Kidney International, Vol. 63 (2003), pp. 927–935 Dose-dependent effects of strontium on bone of chronic renal failure rats IRIS SCHROOTEN,GEERT J.S. BEHETS,WALTER E. CABRERA,SVEN R. VERCAUTEREN, LUDWIG V. LAMBERTS,STEVEN C. VERBERCKMOES,AN J. BERVOETS,GEERT DAMS, WILLIAM G. GOODMAN,MARC E. DE BROE, and PATRICK C. D’HAESE Department of Nephrology-Hypertension, University of Antwerp, Belgium; Department of Nephrology, University of Asunc ¸ion, Paraguay; and UCLA Medical Center, Division of Nephrology, Los Angeles, California, USA and osteoblastic activity, which in the presence of a low to Dose-dependent effects of strontium on bone of chronic renal normal amount of osteoid (2.7 1.9%) points to the develop- failure rats. ment of the adynamic type of renal osteodystrophy. Interest- Background. We previously reported on increased bone ingly, compared to the control-CRF group, histodynamic and strontium (Sr) levels in dialysis patients with osteomalacia ver- histologic parameters of the Sr-75 group did not differ signifi- sus those presenting other types of renal osteodystrophy. A causal role of strontium in the development of osteomalacia cantly and a substantial osteoblastic activity (7.6 4.0%) was was established in a chronic renal failure (CRF) rat model. seen also. In the Sr-150 group, the various osteoid parameters Methods. In the present study we investigated whether the were significantly (P 0.05) increased vs. all other groups and effect of Sr on bone was related to dosage. Four groups of were accompanied by a reduced BFR and mineral apposition CRF rats were studied: a control group (control-CFR; N 6) rate (MAR) and an increased mineralization lag time (MLT), not receiving strontium and three groups of animals loaded indicating a mineralization defect and the development of os- orally with Sr during 18 weeks by adding the element as the teomalacia. SrCl 2 ·H 2 0 compound to the drinking water at concentrations Conclusions. Our findings indicate that the role of Sr in the of 0.03 g/100mL (Sr-30; N 6), 0.075 g/100mL (Sr-75; N development of bone lesions in renal failure is complex and 6), or 0.15 g/100mL (Sr-150; N 6) respectively. A fifth group that, depending on the dose, the element may act via multiple consisting of seven animals with intact renal function (control- pathways. NRF), not receiving Sr served as controls for the effect of CRF on bone histology. Results. As compared to the control-NRF and control-CRF Recently, we assessed the trace element status in 100 groups, Sr administration resulted in a dose-dependent increase in bone and serum Sr levels. No difference in body weight and bone biopsies of dialysis patients presenting the various biochemical serum and urinary parameters [i.e., calcium (Ca), types of renal osteodystrophy and found bone strontium phosphorus (P), and creatinine] was noted between the various (Sr) levels, as well as Sr/calcium (Ca) ratios to be increased CRF groups. At sacrifice, intact parathyroid hormone (iPTH) in patients with osteomalacia [1, 2]. Bone Sr and Sr/Ca levels of CRF groups were significantly (P 0.05) higher than the values measured in the control-NRF group indicating the levels were not only elevated compared to individuals development of hyperparathyroidism secondary to the installa- with a normal bone histology, but also in comparison to tion of the CRF. This is further supported by the differences in all other types of renal osteodystrophy. Data from a bone histomorphometry between the control-CRF and control- subsequent epidemiologic study revealed that patients NRF animals, which, respectively, showed an increased amount of osteoid (mean SEM 3.4 1.2% vs. 0.37 0.14%, P coming from particular dialysis centers were at an in- 0.05) in combination with a distinct osteoblastic activity (35 creased risk for accumulation of Sr which mainly origi- 11% vs. 2%, P 0.05) and an increased bone formation rate nated from the use of Sr-contaminated acetate-based [(BFR), 677 177 m 2 /mm 2 /day vs. 130 50 m 2 /mm 2 /day, concentrates, used to prepare the final dialysis fluid [3]. P 0.05]. Bone surface area and erodic perimeter did not A causal role of Sr in the development of osteomalacia differ between the various study groups. In the Sr-30 group, Sr loading went along with a dramatic reduction of the BFR was established in an experimental study. Here, oral as indicated by the total absence of double tetracyclin labels administration of the element to a chronic renal failure (CRF) rat model over a 12-week period by adding the Key words: osteomalacia, mineralization, osteoblast function, remnant element to the drinking water at a concentration of 0.34 kidney, trace element. g/100mL resulted in the development of distinct osteo- malacic lesions in contrast to the animals that had not Received for publication July 25, 2002 Accepted for publication October 15, 2002 received the compound. An additional interesting find- ing of this study was that rats loaded with aluminum 2003 by the International Society of Nephrology 927

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Kidney International, Vol. 63 (2003), pp. 927–935
Dose-dependent effects of strontium on bone of chronic renalfailure rats
IRIS SCHROOTEN, GEERT J.S. BEHETS, WALTER E. CABRERA, SVEN R. VERCAUTEREN,LUDWIG V. LAMBERTS, STEVEN C. VERBERCKMOES, AN J. BERVOETS, GEERT DAMS,WILLIAM G. GOODMAN, MARC E. DE BROE, and PATRICK C. D’HAESE
Department of Nephrology-Hypertension, University of Antwerp, Belgium; Department of Nephrology, University of Asuncion,Paraguay; and UCLA Medical Center, Division of Nephrology, Los Angeles, California, USA
and osteoblastic activity, which in the presence of a low toDose-dependent effects of strontium on bone of chronic renalnormal amount of osteoid (2.7 � 1.9%) points to the develop-failure rats.ment of the adynamic type of renal osteodystrophy. Interest-Background. We previously reported on increased boneingly, compared to the control-CRF group, histodynamic andstrontium (Sr) levels in dialysis patients with osteomalacia ver-histologic parameters of the Sr-75 group did not differ signifi-sus those presenting other types of renal osteodystrophy. A
causal role of strontium in the development of osteomalacia cantly and a substantial osteoblastic activity (7.6 � 4.0%) waswas established in a chronic renal failure (CRF) rat model. seen also. In the Sr-150 group, the various osteoid parameters
Methods. In the present study we investigated whether the were significantly (P � 0.05) increased vs. all other groups andeffect of Sr on bone was related to dosage. Four groups of were accompanied by a reduced BFR and mineral appositionCRF rats were studied: a control group (control-CFR; N � 6) rate (MAR) and an increased mineralization lag time (MLT),not receiving strontium and three groups of animals loaded indicating a mineralization defect and the development of os-orally with Sr during 18 weeks by adding the element as the teomalacia.SrCl2 · H20 compound to the drinking water at concentrations Conclusions. Our findings indicate that the role of Sr in theof 0.03 g/100mL (Sr-30; N � 6), 0.075 g/100mL (Sr-75; N � development of bone lesions in renal failure is complex and6), or 0.15 g/100mL (Sr-150; N � 6) respectively. A fifth group that, depending on the dose, the element may act via multipleconsisting of seven animals with intact renal function (control- pathways.NRF), not receiving Sr served as controls for the effect of CRFon bone histology.
Results. As compared to the control-NRF and control-CRFRecently, we assessed the trace element status in 100groups, Sr administration resulted in a dose-dependent increase
in bone and serum Sr levels. No difference in body weight and bone biopsies of dialysis patients presenting the variousbiochemical serum and urinary parameters [i.e., calcium (Ca), types of renal osteodystrophy and found bone strontiumphosphorus (P), and creatinine] was noted between the various
(Sr) levels, as well as Sr/calcium (Ca) ratios to be increasedCRF groups. At sacrifice, intact parathyroid hormone (iPTH)in patients with osteomalacia [1, 2]. Bone Sr and Sr/Calevels of CRF groups were significantly (P � 0.05) higher than
the values measured in the control-NRF group indicating the levels were not only elevated compared to individualsdevelopment of hyperparathyroidism secondary to the installa- with a normal bone histology, but also in comparison totion of the CRF. This is further supported by the differences in all other types of renal osteodystrophy. Data from abone histomorphometry between the control-CRF and control-
subsequent epidemiologic study revealed that patientsNRF animals, which, respectively, showed an increased amountof osteoid (mean � SEM 3.4 � 1.2% vs. 0.37 � 0.14%, P � coming from particular dialysis centers were at an in-0.05) in combination with a distinct osteoblastic activity (35 � creased risk for accumulation of Sr which mainly origi-11% vs. �2%, P � 0.05) and an increased bone formation rate nated from the use of Sr-contaminated acetate-based[(BFR), 677 � 177 �m2/mm2/day vs. 130 � 50 �m2/mm2/day,
concentrates, used to prepare the final dialysis fluid [3].P � 0.05]. Bone surface area and erodic perimeter did notA causal role of Sr in the development of osteomalaciadiffer between the various study groups. In the Sr-30 group,
Sr loading went along with a dramatic reduction of the BFR was established in an experimental study. Here, oralas indicated by the total absence of double tetracyclin labels administration of the element to a chronic renal failure
(CRF) rat model over a 12-week period by adding theKey words: osteomalacia, mineralization, osteoblast function, remnant element to the drinking water at a concentration of 0.34kidney, trace element. g/100mL resulted in the development of distinct osteo-
malacic lesions in contrast to the animals that had notReceived for publication July 25, 2002Accepted for publication October 15, 2002 received the compound. An additional interesting find-
ing of this study was that rats loaded with aluminum 2003 by the International Society of Nephrology
927

Schrooten et al: Dose-related effects of strontium on bone928
(Al) developed adynamic bone, whereas in the group ofanimals loaded with both Sr and Al some rats developedadynamic bone while in others an even more severedegree of osteomalacia was observed [4].
As suggested in literature, Sr may exert a number ofeffects on bone, which may either be beneficial [5–11]or toxic [12–16]. Such an ambiguous activity on bone haspreviously been reported for Al also [17–19]. Sr, whenadministered as the ranelate (S12911) compound hasbeen attributed the ability to act as an uncoupling agentby increasing the osteoblastic activity without increasingbone resorption [10, 20]. This and the recent in vitrofinding that the compound may increase cartilage forma-tion provides the basis for its potential use in the treat-ment of osteoporosis [10, 20, 21] and osteoarthritis [22].
As previously demonstrated in rats with normal renalfunction Sr either directly or indirectly interacts withbone metabolism in a dose-dependent way. While lowdoses of Sr seem to stimulate bone formation [8, 9], highdoses of the element induce a mineralization defect andincrease the amount of osteoid and decrease bone growth[8, 9, 11]. Indirectly, administration of high Sr dosesleads to hypocalcemia and inhibition of 1�-hydroxylaseactivity [8, 12, 13, 23, 24], whereas lower doses of theelement induce a small transient decrease in serum Calevels and appear not to influence intact parathyroidhormone (iPTH) or vitamin D levels [8].
Following our previous experimental investigations in Fig. 1. Loading, labeling, and sampling time schedule. Abbreviationsare: Sr, strontium, Al, aluminum, Ca, calcium, P, phosphorus.CRF rats loaded with a relatively high Sr dose [4], the
present study was set up to determine whether the effectof Sr on bone of CRF rats is dose-related and/or differsdepending on the dose administered. tion were checked and recorded daily. The loading proto-
col was continued over 18 weeks. Rats were sacrificedthe day following the end of the loading protocol. FiveMETHODSand 2 days before sacrifice, respectively, a demeclocyclinExperimental design(30 mg/kg) and tetracyclin HCl (30 mg/kg) labeling wasUsing the “remnant kidney” model, CRF was inducedperformed. At regular time intervals during the loadingin male Wistar rats at 12 weeks of age. Under sodiumperiod, blood and urine samples were taken and frozenpentobarbital anesthesia (60 mg/kg) two branches of theat �80�C until analysis (Fig. 1). Bone and blood samplesrenal artery of the right kidney were ligated and 2 weekswere also taken in the control-NRF animals at sacrifice.later the left kidney was removed. Four weeks after
Twenty-four–hour urine samples were collected afternephrectomy rats were divided into four groups: a con-housing the animals in individual metabolic cages. Bloodtrol group (control-CRF; N � 6), which did not receivewas drawn from the tail vein during the loading periodSr and three groups of six animals each, loaded orallyand by cardiac puncture at sacrifice under ether anesthe-with 0.03 g/100 mL (Sr-30), 0.075 g/100mL (Sr-75) or 0.15sia. Bone and soft tissues were removed at sacrifice andg/100mL (Sr-150) Sr, respectively, added to the drinkingstored at �20�C until analysis.water as SrCl2 · H20. A fifth group (control-NRF; N �
The experimental protocol was approved by the local7) consisting of animals with intact renal function notEthical Committee for Animal Experiments of the Uni-receiving Sr and having the same age as the CRF ratsversity of Antwerp.at sacrifice (9 months) was included to control for the
effect of CRF on histologic and histodynamic bone pa-Biochemical and chemical determinationsrameters. The choice of the various Sr doses was based
Creatinine in serum and urine was determined accord-on data of our previous experimental study [4].ing to the Jaffe method. iPTH in serum was measuredRats were pair fed and weighed weekly. Animals had
free access to drink and food. Water and food consump- using the INS-PTH kit (Incstar Corp., Stillwater, MN,

Schrooten et al: Dose-related effects of strontium on bone 929
USA), validated for the analysis of rat serum. Proteinuria (MLT) (days), mean time interval between depositionand mineralization of any infinitesimal volume of matrix,was determined according to the method of Bradford.
Sr in serum, urine, and bone was analyzed using a Zee- averaged over the entire life span of the osteoid seam;and bone formation rate (BFR) (�m2/mm2/day), the vol-man 3030 atomic absorption spectrometer equipped with
an HGA-600 graphite furnace, an AS-60 autosampler ume of bone formed per unit of time, calculated as theproduct of mineral apposition rate and mineralizing sur-and an Anadex DP-9500B silent scribe printer, all from
Perkin-Elmer (Norwalk, CT, USA). To determine Sr face; osteoblast perimeter (%), percentage of osteoidperimeter covered by cuboidal (active) osteoblasts.in serum, samples were diluted fourfold in a 0.5 mL/L
TritonX-100 to1 mL/L HNO3 solution, whereas urineStatisticssamples were diluted 1:20 in a 2 mL/L HNO3 solution.
Bone samples were digested with concentrated HNO3 Statistical analysis of the data was done using theKruskal-Wallis test followed by the Mann-Whitney testin stoppered polytetrafluoroethylene (PTFE) (Teflon�)
tubes. Methods for the determination of Sr have pre- for unpaired comparisons when differences betweengroups were noted. Data are expressed as mean � SEM.viously been described in detail [25]. Ca and phosphorus
(P) in serum and urine were determined with a Vitros A P value �0.05 was considered to be significant at atwo-tailed level.750 XRC auto-analyzer (Ortho Clinical Diagnostics,
Beersel, Belgium). Ca determinations in urine and bonewere done by flame-atomic absorption spectrometry
RESULTS(Model 3110; Perkin-Elmer) after diluting the samples
Biochemical and chemical data1:500 in reverse osmosis-water to which 1 g/L lanthanumwas added to avoid phosphate interferences. The daily food and drank consumption did not differ
between the study groups resulting in comparable weightsBone histology at sacrifice.
As shown in Figure 2A, the comparison of serum creat-At sacrifice, femurs and tibiae were freed of soft tissue.Of each rat, one bone sample was, after removal of skin inine levels before installation of the CRF (week 0), after
stabilization of the CRF (week 6) and at sacrifice versusand muscle tissue, weighed immediately and stored at�20�C until atomic absorption spectrometric bulk analy- the control-NRF group indicates that a moderate CRF
was induced. Urinary protein excretion was significantlysis. The second sample was used for histologic examina-tion after 24 hours’ fixation in Burkhardt solution and increased in all CRF groups at sacrifice (Fig. 2B). As
shown in Figure 2C, serum iPTH levels increased duringsubsequent transfer to a 70% ethanol solution until fur-ther processing. Bone samples were then embedded in the loading period in all CRF groups and, at sacrifice,
were significantly (P � 0.05) higher than those noted in100% methylmetacrylate. Longitudinal sections (5 �m)of the proximal tibia were cut with a Jung K microtome the control-NRF group indicating the development of a
substantial degree of hyperparathyroidism.and stained according to Goldner for descriptive histol-ogy. Bone histologic data, as well as dynamic parameters, Serum Ca and P concentrations before loading were
within the normal range in all groups and had not changedare reported using standardized nomenclature and defi-nitions [26]. The parameters measured include total bone at sacrifice (Fig. 3 A and B). In each group a significant
increase in the urinary Ca excretion was noted at thearea (%), the area of trabecular bone, including bothmineralized bone and osteoid, expressed as a percentage start of Sr loading vs. baseline levels (i.e., before the
installation of CRF), which again dropped at sacrificeof the total tissue area; osteoid area (%), the measuredarea of osteoid expressed as a percent of the total bone (Fig. 3C). A similar, be it less pronounced pattern was
noted for the urinary P excretion (Fig. 3D).area), osteoid width (�m); the mean width of surfaceosteoid seams, calculated by dividing the measured oste- Loading of the animals with different Sr concentra-
tions led to a significant dose-dependent accumulationoid area by the length of the osteoid seams; osteoid perim-eter (%), trabecular bone perimeter occupied by osteoid of the element in the respective groups. In order to correct
for bone density, we also determined the Ca concentra-as a percent of the total bone perimeter; erodic perimeter(%), the percentage of trabecular bone perimeter char- tion in bone. The bone Ca content did not differ between
the groups under study. Hence, Sr/Ca ratio’s showed theacterized by the presence of scalloped bone resorptivelacunae; double-labeled perimeter (%), percentage of same trend as noted for the absolute concentrations (Fig.
4B). As for bone, serum Sr concentrations also signifi-total endosteal surface exhibiting a double fluorescenttetracyclin label; mineral apposition rate (MAR) (�m/ cantly increased in a dose-dependent way (Fig. 4A).day), the rate by which bone is mineralized, calculated
Histologic dataas the average distance between the midpoints of twoconsecutive tetracyclin labels, divided by the time inter- Figure 5 shows Goldner stainings of representative
animals of the various study groups. Compared to theval between the labeling periods; mineralization lag time

Schrooten et al: Dose-related effects of strontium on bone930
amount of osteoid is low to normal for the degree of renalfailure. No osteoblasts are seen (Fig. 5D) in contrast tothe Sr-75 group where cuboidal, active cells are observed(Fig. 5E). In the latter group, the amount of osteoid iscomparable to that of the control CRF rats. In the highestSr group, however, in the absence of any osteoblasticactivity the amount of osteoid is distinctly increased ascompared to all other groups (Fig. 5F).
Detailed quantitative histomorphometric data per groupare presented in Figure 6. Bone area and erodic perime-ter did not differ significantly between the various groups.Comparison of the histomorphometric data of the con-trol-NRF group with those of the control-CRF groupclearly shows the development of hyperparathyroid bonedisease in the CRF animals as indicated by the significant(P � 0.05) increase of the BFR (677 � 177 vs. 130 � 50�m2/mm2/day), MAR (2.36 � 0.1 vs. 0.86 � 0.18 �m/day), osteoid area (3.4 � 1.2 vs. 0.37 � 0.14%), osteoidperimeter (17.4 � 5.31 vs. 3.7 � 1.49%), and the amountof active osteoblasts (osteoblast perimeter) (35 � 11 vs.�2%). The increase in osteoid area and osteoid perime-ter in the absence of any change in osteoid width in thecontrol-CRF group further reflects the development ofhyperparathyroidism. In line with this notion and theincreased osteoblastic activity are the significant correla-tions between MAR and the osteoid area (r � 0.97, P �0.05) and osteoid perimeter (r � 0.88, P � 0.05).
Comparing the control-CRF animals to those receiv-ing Sr, a distinct effect could already be observed at thelowest dose administered. Indeed, in the Sr-30 groupdouble tetracyclin labels were completely absent in allrats, while in all but one animal the reduced mineraliza-tion rate was accompanied by a distinctly lower osteoidarea (0.84 � 0.29%) and osteoid perimeter (5.4 � 1.7%),thus suggesting the development of adynamic bone.
In the Sr-75 group, the osteoid area was comparableto the mean value noted in the control-CRF animals anda substantial osteoblastic activity (osteoid perimeter)(7.6 � 4%) was observed. There was little variance in
Fig. 2. The various study groups included pre-chronic renal failure osteoid width and osteoid perimeter between rats of(CRF) (�), start loading (week 6) ( ), and at sacrifice (week 20) (�).this group. Interestingly, in contrast to the Sr-30 group,(A ) Serum creatinine, (B ) Urinary protein. (C ) Serum PTH levels.
Abbreviations are: C-crf, control-chronic renal failure; C-nrf, control- double tetracyclin labels were seen in all animals of theintact renal function not receiving Sr; Sr-30, 0.03 g/100 mL Sr; Sr-75, Sr-75 group and the calculated values for double-labeled0.075 g/100mL Sr; Sr-150, 0.15 g/100mL Sr. †P � 0.05 vs. week 0; *P �
perimeter, BFR, MAR, and MLT were highly compara-0.05 vs. week 6; #P � 0.05 vs. C-nrf.
ble to those of the control-CRF group, indicating Sr toexert only a minimal effect at this particular dose.
Finally, in all animals of the Sr-150 group double labelscontrol-NRF animals (Fig. 5C) bone histologic findingswere completely absent, which is similar to the Sr-30of rats of the control-CRF group reveal an increasedgroup. In contrast to this latter group however, the re-amount of osteoid in the presence of active cuboidalduced tetracyclin incorporation was accompanied by aosteoblasts (Fig. 5 A and B), findings which in viewsignificantly increased amount of osteoid in all animalsof the increased serum iPTH levels (Fig. 2C) and theas reflected by the increased osteoid area, osteoid perim-presence of double tetracyclin labels (not shown; seeeter, and osteoid width, pointing to a mineralization de-also quantitative data, Fig. 6) are indicative for the devel-
opment of hyperparathyroidism. In the Sr-30 group the fect and the development of osteomalacia.

Schrooten et al: Dose-related effects of strontium on bone 931
Fig. 3. The various study groups included pre-chronic renal failure (CRF) (�), start loading (week 6) ( ), and at sacrifice (week 20) (�). (A )Serum calcium. (B ) Serum phosphorus. (C ) Urinary calcium. (D ) Urinary phosphorus levels. Abbreviations are: C-crf, control-chronic renalfailure; C-nrf, control-intact renal function not receiving Sr; Sr-30, 0.03 g/100 mL Sr; Sr-75, 0.075 g/100mL Sr; Sr-150, 0.15 g/100mL Sr. †P � 0.05vs. week 0; *P � 0.05 vs. week 6; #P � 0.05 vs. C-nrf.
DISCUSSION The experiments described in this paper were designedto study whether at lower doses (Sr �0.34 g/100mL) (i.e.,As reported previously, bone Sr concentrations as wellthe dose used in our first experimental study) Sr was alsoas Sr/Ca ratios are increased in dialysis patients withable to induce osteomalacia. In addition, these studiesosteomalacia in comparison to those presenting the othermust allow us to find out whether, following observationstypes of renal osteodystrophy [1]. Such an associationin animals with normal renal function, the effects in CRFhas recently been reported by others also [27]. Findingsrats also are dose-related and multiple [8–10]. Comparedof a prospective epidemiologic study revealed that dial-to our previous experimental study, the use of lower Srysis patients treated in particular dialysis centers weredoses also offers the advantage that they approach theat an increased risk for accumulation of the element,exposure in the clinical setting of dialysis.which mainly originated from the use of Sr-contaminated
In rats with normal renal function, literature data indi-concentrates to prepare the final dialysis fluid [3]. Datacated that Sr can exert different effects on bone, whichthus provided evidence for the existence of a so-far un-appear to be dose-dependent. Whereas low doses of theidentified disease entity within the dialysis population.element can stimulate bone formation, high doses ofSupport for a causal role of the element in the develop-the element may induce a mineralization defect [7, 8].ment of this type of renal osteodystrophy was providedMoreover, due to their versatile effects on bone andby data of an experimental study, in which we were ableability to uncouple osteoclastic resorption from osteo-to induce a bone disease reflecting the histologic pictureblastic activity [10] and increase cartilage formation, Srof osteomalacia in CRF rats, loaded with Sr during a 12-compounds have been proposed as potential tools in theweeks period by adding the element to the drinkingtreatment of osteoporosis and osteoarthritis [20, 22].water. An interesting additional finding of this study
An ambiguous activity on bone, similar to that of Srwas that rats loaded with Al developed adynamic bone,has also been shown for Al; an element that within thewhereas in the group of animals loaded with both Sr anddialysis population is now well recognized to play a roleAl some rats developed adynamic bone, while in others
a more severe osteomalacia was noted [4]. in the development of both osteomalacia and adynamic

Schrooten et al: Dose-related effects of strontium on bone932
tein excretion reflected the induction of a moderate CFR.Comparison of the iPTH levels of the control-NFR ani-mals at sacrifice and CRF groups before the installationof the CFR to those of the CRF rats at sacrifice revealeda distinct increase of this parameter. These data thusindicate the development of a substantial degree of hy-perparathyroidism and again demonstrate that the “rem-nant kidney” rat model reflects well the CFR situationin humans. Serum Ca and P concentrations did not differbetween the various groups. Compared to levels foundbefore induction of CRF, a hypercalciuria was notedduring the first weeks following the installation of CRF,which reversed to nearly baseline levels at sacrifice. Thedecreased urinary P levels at sacrifice seen in control-CRF rats as compared to the control-NRF animals mightbe due to the severity of the renal insufficiency [30] at thistime point either or not in combination with a possibleinhibitory effect of Sr on the 1�-hydroxylase activity [12].
Compared to the rats with normal renal function histo-morphometric bone analysis in the control-CRF animalsclearly showed an increased amount of osteoid and num-ber of active osteoblasts in the presence of a distinctlyincreased BFR, again indicating the development of hy-perparathyroidism. Of interest was that these animalsdeveloped a high bone turnover without lowering thedietary Ca intake and/or increasing the P content of thediet [30].
In all animals of the highest Sr group (0.15 g/100 mL),superimposed upon the hyperparathyroidism, an im-paired mineralization was noted as indicated by a dra-matically increased mineralization lag time that, in turn,resulted in a distinctly increased amount of osteoid, thus
Fig. 4. Sr levels measured at sacrifice. (A ) Serum Sr levels. (B) Bone featuring the hallmarks of osteomalacia.Sr/Ca ratio. A dose-dependent increase was noted. Abbreviations are: In rats exposed to the intermediate Sr dose (0.075C-crf, control-chronic renal failure; C-nrf, control-intact renal function
g/100 mL) bone histomorphometric parameters did notnot receiving Sr; Sr-30, 0.03 g/100 mL Sr; Sr-75, 0.075 g/100mL Sr; Sr-150, 0.15 g/100mL Sr. †P � 0.05 vs. C-crf; #P � 0.05 versus C-nrf. substantially differ from those of the control-NRF group.
Hence, at this concentration and in the presence of hy-perparathyroidism the element appears not to have anyeffect on bone. Evidence has been presented in literaturebone disease. Whereas in these patients Al-induced os-that at comparable doses given to rats with normal renalteomalacia in general only develops in the presence offunction, Sr increases the BFR due to a stimulative effectdistinctly elevated bone Al levels the adynamic lesionon osteoblastic activity [8, 9], an effect which reasonablymay already occur at normal to slightly elevated levels.would not be expected in the presence of a an alreadyStudies in rats with normal renal function demonstratedstimulated bone turnover in the context of CRF.that administration of high doses of the element may
In the lowest Sr group (0.03 g/100 mL) double labelslead to a decrease in bone and matrix formation [28, 29],were absent indicating a dramatic decrease in BFR inwhile others in both experimental and in vitro studiesall animals. However, in contrast to the rats receivingfound that low doses of Al could stimulate bone forma-the highest dose (0.15 g/100 mL), this was not accompa-tion [17–19].nied by an increased amount of osteoid. Rather, bothIn the present study the “remnant kidney” rat modelthe osteoid area and osteoid perimeter were decreasedwas used, which is generally accepted to be a suitableversus the other groups and even did not differ from themethod to induce a moderate, stable CRF in animals.control-NRF animals. This together with the absence ofLoading of the rats was done over a relatively long periodany osteoblastic activity points to the development of a(18 weeks). This relatively extended loading protocolso-called adynamic bone.resembles well the biochemical setting of CRF.
The increased serum creatinine levels and urinary pro- Despite the various histologic pictures seen in the dif-
Schrooten et al: Dose-related effects of strontium on bone 933
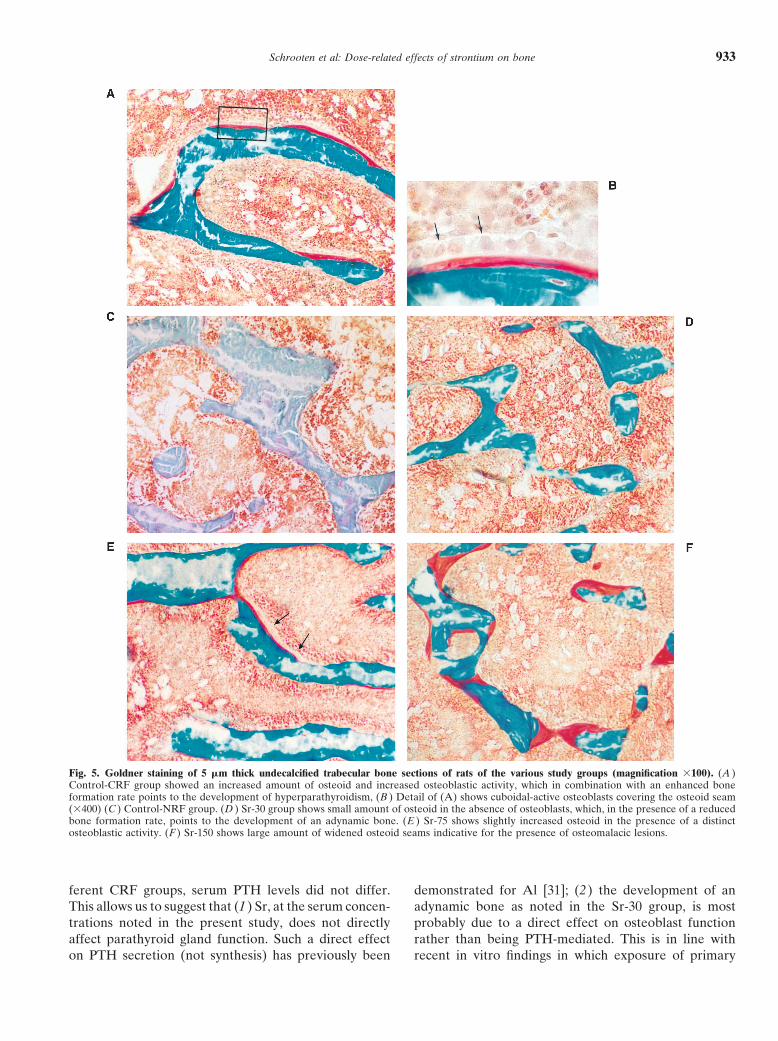
Fig. 5. Goldner staining of 5 �m thick undecalcified trabecular bone sections of rats of the various study groups (magnification �100). (A )Control-CRF group showed an increased amount of osteoid and increased osteoblastic activity, which in combination with an enhanced boneformation rate points to the development of hyperparathyroidism, (B ) Detail of (A) shows cuboidal-active osteoblasts covering the osteoid seam(�400) (C ) Control-NRF group. (D ) Sr-30 group shows small amount of osteoid in the absence of osteoblasts, which, in the presence of a reducedbone formation rate, points to the development of an adynamic bone. (E ) Sr-75 shows slightly increased osteoid in the presence of a distinctosteoblastic activity. (F ) Sr-150 shows large amount of widened osteoid seams indicative for the presence of osteomalacic lesions.
ferent CRF groups, serum PTH levels did not differ. demonstrated for Al [31]; (2) the development of anadynamic bone as noted in the Sr-30 group, is mostThis allows us to suggest that (1) Sr, at the serum concen-
trations noted in the present study, does not directly probably due to a direct effect on osteoblast functionrather than being PTH-mediated. This is in line withaffect parathyroid gland function. Such a direct effect
on PTH secretion (not synthesis) has previously been recent in vitro findings in which exposure of primary

Schrooten et al: Dose-related effects of strontium on bone934
Fig. 6. Histologic data of the various groups. Abbreviations are: C-crf, control-chronic renal failure; C-nrf, control-intact renal function notreceiving Sr; Sr-30, 0.03 g/100 mL Sr; Sr-75, 0.075 g/100mL Sr; Sr-150, 0.15 g/100mL Sr. †P � 0.05 vs. C-crf; *P � 0.05 vs. Sr-30; ¶P � 0.05 vs.Sr-75, #P � 0.05 vs. C-nrf. Data are mean � SEM of six animals except control-NRF (N � 7) and Sr-30 (N � 5).
osteoblasts to relatively low Sr levels resulted in a re- In order to explain the findings of the present study,the following hypothesis can be formulated. In the lowestduced osteoblastic activity and impaired cellular differ-
entiation [abstract; Verberckmoes SC et al, J Am Soc Sr group, in the absence of osteoblasts no osteoid isdeposited and hence no mineralization takes place, thusNephrol 12:748, 2001]; and (3) at high levels the osteo-
malacic lesions most likely result from a chemical inter- reflecting the characteristics of adynamic bone. In theSr-75 group the suppressive effect on osteoblast functionference of the element with the hydroxyapatite deposi-
tion; an observation corroborating previous in vitro and is no longer observed and mineralization remains intact.In the Sr-150 group, Sr induces an osteomalacic lesionin vivo findings also [9] [abstract; Verberckmoes SC et
al, J Am Soc Nephrol 12:748, 2001]. as was noted in our previous study also [4].

Schrooten et al: Dose-related effects of strontium on bone 935
11. Matsumoto A: Effect of strontium on the epiphyseal cartilage plateCONCLUSIONof rat tibiae-histological and radiographic studies. Jpn J Pharmacol26:675–681, 1976In conclusion, our findings indicate that the role of Sr
12. Omdahl JL, Deluca HF: Rachitogenic activity of dietary stron-in the development of osteomalacia is dose-related andtium. Inhibition of intestinal calcium absorption and 1,25 dihydrox-
that the element may exert different effects on bone, ycholecalciferol synthesis. J Biol Chem 247:5520–5526, 197213. Omdahl JL: Control of kidney 25-hydroxyvitamin D3 metabolismdepending on the dose used. They are in line with previ-
strontium and the involvement of parathyroid hormone. Arch Bio-ous literature data from experimental studies using ani-chem Biophys 184:172–178, 1977
mals with intact renal function in which a dose-depen- 14. Mattar AG, Siegel BA: Bone tracers: Radionuclide imaging andrelated techniques, in Skeletal research: An Experimental Ap-dent effect of Sr on bone, be it in a different way, wasproach, edited by Simmons DJ, Kusrin AS, New York, Academicsuggested also. With regard to the potential therapeuticPress, 1979, pp 455–486
use of Sr compounds [20] the relevance of our data may 15. Johnson A: The influence of strontium on characteristic factorsof bone. Calcif Tissue Res 11:215–221, 1973surpass the scope of renal osteodystrophy and be of
16. Eisenberg E: The biological metabolism of strontium, in Biologicalinterest in the search for optimal therapeutic doses inMineralization, edited by Zipkin I, New York, John Wiley & Sons,
the treatment of particular bone diseases such as osteo- 1973, pp 435–44217. Quarles LD, Gitelman HJ, Drezner MK: Induction of de novoporosis, which is observed particularly in elderly patients
bone formation in the beagle: a novel effect of aluminum. J Clinwith an already slightly decreased renal function [32].Invest 81:1056–1066, 1988
18. Lieberherr M, Grosse B, Cournot-Witmer G, et al: Aluminumaction on mouse bone cell metabolism and response to PTH andACKNOWLEDGMENTS1,25 (OH)2D3. Kidney Int 31:736–743, 1987
The authors are indebted to D. De Weerdt for his excellent drawings. 19. Quarles LD: Paradoxical toxic and trophic osseous actions ofI. Schrooten is a recipient of a postgraduate research grant of the aluminum: potential explanations. Min Electrolyte Metab 17:233–
Flemish Institute for the promotion of Scientific Technological Re- 239, 1991search in Industry (IWT) while W. Cabrera participated in the study 20. Marie PJ, Ammann P, Boivin G, Rey C: Mechanism of actionin the frame of an ISN Sister Program. and therapeutic potential of strontium in bone. Calcif Tissue Int
169:121–129, 2001Reprint requests to Marc E. De Broe, M.D., Ph.D. p/a, University 21. Grynpas MD, Hamilton E, Cheung R, et al: Strontium increases
Hospital Antwerp, Wilrijkstraat 10 B-2650, Edegem/Antwerp, Belgium. vertebral bone volume in at a low dose that does not induceE-mail: [email protected] detectable mineralization defect. Bone 18:253–259, 1996
22. Henrotin Y, Labasse A, Zheng SX, et al: Strontium ranelateincreases cartilage matrix formation. J Bone Miner Res 16(2):299–REFERENCES308, 2001
23. Omdahl JL, Deluca HF: Strontium induced rickets: Metabolic1. D’Haese PC, Schrooten I, Goodman WG, et al: Increased bonestrontium levels in dialysis patients with osteomalacia. Kidney Int basis. Science 174:949–951, 1971
24. Corradino R, Wasserman R: Strontium inhibition of vitamin D3-57:1107–1114, 20002. D’Haese PC, Couttenye M-M, Lamberts LV, et al: Aluminium, induced calcium binding protein (Ca-BP) and calcium absorption
in chick intestine. Proc Soc Exp Biol Med 133:960–963, 1970iron, lead, cadmium, copper, zinc, chromium, magnesium, stron-tium and calcium content in bone of end-stage renal failure pa- 25. D’Haese PC, Van Landeghem GF, Lamberts LV, et al: Measure-
ment of strontium in serum, urine, bone and soft tissues by Zeemantients. Clin Chem 45:1548–1556, 19993. Schrooten I, Elseviers MM, Lamberts LV, et al: Increased serum atomic absorption spectrometry. Clin Chem 43:121–128, 1997
26. Parfitt AM: Bone histomorphometry: proposed system for stan-strontium levels in dialysis patients. An epidemiological survey.Kidney Int 56:1886–1892, 1999 dardization of nomenclature, symbols and units. Calcif Tissue Int
42:284–286, 19884. Schrooten I, Cabrera WE, Dauwe S, et al: Strontium causesosteomalacia in chronic renal failure rats. Kidney Int 54:448–456, 27. Cohen-Solal ME, Augry F, Mauras Y, et al: Fluoride and stron-
tium accumulation in bone does not correlate with osteoid tissue19985. Cabrera WE, Schrooten I, De Broe ME, D’Haese PC: Review: in dialysis patients. Nephrol Dial Transplant 17:449–454, 2002
28. Goodman WG: Short-term aluminum administration in the rat:Strontium and bone. J Bone Miner Res 14:661–668, 19996. Shorr E, Carter AC: The value of strontium as an adjuvant to Reductions in bone formation without osteomalacia. J Lab Clin
Med 103:749–757, 1984calcium in the mineralization of the skeleton in osteoporosis inman. Bull Hosp Joint Dis 13:59–66, 1952 29. Goodman WG, Gilligan J, Horst R: Short-term aluminum admin-
istration in the rat. Effects on bone formation and relationship to7. McCaslin F, Janes JM: The effect of strontium lactate on thetreatment of osteoporosis. Proc Staff Meet Mayo Clin 34:329–334, renal osteomalacia. J Clin Inv 73:171–181, 1984
30. Bover J, Rodriguez M, Trinidad P, et al: Factors in the develop-19598. Marie JP, Garba MT, Hott M, Miravet L: Effect of low doses ment of secondary hyperparathyroidism during graded renal fail-
ure in the rat. Kidney Int 45(4):953–961, 1994of stable strontium on bone metabolism in rats. Miner ElectrolMetab 11:5–13, 1985 31. Smans KA, D’Haese PC, Van Landeghem GF, et al: Transferrin-
mediated uptake of aluminum by human parathyroid gland cells9. Grynpas M, Marie JP: Effects of low doses of strontium on bonequality and quantity in rats. Bone 11:313–319, 1990 result in hypoparathyroidism. Nephrol Dial Transplant 15:1328–
1336, 200010. Marie JP, Hott M, Modrowski D, et al: An uncoupling agentcontaining strontium prevents bone loss, depressing bone resorp- 32. Elseviers MM, Verpooten GA, De Broe ME, De Backer GG.
Interpretation of creatinine clearance [letter]. Lancet 1(8530):457,tion and maintaining bone formation in estrogen-deficient rats. JBone Min Res 8:607–615, 1993 1987
Related Documents











