–20
Bjarngard B E, Tsai J S and Rice R K 1990 Doses on the central axis of narrow 6-MV x-ray beams Med. Phys. 17 794–9BJR and IPEMB Joint Working Party 1996 Central axis depth dose data for use in radiotherapy Br. J. Radiol. Suppl.
25Caldeira Filho A M 2004 Analise da solucao Fricke modificada e irradiada atraves da espectroscopia fotoacustica
MSc Thesis Sao Paulo University (FFCLRP/DFM)Costa R T 2001 Avaliando a viabilidade do uso do dosımetro Fricke modificado na radioterapia MSc Thesis Sao Paulo
University (FFCLRP/DFM)De Vlamynck K, De Wagter C and De Neve W 1999 Diamond detector measurements near simulated air channels
for narrow photon beams Radiother. Oncol. 53 155–9Duggan D M and Coffey C W 1998 Small photon field dosimetry for stereotactic radiosurgery Med. Dosim. 23 153–9Felipe D S 2003 Desenvolvimento, teste e aplicacao de prototipo para dosimetria da solucao Fricke modificada MSc
Thesis Sao Paulo University (FFCLRP/DFM)Findley D O, Forell B W and Wong P S 1987 Dosimetry of a dual photon energy linear accelerator Med. Phys. 14 270–3Haryanto F, Fippel M, Laub W U, Dohm O and Nusslin F 2002 Investigation of photon beam output factors for
conformal radiation therapy—Monte Carlo simulations and measurements Phys. Med. Biol. 47 N133–43

Dosimetric parameters for small field sizes using Fricke xylenol gel, TLD and IC 1439
Heydarian M, Hoban P W and Beddoe A H 1996 A comparison of dosimetry techniques in stereotactic radiosurgeryPhys. Med. Biol. 41 93–110
International Atomic Energy Agency (IAEA) 2000 Absorbed dose determination in external beam radiotherapy: aninternational code of practice for dosimetry based on standards of absorbed dose to water IAEA Technical ReportSeries TRS-398 (Vienna: IAEA)
ICRU 1976 Determination of absorbed dose in a patient irradiated by beams of x or gamma rays in radiotherapyprocedures ICRU Report 24 (Bethesda, MD: ICRU)
Khan F M 1997 The Physics of Radiation Therapy (Baltimore, MD: Williams & Wilkins)Laub W U and Wong T 2003 The volume effect of detectors in the dosimetry of small field used in IMRT Med.
Phys. 30 341–7Mack A, Scheib S G, Major J, Gianolini S, Pazmandi G, Feist H, Czempiel H and Kreiner H J 2002 Precision
dosimetry for narrow photon beams used in radiosurgery determination of gamma knife output factors Med.Phys. 29 2080–9
McLaughlin W L and Soares C G 1994 The use of a radiochromic detector for the determination of stereotacticradiosurgery dose characteristics Med. Phys. 21 379–88
Nizin P S 1993 Eletronic equilibrium and primary dose in collimated photon beams: basic concepts and definitionsMed. Phys. 26 1893–900
Perucha M, Sanchez-Doblado F, Leal A, Ricon M, Arrans R, Nunez L and Carrasco E 2003 Investigation ofradiosurgical beam profiles using Monte Carlo method Med. Dosim. 28 1–6
Prasad G, Parthasaradhi K, Des Rosiers C, Bloomer W and LsCombe M 1997 Dosimetric analysis and clinicalimplementation of 6 MV x-ray radiosurgery beam Med. Dosim. 22 127–33
Robar J L and Clark B G 1999 The use of radiographic film for linear accelerator sterotactic radiosurgical dosimetryMed. Phys. 26 2144–50
Sanchez-Doblado F, Andreo P, Capote R, Leal A, Perucha M, Arrans R, Nunez L, Mainegra E, Lagares J and CarrascoE 2003 Ionization chamber dosimetry of small photon fields: a Monte Carlo study on stopping-power ratios forradiosurgery and IMRT beams Phys. Med. Biol. 48 2081–99
Santos W M, Hazin C A, De Souza C N, Monti C R, Kawakami N S and Lazarini P G 2001 Medidas das caracteristicasde feixes de fotons de 6 MV usados em radiocirurgia e radioterapia estereotaxica, IV Congreso Internacionalde proteccion radiologica, IRPA
Serago C F, Houdek P V, Hartmann G H, Saini D S, Serago M and Kaydee A 1992 Tissue maximum ratios (and otherparameters) of small circular 4, 6, 10, 15 and 24 MV x-ray beams for radiosurgery Phys. Med. Biol. 37 1943–56
Sibata C H, Mota H C, Beddar A S, Higgins and Shin K H 1991 Influence of detector size in photon beam profilemeasurements Phys. Med. Biol. 36 621–31
Somigliana A, Cattaneo G M, Fiorino C, Borelli S, Del Vecchio A, Zonca G, Pignoli E, Loi G, Calandrino R andMarchesini R 1999 Dosimetry of gamma knife and linac-based radiosurgery using radiochromic and diodedetectors Phys. Med. Biol. 44 887–97
Vahc Y W, Chung W K, Park K R, Lee J Y, Lee Y H, Kwon O and Kim S 2001 The properties of theultramicrocylindrical ionization chamber for small field used in stereotactic radiosurgery Med. Phys. 28 303–9
Venselaar J, Welleweerd H and Mijnheer B 2001 Tolerances for the accuracy of photon beam dose calculations oftreatment planning systems Radiother. Oncol. 60 191–201
Verhaegen F, Das I J and Palmans H 1998 Monte Carlo dosimetry study of a 6 MV stereotactic radiosurgery unitPhys. Med. Biol. 43 2755–68
Westermark M, Arndt J, Nilson B and Brahme A 2000 Comparative dosimetry in narrow high-energy photon beamsPhys. Med. Biol. 45 685–702
Related Documents











