Ventilator Induced Lung Injury Ventilator Induced Lung Injury Ventilator Strategies Ventilator Strategies Pathophysiology Matters Pathophysiology Matters Donald M. Null, Jr., MD Donald M. Null, Jr., MD Donald M. Null, Jr., MD • I am a consultant for Draeger Medical Company I am a consultant for Draeger Medical Company

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Ventilator Induced Lung InjuryVentilator Induced Lung InjuryVentilator Strategies Ventilator Strategies
Pathophysiology MattersPathophysiology Matters
Donald M. Null, Jr., MD
Donald M. Null, Jr., MDDonald M. Null, Jr., MD
•• I am a consultant for Draeger Medical CompanyI am a consultant for Draeger Medical Company

Factors which predispose Factors which predispose immature lung to injuryimmature lung to injury
• Surfactant deficiency– Poor saccular compliance– Diffuse atelectasis
• Compliant tracheobronchial tree• Increased surface tension• Marked V/Q mismatch
Factors which predispose Factors which predispose immature lung to injury immature lung to injury
(continued)(continued)
• An increased Vd/Vt• An apparent predilection to edema formation• Decreased tissue antioxidants• Presence of a patent ductus arteriosus
Barotrauma/VolutraumaBarotrauma/VolutraumaBiotrauma Biotrauma
• Distal airway rather than primitive alveolus is the most compliant part of the respiratory tract
• Distal airway disruption– Interstitial emphysema– Pneumothorax– Pneumomediastinum– Pneumopericardium
Barotrauma Barotrauma (continued)(continued)
• Interstitial space
– Larger than an adult– More distensible– PIE worsens compliance

Barotrauma Barotrauma (continued)(continued)
• Distal airway overdistention
– Protein leak– Edema– Hyaline membrane formation
Ventilator Associated Lung Injury
• PIP
• Volume
Hernandez et. al.
Dreyfus et. al.
Carlton et. al.

Oxygen Injury
• Oxygen is toxic to all tissues
• Lack of antioxidant protection
• O2 injury perpetuates alveolar noncompliance
BiotraumaBiotrauma
EpigeneticsEpigenetics
Goals of Respiratory SupportGoals of Respiratory Support
•• Achieve uniform inflationAchieve uniform inflation•• Minimize over and under inflationMinimize over and under inflation•• Minimize inspired oxygen concentrationMinimize inspired oxygen concentration•• Early appropriate extubation Early appropriate extubation
Lung RecruitmentLung Recruitment•• Increase Mean Airway PressureIncrease Mean Airway Pressure
•• Increase PEEPIncrease PEEP•• Increase Inspiratory TimeIncrease Inspiratory Time•• Increase Ventilator RateIncrease Ventilator Rate•• Increase Peak Inspiratory PressureIncrease Peak Inspiratory Pressure•• Increase Tidal VolumeIncrease Tidal Volume

VentilationVentilation•• Increase PressureIncrease Pressure•• Increase VolumeIncrease Volume•• Increase RateIncrease Rate•• Decrease overexpansionDecrease overexpansion•• Improve underexpansionImprove underexpansion
Synchronized Assisted Synchronized Assisted Ventilation in Infants Ventilation in Infants (SAVI,SIMV and AC)(SAVI,SIMV and AC)
Theoretical Advantages•• Decreased barotraumaDecreased barotrauma
–– AirleakAirleak–– BPDBPD
• Decreased ventilator time• Decreased intraventricular hemorrhage• Consistent tidal volume delivery

Volume VentilationVolume VentilationTheoretical AdvantagesTheoretical Advantages
– Stabilization of lung volume
– Improved ventilation - perfusion
– Stabilization of cerebral blood flow
– Decreased air leaks
VGPS and VAPSVGPS and VAPS
Theoretical AdvantagesTheoretical Advantages
– Stabilization of lung volume– Improved ventilation - perfusion– Stabilization of cerebral blood flow– Decreased air leaks– Weaning

MMVMMV
High Frequency Types High Frequency Types and Differencesand Differences
–– High frequency positive pressure ventilationHigh frequency positive pressure ventilation–– High frequency flow interruption ventilationHigh frequency flow interruption ventilation–– High frequency jet ventilationHigh frequency jet ventilation–– High frequency oscillatory ventilationHigh frequency oscillatory ventilation

Pressure TransmissionPressure Transmission

Ventilation Ventilation --Conventional vs High FrequencyConventional vs High Frequency
CV CV -- V = (TVV = (TV--DV) x FDV) x FV = AV x FV = AV x F
HF HF -- V = TVV = TV22 x Fx F
OxygenationOxygenation
–– Mean airway pressureMean airway pressure
–– Delta pressure (tidal volume)Delta pressure (tidal volume)
–– FrequencyFrequency

Pathophysiology and Pathophysiology and Ventilator StrategiesVentilator Strategies
Diffuse Alveolar Disease Diffuse Alveolar Disease -- Need complete recruitmentNeed complete recruitment

Mechanisms to Mechanisms to Achieve RecruitmentAchieve Recruitment
1. Surfactanta. Delivery technique
2. Adequate mean and end expiratory pressure to prevent collapse
Mechanisms to Mechanisms to Achieve RecruitmentAchieve Recruitment
3. Recruitment maneuversa. Sighb. Inspiratory time
4. Adequate target volume

MistakesMistakes
1. Inappropriate pressure changes PIP, PAW, PEEP
2. Use of high FiO2 to treat intrapulmonary shunts
MistakesMistakes
3. Distensability of airways with effecton tidal volumes
4. Inappropriate ventilator rates that predispose to airtrapping

MistakesMistakes
5. Mucus plugging not appropriatelyaddressed

Meconium AspirationMeconium Aspiration
1. Diffuse Disease
2. Patchy – Overdistention/Atelectasis

StrategiesStrategies
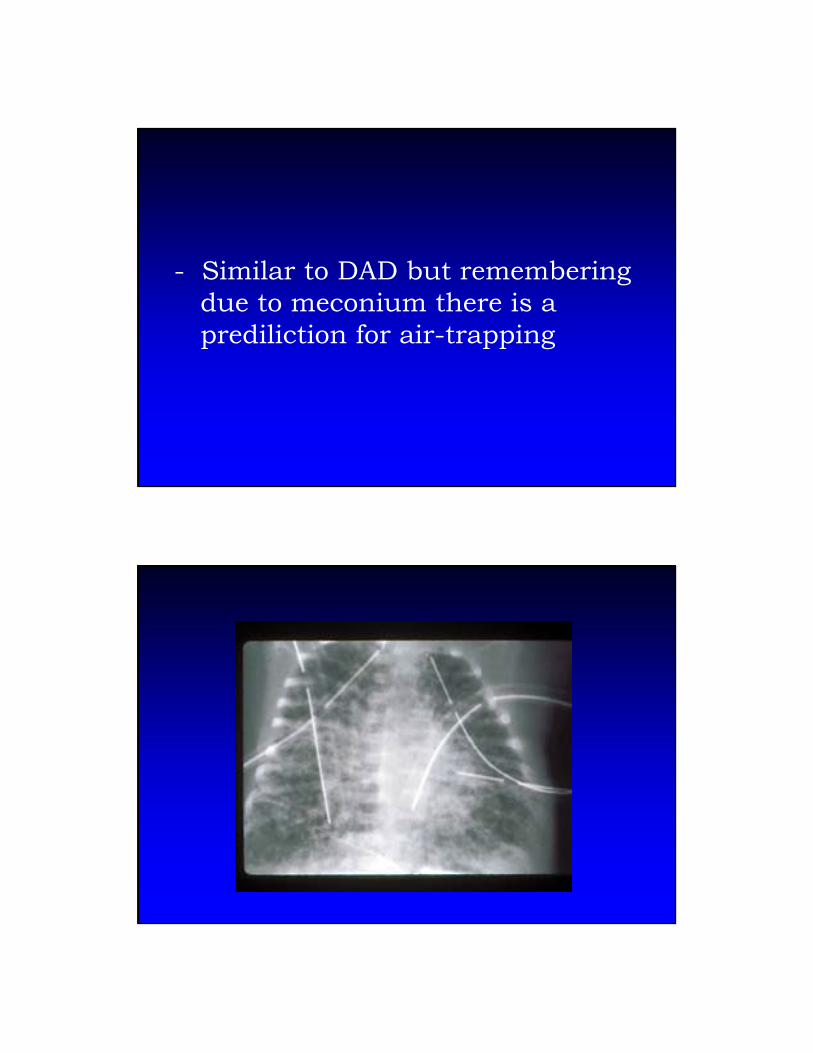
- Similar to DAD but rememberingdue to meconium there is a prediliction for air-trapping
- Goal is to minimize overdistentionand air-trapping. Recruitment of atelectatic areas as possible.
Basic StrategyBasic Strategy
•• Lower rates for HF or conventional Lower rates for HF or conventional yielding longer expiratory timesyielding longer expiratory times
•• Larger tidal volumes for HF or Larger tidal volumes for HF or conventionalconventional
•• Surfactant usageSurfactant usage

MistakesMistakes
- Too small tidal volumes- Too rapid rates- Preconceived appropriate tidal
volume
MistakesMistakes
Failure to deal with cardiac issuesPPHN

Pulmonary HypoplasiaPulmonary Hypoplasia
Bilateral/DiffuseBilateral/Diffuse
- Maintain adequate inflation
- Avoid overexpansion
- Surfactant treatment
- Pulmonary hypertension
UnilateralUnilateral
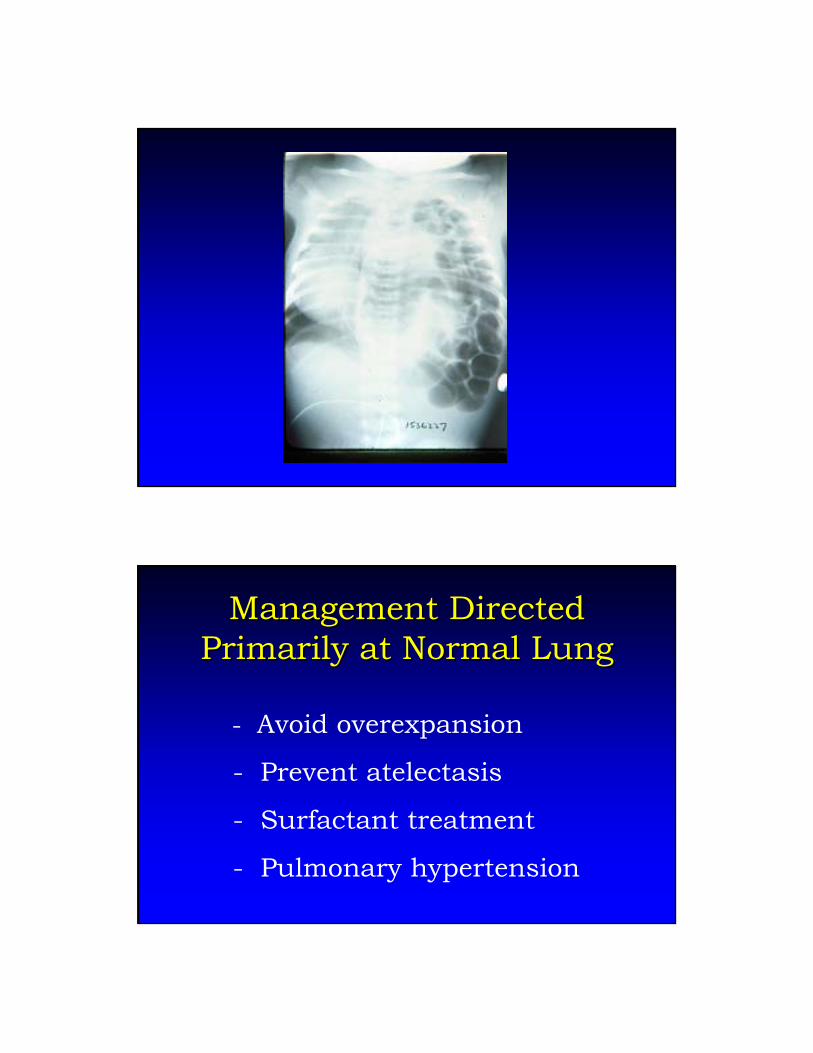
Management Directed Management Directed Primarily at Normal LungPrimarily at Normal Lung
- Avoid overexpansion
- Prevent atelectasis
- Surfactant treatment
- Pulmonary hypertension

MistakesMistakes
1. Using too large tidal volume
2. Failure to address cardiac/pulmonary hypertension issues
3. Adequate expansion misinterpreted on x-ray
MistakesMistakes
1. Rib counting
2. Tidal volume

SevereSevereAir LeakAir Leak
StrategiesStrategies
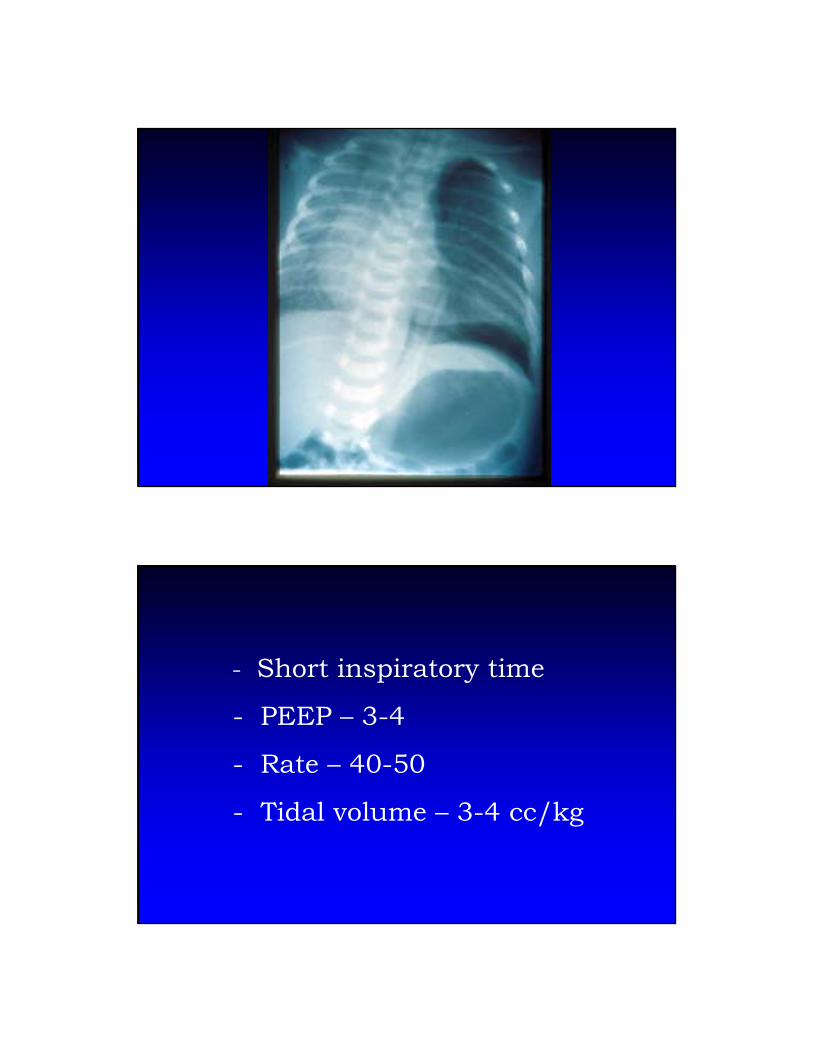
Premature PIE

- Short inspiratory time
- PEEP – Adequate to keepairways open
- Rate 40-50
- Tidal volume – 3-4 cc/kg

HFVHFV
•• Paw 1 cm HPaw 1 cm H220 < CV0 < CV•• Frequency 10Frequency 10--15 Hz15 Hz•• Delta pressure Delta pressure –– minimal chest minimal chest
wall movementwall movement
Gross Air LeakGross Air LeakAdequate InflationAdequate Inflation
- Short inspiratory time
- PEEP – 3-4
- Rate – 40-50
- Tidal volume – 3-4 cc/kg

HFVHFV
–– Gross Air LeakGross Air Leak•• Paw = or 1 cm HPaw = or 1 cm H220 > CV0 > CV•• Frequency 10Frequency 10--15 Hz15 Hz•• Delta pressure Delta pressure –– chest wall movementchest wall movement
Gross Air LeakGross Air LeakGenerally Poor InflationGenerally Poor Inflation

- Inspiratory time – .35-.4
- PEEP – 5-7
- Rate – 40
- Tidal volume – 5-6 cc/kg

HFVHFV
–– Gross air leak, generally poor inflationGross air leak, generally poor inflation•• Paw 1Paw 1--2 cm H2 cm H220 > CV0 > CV•• Frequency 10 HzFrequency 10 Hz•• Delta pressureDelta pressure--chest wall movementchest wall movement
SummarySummary
The enemy of good is better

- Applying ventilatory support in the least traumatic way is best accomplished by applying the support over the mid-portion of the pressure volume curve.

Issues with VentilationIssues with Ventilation
• A 5 cc/kg tidal volume does not insure prevention of over-expansion or injury
• A 10 cc/kg tidal volume does not insure over- expansion and injury
Issues with Ventilation Issues with Ventilation (continued)(continued)
• Weaning which results in keeping the lung on the lower portion of the PV curve will injure the lung not protect it

- The lung is most vulnerable to injury during recruitment
One must tailor ventilator One must tailor ventilator strategies to match strategies to match cardiopulmonary pathophysiologycardiopulmonary pathophysiology

Remember:Remember:Cookbooks are good butCookbooks are good butpatients are individualspatients are individuals
QuestionsQuestions
Related Documents











