RESEARCH ARTICLE Open Access Does improvement towards a normal cervical sagittal configuration aid in the management of cervical myofascial pain syndrome: a 1- year randomized controlled trial Ibrahim M. Moustafa 1,2* , Aliaa A. Diab 2 , Fatma Hegazy 1 and Deed E. Harrison 3 Abstract Background: There is a growing interest concerning the understanding of and rehabilitation of the sagittal configuration of the cervical spine as a clinical outcome. However, the literature on the topic specific to conservative treatment outcomes of patients with chronic myofascial cervical pain syndrome (CMCPS) has not adequately addressed the relationship between cervical sagittal alignment and improved pain, disability and range of motion. Methods: A randomized controlled study with a 1-year follow-up. Here, 120 (76 males) patients with chronic CMCPS and defined cervical sagittal posture abnormalities were randomly assigned to the control or an intervention group. Both groups received the Integrated neuromuscular inhibition technique (INIT); additionally, the intervention group received the denneroll cervical traction device. Alignment outcomes included two measures of sagittal posture: cervical angle (CV), and shoulder angle (SH). Patient relevant outcome measures included: neck pain intensity (NRS), neck disability (NDI), pressure pain thresholds (PPT), cervical range of motion using the CROM. Measures were assessed at three intervals: baseline, 10 weeks, and 1 year after the 10 week follow up. Results: After 10 weeks of treatment, between group statistical analysis, showed equal improvements for both the intervention and control groups in NRS (p = 0.36) and NDI (p = 0.09). However, at 10 weeks, there were significant differences between groups favoring the intervention group for PPT (p<0.001) and all measures of CROM (p<0.001). Additionally, at 10 weeks the sagittal alignment variables showed significant differences favoring the intervention group for CV p<0.001 and SH (p<0.001) indicating improved CSA. Importantly, at the 1-year follow-up, between group analysis identified a regression back to baseline values for the control group for the non-significant group differences (NRS and NDI) at the 10-week mark. Thus, all variables were significantly different between groups favoring the intervention group at 1-year follow up: NRS (p<0.001), NDI (p<0.001), PPT p<0.001), CROM (p<0.001), CV (p<0.001), SH (p<0.001). (Continued on next page) * Correspondence: [email protected]; [email protected] 1 Department of Physiotherapy, College of Health Sciences, University of Sharjah, Sharjah, United Arab Emirates 2 Basic Science Department, Faculty of Physical Therapy, Cairo University, 7 Mohamed Hassan El gamal Street-Abbas El Akaad, Nacer City, Egypt Full list of author information is available at the end of the article © The Author(s). 2018 Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated. Moustafa et al. BMC Musculoskeletal Disorders (2018) 19:396 https://doi.org/10.1186/s12891-018-2317-y

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
-
RESEARCH ARTICLE Open Access
Does improvement towards a normalcervical sagittal configuration aid in themanagement of cervical myofascial painsyndrome: a 1- year randomized controlledtrialIbrahim M. Moustafa1,2* , Aliaa A. Diab2, Fatma Hegazy1 and Deed E. Harrison3
Abstract
Background: There is a growing interest concerning the understanding of and rehabilitation of the sagittalconfiguration of the cervical spine as a clinical outcome. However, the literature on the topic specific toconservative treatment outcomes of patients with chronic myofascial cervical pain syndrome (CMCPS) has notadequately addressed the relationship between cervical sagittal alignment and improved pain, disability and rangeof motion.
Methods: A randomized controlled study with a 1-year follow-up. Here, 120 (76 males) patients with chronic CMCPSand defined cervical sagittal posture abnormalities were randomly assigned to the control or an intervention group.Both groups received the Integrated neuromuscular inhibition technique (INIT); additionally, the intervention groupreceived the denneroll cervical traction device. Alignment outcomes included two measures of sagittal posture: cervicalangle (CV), and shoulder angle (SH). Patient relevant outcome measures included: neck pain intensity (NRS), neckdisability (NDI), pressure pain thresholds (PPT), cervical range of motion using the CROM. Measures were assessed atthree intervals: baseline, 10 weeks, and 1 year after the 10 week follow up.
Results: After 10 weeks of treatment, between group statistical analysis, showed equal improvements for both theintervention and control groups in NRS (p = 0.36) and NDI (p = 0.09). However, at 10 weeks, there were significantdifferences between groups favoring the intervention group for PPT (p
-
(Continued from previous page)
Conclusion: The addition of the denneroll cervical orthotic to a multimodal program positively affected CMCPSoutcomes at long term follow up. We speculate the improved sagittal cervical posture alignment outcomes contributedto our findings.
Trial registration: Pan African Clinical Trial Registry Clinical Trial Registry: PACTR201801002968301, registered 11 January2018 (retrospectively registered).
Keywords: Randomized controlled trial, Cervical lordosis, Cervical posture, Cervical pain, Myofascial pain, Traction
BackgroundChronic myofascial pain syndrome (CMPS) is a muscu-loskeletal condition or syndrome that is typically associ-ated myofascial trigger points (MTrP). CMPS has alifetime prevalence of up to 85% with variations as lowas 15% for a point prevalence [1, 2]. CMPS significantlyimpacts a patient’s health related quality of life outcomeswith studies including: disability, financial status, depres-sion, anxiety, and generalized neck pain [3, 4].Myofascial pain syndrome remains one of the most
common sources of pain in chronic non-specific neckpain. Factors commonly cited as predisposing to MPSamong subjects with chronic non-specific neck paininclude abnormal postural, inadequate rest, overstretch-ing, over-shortening or more generally, repetitive mechan-ical stress [1, 2]. In clinical practice, different approachessuch as massage, acupuncture and electro-thermotherapyare quite commonly used in the treatment of CMPS [3, 4].However, the effectiveness of many of these approachesdid not appear to be superior to placebo [3]. A recent sys-tematic review found that functional exercise protocolshave very low quality evidence for a positive small-to-moderate effect on pain intensity in patients sufferingfrom MPS [5].Identification of causative variables for MTrPs is a first
step to prevent development and secondarily to developpotential treatments preventing recurrence. Althoughthe exact mechanisms are still unknown, [6, 7] it is ac-cepted that mechanical factors are thought to be factorsassociated in the development of MTrPs [1, 2, 8]. In thisregard, various studies have confirmed that prolongedabnormal postures have been regarded as one of thecauses of MPS [9, 10].In the cervical region, various studies point to the fact
that altered sagittal plane alignment of the cervical spinesuch as straightened, s-curves, reversed curves, andanterior head translation can result in abnormal stressesand strains leading to premature and acceleration ofdegenerative changes in the muscles, ligaments, bonystructures and neural elements [11–13]. Furthermore,preliminary randomized trials have demonstrated improvedneck pain, dizziness, disability, positioning sense, flexion /extension kinematics, arm pain, and somatosensory evokedpotentials in patient groups receiving devices aimed at
restoration of the cervical curve and posture [14–17]. Onesuch device for the rehabilitation of sagittal cervicalalignment is the cervical denneroll spine orthotic out ofSydney, Australia. Two previous clinical trials have dem-onstrated the denneroll is a reliably placed three-pointbending extension traction device that is relatively easy touse by both the patient and treating therapist, and it iseffective at improving cervical lordosis (10°-14° improve-ment) and reducing anterior head translation (10-25 mmreduction) [15, 16].Although the previously mentioned studies make a sig-
nificant contribution to understanding the important roleof a normal cervical lordotic curve and rehabilitation toolsto enhance correction, the literature on the topic specificto conservative treatment outcomes of patients with MPShas not adequately addressed the relationship betweencervical sagittal alignment and improved pain and disabil-ity at short and at long term follow up.Accordingly, the present randomized controlled trial
was undertaken to investigate the functional and painresponse outcomes of denneroll cervical extension trac-tion compared to standard care in patient cases withchronic MPS, with a verified hypo-lordosis and anteriortranslation of the cervical spine. Two primary hypoth-eses were tested: 1) that denneroll cervical traction willimprove the sagittal alignment of the cervical spine. 2)The secondary hypothesis tested was whether restor-ation of normal cervical sagittal alignment will improveboth short and long-term outcomes in cervical myofas-cial pain syndrome patients.
MethodsPatientsA prospective, investigator-blinded, parallel-group, random-ized clinical trial was conducted at one of our university’sresearch departments, the trial was registered with the Clin-ical Trial Registry PACTR201801002968301. Cairo univer-sity institutional review board approval was obtained priorto the study and all subjects were recruited from our insti-tutions local outpatient clinic. Patients with cervical MPSwere recruited from our university’s rehabilitation clinic.Patients were recruited and treated from March 2016 toOctober 2017 including a 1-year of follow-up.
Moustafa et al. BMC Musculoskeletal Disorders (2018) 19:396 Page 2 of 13
https://pactr.samrc.ac.za/TrialDisplay.aspx?TrialID=2968
-
Participants were screened prior to inclusion for alter-ations in two primary cervical alignment variables: lossof the cervical lordosis and anterior head translation. Aspart of our University’s IRB approved protocol, each par-ticipant was only to receive initial cervical spine radiog-raphy (with no follow up spine radiography) because aprimary goal of the cervical denneroll orthotic is to re-store the cervical lordosis, thus participants were neces-sarily screened for hypo-lordosis. Participants wereincluded if their cervical lordosis was less than 25° asmeasured using the intersection of two lines drawnalong the posterior body margins of C2 and C7 [12]. Ini-tial cervical radiological assessment was important toidentify the cervical curve apex to determine where asubject should properly place the apex of the dennerollin their cervical spine [16, 18].Concerning anterior head translation, the participant
had to have significant anterior head translation as mea-sured by the craniovertebral angle (CVA). If the CVA wasless than 50°, then a participant was referred to the study.Our selection of 50° as a reference angle was guided bythe study of Yib et al. [19]. Consecutive patients were in-cluded if they had active, palpable MTrPs on a single sideor both sides of the upper trapezius muscle. Diagnosis wasmade according to Travell and Simons’ criteria, wherebyfive major and at least one minor criteria are required forclinical diagnosis [20]. The major criteria are (1) localizedneck pain; (2) pain or altered sensations in expected re-ferred pain area for given trigger point; (3) taut bandwithin the muscle; (4) exquisite tenderness in a pointalong taut band; (5) restricted range of motion. The minordiagnostic criteria for MPS are (1) reproduction of thepatient’s chief pain complaint by manual pressure onMTrP nodule; (2) a local twitch response; and (3) painrelief obtained by muscular treatment. Participants wereexcluded if any signs or symptoms of medical “red flags”were present: tumor, fracture, rheumatoid arthritis, osteo-porosis, and prolonged steroid use. Additionally, subjectswere excluded with previous spine surgery and any examfindings consistent with neurological diseases and vasculardisorders.An independent research assistant performed a concealed
permuted block randomization using a computer-generatedrandomization schedule with a random block size.
RandomizationOur study design randomly assigned eligible participantsto 1 of 2 groups: an intervention group (n = 60) or controlgroup (n = 60). Examiner blinding was obtained throughan independent research assist; not knowing the study de-sign and not specifically involved in any aspect of the trial.This research assistant created a concealed permutedblock randomization for subject group allocation; where
equal numbers were placed in each group using a per-muted block design of different sizes.
Treatment methodsBoth the control group and the intervention groups re-ceived the treatment interventions including: Integratedneuromuscular inhibition technique (INIT), IschemicCompression, Strain Counterstrain (SCS), and muscleenergy technique (MET). Additionally, the participantsin the intervention group received the denneroll cervicaltraction. The control group was treated also with a pla-cebo treatment using a small cervical towel applied inthe supine position located in the mid cervical spine asan intervention to mimic the denneroll traction time;but without applying significant extension bending ofthe cervical spine.Following 30 sessions, participants were re-evaluated a
minimum of 24 h after their last session and then eachsubject was again followed for an additional 1-year timeframe with no supervised treatment. The treating ther-apist (F.H), for both the control and intervention groups,was un-blinded to the treatment method but the sub-jects and assessor (A.I.M.M. and A.A.D.) who conductedthe measurements were blinded.
Denneroll extension traction for the intervention groupThe participants in the intervention group additionallyreceived the denneroll cervical extension traction (Den-neroll Industries, Sydney Australia; http://www.denner-oll.com) following previously published protocols [18,21]. The patients were instructed to lie supine and keeptheir legs extended. Based on the apex of each partici-pant’s cervical curvature on the initial radiograph, thetherapist positioned the apex of the denneroll in one oftwo regions (mid cervical placement or lower cervicalplacement). The duration of the traction session startedat 2–3 min and increased 1 min per session until reach-ing the goal of 20 min, the traction was repeated threetimes per week for 10 weeks. See Fig. 1.
Integrated neuromuscular inhibition technique (INIT)The treating therapist first identified the TrPs to betreated within the upper trapezius muscle. The practi-tioner evaluated the fibers of the upper trapezius, mak-ing note of any active TrPs, by firmly pinching using thethumb and the forefinger. Ischemic compression wasapplied by placing the thumb and index finger over theactive TrP. The therapist applied slow, increasing levelsof sustained pressure to the area until a relaxation of thetissue barrier was felt. Following a release of pressure,the therapist again applied increased pressure until anew barrier was felt. This process was repeated until thepatient indicated the area was no longer tender or until90 s had elapsed; whichever came first. All identified
Moustafa et al. BMC Musculoskeletal Disorders (2018) 19:396 Page 3 of 13
http://www.denneroll.comhttp://www.denneroll.com
-
TrPs were treated in the above manner per generally ac-cepted methodology reported in the literature [6–8].
Ischemic compression and strain Counterstrain (SCS)Here, moderate pressure was applied by the therapist tothe identified MTrP while each patient rated their levelof pain on a scale from 1 to 10. Once the patient’s painwas reproduced, the therapist maintained pressure overthe active MTrP and located a position that eased thepatient’s perception of pain. This position of ease wasgenerally identified as positioning the affected muscle ina shortened/relaxed state; where a reduction in pain in-tensity of 70% was indicated by the patient. Once identi-fied, the position of ease was held for 20–30 s and thiswas repeated for three to five repetitions by the therap-ist; similar to other generally accepted methodology re-ported in the literature [6–8].
Muscle energy technique (MET)Following SCS, the participants received MET applied tothe affected upper trapezius. Here, an isometric contrac-tion was held for 7–10 s and was followed by furthercervical spine contralateral side bending, flexion, and ip-silateral rotation to maintain and increase the soft tissuestretch as the muscle belly relaxes. The MET stretchposition was repeated three to five times per treatmentsession and was maintained for 30 s. This protocol issimilar to other generally accepted methodology re-ported in the literature [6–8].All the participant received the treatment by the same
physiotherapist, who had 15 years of experience in man-ual therapy.
Home exercise protocolParticipants were advised to perform a home exercise pro-gram once daily. The program included strengthening
exercises for scapular retractors, deep cervical flexors, andneck extensors. This protocol has been previously re-ported [18, 21]. The participants were instructed to prac-tice the same home exercise program at least twice a weekduring the 1 year follow up period. During the follow upperiod, participants were followed up by telephone inter-views every 3 months.
Outcome measuresThe participants underwent a series of assessments atthree time intervals: prior to treatment, after 10 weeksof intensive treatment, and at 1 year of follow-up. Theorder of measurements was the same for all participants.
Primary outcome measure
� The Neck Disability Index (NDI), consisting of 10items related to daily living activities, was ourprimary patient-reported outcome measure. Thereliability, construct validity, and responsiveness tochange of the NDI have all been assessed [18, 21].
Secondary outcome measures
� Cervical sagittal alignment, neck pain on anumerical rating scale, cervical ROM and painpressure thresholds via an algometric score weresecondary outcome measures.
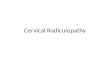
Postural cervical sagittal alignmentStanding cervical and shoulder posture was measuredwith photogrammetry, which provide valid and reliableindicators of the spine [16]. Two angles of measurementwere used cervical angle (CV), and shoulder angle (SH)(Fig. 2) - and obtained in the sagittal view as follows:
Cervical angle - The cervical angle is highly reliable toassess forward head translation [17]. It is defined as theangle between the true horizontal line through thespinous process of C7 and a line connecting spinousprocess of C7 with the tragus. In this study, if the anglewas less than 50°, the participant was considered tohave forward head posture; where subjects with FHPhave a significantly smaller CV when compared withnormal subjects [22].Shoulder angle - A line was drawn between themidpoint of the humerus and spinous process of C7,and the angle of this line to the horizontal line throughthe midpoint of the humerus was calculated in degrees.In the present study, we considered 52° as the referenceangle based on Brink et al. [23].
Pain intensity Neck pain intensity was measured usingthe numerical pain rating scale (NPRS) [24]. The patients
Fig. 1 Denneroll cervical spine extension traction. ©Copyright CBPSeminars, reprinted with permission
Moustafa et al. BMC Musculoskeletal Disorders (2018) 19:396 Page 4 of 13
-
were asked to place a mark along the line indicating theircurrent pain intensity; 0 reflecting “no pain” and 10reflecting the “worst pain”.
Pressure-pain threshold (PPT) algometric measurementA pressure threshold algometer (Lutron electronic,FG5005, RS232) was used to measure PPT in the mosttender point (MTP) of the upper trapezius muscle beforeand after treatment. The average value of 3 repetitivemeasurements with an interval of 30 to 60 s (expressedas kilograms per square centimeter) was taken for dataanalysis of the PPT [25].
Cervical ROMCervical spine global range-of-motion was measuredusing the valid and reliable cervical range-of-motion(CROM) device [26]. The participant was instructed toperform flexion, extension, right/left lateral flexion,right/left rotation in upright sitting. The patient wasinstructed to perform each movement when he/sheattained the maximum active range of motion. Three tri-als were conducted for each direction of movement, andthe average of the three measurements were recordedfor analysis. All measurements were taken by the sameresearcher who has postgraduate qualifications and15 years of clinical experience in musculoskeletalphysiotherapy.
Data analysisDescriptive statistics were calculated including mean ±standard deviation (SD) for age, height and weight. Theoutcome measures of NDI, pain intensity, algometric
score, CROM, CV angle and SH angle were measuredusing repeated measures one-way analysis of variances(ANOVA) to compare measurements made before treat-ment, after the 10 weeks of treatment, and at 1-year fol-low up. Tukey’s post-hoc multiple comparisons wasimplemented when necessary. The baseline score foroutcomes were used as covariates in a one-way analysisof covariance (ANCOVA) when baseline differences aresubstantial enough to influence the study outcomes. Weconsidered a mean difference of more than 10.5 pointson the NDI as a MCID. Effect sizes measured usingCohen’s d were calculated to examine the average impactof the intervention [27]. According to the method of Co-hen, d ≈ 0.2 indicates a small effect and negligible clinicalimportance, d ≈ 0.5 indicates a medium effect and mod-erate clinical importance and d ≈ 0.8 indicates a large ef-fect and high clinical importance [24]. For all statisticaltests the level of significance was set at p < 0.05. Correla-tions (Pearson’s r) were used to examine the relation-ships between the amount of changes in CV and SH (inthe study group) and the amount of change in NDI, painintensity, ROM, and pressure algometry.
Sample sizeA sample size of 100 patients provided a 90% power of de-tecting minimal clinically important change (MCIC) onthe Neck Disability Index (NDI) of 10.5 points (scale range0–50. To account for possible participant drop-outs, thesample size was increased by 20% in each group.Missing values were addressed by using multiple regres-
sion models. Model parameters were estimated with mul-tiple regression applied to each imputed data setseparately. These estimates and their standard errors werecombined into one overall estimate using Rubin’s rules.
ResultsA diagram of patient flow and randomization for ourstudy is shown in Fig. 3. Two hundred and fifteen pa-tients were initially screened with 120 of them being eli-gible to participate in the study. In total 120 (100%)completed the first study follow up after 30 visits or10 weeks of treatment. At the 1-year follow up, 102(85%) participants completed the entire study duration.At baseline, both groups were comparable with regardto all variables and had no statistically or clinically rele-vant differences, except for the cervical rotation ROMand Algometric pressure (Table 1).
Primary outcome measureNDIThe difference between the intervention group and thecontrol group was not significant after 10 weeks (p = .09;95% CI [− 1.59 to .131]), however, it was significant at1-year follow up (< 0.001*; 95% CI [− 11.9–10.23]). The
Fig. 2 Adhesive marker placement and postural angles used tomeasure anterior head translation. a. cervical angle; b. shoulder angle
Moustafa et al. BMC Musculoskeletal Disorders (2018) 19:396 Page 5 of 13
-
effect size (Cohen’s d) was 0.9 (Table 2). These findings in-dicated a greater improvement in the interventional groupin the NDI and a regression back to baseline-pre-treatmentvalues in the NDI for the control subjects.
Secondary outcome measuresPain intensity and algometric pressureSubsequent analyses depending on the presence of inter-actions for main effects, revealed that after 10 weeks oftreatment, the two arms of treatment (both interven-tional and control groups) seemed roughly equally suc-cessful in improving the pain intensity, and pressurealgometry outcome measures. At 10 weeks, the unpairedt test analysis revealed insignificant differences betweenthe experimental and control groups for pain intensity(p = 0.36), while there was a significant difference foralgometry (p
-
extension (p
-
those reported in two earlier trials using this patient pre-scribed orthotic device [15, 16]. Devices such as the den-neroll, act as three-point-bending cervical extensiontraction devices; where structures located anterior to theaxis of extension rotation will be exposed to significanttension loads and structures posterior will experiencecompression. The anterior tension loading likely unloadsthe intervertebral disc, causing tension on the anteriorcervical spine muscles, and anterior longitudinal ligament,leading to visco-elastic creep deformation resulting in in-creasing the cervical lordosis and reducing anterior headtranslation [16, 18, 28].Anterior head translation and protraction or rounding
of the shoulders are likely two postures that are coupledtogether. In our current study, we identified that theintervention group receiving the cervical denneroll wasfound to have a reduction in both anterior head postureand a more retracted shoulder / scapular position fol-lowing treatment. Reduction in anterior head translationis likely responsible for the improvement in shoulderalignment. Similarly, Diab et al., identified that reductionin sagittal head posture was an effective means for im-proving 3-D spinal posture of the thoracic region andpelvis [29]. Collectively, the finding that rehabilitation ofcervical sagittal posture may subtly improve full spineposture measures indicates that there must exist a topdown neurophysiological regulation of upright humanposture that is driven by the sagittal alignment of thecervical lordosis and forward head posture [30, 31].
Forward head posture and neck disability indexIt is interesting that the application of an integratedneuromuscular inhibition technique alone or in con-junction with an intervention program for forward head
posture reduction (denneroll orthotic) seem roughlyequally successful in improving neck disability statusafter 10 weeks of treatment. However, our 1-year followup data revealed a significant decline in the neckdisability index for the control group. The temporalimprovement in the control group may be attributed tothe strong association between pain relief in bothgroups and functional status. However, over time, thecontinuous increased and / or asymmetrical loadingfrom forward head posture may be the possible explan-ation for the decline in functional disability status forthe control group at 12 months follow up. This conceptof biomechanical dysfunction resulting from anteriorhead translation is supported by predictions fromexperimental and biomechanical spine-posture model-ing studies [15, 19, 32, 33] as well as from post-surgicaloutcomes [34, 35] and large scale cross-sectional inves-tigations [36].Specifically, Tang et al. [34] identified that anterior
translation distance of C2 relative to C7 (termed the SVA)on lateral cervical radiographs positively correlated withthe neck disability index in 113 patients receiving poster-ior cervical spine fusions. Similar results were identified ina prospective sample of 49 patients by Roguski et al. [35].In a large cross sectional analysis of 656 subjects, Oe et al.[36] identified strong correlations between activities ofdaily living on the EuroQOL questionnaire and theC2-C7 SVA. These three studies [34–36] are supportedby the results of the current investigation where weidentified a statistically significant correlation betweenour experimental groups improvement in their anteriorhead translation (CV angle) and their consequent im-provement in NDI 10-weeks post treatment and at longterm follow up.
Table 3 The changes in secondary outcomes; pain intensity and algometry in experimental and control groups vs time
Outcome Experimental group Control group Mean difference (95% CI) P value effect size (Cohen’s d) Effect size r
Pain intensity
Baseline 5.3 ± .7 5.1 ± .8 [−.05 .5] .11
After 10 weeks 1.4 ± .9 1.6 ± .8 [−.5 .17] .36
1-year follow up .4 ± .4 4.2 ± .7 [−4.1-3.6] < 0.001 .6 .9
G < 0.001
T < 0.001
G*T < 0.001
Algometric pressure
Baseline 1.9 ± .2 1.71 ± .3 [.15.3] < 0.001
After 10 weeks 3.6 ± .3 3.3 ± .5 [.13.5] < 0.001 .7 .8
1-year follow up 3.9 ± .2 2 ± .4 [1.8 2.1] < 0.001 .9 .9
G < 0.001
T < 0.001
G*T < 0.001
G: group T: time G vs T: group versus time
Moustafa et al. BMC Musculoskeletal Disorders (2018) 19:396 Page 8 of 13
-
Table 4 Changes in secondary outcomes; cervical ROM and posture parameters
Cervical angle (CV)
Experimental group Control group Mean difference (95% CI) P value effect size (Cohen’s d) Effect size r
Baseline 44. 8 ± 3.5 45 ± 3.2 [−1.5 .94] .6
After 10 weeks 54.8 ± 2.5 45 ± 3.3 [8.8 10.9] < 0.001 5.2 .9
1-year follow up 54.2 ± 2.7 44.5 ± 3.1 [8.7 10.8] < 0.001 5.7 .9
G < 0.001
T < 0.001
G*T < 0.001
Shoulder angle
Baseline 48.2 ± 2.1 48.3 ± 1.7 [−.77 .6] .8
After 10 weeks 57.7 ± 2.9 48.06 ± 1.6 [8.7 10.4] < 0.001 4.1 .9
1-year follow up 56.9 ± 3.1 48.3 ± 1.4 [7.71 9.4] < 0.001 3.7 .9
G < 0.001
T < 0.001
G*T < 0.001
Flexion
Baseline 42.3 ± 2 41.9 ± 2.1 [−.31 1.2] .2
After 10 weeks 46.7 ± 1.5 43.3 ± 1.7 [2.8 4.1] < 0.001 2.5 .7
1-year follow up 46.3 ± 1.4 42.9 ± 2.3 [2.7 4.1] < 0.001 1.7 .7
G < 0.001
T < 0.001
G*T < 0.001
Extension
Baseline 68.1 ± 1.2 67.6 ± 2.5 [−.14 1.3] .1
After 10 weeks 75.2 ± 1.8 68.2 ± 2.4 [6.3 7.8] < 0.001 3.2 .9
1-year follow up 74.4 ± 1.7 67.6 ± 1.9 [6.2 7.3] < 0.001 3.8 .9
G < 0.001
T < 0.001
G*T < 0.001
Right rotation
Baseline 72.3 ± 2.4 73.7 ± 2.6 [−2.3 -.4] < 0.001
After 10 weeks 79.7 ± 1.4 74.8 ± 2.3 [4.2 5.5] < 0.001 2.6 .8
1-year follow up 78.8 ± .9 74.8 ± 2.1 [3.4 4.6] < 0.001 2.5 .8
G < 0.001
T < 0.001
G*T < 0.001
Left rotation
Baseline 72.3 ± 2.4 74.3 ± 2.8 [−2.94-1.05] < 0.001
After 10 weeks 79.6 ± 1.4 74.8 ± 2.3 [4.21 5.4] < 0.001 2.6 .8
1-year follow up 78.8 ± .9 74.8 ± 2.1 [3.4 4.6] < 0.001 2.5 .8
G < 0.001
T < 0.001
G*T < 0.001
Right tilt
Baseline 42.3 ± 2 41.9 ± 2.1 [−.31 1.18] .2
Moustafa et al. BMC Musculoskeletal Disorders (2018) 19:396 Page 9 of 13
-
Pain intensity and algometric pressureOverall, our findings revealed a significant and stable de-crease in pain intensity for the study group. This longlasting improvement of pain for the study group seemsattributable to the restoration of normal posture. It isgenerally accepted that spinal function is directly relatedto spinal structure. Abnormal posture elicits abnormalstresses and strains in many structures, including bones,intervertebral discs, facet joints, musculotendinous tis-sues, and neural elements [13, 27, 32, 33], that can beconsidered as a predisposing factor for pain from an al-teration in mechanical loading. Of interest, in FHP, re-ciprocal postural compensation was observed in theupper and lower cervical spine to maintain horizontalgaze. FHP caused flexion in the lower segments andextension in the atlanto-occipital and atlantoaxial seg-ments. The transition between flexion and extension oc-curred in the C2–C4 region. These compensations haveimplications towards increased abnormal stresses andstrains [37]. Thus, restoring the normal sagittal configur-ation is likely to minimize the abnormal stresses.This mechanical relationship between prolonged ab-
normal postures and MPS has previously been identifiedin different studies [9, 10]. However, few studies havedirectly evaluated the relationship between forward headposture and MPS in neck and shoulder. Sun et al., exam-ined the correlation between the presence of MPS andabnormal cervical sagittal alignment concluding that“there was no relationship between the forward headposition and the presence, location, and number of trig-ger points” [38]. While Penas et al., highlighted the posi-tive relationship between forward head posture and thepresence of active trigger points [39].The discrepancy and conflict regarding the relation-
ship between abnormal forward head posture with MPS
identified by earlier authors cannot be directly comparedwith our current study because earlier studies arecross-sectional correlation studies without an ability toascribe cause and effect. In the current study, the signifi-cant correlations between the amount of change in theCV angle in the intervention group and neck disability,pain intensity, and algometry outcomes indicates thatforward head posture reduction improves the outcomesof MPS.Concerning the pain level outcomes in the control
group, the temporal reduction of pain may be attributedto short term effects of integrated neuromuscular inhib-ition technique. For example, Hu et al. [40] reported thatpain reduction, improvement of MTrP sensitivity, andincrease in ROM after various modalities for cervicalmyofascial pain and trigger-point sensitivity may not bemaintained long term. Similarly, the systematic review ofVernon and Schneider [41] provides moderately strongevidence to support the use of some manual therapies inthe immediate relief of TrP tenderness. However, onlylimited evidence to support the use of manual therapiesover longer courses of treatments in the management ofTrPs and MPS was found.
Cervical ROMOne might speculate that the improvement of ROM isattributed to a decrease of pain intensity. However, thesignificant differences between our study and controlgroups at the two measurement intervals favoring thestudy group indicate that the loss in ROM is not or notonly driven by the presence of myofascial pain [34, 42].Other factors associated with restricted ROM besides in-creased muscle tension and pain need considered.Mechanically though, forward head translation alters theanatomic alignment of the cervical spine joints in the
Table 4 Changes in secondary outcomes; cervical ROM and posture parameters (Continued)
Cervical angle (CV)
Experimental group Control group Mean difference (95% CI) P value effect size (Cohen’s d) Effect size r
After 10 weeks 46.7 ± 1.5 43.3 ± 1.7 [2.8 4.05] < 0.001 2.5 .7
1-year follow up 46.3 ± 1.4 42.9 ± 2.3 [2.724 4.1] < 0.001 1.7 .7
G < 0.001
T < 0.001
G*T < 0.001
Left Right tilt
Baseline 42.5 ± 2.1 42.2 ± 2.1 [−.42 1.12] .3
After 10 weeks 46.7 ± 1.6 43.45 ± 1.8 [2.6 3.9] < 0.001 2.5 .7
1-year follow up 46.4 ± 1.4 43.15 ± 2.3 [2.5 3.9] < 0.001 1.7 .7
G < 0.001
T < 0.001
G*T < 0.001
G: group T: time G vs T: group versus time
Moustafa et al. BMC Musculoskeletal Disorders (2018) 19:396 Page 10 of 13
-
sagittal plane, alters the lever arms of the cervical spinemuscles and thus this is the most plausible explanationfor altered cervical spine ROM [35]. This statement isfurther supported by the significant correlation betweenthe amount of change in the CV angle in the interven-tion group and all ROM outcomes. The current studyresults are logical and agree with those of four otherstudies [35, 36, 43, 44], each of which investigated theassociation between forward head and cervical ROM.
LimitationsThe current study has some potential limitations. First,our study lacked blinding of participants and treatmentproviders. Due to the nature of the interventions, it wasnot be possible to blind participants and treatment pro-viders to the interventions provided. Second, we used a
sample of convenience from 1 clinic; which may not berepresentative of the entire population of patients withCMCPS. Additionally, we chose selective but relevant pa-tient outcome measures (NDI, pain scale, pain pressurethresholds, range of motion) to identify if changes in sagit-tal plane posture deviations are related to CMCPS im-provement. It is possible that other measures of CMCPSoutcomes would have different relationships (greater orless improved) with posture alignment changes and thatdifferent interventions than those tested herein may im-prove patients with CMCPS more considerably.Third, although the correlations identified between
our postural measures and patient outcomes were statis-tically significant, they would be classified in the moder-ate range. This indicates that there are other variables,not accounted for in the current study design, which
Table 5 Pearson’s r correlation matrix for outcome variables in the intervention group
Δ cervical angle 0-10w Δ cervical angle 10-1Y Δ shoulder angle 0-10w Δ shoulder angle 10w -1Y
Δ pain 0-10 W −.2P = .05
−.2P = .015
Δ pain 10 W-1Y −.1P = .2
−.05P = .3
Δ NDI 0-10w −.24P = .032
−.11P = .196
Δ NDI 10 w-1Y .2P = .0
.07P = .2
Δ algometric 0–10 w .24P = .033
.29P = .012
Δ algometric 10w-1 Y −.027P = .4
−.002P = .4
ROM flexion 0–10 w .2P = .028
.15P = .1
ROM flexion 10w-1 Y −.16P = .1
−.007P = .4
ΔROM extension 0–10 w .34P = .003
−.06P = .3
ΔROM extension 10w-1 Y .06P = .3
.053P = .3
ΔROM RT rotation 0–10 w .25P = .026
.14P = .1
ΔROM RT rotation 10w-1 Y −.11P = .1
.033P = .4
ΔROM left rotation 0–10 w .4P = .036
.03P = .4
ΔROM rotation lt 10w-1 Y −.1P = .1
.013P = .4
ΔROM RT lateral flex 0–10 w .2P = .020
.12P = .1
ΔROM RT lateral flex 10w-1 Y .14P = .1
ΔROM left lateral flex 0–10 w .2P = .021
.05P = .3
ΔROM left lateral flex 10w-1 Y .04P = .3
−.1P = .2
Moustafa et al. BMC Musculoskeletal Disorders (2018) 19:396 Page 11 of 13
-
have determining effects on neck disability, pain, andrange of motion outcomes. Along this line, we were un-able to obtain follow-up lateral cervical radiographs.Thus, we do not if know the cervical lordosis was im-proved in the experimental group receiving the denne-roll and if this may have added any significance to thecorrelation to patient outcomes.Within these limitations, the unique contribution of
this study is that it evaluated the independent effect ofstructural rehabilitation of the cervical spine sagittal pos-ture on the short and long term severity of the signs andsymptoms associated with CMCPS; which to our know-ledge has not been previously reported. A major strengthof the present study is the information as to how longpain relief lasted after treatment; up to 1-year. Whereasadditional post-treatment measurements with longerthan a 1-year interval might have identified a waning ef-fectiveness of treatment.
ConclusionThis study identified that restoring a more normal cervicalsagittal alignment with denneroll traction has a strongpositive impact on pain, function, and ROM in patientswith myofascial pain syndrome. Our one-year follow-uprevealed stable improvement in all measured variables.The findings provide objective evidence that biomechan-ical dysfunction in terms of abnormal head and cervicalposture influences the outcome measures of MPS. Theseobserved effects should be of value to clinicians and healthprofessionals involved in the treatment of MPS where cer-vical spine alignment rehabilitation can be added to theinterventions for MPS patients who present with signifi-cant posture abnormality.
AbbreviationsCMCPS: Chronic myofascial cervical pain syndrome; CV: Cervical angle;INIT: Neuromuscular inhibition technique; NDI: Neck disability index;NRS: Neck pain intensity; PPT: Pressure pain thresholds; SH: Shoulder angle
AcknowledgementsWe thank the CBP NonProfit, Inc. for supplying the Dennerolls used is this study.
FundingThis study was financially supported by funding from the ChiropracticBiophysics Non-profit, Inc., Inc. The contribution in terms of supplying theDennerolls used is this study.Chiropractic Biophysics Non-profit, Inc. is anonprofit corporation dedicated to the advancement of chiropracticprinciples through scientific research.
Availability of data and materialsThe datasets used and analysed in this study are available from thecorresponding author on reasonable request.
Authors’ contributionsIMM and AAD, involved in study conception and design, as well asimplementation, analysis and interpretation of data, and manuscriptpreparation FH made substantial contributions to the conception and designof the study and the drafting of the article, DEH made substantialcontributions to the conception and design of the study, the analysis andinterpretation of the data and the revision of the article. All authors havereviewed and approved the final manuscript.
Ethics approval and consent to participateThe study has received ethical approval from the Research EthicsCommittee-Faculty of Physical Therapy-Cairo University. All participatingsubjects have signed an informed consent form before entering the study.
Consent for publicationWritten consent to publish the content of this report along with theaccompanying images was obtained from all patients.
Competing interestsDEH is the president of a company that distributes the cervical Dennerollproduct to health care providers in North America. IMM and AAD and FHhave no conflicts of interest related to this project.
Publisher’s NoteSpringer Nature remains neutral with regard to jurisdictional claims in publishedmaps and institutional affiliations.
Author details1Department of Physiotherapy, College of Health Sciences, University ofSharjah, Sharjah, United Arab Emirates. 2Basic Science Department, Faculty ofPhysical Therapy, Cairo University, 7 Mohamed Hassan El gamal Street-AbbasEl Akaad, Nacer City, Egypt. 3CBP Nonprofit (a spine research foundation),Eagle, ID, USA.
Received: 12 February 2018 Accepted: 24 October 2018
References1. KADEFORS R, Forsman M, Zoéga B, Herberts P. Recruitment of low
threshold motor-units in the trapezius muscle in different static armpositions. Ergonomics. 1999;42:359–75 [cited 2018 Jul 4] Available from:http://www.ncbi.nlm.nih.gov/pubmed/10024852.
2. Kostopoulos D, Rizopoulos K. The manual of trigger point and myofascialtherapy: Slack; 2001.
3. Rickards LD. The effectiveness of non-invasive treatments for activemyofascial trigger point pain: A systematic review of the literature. Int JOsteopath Med. 2006;9:120–36 Elsevier; [cited 2018 Jan 11] Available from:https://www.sciencedirect.com/science/article/pii/S1746068906000952.
4. Dommerholt J, Grieve R, Layton M, Hooks T. An evidence-informed reviewof the current myofascial pain literature – January 2015. J Bodyw Mov Ther.2015;19:126–37 Churchill Livingstone [cited 2018 Jan 11] Available from:https://www.sciencedirect.com/science/article/pii/S1360859214001922.
5. Mata Diz JB, de Souza JRLM, Leopoldino AAO, Oliveira VC. Exercise,especially combined stretching and strengthening exercise, reducesmyofascial pain: a systematic review. J Physiother. 2017;63:17–22 [cited 2017May 21] Available from: http://www.sciencedirect.com/science/article/pii/S1836955316300911.
6. Fernández-de-las-Peñas C, Dommerholt J. Myofascial trigger points: peripheralor central phenomenon? Curr Rheumatol Rep. 2014;16:395 [cited 2017 Dec 2]Available from: http://www.ncbi.nlm.nih.gov/pubmed/24264721.
7. Pace MC, Mazzariello L, Passavanti MB, Sansone P, Barbarisi M, Aurilio C.Neurobiology of pain. J Cell Physiol. 2006;209:8–12 [cited 2017 Dec 2]Available from: http://www.ncbi.nlm.nih.gov/pubmed/16741973.
8. Gerwin R. Myofascial pain syndrome: Here we are, where must we go? JMusculoskelet Pain. 2010;18:329–47 Taylor & Francis [cited 2017 Dec 2] Availablefrom: http://www.tandfonline.com/doi/full/10.3109/10582452.2010.502636.
9. Yoo W-G. Effect of the Neck Retraction Taping (NRT) on Forward HeadPosture and the Upper Trapezius Muscle during Computer Work. J PhysTher Sci. 2013;25:581–2 Society of Physical Therapy Science [cited 2017 Dec2] Available from: http://www.ncbi.nlm.nih.gov/pubmed/24259806.
10. Gupta BD, Aggarwal S, Gupta B, Gupta M, Gupta N. Effect of deep cervicalflexor training vs. conventional isometric training on forward head posture,pain, neck disability index in dentists suffering from chronic neck pain.J Clin Diagnostic Res. 2013;7:2261–4 [cited 2017 Dec 2] Available from:http://www.ncbi.nlm.nih.gov/pubmed/24298492.
11. McAviney J, Schulz D, Bock R, Harrison DE, Holland B. Determining therelationship between cervical lordosis and neck complaints. J ManipulativePhysiol Ther. 2005;28:187–93 [cited 2016 Apr 25] Available from:http://www.ncbi.nlm.nih.gov/pubmed/15855907.
Moustafa et al. BMC Musculoskeletal Disorders (2018) 19:396 Page 12 of 13
http://www.ncbi.nlm.nih.gov/pubmed/10024852https://www.sciencedirect.com/science/article/pii/S1746068906000952https://www.sciencedirect.com/science/article/pii/S1360859214001922http://www.sciencedirect.com/science/article/pii/S1836955316300911http://www.sciencedirect.com/science/article/pii/S1836955316300911http://www.ncbi.nlm.nih.gov/pubmed/24264721http://www.ncbi.nlm.nih.gov/pubmed/16741973http://www.tandfonline.com/doi/full/10.3109/10582452.2010.502636http://www.ncbi.nlm.nih.gov/pubmed/24259806http://www.ncbi.nlm.nih.gov/pubmed/24298492http://www.ncbi.nlm.nih.gov/pubmed/15855907
-
12. Harrison DD, Janik TJ, Troyanovich SJHB. Comparisons of lordotic cervicalspine curvatures to a theoretical ideal model of the static sagittal cervicalspine. Spine (Phila Pa 1976). 1996;21:667–75.
13. Harrison DDE, Cailliet R, Harrison DDE, Troyanovich SJ, Harrison SO. A reviewof biomechanics of the central nervous system--part II: spinal cord strainsfrom postural loads. J Manipulative Physiol Ther. 1999;22:322–32 [cited 2016Apr 25] Available from: http://www.ncbi.nlm.nih.gov/pubmed/10395435.
14. Diab AA, Moustafa IM. The efficacy of forward head correction on nerveroot function and pain in cervical spondylotic radiculopathy: a randomizedtrial. Clin Rehabil. 2012;26:351–61 [cited 2016 Apr 30] Available from:http://www.ncbi.nlm.nih.gov/pubmed/21937526.
15. Moustafa IM, Diab AA, Taha S, Harrison DE. Addition of a sagittal cervicalposture corrective orthotic device to a multimodal rehabilitation programimproves short- and long-term outcomes in patients with discogeniccervical radiculopathy. Arch Phys Med Rehabil. 2016;97:2034–44 [cited 2017Dec 2] Available from: http://www.ncbi.nlm.nih.gov/pubmed/27576192.
16. Singla D, Veqar Z, Hussain ME. Photogrammetric assessment of upper bodyposture using postural angles: a literature review. J Chiropr Med. 2017;16:131–8 Elsevier [cited 2018 Jul 4] Available from: http://www.ncbi.nlm.nih.gov/pubmed/28559753.
17. Shumway-Cook A, Woollacott MH. Motor control : theory and practicalapplications [Internet]. Lippincott Williams & Wilkins; 2001 [cited 2018 Jan11]. Available from: https://books.google.ae/books/about/Motor_Control.html?id=301hQgAACAAJ&redir_esc=y
18. Juul T, Søgaard K, Davis AM, Roos EM. Psychometric properties of the neckoutcome score, neck disability index, and short form–36 were evaluated inpatients with neck pain. J Clin Epidemiol. 2016;79:31–40 [cited 2018 Jan 11]Available from: http://linkinghub.elsevier.com/retrieve/pii/S0895435616300270.
19. Yip CHT, Chiu TTW, Poon ATK. The relationship between head posture andseverity and disability of patients with neck pain. Man Ther. 2008;13:148–54 [cited2016 Apr 30] Available from: http://www.ncbi.nlm.nih.gov/pubmed/17368075.
20. Institute of Medicine (US) Committee on Pain, Disability and CIB, OsterweisM, Kleinman A, Mechanic D. Appendix myofascial pain syndromes due totrigger points. National Academies Press (US); 1987 [cited 2017 Dec 6];Available from: https://www.ncbi.nlm.nih.gov/books/NBK219241/
21. MacDermid JC, Walton DM, Avery S, Blanchard A, Etruw E, McAlpine C, et al.Measurement properties of the neck disability index: a systematic review.J Orthop Sports Phys Ther. 2009;39:400–17 [cited 2016 Apr 30] Availablefrom: http://www.ncbi.nlm.nih.gov/pubmed/19521015.
22. Falla D, Jull G, Russell T, Vicenzino B, Hodges P. Effect of neck exercise on sittingposture in patients with chronic neck pain. Phys Ther. 2007;87:408–17 [cited 2017Dec 6] Available from: http://www.ncbi.nlm.nih.gov/pubmed/17341512.
23. Brink Y, Crous LC, Louw QA, Grimmer-Somers K, Schreve K. The associationbetween postural alignment and psychosocial factors to upper quadrantpain in high school students: a prospective study. Man Ther. 2009;14:647–53[cited 2017 Dec 6] Available from: http://linkinghub.elsevier.com/retrieve/pii/S1356689X09000411.
24. Cohen J. Statistical power analysis for the behavioral sciences (2nd ed.) NewYork: Academic Press; 1977.
25. Tsai C-T, Hsieh L-F, Kuan T-S, Kao M-J, Chou L-W, Hong C-Z. Remote effectsof dry needling on the irritability of the myofascial trigger point in theupper trapezius muscle. Am J Phys Med Rehabil. 2010;89:133–40 [cited 2018Jan 11] Available from: http://www.ncbi.nlm.nih.gov/pubmed/19404189.
26. Audette I, Dumas J-P, Côté JN, De Serres SJ. Validity and between-dayreliability of the Cervical Range of Motion (CROM) device. J Orthop SportPhys Ther. 2010;40:318–23 [cited 2018 Feb 8] Available from: http://www.ncbi.nlm.nih.gov/pubmed/20436238.
27. Harrison DE, Harrison DD, Harrison SOTS. A review of biomechanics of thecentral nervous system. Part 1: spinal canal deformations caused bychanges in posture. J Manip Physiol Ther. 2000;23:217–20.
28. Kourtis D, Magnusson ML, Smith F, Hadjipavlou A, Pope MH. Spine heightand disc height changes as the effect of hyperextension using stadiometryand MRI. Iowa Orthop J. 2004;24:65–71 [cited 2016 Apr 30] Available from:http://www.ncbi.nlm.nih.gov/pubmed/15296209.
29. Diab AA. The role of forward head correction in management of adolescentidiopathic scoliotic patients: a randomized controlled trial. 2012 [cited 2016may 10];26. Available from: http://www.ncbi.nlm.nih.gov/pubmed/22801470.
30. Morningstar MW, Strauchman MN, Weeks DA. Spinal manipulation andanterior headweighting for the correction of forward head posture andcervical hypolordosis: a pilot study. J Chiropr Med. 2003;2:51–4 Elsevier [cited2018 Jan 11] Available from: http://www.ncbi.nlm.nih.gov/pubmed/19674595.
31. Ledin T, Hafström A, Fransson PA, Magnusson M. Influence of neckproprioception on vibration-induced postural sway. Acta Otolaryngol. 2003;123:594–9 [cited 2018 Jan 11] Available from: http://www.ncbi.nlm.nih.gov/pubmed/12875581.
32. Harrison DE, Colloca CJ, Harrison DD, Janik TJ, Haas JW, Keller TS. Anteriorthoracic posture increases thoracolumbar disc loading. Eur Spine J. 2005;14:234–42 Springer [cited 2018 Jan 11] Available from: http://www.ncbi.nlm.nih.gov/pubmed/15168237.
33. Keller TS, Colloca CJ, Harrison DE, Harrison DD, Janik TJ. Influence of spinemorphology on intervertebral disc loads and stresses in asymptomaticadults: implications for the ideal spine. Spine J. 2005;5:297–309 [cited 2018Jan 11] Available from: http://www.ncbi.nlm.nih.gov/pubmed/15863086.
34. Gerwin RD, Dommerholt J, Shah JP. An expansion of Simons’ integratedhypothesis of trigger point formation. Curr Pain Headache Rep. 2004;8:468–75[cited 2018 Jan 11] Available from: http://www.ncbi.nlm.nih.gov/pubmed/15509461.
35. Walmsley RP, Kimber P, Culham E. The effect of initial head position onactive cervical axial rotation range of motion in two age populations. Spine(Phila Pa 1976). 1996;21:2435–42 [cited 2018 Jan 11] Available from:http://www.ncbi.nlm.nih.gov/pubmed/8923628.
36. Fernández-de-las-Peñas C, Alonso-Blanco C, Cuadrado M, Pareja J. Forwardhead posture and neck mobility in chronic tension-type headache.Cephalalgia. 2006;26:314–9 [cited 2017 may 14] Available from: http://www.ncbi.nlm.nih.gov/pubmed/16472338.
37. Patwardhan AG, Havey RM, Khayatzadeh S, Muriuki MG, Voronov LI,Carandang G, et al. Postural consequences of cervical sagittal imbalance: anovel laboratory model. Spine (Phila Pa 1976). 2015;40:783–92 [cited 2018Jan 11] Available from: http://content.wkhealth.com/linkback/openurl?sid=WKPTLP:landingpage&an=00007632-201506010-00006.
38. Sun A, Yeo HG, Kim TU, Hyun JK, Kim JY. Radiologic assessment of forwardhead posture and its relation to myofascial pain syndrome. Ann RehabilMed. 2014;38:821–6 [cited 2018 Jan 11] Available from: https://synapse.koreamed.org/DOIx.php?id=10.5535/arm.2014.38.6.821.
39. Fernandez-de-las-Penas C, Alonso-Blanco C, Cuadrado ML, Gerwin RD,Pareja JA. Trigger points in the suboccipital muscles and forward headposture in tension-type headache. Headache J Head Face Pain. 2006;46:454–60 [cited 2018 Jan 11] Available from: http://www.ncbi.nlm.nih.gov/pubmed/16618263.
40. Hou C-R, Tsai L-C, Cheng K-F, Chung K-C, Hong C-Z. Immediate effects ofvarious physical therapeutic modalities on cervical myofascial pain andtrigger-point sensitivity. Arch Phys Med Rehabil. 2002;83:1406–14 [cited2018 Jan 11] Available from: http://www.ncbi.nlm.nih.gov/pubmed/12370877.
41. Vernon H, Schneider M. Chiropractic management of myofascial triggerpoints and myofascial pain syndrome: a systematic review of the literature.J Manipulative Physiol Ther. 2009;32:14–24 [cited 2018 Jan 11] Availablefrom: http://www.ncbi.nlm.nih.gov/pubmed/19121461.
42. Simons DG. Understanding effective treatments of myofascial triggerpoints. J Bodyw Mov Ther. 2002;6:81–8 Churchill Livingstone [cited 2018Jan 11] Available from: https://www.sciencedirect.com/science/article/pii/S1360859202902718.
43. De-La-Llave-Rincón AI, Fernández-De-Las-PeÑas C, Palacios-CeÑa D, ClelandJA. Increased forward head posture and restricted cervical range of motionin patients with carpal tunnel syndrome. J Orthop Sport Phys Ther. 2009;39:658–64 [cited 2018 Jan 11] Available from: http://www.ncbi.nlm.nih.gov/pubmed/19721213.
44. Yoo W-G, An D-H. The relationship between the active cervical range ofmotion and changes in head and neck posture after continuous VDT work.Ind Health. 2009;47:183–8 [cited 2018 Jan 11] Available from: http://www.ncbi.nlm.nih.gov/pubmed/19367048.
Moustafa et al. BMC Musculoskeletal Disorders (2018) 19:396 Page 13 of 13
http://www.ncbi.nlm.nih.gov/pubmed/10395435http://www.ncbi.nlm.nih.gov/pubmed/21937526http://www.ncbi.nlm.nih.gov/pubmed/27576192http://www.ncbi.nlm.nih.gov/pubmed/28559753http://www.ncbi.nlm.nih.gov/pubmed/28559753https://books.google.ae/books/about/Motor_Control.html?id=301hQgAACAAJ&redir_esc=yhttps://books.google.ae/books/about/Motor_Control.html?id=301hQgAACAAJ&redir_esc=yhttps://books.google.ae/books/about/Motor_Control.html?id=301hQgAACAAJ&redir_esc=yhttp://linkinghub.elsevier.com/retrieve/pii/S0895435616300270http://www.ncbi.nlm.nih.gov/pubmed/17368075https://www.ncbi.nlm.nih.gov/books/NBK219241/http://www.ncbi.nlm.nih.gov/pubmed/19521015http://www.ncbi.nlm.nih.gov/pubmed/17341512http://linkinghub.elsevier.com/retrieve/pii/S1356689X09000411http://linkinghub.elsevier.com/retrieve/pii/S1356689X09000411http://www.ncbi.nlm.nih.gov/pubmed/19404189http://www.ncbi.nlm.nih.gov/pubmed/20436238http://www.ncbi.nlm.nih.gov/pubmed/20436238http://www.ncbi.nlm.nih.gov/pubmed/15296209http://www.ncbi.nlm.nih.gov/pubmed/22801470http://www.ncbi.nlm.nih.gov/pubmed/19674595http://www.ncbi.nlm.nih.gov/pubmed/12875581http://www.ncbi.nlm.nih.gov/pubmed/12875581http://www.ncbi.nlm.nih.gov/pubmed/15168237http://www.ncbi.nlm.nih.gov/pubmed/15168237http://www.ncbi.nlm.nih.gov/pubmed/15863086http://www.ncbi.nlm.nih.gov/pubmed/15509461http://www.ncbi.nlm.nih.gov/pubmed/15509461http://www.ncbi.nlm.nih.gov/pubmed/8923628http://www.ncbi.nlm.nih.gov/pubmed/16472338http://www.ncbi.nlm.nih.gov/pubmed/16472338http://content.wkhealth.com/linkback/openurl?sid=WKPTLP:landingpage&an=00007632-201506010-00006http://content.wkhealth.com/linkback/openurl?sid=WKPTLP:landingpage&an=00007632-201506010-00006https://synapse.koreamed.org/DOIx.php?id=10.5535/arm.2014.38.6.821https://synapse.koreamed.org/DOIx.php?id=10.5535/arm.2014.38.6.821http://www.ncbi.nlm.nih.gov/pubmed/16618263http://www.ncbi.nlm.nih.gov/pubmed/16618263http://www.ncbi.nlm.nih.gov/pubmed/12370877http://www.ncbi.nlm.nih.gov/pubmed/12370877http://www.ncbi.nlm.nih.gov/pubmed/19121461https://www.sciencedirect.com/science/article/pii/S1360859202902718https://www.sciencedirect.com/science/article/pii/S1360859202902718http://www.ncbi.nlm.nih.gov/pubmed/19721213http://www.ncbi.nlm.nih.gov/pubmed/19721213http://www.ncbi.nlm.nih.gov/pubmed/19367048http://www.ncbi.nlm.nih.gov/pubmed/19367048
AbstractBackgroundMethodsResultsConclusionTrial registration
BackgroundMethodsPatientsRandomizationTreatment methodsDenneroll extension traction for the intervention groupIntegrated neuromuscular inhibition technique (INIT)Ischemic compression and strain Counterstrain (SCS)Muscle energy technique (MET)Home exercise protocolOutcome measuresPrimary outcome measureSecondary outcome measuresPostural cervical sagittal alignmentPressure-pain threshold (PPT) algometric measurementCervical ROM
Data analysisSample size
ResultsPrimary outcome measureNDI
Secondary outcome measuresPain intensity and algometric pressureCervical angle and shoulder angleCervical range of motion
Correlation of posture parameters to primary and secondary outcomes
DiscussionForward head posture and neck disability indexPain intensity and algometric pressureCervical ROMLimitations
ConclusionAbbreviationsAcknowledgementsFundingAvailability of data and materialsAuthors’ contributionsEthics approval and consent to participateConsent for publicationCompeting interestsPublisher’s NoteAuthor detailsReferences
Related Documents