University of Gloucestershire BA (Hons) Education Studies May 2014 An exploration into the Total Communication approach when supporting the communication difficulties in children with an Autism Spectrum Disorder: a case study Name: Michelle Oak Student number: xxxxxxxxx Dissertation Tutor: Richard Millican 1

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

University of Gloucestershire
BA (Hons) Education Studies
May 2014
An exploration into the Total Communication approach when
supporting the communication difficulties in children with an
Autism Spectrum Disorder: a case study
Name: Michelle Oak
Student number: xxxxxxxxx
Dissertation Tutor: Richard Millican
Presented as part of the requirement for an undergraduate award within the
Academic Regulations for Taught Provision at the University of
Gloucestershire.
1

Declaration
DECLARATION: This dissertation is the product of my own work and does
not infringe the ethical principles set out in the University’s Guidelines for
Research Ethics. I agree that it may be made available for reference and
photocopying at the discretion of the University.
Signed: M. L. OAK
Name: Michelle Oak
Date: 1st May 2014
Word count: 10, 844
i
Acknowledgements
I would like to take this opportunity to offer my gratitude to my
dissertation tutor, and my placement mentor. This dissertation would not
have been completed without their invaluable advice and guidance.
ii
Abstract Page This study provides an exploration into the how the Total
Communication approach supports the communication difficulties of children
on the Autistic Spectrum. It also explores how the Total Communication
approach is tailored to the individual child. There was a wealth of literature
surrounding the topic, comprising mainly positive aspects of the Total
Communication approach, and the strategies used within. This case study
was conducted within a local Special school, with the principle focus on four
children who have a formal diagnosis of autism, all whom have a variety of
difficulties with their communication. The research methods used to collect
primary data were through observations of the four children, and through
interviews of four practitioners that work closely with the children. The
findings illuminated how the Total Communication was a successful
approach and how it was used for all children in a global sense, as well as
how it was tailored to support the children individually. Suggested
implications for education included understanding the child’s communication
difficulties to enable an individualised version of the approach, as well as
possibly implementing the approach for non-autistic children, whom have
communication difficulties, such as with people with are deaf or have learning
disabilities.
iii

Contents
Declaration....................................................................................................... i
Acknowledgements......................................................................................... ii
Abstract Page................................................................................................. iii
List of Figures.................................................................................................vi
Introduction.....................................................................................................1
Literature Review............................................................................................3
Introduction..................................................................................................3
Overview of Autistic Spectrum Disorder......................................................3
Communication and Autism.........................................................................9
Total Communication Approach................................................................14
Outcome of Literature................................................................................17
Methodology..................................................................................................18
Context......................................................................................................18
Paradigm...................................................................................................18
Data Collection..........................................................................................19
Reliability and Validity................................................................................22
Ethical considerations................................................................................23
Data Analysis and Presentation of Findings..................................................24
Introduction................................................................................................24
Data Analysis Process...............................................................................24
Overall Findings.........................................................................................26
Findings for Child J....................................................................................29
Findings for Child J.M................................................................................32
Findings for Child L....................................................................................34
iv

Findings for Child N...................................................................................36
Conclusion.................................................................................................38
Discussion.....................................................................................................39
Introduction................................................................................................39
Discussion of Child J.................................................................................41
Discussion of Child J.M.............................................................................42
Discussion of Child L.................................................................................43
Discussion of Child N................................................................................44
Conclusion....................................................................................................47
Critique on the research process...............................................................48
Implications for future practice...................................................................50
Implications for further study.....................................................................51
Bibliography..................................................................................................52
Appendices...................................................................................................63
Contents of appendices:............................................................................63
v

List of Figures Figure 1: Continuum of ASD...........................................................................4
Figure 2: Overall observational findings for all children.................................26
Figure 3: Overall type of responses given for all children.............................27
Figure 4: Overall observational findings for Child J.......................................29
Figure 5: Overall type of responses given by Child J....................................30
Figure 6: Overall observational findings for Child J.M...................................32
Figure 7: Overall type of responses given by Child J.M................................33
Figure 8: Overall observational findings for Child L.......................................34
Figure 9: Overall type of responses given by Child L....................................35
Figure 10: Overall observational findings for Child N....................................36
Figure 11: Overall types of responses given by Child N...............................37
vi
Introduction
Autism is a neurodevelopmental disorder which includes the trio of
impairments in social interaction, social imagination and social
communication (Mackenzie, 2008, p19). Communication difficulties are
universally present in individuals with autism (Tavalari, 2004, p13), where
usually a child with autism has difficulties with their receptive and expressive
communication, as well as the difficulty of having the understanding of non-
verbal communicative behaviours (American Psychiatric Association, 1994).
Therefore, communication in children with autism can be seen as a
common difficulty that they encounter. These difficulties will need to be
supported in an education setting, thus practitioners will need to use
strategies and approaches to enable this support (Hollander et al, 2011,
p550). One such approach that could be used is called the Total
Communication approach (Bell, 2011). This approach comprises the
principles of the Communication Bill of Rights 1992 (ASHA, 2014), where
communication is a right to everyone. It enables the child to use a
combination of alternative modes of communication to allow for
communication, thus supporting their communication difficulties (Sanderson,
2011, p6; NHS Cambridgeshire, 2013). Thus, using the Total Communication
approach means ‘a willingness to supplement the spoken word by using
objects, photographs, line drawings, symbols or sign’ (Sanderson, 2011, p6).
However, it is commonly known that children with autism exhibit
difficulties and needs in their communication in various ways, to various
degrees (Kenny, 2012; NHS, 2012). The extent of their difficulties could be
1

seen as a spectrum, where some experience more difficulties than others.
So, the children with these varying difficulties will need an approach that can
be tailored to the individual, to enable for their difficulties to be supported on
an individual basis (Waldock, 2014). It was in the researcher’s interest to
explore whether the Total Communication approach can provide the flexibility
to utilise the approach differently according to the individual’s needs; creating
a person centred approach. This will be conducted in the Special school
setting where the researcher works, to ascertain the value of this approach
with four selected children, whom have a formal diagnosis of autism.
Therefore, the overall aim of this study is to explore the Total
Communication approach, and how this supports and develops the
communication difficulties in children with autism. Accordingly, there are two
specific aims within this study;
1. To explore how the Total Communication approach supports children
with communication difficulties on the Autistic Spectrum.
2. To explore how the Total Communication approach is adapted and
modified to support these children individually.
This dissertation will follow a case study design, providing a review of
literature on autism, communication difficulties with autism, and the Total
Communication (TC) approach. This dissertation will also provide a
methodology outline, an analysis of the findings, and a discussion on these
findings coupled with a conclusion of the study.
2

Literature Review
Introduction
In this section, the literature surrounding autism and the
characteristics that depict autism will be explored. This will then filter down to
autism and communication difficulties, and finally the TC approach.
Overview of Autistic Spectrum Disorder
Definitions and overview
The National Autistic Society (NAS, 2014) and the National Health
Service (NHS, 2012) define autism as ‘a lifelong developmental disability that
affects how a person communicates with, and relates to, other people’. It is
also defined by Landa (2007, p16) as ‘a neurodevelopmental disorder
defined by impairments in social and communication development,
accompanied by stereotyped patterns of behaviour and interest’. It is on the
Autism Spectrum and it is commonly referred to as an Autism Spectrum
Disorder (ASD) (NAS, 2014). The term ‘spectrum’ is used because, while all
people with autism share certain difficulties, ‘the condition affects them
differently’ (NHS, 2012). Autism also shares certain difficulties with
Asperger’s Syndrome, Pervasive Development Disorder – Not Otherwise
Specified and Child Disintegrative Disorder.
3

Figure 1 below illustrates the continuum of ASD:
Figure 1: Continuum of ASD
The NHS highlight that it is a lifelong developmental disability, not a learning
disability or a mental health problem. However, people with autism can have
accompanying learning disabilities and mental health problems (NHS, 201 2).
Prevalence of autism
Statistics from the latest prevalence studies indicate that around 1.1%
of the UK population may have autism (The National Autistic Society, 2014).
This equates to over 695,000 people in the UK (The National Autistic Society,
2014), and around 100,000 of these people are children (The Office of
National Statistics, 2005). These statistics were taken from two relatively
recent prevalence studies on adults (Brugha et al, 2009) and on children
(Baird G et al, 2006, p210). To support this, The Office of National Statistics
(2005) states ‘Autism now affects about one in 100 children… with around
half a million family members directly affected by the condition’. Even though
this was reported in 2005 by the ONS, it can be seen from the triangulation of
research how common autism was previously and in the present.
Alongside this, interestingly, there are ‘five times as many males as
females who are diagnosed with autism’ (The National Autistic Society,
2014). Supporting this Carter (2007, p86) states ‘Autism is three to five times
4

more common in males than in females’. The most recent study by
Fombonne (et al, 2011, p904) found a mean of 5.5 males to 1 female in their
research paper.
Historical context
Autism was first identified by Leo Kanner in a paper published in 1943
entitled ‘Autistic disturbances of effective contact’ (Boucher, 2009, p4;
Mccallister, 2010, p23). He was the first scholar to identify many features of
autism and he ‘captured the three core features of what later came to be
called Autism Spectrum Disorders’ (Thompson, 2007, p2). It was defined as
disturbances of social relationships, limited use of language to communicate
and fixed repetitive routines and interests (Thompson, 2007, p2).
Autism was formally recognised as a condition in 1980, when the third
edition of Diagnostic and Statistical Manual of Mental Disorders (DSM-III)
was published. It was known as ‘Infantile Autism’ and the core impairment
was seen to be language (Boucher, 2009, p10). As autism was thought of in
terms of a physical illness, Kanner would apply autism to the medical model
(Boucher, 2009, p4), where it was thought it was the person’s ‘problem’ and it
should be fixed (Moore, 2002, p402).
Causes of autism: Neurological/ biological and socio environmental causes
‘There is no known single cause for autism, but it is generally accepted
that it is caused by abnormalities in the brain structure or function’ (Autism
Society, 2013). Autism Society (2013) describes how brain scans have
shown differences in the shape and structure of the brain in children with
5

autism, compared to neuro-typical children. A neuro-typical person means
someone who is not on the Autistic Spectrum (Webster, 2010).
Autism also could be holistically developed through links among
heredity, genetics and medical problems (Autism Society, 2013). Sometimes,
there can be patterns of autism or related disabilities within families, which
supports the phenomenon that it could be hereditary causes, and that it has
genetic foundations (Autism Society, 2013). Supporting this, (Bailey et al,
1995) states approximately 92% of identical twins and 10% of fraternal twins
will also have autism (Dodd, 2005, p20). Following on this Dodd (2005, p20)
highlights ‘these findings support the hypothesis that there is a strong genetic
basis to Autism’.
There has been considerable speculation about whether autism could
be caused by ill-parenting (Whitman, 2004, p102). Kanner (1943 in Whitman,
2004, p102) observed parental behaviour with children with autism, and they
appeared to be ‘cold and aloof’. This is known as the ‘Refrigerator Mother
Theory’ (Bernier & Gerdts, 2010, p46). They were more preoccupied with
occupational and personal pursuits than their children, and according to
Bettelheim (in Bernier & Gerdts, 2010, p46), ‘it is the mothers’ coldness that
ultimately results in the child turning inward and retreating to Autism’.
However, there is little evidence to currently support this theoretical stance,
as parents with autistic children are variable in their parenting styles and
characteristics (Whitman, 2004, p102). Also, this does not account for the
parents who have neuro-typical siblings for the child with autism (Bernier &
Gerdts, 2010, p48). Although, Whitman (2004, p102) states that ‘it is not
unreasonable to assume that parents can exert considerable influence on the
6

general development of their children’. The parents who are proactive and
knowledgeable about autism may influence a better development that those
who are less involved. Therefore, this could cause the child with autism to
develop in a different way (Whitman, 2004, p102).
How is autism diagnosed?
Autism is diagnosed based on the features that the individual child is
showing. A team of professionals would carry out assessments on the child
(NHS Choices, 2014). They would be assessed on physical aspects,
behavioural aspects, language aspects and cognitive aspects, as well as
their interaction patterns (NHS Choices, 2014). Once this process is
complete, a diagnosis of ASD would be confirmed (NHS Choices, 2014).
Cure for autism
Currently, there is no known ‘cure’ for autism (TNAS, 2014). However,
interventions can be put in place to help. As more research increases our
understanding of autism, ‘more interventions will undoubtedly become
available’ (TNAS, 2014).
Due to the variable factor of severity in autism, individuals’ intervention
plans should be put in place, which ‘should be tailored to address specific
needs’ (Hutchings, 2013). These intervention plans can involve behavioural
treatments, medicines or both (Hutchings, 2013). Some of these intervention
programmes include playgroups, nursery classes for special needs and
speech and language therapy (TNAS, 2014).
7

Characteristics of Autism
Autism impacts the development of the brain in the areas of
communication skills, social interaction, and cognitive function (National
Autism Association, 2013). Individuals with autism typically have difficulties in
verbal and non-verbal communication, social interactions, and leisure or play
activities (National Autism Association, 2013).
Wing and Gould in 1979 (in Dodd, 2005, p2) created the term ‘triad of
impairments’ to describe a person with autism, as a result of a study they had
conducted on children with autism. The study concluded the three distinctive
impairments of autism as;
An impairment of social interaction/relationships
An impairment of social communication and
An impairment of social imagination
(Dodd, 2005, p2)
Not only did Wing (in Davis, 2013) define autism by categorising the
three characteristics, but she also looked at the behaviours, interests and
activities of people with autism too.
Social Interaction/relationships
The impairment in social interaction and relationships means that the
person with autism will have deficits in understanding how to behave and
interact with other people (Brookdale, 2011). They will have difficulty
recognising and understanding people’s feelings and managing their own
feelings (NHS, 2012). This is supported by the ‘Mind Blindness Theory’ by
8

Baron-Cohen (1997, p1), where he viewed a person with autism as being
‘aware of physical things but were blind to the existence mental things’
(Baron-Cohen, 1997, p1).
Social Imagination
Impairment in social imagination for people with autism will mean a
deficit in ‘flexible thinking regarding interests, routines, perspectives and
rules’ (Brookdale, 2011). They will have difficulty predicting other people’s
behaviours and intentions, as well as imagining situations that are outside of
their routine (NHS, 2012).
Behaviours, interests or actions
Wing (in Davis, 2013) described how people with autism may display
some ‘abnormal behaviours’. Examples of these behaviours could be;
becoming obsessed with a certain topic or object, focusing on routines and
rituals which have no practical function, extra sensitive or under sensitive to
smells, sounds, tastes or textures, as well as repeating actions, like hand
flapping (Davis, 2013).
Communication and Autism
Alongside social interaction, social imagination and behaviours, the
deficits in social communication could be crucial to how a person with autism
interacts, communicates and live their lives on a daily basis. Before exploring
the difficulties that a person with autism may experience when
communicating, it is significant that it is understood what communication
means and how we begin to communicate.
9

What is communication?
The definition of communication has always been unclear and
according to Steinberg (2007, p39), ‘there is little agreement among
communication scholars about a definition’. Communication could be defined
as:
‘Any act by which one person gives to or receives from another person
information about that person's needs, desires, perceptions, knowledge, or
affective states. Communication may take linguistic or nonlinguistic forms,
and may occur through spoken or other modes’
(National Joint Committee for the Communicative Needs of Persons with
Severe Disabilities, 1992, in Matson, 2011, p168)
Additionally, communication could be based on two views: a
technical view and a meaning-centred view (Steinberg, 2007, p39). ‘From a
technical point of view, communication can be defined as the transmission of
messages from one person to the other’ (Steinberg, 2007, p39). This is seen
as the physical act of communicating. Whereas, from the meaning-centred
view of communicating, alongside the transmission of the messages is the
interpretation and meaning. From this perspective, communication can be
defined as ‘a dynamic process of exchanging meaningful messages’
(Steinberg, 2007, p39).
When looking at this view of communication, though the lens of the
definition of autism, it is clear how people with autism can find difficulty
communicating. The definition states how people with autism have deficits in
communicating with people and relating to other people, so in regards to the
10

technical view of communication they may find difficulty with the physical act
of communicating. Additionally, in regards to the meaning-centred view,
people with autism tend to have difficulty understanding and recognising
other peoples’ feelings, as well as understanding what the meaning is
actually put across in a conversation. An example of this could be when
someone is using sarcastic language or if they are metaphorically speaking,
where the person with autism may take what is said literally (Miller, 2006,
p146).
When does communication start?
‘Communication begins long before we learn to talk’ (The Hanen
Centre, 2011). Babies show their interest in communicating by listening
intently, looking at people’s faces when they talk, and engaging in babbling
games with their parents, all in the first few months of life (The Hanen Centre,
2011). These exchanges of sounds and facial expressions are the first
conversations between a baby and parent, ‘even though the baby has never
uttered a word’ (The Hanen Centre, 2011). Infants start to imitate their
parents’ single words and actions, followed by the child starting to use their
first words on their own. Their language acquisition then leads onto two and
three word sentences (The Hanen Centre, 2011).
Verbal and Non-verbal communication and Autism
Having autism can affect communication through the means of verbal
and nonverbal communication to varying degrees. To support this, a study
shows that ‘some children with autism have normal language skills; for other
11

children, their language skills are significantly below age expectations’
(Kjelgaard and Flusberg, 2001, p287).
Verbal communication
Verbal communication can be divided into two main parts; expressive
(output) and receptive language (input). ‘Expressive language is our ability to
convey our thoughts into words with meaning, basically our ability to talk’
(Marrs, 2013). On the other hand, ‘our receptive language is our
understanding of what is being said to us’ (Marrs, 2013) and both of these
skills are needed to become an effective communicator (Marrs, 2013). A
study showed that in pre-schoolers with autism, there was a ‘greater
impairment in receptive compared with expressive language abilities’ (Hudry
et al, 2010, p681). This may possibly be because people with autism tend to
not understand the message that others put across in conversation, and lack
the ability to understand feelings and emotions (NHS, 2012). However,
according to Marrs (2013), ‘very often expressive language is impacted to a
greater degree than receptive language’ in people with autism. Additionally,
they may experience abnormal speech production, difficulty with intonation
and prosodic cues, may not respond to verbal cues, and have a difficulty with
meanings, prepositions, verbs and adjectives (NDCCD, 1998; Loita, 2002).
Supporting the concept of people with autism having expressive and
receptive communication deficits, a study showed that children diagnosed as
autistic had a more deviant language development than non-autistic children,
as well as having a more severe comprehension defect, a more extensive
language disability and also showed a defect in the social usage of the
language they possessed (Bartak et al, 1974, p127).
12

Non-verbal communication
Non-verbal communication involves all behaviours that are not in the
form of words (Guerrero and Floyd, 2006, p4). These behaviours could be
eye contact, body language, gestures and facial expressions (Tassoni, 2003,
p103; Ekman and Frieson, 1969 in Mehrabian, 2009, p1). This mode of
communication could arguably be the most important form. Mehrabian
(1967) created the Communication Model (Mehrabian, 2009, p182). This
shows that communication comprises of 7% of messages pertaining to
feelings and attitudes are words that are spoken. 38% of messages are
paralinguistic (the way that the words are said) and 55% of messages are is
in facial expression. Therefore, ‘facial expressions are the most dominant,
the vocal component ranks second and words are least significant’
(Mehrabian, 2009, p182). Thus, in relation to a child with autism, they may
experience great difficulty when non-verbally communicating, when having to
use eye contact or facial expressions. Tassoni (2003, p103) supports this by
stating ‘Some children with Autism may have difficulties understanding the
non-verbal signs that people send out’.
Supporting the niche of non-verbal deficits in people with autism, Stone
(et al, 1997, p677) conducted a study on children with autism and non-verbal
behaviours. They found that children with autism were less likely to point,
show objects, or use eye contact to communicate, but were more likely to
directly manipulate the examiner's hand. This showed that the children with
autism were less concerned about socially interacting, but were more
concerned to use communication as a tool to fulfil their needs
How do people with Autism communicate?
13

According to The National Autistic Society (TheNAS, 2014), a child
with autism may use different ways to communicate with others. Some of
these methods of communicating include; crying, looking at an object they
desire, reaching, and using pictures, taking an adults hand to the object they
desire and echolalia (TheNAS, 2014).
Echolalia is ‘the repetition of other people’s words and is a common
feature of the child with ASD’ (TheNAS, 2014). According to Roberts (1988)
(Dodd, 2005, p63) it should be seen as a language acquisition strategy, and
research suggests that echolalia is used to assist communication – to make
sense of what others say and to develop functional language skills. Initially,
when the child uses echolalia, it is likely that they are not aware of the
communicative content of the words that they are repeating, however it is
significant to recognise that it is a sign of emerging linguistic awareness, and
not an undesirable behaviour (Dodd, 2005, p63). When in a rich language
environment, the child ‘will begin to use the repeated words and phrases to
communicate something significant’ (TheNAS, 2014), therefore shifting to the
use of the meaning-centred communicative perspective.
Total Communication Approach
As people with autism primarily have deficits with communication,
there are ways to support this. One way could be using the Total
Communication approach (TC). The TC approach is going to be explored, as
well as the research surrounding TC and autism.
What is Total Communication?
14

The TC approach is defined as ‘an approach that requires the
incorporation of appropriate aural, manual and oral modes of communication
to ensure effective communication’ (Northern and Downs, 2002, p366). This
approach was found based on the principles of The Communication Bill of
Rights 1992 (ASHA, 2014), where everyone has a right to communicate
(ASHA, 2014). It ‘involves using any means of communicating’ (NHS
Cambridgeshire, 2013) and requires the use of a range of methods of
communication, as a combination, where some of these methods are
stressed differently for different people depending on their strengths and
weaknesses. A child’s communication needs will change over time, and will
benefit from different modes of communication as a result (NHS
Cambridgeshire, 2013). Supporting this, Waldock (2014) presents the view
that ‘Total Communication means using different ways of communicating
according to each situation and person’. These tools of communication can
be both verbal and non-verbal:
Speech and spoken language
Non-verbal cues: gesture, body language
Makaton signing
Photographs
Symbols: pictures, line drawings and objects
Written words
Song
(NHS Cambridgeshire, 2013; TC, 2014)
‘Makaton signing is a language programme using signs to help people
to communicate’ (The Makaton Charity, 2014). It is used to support spoken
15

language, through a combination of auditory and visual input, and the signs
are used in spoken word order (The Makaton Charity, 2014). Over time, as
the child’s speech develops, they can start to drop off some signs used to
support their speech. Additionally, Makaton can be flexibly used to support
individual needs (The Makaton Charity, 2014). Aarons & Gittens (2001, p73)
suggest that using Makaton signing is good for children with autism, as they
normally respond well to visual strategies, as well as reducing the pressure to
respond verbally.
Additionally, symbols are a way of visually communicating with the
child with autism, and it is recommended that the symbols should be
accompanied by the verbal expression when shown (TC, 2014). They can be
in the form of pictures, objects or line drawings (TC, 2014). They can be used
to develop language, as TC (2014) states ‘using symbols increases language
stimulation and gives a purpose for communication’.
Also, photographs are a visual method of communication with the
child, which is normally used in unison with speech, and sometimes written
words (Hawthorn, 2005). As well as this, song is used as a main purpose to
communicate the start and end of activities to develop awareness (Hawthorn,
2005).
‘50% of persons with autism has insufficient speech to meet their daily
communicative needs’ (Wing & Atwood, in Matson & Minshawi, 2006, p83)
so the ‘mixing and matching of communication methods should be
encouraged to produce optimal communication skills’ (ibid). Studies indicate
that Total Communication results in faster and more complete receptive
16
and/or expressive vocabulary acquisition than does using speech alone, in
children with autism (Yoder & Layton, 1988 in Mirenda, 2003, p204;
Remington, 1983, in Mirenda, 2003, p204). Additionally, the TC approach
appears to be particularly effective with low-verbal children with ASD, who
have poor verbal imitation’ (Lubetsky et al, 2011, p182). A further study
demonstrates the effects of TC in all areas of development, such as
academic, linguistic and psychosocial (Vernon & Andrews, 1990, p10).This
indicates how TC can be used as a successful method for developing
communication
However, the TC approach may have some limitations. Kurtz (2008,
p108) states that while some children with autism learn more easily when
using signed speech, others have trouble associating auditory with visual
symbols, and are best taught using sign alone. Also, another study suggests
that the TC may result in less developed speech skills (Geers and Moog,
1992, p1384).
Outcome of Literature
Reviewing this literature has given the knowledge basis to enable the
identified aims to be fulfilled. It has given a strong theoretical basis and
conceptual framework to work from in regards to autism, communication and
the Total Communication approach. All three entities are going to be
explored in relation to another with the participants of the study
17

Methodology
Introduction
This chapter will outline the context, the participants, the research
paradigm, the research methods, the reliability, validity and the ethical
considerations within this study.
Context
This research project will be conducted within a local special school.
The researcher works within an Early Years class, with eight pupils who have
a formal diagnosis of autism with communication difficulties. Four of these
children have been chosen to participate in this study. Therefore, the non-
probability purposive sampling method to select the participants has been
used for this study (Blankenship, 2010, p86). According to Blankenship
(2010, p86), this type of sampling provides ‘a focused effort in gathering rich
data to answer the research question’… it allows the researcher to identify
specific individuals who have the answer to the research question’
(Blankenship, 2010, p86; Adler & Clarke, 2011, p132). This sampling method
was also used for the four practitioners being interviewed in this study,
because they work closely with the four participants. The profiles of the
participants are in the appendices (Appendix Two).
Paradigm
According to Basit (2010, p14) ‘paradigms are models, perspectives or
conceptual frameworks that help us to organise our thoughts, beliefs, views,
and practices into a logical whole and consequently inform our research
18

design’. There are two types of paradigms in research; the normative
paradigm, and the interpretive paradigm (Basit, 2010, p14; Wimmer and
Dominick, 2013, p11; Kwanjai, 2013).
The normative paradigm focuses on ‘observing, experimenting on, or
interrogating a large number of subjects, resulting in findings that can be
statistically analysed, and therefore believe to be generalizable’ (Basit, 2010,
p14). Alternatively, the interpretive paradigm focuses on ‘smaller and in depth
analysis of human behaviour and perceptions, acknowledging differences as
well as similarities’ (Basit, 2010, p14), usually through the dominant methods
of observations and interviews (Golafshani, 2003, p600).
For this dissertation, the interpretive paradigm has been selected for
research. The justification for this being that this case study will be focusing
on a smaller and in depth analysis of behaviour and perceptions.
Data Collection
The case study approach within the qualitative approach has been
selected for this study. A case study is defined by Yin (2009, p18) as
‘empirical inquiry that investigates a contemporary phenomenon in depth
within its real-life context’. As well as this, a qualitative research approach
could be described as ‘any kind of research that produces findings not
arrived at by means of statistical procedures or other means of quantification’
(Strauss and Corbin, 1990, p. 17). This selection was made to allow for
qualitative research methods to enable the collection of empirical, primary
data. The methods selected for this case study are observations (of the
19

children) and interviews (with the practitioners). Selecting both of these
methods has enabled the findings in this study to gain triangulation.
According to Flick (et al, 2004, p178), ‘the term triangulation is used to
refer to the observation of the research issue from at least two different
points’. The observations will be of the TC approach in practice, and the
interviews will be with the practitioners in the setting who work closely with
the four children. This will display different perspectives of the research
conducted. Golafina (2003, p600) supports the concept of triangulation by
stating, ‘triangulation is typically a test for improving the validity and reliability
of research… it strengthens a study by combining methods’.
Observations
Observations will be taken over a five week period, where all four
children will be observed weekly, equating to twelve observations per child.
Clough and Nutbrown (2012, p54) define observations as simply ‘looking’.
This means ‘looking critically, looking openly and looking for information’
(Clough and Nutbrown, 2012, p54). Using this data collection tool will enable
the ‘opportunity to gather live data from naturally occurring social situations’
(Cohen at al, 2007, p397). This means the researcher will be able to observe
the children communicating and responding to communication methods in
their natural setting.
The observational approach that will be adopted is the ‘inactive and
unknown’ approach, in a naturalistic setting (Newby, 2010, p268). This
means that the data collection will be non-interventionist, as it ‘will not seek to
manipulate the situation or subjects’ (Adler and Adler, 1994 in Cohen at al,
20
2010, p397). The children will be observed in their classroom setting, where
the researcher will be completely detached from the situation. The
justification for this observational approach is to attempt to minimize the
‘Hawthorn Effect’, which means that participants may adjust their behaviour
because they are being observed (Jamison, 2006, p27; Newby, 2010, p122).
The observations will be semi-structured which means that these
observations ‘will have an agenda of issues, but will gather data to illuminate
these issues in a far less predetermined manner’ (Cohen at al, 2010, p397).
The researcher will be looking for communicative engagement with the
strategies used within the TC approach between the practitioner and each
child. These will be recorded through taking field notes which are ‘brief notes
during the observation, and then later expand the account of the observation
as field notes’ (Ary et al, 2013, p463).
Interviews
Interviews will be conducted with the practitioners following the five
week observation period. This method has been selected because it could
‘be used to collect facts… the questions seek to elicit information about
attitudes and opinions, perspectives and meanings’ (Hannan, 2007).
The chosen four practitioners, who work closely with the four children,
will be interviewed using a semi-structured interview. This means that there
will be a set list of questions (Appendix Three), with the ability to allow for
flexibility of additional questions or topics to be raised and discussed
(Hannan, 2007). These interviews will be recorded using an audio recording
21

device, which the participants will be made aware of before the interview
commences.
Reliability and Validity
According to Cohen (et al, 2007, p133), ‘validity is an important key to
effective research… if a piece of research is invalid then it is worthless’, thus
it is a requirement to any body of research. Validity could be defined as the
extent to which a research procedure measures what it is supposed to
measure, through the honesty, depth, richness and scope of the data
achieved, the participants approached and the extent of triangulation (Cohen
et al, 2007, p133; Bronfenbrenner, 1979, p29). In attempt to build out
invalidity, precautionary measures were taken. Firstly, the appropriate
qualitative research methods were selected for collecting data to answering
the research questions. Also, a multi-method approach will be used, to
triangulate findings. Additionally, appropriate clear aims have been selected
for the study (Cohen et al, 2007, p144).
Alongside this, the reliability of research is significant. Lincoln and
Guba (in Cohen et al, 2003, p148) prefer to replace the term ‘reliability’ in
qualitative research with ‘credibility’ or ‘dependability’. This is because
LeCompte and Preissle (in Cohen et al, 2003, p148; Thompson, 2010)
suggest that the canons of reliability for quantitative research may be simply
unworkable for qualitative research, as in qualitative research we are not
looking at scientific and statistical findings, but meanings instead. It has been
attempted to enhance the credibility of this research study by attempting to
standardise the data collection techniques. Also, by using the same basic
22

question protocol for the semi-structured interviews, and using the same
conceptual framework when observing the participants.
Ethical considerations
Good ethical practice and principles are a vital part to any form of
research. According to the University of Gloucestershire ‘the primary
responsibility for the conduct of ethical research lies with the researcher’
(University of Gloucestershire, 2008). Thus, to ensure ethical research,
ethical guidelines were present throughout the planning, implementing and
analysing procedures of this research project. It was vital that adherence to
the British Educational Research Association (2011) and University of
Gloucestershire guidelines (2008) ethical guidelines was ensured.
Under these guidelines, there are general responsibilities towards the
participants within ethical research. This includes; obtaining informed
consent, ensuring confidentiality and anonymity, informing the participant of
the ability to withdraw at any time and fully informing the participant on the
research to avoid deception (University of Gloucestershire, 2008).
It was the responsibility of the researcher to conduct a letter of
consent to obtain informed consent from the parent or guardian of the four
children (Appendix Four). A letter of consent was also conducted for the
practitioners in the setting to be interviewed (Appendix Five). This letter
displayed all of the relevant ethical guidelines applicable to this study.
23

Data Analysis and Presentation of Findings
Introduction
In this chapter, there will be a representation of the findings from the
observations and interviews that were conducted in this study. The global
observational findings of all children will be presented in graphs first, coupled
with a description of the findings. Then, the global interview findings of all
children will be described secondly. Following this, the totalled observational
findings will be presented in graphs and the interview findings will be
displayed individually for each child.
Data Analysis Process
Observations
It is important to gain an insight of the analysis process of the
observation data. Firstly, raw data was collected through field notes and
these were written up into twelve separate observations for each child, for
examples, see appendix six. Following this, these observations were coded
using a framework of strategies within the TC approach. These were:
Makaton signing, speech, symbols, photographs, non-verbal cues, written
words and song. In this study, the ‘symbols’ strategy was the use of basic
drawings to symbolise something, for example a drawing of a toilet. Also,
non-verbal cues included using gesture, hand/body movements, eye-contact,
facial expression and pointing (Tassoni, 2003, p103). The coding was
carried out for two purposes: to examine how many times the practitioner
used each strategy, and to see how many times the child would engage with
24

each strategy. This coding was then accumulated for each individual child, to
provide the overall representation that child.
Secondly, the type of responses from each child was explored. This
was to see how the child would respond to the strategies. This was coded by
the type of response the child gave which fell into three categories: verbal,
non-verbal and song. Verbal was identified as any form of speech used. Non-
verbal communicative behaviours included any form of gesture, body
movement, eye-contact, facial expression or pointing that indicated the child
was engaged. Also, song was identified as any form of singing that displayed
the child’s engagement.
Finally, the both sets of coded data were then accumulated for all
children, to provide a global perspective of the engagement of all children
and the general type of response that all the children gave.
Interviews
For the interviews, the data analysis process is as follows. Firstly, raw
data was collected from the practitioners, through four semi-structured
interviews, using an audio recording instrument to document this. These
interviews were targeted to the individual, through asking the same set of
questions, but with a focus on a particular child. These interviews were then
transcribed, followed by the needless data being rejected, revealing the main
findings of the interviews. The principal findings were extracted from the
interviews as an overall depiction, as well as looking at the findings for each
individual child.
25
Overall Findings
Overall observational findings
Firstly, the accumulated findings from all of the observations are
presented in Figure 2 below;
26

Figure 2 illustrates that the method used mostly within the Total
Communication approach was speech at 186 times. This received 126
responses (68%). Secondly, non-verbal cues were the second most used
method for communicating; it was used 104 times by the practitioners and
was responded to 82 times. In comparison to speech, this received a high
engagement rate of 79%. Thirdly, Makaton signing was the third most used
method of communication; it was used 42 times overall. This method
received engagement 34 times (81%).
Also, written words, photos and symbols were mainly used in unison
with each other, which all received a high response rate. Written words were
used 11 times, and were responded to 10 times, thus an engagement rate of
90%. Photos were used 10 times, and were responded to 9 times; giving an
engagement rate of 90%. Also, symbols were used to aid communication 12
times and received a response rate of 11 times; so again, this strategy
received a response rate of 90%. Additionally, song was used 5 times as a
method of communication, and received a response rate of 90%, thus it was
unsuccessful in one situation.
Therefore, it appears that speech, non-verbal cues and Makaton
signing were the main methods of communication used by the practitioner,
followed by symbols, written words, photos and song. The engagement rates
were high for most methods, apart from speech. However, speech is used in
27

unison with most methods, thus possibly meaning that using speech
independently as a method is not engaging for the children.
Figure 3 below illustrates the type of response that the child
participants gave to the methods used by the practitioner in Figure 2;
There were a total of 276 responses to 370 situations from the entire
48 observations from all child participants; thus a 75% response rate from all
children. These were divided into verbal responses, non-verbal responses
and responses by singing. Firstly, the child participants mostly responded to
the methods in Figure 2 non-verbally; 72% of the time. Secondly, the child
participants responded to the methods using verbal expression; 27% of the
time. Additionally, in one instance a child participant responded using song.
Overall interview findings
28
Figure 3: Overall type of responses given for all children
When examining the four interviews for general principal findings, the
themes that have emerged are: the effectiveness of the TC approach when
using it with the children, what methods are used to support the children’s
communication difficulties, and how this develops the communication skills of
the children.
All four interviewees appear to communicate positive aspects of the
TC approach, and the significance of it ‘I think it (TC) is essential really, if
we’re going to communicate’ (Interviewee Three). Additionally, all
interviewees highlight that a range of methods are used, which are
differentiated and adapted to suit the needs of the child ‘TC takes in every
aspect of the child’s communication and it is about us changing what we do
which is led by the individual child’ (Interviewee Two). They all appear to be
in agreement that it is a mixed method approach used, where some methods
are stressed more or less depending on the child ‘obviously we do use
gesture, Makaton signing, it’s because they’re visual learners’ (Interviewee
Two), also ‘it could be methods of communication like speech, using
symbols, signing, gesture, and it also depends on each child with what
method you use’ (Interviewee Four). They highlighted the importance of the
methods used to enable appropriate support for each child, depending on
their communication requirements. They all also relish on how the TC
approach has successfully supported the children, enabling progression and
development in their communication ‘more speech is being used now’
(Interviewee One) and ‘we have seen big progress’ (Interviewee Two).
Findings for Child J
Observational findings
29

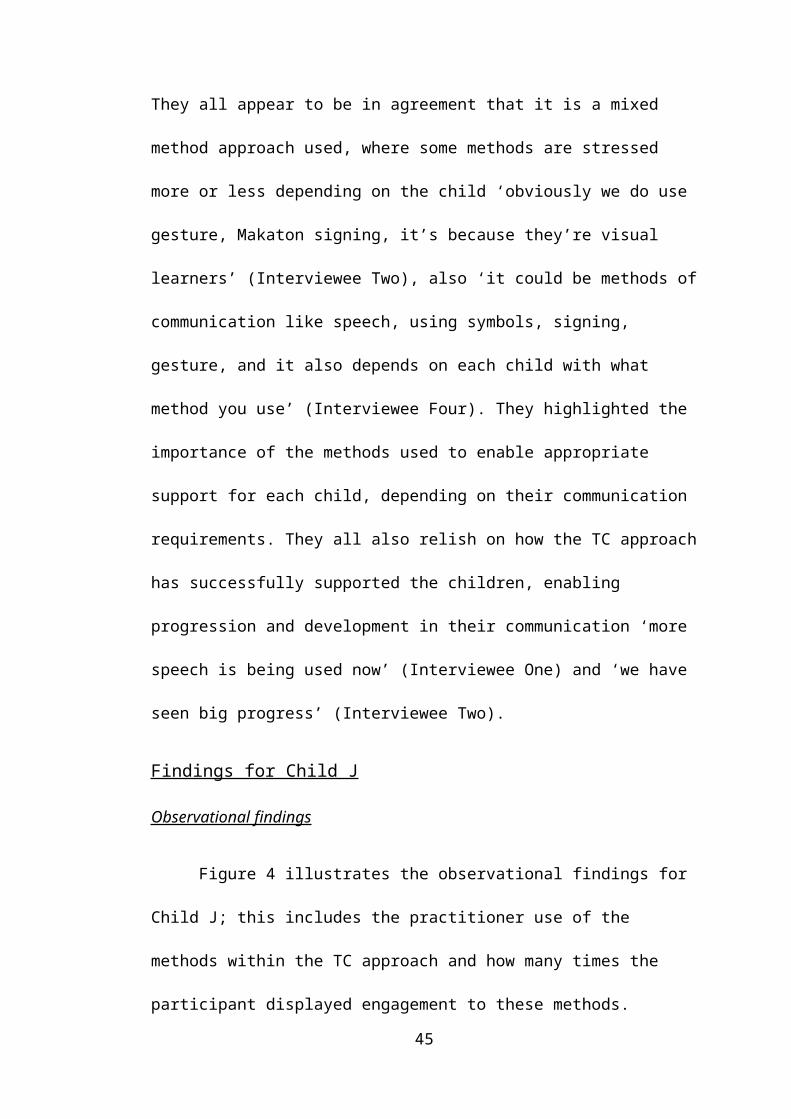
Figure 4 illustrates the observational findings for Child J; this includes
the practitioner use of the methods within the TC approach and how many
times the participant displayed engagement to these methods.
30
Figure 4: Overall observational findings for Child J

Figure 4 illustrates that Child J responded to speech 30 out of 47
times, this was 63% of the time. Non-verbal cues were the second most used
method, where Child J displayed engagement 20 out of 30 times; this was
66% of the time. Following this, Makaton signing was the thirdly most used
method by the practitioner, where Child J responded 12 out of 14 times, thus
a high response rate of 86%. Additionally, following this was song, where he
responded both times that it was used, and then symbols were the least used
method of communication, where he responded to the one situation it was
used.
Figure 5 displays the type of responses given to the methods in Figure
4. Child J gave 66 responses, and these are divided into verbal, non-verbal
and song. Child J mainly used non-verbal means of communication as a
31
Figure 5: Overall type of responses given by Child J
response to the practitioner, as he used this method 60% of the time. Child J
also would respond using verbal expression at 38%. Child J also responded
by singing on one occasion (2%).
Interview findings
Principal findings that have been extracted from the interviews are his
communication needs and difficulties, how his needs are supported, and the
effectiveness of the TC approach when supporting and developing his
communication.
The interviewees highlighted that he has communication difficulties as
a result of both his formal diagnosis of autism, as well as using English as an
additional language (EAL) (DEECD, 2013), ‘Child J’s first language isn’t
English, so it has been quite difficult to understand what he wants’
(Interviewee One), and that his expressive abilities are particularly poor due
to his autism and the ‘barrier of language’ (Interviewee Four). It was
highlighted that the TC is essential for communicating with him, ‘it’s essential
to get any joint understanding and co-operation with Child J’ (Interviewee
Three), and that methods used were very visually based ‘Child J responds
well to picture materials, symbols, photographs, facial expression and
gesture’ (Interviewee Three). They state how the approach has been shifted
to a more language rich environment where ‘I have used increasingly more
language’ (Interviewee Three) to develop his expressive abilities where he is
listening, understanding and using speech more now. Although, the speech
is usually imitating practitioner’s words, and very minimal language use. The
Total Communication has been essential for his language development as
32

‘he is using more speech now’ (Interviewee One) and ability to communicate,
‘his communication has definitely developed’ (Interviewee Four).
Findings for Child J.M
Observational findings
Figure 6 illustrates the observational findings for Child J.M; this
includes the practitioner use of the methods within the TC approach and how
many times the participant displayed engagement to these methods.
Figure 6 illustrates that the practitioner uses speech as a main mode
of communication with Child J.M, where he showed engagement 35 out of 43
times; thus a response rate of 81%. Secondly, non-verbal cues received
engagement 26 out of 31 times, thus a response rate of 84%. Additionally,
Makaton signing was received engagement 10 out of 15 times; thus
33
Figure 6: Overall observational findings for Child J.M

engagement rate of 67%. Also, song received engagement 2 out of 3 times
and symbols were successful in its one use.
Figure 7 illustrates how Child J.M responded to the methods outlined
in Figure 6. Child J.M mainly used non-verbal expression 65% of the time as
a response. In comparison, Child J.M used verbal expression 35% of the
time as a response. Therefore, this demonstrates that Child J.M could be
very non-verbal based in this communication to the practitioner.
Interview findings
Main findings that have been extracted from the interviews about Child
J.M are his communication difficulties, how his difficulties are supported, and
the effectiveness of the TC approach when supporting and developing his
communication.
The interviewees appear to be aligned when expressing their thoughts
on Child J.M’s communication difficulties. He firstly had poor expressive
abilities when he joined the school, where ‘his speech was unclear and quite
34
Figure 7: Overall type of responses given by Child J.M

difficult to understand’ (Interviewee One), and as a result the practitioners
‘halved the amount of language used, emphasised sounds, and got his
listening primed for sounds’ (Interviewee Three). They found this approach to
be effective as ‘he uses a lot more clear speech now’ (Interviewee Four)
since starting school.
It was also found that Child J.M has poor receptive abilities ‘he has
issues with storing things in his head and understanding’ (Interviewee Three).
Thus, the interviewees highlighted that they give him time to digest
information, and time to respond ‘he always needs time to think about it, to
process it’. This has been successful when supporting his communication
difficulties because when asked, Interviewee One and Three agreed that it
has supported and developed his communication skills.
Findings for Child L
Observational findings
Figure 8 illustrates the observational findings for Child L; this includes
the practitioner use of the methods within the Total Communication approach
35

and how many times the participant displayed engagement to these
methods.
Figure 8 illustrates that Child L responded to speech 37 out of 63
times, which was 59% of the time. Non-verbal cues were the second most
used method, which were responded to almost every time at 90%. Then,
Makaton signing was the next most used method, which was responded to
also at 90% of the time.
Figure 9 illustrates the type of responses that Child L gave as a
response to the methods used by the practitioners in Figure 8. Child L mainly
used non-verbal cues as a communicative response 83% of the time. This
means that he used verbal expression only 17% of the time as a response.
Interview findings
36
Figure 9: Overall type of responses given by Child L

Main findings that have been extracted from the interviews about Child
L are his communication difficulties, how his difficulties are supported, and
the effectiveness of the TC approach when supporting and developing his
communication.
The interviewees were all in alliance when discussing Child L’s
communication needs, and how these are supported. When Child L started
school, his expressive abilities were poor, ‘when he first came to class, he
wasn’t using any language’ (Interviewee One), but Interviewee Three states
how they used visual based methods to ‘allow him to have options, which has
taken the pressure off his verbal expression’ (Interviewee Three). She also
claims that by using this approach, it has ‘caused him to use more language’
(Interviewee Three). As a result of this increasing verbal communication,
Interviewee Three states how they ‘are using less gesture, less Makaton
signing and increasing the use of verbal communication’.
Findings for Child N
Observational findings
Figure 10 illustrates the observational findings for Child N; this
includes the practitioner use of the methods within the Total Communication
37
approach and how many times the participant displayed engagement to
these methods. Figure 11 displays the type of responses given.
Figure 10 illustrates that Child N responded to speech 24 out of
33 times giving a response rate of 73%. Alongside this, non-verbal cues were
responded to 8 out of 12 situations (67%), as well as written words was
responded to 10 out of 11 times (90%). Also, symbols and photos were both
responded to 9 out of 10 times (90%). Makaton signing was a successful
method of communication, as this received a response rate of 100%.
Figure 11 illustrates the type of responses that Child N gave as a
response to the methods used by the practitioners in Figure 10. Out of 66
responses, Child N gave a total of 53 non-verbal responses (80%), and 13
verbal responses (20%). This demonstrates that Child N can be very non-
verbal in his communication.
Interview findings
38
Figure 11: Overall types of responses given by Child N

Principal findings that have been extracted from the interviews about
Child N are his communication difficulties, how his difficulties are supported,
and the effectiveness of the TC approach when supporting and developing
his communication.
Interview findings state that Child N has difficulties with his non-verbal
communication, as well as his expressive communication abilities ‘he was a
child, who used no language, and he would scream or take us to what he
needed’ (Interviewee Two). So, to support these difficulties, the interviewee
stated ‘we are using a mixture of photos, symbols and written words, as well
as gesture and Makaton signing, because he is a visual learner’ (Interviewee
Two). This approach has enabled him ‘to use a lot of language now, so it
(TC) works very well’ (Interviewee Two). Therefore, the TC approach has
been very effective for him ‘we have seen big progress from Child N, and it’s
through using the Total Communication approach’ (Interviewee Two), and
has enabled him to verbalise more ‘he is verbalising more, and he
understand a lot more vocal language’ (Interviewee Two).
Conclusion
To conclude, this section has offered a representation of the
observational data, displaying the findings from the child participants globally,
and on an individual basis. This chapter has also offered an insight to the
findings from the interviews for the children on an individual basis. These
findings have given the evidential basis to pursue further with a discussion on
each child participant with regards to the aims set out in the study.
39

Discussion
Introduction
This chapter is going to present a discussion, which will synthesise the
findings and the relevant literature in relation to the initial aims set out in the
study. It will follow the format of discussing the children globally; by looking at
the TC as a universal concept with all of the children. Following this, this
chapter will provide a discussion of the children individually, and how the TC
is differentiated and adapted to the children on an individual basis.
Global discussion of the TC approach with all four children
Whilst all children presented a variety of communication difficulties,
the TC approach appears to be a successful universal approach for all of the
four children. This is reflected in all four interviews, where the practitioners
tend to express the positive aspects of the TC approach, and how it has been
successful for all four children, ‘we have seen big progress, it’s through using
the Total Communication approach’ (Interviewee Two). This aligns with the
suggestion by Yoder and Layton (in Mirenda, 2003, p204), who indicate how
TC can be used as a successful method for developing communication in all
children with autism.
It is apparent that the practitioners use a similar framework of the TC
approach to support all of the children, which is then adapted to suit the
child’s needs. From drawing in the observation data, as well as the interview
findings, it is evident that all four children receive a mixed method approach,
where methods are stressed more or less depending on their individual
circumstances (NHS Cambridgeshire, 2013). This is essential as Wing and
40

Attwood (in Matson and Minshawi, 2006, p83) state ‘the mixing of
communication methods should be encouraged to produce optimum
communication skills’, which can be both verbal and non-verbal (Waldock,
2014). This is something that the practitioner’s viewed as an essential part of
TC, which then relieves the pressure to communicate using just verbal
expression (Interviewee Three) which aligns with the suggestion by (Aarons
& Gittens 2001, p73).
It is also apparent that all of the practitioners use a language rich
environment, something that The National Autistic Society (2014) endorses.
Additionally, it is also evident that the TC approach is very visually based for
all four children. This is reflected in the observational data, where all children
particularly receive Makaton signing, as well as other visual strategies (child
dependant). This aligns with the interview findings as Interviewee Two states
‘the children are visual learners’. To support this, Aarons and Gittens (2001,
p73) suggest that using Makaton signing is good for children with autism, as
they normally respond well to visual strategies.
Thus, it appears that the practitioners use the TC approach as a
successful method to support the children’s communication difficulties in a
global sense, where a similar framework is used for all children. Therefore,
this part of the discussion fulfils the first aim of this study ‘to explore how the
TC approach supports children with communication difficulties on the Autistic
Spectrum’.
However, it is also evident from the findings in this study that the TC
approach is adapted and modified to support these children individually,
41

which supports the notion by Waldock (2014), ‘TC means using different
ways of communication according to each situation and person’. The
discussion will now progress onto looking at the children’s difficulties and
how they are supported individually.
Discussion of Child J
Child J presents difficulties with his communication, as a result of two
factors: he has a formal diagnosis of autism, and he is Polish, so English is
used as an additional language (EAL) (DEECD, 2013). He mainly has
difficulties with his verbal communication, in both subsets of receptive and
expressive language, but particularly his expressive language, which are
both skills needed to be an effective communicator (Marrs, 2013). This is
reflected in the observation findings, where his type of response was mainly
non-verbal (66%).
The expressive difficulties presented in Child J are supported through
the use of the TC approach. The practitioners have used a mixed-method
approach with Child J, mainly focusing on speech, song, Makaton signing
and non-verbal cues. Non-verbal cues and Makaton signing were particularly
stressed for him as reflected in the observations, which consequently have
attempted to support his impaired expressive abilities (TheNAS, 2014).
The practitioners described in the interview how they used a very
visual based approach with Child J, but have recently moved onto creating a
more language rich environment for him. Thus, as a result of his progression,
they have adapted the methods used to support his communication
difficulties (Waldock, 2014).
42

As a result, Child J’s language developed, where his verbal
expressions were presented usually as one word sentences and through
using very simple language, usually as a result of imitation of the practitioner.
Therefore, Child J was demonstrating the use of echolalia, which is ‘a
common feature of a child with ASD’ (TheNAS, 2014). Thus, this has enabled
Child J to communicate through the technical view of communication, where
he can transfer a message to another (Steinberg, 2007, p39). This aligns with
the view by Lubetsky (et al, 2011, p182), where the TC approach is
particularly effective with low-verbal children.
Discussion of Child J.M
Child J.M principally presents communication difficulties with his
expressive and receptive abilities, which are both delayed. His expressive
abilities are greater than his receptive abilities however, which aligns with the
study conducted by Hudry (et al, 2010, p681).
In theory, due to his poor receptive abilities, Child J.M may have
difficulty communicating with a meaning, thus through the meaning-centred
view of communication, he may not understand communicative messages
(Steinberg, 2007, p39). However, the observational findings suggest
otherwise, as Child J.M responded 74 times to 93 communicative situations.
This means that he is demonstrating possibly good receptive abilities. This
may be as a result of the change in the approach used by the practitioners to
support him. Interview findings suggest that Child J.M had poor receptive
abilities when he joined the school, so the practitioners halved the language
used, and presented more processing and response time for Child J.M, thus
supporting and improving his receptive abilities. Additionally, they used
43

Makaton signing and non-verbal cues strategies in unison with speech to
reinforce ‘optimal communication skills’ as a result of a mixed-method
approach (Wing and Atwood, in Matson and Minshawi, 2006, p83).
Additionally, Child J.M’s expressive delay is evident in the
observational findings. Out of 93 communicative situations with the
practitioner, Child J.M responded using speech only 26 times. This may
mean that his expressive abilities are still developing. When he uses speech,
it is usually very minimal and unclear, by mainly using two or three word
sentences and this is an important stage of a child’s language acquisition
(The Hanen Centre, 2011). To support his expressive communication
development, the practitioners used a very verbal based approach, using
only literal speech, with his listening primed for clear sounds. This aligns with
the statement by Loita (2002), that children with autism have difficulty with
non-literal speech. As found in the interviews, this has been successful for
supporting his speech, as the practitioners expressed that he is using more
clear speech now. Thus, a verbally based mixed-method approach is a
supportive approach to communicating with Child J.M, and for supporting and
developing his communication difficulties.
Discussion of Child L
Child L presents communicative difficulties with mainly his expressive
abilities, which is not unusual in children with autism (Marrs. 2013). He only
uses language in a minimal sense to convey his needs, and initially it was not
for any social purposes (Bartak et al, 1974, p127).
44

To support his poor expressive abilities, the practitioners used a very
visual approach (Interviewee Three), as evident also in the observational
findings. They mainly used Makaton signing and non-verbal cues in unison
with speech. They also had previously used symbols and pictures, before his
language started to develop, which are methods that have now been faded
(Interviewee Three). This aligns with the suggestion of how methods should
be adapted to suit the individual’s need (Waldock, 2014) which will enable
development. They then moved on to creating a language rich environment
for him, thus exposing him to more sounds and vocabulary (The National
Autistic Society, 2014). Interviewee Three also stated how they dropped off
some Makaton signs, to be replaced with speech, which is seen as a
developmental progression (The Makaton Charity, 2014).
The adapted TC approach, where the practitioners moved from a
heavily visual based approach, to an approach which is now dominantly
speech, Makaton signing and non-verbal cues, is a successful way to support
Child L’s communication difficulties. He now uses more verbal expression,
where he uses speech to communicate for more reasons than to just fulfil his
needs (Interviewee Three). Thus, he is now communicating through the
meaning-centred view of communication (Steinberg, 2007, p39), with some
social elements to his communication.
Discussion of Child N
Child N principally presents difficulties with his non-verbal
communication, and with his expressive abilities. This means that not only
does he have difficulty with verbal expression, but he has difficulty
communicating with non-verbal cues and behaviours, which is arguably the
45

‘most important form of communication’ (Mehrabian 1967). This comprises
55% of all communication according to the Communication Model by
Mehrabian (1967). Thus, Child N may have difficulty communicating
meanings (Steinberg, 2007, p39; Tassoni, 2003, p103), and instead will
manipulate the practitioner’s hand to his needs (Interviewee Two). This aligns
with the study by Stone (et al, 1997, p677).
To support these communication difficulties, it is evident that the
practitioners use a wider range of methods within the TC approach to
communicate with him, to accommodate both his poor non-verbal
communication and his expressive abilities. The practitioners used some
methods in unison, to reinforce meanings and aid understanding (TC, 2014),
such as written words, symbols and photographs (Interviewee Two). The
practitioners also used Makaton signing, speech and non-verbal cues with
Child N. Thus, his approach is very visually based with the support of some
language. Interviewee Two states that this approach is progressive, and so
when Child N develops more language, then some methods will be dropped,
as the child’s communicative needs will have changed (NHS
Cambridgeshire, 2013).
This methodological approach with Child N has been a successful way
to support and develop his communication skills, particularly his expressive
abilities (Interviewee Two). The mixture of methods has offered him both
verbal and non-verbal means of communicating to encourage him to
‘produce optimal communication skills’ (Wing and Attwood, in Matson and
Minshawi, 2006, p83). Also, his development aligns with the statement by
46
Lubetsky (et al, 2011, p182), where this approach is particularly effective with
low-verbal children with ASD.
Therefore, it is evident that the children have all moved through
progressive stages at different degrees, when being supported by the TC
approach. It is clear that all of the children were initially supported heavily
through visual based strategies to enable them to communicate through
alternative ways to speech, which consequently has enabled them to develop
their verbal abilities alongside using visual aids. It can be seen how this is
done on an individual basis for each child, where the TC is modified and
differentiated to support the individual. Therefore, this part of the discussion
fulfils the second aim of this study ‘to explore how the Total Communication
approach is adapted and modified to support these children individually’.
47

Conclusion
The purpose of this chapter is to offer a summary of the study and
examine the understanding that has been gained, as well as to relate back to
the identified aims. This chapter will then offer a critique on this research
process, by examining the strengths and limitations that may have impacted
on the research. Following this, there will be an insight of the implications for
future professional practice and the implications for further study.
This case study aimed to explore the Total Communication approach,
and how this approach supports the communication difficulties in children
with autism. Accordingly, this led to two specific aims within the study:
1. To explore how the Total Communication approach supports the
children with communication difficulties on the Autistic Spectrum
2. To explore how the Total Communication approach is adapted and
modified to support these children individually.
It is felt that the aims in this research study have been achieved. The
findings in this study have offered an evidential basis to suggest that the TC
approach has been positively effective when supporting the communication
difficulties of the four children in this case study, and this has also been
explored into how this approach supports the children globally, thus
achieving the first specific aim. Additionally, the findings of this case study
enabled the exploration of the four children with an individual focus, by
looking at how the TC approach is modified and adapted to differentiate
between the four children, and to support their communication difficulties on
48
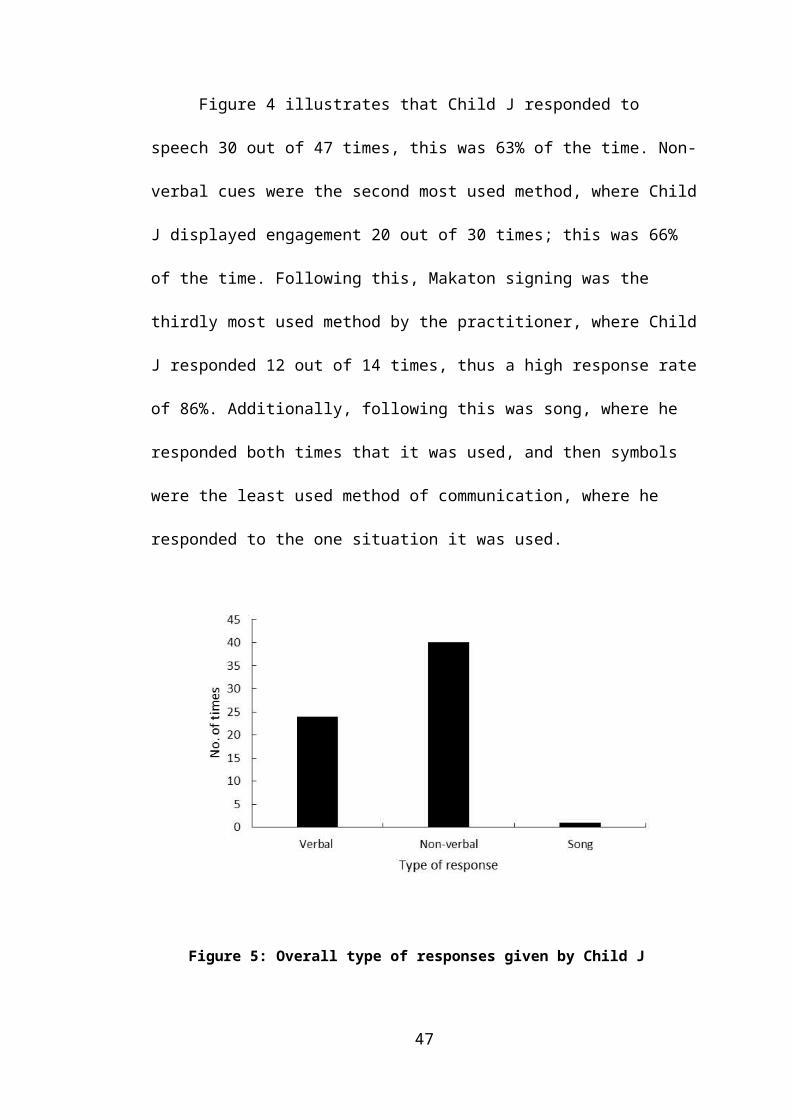
an individual basis. Therefore, this has enabled the second specific aim of
this study to be achieved.
This research process has offered the understanding that the TC
approach is an appropriate approach to enable children with autism, whom
have an array of communication difficulties, to communicate in a variety of
ways. The offer of alternative modes of communication appears to have a
positive effect on supporting the individual’s communication difficulties, which
has consequently developed all four of the children’s communication skills to
separate extents. Thus, conclusions could be drawn that the TC approach
could be an effective method to use when supporting the communication
difficulties in children with autism, something that is strongly reflected in the
surrounding literature (Yoder and Layton, in Mirenda, 2003, p204;
Remington, 1983, in Mirenda, 2003, p204; Wing and Atwood, in Matson and
Minshawi, 2006, p83). Using the TC approach to support communication
difficulties in children with autism could also be a recommendation as a result
of this research project.
Critique on the research process
This small scale case study was chosen to focus on four children who
had the formal diagnosis of autism, whom all have a variety of
communication difficulties. Adopting the case study method has enabled the
collection of unique data, to explore a particular phenomenon (Wallace,
2006, p161). However as the research was conducted on a small scale due
to time restraints, the collection of in depth data is questionable (Hodkinson
and Hodkinson, 2001, p9). Using a case study approach also lends itself to
the lack of ecological validity, meaning that the findings are not generalizable
49

in a conventional sense, and typical claims cannot be made (Hodkinson and
Hodkinson, 2001, p9). Although, it is possible to generalise that the TC
approach may be a suitable approach to adopt for all children with
communication difficulties, regardless of whether they have a formal
diagnosis of autism or not.
The first research instrument to gather data was observations. The
main strength of using this method was ‘the direct access to the social
phenomena under construction’ (University of Strathclyde, 2014). This
enabled the collection of first hand raw primary data. Additionally, using the
observational ‘inactive and unknown’ approach (Newby, 2010, p268) ensured
the limitation of the ‘observer effect’, where the ‘Hawthorn effect’ (Jamison,
2006, p27; Newby, 2010, p122) was minimised due to the unobtrusive nature
of the observations.
However, the principal limitation of using this research method is that
the data is susceptible to observer bias, where the observer may display
subjectivity (Szarkowicz, 2006, p22). This can undermine the reliability of the
data collected, and thus impact on the validity of the findings (University of
Strathclyde, 2014).
The second research method to gather data was semi-structured
interviews. The main strength of using this method was the flexibility of
questioning that enabled the exploration of more in-depth answers (Mitchell
and Jolley, 2007, p302; Hannan, 2007). This allowed for elaboration and
further investigation, however, this further exploration is susceptible to
interviewer bias, where the interviewer can have an influence on the
50

participants answering (Mitchell and Jolley, 2007, p291). Therefore, the
reliability of the findings may have been affected, which may have had an
impact on the validity of this study.
Therefore, the research process behind this case study holds both
strengths and limitations, which may have impacted on the reliability and
validity of this research body. The combining of the two research instruments
have enabled triangulation on the findings, and thus, this has attempted to
build out the unreliability and invalidity of this research, by offering different
data perspectives (Golafina, 2003, p600; Flick et al, 2004, p178).
Implications for future practice
Firstly, this research project offers the literature to enable a
practitioner an understanding on autism, and the characteristics that manifest
themselves in children with autism. The literature also offers an insight to the
array of communication difficulties that children with autism may exhibit.
Carrying out this research has highlighted the importance of supporting
children with autism, whom have communication difficulties (ASHA, 2014),
and how this can be supported; through the TC approach. Thus, this
research project offers an insight to how the TC approach is used to support
the children, and how it is differentiated to support the children’s individual
needs. It can be hoped that this study is a valuable addition to the existing
body of research in this field.
The findings from this research could be applied in professional
settings to advise practitioners of the importance of offering alternative
modes of communication (NHS Cambridgeshire, 2013) when supporting the
51
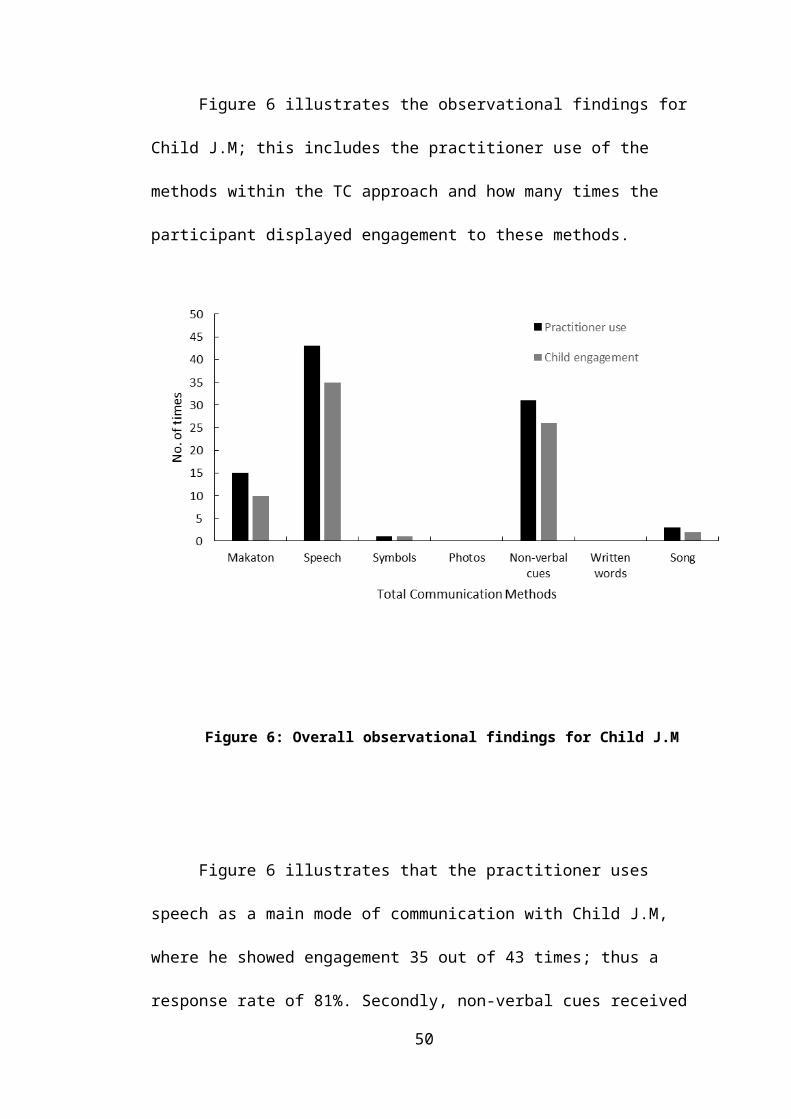
communication difficulties of children. The findings could also possibly reach
out to supporting children who do not have a formal diagnosis of autism, but
do have communication difficulties, such as deaf people (Branson and Miller,
2002, p215), EAL children or people with learning difficulties (Cameron and
Murphy, 2002, p105). Additionally, the understanding gained from this
research could offer advice on how to implement the TC approach on an
individual basis for children, where their communicative needs are targeted
and supported.
Implications for further study
As this research process was conducted over a short period of time, it
can only offer a small scale insight of the developmental process of the
children’s communication. Thus, if the opportunity for further study on this
research project was available it would be interesting to explore the TC
approach over a larger scale of time, to examine the true benefits of the
approach when supporting the children, and to explore the developmental
extent of the children as a result of this support.
52
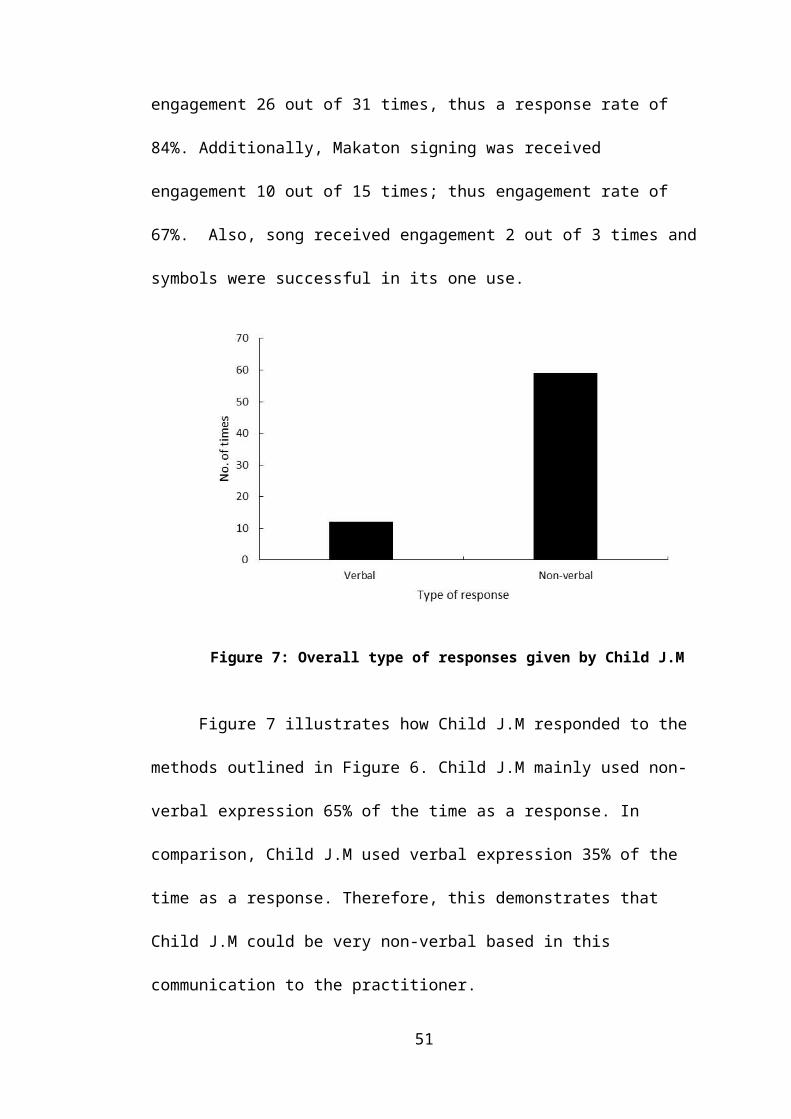
Bibliography Aarons, M & Gittens, T (2001). The Handbook of Autism: A Guide for
Parents and Professionals. 2nd ed. London: Routledge. p73.
Adler, E & Clarke, R (2011). An Invitation to Social Research. USA:
Wadsworth Cengage Learning. p132.
American Psychiatric Association (1994): Diagnostic and Statistical
Manual of Mental Disorders, American Psychiatric Association. 4th
edition, Washington DC:
Ary, D. Jacobs, L. Sorenson, C & Walker, D (2013). Introduction to
Research in Education. 9th ed. London: Cengage Learning. p463.
ASHA. (2014). Communication Bill of Rights. Available:
http://www.asha.org/NJC/bill_of_rights.htm. Last accessed 19th Jan 2014.
Autism Society. (2013). Causes. Available: http://www.autism-
society.org/about-autism/causes/. Last accessed 6th Jan 2014.
Baird, G. et al. (2006) Prevalence of disorders of the autism spectrum in a
population cohort of children in South Thames: the Special Needs and
Autism Project (SNAP). The Lancet, 368 (9531), pp. 210-215.
Baron-Cohen, S (1997). Mind Blindness. USA: The MIT Press. p1.
Bartak, L, Cox, A & Rutter, M. (1975). A Comparative Study of Infantile
Autism and Specific Developmental Receptive Language Disorder. The
British Journal of Psychiatry. 126 (10), 127-145.
53

Basit, T (2010). Conducting Research in Educational Contexts. London:
Contiuum Books. p14.
Bell, I. (2011). Providing a Total Communication Approach. Available:
http://ianpbell.files.wordpress.com/2011/08/article-2.pdf. Last accessed
26th Apr 2014.
Bernier, R & Gerdts, J (2010). Autism Spectrum Disorders. California:
ABC-CLIO. p46-48
Blankenship, D (2010). Applied Research and Evaluation Methods. USA:
Human Kinetics. p86.
Boucher, J (2009). The Autistic Spectrum: Characteristics, Causes and
Practical Issues. London: SAGE Publications. p4.
Branson, J and Miller, D. (2002). Damned for their Difference. USA:
Gallaudet University Press. p215
British Educational Research Association. (2011). Ethical Guidelines for
Educational Research. Available: http://www.bera.ac.uk/. Last accessed
25th Jan 2014.
Bronfenbrenner, U (1979). The Ecology of Human Development::
experiments by nature and design. USA: Harvard College. p29.
Brookdale. (2011). What is Autism?. Available:
http://www.brookdalecare.co.uk/what-is-autism. Last accessed 8th Jan
2014.
54
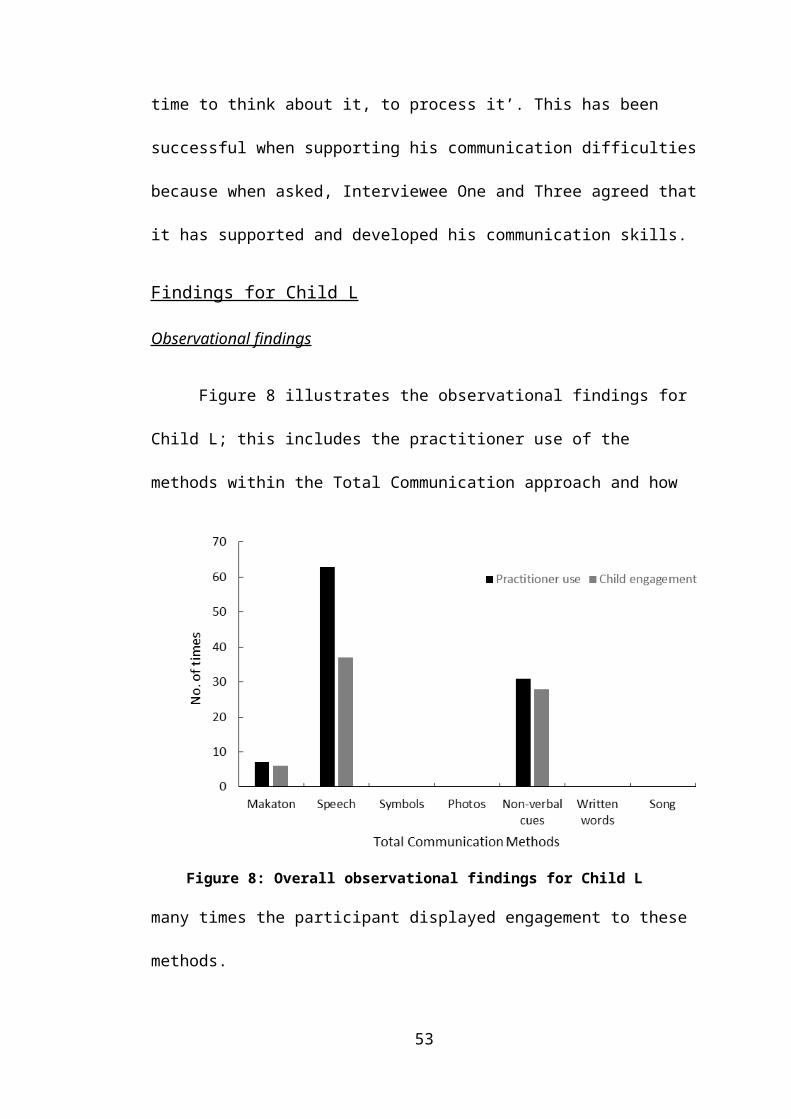
Brugha, T. et al (2009) Autism spectrum disorders in adults living in
households throughout England: report from the Adult Psychiatric
Morbidity Survey, 2007. Leeds: NHS Information Centre for Health and
Social Care. Available to download at
http://www.hscic.gov.uk/catalogue/PUB01131 [Accessed 10/05/2013]
Cameron, L. & Murphy, J. (2002). Enabling young people with a learning
disability to make choices at a time of transition. British Journal of
Learning Disabilities, 30, p105-112.
Carter, A.S, et. al. (2007, January). Sex differences in toddlers with
autism spectrum disorders. Journal of Autism and Developmental
Disorders, 37 (1): 86-97.
Clough, P and Nutbrown, C (2012). A Student's Guide to Methodology.
3rd ed. London: SAGE Publications. p41-54
Cohen, L. Manion, L and Morrison, K (2007). Research Methods in
Education. Oxon: Routledge. p133 - 397.
Davis, D. (2013). Autism Defined. Available:
http://calgaryautism.com/defined.htm. Last accessed 13th Jan 2014.
Dodd, S (2005). Understanding Autism. Australia: Elsevier Australia. p2-
20
Flick, U. Kardorff, E & Steinke, I. (2004). A Companion to Qualitative
Research. London: SAGE Publications. p178.
55

Fombonne, E. Young Shin, K. Leventhal, B. Laska, E. Lim, E. Cheon, K.
Kim, S. Kim, Y. Lee, H. Grinker, R & Song, D. . (2011). Prevalence of
Autism Spectrum Disorders in a Total Population Sample. The American
Journal of Psychiatry. 168 (9), p904-912.
Geers, A and Moog, S. (1992). Speech Perception and Production Skills
of Students With Impaired Hearing From Oral and Total Communication
Education Settings. Journal of Speech, Language, and Hearing
Research. 35, p1384.
Golafshani, N. (2003). Understanding Reliability and Validity in Qualitative
Research. The Qualitative Report. 8 (4), p600.
Guerrero, L and Floyd, K. (2006). Nonverbal Communication in Close
Relationships. New Jersey: Lawrence Erlbaum Associates. p4.
Hannan, A. (2007). Interviews in Education Research. Available:
http://www.edu.plymouth.ac.uk/resined/interviews/inthome.htm. Last
accessed 2nd Feb 2014.
Hawthorn, M. (2005). Dismantling the Barriers: Giving a Voice to Disabled
Young People in Care. Facing Forward: Residential child care in the 21st
century. p57-68
Hodkinson, P and Hodkinson, H. (2001). The Strengths and Limitations of
Case Study Research. Learning and Skills Development Agency. p2-9.
Hollander, E. Kolevzon, A. Coyle, T. (2011). Textbook of Autism
Spectrum Disorders. USA: American Psychiatric Publishers. p550.
56

Hudry K, Leadbitter K, Temple K, Slonims V, McConachie H, Aldred C,
Howlin P, Charman T. (2010). Preschoolers with autism show greater
impairment in receptive compared with expressive language abilities.
Centre for Research in Autism and Education. 45 (6), p681.
Hutchings, J. (2013). How Is Autism Treated?. Available:
http://www.autismspeaks.org/what-autism/treatment. Last accessed 7th
Jan 2014.
Jamison, J (2006). Research Methods in Psychology. Lincoln: iUniverse.
p27.
Kenny, T.. (2012). Autism Spectrum Disorders. Available:
http://www.patient.co.uk/health/autistic-spectrum-disorders. Last
accessed 26th Apr 2014.
Kjelgaard, M and Flusberg, H. (2001). An Investigation of Language
Impairment in Autism: Implications for Genetic Subgroups. National
Institutes of Health. 16 (2-3), p287
Kurtz, L (2008). Understanding Controversial Therapies for Children with
Autism, Attention Deficit Disorder & Other Learning Difficulties. London:
Jessica Kingsley Publishers. p108.
Kwanjai, M. (2013). Research Paradigms. Available:
http://khwanjaiphd.blogspot.co.uk/2013/08/research-paradigm.html. Last
accessed 30th Jan 2014.
57

Landa, R. (2007). Early communication development and intervention
with children with autism. Mental Retardation & Developmental
Disabilities Research Reviews, 13 (1): p16-25.
Loita, M. (2002). Autism and Communication. Available:
http://autism14.tripod.com/. Last accessed 9th Jan 2014.
Lubetsky, M. Handen, B and Mcgonigle, J. (2011). Autism Spectrum
Disorder. Oxford: Oxford University Press. p182.
Mackenzie, H (2008). Reaching and Teaching the Child with Autism
Spectrum Disorder. London: Jessica Kingley Publications. p19.
Marrs, I. (2013). How Autism Affects Speech, Language and Eating.
Available: http://www.speechlanguagefeeding.com/autism-affects-speech-
language-eating/. Last accessed 9th Jan 2014.
Matson, J & Minshawi, N (2006). Early Intervention for Autistic Spectrum
Disorders. Oxford: Elsevier Ltd. p83.
Matson, J (2011). Clinical Assessment and Intervention for Autism
Spectrum Disorders. Oxford: Academic Press. p168.
Mccallister, J (2010). A Needs Assessment of Autism. Florida: Boca
Raton. p23.
Mehrabian, A (2009). Non Verbal Communication. 3rd ed. USA:
Transaction Publishers. p1, 182.
58

Miller, C. (2006). Developmental Relationships between Language and
Theory of Mind. American Journal of Speech-Language Pathology. 15,
p146.
Mirenda, P. (2003). Toward Functional Augmentative and Alternative
Communication for Students With Autism: Manual Signs, Graphic
Symbols, and Voice Output Communication Aids. American Speech-
Language-Hearing Association. 34 (1), p204.
Mitchell, M and Jolley, J. (2007). Research Design Explained. 8th ed.
USA: Wadsworth Cengage Learning. p291, 302.
Moore, S (2002). Social Welfare Alive!. 3rd ed. Cheltenham: Nelson
Thornes Ltd. p402.
NAS. (2014). What is Autism?. Available: http://www.autism.org.uk/about-
autism/autism-and-asperger-syndrome-an-introduction/what-is-
autism.aspx. Last accessed 1st Jan 2014.
National Autism Association. (2013). Autism Fact Sheet. Available:
http://nationalautismassociation.org/resources/autism-fact-sheet/. Last
accessed 9th Jan 2014.
NDCCD - National Dissemination Centre for Children with Disabilities.
(1998). Pervasive Developmental Disorders (Fact Sheet 20 - FS20).
Washington, DC: Author.
Newby, P (2010). Research Methods for Education. Essex: Pearson
Education Limited. p115-370.
59
NHS Cambridgeshire. (2013). Total Communication. Available:
http://www.slc.cambridgeshire.nhs.uk/ActivitiesIdeasandInfo/SpecialScho
ol/TotalCommunication/tabid/1626/language/en-GB/Default.aspx. Last
accessed 11th Jan 2014.
NHS. (2012). Autism Spectrum Disorder. Available:
http://www.nhs.uk/conditions/autistic-spectrum-disorder/Pages/Introductio
n.aspx. Last accessed 8th Jan 2014.
Northern, J & Downs, M (2002). Hearing in Children. 5th ed. USA:
Lippincott Williams & Wilkins. p366.
Sanderson, H.. (2011). Total Communication: Person Centred Thinking,
Planning and Practice.. Care Services Improvement Partnership. p6
Steinberg, S (2007). An Introduction to Communication Studies. London:
Juta and Company Ltd. p39.
Stone, W. Ousley, O. Yoder, P. Hogan, K & Hepburn, S. (1997).
Nonverbal Communication in Two- and Three-Year-Old Children with
Autism. Journal of Autism and Developmental Disorders. 27 (6), p677-
696.
Strauss, A., & Corbin, J. (1990). Basics of qualitative research: Grounded
theory procedures and techniques. Newbury Park, CA: Sage Publications,
Inc. p17
Szarkowicz, D (2006). Observations and Reflections in Childhood.
Australia: Cengage Learning Australia. p22.
60

Tassoni, P (2003). Supporting Special Needs: Understanding Inclusion in
the Early Years. Oxford: Heinemann. p103.
Tavalari, D. (2004). Communication in children with Autism Spectrum
Disorders (ASDs): An inquiry, by means of a case study, into how a pre-
school specialist provision for children with ASDs interprets theoretical
models of. MA Education of Children and Young People with Autism.
p13.
TC. (2014). Total Communication Gloucestershire. Available:
http://www.totalcommunication.org.uk/. Last accessed 11th Jan 2014
The Hanen Centre. (2011). How Autism Affects Communication in Young
Children. Available: When does communication start? Communication
begins long before we learn to talk. In the first few months of life, babies
show their interest in communicating by listening intently to the sound of
them. Last accessed 9th Jan 2014.
The Makaton Charity. (2014). About Makaton. Available:
http://www.makaton.org/aboutMakaton/. Last accessed 19th Jan 2014
The Office of National Statistics (2005), The Office of National Statistics
recently reported a rate of autism of 1% in the population of school-age
children. Mental health of children and young people in Great Britain,
London: Palgrave Macmillan.
TheNAS. (2014). Communication and Interaction. Available:
Communication and interaction. Last accessed 9th Jan 2014.
61

Thompson, P. (2010). Validity and Reliability of Qualitative Research.
Available:www.mubs.ac.ug/procdocs/Moral%20Distress/validity_and_relia
bility.ppt. Last accessed 2nd Feb 2014.
Thompson, T (2007). Autism Spectrum Disorders: Definitions and
Implications. Minnesota: The College of Education and Human
Development. p2.
TNAS (The National Autistic Society). (2014). Statistics: how many
people have autism spectrum disorders?. Available:
http://www.autism.org.uk/about-autism/myths-facts-and-statistics/statistics
-how-many-people-have-autism-spectrum-disorders.aspx. Last accessed
1st Jan 2014.
TNAS. (2014). Is There A Cure?. Available:
http://www.autism.org.uk/about-autism/autism-and-asperger-syndrome-
an-introduction/what-are-the-causes-is-there-a-cure/is-there-a-cure.aspx.
Last accessed 7th Jan 2014.
University of Gloucestershire. (2008). Research Ethics: A Handbook of
Principles and Procedures . Available:
http://insight.glos.ac.uk/researchmainpage/researchoffice/Documents/
Research%20Ethics%20Handbook%20final%20Nov%2010.pdf. Last
accessed 25th Jan 2014.
University of Strathclyde. (2014). Advantages and disadvantages of
observation. Available:
http://www.strath.ac.uk/aer/materials/3datacollection/unit5/advantagesand
disadvantagesofobservation/. Last accessed 23rd Apr 2014.
62

Vernon, M. & Andrews, J. (1990). Psychology of deafness. New York, NY:
Longman. p12
Waldock, A. (2014). Total Communication. Available:
http://www.oxtc.co.uk/whatisTC.shtml. Last accessed 11th Jan 2014.
Wallace, M (2006). Action Research for Language Teachers. 10th ed.
Cambridge: Cambridge University Press. p161.
Webster, J. (2010). Neurotypical. Available:
http://specialed.about.com/od/glossary/g/neurotypical.htm. Last accessed
6th Jan 2014.
Whitman, T (2004). The Development of Autism. London: Jessica
Kingsley Publishers. p102.
Wimmer, R & Dominick, J (2013). Mass Media Research. London:
Cengage Learning. p117.
Yin, R. (2009) Case Study Research. 4th Ed. London. Sage. p18
63

Appendices
Contents of appendices:
Appendix One: Tracking sheet
Appendix Two: Participant profiles
Appendix Three: Semi-structured interview questions
Appendix Four: Informed consent; form for parents/guardians
Appendix Five: Informed consent; form for practitioners
Appendix Six: Example of written up observations
64
Appendix One: Research Proposal and tracking sheet
Section 1
Ideas for a title:
An exploration into the Total Communication Aproach when supporting the
communication difficulties in children with an Autism Spectrum Disorder: a
case study.
What do I want to find out?:
1. To explore how the Total Communication approach supports children
with communication difficulties on the Autistic Spectrum.
2. To explore how the Total Communication approach is adapted and
modified to support these children individually
Why am I interested in this?:
I have been working at an SEN Early Years placement since September.
This is a new setting to me, and one that I have found fascinating. I have
been put in a class with children who are Autistic, and have communication
difficulties. The teacher and Learning Support Workers (LSWs) use a variety
of methods of interaction with the children, such as Makaton, visual aids and
oral speech in combination, and these methods are stressed differently for
different children depending on their strengths and weaknesses. This
provoked me to research into this further, and I discovered that this approach
was named the Total Comunication Approach. This is something I wished to
explore in depth.
Key research words:
Total Communication Approach. Autistic Spectrum Disorder. Communication
difficulties. Case study. Interpretive paradigm. Observations. Interviews.
How will I gather data to help me answer my questions?:
65

I intend to use semi-structured interviews and observations as instruments
for my data collection. I will be interviewing practitioners, and observing four
children with autism.
What type of research would it be?:
It would be in the Interpretive paradigm. The reseach will be qualitative,
using empirical primary data.
What books, journals, websites have I found that might be useful?
TEACCH. (2013). Faciliatated Communication. Available:
http://www.autism.org.uk/living-with-autism/strategies-and-approaches/
alternative-and-augmentative-communication/facilitated-communication.aspx.
Last accessed 8th Nov 2013.
Lubetsky, M. Handen, B & Mcgonigle, J. (2011). Autism Spectrum Disorder.
Oxford: Oxford University Press.
Stewart, D. (1992). Initiating Reform in Total Communication Programs.The
Journal of Special Education. 26 (1), p68-84.
The Milestone School. (2012). SEN policy. Available:
http://www.themilestoneschool.ik.org/attachments/SEN_Policy_Nov_12.pdf.
Last accessed 8th Nov 2013
Gloucestershire County Council. (2013). Total Communication.Available:
http://www.totalcommunication.org.uk/. Last accessed 8th Nov 2013.
Haynes, W. Moran, M & Pindzola, R (2006). Communication Disorders in the
Classroom. 4th ed. London: Jones and Bartlett Publishers.
What ideas, models, approaches, theories, frameworks have I found that might be useful to help me understand my topic, or analyse my data?:
Data analysis - Qualitative Data Analysis (QDA) -
Taylor, C and Gibbs, G (2010) What is Qualitative Data Analysis? (QDA)',
Available: http://www. style="line-height:
66

1.231;">onlineqda.hud.ac.uk/Intro_QDA/what_is_qda.php. Last accessed
11th Nov 2013.
Theory and practice - Total Communication Approach
Communication Model:
Mehrabian, A (2009). Non Verbal Communication. 3rd ed. USA: Transaction
Publishers. p1, 182.
Proposed time scale of targets:
Plan and Literature Review (First draft) - End of January
Data Collection - Collected by February
Data Analysis - End of February
Findings and overview - End of March
Final draft by Easter
Confirmation of having read the University ethics guidelines at:
http://insight.glos.ac.uk/researchmainpage/researchoffice/pages/
researchethics.aspx
I have read the University ethics guidelines and agree to abide by them*
‘Signed’ Michelle Oak: Date:11th Nov 2013
Section 2 (completed by tutors)
Dissertation approval panel feedback (by 15/11/13):
Approval given: Yes - on supervisor's approval of your methodology
Name of supervisor: Richard
Comments: An interesting topic.
Signed: Paul Dated: 13/11/13
67
Appendix Two
Participant One: Child J
Child J is five years old, and is in his first year at the school. He is Polish, so
English is an additional language (EAL) for him. His formal diagnosis is
Autism, and he also has severe communication difficulties. He responds well
to visual structure, Makaton signing, photographs and symbols. His means of
communicating tends to be facial expressions, body movement and
vocalisations, with the knowledge of simple words from separate categories,
such as animals, colours and numbers.
Participant Two: Child J.M
Child J.M is six years old, and is in his first year at the school. He was
referred to the Communication and Interaction team at this school last year,
and subsequently was transferred last September from a mainstream primary
school. His formal diagnosis is Autism with ADHD, and presents problems
with expressive and receptive language delay, speech delay and additionally
social communication difficulties. His communication profile describes that he
uses speech to communicate effectively for most purposes, and that he has
strong likes and dislikes. His receptive abilities are not as strong as his
expressive abilities.
Participant three: Child L
Child L is six years old, and is in his second year at the school. He has the
formal diagnosis of Autism, and he also has severe communication
difficulties. His receptive abilities are stronger than his expressive abilities.
68

He uses language that includes key words and short phrases to convey his
needs, likes and dislikes. Additionally, he responds well to visual structure,
Makaton signing, photographs and symbols.
Participant four: Child N
Child N is six years old, and in his second year at the school. He has the
formal diagnosis of Autism; where he presents many severe communication
difficulties. He has difficulties with his non-verbal communication, as well as
his expressive communication abilities. His means of communicating tend to
be through using symbols, pictures, minimal language and non-verbal cues.
69
Appendix Three
Interview questions
‘I have asked you to participate in my study by being interviewed because
you work closely with the four participants within the study. I am going to ask
you a series of questions surrounding the four participants, and how the Total
Communication approach is used to support each of these participants
individually. All data collected from this interview will be kept confidential and
will only be used for my research study. You have the right to withdraw at any
time’.
These questions will be asked with the focus on a particular child.
Questions:
1. What is your understanding of the Total Communication approach?
2. Do you feel that the Total Communication approach is an effective
way to communicate [named participant]?
--If so, how? Which methods do you use?
3. Do you feel that using a range of methods communication, within the
Total Communication approach is beneficial when developing [named
participants] communication skills?
4. Has [named participant] always responded to the same methods, or
have some methods been faded/added?
70

Appendix Four: Parent Informed Consent Form
I am an undergraduate student at the University of
Gloucestershire, studying for a BA in Education Studies.
As part of my degree, I have to conduct a research project. I wish
to explore the Total Communication approach and how this helps
to develop the communication skills of children on the Autistic
Spectrum. I wonder whether you would be willing to let your child
participate by being observed. This means I will be taking
observations of your child in their school setting.
The title of my research project is; an exploration into the Total Communication approach when developing communication skills in children on the Autism Spectrum; a case study.
Any information gathered will remain anonymous and would only
be used for my research project. It would not be used for any
other purpose and it would be destroyed immediately afterwards.
You would be free to withdraw your child at any stage should you,
or your child, not wish to continue.
If you are happy for your child to able to assist me in my study I
would be most grateful and would be pleased if you could sign
below to indicate your consent.
With thanks
MICHELLE OAK
I would like my child to take part in this study.
71

Signed ……………………………………
Print ……………………………………
Date. ……………………………………….
72
Appendix Five: Staff Informed Consent Form
I am an undergraduate student at the University of
Gloucestershire, studying for a BA in Education Studies.
As part of my degree, I have to conduct a research project. I wish
to explore the Total Communication Approach and how this helps
to develop the communication skills of children on the Autistic
Spectrum and I wonder whether you would be willing to participate
by being interviewed.
The title of my research project is; an exploration into the Total Communication Approach when developing communication skills in children on the Autism Spectrum; a case study.
Any information gathered will remain anonymous and would only
be used for my research project. It would not be used for any
other purpose and it would be destroyed immediately afterwards.
You would be free to withdraw at any stage should you not wish to
continue.
If you are able to assist me in my study I would be most grateful
and would be pleased if you could sign below to indicate your
consent.
With thanks
MICHELLE OAK
I would like to take part in this study.
73
Signed ……………………………………
Print ……………………………………
Date. ……………………………………….
74
Appendix Six
Examples of some observations that have been written up
These examples have been selected completely at random.
Observation example one
Context: Child J was asked to join the practitioner in a one on one session.
This session involved playing animal bingo, where the child has to match the
number of ladybird spots corresponding to the number on the ‘number card’.
Firstly the practitioner used speech to gain attention from Child J. She asked
him three times to look at the ladybird which she was pointing at on the table.
Child J was not paying attention, so the practitioner lifted the symbol of the
ladybird to Child J’s eye level. Once she had gained his visual attention, the
picture was placed back onto the table, followed by an instruction to count
how many spots the ladybird had. He mildly responded to this vocal
instruction, by repeating the word ‘ladybird’ three times. The practitioner than
placed his fingers on the dots to count them, and cued him to start counting.
He then consecutively counted the spots individually. Child J was then
distracted by another child playing within the class, so the practitioner then
used the Makaton sign ‘listen’, to regain his attention. She used this sign
twice, before Child J responded verbally with ‘ladybird’. The practitioner than
asked Child J to point to which number resembled the amount of spots on the
ladybird, to which he pointed at with the practitioner using verbal expression
to aid him.
75

Observation example two
Context: All of the children are sat down around a long table to have morning
snack. The practitioner is sat facing them all, giving them the choice of
blackcurrant or milk, and apple or pears.
Child J.M was given the choice of apples or pears verbally and visually (the
practitioner pointed to each fruit whilst verbally expressing the name of the
fruit), to which he quietly and unclearly responded with pears. He was asked
to repeat his choice louder for the practitioner to hear to which he did.
Following this, the practitioner asked Child J.M if he would like some more.
He did not respond, so she asked him to look at her, to gain eye contact. He
went to grab more pears from the table, but the practitioner interrupted him
by signing and saying ‘wait’ at his eye level. She then gave him the pears,
after he said ‘please’ nicely.
76
Related Documents











