UNCORRECTED PROOF 1 Dopamine abnormalities in the neocortex of patients with temporal lobe epilepsy 2 Luisa Q1 Rocha a, ⁎, Mario Alonso-Vanegas b , Juana Villeda-Hernández b , Mario Mújica b , 3 José Miguel Cisneros-Franco b , Mario López-Gómez b , Cecilia Zavala-Tecuapetla a , 4 Christian Lizette Frías-Soria a , José Segovia-Vila c , Anna Borsodi d 5 a Departamento de Farmacobiología, Centro de Investigación y de Estudios Avanzados, Mexico Q3 6 b Instituto Nacional de Neurología y Neurocirugía “Manuel Velasco Suárez”, Mexico 7 c Departamento de Fisiología, Biofísica y Neurociencias, Centro de Investigación y de Estudios Avanzados, Mexico 8 d Biological Research Center of the Hungarian Academy of Sciences, Szeged, Hungary 9 10 abstract article info 11 Article history: 12 Received 15 June 2011 13 Revised 3 September 2011 14 Accepted 13 September 2011 15 Available online xxxx 16 17 18 19 Keywords: 20 Temporal lobe epilepsy 21 Dopamine 22 D1 receptors 23 D2 receptors 24 Dopamine transporter 25 Neuropsychiatric disorders 26 Experiments were designed to evaluate different variables of the dopaminergic system in the temporal cortex 27 of surgically treated patients with temporal lobe epilepsy (TLE) associated with mesial sclerosis (MTLE, 28 n = 12) or with cerebral tumor or lesion (n = 8). In addition, we sought to identify dopaminergic abnormal- 29 ities in those patients with epilepsy that had comorbid anxiety and depression. Specifically, we investigated 30 changes in dopamine and its metabolites, D1 and D2 receptors, tyrosine hydroxylase (TH) and dopamine 31 transporter. Results obtained from patients with epilepsy were compared with those found in experiments 32 using autopsy material. The neocortex of patients with MTLE demonstrated high D1 expression (1680%, 33 p b 0.05) and binding (layers I–II, 31%, p b 0.05; layers V–VI, 28%, p b 0.05), and decreased D2 expression 34 (77%, p b 0.05). The neocortex of patients with TLE secondary to cerebral tumor or lesion showed high expres- 35 sion of D1 receptors (1100%, p b 0.05), and D2-like induced activation of G proteins (layers I–I, 503%; layers 36 III–IV, 557%; layers V–VI, 964%, p b 0.05). Both epileptic groups presented elevated binding to the dopamine 37 transporter and low tissue content of dopamine and its metabolites. Analysis revealed the following correla- 38 tions: a) D1 receptor binding correlated negatively with seizure onset age and seizure frequency, and posi- 39 tively with duration of epilepsy; b) D2 receptor binding correlated positively with age of seizure onset and 40 negatively with duration of epilepsy; c) dopamine transporter binding correlated positively with duration 41 of epilepsy and frequency of seizures; d) D2-like induced activation of G proteins correlated positively 42 with the age of patients. When compared with autopsies and patients with anxiety and depression, patients 43 without neuropsychiatric disorders showed high D2-like induced activation of G proteins, an effect that cor- 44 related positively with age of patient and seizure onset age, and negatively with duration of epilepsy. The 45 present study suggests that alterations of the dopaminergic system result from epileptic activity and could 46 be involved in the physiopathology of TLE and the comorbid anxiety and depression. 47 © 2011 Published by Elsevier Inc. 48 49 50 51 52 Introduction 53 Epilepsy Q4 is the second most important neurologic disorder with 54 diverse etiology. Temporal lobe epilepsy (TLE) is the most frequent 55 and becomes pharmacologically untreatable in a high percentage of 56 patients (Engel, 1996). In TLE associated with mesial sclerosis (MTLE), 57 the hippocampus represents the epileptic focus, while the temporal 58 neocortex is involved in propagation of epileptic seizures to other 59 brain areas (Chagnac-Amitai and Connors, 1989; Chervin et al., 1988; 60 Sloviter, Q5 1994). Neocortex has been proposed to be involved in 61 secondary epileptogenesis as a consequence of progressive extension 62 of the primary epileptogenic zone with increased duration of epilep- 63 sy (Morrell et al., 1987). 64 Epilepsy involves changes in several neurotransmitters (Fisher 65 and Leppik, 2008; Olsen and Avoli, 1997). Concerning the dopaminer- 66 gic system in temporal neocortex of patients with MTLE, studies using 67 Positron Emission Tomography (PET) indicate a reduction of D2/D3 68 receptor binding in the pole and lateral areas, ipsilateral to the epileptic 69 focus (Werhahn et al., 2006). Regarding tissue content of dopamine and 70 its metabolites, the results are controversial and it seems that changes 71 depend on the presence of epileptiform activity in the neocortex 72 (Louw et al., 1989; Mori et al., 1987; Pacia et al., 2001; Pintor et al., 73 1990). In relation with tyrosine hydroxylase (TH), the enzyme respon- 74 sible for DOPA synthesis (the precursor of dopamine), its activity is 75 not modified (Pintor et al., 1990). Despite the fact that D1 receptors 76 play a modulating role in the synaptic activity of the neocortex Neurobiology of Disease xxx (2011) xxx–xxx ⁎ Corresponding autor at: Depto. Farmacobiología, Cinvestav-Sede Sur, Calz. Tenorios 235, Col. Granjas Coapa, México, D.F. C.P. 14330, Mexico. E-mail address: [email protected] (L. Rocha). Available online on ScienceDirect (www.sciencedirect.com). YNBDI-02525; No. of pages: 9; 4C: 0969-9961/$ – see front matter © 2011 Published by Elsevier Inc. doi:10.1016/j.nbd.2011.09.006 Contents lists available at SciVerse ScienceDirect Neurobiology of Disease journal homepage: www.elsevier.com/locate/ynbdi Please cite this article as: Rocha, L., et al., Dopamine abnormalities in the neocortex of patients with temporal lobe epilepsy, Neurobiol. Dis. (2011), doi:10.1016/j.nbd.2011.09.006

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1
2Q1
3
4
5Q3678
9
10111213141516171819202122232425
50
51
52
53Q454
55
56
57
58
59
60Q5
Neurobiology of Disease xxx (2011) xxx–xxx
YNBDI-02525; No. of pages: 9; 4C:
Contents lists available at SciVerse ScienceDirect
Neurobiology of Disease
j ourna l homepage: www.e lsev ie r .com/ locate /ynbd i
OO
F
Dopamine abnormalities in the neocortex of patients with temporal lobe epilepsy
Luisa Rocha a,⁎, Mario Alonso-Vanegas b, Juana Villeda-Hernández b, Mario Mújica b,José Miguel Cisneros-Franco b, Mario López-Gómez b, Cecilia Zavala-Tecuapetla a,Christian Lizette Frías-Soria a, José Segovia-Vila c, Anna Borsodi d
a Departamento de Farmacobiología, Centro de Investigación y de Estudios Avanzados, Mexicob Instituto Nacional de Neurología y Neurocirugía “Manuel Velasco Suárez”, Mexicoc Departamento de Fisiología, Biofísica y Neurociencias, Centro de Investigación y de Estudios Avanzados, Mexicod Biological Research Center of the Hungarian Academy of Sciences, Szeged, Hungary
⁎ Corresponding autor at: Depto. Farmacobiología, Cin235, Col. Granjas Coapa, México, D.F. C.P. 14330, Mexico.
E-mail address: [email protected] (L. Rocha).Available online on ScienceDirect (www.scienced
0969-9961/$ – see front matter © 2011 Published by Eldoi:10.1016/j.nbd.2011.09.006
Please cite this article as: Rocha, L., et al., D(2011), doi:10.1016/j.nbd.2011.09.006
Ra b s t r a c t
a r t i c l e i n f o26
27
28
29
30
31
32
33
34
35
36
37
Article history:Received 15 June 2011Revised 3 September 2011Accepted 13 September 2011Available online xxxx
Keywords:Temporal lobe epilepsyDopamineD1 receptorsD2 receptorsDopamine transporterNeuropsychiatric disorders
38
39
40
41
42
43
44
45
46
RRECTED PExperiments were designed to evaluate different variables of the dopaminergic system in the temporal cortexof surgically treated patients with temporal lobe epilepsy (TLE) associated with mesial sclerosis (MTLE,n=12) or with cerebral tumor or lesion (n=8). In addition, we sought to identify dopaminergic abnormal-ities in those patients with epilepsy that had comorbid anxiety and depression. Specifically, we investigatedchanges in dopamine and its metabolites, D1 and D2 receptors, tyrosine hydroxylase (TH) and dopaminetransporter. Results obtained from patients with epilepsy were compared with those found in experimentsusing autopsy material. The neocortex of patients with MTLE demonstrated high D1 expression (1680%,pb0.05) and binding (layers I–II, 31%, pb0.05; layers V–VI, 28%, pb0.05), and decreased D2 expression(77%, pb0.05). The neocortex of patients with TLE secondary to cerebral tumor or lesion showed high expres-sion of D1 receptors (1100%, pb0.05), and D2-like induced activation of G proteins (layers I–I, 503%; layersIII–IV, 557%; layers V–VI, 964%, pb0.05). Both epileptic groups presented elevated binding to the dopaminetransporter and low tissue content of dopamine and its metabolites. Analysis revealed the following correla-tions: a) D1 receptor binding correlated negatively with seizure onset age and seizure frequency, and posi-tively with duration of epilepsy; b) D2 receptor binding correlated positively with age of seizure onset andnegatively with duration of epilepsy; c) dopamine transporter binding correlated positively with durationof epilepsy and frequency of seizures; d) D2-like induced activation of G proteins correlated positivelywith the age of patients. When compared with autopsies and patients with anxiety and depression, patientswithout neuropsychiatric disorders showed high D2-like induced activation of G proteins, an effect that cor-related positively with age of patient and seizure onset age, and negatively with duration of epilepsy. Thepresent study suggests that alterations of the dopaminergic system result from epileptic activity and couldbe involved in the physiopathology of TLE and the comorbid anxiety and depression.
47
vestav-Sede Sur, Calz. Tenorios
irect.com).
sevier Inc.
opamine abnormalities in the neocortex of pa
© 2011 Published by Elsevier Inc.
4849
O61
62
63
64
65
66
67
68
69
70
UNCIntroduction
Epilepsy is the second most important neurologic disorder withdiverse etiology. Temporal lobe epilepsy (TLE) is the most frequentand becomes pharmacologically untreatable in a high percentage ofpatients (Engel, 1996). In TLE associated with mesial sclerosis (MTLE),the hippocampus represents the epileptic focus, while the temporalneocortex is involved in propagation of epileptic seizures to otherbrain areas (Chagnac-Amitai and Connors, 1989; Chervin et al., 1988;Sloviter, 1994). Neocortex has been proposed to be involved in
71
72
73
74
75
76
secondary epileptogenesis as a consequence of progressive extensionof the primary epileptogenic zone with increased duration of epilep-sy (Morrell et al., 1987).
Epilepsy involves changes in several neurotransmitters (Fisherand Leppik, 2008; Olsen and Avoli, 1997). Concerning the dopaminer-gic system in temporal neocortex of patients with MTLE, studies usingPositron Emission Tomography (PET) indicate a reduction of D2/D3receptor binding in the pole and lateral areas, ipsilateral to the epilepticfocus (Werhahn et al., 2006). Regarding tissue content of dopamine andits metabolites, the results are controversial and it seems that changesdepend on the presence of epileptiform activity in the neocortex(Louw et al., 1989; Mori et al., 1987; Pacia et al., 2001; Pintor et al.,1990). In relation with tyrosine hydroxylase (TH), the enzyme respon-sible for DOPA synthesis (the precursor of dopamine), its activity isnot modified (Pintor et al., 1990). Despite the fact that D1 receptorsplay a modulating role in the synaptic activity of the neocortex
tients with temporal lobe epilepsy, Neurobiol. Dis.

77
78
79
80
81
82
83
84
85
86
87
88
89
90
91
92
93
94
95
96
97
98
99
100
101
102
103
104
105
106
107
108
109
110
t1:1
t1:2t1:3
t1:4
t1:5
t1:6
t1:7
t1:8
t1:9
t1:10
t1:11
t1:12
t1:13
t1:14
t1:15
t1:16
t1:17
t1:18
t1:19
t1:20
t1:21
t1:22
t1:23
t1:24
t1:25
t1:26
t1:27
t1:28
t1:29
t1:30
2 L. Rocha et al. / Neurobiology of Disease xxx (2011) xxx–xxx
(Bandyopadhyay and Hablitz, 2007; Wu and Hablitz, 2005), it is cur-rently unknown if they are altered in the brain of patients with MTLE.
It is described that dopaminergic system is involved in anxiety anddepression (Lehto et al., 2008; Sarkisova et al., 2008). Although studiessupport a bidirectional relationship between depression and epilepsy(Kanner, 2011), at present no evidence exists to support that dopami-nergic system represents a common potential pathogenic mechanismsoperant in both disorders.
The present study was designed to determine the precise condi-tion of dopaminergic system in the temporal neocortex of patientswith MTLE. With the purpose to investigate the influence of clinicalfactors on dopaminergic alterations, the results obtained were corre-lated with subject's age, age of seizure onset, duration of epilepsy andfrequency of ictal events. Additionally, data were compared with anaged matched group of patients with TLE secondary to brain tumoror lesion that had shorter epilepsy duration and older age at seizureonset. Dopaminergic abnormalities were also investigated in thosepatients with epilepsy that had comorbid anxiety and depression.
UNCO
RRECT
Table 1Summary of clinical data from patients with Temporal Lobe Epilepsy and Autopsies.
Patient Gender Age(years)
Seizureonset age(years)
Precipitatingfactors
Side offocus
Duration ofepilepsy(years)
Seizurefrequency(month)
P56 M 27 4 Hypoxia febrileseizures inchildhood
Right 23 3
P81 F 38 6 No Left 32 3
P88 F 29 8 No Right 21 30P93 M 25 7 Hypoxia Left 18 16P95 F 47 25 Cerebral
thrombosisRight 22 14
P98 M 32 8 Hypoxia Left 24 7.5
P104 M 60 6 No Left 54 9P105 M 24 6 Hypoxia febrile
seizures inchildhood
Right 18 4
P107 M 34 6 Cerebral injury Left 28 3
P123 M 35 13 Cerebral injury Left 22 12.5
P125 M 45 17 No Left 28 48
P127 F 38 3 Cerebral injuryfebrile seizuresin childhood
Left 35 15
P37 F 27 11 – Right 16 32
P54 F 34 1.33 – Right 32.6 38
P92 F 27 27 – Left 0.33 1
P99 F 48 46 – Left 2 18
P103 M 28 13 – Right 15 3
P112 M 40 40 – Right 0.16 1
P116 F 24 10 – Left 14 102
P119 M 32 28 – Left 4 1
C1 M 40 – – – – –
C2 M 29 – – – – –
C3 M 37 – – – – –
C4 M 33 – – – – –
C5 M 47 – – – – –
C6 M 51 – – – – –
AED, antiepileptic drugs; CBZ, carbamazepine; CLB, clobazam; CNZ, clonazepam; F, femaleepilepsy; OXCBZ, oxcarbazepine; PMI, POSTMORTEM INTERVAL; VAP, valproic acid; TOP, to
Please cite this article as: Rocha, L., et al., Dopamine abnormalities in th(2011), doi:10.1016/j.nbd.2011.09.006
F
Materials and methods
Patients and tissue collection
Temporal neocortex samples were collected from a group of 12patients with MTLE (7 men and 5 women) and from 8 patients withTLE secondary to brain tumor or lesion (4 men and 4 women).Table 1 includes a summary of relevant clinical data and location ofthe epileptic focus for each patient. Patients were submitted to theprotocol set out by the Epilepsy Surgery Program of the NationalInstitute of Neurology and Neurosurgery “Manuel Velasco Suarez” inMexico, which comprises an extensive pre-surgical clinical evalua-tion, video-electroencephalogram (EEG) record, magnetic resonanceimaging (MRI) and single photon emission computed tomography(SPECT). The EEG was used essentially to locate interictal epilepti-form activity. The video-EEG allowed at least the record of twocomplex partial seizures in each patient. Since ictal SPECT was not per-formed in every patient, interictal SPECT revealed valuable information
ED P
RO
O
AED beforesurgery
Psychiatriccomorbidity
Surgical outcome(Engel's classification)
Final diagnosis or cause ofdeath (PMI in hours)
CBZ, LMG,CNZ
No Class I MTLE
OXCBZ Depressionanxiety
Class II MTLE
VAP, CLB No Class I MTLECBZ, CNZ Depression Class I MTLELMG, CNZ,ZNS
Depression Class I MTLE
VAP, LMG,CLB
No Class IV Class IV
CBZ, LMG No Class I MTLEVAP, TOPCNZ
Depression Class I MTLE
VAP, CBZ,CLB
Depressionanxiety
Class II MTLE
VAP, CBZ,LMG
No Class I MTLE
OXCBZ, TOP,CLB
Anxiety Class I MTLE
VAP, LMGOXCBZ
Depressionanxiety
Class I MTLE
PHE, CBZ No Class III Astrocytoma inoccipitotemporal gyrus
CBZ, LMG No Class II Cavernoma inoccipitotemporal
DFH, VAP No Class I Oligoastrocitoma insuperior temporal gyrus
VAP, CNZ Depressionanxiety
Class I Cavernoma in hippocampusand parahippocampus
VAP, CBZ,CNZ
No Class I Glioma in hippocampusand parahippocampus
PHE No Class I Oligoastrocitoma in superiortemporal gyrus
CBZ No Class I Neuroectodermal tumorin temporal pole
PHE, CBZ Depression Class i Oligoastrocitoma insuperior temporal gyrus
– – – Asphyxia (5)– – – Hypovolemic shock (5)– – – Hypovolemic shock (10)– – – Hypovolemic shock (14)– – – Lymphoma (2)– – – Pulmonary cancer (4)
: HS, hipoccampal sclerosis; LMG, lamotrigine; M, male; MTLE, Mesial temporal lobepiramate; ZNS, zonizamida.
e neocortex of patients with temporal lobe epilepsy, Neurobiol. Dis.

T
111
112
113
114
115
116
117
118
119
120
121
122
123
124
125
126
127
128
129
130
131
132
133
134
135
136
137
138
139
140
141
142
143
144
145
146
147
148
149
150
151
152
153
154
155
156
157
158
159
160
161
162
163
164
165
166
167
168
169
170
171
172
173
174
175
176
177
178
179
180
181
182 Q6183
184
185
186
187
188
189
190
191
192
193
194
195
196
197
198
199
200
201
202
203
204
205
206
207
208
209
210
211
212
213
214
t2:1
t2:2t2:3
t2:4
t2:5
t2:6
t2:7
3L. Rocha et al. / Neurobiology of Disease xxx (2011) xxx–xxx
UNCO
RREC
about the hypoperfusion area (Huberfeld et al., 2006; Tae et al., 2005).MRI was performed with a 1.5 or 3 T unit and revealed the presenceof mesial sclerosis and volume reduction in the temporal pole area,but no significant changes in T2 and T3 gyri in patients with MTLE.MRI findings showed a clear concordance with EEG records. Patientswith focal cortical dysplasia were specifically excluded.
Patients were assessed with the Beck Depression Inventory (BDI),Montgomery-Asberg Depression Rating Scale (MADRS) and HamiltonAnxiety Scale (HAMA). They were classified as having a depressivesyndrome when BDI andMADRS scales indicated so by means of stan-dard cut-off points (14 points in the BDI and 20 points in the MADRS).Anxiety syndrome was established by means of a standard cut-offpoint (18 points) in the HAMA scale. The diagnosis of generalizedanxiety disorder was confirmed according to the results obtainedfrom the Structured Clinical Interview for DSM-IV Axis I Disorders(SCIDI), which diagnoses lifetime and current axis I psychiatric disor-ders (First et al., 1999; Lopez-Gomez et al., 2008). The scientific com-mittees of the institutions involved in this investigation approved thisstudy and informed consent was obtained from each patient.
An electrocorticographic (ECoG) record with 4×8-electrode grids(Ad-Tech, Racine, WI) was performed during epilepsy surgery to iden-tify neocortex with epileptiform activity for subsequent resection. Tis-sue (T2 and T3 gyri) was collected immediately after resection, frozenin milled dry ice and stored at−70 °C until processing. Tissue samplesused for the present study did not involve the tumor or any knownpathology.
Results obtained from patients with MTLE and TLE secondary tobrain tumor or lesion were compared to those obtained from temporalneocortex of 6 subjects (6 men) who died due to different causes, andhad no history of neurologic disease. T2 and T3 gyri were collected atthe time of the autopsy with a post-mortem interval (PMI) of 2 to14 h, and were immediately stored at −70 °C (Table 1).
Three fragments were obtained from each brain sample of patientswith epilepsy and from the autopsies. The fragmentation was donemaintaining the tissue frozen, a situation that allowed to preserve theproper conditions for the dopaminergic system (Nyberg et al., 1982).A fragment including only graymatterwas used to determine the tissuecontent of dopamine and its metabolites, 3,4-dihydroxyphenylaceticacid and homovanillic acid (DOPAC and HVA, respectively). A secondgray matter fragment was used for Western blot analysis to examineprotein expression of D1 and D2 receptors, and TH. The third fragmentthat included both, gray and white matter, was used for autoradiogra-phy experiments.
Autoradiography experiments
Preparation of tissue sectionsFrozen sections of 20m were cut in a cryostat, thaw-mounted on
gelatin-coated slides, and stored again at −70 °C. Serial and parallelsections were obtained from each sample for quantitative and func-tional autoradiography.
Quantitative autoradiographyTable 2 includes a summary of the experimental conditions for the
autoradiography experiments. Initially, brain sections were washed to
Table 2Conditions for autoradiography experiments.
Binding Ligand (nM) S.A. Buffer pH 7.6
D1 receptor 3H-SCH23390 (1.62 nM) 85 Ci/mmol Tris HCl (50 mM), 120 mM5 mM KCl 1 mM MgCl2 2 m
D2 receptor 3H-Raclopride (4 nM) 60 Ci/mmol Tris HCl (50 mM) 150 mMNaCl 0.1% Ascórbic Ac.
Dopamine transporter 3H-Mazindol (4 nM) 20.6 Ci/mmol Tris HCl (50 mM), 300 mMNaCl, 5 mM KCl
S.A., specific activity; RT, room temperature.
Please cite this article as: Rocha, L., et al., Dopamine abnormalities in th(2011), doi:10.1016/j.nbd.2011.09.006
ED P
RO
OF
remove endogenous ligands, and they were subsequently incubated ina solution with the specific ligand labeled with tritium (3H) in presenceor absence of a non-labeled specific ligand. The specific binding valueswere determined from the difference of values obtained from bothexperimental conditions. Incubation was completed with two consecu-tive washings in buffer solution and then rinsed with distilled water(2 s) at 4 °C. Sections were immediately dried in a gentle steam ofcold air.
Preparations were placed in X-ray cassettes together with 3H stan-dards (Amersham) and were exposed to 3H-sensitive film (Kodak MR)at room temperature. Films were developed with Kodak D19 developerand fast fixer at room temperature. Optical densities of cortical layers ofeach brain section were determined using image analysis software(JAVA Jandel). Optic density readings of the standardswere used to calcu-late radioactivity values of accompanying tissue sections. Finally, theywere converted into fmol/mg of protein based on the specific activity ofeach 3H-labeled ligand and tissue thickness (20 μm).
Functional autoradiographyAgonist-stimulated [35S]GTPγS autoradiography was performed
as described previously (Sim and Childers, 1997; Sim et al., 1996).Sections were soaked for 10 min at 25 °C in 50 mM Tris–HCl buffer(pH 7.4) to remove endogenous catecholamines. They were then pre-incubated for 15 min in the same buffer, to which 100 mM NaCl,3 mM MgCl2, 0.2 mM EGTA and 2 mM GDP were added. Forty pM[35S]GTPγS was then added to this solution, for a 2 h incubation at25 °C in basal conditions. Basal binding was measured in absence ofthe tested compound. To evaluate stimulated condition due to G pro-teins activity dependent of D2-like receptor activation it was useddopamine 100 μM in the presence of SCH23390 500 μM (Sigma, St.Louis, MO, USA), a non-selective D1-like DA receptor antagonist. Inother sections, the effects of dopamine receptor antagonist wereexamined on the activation evoked by dopamine 100 μM in the pres-ence of SCH23390 and sulpiride (non-selective D2-like receptor antago-nist), 500 μMeach (Sigma, St. Louis,MO, USA). Non-specific bindingwasdetermined in presence of 10 μMunlabelled GTPγS and subtracted frombasal binding. Finally, slides were washed twice in buffer and once indistilled water at 4 °C. The autoradiograms were produced on KodakBiomax MR™ film, exposed for 48–72 h along with 14C standards(Amersham) and processed in GBX™ (Kodak) developer. Optical densi-ties were obtained following the same procedure of autoradiographyand results were represented as mean values±SD in fmol/mg proteinafter subtracting non-specific value to the basal and stimulatedvalues. Net agonist-stimulated [35S]GTPγS binding was calculatedby subtracting basal binding (obtained in absence of agonist) fromagonist-stimulated binding, and expressed as percentage stimula-tion above basal.
Tissue content of monoamines
Brain tissue was thawed and manually and individually homoge-nized into a mixture of perchloric acid (0.1 M, Baker), sodium meta-bisulphite (4 mM Na2S2O3, Sigma) and ethylenediaminetetraaceticacid (0.1 mM EDTA, Sigma). The homogenate was centrifuged at12,600 rpm for 20 min at 4 °C. Subsequently, 10 μL of the previously
Incubation conditions Exposition (R.T.) Non-labeled ligand
NaClM CaCl2
90 min+1 μM mianserin 22°C 12 weeks SCH23390 (1 μM)
45 min 22°C 8 weeks Butaclamol (1 μM)
40 min+0.3 μM desipramine 4°C 12 weeks GBR12935 (1 μM)
e neocortex of patients with temporal lobe epilepsy, Neurobiol. Dis.

T
215
216
217
218
219
220
221
222
223
224
225
226
227
228
229
230
231
232
233
234
235
236
237
238
239
240
241
242
243
244
245
246
247
248
249
250
251
252
253
254
255
256
257
258
259
260
261
262
263
264
265
266
267
268
269
270
271
272
273
274
275
276
277
278
279
280
281
282
283
284
285
286
287
288
289
290
291
292
293
294
295
296
297
298
299
300
301
302
303
304
305
306
307
308
309
310
311
312
313
314
315
316
317
318
319
320
321
322
323
324
325
326
327
328
329
330
331
332
333
334
335
336
4 L. Rocha et al. / Neurobiology of Disease xxx (2011) xxx–xxx
UNCO
RREC
filtered supernatant (Millex®-HV filters, 0.45 μm pore) were injectedinto the chromatographer. An isocratic system with a mobile phaseflow of 0.350 mL/min at 30 °C with +560 mV was used for the elutionof dopamine and its metabolites (DOPAC and HVA). A chromatographysystem coupled to an electrochemical detector (Waters® model 2465)with Atlantis dC18 precolumn (3.9×20 mm) and Atlantis dC18 reversephase column (3.9×50 mm), both with 3 μm pore, was used. Mobilephase was a combination of EDTA (0.054 mM Sigma), 10.5 g/L of citricacid (Sigma), octanesulfonic acid (21.61 mg/L Sigma) and methanol(3% Merck), pH 2.9 adjusted with sodium hydroxide. Quantification ofdopamine and its metabolites was performed with the Empower v.1software by Waters, from a calibration curve obtained with differentconcentrations of external standards.
Determination of proteins
Protein quantification was performed according to the protocoldescribed by Lowry et al. (1951) using the remnant pellet in theEppendorf tube after separating the brain homogenate supernatant(see above). The pellet was suspended in 250 μL of miliQ water andfrom this solution, a 1:40 dilution with water (1 μL of sample and39 μL of water) was prepared. An aliquot of 100 μL of this dilutionwas added with 500 μL of reagent A (100 μL of 1% CuSO4, 100 μL of2% potassium sodium tartrate and 10 mL of 2% Na2CO3). The mixturewas stirred and stored at room temperature for 10 min. Subsequently,reagent B (2 N Folin & Ciocalteu phenol reagent (Sigma) diluted 1:2 inmiliQ water) was added. The mixture was stirred and stored at roomtemperature in the dark for 30 min. Then, absorbance of the sampleswas determined using an UV–VIS spectrophotometer (Beckman DU640) at 700 nm. Protein concentration in samples was calculatedbased on a standard curve prepared with different concentrations ofbovine albumin fraction V (Gibco). The obtained values allowedexpressing the values resulting from the high performance liquidchromatography in ng/mg of proteins.
Western blot assay
Tissue was homogenized in 1 mL of “TriPure” reagent (RocheDiagnostics) in order to allow protein isolation. The homogenatewas added with 0.2 mL of chloroform, followed by isopropanol toprecipitate total proteins. Samples were centrifuged at 12,000 rpmfor 10 min at 4 °C, and washed 3 times with 0.3 M guanidine hydro-chloride in 95% ethanol and a final washing was performed with100% ethanol. Samples were centrifuged according to the previouslydescribed procedure (Perez-Severiano et al., 2002), and the resultingpellet was suspended in 1% sodium dodecyl sulfate (SDS). Volumesequivalent to 50 μg of proteins (determined by the bicinchoninic acidmethod) were transferred to 8% polyacrylamide gel, separated usingelectric current at 150 V and transferred again to a nitrocellulosemembrane (Immun-Blot PVD, Bio-Rad). Subsequently, membraneblockage was performed with 5% half-skimmed milk and 0.05%Tween-20 for 30 min at room temperature, followed by incubation for12 h at 4 °C with one of the following antibodies: polyclonal antibodyto TH (1:1000, Cell Signaling 2792), polyclonal antibody to D1 receptor(1:200, Santa Cruz, SC-14001) or monoclonal antibody to D2 receptor(1:200, Santa Cruz, SC-5303). After 24 h, membranes were washedand exposed to secondary antibodies labeled with peroxidase for THlabeling, and antibodies to rabbit and mouse for D1 and D2 receptors,respectively (1:3000; Invitrogen), in blocking solution for 1 h at roomtemperature. Membranes were washed and protein labeling was ana-lyzed using a Western chemiluminescent detection system (PerkingElmer LAS, Inc). Then, the aforementioned antibodies were removedfrom the membranes for incubation with a monoclonal antibody toβ-actin (Garcia-Tovar et al., 2001). The latter assay was used as controlto standardize the values of protein level expression. The procedure toremove antibodies from membranes was as follows: first, membranes
Please cite this article as: Rocha, L., et al., Dopamine abnormalities in th(2011), doi:10.1016/j.nbd.2011.09.006
ED P
RO
OF
were washed four times with phosphate buffer solution and salinesolution (0.015 M, 0.9% NaCl, pH 7.4). Then, they were immersed intoa solution containing 2-mercaptoethanol (100 mM), SDS (2%) andTris–HCl buffer solution (62.5 mM, pH 6.7) for 30 min at 60 °C withslow stirring. Membranes were washed five times in phosphate buffersolution and saline solution with 0.05% Tween-20. The obtained imageswere digitalized using the BioDoc-It system (UVP) and optical densitywas determined using image capture and analysis software (UVP),according to the previously stated description (Perez-Severiano et al.,2002).
Statistical analysis
Values are expressed as mean±standard deviation (SD) and wereexamined using ANOVA test and Dunnett's post-hoc test. Pearson'scorrelation coefficients were calculatedwith amultiple regression anal-ysis against the values obtained in different experiments performed todetermine the possible influence of subject's age, age of seizure onset,duration of epilepsy and frequency of ictal events.
Results
The clinical data from patients with MTLE were as follows (mean±SD): age of subjects, 36.5±10.8 years (ranged from 24 to 60 years); ageat seizure onset, 9.18±6.6 years; years of epilepsy duration, 27.3±10.4; and seizures per month, 14.8±13.4. Patients with TLE secondaryto tumor or lesion presented similar age (32.6±8.1 years old, rangedfrom 24 to 48 years old, pb0.4) and seizure frequency (24.5±34seizures per month, pb0.409), but the age at seizure onset (22.1±15.8 years) and epilepsy duration (10.5±11.2 years)were significantlydifferent (pb0.01 and pb0.001, respectively), when compared withpatients with MTLE. The average age of patients with MTLE and TLEsecondary to tumor or lesion was not significantly different whencompared with subjects from autopsies (39.5±8.3 years, rangingfrom 21 to 51 years, pb0.51). Fifty-eight % (n=7) of patients withMTLE and 25% (n=2) of patients with TLE secondary to tumor or lesionpresented comorbid anxiety and depression. Postoperative outcomeevaluated 1 year after epilepsy surgery was similar for both epilepsygroups: nine patients (75%) from the MTLE group and 6 patients(75%) from the lesional TLE group achieved seizure freedom (Engelclass I); two patients (16.6%) from MTLE group and one patient(12.5%) with TLE secondary to tumor or lesion showed rare disablingseizures (Engel class II); one patient (12.5%) from TLE secondary totumor or lesion demonstrated worthwhile improvement (Engel classIII); and one patient (8.3%) from the MTLE group exhibited no worth-while improvement (Engel class IV) (Table 1).
Autopsies
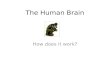
Tissue levels of dopamine, DOPAC and HVA (mean±SD) from theautopsies were 2.9±2.2, 13.9±10.38 and 18.7±13.97 nM/mg ofprotein, respectively (Fig. 1). The Western blot experiments allowedthe evaluation of protein expression in D1 and D2 receptors, as wellas in TH (Fig. 2). Binding of 3H-SCH23390, 3H-Raclopride and 3H-Mazindol to D1 and D2 receptors, and to the dopamine transporter,respectively, was widely distributed in the various temporal neocor-tex layers. We detected high values for binding to 3H-Mazindol (ap-proximately 400 fmol/mg protein), while values for binding to 3H-SCH23390 and 3H-Raclopride were low (around 50 fmol/mg protein)(Fig. 3). Functional autoradiography revealed that in the presence ofSCH23390, dopamine induced a [35S]GTPγS incorporation of 14.3%in layers I–II, 7.6% in layers III–IV and 4.4% in layers V–VI (Fig. 4).
In order to determine the post-mortem stability of tissue, valuesobtained from the different experiments were subjected to correla-tion analysis with PMI. Data obtained from this examination indicatedthat, under our experimental conditions, post-mortem delay did not
e neocortex of patients with temporal lobe epilepsy, Neurobiol. Dis.

TED P
RO
OF
337
338
339
340
341
342
343
344
345
346
347
348
349
350
351
352
353
354
355
356
357
358
359
360
361
362
363
364
365
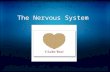
Fig. 1. Tissue levels of dopamine, 3,4-dihydroxyphenylacetic acid (DOPAC) and homo-vanillic acid (HVA) in neocortex obtained from autopsies and patients with MTLE orTLE secondary to brain tumor or lesion. The values represent the mean±SD expressedin nM/mg of protein. *pb0.05; **pb0.01, regarding the autopsy values.
Fig. 3. Binding of 3H-SCH23390 (D1), 3H-Raclopride (D2) and 3H-Mazindol (Transporter)in external (I–II), middle (III–IV) and deep (V–VI) cortical layers in samples of autopsiesand patients with MTLE or TLE secondary to brain tumor or lesion. The values representthemean±SDexpressed in fmol/mg of protein. *pb0.05; **pb0.01, regarding the autopsyvalues.
5L. Rocha et al. / Neurobiology of Disease xxx (2011) xxx–xxx
RREC
affect the different components of the dopaminergic system evaluat-ed in the present study (Table 3).
Patients with epilepsy
The diagnosis of each patient with epilepsy was performed accordingto clinical, MRI and electrophysiological criteria. Every patient presentedinterictal epileptiformactivity in the temporal cortex ipsilateral to the ep-ileptogenic focus. Nomorphological alterationwas identified in the later-al temporal neocortex. SPECT revealed interictal hypoperfusion inmesialstructures in patients with MTLE. ECoG performed intraoperatively con-firmed the presence of epileptiform activity in T2 and T3 gyri.
Patients with MTLEThe values for tissue content of dopamine, DOPAC and HVA
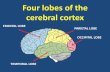
were significantly lower (60%, pb0.05; 96%, pb0.01; and 79%, pb0.01,respectively) than those obtained in autopsies' tissue (Fig. 1). The tem-poral neocortex obtained from patients with MTLE presented high(1680%, pb0.05) and low (77%, pb0.05) protein expression of D1 andD2 receptors, respectively, while the expression of TH showed no signifi-cant changes (Fig. 2). Likewise, an increasewas detected in binding of 3H-SCH23390 (layers I-II, 31%, pb0.05; layers V-VI, 28%, pb0.05), as well asof 3H-Mazindol (layers I–II, 89%, pb0.05; layers III–IV, 141%, pb0.01;layers V–VI, 114%, pb0.01) (Fig. 3). Functional autoradiography demon-strated a D2-like induced [35S]GTPγS incorporation similar to thatdetected in autopsy samples (Fig. 4).
Correlations between these results and clinical data suggest the fol-lowing: the younger the age of seizure onset, the higher the binding toD1 receptors in all temporal cortex layers and the lower the binding to
UNCO 366
367
368
Fig. 2. Protein expression of D1 and D2 receptors, and tyrosine hydroxylase (TH) in neocor-tex obtained from autopsies and patients with MTLE or TLE secondary to brain tumor or le-sion. Western blot analyses representative of each experiment are shown in the upper partof the graphs. Values obtained in the image densitometric analysis are shown in bars; theywere corrected for β-actin values. The graphs show themean±SD of the ratio between op-tical density (OD) and β-actin expression. *pb0.05, regarding the autopsy values.
Please cite this article as: Rocha, L., et al., Dopamine abnormalities in th(2011), doi:10.1016/j.nbd.2011.09.006
D2 receptors in layers I–II and V–VI; the higher the frequency of sei-zures, the lower the binding to D1 receptor in all temporal cortexlayers; the older the age of the patient, the higher the D2-like in-duced Gi stimulation in layers V-VI (Table 4). Results from high per-formance liquid chromatography and Western blot revealed nosignificant correlations with clinical data.
369
370
371
372
373
374
375
376
377
378
379
380
381
382
383
384
Patients with TLE secondary to brain tumor or lesionAs compared with the results obtained from biopsies, neocortex of
patients with TLE secondary to tumor or brain lesion presented signifi-cant lower values for tissue content of dopamine, DOPAC and HVA(81%, pb0.01; 98%, pb0.01; and 89%, pb0.01, respectively) (Fig. 1).This tissue presented an increase in the protein expression of D1 recep-tors (1100%, pb0.05), while expression of D2 receptors and TH showedno significant changes (Fig. 2). Likewise, an increase in binding of3H-Mazindol (layers I–II, 89%, pb0.01; layers III–IV, 127%, pb0.01;layers V–VI, 98%, pb0.01) was detected, in contrast with binding of3H-SCH23390 and 3H-Raclopride, which presented no alterations(Fig. 3). In contrast with autopsies and MTLE patients, tissue obtainedfrom patients with TLE secondary to tumor or lesion demonstrated asignificant increase of [35S]GTPγS incorporation in all cortical layers(layers I–II, 503%, pb0.05; layers III–IV, 557%, pb0.05; layers V–VI,964%, pb0.01) (Fig. 4).
e neocortex of patients with temporal lobe epilepsy, Neurobiol. Dis.

T
RO
OF
385
386
387
388
389
390
391
392
393
394
395
396
397
398
399
400
401
402
403
404
405
406
407
408
409
410
411
412
413
414
415
416
417
Fig. 4. Binding of [35S]GTPγS in external (I–II), middle (III–IV) and deep (V–VI) corticallayers in A) samples of autopsies and patients with MTLE or TLE secondary to braintumor or lesion; and B) samples of autopsies and patientswith epilepsy that had comorbiddepression and anxiety (D/A), and without psychiatric disorders (NO D/A). The values areexpressed as average of percentage stimulation above basal±SD. *pb0.05; **pb0.01,regarding the autopsy values.
t3:1
Q2t3:2t3:3
t3:4
t3:5
t3:6
t3:7t3:8
t3:9
t3:10
t3:11
t3:12t3:13
Table 4 t4:1
Correlations between clinical data and binding in temporal neocortex of patients withMTLE.
t4:2t4:3Binding and
ligandAge ofpatient
Seizure onsetage
Duration ofepilepsy
Frequency ofseizures
t4:4D1 3H-SCH23390t4:5Layers I–II −0.2768 −0.5261⁎ 0.2568 −0.5503⁎
t4:6Layers III–IV −0.3412 −0.5047⁎ −0.1467 −0.7180⁎⁎
t4:7Layers V–VI −0.1627 −0.6614⁎⁎ −0.1718 −0.6740⁎
t4:8
t4:9D2 3H-Raclopridet4:10Layers I–II 0.2799 0.6639⁎ −0.1467 −0.0951t4:11Layers III–IV 0.0552 0.3602 −0.1718 −0.1580t4:12Layers V–VI 0.2303 0.5718⁎ −0.0743 0.0232t4:13
t4:14Transporter 3H-Mazindolt4:15Layers I–II 0.0566 0.1976 −0.0689 −0.3277t4:16Layers III–IV 0.2226 0.2743 0.0422 −0.1705t4:17Layers V–VI 0.2888 0.3485 −0.0539 0.1998t4:18
t4:19Gi Protein 35S-GTPγSt4:20Layers I–II −0.2336 −0.0205 −0.2116 0.1823t4:21Layers III–IV 0.2861 0.2579 0.1143 0.1324t4:22Layers V–VI 0.5683⁎ 0.2599 0.3841 0.0693
Values represent the Pearson Correlation Coefficients.t4:23⁎ pb0.05. t4:24
⁎⁎ pb0.01. t4:25
Table 5 t5:1
Correlations between clinical data and binding in temporal neocortex of patients withTLE secondary to tumor or brain lesion.
t5:2t5:3Binding and
ligandAge ofpatient
Seizureonset age
Durationof epilepsy
Frequencyof seizures
t5:4D1 3H-SCH23390t5:5Layers I–II 0.3209 −0.2379 0.5674⁎ 0.1575t5:6Layers III–IV 0.3558 −0.0158 0.2359 −0.0957
6 L. Rocha et al. / Neurobiology of Disease xxx (2011) xxx–xxx
CO
RREC
Correlations of clinical data with the obtained results suggest thatthe longer the duration of epilepsy, the higher the D1 (layers I–II) andthe lower the D2 (layers III–IV and V–VI) receptor binding; the olderthe age of epilepsy onset, the higher the binding to D2 receptors inlayers III–IV and V–Vl; the higher the frequency of seizures, the higherthe binding to dopamine transporter in layers I–II and III–IV; the olderthe age of the patient, the higher the D2-like induced [35S]GTPγSincorporation in layers III–IV and V–VI. No other significant correlationswere detected (Table 5).
Patients with epilepsy and psychiatric comorbidity
Concerning dopaminergic changes in patients with psychiatric co-morbidity, patients with MTLE and with TLE secondary to tumor or le-sion were combined because no significant differences were detectedbetween both epilepsy groups (data not shown). Analysis revealedthat neocortex of patients with anxiety and depression showed 35S-GTPγS binding values similar to autopsy samples, whereas neocortexof patients without psychiatric comorbidity presented higher 35S-GTPγS binding incorporation in layers I–II (494%, pb0.05), III–IV(228%, pb0.01) and layers V–VI (112%, pN0.05) (Fig. 4). No furtherchanges were detected.
UN
Table 3Correlations between the values obtained in autopsy samples and the interval betweendeath and tissue collection (post-mortem interval).
D13H-SCH23390
D23H-Raclopride
Transporter3H-Mazindol
Gi35S-GTPγS
Layers I–II −0.3719 −0.4328 0.6119 −0.1057Layers III–IV −0.1273 −0.1755 −0.4409 0.1599Layers V–VI −0.1854 0.2989 −0.5325 0.1148
Western blot HPLC
D1 Dopamine −0.5861 −0.2678D2 DOPAC 0.2044 0.5326TH HVA 0.3736 0.3466
DOPAC, 3,4-dihydroxyphenylacetic acid;HVA,homovanillic acid; TH, tyrosine hydroxylase.Values represent Pearson Correlation Coefficients.
Please cite this article as: Rocha, L., et al., Dopamine abnormalities in th(2011), doi:10.1016/j.nbd.2011.09.006
ED PIn both groups of patients (with and without anxiety and depres-
sion), D1 receptor binding correlated positively with duration of epi-lepsy, whereas D2 receptor binding correlated positively with the ageof seizure onset. In patients with anxiety and depression, D2 receptorbinding correlated positively with age of patients, while transporterbinding correlated positively and negatively with duration of epilepsyand age of seizure onset, respectively. In patients without psychiatriccomorbidily, transporter binding correlated positively with seizurefrequency, whereas 35S-GTPγS binding correlated positively withage of patient and age of seizure onset, and negatively with durationof epilepsy. In contrast, patients with anxiety and depression did notshow significant correlations between clinical data and 35S-GTPγSbinding (Tables 6 and 7). No further correlations were detected.
t5:7Layers V–VI 0.3342 0.1148 0.0824 −0.3332t5:8
t5:9D2 3H-Raclopridet5:10Layers I–II −0.1660 0.2378 −0.4581 −0.0457t5:11Layer III–IV 0.5245 0.8194⁎⁎ −0.7782⁎ −0.1840t5:12Layer V–VI 0.5186 0.7526⁎ −0.6864⁎ −0.4172t5:13
t5:14Transporter 3H-Mazindolt5:15Layers I–II −0.5601 −0.6166 0.4683 0.6557⁎
t5:16Layers III–IV −0.4480 −0.5951 0.5186⁎ 0.6681⁎
t5:17Layers V–VI −0.3630 −0.5646 0.5380⁎ 0.4128t5:18
t5:19Gi Protein 35S-GTPγSt5:20Layers I–II 0.1810 0.2191 −0.4018 −0.3910t5:21Layers III–IV 0.5592⁎ −0.4327 −0.1290 −0.1368t5:22Layers V–VI 0.5372⁎ 0.4238 −0.2121 −0.2802
Values represent the Pearson Correlation Coefficients.t5:23⁎ pb0.05. t5:24
⁎⁎ pb0.01. t5:25
e neocortex of patients with temporal lobe epilepsy, Neurobiol. Dis.

T418
419
420
421
422
423
424
425
426
427
428
429
430
431
432
433
434
435
436
437
438
439
440
441
442
443
444
445
446
447
448
449
450
451
452
453
454
455
456
457
458
459
460
461
462
463
464
465
466
467
468
469
470
471
472
473
474
475
476
477
478
479
480
481
482
483
484
485
486
487
488
489
490
491
492
493
494
495
496
497
498
Table 6t6:1
Correlations between clinical data and binding in temporal neocortex of patients withTLE and anxiety and depression.
t6:2t6:3 Binding and
ligandAge ofpatient
Seizureonset age
Durationof epilepsy
Frequencyof seizures
t6:4 D1 3H-SCH23390t6:5 Layers I–II −0.0709 −0.5382 0.6093⁎ 0.0290t6:6 Layers III–IV 0.0276 −0.2524 0.3335 −0.1158t6:7 Layers V–VI −0.0790 −0.4785 0.5292⁎ −0.0224t6:8
t6:9 D2 3H-Raclopridet6:10 Layers I–II 0.4765 0.2854 0.0195 −0.0458t6:11 Layers III–IV 0.6626⁎ 0.6148⁎ −0.0242 −0.0415t6:12 Layers V–VI 0.7156⁎ 0.3586 0.1159 −0.0065t6:13
t6:14 Transporter 3H-Mazindolt6:15 Layers I–II −0.0647 −0.3409 0.3705 −0.0906t6:16 Layers III–IV −0.0332 −0.5935⁎ 0.7070⁎ 0.0068t6:17 Layers V–VI −0.0715 −0.3649 0.3948 0.1058t6:18
t6:19 Gi Protein 35S-GTPγSt6:20 Layers I–II −0.0761 −0.0227 −0.0313 −0.1337t6:21 Layers III–IV 0.4203 0.0042 0.4791 0.4807t6:22 Layers V–VI −0.1026 0.3600 −0.4247 −0.3024
Values represent the Pearson Correlation Coefficients.t6:23 ⁎ pb0.05.t6:24
Table 7 t7:1
Correlations between clinical data and binding in temporal neocortex of patients withTLE without anxiety and depression.
t7:2t7:3Binding and
ligandAge ofpatient
Seizure onsetage
Duration ofepilepsy
Frequency ofseizures
t7:4D1 3H-SCH23390t7:5Layers I–II −0.0995 −0.2459 0.7333⁎ −0.0105t7:6Layers III–IV −0.3024 −0.0920 0.5810⁎ −0.1698t7:7Layers V–VI −0.0868 0.0070 0.4979⁎ −0.2982t7:8
t7:9D2 3H-Raclopridet7:10Layers I–II −0.0994 0.0080 0.1682 −0.0590t7:11Layers III–IV −0.0557 0.0174 0.0945 −0.0663t7:12Layers V–VI 0.0817 0.5085⁎ −0.2099 −0.2524t7:13
t7:14Transporter 3H-Mazindolt7:15Layers I–II 0.0885 −0.2371 −0.0536 0.4656⁎
t7:16Layers III–IV 0.0637 −0.3136 0.1346 0.6304⁎
t7:17Layers V–VI 0.1890 −0.2320 0.2188 0.3966t7:18
t7:19Gi Protein 35S-GTPγSt7:20Layers I–II 0.1388 0.5633⁎ −0.5465⁎ −0.2739t7:21Layers III–IV 0.5081⁎ −0.2191 −0.1876 −0.0840t7:22Layers V–VI 0.5581⁎ −0.2959 −0.2401 −0.1941
Values represent the Pearson Correlation Coefficients.t7:23⁎ pb0.05. t7:24
7L. Rocha et al. / Neurobiology of Disease xxx (2011) xxx–xxx
UNCO
RREC
Discussion
The present study supports the idea that dopaminergic neurotrans-mission is altered in the temporal neocortex of patients with MTLE orTLE secondary to tumor or lesion. Our experiments allowed us to eval-uate different issues of dopaminergic neurotransmission and analyzethe possible influence of clinical factors.
Values obtained from the surgical material of patients with MTLEor with TLE secondary to brain tumor or lesion were compared tovalues from autopsies of subjects of similar age in order to reduce var-iables such as subjects' age that normally influence the dopaminergicsystem (Zelnik et al., 1986). In the present study, correlation analysissupported that PMI up to 14 h did not exert a significant effect on thelevels of dopamine, its metabolites, transporter, TH and receptors. Al-though this information and results obtained from other authors(Gilmore et al., 1993; Nyberg et al., 1982; Staley et al., 1995; Tupalaet al., 2006; Wolf et al., 1991) led to suggest that tissue from autop-sies can serve as control, further experiments should be conductedin rodents to determine the precise impact of post-mortem delayon dopaminergic system.
Our data indicate that the temporal neocortex of patients withMTLEpresents changes in dopamine receptors and transporter, which are dif-ferent from those detected in the neocortex of patients with lesionalTLE. This situation can be explained because patientswithMTLEpresentlonger duration of epilepsy and younger age at seizure onset. Indeed,the increased duration of epilepsy, considered as predictor of poor out-come (Hennessy et al., 2001; Rodin, 1968), has been associatedwith re-cruitment of the adjacent cortex into the epileptogenic zone (Morrellet al., 1987), a situation that may involve progressive impairment ofthe dopaminergic system. An important aspect of the present study isthat many of the variables evaluated correlated with clinical data, lead-ing to suggest that dopaminergic changes result from epileptic activityand/or antiepileptic therapy.
Our experiments revealed a decrease in the tissue levels of dopamineand itsmetabolites in the temporal neocortex of patientswithMTLE andwith TLE secondary to tumor or lesion, and support the results obtainedbyMori et al. (1987) and Pacia et al. (2001). The reduction in tissue con-tent of DOPAC and HVA insinuates a decrease in metabolism and/orrelease of dopamine. Since there are no changes in TH expression (pre-sent study) and activity (Pintor et al., 1990), it is not possible to suggestalterations in the synthesis of DOPA, the dopamine precursor. Another
Please cite this article as: Rocha, L., et al., Dopamine abnormalities in th(2011), doi:10.1016/j.nbd.2011.09.006
ED P
RO
OF
possibility to explain the low levels of dopamine is an increase in theexpression of monoamine oxidase (MAO), enzyme involved in the deg-radation of this catecholamine. The increase of binding to B-typeMAO inthe cerebral cortex of patientswith TLE sustains this idea (Kumlien et al.,1995). Regarding alterations in reuptake, we found that dopaminetransporter binding was increased in the temporal cortex of patientswith MTLE and with TLE secondary to brain tumor or lesion, and in thelatter this change was positively correlated to frequency of seizures.These findings are similar to those reported by Del Sole et al. (2010) inpatients with epilepsy associated with ring chromosome 20 syndrome.Similarly, patients with generalized idiopathic epilepsy present anincrease in the expression of the geneencoding the dopamine transport-er (Sander et al., 2000). The positive correlation between seizure fre-quency and dopamine transporter binding observed in this study andin the study by Del Sole et al. (2010) can represent a compensatorymechanism to remove dopamine released as a result of ictal activity(Meurs et al., 2008) or prolonged administration of antiepileptic drugs(Clinckers et al., 2005; Murakami et al., 2001; Okada et al., 1997).However, further studies are necessary to support this idea.
Our results indicate an increase in protein expression and bindingof D1 receptors in the temporal neocortex of patients with MTLE. Animportant factor to be considered is that the increase in glutamatergicneurotransmission characterizing pharmacoresistant MTLE (Duringand Spencer, 1993; Luna-Munguia et al., 2011) has been associatedwith increased D1 receptors binding (Sarantis et al., 2009; Scott andAperia, 2009). In contrast, neocortex of patients with TLE secondaryto tumor or lesion did not present significant changes in D1 receptorbinding in spite of a higher protein expression. It is possible thathigher D1 receptor binding is evident after a long duration of epilepsyand/or in patients in whom the epileptic activity started at an earlierage, an idea supported by correlation analysis.
Although protein expression of D2 receptorswas reduced inpatientswith MTLE, its binding was not modified, which might be explained bya compensatory increase in receptor affinity. The absence of changes inD2 receptor binding found in our autoradiography experiments is indisagreement with the decrease in binding of 18F-Fallypride in corticalareas surrounding the epileptic foci of patients with MTLE detected byPET (Werhahn et al., 2006). Although 18F-Fallypride and 3H-Racloprideare both antagonists of the D2–D3 receptor family, diverse methodolo-gy differences between PET and in vitro autoradiography may be re-sponsible for the discrepancies between Werhahns's study and the
e neocortex of patients with temporal lobe epilepsy, Neurobiol. Dis.

T
499
500
501Q7502
503
504
505
506
507
508
509
510
511
512
513
514
515
516
517
518
519
520
521
522
523
524
525
526
527
528
529
530
531
532
533
534
535
536
537
538
539
540
541
542
543
544
545
546
547548549550551552553554555556557558559560561562
563564565566567568569570571572573574575576577578579580581582583584585586587588589590591592593594595596597598599600601602603604605606607608609610611612613614615
8 L. Rocha et al. / Neurobiology of Disease xxx (2011) xxx–xxx
EC
results obtained in the present study. For example, the presence of en-dogenous competitors such as dopamine appears to alter themeasuredspecific binding of some ligands during PET studies (Morris and Yoder,2007).
In the present study, correlation analysis suggests high D2 recep-tor binding (patients with MTLE and lesional TLE) and elevated D2-like induced activation of G proteins (patients with epilepsy withoutpsychiatric comorbidity) when epilepsy initiates at later ages andwhen duration of illness is short. If activation of dopamine D2 sub-family receptors has an inhibitory role in the cerebral neocortex ofpatients with epilepsy (Barone et al., 1991), and alleviates symptomsproduced by depression (Bonci and Hopf, 2005; Breuer et al., 2009),these effects might be predominant during the early years followingepilepsy onset and might avoid psychiatric disorders. This idea is sup-ported by the increase in D2-like-induced activity on [35S]GTPgSbinding observed in the temporal neocortex of patients with TLE sec-ondary to tumor or lesion, who presented a shorter duration of epi-lepsy and less comorbid anxiety and depression. Further studiesshould be conducted to establish a relationship between alterationsin D2 receptor-induced neurotransmission and interictal psychiatricdisorders commonly occurring in patients with refractory epilepsyof longer duration (Briellmann et al., 2007; Hermann and Wyler,1989; Jackson and Turkington, 2005; Kanner and Balabanov, 2002).
Finally, we acknowledge that the number of surgically treated pa-tients involved in the present studywas not enough to obtain definitiveresults about the influence of dopaminergic systemon neuropsychiatricdisorders of patients with pharmacoresistant TLE. Another significantlimitation of the present study is that the impact of preoperative phar-macological treatment on alterations in the dopaminergic system couldnot be systematically assessed because of the high variability in antiepi-leptic medication (type and number of antiepileptic drugs, duration oftreatment, dosage, monotherapy, polytherapy, etc.) among patients. Inaddition, larger patient cohorts need to be evaluated to determinea) the impact of clinical factors on changes in the dopaminergic system,b) the relationship between dopaminergic alterations and surgical out-come, and c) if changes in the dopaminergic system represent the effector the cause of epilepsy. Finally, since dopamine could be important inthe comorbidity of epilepsy and neuropsychiatric disorders, furtherstudies are necessary to determine if dopaminergic abnormalities inthe brain of patients with TLE are bilateral.
616617618619620621622623624625626627
CORR
Acknowledgments
We thank Ms. Leticia Neri Bazan, Ms. Paula Vergara and Mr. HectorVazquez Espinosa for their excellent technical assistance and Dr. ErikaBrust Mascher for English improvement. This study was supported bythe National Council for Sciences and Technology of Mexico (grantsJ010.0170/2010 and 98386) andAcademy of Sciences of Hungary (grantsETT577/2006, RET67/2005).
628629630631632633634635636637638639640641642643644645646647648
UN
References
Bandyopadhyay, S., Hablitz, J.J., 2007. Dopaminergic modulation of local network activityin rat prefrontal cortex. J. Neurophysiol. 97, 4120–4128.
Barone, P., Palma, V., DeBartolomeis, A., Tedeschi, E., Muscettola, G., Campanella, G., 1991.Dopamine D1 and D2 receptors mediate opposite functions in seizures induced bylithium–pilocarpine. Eur. J. Pharmacol. 195, 157–162.
Bonci, A., Hopf, F.W., 2005. The dopamine D2 receptor: new surprises from an oldfriend. Neuron 47, 335–338.
Breuer, M.E., Groenink, L., Oosting, R.S., Buerger, E., Korte, M., Ferger, B., Olivier, B.,2009. Antidepressant effects of pramipexole, a dopamine D3/D2 receptor agonist,and 7-OH-DPAT, a dopamine D3 receptor agonist, in olfactory bulbectomizedrats. Eur. J. Pharmacol. 616, 134–140.
Briellmann, R.S., Hopwood, M.J., Jackson, G.D., 2007. Major depression in temporal lobeepilepsy with hippocampal sclerosis: clinical and imaging correlates. J. Neurol.Neurosurg. Psychiatry 78, 1226–1230.
Chagnac-Amitai, Y., Connors, B.W., 1989. Horizontal spread of synchronized activity inneocortex and its control by GABA-mediated inhibition. J. Neurophysiol. 61, 747–758.
Please cite this article as: Rocha, L., et al., Dopamine abnormalities in th(2011), doi:10.1016/j.nbd.2011.09.006
ED P
RO
OF
Chervin, R.D., Pierce, P.A., Connors, B.W., 1988. Periodicity and directionality in thepropagation of epileptiform discharges across neocortex. J. Neurophysiol. 60,1695–1713.
Clinckers, R., Smolders, I., Meurs, A., Ebinger, G., Michotte, Y., 2005. Hippocampal dopamineand serotonin elevations as pharmacodynamic markers for the anticonvulsant efficacyof oxcarbazepine and 10,11-dihydro-10-hydroxycarbamazepine. Neurosci. Lett. 390,48–53.
Del Sole, A., Chiesa, V., Lucignani, G., Vignoli, A., Giordano, L., Lecchi, M., Canevini, M.P.,2010. Exploring dopaminergic activity in ring chromosome 20 syndrome: a SPECTstudy 2010 Oct Q. J. Nucl. Med. Mol. Imaging 54 (5), 564–569.
During, M.J., Spencer, D.D., 1993. Extracellular hippocampal glutamate and spontaneousseizure in the conscious human brain. Lancet 341, 1607–1610.
Engel Jr., J., 1996. Introduction to temporal lobe epilepsy. Epilepsy Res. 26, 141–150.First, M.B., Spitzer, R.L., Gibbon, M., Williams, J.B.W., 1999. Entrevista clínica estructurada
para los trastornos del eje I del DSM-IV. Versión clínica (SCID-I). Masson, S.A,Barcelona.
Fisher, R.S., Leppik, I., 2008. Debate: when does a seizure imply epilepsy? Epilepsia 49(Suppl 9), 7–12.
Garcia-Tovar, C., Perez, A., Luna, J., Osorio, B., Aleman, V., Mondragon, R., Mornet, D.,Rendón, A., Hernandez, J.M., 2001. Biochemical and histochemical analysis of 71kDa dystrophin (dp 71f) in rat brain. Acta Histochem. 103, 209–224.
Gilmore, J.H., Lawler, C.P., Eaton, A.M.,Mailman, R.B., 1993. Postmortem stability of dopamineD1 receptor mRNA and D1 receptors. Mol. Brain Res. 18, 290–296.
Hennessy, M.J., Elwes, R.D., Honavar, M., Rabe-Hesketh, S., Binnie, C.D., Polkey, C.E.,2001. Predictors of outcome and pathological considerations in the surgical treat-ment of intractable epilepsy associated with temporal lobe lesions. J. Neurol. Neu-rosurg. Psychiatry 70, 450–458.
Hermann, B.P., Wyler, A.R., 1989. Depression, locus of control, and the effects of epilepsysurgery. Epilepsia 30, 332–338.
Huberfeld, G., Habert, M.O., Clemenceau, S., Maksud, P., Baulac, M., Adam, C., 2006. Ictalbrain hyperperfusion contralateral to seizure onset: the SPECTmirror image. Epilepsia47, 123–133.
Jackson, M.J., Turkington, D., 2005. Depression and anxiety in epilepsy. J. Neurol. Neurosurg.Psychiatry 76 (Suppl. 1), i45–i47.
Kanner, A.M., 2011. Depression and epilepsy: a bidirectional relation? Epilepsia 52(Suppl. 1), 21–27.
Kanner, A.M., Balabanov, A., 2002. Depression and epilepsy: how closely related arethey? Neurology 58 (Suppl. 5), S27–S39.
Kumlien, E., Bergström,M., Lilja, A., Andersson, J., Szekeres, V.,Westerberg, C.E., Antoni, G.,Långström, B., 1995. Positron emission tomographywith [11C]deuterium-deprenyl intemporal lobe epilepsy. Epilepsia 36, 712–721.
Lehto, S.M., Kuikka, J., Tolmunen, T., Hintikka, J., Viinamäki, H., Vanninen, R., Haatainen,K., Koivumaa-Honkanen, H., Honkalampi, K., Tiihonen, J., 2008. Temporal cortexdopamine D2/3 receptor binding in major depression. Psychiatry Clin. Neurosci.62, 345–348.
Lopez-Gomez, M., Espinola, M., Ramirez-Bermudez, J., Martinez-Juarez, I.E., Sosa, A.L.,2008. Clinical presentation of anxiety among patients with epilepsy. Neuropsychiatr.Dis. Treat. 4, 1235–1239.
Louw, D., Sutherland, G.R., Glavin, G.B., Girvin, J., 1989. A study of monoaminemetabolismin human epilepsy. Can. J. Neurol. Sci. 16, 394–397.
Lowry, O.H., Rosenbrough, N.J., Farr, R.J., Randall, R.J., 1951. Protein measurement withthe Folin phenol reagent. J. Biol. Chem. 193, 265–273.
Luna-Munguia, H., Orozco-Suarez, S., Rocha, L., 2011. Effects of high frequency electricalstimulation and R-verapamil on seizure susceptibility and glutamate and GABA releasein a model of phenytoin-resistant seizures. Neuropharmacol. 61, 807–814.
Meurs, A., Clinckers, R., Ebinger, G., Michotte, Y., Smolders, I., 2008. Seizure activity andchanges in hippocampal extracellular glutamate, GABA, dopamine and serotonin.Epilepsy Res. 78, 50–59.
Mori, A., Hiramatsu, M., Namba, S., Nishimoto, A., Ohmoto, T., Mayanagi, Y., Asakura, T.,1987. Decreased dopamine level in the epileptic focus. Res. Commun. Chem.Pathol. Pharmacol. 56, 157–164.
Morrell, F., Wada, J., Engel Jr., J., 1987. Appendix 111: potential relevance of kindling andsecondary epileptogenesis to the consideration of surgical treatment for epilepsy.In: Engel Jr., J. (Ed.), Surgical treatment of the epilepsies. Raven Press, New York, pp.701–707.
Morris, E.D., Yoder, K.K., 2007. Positron emission tomography displacement sensitivity:predicting binding potential change for positron emission tomography tracersbased on their kinetic characteristics. J. Cereb. Blood Flow Metab. 27, 606–617.
Murakami, T., Okada,M., Kawata, Y., Zhu, G., Kamata, A., Kaneko, S., 2001. Determination ofeffects of antiepileptic drugs on SNAREs-mediated hippocampal monoamine releaseusing in vivo microdialysis. Br. J. Pharmacol. 134, 507–520.
Nyberg, P.,Winblad, B., Carlsson, A., 1982.Monoamine concentrations in the human brain.A comparison between two methods of tissue handling. J. Neural Transm. 54, 85–90.
Okada, M., Kawata, Y., Kiryu, K., Mizuno, K., Wada, K., Inomata, H., Tasaki, H., Kaneko, S.,1997. Effects of non-toxic and toxic concentrations of phenytoin on monoamineslevels in rat brain. Epilepsy Res. 28, 155–163.
Olsen, R.W., Avoli, M., 1997. GABA and epileptogenesis. Epilepsia 38, 399–407.Pacia, S.V., Doyle, W.K., Broderick, P.A., 2001. Biogenic amines in the human neocortex
in patients with neocortical and mesial temporal lobe epilepsy: identification within situ microvoltammetry. Brain Res. 899, 106–111.
Perez-Severiano, F., Escalante, B., Vergara, P., Ríos, C., Segovia, J., 2002. Age-dependentchanges in nitric oxide synthase and proteína expresión in striata of mice transgenicfor the Huntington's disease mutation. Brain Res. 951, 36–42.
Pintor, M., Mefford, I.N., Hutter, I., Pocotte, S.L., Wyler, A.R., Nadi, N.S., 1990. Levels ofbiogenic amines, their metabolites, and tyrosine hydroxylase activity in thehuman epileptic temporal cortex. Synapse 5, 152–156.
e neocortex of patients with temporal lobe epilepsy, Neurobiol. Dis.

649650651652653654655656657658659660661662663664665666667668669670
671672673674675676677678679680681682683684685686687688689690691692
694
9L. Rocha et al. / Neurobiology of Disease xxx (2011) xxx–xxx
Rodin, E.A., 1968. ThePrognosis of Patientswith Epilepsy. Charles C Thomas, Springfield, ILL.Sander, T., Berlin, W., Ostapowicz, A., Samochowiec, J., Gscheidel, N., Hoehe, M.R.,
2000. Variation of the genes encoding the human glutamate EAAT2, serotoninand dopamine transporters and susceptibility to idiopathic generalized epilepsy.Epilepsy Res. 41, 75–81.
Sarantis, K., Matsokis, N., Angelatou, F., 2009. Synergistic interactions of dopamine D1 andglutamateNMDA receptors in rat hippocampus and prefrontal cortex: involvement ofERK1/2 signaling. Neuroscience 163, 1135–1145.
Sarkisova, K.Y., Kulikov, M.A., Midzyanovskaya, I.S., Folomkina, A.A., 2008. Dopamine-dependent nature of depression-like behavior in WAG/Rij rats with genetic ab-sence epilepsy. Neurosci. Behav. Physiol. 38, 119–128.
Scott, L., Aperia, A., 2009. Interaction between N-methyl-D-aspartic acid receptors and D1dopamine receptors: an important mechanism for brain plasticity. Neuroscience 158,62–66.
Sim, L.J., Childers, S.R., 1997. Anatomical distribution of mu, delta, and kappa opioid- andnociceptin/orphanin FQ-stimulated [35S]guanylyl-5′-O-(gamma-thio)-triphosphatebinding in guinea pig brain. J. Comp. Neurol. 386, 562–572.
Sim, L.J., Selley, D.E., Dworkin, S.I., Childers, S.R., 1996. Effects of chronic morphine ad-ministration on mu opioid receptor-stimulated [35S]GTPgammaS autoradiographyin rat brain. J. Neurosci. 16, 2684–2692.
Sloviter, R.S., 1994. The functional organization of the hippocampal dentate gyrus and itsrelevance to the pathogenesis of temporal lobe epilepsy. Ann. Neurol. 35, 640–654.
UNCO
RRECT
693
Please cite this article as: Rocha, L., et al., Dopamine abnormalities in th(2011), doi:10.1016/j.nbd.2011.09.006
F
Staley, J.K., Boja, J.W., Carroll, F.I., Seltzman, H.H., Wyrick, C.D., Lewin, A.H.,Abraham, P., Mash, D.C., 1995. Mapping dopamine transporters in thehuman brain with novel selective cocaine analog [125I] RTI-121. Synapse 21,364–372.
Tae, W.S., Joo, E.Y., Kim, J.H., Han, S.J., Suh, Y.L., Kim, B.T., Hong, S.C., Hong, S.B., 2005.Cerebral perfusion changes in mesial temporal lobe epilepsy: SPM analysis ofictal and interictal SPECT. NeuroImage 24, 101–110.
Tupala, E., Halonen, P., Tiihonen, J., 2006. Visualization of the cortical dopamine trans-porter in type 1 and 2 alcoholics with human whole hemisphere autoradiography.Eur. Neuropsychopharmacol. 16, 552–560.
Werhahn, K.J., Landvogt, C., Klimpe, S., Buchholz, H.G., Yakushev, I., Siessmeier, T., Müller-Forell, W., Piel, M., Rösch, F., Glaser, M., Schreckenberger, M., Bartenstein, P., 2006.Decreased dopamine D2/D3-receptor binding in temporal lobe epilepsy: an [18F]fallypride PET study. Epilepsia 47, 1392–1396.
Wolf, M.E., LeWitt, P.A., Bannon, M.J., Dragovic, L.J., Kapatos, G., 1991. Effect of aging ontyrosine hydroxylase protein content and the relative number of dopamine nerveterminals in human caudate. J. Neurochem. 56, 1191–1200.
Wu, J., Hablitz, J.J., 2005. Cooperative activation of D1 andD2dopamine receptors enhances ahyperpolarization-activated inward current in layer I interneurons. J. Neurosci. 25,6322–6328.
Zelnik, N., Angel, I., Paul, S.M., Kleinman, J.E., 1986. Decreased density of human striataldopamine uptake sites with age. Eur. J. Pharmacol. 126, 175–176.
O
ED P
RO
e neocortex of patients with temporal lobe epilepsy, Neurobiol. Dis.
Related Documents